
Submitted:
04 April 2025
Posted:
08 April 2025
You are already at the latest version
Abstract
Background: The development of non-dairy probiotic products is a challenge for the food industry while cereals as probiotic carriers provide the means to incorporate probiotics, prebiotics, and fiber into the human diet. The present study investigated the effects of Lactococcus cremoris spp. immobilized oat flakes on blood and urine biomarkers in a randomized placebo-controlled single-blind clinical trial. Methods: Fifty-four eligible participants were randomized to placebo or probiotic group that consumes 5g of oat flakes daily, tor 12 weeks. Blood and urine samples were collected at the baseline and at the 6th and 12th week of consumption. Glycemic, lipemic, inflammatory, immunological, antioxidant biomarkers and vitamins were analyzed. Results: Compared to the control group, IL-6 (p=0.045) and hs-CRP (p=0.02) were significantly decreased at week 6 and 12 respectively in the intervention group. Conclusions: Lactococcus cremoris spp immobilized on oat flakes seems to improve biomarkers related to human health. However, further studies are required to characterize the probiotic properties of the studied strain.
Keywords:
functional foods
; probiotics
; oat flakes
1. Introduction
Probiotics are defined as viable microorganisms (bacteria or yeasts) that, when ingested in adequate concentrations, exert various beneficial effects on the host. The most common microorganisms used as probiotics are lactic acid bacteria (LAB), like Lactococcus, Lactobacillus, Streptococcus, Enterococcus and Bifidobacterium; however, not all the bacteria can be probiotic, as they need to be strain-specific [1]. To exhibit beneficial health impact, probiotic microbes should be able to survive in the acidic conditions of the stomach and gastrointestinal tract (GT) of humans which means to withstand the gastric juice and bile salt, survive passage through the upper GT, multiply, colonize, and function in the gut [2].
The health benefits associated with probiotic consumption have been extensively investigated in animal models and human studies, therefore probiotic application in foods aim to improve host health and treat different infectious and non-infectious pathologies [3]. The probiotic action of beneficial bacteria can be attributed to various metabolic pathways and is expressed by different mechanisms. Firstly, probiotics play a crucial role on gut barrier function by causing modulations, which affect barrier robustness and thereby influence disease states [4]. Moreover, consumption of different probiotic strains may modulate the microbiota, in order to maintain optimal gut health, and preventing/treating chronic inflammatory and immunity related diseases [5]. Also, probiotics can change microbiota’s metabolic properties by competing with the absorption of several nutritional substances. Specifically, when health promoting bacteria are present in the gut, they utilize more nutrients, leaving fewer nutrients for pathogenic bacteria, which may suffer starvation, and thus not survive [6,7].
The ability of probiotics to exert beneficial effects on health is a strain- specific trait [8]. Consequently, the in vitro and subsequent in vivo assessment of the probiotic characteristics of wild- type presumptive probiotic strains, as well as clinical trials, are essential in order to confirm the health-promoting effects. In the present study, the wild- type Lactococcus cremoris FBMS_5810 strain, isolated from white mushrooms, was selected taking into consideration its high cholesterol assimilation activity in vitro (Pavlatou et al., 2025). High levels of blood cholesterol are considered a significant risk factor for the development of cardiovascular disease, obesity and other metabolic disorders [9,10]. Thus, the selection of probiotic strains with promising cholesterol removal activity could be considered an alternative therapeutic approach for hypercholesterolemia.
Probiotic delivery has been consistently associated with foods, especially dairy, however there is an increasing trend toward using probiotics in different food matrixes despite their original source of isolation [11]. In this sense, food ingredients rich in dietary fibers, such as oat flakes, could serve as an excellent probiotic vehicle, since there is evidence suggesting the positive impact of dietary fibers on health [12]. Of note, the consumption of oat flakes has been linked with reduction in cholesterol levels, mainly due to the presence of oat β-glucans that modulate cholesterol metabolism [13]. However, the incorporation of probiotic bacteria in food presents many challenges related to their growth, survival, viability, stability and functionality in food processing, storage and consumption as well as changes of sensory characteristics of probiotic foods [14]. Probiotic strains exhibit different nutritional and therapeutic functions, due to various factors, such as the genetic make-up of the strain, amount of the probiotics used in the product, the purpose it is used for, and its shelf life [15]. Interest on the development of functional foods consisting of both probiotics and prebiotics have been increased due to increased awareness of their health-promoting properties [16]. Although diverse functional lactic acid bacteria have been applied in commercial probiotic fermented foods worldwide, the market for bio-functional products is in continuous need for the diversification of the available products [17,18]. For this purpose, a growing number of scientific studies focused on the selection of new strains with specific functional properties.
Lactic acid bacteria are widely used in the production of fermented food products while their metabolic and probiotic characteristics have attracted more attention [19]. Specifically, they have been associated with a variety of products including short-chain fatty acids, amines, bacteriocins, vitamins and exopolysaccharides during metabolism [20]. Lactococcus cremoris sub sp. cremoris was initially identified in fermented milk, while its potential health advantages for humans remain unexplored [21]. In a recent clinical trial, the consumption of a supplement containing L. cremoris was found to enhance not just the frequency of bowel movements and the composition of intestinal microbiota, but also various immunological parameters [22]. A study of similar design examined the effects of fermented milk containing Lactococcus lactis subsp. cremoris on bowel movements in healthy young Japanese women showed increases in the frequency of defecation (days/week and times/week), and stool volume. [23].
Therefore, while there is research data on the effect of L. cremoris strains on the gastrointestinal tract, its effect on human health has not been sufficiently studied. The purpose of this interventional study-clinical trial was to evaluate the effects of the wild- type L. cremoris FBMS_5810 strain immobilized on oat flakes, which has previously been in vitro evaluated for its probiotic properties (Pavlatou et al., 2025; submitted), on blood and urine biomarkers of associated with human health.
2. Materials and Methods
2.1. Preparation of Freeze-Dried Immobilized L. cremoris Cells on Oat Flakes
L. cremoris was cultured in 15 L synthetic food grade medium with the following composition: Glucose (20 g/ L), yeast extract (25 g/L), KH2PO4 (2 g/ L), CH3COONa (6 g/L), MgSO4 (0.3 g/ L), and MnSO4 (0.005 g/ L) (pH of 6.5) and incubated at 30 °C for 24 h at aFermac 300 bioreactor (Electrolab Biotech Ltd, UK) (QLC, Patras, Greece). The freshly grown culture was centrifuged (8500 x g, 15 min, 4 °C), washed with 1 L sterile ¼ Ringer’s solution (VWR International GmbH, Radnor, PA, USA) and centrifuged again. Then, the cell biomass was resuspended in sterile ¼ Ringer’s solution to the initial culture volume and 7 kg of oat flakes (previously pre-heated at 140 °C for 30 min to avoid contamination) were introduced to the cell suspension. The mixture was left undisturbed for 30 min at ambient temperature and, subsequently, strained and washed with 1 L of sterile ¼ Ringer’s isotonic solution. Then, freeze-drying in a Zirbus (ZIRBUS technology GmbH, Model VaCo 10, Bad Grund, Germany) freeze- dryer was carried out, following the method described by Prapa et al. (2025) [24].
2.2. Study Design
The present study was a 12-week randomized, placebo-controlled, single-blind clinical trial that was carried out between February and July 2023 at Agia Eleni-Spiliopoulio Pathological Hospital of Athens, Greece. The study protocol was approved by the Research Ethics and Ethics Committee of the University of the Aegean (approval 3343/February 15th, 2022) and it was registered at www.clinicaltrials.gov (ClinicalTrials.gov identifier NCT06293859). All patients were screened after obtaining their written informed consent.
2.3. Participants
The present study was advertised to potential volunteers via recruitment flyers which were distributed in the hospital premises or posted on social media. Initially, 73 volunteers agreed to participate in the study and had in-person screening appointments. The participants were screened using an eligibility checklist containing the inclusion and exclusion criteria. The inclusion criteria were i) participants to be aged between 18 and 65 years, ii) clinically tested with fasting plasma glucose less than 100 mg/dL and cholesterol less than 220 mg/dL and iii) otherwise healthy. Patients complying with any of the following exclusion criteria were excluded from the study: i) body mass index [BMI] higher than 40 kg/m2 (morbidly obese), ii) following a diet plan for weight loss, iii) following a contraceptive treatment or taking probiotic supplements, iv) following medication with an effect on lipemia or glycemia indicators, v) having any allergies/intolerances to trial ingredients, vi) pregnant or planning to become pregnant, vii) breast feeding, viii) users of illicit drug, having a chronic alcoholism or total daily alcohol intake more than 50 g per day, ix) diagnosed with a chronic condition (cancer, active liver disease, severe kidney dysfunction, severe stroke in the last six months and conditions associated with an increased risk of bleeding) or any other serious medical condition that may affect the individual’s ability to participate in a dietary intervention study, x) considered unreliable by the researcher or having a shorter life expectancy than the expected duration of the study due to some illness or if they were in any situation in which by the researcher’s opinion their participation in the study was not considered safe (e.g., drug addiction, alcohol abuse). All participants were informed of the study aims and procedures and provided written informed consent prior to commencing the trial. The compliance to any of the above exclusion criteria during the trial would result in the immediate cessation of participation in the study.
