
Submitted:
04 April 2025
Posted:
08 April 2025
You are already at the latest version
Abstract
Background/objectives: Despite advancements in early diagnosis and clinical practices guided by standardized care protocols, Merkel cell carcinoma (MCC) is still marked by an unfavorable prognosis with a 5-year relative survival rate of 65%. Indeed, regional nodal metastases affect 40-50% of MCC patients, while approximately 33% experience distant dissemination. Among these, bone and bone marrow metastases are particularly notable, although the characteristics and clinical implications of this metastatic disease in MCC remain poorly understood. Methods: A comprehensive review was conducted using the Medline database (via PubMed) up to January 2024. The search strategy included the string “(Merkel cell carcinoma AND (bone OR marrow))”. Results: A total of 1,133 (69.3% male and 30.7% female) patients diagnosed with advanced MCC were collected. The median (IQR) age at diagnosis was 67.5 (12.65) years old. 201 (20.8%) cases of bone and/or bone marrow metastases were identified and linked to a primary known MCC in 75.7% of cases. Bone metastases (BMs) appear as the third most common metastatic site, following the liver (2nd) and lymph nodes (1st). They show a mixed biological and radiological behavior, with a marked preference for the axial skeleton over the appendicular one. Addressing characteristics of bone metastatic disease, neurological symptoms were the most documented, whereas bone marrow involvement and leukemic spread seemed to be primarily related to immunosuppression. Multimodal treatment including platinum-based chemotherapy and radiotherapy represented the primary approach for effective management. Conclusions: The pattern of metastatic spread in MCC differ among studies, with the bones resulting as the third most common site of distant spread. Excluding head and neck MCC, which seems to be more regularly associated with liver metastases, the relationship between the primary tumor site and the development of bone or bone marrow metastases appears inconsistent. Overall, BMs mostly correlated with advanced MCC stages and poorer survival outcomes, with a median OS of 8 months (range 12.75-4). The integration of international guidelines alongside the ongoing findings from clinical trials will contribute to improve systemic disease control and enhance patient care.
Keywords:
Merkel cell carcinoma
; metastasis
; bone
; bone marrow
; diagnosis
; dermoscopy
; reflectance confocal microscopy
; treatment
; therapy
; etiology
; origin
; MCC
; MCCUP
; RCM
1. Introduction
Merkel cell carcinoma (MCC) is a rare yet highly aggressive neuroendocrine skin tumor that predominantly affects elderly men, with the head and extremities being the most common sites of occurrence [1]. In recent years, notable advancements have been achieved in the diagnosis and management of MCC, particularly through the introduction of immunotherapy for locally advanced, inoperable, and metastatic disease [2].
Clinical practice is further guided by several guidelines, which aim to standardize care for MCC patients [2,3,4]. Despite these advancements, the overall prognosis remains guarded, with a 5-year relative survival rate of 65% across all Surveillance, Epidemiology, and End Results (SEER) stages combined [5]. Moreover, MCC is associated with a high incidence of local recurrence, particularly within the first 2-3 years following the primary tumor excision. Regional nodal metastases develop in 40–50% of patients, while approximately 33% of them experience distant secondaries affecting various anatomical sites [4]. Among these, bone metastases (BMs) have been identified as the fourth [6] or even the third [7] most common site of distant spread.
Nevertheless, despite the increasing recognition of BMs and bone marrow involvement in MCC, current literature lacks a comprehensive focus on their biological and radiological behavior, the patterns of metastatic spread, and related clinical, demographic, and treatment profiles. This review seeks to offer a comprehensive summary of the latest evidence on MCC epidemiology, etiology, diagnosis, and management, with a focus on the characteristics and impact of bone and bone marrow metastases.
2. Materials and Methods
A comprehensive review was conducted from Medline database (via PubMed) up to January 2024. To address our focus, the search strategy included the string “(Merkel cell carcinoma AND (bone OR marrow))”. Additionally, relevant keywords were used in different combinations for free-hand search and bibliography of selected articles was reviewed.
3. Epidemiology of MCC
Determining precise global incidence rates for Merkel cell carcinoma remains challenging due to geographic and demographic variability, as well as the lack of global epidemiological studies. However, between 2000 and 2013 MCC diagnosis surged by 95%, almost doubling the 57% increase of melanoma cases [8].
In the United States, data from the SEER registry revealed an MCC incidence rate of 0.7 cases per 100,000 person-years in 2013, corresponding to approximately 2,488 cases annually [8]. On a global scale, the incidence of MCC is estimated at 0.6 cases per 100,000 people annually, based on data derived from different individual regions and isolated case reports [9].
Notably, countries in the southern hemisphere, such as Australia (2.5 per 100,000) and New Zealand (0.96 per 100,000), report the highest incidence rates, significantly exceeding those observed in the northern hemisphere [9,10]. Furthermore, nations such as Norway, Denmark, and Japan, which have shown stable incidence rates over time, represent an exception to the overall increasing trend in MCC incidence [11].
As regard the age of MCC patients, the incidence generally rises with it, peaking between 70 and 80 years [11]. Indeed, MCC is relatively rare in younger individuals with only 0.07% of cases occurring in those under 30 years of age [11]. However, when affecting young adults, MCC is often diagnosed at more advanced stages [12].
Based on these data, the trend of incidence is matter of debate. However, several key factors should be considered to understand the phenomenon, combining demographic shifts with environmental exposures and improved diagnostic accuracy: aging population [10], UV-exposure rates [13], increasing MCC awareness among healthcare providers and patients, use of non-invasive diagnostic tools (e.g., dermoscopy, reflectance confocal microscopy) [14,15], greater efficacy and reliance on immunosuppressive therapies [16,17].
4. Etiology and Risk Factors for MCC
4.1. Two (Viral- and UV-Related) Driving Mechanisms for MCC Onset
Similar to other cutaneous malignancies, the pathogenesis of Merkel cell carcinoma is likely the result of a complex interaction between genetic, molecular, and environmental factors. However, MCC recognize two main determinants of pathogenesis: viral and ultraviolet (UV) exposure-related driving mechanisms.
In 2008, researchers identified the integration of a mutated Merkel cell polyomavirus (MCPyV) genome as a key causative factor in the majority of MCC cases [18]. MCPyV, a circular double-stranded DNA virus, is usually acquired during childhood, as defined by the high prevalence of antibodies detectable in the general population against its capsid protein VP1. Despite this virus’ widespread occurrence, primary MCPyV infection is typically asymptomatic, with only a small fraction of individuals developing MCC over time [19]. Therefore, MCC is generally classified as MCPyV-positive or -negative cancer. MCPyV-positive MCC, also defined as Merkel-type sarcoma, represents a pure neuroendocrine carcinoma characterized by the expression of viral oncoproteins, a low tumor mutational burden [20], and a relatively favorable prognosis compared to the counterpart [21]. This variant is thought to arise from dermal fibroblasts or pre/pro B-cells [22,23]. Conversely, patients with MCC often have a history of other cancers, particularly those linked to UV exposure, indicating possible shared etiological factors with these malignancies [24,25,26].
In this regard, approximately 20% of MCC cases are UV-associated MCPyV-negative, a form referred to as squamous cell carcinoma, Merkel type. This subtype of MCC, which was found to be more prevalent in certain geographic regions with high levels of sun exposure [27], arises from UV-induced DNA damages and displays characteristic oncogenetic features: high mutational burden, high p63 expression, inactivation of tumor suppressor genes such as Retinoblastoma 1 (Rb1) and tumor protein 53 (TP53) [28], and high frequency of NOTCH1 and FAT1 mutated [27]. In addition, UV exposure is also responsible for the inactivation of genes involved in DNA damage repair, including KMT2A, KMT2C KMT2D, ASXL1, ARID1A, ARID1B, SMARCA4, and in chromatin-modifying pathways, such as ATM, MSH2, BRCA1, BRCA2, and BCOR [29]. Moreover, also UV-associated MCPyV-negative MCC has been linked with the activation of JAK-STAT pathway, MAPK (HRAS, NF1) pathway [30], PI3K pathway (PIK3CA, AKT1, PIK3CG) and the receptor tyrosine kinase FGFR2 [27]. This subtype, which is mostly associated with a poorer prognosis [21], appears to originate from keratinocytes, epidermal stem cells, or Merkel cells. It exhibits neuroendocrine characteristics or displays a combination of features from both neuroendocrine and squamous cell carcinoma (SCC) cells [1]: it seems to arise from or in association with SCC [20,31,32,33].
The absence of detected MCPyV in these combined tumors suggests that viral involvement is limited to MCPyV-positive MCC cases [34,35].
Beyond the prolonged exposure to UV radiation and MCPvV infection as established causal mechanisms, several risk factors for MCC are identified. Among these, immunosuppression (e.g., HIV positive or AIDS patients, organ transplant recipients, or patients undergoing immunosuppressive treatments) [16,36,37], advanced age (over 70 years old) [11], male gender [10,11], fair skin [13], personal history of other skin cancers are the main recognized.
4.2. The Debate of MCC Cell of Origin
The identification of the two driving mechanisms in Merkel cell carcinoma pathogenesis has led to a reassessment of its cellular origin, which was originally believed to be the epidermal Merkel cells (from which the tumor gets its name).
Alternative proposed origins for MCC include epithelial progenitor cells, fibroblasts, dermal stem cells, and pre/pro B cells [38,39,40,41] (Table 1). Merkel cells are highly specialized epithelial cells that function as mechanoreceptors, located in the basal layer of the epidermis and the external part of the hair follicle. Both Merkel cells and MCC share several features. Firstly, both cell types exhibit high expression of the ion channel Piezo2, a protein that facilitates the conversion of mechanical signals into electrical signals [42,43]. Secondly, the differentiation of Merkel cells is driven by the expression of specific transcription factor known as atonal homolog 1 (ATOH1) [44], which is also represented in MCC [45]. Additionally, immunohistochemical studies have shown that both Merkel cells and MCC express common markers, such as cytokeratin 20 (CK-20) and neuroendocrine markers like chromogranin A and synaptophysin [22].
However, Merkel cells are primarily post-mitotic, thus exhibiting low sensitivity to oncogenic stimuli [44]. Moreover, they are placed in the basal layer of the epidermis, while MCC typically affects the dermis and subcutaneous tissues [41]. Furthermore, Merkel cells are mostly represented in the palms and soles [46], whereas MCC predominantly occurs in sun-exposed areas, such as the head and neck, or limbs [10,38]. Lastly, no reports of Merkel cells being infected by Merkel cell polyomavirus (MCPyV) have been described [47], and MCPyV small T-antigen (ST) has failed to induce Merkel cell proliferation or transformation in transgenic murine models [48]. The similarities between Merkel cells and MCC may be linked to the acquisition of the neuroendocrine phenotype from different cell type during the oncogenic process of MCC [49]. In MCC, both sun exposure and virus-induced oncogenic triggers may act on shared molecular pathways, notably involving the loss of the retinoblastoma protein (Rb). In this sense, the sequestration of the tumor suppressor Rb by MCPyV is a critical step in the pathogenesis of MCPyV-positive MCC [28,50]. Alternatively, MCPyV-negative MCC tumors lose Rb expression due to somatic mutations [28,51]. In other types of skin tumors, the loss of Rb has been demonstrated to play a role in the development of a neuroendocrine phenotype [52,53,54]. Moreover, Rb inactivation may lead to increased expression of ATOH1, a transcription factor involved in Merkel cell differentiation [55].
Based on these findings, alternative origins for MCC cells have been proposed, including epithelial non-Merkel cells, fibroblastic cells, and B-cell lineages [22]. Among these, epithelial stem cells - considered the most likely progenitors of differentiated Merkel cells [56,57,58] - have been proposed as a potential cell of origin for MCC [22,41].
Observations of MCC tumors suggest that UV-induced cases likely originate from a progenitor cell within the epidermis [59]. The UV mutation signature observed in MCPyV-negative MCC indicates that this cancer may have an epithelial origin, specifically arising from keratinocyte progenitor in the interfollicular epidermis, and acquiring the ability to differentiate into Merkel cells during the oncogenic process [22,41]. In MCC, this signature is characterized by specific types of mutations, particularly C to T transitions, frequently involving key tumor suppressor genes like tumor protein 53 (TP53) and Rb1. The dual inactivation of the TP53 and Rb1 genes is also observed in small cell lung cancer (SCLC), a neuroendocrine carcinoma that shares significant phenotypic similarities with MCC. In SCLC, the inactivation of these genes drives both transformation and neuroendocrine differentiation in epithelial cells [60,61]. Intriguingly, the notion that an epithelial cell serves also as the origin of MCPyV-positive MCC remains a topic of debate, primarily due to the inability of epidermis-targeted T-antigen expression to produce MCC tumors in pre-clinical models [22,23]. Alternatively, the occurrence of MCPyV-positive MCC could be explained by the integration of MCPyV in cutaneous appendages enriched with Merkel cell precursors [22,23]. Nevertheless, the specific cell type in which MCPyV integration occurs is still unclear.
The absence of connection between MCC tumor cells and the epidermis, along with the lack of a UV mutation signature, suggests a potential non-epithelial origin for this neoplasia Indeed, MCPyV-positive MCC may originate from dermal mesenchymal cells for several reasons. First, a non-epithelial origin could account for the low tumor mutational burden and the absence of the UV signature typically seen in MCPyV-negative MCC. Second, the deep localization of fibroblast stem cells might account for the predominantly dermal occurrence of MCC [40]. Moreover, this hypothesis aligns with the virus’ natural life cycle, according to studies that shows how dermal fibroblasts support the complete MCPyV cycle in vitro [62,63].
Finally, fibroblasts have the potential to be reprogrammed into pluripotent cells [64] suggesting the possibility that they could adopt a Merkel cell phenotype. However, this theoretical concept still needs to be experimentally validated.
In addition to the absence of epidermal connection, MCC may express B cell markers, such as TdT and PAX5, with some MCPyV-positive MCC cases exhibiting immunoglobulin (Ig) rearrangement. These findings indicate that MCPyV-positive MCC may originate from pre-/pro-B cells [65]. Furthermore, both MCCs often shares phenotypic similarities with B-cell neoplasia, and MCPyV can integrate itself into hematopoietic cells, potentially guiding the transformation of B cells. To date, the failure to acquire a Merkel cell phenotype in these instances argues against B-cell origin of MCC [23].
5. Clinical Features and Diagnosis of MCC
The diagnosis of Merkel cell carcinoma is established through a comprehensive approach that includes clinical assessment, noninvasive imaging, and histopathological analysis with immunohistochemistry.
