
Submitted:
31 March 2025
Posted:
31 March 2025
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Background: The COVID virus was recognized in January 2020 and it started almost immediately the most controversial epidemic of our history there the combination of a somatic disease and the weaknesses of human rationalism literally stopped the World and turned our life upside-down. Objective: Specifying and measuring the major errors in the interpretation and communicating epidemic data, that violated the rules of evidence based medicine and rational respect for the objective reality. Methods: 1. The maximal possible number of “true” COVID deaths were estimated from the frequency of viral test positivity in the tested general population. The difference between the reported and theoretical maximum of COVID deaths were the result of “hearsay” determinations of the UCOD (not supported by laboratory test) i.e. highly questionable. 2. The number of statistically expected “regular deaths” (from the Actuary tables) provided an estimate how many persons died “with” COVID infection but not “due to” of the virus disease. Only the excess deaths could have been the result of the virus contribution, with statistical certainty. All original data in this study were collected from publicly available, official databases and evaluated by using simple well known statistical methods. A “political score” was used to characterize the states on a continuous left (democrat) to right (republican) scale based on the political attitude of the citizens as determined and available from published opinion research. 1) COVID as the Underlying Cause of Death (UCOD) haven’t been verified by specific laboratory viral test in ca. 40.3% of reported causes. These, exclusively HEARSAY information based cases violated the WHO guidelines for reporting COVID related deaths.(Use of U07.1 code); 2) Large number of natural, age related, expected deaths have been reported as COVID related deaths even if the virus reasonably couldn’t play any causative role as UCOD. These PSEUDO COVID deaths were ca 46% of all reported COVID deaths. The oldest persons in this group were 85+ years old and comprised as much as 28% to all allegedly COVID fatalities (the GERONTO COVID deaths). These errors significantly inflated the number of COVID deaths and the related mortality statistic. Conclusions: The number of correctly identified COVID related deaths in our study is about 32% of the officially published number [171K instead of 533K, respectively]. The average FATALITY of COVID stays at ~0.54% and the MORTALITY 53/100K (On May 2021).
Keywords:
COVID
; Pandemic
; CDC
; USA
; Underlying cause of death
; UCOD
; Code U07.1
; Mortality
Summary
The enormous and persisting negative consequences of COVID epidemic demand the strictly scientific and critical review / revision of a series of medical-political decisions and procedures which determined an excessive and potentially self-destructing reaction to this “hidden enemy”.
Numerous flaws can be detected in collecting, analyzing and presenting the COVID epidemic data which intentionally or accidentally mislead the political leaders of this country, had been amplified by the media and now it is causing much more damage to the American people than the virus itself could ever cause.
We dismiss 60% of all allegedly COVID deaths because the Underlying Cause of Death (UCOD determination haven’t been supported by positive viral test for COVID and/or by negative viral test for common flu.
Additional 9% of all allegedly COVID deaths determinations can be the result of a simple logical error in counting.
Our recent and previous [1] reviews indicate the presence of very large amount of “hearsay” “information” in our recent - largely fear-driven - reaction and misunderstanding the nature and gravity of COVID epidemic.
Introduction
Six months passed since the entry of the allegedly ‘Chinese virus’ into our life and drastically inter-fe[a]res with our constitutionally protected “pursuit of happiness”. The impact of the COVID epidemic is significant and it will probably influence the presidential election in November 2020 and our life thereafter. Therefore it is urgently in our interest to correctly understand what is going on.
It was observed rather early that this virus epidemic had very unusual “modus operandi” that hadn’t been seen before and the reaction of the experts also turned out to be exceptional.
Previously [1] we described some signs of ignorance and/or bias in the presentation of COVID to the public by “experts”, media and politicians. This study is to analyze how this very expensive misinterpretation of a viral infection was/is possible; if it is the result of intentional political demagogy or just another sign of the human ignorance and psychological vulnerability.
Source of Statistical Data and Interpretation
The Center for Disease Control and Prevention (CDC) served as the main source of COVID related statistics, directly from its website [2] or indirectly from reliable reference websites, like Worldometer [3] The epidemic statistics is changing every day, therefore the concrete numbers in this article are certainly outdated, however the statistical contexts, patterns, detected rules are supposedly stable and reliable as we are in the 6th month of the pandemics.
Some important statistical data was not available (probably intentionally withheld by the source), like U07.1 and U07.2 rapports which were intended to distinguish between confirmed and suspected COVID deaths. In the absence of primary data it was necessary to rely on indirect data and try to calculate the missing information. This kind of approach is dependent on the correct interpretation of the meaning of the source information.
First of all, the “NEW DEATHS” and “TOTAL DEATHS” statistics is presented to the public as “Deaths with confirmed or presumed COVID-19”, coded to ICD–10 code U07.1”.
This is misleading, because ICD–10 code U07.1 is assigned to unmistakable identification of COVID-19 deaths confirmed by laboratory testing (viral test). The ICD-10 code of U07.2 should be used where laboratory confirmation is inconclusive or not available’ [4]. The correct classification of COVID deaths is absolute requirement of a correct (usable) statistics, mortality calculation [5].
In the absence of this vital data it was necessary to rely on calculation of the confirmed and supposed COVID deaths, using the equation:
[CT? & PNEU] = [CT+ & CT? & PNEU] - [CT+ & PNEU]
The (sum of ‘COVID test missing’ and ‘pneumonia’ deaths) [CT? & PNEU] is equal to the difference between the (sum of COVID test confirmed + COVID test missing + pneumonia deaths) [CT+ & CT? & PNEU] and the sum of (COVID test confirmed + pneumonia deaths) [ [CT+ & PNEU].
We found that the number of seasonal influenza (FLU-2) deaths is much larger than that publicly released by CDC (FLU-1). FLU-2 was calculated as the difference between two published groups of data, using the equation:
FLU-2 = [CT+ & CT? & PNEU & FLU] - [CT+ & CT? & PNEU]
Summary of terms, abbreviations, calculations and some main statistical data are available in Figure 1
DESCRIPTION AND ANALYZES
- Viral test positive (recent cases) and serology test positive (recovered, old cases) are pooled. Confusing infection and immunity and reporting it as “New Covid Cases” is a gross methodical error that is known, but not corrected, by the medical / epidemic experts (Center for Disease Control, CDC [6] and others). The magnitude of this error is not known.
The availability of antibody testing provided very “good news” to the public already in April [7], namely that surprisingly many persons (6-times more than recognized by viral test [8]) cached the COVID virus without any symptoms and developed immunity. It drastically reduced the mortality of the disease from ca 10% to ca. 0.7% (close to seasonal flu’s that is ~0.1%). This good news were not publicized by the mass-media because it was regarded to be premature to cool down the public’s worry for the infection.
- 2.
-
The confirmed (viral test positive) and the unconfirmed, but suspected or probable (?!) COVID deaths should be reported separately (coded U07.1 [9] and U07.2 [10] respectively). This WHO recommendation had been intentionally abandoned by CDC with the sole purpose to increase the number of COVID associated deaths. It is inappropriate of several reasons:
- a)
- The viral test positivity is an absolute requirement to the correct determination of a COVID death. Even this minimal diagnostic requirement seems to overestimate (!) the number of COVID deaths. The reason is that in average ~ 7-9% of all tested people are viral test positives, (mostly without becoming ill). With the same token ca. 7-9% of all terminally ill persons are expected to be viral test positives (similarly to the general population) even if the virus itself has nothing to do with their terminal condition. The number of expected, “normal”, “regular” non-Covid death were calculated to be: ca. 2.8M persons/year (2018 years statistic) that is 7.779 a day (SIC!). Nine percent of these persons – 700 / day - can be Covid positives (similarly to the general population). These persons automatically – and incorrectly – could be regarded as Covid victims.