2.4. Intervention
All eligible and consenting participants were assigned a unique code as an identifier, and they were randomly allocated to receive either probiotic or placebo oat product. The probiotic group received freeze- dried immobilized L. cremoris FBMS_5810 cells on oat flakes provided by QLC (Patras, Greece) bearing 1.7 x 109 CFU/ g (Pavlatou et al. 2025). Since the recommended probiotic consumption is ≤ 2 × 10⁹ CFU daily (Ouwehand et al., 2017), 2.85 g of freeze-dried immobilized L. cremoris FBMS_5810 cells on oat flakes was defined as the suitable amount to achieve the daily dose of 2 × 10⁹ CFU, and was mixed with 2.15 g of oat flakes without L. cremoris FBMS_5810 cells. The placebo group received oat flakes indistinguishable in color, smell, and taste from the flakes with immobilized probiotics. The participants were given written instructions regarding the storage of the product, according to which the product they received had to be stored under refrigerated conditions. All participants were asked to consume 5 g of oats daily as part of a meal (e.g., alongside yogurt intake), provided the meal was at a temperature below 35 °C and was not acidic. The participants were asked to record the days and the way of consuming the intervention products in a diary given to them, and to return every six weeks to hand back the unused product and be given fresh refills to monitor their compliance with the study protocol. The participants were also asked not to alter their habitual dietary intake or routine physical activity, and to report any side effects.
2.5. Anthropometric and Biochemical Measurements
Data were collected at enrollment (week 0), the 6th and the 12th week of intervention. Participants’ anthropometric characteristics were measured following standard procedures. Weight (kg) was measured using a suitable body composition monitor (Tanita SC 330 P, Tokyo, Japan), height (cm) was measured using a height meter (Tanita HR 001), and hip and waist circumference (cm) were measured with a measuring tape. To evaluate their medical history, participants were asked to self-complete a medical questionnaire with two demographic questions on their sex and age and three questions on their medical history, namely “Have you been on any medication therapy in the last three months?”, “Do you take nutritional supplements during the last trimester?”, “Are you confronted with any clinical illnesses?”. At the same time, information was collected about potential gastrointestinal disorders and the weekly frequency of bowel movements. Participants were asked to complete another brief questionnaire to evaluate their nutritional attitudes and general habits. This included a food frequency questionnaire, as well as questions on smoking, physical activity, and alcohol consumption during the preceding 3-month period.
Blood samples were collected by venipuncture at three-time points, before intervention, at 6th and 12th week. Specifically, 10 ml of blood were collected by a cooperating nursing stuff in clot activator tubes for serum collection and in ethylenediaminetetraacetic acid (EDTA). Tubes at each sampling time point were centrifuged in a Thermo Scientific ST16R refrigerated centrifuge (Thermo Fisher Scientific, Waltham, MA, USA) at 3000 g and 4 °C for 15 min and 10 min for serum and plasma, respectively. Plasma and serum were then aliquoted and stored at −40 ◦C until further analysis. Once the study was completed, serum samples (for all time points tested) were analyzed with a COBAS c111 automated biochemical analyzer (Roche, Basel, Switzerland) for High-Density Lipoprotein Cholesterol (HDL-C) and Low-Density Lipoprotein Cholesterol (LDL-C), Total Cholesterol (TC), Triglycerides (TGL), high sensivity C-Reactive Protein (hs-CRP) and Uric Acid (UA). Moreover, Insulin (INS), Cortisol, Immunoglobulin A (Ig-A), Interleukin-6 (IL-6), Folate, Vitamin B12 (VitB12), Vitamin D (VitD) determination was conducted using a Maglumi 2000 Plus automated immunoassay system (Snibe, Shenzhen, China). The EDTA plasma was used to determine Total Antioxidant Capacity (TAC) at each time point examined, using the Ferric Reducing Antioxidant Power (FRAP) assay, as described by Benzie at al. [25], and for the evaluation of blood glucose levels (biochemical analysis).
Urine samples were delivered by participants to the study investigators on the days of hospital visits, as in the case of blood samples. The volunteers were given written instructions and consumables for the sample collection. To examine urine phosphates, urine samples were acidified with a concentrated HCl 37% to pH < 3 and stored at a refrigerated temperature of 6-8 oC until further analysis. For urine magnesium analysis, samples were acidified to pH 1 with a concentrated HCl 37% and stored at −40 ◦C until further analysis. Once the study was completed, urine samples were centrifuged in a Thermo Scientific ST16R refrigerated centrifuge (Thermo Fisher Scientific, Waltham, MA, USA) at 1 500 × g and 4 °C for 5 min and were analyzed with a COBAS c111 automated biochemical analyzer (Roche, Basel, Switzerland).
2.6. Statistical Analysis
2.6.1. Sample Size
According to sample size calculations 42 individuals were adequate to detect a significant group interaction effect with an effect size of 0.2, at 5% level with 80% power. To account for 30% drop out rate the final sample size increased to 54 individuals. The sample size was calculated using G*power 3.1 (University of Düsseldorf, Germany).
2.6.2. Data Analysis
Descriptive statistics for the concentration and incremental changes of biomarkers tested, are shown as mean (Standard Deviation, SD). Normality was assessed using the Kolmogorov–Smirnov test. Paired-sample t tests were used to detect within-group differences. For comparison of categorical variables, Wilcoxon Signed rank test was conducted. Two-way analysis of variance (ANOVA) was used to evaluate between-group changes in variables during the study. The significance level was set at 0.05. Statistical analysis carried out using SPSS V21.0 for Windows (IBM Corporation, New York, NY, United States).
3. Results
3.1. Participants
A total of 73 potential participants were initially screened based on the inclusion and exclusion criteria; 13 participants did not meet the conditions for participation in the study and 6 people decided not to participate after the evaluation process, as they could not meet the schedule that was set. Finally, 54 individuals (n= 15 men and n= 39 women) were eligible and provided informed consent. Participants were randomly assigned to either the placebo or the probiotic group, and this distribution was unknown to them. The study was completed with 46 volunteers (30% men; probiotic group n=24, placebo group n=22) as 8 people dropped out during the 12-week intervention. The flowchart of the study is shown in Figure 1.
Participants baseline characteristics are shown in Table 1. The participants’ gender distribution, mean age, waste-to-hip ratio (WHR), lifestyle habits, total cholesterol, fasting glucose did not differ between probiotic and placebo group at the baseline (all p-values > 0.05). Statistically significant differences were found in the participants' body mass index between the intervention groups, where the average of the probiotic group appeared to be overweight (BMI > 25.0 kg/m2), while in the control group, the weight of the volunteers appeared to be at normal levels (BMI < 24.9 kg/m2) [27].
3.2. Dietary Habits
Comparisons of dietary intakes at baseline, week 6 and at the end of the trial revealed no significant changes in dietary macronutrient intakes in terms of energy (calories), carbohydrates, proteins, fats and total dietary fibers within groups.
3.3. Blood Biomarkes
3.3.1. Inflammatory & Immunological Biomarkers
Among the inflammatory markers, CRP and IL-6 were selected for further study. Specifically, serum hs-CRP levels significantly reduced in the probiotic group compared with the control group at the 12th week of intervention (p=0.02). Similarly, IL-6 levels significantly reduced at the 12th week for the probiotic group (p=0.045), following a between-group comparison. Among immune-related biomarkers, IgA was examined, and no statistically significant differences were detected between groups (p<0.05). Results are presented in detail at Table 3.
3.3.2. Lipemia Biomarkers
To assess the impact of the intervention on the lipid profile of the participants, key indicators such as total, HDL-, LDL- cholesterol and triglycerides were examined. According to the results, none of the above indicators presented statistically significant differences between the groups (p>0.05) (Table 3).
3.3.3. Glycemia Biomarkers
The glycemic biomarkers examined were fasting glucose and insulin. The results showed no statistically significant differences between the intervention group and the control group for either biomarker (p>0.05) (Table 3).
3.3.4. Folate, VitB12, VitD
Among the inflammatory markers, CRP and IL-6 were selected for further study. Specifically, serum hs-CRP levels significantly reduced in the probiotic group compared with the control group at the 12th week of intervention (p= 0.02). Similarly, IL-6 levels significantly reduced at the 12th week for the probiotic group (p= 0.045), after between group comparison. Among immune-related biomarkers, IgA was examined, and no statistically significant differences was detected between groups. Table 3. shows the results in detail.
3.3.4. Cortisol, Uric Acid, Antioxidan Capacity
Cortisol levels showed a statistically significant reduction within probiotic group at the 6th (p=0.003) and the 12th (p=0.002) week of intervention, without a statistically significant difference between the intervention and control group (p>0.05). Uric acid did not differ significantly between groups, while total plasma antioxidant capacity increased significantly at the 12th week of intervention for the probiotic group (p=0.026), without this implying statistically significant differences between groups (Table 3).
3.3.5. Urine Biomarkers
Among urine biomarkers, magnesium and phosphorus were selected for further study. Specifically, urine magnesium levels significantly reduced in the probiotic group compared with the control group at the 6th week of intervention (p=0.01). Regarding the results of urinary phosphates, no statistically significant changes were noted between the groups (p<0.05). Results are presented in detail in Table 4.