From a clinical perspective, MCC typically presents as a pink or red-violaceous, painless, firm, rapidly growing nodule or plaque, this last one theoretically more detectable in the early stages of the disease [1]. Four distinct clinical presentations have been proposed and described as representative of MCC: Pinkish plaque, cherry red nodular, ulcerated erythematous nodular, and hyperkeratotic nodular MCC [66]. Interestingly, while the first three clinical findings were histologically consistent with "classic MCC," the final one was identified as MCC associated with SCC [66]. Compared to pure MCC, the coexistence of MCC and SCC is a rare occurrence, more commonly observed in immunosuppressed patients and associated with poorer outcomes [67,68]. Additionally, MCC can occasionally coexist with Bowen’s disease (BD), with a recent review identifying 13 cases of MCC overlapping with BD [69]. This combination appears to be more common in females, typically presenting as a rapidly growing single nodule on a red-brownish plaque, often located on the face [69].
Although MCC is commonly found in sun-exposed areas, it can also rarely arise from the oral mucosa and/or lips, which are of dermatological interest as potential primary tumor sites. This has been reported in both adults [70,71,72,73,74,75,76] and young individuals, starting from the age of 14 [77,78,79]. In these cases, MCC typically presents as an ulceroproliferative or pinkish-red, rapidly growing nodule, especially when located at the vermillion border or labial semi-/mucosa [75]. Furthermore, cases of MCC involving the penile or scrotal region have been documented less frequently (n=2) [80,81] compared to those occurring in the vulvar region (n=18) [82,83]. Pain and perilesional erythema have also been noted as additional characteristics for these specific locations.
Along with clinical evaluation, dermoscopy and reflectance confocal microscopy (RCM) represent two non-invasive imaging techniques that have proven to be highly valuable in diagnosing MCC [85]. The primary dermoscopic features of MCC include a variably focused and dilated polymorphous vessels set on homogeneous pinkish, milky red structureless background, togheter with shiny or not-shiny white areas [66,84].
Differently from BD and its glomerular and/or dotted vessels at dermoscopy [86], in MCC the dermoscopic vascular pattern is characterized by irregular linear vessels, either alone or in combination with glomerular or arborizing vessels (vascular polymorphism) supporting the differential diagnosis [66].
In RCM, MCC displays aggregates of hyporeflective small cells bordered by fibrotic linear septae, which have been previously reported as highly suggestive of the disease [85] in support of a clinical and dermoscopic suspicion of MCC [66]. Additionally, larger polymorphic hyper-reflective cells, likely representing highly proliferative cells, may also be observed [85].
Given the above, MCC final diagnosis relies on histological examination revealing the infiltration of the dermis/hypodermis by small, round, blue proliferating tumor cells (with hematoxylin-eosin staining), which exhibits immunohistochemical features of high-grade neuroendocrine carcinoma [86]. Notably, MCC cells express various cytoskeletal keratins (CKs), including CK20 (membranous and/or paranuclear dot-like), CK8, CK18, CK19; and neuroendocrine markers such as chromogranin A, synaptophysin, cluster of differentiation (CD) 56, and neuron-specific enolase (NSE). Conversely, they are typically negative for thyroid transcription factor 1 (TTF1), leukocyte common antigen (LCA), protein S100, melan A, vimentin and CK7(3). Less than 10% of MCC cases are negative for CK20(3).
Thus, immunohistochemical staining showing neurofilament positivity (+), CK-20 positivity (+), CK-7 negativity (-), and TTF-1 negativity (-) offers high sensitivity and specificity in differentiating MCC from common histopathological mimics, such as SCLC, neuroblastoma, Ewing sarcoma, melanoma, and lymphoma [87,88,89] (Table 2). In rare cases, MCC may test positive for TTF1 or CK7, so the interpretation of staining patterns for these two antigens should be done with caution [3,90].
6. Staging System (AJCC 8th Edition) and Prognostic Factors
Staging of Merkel Cell Carcinoma involves the TNM system, evaluating the size and extent of the primary tumor (T), the involvement of regional lymph nodes (N), and the presence of distant metastases (M) [93]. The American Joint Committee on Cancer (AJCC) classification (8th edition) refines this by distinguishing lymph node involvement into clinical (N) and pathological (pN) stages, based on whether lymph nodes are assessed through physical examination or histopathological evaluation [93]. According to this system (Table 3), MCC is classified as follows: stages I and II for skin-limited disease; stage III for regional lymph node involvement or an undetectable primary tumor; and stage IV for distant metastatic disease beyond regional lymph nodes [93].
Clinical staging relies on physical examination, lymph node palpation, and imaging studies, though routine baseline imaging is not always recommended [2]. However, 2-deoxy-2-[18F] fluoro-D-glucose ([18F] FDG) positron emission tomography (PET)/computed tomography (CT) (FDG PET/CT) scan is a critical tool for staging and re-staging MCC, as it effectively identifies metastatic disease particularly in the bone and bone marrow, which may be missed by standard CT scans [94].
Sentinel lymph node biopsy (SLNB) represents the most reliable method for detecting subclinical nodal involvement, utilizing a specific immunohistochemical panel [3]. Pathological staging involves microscopic examination of tissue samples obtained through lymph node biopsies, organ biopsies, or needle biopsies [88,93,95].
Survival in MCC is mainly determined by the stage at diagnosis. The 5-year overall survival (OS) rate drops significantly as the stage advances, from 62.8% at stage I to 13.5% at stage IV (AJCC 8th edition) [96,97]. However, a recent cohort study interestingly found that only 65% of deaths were directly attributed to MCC-related causes [98].
In terms of prognosis, MCC is characterized by its high recurrence rates: local recurrence (27-60%), regional lymph node involvement (45-91%), and distant metastasis (13-52%) [93,99,100].
Integrating current evidence, MCC patients are considered as high-risk for recurrence if they exhibit one or more modified adverse risk factors (mARF), including tumor size ≥2 cm (or >1 cm per NCCN guidelines v1.2024), chronic immunosuppression (e.g., HIV, chronic lymphocytic leukemia, or solid organ transplant), head and neck primary sites, lymphovascular invasion, pathologically positive lymph nodes, or incomplete lymph node evaluation [2,3,4,101,102].
On the other hand, several factors, including Rb protein expression, intratumoral CD8 T-lymphocyte infiltration, and MCPyV LT antigen expression, show promise as positive prognostic markers but need further validation [3]. In this context, testing for MCPyV oncoprotein antibodies should be performed in the initial assessment, as seropositive patients could potentially use antibody levels to monitor recurrence, thereby reducing the need for frequent imaging [103]. Conversely, seronegative patients face a 42% higher recurrence risk and necessitate a closer surveillance [103].
Due to the rarity of MCC, the understanding of metastatic patterns and prognosis at stage IV remains incomplete, with data showing considerable variability. Patients with bone or liver metastases report significantly worse OS (p < 0.01) and an increased risk of Merkel-specific death (HR: 3.06 for bone metastases and HR: 2.09 for liver metastases, p<0.001) [7]. However, another study found that although liver and brain metastases were significantly associated with poorer disease-specific survival (DSS), bone metastases did not show the same correlation [104]. Additionally, patients with metastases to the bone, liver, and distant lymph nodes seemed to also have a higher risk of regional lymph node involvement [101].
Excluding the following articles due to the lack of individual data [6,104,111,127,131,140,142,157] (Table 4), the median OS for bone and bone marrow metastatic MCC was 8 months (range 12.75-4).
Further studies are needed to provide definitive and comprehensive evaluations.
7. Bone and Bone Marrow Metastases in MCC
7.1. Type of Bone Metastases
Bone metastases (BMs) can be classified in two types according to histopathology: osteoblastic or bone-forming BMs, as reported in prostate cancer and breast cancer; osteolytic or bone-destructive BMs, as metastases from kidney, thyroid, lung cancers, multiple myeloma; and mixed BMs, that is the combination of both osteoblastic and osteolytic processes (as less often reported in breast cancer) [105].
Considering literature data about the biological behavior of these different pathological bone secondaries, the diversification partially influences prognosis since osteolytic lesions are often more aggressive, and generally show quicker progression compared to the sclerotic metastases [105,106]. Additionally, tumor cell proliferation within bone marrow precedes bone destruction, making bone damage a relatively delayed feature of bone metastasis [106,107], and explaining the variable development of bone pain and fractures.
Few data are reported about the nature of BMs in Merkel cell carcinoma. The evidence derived from imaging studies suggests a major mixed behavior for BMs in MCC, as demonstrated by the radiopaque/hyperdense (when osteoblastic) or radiolucent/hypodense (when osteolytic) signal on radiography (X-ray) or computed tomography (CT) scan, respectively [108]. Cases of intracranial metastasis through [109] or without [110] bone destructions have been reported, although arterial or venous spread represent the most common via of bone dissemination [110]. The specific venous drainage and veno-lymphatic anastomoses generated by MCC neoplastic clones may explain the evidence.
7.2. Pattern of Metastatic Spread and Association Between Primary MCC and BMs
Merkel cell carcinoma has a high recurrence rate, especially within the first 2-3 years after excision, with 40-50% of patients developing regional lymph node (LN) metastases and about 33% experiencing distant metastases [4].
Common distant metastasis sites include non-regional LNs (41%), skin/soft tissue (25%), liver (23%), bone (21%), pancreas (8%), lung (7%), and brain (5%) (percentages exceeded 100% because some patients had metastatic disease involving multiple sites) [6].
However, the reported patterns of metastatic spread in the literature vary across different studies. In 2024, Kim et al. analyzed 151 patients who had received treatment for MCC and examined the relationship between primary tumor site and distant metastasis. They found that after a median follow-up of 11 months, 58.9% of patients had a single metastatic site, while 41.1% had multiple. The most common metastasis sites were distant LNs (62.3%), followed by skin/soft tissues (26.5%) and bone (26.5%) [7].
Different authors reported different data about the most common distant metastatic sites in MCC, and BMs are typically preceded by other involvements such as non-regional LNs (the most frequent), skin, and lung [96] or abdominal organs [100]. Nevertheless, non-regional LNs are not always the primary sites affected by distant metastases. Gonzalez et al. reported that the most common metastatic sites were the liver (39.3%), followed by distant LNs (38.3%), bone (27.7%), and lung (21.9%) [101]. Similarly, Xia et al. found liver metastasis to be the most common (13.5%), followed by bone (11.3%) and lung (8.4%) secondaries [111].
Regarding the association between the primary MCC and BMs, notably, patients with upper limb/shoulder primaries were less likely to develop distant LNs or liver metastases (p=0.02 and p=0.04), while those with head and neck primaries were more likely to develop liver metastases (p<0.01) [7]. This observation was supported by Maloney et al., who demonstrated that head and neck primary MCC was associated with liver metastases (p=0.0003), in contrast to primary tumors in the lower limbs [104]. These findings regarding the likelihood of liver metastasis in MCC are consistent with previously published data, which show a higher incidence in head/neck primary tumors (43% of 58 patients) compared to lower limb primaries (5% of 39 patients; p<0.0001) [6].
On the other hand, patients with trunk primary MCCs exhibited higher rates of positive lymph nodes and seemed more prone to developing bone metastases (p=0.0049) [112]. Nevertheless, this data is not fully corroborated, as Kim et al. found bone metastases to be more frequently associated with head and neck (37.5%) or upper limb primaries (22.5%) than with trunk primaries (17.5%) [7].
In this review, we summarized the prevalence of single metastatic localizations from SEER databases and retrospective mono-/multi-centric studies, collecting a total of 967 metastatic events at presentation or during follow up reports. In decreasing order of prevalence, the pattern of metastatic spread was as follows: LNs (27.8%, n=269), liver (21.2%, n=205), bone (19%, n=184), lung (10.5%, n=102), skin and subcutaneous tissue (8.6%, n=83), brain (3.1%, n=30), gastric (2.3%, n=23), spinal cord (2.2%, n=21), bone marrow (1.8%, n=17), pancreas (1.4%, n=14), testis (1.2%, n=12), retroperitoneum/thyroid gland (0.4%, n=3 each), and heart (0.1%, n=1) [6,7,102,104,110,111,113,114,115,116,117,118,119,120,121,122,123,124,125,126,127,128,129,130,131,132,133,134,135,136,137,138,139,140,141,142,143,144,145,146,147,148,149,150,151,152,153,154,155,156]. Overall, BMs and bone marrow involvement in MCC are linked to advanced stages [142,143,144] and associated with poorer survival outcomes [101,113].
7.3. Clinical and Demographic Data
44. articles retrieved out of 148 reported bone/bone marrow as metastatic site involved (Table 4). A total of 1,133 (69.3% male and 30.7% female) patients diagnosed with advanced MCC were collected. The median (IQR) age at diagnosis was 67.5 (12.65) years old. 201 (20.8%%) cases of bone and/or bone marrow metastasis were identified and linked to a primary known and unknown MCC in 75.7% and 24.3%, respectively. Sometimes the nature of the primary MCC was not otherwise specified [104,140].
Except for one istance [131], in single-case reports of bone/bone marrow MCC metastasis specifically detailing primary tumor sites (n=30) [110,116,122,124,125,126,127,128,129,130,131,132,133,134,135,136,137,138,139,141,142,143,144,145,146,147,149,150,151,152,153,154,155,156,157,158,159], the anatomical distribution of the primary MCC aligned with typical patterns described in literature to date for this neuroendocrine skin tumor, that are the head and neck (12/28), trunk (8/28), upper (6/28) and lower arms (2/28), and hand (1/28). Notably, an extremely rare case of MCC arising on the vulva was described [142].
Considering bone localization among all cases reviewed, the specific type of skeletal involvement other than “bone involvement” was documented in 37 patients, with a notable predilection for the axial skeleton (35 cases) [110,116,122,124,125,126,127,128,129,130,131,132,133,134,135,136,137,138,139,141,142,143,144,147,149,150,151,152,153,154,155,157,158,159] over the appendicular one (2 cases) [145,146].
17 cases of bone marrow were collected [126,127,128,129,130,131,132,133,134,135,136,137,139,142,158,159]. When extramedullary intraspinal MCC metastases were documented, the involvement of the epidural space [122,141,143,144,150,151,152] resulted more common than the intradural one [122,124,142].
Other than pain [144,145,155], the neurological symptoms were the most observed with seizures [138], signs resulting from compression of the spinal nerve roots [152], weakness/numbness [143,150,155], paresthesia [144,156] balance disturbance [122], paraplegias following extra-dural spinal masses [141,150] as the most characteristic; headache was also noted [122]. However, based on detailed case reports, only 10 out of 39 (25%) documented symptomatic disease, suggesting that metastatic bone or bone marrow MCC is typically asymptomatic. Interestingly, leukemic spread during bone marrow disease was documented and linked to certain forms of immunosuppression, suggesting a potential association. These included patients receiving organ transplantation [129,132,158,159], patients with concomitant autoimmune disorders and treated with immunosuppressant therapies (systemic lupus erythematous [126,133], rheumatoid arthritis [128,137,159]), and patients affected by various hematologic conditions (Waldenström macroglobulinemia, plasma cell myeloma, myelodysplastic syndrome, JAK2-positive polycythemia vera, chronic lymphocytic leukemia) [127,130,131,136]. In one case, MCC affected a pregnant woman leading to a rapidly progressing visceral multi-metastatic disease that proved fatal [155].
