
Submitted:
07 April 2025
Posted:
07 April 2025
You are already at the latest version
Abstract
Background/Objectives: Research on eating disorders (EDs) in individuals with multiple sclerosis (MS) is limited. In ED populations, neuroticism has been linked to ED symptoms through lower self-esteem and greater body dissatisfaction, but these relationships remain unexplored in MS. This study aimed to examine whether self-esteem and body dissatisfaction mediate the link between neuroticism and ED symptoms in individuals with MS. Methods: The current sample consisted of 275 participants who reported a neurologist-confirmed diagnosis of MS (M age = 43.0, SD = 12.9). Participants completed an online questionnaire measuring neuroticism (Big Five Inventory), self-esteem (Rosenberg Self-esteem Scale), body dissatisfaction (Body Shape Questionnaire), and ED symptoms (Eating Attitudes Test-26). Results: A serial mediation analysis controlling for age, sex, and ambulation level revealed that the association between neuroticism and ED symptoms is respectively and serially explained by self-esteem and body dissatisfaction in individuals with MS. The total model accounted for 43% of the variance in ED symptoms. Conclusions: Findings suggest that self-esteem and body dissatisfaction are important in understanding the relationship between neuroticism and ED symptoms and should be considered in the assessment and treatment of ED symptoms in individuals with MS.
Keywords:
eating disorder
; neuroticism
; body-dissatisfaction
; self-esteem
; multiple sclerosis
1. Introduction
Multiple sclerosis (MS) is a chronic autoimmune disease that affects the central nervous system, often leading to physical disability, cognitive difficulties, and emotional distress [1]. These psychological challenges may contribute to body image concerns and disordered eating (DE) behaviours, yet research on these symptoms in individuals with MS remains limited [2]. Eating disorders (EDs) are characterised by disturbances in eating behaviours and body image [3,4], with personality factors such as neuroticism playing a key role in their development and maintenance [5,6]. Higher levels of neuroticism have been linked to greater DE symptoms [7,8], body dissatisfaction [9,10], and self-esteem [11,12] in community and inpatient and outpatient ED populations. Several studies have demonstrated that self-esteem and body dissatisfaction function as mediating variables in the association between neuroticism and DE symptoms [13,14,15]. However, these associations remain unexplored in individuals with MS, despite the potential impact of MS-related physical and psychological changes on body image concerns and eating behaviours [16]. The present study therefore aimed to examine the relationships between neuroticism, self-esteem, body dissatisfaction and DE symptoms in individuals with MS.
Eating Disorder Symptoms and Multiple Sclerosis
Although EDs have been widely studied in the general population [17] and among individuals with psychiatric disorders [18], research on body image concerns and DE symptoms in chronic illnesses such as MS remains limited. Chronic conditions that impact physical appearance and mobility have been linked to heightened vulnerability to body dissatisfaction and DE [19,20,21]. Emerging evidence suggests that DE may be more prevalent in individuals with chronic illnesses due to disease-related changes and their psychosocial consequences. For instance, conditions such as rheumatoid arthritis [19], diabetes [21], and cancer [20] have been associated with significant body image concerns, with studies indicating that DE behaviours in these populations may worsen over time.
Individuals with MS often experience symptoms such as fatigue, muscle weakness, motor impairments, and cognitive deficits, which can significantly impact their quality of life [1]. Beyond the physical manifestations of the disease, psychological factors such as depression, anxiety, and reduced self-esteem are highly prevalent in this population [22,23,24]. Emerging research suggests that body image disturbances and DE behaviours may also be concerns for individuals with MS, though this area remains underexplored [2,25,26,27]. It is possible that the presence of MS-related physical disabilities and weight fluctuations as well as obesity may contribute to concerns about body image, which in turn can influence eating behaviours. Corticosteroid treatments often prescribed for MS management are known to cause weight gain and changes in body composition, which may exacerbate body dissatisfaction and increase vulnerability to maladaptive eating behaviours [28]. Additionally, fatigue and mobility impairments may alter physical activity levels, leading to frustration with body changes and increased risk for DE patterns [29].
Research on the role of diet in the treatment of MS is also inconclusive, with variability in dietary recommendations. While some studies suggest that fat intake may worsen disease progression and vegetable consumption may be protective, a few meta-analyses indicated insufficient high-quality evidence to confirm the effectiveness of specific dietary interventions [30,31]. Such inconsistent findings may also partially cause body dissatisfaction and DE in several ways. First, the lack of clear dietary recommendations for MS may contribute to confusion and anxiety among patients, potentially leading to restrictive or DE behaviours to manage their symptoms. Patients may internalise messages about "good" and "bad" foods, increasing food-related distress and body dissatisfaction, particularly if weight gain or metabolic disorders associated with MS become a concern. Additionally, the emphasis on dietary control as a means of managing MS symptoms could heighten preoccupation with food and body image, further increasing the risk of DE patterns. Overall, the uncertainty surrounding dietary advice may leave patients vulnerable to misinformation, restrictive dieting, compensatory behaviours, or heightened body image concerns to exert control over their health.
Research on body image concerns in MS has also yielded mixed findings, highlighting the complexity of this issue [2,25,26,27]. Pfaffenberger et al. [27] found that individuals with MS reported greater concerns about physical deficits, poorer body appraisal, and more sexual difficulties compared to healthy controls, with notable gender-specific differences. This study established a foundational understanding of how MS-related physical changes may impact body image. Building on this, Bailey et al. [26] explored the broader sociocultural factors influencing body image in MS, emphasising the interplay between aging, disability, and societal beauty standards. Their findings suggest that body image concerns in MS are not only shaped by disease-related changes but also by external societal pressures. Further refining this understanding, Stevens et al. [2] examined body image dissatisfaction in MS and found that, while overall levels of body dissatisfaction were comparable to the general population, it was more pronounced in women and associated with higher body mass index (BMI), depression, and experiences of stigma. This study highlighted the need to consider individual differences, particularly in relation to psychological distress and weight-related concerns, when assessing body image in MS. In contrast, Reininghaus et al. [25] reported that MS patients experienced fewer sexual problems than normative body image concern values and maintained stable relationships, suggesting that body image concerns may not be universally heightened across all individuals with MS. These varying findings underscore the need for further research to clarify the conditions under which body image disturbances and DE emerge in MS.
The Role of Neuroticism in Eating Disorders in Individuals with Multiple Sclerosis
Neuroticism is a personality trait characterised by a heightened tendency to experience negative emotions such as anxiety, depression, and emotional instability [32]. Research has consistently demonstrated that neuroticism is a key risk factor for the development and maintenance of DE symptoms, as individuals high in neuroticism are more likely to engage in maladaptive coping mechanisms, including restrictive eating, binge eating, and purging behaviours [5]. A large body of literature has established a link between neuroticism and DE symptoms in community [7] and inpatient and outpatient ED populations [5].
Individuals with MS often also exhibit elevated levels of neuroticism compared to the general population, potentially due to the unpredictable and progressive nature of the disease [33,34]. The psychological distress associated with MS, including uncertainty about disease progression, functional limitations, and social isolation, may amplify the impact of neuroticism on maladaptive eating behaviours. Given that neuroticism is linked to heightened sensitivity to stress and negative self-perception [35,36], individuals with MS who score high on this trait may be particularly susceptible to developing low self-esteem, which in turn could lead to body dissatisfaction and DE behaviours. However, no studies have examined the role of neuroticism and its relationship with DE symptoms in individuals with MS, representing a significant gap in the literature.
The Mediating Role of Self-Esteem and Body Dissatisfaction
Self-esteem, defined as an individual's overall sense of self-worth, is an important psychological factor in the development of EDs [37]. Low self-esteem has been identified as a key contributor to the onset and maintenance of DE symptoms, as individuals with poor self-worth are more likely to engage in maladaptive eating behaviours as a means of coping with negative emotions [38,39,40]. Research suggests that self-esteem plays a crucial mediating role in the relationship between body dissatisfaction and DE, with additional influences from depression and negative affect. Brechan et al. [39] found that the effect of body dissatisfaction on DE was fully mediated by self-esteem and depression. Their findings indicate that self-esteem and depression are more proximal factors in predicting DE than body dissatisfaction itself. Similarly, Cruz-Sáez et al. [40] demonstrated that self-esteem and negative affect sequentially mediated the relationship between body dissatisfaction and DE, with self-esteem serving as a particularly strong mediator among boys. Additionally, Murray et al. [38] provided longitudinal evidence that stress indirectly predicted body dissatisfaction through reductions in self-esteem and heightened body image importance, further reinforcing the role of self-esteem as a central mechanism linking negative emotional states to body dissatisfaction. Collectively, these studies suggest that interventions targeting self-esteem may be particularly effective in mitigating the impact of body dissatisfaction on DE, potentially offering more sustainable benefits than interventions focused solely on body image concerns.