4. Discussion
Novel functional foods incorporating probiotics represent a rapidly expanding sector within the food industry, drawing particular attention from the field of nutrition owing to their advantageous impact on human health [28]. Non-dairy probiotic products are of great importance worldwide due to the ongoing trend of vegetarianism, milk cholesterol content, and the high prevalence of lactose intolerance in many populations around the world [29]. Non-dairy foods such as fruits, vegetables, cereals, soy, and meat, known for their abundance in protein, minerals, vitamins, dietary fibers, antioxidants, and various bioactive substances, have been examined for their potential to support the survival and stability of probiotics [30]. Oats are a rich source of β-glucan, which act as prebiotics that selectively fermented by butyrate-producing microorganisms, antioxidant phenolic compounds, dietary lipids, and soluble fibers [31]. Probiotic immobilization in oat flakes may serve the concept of “synbiotics,” a blend of probiotics and prebiotics, and appears to be a potential strategy to improve intestinal survival and implantation of live microbial supplements [32].
The present study tested the hypothesis that Lactococcus cremoris spp immobilized in oat flakes may have a positive effect on blood and urine biomarkers, related to chronic diseases and/or nutrient deficiencies, in healthy participants. The primary outcomes of the present study were markers related to inflammation, and specifically hs-CRP and IL-6 biomarkers reduced significantly in the 12th week of intervention for the probiotic group. Literature data indicate that the gut microbiota has an influence on the development and maintenance, not only of the mucosal, but also the systemic immune response [33]. Some studies have linked this beneficial effect of probiotics with their potential ability to inhibit production of pro-inflammatory [34]. Several meta-analysis have investigated the effects of probiotics on inflammatory markers in various disease conditions, however limited number of studies have examined the effect of probiotics on inflammation in healthy individuals [35]. Among the different strains, a statistically significant probiotic effect was noted on inflammatory biomarkers after six weeks of consumption [36], while in a corresponding 8-week study, no differences were noted between groups [37].
Immunoglobulin A (IgA) stands out as the predominant antibody isotype, playing a crucial role in the initial defense against pathogens at mucosal surfaces and contributing to the maintenance of mucosal balance [38]. Secretory IgA plays an important role in protection against infections caused by enteropathogenesis in both human and animal models [39]. IgA is enhanced by probiotics as a reaction related to the mucosal immunity of the host intestine. Intestinal micro-organisms may contribute to the development of the acquired immune system of infants, especially in the development of mucosal immunity and the production of endogenous IgA [40]. However, it should be noted that in the present study, no statistically significant effect of probiotic consumption on IgA levels was observed. This may be attributed to both the strain and dose of probiotics administered in the present study.
The effect of probiotics on biomarkers related to the lipid profile has been studied extensively in recent years, and research results indicate that the estimated time needed to observe more definite results using probiotics in isolation appears to be 6 weeks [41]. According to a meta-analysis that included studies of different probiotic strains in healthy adults, probiotics can significantly reduce serum TC, whereas the same study assumed that different intervention groups with single or multiple strains and low or high doses did not show significant differences in lowering TC [42]. In the present study, no statistically significant differences were detected between the two groups, whereas in the probiotic group, there was an increase in total cholesterol levels. Similarly, for triglyceride levels, no statistically significant differences were noted between the groups; however, there was an increase in triglyceride levels within the probiotic group. Literature suggests that serum cholesterol and triglyceride levels may be more dependent on the degree of adiposity in volunteers than on the frequency of consumption of fat, sugar, starch, or alcohol [43]. This justifies the increase in cholesterol and triglyceride lipid levels in the probiotic group, while, as shown above, the probiotic group appears to have a significantly higher BMI compared to the control group.
In conjunction with triglyceride levels, both HDL and LDL cholesterol levels serve as risk factors for cardiovascular disease. The effect of probiotics on HDL and LDL cholesterol levels is highly heterogeneous; however, it can be observed that in individuals with higher metabolic risk, the effect of probiotics in reducing LDL and increasing HDL cholesterol is higher [44,45,46]. In clinical trials employing a similar design, there were no discernible metabolic variations observed in the aforementioned biomarkers among healthy participants [47,48]. In the present study, no statistically significant effect of probiotic consumption on HDL- and LDL- cholesterol levels was observed. This may be attributed to the health status of the participants, as they were not individuals with a higher metabolic risk. Moreover, the lack of change in the examined biomarkers may be strain-related.
Abnormal glucose metabolism is causally related to a greater risk of several chronic disorders, including dyslipidemia and cardiovascular diseases, and dietary constituents and supplements have been proposed to improve glycemic control [49]. Several trials have suggested that probiotic consumption may prevent or reduce elevated blood glucose levels while the glucose-lowering effect of Lactobacillus and Bifidobacteria has been investigated in several human studies [50]. In the present study, examining the effect of Lactococcus cremoris spp., no statistically significant differences were found between the two groups. In parallel with glucose metabolism, the impact of probiotics on insulin levels is an area of ongoing research, and several studies suggest that probiotic supplementation may improve insulin metabolism [51]. According to the results of the present study, a significant reduction in insulin levels was detected within the probiotic group at the 6th week of intervention, which returned to baseline values during the 12th week of intervention. However, no statistically significant differences were found between probiotic and control group.
Further examination of biomarkers associated with cardiovascular diseases, such as serum cortisol, uric acid levels and plasma total antioxidant capacity (TAC), was performed. Cortisol, which is synthesized from cholesterol, is the main glucocorticoid in the zona fasciculata of the human adrenal cortex [52], and it was recently recognized that cortisol may be involved in a number of forms of hypertension [53] and other cardiovascular risk factors such as hyperinsulinemia, hyperglycemia, insulin resistance, and dyslipidemia [54]. Data on the effects of probiotic strains on cortisol, as well as the metabolic mechanisms that bring about possible changes, are limited. A symbiotic consisting of Lactobacillus spp., Bifidobacterium spp., and prebiotics reduced serum cortisol levels after 12 weeks of consumption [55], whereas a study with a similar intervention product observed a reduction in urinary cortisol over 8 weeks [56]. However, a study of functional yogurt containing Lactobacillus spp. and Bifidobacterium spp. observed no statistically significant differences in cortisol secretion over a 12-week period [57]. In the present study, a statistically significant reduction in cortisol secretion was identified during the 6th week of intervention in the probiotic group, which was maintained during the 12th week of intervention. However, no statistically significant differences were found between the two groups.
While the correlation between serum uric acid and cardiovascular disease has long been acknowledged, it remains inconclusive whether serum uric acid acts as a causative agent in cardiovascular disease or merely represents a risk factor strongly linked to established cardiovascular risk factors such as hypertension and dyslipidemia [58]. Considerable clinical and epidemiological evidence supports that probiotics reduce serum uric acid levels, through three often overlooked mechanisms: (1) metabolizing purines into compounds distinct from uric acid; (2) diminishing the activity of xanthine oxidase (liver enzyme associated with uric acid production); and (3) enhancing the expression of uric acid transporter proteins to facilitate the excretion of uric acid [59]. In an 8-week randomized trial, the daily consumption of yogurt enriched with Lactobacillus acidophilus and Bifidobacterium lactis significantly reduced serum uric acid levels in patients with metabolic syndrome [60]. In a same-design study, a yogurt beverage enriched with Lactobacillus gasseri reduced serum uric acid levels in patients with hypouricemia [61]. The present study detected no difference between groups in serum uric acid levels, probably because healthy volunteers with values within normal limits participated.
In recent years, the number of studies, both in vitro and in vivo, related to the antioxidant properties of probiotics has significantly increased, while the development of probiotics that exert antioxidant activity and counteract oxidative stress is a novel approach to reduce oxidative stress [62]. Oxidative stress is also a key factor in the pathogenesis of CVD (e.g., atherosclerosis), and a disorder of prooxidant/antioxidant balance and domination of prooxidative reactions may lead to oxidative stress in the nervous system, which may affect brain development and function [63]. In a seven-week study, a synbiotic capsule containing Lactobacillus casei with inulin was found to be an effective compound that protects the human body from oxidative stress damage and increases total antioxidant plasma capacity [64]. However, in the present study no statistically significant differences were found between the two groups.
Given humans' inability to internally synthesize most vitamins, reliance on exogenous sources is necessary; the utilization of microorganisms capable of producing vitamins presents a potentially more natural and consumer-friendly alternative to fortification with chemically synthesized pseudo-vitamins [65]. Folate is a B-group vitamin that is involved in many metabolic pathways, such as energy usage, nucleic acid synthesis, and one-carbon metabolism, while recent findings link folate levels with the reduction of neural tube defects, coronary heart diseases, and cancer [66]. LAB have been reported to be folate producers; however, the ability of microbial cultures to produce or utilize folate varies considerably and is a strain-dependent trait [67]. Research indicates that the substantial folate synthesis within the human gastrointestinal tract could be clinically relevant if bioavailable, with direct in vivo evidence demonstrating the absorption of bacterially synthesized folate across the intact large intestine and its incorporation into tissues [68]. Vitamin B12, like folate, are associated with preventing chronic diseases associated with aging through the methylation of homocysteine [69]. Vitamin B12, otherwise known as cobalamin, has the most complex structure of all the vitamins synthesized by bacteria requiring about 30 genes for its biosynthesis [70]. Apart from the production of vitamin B12 by some probiotic bacteria, probiotics might improve vitamin B12 status by altering the composition of the gut microbiome and reducing the abundance of intestinal bacteria involved in B12 catabolism [71]. Improvements in nutrient status following the administration of certain probiotics have been noted for B-group vitamins (folate and B12) [72,73,74]; however, clinical trials assessing probiotic supplementation have yielded varying outcomes across diverse micronutrients. In the present study, the impact of the Lactococcus cremoris strain on folate levels in healthy volunteers was assessed, revealing no statistically significant differences between the intervention groups, likely attributable to the inability of the strain to produce folate. Vitamin B12 levels were significantly increased within probiotic group, however this change was not detected between groups.
