
Submitted:
07 April 2025
Posted:
08 April 2025
You are already at the latest version
Abstract
Background: Multiple Chemical Sensitivity is a complex and disabling condition characterized by a range of non-specific symptoms triggered by low-level exposure to common environmental chemicals. It often leads to significant impairment in quality of life, psychological well-being, and daily functioning. Non-pharmacological approaches—such as lifestyle modifications and psychological interventions—are frequently used in clinical practice, but their effectiveness remains uncertain. Objective: To evaluate the effectiveness of lifestyle-based interventions in improving outcomes in adults with MCS. Methods: A systematic review was conducted following PRISMA guidelines (PROSPERO: CRD420251013537). Searches were performed in MEDLINE, Google Scholar, CINAHL, and ResearchGate from March to April, 2025. Eligible studies included adults (≥18 years) with a verified diagnosis of Multiple Chemical Sensitivity, reporting outcomes such as stress perception, anxiety, depressive symptoms, or quality of life. Methodological quality and risk of bias were assessed using PEDro, NIH, CEBMa, and RoB 2.0 tools. Results: Twelve studies (n = 378) were included. Cognitive and behavioral therapies consistently demonstrated reductions in symptom severity, maladaptive thought patterns, and functional limitations. Mindfulness-based stress reduction showed beneficial effects, while other mindfulness-based approaches were less conclusive. Exposure-based therapies helped improve chemical tolerance and reduce avoidance behaviors. Electromagnetic and biomedical interventions showed preliminary but limited evidence of effectiveness, and aromatherapy was well tolerated though minimally effective. Conclusions:Among lifestyle-based interventions, cognitive and behavioral therapies appear most effective for managing symptoms of Multiple Chemical Sensitivity. Nevertheless, heterogeneity in study design, intervention protocols, and outcome measures limits the generalizability of findings.
Keywords:
Multiple Chemical Sensitivity
; lifestyle interventions
; cognitive-behavioral therapy
; transcranial direct current stimulation
; psychological well-being
; symptom severity
; quality of life
1. Introduction
Multiple Chemical Sensitivity (MCS) or Idiopathic Environmental Intolerance (IEI) is an acquired, chronic condition characterized by the recurrence of non-specific, multisystem symptoms triggered by exposure to environmental chemicals at concentrations that are not typically considered toxic to the general population [1,2]. Originally described by Cullen in 1987 [3], MCS presents with an estimated prevalence ranging from 0.1% to 5%, with a higher incidence reported among those with a history of allergic conditions [4,5]. Importantly, approximately 30% to 50% of MCS patients also meet diagnostic criteria for chronic fatigue syndrome or fibromyalgia [6], pointing toward potential overlapping pathophysiological mechanisms [7,8].
The clinical presentation of MCS is heterogeneous and may involve multiple organ systems such as respiratory, ocular, gastrointestinal, musculoskeletal, gynecological, and nervous [9]. Neurological symptoms including headaches [10], cognitive impairment [12], sleep disturbances [3,13], and irritability are particularly disabling and significantly contribute to reduced quality of life, functional limitations, and social withdrawal [14,15]. Furthermore, the most frequently reported neurological symptom is cacosmia, a sensory alteration marked by heightened sensitivity to odors (hyperosmia), and a distorted perception of smells (dysosmia) in response to specific chemical stimuli. [16]. Symptom onset typically occurs during or shortly after exposure and may persist for several days even after the stimulus has ceased. Although olfactory triggers are the most common [17], some patients also report symptom exacerbation following exposure to auditory [18], dietary [19], or pharmacological agents [1,10].
Despite increasing recognition of MCS as a chronic, multifactorial condition, therapeutic options remain limited and often unsatisfactory. Common approaches such as chemical avoidance [10,20], nutritional supplementation [21], and various alternative therapies remain controversial due to limited scientific evidence and, in some cases, the risk of symptom exacerbation. Among the available treatment options, cognitive behavioral therapy (CBT) [22,23], supportive psychotherapy [24] and olfactory desensitization techniques [25], have shown the most consistent benefits in improving patients’ ability to cope with chemical sensitivities and reducing symptom intensity.
Lastly, there is growing scientific and clinical interest in the role of complementary, accessible, non-pharmacological lifestyle interventions such as tailored nutrition [19,26], regular physical activity [27], stress-reduction strategies (e.g., mindfulness, yoga), and environmental adaptations [28,29]. These interventions align with patient-centered approaches and may offer significant benefits by targeting modifiable behavioral and environmental factors. Preliminary studies and observational reports have indicated potential improvements in symptom management, functional capacity, and quality of life [30,31].
Nonetheless, the existing body of evidence remains fragmented, methodologically heterogeneous, and lacks an integrated, systematic appraisal. To date, no comprehensive systematic review has rigorously examined the effectiveness, safety, and scope of lifestyle-based interventions in individuals with MCS, thereby underscoring a critical gap in the literature and the pressing need for evidence-based clinical guidance. Accordingly, the objective of the present systematic review is to evaluate the efficacy of lifestyle interventions in adults diagnosed with MCS, with particular emphasis on their impact on symptom severity, functional capacity, quality of life, and overall well-being.
2. Materials and Methods
2.1. Data Sources and Search Strategy
A systematic literature review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [32]. The review protocol was prospectively registered in the PROSPERO database (CRD420251013537), ensuring methodological transparency and adherence to established standards.
The literature search was carried out between March 17, 2025, and April 6, 2025, with the aim of identifying all relevant studies that examined the effectiveness of interventions targeting physical and psychological symptoms in patients diagnosed with MCS. The following electronic databases were systematically searched: MEDLINE (PubMed), Google Scholar, CINAHL Complete, and ResearchGate. For MEDLINE, the search strategy included the following terms: "multiple chemical sensitivity" [MeSH] OR "environmental sensitivity" [Tiab] OR "chemical intolerance" [Tiab] OR "environmental illness" [Tiab]. Equivalent search queries, adapted to each platform’s syntax, were applied to Google Scholar, CINAHL, and ResearchGate to ensure comprehensive coverage of the topic.
The initial screening process was conducted independently by two reviewers (D.P.C. and C.P.R.) who assessed titles and abstracts for potential eligibility. Full-text articles were then evaluated by a blinded third reviewer (S.E.M.P.). In cases of disagreement, a fourth reviewer (I.M.M.P.) was consulted to resolve discrepancies and reach consensus. The complete search strategy, including the combination of keywords and Boolean operators used across all databases, is detailed in Table 1.
2.2. Study Selection
The selection of the studies was carried out according to predefined eligibility criteria to ensure the scientific rigor and relevance of the included evidence. Eligible studies comprised: (1) randomized or non-randomized controlled trials, case-control studies, case series, case reports, or ongoing studies (2) published from the earliest available date up to March 31, 2025, (3) written in English or Spanish, and (4) available in full-text format. The target population included (5) adults (≥18 years) with a confirmed diagnosis of MCS. In addition, (6) studies had to evaluate interventions based on lifestyle modifications—such as dietary changes, environmental adaptations, physical activity, or mind-body practices—aimed at improving the management of MCS. Finally, (7) studies were required to report at least one outcome variable related to stress perception, illness perception, anxiety, depressive symptoms, work capacity, or quality of life.