Previous research has shown that individuals with MS also report lower self-esteem compared to controls [41], and this reduction in self-worth is often linked to increased depressive symptoms and poorer quality of life [42]. Given the well-established relationship between low self-esteem and DE [38,39,40], it is plausible that individuals with MS who experience diminished self-esteem may be at heightened risk for engaging in DE behaviours as a means of coping with perceived inadequacies. However, no studies have directly investigated the role of self-esteem in mediating the relationship between neuroticism and DE in MS, marking another significant gap in the literature. The present study seeks to fill this gap by investigating whether neuroticism contributes to DE symptoms through self-esteem and body dissatisfaction, thereby offering a more comprehensive understanding of the psychological mechanisms involved.
The Present Study
Existing studies have found that lower levels of self-esteem and higher levels of body dissatisfaction significantly mediate the relationship between personality, namely neuroticism, and DE in individuals with EDs [13,14,15]. However, these relationships have been unexplored in individuals with MS. Hence, the aim of the current study was to investigate the mediating roles of self-esteem and body dissatisfaction in the relationship between neuroticism and DE in individuals with MS. Specifically, as illustrated in Figure 1, we proposed that neuroticism would be significantly associated with lower self-esteem, which in turn would be linked to increased body dissatisfaction, ultimately leading to more severe DE in people with MS (see Figure 1).
2. Materials and Methods
Participants and Procedure
Participants were recruited from 2019 to 2023 as part of a research program examining transdiagnostic psychological mechanisms underlying depression, anxiety, and EDs in community, medically ill, and psychological help-seeking populations. Participants were recruited using online advertisements on peer support Facebook groups, websites, and forums; newsletters of relevant organisations and support services (e.g., MS Australia); and advertisements posted on the Royal Melbourne Hospital noticeboards. Interested participants were invited to complete an online survey. All participants provided informed consent to participate and for their data to be used for publication purposes. This study was approved by [blinded for review]. Data from a total of 275 participants with MS (Mage = 43.03 years, 79.3% female, 68.3% relapsing-remitting MS) was included in the final analysis.
Materials
Sociodemographic and Clinical Characteristics
Data on age, gender, ethnicity, country of residence, highest education level, employment and marital status were collected. Participants were asked to self-report whether they had received a physician-confirmed diagnosis of MS and prior or current diagnosis of depression, anxiety, and EDs. Participants were also asked to report disease-related characteristics, including MS type, duration since MS diagnosis and onset, MS relapse, and whether they were taking disease-modifying medication. Ambulation level was assessed using the Self-Reported Disability Status Scale (SRDSS) [43]. The SRDSS is a self-report proxy measure used to estimate categories of the Expanded Disability Status Scale (EDSS), which is the most commonly used measure of disability in MS [44]. Responses to three mobility-related questions on the SRDSS result in three outcomes: SRDSS < 3.5, 4 to 6.5, and > 7, with higher scores indicating greater level of ambulation difficulty. Participants also self-reported their height (centimetres or inches) and weight (kilograms or pounds), based on which BMI was calculated.
Psychological Variables
Neuroticism was assessed using the 44-item Big Five Inventory (BFI) [45]. The BFI-Neuroticism subscale consists of eight items and measures a predisposition towards negative emotions (e.g., depression, anxiety, stress, anger) and emotional instability [46]. Participants responded to statements (e.g., ‘I can be moody’, ‘I am someone who is emotionally stable, not easily upset’) on a five-point Likert scale ranging from 1 (disagree strongly) to 5 (agree strongly). Three items were reverse scored. A total score was created by summing all items, with higher scores indicating higher levels of neuroticism. The BFI Neuroticism subscale demonstrated good internal reliability in the present sample (Cronbach’s α = .82).
Self-esteem was measured using the 10-item Rosenberg Self-esteem Scale (RSES-10) [47]. Participants rated the degree to which they agreed with statements (e.g., ‘I feel that I have a number of good qualities’) on a four-point Likert scale ranging from 0 (strongly disagree) to 3 (strongly agree). Five items were reverse scored, so that higher total score correspond to higher self-esteem. Internal reliability of the RSE scale was good in the current sample (α = .87).
Body dissatisfaction was examined using the eight-item Body Shape Questionnaire (BSQ-8) [48]. Items reflect concerns about body shape and body dissatisfaction and are rated on a scale from 1 (never) to 6 (always). Higher scores indicate higher body dissatisfaction. In the current sample, the BSQ-8 was found to have excellent reliability (α = .90).
DE symptoms were assessed using the 26-item Eating Attitudes Test (EAT-26) [49]. Participants rated the frequency of attitudes, feelings, and behaviours related to food and eating (e.g., ‘I vomit after I have eaten’, ‘I am preoccupied with a desire to be thinner’) on a six-point Likert scale ranging from 0 (never, sometimes, rarely) to 3 (always). The EAT-26 items form three subscales, including dieting, bulimia and food preoccupation, and oral control. In the current study, the total EAT-26 score was used by summing all items. A total score of 20 or greater indicates a probable ED and requires further diagnostic investigation from a qualified professional [50]. A total score below 20 indicates a low level of concern about dieting, body weight, or problematic eating behaviours. Internal reliability of the total EAT-26 was excellent in the present sample (α = .94).
Statistical Analyses
Data Inspection
All analyses were conducted in R [51]. A total of 309 participants with MS accessed the online survey with a final sample of 275 participants with MS who completed the questionnaires. All primary variables included in the model were within acceptable limits for skewness and kurtosis (i.e., + 1). The percentage of missing data ranged from 0% to 2.9% across variables, with 101 incomplete cases. Following recommended practices [52,53], missing data was handled using multiple imputation with predictive-mean matching (100 datasets and 20 iterations) via the mice package [54]. Model parameters were estimated in each imputed dataset separately and combined using Rubin’s rule [55]. Sensitivity analysis with complete cases suggested that imputation did not alter path coefficients nor significance (see Appendix A). There was no evidence of multicollinearity between variables according to the variance inflation factor (VIF) and Pearson bivariate correlations.
Serial Mediation Model
The serial mediation model was fitted using the lavaan [56], lavaan.mi [57], and semTools [58] packages. We specified a path model with no latent construct using sum scores of the BFI-Neuroticism, RSES-10, BSQ-8, and the EAT-26. Therefore, model fit indices were not computed. R-squares for the mediating and dependent variables were reported to assess the robustness of the results. Monte-Carlo confidence intervals based on 50,000 replications were constructed to test the statistical significance of hypothesised pathways. Potential demographic and disease-related correlates of DE in both ED and MS samples (i.e., age [59], sex [14], BMI [2], and level of ambulation [60]) were included as covariates. Reported path coefficients are unstandardised. To further explore the single and serial mediating effects of self-esteem and body dissatisfaction, we also compared specific indirect pathways. The current sample size has been considered adequate for a serial mediation analysis using a path modelling approach [61]. Further details of the planned statistical analyses and sample size justification can be found in our registration document: https://osf.io/bamrv.
3. Results
Sample Characteristics
Table 1 presents sociodemographic and MS characteristics of the included sample (N = 275). Most participants identified as female (79.27%), of Anglo-Celtic background (76.73%), and reported a diagnosis of relapsing-remitting MS (67.27%). The mean age was 43.03 years (SD = 12.88), with ages ranging from 19 to 81 years. Participants reported a mean duration of 8.43 years (SD = 8.13) since MS diagnosis and 12.15 years (SD = 11.11) since MS onset. The mean BMI was 29.13 kg/m2 (SD = 11.38).
Previous and current mental health diagnoses are summarised in Table 2. Approximately 21% reported a lifetime diagnosis of ED (N = 58/275), with anorexia nervosa being the most common. Among participants diagnosed with ED, 67.24% (N = 39/275) reported having a current diagnosis. The total EAT-26 score indicated that 76 (27.64%) participants were at risk of an ED (provided a score of > 20). In addition, a small proportion of participants reported having comorbid ED and depression (N = 39, 14.18%), ED and anxiety (N = 39, 14.18%), or ED, depression, and anxiety (N = 33, 12.00%). Nearly half of participants (N = 132, 48.00%) reported currently taking anti-depressant or anti-anxiety medication.
Descriptive Statistics and Correlations
Means, standard deviations, and correlations between continuous study variables are reported in Table 3. All variables in the mediation model were significantly correlated.