Vitamin D, a fat-soluble vitamin, is essential for the development and maintenance of bone tissue, as well as for normal homeostasis of calcium and phosphorus and normal functioning of the immune system [75]. Implicated in the onset of various chronic endocrine and metabolic disorders, vitamin D deficiency is associated with a decreased risk of cardiovascular diseases, diabetes, and metabolic syndrome, as indicated by meta-analyses emphasizing the importance of maintaining sufficient vitamin D concentrations in adults [76]. Evidence from a clinical trial suggested the role of the probiotic bacteria Lactobacillus reuteri in increasing vitamin D levels [77], while further data on the effect of probiotic ingredients on vitamin levels are needed. In the present study, no significant changes were observed in vitamin D levels between the groups.
Moving on to urine biomarkers, phosphate and magnesium levels were examined. Urine magnesium (Mg) levels indicates Mg body content while Mg-deficient volunteers tend to retain a greater proportion of a Mg load and, consequently, excrete less Mg in urine than normal individuals do [78]. Probiotics can stimulate the quantitative or qualitative composition of the intestinal microflora to improve and magnesium bioavailability [79]. According to in vivo results, multi strain probiotic consumption tend to affect magnesium levels in some organs through the absorption and distribution process in the organism. The present study detected a significant reduction of urine magnesium levels at the 6th week of intervention for the probiotic group which indicates that magnesium has been incorporated into the cells due to its necessity. In the case of urine phosphorus, data remain limited, while a study examining the effects of probiotics on urine phosphorus absorption did not detect statistically significant differences [80]. These data are consistent with the results of the present study, according to which no statistically significant differences in urine phosphorus absorption were detected between the two groups.
Also, it should be stated that the present study had some limitations. First, a 12- week dietary intervention might not be sufficient to change the gut microbiota composition and blood markers in healthy subjects due to an unhealthy lifestyle. However, prolonging the duration of the study could potentially impact compliance, thereby negating any potential benefits. Second, during the conduct of the study the volunteers were not given a dispenser for the intervention product but clear instructions to use household utensils as dispensers. This may have caused discrepancies in the consumption of the intervention product among the volunteers. Despite the above, the study was significantly and adequately powered to investigate the efficacy of probiotic immobilized oat flakes on blood and urine biomarkers.
5. Conclusions
In this randomized, placebo-controlled, single-blind clinical trial we found a positive effect of Lactococcus cremoris spp. immobilized on oat flakes on inflammatory biomarkers after a 12-week consumption. However, it is essential to approach these findings with caution, and additional research is needed owing to the diversity of health outcomes, variations in the assays employed in the studies, and the complexity of the pathways in which gut microbiota play a role in the inflammation and anti-inflammation balance in different diseases.
Author Contributions
Conceptualization, Panoraia Bousdouni, Panagiota Potsaki, Andreas Tzakos, Yiannis Kourkoutas and Antonios Koutelidakis; Data curation, Aikaterini Kandyliari, Ioanna Prapa, Gregoria Mitropoulou and Antonios Koutelidakis; Formal analysis, Panoraia Bousdouni, Aikaterini Kandyliari, Panagiota Potsaki, Nikoletta Stathopoulou, Maria Kapsokefalou, Vasiliki Bountziouka and Gregoria Mitropoulou; Funding acquisition, Andreas Tzakos, Yiannis Kourkoutas and Antonios Koutelidakis; Investigation, Panoraia Bousdouni, Anastasia Kargadouri, Panagiota Potsaki, Olga Papagianni, Maria-Eleni Stylianou, Nikoletta Stathopoulou, Maria Kapsokefalou, Anastasia Kolomvotsou, Ioanna Prapa, Chrysoula Pavlatou and Yiannis Kourkoutas; Methodology, Panoraia Bousdouni, Aikaterini Kandyliari, Anastasia Kargadouri, Olga Papagianni, Maria-Eleni Stylianou, Nikoletta Stathopoulou, Panagiota Andrianopoulou, Anastasia Kolomvotsou, Ioanna Prapa, Gregoria Mitropoulou, Chrysoula Pavlatou and Panayiotis Panas; Project administration, Panayiotis Panas and Antonios Koutelidakis; Resources, Panoraia Bousdouni, Anastasia Kargadouri, Maria-Eleni Stylianou, Nikoletta Stathopoulou, Panagiota Andrianopoulou, Maria Kapsokefalou, Anastasia Kolomvotsou, Ioanna Prapa, Chrysoula Pavlatou, Andreas Tzakos, Panayiotis Panas and Yiannis Kourkoutas; Software, Panoraia Bousdouni, Aikaterini Kandyliari, Panagiota Potsaki, Olga Papagianni and Vasiliki Bountziouka; Supervision, Antonios Koutelidakis; Validation, Panoraia Bousdouni, Aikaterini Kandyliari, Anastasia Kargadouri, Olga Papagianni, Panagiota Andrianopoulou, Andreas Tzakos, Yiannis Kourkoutas and Antonios Koutelidakis; Visualization, Vasiliki Bountziouka, Andreas Tzakos and Antonios Koutelidakis; Writing – original draft, Panoraia Bousdouni and Aikaterini Kandyliari; Writing – review & editing, Vasiliki Bountziouka, Gregoria Mitropoulou, Yiannis Kourkoutas and Antonios Koutelidakis. All authors have read and agreed to the published version of the manuscript.
Funding
This research is part of the project, “Infrastructure of Microbiome Applications in Food Systems-FoodBiomes”, which is co-funded by the European Regional Development Fund (ERDF), under the Operational Program “Competitiveness, Entrepreneurship and Innovation-EPANEK 2014–2020”, Call 111 “Support for Regional Excellence”.
Institutional Review Board Statement
The study protocol was approved by the Research Ethics and Ethics Committee of the University of the Aegean (approval 3343/February 15th,2022) and it was registered at www.clinicaltrials.gov before enrolment of the first patient (ClinicalTrials.gov identifier NCT05612243).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patient(s) to publish this paper” if applicable.
Data Availability Statement
The data is available after demand.
Acknowledgments
We thank all the volunteers who participated to the study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- de Melo Pereira, G.V.; de Oliveira Coelho, B.; Magalhães Júnior, A.I.; Thomaz-Soccol, V.; Soccol, C.R. How to Select a Probiotic? A Review and Update of Methods and Criteria. Biotechnology Advances 2018, 36, 2060–2076. [Google Scholar] [CrossRef] [PubMed]
- Maldonado Galdeano, C.; Cazorla, S.I.; Lemme Dumit, J.M.; Vélez, E.; Perdigón, G. Beneficial Effects of Probiotic Consumption on the Immune System. Annals of Nutrition and Metabolism 2019, 74, 115–124. [Google Scholar] [CrossRef]
- Gill, H.S.; Guarner, F. Probiotics and Human Health: A Clinical Perspective. Postgrad Med J 2004, 80, 516–526. [Google Scholar] [CrossRef]
- Wang, J.; Ji, H.; Wang, S.; Liu, H.; Zhang, W.; Zhang, D.; Wang, Y. Probiotic Lactobacillus Plantarum Promotes Intestinal Barrier Function by Strengthening the Epithelium and Modulating Gut Microbiota. Frontiers in Microbiology 2018, 9. [Google Scholar] [CrossRef]
- Lin, C.-S.; Chang, C.-J.; Lu, C.-C.; Martel, J.; Ojcius, D.M.; Ko, Y.-F.; Young, J.D.; Lai, H.-C. Impact of the Gut Microbiota, Prebiotics, and Probiotics on Human Health and Disease. Biomed J 2014, 37, 259–268. [Google Scholar] [CrossRef]
- O’Toole, P.W.; Cooney, J.C. Probiotic Bacteria Influence the Composition and Function of the Intestinal Microbiota. Interdisciplinary Perspectives on Infectious Diseases 2008, 2008, e175285. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, B.; Claes, I.; Lebeer, S. Functional Mechanisms of Probiotics. Journal of Microbiology, Biotechnology and Food Sciences 2015, 04, 321–327. [Google Scholar] [CrossRef]
- Maftei, N.-M.; Raileanu, C.R.; Balta, A.A.; Ambrose, L.; Boev, M.; Marin, D.B.; Lisa, E.L. The Potential Impact of Probiotics on Human Health: An Update on Their Health-Promoting Properties. Microorganisms 2024, 12, 234. [Google Scholar] [CrossRef] [PubMed]
- Cimminiello, C.; Zambon, A.; Polo Friz, H. Hypercholesterolemia and cardiovascular risk: advantages and limitations of current treatment options. G Ital Cardiol (Rome) 2016, 17, 6S–13. [Google Scholar] [CrossRef]
- Bhat, B.; Bajaj, B.K. Multifarious Cholesterol Lowering Potential of Lactic Acid Bacteria Equipped with Desired Probiotic Functional Attributes. 3 Biotech 2020, 10, 200. [Google Scholar] [CrossRef]
- Rigobelo, E. Probiotics; BoD – Books on Demand, 2012; ISBN 978-953-51-0776-7.