- b)
- A major source of flaws in Covid statistics is the possibility to classify a death as Covid related even in the absence of positive viral test. These suspected (presumed or probable) virus deaths are in the doctor’s discretion, based on epidemiological data which means that doctors are strongly influenced by external circumstances, like media rapports, opinion of relatives. These kinds of evidence of the case of death in a hospital is analogue to the hearsay evidence on the courts: strongly questionable.
The magnitude of this “hearsay” medical determinations is not known, because certain and probable causes are not reported separately. An estimate from NYC [11] suggests that 26% of Covid related deaths were not confirmed by laboratory tests (i.e. may or may not be true causes of deaths).
[In Italy the frequency of “hearsay” COD determinations were found to be 88% i.e. only 12% of COVID deaths were confirmed by viral tests.]
[During March 11–May 2, 2020, a total of 32,107 deaths were reported to DOHMH; of these deaths, 24,172 (95% confidence interval = 22,980–25,364) were found to be in excess of the seasonal expected baseline. Included in the 24,172 deaths were 13,831 (57%) laboratory-confirmed COVID-19–associated deaths and 5,048 (21%) probable COVID-19–associated deaths, leaving 5,293 (22%) excess deaths that were not identified as either laboratory-confirmed or probable COVID-19–associated deaths, on July 1st, 2020.
- c)
- During the past 123 days of epidemic with reported deaths in USA 128.024 persons are suspected to be the victims of the virus that is in average 1041 deaths/day (on July 1st, 2020). We can assume, say, that 71% (739) were test confirmed cases (as reported in NYC). 700 of these were accidentally positive cases, meaning the Covid positivity and death coincides without any obvious causality.
- d)
- The statistical conclusion of these arguments above may be, that 39 persons died in average a day caused by the Covid disease (and not anything else) i.e. 4797 total (and not 128K as it is suggested to us by the media. With other words, the epidemic in USA is grossly overestimated by a factor of ca. 26.6 x!). (A more realistic calculation is below).
- 3
- The presentation of ACTIVE CASES in United State – “Active cases” or “Number of Infected People” and related remarks are misleading.
For ex. July 05 – Currently Infected: 1 560 795 – tells the reader that a huge number of persons are ill and the risk to be infected is large. In reality only the virus test positive cases of the last 30 days have any medical significance, the rest became ‘as healthy and as old’ as they were before catching the virus.
- It takes time to develop the first symptoms (even viral test positivity). The estimate is (with generous marginal) 14 days. (Quarantine period: 14 days).
- A Covid sick person is in average regarded to be contagious ca 7-14 days after the first symptoms. The virus level drops after 10-11 days and the hospitalized persons can be released.
- Following ca. 7 fever-free days the Covid-sick person is usually no longer infectious.
- A rough estimate gives about 30 days (with marginal) when an infected person may be contagious for others.
The number of “active cases” or the number of “infected people” (meaning: Covid viral test positives) in the USA, today (2020.07.18) is around 1.3M of 18M tested persons (or ca 7.1% of US population). 21,136 persons died under the same 30d period, that is, the mortality rate is ~ 1.6% today.
The calculation of active cases suggests that ~57 of viral test positive cases are probably no longer carries the virus, but theoretically, 43% still can infect others. However the example illustrates at the same time that it can be very misleading. The number of active cases depends on the number of total tests during the last 30 days. Consequently it can be unrealistically high in countries, like USA, there the number of tests increased during the last weeks. It explains even the extreme variation between countries in this respect. ……See Figure 2
- 4.
-
Ca. 70% OF COVID DEATHS DETERMINATIONS ARE BASED ON “HEARSAY” [12] - COVID INFECTION AS THE CASE OF DEATH IS BASED ON “HEARSAY” AND ONLY 30 % ON POSITIVE VIRAL TEST.
- a)
-
There is only one publication that may serve a clue about the magnitude of hearsay-based (probable, suspected but not confirmed by viral test) Covid deaths from New York in April suggesting 22% “hearsay” diagnoses and 57% test based cases of deaths. Otherwise this ratio is a well-kept secret.[Hearsay: information received from other people that one cannot adequately substantiate; rumor. Hearsay evidence in a legal forum to prove the truth is usually inadmissible in most of the courts].
- b)
- We estimate the ratio of hearsay vs. test-based Covid-death diagnoses to be as much as 61:39% in average (calculated as the difference between “Deaths involving Pneumonia, with or without COVID-19, excluding Influenza deaths“ and “Deaths involving COVID-19 and Pneumonia, excluding Influenza” from the CDC reports [13].
- c)
Figure 3.
WEEKLY COVID-RELATED DEATHS IN USA. The COVID related deaths in USA during the first 5 months of the epidemics are plotted in six groups, as it had been published by CDC or calculated. These groups are comprised of subgroups depending on the COD and the main contributing condition, there *COVID viral test positive, confirmed (CT+); *COVID viral test missing, suspected (CT?); *pneumonia (PNE); *influenza, non-COVID (FLU) deaths are separated. See even Figure 1.
Figure 3.
WEEKLY COVID-RELATED DEATHS IN USA. The COVID related deaths in USA during the first 5 months of the epidemics are plotted in six groups, as it had been published by CDC or calculated. These groups are comprised of subgroups depending on the COD and the main contributing condition, there *COVID viral test positive, confirmed (CT+); *COVID viral test missing, suspected (CT?); *pneumonia (PNE); *influenza, non-COVID (FLU) deaths are separated. See even Figure 1.
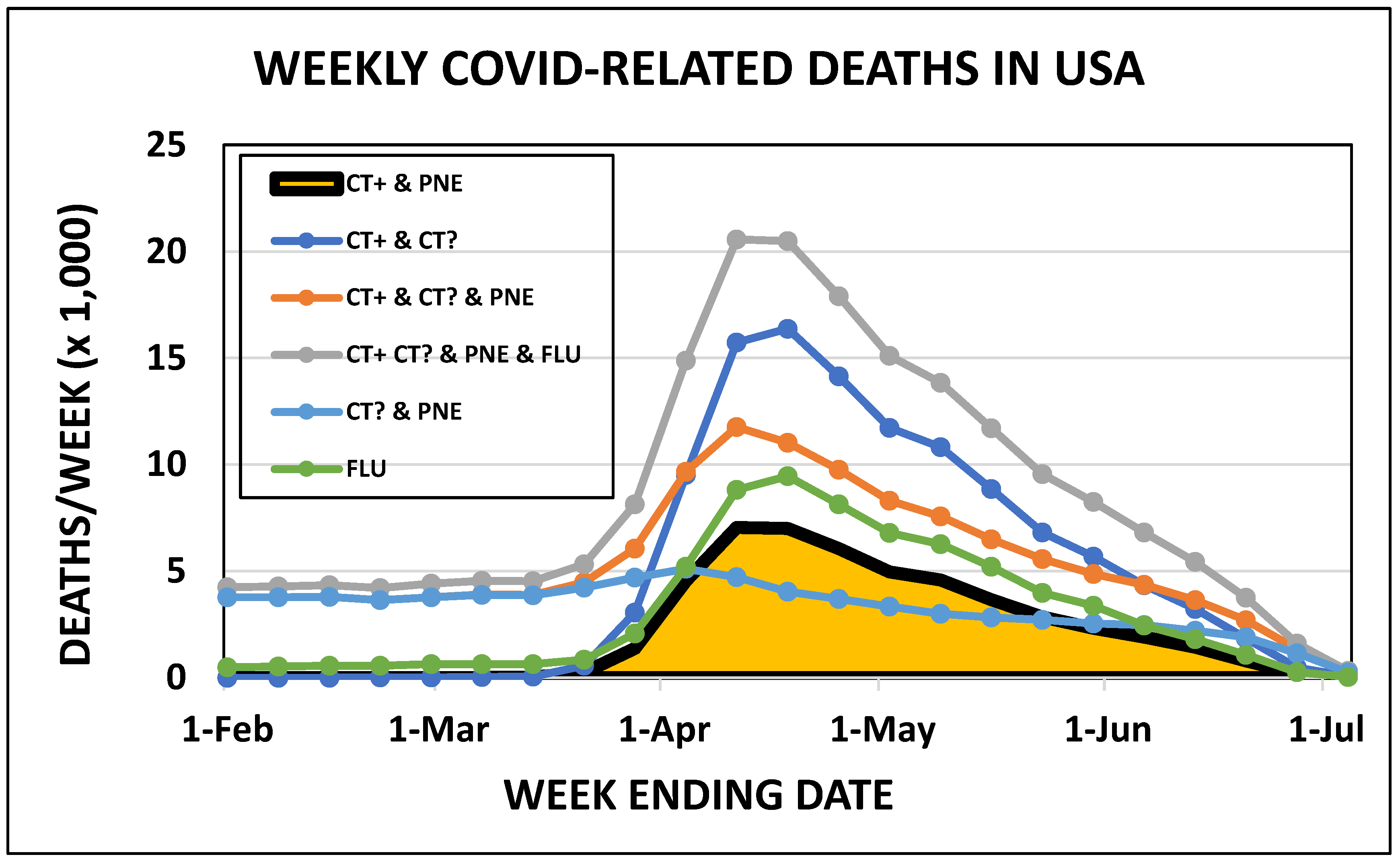
Figure 4.
