
Submitted:
31 March 2025
Posted:
01 April 2025
You are already at the latest version
Abstract
Systemic arterial hypertension (SAH), characterised by a persistent increase in blood pressure (BP) beyond the reference values for the species, is a concerning and detri-mental clinical condition. The aim of this manuscript is to present the state of the art on SAH in companion animals, including the different types of hypertension, diagnos-tic and therapeutic approaches, and the factors associated with its occurrence, such as the role of stress. It also discusses the benefits and challenges related to the measure-ment process. The SAH is categorised into types based on the underlying cause: situa-tional, secondary, and idiopathic (the least frequently observed). The situational type occurs when stress is the primary factor, such as during veterinary visits, contact with other animals, or in cases of white coat syndrome. If the stressor is removed, BP values tend to normalise. The most common type of SAH is the secondary form, which is as-sociated with an underlying condition, such as renal, cardiac, endocrine, or neurologi-cal diseases, or a combination of these. Diagnosing SAH is a challenging task for many veterinarians due to factors related to handling the animal, managing the equipment, and interpreting the results. Consequently, many professionals either take inaccurate measurements or misinterpret the results, often prescribing antihypertensive medica-tions prematurely or unnecessarily. Despite being a well-standardised and well-documented process, challenges persist. Treatment often involves antihyperten-sive drugs, either alone or in combination, alongside management of the underlying causes, when present. Therefore, BP values should be obtained correctly using a stand-ardised protocol, with clinical-therapeutic decisions carefully aligned with the factors that may influence them.
Keywords:
behavioural factors
; hypertension
; haemodynamics
; stress
; white coat syndrome
1. Introduction
Cardiovascular diseases are clinical conditions that can be either primary or secondary to other events. Regardless of how they are characterised, they are routinely observed. The presence of cardiovascular disturbances or alterations is marked by significantly deleterious and/or harmful situations, which can cause discomfort for both the patient and their caregiver. These may include physical and mental fatigue, as well as a reduction in quality of life and life expectancy [1]. Generally, depending on the disease progression and other associated factors such as age, breed, and the type of condition, animals may frequently experience decompensated episodes, which should be effectively managed to ensure success in diagnostic and therapeutic management. New characteristics of urban centres, such as verticalisation, methods of animal husbandry, and emotional/behavioural support, contribute to increased vigilance from caregivers in observing clinical conditions that interfere with the animals’ lifestyle, as well as a greater dedication to health-related matters [1]. Among the various cardiovascular conditions and alterations, congenital diseases, acquired conditions, and those associated with blood pressure are noted.
Systemic arterial hypertension (SAH) is a condition characterised by the elevation of blood pressure values above the reference values for the species, in a chronic manner. It can be classified into three types [1,2]. Frequently, most cases of SAH are associated with underlying causes such as renal, endocrine, or neoplastic diseases, among others. However, it is important to note that SAH can also be caused by situational factors, primarily induced by stress, as well as primary aspects (absence of underlying diseases). Stress is one of the main factors associated with situational hypertension, which is often observed in veterinary clinics and hospitals due to the occurrence of an exaggerated sympathetic discharge. When animals are exposed to unfamiliar situations, such as new environments, the presence of other dogs and/or cats, and various odours, the release of circulating catecholamines can occur, maintaining the sympathetic system in a state of alert [3]. Therefore, the clinical evaluation of animals in a state of stress may be under- or over-influenced, meaning that the variables collected may not reflect the true condition of the animal. It is expected that blood pressure values in dogs influenced by sympathetic activation will be higher when compared to patients in calmer environments. Thus, it is essential to consider stress during blood pressure measurement to minimise its effects as much as possible. According to Sousa et al. [1], “hypertension often presents silently, and as such, its identification by caregivers becomes imperceptible, as animals remain asymptomatic.” Diagnosing hypertension can be challenging, especially due to "white coat syndrome." It is emphasised that measurements should be taken in a standardised manner and at different times [2]. The diagnosis of hypertension can be established when elevated blood pressure values are consistently observed across multiple measurements taken at different times. Treatment is variable and depends partly on the pre-existing underlying cause, such as the use of blood pressure-regulating medications, either alone or in combination. The aim of this manuscript is to explore systemic arterial hypertension in companion animals, outlining its types, diagnostic and therapeutic approaches, associated factors such as stress, and the benefits and challenges of accurate and well-executed measurement.
2. Blood Pressure
The measurement of blood pressure (BP) has taken on an important role in veterinary medicine, and the recognition of systemic hypertension in dogs in recent years underscores the importance of this measurement being performed in a systematic and standardised manner. Notably, understanding blood pressure and its disorders in companion animals, as well as the technology for its measurement, has evolved over time [2]. The measurement of BP in dogs and cats is a method derived from human medicine, with the first recorded blood pressure measurement taking place in 1733 by Stephen Hales using an invasive method (later described) in a mare. Later, around 1895, the Italian Riva-Rocci determined blood pressure through digital palpation. The significant achievement of the auscultatory method was made by the Russian Korotkoff, crowning medicine with an examination of great importance and implications in various diseases [4,5,6]. Given the prominence of blood pressure evaluation, several studies and guidelines similar to those developed for humans have been conducted and published in veterinary medicine, such as the Consensus Statement of the American College of Veterinary Internal Medicine (ACVIM). Moreover, there is a strong emphasis on veterinarians using BP measurement as a requirement to be evaluated during medical consultations, given that more than 80% of hypertensive cases are secondary to other diseases [7]. Consequently, understanding blood pressure and its consequences in companion animals becomes fundamental in attempting to predict the potential developments of elevated blood pressure.
Cardiovascular function is based on central strategies with the ultimate goal of ensuring adequate blood volume supply that can promote proper cardiac pumping, oxygenation, nutrition, and tissue and/or organ perfusion [8,9,10]. For this, intrinsic and extrinsic regulatory processes are required. For proper cardiac pumping, there must be cardiac output (CO) and venous return (VR); however, depending on the present condition, haemodynamic variations may occur [9]. Such modifications are mediated by need, so that the greater the volumetric demand (e.g., intense physical exercise), the greater the amount of blood supplied [8]. Situations involving variability in preload and afterload values may lead to haemodynamic modifications, with the potential for organ depletion and/or damage [8].
Blood pressure dysregulation is swiftly controlled by the activation of compensation mechanisms, whether acute or chronic, aimed at controlling or halting the causal process. It is important to emphasise that although compensatory, cardiovascular afflictions are progressive, which can aggravate the problem through hyperactivation of regulatory mechanisms, leading to harmful and detrimental processes [8,9,10]. Several haemodynamic regulatory processes are described, such as the Frank-Starling and Laplace laws, the sympathetic nervous system (SNS), and the activation of the renin-angiotensin system (RAS), as well as acute or long-term local controls (e.g., vasodilatory theory, oxygen demand), among others [8,9]. Regardless of the type of regulation, whether isolated or not, the central goal is to regulate and maintain haemodynamic status to avoid temporary and/or permanent damage and loss [8,9].
In this context, the blood pressure values of dogs and cats are variable, and various factors, such as the skill of the operator performing the measurement, the method employed, the behaviour of the animals, and the choice of cuff, can interfere with the results [2]. Therefore, standardising the measurement process to reduce measurement bias is strongly recommended [2]. Other variables such as the animal's size, breed, sex, body condition, and environment can also cause blood pressure variability [2,11]. In humans, age is a variable that affects arterial structure, which could explain why elderly individuals tend to have higher blood pressure values [12]. According to Acierno et al. [2], the effect of age on the blood pressure of dogs remains under-studied. Bodey & Michell [13] found evidence of an annual increase in blood pressure of approximately 1-3 mmHg. This phenomenon was also described by Bodey & Sanson [14], Bright & Dentino [15], and Payne et al. [16]. Bijsmans et al. [17] conducted an experiment with senior cats to evaluate if blood pressure increased with age and observed that blood pressure values were higher in felines over 9 years old, particularly in those with underlying disease.
Regarding sex, there are still gaps in fully understanding the influence of sex on blood pressure values [13,18,19]. Bodey & Michell [13], after analysing more than 1,900 dogs, found that sex influenced blood pressure, with lower BP observed more strongly in females. It is important to note that the difference in blood pressure between neutered and intact individuals was 10 mmHg [13]. According to Bodey & Sansom [14] and Mishina et al. [20], the influence of sex is not well-established in studies because many studies work with neutered animals, reducing the influence of sex hormones. Payne et al. [16] found that, in cats, the average blood pressure was higher in males compared to females (122.2 mmHg vs. 119.6 mmHg), with the increase being more pronounced in neutered cats. Breed is strongly associated with blood pressure, with Acierno et al. [2] suggesting that BP should be described by breed. Some studies have shown that Greyhounds and Great Danes have BP values 10-20 mmHg higher than mixed-breed dogs [13,18]. Bodey & Rampling [21] highlighted that hunting dogs had higher BP values than retriever breeds. However, according to Payne et al. [16], the racial component is still not well-defined. For Bodey & Michell [13] and Rattez et al. [22], blood pressure can also vary with temperature values, with fluctuations of around 7-10 mmHg. However, most studies do not assess the influence of temperature on blood pressure. According to Bodey & Mitchell [13], "systolic blood pressure is the most variable pressure parameter and depends on age, breed, sex, temperament, disease status, exercise regimen, and, to a lesser extent, diet," indicating that blood pressure variability is influenced by numerous causes. The relationship between obesity and blood pressure in SAH has been demonstrated in various studies [23,24]. According to Mendes et al. [25], "obesity is associated with chronic cardiac volume overload, increased cardiac output, and activation of the renin-angiotensin-aldosterone system (RAAS) and the sympathetic nervous system (SNS)."
The influence of obesity on blood pressure is often associated with underlying cardiovascular repercussions [19,26]. In the study by Pereira-Neto et al. [26], the authors observed that the presence of adipose tissue influenced blood pressure measurements, as the vascular method showed differences compared to the oscillometric method in obese dogs. In the study by Payne et al. [16], the "body condition" factor was correlated with blood pressure values, with cats scoring below ideal (4/9) showing lower blood pressure values compared to those with scores of 5 or higher. Rondeau et al. [27] and Mooney et al. [28] described that sarcopenic processes and muscle evaluation can lead to variability in blood pressure values, especially if measured in the radial artery. In general, Acierno et al. [2] emphasise that "blood pressure measurement results in normal animals are highly variable based on breed, temperament, patient position, measurement method, operator experience, and intra-patient variability, making it difficult to determine a single value or range that applies to all dogs or cats."
3. Systemic Blood Pressure Regulation Systems
The BP can be regulated locally and/or systemically through the activation of compensatory and regulatory systems [10]. Pressure compensation is based on physiological strategies, both short-term and long-term, aimed at stabilising the body in response to the newly imposed condition. Intrinsic and extrinsic mechanisms may be activated, either independently or together, to support the organ system and prevent the onset or worsening of secondary conditions resulting from pressure fluctuations, such as hypoxia and tissue/organ ischaemia [8]. The primary regulatory systems are the sympathetic nervous system (SNS) and the renin-angiotensin system (RAS).
3.1. Sympathetic Nervous System
The SNS, along with the parasympathetic nervous system (PNS), forms the autonomic nervous system, with the former exerting a more significant regulatory effect on BP. Neural control of BP is governed by the nervous system, which regulates blood flow, pressure, and cardiac function, alongside the presence of sympathetic fibres that induce changes in volumetric and peripheric vascular resistance (PVR) [10]. Primary regulation via the SNS is associated with a greater number of sympathetic fibres, resulting in heightened responsiveness of various parts of the body, such as the kidneys, skin, and intestines, to norepinephrine [29]. The system is activated in response to a drop in BP and changes in the distensibility of blood vessels, conditions promptly detected by baroreceptors, which transmit information via afferent pathways to the brainstem (vasomotor centre), facilitating the release of norepinephrine and its binding to alpha-1 receptors (Figure 1) [29]. Following this process, the smooth muscle layers of the arteries contract, increasing PVR. Additionally, there is an enhancement in the automaticity of the sinoatrial node, resulting in an increased heart rate, cardiac output, stabilisation of vascular resistance, and the re-establishment of haemodynamic balance [29]. However, while these haemodynamic adjustments are initially beneficial, as the system becomes hyperactivated, there is impairment in the relaxation and volumetric accommodation phases, leading to cardiac cycles with lower cardiac output and reduced perfusion [9,10]. In this regard, Sousa [10] emphasises that the system ceases to be beneficial and, over the long term, becomes detrimental.
3.2. Renin Angiotensin System
The RAS is another compensatory organ system that can be activated locally and/or systemically, playing a key role in compensating for haemodynamic changes, particularly through renal function [10]. The function of the RAS is based on blood pressure regulation [30,31,32,33], PVR regulation [34,35], and the maintenance of hydroelectrolytic balance 31,36,37]. Activation of the RAS is triggered by conditions related to organic, tissue, and haemodynamic disturbances [38]. RAS compensation can be acute and/or chronic; however, most compensation arises from chronic activation [32,34]. According to Sousa [10], compensation is initially beneficial to organic control; however, over time, as the condition progresses, the RAS becomes a detrimental and harmful system. McKinney et al. [31] argue that the system becomes damaging when there is persistent tissue damage and/or injury, along with hyperfunction and hyperactivity of the cardiorenal system, as well as organic imbalance. As a pleiotropic system, compensation occurs through the reduction of blood pressure and alterations in water and electrolyte availability, with the kidneys (macula densa) detecting these changes [10,39,40]. According to Vargas et al. [41], the juxtaglomerular cells, located in the middle of the afferent arterioles [36], detect the decrease in circulating sodium and chloride ions in the distal convoluted tubule [37], which triggers the conversion of prorenin to renin (34,36,42]. It is renin that initiates the entire compensatory process via the RAS after stimulation [40].
Renin facilitates the breakdown of angiotensinogen into angiotensin I (which has low vasoconstrictor activity) [10,33,34,35,38,40,42,43,44,45,46]. Angiotensin I is quickly converted into angiotensin II by the angiotensin-converting enzyme (ACE) [38]. Once formed, angiotensin II plays roles in blood pressure control, cardiac adjustment, haemodynamic regulation, and electrolyte balance [36]. Much of the effects of angiotensin II are variable and associated with vascular, nervous, and hormonal actions, cardiovascular remodelling, as well as free radicals and reactive oxygen species [10]. It is emphasised that, according to Sousa [10], the effects mediated by angiotensin II and the compensatory RAS system are initially beneficial; however, as the condition worsens, clinical changes become evident and extremely harmful to organic balance. Figure 2 summarises the RAS system.