Serial Mediation Model
A serial mediation analysis was conducted to examine the relationship between neuroticism, DE, self-esteem, and body dissatisfaction. Age, gender, BMI, and level of ambulation were included as covariates. Figure 2 presents the pooled unstandardised path coefficients of the hypothesised model across 100 multiply imputed datasets.
Table 4 reports standardised path coefficients and comparisons of specific mediation effects. The total indirect effect of neuroticism on DE symptoms was significant, β = 0.40, SE = 0.08, 95% CI: [0.25, 0.57]. The direct effect of neuroticism on DE symptoms accounting for self-esteem and body dissatisfaction was also significant, β = -0.26, SE = 0.10, 95% CI: [-0.46, -0.05]. However, the total model effect (β = 0.15, SE = 0.11, 95% CI: [-0.07, 0.37]) was not significant. Of note, there was evidence for a serial mediation effect of neuroticism via self-esteem and body dissatisfaction, β = 0.12, SE = 0.04, 95% CI: [0.06, 0.20]. The indirect effects of neuroticism on DE symptoms through self-esteem (β = 0.10, SE = 0.05, 95% CI: [0.01, 0.20]) and body dissatisfaction (β = 0.19, SE = 0.06, 95% CI: [0.06, 0.33]) were significant. Pairwise comparisons indicated no significant differences between the single and serial mediating pathways. The full model accounted for accounted for 43.0% of the variance in DE symptoms. The proportion of variance accounted for in self-esteem and body dissatisfaction were 34.6% and 26.4%, respectively.
4. Discussion
In the current study we assessed whether neuroticism would be significantly associated with lower self-esteem, which in turn would be linked to increased body dissatisfaction, ultimately leading to more severe DE symptoms. The hypothesis that self-esteem and body dissatisfaction play a mediating role in the relationship between neuroticism and DE symptoms in individuals with MS was supported. Our results also showed significant relationships between self-esteem and body dissatisfaction, and both factors were significantly related to DE symptoms in the current MS sample. The hypothesized serial pathway (neuroticism → self-esteem → body dissatisfaction → DE symptoms) was significant, suggesting that the interplay between these two factors is relevant in understanding how neuroticism is linked to DE symptoms.
Consistent with research that has demonstrated significant relationships between neuroticism and lower self-esteem [13,15,16] and neuroticism and increased body dissatisfaction [14] in community and clinical samples with EDs, our results show that these relationships are also significant in people with MS. More specifically, individuals with MS who reported higher levels of neuroticism also experienced lower self-esteem, which may increase body dissatisfaction and, in turn, more DE symptoms. The present study builds upon previous findings by demonstrating that neuroticism is associated with DE symptoms in MS [7,8], and that self-esteem and body dissatisfaction are important factors to consider in understanding DE symptoms in MS [9,10,11,12]. The sequential effects of self-esteem and body dissatisfaction further indicate that low self-esteem is associated with DE symptoms through more body image concerns in people with MS. However, the proposed model only provides one plausible pathway through which neuroticism, self-esteem, body dissatisfaction, and DE symptoms are related. Future longitudinal studies may utilise this model to determine how neuroticism facilitates adverse DE outcomes in people with MS over time.
Interestingly, our findings showed a suppression effect of self-esteem and body dissatisfaction on DE symptoms. That is, while the total indirect effect of neuroticism on DE symptoms was positive, the negative direct effect indicates that higher neuroticism was associated with fewer ED symptoms when holding self-esteem and body dissatisfaction constant. This was likely due to confounding factors that were not accounted for in our model, such as other personality traits (e.g., conscientiousness [6], extraversion [8], openness to experience [62], and perfectionism [6]) and cognitive vulnerabilities (e.g., intolerance of uncertainty [63], emotion regulation [64], and distress tolerance [65]) that have been robustly linked to both neuroticism and EDs. However, it is also possible that the relationship between neuroticism and DE in our MS sample differs from that observed in other populations. Prior research has supported the existence of ‘healthy neuroticism’ [66,67], where individuals with higher levels of neuroticism and conscientiousness report better health outcomes due to increased body vigilance [68], greater likelihood of seeking medical attention [69], and less engagement in maladaptive health behaviours [69,70,71]. For instance, at high levels of conscientiousness, high neuroticism has been associated with lower odds of smoking [70], problematic alcohol consumption [71], lower levels of inflammatory biomarkers [72], and higher levels of physical activity [69,73]. Similarly, recent findings from a community sample of 712 adults suggest that high levels of trait neuroticism and conscientiousness reliably predicted reduced DE behaviours such as less disinhibited eating and hunger and increased self-regulatory eating restraint [74]. In addition, evidence from the broader ED literature has identified mixed associations between neuroticism and DE, particularly when specific facets of neuroticism and specific DE behaviours are considered [7]. For example, the impulsiveness facet of neuroticism reflecting low self-control has been positively associated with binge or emotional eating, compensatory behaviours, and global eating pathology but negatively associated with dietary restraint [7]. Other facets of neuroticism demonstrated a consistent positive association with DE behaviours [7]. Together, these findings suggest that the neuroticism-ED link in MS is complex and nuanced, and results from our study should be taken as the first attempt to explore this relationship. As conscientiousness was not examined in our study, the potential presence and prevalence of healthy neuroticism in people with MS and its relationship to DE behaviours warrants further examination. Future studies may also adopt a facet-level approach to measuring neuroticism and distinguishing between specific DE behaviours associated with different ED phenotypes, to further elucidate the effect of neuroticism on DE symptoms in MS.
The current study found that 21% of participants reported a diagnosis of an ED, with anorexia nervosa and bulimia nervosa being the most common. This is higher than the prevalence rates of EDs identified in non-MS samples with 12-month and lifetime rates being up to 2.58% in females [17]. Relatedly, over half of our sample (53.45%) reported a co-morbid depressive disorder, with major depressive disorder being the most common, and nearly half of the sample (47.27%) reported a co-morbid anxiety disorder, with GAD being the most common disorder. Relatedly, nearly half of the current sample (48%) also indicated that they are taking anti-depressant or anti-anxiety medication. This is consistent with previous research that has found high rates of depression and anxiety in individuals with MS [24].
Clinical Implications
Given the study’s findings that self-esteem and body dissatisfaction are significantly related to DE symptoms in individuals with MS, these factors should be considered in models of DE in individuals with MS. Consideration should also be given in integrating routine screening for DE in clinical settings. A practical first step would be to employ additional validated screening tools such as the SCOFF questionnaire [75], which is a five-item self-report measure that can quickly identify individuals at risk of eating disorders. In addition, incorporating brief assessments of self-esteem and body dissatisfaction, such as the measures included in the current study, may help identify psychosocial vulnerabilities that contribute to DE symptoms.
Findings suggest that preventive interventions and psychological support for individuals with MS should not only address mood and physical function but also self-image and eating behaviours. Cognitive-behavioural approaches tailored to body image concerns, self-worth, and coping strategies related to disease progression and physical changes of MS (e.g., [76,77,78]) may be beneficial. Psychoeducation and mindfulness-based interventions targeting body acceptance and self-compassion [79,80,81] may also help reduce the risk of DE symptoms in those with MS. Importantly, interdisciplinary care involving neurologists, psychologists, dietitians, and rehabilitation specialists [82] can foster early detection and a more holistic approach to support individuals with MS who may be vulnerable to DE.
Finally, mental health professionals should also consider screening for co-occurring depressive and anxiety symptoms, given the high prevalence of these symptoms in the current MS sample. Targeted interventions that address this comorbid presentation are crucial, as the combination of DE [83], body dissatisfaction [78], low self-esteem [23], and affective symptoms [84] may compound distress and interfere with disease management and quality of life in those affected by MS. Multimodal psychological approaches that integrate mood regulation, body image work, and self-esteem enhancement may be particularly effective in supporting individuals with MS who present with overlapping challenges.
Limitations and Future Directions
There were several limitations to the current study. Firstly, the serial mediation model was examined using cross-sectional data. It is recommended that future studies employ a longitudinal design, such as cross-lagged panel models, to facilitate accurate inferences about the presence, strength, and direction of causal relationships [85], thus determining precise intervention targets for body image concerns, low self-esteem and DE symptoms in MS. Secondly, the current study used self-report measures for symptoms and diagnoses of depression, anxiety, and EDs, which may not capture symptomatology as accurately relative to structured clinical interviews undertaken by a mental health professional. Thirdly, future research would benefit from replicating the current associations in a larger longitudinal sample and using latent variable models to account for measurement error. Such an approach would provide a more comprehensive representation of the relationships between variables and increase the robustness of findings. Fourthly, the study did not differentiate between specific DE symptoms. As a result, it remains unclear whether individuals with MS were more likely to engage in restrictive eating, binge eating, or compensatory behaviours such as purging. Future studies should aim to assess specific DE symptom profiles to better understand risk patterns and to tailor interventions accordingly. Finally, the study included individuals with different types of multiple sclerosis (e.g., relapsing-remitting, primary progressive), which were statistically controlled for in the analyses. However, grouping these subtypes may mask meaningful differences in psychological or behavioural outcomes. Future research should explore whether the observed relationships vary across MS subtypes.