Studies were excluded if they: (1) involved individuals under the age of 18, (2) lacked a confirmed diagnosis of MCS, or (3) focused exclusively on pharmacological treatments or diagnostic procedures unrelated to lifestyle modification. Furthermore, (4) studies not available in full text, (5) those written in languages other than English or Spanish, and (6) those categorized as reviews, editorials, commentaries, letters to the editor, or conference abstracts without original data were excluded. Lastly, (7) studies addressing occupational or environmental exposure without a therapeutic component, or in which MCS was not the primary condition under investigation, were not considered eligible.
2.3. Data Extraction
Data extraction was performed independently by two authors (D.P.C. and C.P.R.) using a standardized PICO-based template to extract relevant information. The extracted data included study characteristics (authors, year, and country of publication), study design, study objectives, sample characteristics (sample size, demographic data, disease classification, intervention details), and outcome measures. Additionally, details regarding the intervention and control groups, statistical results, and conclusions were recorded. A pilot test was conducted to ensure the reliability of the data extraction process, following the Cochrane Handbook for Systematic Reviews of Interventions (v.5.1.0). In cases of disagreement, a third author (S.M.P.) resolved the discrepancies.
2.4. Methodological Quality Assessment
The methodological quality of the included studies was assessed using standardized tools based on study design. For randomized controlled trials, the PEDro scale [33] was applied to evaluate internal validity and statistical interpretability. Studies were classified as excellent (scores 9–10), good (6–8), fair (4–5), or poor (<4). Case series were evaluated using the NIH Quality Assessment Tool for Case Series Studies [34], which examines domains such as study objectives, population selection, data collection, outcome measures, statistical analysis, and ethical considerations.
For case reports, the CEBMa Case Study Evaluation Tool [35] was used, focusing on the clarity of the clinical problem, methodological rigor, data analysis, practical implications, and ethical compliance. The use of these validated tools allowed for a structured and transparent appraisal of methodological quality across study types, enhancing the reliability of the review outcomes.
2.5. Risk of Bias Assessment
The risk of bias in randomized clinical trials was assessed using the Cochrane Risk of Bias Tool (RoB 2.0) [36], which evaluates critical aspects of study methodology. This tool assesses randomization processes, deviations from intended interventions, missing outcome data, outcome measurement, and selective reporting. Studies were classified as having low risk, some concerns, or high risk of bias, depending on the likelihood that the biases identified could alter the study outcomes. In cases of conflicting evaluations, discrepancies were discussed among the reviewers, and the final decision was made by the third investigator (S.M.P.).
2.6. Grade of Recommendation
Finally, the certainty of the evidence was determined using the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) framework [37]. This system classifies evidence based on five domains: study design, imprecision, indirectness, inconsistency, and publication bias. The certainty of the evidence was categorized into four levels: high quality, when all domains were satisfied; moderate quality, when one domain was not met; low quality, when two domains were not met; and very low quality, when three or more domains were not satisfied.
3. Results
3.1. Study Selection
A total of 137 records were initially identified through systematic searches across five major international databases: MEDLINE (PubMed) (n = 32), PEDro (n = 32), Scopus (n = 28), CINAHL (n = 20), and Web of Science (n = 25). Following the removal of 16 duplicate records, 121 references remained and were screened for relevance based on titles and abstracts. As a result, 63 records were excluded in this phase.
The remaining 58 full-text articles were assessed for eligibility according to predefined inclusion and exclusion criteria. Of these, 45 articles were excluded for the following reasons: inappropriate diagnosis (n = 12), non-eligible study design (n = 18), and language not meeting inclusion criteria (n = 16).
Ultimately, 12 studies met all eligibility criteria and were included in the qualitative synthesis. These selected studies provide evidence regarding lifestyle-based interventions in adults diagnosed with MCS, focusing on outcomes such as stress perception, illness perception, anxiety, depressive symptoms, work capacity, and quality of life. The study selection process is illustrated in Figure 1, which displays the PRISMA 2020 flow diagram summarizing each step of the review.
3.2. Characteristics of the Included Studies
A total of 12 studies were included, encompassing a range of research designs such as RCTs [40,41,42], pilot studies [44,45], case reports [38,43,46,47], a case series [48], a single-case experimental design [39], and an ongoing observational case-control study [49], with a combined sample size of 378 participants [38,39,40,41,42,43,44,45,46,47,48,49]. Most studies focused on individuals diagnosed with MCS or IEI [38,39,40,41,42,43,44,45,46,47,48], with the exception of one observational case-control study conducted on healthy individuals, age- and gender-matched to IEI patients, as part of a matched-control comparison [49].
Psychological and biopsychosocial interventions were predominant, particularly those based on CBT [38,39,40,48,49,50]. These interventions typically incorporated components such as cognitive restructuring, relaxation techniques, psychoeducation, and graded exposure. Mindfulness-based interventions (MBIs) were also prominent, including mindfulness-based cognitive therapy (MBCT) [41,42] and mindfulness-based stress reduction (MBSR) [45]. The duration of these interventions varied widely, ranging from brief programs to structured 8-week interventions, and up to 11 months in some cases [46].
Additional therapeutic approaches included pulsed electromagnetic field (PEMF) therapy [40], electroconvulsive therapy (ECT) [43], and aromatherapy massage [44]. While all were reported as feasible and well-tolerated, clinical outcomes varied across studies. Several interventions also integrated biomedical education and lifestyle modifications within a broader biopsychosocial framework [46].
Follow-up periods extended up to six months in some studies [38,49], allowing for limited assessment of long-term effects. Geographically, the studies were conducted in Denmark [40,41,42,43], Sweden [39], the United States [38,48], Canada [45,46,47], Japan [44], and France [49], reflecting a diverse and international evidence base. A summary of study characteristics and key findings is presented in Table S2.
3.3. Methodological Quality Assessment
The overall methodological quality of the studies included in this review varied from low to excellent, with an average score of 6.2 out of 10 (SD = 2.39), as assessed using a modified 10-item version of the PEDro scale. Among the five studies evaluated, one study was rated as having excellent methodological quality [40], two were classified as good quality [41,42], one as acceptable [43], and one as having low methodological quality [44].
A recurring methodological limitation across these studies was the lack of blinding procedures. Only one study reported blinding of participants, therapists, and outcome assessors [40]. In contrast, the remaining studies did not include blinding of participants [41,42,43,44], therapists [41,42,43,44], or assessors [41,42,43], which may increase the risk of performance and detection bias. This limitation is common in psychological and behavioral intervention trials, where full blinding is often infeasible due to the nature of the interventions. Table 1 presents a detailed overview of the methodological quality assessment based on the 10-item PEDro criteria.

Table 1.