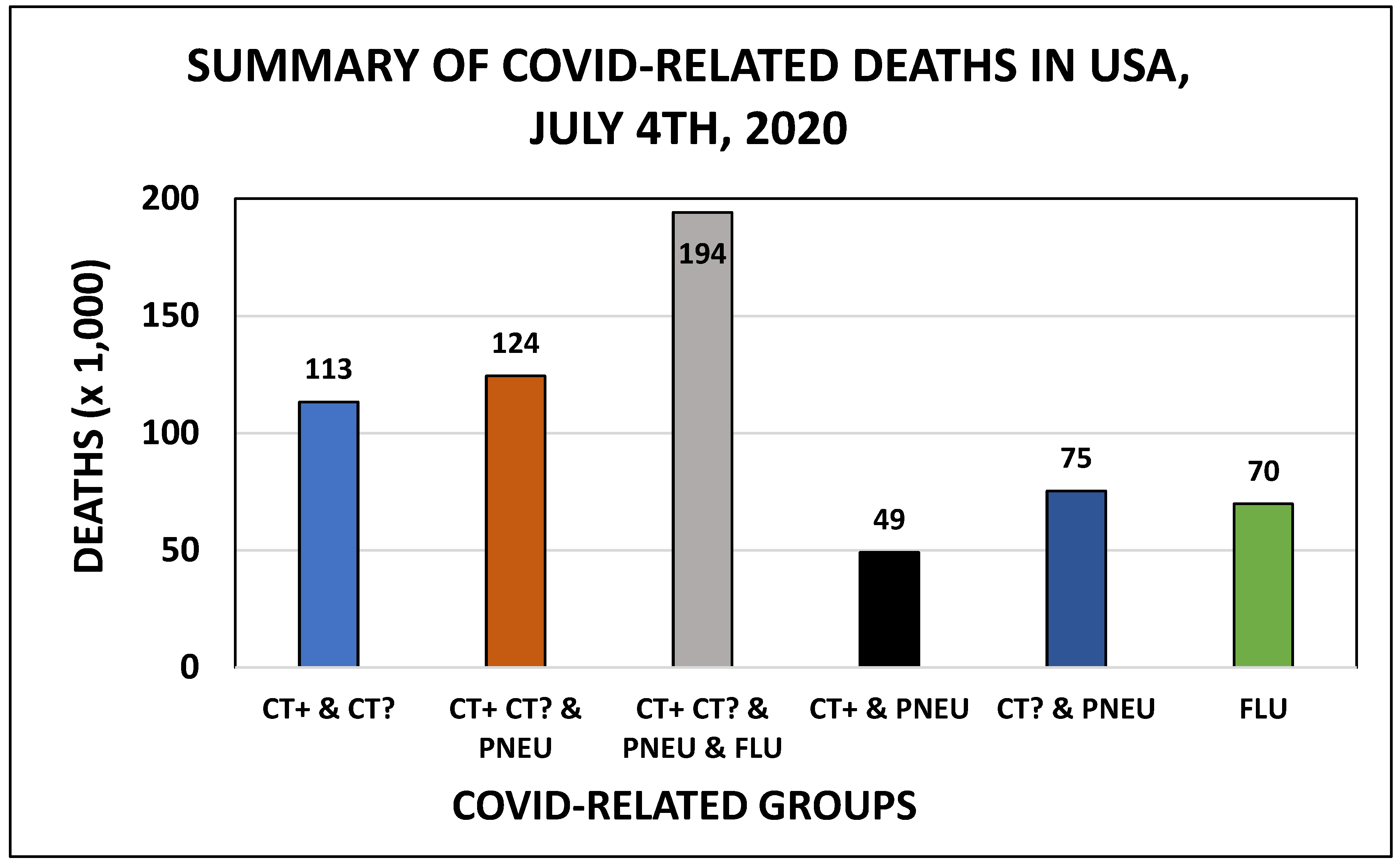
SUMMARY OF COVID-RELATED DEATHS IN USA during the first five months of the epidemics. See legend to Figure 1 and Figure 3 for details.
- 5.
- EXTRA DEATHS UNRELATED TO COVID INFECTION ITSELF.
It is well recognized, that being COVID viral test positive doesn’t mean, that the carrier is sick. Vast majority of all virus-positive persons, especially young persons without preexisting condition, not even notice any infection. Consequently it is logically not reasonable to suppose, that all persons who dies as COVID positives are killed by the COVID. It is more logical to suppose, that a fraction of terminal and COVID positive persons dies due to age and chronic disease that is completely independent of the virus. The tested / positive cases ratio may help to estimate the magnitude of this “accidental” statistical error in counting the COVID deaths. Figure 5
The assumption that all COVID positive persons who dies are killed by COVID disease has no scientific ground: it is also a “hearsay” argument.
- 6.
- SIGNS OF “POLITICAL BIAS”
The statistical difference between democrat- vs. republican dominated states could be detected even after dissecting of the group of poorly defined pool of ‘ALL COVID DEATHS’ which is contaminated with the “hearsay” COD determinations (CT?) and the absence of pneumonia (PNE). Surprisingly the mathematical difference between [CT+ & CT? & PNE & FLU] and [CT+ & CT? & PNE] - both present in the CDC tables - defined a distinct group (FLU-2) of deceased persons there the “regular”, “seasonal” (non-COVID) influenza had been detected and reported. Figure 6
This FLU group is large, larger than the group of confirmed COVID deaths and is practically concealed in the official, published and media-reported comments on the epidemics. The officially reported influenza cases (FLU-1) is much smaller than our suggested (calculated) number.
- 7.
- Influenza (the regular seasonal flu) epidemic have been observed simultaneously with the COVID epidemic and contributed to the deaths but its significance was largely ignored and withheld from the public.
We could find 79.612 deaths there FLU was recorded as pre-existing condition to COVID deaths. This is confusing information, because the traditional medical experience is that one viral infection protects against another. The coexistence of 2 different viral infections is not new in the medical literature but it is regarded to be a rarity [14,15]. Consequently we may be skeptical regarding the possibility of two different viral epidemics at the same time (called syndemic) or is it possible that we already have one?
Recognition of the possibility of co-infection suggests that a) COVID death as COD is questionable even in the presence of positive viral test for COVID but without negative viral test for flu viruses; b) COVID death diagnosis is not possible in the absence of positive COVID viral test. Wisely the FDA authorized the use of COVID-19 Combination Diagnostic Test Ahead of (next) Flu Season [16]
- 8.
