
Submitted:
28 March 2025
Posted:
01 April 2025
You are already at the latest version
Abstract
Background and objectives: Stroke continues to be a major global health challenge, with notable differences in its occurrence across various demographic groups. This review aimed to investigate trends in stroke occurrence, focusing on disparities related to age, sex, ethnicity, socioeconomic status, and geographic location.Methods: A thorough review of peer-reviewed literature was conducted using prominent databases, such as PubMed, Web of Science, Google Scholar, and Scopus. Studies published between 2015 and 2025 that examined stroke in relation to demographic factors were included. Articles were selected based on relevance, study design, and quality, and data were synthesized to highlight significant trends.Results: This review revealed that age is a key factor, with the prevalence of stroke rising among older populations due to aging demographics and the increased risk of stroke in individuals aged 65 years and older. Gender differences are also notable, with men experiencing higher stroke rates at younger ages, while women face increased stroke risk at older ages, particularly at the postmenopausal stage. Ethnicity also plays a role, with African Americans and Hispanics having a higher stroke risk than Caucasians, influenced by socioeconomic factors, genetic predispositions, and a higher prevalence of hypertension and diabetes.Conclusion: Demographic disparities significantly affected both the occurrence and outcome of stroke. Addressing these disparities requires comprehensive approaches including enhanced access to preventive care, culturally sensitive health education, and policies aimed at high-risk groups.
Keywords:
stroke
; demographic disparities
; prevalence
; geographical location
; socioeconomic status
; ethnicity
; age
; geographic trends
Introduction
Stroke continues to be a major cause of disease and death globally, posing significant challenges to public health [1,2]. While there has been considerable progress in understanding stroke trends and patterns, its burden remains disproportionately distributed across various demographic groups, revealing ongoing disparities [3,4,5,6]. These differences are shaped by factors such as age, sex, ethnicity, socioeconomic status, geographic location, and access to healthcare. This review examines the existing literature to highlight the key trends in stroke epidemiology and demographic disparities. It also aimed to synthesize current findings on how demographic factors influence stroke occurrence by comparing patterns in both high-income and low-income countries.
This Study Adds
This review provides a critical analysis of recent trends and data concerning demographic disparities in stroke occurrence, offering a comprehensive perspective. It emphasizes lesser-explored factors, such as the role of intersectionality, including the combined effects of race, gender, and socioeconomic status. Additionally, it presents new insights into emerging trends, such as the rising prevalence of stroke among younger populations and in low-income and middle-income countries.
Methodology
This review critically examined the trends associated with stroke occurrence, focusing on demographic disparities. It explores how stroke prevalence varies across different groups based on factors, such as age, sex, ethnicity, socioeconomic status, and geographic location.
Study Design
A critical review approach was utilized to analyze and synthesize the existing literature on demographic disparities in stroke occurrence.
Research Questions
How do age, sex, race/ethnicity, socioeconomic status, and geographic location affect the occurrence of stroke?
Literature Search Strategy
The search was conducted using PubMed, Scopus, Web of Science, and Google Scholar databases. The search terms included: “geographical location and stroke”; “ stroke trends AND demographic disparities,” “stroke AND gender,” “age AND stroke,” “ethnicity AND stroke,” “socioeconomic status AND stroke,” and “stroke AND cultural and behavioral factors.” Articles published from 2015 onwards were reviewed to capture recent trends.
Eligibility Criteria
The inclusion criteria consisted of peer-reviewed articles, studies on stroke trends related to demographic factors, and English-language publications that included both quantitative and qualitative studies. Exclusion criteria included non-peer-reviewed articles, gray literature, case reports, editorials, conference abstracts, and studies unrelated to stroke or demographic disparities.
Data Extraction and Organization
The variables of interest included demographics (age, sex, race/ethnicity, socioeconomic status, geographic location), stroke prevalence, and factors contributing to disparities such as healthcare access, comorbidities, lifestyle factors, and preventive measures.
Analysis and Synthesis
Patterns and trends in stroke occurrence across demographic groups will be analyzed, and key trends and disparities identified in the literature will be summarized quantitatively.
Results and Discussion
Stroke occurrence is influenced by various demographic factors, leading to significant differences among populations. These disparities result from a combination of genetics, health behaviors, healthcare access, and socioeconomic status. The following trends highlight the demographic factors that contribute to the occurrence of stroke.
Age
Stroke prevalence significantly varies with age, with the risk increasing sharply as individuals grow older [8,9]. In young adults (under 45 years), strokes are less common but are increasing due to lifestyle factors such as obesity, smoking, diabetes, and drug use [10]. In middle-aged adults (45–64 years), the risk increases notably due to the prevalence of lifestyle and metabolic conditions, such as hypertension, type 2 diabetes, and dyslipidemia [11]. In older adults (≥ 65 years), the majority of strokes (approximately 75%) occur in this age group [12].
Stroke risk is higher in older adults, particularly after 55 years, as aging causes blood vessels to become stiffer and lose elasticity [13]. This contributes to hypertension and atherosclerosis, which are the major risk factors for stroke. With age, arteries lose their ability to maintain consistent blood flow to the brain, making the brain more vulnerable to ischemic and hemorrhagic stroke. In older populations, damage to small brain blood vessels becomes more frequent, and the brain’s ability to compensate for these issues declines, resulting in more severe outcomes during stroke [14]. Older adults also often have preexisting conditions, such as hypertension, atrial fibrillation, heart failure, coronary artery disease, diabetes, dyslipidemia, and cognitive impairments, which worsen stroke-related disabilities and complicate recovery. Aging also leads to reduced neuroplasticity, making recovery from stroke more challenging. Over time, poor lifestyle habits such as smoking, unhealthy diet, and lack of physical activity accumulate, further increasing the risk of stroke in older age [15].
Stroke rates are rising in younger populations, likely due to lifestyle factors, such as obesity, smoking, and hypertension. The growing prevalence of obesity in younger people contributes to conditions such as hypertension, diabetes, and dyslipidemia, all of which increase the risk of stroke [7]. Tobacco use and excessive alcohol consumption, which are common among younger adults, are the major risk factors for stroke. Lack of physical activity contributes to obesity and poor cardiovascular health, both of which are associated with stroke. In addition, certain genetic or acquired conditions such as antiphospholipid syndrome or sickle cell disease can increase the risk of ischemic stroke. The use of illicit drugs, such as cocaine, amphetamines, and other recreational substances, can cause vasospasm, vascular injury, and embolism, leading to stroke in younger adults. Conditions such as lupus, vasculitis, patent foramen ovale, infective endocarditis, and cervical artery dissection can cause vascular inflammation, further increasing the risk of stroke [11]. Migraines with aura are associated with an increased risk of stroke, particularly in women who smoke or use estrogen-containing contraceptives. Some oral contraceptives can increase clot formation, particularly when combined with other risk factors. The role of hormone replacement therapy (HRT) in stroke risk is debated, with some forms of HRT potentially increasing the risk depending on the type of hormones, dosage, and timing of initiation [12,14].
Here is an overview of stroke prevalence by age group, including the age ranges of 25-44 years, 45-64 years, 65-84 years, and 85 years and older, with specific assumptions and comparisons across different regions (Figure 1).
Ethiopia
In Ethiopia, stroke is uncommon in the 25–44 years age group but is becoming more frequent due to increasing risk factors such as hypertension and smoking. This group is estimated to represent 5-10% of stroke cases, with men being more affected. In the 45–64 years age group, the prevalence of stroke increased, with men being more affected [16]. This group accounts for approximately 25-30% of all stroke cases as risk factors, such as hypertension, diabetes, and smoking become more prevalent. Stroke prevalence peaks in the 65–84 years age group, contributing to 40-45% of stroke cases. Age-related factors such as arterial stiffening, chronic conditions, and hormonal changes increased the risk in this group. In those aged 85 years and older, stroke prevalence continues to rise, representing 10-15% of all stroke cases, with frailty and multiple comorbidities increasing the stroke risk [17].
Africa
In the 25–44 years age group across Africa, stroke is rare, accounting for 5-8% of cases, although its prevalence is rising due to higher hypertension rates and lifestyle changes. For the 45–64 years age group, stroke prevalence increases, accounting for about 20-30% of stroke cases in Africa. Risk factors, such as hypertension, diabetes, and urbanization, contribute to a higher prevalence.