5. Conclusions
Despite these limitations, this study represents the first attempt to explore neuroticism, self-esteem, and body dissatisfaction as correlates of DE symptoms in a sample of people with MS. Existing mediating relationships of self-esteem and body dissatisfaction in the relationship between neuroticism and DE symptoms identified in community and ED samples appear to extend to people with MS. Our findings suggest that self-esteem and body dissatisfaction need to be considered in models explaining the development and maintenance of EDs in individuals with MS. Targeting self-esteem and body dissatisfaction may be relevant for treating and preventing DE symptoms in individuals with MS who have high levels of neuroticism.
Author Contributions
Conceptualization, LK, IK Methodology, LK IK; Software, LD; Validation, LK, IK, LD.; Formal Analysis, LD; Investigation, LK, IK, LD; Resources, LK; Data Curation, LK, LD; Writing – Original Draft Preparation, LK, IK, LD; Writing – Review & Editing, LK, IK, LD; Supervision, LK, IK; Project Administration, LK; Funding Acquisition, LK. All authors agreed to submitted version of the manuscript.
Funding
This research was partly funded by a Melbourne School of Psychological Sciences research incentives grant.
Institutional Review Board Statement
The study was approved by the Ethics Committee of The University of Melbourne (HREC Project number: 2023-12495-37995-10 and date of approval: 21/03/2019).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
De-identified data related to the results of this study can be requested from the corresponding author upon reasonable request. A data sharing agreement will be developed with the corresponding author and researchers.
Acknowledgments
We thank all participants who took part in this research.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| MS | Multiple sclerosis |
| ED | Eating disorder |
| DE | Disordered eating |
| BFI | Big Five Inventory |
| RSES | Rosenberg Self-esteem Scale |
| BSQ | Body Shape Questionnaire |
| EAT-26 | Eating Attitudes Test |
Appendix A

Table A1.
Standardised and unstandardised path coefficients of the serial mediation model controlling for age, gender, BMI, and ambulation level (complete case analysis).
Table A1.
Standardised and unstandardised path coefficients of the serial mediation model controlling for age, gender, BMI, and ambulation level (complete case analysis).
| Model pathway | β | SE | z | p | LL 95% CI | UL 95% CI |
| Neuroticism → Self-esteem (a1) | -0.42 (-0.46) | 0.06 | -7.17 | < .001 | -0.54 | -0.31 |
| Neuroticism → Body dissatisfaction (a2) | 0.23 (0.15) | 0.12 | 1.98 | .048 | 0.00 | 0.45 |
| Self-esteem → ED symptoms (b1) | -0.27 (-0.14) | 0.13 | -2.00 | .046 | -0.53 | -0.01 |
| Body dissatisfaction → ED symptoms (b2) | 0.68 (0.59) | 0.08 | 9.05 | < .001 | 0.53 | 0.82 |
| Self-esteem → Body dissatisfaction (d) | -0.44 (-0.27) | 0.13 | -3.36 | .001 | -0.70 | -0.18 |
| Total model effect | 0.16 (0.09) | 0.13 | 1.29 | .198 | -0.09 | 0.41 |
| Direct effect (c’) | -0.23 (-0.13) | 0.12 | -2.00 | .045 | -0.45 | -0.00 |
| Total indirect effect | 0.39 (0.23) | 0.10 | 4.12 | < .001 | 0.21 | 0.58 |
| Neuroticism → Self-esteem → ED symptoms (ind1) | 0.11 (0.07) | 0.06 | 1.92 | .054 | 0.00 | 0.23 |
| Neuroticism → Body dissatisfaction → ED symptoms (ind2) | 0.15 (0.09) | 0.08 | 1.94 | .053 | 0.00 | 0.32 |
| Neuroticism → Self-esteem → Body dissatisfaction → ED symptoms (ind3) | 0.13 (0.07) | 0.04 | 2.89 | .053 | 0.05 | 0.22 |
| Pairwise comparisons of indirect effects | ||||||
| Ind1 – Ind2 | -0.04 (-0.03) | 0.10 | -0.42 | .673 | -0.25 | 0.16 |
| Ind1 – Ind3 | -0.01 (-0.01) | 0.07 | -0.19 | .851 | -0.16 | 0.13 |
| Ind2 – Ind3 | 0.03 (0.02) | 0.10 | 0.28 | .777 | -0.18 | 0.23 |
Note. N = 174. Significant pathways are noted in bold (95% confidence interval does not cross zero). 95% confidence intervals around estimates of unstandardised effects were obtained from Monte-Carlo simulations with 50,000 replications. Unstandardised effects are shown outside parentheses. Standardised effects are shown inside parentheses. The full model accounted for 45.5% of variance in ED symptoms. The proportion of variance accounted for in self-esteem and body dissatisfaction were 35.0% and 25.5%, respectively.
References
- Ward, M.; Goldman, M.D. Epidemiology and pathophysiology of multiple sclerosis. Continuum (Minneap Minn) 2022, 28, 988–1005. [Google Scholar] [CrossRef] [PubMed]
- Stevens, S.D.; Thompson, N.R.; Sullivan, A.B. Prevalence and correlates of body image dissatisfaction in patients with multiple sclerosis. Int J MS Care 2019, 21, 207–213. [Google Scholar] [CrossRef]
- Glasofer, D.R.; Attia, E.; Pike, K.M. Eating disorders. In Psychopathology: From science to clinical practice, Castonguay, L.G., Oltmanns, T.F., Eds.; The Guilford Press: 2013; pp. 198-240.
- Crone, C.; Fochtmann, L.J.; Attia, E.; Boland, R.; Escobar, J.; Fornari, V.; Golden, N.; Guarda, A.; Jackson-Triche, M.; Manzo, L.; et al. The american psychiatric association practice guideline for the treatment of patients with eating disorders. Am J Psychiatry 2023, 180, 167–171. [Google Scholar] [CrossRef]
- Cassin, S.E.; von Ranson, K.M. Personality and eating disorders: A decade in review. Clin Psychol Rev 2005, 25, 895–916. [Google Scholar] [CrossRef] [PubMed]
- Farstad, S.M.; McGeown, L.M.; von Ranson, K.M. Eating disorders and personality, 2004–2016: A systematic review and meta-analysis. Clinical Psychology Review 2016, 46, 91–105. [Google Scholar] [CrossRef]
- Gilmartin, T.; Gurvich, C.; Sharp, G. The relationship between disordered eating behaviour and the five factor model personality dimensions: A systematic review. J Clin Psychol 2022, 78, 1657–1670. [Google Scholar] [CrossRef]
- Miller, J.L.; Schmidt, L.A.; Vaillancourt, T.; McDougall, P.; Laliberte, M. Neuroticism and introversion: A risky combination for disordered eating among a non-clinical sample of undergraduate women. Eat Behav 2006, 7, 69–78. [Google Scholar] [CrossRef]
- Allen, M.S.; Robson, D.A. Personality and body dissatisfaction: An updated systematic review with meta-analysis. Body Image 2020, 33, 77–89. [Google Scholar] [CrossRef] [PubMed]
- Swami, V.; Taylor, R.; Carvalho, C. Body dissatisfaction assessed by the photographic figure rating scale is associated with sociocultural, personality, and media influences. Scand J Psychol 2011, 52, 57–63. [Google Scholar] [CrossRef]
- Clague, C.A.; Prnjak, K.; Mitchison, D. "I don't want them to judge me": Separating out the role of fear of negative evaluation, neuroticism, and low self-esteem in eating disorders. Eat Behav 2023, 49, 101708. [Google Scholar] [CrossRef]
- Jones, H.; McIntosh, V.V.W.; Britt, E.; Carter, J.D.; Jordan, J.; Bulik, C.M. The effect of temperament and character on body dissatisfaction in women with bulimia nervosa: The role of low self-esteem and depression. Eur Eat Disord Rev 2022, 30, 388–400. [Google Scholar] [CrossRef] [PubMed]
- Skorek, M.; Song, A.V.; Dunham, Y. Self-esteem as a mediator between personality traits and body esteem: Path analyses across gender and race/ethnicity. PLoS One 2014, 9, e112086. [Google Scholar] [CrossRef] [PubMed]
- MacNeill, L.P.; Best, L.A.; Davis, L.L. The role of personality in body image dissatisfaction and disordered eating: Discrepancies between men and women. J Eat Disord 2017, 5, 44. [Google Scholar] [CrossRef]
- Cervera, S.; Lahortiga, F.; Martinez-Gonzalez, M.A.; Gual, P.; de Irala-Estevez, J.; Alonso, Y. Neuroticism and low self-esteem as risk factors for incident eating disorders in a prospective cohort study. Int J Eat Disord 2003, 33, 271–280. [Google Scholar] [CrossRef]
- Krauss, S.; Dapp, L.C.; Orth, U. The link between low self-esteem and eating disorders: A meta-analysis of longitudinal studies. Clinical Psychological Science 2023, 11, 1141–1158. [Google Scholar] [CrossRef]