- DOCTOR’S OBJECTIVITY IS COMPROMISED BY THE MEDIA AND THE PROFIT INTEREST OF THEIR EMPLOYERS.
THE PRESSURE ON DOCTORS TO PROVIDE “HEARSAY” DETERMINATION OF ‘COD’ (WITHOUT VIRAL TEST) FORCES THEM IN A PROFESSIONAL CONFLICT AND WEAKENS THEIR PROFESSIONAL OBJECTIVITY.
It is well recognized by the courts that members of a jury are vulnerable to the media attention around their case. Therefore they are carefully instructed not to access external information from media, internet, not to discuss the case with anybody, not even with each other. In high profile cases the jury members are even accommodated in hotels during the trial to guaranty their isolation from external opinion.
Doctors are in similar situation now when they are expected to distinguish between two very similar diseases, - seasonal or “regular” flu and COVID - even without specific viral test(s). In case of death the role of underlying conditions will further increase the difficulties to determine the role of COVID (also without viral test). In these discretionary decisions the influence of environment might be decisive. The doctor will determine the COD: COVID. Why not, when everybody is speaking about it?
An even more serious problem is the retaliation if a doctor is not bending for the wind. 1) Doctors Dan Erickson and Artin Massihi (Bakersfield, CA) were banned from YouTube for publishing evidence against the necessity of government restrictions against a “flu” called COVID; 2) Minnesota senator and practicing Doctor Scott M. Jensen was reported to the State Medical Board because somebody didn’t like his request for viral test when determining COVID as COD and 3) Simone Gold MD., JD with the America’s Frontline Doctors were censored for speaking about the side effects of COVID restrictions.
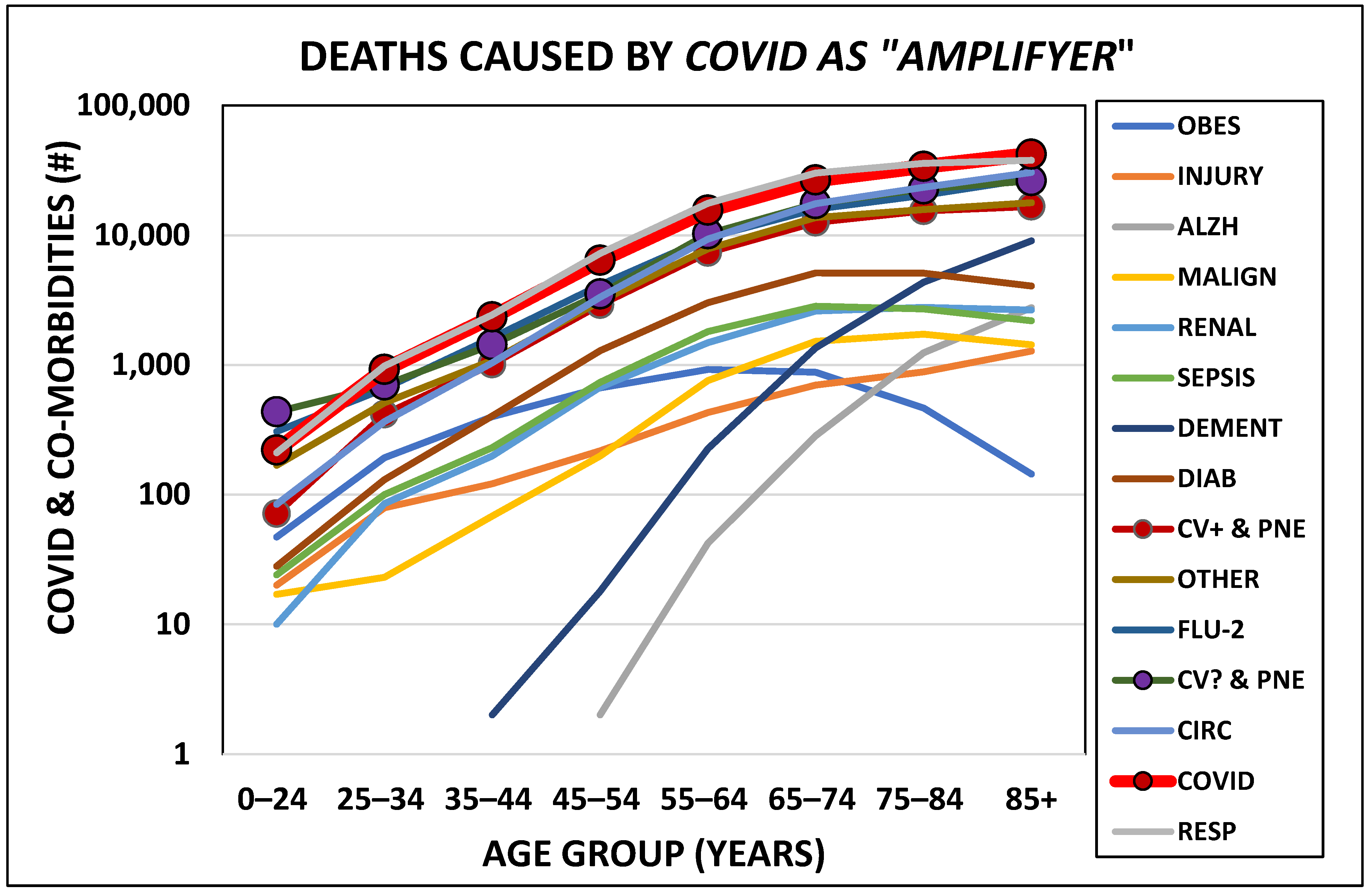
Comparison of the age normalized morbidity of different diseases suggests that COVID is rather similar to other diseases but amplifies their effects. There is no dramatic difference between the morbidity of different illnesses. Figure 7. The widely known suggestion, that COVID targets primarily elderly, is not as obvious as the selective effect of Alzheimer.
We can suppose that many doctors BECAME SLAVES OF THE MEDIA AND HOSPITAL MANAGEMENT in their attitude to the COVID infection, disease and mortality.
We are experiencing an epidemic of fear there we are blaming COVID for our own weaknesses, all kinds of diseases and even the biological limitations of our life (mortality). We can ironically call it “the COVIDISATION” of regular deaths.
- 9.
- THE DIAGNOSTIC “TRINITY” OF “COVID DEATH”: A. VIRAL TEST, B. X-RAY, C. FLU.
A “close to death” person usually presents a complex clinical picture to the physician. To recognize the flu is usually not difficult in most of the cases but can be challenging when the patient is old with preexisting conditions. There are three cardinal clinical/laboratory signs of a COVID disease:
- A)
- Positive viral test for COVID. To distinguish seasonal flu (bagatelle) from Covid disease (serious) is simply not possible without viral test. Stating that somebody has COVID disease, because a “neighbor recently tested positive for COVID” is “hearsay” statement and not serious medical opinion.
- B)
- Chest X-ray confirmed pneumonia. The COVID infection itself is not equal to the COVID disease without some effect on the lungs and its function. Therefore the association of viral-test positivity with objectively determined (X-ray) pneumonia confirms the COVID disease. Pneumonia itself, without viral test positivity is not sufficient to the correct diagnoses. Pneumonia is a very common cause of death of hospitalized patients with restricted mobility.
- C)
- The symptoms of COVID are identical to the symptoms of seasonal flu. Therefore a negative flu viral test may be necessary to confirm suspected COVID infection and death.
Discussion
The clinical symptoms of seasonal flu and COVID disease are identical, the difference – if any – is statistical: like *time to develop symptoms (incubation period), *time while remaining contagious, *speed of spreading, *possible complications [17]. Most of the major epidemic diseases have some highly specific and well detectable sign that promptly distinguish them from any other diseases (for ex. characteristic skin rash). There is not a single symptom or sign that is unique for COVID consequently the basic physical examination is not decisive, especially not when preexisting conditions interfere with the clinical appearance of the disease. The only way to diagnose COVID disease (and COVID death) is the positive viral test. Specific changes on the lung X-ray helps with the diagnosis, but never replaces the specific laboratory confirmation.