Methodological Quality Analysis (PEDro Scale).
| Year, Author | Score | Quality | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 |
| Tran et al. (2016) [40] | 10 | Excellent | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Haugue et al. (2015) [41] | 7 | Good | Yes | Yes | Yes | Yes | No | No | No | Yes | Yes | Yes | Yes |
| Araki et al. (2012) [42] | 6 | Good | Yes | Yes | Yes | No | No | No | No | Yes | Yes | Yes | Yes |
| Skovbjerg et al. (2012) [43] | 5 | Acceptable | Yes | Yes | Yes | Yes | No | No | No | No | No | No | Yes |
| Sampalli et al. (2009) [44] | 3 | Low | Yes | No | No | Yes | No | No | No | No | No | Yes | Yes |
Methodological quality assessment of the included studies was conducted using the PEDro Scale [33], which consists of 11 items: (1) eligibility criteria (not scored), (2) random allocation, (3) concealed allocation, (4) baseline comparability, (5) blinding of subjects, (6) blinding of therapists, (7) blinding of assessors, (8) adequate follow-up (>85%), (9) intention-to-treat analysis, (10) between-group statistical comparisons, and (11) reporting of point estimates and variability. The total PEDro score ranges from 0 to 10 (excluding item 1), with higher scores indicating greater methodological quality.
3.3.1. Case Series
The methodological quality of the included case series, assessed using the NIH Case Series Quality Assessment Tool [34], was rated as moderate overall. One study met 7 out of 9 applicable criteria and was therefore rated as having good methodological quality [39]. The second study fulfilled 5 out of 9 criteria, corresponding to an acceptable quality rating [48]. Both studies exhibited certain limitations. Notably, the study rated as acceptable [48] did not report whether participants were recruited consecutively and lacked clearly defined inclusion and exclusion criteria. Furthermore, both studies lacked blinding of outcome assessors and did not conduct or report statistical analyses to support their findings.
Table 2.
Methodological Quality Analysis (NIH Case Series Quality Assessment Tool).
| Year, Author | Score | Quality | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
| Amin & Forslund (2018) [39] | 7/9 | Good | + | + | + | ? | + | + | + | + | ? | NA |
| Guglielmi et al. (1994) [48] | 5/9 | Acceptable | - | ? | ? | + | + | + | - | + | + | NA |
Methodological quality assessment of the included studies was conducted using the NIH Case Series Quality Assessment Tool [34], which consists of 10 items: (1) Clear objective; (2) Defined population, (3) Consecutive inclusion; (4) Intervention described, (5) Valid/reliable measures · (6)Adequate follow-up; (7) Complete outcomes; (8): Statistical analysis; (9) Outcomes described; (10) Prospective design.
3.3.2. Case Reports
The methodological quality of the included case reports was assessed using the CEBMa Case Study Evaluation Tool [35], which includes ten criteria focused on transparency, replicability, and clinical relevance. The studies scored between 6 and 9 out of 10, with a mean score of 7.3, indicating moderate to good methodological quality across the four included reports [38,44,46,47].
All case reports provided a clear description of the clinical problem, the intervention implemented, and the observed outcomes [38,44,46,47]. However, consistent limitations were identified in items 5 to 7, particularly regarding the clarity and replicability of the intervention [44,46,47], the completeness of outcome reporting [44,46], and the inclusion of adverse events [44,46,47].
In several cases, the interventions were not described in sufficient detail to ensure replicability [44,46,47], and follow-up periods were either short or not clearly specified [44,46]. Furthermore, none of the reports referenced similar previously published cases, which limits their external validity and generalizability.
Table 3.
Methodological Quality Analysis (Case Report Evaluation Tool, CEBMa).
| Year, Author | Score | Quality | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
| Woolfolk et al (2018) [38] | 9/9 | Good | + | + | + | + | + | + | ? | + | + | + |
| Elberling et al. (2010) [44] | 6/9 | Acceptable | + | + | + | ? | ? | - | - | + | + | + |
| Busse et al (2008) [46] | 7/9 | Good | + | + | + | + | - | - | - | + | + | + |
| Stenn et al (1998) [47] | 7/9 | Good | + | + | + | + | ? | ? | - | + | + | + |
Methodological quality assessment of the included studies was conducted using the NIH Case Series Quality Assessment Tool [35], which consists of 10 items: (1) Clear description of the case, (2) Clear timeline, (3) Diagnostic tests/results clearly described; (4) Intervention(s) clearly described, (5) Post-intervention outcomes clearly described, (6) Adverse events reported; (7) Takeaway lessons provided; (8) Patient’s perspective included; (9) Ethical approval stated, (10) Conclusions grounded in evidence.
3.4. Risk of Bias Analysis
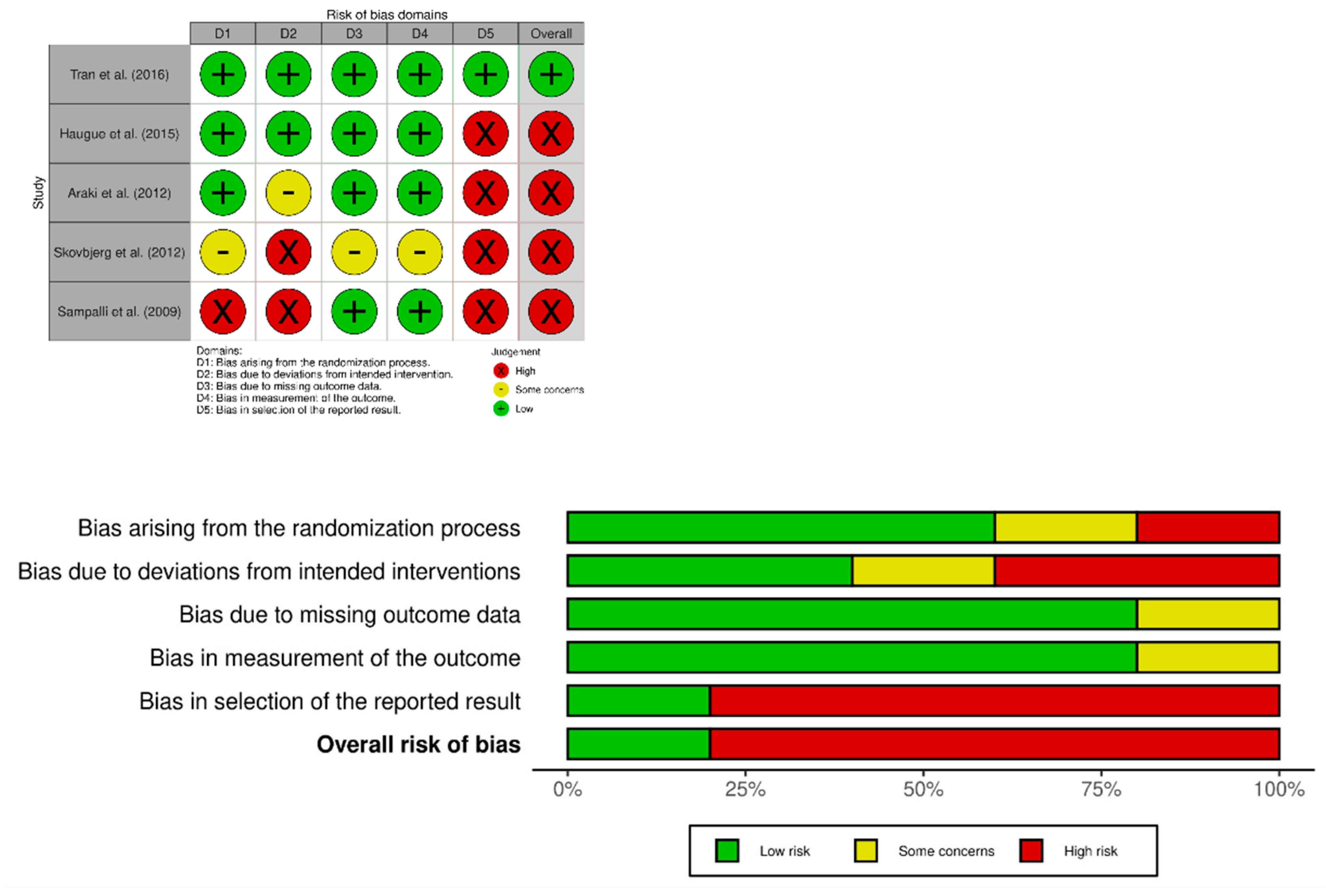
The risk of bias across the five included randomized controlled trials was assessed using the Cochrane Risk of Bias 2.0 (RoB 2.0) tool [36], which evaluates five domains: bias arising from the randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported result. As shown in Figure S4, the overall risk of bias was judged to be high in the majority of studies, with only one study rated as having low risk across all domains [40].