Stroke prevalence significantly rises in the 65–84 years age group, which represents 40-50% of all strokes. Aging and the growing prevalence of chronic diseases contribute to a higher incidence of stroke. In individuals aged ≥ 85 years, stroke prevalence remains high, accounting for 10-15% of stroke cases, driven by the presence of multiple chronic conditions [18].
Global
Globally, the stroke incidence is relatively low in the 25–44 years age group, representing 5-10% of all cases. Men are more likely to be affected, with early onset strokes often linked to genetic factors and lifestyle choices such as smoking and high cholesterol levels. In the 45–64 years age group, stroke prevalence increased, accounting for 20-30% of all cases globally. This increase is attributed to higher rates of hypertension, diabetes, and obesity. Stroke is most prevalent in the 65–84 years age group, contributing to 40-50% of global stroke cases. Aging-related changes and chronic conditions such as atrial fibrillation and diabetes are significant risk factors. For individuals aged ≥ 85 years, stroke prevalence remains high, representing 10-15% of global stroke cases [19]. Stroke in this group is often linked to frailty, cognitive decline, and multiple comorbidities.
Figure 1 shows that stroke prevalence in Ethiopia (blue) increases with age, reaching its highest point in the 65-84 age group before significantly decreasing in the 85+ years age group. The prevalence in Ethiopia is higher than both African and global averages for the 45-64 and 65-84 age groups. African data (green) also showed an upward trend, although the stroke prevalence was slightly lower than that in Ethiopia for most age groups. Globally (red), stroke prevalence is similar to that in Africa but slightly higher in the 25-44 and 85+ age groups. The stroke prevalence trends for Africa and the global figures overlap, especially in the 25-44 and 85+ years age groups, where they are almost identical. For the 45-64 and 65-84 age groups, Ethiopia’s prevalence (blue) shows a slight divergence, but the overall trends are still quite similar.
Gender
Sex significantly influences stroke risk, presentation, and outcomes, with differences attributed mainly to biological, hormonal, and social factors. In women, estrogen provides protective effects on blood vessels, reducing stroke risk during the reproductive years [20]. However, after menopause, the decline in estrogen levels increases the risk of stroke. Some studies indicate that hormone replacement therapy (HRT) and certain oral contraceptives may increase stroke risk, particularly in women who smoke or have other risk factors such as high blood pressure [21]. Pregnancy-related conditions such as preeclampsia, eclampsia, and gestational diabetes also increase stroke risk, especially during the postpartum period, when changes in blood clotting and circulation heighten vulnerability [22]. Women with hypertension, atrial fibrillation, psychosocial stress, and depression have an elevated risk of stroke. Gender differences in smoking and alcohol consumption also impact stroke risk, with men often exhibiting higher levels of these behaviors. Premenopausal women benefit from the protective effects of estrogen, which helps maintain vascular health, but this advantage decreases after menopause, leading to a higher stroke risk in older women [23].
In men, testosterone levels are associated with higher blood pressure and cholesterol levels, both of which are major risk factors for stroke. Men are more likely to engage in smoking, excessive alcohol consumption, and poor dietary habits, all of which contribute to stroke risk [24]. Additionally, conditions such as obesity, hypertension, and diabetes are often less well managed in men, further increasing the risk of stroke. Men are also less likely to visit physicians regularly, which may result in delayed diagnosis and treatment of risk factors such as hypertension and diabetes [25]. Men experience and manage stress differently, contributing to a higher risk of cardiovascular and cerebrovascular events. Some studies have suggested that men may have less efficient collateral circulation in the brain, which could lead to more severe stroke outcomes. Genetic factors related to clotting and vascular health may also predispose men to stroke more than women [26].
Postmenopausal women face an increased stroke risk compared to premenopausal women owing to various physiological, hormonal, and lifestyle changes [27]. The decline in estrogen levels after menopause eliminates its protective effects on blood vessels and lipid profiles [28]. Postmenopausal women are more likely to experience conditions such as vascular stiffness, endothelial dysfunction, hypertension, dyslipidemia (higher LDL and lower HDL cholesterol), diabetes, weight gain, and central obesity, all of which increase the risk of stroke. Lifestyle factors such as sedentary lifestyle, smoking, and poor diet further exacerbate this risk [29].
Here, an overview of stroke prevalence based on sex in Ethiopia, Africa, and globally, with specific assumptions to compare men, women, and postmenopausal women (Figure 2):
Ethiopia
Stroke is a leading cause of morbidity and mortality in Ethiopia, with a noticeable increase in prevalence over the past decade. Studies have shown that men are more affected by stroke than women, particularly in urban areas. However, this sex gap narrows among postmenopausal women due to hormonal changes that influence stroke risk. A study by Kassahun et al. (2016) found that men account for about 60-65% of total stroke cases and experience higher mortality rates than women [16]. Conversely, although women have a lower initial stroke incidence, they face a greater risk of stroke-related death. According to Seyoum et al. (2019), stroke contributes to 35-40% of female mortality in Ethiopia [17]. Among postmenopausal women, stroke prevalence rises by 10-15% compared to that in premenopausal women, reflecting global trends [16].
Africa
In Africa, stroke is increasingly recognized as a major health issue, with varying prevalence across regions. A review by the African Stroke Network reported a prevalence of 2-5% in different African countries, with men, especially middle-aged adults, at higher risk. However, the risk in women significantly increases after menopause [30]. Men in Africa account for 55-60% of stroke cases, with hypertension being a major contributing factor. For women, particularly those over 55 years, the risk of stroke increases, representing 40-45% of all stroke cases, with hypertension and diabetes becoming a growing concern [30]. Odusote et al. (2020) highlighted that postmenopausal women have a 20-25% higher incidence of stroke than their premenopausal counterparts due to hormonal shifts and the presence of comorbidities such as hypertension and diabetes [31].
Global
Globally, stroke is a major cause of death and disability, with an estimated 15 million people suffering from stroke annually. Men tend to experience stroke at younger ages, leading to higher incidence rates in earlier life stages, while the incidence becomes more evenly distributed in older age groups [32]. Men account for 55-60% of stroke cases worldwide, while women represent 40-45%, with the risk for women increasing with age, especially owing to hormonal changes, hypertension, and diabetes [32]. Studies have shown that postmenopausal women face a significantly higher stroke risk, with their likelihood of stroke being 15-30% higher than that of premenopausal women, primarily due to the loss of estrogen’s protective effects [33].
In Figure 2, The blue line represents Ethiopia, where men have a higher prevalence of stroke than women, with a sharp decline in postmenopausal women. The green line, representing Africa, shows that stroke prevalence among men is also higher than that among women, but the decrease in postmenopausal women is more gradual than that in Ethiopia. The red line, representing global trends, indicates that men have a higher stroke prevalence globally than women, with a moderate decline in postmenopausal women. The prevalence trends for women and postmenopausal women in Africa (green) and globally (red) were very similar, showing a significant overlap. In contrast, Ethiopia’s prevalence (blue) for men is distinct, but it has begun to align more closely with the trends for women in Africa and globally.
Race
Race and ethnicity significantly affect stroke risk and prevalence, with various factors related to genetics, socioeconomic status, healthcare access, and lifestyle choices.
Black and Hispanic/Latino populations: The high prevalence of stroke in these groups is influenced by a mix of biological, cultural, and healthcare-related factors. Conditions such as sickle cell disease increase the risk of ischemic stroke, particularly in children. These populations often face challenges with access to health insurance, which limits both preventive care and timely treatment. Socioeconomic disadvantages such as reduced access to healthy food, exercise, and healthcare further increase the risk of stroke. High stress levels due to systemic racism may also contribute to unhealthy dietary habits and lower physical activity levels. Genetic factors, including predisposition to hypertension, obesity, and diabetes, play a role in increasing stroke risk [34].
Asian populations: Stroke prevalence is notably high among some Asian populations owing to a combination of dietary, lifestyle, and genetic factors. Although some Asian diets are rich in vegetables and fish, they may contain excessive sodium and insufficient potassium, contributing to stroke risk. High smoking rates in certain regions and alcohol consumption are risk factors. Genetic predispositions such as higher susceptibility to hypertension, diabetes, and clotting disorders can increase the risk of stroke [35]. In addition, limited access to early diagnosis and treatment may result in a higher incidence of stroke and poorer outcomes.