Specific viral test for COVID was not available at the beginning of the epidemic and the diagnosis – incl. the determination of COD due to COVID - was based on “qualified guesswork” of the doctors. We know well that this kind of diagnoses is subjective and often erroneous and should be abandoned as soon as laboratory tests becomes widely available. It was very important to distinguish between reliable ‘test-based’ and un-reliable ‘test-less’ diagnoses especially when the entire society introduced serious restrains on the citizens as protection against an allegedly very dangerous disease, that “could predictably kill millions”. Therefore it was recommended to rapport test-based (confirmed) and test-less (presumed, suspected) deaths separately (ICD-10 code U07.1 and U07.2, respectively). However CDC abandoned this request for “separation of gold from sand” and pooled all possible and impossible COVID deaths under U07.1 rules and legitimized (“confirmed”) “hearsay” based diagnoses.
(This decision was motivated – as explained to the public - by the lack of distinction between confirmed and suspected COVID deaths in other countries. Consequently CDC lowered the American diagnostic standard to secure uniformity in reporting).
The tremendous influence of doctors’ subjective, discretionary diagnoses on the COVID statistics had been observed in Italy already in March 2020. “On re-evaluation by the National Institute of Health, only 12 per cent of death certificates have shown a direct causality from coronavirus…” [18]. It was concluded, that “The way in which we (Italian doctors) code deaths in our country (Italy) is very generous in the sense that all the people who die in hospitals with the coronavirus are deemed to be dying of the coronavirus”.
Today, - after months of being “gaged” by mandatory mask-wearing and living in house arrest in solitary confinement (called social distancing) – we learned, that a) the median age of persons who died as “COVID victims” was 78 years compared to the current life expectancy for U.S. in 2020 that is (was?) 78.93 years; b) 50% of them lived in nursing homes; 99.96% were adults; c) 59% (75,823) lived over (SIC!) the current life expectancy; d) 15% (19,290) were documentedly dement (Alzheimer and vascular [19]).
Majority of the COVID positive persons didn’t notice any illness, however some – even young and perfectly healthy persons - experience flu-like symptoms followed by complete recovery. However it is unclear if COVID itself can be responsible for the death of any healthy person, young or old. An early estimate (April 2020) suggested that less than 2% of deaths occurred without any known underlying health condition. [20,21,22].
Given the massive effect of aging and underlying conditions it is difficult to estimate the biological impact of COVID epidemic and evaluate the adequacy of society’s protective response. The number of Excess Deaths (recently +7%) includes significant number of non-COVID excesses that is caused by social stress of the epidemic and not the COVID itself.
Conclusions
The recent and previous [1] reviews convinced us that the presentation of COVID related information (to the public, media, politicians) should be significantly improved and corrected for obvious flaws. An honest correction by removing the unconfirmed (no viral test) “hearsay-based” cases of deaths (60%) and the accidental, irrelevant test positive cases (7-9%) will reduce the COVID deaths by ca 63% (from 150,444 to 51,136 lethality’s today 2020.07.27). It is also necessary to split the New Cases rubric into viral test vs. antibody test determined subgroups. The frighteningly large group of Active Cases should be corrected and limited to the sum of the last 30 days New Cases (i.e. those who may be contagious for other). It is absolutely necessary to inform the public about the magnitude of the “regular” (non-COVID related) deaths (that is >7,000 a day) and remind everybody the existence of “natural” death that is a non-negotiable condition of living, even without COVID.
Addendum
IS THE COVID EPIDEMIC THREAT OR BLESSING? – ETHICAL CONSIDERATIONS.
Death is a central issue of life, consequently of every philosophical, ethical concepts. Protecting life (generally) and the survival of our relatives (particularly) is a deep-rooted demand often formulated as fundamental laws and religious obligation. However protecting or saving all kinds of life or human life is not realistic. The life of every person has an individual value determined by the assumed value of all other life in the reference population.
Medical doctors are professionally trained and ethically obliged to protect and save all form of human life without ever setting a monetary value on any individual life. Even if most doctors knows from their own experience that “not everyone is created equal”, you will never hear it publicly from any doctor. It is taboo, protected by political correctness (whatever that can mean). However speaking about quality of life - and not only years spent alive - is more accepted and it is the source of endless discussions.
There is a rule in the medical “business” that is similar but opposite to the Moore’s law in computer business. Moore’s Law means ever-more powerful personal computers for less and less money. The law of aging means that a senior gets less and less health for ever more medical procedures and costs. The value (quality) of life is progressively decreasing for the senior patients, but exponentially increases for the medical service providers. In extreme circumstances death can be a release for the very old and very sick persons, but at the same time a huge loss of income for the medical & pharmaceutical business.
I think it is reasonable to consider that, say, force-feeding and force medicating an 80+ years senile dement lady for several weeks - and discharging her with a million $ bill for a natural death only some weeks later - is not respect for the life, but arrogance and disrespect for the human values. She can die, as anybody else, but not in Covid and not under the watch of a doctor. Nobody was permitted to die in COVID in the federally financed COVID care in America.
Declaration of Conflict of Interest
The author of this article has no monetary or scientific interest in writing this rapport.
However he honestly discloses, that he is under oath to follow the ethical rules of his profession (medicine) and he is obliged by his oath of allegiance to work for the USA and protect the Constitution. It might be interpreted by some persons as bias or prejudice.
Checklist of Serious Flows in Collecting & Presenting Covid Statistics and Related Information in USA, August 2020
- A.
-
DATA COLLECTION & MANAGEMENT ERRORS
- 1.
- INFLATING COVID DEATHS NUMBER BY POOLING CONFIRMED (VIRAL TEST BASED) AND SUSPECTED (VIRAL TEST MISSING, “HEARSAY” ONLY) CAUSES.
- 2.
- IGNORING THE “HARMLESS” COVID POSITIVITY OF A PORTION OF DYING PERSONS.
- 3.
- CONFUSING “VIRAL TEST” AND “ANTIBODY TEST” POSITIVE CAUSES AND POOLING IN A SINGLE “NEW CAUSE” GROUP.
- 4.
- POOR DISTINCTION BETWEEN “RECOVERED” (NATURALLY IMMUNIZED) AND STILL “ACTUAL” (CONTAGIOUS) COVID POSITIVE GROUPS AND OVERESTIMATING THE LATER.
- 5.
- WITHHOLDING THE RESULT OF “ANTIBODY TESTS”, I. E. THE EXPECTED NUMBER OF ALREADY IMMUNE PERSONS.
- 6.
- IGNORING / UNDER-ESTIMATING THE DEATHS DUE TO “REGULAR FLU”.
- 7.
- B.
-
INFORMATION MANAGEMENT & SHARING ERRORS
- 8.
- UNCRITICALLY ACCEPTING AND MEDIA-AMPLIFYING THE “BAD NEWS” – FOREIGN AND/OR DOMESTIC (BLOWING UP) – AND AT THE SAME TIME WITHHOLDING THE “POSITIVE NEWS”.
- 9.
- SUPPRESSING / CENSORING / RETALIATING ANY OPPOSITION CRITICAL TO THE MAGNITUDE AND SIDE EFFECTS OF THE CATASTROPHIC ACTIONS AGAINST A RELATIVELY MILD EPIDEMICS.
- 10.
- SYSTEMATICALLY CONFUSING FEAR & FACTS.
- 11.
- POLITICIZING A NATURE-MADE (BIOLOGICAL) DANGER AFFECTING (ORIGINALLY) ONLY A TINY FRACTION OF THE POPULATION AND CREATING A GENERAL PROBLEM WITH NEGATIVE EFFECTS ON THE ENTIRE SOCIETY.