A high risk of bias was most frequently observed in the domains of selection of the reported result and deviations from intended interventions, affecting over half of the trials [42,43,44].Common issues included the lack of blinding of participants and personnel and selective outcome reporting, particularly in pilot or exploratory studies [42,43,44].
In the domain related to the randomization process, three studies [43,44] were rated as high risk due to inadequate concealment of allocation or insufficient reporting. While most studies showed low concerns regarding missing outcome data and outcome measurement, some concerns remained due to the reliance on self-reported outcomes and the absence of pre-registered protocols.
Given these findings, and considering the exploratory nature of several included trials, the internal validity of results should be interpreted with caution. A detailed summary of the individual risk of bias judgments is presented in Table 4, and the distribution across domains is illustrated in Figure 2.
3.5. Synthesis of Main Results
3.5.1. Cognitive Behavioral Therapy in Reducing MCS Symptoms
CBT and its adaptations were the most frequently applied interventions across the included studies [38,39,40,46,47,48]. Overall, CBT demonstrated consistent effects in reducing symptom severity related to MCS, with participants reporting improvements in somatic complaints, hypersensitivity reactions, and overall symptom burden. Several studies also noted reductions in catastrophic thinking and symptom-related anxiety, highlighting cognitive restructuring as a key mechanism of action [38,39,48].
Regarding functional outcomes, participants who received CBT showed enhanced daily life engagement, return to work, and reduced avoidance of environmental triggers [46,47]. Notably, in studies with longer intervention durations, these effects were maintained at follow-up [38,47]. Moreover, graded exposure was a central component in several CBT protocols and appeared to play a crucial role in the desensitization to chemical stimuli and behavioral reengagement.
3.5.2. Mindfulness-Based Therapy in Reducing MCS Symptoms
MBIs were assessed in three studies using different delivery formats, including MBCT [41,43] and MBSR [44]. Overall, results were mixed. Among the included studies, MBSR showed the most promising outcomes, with statistically significant reductions in psychological distress, and improvements across multiple mental health domains both post-intervention and at follow-up [44].
3.5.3. Exposure-Based Therapies in Reducing MCS Symptoms
Exposure techniques, either as standalone strategies or as components within broader CBT frameworks, were described in four studies [38,46,47,48]. These interventions aimed to gradually increase tolerance to chemical stimuli perceived as aversive or harmful. Reported outcomes included reduced avoidance behavior, increased tolerance to environmental triggers (e.g., perfumes, synthetic fabrics), and functional recovery in activities of daily living [46,47]. The effectiveness of these programs appeared to depend on factors such as structured progression, therapist guidance, and integration with cognitive strategies aimed at addressing maladaptive beliefs and anxiety.
3.5.4. Electromagnetic and Biomedical Therapies
One randomized clinical trial evaluated Transcranial PEMF in individuals with MCS [40]. The intervention resulted in a significant reduction in symptom severity, although no significant effects were observed regarding life impact or functional outcomes. Post hoc analyses revealed reductions in hyperalgesia among PEMF responders. In addition, ECT was described in a single case report involving a patient with severe MCS and no comorbid depression [44]. The case documented substantial improvements in symptom scores and restoration of social functioning, with effects sustained during a biweekly maintenance ECT phase.
3.5.5. Complementary Interventions in Reducing MCS Symptoms
A pilot crossover study evaluated the effects of aromatherapy with essential oils in individuals with IEI [42]. The intervention produced short-term improvements in mood, as measured by the Profile of Mood States (POMS), but did not result in significant changes in MCS symptoms or anxiety levels. The therapy was reported to be well tolerated and subjectively perceived as relaxing, though the findings suggest it may be more appropriate as a supportive rather than primary treatment strategy.
4. Discussion
This systematic review critically integrates the current evidence on the effectiveness lifestyle-based interventions for adults with MCS, highlighting encouraging results across cognitive-behavioral [38,39,40,46,47,48], mindfulness-based [41,43,44], and exposure-focused therapies [38,46,47,48]. Despite variability in study designs and certain methodological limitations that preclude definitive conclusions, the findings nevertheless align with prevailing neurophysiological and biopsychosocial models that frame MCS as a functional somatic disorder primarily mediated by central mechanisms of symptom perception and regulation [40,41,46].
Notably the reviewed interventions, CBT emerged as the most extensively studied and consistently effective modality. Across studies, CBT-based protocols were recurrently associated with reductions in somatic symptom burden, maladaptive cognitions (such as catastrophizing), and avoidance behaviors, in parallel with meaningful improvements in daily functioning and social reintegration [38,39,40,46,47,48]. Taken together, these therapeutic outcomes lend empirical support to the hypothesis that CBT exerts its benefits through top-down modulation of central nervous system circuits, particularly those involving limbic structures responsible for threat detection [50], interoception [51], and emotional regulation [40,46,48].
Moreover, neuroimaging data further substantiate this model. Adults with MCS demonstrate hyperactivation of the amygdala, insular cortex, and anterior cingulate cortex (ACC) in response to minimal chemical exposures, thereby resulting in exaggerated limbic responsivity and enhanced salience attribution to environmental cues [40,51,52,53]. In particular, reduced 5-HT₁A receptor binding in the ACC and amygdala has been correlated with increased harm avoidance and emotional dysregulation in this population [54,55].