4. Systemic Arterial Hypertension
The SAH is a clinical condition characterised by persistently elevated blood pressure values in relation to the reference parameters for the species [2]. However, according to Sousa et al. [1], the diagnosis of SAH should be based on certain factors that could interfere with obtaining reliable values. Therefore, the diagnosis should be based on measurements that are in accordance with the environment and the behaviour of the animal, “in order to avoid underestimating or overestimating blood pressure values” [1]. Currently, conditions of measurement, waiting for clinical attention, patient management, interaction with other animals and/or species during pre-consultation periods, transportation, and acclimatisation to the environment are factors that influence blood pressure [1]. In this context, it is emphasised that the identification of SAH should be approached with caution, supported by clinical evidence, and in accordance with the animal’s environment and behaviour, as pharmacological therapy should only be administered after the diagnosis.
According to Acierno et al. [2], SAH can be subclassified into three types: situational, idiopathic, and secondary. The categorisation process was based on the presence of situations that led to blood pressure changes but which could have another underlying cause, such as stress, conditions that cause vascular and haemodynamic alterations, or periods when potential causes were ruled out, and blood pressure values remained elevated [1]. It should be noted that many professionals, unfortunately, still make incorrect diagnoses of SAH due to factors such as errors in the measurement process, single and isolated measurements, or failure to consider influencing factors. As a result, the existence of inaccurate diagnoses affects clinical and therapeutic management.
4.1. Situational Arterial Hypertension
Situational SAH is characterised by a temporary or momentary increase in blood pressure, often triggered by the presence of one or more stress-inducing factors [1,47]. According to Acierno et al. [2], it is "caused by alterations in the autonomic nervous system resulting from the effects of arousal or anxiety on the higher centres of the central nervous system." Sousa et al. [1] state that this form of hypertension is frequently observed in veterinary clinic and hospital settings and is associated with the "white coat syndrome." Data suggests that the sight of individuals wearing white attire can induce a certain repulsion, which may explain the occasional increases in blood pressure.
As noted by Lyberg et al. [11], factors such as veterinary environments, the process of acclimatisation in transport boxes, transportation, waiting, and return to the home environment can contribute to temporary increases in blood pressure values. The auditory and olfactory influence of animals' exposure in veterinary clinics and hospitals should also be emphasised. The unfamiliar environment and the physical restraint for clinical and supplementary assessments can affect temporary hypertension [1]. It is certain that blood pressure values obtained may be influenced, potentially leading to underestimation or overestimation [11] (Figure 3).
4.2. Idiopathic Arterial Hypertension
Idiopathic SAH, or true hypertension, is characterised by a persistent increase in blood pressure values, provided that contributing factors such as stress and secondary diseases are ruled out. Idiopathic hypertension is associated with intrinsic and/or extrinsic variables, lacks an underlying cause, and, given that a significant number of animals present with clinical conditions that interfere with their haemodynamic status, its diagnosis can be challenging [2]. Moreover, according to Acierno et al. [2], "the presence of chronic hypertension suggests that one or more of the neuro-humoral and renal systems responsible for regulating blood pressure are abnormal," once again highlighting the influence of the cardiovascular-renal-neuroendocrine axis in the occurrence of hypertension. The diagnosis of true hypertension focuses on excluding all potential causes of hypertension, with the aid of diagnostic tests that rule out hepatic, renal, endocrine, and other alterations [2]. Specifically for felines, approximately 13-20% of these cases are idiopathic hypertension [48,49,50] (Figure 4).
4.3. Secondary Arterial Hypertension
The most frequently diagnosed form of SAH is secondary hypertension, which arises from an underlying cause, typically linked to a specific clinical condition. According to Acierno et al. [2], this condition is characterised by a consistent increase in blood pressure resulting from a baseline condition that is sufficiently capable of elevating blood pressure values. It is important to highlight the role of certain medications and neoplasms in this form of hypertension [2]. Such increases in blood pressure, caused by an underlying condition, are more commonly observed in middle-aged and geriatric patients, as diseases related to hypertensive phenomena, such as CKD and endocrinopathies, are frequently seen [2]. Often, secondary hypertension presents as clinical symptoms rather than as an isolated clinical condition. Even though therapeutic management of the underlying cause may be implemented, blood pressure control may not always be effective. In some cases, blood pressure values may not decrease, may return to reference levels, or may even increase [51,52]. Due to the presence of an underlying cause, continuous clinical and laboratory monitoring is necessary. A study by Sparkes et al. [53] confirmed the influence of underlying conditions in the onset of hypertension, particularly the concomitant presence of chronic kidney disease (CKD) and/or hyperthyroidism (Figure 5).
5. Stress and Catecholamine Release
Stress is a physiological response of the organism to situations that induce overactivation and the release of circulating catecholamines. These stress responses can be triggered by various conditions, such as blood sample collection, fight-or-flight situations, and conflicts with other animals. Since 1998, Broom [54] has defined stress as an organic reflex triggered by the perception of an event considered an obstacle to the animal's equilibrium, initiating both behavioral and physiological changes to confront the stressor. Lucassen et al. [3] further describe stress, noting that aversive, unpleasant, or threatening situations activate the organism in response. According to Mârza et al. [55], stress is often linked to environmental factors, where poor environmental enrichment, spatial restrictions, and limited sensory and cognitive stimulation are common stressors. Broom [54] and Mârza et al. [55] highlight that stress can be acute or chronic, with continuous hyperactivation and hypervigilance being more harmful than transient, short-lived situations. Thus, while stress is a physiological response to an inciting event, its impact can have significant detrimental effects.
Lucassen et al. [3] describe stress as mediated by two responses: the alarm phase and the glucocorticoid-regulated phase. The first phase, the alarm phase, is based on the fight-or-flight response mediated by the sympathetic nervous system (SNS), which leads to the release of epinephrine and norepinephrine. These hormones trigger organic changes such as increased metabolism, blood pressure, and respiration, as well as heightened vasoconstriction, which redirects blood flow to vital organs like the brain and muscles. The second phase involves the release of glucocorticoids (e.g., cortisol), which help the organism adapt to the stressor by influencing metabolic variables [3].
Stress in veterinary medicine has become an area of growing concern, especially as pet owners increasingly focus on their animals' well-being. Companion animals, for example cats and dogs, face multiple stressors in various situations, including veterinary evaluations, transportation to veterinary clinics, exposure to odors, physical restraint for examinations, and unfamiliar environments. Especially in cats, the stress component is more commonly observed, particularly in relation to containment and handling processes. This justifies the use and need for CatFriendly practices to ensure a lesser negative impact during veterinary evaluations. Additionally, animals subjected to continuous stress, such as those in poor living conditions (e.g., chained, confined to small kennels with poor hygiene, or lacking socialization), are also notably affected. In veterinary settings, stress can complicate or even prevent the proper conduct of clinical and supplementary examinations, leading to potential diagnostic and therapeutic errors. Lee et al. [56] found that environments with ample space, socialization opportunities, and environmental enrichment strategies were associated with reduced stress.
Research by Vincent & Michell [57] showed that animals prone to stress could exhibit elevated blood pressure levels. Stress is a significant factor contributing to situational hypertension, particularly in association with "white coat syndrome," where physiological responses are triggered in dogs upon encountering the white coat, due to fear, aversion, or hypervigilance. This suggests that animals under stress are experiencing momentary organ hyperfunction, making blood pressure measurement in these situations inadvisable. Situational hypertension tends to resolve once the causal stressors are controlled or eliminated, reducing or eliminating physiological stimuli with an anxiolytic effect [2]. Acierno et al. [2] recommend that blood pressure measurements be taken after a 10-15 minute acclimatization period to allow stressors and circulating catecholamine levels to decrease. It is notable that blood pressure measurements can exhibit significant variability depending on the environment in which they are taken. In human medicine, the phenomenon of “masked hypertension” may occur, where a patient’s blood pressure readings decrease upon entering a hospital setting [58,59]. Given this possibility, home blood pressure monitoring has been considered a complementary or auxiliary assessment method [58,59]. However, this period may sometimes be insufficient for these changes to occur. In some cases, blood pressure measurements at home, where animals are in a familiar environment, can provide more accurate readings [2].
Studies highlight the variability in blood pressure readings between different environments, with values generally lower at home. Soares et al. [60] compared blood pressure readings in 45 dogs and found the mean blood pressure at home was 136.3 mmHg, while in the veterinary office it was 154.7 mmHg, with the environmental variable being the most likely cause of the difference. Preliminary results from Queiroz et al. [61] indicated that the mean hospital blood pressure was 189.5 mmHg, while home readings were within the species' reference range (138 mmHg). Queiroz et al. [61] attributed this blood pressure variability to stress, suggesting that environmental factors contribute to the increase in values. Koo & Carr [62] also found that both systolic and diastolic blood pressure were higher in a veterinary office, likely due to "white coat syndrome." Given these findings, it is essential to consider the environmental variable, whether associated with stress or not, before making diagnostic and therapeutic decisions regarding hypertension. Since situational hypertension is temporary and caused by stress without underlying issues, therapeutic management is not required. Instead, the focus should be on monitoring and re-measuring after the stressor is removed or controlled [62]. Identifying the specific stressor responsible for the changes is crucial, as each animal responds differently, making it challenging to pinpoint the exact cause. Sousa et al. [1] emphasize that many professionals are unaware of how catecholamines and stressful events influence cardiovascular hemodynamics. This lack of understanding could lead to unnecessary prescriptions of antihypertensive drugs.
6. Laboratory Biomarkers of Stress
6.1. Cortisol
In addition to catecholamines, which play a crucial role in stress development, cortisol is another important factor. Cortisol is a glucocorticoid produced by the adrenal glands, and it is involved in the body's regulatory processes, playing a key role in the stress response [55]. The role of cortisol in veterinary practice gained prominence due to its impact on endocrine and behavioral disorders, and it is often considered a biomarker of stress [55,63]. However, it’s important to note that elevated serum cortisol levels do not necessarily lead to negative outcomes, especially in animals for whom alertness is essential, such as hunting dogs or guide dogs for the visually impaired [55,64].
Cortisol is produced in the fasciculata region of the adrenal glands in response to corticotropin-releasing hormone and adrenocorticotropic hormone (Figure 3) [65,66]. The presence of adrenocorticotropic hormone stimulates cortisol production and release into the bloodstream, which is necessary for dogs to manage stress and regulate metabolic and immune functions [55]. Cortisol levels can be influenced by various factors, including the environment, physiological states, and behavior, making its regulation a complex process [55,63].
Cortisol is regulated by a feedback loop involving the hypothalamic-pituitary-adrenal axis, which is crucial for the body’s adaptation to stress, both acutely and chronically (Figure 3) [8,55]. Environmental factors also influence cortisol levels, with positive interactions and the presence of owners helping to reduce circulating cortisol levels, while the opposite can be true as well [55]. Petterson et al. [67] suggest that cortisol levels in both owners and animals can be influenced by how they interact and respond to each other. This environmental influence may also explain why blood pressure measurements are typically lower at home compared to veterinary offices or hospitals, as the home environment is more familiar and comfortable. It is also important to note that cortisol levels can fluctuate throughout the day, particularly in high-competition environments, such as when animals compete for space, food, or during testing [55,63] (Figure 6).
From a behavioral perspective, cortisol measurements are valuable for assessing the environment in which animals are placed, as well as the strategies for veterinary assessment and management. It can also help monitor strategies aimed at stress reduction [55,63]. Mârza et al. [55] discuss how individuals may exhibit behavioral differences, which can be categorized as the "shy versus bold behavioral syndrome." "Bold" animals tend to be more exploratory and risk-prone, while "shy" animals are more cautious and risk-averse. These differences are linked to cortisol responses, with "bold" animals showing larger increases in cortisol levels (due to lower baseline levels), whereas "shy" animals show smaller increases due to higher baseline levels. The behavioral characteristics of each animal may influence their response to stress and coping mechanisms. Furthermore, Mârza et al. [55] explain that cortisol regulation is influenced by both environmental and social factors, and dysregulation can affect stress dynamics and overall physiological functioning.
Cortisol levels can be measured using various methods, such as blood, saliva, urine, hair, and fecal samples. For stress assessment, cortisol is a prominent biomarker, as it reflects both stress levels and overall well-being [55]. Rosado et al. [68] highlight that elevated cortisol levels can also be linked to territorial dominance. Each method of cortisol measurement has its specific advantages and challenges. Blood sampling is an invasive technique that may cause temporary stress following collection, but it provides definitive results [69,70]. Saliva samples are less invasive and can offer insights into immediate stress levels [55,71,72].
Urine samples can also be used to measure cortisol, though they are more useful for detecting chronic stress [55]. The cortisol-to-creatinine ratio in urine is particularly valuable for evaluating cortisol, especially in endocrine conditions [55,73]. However, urinary cortisol measurements are more commonly used for assessing chronic stress rather than acute stress [55]. It’s worth noting that cortisol measurements in urine can vary by breed; for example, Akita dogs tend to have higher cortisol levels compared to Labrador Retrievers, as shown by Nagasawa et al. [74]. For chronic stress evaluations, hair and fecal samples are also useful [75]. The choice of method depends on the context and the type of stress being evaluated.
6.2. Glucose
Laboratory changes in glucose levels are commonly observed during stressful situations. According to Hagley et al. [76], episodes of hyperglycemia can occur as a result of stress, even in the absence of underlying diseases. Magomedova & Cummins [77] explain that the increase in serum glucose due to stress is part of an organic response, where the central nervous system stimulates the hypothalamic-pituitary-adrenal axis. Additionally, Liu et al. [78] describe an increase in serum glucose mediated by the hypothalamic-sympathetic-liver axis, without necessarily involving adrenal function during stress, as shown in a murine model. This mechanism is known as "stress-induced hyperglycemia" [76], and it is frequently observed in cats [79,80].
The "stress-induced hyperglycemia" mechanism, as described by Rand et al. [79], leads to a transient increase in glucose levels, which can sometimes cause confusion in the diagnosis of diabetes mellitus. Liu et al. [78] explain that, during acute stress, the body releases glucose into the bloodstream to ensure an energy reserve. This excessive release of blood glucose is understood in the context of survival mechanisms between predator and prey [78]. In such predatory situations, the vulnerable prey must have higher glucose levels to fuel an escape response. Liu et al. [78] suggest that "stress-induced hyperglycemia" occurs in stages: the rapid stage (around 3 minutes), driven by the hypothalamic-sympathetic-liver axis; the delayed stage (3-30 minutes), mediated by the adrenal glands; and the late stage (15 minutes), influenced by the hypothalamic-pituitary-adrenal axis, completing within 45 minutes.
Thus, the occurrence of hyperglycemia is linked to the presence of corticosteroids in the bloodstream, which promote gluconeogenesis and the release of glucagon [81]. This process causes insulin resistance, meaning that insulin is unable to regulate blood glucose levels, allowing for a transient accumulation of glucose [81]. Certain stress-inducing situations in dogs, such as those caused by heat, may also lead to changes in glucose levels. Azeez et al. [82] observed that in environments with high temperature and relative humidity, glucose levels were lower compared to environments with lower humidity, which also affected cortisol levels. While the pathway of hyperglycemia during acute stress is well-documented, few studies have focused on this relationship in veterinary patients.