- Alahmari, L.A. Dietary Fiber Influence on Overall Health, with an Emphasis on CVD, Diabetes, Obesity, Colon Cancer, and Inflammation. Front Nutr 2024, 11, 1510564. [Google Scholar] [CrossRef] [PubMed]
- Joyce, S.A.; Kamil, A.; Fleige, L.; Gahan, C.G.M. The Cholesterol-Lowering Effect of Oats and Oat Beta Glucan: Modes of Action and Potential Role of Bile Acids and the Microbiome. Front Nutr 2019, 6, 171. [Google Scholar] [CrossRef] [PubMed]
- Min, M.; Bunt, C.R.; Mason, S.L.; Hussain, M.A. Non-Dairy Probiotic Food Products: An Emerging Group of Functional Foods. Critical Reviews in Food Science and Nutrition 2019, 59, 2626–2641. [Google Scholar] [CrossRef]
- Ghishan, F.K.; Kiela, P.R. From Probiotics to Therapeutics: Another Step Forward? J Clin Invest 2011, 121, 2149–2152. [Google Scholar] [CrossRef]
- Ranjha, M.M.A.N.; Shafique, B.; Batool, M.; Kowalczewski, P.Ł.; Shehzad, Q.; Usman, M.; Manzoor, M.F.; Zahra, S.M.; Yaqub, S.; Aadil, R.M. Nutritional and Health Potential of Probiotics: A Review. Applied Sciences 2021, 11, 11204. [Google Scholar] [CrossRef]
- Ranadheera, R.D.C.S.; Baines, S.K.; Adams, M.C. Importance of Food in Probiotic Efficacy. Food Research International 2010, 43, 1–7. [Google Scholar] [CrossRef]
- From Probiotics to Prebiotics and a Healthy Digestive System - Gibson - 2004 - Journal of Food Science - Wiley Online Library. Available online: https://ift.onlinelibrary.wiley.com/doi/abs/10.1111/j.1365-2621.2004.tb10724.x?casa_token=YzW3rNy_DMoAAAAA:UDFodGkqNynYTBpVp6IR8OXq09o0-ZEg8QaW16YNnlrxWtRicBkb4--09EbIMLxArFHPtFH1-2Ji42s (accessed on 19 October 2023).
- Axelsson, L.; Ahrné, S. Lactic Acid Bacteria. In Applied Microbial Systematics; Priest, F.G., Goodfellow, M., Eds.; Springer Netherlands: Dordrecht, 2000; pp. 367–388. ISBN 978-0-7923-6518-1. [Google Scholar]
- Wang, Y.; Wu, J.; Lv, M.; Shao, Z.; Hungwe, M.; Wang, J.; Bai, X.; Xie, J.; Wang, Y.; Geng, W. Metabolism Characteristics of Lactic Acid Bacteria and the Expanding Applications in Food Industry. Frontiers in Bioengineering and Biotechnology 2021, 9. [Google Scholar] [CrossRef]
- Ishida, T.; Yokota, A.; Umezawa, Y.; Toda, T.; Yamada, K. Identification and Characterization of Lactococcal and Acetobacter Strains Isolated from Traditional Caucasusian Fermented Milk. Journal of Nutritional Science and Vitaminology 2005, 51, 187–193. [Google Scholar] [CrossRef]
- Watanabe, M.; Maruo, T.; Suzuki, T. Effects of Intake of Lactococcus Cremoris Subsp. Cremoris FC on Constipation Symptoms and Immune System in Healthy Participants with Mild Constipation: A Double-Blind, Placebo-Controlled Study. International Journal of Food Sciences and Nutrition 2023, 74, 695–706. [Google Scholar] [CrossRef]
- Ozaki, K.; Maruo, T.; Kosaka, H.; Mori, M.; Mori, H.; Yamori, Y.; Toda, T. The Effects of Fermented Milk Containing Lactococcus Lactis Subsp. Cremoris FC on Defaecation in Healthy Young Japanese Women: A Double-Blind, Placebo-Controlled Study. International Journal of Food Sciences and Nutrition 2018, 69, 762–769. [Google Scholar] [CrossRef]
- Prapa, I.; Pavlatou, C.; Kompoura, V.; Nikolaou, A.; Stylianopoulou, E.; Skavdis, G.; Grigoriou, M.E.; Kourkoutas, Y. A Novel Wild-Type Lacticaseibacillus Paracasei Strain Suitable for the Production of Functional Yoghurt and Ayran Products. Fermentation 2025, 11, 37. [Google Scholar] [CrossRef]
- Benzie, I.F.F.; Strain, J.J. The Ferric Reducing Ability of Plasma (FRAP) as a Measure of “Antioxidant Power”: The FRAP Assay. Analytical Biochemistry 1996, 239, 70–76. [Google Scholar] [CrossRef]
- CONSORT 2010 Statement: Updated Guidelines for Reporting Parallel Group Randomised Trials | The BMJ. Available online: https://www.bmj.com/content/340/bmj.c332 (accessed on 23 February 2023).
- A Healthy Lifestyle - WHO Recommendations. Available online: https://www.who.int/europe/news-room/fact-sheets/item/a-healthy-lifestyle---who-recommendations (accessed on 13 February 2024).
- Yeo, S.-K.; Ewe, J.-A.; Tham, C.S.-C.; Liong, M.-T. Carriers of Probiotic Microorganisms. In Probiotics: Biology, Genetics and Health Aspects; Liong, M.-T., Ed.; Microbiology Monographs; Springer: Berlin, Heidelberg, 2011; pp. 191–220. ISBN 978-3-642-20838-6. [Google Scholar]
- Granato, D.; Branco, G.F.; Nazzaro, F.; Cruz, A.G.; Faria, J.A.F. Functional Foods and Nondairy Probiotic Food Development: Trends, Concepts, and Products. Comprehensive Reviews in Food Science and Food Safety 2010, 9, 292–302. [Google Scholar] [CrossRef] [PubMed]
- Rivera-Espinoza, Y.; Gallardo-Navarro, Y. Non-Dairy Probiotic Products. Food Microbiology 2010, 27, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Rasika, D.M.D.; Vidanarachchi, J.K.; Luiz, S.F.; Azeredo, D.R.P.; Cruz, A.G.; Ranadheera, C.S. Probiotic Delivery through Non-Dairy Plant-Based Food Matrices. Agriculture 2021, 11, 599. [Google Scholar] [CrossRef]
- Nagpal, R.; Kaur, A. Synbiotic Effect of Various Prebiotics on In Vitro Activities of Probiotic Lactobacilli. Ecology of Food and Nutrition 2011, 50, 63–68. [Google Scholar] [CrossRef]
- Lee, Y.K.; Menezes, J.S.; Umesaki, Y.; Mazmanian, S.K. Proinflammatory T-Cell Responses to Gut Microbiota Promote Experimental Autoimmune Encephalomyelitis. Proc Natl Acad Sci U S A 2011, 108 Suppl 1, 4615–4622. [Google Scholar] [CrossRef]
- Lye, H.-S.; Kuan, C.-Y.; Ewe, J.-A.; Fung, W.-Y.; Liong, M.-T. The Improvement of Hypertension by Probiotics: Effects on Cholesterol, Diabetes, Renin, and Phytoestrogens. International Journal of Molecular Sciences 2009, 10, 3755–3775. [Google Scholar] [CrossRef]
- Kazemi, A.; Soltani, S.; Ghorabi, S.; Keshtkar, A.; Daneshzad, E.; Nasri, F.; Mazloomi, S.M. Effect of Probiotic and Synbiotic Supplementation on Inflammatory Markers in Health and Disease Status: A Systematic Review and Meta-Analysis of Clinical Trials. Clinical Nutrition 2020, 39, 789–819. [Google Scholar] [CrossRef]
- Rajkumar, H.; Kumar, M.; Das, N.; Kumar, S.N.; Challa, H.R.; Nagpal, R. Effect of Probiotic Lactobacillus Salivarius UBL S22 and Prebiotic Fructo-Oligosaccharide on Serum Lipids, Inflammatory Markers, Insulin Sensitivity, and Gut Bacteria in Healthy Young Volunteers: A Randomized Controlled Single-Blind Pilot Study. J Cardiovasc Pharmacol Ther 2015, 20, 289–298. [Google Scholar] [CrossRef]
- Gomes, A.C.; de Sousa, R.G.M.; Botelho, P.B.; Gomes, T.L.N.; Prada, P.O.; Mota, J.F. The Additional Effects of a Probiotic Mix on Abdominal Adiposity and Antioxidant Status: A Double-Blind, Randomized Trial. Obesity (Silver Spring) 2017, 25, 30–38. [Google Scholar] [CrossRef] [PubMed]
- Nihei, Y.; Suzuki, H.; Suzuki, Y. Current Understanding of IgA Antibodies in the Pathogenesis of IgA Nephropathy. Front Immunol 2023, 14, 1165394. [Google Scholar] [CrossRef]
- Marcotte, H.; Lavoie, M.C. Oral Microbial Ecology and the Role of Salivary Immunoglobulin A. Microbiol Mol Biol Rev 1998, 62, 71–109. [Google Scholar] [CrossRef] [PubMed]
- Walker, W.A. Role of Nutrients and Bacterial Colonization in the Development of Intestinal Host Defense. J Pediatr Gastroenterol Nutr 2000, 30 Suppl 2, S2–7. [Google Scholar] [CrossRef]
- Gadelha, C.J.M.U.; Bezerra, A.N. Effects of Probiotics on the Lipid Profile: Systematic Review. J. vasc. bras. 2019, 18, e20180124. [Google Scholar] [CrossRef]