- 12.
- DIVIDING THE ENTIRE SOCIETY THAT IS THE WORST POSSIBLE ACTION WHEN A SOCIETY FACES A GENERAL THREAT.
- 13.
-
NATIONWIDE CATASTROPHES HISTORICALLY UNITE THE NATIONIN DEFENSE. THE RECENT ABSENCE OF THIS UNITY IS – IN OUR MIND - A VERY STRONG AND OBVIOUS SING OF THE “MAN-MADE”, “ARTIFICIAL” NATURE OF THE RECENT COVID SITUATION IN USA.
- 14.
- IGNORING THE “BIG PICTURE” OF MORTALITY SITUATION IN USA, I.E. THE WELL ESTABLISHED FACT, THAT WASTE MAJORITY OF COVID DEATHS ARE “COVID-ASSISTED” BUT ALMOST NEVER ONLY (EXCLUSIVELY) “COVID-CAUSED”.
- 15.
- MISUSING AN ALREADY BAD AND DANGEROUS SITUATION FOR PETTI PERSONAL PURPOSES, LIKE EXERCISING POWER, BUILDING PROFESSIONAL (?) LEGACY (?, “SAVING THE PEOPLE FROM DEATHS” (?) , OCCASION FOR BEING SEEN AND HEARD, EXTRA PROFIT OPPORTUNITY, …
- 16.
- GENERATING (LEGAL AND ILLEGAL) PROTESTS, RIOTS.
- 17.
- MISUSING THE SITUATION FOR DESTROYING THE TRADITIONAL HUMAN VALUES AND INSTITUTIONS, LIKE SCHOOLS (EDUCATION) AND POLICE (LAW AND ORDER).
- 18.
- MISUSING THE SITUATION FOR DESTROYING THE TRADITIONAL HUMAN DEFENSE LINES AGAINST FATE AND CHAOS, LIKE RELIGION (CLOSING CHURCHES), POLICE (DEFUNDING), EDUCATION (CLOSING SCHOOLS).
- 19.
- PREPARING FOR A KIND OF “SOCIAL REVOLUTION” (POLITICAL COUP?) PROBABLY ERUPTING AROUND AND ASSOCIATED TO THE ELECTION IN NOVEMBER.
(A historical association is the Bolshevik revolution, dated November 7, 1917.
Ironically this prophecy turned out to be valid and the election on November 2nd, 2001 resulted in a historical turnaround in the American life).
References
- BIRO JC: THE “POLITI-COVID (USA)” EPIDEMIC IN THE “PRE-ELECTION” AMERICA, 2020 – 2020.06.02.
- Available online: https://www.cdc.
- Available online: https://www.worldometers.info/coronavirus/.
- Emergency use ICD codes for COVID-19 disease outbreak. Available online: https://www.who.int/classifications/icd/covid19/en/.
- INTERNATIONAL GUIDELINES FOR CERTIFICATION AND CLASSIFICATION (CODING) OF COVID-19 AS CAUSE OF DEATH Based on ICD International Statistical Classification of Diseases (16 April 2020). Available online: https://www.who.int/classifications/icd/Guidelines_Cause_of_Death_COVID-19.pdf?ua=1.
- CDC: Center for Disease Control.
- New York State study, published April 23.
- Available online: https://hartfordhealthcare.org/about-us/news-press/news-detail?articleid=26868&publicId=395.
- An emergency ICD-10 code of ‘U07.1 COVID-19, virus identified’ is assigned to a disease diagnosis of COVID-19 confirmed by laboratory testing. Available online: https://www.who.int/classifications/icd/covid19/en/.
- An emergency ICD-10 code of ‘U07.2 COVID-19, virus not identified’ is assigned to a clinical or epidemiological diagnosis of COVID-19 where laboratory confirmation is inconclusive or not available. Available online: https://www.who.int/classifications/icd/covid19/en/.
- Preliminary Estimate of Excess Mortality during the COVID-19 Outbreak — New York City, March 11–May 2, 2020. MMWR Morb Mortal Wkly Rep 2020, 69, 603–605. [CrossRef]
- Definitions from Oxford Languages. Available online: https://languages.oup.com/google-dictionary-en/.
- Available online: https://www.cdc.gov/nchs/nvss/vsrr/covid19/index.htm (accessed on 6 July 2020).
- Wu X, Cai Y, Huang X, et al. Co-infection with SARS-CoV-2 and Influenza A Virus in Patient with Pneumonia, China. Emerging Infectious Diseases 2020, 26, 1324–1326. [CrossRef] [PubMed]
- Konala VM, Adapa S, Gayam V, et al. Co-infection with Influenza A and COVID-19. Eur J Case Rep Intern Med. 2020, 7, 001656. [CrossRef]
- FDA – JULY 22ND, 2020. Available online: https://www.fda.gov/news-events/press-announcements/coronavirus- covid-19-update-fda-authorizes-additional-covid-19-combination-diagnostic-test-ahead-flu.
- Similarities and Differences between Flu and COVID-19. CDS Publication. 2020.07.10. Available online: https://www.cdc.gov/flu/symptoms/flu-vs-covid19.htm.
- Sarah Newey: Why have so many coronavirus patients died in Italy? – The Telegraph - 23 March 2020.
- G30, F01, F03. Available online: https://www.cdc.gov/nchs/nvss/vsrr/covid_weekly/index.htm#Comorbidities (accessed on 22 July 2020).
- New York State Department of Health. COVID-19 Tracker. Available online: https://covid19tracker.health.ny.gov/views/NYS-COVID19- Tracker/NYSDOHCOVID-19TrackerFatalities?%3Aembed=yes&%3Atoolbar=no&%3Atabs=n.
- NEWS Boston, April 28th, 2020. Available online: https://whdh.com/news/nearly-every-mass-coronavirus-death-was- patient-with-underlying-medical-condition-data-shows/.
- FIT Consulting. Available online: https://www.fticonsulting.com/~/media/Files/us- files/insights/articles/2020/may/prevalence-underlying-health-conditions-among-covid-19- deaths.pdf.
- Woolf SH, Chapman DA, Sabo RT, Weinberger DM, Hill L. Excess Deaths From COVID-19 and Other Causes, March-April 2020. JAMA. Published online July 01, 2020. [CrossRef]
- 35% of excess deaths from pandemic not caused by COVID-19 – Medical News Today, - July 6, 2020. Dated and signed: San Diego, 2020.08.04. Available online: https://www.medicalnewstoday.com/articles/35-percent-of-excess-deaths-from-pandemic-not-caused-by-covid-19.
Figure 1.
1Deaths with confirmed or presumed COVID-19, coded to ICD–10 code U07.1 An emergency ICD-10 code of ‘U07.1 COVID-19, virus identified’ is assigned to a disease diagnosis of COVID-19 confirmed by laboratory testing. An emergency ICD-10 code of ‘U07.2 COVID-19, virus not identified’ is assigned to a clinical or epidemiological diagnosis of COVID-19 where laboratory confirmation is inconclusive or not available. 2Percent of expected deaths is the number of deaths for all causes for this week in 2020 compared to the average number across the same week in 2017–2019. Previous analyses of 2015–2016 provisional data completeness have found that completeness is lower in the first few weeks following the date of death (<25%), and then increases over time such that data are generally at least 75% complete within 8 weeks of when the death occurred (8). 3Counts of deaths involving pneumonia include pneumonia deaths that also involve COVID-19 and exclude pneumonia deaths involving influenza. 4Counts of deaths involving influenza include deaths with pneumonia or COVID-19 also listed as a cause of death. 5Deaths with confirmed or presumed COVID-19, pneumonia, or influenza, coded to ICD–10 codes U07.1 or J09–J18.9. Influenza and pneumonia J09-J18.
Figure 1.