6.3. Stress leukogram
The stress leukogram is a laboratory condition that occurs in animals experiencing high levels of stress, characterized by changes in hematological components such as neutrophils, eosinophils, lymphocytes, and monocytes [83]. This condition is typically observed in animals under stress, often in situations that complicate sample collection, such as restraint or repeated blood draws. While the stress leukogram is more commonly seen in felines due to their inherent stress sensitivity [84], it can also occur in dogs and influence diagnostic and therapeutic decisions.
Physiological stress, a specific type of stress, is associated with the production of adrenocorticotropic hormone and the release of cortisol. These hormones can affect various cellular groups, including lymphocytes, neutrophils, monocytes, and eosinophils [83]. The most common alteration in a stress leukogram is lymphopenia, which results from lymphocyte death, along with a shift in cell populations [83]. Additionally, neutrophilia may occur, manifesting as an increase in neutrophil numbers without a shift, with the neutrophils often appearing hypersegmented [83]. Eosinopenia is another common feature, due to the influence of cortisol, and monocytosis can also be observed [83]. Although platelet aggregation is not officially classified as part of the stress leukogram, it can still provide valuable insight into the animal's stress levels during sample collection. A study by Benjamin et al. [85] showed a reduction in platelet aggregates in patients following the administration of trazodone, suggesting that pharmacological tranquilizers can mitigate platelet alterations caused by stress.
7. Diseases Associated with SAH
The SAH can be associated with a variety of underlying conditions, and it is crucial to confirm or rule out these causes before making a definitive diagnosis of elevated blood pressure. These conditions often have different levels of cardiovascular repercussions, which can lead to clinical alterations in various physiological aspects. Hemodynamic changes, the effects of urinary conditions linked to the heart-kidney axis, hormonal influences, and toxicity from harmful substances are all factors that can contribute to cardiovascular changes, potentially triggering hypertension. Therefore, it is essential to suspect and thoroughly investigate the presence of these conditions.
7.1. Chronic Kidney Disease (CKD) and Urinary Disorders
The CKD and its associated urinary manifestations are primary underlying causes of hypertension [86], characterized by both functional and structural kidney failure. According to Sousa et al. [1], CKD is marked by a "failure in the excretory, regulatory, and endocrine functions of the kidneys." Lawson & Jepson [87] define the diagnosis of CKD as the presence of renal alterations lasting for more than three consecutive months. Animals affected by CKD often experience significant morphofunctional changes, including the replacement of nephric tissue with fibrous mass, which impairs renal function [1]. Several conditions associated with CKD, such as alterations in sodium concentrations, glomerular filtration rate (GFR), glomerular hypertension, supernephrons leading to higher filtration rates, and renal sclerosis, contribute to the development of hypertension [1]. Notably, these conditions are frequently accompanied by proteinuria, which can vary in severity depending on the stage of CKD [88]. Moreover, the influence of the SNS, RAS, vascular changes, and reduced levels of vasodilators play key roles in the pathophysiology of both CKD and hypertension [87,88,89]. Hypertension is commonly observed in patients with CKD [53].
7.2. Endocrine Disorders
Endocrine diseases such as hyperthyroidism, diabetes mellitus, hyperaldosteronism, and hyperadrenocorticism are conditions frequently associated with blood pressure alterations [1]. Hyperthyroidism, characterized by excessive production of thyroid hormones, is more commonly observed in felines [91]. Thyroid hormones are believed to influence inotropic and chronotropic actions [92], with increased sensitivity of catecholamines to adrenergic receptors. This leads to an elevation in heart rate and contractility [93]. Williams et al. [94] note that hypertension in hyperthyroid animals is often linked to associated conditions rather than the disease itself, though blood pressure tends to improve following treatment [95].
Diabetes mellitus, a complex and multifactorial condition characterized by impaired insulin production and/or action, is also associated with hypertension [96]. Reusch et al. [7] point out that the origin of hypertension in diabetes is not fully understood, although reduced vasodilation due to insulin deficiency is suggested as a potential cause. Acierno et al. [2] report that hypertension occurs in 35-46% of diabetic cases. Hyperaldosteronism, which involves excessive aldosterone production by the adrenal glands, leads to hypertension through hydroelectrolytic and hemodynamic alterations, such as increased sodium retention and PVR [7].
The primary condition causing hypertension in animals is hyperadrenocorticism, which is characterized by excessive glucocorticoid (mainly cortisol) production and is most commonly seen in dogs [97,98,99,100]. In cases where hyperadrenocorticism is ACTH-dependent, hypertension is observed in 86% of untreated cases, and even when treated, hypertension may remain persistent [52,101]. Goy-Thollot et al. [52] suggest that elevated cortisol levels may influence the vasculature, contributing to hypertension. Chen et al. [102] found that blood pressure in dogs with hyperadrenocorticism was higher than in control groups. Evidence points to superactivation of the RAS and increased vascular sensitivity to angiotensin II, contributing to blood pressure variability in these dogs [52,101], although further research is needed [93].
7.3. Neoplastic Causes, Drugs and Toxins
The SAH can also be mediated by factors such as neoplasms, drugs, and toxins, making it crucial to investigate the use of these substances. One example is pheochromocytoma, a neoplasm of chromaffin cells in the adrenal glands, which leads to increased production and concentration of catecholamines [86,93]. In these cases, hyperactivation of adrenergic receptors often occurs, resulting in hypertension [86]. The overstimulation of adrenergic pathways can lead to increases in heart rate, contractile force, and PVR, all of which contribute to elevated blood pressure [93]. Additionally, certain drugs and toxins, such as glucocorticoids, mineralocorticoids, erythropoietin stimulants, phenylephrine hydrochloride, ephedrine, toracenib, cocaine, and amphetamines, can also be contributing factors to hypertension [2].
8. Target Organ Damage
Target organ lesions (TOD) are common manifestations observed in patients with SAH [87]. A significant number of animals diagnosed with SAH are at high risk of developing TOD during their lives. The presence of TOD is determined by the organs that depend heavily on a constant blood supply to function properly. Persistently elevated blood pressure can predispose these organs to changes that result in secondary, often harmful, manifestations. Organs most likely to experience TOD include the kidneys, eyes, nervous system, and heart, particularly due to structural and functional modifications in the cardiovascular system [93]. Acierno et al. [2] suggest that the presence of TOD indicates that therapeutic management should be initiated to prevent further progression and adverse outcomes. Target organs, with higher blood demands, often try to compensate for blood pressure fluctuations, but in SAH patients, this compensation is insufficient, leading to specific and damaging lesions [87,93].
Cardiovascular TOD primarily result from direct damage caused by SAH [2]. Evidence indicates underlying heart diseases, such as hypertensive heart disease in dogs, may be present [93,103,104]. Thoracic radiographs are a valuable tool in assessing aortic remodelling due to SAH, as they can reveal vascular remodelling and enlargement [104] (Figure 7).
The ocular system can also be affected, with various studies identifying distinct symptoms and conditions [2,106,107,108,109,110,111,112]. Hypertensive retinopathy and choroidopathy are the most commonly observed ocular conditions, with retinal detachment being the most frequent [107,110,111]. A study by Cole et al. [111] found that about 16% of dogs showed signs of hypertensive retinopathy. Chalhoub & Palma [86] and Holt et al. [112] indicated these conditions result from the breakdown of the blood-retinal barrier, leading to fluid and protein leakage. Most ocular disorders caused by SAH are irreversible [48] and are more common in cats [93]. While blood pressure management can help control the condition, it may not restore ocular health [107], with funduscopy recommended for assessment [110] (Figure 7).
Renal TOD occur due to the kidneys' rich vascularisation, which allows for the detection of proteinuria and renal injury [87,88,93]. Proteinuria is an early indicator of CKD, and following the initiation of antihypertensive therapy, it is expected that renal damage progression will be controlled, along with a reduction in proteinuria [1,88]. Glomerulosclerosis and hyperplastic arteriolosclerosis may prevent effective blood pressure control [113]. Given the risk of renal TOD, the IRIS [88] recommends sub-staging animals based on their blood pressure, which guides diagnostic and therapeutic decisions. According to IRIS [88], "patients are sub-staged by systolic blood pressure according to the degree of target organ injury risk and whether evidence of target organ injury or complications is present" (Figure 7).
Neurological TOD, including hypertensive encephalopathy and white matter oedema, are also associated with SAH [87,93]. These conditions are more common in cats [48,93,114]. Mathur et al. [115] found that antihypertensive management could help control these neurological disturbances. SAH-related neurological symptoms may include "ataxia, circling, stupor, coma, seizures, blindness, nystagmus, and behavioural and balance changes" [93]. Additionally, evidence suggests the occurrence of haemorrhage, infarcts, vasogenic oedema, and cervical myelopathy due to ischaemia [116,117,118] (Figure 7).
9. Diagnosis and Devices of Measurement
The diagnosis of hypertension requires serial blood pressure (BP) measurements [1], considering factors that may interfere with accuracy. To obtain reliable results, it is essential to follow a standardized protocol that can be consistently replicated. Variability and potential unreliability in BP data are often due to changes in technique, patient position, and the operator's experience. Situational SAH can be minimized by measuring BP in a quiet area after the animal has acclimatized, away from other animals, and before any procedures [2]. If possible, having the animal's owner present and minimizing restraint is beneficial, as BP and heart rate may be elevated when measurements are made without the owner [119].
Stress, a major cause of BP fluctuations, can be controlled through routine strategies in veterinary practice. Canine-friendly handling techniques facilitate patient management and help reduce stress, which is one of the main barriers to accurate BP measurement. A study by Navarro et al. [120] found that 86% of veterinary professionals use non-invasive BP measurement in cats. However, 4.1% of cases did not perform BP measurements, primarily due to anxiety, fear, and stress in animals. Discomfort during the procedure and difficulty in execution were also significant issues for 40% and 57% of professionals, respectively [120]. Approximately 90% of veterinary professionals apply techniques to reduce situational SAH, with the most common methods being: quiet location (71.7%), minimal restraint (49.9%), measurement before any procedure (47.7%), avoiding other animals (34.6%), and allowing acclimatization time (26.4%).
The operator's experience significantly influences BP measurement accuracy. Operators should be qualified and experienced in patient handling and equipment use [2]. Gouni et al. [121] demonstrated that professionals with more training are more likely to obtain reliable and faster BP values. Proper cuff selection is also crucial for accurate measurements, with the cuff's width being 30-40% of the circumference of the measurement site [2]. Smaller cuffs tend to overestimate BP, while larger cuffs underestimate it, affecting clinical decisions regarding SAH diagnosis [1]. It is important that measurements are taken correctly, standardized, and at multiple time points in a calm environment, after acclimatization, and without stress. This approach will guide the clinical approach to managing SAH. Prost [122] found that 80% of veterinary professionals do not recommend BP measurement in cats over 7 years old due to cost, stress, and time constraints, and when it is performed, it is usually in the presence of comorbidities.
According to Acierno et al. [2], SAH cases can be diagnosed and classified into stages based on BP values, which help direct clinical and emergency management strategies. Reliable measurements are critical for this classification, with systolic BP being commonly used for diagnostic purposes [2,123]. Correct measurements are essential for therapeutic management decisions, as incorrect readings cannot form the basis for an SAH diagnosis [1]. Given the complications associated with TOD (target organ damage), the presence of lesions from a single BP measurement already suggests the need for antihypertensive management. However, subsequent confirmation with additional measurements is recommended [2]. Acierno et al. [2] suggest that animals showing signs of pre-hypertension or moderate TOD risk should have BP measurements every 4-8 weeks, while those with higher BP values and high TOD risk should be monitored every 1-2 weeks [2] (Table 1).
BP measurement can be performed using invasive and non-invasive methods, with the latter being more commonly used in routine practice [1]. Although the invasive method is the gold standard for BP measurement, the required infrastructure and operator experience can make it impractical for routine use. This method involves inserting a catheter into an artery connected to a device that measures BP [1,124]. The main challenges include the operator's experience and the pain associated with the procedure, so it is typically restricted to anesthesia or intensive care cases [1,124].
Non-invasive methods such as Doppler vascular devices and oscillometry are more commonly used. The Doppler method involves complete arterial occlusion with a sphygmomanometer, and BP is measured as blood flow is restored during deflation. The oscillometric method, as described by Sousa et al. [1], "is based on occlusion and release of arterial flow, monitoring returning pulses, and emitting systolic, diastolic, and mean pressure values along with heart rate." Studies comparing non-invasive methods have produced mixed results. Vachon et al. [124] compared oscillometric and Doppler methods with invasive BP measurements in medium to large breed dogs under anesthesia. Oscillometry showed better correlation with invasive BP, particularly for mean and diastolic BP values, while Doppler was less effective. Stethoscopes can assist in BP measurement, especially for patients sensitive to noise. While Gill et al. [125] found no difference in BP values when using stethoscopes, the results were more precise. In contrast, a study by Uematsu et al. [126] showed that stethoscopes reduced BP readings in elderly cats (137 ± 17 mmHg vs. 125 ± 15 mmHg).
Navarro et al. [120] found that nearly 70% of veterinary professionals prefer the Doppler vascular method due to its reliability. Taylor et al. [123] noted that oscillometry presents challenges, and in some cases, the device may fail to measure BP. Martel et al. [127] found a positive correlation between systolic BP values obtained by invasive and high-definition oscillometric devices in cats. Anjos et al. [128] compared oscillometry and Doppler in conscious healthy cats and observed significant differences in average values, though these differences were not clinically relevant. Nevertheless, both methods consistently showed higher BP values. Moreover, in 2025, Mantovani et al. [129] conducted a study aimed at comparing the accuracy of linear deflation oscillometry (LDO) and Doppler measurements against invasive BP monitoring in dogs under anaesthesia. The authors observed that Doppler tends to overestimate systolic BP values during hypotensive episodes. Additionally, they found that LDO is effective in detecting hypotension in anaesthetised dogs.
10. Therapeutic Management
Antihypertensive therapy should be initiated once the presence of either idiopathic or secondary hypertension is confirmed, provided that BP values exceed the reference threshold after successive, accurate, and reliable measurements. Yamato [93] identifies five key factors to consider when starting antihypertensive management: serially elevated blood pressure, the presence of secondary diseases, evidence of TOD, impairment due to TOD, and the exclusion of situational hypertension. Timely clinical and therapeutic monitoring is essential for patients with secondary diseases to control the effects of elevated blood pressure [2]. Once antihypertensive therapy begins, affected animals are unlikely to return to normotension and remain at risk for TOD [2]. Acierno et al. [2] emphasize that "the treatment of a patient's hypertension should not be delayed until the underlying condition is controlled." Additionally, it is crucial that pet owners are informed about their animal's condition, its consequences, potential complications, and the need for ongoing treatment.