In this context, CBT may counteract these neural dysfunctions by promoting cognitive reappraisal, enhancing inhibitory control within prefrontal-limbic circuits, and attenuating autonomic hyperreactivity [40,46,48]. Specifically, through mechanisms such as the restructuring of dysfunctional beliefs [56], graduated exposure to feared stimuli [57], and behavioral activation [58], CBT may restore prefrontal regulation over subcortical emotional responses, thus mitigating symptom amplification and perceptual sensitization to environmental triggers [40,47,48].
Importantly, these clinical and neurobiological findings converge with predictive coding frameworks of functional somatic disorders [59,60,61], which propose that maladaptive prior beliefs can override ambiguous sensory input, ultimately generating distressing symptoms in the absence of identifiable physiological abnormalities [49,55]. From this perspective, CBT may serve to recalibrate the balance between sensory evidence and cognitive prediction, offering a mechanistically grounded explanation for its therapeutic efficacy in MCS.
In parallel to CBT, MBIs such as MBSR and MBCT were associated with significant reductions in psychological distress [41,42,45] and modest improvements in illness perception and perceived control [62]. These effects are plausible, given evidence that mindfulness practices modulate prefrontal and ACC activity, enhance parasympathetic tone, and suppress hypothalamic-pituitary-adrenal (HPA) axis reactivity [64]. However, MBCT trials reported limited or non-significant effects on MCS-specific outcomes, suggesting that while MBIs may bolster emotional resilience and coping capacities [3,29], they may require integration with targeted exposure or cognitive techniques to influence core symptom domains.
Furthermore, exposure-based therapies, whether employed independently or embedded within CBT protocols, consistently demonstrated clinically relevant reductions in environmental avoidance and enhanced chemical tolerance [38,39,45,46,47,48]. Such findings are congruent with established mechanisms of fear extinction and desensitization [65], in which repeated, controlled exposure to conditioned stimuli leads to downregulation of threat-related limbic activation [66,67]. Consequently, this process likely contributes to the normalization of cognitive threat appraisal and the modulation of central sensitization circuits.
Although less frequently examined, biomedical and neuromodulatory interventions such as transcranial PEMF therapy [40,68] and ECT [44] also yielded reductions in symptom severity, potentially through central neuromodulatory effects. PEMF has been hypothesized to alter cortical excitability, reduce neuroinflammatory responses, and modulate autonomic function [69], while ECT is known to affect global neural connectivity and neurotransmitter balance, thus offering therapeutic benefits in severe, refractory cases of MCS [70].
Lastly, complementary therapies, including aromatherapy, demonstrated limited efficacy in alleviating core MCS symptoms but were associated with transient mood improvement and high tolerability [3,10,42,71]. As such interventions may serve as supportive strategies to enhance psychological well-being and overall quality of life when integrated into comprehensive, multimodal treatment plans.
4.1. Clinical Implications and Future Research Directions
The findings of this review support a biopsychosocial model of MCS, emphasizing the role of central sensitization, maladaptive beliefs, and behavioral avoidance in symptom persistence. Clinicians are encouraged to move beyond purely environmental or somatic explanations, integrating evidence-based psychological and behavioral interventions into routine care.
On the one hand, CBT should be considered a frontline approach, particularly for addressing catastrophic thinking, avoidance behaviors, and emotional dysregulation. On the onthe hand, mindfulness-based programs offer additional benefits by promoting stress resilience, emotional regulation, and improved interoceptive awareness. Both modalities are adaptable to individual or group settings and demonstrate high feasibility and acceptability in clinical contexts.
Furthermore, professionals should adopt a graded and individualized reactivation plan, aiming to reduce excessive avoidance and promote psychological flexibility. Environmental control strategies should be balanced to avoid reinforcing symptom chronicity. A multidisciplinary, integrative treatment plan—incorporating psychological therapy, autonomic regulation (e.g., HRV training), and lifestyle changes (e.g., sleep hygiene, activity pacing)—may yield the most sustainable outcomes.
To enhance clinical decision-making, practitioners are encouraged to follow developments in biomarker research and neurophysiological monitoring, which may soon help guide personalized interventions. Meanwhile, emphasis should be placed on long-term follow-up, outcome standardization, and functional improvement as key therapeutic goals.
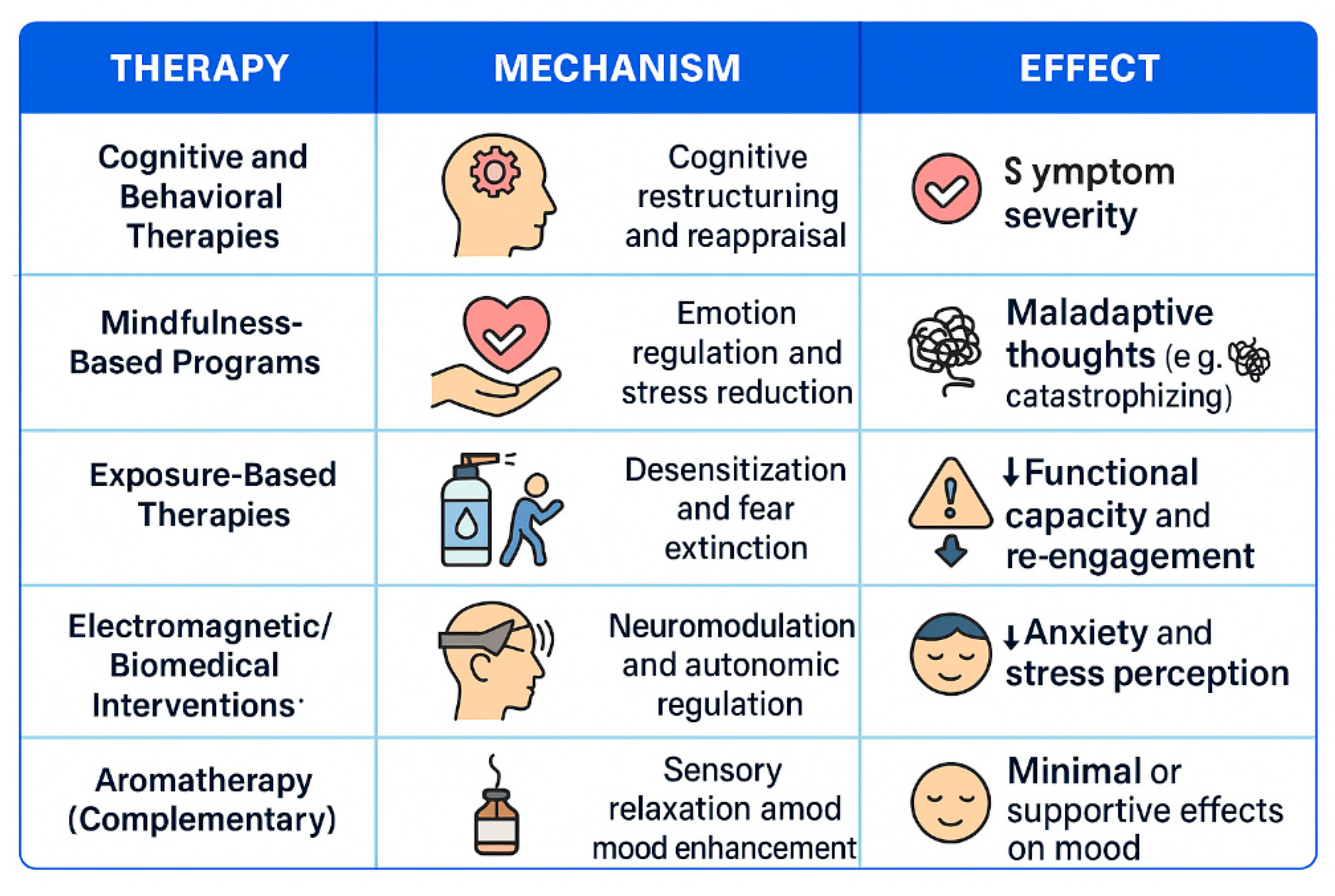
Figure 3.