7.4. Imaging Features of MCC Across Different Diagnostic Techniques
Imaging represents an essential tool in Merkel cell carcinoma management, from early detection to accurate staging. Whole-body FDG-PET/CT or whole-body contrast-enhanced CT scans are mandatory to assess disease extension [3]. PET/CT scan has been reported as more sensitive than CT alone, resulting in an upstage of the disease (7% of cases, mainly stage I/II to stage III) [94,160] and therefore it should be preferred over CT alone when available [161]. Additionally, 8 to 14-megahertz regional lymph nodes ultrasound (US) should be integrated to examine all the main lymph node basins in patients with clinical stage I-II at baseline [3].
To date, the indications about the execution of head/brain imaging slightly differs among the guidelines considered: while ESMO-EURACAN Clinical Practice Guideline indicated brain imaging for head/neck located MCC primaries [3], the European consensus-based interdisciplinary guideline did not routinely recommend brain imaging in asymptomatic stage I/II patients [4].
A synthesis of literature data supports the use of whole-body imaging, such as PET/CT scans, extending to the neck when the primary tumor is located in the head or neck region, as part of the baseline assessment. Additionally, brain MRI should be conducted in cases of neurological symptoms or when a direct cranial extension of the tumor is suspected [2,3,4]. In our experience, for elderly patients with head and neck MCC presenting with at least one mARF or a negative sentinel lymph node biopsy (SLNB), we typically recommend whole-body PET/CT imaging integrated with head and neck CT or MRI scan.
Primary MCC has nonspecific strictly imaging features [108,162]. Nevertheless, certain suggestive findings can aid in its identification: cutaneous or subcutaneous firm nodule, mass within or around muscle tissue; necrosis in larger lesions (>2cm), rare calcifications [108]; significant contrast uptake both for CT and MRI, in accordance with the pathology of fibrovascular separation between clusters of tumor cells and enriched blood sinuses [47]. Among the different imaging techniques available primary MCC mainly appears as follows: a) on US, it shows heterogeneous echogenicity (mainly hypoechoic nodules arising from the dermis/hypodermis), prominent branching/chaotic vascularity, occasional perpendicular hypoechoic linear bands resembling “columns of smoke”; b) on CT, focal skin thickening associated with the cutaneous/subcutaneous nodule, contrast enhancing particularly evident for lesions located in the subcutaneous tissue, signs of tissue edema (fat stranding near the primary lesion); c) on MRI, hypo- to isointensity on T1-weighted images and either hyperintensity or isointensity on T2-weighted images and STIR sequences; d) on FDG PET/CT, hypermetabolic signal is consistent with a malignant proliferation [7,47,162], particularly, for a SUV value of 7.5 ± 3.9 (mean ± SD) [163]. A recent umbrella review of meta-analyses aimed to provide updated evidence to guide appropriate referrals for specific radiopharmaceutical PET/CT or PET/MRI in solid cancers. This review reported a sensitivity and specificity of 0.91 (95% CI 0.85–0.95) and 0.93 (95% CI 0.86–0.97), respectively, for nodal staging in MCC using FDG PET/CT. It also recommended FDG PET/CT for initial lymph node staging and for cases of nodal or distant metastases from unknown primary MCC. Otherwise, DOTA-peptide imaging can be considered in case of FDG PET/CT negativity [163].
Limited data have been published in literature regarding imaging features of bone metastatic MCC. PET/CT, PET/MRI and CT scans are more effective than MRI alone in detecting bone abnormalities (cortical destruction and/or periosteal reaction) and accurately defining bone signals, as particularly demonstrated in well-known metastatic bone cancers [164]. However, MRI for its highly sensitivity can be particularly indicated for detection of bone marrow involvement and extraosseous extension of the tumor [144,165]. Additionally, MRI is the technique of choice in case of cord compression from pathologic vertebral body fracture and/or concomitant spinal cord oedema (focal high T2 phase) [152]. In any case, with the use of intravenous contrast, T1-weighted MRI with fat saturation (STIR) will show intense uptake in the metastatic body, along with any associated variable focal areas of hypointense necrosis [166].
As mentioned above, the mixed nature of BMs in MCC is responsible of the combined response to X-ray-based imaging, depending on the grade of absorption [108]. Practically, on X-ray or CT scan while the osteoblastic lesions appear as round/nodular, well-defined, radiodense or hyperdense bone lesions, the osteolytic BMs in MCC are described as ill-defined, thinned/with absent trabeculae, lucent or hypodense bone lesions [146]. When contrast enhancement is performed, hypervascularity during the arterial phase of enhancement explains the signal increase [167].
On FDG PET/CT, a focal rediotracer uptake in the bones involved is typical (hypermetabolic lesions), with osteolytic metastases presenting as photopenic and characterized by increased activity peripherally [168,169]. Whole-body PET/MRI has demonstrated superior detection of liver metastases compared to PET/CT, although this data has not yet been tested for MCC [170].
Among the other imaging techniques generally adopted to detect BMs and cited in current guidelines, bone scintigraphy is useful and generally used as first-line modality in patient with suspect bone metastasis. Using a radioactive substance, typically technetium-99m (Tc-99m) labeled with a bone-seeking compound like methylene diphosphonate (MDP), it provides whole-body imaging, and although less specific, it needs much smaller change in normal-to-abnormal bone for detection compared to plain radiographs [171]. Moreover, the overall sensitivity among the different radiologic techniques is the following: plain radiographs have low sensitivity (~50%) compared to bone scintigraphy (80%, range 62-100%), CT (85%, range 71-100%), and MRI (90%, range 82-100%) [171,172].
7.5. Treatment of Metastatic Bone/Bone Marrow MCC
The treatment of metastatic bone/bone marrow Merkel cell carcinoma varies widely, ranging from single-modality approaches to multimodal regimens.
Among the 201 cases reviewed, chemotherapy (CHT) alone was utilized in 13 cases (6.4%) [110,126,134,135,139,140,148,152,158,159], with median Merkel specific survival (MSS) (IQR) of 8 (8) months. The treatment regimens mainly included platinum-based agents, often combined with etoposide [110,134,135,139,152,158]. Cyclophosphamide, typically in combination with doxorubicin or vincristine, was also utilized [126,139]. Additionally, other agents such as bleomycin [152], 5-fluorouracil, methotrexate [110,159], topotecan hydrochloride, and paclitaxel [110] were sporadically adopted. Furthermore, radiotherapy (RT) alone [116,159] and surgical intervention alone [145,151] were administered in two (1%) cases both, respectively.
Multimodal approaches were more adopted, with CHT combined with RT described in 73 cases (36.3%) [6,128,136,138,142,144,147,150,154,155], or with immunotherapy in 11 cases (5.5%) [113,125]. A comprehensive regimen including CHT, RT, and surgery was applied in 32 cases (16%) [111,153], with immunotherapy instead of CHT utilized in 40 patients (20%) within the triple-therapy regimen group [7]. Dual-modality treatments were also documented, with CHT with immunotherapy in 11 cases (5.5%) [113,125], RT and surgery in 4 cases (2%) [122,141,143,146], and RT combined with immunotherapy in 2 cases (1%) [124,149]. Unfortunately, 7 (3.4%) patients died before receiving the specific adjuvant treatment or immediately after surgery of the primary tumor [129,130,132,133,151,156,158].
For patients undergoing immunotherapy, the treatment involved immune checkpoint inhibitors (ICI), specifically Avelumab, an anti-programmed cell death protein-ligand 1 (PD-L1) human immunoglobulin G1 (IgG1) antibody [124,125,149]. However, this data is not consistently defined [7,113].
In general, the management of metastatic bone MCC needs to be individually tailored. While surgery, potentially involving prosthetic replacement, may be an option for a single metastatic site, stereotactic hypofractionated radiotherapy should be considered for fit patients with oligometastatic bone disease (defined as ≤3 sites). Interestingly, a multivariate analysis by Gonzalez et al. revealed that MCC patients with bone metastases who underwent surgery to remove one of the metastatic sites (bone or other) had 0.92 times lower risk of death [101]. This finding aligns with existing literature, which highlights that incorporating surgery into multimodal treatment can be a favorable prognostic factor for disease-free survival in MCC [173,174]. Nevertheless, systemic immunotherapy should be prioritized in the absence of contraindications with the available options including Avelumab (anti-PD-L1 human monoclonal IgG1 antibody, FDA and EMA approved), Pembrolizumab (anti-PD-1 humanized monoclonal IgG4 antibody, FDA approved), Retifanlimab (anti-PD-1 humanized monoclonal IgG4 antibody, FDA and EMA approved), and Nivolumab (anti-PD-1 human monoclonal IgG4 kappa antibody, not FDA nor EMA approved). Given the limited published data, priority should be given to enrolling patients in clinical trials whenever possible, alongside decisions guided by a multidisciplinary treatment team following tumor board consultation.
8. MCC General Management
Treatment of Merkel cell carcinoma involves a combination of surgery, radiation, and systemic immunotherapy, with this latter playing a significant role in improving patient outcomes and prognosis [175]. The standard of care for early-stage (stage I-II) MCC involves performing a wide local excision (WLE) or Mohs micrographic surgery (MMS), with MMS being preferred when WLE is impractical or for tumors located in the head and neck area to minimize the need for additional procedures [176,177,178,179,180]. After surgery, adjuvant radiotherapy (RT) is recommended for residual macroscopic (R2) (better if < 1cm) or microscopic (R1) disease, or when mARFs are detected despite clear margins [2].
During surgery, a sentinel lymph node biopsy (SLNB) should be also performed. If the results are negative, the decision between observation or adjuvant RT to the nodal basin should be made by a multidisciplinary team. In cases where SLNB is unreliable - due to immunosuppression, anatomical constraints, or atypical lymph node drainage - or if SLNB is not feasible with risk of false negatives (e.g., patients with immunosuppression, unusual lymph node drainage, or multiple lymph node basins, such as in head and neck or midline trunk MCC) [2,3], adjuvant RT to both the primary site and the nodal basin should be considered.
Since the high recurrence risk of stage III MCC, after SLNB or biopsy confirmation of clinically/imaging-detected nodal metastases, adjuvant RT to the nodal basin combined with complete lymph node dissection (CLND) is recommended, especially for patients with multiple affected lymph nodes or extranodal disease extension [3]. This approach aids in reducing recurrence and enhancing survival outcomes.
For patients with clinically evident nodal disease (stage IIIB), the preferred treatment involves combined CLND plus RT, or clinical trials that incorporate neoadjuvant systemic therapy, as neither adjuvant RT nor chemotherapy (CHT) has demonstrated a statistically significant improvement in OS [181]. Similarly, in cases of in-transit metastases (also stage IIIB), treatment typically includes surgery and/or RT, or participation in clinical trials [2]. For these patients, adjuvant CHT is not recommended [3].
Different approaches may be assessed for MCC of unknown primary (MCCUP), which typically is characterized by better outcomes than the primary known’ counterpart [97,182,183]. In these cases, after performing a FDG PET/CT scan to rule out distant metastases, the management generally follows the same guidelines as for stage III known MCC [3]. However, due to the better prognosis associated with MCCUP, patients with exclusive nodal involvement may be candidates for CLND or RT alone, before considering a combined treatment approach.
Despite recent advancements in the diagnosis and treatment of MCC, advanced (stage III) and metastatic (stage IV) disease can still be difficult to cure. For these cases, immunotherapy is recommended as a first- or second-line treatment [3]. Particularly, Nivolumab may be proposed in the neoadjuvant setting when curative surgery or radiotherapy are not feasible, potentially allowing for surgical eligibility. Otherwise, systemic immunotherapy alone is also indicated with a preference for Avelumab and Pembrolizumab [2]. In case of recurrent locally advanced disease, Pembrolizumab and Retifanlimab should be indicated as treatment options over Avelumab [2].
Instead, in metastatic disease all four mentioned ICIs, other than clinical trials, are viable treatment options [2,4]. Otherwise, CHT primarily consisting of platinum-based agents and etoposide, is just reserved for specific circumstances [2].
A practical diagnostic-therapeutic flowchart following the current evidence has proposed in Figure 1.
Due to the aggressive nature of MCC and the limited systemic control of the disease, regular follow-up visits are crucial for patients’ outcome. Complete skin and lymph node examinations are recommended every 3-6 months for the first 3 years and every 12 months until the 5th year for primary tumors without additional high-risk factors. In case of mARFs or stage III patient the schedule plans should be improved and maintained for a lifetime [4,103,175,176].
US of the primary scar, as well as the surrounding area and lymph nodes, should go with the clinical visits [4]. Additionally, stage III patients should also receive whole-body FDG PET/CT scan or contrast-enhanced CT scan of the neck, thorax, abdomen, and pelvis, along with brain MRI or CT (when indicated), every 3-6 months during the first 3 years. Afterward, follow-up imaging should take place every 6-12 months for the next 2 years. For frail patients and those with stage IV disease, a personalized monitoring plan should be implemented [4].
Recent clinical trials have explored the use of adjuvant immunotherapy in surgically treated Merkel cell carcinoma to enhance systemic disease control. Adjuvant immunotherapy with Ipilimumab, when compared to observation in completely resected MCC, has been found to be ineffective in preventing disease progression and is associated with significant toxicity [184]. In contrast, Nivolumab has demonstrated a reduction in the absolute risk of recurrence, with disease-free survival (DFS) rates of 85% at 12 months and 84% at 24 months, compared to 77% and 73%, respectively, in the observation group [185].
Furthermore, a post hoc analysis of DFS by disease stage revealed that although median DFS was not reached for stage IIIA versus IIIB patients, at 48 months, stage IIIB patients receiving immunotherapy had a 70% two-year DFS, compared to just 32% in those who did not receive adjuvant treatment [185].
Several ongoing clinical trials are investigating ICIs, either in combination with RT for advanced MCC or as monotherapy for earlier stages of the disease (NCT04291885, NCT03712605, NCT03271372). Notably, the phase 3 randomized, placebo-controlled ADAM trial (NCT03271372) is expected to provide crucial insights, evaluating Avelumab monotherapy as an adjuvant treatment for stage III MCC patients who have completed definitive therapy, including surgery and/or RT, for clinically detected metastases.
9. Conclusions
Merkel cell carcinoma (MCC) is a rare and aggressive neuroendocrine skin cancer, whose prognosis is still largely dependent on early diagnosis and accurate staging.
While two primary mechanisms (UV-induced and MCPyV-related) have been defined in MCC etiopathology, the precise cellular origin remains unclear.
According to our results, the pattern of metastatic spread in MCC differ among studies, with the bones resulting as the third most common site of distant spread after the liver (2nd) and lymph nodes (1st). Excluding head and neck MCC, which seems to be more regularly associated with liver metastases, the relationship between the primary tumor site and the development of bone or bone marrow metastases appears inconsistent. Furthermore, bone involvement does not reliably correlate with the poorest prognosis among metastatic sites. Nevertheless, the median OS for patients with metastatic bone/bone marrow MCC was 8 months (range 12.75-4).