Antihypertensive therapy should be implemented alongside the treatment of any underlying conditions [2]. Early identification and the establishment of treatment strategies are necessary for optimal management. After initiating antihypertensive therapy, animals must be reassessed regularly to monitor BP values and determine whether the prescribed medication(s) and dosages are appropriate, or if adjustments are needed [1]. Like any clinical treatment, management must be individualized to suit each patient's specific needs [1]. Acierno et al. [2] recommend gradual BP control and management to avoid complications from sudden reductions in BP.
From a pharmacological standpoint, the first-line treatment for dogs involves medications that target the RAS [2], such as ACE inhibitors, angiotensin II receptor blockers (ARBs), and aldosterone inhibitors [2,93], with ACE inhibitors being the most commonly recommended [1]. ACE inhibitors are particularly beneficial for controlling blood volume, PVR, and maintaining proteinuria [93]. King et al. [130] demonstrated that benazepril effectively controls proteinuria. Mishina & Watanabe [131] showed that benazepril (2 mg/kg, q24h, for 2 weeks) effectively reduced blood pressure, angiotensin II, and aldosterone levels, with values returning to baseline after discontinuation. Ames et al. [132] noted that benazepril or enalapril effectively block ACE activity, which is beneficial for blood pressure control. Telmisartan has also been shown to control blood pressure, with potential for combination therapy with benazepril. Fowler et al. [133] found that combining ACE inhibitors (mean dose 1.75 mg/kg, q24h) with telmisartan (mean dose 0.93 mg/kg, q24h) resulted in a 13 mmHg reduction in BP and a decrease in the protein/creatinine ratio in urine. However, LeCavalier et al. [134] found that using telmisartan alone did not alter BP values. Diuretics like spironolactone may be considered in combination with ACE inhibitors or ARBs [93].
Patients with specific conditions, such as adrenal tumors and aldosterone overproduction, may benefit from blood pressure control using alpha or beta blockers [93]. Amlodipine may also be advantageous when combined with other medications, as monotherapy can cause glomerular injury [93]. For cats, the use of amlodipine was evaluated by Morita et al. [135], including its impact on prognosis. In this study, amlodipine was more frequently used as a monotherapy rather than in combination with other treatments. Its administration was effective in reducing systolic blood pressure values; however, it may have a detrimental impact on patient survival. The use of diuretics in such cases is controversial and generally avoided in patients with underlying conditions like CKD or other complicating factors. Furthermore, caution is advised when using ACE inhibitors and diuretics due to the risk of dehydration and worsening clinical conditions [2,93].
11. Conclusions
The importance of performing blood pressure measurements as a standard clinical practice in veterinary settings is clear. Hypertension is defined by a persistent elevation in blood pressure values and can be classified into three types: one caused by catecholamine excess, another linked to underlying diseases, and true hypertension, where other causes have been excluded. Hypertension is a condition with variable progression, impact, and severity, and is often described as a silent process. Therefore, serial measurements are essential, taking into account variables that may influence the values, such as stress, size, environment, and the method of measurement. It is crucial to understand that hypertension carries the potential risk of organ damage, which can affect different organs, with the consequences varying depending on the organ involved. Early and accurate identification of hypertension, whether idiopathic or secondary to an underlying cause, enables the initiation of pharmacological therapy to prevent the condition from worsening and minimize the onset of organ damage. Veterinary professionals must be aware of the importance of blood pressure measurement and ensure that it is performed in a standardized manner and at regular intervals. This approach will allow for a timely diagnosis of hypertension, guiding the implementation of clinical and/or emergency pharmacological therapy. Such measures will ultimately impact the patient's life expectancy and quality of life, as well as that of the owner.
Author Contributions
Conceptualization, F.G.S., F.Q. and S.L.; methodology, F.G.S., F.Q. and S.L.; validation, F.G.S., F.Q.; R.M.; J.C.V. and S.L.; formal analysis, F.G.S., F.Q.; R.M.; J.C.V. and S.L.; investigation, F.G.S., F.Q.; R.M.; J.C.V. and S.L.; data curation, F.G.S. and F.Q.; writing—original draft preparation, F.G.S. and F.Q.; writing—review and editing, F.G.S., F.Q.; R.M.; J.C.V. and S.L.; visualization, F.G.S., F.Q.; R.M.; J.C.V. and S.L.; supervision, S.B.; project administration, F.G.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.Conflicts of Interest: The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ACE | Angiotensin-converting enzyme |
| ACVIM | American College Veterinary Internal Medicine |
| ARBs | Angiotensin II receptor blockers |
| BP | Blood pressure |
| CKD | Chronic kidney disease |
| CO | Cardiac output |
| IRIS | International Renal Interest Society |
| mmHg | millimeters of mercury |
| PNS | Parasympathetic nervous system |
| PVR | Peripheric vascular resistance |
| RAAS | Renin-angiotensin-aldosterone system |
| RAS | Renin-angiotensin system |
| SAH | Systemic arterial hypertension |
| SNS | Sympathetic nervous system |
| TOD | Target organ damage |
| VR | Venous return |
References
- Sousa, F.G.; Oliveira, B.C.G.; Ferreira, N.S.; Baldi, M.L.C.; Queiroz, F.S.F.; Beier, S.L. Hipertensão arterial sistêmica e as diretrizes para identificação, avaliação, controle e manejo hipertensivo em cães e gatos. Vet. Zootec. 2023, 30, 1–23. [Google Scholar] [CrossRef]
- Acierno, M.J.; Brown, S.; Coleman, A.E.; Jepson, R.E.; Papich, M.; Stepie, R.L.; Syme, H.M. ACVIM consensus statement: Guidelines for the identification, evaluation, and management of systemic hypertension in dogs and cats. J. Vet. Intern. Med. 2018, 32, 1803–1822. [Google Scholar] [CrossRef]
- Lucassen, P.J.; Pruessner, J.; Sousa, N.; Almeida, O.F.X.; Van Dam, A.M.; Rajkowska, G.; Swaab, D.F.; Czéh, B. Neuropathology of stress. Acta Neuropathol. 2014, 127, 109–135. [Google Scholar] [CrossRef] [PubMed]
- Amodeo, C.E.; Lima, N.; da Costa e Nobre, F. História da monitorização ambulatorial da pressão arterial. Rev. Bras. Hipertens. 1998, 5, 151–152. [Google Scholar]
- Ramos, O. Histórico do tratamento da hipertensão arterial. Rev. Bras. Hipertens. 1998, 5, 230–232. [Google Scholar]
- Estañol, B.; Delgado, G.; Borgstein, J. Korotkoff sounds – The improbable also occurs. Arq. Bras. Cardiol. 2013, 101, 531–536. [Google Scholar] [CrossRef]
- Reusch, C.E.; Schellenberg, S.; Wenger, M. Endocrine Hypertension in Small Animals. Vet. Clin. North Am. Small Anim. Pract. 2010, 40, 335–52. [Google Scholar] [CrossRef]
- Guyton, A.; Hall, J.E. Textbook of Medical Physiology, 14th ed.; Elsevier: Philadelphia, 2021; pp. 205–258. [Google Scholar]
- Neto, M.L.; Ribeiro, V.R.F.R. Fisiologia do Sistema Cardiovascular. In Tratado de Cardiologia Veterinária; Larsson, M.H.M.A., Ed.; Interbook: São Paulo, Brazil 2020; pp. 7–29. [Google Scholar]
- Sousa, F.G. Avaliação de efeitos cardiovasculares da angiotensina (1-7) após administração do peptídeo em formulação oral em felinos. Dissertation, Programa de Pós-Graduação em Ciência Animal, Escola de Veterinária, Universidade Federal de Minas Gerais, 2024. [Google Scholar]
- Lyberg, M.; Ljungvall, I.; Häggström, J.; Wilson, H.; Palmer, L. Impact of equipment and handling on systolic blood pressure measurements in conscious dogs in an animal hospital environment. J. Vet. Intern. Med. 2021, 35, 739–746. [Google Scholar] [CrossRef]
- Safar, M. Ageing and its effects on the cardiovascular system. Drugs 1990, 39, 1–8. [Google Scholar] [CrossRef]
- Bodey, A.R.; Michell, A.R. Epidemiological study of blood pressure in domestic dogs. J. Small Anim. Pract. 1996, 37, 116–125. [Google Scholar] [CrossRef]
- Bodey, A.R.; Sansom, J. Epidemiological study of blood pressure in domestic cats. J. Small Anim. Pract. 1998, 39, 567–573. [Google Scholar] [CrossRef] [PubMed]
- Bright, J.M.; Dentino, M. Indirect arterial blood pressure measurement in nonsedated Irish wolfhounds: reference values for the breed. J. Am. Anim. Hosp. Assoc. 2002, 38, 521–526. [Google Scholar] [CrossRef] [PubMed]
- Payne, J.R.; Brodbelt, D.C.; Luis Fuentes, V. Blood Pressure Measurements in 780 Apparently Healthy Cats. J. Vet. Intern. Med. 2017, 31, 15–21. [Google Scholar] [CrossRef]
- Bijsmans, E.S.; Jepson, R.E.; Chang, Y.M.; Syme, H.M.; Elliott, J. Changes in systolic blood pressure over time in healthy cats and cats with chronic kidney disease. J. Vet. Intern. Med. 2015, 29, 855–861. [Google Scholar] [CrossRef]
- Surman, S.; Couto, C.G.; Dibartola, S.P.; Chew, D.J. Arterial blood pressure, proteinuria, and renal histopathology in clinically healthy retired racing greyhounds. J. Vet. Intern. Med. 2012, 26, 1320–1329. [Google Scholar] [CrossRef]
- Pérez-Sánchez, A.P.; Del-Angel-Caraza, J.; Quijano-Hernández, I.A.; Barbosa-Mireles, M.A. Obesity-hypertension and its relation to other diseases in dogs. Vet. Res. Commun. 2015, 39, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Mishina, M.; Watanabe, T.; Fujii, K.; Maeda, H.; Wakao, Y.; Takahashi, M. Non-invasive blood pressure measurements in cats: clinical significance of hypertension associated with chronic renal failure. J. Vet. Intern. Med. 1998, 60, 805–808. [Google Scholar] [CrossRef]
- Bodey, A.R.; Rampling, M.W. Comparison of haemorrheological parameters and blood pressure in various breeds of dog. J. Small Anim. Pract. 1999, 40, 3–6. [Google Scholar] [CrossRef]
- Rattez, E.P.; Reynolds, B.S.; Concordet, D.; Laysol-Lamour, C.J.; Segalen, M.M.; Chetboul, V.; Lefebvre, H.P. P. Within-day and between-day variability of blood pressure measurement in healthy conscious beagle dogs using a new oscillometric device. J. Vet. Cardiol. 2010, 12, 35–40. [Google Scholar] [CrossRef]
- Brown, S.A.; Brown, C.A.; Hendi, R. Does systemic hypertension damage the canine kidney? J. Vet. Intern. Med. 2000, 14, 805–808. [Google Scholar]
- Montoya, J.A.; Morris, P.J.; Bautista, I.; Juste, M.C.; Suarez, L.; Peña, C.; Hackett, R.M.; Rawlings, J. Hypertension: a risk factor associated with weight status in dogs. J. Nutr. 2006, 136, 2011S–2013S. [Google Scholar] [CrossRef]
- Mendes, A.C.R.; Sousa, F.G.; Oliveira, B.C.S.; Miranda, G.C.; Kwong, M.A.C. Fatores de risco associados à obesidade e sobrepeso em cães. Medicina Veterinária (UFRPE), 2023, 17, 11–26. [Google Scholar] [CrossRef]
- Pereira-Neto, G.B.; Brunetto, M.A.; Champion, T.; Ortiz, E.M.G.; Carciofi, A.C.; Camacho, A.A. Avaliação da pressão arterial sistêmica em cães obesos: comparação entre os métodos oscilométrico e doppler ultrassônico. Pesq. Vet. Bras. 2014, 34, 87–91. [Google Scholar] [CrossRef]
- Rondeau, D.A.; Mackalonis, M.E.; Hess, R.S. Effect of body position on indirect measurement of systolic arterial blood pressure in dogs. J. Am. Vet. Med. Assoc. 2013, 242, 1523–7. [Google Scholar] [CrossRef] [PubMed]
- Mooney, A.P.; Mawby, D.I.; Price, J.M.; Whittemore, J.C. Effects of various factors on Doppler flow ultrasonic radial and coccygeal artery systolic blood pressure measurements in privately-owned, conscious dogs. Peer J. 2017, 5, e3101. [Google Scholar] [CrossRef] [PubMed]
- Pereira, G.G.; Yamato, R.J. Insuficiência cardíaca congestiva. In Tratado de Cardiologia Veterinária; Larsson, M.H.M.A., Ed.; Interbook: São Paulo, Brazil 2020; pp. 331–358. [Google Scholar]
- Gomes, E. R. M.; Santos, R. A. S.; Guatimosim, S. Angiotensin-(1-7)-mediated signaling in cardiomyocytes. Int. J. Hypertens. 2012, 2012, 493129. [Google Scholar] [CrossRef]
- McKinney, C.A.; Fattah, C.; Loughrey, C.M.; Milligan, G.; Nicklin, S.A. Angiotensin-(1–7) and angiotensin-(1–9): function in cardiac and vascular remodeling. Clin. Sci. 2014, 126, 815–827. [Google Scholar] [CrossRef]
- Cruz-López, E.O.; Ye, D.; Wu, C.; Lu, H.S.; Uijl, E.; Colafella, K.M.M.; Danser, A.H.J. Angiotensinogen suppression: A new tool to treat cardiovascular and renal disease. Hypertension 2022, 79, 2115–2126. [Google Scholar] [CrossRef]
- Gambaryan, S.; Mohagaonkar, S.; Nikola, E.V. Regulation of the renin-angiotensin-aldosterone system by cyclic nucleotides and phosphodiesterases. Front. Endocrinol. 2023, 14, 1239492. [Google Scholar] [CrossRef]
- Fountain, J.; Kaur, J.; Lappin, S. L. Physiology, Renin Angiotensin System. [s.l.] StatPearls Publishing. 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK470410/ (accessed on 23 November 2023).