Summary of lifestyle-based interventions for Multiple Chemical Sensitivity, illustrating therapeutic categories, proposed mechanisms of action, and associated clinical effects. Cognitive-behavioral and exposure-based therapies showed the most consistent benefits, while complementary and biomedical approaches demonstrated more limited but supportive outcomes.
Figure 3.
Summary of lifestyle-based interventions for Multiple Chemical Sensitivity, illustrating therapeutic categories, proposed mechanisms of action, and associated clinical effects. Cognitive-behavioral and exposure-based therapies showed the most consistent benefits, while complementary and biomedical approaches demonstrated more limited but supportive outcomes.
4.2. Limitations
This review presents several limitations that should be considered when interpreting its findings. Firstly, the limited number of high-quality randomized controlled trials weakens the overall evidence base. Many included studies were pilot trials, case reports, or non-randomized designs, frequently lacking control groups—factors that increase the risk of bias and may overestimate treatment effects. Secondly, the absence of adequate blinding, particularly in studies involving psychological and behavioral interventions, raises concerns due to the influence of expectations on subjective outcomes.
Thirdly, the substantial heterogeneity in intervention types, dosages, outcome measures, and follow-up periods hinders comparability and prevents meta-analytic synthesis. Moreover, the scarcity of studies specifically examining tDCS in MCS limits conclusions regarding its efficacy and underlying mechanisms. These limitations highlight the need for more rigorous, standardized, and adequately powered research in this field.
5. Conclusions
This systematic review critically examined the effectiveness of lifestyle-based interventions for adults with MCS. The evidence indicates that approaches such as cognitive-behavioral therapy, mindfulness-based interventions, and exposure-based strategies are associated with improvements in psychological outcomes, including reductions in distress, maladaptive cognitions, and functional limitations. Future research should focus on well-designed randomized controlled trials, standardization of interventions, and inclusion of objective biomarkers to clarify mechanisms and optimize treatment strategies for this complex condition.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org: Table S1: Search Strategy and Table S2: Characteristics of the included studies.
Author Contributions
Conceptualization, S.E.M.P. and I.M.M.P.; methodology, S.E.M.P. and I.M.M.P.; software, S.E.M.P. and I.M.M.P.; validation, S.E.M.P. and I.M.M.P.; formal analysis, S.E.M.P. and I.M.M.P.; investigation, S.E.M.P., D.P.C., C.P.R., and I.M.M.P.; resources, S.E.M.P. and I.M.M.P.; data curation, S.E.M.P. and I.M.M.P.; writing—original draft preparation, D.P.C., C.P.R.;writing—review and editing, S.E.M.P. and I.M.M.P.; visualization, S.E.M.P. and I.M.M.P.; supervision, S.E.M.P. and I.M.M.P.; and project administration, S.E.M.P. and I.M.M.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable. This study is a systematic review and meta-analysis and did not involve human or animal subjects. The review was conducted in accordance with PRISMA guidelines and was prospectively registered in the International Prospective Register of Systematic Reviews (PROSPERO; registration number CRD420251013537)
Informed Consent Statement
Not applicable. This study is a systematic review and meta-analysis and did not involve human subjects.
Data Availability Statement
Data supporting the reported results can be found in the manuscript.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study, in the collection, analyses, or interpretation of data, in the writing of the manuscript, or in the decision to publish the results.
References
- Rossi, S.; Pitidis, A. Multiple Chemical Sensitivity: Review of the State of the Art in Epidemiology, Diagnosis, and Future Perspectives. J. Occup. Environ. Med. 2018, 60, 138–146. [Google Scholar] [CrossRef] [PubMed]
- Del Casale, A.; Ferracuti, S.; Mosca, A.; Pomes, L.M.; Fiaschè, F.; Bonanni, L.; Borro, M.; Gentile, G.; Martelletti, P.; Simmaco, M. Multiple Chemical Sensitivity Syndrome: A Principal Component Analysis of Symptoms. Int. J. Environ. Res. Public Health 2020, 17, 6551. [Google Scholar] [CrossRef]
- Jacques, L. Multiple Chemical Sensitivity: A Clinical Perspective. Brain Sci. 2024, 14, 1261. [Google Scholar] [CrossRef]
- Cullen, M.R. The Worker with Multiple Chemical Sensitivities: An Overview. Occup. Med. (Chic. Ill.) 1987, 2, 655–661. [Google Scholar]
- Steinemann, A. National Prevalence and Effects of Multiple Chemical Sensitivities. J. Occup. Environ. Med. 2018, 60, e152–e156. [Google Scholar] [CrossRef]
- Caress, S.M.; Steinemann, A.C. National Prevalence of Asthma and Chemical Hypersensitivity: An Examination of Potential Overlap. J. Occup. Environ. Med. 2005, 47, 518–522. [Google Scholar] [CrossRef]
- Alameda Cuesta, A.; Pazos Garciandía, Á.; Oter Quintana, C.; Losa Iglesias, M.E. Fibromyalgia, Chronic Fatigue Syndrome, and Multiple Chemical Sensitivity: Illness Experiences. Clin. Nurs. Res. 2021, 30, 32–41. [Google Scholar] [CrossRef]
- Meggs, W.J. Mechanisms of Allergy and Chemical Sensitivity. Toxicol. Ind. Health 1999, 15, 331–338. [Google Scholar] [CrossRef] [PubMed]
- Bell, I.R. Clinically Relevant EEG Studies and Psychophysiological Findings: Possible Neural Mechanisms for Multiple Chemical Sensitivity. Toxicology 1996, 111, 101–117. [Google Scholar] [CrossRef]
- Zucco, G.M.; Doty, R.L. Multiple Chemical Sensitivity. Brain Sci. 2022, 12, 46. [Google Scholar] [CrossRef]
- Suzuki, K.; Okamura, M.; Haruyama, Y.; Suzuki, S.; Shiina, T.; Kobashi, G.; Hirata, K. Exploring the Contributing Factors to Multiple Chemical Sensitivity in Patients with Migraine. J. Occup. Health 2022, 64, e12328. [Google Scholar] [CrossRef] [PubMed]