- Qian, J.; Wu, Y.; Liu, F.; Zhu, Y.; Jin, H.; Zhang, H.; Wan, Y.; Li, C.; Yu, D. An update on the prevalence of eating disorders in the general population: A systematic review and meta-analysis. Eat Weight Disord 2022, 27, 415–428. [Google Scholar] [CrossRef]
- Galmiche, M.; Dechelotte, P.; Lambert, G.; Tavolacci, M.P. Prevalence of eating disorders over the 2000-2018 period: A systematic literature review. Am J Clin Nutr 2019, 109, 1402–1413. [Google Scholar] [CrossRef] [PubMed]
- Leon, L.; Clemente, D.; Heredia, C.; Abasolo, L. Self-esteem, self-concept, and body image of young people with rheumatic and musculoskeletal diseases: A systematic literature review. Semin Arthritis Rheum 2024, 68, 152486. [Google Scholar] [CrossRef]
- Bahrami, M.; Mohamadirizi, M.; Mohamadirizi, S.; Hosseini, S.A. Evaluation of body image in cancer patients and its association with clinical variables. J Educ Health Promot 2017, 6, 81. [Google Scholar] [CrossRef]
- Troncone, A.; Cascella, C.; Chianese, A.; Zanfardino, A.; Piscopo, A.; Borriello, A.; Casaburo, F.; Del Giudice, E.M.; Iafusco, D. Body image problems and disordered eating behaviors in italian adolescents with and without type 1 diabetes: An examination with a gender-specific body image measure. Front Psychol 2020, 11, 556520. [Google Scholar] [CrossRef]
- Gascoyne, C.R.; Simpson, S., Jr.; Chen, J.; van der Mei, I.; Marck, C.H. Modifiable factors associated with depression and anxiety in multiple sclerosis. Acta Neurol Scand 2019, 140, 204–211. [Google Scholar] [CrossRef]
- Mikula, P.; Timkova, V.; Fedicova, M.; Szilasiova, J.; Nagyova, I. Self-management, self-esteem and their associations with psychological well-being in people with multiple sclerosis. Mult Scler Relat Disord 2021, 53, 103069. [Google Scholar] [CrossRef] [PubMed]
- Kiropoulos, L.A.; Kilpatrick, T.; Holmes, A.; Threader, J. A pilot randomized controlled trial of a tailored cognitive behavioural therapy based intervention for depressive symptoms in those newly diagnosed with multiple sclerosis. BMC Psychiatry 2016, 16, 435. [Google Scholar] [CrossRef]
- Reininghaus, E.; Reininghaus, B.; Fitz, W.; Hecht, K.; Bonelli, R.M. Sexual behavior, body image, and partnership in chronic illness: A comparison of huntington's disease and multiple sclerosis. J Nerv Ment Dis 2012, 200, 716–720. [Google Scholar] [CrossRef] [PubMed]
- Bailey, K.A.; Dagenais, M.; Gammage, K.L. Is a picture worth a thousand words? Using photo-elicitation to study body image in middle-to-older age women with and without multiple sclerosis. Qual Health Res 2021, 31, 1542–1554. [Google Scholar] [CrossRef]
- Pfaffenberger, N.; Gutweniger, S.; Kopp, M.; Seeber, B.; Sturz, K.; Berger, T.; Gunther, V. Impaired body image in patients with multiple sclerosis. Acta Neurol Scand 2011, 124, 165–170. [Google Scholar] [CrossRef] [PubMed]
- Matusik, E.; Durmala, J.; Ksciuk, B.; Matusik, P. Body composition in multiple sclerosis patients and its relationship to the disability level, disease duration and glucocorticoid therapy. Nutrients 2022, 14. [Google Scholar] [CrossRef]
- Taul-Madsen, L.; Connolly, L.; Dennett, R.; Freeman, J.; Dalgas, U.; Hvid, L.G. Is aerobic or resistance training the most effective exercise modality for improving lower extremity physical function and perceived fatigue in people with multiple sclerosis? A systematic review and meta-analysis. Arch Phys Med Rehabil 2021, 102, 2032–2048. [Google Scholar] [CrossRef]
- Jagannath, V.A.; Filippini, G.; Di Pietrantonj, C.; Asokan, G.V.; Robak, E.W.; Whamond, L.; Robinson, S.A. Vitamin d for the management of multiple sclerosis. Cochrane Database Syst Rev 2018, 9, CD008422. [Google Scholar] [CrossRef]
- Parks, N.E.; Jackson-Tarlton, C.S.; Vacchi, L.; Merdad, R.; Johnston, B.C. Dietary interventions for multiple sclerosis-related outcomes. Cochrane Database Syst Rev 2020, 5, CD004192. [Google Scholar] [CrossRef]
- McCrae, R.R.; Costa, P.T. The neo personality inventory: Using the five-factor modei in counseling. Journal of Counseling & Development 2011, 69, 367–372. [Google Scholar] [CrossRef]
- Roy, S.; Drake, A.S.; Eizaguirre, M.B.; Zivadinov, R.; Weinstock-Guttman, B.; Chapman, B.P.; Benedict, R.H. Trait neuroticism, extraversion, and conscientiousness in multiple sclerosis: Link to cognitive impairment? Mult Scler 2018, 24, 205–213. [Google Scholar] [CrossRef]
- Maggio, M.G.; Cuzzola, M.F.; Latella, D.; Impellizzeri, F.; Todaro, A.; Rao, G.; Manuli, A.; Calabro, R.S. How personality traits affect functional outcomes in patients with multiple sclerosis: A scoping review on a poorly understood topic. Mult Scler Relat Disord 2020, 46, 102560. [Google Scholar] [CrossRef] [PubMed]
- Thomson, W. Depression, neuroticism, and the discrepancy between actual and ideal self-perception. Personality and Individual Differences 2016, 88, 219–224. [Google Scholar] [CrossRef]
- Uliaszek, A.A.; Zinbarg, R.E.; Mineka, S.; Craske, M.G.; Sutton, J.M.; Griffith, J.W.; Rose, R.; Waters, A.; Hammen, C. The role of neuroticism and extraversion in the stress-anxiety and stress-depression relationships. Anxiety Stress Coping 2010, 23, 363–381. [Google Scholar] [CrossRef]
- Fairburn, C.G.; Cooper, Z.; Shafran, R. Cognitive behaviour therapy for eating disorders: A "transdiagnostic" theory and treatment. Behav Res Ther 2003, 41, 509–528. [Google Scholar] [CrossRef] [PubMed]
- Murray, K.; Rieger, E.; Byrne, D. A longitudinal investigation of the mediating role of self-esteem and body importance in the relationship between stress and body dissatisfaction in adolescent females and males. Body Image 2013, 10, 544–551. [Google Scholar] [CrossRef]
- Brechan, I.; Kvalem, I.L. Relationship between body dissatisfaction and disordered eating: Mediating role of self-esteem and depression. Eat Behav 2015, 17, 49–58. [Google Scholar] [CrossRef]
- Cruz-Saez, S.; Pascual, A.; Wlodarczyk, A.; Echeburua, E. The effect of body dissatisfaction on disordered eating: The mediating role of self-esteem and negative affect in male and female adolescents. J Health Psychol 2020, 25, 1098–1108. [Google Scholar] [CrossRef]
- McCabe, M.P. Mood and self-esteem of persons with multiple sclerosis following an exacerbation. J Psychosom Res 2005, 59, 161–166. [Google Scholar] [CrossRef]
- Mikula, P.; Nagyova, I.; Krokavcova, M.; Vitkova, M.; Rosenberger, J.; Szilasiova, J.; Gdovinova, Z.; Stewart, R.E.; Groothoff, J.W.; van Dijk, J.P. Self-esteem, social participation, and quality of life in patients with multiple sclerosis. J Health Psychol 2017, 22, 984–992. [Google Scholar] [CrossRef] [PubMed]
- Kaufmann, M.; Salmen, A.; Barin, L.; Puhan, M.A.; Calabrese, P.; Kamm, C.P.; Gobbi, C.; Kuhle, J.; Manjaly, Z.M.; Ajdacic-Gross, V.; et al. Development and validation of the self-reported disability status scale (srdss) to estimate edss-categories. Mult Scler Relat Disord 2020, 42, 102148. [Google Scholar] [CrossRef]
- Kurtzke, J.F. Rating neurologic impairment in multiple sclerosis: An expanded disability status scale (edss). Neurology 1983, 33, 1444–1452. [Google Scholar] [CrossRef]
- John, O.P.; Srivastava, S. The big-five trait taxonomy: History, measurement, and theoretical perspectives. In Handbook of personality: Theory and research; Guilford Press: New York, 1999; Volume 2, pp. 102–138. [Google Scholar]
- Costa Mastrascusa, R.; de Oliveira Fenili Antunes, M.L.; de Albuquerque, N.S.; Virissimo, S.L.; Foletto Moura, M.; Vieira Marques Motta, B.; de Lara Machado, W.; Moret-Tatay, C.; Quarti Irigaray, T. Evaluating the complete (44-item), short (20-item) and ultra-short (10-item) versions of the big five inventory (bfi) in the brazilian population. Sci Rep 2023, 13, 7372. [Google Scholar] [CrossRef]
- Rosenberg, M. Rosenberg self-esteem scale (rses). Available online: https://www.apa.org/obesity-guideline/rosenberg-self-esteem.pdf (accessed on 3 January).