Addressing the characteristics and impact of bone metastases (BMs), BMs exhibit a mixed biological (osteoblastic/osteolytic) and radiological behavior, with a marked preference for the axial skeleton over the appendicular skeleton. Neurological symptoms are the most observed, whereas leukemic spread during bone marrow disease in immunosuppressed patients may suggest a reasonable correlation.
Due to the absence of approved adjuvant treatments for systemic disease control following surgery, early diagnosis through clinical assessment and non-invasive imaging techniques for primary MCC remains critical to improve patient outcomes. Moreover, routine baseline total-body imaging, including PET/CT scans and regional lymph node ultrasounds, is recommended to detect micro-metastatic or clinically occult disease.
Multimodal treatment, primarily involving platinum-based chemotherapy and radiotherapy, represents the primary approach for effective management of bone/bone marrow disease in MCC. Finally, integrating international guidelines alongside the ongoing findings from clinical trials will contribute to enhance patient care.
Author Contributions
Conceptualization: B.S., E.B. and E.D.; methodology: B.S. and E.B.; validation: B.S. and B.S.; formal analysis: B.S. and E.B.; data curation: E.B. and B.S.; writing—original draft preparation: B.S. and E.B.; writing—review and editing: B.S., E.B., C.R., B.C., C.M., C.B., S.V., F.V., E.M., T.F., G.A., B.M., D.C., E.C., M.F. and E.D.; visualization: B.S., E.B., E.D. and M.F.; supervision: E.D., and M.F.; All authors have read and agreed to the published version of the manuscript.
Funding
Finanziato dall’Unione Europea – NextGenerationEU a valere sul Piano Nazionale di Ripresa e Resilienza (PNRR) – Missione 4 Istruzione e ricerca – Componente 2 Dalla ricerca all’impresa – Investimento 1.1, Avviso Prin2022 indetto con DD N. 104 del 2/2/2022, codice proposta: 2022RY8549_002 – CUP: J53D23003260006.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations not otherwise mentioned in the text are used in this manuscript:
| AIDS | Acquired Immunodeficiency Syndrome |
| ATM | Ataxia-Telangiectasia Mutated |
| AKT1 | A serine/threonine kinase |
| ARID1 | AT-Rich Interactive Domain-Containing Protein 1 |
| ASXL1 | Additional Sex Combs-Like 1 |
| BCOR | BCL6 Corepressor |
| BRCA1/2 | Breast Cancer 1/2 |
| DNA | Deoxyribonucleic Acid |
| DOTA | 1,4,7,10-Tetraazacyclododecane-1,4,7,10-tetraacetic acid |
| EMA | European Medicines Agency |
| FAT1 | FAT Atypical Cadherin 1 |
| FDA | Food and Drug Administration |
| HRAS | Harvey Rat Sarcoma Viral Oncogene Homolog |
| HIV | Human Immunodeficiency Virus |
| HR | Hazard Ratio |
| ICI | Immune Checkpoint Inhibitor |
| IQR | Interquartile Range |
| JAK-STAT | Janus Kinase-Signal Transducer and Activator of Transcription |
| KMT2 | Lysine Methyltransferase 2 |
| MAPK | Mitogen-Activated Protein Kinase |
| MSH2 | MutS Homolog 2 |
| NCCN | National Comprehensive Cancer Network |
| NF1 | Neurofibromin 1 |
| NOTCH1 | Notch homolog 1 |
| PAX5 | Paired Box 5 |
| Piezo2 | Piezo-type mechanosensitive ion channel component 2 |
| PIK3CA | Phosphatidylinositol-4,5-Bisphosphate 3-Kinase Catalytic Subunit Alpha |
| PI3K | Phosphoinositide 3-Kinase |
| SMARCA4 | SWI/SNF Related, Matrix Associated, Actin Dependent Regulator of Chromatin Subfamily A, Member 4 |
| STIR | Short Tau Inversion Recovery |
| TdT | Terminal deoxynucleotidyl Transferase |
| VP1 | Viral Protein 1 |
References
- Dika E, Pellegrini C, Lambertini M, Patrizi A, Ventura A, Baraldi C, Cardelli L, Mussi M, Fargnoli MC. Merkel cell carcinoma: an updated overview of clinico-pathological aspects, molecular genetics and therapy. Eur J Dermatol. 2021 Dec 1;31(6):691-701. [CrossRef]
- Schmults CD, Blitzblau R, Aasi SZ, Alam M, Amini A, Bibee K, Bolotin D, Bordeaux J, Chen PL, Contreras CM, et al. NCCN Guidelines Insights: Merkel Cell Carcinoma, Version 1.2024. J Natl Compr Canc Netw. 2024 Jan;22(1D):e240002.
- Lugowska I, Becker JC, Ascierto PA, Veness M, Blom A, Lebbe C, Migliano E, Hamming-Vrieze O, Goebeler M, Kneitz H, et al. ESMO-EURACAN Clinical Practice Guideline for diagnosis, treatment and follow-up. Merkel cell carcinoma: ESMO Open. 2024 May;9(5):102977.
- Gauci ML, Aristei C, Becker JC, Blom A, Bataille V, Dreno B, Del Marmol V, Forsea AM, Fargnoli MC, Grob JJ, et al. Diagnosis and treatment of Merkel cell carcinoma: European consensus-based interdisciplinary guideline - Update 2022. Eur J Cancer. 2022 Aug;171:203-231. [CrossRef]
- SEER*Explorer: An interactive website for SEER cancer statistics [Internet]. Surveillance Research Program, National Cancer Institute. Accessed at https://seer.cancer.gov/explorer/ on December 23, 2024.
- Lewis CW, Qazi J, Hippe DS, Lachance K, Thomas H, Cook MM, Juhlin I, Singh N, Thuesmunn Z, Takagishi SR, et al. Patterns of distant metastases in 215 Merkel cell carcinoma patients: Implications for prognosis and surveillance. Cancer Med. 2020 Feb;9(4):1374-1382. [CrossRef]
- Kim EY, Liu M, Giobbie-Hurder A, Bahar F, Khaddour K, Silk AW, Thakuria M. Patterns of initial distant metastases in 151 patients undergoing surveillance for treated Merkel cell carcinoma. J Eur Acad Dermatol Venereol. 2024 Jun;38(6):1202-1212. [CrossRef]
- Paulson KG, Park SY, Vandeven NA, Lachance K, Thomas H, Chapuis AG, Harms KL, Thompson JA, Bhatia S, Stang A, et al. Merkel cell carcinoma: Current US incidence and projected increases based on changing demographics. J Am Acad Dermatol. 2018 Mar;78(3):457-463.e2. [CrossRef]
- Li Z, Ji W, Hu Q, Zhu P, Jin Y, Duan G. Current status of Merkel cell carcinoma: Epidemiology, pathogenesis and prognostic factors. Vol. 599, Virology. Academic Press Inc.; 2024. [CrossRef]
- Mohsen ST, Price EL, Chan AW, Hanna TP, Limacher JJ, Nessim C, Shiers JE, Tron V, Wright FC, Drucker AM. Incidence, mortality and survival of Merkel cell carcinoma: a systematic review of population-based studies. Br J Dermatol. 2024 May 17;190(6):811-824. [CrossRef]
- Becker JC SASDUS. Merkel Cell Carcinoma: Integrating Epidemiology, Immunology, and Therapeutic Updates. Am J Clin Dermatol. 2024;25(4):541–57.
- Paulson KG, Nghiem P. One in a hundred million: Merkel cell carcinoma in pediatric and young adult patients is rare but more likely to present at advanced stages based on US registry data. J Am Acad Dermatol. 2019 Jun 1;80(6):1758–60. [CrossRef]
- Stang A, Becker JC, Nghiem P, Ferlay J. The association between geographic location and incidence of Merkel cell carcinoma in comparison to melanoma: An international assessment. Eur J Cancer. 2018 May 1;94:47–60. [CrossRef]
- Scotti B, Vaccari S, Maltoni L, Robuffo S, Veronesi G, Dika E. Clinic and dermoscopy of genital basal cell carcinomas (gBCCs): a retrospective analysis among 169 patients referred with genital skin neoplasms. Arch Dermatol Res. 2024 May 31;316(6):307. [CrossRef]
- Rapparini L, Alessandrini A, Scotti B, Dika E. Invasive penile glans Squamous Cell Carcinoma (peSCC) and Reflectance Confocal Microscopy (RCM): is it a valuable alternative to histopathology? Skin Research and Technology. John Wiley and Sons Inc; 2024.
- Montano-Loza AJ, Rodríguez-Perálvarez ML, Pageaux GP, Sanchez-Fueyo A, Feng S. Liver transplantation immunology: Immunosuppression, rejection, and immunomodulation. Journal of Hepatology. 2023. p. 1199–215. [CrossRef]
- Jallah BP, Kuypers DRJ. Impact of Immunosenescence in Older Kidney Transplant Recipients: Associated Clinical Outcomes and Possible Risk Stratification for Immunosuppression Reduction. Drugs and Aging. 2024. p. 219–38. [CrossRef]
- Feng H, Shuda M, Chang Y, Moore PS. Clonal integration of a polyomavirus in human Merkel cell carcinoma. Science. 2008 Feb 22;319(5866):1096–100. [CrossRef]
- Tolstov YL, Pastrana DV, Feng H, Becker JC, Jenkins FJ, Moschos S, Chang Y, Buck CB, Moore PS. Human Merkel cell polyomavirus infection II. MCV is a common human infection that can be detected by conformational capsid epitope immunoassays. Int J Cancer. 2009 Sep 15;125(6):1250-6. [CrossRef]
- Tsai KY. The Origins of Merkel Cell Carcinoma: Defining Paths to the Neuroendocrine Phenotype. Vol. 142, Journal of Investigative Dermatology. 2022. p. 507–9. [CrossRef]
- Nirenberg A, Steinman H, Dixon J, Dixon A. Merkel cell carcinoma update: the case for two tumours. Vol. 34, Journal of the European Academy of Dermatology and Venereology. 2020. p. 1425–31.
- Kervarrec T, Samimi M, Guyétant S, Sarma B, Chéret J, Blanchard E, Berthon P, Schrama D, Houben R, Touzé A. Histogenesis of Merkel Cell Carcinoma: A Comprehensive Review. Front Oncol. 2019 Jun 10;9:451. [CrossRef]
- Samimi M, Kervarrec T, Touze A. Immunobiology of Merkel cell carcinoma. Current Opinion in Oncology. 2020. p. 114–21.
- Miller RW, Rabkin CS. Merkel cell carcinoma and melanoma: etiological similarities and differences. Cancer Epidemiol Biomarkers Prev. 1999 Feb;8(2):153-8.
- Howard RA, Dores GM, Curtis RE, Anderson WF, Travis LB. Merkel cell carcinoma and multiple primary cancers. Cancer Epidemiology Biomarkers and Prevention. 2006 Aug;15(8):1545–9. [CrossRef]
- Goessling W, McKee PH, Mayer RJ. Merkel cell carcinoma. J Clin Oncol. 2002 Jan 15;20(2):588-98.
- Wong SQ, Waldeck K, Vergara IA, Schröder J, Madore J, Wilmott JS, Colebatch AJ, De Paoli-Iseppi R, Li J, Lupat R, et al. UV-Associated Mutations Underlie the Etiology of MCV-Negative Merkel Cell Carcinomas. Cancer Res. 2015 Dec 15;75(24):5228-34.
- Sahi H, Savola S, Sihto H, Koljonen V, Bohling T, Knuutila S. RB1 gene in Merkel cell carcinoma: Hypermethylation in all tumors and concurrent heterozygous deletions in the polyomavirus-negative subgroup. APMIS. 2014 Dec 1;122(12):1157–66. [CrossRef]
- Pedersen EA, Verhaegen ME, Joseph MK, Harms KL, Harms PW. Merkel cell carcinoma: updates in tumor biology, emerging therapies, and preclinical models. Frontiers in Oncology. 2024. [CrossRef]
- Iwasaki T, Hayashi K, Matsushita M, Nonaka D, Kohashi K, Kuwamoto S, Umekita Y, Oda Y. Merkel cell polyomavirus-negative Merkel cell carcinoma is associated with JAK-STAT and MEK-ERK pathway activation. Cancer Sci. 2022 Jan;113(1):251-260. [CrossRef]
- Harms PW, Verhaegen ME, Hu K, Hrycaj SM, Chan MP, Liu CJ, Grachtchouk M, Patel RM, Udager AM, Dlugosz AA. Genomic evidence suggests that cutaneous neuroendocrine carcinomas can arise from squamous dysplastic precursors. Mod Pathol. 2022 Apr;35(4):506-514. [CrossRef]
- Kervarrec T, Appenzeller S, Samimi M, Sarma B, Sarosi EM, Berthon P, Le Corre Y, Hainaut-Wierzbicka E, Blom A, Benethon N, et al. Merkel Cell Polyomavirus‒Negative Merkel Cell Carcinoma Originating from In Situ Squamous Cell Carcinoma: A Keratinocytic Tumor with Neuroendocrine Differentiation. J Invest Dermatol. 2022 Mar;142(3 Pt A):516-527. [CrossRef]
- Ríos-Viñuela E, Mayo-Martínez F, Nagore E, Millan-Esteban D, Requena C, Sanmartín O, Llombart B. Combined Merkel Cell Carcinoma and Squamous Cell Carcinoma: A Systematic Review. Cancers. 2024 Jan 18;16(2):411. [CrossRef]
- Reisinger DM, Shiffer JD, Cognetta AB, Chang Y, Moore PS. Lack of evidence for basal or squamous cell carcinoma infection with Merkel cell polyomavirus in immunocompetent patients with Merkel cell carcinoma. J Am Acad Dermatol. 2010 Sep;63(3):400–3. [CrossRef]
- DeCaprio JA. Molecular Pathogenesis of Merkel Cell Carcinoma. Annu Rev Pathol. 2021 Jan 24;16:69-91. [CrossRef]
- Engels EA, Frisch M, Goedert JJ, Biggar RJ, Miller RW. Merkel cell carcinoma and HIV infection. Lancet. 2002 Feb 9;359(9305):497-8. [CrossRef]
- An KP, Ratner D. Merkel cell carcinoma in the setting of HIV infection. J Am Acad Dermatol. 2001;45(2):309–12. [CrossRef]
- Harms PW, Harms KL, Moore PS, DeCaprio JA, Nghiem P, Wong MKK, Brownell I; International Workshop on Merkel Cell Carcinoma Research (IWMCC) Working Group. The biology and treatment of Merkel cell carcinoma: current understanding and research priorities. Nat Rev Clin Oncol. 2018 Dec;15(12):763-776. [CrossRef]
- Czapiewski P, Biernat W. Merkel cell carcinoma - Recent advances in the biology, diagnostics and treatment. International Journal of Biochemistry and Cell Biology. 2014. p. 536–46.