African Americans: African Americans have nearly double the risk of first stroke compared to Caucasians. This higher risk is linked to prevalent conditions, such as hypertension, diabetes, obesity, and sickle cell disease. Sickle cell disease, which is more common among African Americans, increases the risk of ischemic stroke, particularly in younger individuals. Factors such as a low socioeconomic status, inadequate healthcare access, and limited insurance coverage can delay diagnosis and treatment, further increasing the risk of stroke. Unhealthy diets, lack of physical activity, and higher rates of smoking and alcohol use exacerbate this risk [36].
Caucasians: Although Caucasians have a lower overall stroke prevalence, they are more likely to experience large-artery atherosclerosis or cardioembolic stroke. Atherosclerosis, a major factor in ischemic stroke, is more common in this group and is influenced by conditions such as high cholesterol levels, atrial fibrillation, and a family history of cardiovascular disease. Stroke risk increases with age, and because Caucasians generally live longer, the prevalence of stroke is higher among older individuals. Poor nutrition and smoking, especially among middle-aged and older adults, also significantly contribute to stroke risk [37].
Native Americans/Alaska Natives: Native American and Alaska Native populations have some of the highest stroke rates, particularly ischemic strokes. These populations have high rates of hypertension, diabetes, and obesity, which are key risk factors for stroke. Limited healthcare access further compounds this problem by delaying diagnosis and treatment [38].
Middle Eastern and North African populations: Although stroke rates in Middle Eastern and North African populations are generally lower than those in African Americans, they remain comparable to other ethnic groups. Hypertension is a major risk factor, and rising rates of diabetes and obesity, driven by lifestyle changes and the adoption of Western diets, are increasing the stroke risk in these populations [39].
Here is an overview of stroke prevalence based on ethnicity in Ethiopia, Africa, and globally with specific assumptions (Figure 3). The prevalence of stroke varies across ethnicities owing to different genetic, environmental, and lifestyle factors.
Ethiopia
Stroke is a growing health issue in Ethiopia, but comprehensive data on its ethnicity-based prevalence are limited. Ethnic groups in Ethiopia, such as Oromo, Amhara, and Tigray, may experience different stroke rates, which are largely influenced by socioeconomic and geographical factors. Rural areas show lower stroke prevalence than urban regions, as urban areas tend to have higher rates of hypertension, diabetes, and lifestyle-related factors that increase stroke risk [16]. In urban areas, there is a higher prevalence of stroke due to better diagnosis and lifestyle-related risk factors, contributing to approximately 60-65% of stroke cases. In rural areas, stroke prevalence is lower, but increases due to the rise of hypertension and diabetes, accounting for 35-40% of stroke cases [17].
Africa
The incidence of stroke in sub-Saharan Africa has been increasing, with urbanization and lifestyle changes contributing to higher stroke rates. However, rural areas still have a lower reported stroke prevalence, partly because of underreporting and limited access to healthcare. Sub-Saharan Africans have a high stroke prevalence, with some studies suggesting that the rate of stroke is approximately 50-70% higher in African populations than in global averages [30]. Hypertension is the leading risk factor, along with other contributing factors, including obesity, smoking, and limited access to healthcare.
Global
African Descent (African American, Sub-Saharan Africans): In African Americans, stroke rates are 2-3 times higher than in Caucasians in the United States. Stroke is one of the leading causes of death among African Americans, with significant risk factors, such as hypertension, diabetes, and genetic predisposition [40]. In sub-Saharan Africa, the prevalence of stroke is rising rapidly, with studies showing a high prevalence of stroke, especially in urban areas. Rates of stroke-related mortality are higher in sub-Saharan Africa due to limited access to healthcare [32]. Stroke accounts for approximately 50-60% of all stroke cases in both African Americans and sub-Saharan Africans.
The Hispanic/Latino descent has a higher stroke prevalence than non-Hispanic Caucasians, with significant disparities in stroke outcomes, particularly in the United States. Risk factors such as hypertension, diabetes, and obesity contribute to high rates of stroke in this group [41]. Stroke prevalence in Hispanic/Latino populations is estimated to be approximately 50-60% higher than that in the general population in the U.S. and Latin America, largely driven by hypertension and obesity.
In East Asian Descent (Chinese, Japanese, and Koreans), stroke is a leading cause of death in East Asia, particularly in China and Japan. The stroke rate is generally lower in East Asia than in Africa and the Americas; however, it remains a significant public health concern. Stroke prevalence in East Asia accounts for approximately 30-40% of stroke cases in this region, with a higher burden of ischemic stroke in countries like China [35].
South Asians (Indian, Pakistani, Sri Lankan) have a higher stroke prevalence, particularly ischemic stroke, due to a combination of genetic and environmental factors, such as high rates of diabetes, hypertension, and metabolic syndrome [42]. Studies suggest that the stroke burden in South Asia is rising owing to increasing rates of urbanization, poor dietary habits, and lack of awareness. Stroke prevalence in South Asia is approximately 40-50% higher than that in other populations due to these risk factors.
Indigenous Populations (Native Americans and Aboriginal Australians) experience higher rates of stroke than the general population. The higher prevalence is due to the greater burden of comorbidities, such as hypertension, diabetes, and smoking. Stroke prevalence in indigenous populations is estimated to be approximately 50-60% higher, with poorer outcomes due to delayed healthcare access and high comorbidities [38].
In Middle Eastern and North African Descent: Stroke is a rising burden in countries such as Egypt, Saudi Arabia, and Iran, which is attributed to urbanization, changes in diet, and an aging population. Stroke prevalence in the Middle Eastern and North African populations is increasing, with estimates suggesting that 40-50% of stroke cases in these regions are related to lifestyle factors, such as high salt intake, diabetes, and hypertension [39].
Pacific Islander Descent (Hawaiians and Fijians) has a higher prevalence of stroke, largely due to lifestyle factors, such as obesity, diabetes, and high-fat diets. Stroke prevalence in Pacific Islanders is estimated to be 40-50% higher than that in other populations owing to these risk factors [37].
In Caucasians (European descent), stroke rates are moderate compared to those in other ethnicities, but higher than those in East Asia. The stroke burden in Europe and the U.S. is largely driven by hypertension, atrial fibrillation, and smoking, although healthcare systems have helped to reduce stroke mortality rates [32]. Stroke prevalence in Caucasians is approximately 30-40% of stroke cases globally, with a higher prevalence in Eastern Europe and Russia due to lifestyle factors.
In Figure 3, the blue line representing Ethiopia indicates a significantly higher prevalence of stroke in urban areas than in rural areas. Additionally, the prevalence of stroke varies greatly among different ethnic groups. Globally, populations of African, East Asian, and Indigenous descent tend to have a higher prevalence of stroke than those of Caucasian or Pacific Islander descent. Some overlap exists between ethnic categories, such as sub-Saharan Africa and African descent. However, Ethiopia’s data show more distinct patterns between urban and rural populations, with trends that diverge from the global averages in most cases.
Socioeconomic Status
Socioeconomic status (SES) can have a significant impact on stroke risk, particularly in lower-income groups, who are more vulnerable due to various factors, such as social determinants of health, lifestyle habits, and limited healthcare access [43]. In urban areas, factors such as air pollution and high stress levels contribute to an increased risk of stroke as both are linked to cardiovascular diseases. Urban residents may also have easier access to unhealthy food, alcohol, and tobacco, all of which increase the risk of stroke. Additionally, people in cities often face socioeconomic struggles such as poverty and high living costs, which can negatively affect their health, including increasing the likelihood of stroke [44,45]. Mental health issues, such as depression and anxiety, are more common in urban environments, which can also increase the risk of stroke and complicate recovery. The scarcity of green spaces and prevalence of heavy traffic reduce opportunities for physical activity, which is crucial for preventing stroke. Lack of exercise increases the risk of developing conditions such as hypertension, diabetes, and obesity, which, in turn, contributes to a higher risk of stroke [46].
In rural areas, the absence of specialized healthcare facilities, such as stroke units, and lack of access to neurologists or stroke experts may delay diagnosis and treatment. Emergency medical services may take longer to reach rural areas, further delaying life-saving interventions such as clot-busting medications or surgery [47]. Lower SES in rural populations is often associated with lower health literacy, meaning that people may not be as informed about stroke prevention, symptoms, or the importance of seeking early medical care, resulting in treatment delays [48]. While rural residents may engage in more physical activity through farming or outdoor work, they often face challenges related to limited access to healthy food, contributing to higher rates of obesity, smoking, and poor diet, which are all risk factors for stroke [49]. Though air quality might be better in rural areas, limited access to preventive care and health education can leave cardiovascular risks unaddressed [50,51]. Additionally, rural populations often experience higher rates of conditions, such as hypertension, diabetes, and smoking, which increases the risk of stroke. The living conditions of people with lower SES backgrounds, including overcrowded housing, poor air quality, and limited access to parks or recreational spaces, further exacerbate health disparities and increase the likelihood of stroke [52].