- Cooper, P.; Taylor, M.; Cooper, Z.; Fairburn, C.G. The development and validation of the body shape questionnaire. Int J Eat Disord 1987, 6, 485–494. [Google Scholar] [CrossRef]
- Garner, D.M.; Olmsted, M.P.; Bohr, Y.; Garfinkel, P.E. The eating attitudes test: Psychometric features and clinical correlates. Psychol Med 1982, 12, 871–878. [Google Scholar] [CrossRef]
- Papini, N.M.; Jung, M.; Cook, A.; Lopez, N.V.; Ptomey, L.T.; Herrmann, S.D.; Kang, M. Psychometric properties of the 26-item eating attitudes test (eat-26): An application of rasch analysis. J Eat Disord 2022, 10, 62. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A language and environment for statistical computing. 2024.
- Schoemann, A.M.; Moore, E.W.G.; Yagiz, G. How and why to follow best practices for testing mediation models with missing data. Int J Psychol 2025, 60, e13257. [Google Scholar] [CrossRef]
- Austin, P.C.; White, I.R.; Lee, D.S.; van Buuren, S. Missing data in clinical research: A tutorial on multiple imputation. Can J Cardiol 2021, 37, 1322–1331. [Google Scholar] [CrossRef]
- Buuren, S.v.; Groothuis-Oudshoorn, K. Mice: Multivariate imputation by chained equations in r. J Stat Softw 2011, 45. [Google Scholar] [CrossRef]
- Rubin, D.B. Multiple imputation for nonresponse in surveys; John Wiley & Sons, Inc.: 1987.
- Rosseel, Y. Lavaan: An r package for structural equation modeling. J Stat Softw 2012, 48. [Google Scholar] [CrossRef]
- Jorgensen, T. Lavaan.Mi: Fit structural equation models to multiply imputed data. Available online: https://CRAN.R-project.org/package=lavaan.
- Jorgensen, T.; Pornprasertmanit, S.; Schoemann, A.M.; Rosseel, Y. Semtools: Useful tools for structural equation modeling. Available online: https://CRAN.R-project.org/package=semTools (accessed on 15 March).
- Rohde, P.; Stice, E.; Shaw, H.; Gau, J.M.; Ohls, O.C. Age effects in eating disorder baseline risk factors and prevention intervention effects. Int J Eat Disord 2017, 50, 1273–1280. [Google Scholar] [CrossRef]
- Lo Buono, V.; Bonanno, L.; Corallo, F.; Cardile, D.; D'Aleo, G.; Rifici, C.; Sessa, E.; Quartarone, A.; De Cola, M.C. The relationship between body image, disability and mental health in patients with multiple sclerosis. J Clin Med 2023, 12. [Google Scholar] [CrossRef] [PubMed]
- Sim, M.; Kim, S.Y.; Suh, Y. Sample size requirements for simple and complex mediation models. Educ Psychol Meas 2022, 82, 76–106. [Google Scholar] [CrossRef]
- Claes, L.; Vandereycken, W.; Luyten, P.; Soenens, B.; Pieters, G.; Vertommen, H. Personality prototypes in eating disorders based on the big five model. J Pers Disord 2006, 20, 401–416. [Google Scholar] [CrossRef]
- Clarke, E.; Kiropoulos, L.A. Mediating the relationship between neuroticism and depressive, anxiety and eating disorder symptoms: The role of intolerance of uncertainty and cognitive flexibility. Journal of Affective Disorders Reports 2021, 4. [Google Scholar] [CrossRef]
- Dingemans, A.; Danner, U.; Parks, M. Emotion regulation in binge eating disorder: A review. Nutrients 2017, 9. [Google Scholar] [CrossRef]
- Mattingley, S.; Youssef, G.J.; Manning, V.; Graeme, L.; Hall, K. Distress tolerance across substance use, eating, and borderline personality disorders: A meta-analysis. J Affect Disord 2022, 300, 492–504. [Google Scholar] [CrossRef]
- Friedman, H.S. Long-term relations of personality and health: Dynamisms, mechanisms, tropisms. J Pers 2000, 68, 1089–1107. [Google Scholar] [CrossRef]
- Friedman, H.S. Neuroticism and health as individuals age. Personal Disord 2019, 10, 25–32. [Google Scholar] [CrossRef]
- Weston, S.J.; Jackson, J.J. The role of vigilance in the relationship between neuroticism and health: A registered report. J Res Pers 2018, 73, 27–34. [Google Scholar] [CrossRef]
- Graham, E.K.; Weston, S.J.; Turiano, N.A.; Aschwanden, D.; Booth, T.; Harrison, F.; James, B.D.; Lewis, N.A.; Makkar, S.R.; Mueller, S.; et al. Is healthy neuroticism associated with health behaviors? A coordinated integrative data analysis. Collabra Psychol 2020, 6. [Google Scholar] [CrossRef]
- Weston, S.J.; Jackson, J.J. Identification of the healthy neurotic: Personality traits predict smoking after disease onset. Journal of Research in Personality 2015, 54, 61–69. [Google Scholar] [CrossRef]
- Turiano, N.A.; Whiteman, S.D.; Hampson, S.E.; Roberts, B.W.; Mroczek, D.K. Personality and substance use in midlife: Conscientiousness as a moderator and the effects of trait change. J Res Pers 2012, 46, 295–305. [Google Scholar] [CrossRef] [PubMed]
- Turiano, N.A.; Mroczek, D.K.; Moynihan, J.; Chapman, B.P. Big 5 personality traits and interleukin-6: Evidence for "healthy neuroticism" in a us population sample. Brain Behav Immun 2013, 28, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Stieger, M.; Robinson, S.A.; Bisson, A.N.; Lachman, M.E. The relationship of personality and behavior change in a physical activity intervention: The role of conscientiousness and healthy neuroticism. Pers Individ Dif 2020, 166. [Google Scholar] [CrossRef]
- Arend, I.; Yuen, K. Association between healthy neuroticism and eating behavior as revealed by the nki rockland sample. Sci Rep 2025, 15, 5858. [Google Scholar] [CrossRef]
- Morgan, J.F.; Reid, F.; Lacey, J.H. The scoff questionnaire: A new screening tool for eating disorders. West J Med 2000, 172, 164–165. [Google Scholar] [CrossRef]
- Tesar, N.; Baumhackl, U.; Kopp, M.; Gunther, V. Effects of psychological group therapy in patients with multiple sclerosis. Acta Neurol Scand 2003, 107, 394–399. [Google Scholar] [CrossRef]
- Paolucci, T.; de Sire, A.; Agostini, F.; Bernetti, A.; Salome, A.; Altieri, M.; Di Piero, V.; Ammendolia, A.; Mangone, M.; Paoloni, M. Efficacy of interoceptive and embodied rehabilitative training protocol in patients with mild multiple sclerosis: A randomized controlled trial. Front Neurol 2022, 13, 1095180. [Google Scholar] [CrossRef]
- McCormack, D.; O'Keeffe, D.F.; Seery, C.; Eccles, D.F. The association between body image and psychological outcomes in multiple sclerosis. A systematic review. Mult Scler Relat Disord 2025, 93, 106226. [Google Scholar] [CrossRef]
- Bogosian, A.; Hughes, A.; Norton, S.; Silber, E.; Moss-Morris, R. Potential treatment mechanisms in a mindfulness-based intervention for people with progressive multiple sclerosis. Br J Health Psychol 2016, 21, 859–880. [Google Scholar] [CrossRef] [PubMed]
- Simpson, R.; Mair, F.S.; Mercer, S.W. Mindfulness-based stress reduction for people with multiple sclerosis - a feasibility randomised controlled trial. BMC Neurol 2017, 17, 94. [Google Scholar] [CrossRef]
- Hocaloski, S.; Elliott, S.; Brotto, L.A.; Breckon, E.; McBride, K. A mindfulness psychoeducational group intervention targeting sexual adjustment for women with multiple sclerosis and spinal cord injury: A pilot study. Sexuality and Disability 2016, 34, 183–198. [Google Scholar] [CrossRef]
- Wills, O.; Probst, Y.; Haartsen, J.; McMahon, A.T. The role of multidisciplinary ms care teams in supporting lifestyle behaviour changes to optimise brain health among people living with ms: A qualitative exploration of clinician perspectives. Health Expect 2024, 27, e14042. [Google Scholar] [CrossRef]
- Saul, A.; Taylor, B.V.; Blizzard, L.; Simpson-Yap, S.; Oddy, W.H.; Probst, Y.C.; Black, L.J.; Ponsonby, A.L.; Broadley, S.A.; Lechner-Scott, J.; et al. Associations between diet quality and depression, anxiety, and fatigue in multiple sclerosis. Mult Scler Relat Disord 2022, 63, 103910. [Google Scholar] [CrossRef] [PubMed]
- Hanna, M.; Strober, L.B. Anxiety and depression in multiple sclerosis (ms): Antecedents, consequences, and differential impact on well-being and quality of life. Mult Scler Relat Disord 2020, 44, 102261. [Google Scholar] [CrossRef]
- Hamaker, E.L.; Kuiper, R.M.; Grasman, R.P. A critique of the cross-lagged panel model. Psychol Methods 2015, 20, 102–116. [Google Scholar] [CrossRef]
Figure 1.