- Molot, J.; Sears, M.; Marshall, L.M.; Bray, R.I. Neurological Susceptibility to Environmental Exposures: Pathophysiological Mechanisms in Neurodegeneration and Multiple Chemical Sensitivity. Rev. Environ. Health 2022, 37, 509–530. [Google Scholar] [CrossRef] [PubMed]
- Winder, C. Mechanisms of Multiple Chemical Sensitivity. Toxicol. Lett. 2002, 128, 85–97. [Google Scholar] [CrossRef] [PubMed]
- Driesen, L.; Patton, R.; John, M. The Impact of Multiple Chemical Sensitivity on People's Social and Occupational Functioning: A Systematic Review of Qualitative Research Studies. J. Psychosom. Res. 2020, 132, 109964. [Google Scholar] [CrossRef]
- Koch, L.; Vierstra, C.; Penix, K. A Qualitative Investigation of the Psychosocial Impact of Multiple Chemical Sensitivity. J. Appl. Rehabil. Couns. 2006, 37, 33–40. [Google Scholar] [CrossRef]
- Molot, J.; Sears, M.; Anisman, H. Multiple Chemical Sensitivity: It's Time to Catch Up to the Science. Neurosci. Biobehav. Rev. 2023, 151, 105227. [Google Scholar] [CrossRef]
- Palmieri, B.; Corazzari, V.; Vadalà, M.; Vallelunga, A.; Morales-Medina, J.C.; Iannitti, T. The Role of Sensory and Olfactory Pathways in Multiple Chemical Sensitivity. Rev. Environ. Health 2021, 36, 319–326. [Google Scholar] [CrossRef]
- Viziano, A.; Micarelli, A.; Alessandrini, M. Noise Sensitivity and Hyperacusis in Patients Affected by Multiple Chemical Sensitivity. Int. Arch. Occup. Environ. Health 2017, 90, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Aguilar-Aguilar, E.; Marcos-Pasero, H.; de la Iglesia, R.; Espinosa-Salinas, I.; de Molina, A.R.; Reglero, G.; Loria-Kohen, V. Characteristics and Determinants of Dietary Intake and Physical Activity in a Group of Patients with Multiple Chemical Sensitivity. Endocrinol. Diabetes Nutr. 2018, 65, 564–570. [Google Scholar] [CrossRef]
- Clark, I. When Avoiding Chemicals Means Avoiding Others: Relational Exposures and Multiple Chemical Sensitivity. Soc. Sci. 2024, 13, 528. [Google Scholar] [CrossRef]
- Gargano, D.; Appanna, R.; Santonicola, A.; De Bartolomeis, F.; Stellato, C.; Cianferoni, A.; et al. Food Allergy and Intolerance: A Narrative Review on Nutritional Concerns. Nutrients 2021, 13, 1638. [Google Scholar] [CrossRef]
- Serrat, M.; Sanabria-Mazo, J.P.; Almirall, M.; Musté, M.; Feliu-Soler, A.; Méndez-Ulrich, J.L.; et al. Effectiveness of a Multicomponent Treatment Based on Pain Neuroscience Education, Therapeutic Exercise, Cognitive Behavioral Therapy, and Mindfulness in Patients with Fibromyalgia (FIBROWALK Study): A Randomized Controlled Trial. Phys. Ther. 2021, 101, pzab200. [Google Scholar] [CrossRef] [PubMed]
- Van den Bergh, O.; Bräscher, A.K.; Witthöft, M. Idiopathic Environmental Intolerance: A Treatment Model. Cogn. Behav. Pract. 2021, 28, 281–292. [Google Scholar] [CrossRef]
- Lavric, C.E.; Migueres, N.; de Blay, F. Multiple Chemical Sensitivity: A Review of Its Pathophysiology. Explor. Asthma Allergy 2024, 2, 350–362. [Google Scholar] [CrossRef]
- Binkley, K.E. Multiple Chemical Sensitivity/Idiopathic Environmental Intolerance: A Practical Approach to Diagnosis and Management. J. Allergy Clin. Immunol. Pract. 2023, 11, 3645–3649. [Google Scholar] [CrossRef]
- Pigatto, P.D.; Rossi, V.; Guzzi, G. Dietary factors and endocrine consequences of multiple chemical sensitivity. Endocrinol. Diabetes Nutr. 2020, 67, 353–354. [Google Scholar]
- Bjerregaard, A.A.; Petersen, M.W.; Skovbjerg, S.; Gormsen, L.K.; Cedeño-Laurent, J.G.; Jørgensen, T.; Linneberg, A.; Dantoft, T.M. Physiological Health and Physical Performance in Multiple Chemical Sensitivity—Described in the General Population. Int. J. Environ. Res. Public Health 2022, 19, 9039. [Google Scholar] [CrossRef]
- Clark, I. When Avoiding Chemicals Means Avoiding Others: Relational Exposures and Multiple Chemical Sensitivity. Soc. Sci. 2024, 13, 528. [Google Scholar] [CrossRef]
- Skovbjerg, S.; Hauge, C.R.; Rasmussen, A.; Winkel, P.; Elberling, J. Mindfulness-Based Cognitive Therapy to Treat Multiple Chemical Sensitivities: A Randomized Pilot Trial. Scand. J. Psychol. 2012, 53, 233–238. [Google Scholar] [CrossRef]
- Fjorback LO, Arendt M, Ørnbøl E, Fink P, Walach H. Mindfulness-based stress reduction and mindfulness-based cognitive therapy: a systematic review of randomized controlled trials. Acta Psychiatr Scand. 2011, 124, 102–119. [Google Scholar] [CrossRef]
- D'Souza, J. Patient Expert Perspectives on Multiple Chemical Sensitivities and the Validity of Access Needs. J. Allergy Clin. Immunol. Pract. 2024, 12, 267. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef] [PubMed]
- National Heart, Lung, and Blood Institute. National Heart, Lung, and Blood Institute. Quality Assessment Tool for Case Series Studies; National Institutes of Health: Bethesda, MD, USA. Quality Assessment Tool for Case Series Studies; National Institutes of Health: Bethesda, MD. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on April 6, 2025).
- Centre for Evidence-Based Management (CEBMa). Critical Appraisal of a Case Study. Case Study Evaluation Tool. Available online: https://www.cebma.org (accessed on April 6, 2025).
- Higgins, J.P.T.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE: An Emerging Consensus on Rating Quality of Evidence and Strength of Recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef]
- Woolfolk, R.L. Cognitive-Behavioural Exposure Therapy for Multiple Chemical Sensitivity: A Case Study. Psychol. Psychother. Res. Stud. 2018, 1, 000507. [Google Scholar] [CrossRef]
- Amin, J.; Forslund, S. Cognitive Behavior Therapy for Multiple Chemical Sensitivity: A Single Case Experimental Design [Dissertation]. Örebro University, 2019. Available online: https://urn.kb.se/resolve?urn=urn:nbn:se:oru:diva-73356 (accessed on April 6, 2025).