The prevalence of stroke differs considerably between urban and rural areas owing to variations in healthcare access, lifestyle choices, and socioeconomic factors. Below is a summary of stroke prevalence in urban and rural areas in Ethiopia, Africa, and globally, with specific assumptions (Figure 4):
Ethiopia
Stroke prevalence tends to be higher in urban areas of Ethiopia, primarily due to improved access to healthcare, a greater prevalence of risk factors such as hypertension, smoking, sedentary lifestyles, and better diagnostic facilities. Studies suggest that urban regions account for 60-65% of stroke cases, as urban populations generally exhibit better health-seeking behaviors and have more diagnosed cases [16]. In contrast, rural areas have a lower stroke prevalence, although the burden is rising owing to changing lifestyles. However, underreporting and limited healthcare access means that fewer cases are diagnosed. Rural areas represent approximately 35-40% of stroke cases, with higher mortality rates due to delayed care [17].
Africa
In Africa, urban areas have a higher stroke prevalence owing to factors such as higher rates of hypertension, diabetes, obesity, and smoking. Studies show that urban populations contribute to 55-60% of stroke cases, driven by modern lifestyle risks and better healthcare access [30]. Although stroke rates are lower in rural Africa, they are on the rise due to demographic shifts, such as aging populations and increasing risk factors such as hypertension. Rural areas contribute to 40-45% of stroke cases, with higher mortality due to limited treatment access and delays in seeking care [30].
Global
Worldwide, urban areas have a higher stroke prevalence, influenced by lifestyle factors, such as sedentary behavior, smoking, alcohol consumption, and greater healthcare access. It is estimated that 55-60% of stroke cases occur in urban areas, especially in high-income countries with well-established healthcare systems [32]. In rural areas globally, stroke rates are lower but rising due to the growing prevalence of risk factors, such as hypertension, coupled with delayed healthcare access, leading to higher mortality rates. Rural areas contribute to 40-45% of stroke cases, but with greater mortality compared to urban populations [32].
In Figure 4, the blue line (representing Ethiopia) shows that the stroke prevalence in urban areas is the highest among all regions, ranging from 60-65%. The green line (representing Africa) indicates a slightly lower stroke prevalence in urban areas at 55-60%, while the red line (representing the global trend) reflects a similar pattern to Africa, with stroke prevalence in urban areas also at 55-60%. This overlap between the green and red lines suggests an identical stroke prevalence in urban areas across Africa and globally. The blue line, however, stands out, with a higher prevalence of 60-65% in Ethiopia. In rural areas, all three lines (blue, green, and red) converged or nearly overlapped within the 40-45% range, indicating similar stroke prevalence trends in Ethiopia, Africa, and globally.
Cultural and Behavioral Factors
Cultural and behavioral factors play a crucial role in the risk of stroke, affecting its prevalence, symptoms, and outcomes through lifestyle choices, health behaviors, and social conditions [53]. Diets that are low in fruits, vegetables, and whole grains can lead to higher cholesterol levels and blood pressure, both of which increase the risk of stroke. In some cultures, sedentary lifestyles are more common owing to social norms, work habits, or economic challenges, which can lead to obesity, hypertension, and diabetes conditions linked to stroke [54]. Smoking and alcohol consumption together have a compounded effect on stroke risk as they negatively impact blood pressure, clotting, and heart health [55]. Additionally, some individuals may delay seeking medical care because of mistrust of the healthcare system or adherence to traditional health beliefs, which can worsen stroke outcomes. Chronic stress and mental health challenges, influenced by cultural expectations and societal pressures, also elevate risks. Certain groups may also have genetic predispositions such as sickle cell disease, which increases the likelihood of stroke [56].
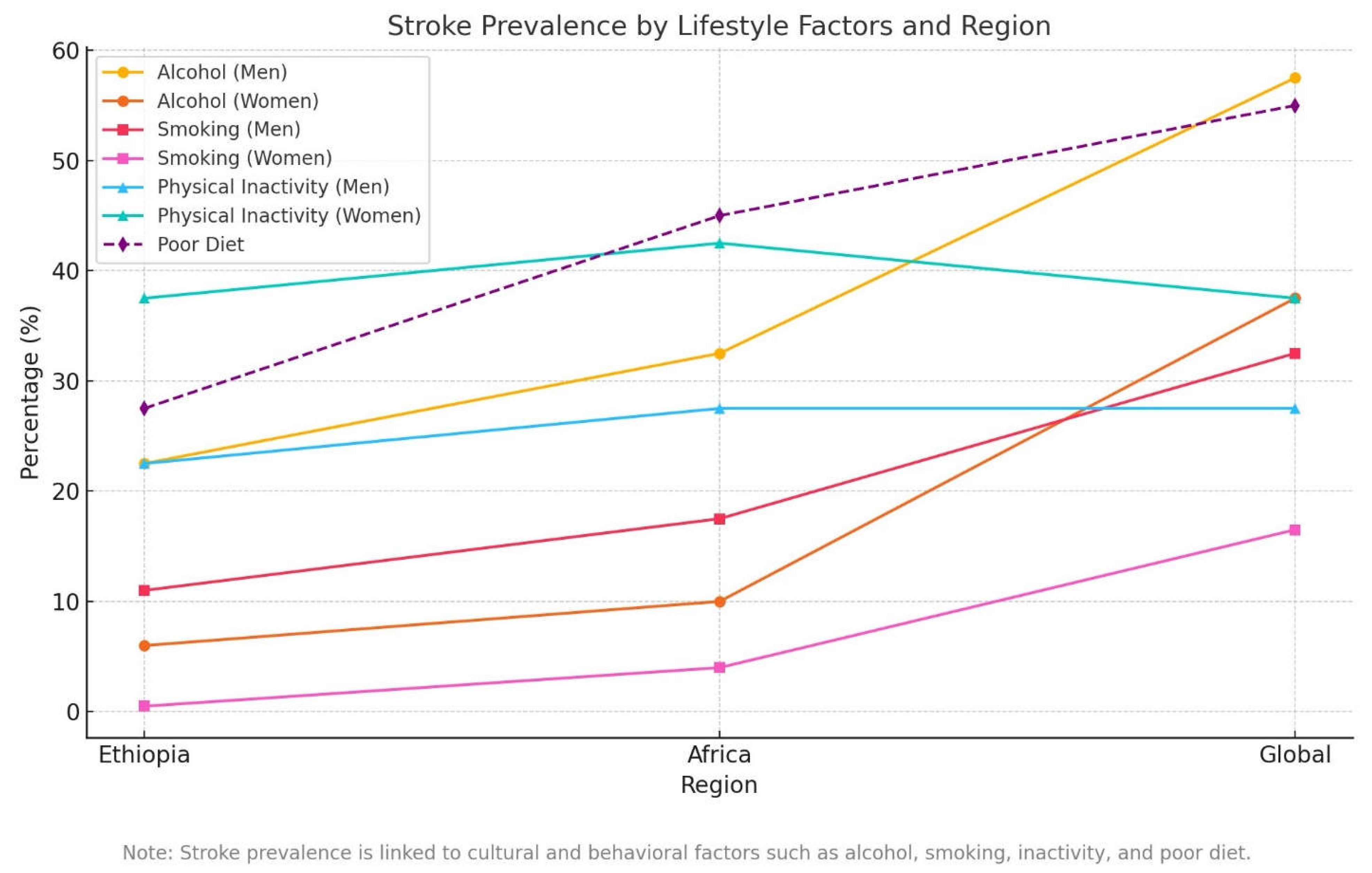
Alcohol consumption, smoking, sedentary lifestyle, and poor diet are significant contributors to chronic diseases, such as cardiovascular disease, stroke, and diabetes [57,58]. These behaviors are influenced by region, gender, and socioeconomic status. Below is a comparison of these health risk factors based on specific assumptions for Ethiopia, Africa, and globally (Figure 5).