1Deaths with confirmed or presumed COVID-19, coded to ICD–10 code U07.1 An emergency ICD-10 code of ‘U07.1 COVID-19, virus identified’ is assigned to a disease diagnosis of COVID-19 confirmed by laboratory testing. An emergency ICD-10 code of ‘U07.2 COVID-19, virus not identified’ is assigned to a clinical or epidemiological diagnosis of COVID-19 where laboratory confirmation is inconclusive or not available. 2Percent of expected deaths is the number of deaths for all causes for this week in 2020 compared to the average number across the same week in 2017–2019. Previous analyses of 2015–2016 provisional data completeness have found that completeness is lower in the first few weeks following the date of death (<25%), and then increases over time such that data are generally at least 75% complete within 8 weeks of when the death occurred (8). 3Counts of deaths involving pneumonia include pneumonia deaths that also involve COVID-19 and exclude pneumonia deaths involving influenza. 4Counts of deaths involving influenza include deaths with pneumonia or COVID-19 also listed as a cause of death. 5Deaths with confirmed or presumed COVID-19, pneumonia, or influenza, coded to ICD–10 codes U07.1 or J09–J18.9. Influenza and pneumonia J09-J18.
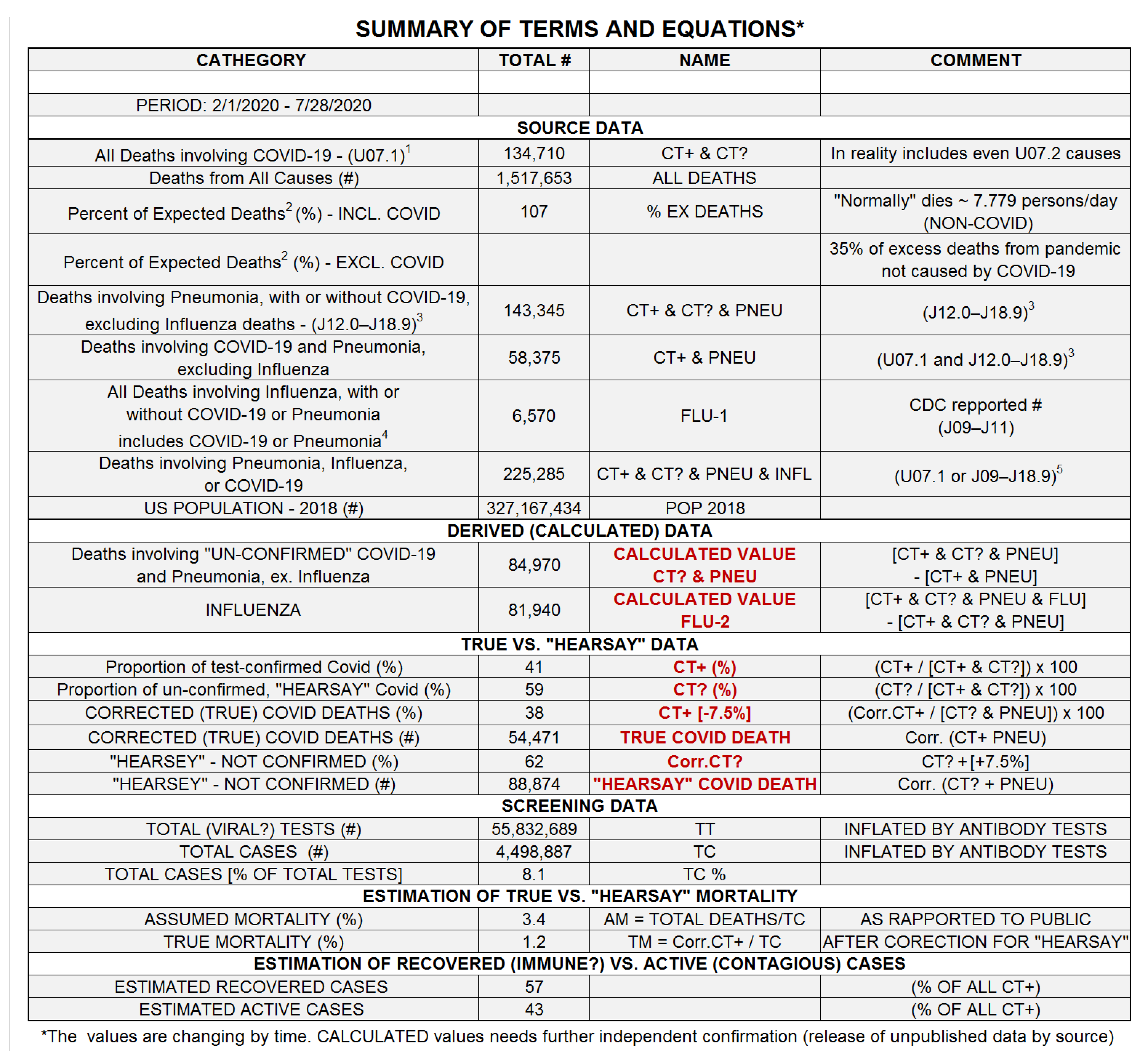
Figure 2.

Figure 5.
CORRECTION FOR “HARMLESS” COVID POSITIVITY was performed by subtracting a fraction of deaths from the confirmed COVID deaths (CT+ & PNEU), corresponding to the frequency of COVID viral test positives even in the general, mostly healthy population (CT+ / TEST (%). The red line and shaded area defines the corrected, certainly COVID-related deaths (CT+ & PNE [CORR]) separated from the “probable” or “suspected” COVID deaths (“HEARSAY” COD determinations).
Figure 5.
CORRECTION FOR “HARMLESS” COVID POSITIVITY was performed by subtracting a fraction of deaths from the confirmed COVID deaths (CT+ & PNEU), corresponding to the frequency of COVID viral test positives even in the general, mostly healthy population (CT+ / TEST (%). The red line and shaded area defines the corrected, certainly COVID-related deaths (CT+ & PNE [CORR]) separated from the “probable” or “suspected” COVID deaths (“HEARSAY” COD determinations).