Proposed serial mediation model.
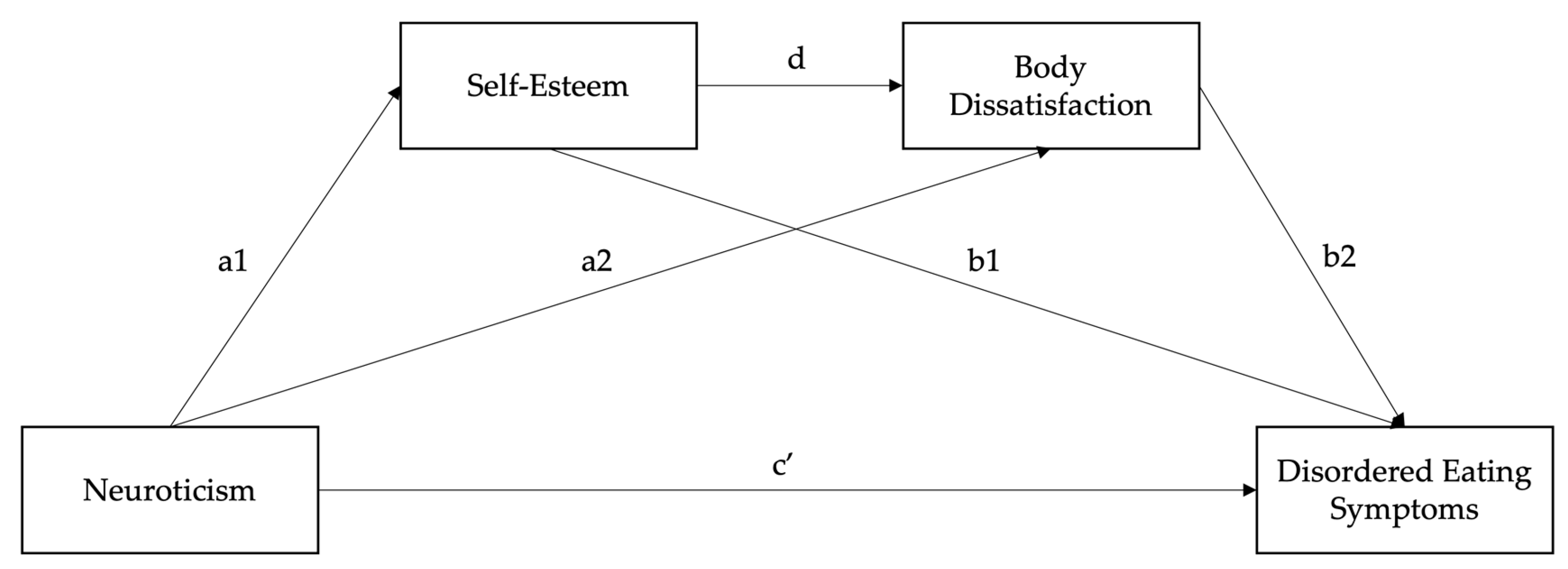
Figure 2.
Serial mediation model with pooled path coefficients (N = 275). Model path coefficients were combined across 100 multiply imputed datasets using Rubin’s rule. Unstandardised path coefficients are depicted. All pathways were significant.
Figure 2.
Serial mediation model with pooled path coefficients (N = 275). Model path coefficients were combined across 100 multiply imputed datasets using Rubin’s rule. Unstandardised path coefficients are depicted. All pathways were significant.
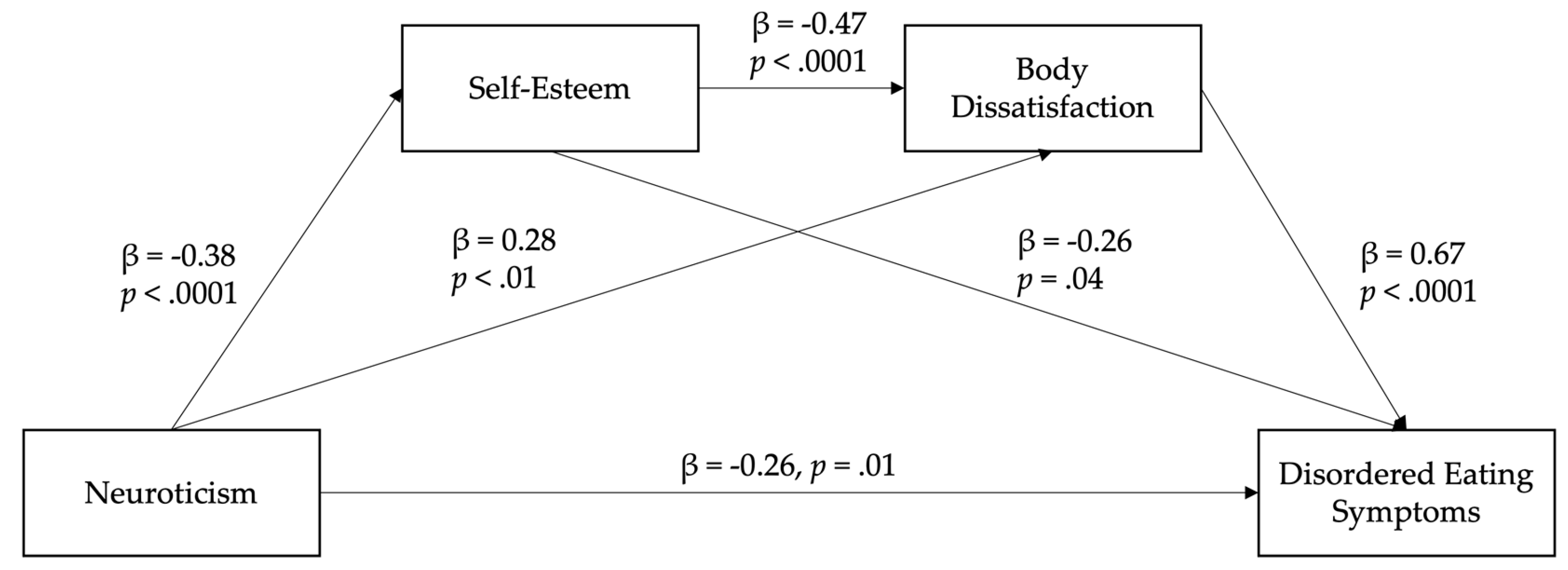
Table 1.