- Kanagula, A.K.; Kaur, J.; Batra, J.; Ankireddypalli, A.R.; Velagapudi, R. Renin-Angiotensin System: Updated Understanding and Role in Physiological and Pathophysiological States. Cureus 2023, 15, e40725–2023. [Google Scholar] [CrossRef]
- Sparks, M.A.; Crowley, S.D.; Gurley, S.B.; Mirotsou, M.; Coffman, T.M. Classical Renin-Angiotensin system in kidney physiology. Compr. Physiol. 2014, 4, 1201–1208. [Google Scholar] [CrossRef] [PubMed]
- Bavishi, C.; Bangalore, S.; Messerli, F.H. Renin Angiotensin Aldosterone System Inhibitors in Hypertension: Is There Evidence for Benefit Independent of Blood Pressure Reduction? Prog. Cardiovasc. Dis. 2016, 59, 253–261. [Google Scholar] [CrossRef]
- Lu, H.; Cassis, L.A.; Kooi, C.W.V.; Daugherty, A. Structure and functions of angiotensinogen. Hypertens. Res. 2016, 39, 492–500. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R.; Thomas, C.M.; Yong, Q.C.; Chen, W.; Baker, K.M. The Intracrine Renin-Angiotensin System. Clin. Sci. 2012, 123, 273–284. [Google Scholar] [CrossRef] [PubMed]
- Varagic, J.; Ahmad, S.; Nagata, S.; Ferrario, C.M. ACE2: Angiotensin II/angiotensin-(1-7) balance in cardiac and renal injury. Curr. Hypertens. Rep. 2014, 16, 420. [Google Scholar] [CrossRef]
- Vargas, R.A.V.; Millána, J.M.V.; Bonilla, E.F. Renin-angiotensin system: Basic and clinical aspects - A general perspective. Endocrinol Diabetes Nutr (Engl Ed) 2022, 69, 52–62. [Google Scholar] [CrossRef]
- Rao, A.; Bhat, S.A.; Shibata, T.; Giani, J.F.; Rader, F.; Bernstein, K.E.; Khan, Z. Diverse biological functions of the renin-angiotensin system. Med. Res. Rev. 2023, 44, 1–19. [Google Scholar] [CrossRef]
- Ranjit, A.; Khajehpour, S.; Aghazadeh-Habashi, A. Update on Angiotensin II Subtype 2 Receptor: Focus on Peptide and Nonpeptide Agonists. Mol. Pharmacol. 2021, 99, 469–487. [Google Scholar] [CrossRef]
- Pedreanez, A.; Mosquera, J.; Munoz, N.; Robalino, J.; Tene, D. Diabetes, heart damage, and angiotensin II. What is the relationship link between them? A minireview. Endocr. Regul. 2022, 56, 55–65. [Google Scholar] [CrossRef]
- Hettiarachchi, S.D.; Kwon, Y.M.; Omidi, Y.; Speth, R.C. Nanoparticle approaches for the renin-angiotensin system. Heliyon, 2023, 9, e16951. [Google Scholar] [CrossRef]
- Mathieu, N.M.; Nakagawa, P.; Grobe, J.L.; Sigmund, C.D. Insights Into the Role of Angiotensin-II AT1 Receptor-Dependent β-Arrestin Signaling in Cardiovascular Disease. Hypertension 2024, 81, 6–16. [Google Scholar] [CrossRef] [PubMed]
- Knies, M.; Kooistra, H.S.; Teske, E. Prevalence of persistent hypertension and situational hypertension in a population of elderly cats in The Netherlands. J. Feline Med. Surg. 2023, 25, 1098612X231172629. [Google Scholar] [CrossRef]
- Maggio, F.; Defrancesco, T.C.; Atkins, C.E.; Sakai, M.; Kallfelz, F.A. Ocular lesions associated with systemic hypertension in cats: 69 cases (1985-1998). J. Am. Vet. Med. Assoc. 2000, 217, 695–702. [Google Scholar] [CrossRef] [PubMed]
- Elliott, J.; Barber, P.J.; Syme, H.M.; Rawlings, J.M.; Markwell, P.J. Feline hypertension: clinical findings and response to antihypertensive treatment in 30 cases. J. Small Anim. Pract. 2001, 42, 122–129. [Google Scholar] [CrossRef]
- Jepson, R.E.; Elliott, J.; Brodbelt, D.; Syme, H.M. Effect of control of systolic blood pressure on survival in cats with systemic hypertension. J. Vet. Intern. Med. 2007, 21, 402–409. [Google Scholar] [CrossRef] [PubMed]
- Goy-Thollot, I.; Péchereau, D.; Kéroack, S.; Dezempte, J.C.; Bonnet, J.M. Investigation of the role of aldosterone in hypertension associated with spontaneous pituitary dependent hyperadrenocorticism in dogs. J. Small Anim. Pract. 2002, 43, 489–492. [Google Scholar] [CrossRef]
- Syme, H.M.; Elliott, J. The prevalence of hypertension in hyperthyroid cats at diagnosis and following treatment. J. Vet. Intern. Med. 2003, 17, 754. [Google Scholar]
- Sparkes, A.; Garelli-Paar, C.; Blondel, T.; Guillot, E. 'The Mercury Challenge': Feline systolic blood pressure in primary care practice - A European survey. J. Feline Med. Surg. 2002, 24, e310–e323. [Google Scholar] [CrossRef]
- Broom, D.M. Psychological Indicators of Stress and Welfare. In Ethics, Welfare. In Ethics, Welfare, Law and Market Forces: The Veterinary Interface; Michell, A.R., Ewbank, R., Eds.; Wheathampstead, UK: U.F.A.W, 1998; pp. 167–175. [Google Scholar]
- Mârza, S.M.; Munteanu, C.; Papuc, I.; Radu, L.; Diana, P.; Purdoiu, R.C. Behavioral, Physiological, and Pathological Approaches of Cortisol in Dogs. Animals 2024, 14, 3536. [Google Scholar] [CrossRef]
- Lee, G.-H.; Jo, W.; Kang, T.-K.; Oh, T.; Kim, K. Assessment of Stress Caused by Environmental Changes for Improving the Welfare of Laboratory Beagle Dogs. Animals 2023, 13, 1095. [Google Scholar] [CrossRef]
- Vincent, I.C.; Michell, A.R. Relationship between blood pressure and stress-prone temperament in dogs. Physiol. Behav. 1996, 60, 135–138. [Google Scholar] [CrossRef]
- Mancia, G.; Fagard, R.; Narkiewicz, K.; Redon, J.; Zanchetta, D.; Böhm, M.; Christiaansen, E.; Cübbel, M.; De Backer, G.; Ducimetière, P.; Escoppel, H.; Hansen, K. 2013 ESH/ESC guidelines for the management of arterial hypertension: the task force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J. Hypertens. 2013, 31, 1281–1357. [Google Scholar] [CrossRef] [PubMed]
- Franklin, S. S.; O'brien, E.; Staessen, J.A. Masked hypertension: understanding its complexity. Eur. Heart J. 2016, 38, 1112–1118. [Google Scholar] [CrossRef]
- Soares, F.A.C.; Neuwald, E.B.; Mombach, V.S.; D'Avila, A.E.R.; Conrado, F.O.; González, F.H.D. Systolic blood pressure of dogs at hospital and domestic environment. Cienc. Rur. 2012, 42, 1243–1248. [Google Scholar] [CrossRef]
- Queiroz, F.S.F.; Rosa, D.B.S.K.; Ferreira, R.H.; Masieiro, J.S.; Silva, N.C.P.; Canta, G.N.; Veado, J.C.C. Estudo comparativo da aferição de pressão arterial sistólica em cães nos ambientes ambulatorial e domiciliar. Simpósio CBNUV 2021 - Polêmicas da Nefrologia, Plataforma online, Brazil, (20 Fev 2021).
- Koo, S.T.; Carr, A.P. Comparison of home blood pressure and office blood pressure measurement in dogs and cats. Can. J. Vet. Res. 2022, 86, 203–208. [Google Scholar] [PubMed]
- Kartashova, I.A.; Ganina, K.K.; Karelina, E.A.; Tarasov, S. A. How to evaluate and manage stress in dogs: A guide for veterinary specialists. Appl. Anim. Behav. Sci. 2021, 243, 105458. [Google Scholar] [CrossRef]
- Fuente-Moreno, E.; Paredes-Ramos, P.; Carrasco-García, A.; Hernandez-Cruz, B.; Alvarado, M.; Edwards, C. Salivary cortisol in guide dogs. Animals 2023, 13, 1981. [Google Scholar] [CrossRef] [PubMed]
- James, K.A.; Stromin, J.I.; Steenkamp, N.; Combrinck, M.I. Understanding the Relationships between Physiological and Psychoso cial Stress, Cortisol and Cognition. Front. Endocrinol. 2023, 14, 1085950. [Google Scholar] [CrossRef]
- Feng, S. Hypothalamic-Pituitary-Adrenal Axis. In The ECPH Encyclopedia of Psychology; Springer: Singapore, 2024; Available online: https://link.springer.com/referenceworkentry/10.1007/978-981-99-6000-2_586-1 (accessed on day month year).
- Petersson, M.; Uvnäs-Moberg, K.; Nilsson, A.; Gustafson, L.-L.; Hydbring-Sandberg, E.; Handlin, L. Oxytocin and Cortisol Levels in Dog Owners and Their Dogs Are Associated with Behavioral Patterns: An Exploratory Study. Front. Psychol. 2017, 8, 1796. [Google Scholar] [CrossRef]
- Rosado, B.; García-Belenguer, S.; León, M.; Chacón, G.; Villegas, A.; Palacio, J. Blood concentrations of serotonin, cortisol and dehydroepiandrosterone in aggressive dogs. Appl. Anim. Behav. Sci. 2010, 123, 124–130. [Google Scholar] [CrossRef]
- Narayan, E.J.; Forsburg, Z.R.; Davis, D.R.; Gabor, C.R. Non-Invasive Methods for Measuring and Monitoring Stress Physiology in Imperiled Amphibians. Front. Ecol. Evol. 2019, 7, 431. [Google Scholar] [CrossRef]
- Chmelíková, E.; Bolechová, P.; Chaloupková, H.; Svobodová, I.; Jovičić, M.; Sedmíková, M. Salivary cortisol as a marker of acute stress in dogs: A review. Domest. Anim. Endocrinol. 2020, 72, 106428. [Google Scholar] [CrossRef]
- Demirbas, S. Y.; Isparta, S.; Saral, B.; Keskin Yilmaz, N.; Adiay, D.; Matsui, H.; Töre-Yargin, G.; Musa, S. A.; Atilgan, D.; Öztürk, H.; Cinar Kul, B.; Şafak, C. E.; Ocklenburg, S.; Güntürkün, O. Acute and chronic stress alter behavioral laterality in dogs. Sci. Rep. 2023, 13, 4092. [Google Scholar] [CrossRef]
- Kähler, E.; Meyer-Lindenberg, A.; Zablotski, Y.; Schroers, M. Salivary cortisol measurements in brachycephalic dog breeds as part of a standardized stress test. Front. Vet. Sci. 2023, 13, 4092. [Google Scholar] [CrossRef]
- Quilez, E.; Burchell, R.K.; Thorstensen, E.B.; Weidgraaf, K.; Parbhu, S.E.; Lopez-Villalobos, N.; Gal, A. Cortisol urinary metabolites in dogs with hypercortisolism, congestive heart failure, and healthy dogs: Pilot investigation. J. Vet. Diagn. Investig. 2020, 32, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Nagasawa, M.; Tomori, S.; Mogi, K.; Kikusui, T. Attachment-like behavioral expressions to humans in puppies are related to oxytocin and cortisol: A comparative study of Akitas and Labrador Retrievers. Peptides 2024, 177, 171224. [Google Scholar] [CrossRef] [PubMed]
- Botschek, T.; Hußlein, V.; Peters, E.M.J.; Brosig, B. Hair Cortisol as Outcome Parameter for Psychological and Neuropsychiatric Interventions—A Literature Review. Front. Psychiatry. 2023, 14, 1227153. [Google Scholar] [CrossRef] [PubMed]
- Hagley, S.P.; Hopper, K.; Epstein, S.E.; Hagley, S.P.; Hopper, K.; Epstein, S.E. Etiology and prognosis for dogs with abnormal blood glucose concentrations evaluated in an emergency room. J. Vet. Emerg. Crit. Care (San Antonio) 2020, 30, 567–573. [Google Scholar] [CrossRef]
- Magomedova, L.; Cummins, C.L. Glucocorticoids and Metabolic Control. Handb. Exp. Pharmacol. 2016, 233, 73–93. [Google Scholar] [CrossRef]
- Liu, L. , Huang, Z., Zhang, J., Wang, M., Yue, T., Wang, W., Wu, Y., Zhang, Z., Xiong, W., Wang, C., Wu, F., Zhan, C., Bi, G., & Liu, J. Hypothalamus-sympathetic-liver axis mediates the early phase of stress-induced hyperglycemia in male mice. Nat. Commun. 2024, 15, 8632. [Google Scholar] [CrossRef]
- Rand, J.S.; Kinnaird, E.; Baglioni, A.; Blackshaw, J.; Priest, J. Acute stress hyperglycemia in cats is associated with struggling and increased concentrations of lactate and norepinephrine. J. Vet. Intern. Med. 2002, 16, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Link, K.R.; Rand, J.S. Changes in blood glucose concentration are associated with relatively rapid changes in circulating fructosamine concentrations in cats. J. Feline Med. Surg. 2008, 10, 583–592. [Google Scholar] [CrossRef]
- Allison, R.W. Avaliação Laboratorial do Pâncreas e Metabolismo da Glicose. In Hematologia e Bioquímica Clínica Veterinária, 2nd ed.; Thrall, M.A., Weiser, G., Allison, R., Campbell, T.W., Eds.; Eds. Roca: São Paulo, 2015; pp. 904–937. [Google Scholar]
- Azeez, O.M.; Olaifa, F.H.; Adah, A.S.; Basiru, A.; Akorede, G.J.; Ambali, H.M.; Suleiman, K.Y.; Sanusi, F.; Bolaji, M. Effect of heat stress on vital and hematobiochemical parameters of healthy dogs. Vet. World 2022, 15, 722–727. [Google Scholar] [CrossRef]
- Weiser, G. Introdução aos leucócitos e ao leucograma. In Hematologia e Bioquímica Clínica Veterinária, 2nd ed.; Thrall, M.A., Weiser, G., Allison, R., Campbell, T.W., Eds.; Eds. Roca: São Paulo, 2015; pp. 257–267. [Google Scholar]
- Nibblett, B.M.; Ketzis, J.K.; Grigg, E.K. Comparison of stress exhibited by cats examined in clinic versus a home setting. Appl. Anim. Behav. Sci. 2015, 173, 68–75. [Google Scholar] [CrossRef]
- Benjamin, E.J.; Nelson, L.; Baumwart, R.; Haines, J. Adverse effects of trazodone in dogs on primary hemostasis and electrocardiogram: A single-blinded placebo-controlled crossover study. J. Vet. Intern. Med. 2013, 37, 2131–2136. [Google Scholar] [CrossRef]
- Chalhoub, S.; Palma, D. Pathophysiology and Clinical Manifestations of Systemic Hypertension. In Textbook of Veterinary Internal Medicine: Diseases of the Dog and the Cat, 8th ed.; Ettinger, S.J., Feldman, E.C., Côté, E., Eds.; Missouri: Elsevier, 2017; pp. 1712–1728. [Google Scholar]
- Lawson, J.S.; Jepson, R.E. The intermingled relationship between chronic kidney disease and hypertension. J. Feline Med. Surg. 2021, 23, 812–822. [Google Scholar] [CrossRef] [PubMed]
- International Renal Interest Society. Iris Guidelines. Available online: http://www.iris-kidney.com/guidelines/ (accessed on 5 January 2025).