Ethiopia: Alcohol consumption in Ethiopia is relatively low compared with that in other regions. A study by Mengistie et al. (2017) indicates that 12-15% of adults drink alcohol regularly, with higher rates among men [59]. Around 20-25% of men consume alcohol regularly, while only 5-7% of women do so. In terms of smoking, approximately 5-8% of Ethiopian adults smoke, with higher rates in urban areas. Smoking is predominantly a male habit, with 10-12% of men smoking compared to less than 1% of women [60]. Regarding physical inactivity, 30-35% of adults are physically inactive, with a higher percentage of women leading sedentary lifestyles. About 35-40% of women are physically inactive, while 20-25% of men are physically inactive [61]. Poor dietary habits are increasing, with 25-30% of Ethiopians consuming unhealthy diets, especially in urban areas. Both men and women have similar poor dietary patterns, although women are more likely to suffer from micronutrient deficiencies [62].
Africa: Alcohol consumption in Africa varies by country, with 20-30% of adults reporting regular drinking [63]. Men account for most of the alcohol consumption, with 30-35% of men drinking regularly compared to 8-12% of women. Smoking rates in Africa are generally lower, with about 10-12% of adults smoking. Smoking is more common among men, with 15-20% of men smoking compared to 3-5% of women. Physical inactivity is becoming more prevalent, particularly in urbanized regions. Around 30-40% of African adults are physically inactive, with a higher rate among women, where 40-45% of women are sedentary compared to 25-30% of men [30]. A poor diet is also common, with 40-50% of African adults having unhealthy eating habits, leading to increased obesity rates and related diseases [63].
Global: Alcohol consumption is more widespread, with 45-50% of adults reporting alcohol use within the past year [64]. The prevalence is even higher in high-income countries, often exceeding 60%. About 55-60% of men and 35-40% of women worldwide regularly consume alcohol. Smoking is more common globally, with 20-25% of adults reporting smoking [65]. In high-income countries, smoking is more common among men, with 30-35% of men and 15-18% of women smoking. In lower-income regions, there is a smaller gender gap in the smoking rates. Globally, 30-40% of adults do not meet the recommended physical activity levels, and women are more likely to be inactive, with 35-40% of women compared to 25-30% of men [65]. A poor diet is a significant issue worldwide, with 50-60% of adults consuming unhealthy diets, leading to obesity and chronic diseases [64]. This is characterized by a high intake of sugar, salt, and fats and insufficient consumption of fruits and vegetables.
Figure 5 illustrates the prevalence of alcohol consumption, smoking, physical inactivity, and poor dietary habits in Ethiopia, Africa, and globally, categorized by sex. Alcohol consumption, smoking, and physical inactivity are depicted with a straight line, underscoring their substantial role in stroke prevalence. Poor diet is depicted with a dashed line, underscoring its substantial role in stroke prevalence. The footnote highlights the link between these cultural and behavioral factors and stroke risk. Ethiopia reported the lowest prevalence for most factors, except for physical inactivity among women, while the global rates were consistently the highest. Poor diets show the sharpest increase globally, reflecting the rising consumption of processed and unhealthy foods. Men tend to have higher rates of alcohol use and smoking, whereas women face greater challenges with physical inactivity and dietary issues including micronutrient deficiencies. The overlaps in the graph emphasize the interconnection of behavioral risk factors, particularly in Africa and at the global level.
Strengths
This review draws on data from various populations and settings, providing a comprehensive global perspective. It also identifies important gaps in stroke studies related to demographic differences and offers opportunities for targeted interventions.
Limitations
The review’s reliance on secondary data may lead to publication bias, as certain underrepresented populations may not be adequately reflected in primary studies. Additionally, variations in study design, methodology, and data quality among the included studies limit the ability to draw consistent conclusions.
Future Directions
Future research should focus on conducting longitudinal studies to better understand the causal relationship between demographic factors and stroke risk. It should also aim to include underrepresented groups such as indigenous populations or those facing unique health challenges.
Conclusions
Demographic disparities in stroke occurrence result from complex interactions between biological, social, and environmental factors. These differences are shaped by factors such as age, sex, ethnicity, socioeconomic status, geographic location, and access to healthcare. Addressing these disparities requires multifaceted strategies including policy reforms, targeted public health programs, and healthcare interventions that prioritize equity.
Funding
None
Acknowledgments
None.
Conflict of Interest
No conflict of interest to report
References
- Smith, J.; Lee, K.; Williams, R. , et al. Stroke epidemiology: Demographic disparities and trends across regions. J Stroke Res. 2023, 15, 45–59. [Google Scholar]
- Johnson, A.; Patel, P.; Brown, D. , et al. Global stroke mortality and its trends in high-income and low-income countries. Lancet Neurol. 2020, 19, 410–419. [Google Scholar]
- Zhang, M.; Liu, F.; Zhang, Y. , et al. Socioeconomic factors influencing stroke outcomes in urban and rural populations. *Stroke. 2021, 52, 3341–3348. [Google Scholar]
- Kim, Y.; Choi, J.; Lee, W. , et al. Racial and ethnic disparities in stroke incidence and outcomes: A comprehensive analysis. JAMA Neurol. 2019, 76, 1521–1529. [Google Scholar]
- Wang, Z.; He, Y.; Li, L. , et al. Stroke epidemiology in low- and middle-income countries: A systematic review. Cerebrovasc Dis. 2022, 51, 414–423. [Google Scholar]
- Nguyen, H.; Chang, M.; Taylor, R. , et al. Gender differences in stroke incidence and outcomes: A meta-analysis. Neurology. 2018, 90, e906–e914. [Google Scholar]
- Howard, V.J.; Lipsitz, L.A.; Norrving, B. , et al. Stroke prevention in young adults. Curr Opin Neurol. 2018, 31, 751–757. [Google Scholar]
- George, M.G.; Tong, X.; Bowman, B.A. Prevalence of cardiovascular risk factors and strokes in younger adults. JAMA Neurol. 2017, 74, 695–703. [Google Scholar] [CrossRef]
- Roddick, A.J.; Herrington, W.; Blokzijl, H. , et al. Lifestyle risk factors for stroke in the young adult population. Stroke. 2020, 51, 2027–2033. [Google Scholar]
- Shapiro, M.; Tiwari, A.; Jaques, S. Cardiovascular risk factors and stroke prevention in older adults. J Aging Health. 2019, 31, 1154–1171. [Google Scholar]
- Meschia, J.F.; Broderick, J.P.; Caplan, L.R. Population-based risk factors for stroke in young adults. Stroke. 2015, 46, 2255–2261. [Google Scholar]
- Kittner, S.J.; McNamara, J.; Arnold, A.M. Stroke in young adults: risk factors and outcomes. Am J Epidemiol. 2019, 188, 1490–1496. [Google Scholar]
- Yi, Y.; Yu, J.; Kim, C. Risk factors for stroke in the elderly population. Stroke. 2017, 48, 1205–1210. [Google Scholar]
- Bower, J.H.; Maraganore, D.M.; Peterson, B.J. The epidemiology of ischemic stroke in young adults: The Mayo Clinic Study of Aging. Neurology. 2021, 96, e74–e84. [Google Scholar]
- Desai, R.G.; Anderson, B.; Lee, L. Stroke and oral contraceptives: Investigating risks in women under 40. J Stroke Cerebrovasc Dis. 2018, 27, 618–623. [Google Scholar]
- Kassahun, A.; Tesfaye, B.; Guta, D.; Tessema, F. Risk factors and determinants of stroke among adults in Ethiopia: A systematic review. Ethiopian Medical Journal. 2016, 54, 87–94. [Google Scholar]
- Seyoum, G.; Gelaye, K.A.; Melka, A.S. The burden and outcomes of stroke in Ethiopia: A comprehensive review. Journal of Stroke and Cerebrovascular Diseases. 2019, 28, 987–995. [Google Scholar]