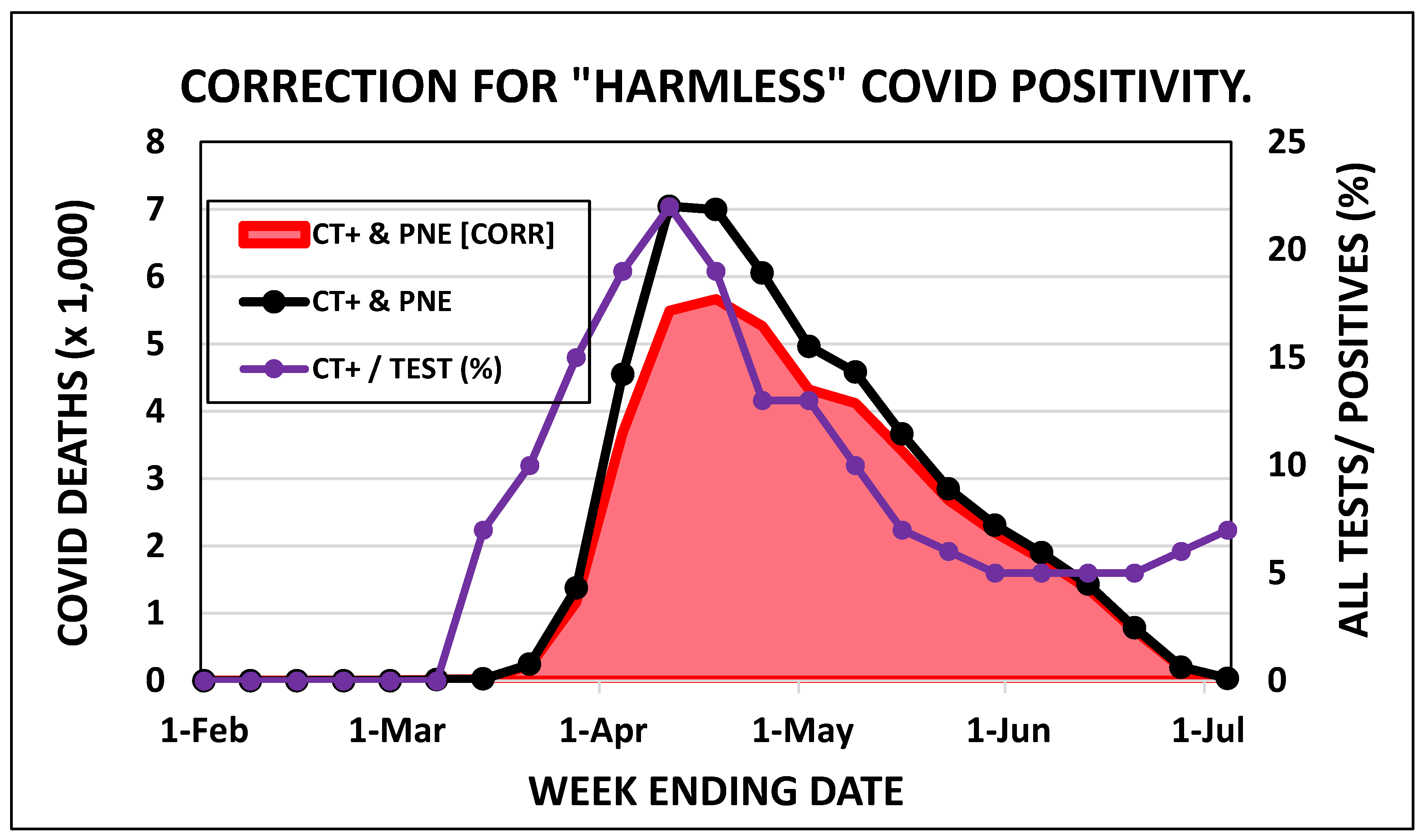
Figure 6.
EFFECT OF STATE’S POLITICS ON THE COVID STATISTICS. Sates were sorted in descending order of the estimated Democrat (DEM) / Republican (REP) ratio of voters in their population (D/R % OF mean). See Figure 1 for the definition of groups and subgroups.
Figure 6.
EFFECT OF STATE’S POLITICS ON THE COVID STATISTICS. Sates were sorted in descending order of the estimated Democrat (DEM) / Republican (REP) ratio of voters in their population (D/R % OF mean). See Figure 1 for the definition of groups and subgroups.
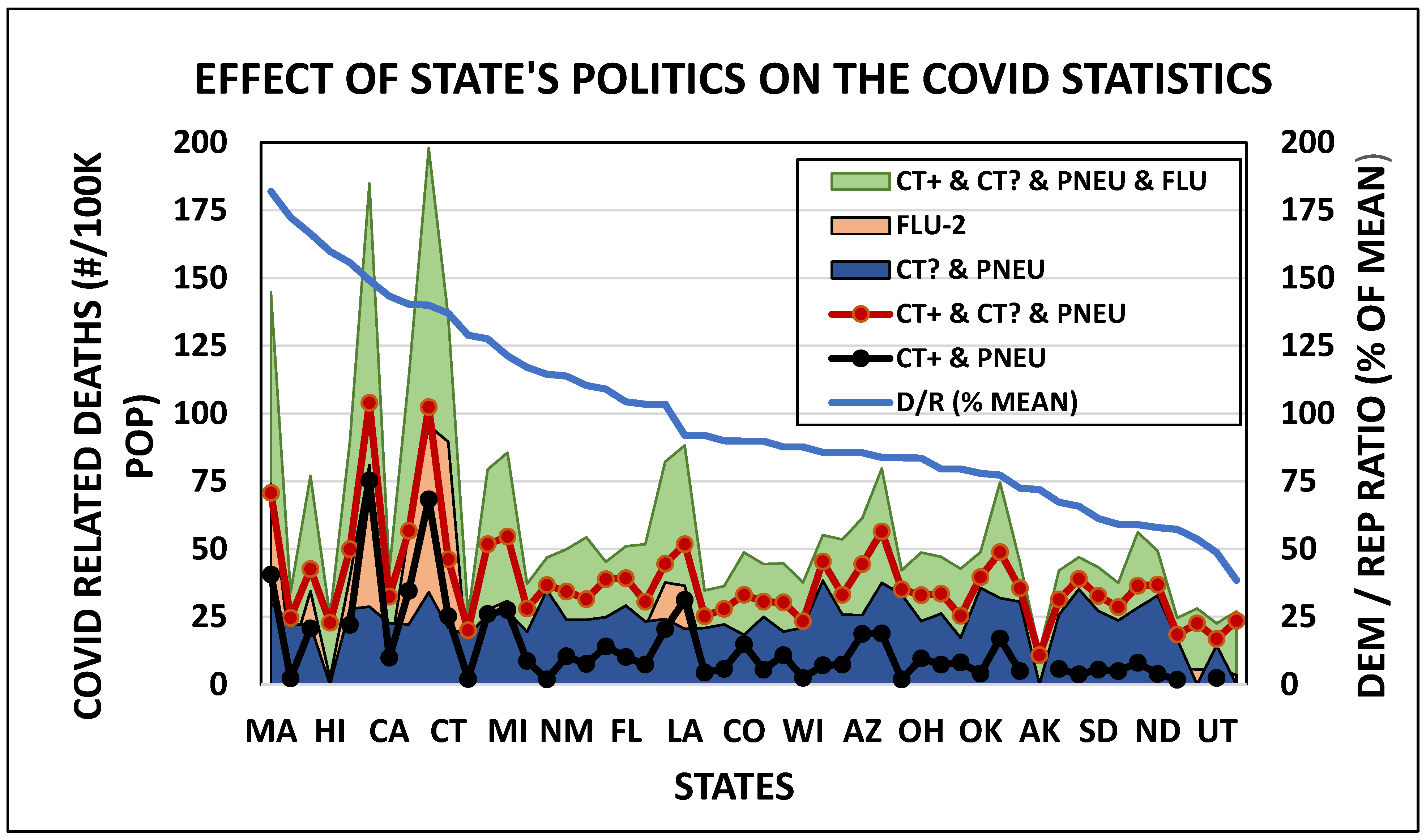
Figure 7.
DEATHS CAUSED BY “COVID AS “AMPLIFIER” in different age-groups. COVID as the primary UCOD were determined (confirmed) by positive viral test (CT+), suspected based on “hearsay” information without viral test (CT?) and pooled into a single ‘COVID’ group (CT+ & CT?). Other, largely parallel lines indicate the most frequent co-existing conditions, like RENAL (kidney) disease, INFLUENZA, CIRCULATORY (heart) disease, INJURY, MALIGN-TUMORS, SEPSIS, DIABETES, RESPIRATORY (lungs) disease, OTHER. Three additional lines are not parallel to the COVID line (OBESITY, ALZHEIMER, DEMENTIA), because these conditions have special age preference. (No documented case could be found there the COVID alone caused the death of a young person).
Figure 7.
DEATHS CAUSED BY “COVID AS “AMPLIFIER” in different age-groups. COVID as the primary UCOD were determined (confirmed) by positive viral test (CT+), suspected based on “hearsay” information without viral test (CT?) and pooled into a single ‘COVID’ group (CT+ & CT?). Other, largely parallel lines indicate the most frequent co-existing conditions, like RENAL (kidney) disease, INFLUENZA, CIRCULATORY (heart) disease, INJURY, MALIGN-TUMORS, SEPSIS, DIABETES, RESPIRATORY (lungs) disease, OTHER. Three additional lines are not parallel to the COVID line (OBESITY, ALZHEIMER, DEMENTIA), because these conditions have special age preference. (No documented case could be found there the COVID alone caused the death of a young person).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