- Quimby, J.M. Update on Medical Management of Clinical Manifestations of Chronic Kidney Disease. Vet. Clin. North Am. Small Anim. Pract. 2016, 46, 1163–1181. [Google Scholar] [CrossRef]
- Ames, M.K.; Atkins, C.E.; Pitt, B. The renin-angiotensin-aldosterone system and its suppression. J. Vet. Intern. Med. 2019, 33, 363–382. [Google Scholar] [CrossRef]
- Nelson, R.W.; Maggiore, A.-Md. Endocrine Disorders. In Small Animal Veterinary Medicine; 6th ed.; Nelson, R.W., Ed.; Couto, C.G., Eds. Phialdelphia: Elsevier, 2020; pp. 740–857. [Google Scholar]
- Klein, I.; Ojamaa, K. Thyroid hormone and the cardiovascular system. N. Engl. J. Med. 2001, 344, 501–509. [Google Scholar] [CrossRef]
- Yamato, R.J. Hipertensão Arterial Sistêmica. In Tratado de Cardiologia Veterinária; Larsson, M.H.M.A., Ed.; Interbook: São Paulo, Brazil, 2020; pp. 302–312. [Google Scholar]
- Williams, T.L.; Elliott, J.; Syme, H.M. Renin-angiotensin-aldosterone system activity in hyperthyroid cats with and without concurrent hypertension. J. Vet. Intern. Med. 2013, 27, 522–529. [Google Scholar] [CrossRef]
- Stammeleer, L.; Xifra, P.; Serrano, S.I.; Rishniw, M.; Daminet, S.; Peterson, M.E. Blood pressure in hyperthyroid cats before and after radioiodine treatment. J. Vet. Intern. Med. 2024, 38, 1–11. [Google Scholar] [CrossRef]
- Kamal, N.; Magbool, F.; Khan, F.; Hassan, F. I.; Momtaz, S.; Abdollahi, M. Comparative occurrence of diabetes in canine, feline, and few wild animals and their association with pancreatic diseases and ketoacidosis with therapeutic approach. Vet. World 2018, 11, 410–422. [Google Scholar] [CrossRef]
- Pöppl, A.G.; Hummel, J.; Vicente, G. Obesidade e Alterações Endócrinas. In Tratado de Fisioterapia e Fisiatria de Pequenos Animais; Paya: São Paulo, 2018; pp. 155–167. [Google Scholar]
- Martins, F.S.M.; Carvalho, G.L.C.; Jesus, L.; Pöpp, A.L.; González, F.H.D. Epidemiological, clinical, and laboratory aspects in a case series of canine hyperadrenocorticism: 115 cases (2010-2014). Pesq. Vet. Bras. 2019, 39, 900–908. [Google Scholar] [CrossRef]
- Jepson, R.E. Hypertension and Adrenal Gland Disease. In Hypertension in the Dog and Cat, 1st ed.; Elliott, J., Syme, H.M., Eds.; Jepson, R.E., Eds. Springer: Switzerland, 2020; pp. 101–130. [Google Scholar]
- San José, P.G.; Bermejo, C.A.; Moral, I.C.; Alvaro, P.C.; Alenza, M.D.P. Prevalence and risk factors associated with systemic hypertension in dogs with spontaneous hyperadrenocorticism. J. Vet. Intern. Med. 2020, 34, 1768–1778. [Google Scholar] [CrossRef] [PubMed]
- Smets, P.M.; Lefebvre, H.P.; Meij, B.P.; Croubels, S.; Meyer, E.; Van De Maele, I.; Daminet, S. Long-term follow-up of renal function in dogs after treatment for ACTH-dependent hyperadrenocorticism. J. Vet. Intern Med. 2012, 26, 565–574. [Google Scholar] [CrossRef]
- Chen, H.Y.; Lien, Y.H.; Huang, H.P. Association of renal resistive index, renal pulsatility index, systemic hypertension, and albuminuria with survival in dogs with pituitary-dependent hyperadrenocorticism. Int. J. Endrocrinol. 2016, 2016, 3814034. [Google Scholar] [CrossRef]
- Sampedrano, C.; Chetboul, V.; Gouni, V.; Levy, J. K.; Falcão, M.; Tissier, R.; Bonnet, M.; Deshayes, A.; Serra, P. Systolic and diastolic myocardial dysfunction in cats with hypertrophic cardiomyopathy or systemic hypertension. J. Vet. Intern Med. 2006, 20, 1106–1115. [Google Scholar] [CrossRef]
- Misbach, C.; Gouni, V.; Tissier, R.; Trehiou-Sechi, E.; Petit, A.M.P.; Sampedrano, C.C.; Pouchelon, J.-L.; Chetboul, V. Echocardiographic and tissue Doppler imaging alterations associated with spontaneous canine systemic hypertension. J. Vet. Intern. Med. 2011, 25, 1025–1035. [Google Scholar] [CrossRef]
- Holland, M.; Hudson, J.; Hofmeister, E. An observational thoracic radiographic study of aortic remodeling in dogs with confirmed systemic hypertension. Vet. Radiol. Ultrasound. 2022, 63, 254–263. [Google Scholar] [CrossRef]
- Sansom, J.; Bodey, A. Ocular signs in four dogs with hypertension. Vet. Rec. 1997, 140, 593–598. [Google Scholar] [CrossRef]
- Leblanc, N.L.; Stepien, R.L.; Bentley, E. Ocular lesions associated with systemic hypertension in dogs: 65 cases (2005-2007). J. Am. Vet. Med. Assoc. 2011, 238, 915–921. [Google Scholar] [CrossRef]
- Carter, J.M.; Irving, A.C.; Bridges, J.P.; Jones, B.R. The prevalence of ocular lesions associated with hypertension in a population of geriatric cats in Auckland, New Zealand. N.Z. Vet. J. 2014, 62, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Violette, N.P.; Ledbetter, E.C. Punctate retinal hemorrhage and its relation to ocular and systemic disease in dogs: 83 cases. Vet. Ophthalmol. 2018, 21, 233–239. [Google Scholar] [CrossRef] [PubMed]
- Geddes, R. F. Hypertension: Why Is It Critical? Vet. Clin. North Am. Small Anim. Pract. 2020, 50, 1037–1052. [Google Scholar] [CrossRef] [PubMed]
- Cole, L.P.; Jepson, R.; Dawson, C.; Humm, K. Hypertension, retinopathy, and acute kidney injury in dogs: A prospective study. J. Vet. Intern. Med. 2020, 34, 1940–1947. [Google Scholar] [CrossRef]
- Holt, E. Hypertension and the Eye. In Hypertension in the Dog and Cat, 1st ed.; Elliott, J., Syme, H.M., Jepson, R.E., Eds.; Springer: Switzerland, 2020; pp. 217–237. [Google Scholar]
- Chakrabarti, S.; Syme, H.M.; Elliott, J. Clinicopathological variables predicting progression of azotemia in cats with chronic kidney disease. J. Vet. Intern. Med. 2012, 26, 275–281. [Google Scholar] [CrossRef]
- Littman, M.P. Spontaneous systemic hypertension in 24 cats. J. Vet. Intern. Med. 1994, 8, 79–86. [Google Scholar] [CrossRef]
- Mathur, S.; Syme, H.; Brown, C.A.; Elliot, J.; Moore, P.A.; Newell, M.A.; Munday, J.S.; Cartier, L.M.; Sheldon, S.E.; Brown, S.A. Effects of the calcium channel antagonist amlodipine in cats with surgically induced hypertensive renal insufficiency. Am. J. Vet. Res. 2002, 63, 833–839. [Google Scholar] [CrossRef]
- Manolio, T.A.; Olson, J.; Longstreth, W.T. Hypertension and cognitive function: pathophysiologic effects of hypertension on the brain. Curr. Hypertens. Rep. 2003, 5, 255–261. [Google Scholar] [CrossRef]
- Lowrie, M.; De Risio, L.; Dennis, R.; Murray, J.; Smith, P.; Hussain, S. Concurrent medical conditions and long-term outcome in dogs with nontraumatic intracranial hemorrhage. Vet. Radiol. Ultrasound 2012, 53, 381–388. [Google Scholar] [CrossRef]
- O'neill, J.; Kent, M.; Glass, E.N.; Platt, S.R. Clinicopathologic and MRI characteristics of presumptive hypertensive encephalopathy in two cats and two dogs. J. Am Anim. Hosp. Assoc. 2013, 49, 412–420. [Google Scholar] [CrossRef] [PubMed]
- Höglund, K.; Hanås, S.; Carnabuci, C.; Ljungvall, I.; Tidholm, A.; Häggström, J. Blood pressure, heart rate, and urinary catecholamines in healthy dogs subjected to different clinical settings. J. Vet. Intern. Med. 2012, 26, 1300–1308. [Google Scholar] [CrossRef] [PubMed]
- Navarro, I.; Summers, S.; Rishniw, M.; Quimby, J. Cross-sectional survey of non-invasive indirect blood pressure measurement practices in cats by veterinarians. J. Feline Med. Surg. 2022, 24, 1195–1202. [Google Scholar] [CrossRef]
- Gouni, V.; Tissier, R.; Misbach, C.; Chezel, J.; Gouni, S.; Del Grosso, A.; Leray, V.; Laurent, R.; Coulomb, A.; Lecomte, P.; Fontenelle, C. Influence of the observer's level of experience on systolic and diastolic arterial blood pressure measurements using Doppler ultrasonography in healthy conscious cats. J. Feline Med. Surg. 2015, 17, 94–100. [Google Scholar] [CrossRef]
- Prost, K. Under pressure: A survey of Canadian veterinarians in the diagnosis and treatment of feline hypertension. Can. Vet. J. 2023, 64, 45–53. [Google Scholar]
- Taylor, S.S.; Sparkes, A.H.; Briscoe, K.; Carter, J.; Sala, S.C.; Jepson, R.E.; Scansen, B.A. ISFM Consensus Guidelines on the Diagnosis and Management of Hypertension in Cats. J. Feline Med. Surg. 2017, 19, 288–303. [Google Scholar] [CrossRef] [PubMed]
- VACHON, C.; BELANGER, M.C.; BURNS, P.M. Evaluation of oscillometric and Doppler ultrasonic devices for blood pressure measurements in anesthetized and conscious dogs. Res. Vet. Sci. 2014, 97, 111–117. [Google Scholar] [CrossRef]
- Gill, I. R.; Price, J. M.; Whittemore, J.C. Indirect Doppler flow systolic blood pressure measurements taken with and without headphones in privately-owned, conscious dogs. Peer J. 2019, 7, e744. [Google Scholar] [CrossRef]
- Uematsu, S.; Summers, S.; Keys, D.; Quimby, J. Effect of audible static on blood pressure measurement by Doppler ultrasonic sphygmomanometry in cats. J. Feline. Med. Surg. 2023, 25, 1098612X231197084. [Google Scholar] [CrossRef]
- Martel, E.; Egner, B.; Brown, S.A.; King, J.N.; Laveissiere, A.; Champeroux, P.; Richard, S. Comparison of high-definition oscillometry—a non-invasive technology for arterial blood pressure measurement—with a direct invasive method using radio-telemetry in awake healthy cats. J. Feline. Med. Surg. 2013, 15, 1104–1113. [Google Scholar] [CrossRef]
- Anjos, T.M.; Veado, J.C.C.; Araújo, R.B.; Leme, F.O.P.; Diniz, S.A.; Castro, M.C.N.; Costa, F.V.A.; Tavares, C.A.P.; David, L.M.; Quites, K.X.; Maia, M.Q. Avaliação e comparação entre métodos de mensuração de pressão arterial sistólica em gatos hígidos conscientes. Arq. Bras. Med. Vet. Zootec. 2016, 68, 611–619. [Google Scholar] [CrossRef]
- Mantovani, M.M.; Costa, A.C.A.; de Lima, M.T.; dos Santos, L.F.N.; Silva, K.F.; Martins, A.R.C.; Navarro, A.W.M.; Akabane, R.S.; Fantoni, D.T. . Agreement and diagnostic accuracy of new linear deflection oscillometry and Doppler devices for hypotension detection compared to invasive blood pressure in anesthetized dogs. Vet. Sci. 2025, 12, 116. [Google Scholar] [CrossRef] [PubMed]
- King, J.N.; Font, A.; Rousselot, J.F.; Ash, R.A.; Bonfanti, U.; Brovida, C.; Crowe, I.D.; Lanore, D.; Pechereau, D.; Seewald, W.; Strehlau, G. Effects of Benazepril on Survival of Dogs with Chronic Kidney Disease: A Multicenter, Randomized, Blinded, Placebo-Controlled Clinical Trial. J. Vet. Intern Med. 2017, 31, 1113–1122. [Google Scholar] [CrossRef] [PubMed]
- Mishina, M.; Watanabe, T. Development of hypertension and effects of benazepril hydrochloride in a canine remnant kidney model of chronic renal failure. J. Vet. Med. Sci. 2008, 70, 455–460. [Google Scholar] [CrossRef] [PubMed]
- Ames, M.K.; Atkins, C.E.; Lee, S.; Lantis, A.C.; Zumbrunnen, J.R. Effects of high doses of enalapril and benazepril on the pharmacologically activated renin-angiotensin-aldosterone system in clinically normal dogs. Am. J. Vet. Res. 2015, 76, 1041–1050. [Google Scholar] [CrossRef]
- Fowler, B. L.; Stefanovski, D.; Hess, R. S.; Mcgonigle, K. Effect of telmisartan, angiotensin-converting enzyme inhibition, or both, on proteinuria and blood pressure in dogs. J. Vet. Intern. Med. 2021, 35, 1231–1237. [Google Scholar] [CrossRef]
- Lecavalier, J.; Fifle, L.; Javard, R. Treatment of proteinuria in dogs with telmisartan: A retrospective study. J. Vet. Intern. Med. 2021, 35, 1810–1818. [Google Scholar] [CrossRef]
- Morita, S.; Mochizuki, Y.; Matsumoto, I.; Horii, A.; Ohmori, T.; Hirao, D.; Hasegawa, H.; Yoshimura, A.; Baba, T.; Suzuki, S.; Fukushima, R. Use of amlodipine in the treatment of cats with systemic hypertension in Japan. J. Vet. Med. Sci. 2024, 86, 533–541. [Google Scholar] [CrossRef]
Figure 1.
Schematic representation of the sympathetic nervous system (SNS), derived from the autonomic nervous system, to ensure haemodynamic stabilisation. BioRender 2025 (https://www.biorender.com/ (accessed on 10 January 2025)). Created by the authors.
Figure 1.