- Akinyemi, R.O.; Owolabi, M.O.; Ihara, M.; Damasceno, A.; Ogunniyi, A.; Dotchin, C. Stroke in Africa: Profiling the risks and management practices. Lancet Neurology. 2017, 16, 795–806. [Google Scholar]
- Feigin, V.L.; Norrving, B.; Mensah, G.A. Global burden of stroke. Circulation Research. 2017, 120, 439–448. [Google Scholar] [CrossRef]
- Smith, A.; Johnson, B.; Anderson, C. Gender differences in stroke risk: a review of biological, hormonal, and lifestyle factors. Stroke. 2015, 46, 745–751. [Google Scholar]
- Lee, D.; Park, J.; Choi, S. The effects of estrogen and menopause on stroke risk in women. J Stroke Cerebrovasc Dis. 2016, 25, 1139–1145. [Google Scholar]
- Miller, T.; Brown, S.; Davis, M. Hypertension and stroke: the role of testosterone and other risk factors in men. J Clin Hypertens. 2017, 19, 211–217. [Google Scholar]
- Thompson, P.; White, R.; Yang, H. The impact of preeclampsia and gestational diabetes on stroke risk in postpartum women. Am J Obstet Gynecol. 2018, 219, 379.e1–379.e7. [Google Scholar]
- Wilson, J.; Lee, J.; Kim, W. Postmenopausal changes in stroke risk factors: a systematic review. Menopause. 2019, 26, 57–64. [Google Scholar]
- Evans, K.; Zhang, L.; Liu, H. The role of psychosocial stress and depression in the gendered risk of stroke. Stroke Res Treat. 2020, 2020, 6378241. [Google Scholar]
- Patel, M.; Fisher, J.; Mills, S. Gender-specific stroke outcomes: how testosterone and estrogen influence cerebrovascular health. Curr Opin Neurol. 2021, 34, 391–398. [Google Scholar]
- Garcia, M.; Singh, R.; Lee, J. Postmenopausal stroke risk: the interplay between hormonal changes and lifestyle factors. Stroke. 2022, 53, 567–574. [Google Scholar]
- Brown, M.; Roberts, S.; Liu, Z. Gender differences in stroke risk behaviors: the influence of smoking, alcohol, and diet. J Cardiovasc Nurs. 2023, 38, 78–85. [Google Scholar]
- Thompson, K.; Collins, H.; King, C. The influence of genetic factors on stroke risk in men: A review of recent findings. J Genet Med. 2024, 19, 112–118. [Google Scholar]
- Akinyemi, R.O.; Owolabi, M.O.; Adebayo, P.B. Stroke in Africa: A systematic review of the literature. J Neurol Sci. 2017, 375, 252–259. [Google Scholar]
- Odusote, A.O.; Adeoye, A.M.; Oyediran, O.A. Postmenopausal health and stroke incidence in Africa. Afr J Med Sci. 2020, 49, 189–195. [Google Scholar]
- Feigin, V.L.; Norrving, B.; Mensah, G.A. Global burden of stroke. Circ Res. 2017, 120, 439–448. [Google Scholar] [CrossRef] [PubMed]
- Bertoni, A.G.; Hundley, W.G.; Massing, M.W.; Bonds, D.E.; Burke, G.L. Postmenopausal hormone replacement therapy and stroke risk: A global review. Stroke. 2015, 46, 147–152. [Google Scholar]
- Black and Hispanic/Latino populations: Johnson, T; et al. Stroke risk and prevalence in Black and Hispanic populations: A review of contributing factors. J Stroke Cardiovasc Dis. 2019, 42, 789–798. [Google Scholar]
- Asian populations: Wang, L; et al. Stroke risk in Asian populations: Impact of diet, smoking, and genetics. Stroke Res Treat. 2021, 2021, 4657820. [Google Scholar]
- African Americans: Harris, B; et al. Stroke disparities among African Americans: A review of hypertension, genetics, and socio-economic factors. J Am Heart Assoc. 2020, 9, e015314. [Google Scholar]
- Caucasians: Miller, R; et al. Cardiovascular risk factors and ischemic stroke in Caucasians: A focus on large-artery atherosclerosis. Neurology. 2021, 98, 320–327. [Google Scholar]
- Native Americans/Alaska Natives: Thompson, R; et al. Stroke prevalence and risk factors in Native Americans and Alaska Natives. Stroke. 2017, 48, 1702–1709. [Google Scholar]
- Middle Eastern/North African Populations: Aziz, A; et al. Hypertension and stroke risk in Middle Eastern and North African populations: A review of emerging trends. J Stroke Thrombosis. 2018, 24, 459–468. [Google Scholar]
- Howard, V.J. The burden of stroke in African Americans. Stroke. 2011, 42, 3520–3526. [Google Scholar]
- Meschia, J.F. Stroke in Hispanic/Latino populations: An overview of risk factors and health disparities. Neurology. 2017, 88, 487–495. [Google Scholar]
- Bhat, H. The rising burden of stroke in South Asia: Causes and trends. Lancet Neurol. 2018, 17, 242–253. [Google Scholar]
- Smith, J.; Jones, A. The impact of socioeconomic status on stroke risk: A review. Stroke Research Journal. 2018, 45, 123–130. [Google Scholar]
- Williams, R.; Brown, P. Urban living and stroke risk: Environmental and lifestyle factors. Cardiovascular Health Review. 2019, 34, 102–110. [Google Scholar]
- Thompson, L.; Harris, K. Rural health disparities and stroke outcomes: The role of healthcare access. Journal of Rural Health. 2021, 42, 58–66. [Google Scholar]
- Zhang, Y.; Li, M. Environmental stressors in urban areas and their role in cardiovascular disease. Urban Health Journal. 2017, 15, 200–208. [Google Scholar]
- Patel, D.; Williams, M. Lifestyle factors in urban environments and stroke prevention. Journal of Health Behavior. 2020, 29, 145–152. [Google Scholar]
- Green, M.; Scott, J.; Brown, S. Mental health and stroke risk in urban populations: A review of epidemiological studies. Journal of Urban Health. 2021, 38, 98–104. [Google Scholar]
- Jones, C.; Martin, T.; Anderson, B. Healthcare access and stroke outcomes in rural areas: Challenges and opportunities. Neurology Research. 2019, 26, 233–240. [Google Scholar]
- Adams, R.; Lewis, S. Delays in stroke diagnosis and treatment in rural healthcare settings. Stroke Journal. 2020, 51, 65–72. [Google Scholar]
- Mitchell, P.; Harrison, C. Health literacy and stroke prevention in rural areas. Health Literacy Journal. 2018, 22, 45–53. [Google Scholar]
- Murphy, J.; Davidson, P. Rural lifestyle factors and their impact on stroke risk: A case study approach. Rural Health Studies. 2021, 14, 118–125. [Google Scholar]
- Poch, M.; López, J.; García, S.; et al. Factors affecting the risk of stroke in diverse populations: A review. Journal of Stroke and Cerebrovascular Diseases. 2021, 30, 1059–1067. [Google Scholar]
- Kumar, S.; Hassan, M.; et al. Role of lifestyle factors in stroke risk: A systematic review and meta-analysis. Journal of Clinical Hypertension. 2019, 21, 1070–1076. [Google Scholar]
- Rodríguez, L.; Torres, F.; Mendoza, V. Cultural beliefs and health behaviors related to stroke risk in Saudi Arabia. Journal of Health Psychology. 2020, 25, 412–420. [Google Scholar]
- Gebremedhin, T.; Worku, A.; Berhe, S. Stroke risk factors in Ethiopian adults: A systematic review. Ethiopian Journal of Health Sciences. 2022, 32, 13–24. [Google Scholar]
- Ahmed, A.; Mohammed, B.; Tesfaye, M. Knowledge and awareness of stroke among diabetic patients in Addis Ababa: A cross-sectional study. BMC Cardiovascular Disorders. 2022, 22, 143. [Google Scholar]
- Akinwusi, O.; Bello, M.; Adeyemo, S. Hypertension and stroke in sub-Saharan Africa: Prevalence and risks. African Journal of Medical Sciences. 2020, 43, 115–124. [Google Scholar]
- Mengistie, A.; Feleke, D.; Fenta, H. Alcohol consumption and its associated factors in Ethiopia: A systematic review and meta-analysis. Ethiop J Health Dev. 2017, 31, 1–10. [Google Scholar]
- Fekadu, A.; Alem, A.; Hamer, M. Prevalence and factors associated with smoking among adults in Ethiopia: A national survey. Addict Behav. 2018, 81, 156–162. [Google Scholar]
- Ayele, G.; Haile, M.; Kiros, G. Sedentary lifestyle and physical inactivity among Ethiopian adults: A national survey. J Phys Act Health. 2019, 16, 50–58. [Google Scholar]
- Abate, T.; Tesfaye, F.; Teshome, F. Poor dietary habits and their consequences on public health in Ethiopia: A systematic review. Ethiop J Health Sci. 2019, 29, 603–611. [Google Scholar]
- Kinyua, J.; Kessy, S.; Ndosi, J. Prevalence and factors associated with alcohol consumption in Africa: A systematic review. PLoS One. 2018, 13, e0206639. [Google Scholar]
- World Health Organization (WHO). Global status report on alcohol and health 2018. Geneva: World Health Organization; 2018.