- Wang, L.; Guo, M.-J.; Gao, Q.; Yang, J.-F.; Yang, L.; Pang, X.-L.; Jiang, X.-J. The Effects of Probiotics on Total Cholesterol. Medicine (Baltimore) 2018, 97, e9679. [Google Scholar] [CrossRef] [PubMed]
- Nichols, A.B.; Ravenscroft, C.; Lamphiear, D.E.; Ostrander, L.D., Jr. Independence of Serum Lipid Levels and Dietary Habits: The Tecumseh Study. JAMA 1976, 236, 1948–1953. [Google Scholar] [CrossRef]
- Kullisaar, T.; Zilmer, K.; Salum, T.; Rehema, A.; Zilmer, M. The Use of Probiotic L. Fermentum ME-3 Containing Reg’Activ Cholesterol Supplement for 4 Weeks Has a Positive Influence on Blood Lipoprotein Profiles and Inflammatory Cytokines: An Open-Label Preliminary Study. Nutr J 2016, 15, 93. [Google Scholar] [CrossRef]
- Rajkumar, H.; Mahmood, N.; Kumar, M.; Varikuti, S.R.; Challa, H.R.; Myakala, S.P. Effect of Probiotic (VSL#3) and Omega-3 on Lipid Profile, Insulin Sensitivity, Inflammatory Markers, and Gut Colonization in Overweight Adults: A Randomized, Controlled Trial. Mediators of Inflammation 2014, 2014, e348959. [Google Scholar] [CrossRef]
- Fuentes, M.C.; Lajo, T.; Carrión, J.M.; Cuñé, J. Cholesterol-Lowering Efficacy of Lactobacillus Plantarum CECT 7527, 7528 and 7529 in Hypercholesterolaemic Adults. British Journal of Nutrition 2013, 109, 1866–1872. [Google Scholar] [CrossRef]
- Angelino, D.; Martina, A.; Rosi, A.; Veronesi, L.; Antonini, M.; Mennella, I.; Vitaglione, P.; Grioni, S.; Brighenti, F.; Zavaroni, I.; et al. Glucose- and Lipid-Related Biomarkers Are Affected in Healthy Obese or Hyperglycemic Adults Consuming a Whole-Grain Pasta Enriched in Prebiotics and Probiotics: A 12-Week Randomized Controlled Trial. J Nutr 2019, 149, 1714–1723. [Google Scholar] [CrossRef] [PubMed]
- Rahayu, E.S.; Mariyatun, M.; Putri Manurung, N.E.; Hasan, P.N.; Therdtatha, P.; Mishima, R.; Komalasari, H.; Mahfuzah, N.A.; Pamungkaningtyas, F.H.; Yoga, W.K.; et al. Effect of Probiotic Lactobacillus Plantarum Dad-13 Powder Consumption on the Gut Microbiota and Intestinal Health of Overweight Adults. World J Gastroenterol 2021, 27, 107–128. [Google Scholar] [CrossRef] [PubMed]
- Ruan, Y.; Sun, J.; He, J.; Chen, F.; Chen, R.; Chen, H. Effect of Probiotics on Glycemic Control: A Systematic Review and Meta-Analysis of Randomized, Controlled Trials. PLoS ONE 2015, 10, e0132121. [Google Scholar] [CrossRef]
- Nikbakht, E.; Khalesi, S.; Singh, I.; Williams, L.T.; West, N.P.; Colson, N. Effect of Probiotics and Synbiotics on Blood Glucose: A Systematic Review and Meta-Analysis of Controlled Trials. Eur J Nutr 2018, 57, 95–106. [Google Scholar] [CrossRef] [PubMed]
- Kassaian, N.; Feizi, A.; Aminorroaya, A.; Jafari, P.; Ebrahimi, M.T.; Amini, M. The Effects of Probiotics and Synbiotic Supplementation on Glucose and Insulin Metabolism in Adults with Prediabetes: A Double-Blind Randomized Clinical Trial. Acta Diabetol 2018, 55, 1019–1028. [Google Scholar] [CrossRef]
- Lee, D.Y.; Kim, E.; Choi, M.H. Technical and Clinical Aspects of Cortisol as a Biochemical Marker of Chronic Stress. BMB Rep 2015, 48, 209–216. [Google Scholar] [CrossRef]
- Whitworth, J.A.; Mangos, G.J.; Kelly, J.J. Cushing, Cortisol, and Cardiovascular Disease. Hypertension 2000, 36, 912–916. [Google Scholar] [CrossRef]
- Whitworth, J.A.; Williamson, P.M.; Mangos, G.; Kelly, J.J. Cardiovascular Consequences of Cortisol Excess. Vascular Health and Risk Management 2005, 1, 291–299. [Google Scholar] [CrossRef]
- Lalitsuradej, E.; Sirilun, S.; Sittiprapaporn, P.; Sivamaruthi, B.S.; Pintha, K.; Tantipaiboonwong, P.; Khongtan, S.; Fukngoen, P.; Peerajan, S.; Chaiyasut, C. The Effects of Synbiotics Administration on Stress-Related Parameters in Thai Subjects—A Preliminary Study. Foods 2022, 11, 759. [Google Scholar] [CrossRef]
- Kazemi, A.; Noorbala, A.A.; Azam, K.; Djafarian, K. Effect of Prebiotic and Probiotic Supplementation on Circulating Pro-Inflammatory Cytokines and Urinary Cortisol Levels in Patients with Major Depressive Disorder: A Double-Blind, Placebo-Controlled Randomized Clinical Trial. Journal of Functional Foods 2019, 52, 596–602. [Google Scholar] [CrossRef]
- Nishihira, J.; Kagami-Katsuyama, H.; Tanaka, A.; Nishimura, M.; Kobayashi, T.; Kawasaki, Y. Elevation of Natural Killer Cell Activity and Alleviation of Mental Stress by the Consumption of Yogurt Containing Lactobacillus Gasseri SBT2055 and Bifidobacterium Longum SBT2928 in a Double-Blind, Placebo-Controlled Clinical Trial. Journal of Functional Foods 2014, 11, 261–268. [Google Scholar] [CrossRef]
- Wu, A.H.; Gladden, J.D.; Ahmed, M.; Ahmed, A.; Filippatos, G. Relation of Serum Uric Acid to Cardiovascular Disease. International Journal of Cardiology 2016, 213, 4–7. [Google Scholar] [CrossRef]
- Zhao, H.; Lu, Z.; Lu, Y. The Potential of Probiotics in the Amelioration of Hyperuricemia. Food & Function 2022, 13, 2394–2414. [Google Scholar] [CrossRef]
- Rezazadeh, L.; Alipour, B.; Jafarabadi, M.A.; Behrooz, M.; Gargari, B.P. Daily Consumption Effects of Probiotic Yogurt Containing Lactobacillus Acidophilus La5 and Bifidobacterium Lactis Bb12 on Oxidative Stress in Metabolic Syndrome Patients. Clinical Nutrition ESPEN 2021, 41, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Yamanaka, H.; Taniguchi, A.; Tsuboi, H.; Kano, H.; Asami, Y. Hypouricaemic Effects of Yoghurt Containing Lactobacillus Gasseri PA-3 in Patients with Hyperuricaemia and/or Gout: A Randomised, Double-Blind, Placebo-Controlled Study. Mod Rheumatol 2019, 29, 146–150. [Google Scholar] [CrossRef]
- Amaretti, A.; di Nunzio, M.; Pompei, A.; Raimondi, S.; Rossi, M.; Bordoni, A. Antioxidant Properties of Potentially Probiotic Bacteria: In Vitro and in Vivo Activities. Appl Microbiol Biotechnol 2013, 97, 809–817. [Google Scholar] [CrossRef] [PubMed]
- Harasym, J.; Oledzki, R. Effect of Fruit and Vegetable Antioxidants on Total Antioxidant Capacity of Blood Plasma. Nutrition 2014, 30, 511–517. [Google Scholar] [CrossRef]
- Kleniewska, P.; Hoffmann, A.; Pniewska, E.; Pawliczak, R. The Influence of Probiotic Lactobacillus Casei in Combination with Prebiotic Inulin on the Antioxidant Capacity of Human Plasma. Oxidative Medicine and Cellular Longevity 2016, 2016, e1340903. [Google Scholar] [CrossRef]
- LeMone, P. Vitamins and Minerals. Journal of Obstetric, Gynecologic, & Neonatal Nursing 1999, 28, 520–533. [Google Scholar] [CrossRef]
- Gangadharan, D.; Nampoothiri, K.M. Folate Production Using Lactococcus Lactis Ssp Cremoris with Implications for Fortification of Skim Milk and Fruit Juices. LWT - Food Science and Technology 2011, 44, 1859–1864. [Google Scholar] [CrossRef]
- Rossi, M.; Amaretti, A.; Raimondi, S. Folate Production by Probiotic Bacteria. Nutrients 2011, 3, 118–134. [Google Scholar] [CrossRef] [PubMed]
- Rong, N.; Selhub, J.; Goldin, B.R.; Rosenberg, I.H. Bacterially Synthesized Folate in Rat Large Intestine Is Incorporated into Host Tissue Folyl Polyglutamates. J Nutr 1991, 121, 1955–1959. [Google Scholar] [CrossRef] [PubMed]
- Clarke, R.; Grimley Evans, J.; Schneede, J.; Nexo, E.; Bates, C.; Fletcher, A.; Prentice, A.; Johnston, C.; Ueland, P.M.; Refsum, H.; et al. Vitamin B12 and Folate Deficiency in Later Life. Age Ageing 2004, 33, 34–41. [Google Scholar] [CrossRef]
- Gu, Q.; Li, P.; Gu, Q.; Li, P. Biosynthesis of Vitamins by Probiotic Bacteria. In Probiotics and Prebiotics in Human Nutrition and Health; IntechOpen, 2016 ISBN 978-953-51-2476-4.