Schematic representation of the sympathetic nervous system (SNS), derived from the autonomic nervous system, to ensure haemodynamic stabilisation. BioRender 2025 (https://www.biorender.com/ (accessed on 10 January 2025)). Created by the authors.
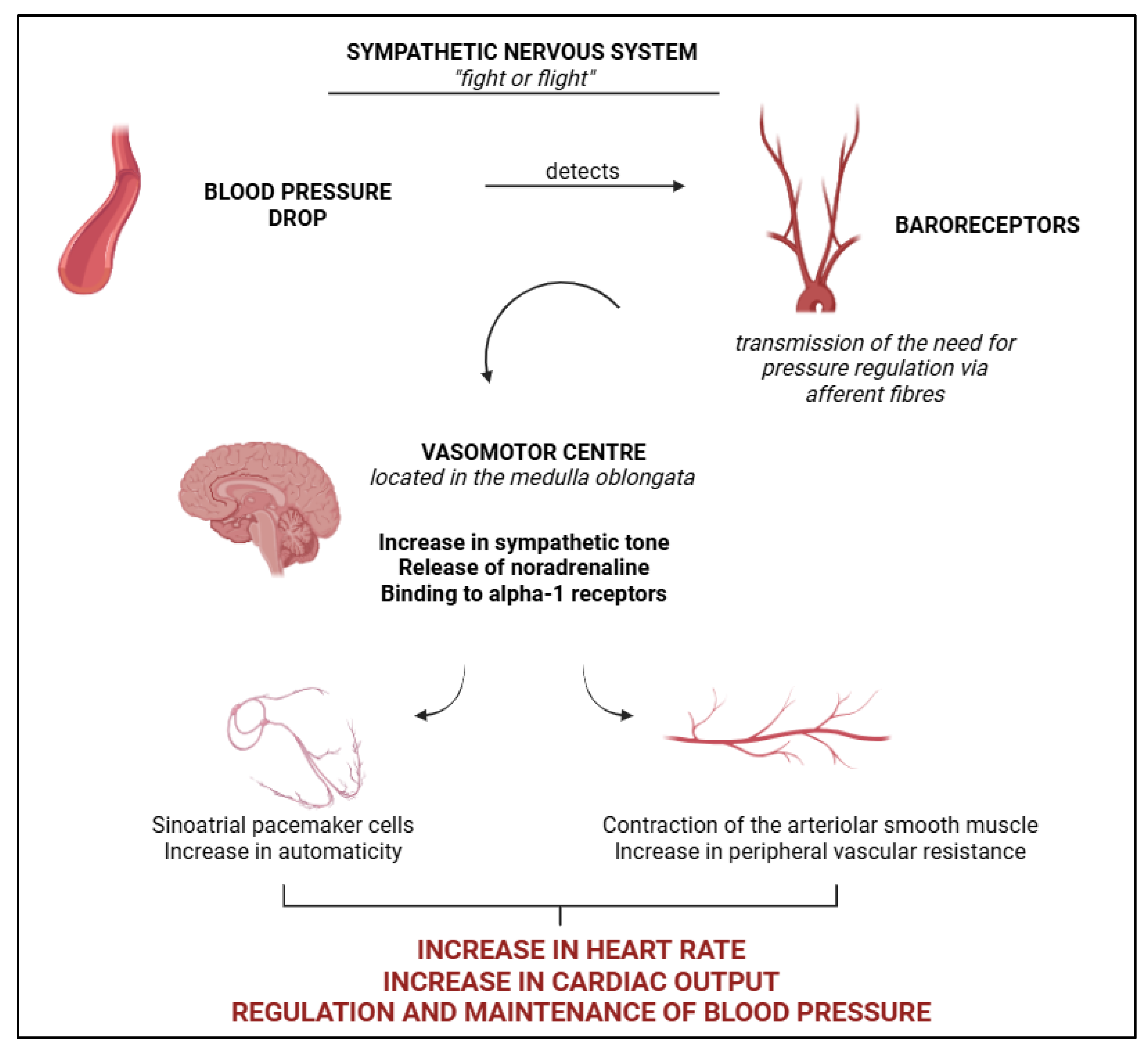
Figure 2.
Schematic representation of the renin-angiotensin system (SRA), highlighting the role of the kidneys in haemodynamic stabilisation. BioRender 2025 (https://www.biorender.com/ (accessed on 10 January 2025)). Created by the authors.
Figure 2.
Schematic representation of the renin-angiotensin system (SRA), highlighting the role of the kidneys in haemodynamic stabilisation. BioRender 2025 (https://www.biorender.com/ (accessed on 10 January 2025)). Created by the authors.
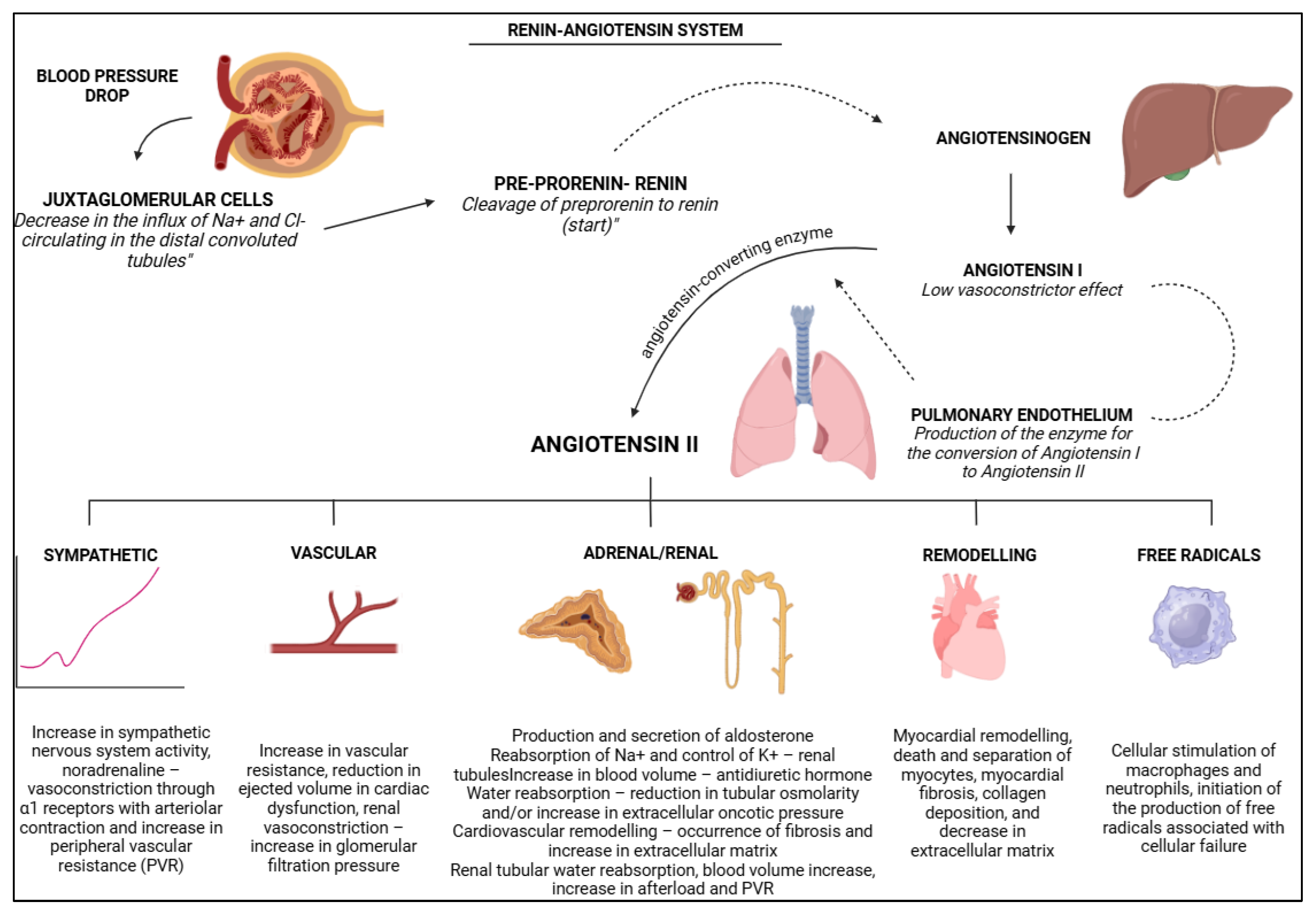
Figure 3.
Schematic representation of situational arterial hypertension, characterised by the presence of an event frequently associated with stress, temporary, capable of elevating blood pressure values. BioRender 2025 (https://www.biorender.com/ (accessed on 10 January 2025)). Created by the authors.
Figure 3.
Schematic representation of situational arterial hypertension, characterised by the presence of an event frequently associated with stress, temporary, capable of elevating blood pressure values. BioRender 2025 (https://www.biorender.com/ (accessed on 10 January 2025)). Created by the authors.
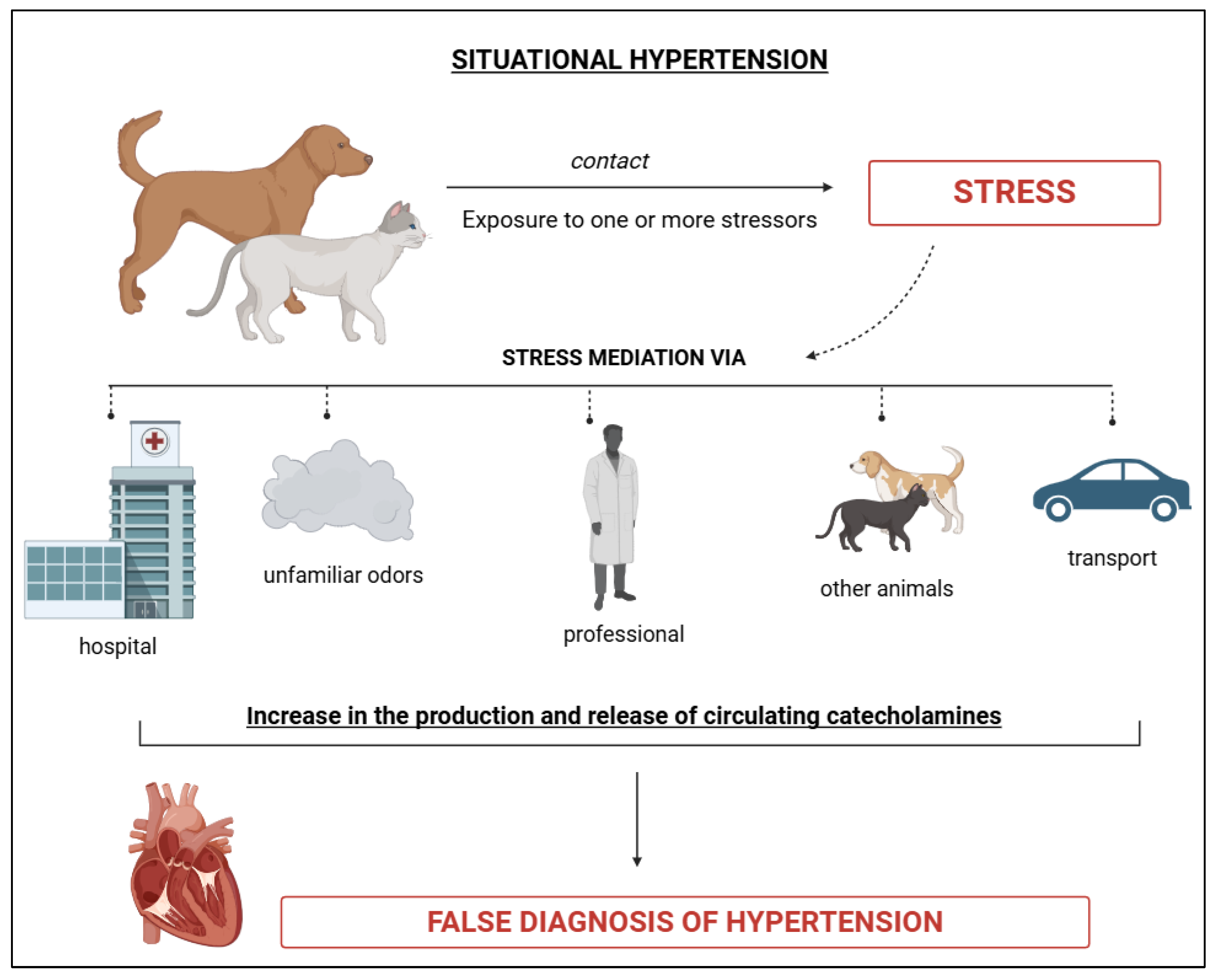
Figure 4.
Schematic representation of idiopathic arterial hypertension, characterised by elevated blood pressure values in the absence of stress or secondary diseases, described as true hypertensive condition. BioRender 2025 (https://www.biorender.com/ (accessed on 10 January 2025)). Created by the authors.
Figure 4.
Schematic representation of idiopathic arterial hypertension, characterised by elevated blood pressure values in the absence of stress or secondary diseases, described as true hypertensive condition. BioRender 2025 (https://www.biorender.com/ (accessed on 10 January 2025)). Created by the authors.