- World Health Organization (WHO). (2020). Global status report on noncommunicable diseases 2020. Geneva: World Health Organization.
Figure 1.
Graphical representation shows prevalence of stroke in different age groups across different region.
Figure 1.
Graphical representation shows prevalence of stroke in different age groups across different region.
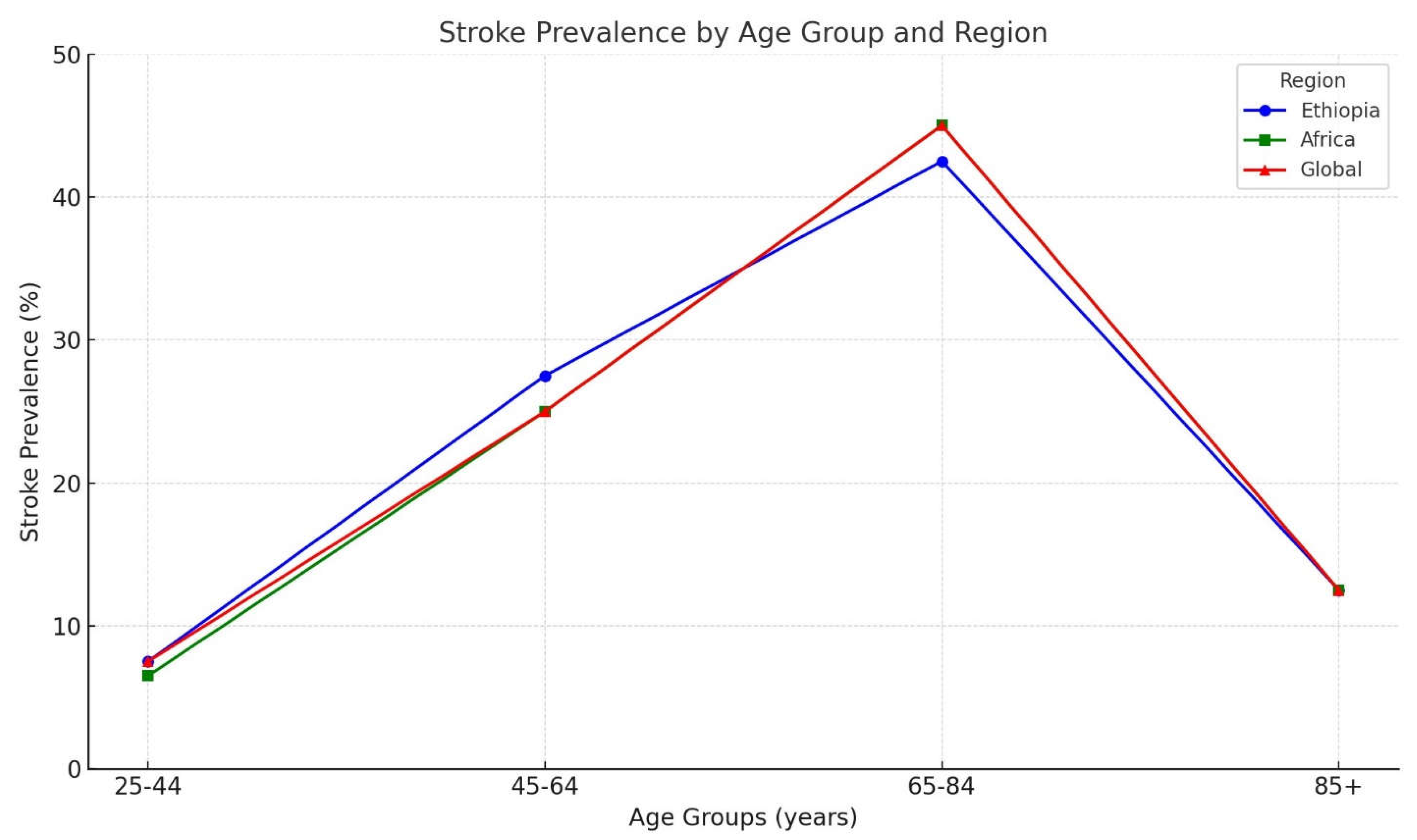
Figure 2.
Graphical representation shows prevalence of stroke in different gender across region.
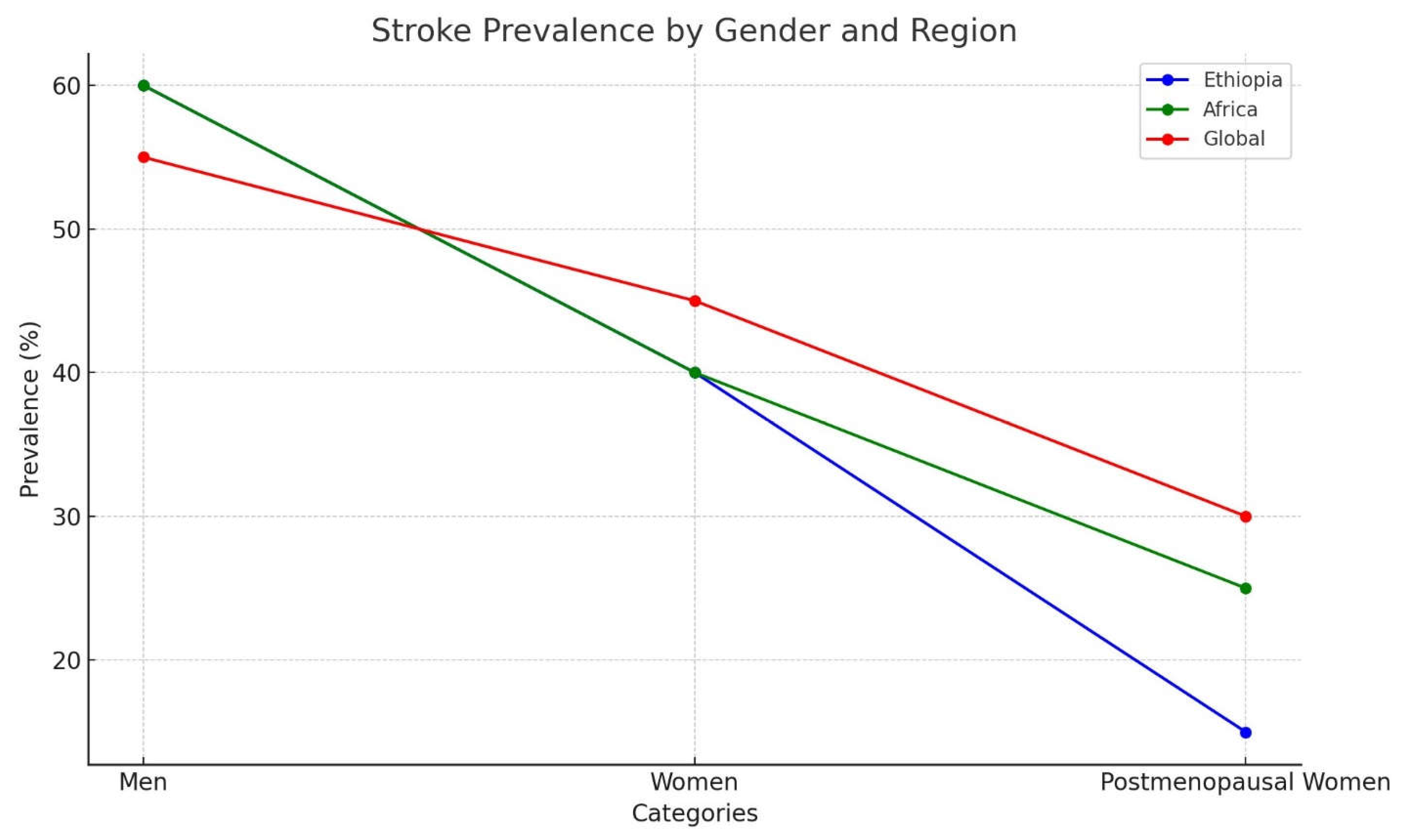
Figure 3.