Sociodemographic and MS-related characteristics of the included sample (N = 275).
| Demographic | N (%) |
| Gender | |
| Male | 55 (20.0%) |
| Female | 218 (79.3%) |
| Non-binary | 2 (< 1.0%) |
| Ethnicity | |
| Anglo-Celtic | 211 (76.7%) |
| Asian (Eastern, Southern, Southeastern) | 8 (2.9%) |
| Indigenous Australian and/or Torres Strait Islander | 12 (4.4%) |
| Hispanic or Latin American | 4 (1.5%) |
| Middle Eastern | 3 (1.1%) |
| African American | 22 (8.0%) |
| Other | 15 (5.5%) |
| Country of current residence | |
| Australia | 145 (52.7%) |
| New Zealand | 6 (2.2%) |
| UK | 14 (5.1%) |
| USA | 88 (32.0%) |
| Other | 22 (8.0%) |
| Highest level of education | |
| Postgraduate | 51 (18.6%) |
| Bachelor’s degree | 76 (27.6%) |
| Year 12 (high school) or equivalent | 38 (13.8%) |
| Diploma or certificate level | 103 (37.5%) |
| Below high school | 7 (2.6%) |
| Relationship status | |
| Married | 173 (62.9%) |
| Partnered/De facto | 13 (4.7%) |
| Single/Never married | 38 (13.8%) |
| Divorced/Widowed/Separated | 51 (18.6%) |
| Employment status | |
| Full-time | 110 (40.0%) |
| Part-time/Casual | 73 (26.6%) |
| Unemployed | 92 (33.5%) |
| MS type | |
| Relapsing-remitting | 185 (68.3%) |
| Progressive (primary or secondary) | 80 (29.1%) |
| Other/Not sure | 10 (3.6%) |
| MS relapses in the past 12 months | |
| None | 129 (46.9%) |
| 1 to 3 | 119 (43.3%) |
| More than 3 | 27 (9.8%) |
| Current MS relapse at the time of survey | |
| Yes | 75 (27.3%) |
| No | 200 (72.7%) |
| Current disease-modifying treatment/s | |
| Yes | 185 (67.3%) |
| No | 90 (32.7%) |
| Level of ambulation | |
| SRDSS < 3.5 | 117 (42.5%) |
| SRDSS 4 to 6.5 | 94 (34.2%) |
| SRDSS > 7 | 18 (6.6%) |
| Missing | 46 (16.7%) |
Table 2.
Self-reported depression, anxiety, and eating disorder diagnoses (N = 275).
| Diagnosis | N (% sample) |
| Depressive disorder diagnosis | |
| Total | 147 (53.5%) |
| Current | 104 (37.8%) |
| Recovered/lifetime | 43 (15.6%) |
| Anxiety disorder diagnosis | |
| Total | 130 (47.3%) |
| Current | 114 (41.5%) |
| Recovered/lifetime | 16 (5.8%) |
| Eating disorder diagnosis | |
| Total | 58 (21.1%) |
| Current | 39 (14.2%) |
| Recovered/lifetime | 19 (6.9%) |
| Depressive disorder typea | |
| Major depressive disorder (incl. post-natal depression) | 52 (18.9%) |
| Persistent depressive disorder | 42 (10.4%) |
| Premenstrual dysphoric disorder | 7 (1.7%) |
| Not sure/other | 55 (13.6%) |
| Anxiety disorder typea | |
| Generalised anxiety disorder (GAD) | 73 (26.6%) |
| Panic disorder | 16 (5.8%) |
| Agoraphobia | 3 (1.1%) |
| Specific phobia | 7 (2.6%) |
| Social anxiety disorder | 33 (12.0%) |
| Health/illness anxiety | 7 (2.6%) |
| Separation anxiety disorder | 13 (4.7%) |
| Not sure/other | 10 (3.6%) |
| Eating disorder typea | |
| Anorexia nervosa (restricting and binge/purging) | 34 (12.4%) |
| Bulimia nervosa (purging and non-purging) | 26 (9.5%) |
| Binge eating disorder | 4 (1.5%) |
| Currently taking antidepressant or anti-anxiety medication | |
| Yes | 132 (48.0%) |
| No | 143 (52.0%) |
aParticipants could report more than one type of disorder. Participants answered the question: “Have you had a diagnosis of a depressive, anxiety, or eating disorder given to you by a health professional?”.
Table 3.
Means, standard deviations, and Pearson correlations between study variables.
| Variables | M | SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| 1.Neuroticism (BFI) | 24.87 | 6.56 | – | ||||||
| 2.Self-esteem (RSES) | 13.87 | 5.69 | -0.50** | – | |||||
| 3.Body dissatisfaction (BSQ) | 24.73 | 9.55 | 0.37** | -0.43** | – | ||||
| 4.DE symptoms (EAT-26) | 13.86 | 11.22 | 0.14* | -0.37** | 0.57** | – | |||
| 5.Age (years) | 43.03 | 12.88 | -0.18** | 0.40** | -0.23** | -0.36** | – | ||
| 6.BMI | 29.13 | 11.38 | 0.00 | -0.13 | 0.19** | -0.06 | -0.01 | – | |
| 7.Ambulation level (SRDSS) | - | - | -0.09 | 0.03 | 0.01 | -0.09 | 0.25** | 0.02 | – |
Note. All correlations are two-tailed. *p < .05. **p < .01. M = mean. SD = standard deviation. BFI = Big Five Inventory. RSES = Rosenberg Self-esteem Scale (10 items). BSQ = Body Shape Questionnaire (8 items). EAT-26 = Eating Attitudes Test (26 items). SRDSS = Self-Report Disability Status Scale (3 items).
Table 4.
Standardised and unstandardised path coefficients of the serial mediation model controlling for age, gender, BMI, and ambulation level.
Table 4.
Standardised and unstandardised path coefficients of the serial mediation model controlling for age, gender, BMI, and ambulation level.
| Model pathway | β | SE | t | p | LL 95% CI | UL 95% CI |
| Neuroticism → Self-esteem (a1) | -0.38 (-0.44) | 0.05 | -7.88 | < .001 | -0.01 | 0.20 |
| Neuroticism → Body dissatisfaction (a2) | 0.28 (0.19) | 0.10 | 2.83 | .005 | 0.09 | 0.47 |
| Self-esteem → DE symptoms (b1) | -0.26 (-0.13) | 0.13 | -2.06 | .039 | -0.46 | -0.05 |
| Body dissatisfaction → DE symptoms (b2) | 0.67 (0.57) | 0.07 | 9.76 | < .001 | 0.53 | 0.80 |
| Self-esteem → Body dissatisfaction (d) | -0.47 (-0.27) | 0.12 | -3.90 | < .001 | -0.70 | -0.23 |
| Total model effect | 0.15 (0.09) | 0.11 | 1.36 | .173 | -0.07 | 0.37 |
| Direct effect (c’) | -0.26 (-0.15) | 0.10 | -2.49 | .013 | -0.46 | -0.05 |
| Total indirect effect | 0.40 (0.22) | 0.08 | 5.06 | < .001 | 0.25 | 0.57 |
| Neuroticism → Self-esteem → DE symptoms (Ind1) | 0.10 (0.06) | 0.05 | 1.98 | .048 | 0.01 | 0.20 |
| Neuroticism → Body dissatisfaction → DE symptoms (Ind2) | 0.18 (0.11) | 0.07 | 2.74 | .006 | 0.06 | 0.33 |
| Neuroticism → Self-esteem → Body dissatisfaction → DE symptoms (Ind3) | 0.12 (0.07) | 0.04 | 2.99 | .003 | 0.05 | 0.20 |
| Pairwise comparisons of indirect effects | ||||||
| Ind1 – Ind2 | -0.09 (-0.05) | 0.09 | -0.98 | .326 | -0.26 | 0.09 |
| Ind1 – Ind3 | -0.02 (-0.01) | 0.06 | -0.29 | .774 | -0.15 | 0.11 |
| Ind2 – Ind3 | 0.07 (0.04) | 0.09 | 0.77 | .440 | -0.10 | 0.24 |
Note. N = 275. Significant pathways are noted in bold (95% confidence interval does not cross zero). 95% confidence intervals around estimates of unstandardised effects were obtained from Monte-Carlo simulations with 50,000 replications. Unstandardised effects are shown outside parentheses. Standardised effects are shown inside parentheses. Ind1 – Ind2 compares the single mediating effects of self-esteem and body dissatisfaction. Ind1 – Ind3 compares the single mediating effect of self-esteem and the serial mediating effect through both mediators. Ind2 – Ind3 compares the single mediating effect of body dissatisfaction and the serial mediating effect.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