- Sunshine JC, Jahchan NS, Sage J, Choi J. Are there multiple cells of origin of Merkel cell carcinoma? Oncogene. 2018. p. 1409–16. [CrossRef]
- Tilling T, Moll I. Which Are the Cells of Origin in Merkel Cell Carcinoma? J Skin Cancer. 2012;2012:1–6.
- Ikeda R, Cha M, Ling J, Jia Z, Coyle D, Gu JG. Merkel cells transduce and encode tactile stimuli to drive aβ-Afferent impulses. Cell. 2014 Apr 24;157(3):664–75. [CrossRef]
- Harms PW, Patel RM, Verhaegen ME, Giordano TJ, Nash KT, Johnson CN, Daignault S, Thomas DG, Gudjonsson JE, Elder JT, et al. Distinct gene expression profiles of viral- and nonviral-associated merkel cell carcinoma revealed by transcriptome analysis. J Invest Dermatol. 2013 Apr;133(4):936-45. [CrossRef]
- Van Keymeulen A, Mascre G, Youseff KK, Harel I, Michaux C, De Geest N, Szpalski C, Achouri Y, Bloch W, Hassan BA, et al. Epidermal progenitors give rise to Merkel cells during embryonic development and adult homeostasis. J Cell Biol. 2009 Oct 5;187(1):91-100.
- Gambichler T, Mohtezebsade S, Wieland U, Silling S, Höh AK, Dreißigacker M, Schaller J, Schulze HJ, Oellig F, Kreuter A, et al. Prognostic relevance of high atonal homolog-1 expression in Merkel cell carcinoma. J Cancer Res Clin Oncol. 2017 Jan;143(1):43-49. [CrossRef]
- Fradette J, Godbout MJ, Michel M, Germain L. Localization of Merkel cells at hairless and hairy human skin sites using keratin 18. Biochem Cell Biol. 1995 Sep-Oct;73(9-10):635-9. [CrossRef]
- Lyu J, Liu S, Lu Y. A case of multiple recurrent facial Merkel cell carcinomas: Treatment and imaging findings. Asian Journal of Surgery. 2023. p. 2548–9. [CrossRef]
- Shuda M, Guastafierro A, Geng X, Shuda Y, Ostrowski SM, Lukianov S, Jenkins FJ, Honda K, Maricich SM, Moore PS, et al. Merkel Cell Polyomavirus Small T Antigen Induces Cancer and Embryonic Merkel Cell Proliferation in a Transgenic Mouse Model. PLoS One. 2015 Nov 6;10(11):e0142329. [CrossRef]
- González-Vela MDC, Curiel-Olmo S, Derdak S, Beltran S, Santibañez M, Martínez N, Castillo-Trujillo A, Gut M, Sánchez-Pacheco R, Almaraz C, et al. Shared Oncogenic Pathways Implicated in Both Virus-Positive and UV-Induced Merkel Cell Carcinomas. J Invest Dermatol. 2017 Jan;137(1):197-206. [CrossRef]
- Hesbacher S, Pfitzer L, Wiedorfer K, Angermeyer S, Borst A, Haferkamp S, Scholz CJ, Wobser M, Schrama D, Houben R. RB1 is the crucial target of the Merkel cell polyomavirus Large T antigen in Merkel cell carcinoma cells. Oncotarget. 2016 May 31;7(22):32956-68. [CrossRef]
- Harms PW, Vats P, Verhaegen ME, Robinson DR, Wu YM, Dhanasekaran SM, Palanisamy N, Siddiqui J, Cao X, Su F, et al. The Distinctive Mutational Spectra of Polyomavirus-Negative Merkel Cell Carcinoma. Cancer Res. 2015 Sep 15;75(18):3720-3727.
- Shamir ER, Devine WP, Pekmezci M, Umetsu SE, Krings G, Federman S, Cho SJ, Saunders TA, Jen KY, Bergsland E, et al. Identification of high-risk human papillomavirus and Rb/E2F pathway genomic alterations in mutually exclusive subsets of colorectal neuroendocrine carcinoma. Mod Pathol. 2019 Feb;32(2):290-305. [CrossRef]
- Meder L, König K, Ozretić L, Schultheis AM, Ueckeroth F, Ade CP, Albus K, Boehm D, Rommerscheidt-Fuss U, Florin A, et al. NOTCH, ASCL1, p53 and RB alterations define an alternative pathway driving neuroendocrine and small cell lung carcinomas. Int J Cancer. 2016 Feb 15;138(4):927-38. [CrossRef]
- Syder AJ, Karam SM, Mills JC, Ippolito JE, Ansari HR, Farook V, Gordon JI. A transgenic mouse model of metastatic carcinoma involving transdifferentiation of a gastric epithelial lineage progenitor to a neuroendocrine phenotype. Proc Natl Acad Sci U S A. 2004 Mar 30;101(13):4471-6. [CrossRef]
- Haigis K, Sage J, Glickman J, Shafer S, Jacks T. The related retinoblastoma (pRb) and p130 proteins cooperate to regulate homeostasis in the intestinal epithelium. Journal of Biological Chemistry. 2006 Jan 6;281(1):638–47. [CrossRef]
- Ostrowski SM, Wright MC, Bolock AM, Geng X, Maricich SM. Ectopic Atoh1 expression drives Merkel cell production in embryonic, postnatal and adult mouse epidermis. Development. 2015 Jul 15;142(14):2533–44.
- Morrison KM, Miesegaes GR, Lumpkin EA, Maricich SM. Mammalian Merkel cells are descended from the epidermal lineage. Dev Biol. 2009 Dec 1;336(1):76–83. [CrossRef]
- Perdigoto CN, Bardot ES, Valdes VJ, Santoriello FJ, Ezhkova E. Embryonic maturation of epidermal merkel cells is controlled by a redundant transcription factor network. Development. 2014 Dec 15;141(24):4690–6. [CrossRef]
- Thibault K. Evidence of an epithelial origin of Merkel cell carcinoma. Mod Pathol. 2022 Apr;35(4):446-448. [CrossRef]
- Park JW, Lee JK, Sheu KM, Wang L, Balanis NG, Nguyen K, Smith BA, Cheng C, Tsai BL, Cheng D, et al. Reprogramming normal human epithelial tissues to a common, lethal neuroendocrine cancer lineage. Science. 2018 Oct 5;362(6410):91-95. [CrossRef]
- Park KS, Liang MC, Raiser DM, Zamponi R, Roach RR, Curtis SJ, Walton Z, Schaffer BE, Roake CM, Zmoos AF, et al. Characterization of the cell of origin for small cell lung cancer. Cell Cycle. 2011 Aug 15;10(16):2806-15. [CrossRef]
- Liu W, Yang R, Payne AS, Schowalter RM, Spurgeon ME, Lambert PF, Xu X, Buck CB, You J. Identifying the Target Cells and Mechanisms of Merkel Cell Polyomavirus Infection. Cell Host Microbe. 2016 Jun 8;19(6):775-87. [CrossRef]
- Liu W, Krump NA, MacDonald M, You J. Merkel Cell Polyomavirus Infection of Animal Dermal Fibroblasts. J Virol. 2018 Feb 15;92(4). [CrossRef]
- Takahashi K, Yamanaka S. Induction of Pluripotent Stem Cells from Mouse Embryonic and Adult Fibroblast Cultures by Defined Factors. Cell. 2006 Aug 25;126(4):663–76.
- Hausen A Zur, Rennspiess D, Winnepenninckx V, Speel EJ, Kurz AK. Early B-Cell differentiation in merkel cell carcinomas: Clues to cellular ancestry. Cancer Research. 2013. p. 4982–7. [CrossRef]
- Scotti B, Cama E, Venturi F, Veronesi G, Dika E. Clinical and dermoscopic features of Merkel cell carcinoma: insights from 16 cases, including two reflectance confocal microscopy evaluation and the identification of four representative MCC subtypes. Arch Dermatol Res. 2025 Mar 17;317(1):587. [CrossRef]
- Suárez AL, Louis P, Kitts J, Busam K, Myskowski PL, Wong RJ, Chen CS, Spencer P, Lacouture M, Pulitzer MP. Clinical and dermoscopic features of combined cutaneous squamous cell carcinoma (SCC)/neuroendocrine [Merkel cell] carcinoma (MCC). J Am Acad Dermatol. 2015 Dec;73(6):968-75. [CrossRef]
- McGowan MA, Helm MF, Tarbox MB. Squamous cell carcinoma in situ overlying merkel cell carcinoma. J Cutan Med Surg. 2016 Nov 1;20(6):563–6. [CrossRef]
- Chen X, Song X, Huang H, Zhang L, Song Z, Yang X, Lei S, Zhai Z. Merkel cell carcinoma overlapping Bowen's disease: two cases report and literature review. J Cancer Res Clin Oncol. 2024 Apr 26;150(4):217. [CrossRef]
- Hayter JP, Jacques K, James KA. Merkel cell tumour of the cheek. Br J Oral Maxillofac Surg. 1991 Apr;29(2):114-6. [CrossRef]
- Mir R, Sciubba JJ, Bhuiya TA, Blomquist K, Zelig D, Friedman E. Merkel cell carcinoma arising in the oral mucosa. Oral Surg Oral Med Oral Pathol. 1988 Jan;65(1):71-5. [CrossRef]
- Yom SS, Rosenthal DI, El-Naggar AK, Kies MS, Hessel AC. Merkel cell carcinoma of the tongue and head and neck oral mucosal sites. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology and Endodontology. 2006. p. 761–8. [CrossRef]
- Longo F, Califano L, Mangone GM, Errico ME. Neuroendocrine (Merkel cell) carcinoma of the oral mucosa: Report of a case with immunohistochemical study and review of the literature. Journal of Oral Pathology and Medicine. 1999;28(2):88–91. [CrossRef]
- de Arruda JAA, Mesquita RA, Canedo NHS, Agostini M, Abrahão AC, de Andrade BAB, Romañach MJ. Merkel cell carcinoma of the lower lip: A case report and literature review. Oral Oncol. 2021 Feb;113:105019. [CrossRef]
- Islam MN, Chehal H, Smith MH, Islam S, Bhattacharyya I. Merkel Cell Carcinoma of the Buccal Mucosa and Lower Lip. Head Neck Pathol. 2018 Jun 1;12(2):279–85. [CrossRef]
- Baker P, Alguacil-Garcia A. Moderately differentiated neuroendocrine carcinoma in the floor of the mouth: a case report. J Oral Maxillofac Surg. 1999 Sep;57(9):1143-7. [CrossRef]
- Prabhu S, Smitha RS, Punnya VA. Merkel cell carcinoma of the alveolar mucosa in a young adult: A rare case report. British Journal of Oral and Maxillofacial Surgery. 2010 Jan;48(1):48–50. [CrossRef]
- Inoue T, Shimono M, Takano N, Saito C, Tanaka Y. Merkel cell carcinoma of palatal mucosa in a young adult: immunohistochemical and ultrastructural features. Oral Oncol. 1997 May;33(3):226-9. [CrossRef]
- Roy S, Das I, Nandi A, Roy R. Primary Merkel cell carcinoma of the oral mucosa in a young adult male: Report of a rare case. Indian J Pathol Microbiol. 2015 Apr 1;58(2):214–6. [CrossRef]
- Tomic S, Warner TF, Messing E, Wilding G. Penile Merkel cell carcinoma. Urology. 1995 Jun;45(6):1062-5. [CrossRef]
- Best TJ, Metcalfe JB, Moore RB, Nguyen GK. Merkel cell carcinoma of the scrotum. Ann Plast Surg. 1994 Jul;33(1):83-5.
- Cwynar M, Chmielik E, Cwynar G, Ptak P, Kowalczyk K. Vulvar Merkel cell carcinoma combined with squamous cell carcinoma of the vulva. Ginekol Pol. 2024;95(6):502–3. [CrossRef]
- Nguyen AH, Tahseen AI, Vaudreuil AM, Caponetti GC, Huerter CJ. Clinical features and treatment of vulvar Merkel cell carcinoma: a systematic review. Gynecol Oncol Res Pract. 2017 Dec;4(1). [CrossRef]
- Koumaki D, Evangelou G, Katoulis AC, Apalla Z, Lallas A, Papadakis M, Gregoriou S, Lazaridou E, Krasagakis K. Dermoscopic characteristics of Merkel cell carcinoma. BMC Cancer. 2024 Jul 1;24(1):785. [CrossRef]
- Dalle S, Parmentier L, Moscarella E, Phan A, Argenziano G, Thomas L. Dermoscopy of merkel cell carcinoma. Dermatology. 2012 May;224(2):140–4.
- Ho J, Collie CJ. What’s new in dermatopathology 2023: WHO 5th edition updates. Journal of Pathology and Translational Medicine. 2023. p. 337–40. [CrossRef]
- Ronen S, Czaja RC, Ronen N, Pantazis CG, Iczkowski KA. Small Cell Variant of Metastatic Melanoma: A Mimicker of Lymphoblastic Leukemia/Lymphoma. Dermatopathology. 2019 Nov 27;231–6. [CrossRef]
- Lewis DJ, Sobanko JF, Etzkorn JR, Shin TM, Giordano CN, McMurray SL, Walker JL, Zhang J, Miller CJ, Higgins HW 2nd. Merkel Cell Carcinoma. Dermatol Clin. 2023 Jan;41(1):101-115.
- Chowdhury S, Kataria SP, Yadav AK. Expression of Neuron-Specific Enolase and Other Neuroendocrine Markers is Correlated with Prognosis and Response to Therapy in Non-Hodgkin Lymphoma. J Lab Physicians. 2022 Dec;14(04):427–34. [CrossRef]
- Bobos M, Hytiroglou P, Kostopoulos I, Karkavelas G, Papadimitriou CS. Immunohistochemical distinction between merkel cell carcinoma and small cell carcinoma of the lung. Am J Dermatopathol. 2006 Apr;28(2):99-104. [CrossRef]
- Kervarrec T, Tallet A, Miquelestorena-Standley E, Houben R, Schrama D, Gambichler T, Berthon P, Le Corre Y, Hainaut-Wierzbicka E, Aubin F, et al. Diagnostic accuracy of a panel of immunohistochemical and molecular markers to distinguish Merkel cell carcinoma from other neuroendocrine carcinomas. Mod Pathol. 2019 Apr;32(4):499-510. [CrossRef]
- Pasternak S, Carter MD, Ly TY, Doucette S, Walsh NM. Immunohistochemical profiles of different subsets of Merkel cell carcinoma. Hum Pathol. 2018 Dec 1;82:232–8. [CrossRef]
- Trinidad CM, Torres-Cabala CA, Prieto VG, Aung PP. Update on eighth edition American Joint Committee on Cancer classification for Merkel cell carcinoma and histopathological parameters that determine prognosis. Journal of Clinical Pathology. 2019. p. 337–40. [CrossRef]
- Hawryluk EB, O'Regan KN, Sheehy N, Guo Y, Dorosario A, Sakellis CG, Jacene HA, Wang LC. Positron emission tomography/computed tomography imaging in Merkel cell carcinoma: a study of 270 scans in 97 patients at the Dana-Farber/Brigham and Women's Cancer Center. J Am Acad Dermatol. 2013 Apr;68(4):592-599. [CrossRef]
- O'Sullivan B, Brierley J, Byrd D, Bosman F, Kehoe S, Kossary C, Piñeros M, Van Eycken E, Weir HK, Gospodarowicz M. The TNM classification of malignant tumours-towards common understanding and reasonable expectations. Lancet Oncol. 2017 Jul;18(7):849-851.