- Barkhidarian, B.; Roldos, L.; Iskandar, M.M.; Saedisomeolia, A.; Kubow, S. Probiotic Supplementation and Micronutrient Status in Healthy Subjects: A Systematic Review of Clinical Trials. Nutrients 2021, 13, 3001. [Google Scholar] [CrossRef]
- Mokhtari, Z.; Karbaschian, Z.; Pazouki, A.; Kabir, A.; Hedayati, M.; Mirmiran, P.; Hekmatdoost, A. The Effects of Probiotic Supplements on Blood Markers of Endotoxin and Lipid Peroxidation in Patients Undergoing Gastric Bypass Surgery; a Randomized, Double-Blind, Placebo-Controlled, Clinical Trial with 13 Months Follow-Up. OBES SURG 2019, 29, 1248–1258. [Google Scholar] [CrossRef]
- Woodard, G.A.; Encarnacion, B.; Downey, J.R.; Peraza, J.; Chong, K.; Hernandez-Boussard, T.; Morton, J.M. Probiotics Improve Outcomes After Roux-En-Y Gastric Bypass Surgery: A Prospective Randomized Trial. J Gastrointest Surg 2009, 13, 1198–1204. [Google Scholar] [CrossRef] [PubMed]
- Valentini, L.; Pinto, A.; Bourdel-Marchasson, I.; Ostan, R.; Brigidi, P.; Turroni, S.; Hrelia, S.; Hrelia, P.; Bereswill, S.; Fischer, A.; et al. Impact of Personalized Diet and Probiotic Supplementation on Inflammation, Nutritional Parameters and Intestinal Microbiota - The “RISTOMED Project”: Randomized Controlled Trial in Healthy Older People. Clin Nutr 2015, 34, 593–602. [Google Scholar] [CrossRef]
- Prentice, A. Vitamin D Deficiency: A Global Perspective. Nutrition Reviews 2008, 66, S153–S164. [Google Scholar] [CrossRef]
- Pereira-Santos, M.; Costa, P.R.F.; Assis, A.M.O.; Santos, C. a. S.T.; Santos, D.B. Obesity and Vitamin D Deficiency: A Systematic Review and Meta-Analysis. Obes Rev 2015, 16, 341–349. [Google Scholar] [CrossRef]
- Jones, M.L.; Martoni, C.J.; Prakash, S. Oral Supplementation with Probiotic L. Reuteri NCIMB 30242 Increases Mean Circulating 25-Hydroxyvitamin D: A Post Hoc Analysis of a Randomized Controlled Trial. J Clin Endocrinol Metab 2013, 98, 2944–2951. [Google Scholar] [CrossRef]
- Musso, C.G. Magnesium Metabolism in Health and Disease. Int Urol Nephrol 2009, 41, 357–362. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Conesa, D.; López, G.; Abellán, P.; Ros, G. Bioavailability of Calcium, Magnesium and Phosphorus in Rats Fed Probiotic, Prebiotic and Synbiotic Powder Follow-up Infant Formulas and Their Effect on Physiological and Nutritional Parameters. Journal of the Science of Food and Agriculture 2006, 86, 2327–2336. [Google Scholar] [CrossRef]
- Scholz-Ahrens, K.E.; Adolphi, B.; Rochat, F.; Barclay, D.V.; de Vrese, M.; Açil, Y.; Schrezenmeir, J. Effects of Probiotics, Prebiotics, and Synbiotics on Mineral Metabolism in Ovariectomized Rats — Impact of Bacterial Mass, Intestinal Absorptive Area and Reduction of Bone Turn-Over. NFS Journal 2016, 3, 41–50. [Google Scholar] [CrossRef]
Figure 1.
CONSORT schematic of participant recruitment, screening, and assessment [26].
Figure 1.
CONSORT schematic of participant recruitment, screening, and assessment [26].
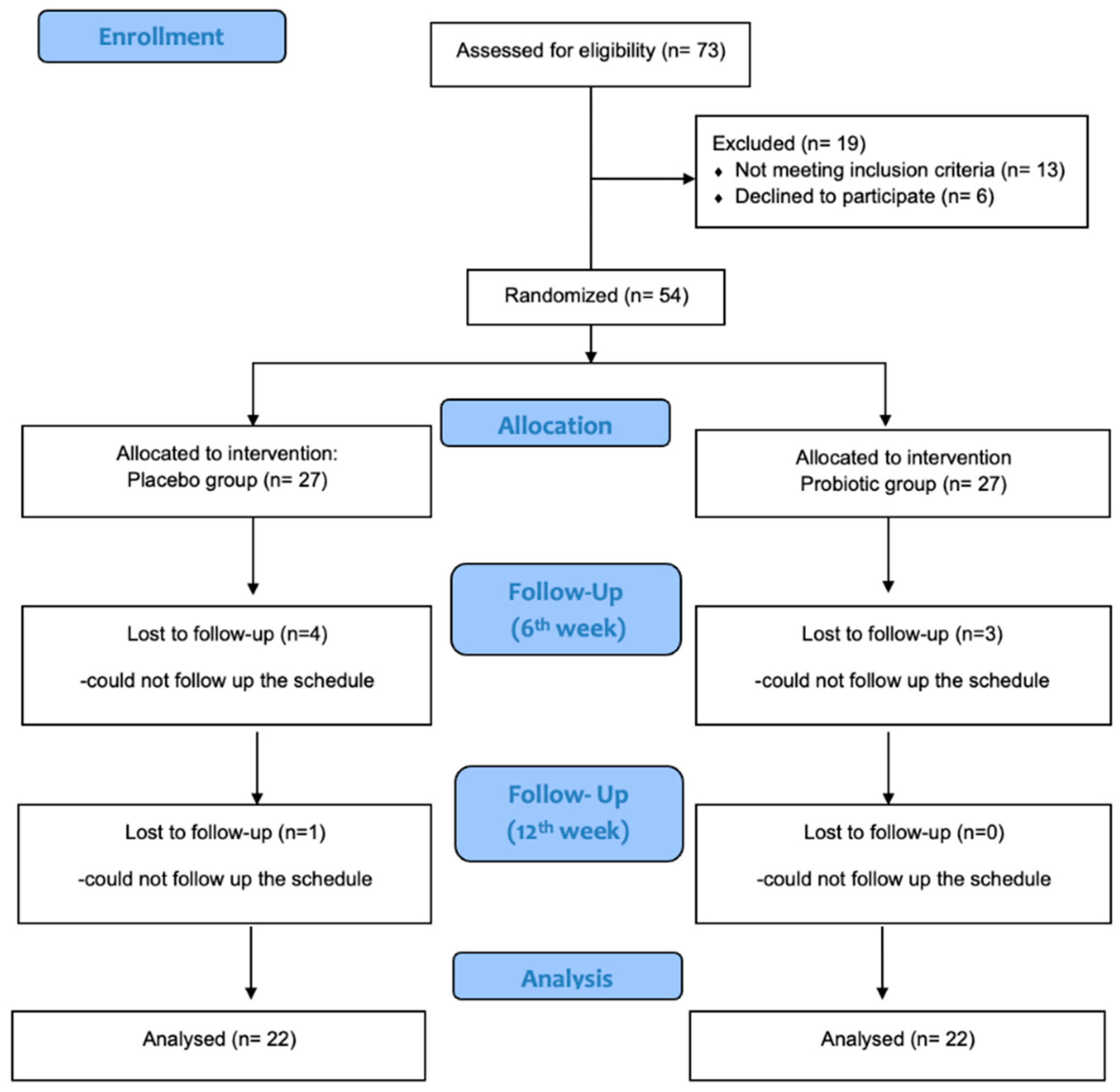

Table 1.