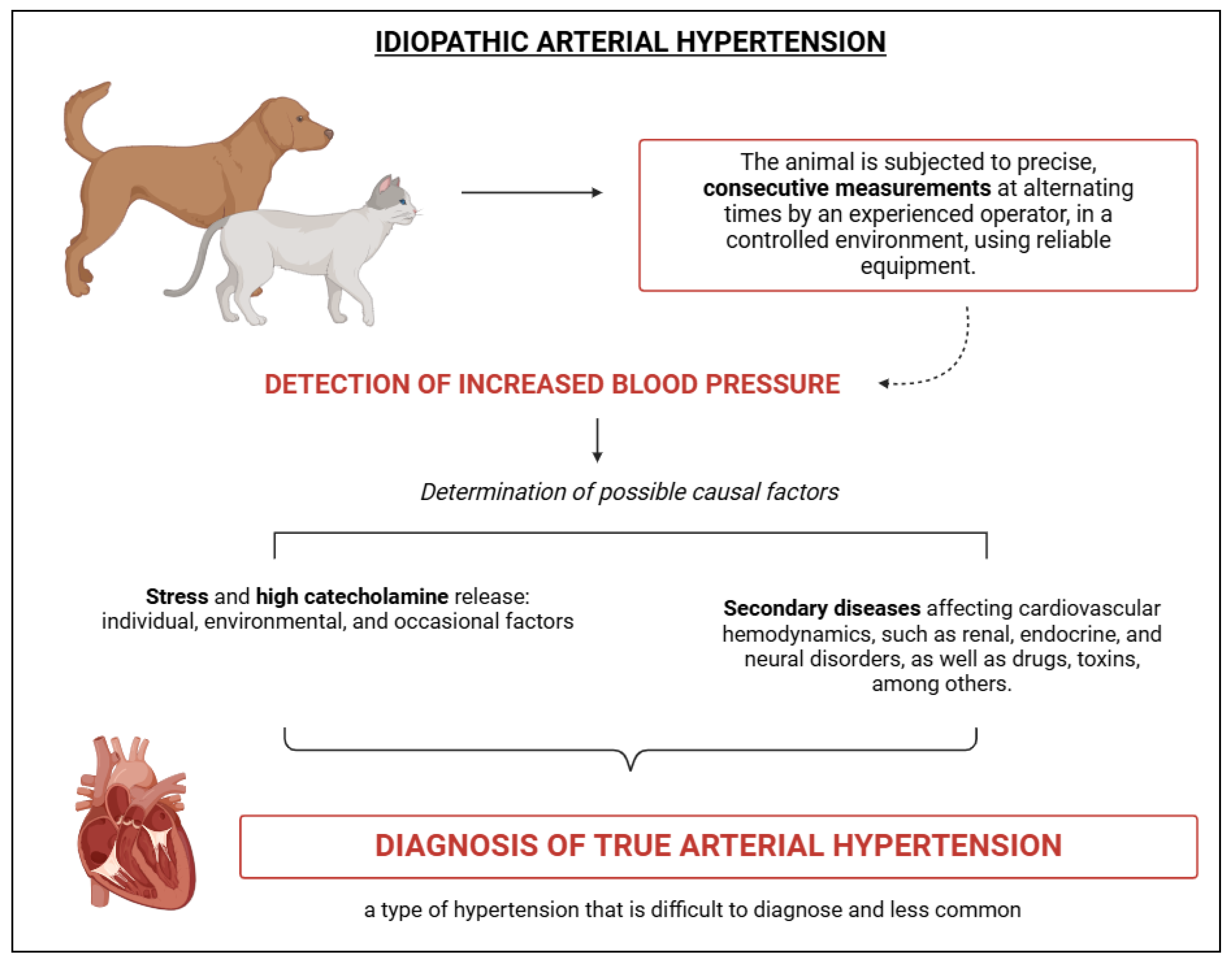
Figure 5.
Schematic representation of secondary arterial hypertension, characterised by elevated blood pressure values resulting from an underlying cause such as nephropathies, endocrinopathies, among others. It is considered the most common type of hypertension. BioRender 2025 (https://www.biorender.com/ (accessed on 10 January 2025)). Created by the authors.
Figure 5.
Schematic representation of secondary arterial hypertension, characterised by elevated blood pressure values resulting from an underlying cause such as nephropathies, endocrinopathies, among others. It is considered the most common type of hypertension. BioRender 2025 (https://www.biorender.com/ (accessed on 10 January 2025)). Created by the authors.
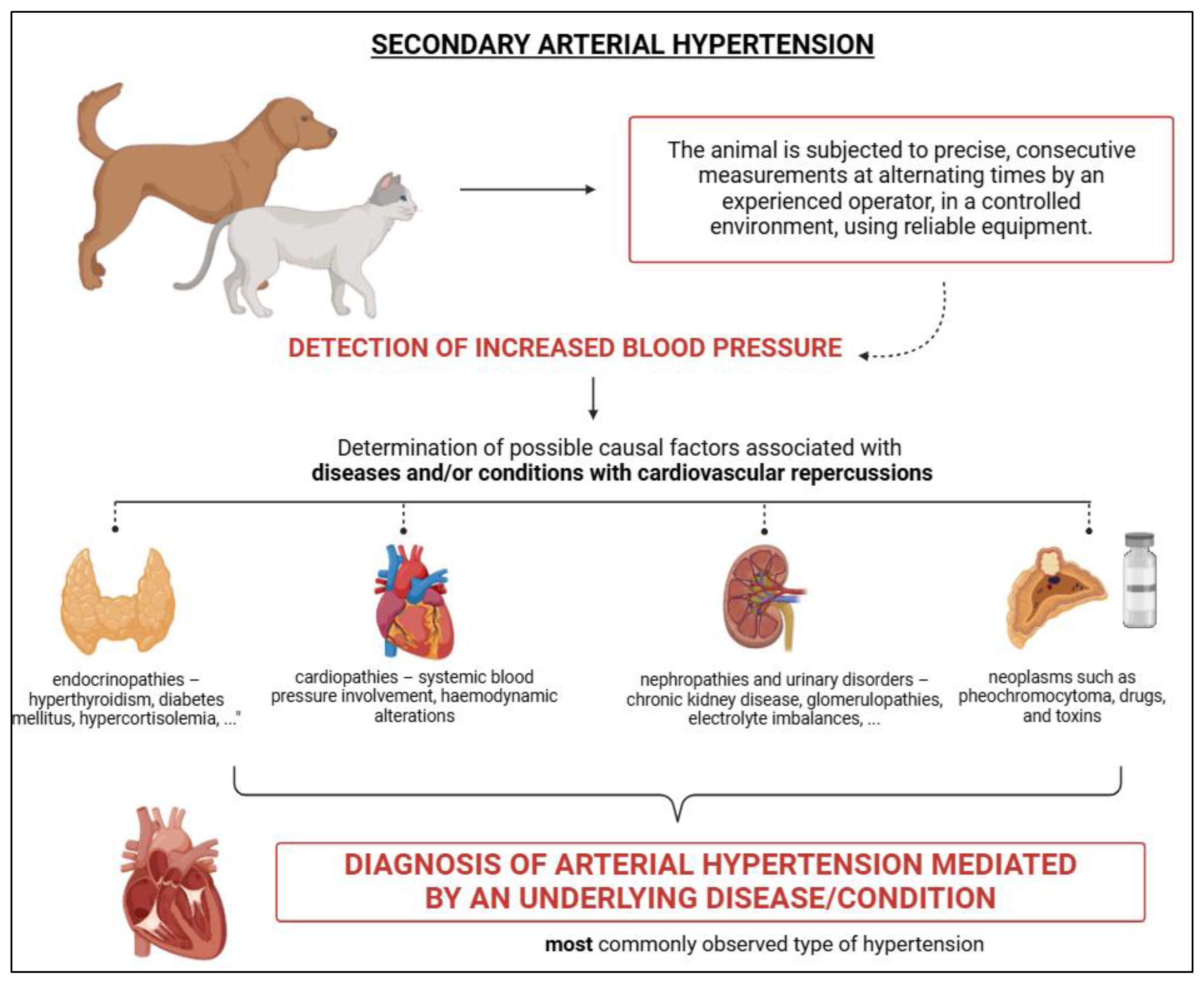
Figure 6.
Schematic representation of cortisol release through the hypothalamic-pituitary-adrenal axis, as well as the samples in which the hormone can be analysed. BioRender 2025 (https://www.biorender.com/ (accessed on 10 January 2025)). Created by the authors.
Figure 6.
Schematic representation of cortisol release through the hypothalamic-pituitary-adrenal axis, as well as the samples in which the hormone can be analysed. BioRender 2025 (https://www.biorender.com/ (accessed on 10 January 2025)). Created by the authors.
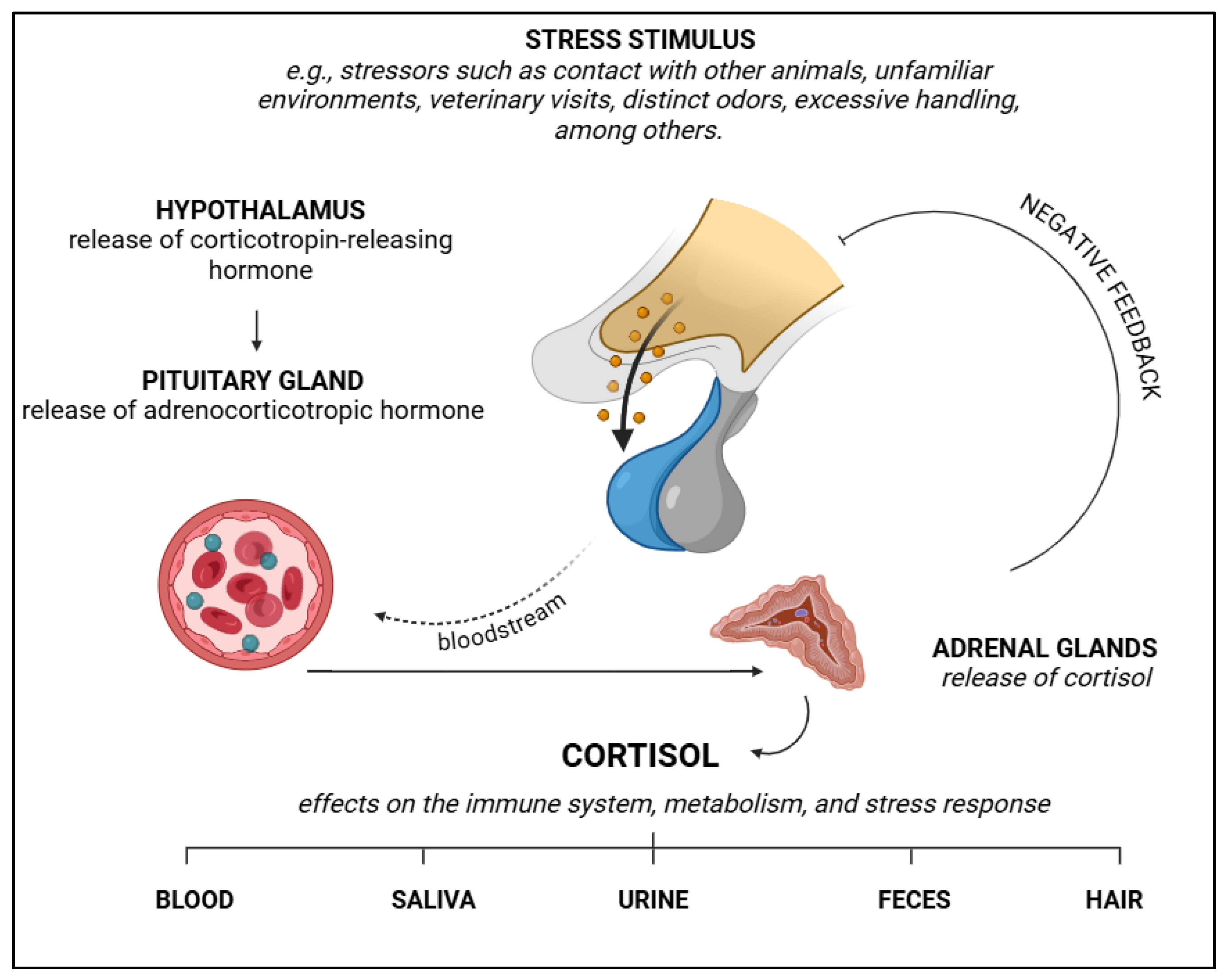
Figure 7.
Schematic representation of target organ damage, including the organs and the most commonly found lesions in the presence of hypertensive conditions. BioRender 2025 (https://www.biorender.com/ (accessed on 10 January 2025)). Created by the authors.
Figure 7.
Schematic representation of target organ damage, including the organs and the most commonly found lesions in the presence of hypertensive conditions. BioRender 2025 (https://www.biorender.com/ (accessed on 10 January 2025)). Created by the authors.
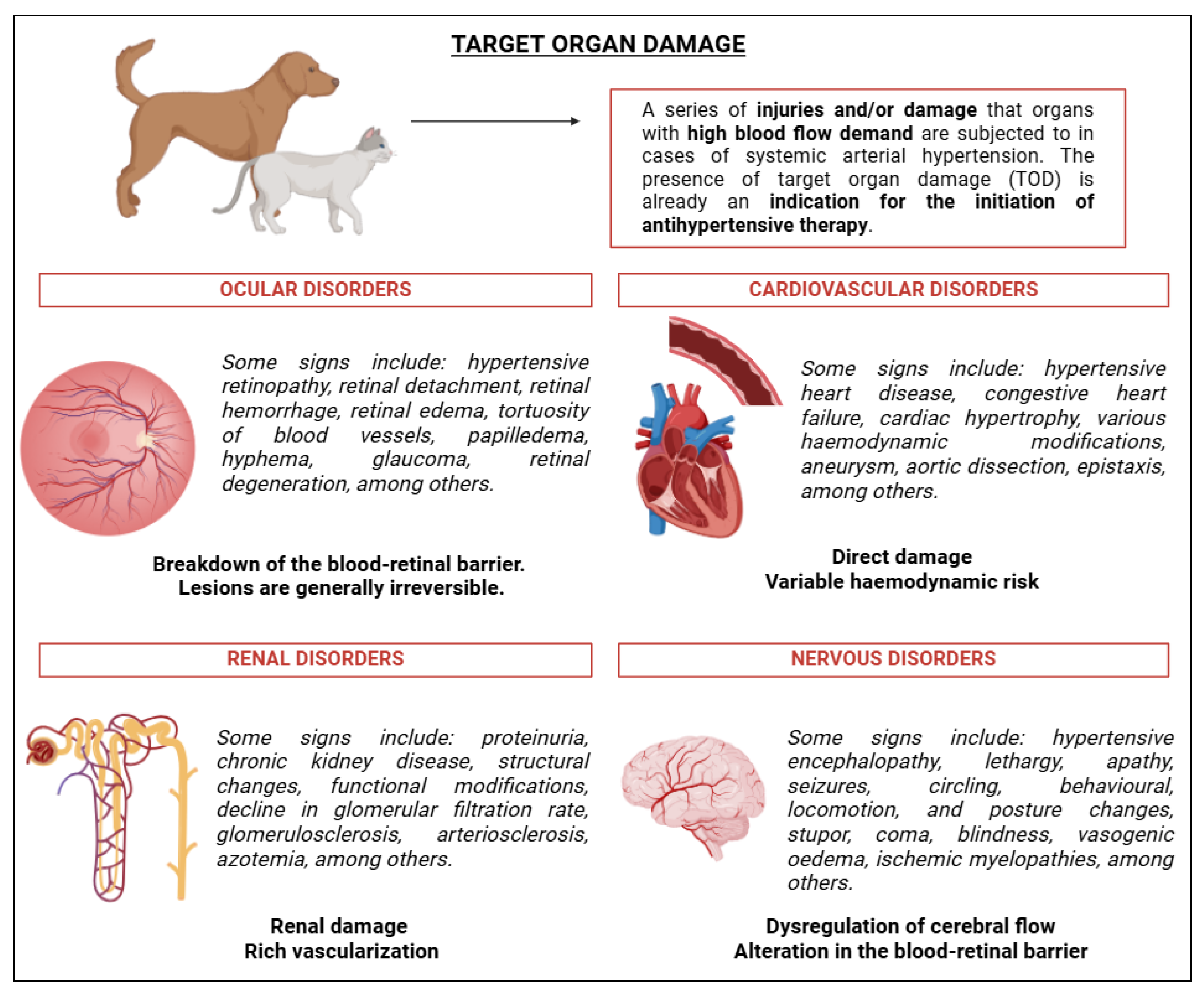
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