- Medina-Franco H, Urist MM, Fiveash J, Heslin MJ, Bland KI, Beenken SW. Multimodality Treatment of Merkel Cell Carcinoma: Case Series and Literature Review of 1024 Cases. 2001.
- Harms KL, Healy MA, Nghiem P, Sober AJ, Johnson TM, Bichakjian CK, Wong SL. Analysis of Prognostic Factors from 9387 Merkel Cell Carcinoma Cases Forms the Basis for the New 8th Edition AJCC Staging System. Ann Surg Oncol. 2016 Oct;23(11):3564-3571. [CrossRef]
- McEvoy AM, Lachance K, Hippe DS, Cahill K, Moshiri Y, Lewis CW, Singh N, Park SY, Thuesmunn Z, Cook MM, et al. Recurrence and Mortality Risk of Merkel Cell Carcinoma by Cancer Stage and Time From Diagnosis. JAMA Dermatol. 2022 Apr 1;158(4):382-389. [CrossRef]
- Pectasides D, Pectasides M, Economopoulos T. Merkel cell cancer of the skin. Annals of Oncology. 2006 Oct;17(10):1489–95. [CrossRef]
- Song Y, Azari FS, Tang R, Shannon AB, Miura JT, Fraker DL, Karakousis GC. Patterns of Metastasis in Merkel Cell Carcinoma. Ann Surg Oncol. 2021 Jan;28(1):519-529. [CrossRef]
- Gonzalez MR, Bryce-Alberti M, Portmann-Baracco A, Castillo-Flores S, Pretell-Mazzini J. Treatment and survival outcomes in metastatic Merkel cell carcinoma: Analysis of 2010 patients from the SEER database. Cancer Treat Res Commun. 2022 Jan 1;33. [CrossRef]
- Moon IJ, Na H, Cho HS, Won CH, Chang SE, Lee MW, Lee WJ. Clinicopathological characteristics and prognosis of Merkel cell carcinoma: a single-center retrospective study in Korea. J Cancer Res Clin Oncol. 2023 Sep;149(12):10065-10074. [CrossRef]
- Bichakjian CK, Olencki T, Aasi SZ, Alam M, Andersen JS, Blitzblau R, Bowen GM, Contreras CM, Daniels GA, Decker R, et al. Merkel Cell Carcinoma, Version 1.2018, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2018 Jun;16(6):742-774.
- Maloney NJ, Nguyen KA, Bach DQ, Zaba LC. Sites of distant metastasis in Merkel cell carcinoma differ by primary tumor site and are of prognostic significance: A population-based study in the Surveillance, Epidemiology, and End Results database from 2010 to 2016. J Am Acad Dermatol. 2021 Feb;84(2):568-570. [CrossRef]
- Fang J, Xu Q. Differences of osteoblastic bone metastases and osteolytic bone metastases in clinical features and molecular characteristics. Clinical and Translational Oncology. 2015. p. 173–9. [CrossRef]
- Høilund-Carlsen PF, Hess S, Werner TJ, Alavi A. Cancer metastasizes to the bone marrow and not to the bone: time for a paradigm shift! European Journal of Nuclear Medicine and Molecular Imaging. 2018. p. 893–7.
- O’Sullivan GJ. Imaging of bone metastasis: An update. World J Radiol. 2015;7(8):202. [CrossRef]
- Akaike G, Akaike T, Fadl SA, Lachance K, Nghiem P, Behnia F. Imaging of merkel cell carcinoma: What imaging experts should know. Radiographics. 2019 Nov 1;39(7):2069–84. [CrossRef]
- Litofsky NS, Smith TW, Megerian CA. Merkel cell carcinoma of the external auditory canal invading the intracranial compartment. Am J Otolaryngol. 1998 Sep-Oct;19(5):330-4. [CrossRef]
- Barkdull GC, Healy JF, Weisman RA. Intracranial spread of Merkel cell carcinoma through intact skull. Annals of Otology, Rhinology and Laryngology. 2004;113(9):683–7. [CrossRef]
- Xia YJ, Cao DS, Zhao J, Zhu BZ, Xie J. Frequency and prognosis of metastasis to liver, lung, bone and brain from Merkel cell carcinoma. Future Oncology. 2020 Jun 1;16(16):1101–13. [CrossRef]
- Scampa M, Kalbermatten DF, Oranges CM. Demographic and Clinicopathological Factors as Predictors of Lymph Node Metastasis in Merkel Cell Carcinoma: A Population-Based Analysis. J Clin Med. 2023 Mar 1;12(5). [CrossRef]
- Khaddour K, Liu M, Kim EY, Bahar F, Lôbo MM, Giobbie-Hurder A, Silk AW, Thakuria M. Survival outcomes in patients with de novo metastatic Merkel cell carcinoma according to site of metastases. Front Oncol. 2024 Sep 16;14:1444590. [CrossRef]
- Thomas M, Mandal A. An Extremely Rare Case of Metastatic Merkel Carcinoma of the Liver. Cureus. 2021 Nov 17. [CrossRef]
- Kobayashi Y, Nakamura M, Kato H, Morita A. Distant recurrence of Merkel cell carcinoma after spontaneous regression. Journal of Dermatology. 2019. p. e133–4. [CrossRef]
- Payne MM, Rader AE, McCarthy DM, Rodgers WH. Merkel cell carcinoma in a malignant pleural effusion: case report. Cytojournal. 2004 Nov 18;1(1):5. [CrossRef]
- Boghossian V, Owen ID, Nuli B, Xiao PQ. Neuroendocrine (Merkel cell) carcinoma of the retroperitoneum with no identifiable primary site. World J Surg Oncol. 2007 Oct 19;5. [CrossRef]
- Quiroz-Sandoval OA, Cuellar-Hubbe M, Lino-Silva LS, Salcedo-Hernández RA, López-Basave HN, Padilla-Rosciano AE, León-Takahashi AM, Herrera-Gómez Á. Primary retroperitoneal Merkel cell carcinoma: Case report and literature review. Int J Surg Case Rep. 2016;19:21-4. [CrossRef]
- Rossini D, Caponnetto S, Lapadula V, De Filippis L, Del Bene G, Emiliani A, Longo F. Merkel cell carcinoma of the retroperitoneum with no identifiable primary site. Case Rep Oncol Med. 2013;2013:131695. [CrossRef]
- Durastante V, Conte A, Brollo PP, Biddau C, Graziano M, Bresadola V. Merkel Cell Carcinoma with Gastric Metastasis, a Rare Presentation: Case Report and Literature Review. J Gastrointest Cancer. 2023 Mar 1;54(1):309–15.
- Vaiciunaite D, Beddell G, Ivanov N. Merkel cell carcinoma: An aggressive cutaneous carcinoma with rare metastasis to the thyroid gland. BMJ Case Rep. 2019 Apr 1;12(4). [CrossRef]
- Abul-Kasim K, Söderström K, Hallsten L. Extensive central nervous system involvement in Merkel cell carcinoma: A case report and review of the literature. J Med Case Rep. 2011;5. [CrossRef]
- Santandrea G, Borsari S, Filice A, Piana S. Merkel Cell Carcinoma: Mind the Genital Metastatic Sites! Dermatology Practical and Conceptual. Mattioli 1885; 2023.
- Pennisi G, Talacchi A, Tirendi MN, Giordano M, Olivi A. Intradural extramedullary cervical metastasis from Merkel cell carcinoma: a case report and literature review. Chin Neurosurg J. 2022 Dec 2;8(1):38. [CrossRef]
- Leão I, Marinho J, Costa T. Long-term response to avelumab and management of oligoprogression in Merkel cell carcinoma: A case report. World J Clin Cases. 2021 Jun 26;9(18):4829–36. [CrossRef]
- Lentz SR, Krewson L, Zutter MM. Recurrent Neuroendocrine (Merkel Cell) Carcinoma of the Skin Presenting as Marrow Failure in a Man With Systemic Lupus Erythematosus. Medical and Pediatric Oncology. 1993.
- Wang HY, Shabaik AS. Metastatic Merkel cell carcinoma involving the bone marrow with chronic lymphocytic leukemia mimicking Richter transformation. Blood. 2013 Oct 17;122(16):2776. [CrossRef]
- Khan A, Adil S, Estalilla OC, Jubelirer S. Bone marrow involvement with Merkel cell carcinoma. BMJ Case Rep. 2020 Jun 28;13(6). [CrossRef]
- Morris KL, Williams B, Kennedy GA. Images in haematology. Heavy bone marrow involvement with metastatic Merkel cell tumour in an immunosuppressed renal transplant recipient. Br J Haematol. 2005 Jan;128(2):133. [CrossRef]
- Kressin MK, Kim AS. Metastatic Merkel cell carcinoma in the bone marrow of a patient with plasma cell myeloma and therapy-related myelodysplastic syndrome. Int J Clin Exp Pathol. 2012;5(9):1007-12.
- Keow J, Kwan KF, Hedley BD, Hsia CC, Xenocostas A, Chin-Yee B. Merkel cell carcinoma mimicking acute leukemia. Int J Lab Hematol. 2024 Oct 1. [CrossRef]
- Durmus O, Gokoz O, Saglam EA, Ergun EL, Gulseren D. A rare involvement in skin cancer: Merkel cell carcinoma with bone marrow infiltration in a kidney transplant recipient. Clinical Medicine, Journal of the Royal College of Physicians of London. 2023 May 1;23(3):275–7. [CrossRef]
- Nemoto I, Sato-Matsumura KC, Fujita Y, Natsuga K, Ujiie H, Tomita Y, Kato N, Kondo M, Ohnishi K. Leukaemic dissemination of Merkel cell carcinoma in a patient with systemic lupus erythematosus. Clin Exp Dermatol. 2008 May;33(3):270-2. [CrossRef]
- Highland B, Morrow WP, Arispe K, Beaty M, Maracaja D. Merkel Cell Carcinoma With Extensive Bone Marrow Metastasis and Peripheral Blood Involvement: A Case Report With Immunohistochemical and Mutational Studies. Applied Immunohistochemistry and Molecular Morphology. 2024 Sep 1;32(8):382–8. [CrossRef]
- Smadja N, De Gramont A, Gonzalez-Canali G, Louvet C, Wattel E, Krulik M. Cytogenetic Study in a Bone Marrow Metastatic Merkel Cell Carcinoma. 1991. [CrossRef]
- Le Gall-Ianotto C, Coquart N, Ianotto JC, Guillerm G, Grall C, Quintin-Roue I, Marion V, Greco M, Berthou C, Misery L. Pancytopaenia secondary to bone marrow dissemination of Merkel cell carcinoma in a patient with Waldenström macroglobulinaemia. Eur J Dermatol. 2011 Jan-Feb;21(1):126-7. [CrossRef]
- Kobrinski DA, Choudhury AM, Shah RP. A case of locally-advanced Merkel cell carcinoma progressing with disseminated bone marrow metastases. European Journal of Dermatology. John Libbey Eurotext; 2018. p. 550–1. [CrossRef]
- Folyovich A, Majoros A, Jarecsny T, Pánczél G, Pápai Z, Rudas G, Kozák L, Barna G, Béres-Molnár KA, Vadasdi K, et al. Epileptic Seizure Provoked by Bone Metastasis of Chronic Lymphoid Leukemia and Merkel Cell Carcinoma. Case Rep Med. 2020 Oct 27;2020:4318638. [CrossRef]
- Vlad R, Woodlock TJ. Merkel Cell Carcinoma after Chronic Lymphocytic Leukemia: Case Report and Literature Review. American Journal of Clinical Oncology: Cancer Clinical Trials. 2003 Dec;26(6):531–4.
- Goepfert H, Remmler D, Silva E, Wheeler B. Merkel cell carcinoma (endocrine carcinoma of the skin) of the head and neck. Arch Otolaryngol. 1984 Nov;110(11):707-12. [CrossRef]
- Goodwin CR, Mehta AI, Adogwa O, Sarabia-Estrada R, Sciubba DM. Merkel Cell Spinal Metastasis: Management in the Setting of a Poor Prognosis. Global Spine J. 2015 Aug 1;5(4):39–43. [CrossRef]
- Haykal T, Towfiq B. Merkel cell carcinoma with intramedullary spinal cord metastasis: a very rare clinical finding. Clin Case Rep. 2018 Apr 6;6(6):1181-1182. [CrossRef]
- Madden N, Thomas P, Johnson P, Anderson K, Arnold P. Thoracic Spinal Metastasis of Merkel Cell Carcinoma in an Immunocompromised Patient: Case Report. Evid Based Spine Care J. 2013 May 1;04(01):054–8. [CrossRef]
- Moayed S, Maldjian C, Adam R, Bonakdarpour A. Magnetic resonance imaging appearance of metastatic Merkel cell carcinoma to the sacrum and epidural space. 2000. [CrossRef]
- Nguyen BD, McCullough AE. Isolated Tibial Metastasis from Merkel Cell Carcinoma. Radiol Case Rep. 2007;2(4):88. [CrossRef]
- Kamijo A, Koshino T, Hirakawa K, Saito T. Merkel cell carcinoma with bone metastasis: a case report. Vol. 7, J Orthop Sci. 2002. [CrossRef]
- Pectasides D, Moutzourides G, Dimitriadis M, Varthalitis J, Athanassiou A. Chemotherapy for Merkel cell carcinoma with carboplatin and etoposide. Am J Clin Oncol. 1995 Oct;18(5):418-20. [CrossRef]
- Pilotti S, Rilke F, Bartoli C, Grisotti A. Clinicopathologic correlations of cutaneous neuroendocrine Merkel cell carcinoma. J Clin Oncol. 1988 Dec;6(12):1863-73. [CrossRef]
- Principe DR, Clark JI, Emami B, Borowicz S. Combined radio-immunotherapy leads to complete clinical regression of stage IV Merkel cell carcinoma. BMJ Case Rep. 2019 Aug 1;12(8). [CrossRef]
- Vijay K, Venkateswaran K, Shetty AP, Rajasekaran S. Spinal extra-dural metastasis from Merkel cell carcinoma: A rare cause of paraplegia. European Spine Journal. 2008 Sep;17. [CrossRef]
- Ng G, Lenehan B, Street J. Metastatic Merkel cell carcinoma of the spine. Journal of Clinical Neuroscience. 2010 Aug;17(8):1069–71. [CrossRef]
- Turgut M, Gökpinar D, Barutça S, Erkuş M. Lumbosacral metastatic extradural Merkel cell carcinoma causing nerve root compression--case report. Neurol Med Chir (Tokyo). 2002 Feb;42(2):78-80. [CrossRef]
- Zhao M, Meng M Bin. Merkel cell carcinoma with lymph node metastasis in the absence of a primary site: Case report and literature review. Oncol Lett. 2012 Dec;4(6):1329–34.