General characteristics of participants at baseline.
| Variables | Probiotic group (n=24) |
Control group (n=22) |
pa value |
|---|---|---|---|
| Female (%) | 70.8 | 68.2 | p> 0.05 |
| Age (years) | 36.6 (13.9) | 30.3 (10.2) | p> 0.05 |
| Height (m) | 1.68 (0.1) | 1.66 (0.1) | p> 0.05 |
| Body mass index (kg/m2) | 26.9 (5.5) | 23.3 (3.5) | p < 0.05 |
| Waist-to-hip ratio | 0.82 (0.1) | 0.80 (0.1) | p> 0.05 |
| Smoking (%) | 25.0 | 18.2 | p> 0.05 |
| Physical Activity (%) | p> 0.05 | ||
| High | 29.2 | 40.9 | |
| Regular | 25.0 | 13.6 | |
| Cholesterol (mg/dL) | 169.3 (23.4) | 172.18 (25.9) | p> 0.05 |
| Glucose (mg/dL) | 79.8 (11.5) | 79.6 (9.7) | p> 0.05 |
Data are presented as mean (SD) unless otherwise indicated. aby independent t-tests.
Table 3.
Serum and plasma biomarkers of each intervention group.
| Probiotics group (n = 24) | Placebo group (n=22) | pb | |||||
| Total Cholesterol | mean (SD) | Δ from baseline | pa | mean (SD | Change | pa | |
| 1st week | 171.0 (24.4) | 172.1 (25.8) | >0.05 | ||||
| 6th week | 190.2 (38.2) | 19.2 (44.0) | 0.039 | 176.1 (40.0) | 4.0 (30.4) | >0.05 | |
| 12th week | 175.8 (28.9) | 4.8 (28.3) | 0.040 | 179.3 (49.7) | 7.1 (33.2) | >0.05 | |
| LDL | |||||||
| 1st week | 86.2 (21.8) | 86.9 (23.4) | >0.05 | ||||
| 6th week | 91.3 (35.9) | 5.2 (28.0) | >0.05 | 80.5 (29.5) | -6.4 (18.0 | 0.005 | |
| 12th week | 91.7 (25.8) | 5.8 (14.0) | >0.05 | 92.3 (34.8) | 5.4 (17.7) | >0.05 | |
| HDL | |||||||
| 1st week | 53.5 (13.2) | 54.1 (9.8) | >0.05 | ||||
| 6th week | 51.6 (16.1) | -1.9 (14.9) | >0.05 | 53.6 (13.2) | -0.5 (13.0) | >0.05 | |
| 12th week | 54.63 (12.0) | 1.1 (9.3) | >0.05 | 58.5 (16.0) | 4.4 (11.4) | >0.05 | |
| TRGL | |||||||
| 1st week | 73.7 (30.4) | 83.5 (64.5) | >0.05 | ||||
| 6th week | 77.1 (37.1) | 3.4 (28.4) | >0.05 | 79.7 (52.9) | - 3.9 (36.5) | >0.05 | |
| 12th week | 82.4 (34.6) | 8.7 (19.1) | 0.04 | 80. 0 (43.9) | -3.5 (29.6) | >0.05 | |
| GLU | |||||||
| 1st week | 79.8 (11.5) | 79.6 (9.7) | >0.05 | ||||
| 6th week | 90.3 (19.4) | 10.5 (21.5) | 0.025 | 86.3 (16.3) | 6.7 (12.4) | 0.019 | |
| 12th week | 93.1 (10.5) | 13.3 (10.4) | <0.001 | 93.9 (11.2) | 14.3 (10.6) | <0.001 | |
| INS | |||||||
| 1st week | 9.5 (3.4) | 7.7 (3.4) | >0.05 | ||||
| 6th week | 7.8 (2.9) | -1.7 (1.9) | <0.001 | 8.2 (4.9) | 0.5 (3.7) | >0.05 | |
| 12th week | 11.2 (5.8) | +1.7 (3.7) | 0.042 | 7.8 (3.0) | 0.1 (2.4) | >0.05 | |
| UA | |||||||
| 1st week | 4.5 (1.4) | 4.5 (1.1) | >0.05 | ||||
| 6th week | 4.0 (1.8) | - 0.5 (0.9 | 0.008 | 4.1 (1.4) | -0.4 (0.9) | 0.025 | |
| 12th week | 4.6 (1.2) | 0.1 (0.6) | >0.05 | 4.7 (1.2) | 0.2 (1.0) | >0.05 | |
| Cortisol | |||||||
| 1st week | 165.7 (64.8) | 154.6 (50.1) | >0.05 | ||||
| 6th week | 131.0 (44.9) | -34.8 (50.6) | 0.003 | 139.8 (52.6) | 14.8 (36.4) | >0.05 | |
| 12th week | 137.5 (48.4) | -28.2 (38.4) | 0.002 | 132.7 (61.3) | 22.0 (58.1) | >0.05 | |
| hs-CRP | |||||||
| 1st week | 20.2 (21.7) | 9.1 (0.0) | 0.02 | ||||
| 6th week | 21.6 (33.0) | 1.4 (32.0) | >0.05 | 7.9 (11.0) | -1.2 (10.2) | >0.05 | |
| 12th week | 16.8 (20.8) | -3.4 (16.3) | >0.05 | 10.3 (12.0) | 1.2 (12.5) | >0.05 | |
| IgA | |||||||
| 1st week | 2352.6 (895.1) | 2188.5 (1179.0) | >0.05 | ||||
| 6th week | 2352.4 (789.8) | -0.3 (608.1) | >0.05 | 2515.4 (1304.1) | 327.9 (1266.7) | >0.05 | |
| 12th week | 2267.5 (782.4) | -85.2 (377.1) | >0.05 | 2213.8 (952.1) | 25.4 (780.4) | >0.05 | |
| IL-6 | |||||||
| 1st week | 4.3 (2.6) | 3.0 (1.8) | 0.045 | ||||
| 6th week | 2.5 (2.0) | -1.8 (2.6) | <0.002 | 1.5 (0.9) | -1.6 (2.2) | 0.001 | |
| 12th week | 2.9 (1.9) | -1.3 (2.9) | 0.03 | 2.9 (2.5) | -0.2 (3.4) | >0.05 | |
| Folate | |||||||
| 1st week | 7.9 (3.7) | 7.7 (3.7) | >0.05 | ||||
| 6th week | 6.8 (3.3) | -1.1 (2.1) | 0.012 | 7.7 (5.7) | -0.1 (1.9) | >0.05 | |
| 12th week | 5.7 (3.4) | -2.2 (2.2) | <0.001 | 5.5 (3.8) | -2.2 (3.2) | 0.004 | |
| VitB12 | |||||||
| 1st week | 468.7 (115.5) | 488.8 (187.5) | >0.05 | ||||
| 6th week | 502.3 (103.3) | 33.6 (83.4) | >0.05 | 511.6 (169.2) | 22.8 (120.4) | >0.05 | |
| 12th week | 522.7 (114.4) | 54.0 (118.7) | 0.036 | 506.8 (121.3) | 18.0 (93.6) | >0.05 | |
| VitD | |||||||
| 1st week | 23.5 (9.1) | 23.3 (8.2) | >0.05 | ||||
| 6th week | 22.3 (8.5) | -1.2 (3.0) | >0.05 | 24.0 (8.3) | 0.7 (4.1) | >0.05 | |
| 12th week3 | 25.9 (6.2) | 2.4 (7.7) | >0.05 | 25.1 (5.2) | 1.7 (6.7) | >0.05 | |
| TAC | |||||||
| 1st week | 0.8 (0.2) | 0.8 (0.2) | |||||
| 6th week | 0.9 (0.2) | 0.04 (0.1) | >0.05 | 0.8 (0.2) | 0.03 (0.1) | >0.05 | >0.05 |
| 12th week | 0.9 (0.2) | 0.06 (0.1) | 0.026 | 0.9 (0.2) | 0.05 (0.1) | >0.05 | |
pa indicates differences within groups; pb indicates differences between groups.
Table 4.
Urine biomarkers of each intervention group.
| Probiotics group (n=24) | Placebo group (n=22) | pb | |||||
| Urine Magnesium | mean (SD) | Δ from baseline | pa | mean (SD) | Change | pa | |
| 1st week | 11.0 (5.7) | 9.8 (7.7) | 0.022 | ||||
| 6th week | 7.9 (3.9) | -3.05 (5.6) | 0.01 | 8.2 (7.4) | -1.7 (9.7) | >0.05 | |
| 12th week | 10.4 (6.6) | -0.6 (8.2) | >0.05 | 9.0 (6.2) | -0.9 (6.4) | >0.05 | |
| Urine Phosphorus | |||||||
| 1st week | 103.7 (54.0) | 98.8 (44.8) | >0.05 | ||||
| 6th week | 105.0 (45.4) | 1.3 (50.3) | >0.05 | 91.0 (41.3) | -7.7 (54.8) | >0.05 | |
| 12th week | 106.1 (66.3) | 2.4 (50.6) | >0.05 | 120.9 (59.3) | 22.1 (73.8) | >0.05 | |
pa indicates differences within groups; pb indicates differences between groups.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