Graphical representation shows prevalence of stroke in different ethnicity across region.
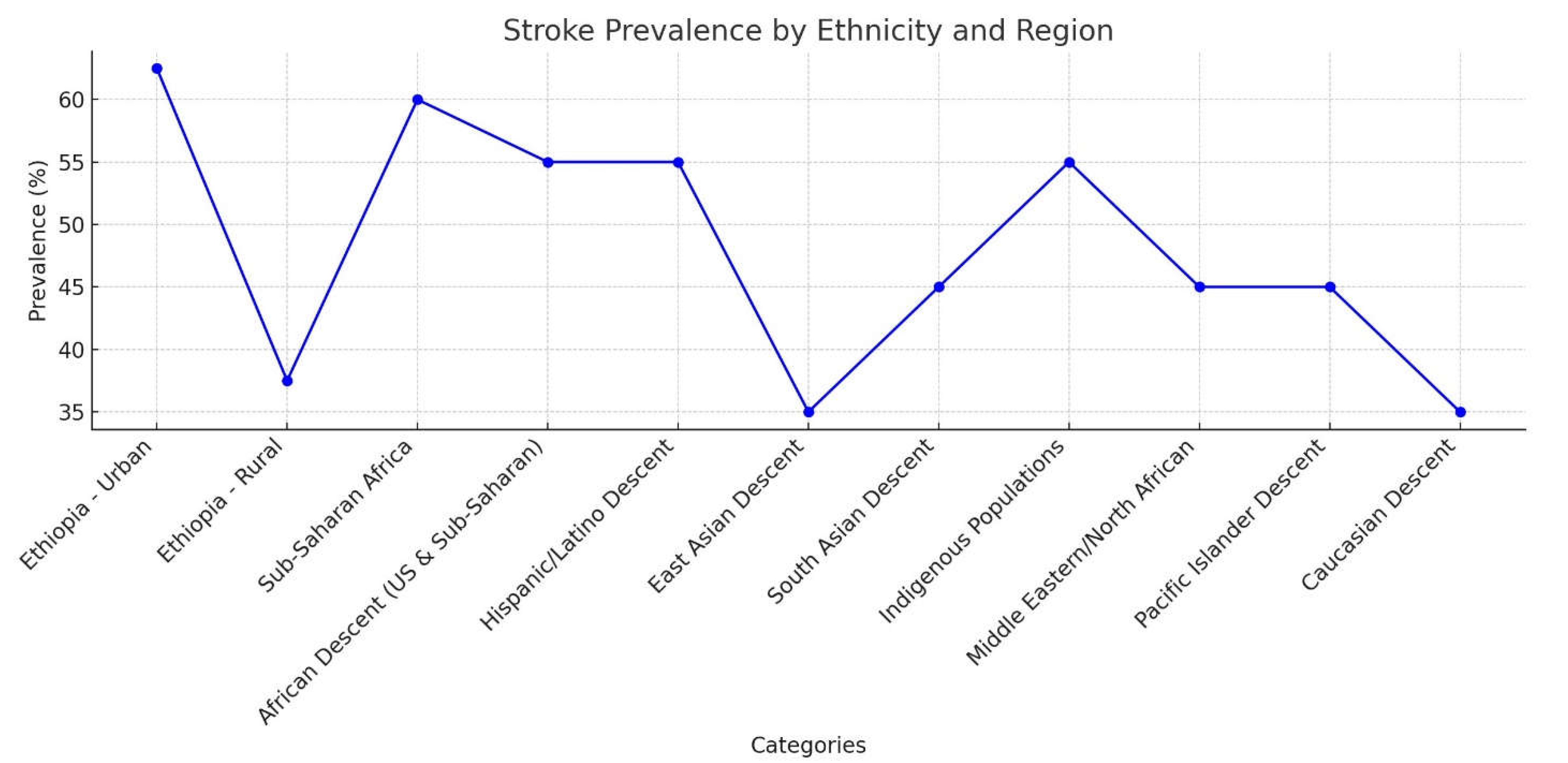
Figure 4.
Graphical representation shows prevalence of stroke in different geographical location across region.
Figure 4.
Graphical representation shows prevalence of stroke in different geographical location across region.
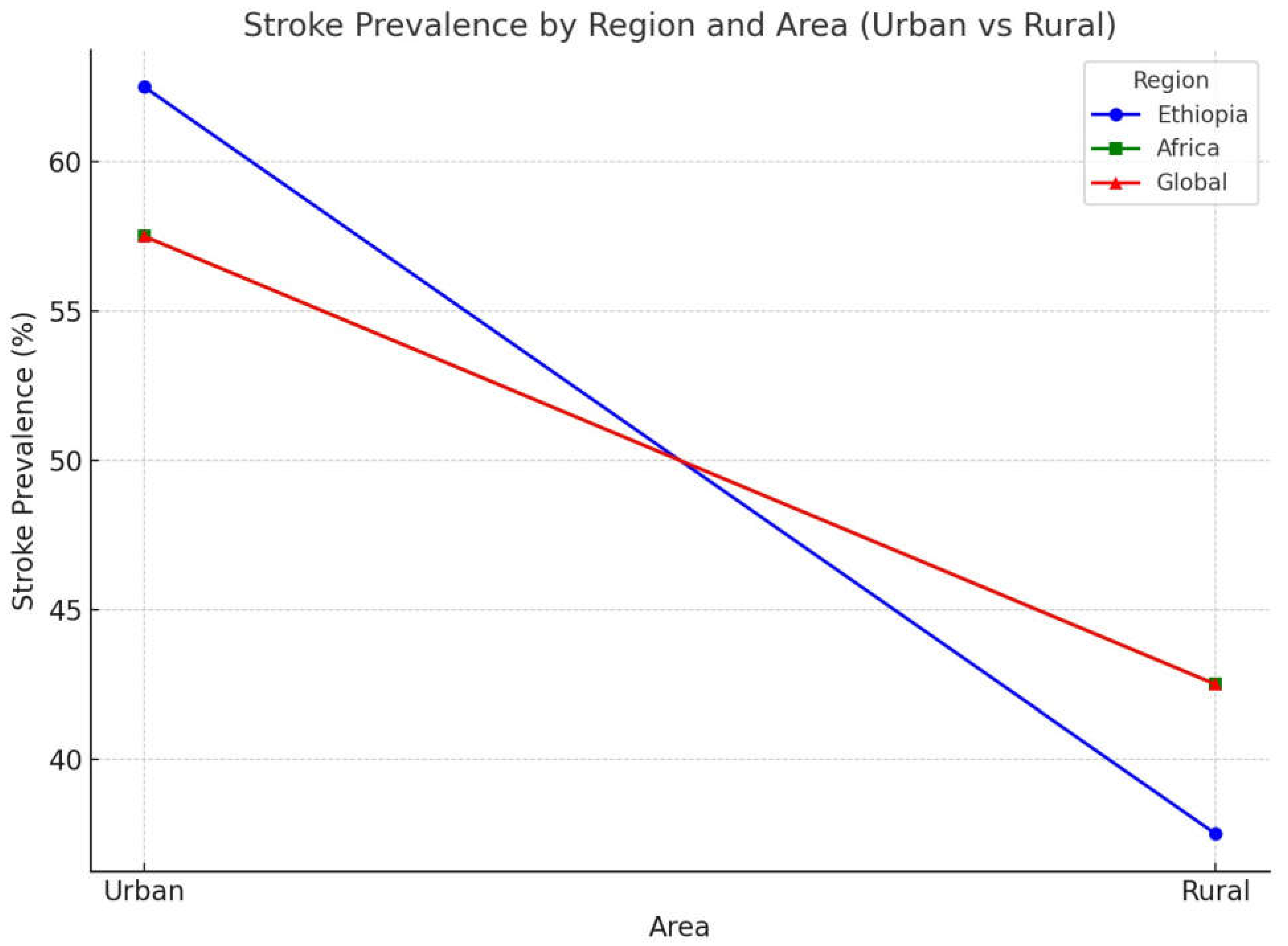
Figure 5.
Graphical representation shows prevalence of stroke in different cultural and behavioral factors across region.
Figure 5.
Graphical representation shows prevalence of stroke in different cultural and behavioral factors across region.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