- Maugeri R, Giugno A, Giammalva RG, Gulì C, Basile L, Graziano F, Iacopino DG. A thoracic vertebral localization of a metastasized cutaneous Merkel cell carcinoma: Case report and review of literature. Surg Neurol Int. 2017 Aug 10;8:190. [CrossRef]
- Chao TC, Park JM, Rhee H, Greager JA. Merkel cell tumor of the back detected during pregnancy. Plast Reconstr Surg. 1990 Aug;86(2):347-51. [CrossRef]
- Park JS, Park YM. Cervical Spinal Metastasis of Merkel Cell Carcinoma. Neurospine. 2009;6(3):197-200.
- Turgut M, Baka M, Yurtseven M. Metastatic Merkel cell carcinoma to the sacrum and epidural space: case report. Magn Reson Imaging. 2004 Nov;22(9):1340. [CrossRef]
- Tam CS, Turner P, McLean C, Whitehead S, Cole-Sinclair M. 'Leukaemic' presentation of metastatic Merkel cell carcinoma. Br J Haematol. 2005 May;129(3):446.
- Gooptu C, Woollons A, Ross J, Price M, Wojnarowska F, Morris PJ, Wall S, Bunker CB. Merkel cell carcinoma arising after therapeutic immunosuppression. Br J Dermatol. 1997 Oct;137(4):637-41. [CrossRef]
- Zijlker LP, Bakker M, van der Hiel B, Bruining A, Klop WMC, Zuur CL, Wouters MWJM, van Akkooi ACJ. Baseline ultrasound and FDG-PET/CT imaging in Merkel cell carcinoma. J Surg Oncol. 2023 Apr;127(5):841-847.
- Shim SR, Kim SJ. Diagnostic Test Accuracy of 18F-FDG PET or PET/CT in Merkel Cell Carcinoma. Clin Nucl Med. 2022 Oct 1;47(10):843–8.
- Oh HY, Kim D, Choi YS, Kim EK, Kim TE. Merkel Cell Carcinoma of the Trunk: Two Case Reports and Imaging Review. Journal of the Korean Society of Radiology. 2023 Sep 1;84(5):1134–9. [CrossRef]
- Kirienko M, Gelardi F, Fiz F, Bauckneht M, Ninatti G, Pini C, Briganti A, Falconi M, Oyen WJG, van der Graaf WTA, et al. Personalised PET imaging in oncology: an umbrella review of meta-analyses to guide the appropriate radiopharmaceutical choice and indication. Eur J Nucl Med Mol Imaging. 2024 Dec;52(1):208-224. [CrossRef]
- Ming Y, Wu N, Qian T, Li X, Wan DQ, Li C, Li Y, Wu Z, Wang X, Liu J, et al. Progress and Future Trends in PET/CT and PET/MRI Molecular Imaging Approaches for Breast Cancer. Front Oncol. 2020 Aug 12;10:1301. [CrossRef]
- Costelloe CM, Rohren EM, Madewell JE, Hamaoka T, Theriault RL, Yu TK, Lewis VO, Ma J, Stafford RJ, Tari AM, et al. Imaging bone metastases in breast cancer: techniques and recommendations for diagnosis. Lancet Oncol. 2009 Jun;10(6):606-14. [CrossRef]
- Uchida N, Sugimura K, Kajitani A, Yoshizako T, Ishida T. MR imaging of vertebral metastases: evaluation of fat saturation imaging. European Journal of Radiology. 1993. [CrossRef]
- Girard R, Djelouah M, Barat M, Fornès P, Guégan S, Dupin N, et al. Abdominal metastases from Merkel cell carcinoma: Prevalence and presentation on CT examination in 111 patients. Diagn Interv Imaging. 2022 Jan 1;103(1):41–8. [CrossRef]
- Li X, Wu N, Zhang W, Liu Y, Ming Y. Differential diagnostic value of 18F-FDG PET/CT in osteolytic lesions. J Bone Oncol. 2020 Jul 13;24:100302. [CrossRef]
- Patel PY, Dalal I, Griffith B. [18F]FDG-PET Evaluation of Spinal Pathology in Patients in Oncology: Pearls and Pitfalls for the Neuroradiologist. American Journal of Neuroradiology. American Society of Neuroradiology; 2022. p. 332–40. [CrossRef]
- Hong SB, Choi SH, Kim KW, Park SH, Kim SY, Lee SJ, Lee SS, Byun JH, Lee MG. Diagnostic performance of [18F]FDG-PET/MRI for liver metastasis in patients with primary malignancy: a systematic review and meta-analysis. Eur Radiol. 2019 Jul;29(7):3553-3563. [CrossRef]
- Choi J, Raghavan M. Diagnostic imaging and image-guided therapy of skeletal metastases. Cancer Control. 2012 Apr;19(2):102-12. [CrossRef]
- Macedo F, Ladeira K, Pinho F, Saraiva N, Bonito N, Pinto L, Goncalves F. Bone Metastases: An Overview. Oncol Rev. 2017 May 9;11(1):321. [CrossRef]
- Schadendorf D, Nghiem P, Bhatia S, Hauschild A, Saiag P, Mahnke L, Hariharan S, Kaufman HL. Immune evasion mechanisms and immune checkpoint inhibition in advanced merkel cell carcinoma. Oncoimmunology. 2017 Aug 31;6(10):e1338237. [CrossRef]
- Tai P. A Practical Update of Surgical Management of Merkel Cell Carcinoma of the Skin. ISRN Surg. 2013 Jan 30;2013:1–17. [CrossRef]
- Cornejo C, Miller CJ. Merkel Cell Carcinoma: Updates on Staging and Management. Vol. 37, Dermatologic Clinics. W.B. Saunders; 2019. p. 269–77.
- Singh B, Qureshi MM, Truong MT, Sahni D. Demographics and outcomes of stage I and II Merkel cell carcinoma treated with Mohs micrographic surgery compared with wide local excision in the National Cancer Database. J Am Acad Dermatol. 2018 Jul 1;79(1):126-134.e3. [CrossRef]
- Shaikh WR, Sobanko JF, Etzkorn JR, Shin TM, Miller CJ. Utilization patterns and survival outcomes after wide local excision or Mohs micrographic surgery for Merkel cell carcinoma in the United States, 2004-2009. J Am Acad Dermatol. 2018 Jan;78(1):175-177.e3.
- Kline L, Coldiron B. Mohs micrographic surgery for the treatment of merkel cell carcinoma. Dermatologic Surgery. 2016;42(8):945–51. [CrossRef]
- Terushkin V, Brodland DG, Sharon DJ, Zitelli JA. Mohs surgery for early-stage Merkel cell carcinoma (MCC) achieves local control better than wide local excision ± radiation therapy with no increase in MCC-specific death. Int J Dermatol. 2021 Aug 1;60(8):1010–2. [CrossRef]
- Tran DC, Ovits C, Wong P, Kim RH. Mohs micrographic surgery reduces the need for a repeat surgery for primary Merkel cell carcinoma when compared to wide local excision: A retrospective cohort study of a commercial insurance claims database. JAAD Int. 2022 Aug 27;9:97-99. [CrossRef]
- Bhatia S, Storer BE, Iyer JG, Moshiri A, Parvathaneni U, Byrd D, Sober AJ, Sondak VK, Gershenwald JE, Nghiem P. Adjuvant Radiation Therapy and Chemotherapy in Merkel Cell Carcinoma: Survival Analyses of 6908 Cases From the National Cancer Data Base. J Natl Cancer Inst. 2016 May 31;108(9):djw042.
- Asgari MM, Sokil MM, Warton EM, Iyer J, Paulson KG, Nghiem P. Effect of host, tumor, diagnostic, and treatment variables on outcomes in a large cohort with merkel cell carcinoma. JAMA Dermatol. 2014;150(7):716–23. [CrossRef]
- Broida SE, Chen XT, Baum CL, Brewer JD, Block MS, Jakub JW, Pockaj BA, Foote RL, Markovic SN, Hieken TJ, et al. Merkel cell carcinoma of unknown primary: Clinical presentation and outcomes. J Surg Oncol. 2022 Nov;126(6):1080-1086. [CrossRef]
- Becker J. C., Hassel J. C., Menzer C., Kähler K. C., Eigentler T. K., Meier F. E., Berking C., Gutzmer R., Mohr P., Kiecker F., et al. Adjuvant ipilimumab compared with observation in completely resected Merkel cell carcinoma (ADMEC): A randomized, multicenter DeCOG/ADO study. Journal of Clinical Oncology. 2018. Vol. 36. No. 15_suppl. p. 9527. [CrossRef]
- Becker JC, Ugurel S, Leiter U, Meier F, Gutzmer R, Haferkamp S, Zimmer L, Livingstone E, Eigentler TK, Hauschild A, et al. Adjuvant immunotherapy with nivolumab versus observation in completely resected Merkel cell carcinoma (ADMEC-O): disease-free survival results from a randomised, open-label, phase 2 trial. Lancet. 2023 Sep 2;402(10404):798-808. [CrossRef]
Figure 1.
Evidence-Based Diagnostic and Therapeutic Flowchart for Merkel Cell Carcinoma.
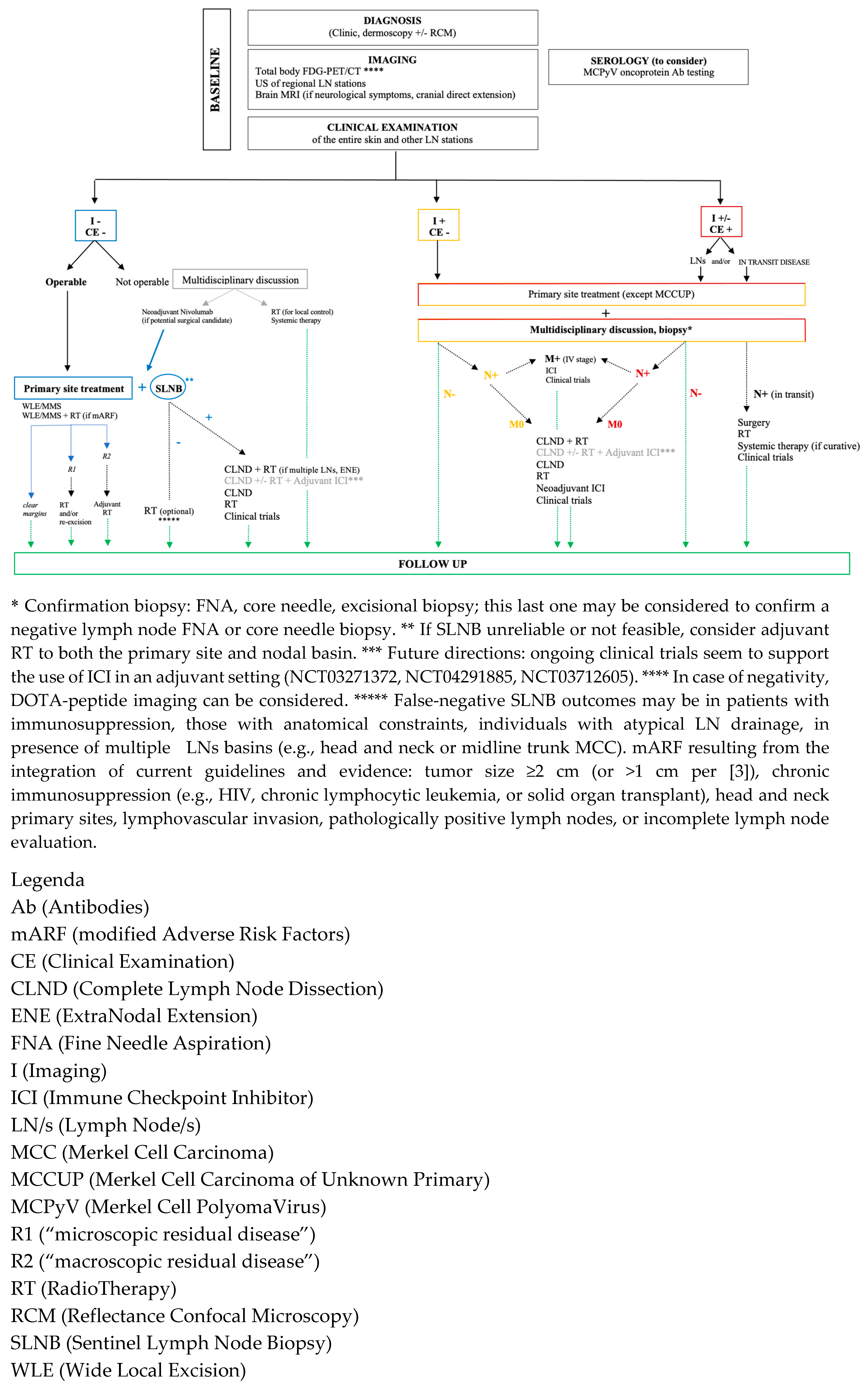

Table 1.
Candidate cell of origin in Merkel cell carcinoma.
| Cell of origin | Driving mechanism | Evidence supporting the origin of MCC from the specific candidate cell | |
| Pros | Cons | ||
| Merkel cell | UV-related | Phenotypic similarities: cytokeratin (CK) 20, neuroendocrine markers (chromogranin A, synaptophysin), Piezo2 and Atoh1. | No mitotic activity. No transformation/proliferation induced by MCPyV T antigens. Different anatomic localization between the candidate cell and MCC. Lack of connection between the tumor cells and the epidermis. |
| Epithelial progenitor | UV-related | Presence of UV-signature (TP53, Rb inactivation). Ability to differentiate into Merkel cell. Ability to differentiate in MCC. Most likely origin of neuroendocrine carcinoma in other sites (SCLC). |
No transformation/proliferation induced by MCPyV T antigens. Lack of connection between tumor cells and the epidermis. |
| Fibroblast and dermal stem cell | MCPyV-related | Ability of MCPyV antigens to induce transformation in these cell types. Explain the exclusive dermal/hypodermal localization of MCC. |
Lack of UV signature. No evidence to suggest that fibroblasts can acquire a Merkel cell-like phenotype. Unpredicted origin for a neuroendocrine carcinoma. |
| Pre/Pro B-cell | MCPyV-related | Epidemiologic data on the association between MCC and B-cell neoplasia. Co-expression of B-cell markers (PAX5, TdT, Ig). Detection of MCPyV integration in B-cell neoplasia. |
Lack of UV signature. No evidence that B-cells can acquire a Merkel cell-like phenotype. Unpredicted origin for a neuroendocrine carcinoma. |
Table 2.
Immunohistochemical differential diagnosis of Merkel cell carcinoma.
| Stain | MCC* | SCLC | Neuroblastoma | Ewing sarcoma | Small-cell melanoma | Lymphoma |
| Neurofilament (NF) | + | − | + | + | − | − |
| Cytokeratin (CK) 20 | + | − | − | − | − | − |
| Cytokeratin (CK) 7 | +/− | +/− | − | − | − | − |
| Thyroid transcription factor-1 (TTF1) | +/− | + | − | − | − | |
| Neuron-specific enolase (NSE) | + | + | + | +/− | − | − |
| Chromogranin A | + | + | + | − | − | − |
| Synaptophysin (SYP) | + | + | + | +/− | − | − |
| Neural cell adhesion molecule (NCAM) or CD56 | + | + | + | +/− | + | +/− |
| S100 | − | − | − | − | + | − |
| Leukocyte common antigen (LCA) or CD45 | − | − | − | − | − | + |
* A small subset of CK7-positive, TTF-1-positive MCCs has been described. Positive (+): the marker is typically expressed in the tumor type; Positive/Negative (+/−): the expression may vary and is not definitive for that tumor type; Negative (−): the marker is typically not expressed in the tumor type.
Table 3.
American Joint Committee on Cancer classification (AJCC) 8th edition for Merkel cell carcinoma.
Table 3.
American Joint Committee on Cancer classification (AJCC) 8th edition for Merkel cell carcinoma.
| AJCC Stage | TNM staging | Primary Tumor | Lymph Node | Metastasis | |
| 0 | Tis, N0, M0 | In situ (within epidermis only) | No regional lymph node metastasis | No distant metastasis | |
| I | Clinical* | T1, N0, M0 | ≤ 2 cm maximum tumor dimension | Nodes negative by clinical exam (no pathological exam performed) |
No distant metastasis |
| Pathologic** | T1, pN0, M0 | ≤ 2 cm maximum tumor dimension | Nodes negative by pathologic exam | No distant metastasis | |
| IIA | Clinical* | T2-3, N0, M0 | > 2 cm tumor dimension | Nodes negative by clinical exam (no pathological exam performed) |
No distant metastasis |
| Pathologic** | T2-3, pN0, M0 | > 2 cm tumor dimension | Nodes negative by pathological exam | No distant metastasis | |
| IIB | Clinical* | T4, N0, M0 | Primary tumor invades bone, muscle, fascia, or cartilage | Nodes negative by clinical exam (no pathological exam performed) |
No distant metastasis |
| Pathologic** | T4, pN0, M0 | Primary tumor invades bone, muscle, fascia, or cartilage |
Nodes negative by pathologic exam | No distant metastasis | |
| III | Clinical* | T0-4, N1-3*****, M0 | Any size / depth tumor | Nodes positive by clinical exam (no pathological exam performed) |
No distant metastasis |
| IIIA | Pathologic** | T1-4, pN1a(sn)*** or pN1a, M0 | Any size / depth tumor | Nodes positive by pathological exam only (nodal disease not apparent on clinical exam) |
No distant metastasis |
| T0, pN1b, M0 | Not detected (“unknown primary”) | Nodes positive by clinical exam, and confirmed via pathological exam | No distant metastasis | ||
| IIIB | Pathologic** | T1-4, pN1b-3, M0 | Any size / depth tumor | Nodes positive by clinical exam, and confirmed via pathological exam OR in-transit metastasis **** | No distant metastasis |
| IV | Clinical* | T0-4, any N, M1 | Any | +/- regional nodal involvement | Distant metastasis detected via clinical exam |
| Pathologic** | T0-4, any pN, M1 | Any | +/- regional nodal involvement | Distant metastasis confirmed via pathological exam |
|
* Clinical detection of nodal or metastatic disease may be via inspection, palpation, and/or imaging. ** Pathological detection/confirmation of nodal disease may be via sentinel lymph node biopsy, lymphadenectomy, or fine needle biopsy; and pathological confirmation of metastatic disease may be via biopsy of the suspected metastasis. *** (sn)= sentinel lymph node. The N1 category defines a regional lymph node metastasis without in-transit metastasis. The N1 category is subdivided in N1a(sn) for clinically occult lymph node metastasis detected only at SLNB in a patient with clinical stage I-II disease; N1a for clinically occult lymph node metastasis detected following lymph node dissection; and N1b for clinically and/or radiologically detected metastasis. **** In transit metastasis: a tumor distinct from the primary lesion and located either (a) between the primary lesion and the draining regional lymph nodes or (b) distal to the primary lesion. ***** N2 is defined as in-transit metastasis without associated lymph node metastasis; N3 is defined as in-transit metastasis with lymph node metastasis.
Table 4.
Summary of the studies investigated bone and bone marrow metastases from Merkel Cell Carcinoma: patient characteristics, nature of the primary MCC, treatment, pattern of metastatic spread, and overall survival.
Table 4.
Summary of the studies investigated bone and bone marrow metastases from Merkel Cell Carcinoma: patient characteristics, nature of the primary MCC, treatment, pattern of metastatic spread, and overall survival.
| Author | Study’ type | Patient/s | Merkel cell carcinoma |
Another site/s of distant metastasis (n., %) * |
Overall Survival for bone/BM metastatic patients | ||||||
| Number (n.) | Age (years) |
Sex | Primary MCC | Bone/bone marrow metastases | |||||||
| Known | Unknown | ||||||||||
| Male n (%) |
Female n (%) |
n. (%) | n. (%) | n. (%) | Therapy | ||||||
| Khaddour et al. [113] | Original article | 34 | 70.2 (51.4) *** |
20 (58.8) |
14 (41.2) | 14 (41.2) | 20 (58.8) | 10 (29.4) | CHT, IT | Regional LNs (28, 82.4) |
8.2 months (median) |
| Xia et al. [111] | Original article | 273 | **** | 200 (73.3) | 73 (26.7) | 184 (67.4) | 89 (32.6) | 31 (11.3) ** |
CHT, RT, surgery | Liver (37, 13.5) | 1-year median OS rate of 38.7% ** |
| Kim et al. [7] | Original article | 151 | 76 (62) *** |
101 (66.9) | 50 (23.1) | 134 (88.8) | 17 (11.2) | 40 (26.5) | IT, RT, surgery | LNs (94, 62.3), skin/soft tissue (40, 26.5) | 15.1 months (median) |
| Lewis et al. [6] | Original article | 215 | / | 176 (82) | 39 (18) | 173 (80) | 42 (20) | 64 (21) | CHT, RT | Non-regional LNs (88, 41%) | / |
| Pilotti et al. [148] | Original article | 50 | 62 (45) *** |
22 (44) | 28 (56) | 40 (80) | 10 (20) | 1 (2) | CHT | Skin (4, 8), liver (2, 4), pancreas (2, 4), lung (1, 2) | 12 months |
| Goepfert et al. [140] | Original article | 41 | 66 (55) *** |
**** | **** | **** | **** | 4 (9.8) | CHT | Skin (5, 12.1%), LNs (4, 9.8%) | / |
| Maloney et al. [104] | Original article | 331 | 74.6 (15.5) *** |
241 (72.8) | 90 (27.2) |
**** | **** | 6 (1.9) | / | Liver (89, 28.7), lung (51, 16.4), brain (6, 1.9) | 5-year median OS rate of 11.2 % |
| Pectasides et al. [147] | Case report # | 1 | 48 | 1 (100) | / | 1 Buttock |
/ | 1 T11, L2 vertebra |
CHT, RT | Regional LNs | 5 months |
| Nguyen et al. [145] | Case report # | 1 | 69 |
1 (100) | / | 1 Cheek |
/ | 1 Tibia |
Surgery | / | 19 months |
| Kamijo et al. [146] | Case report # | 1 | 75 | / | 1 (100) | 1 Cheek |
/ | 1 Femur |
RT, surgery | Subcutaneous tissue | 16 months |
| Wang et al. [127] | Case report # | 1 | 79 | / | 1 (100) | / | 1 | 1 BM |
/ | / | / |
| Khan et al. [128] | Case report # | 1 | 80 | / | 1 (100) | 1 Trunk |
/ | 1 BM |
CHT, RT | Regional LNs | 1 month |
| Morris et al. [129] | Case report # | 1 | 72 | 1 (100) | / | 1 Shoulder |
/ | 1 BM |
Death before starting CHT | Regional LNs | 4 months |
| Le Gall-Ianotto et al. [136] | Case report # | 1 | 65 | 1 (100) | / | / | 1 | 1 BM |
CHT, RT | / | 3 months |
| Kobrinski et al. [137] | Case report # | 1 | 86 | 1 (100) | / | 1 Trunk |
/ | 1 BM |
RT | Regional LNs | 12 months |
| Kressin et al. [130] | Case report # | 1 | 64 | 1 (100) | / | 1 Forehead |
/ | 1 BM |
Death before starting CHT | Regional LNs | 3 months |
| Keow et al. [131] | Case report # | 1 | 71 | 1 (100) | / | 1 | / | 1 BM |
/ | / | / |
| Durmus et al. [132] | Case report # | 1 | 60 | 1 (100) | / | 1 Thigh |
/ | 1 BM |
Death before starting IT | Regional LNs, liver | 7 months |
| Nemoto et al. [133] | Case report # | 1 | 73 | / | 1 (100) | 1 Cheek |
/ | 1 BM |
Death before starting therapy | Regional LNs | 8 months |
| Vlad et al. [139] | Case report # | 1 | 72 | 1 (100) | / | 1 Arm |
/ | 1 BM |
CHT | Regional LNs | 8 months |
| Barkdull et al. [110] | Case report # | 1 | 55 | 1 (100) | / | 1 Scalp |
/ | 1 Sternum |
CHT | Regional LNs, subcutaneous tissue, pancreas |
9 months |
| Leão et al. [125] | Case report # | 1 | 61 | 1 (100) | / | 1 Buttock |
/ | 1 Sacrum |
CHT, IT (Avelumab) | In-transit metastasis | 30 months |
| Lentz et al. [126] | Case report # | 1 | 55 | 1 (100) | / | 1 Scalp |
/ | 1 BM |
CHT | Regional LNs, parotid gland | 12 months |
| Smadja et al. [135] | Case report # | 1 | 34 | / | 1 (100) | 1 Shoulder |
/ | 1 BM |
CHT | Lung, brain | 4 months |
| Vijay et al. [150] | Case report # | 1 | 57 | / | 1 (100) | / | 1 | 1 Extra-dural T8, L4, S1 |
CHT, RT | Non-regional LNs | 1 month |
| Ng et al. [151] | Case report # | 1 | 73 | 1 (100) | / | 1 Arm |
/ | 1 Extra-dural T5-T7 |
Surgery, death before starting CHT/RT | / | 1 month |
| Highland et al. [134] | Case report # | 1 | 74 | 1 (100) | / | 1 Lip |
/ | 1 BM |
CHT | Regional LNs | 13 months |
| Maugeri et al. [154] | Case report # | 1 | 59 | / | 1(100) | 1 Scalp |
/ | 1 T7-T8 vertebra |
CHT, RT | Liver, lung | 8 months |
| Chao et al. [155] | Case report # | 1 |
23 | / | 1 (100) | 1 Back |
/ | 1 Extradural T3-T4 |
CHT, RT | Lung, heart | 23 months |
| Moayed et al. [144] | Case report # | 1 | 70 | 1 (100) | / | / | 1 | 1 Lumbosacral spine, epidural S1, hip |
CHT, RT | Regional LNs | 9 moths |
| Turgut et al. [152] | Case report # | 1 | 63 | 1 (100) | / | 1 Abdomen | / | 1 Extradural L5–S1 |
CHT | “Massive” **** | 2 months |
| Turgut et al. [157] | - | - | - | - | - | - | - | - | - | - | - |
| Payne et al. [116] | Case report # | 1 | 77 | / | 1 (100) | 1 Buttock |
/ | 1 T4 vertebra |
RT | Bone, lung | 12 months |
| Park et al. [156] | Case report # | 1 | 30 | 1 (100) | / | 1 Hand |
/ | 1 C6 vertebra |
Death before starting CHT/RT | / | 1 month |
| Madden et al. [143] | Case report # | 1 | 55 | 1 (100) | / | 1 Neck |
/ | 1 Epidural T6-T8 |
RT, surgery | bone | 4 months |
| Goodwin et al. [141] | Case report # | 1 | 76 | 1 (100) | / | 1 Back |
/ | 1 Epidural T5 |
RT, surgery | bone | 15 months |
| Zhao et al. [153] |
Case report # | 1 | 54 | 1 (100) | / | / | 1 | 1 T6, T12, L2 vertebra |
CHT, RT, surgery | Regional LNs, liver | 21 moths |
| Folyovich et al. [138] | Case report # | 1 | 62 | / | 1 (100) | 1 Arm |
/ | 1 skull |
CHT, RT | Non-regional LNs | 24 months |
| Haykal et al. [142] | Case report # | 1 | 49 | / | 1 (100) | 1 Vulva |
/ | 1 Intradural intramedullary C4-C5 |
CHT, RT | Regional and non-regional LNs, liver | - |
| Pennisi et al. [124] | Case report # | 1 | 73 | / | 1 (100) | 1 Face |
/ | 1 Intradural extramedullary C6-C7 |
IT (Avelumab), RT | Skin, subcutaneous tissue | 5 months |
| Principe et al. [149] | Case report # | 1 | 79 | 1 (100) | / | 1 Ear |
/ | 1 T2, T7, T10-11, L3 vertebra |
IT (Avelumab), RT | Regional LNs, parotid gland | 18 months |
| Abul-Kasim et al. [122] | Case report # | 1 | 65 | 1 (100) | / | / | 1 | 1 Epidural and intradural L1, L5 |
RT, surgery | Non-regional LNs, brain, retroperitoneum, lung | 8 months |
| Tam et al. [158] | Case report # | 1 | 66 | 1 (100) | / | 1 Forearm |
/ | 1 BM |
Death before therapy | / | 6 months |
| - | - | 1 | 55 | 1 (100) | / | / | 1 | 1 BM |
CHT | / | 1.5 month |
| Gooptu et al. [159] | Case report # | 1 | 68 | / | 1 (100) | 1 Leg |
/ | 1 BM |
CHT | Non-regional LNs | 2 months |
| - | - | 1 | 55 | 1 (100) | / | 1 Neck |
/ | 1 Vertebra |
RT | Non-regional LNs, brain | 6 months |
Abbreviations: BM (bone marrow), CHT (chemotherapy), IT (immunotherapy), LNs (lymph nodes), MCC (Merkel cell carcinoma), OS (overall survival), RT (radiotherapy). # For individual case reports, we specified the anatomical site involved in the “Bone metastasis” section when provided; age is recorded in years and prognosis in months. * We included the most commonly reported metastatic site/s alongside bone. ** We considered only single bone-site metastases. *** Median age (IQR) **** Unable to determine due to limitations in the available published data. / None or not intended by the study.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