- Tran, M.T.D.; Skovbjerg, S.; Arendt-Nielsen, L.; Christensen, K.B.; Elberling, J. A Randomised, Placebo-Controlled Trial of Transcranial Pulsed Electromagnetic Fields in Patients with Multiple Chemical Sensitivity. Acta Neuropsychiatr. 2017, 29, 267–277. [Google Scholar] [CrossRef]
- Hauge, C.R.; Bonde, P.J.E.; Rasmussen, A.; Skovbjerg, S. Mindfulness-Based Cognitive Therapy for Multiple Chemical Sensitivity: A Study Protocol for a Randomized Controlled Trial. Trials 2012, 13, 179. [Google Scholar] [CrossRef]
- Skovbjerg, S.; Hauge, C.R.; Rasmussen, A.; Winkel, P.; Elberling, J. Mindfulness-Based Cognitive Therapy to Treat Multiple Chemical Sensitivities: A Randomized Pilot Trial. Scand. J. Psychol. 2012, 53, 233–238. [Google Scholar] [CrossRef]
- Araki, A.; Watanabe, K.; Eitaki, Y.; Kawai, T.; Kishi, R. The Feasibility of Aromatherapy Massage to Reduce Symptoms of Idiopathic Environmental Intolerance: A Pilot Study. Complement. Ther. Med. 2012, 20, 400–408. [Google Scholar] [CrossRef]
- Elberling, J.; Gulmann, N.; Rasmussen, A. Electroconvulsive Therapy Substantially Reduces Symptom Severity and Social Disability Associated with Multiple Chemical Sensitivity: A Case Report. J. ECT 2010, 26, 231–233. [Google Scholar] [CrossRef] [PubMed]
- Sampalli, T. A Controlled Study of the Effect of a Mindfulness-Based Stress Reduction Technique in Women with Multiple Chemical Sensitivity, Chronic Fatigue Syndrome, and Fibromyalgia. J. Multidiscip. Healthc. 2009, 53, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Busse, J.; Reid, S.; Leznoff, A.; Barsky, A.; Qureshi, R.; Guyatt, G. Managing Environmental Sensitivity: An Overview Illustrated with a Case Report. J. Can. Chiropr. Assoc. 2008, 52, 88–95. [Google Scholar]
- Stenn, P.; Binkley, K. Successful Outcome in a Patient with Chemical Sensitivity: Treatment with Psychological Desensitization and Selective Serotonin Reuptake Inhibitor. Psychosomatics 1998, 39, 547–550. [Google Scholar] [CrossRef] [PubMed]
- Guglielmi, S.R.; Cox, D.J.; Spyker, D.A. Behavioral Treatment of Phobic Avoidance in Multiple Chemical Sensitivity. J. Behav. Ther. Exp. Psychiatry 1994, 25, 197–209. [Google Scholar] [CrossRef]
- Institut National de la Santé Et de la Recherche Médicale (INSERM). Study of Cognitive and Behavioural Biases in People With Idiopathic Environmental Intolerance (IEI) Versus Healthy Controls (BELIEFS VS). ClinicalTrials.gov. 2025. Available online: https://clinicaltrials.gov/study/NCT06800976 (accessed on 6 April 2025).
- Fonzo GA, Ramsawh HJ, Flagan TM, Sullivan SG, Simmons AN, Paulus MP, Stein MB. Cognitive-behavioral therapy for generalized anxiety disorder is associated with attenuation of limbic activation to threat-related facial emotions. J Affect Disord. 2014, 169, 76–85. [Google Scholar] [CrossRef]
- Karanassios G, Schultchen D, Möhrle M, Berberich G, Pollatos O. The effects of a standardized cognitive-behavioural therapy and an additional mindfulness-based training on interoceptive abilities in a depressed cohort. Brain Sci. 2021, 11, 1355. [Google Scholar] [CrossRef]
- Hillert L, Musabasic V, Berglund H, Ciumas C, Savic I. Odor processing in multiple chemical sensitivity. Hum Brain Mapp. 2007, 28, 172–182. [Google Scholar] [CrossRef]
- Del Casale, A.; Ferracuti, S.; Mosca, A.; Pomes, L.M.; Fiaschè, F.; Bonanni, L.; Borro, M.; Gentile, G.; Martelletti, P.; Simmaco, M. Multiple Chemical Sensitivity Syndrome: A Principal Component Analysis of Symptoms. Int. J. Environ. Res. Public Health 2020, 17, 6551. [Google Scholar] [CrossRef]
- Andersson L, Claeson A-S, Ledin L, Wisting F, Nordin S. Reduced olfactory performance and 5-HT₁A receptor binding potential in multiple chemical sensitivity. Hum Psychopharmacol Clin Exp. 2014, 29, 548–557. [Google Scholar] [CrossRef]
- Azuma K, Uchiyama I, Tanigawa M, et al. Chemical intolerance: involvement of brain function and networks after exposure to extrinsic stimuli perceived as hazardous. Environ Health Prev Med, 24. [CrossRef]
- Lim JA, Choi SH, Lee WJ, Jang JH, Moon JY, Kim YC, Kang DH. Cognitive-behavioral therapy for patients with chronic pain: implications of gender differences in empathy. Medicine (Baltimore), 2018; 97, e10867. [CrossRef]
- Simons LE, Harrison LE, Boothroyd DB, Parvathinathan G, Van Orden AR, O'Brien SF, Schofield D, Kraindler J, Shrestha R, Vlaeyen JWS, Wicksell RK. A randomized controlled trial of graded exposure treatment (GET living) for adolescents with chronic pain. Pain. 2024, 165, 177–191. [Google Scholar] [CrossRef]
- Jensen KB, Kosek E, Wicksell R, Kemani M, Olsson G, Merle JV, Kadetoff D, Ingvar M. Cognitive Behavioral Therapy increases pain-evoked activation of the prefrontal cortex in patients with fibromyalgia. Pain. 2012, 153, 1495–1503. [Google Scholar] [CrossRef] [PubMed]
- Draganov M, Galiano-Landeira J, Doruk Camsari D, Ramírez JE, Robles M, Chanes L. Noninvasive modulation of predictive coding in humans: causal evidence for frequency-specific temporal dynamics. Cereb, 2023; 3. [CrossRef]
- Yasoda-Mohan A, Vanneste S. Development, Insults and Predisposing Factors of the Brain's Predictive Coding System to Chronic Perceptual Disorders-A Life-Course Examination. Brain Sci. 2024, 14, 86. [CrossRef]
- Ceko M, Eippert F, Moayedi M, Bushnell MC, Schweinhardt P. Brain activity underlying pain-related attention and reappraisal in fibromyalgia. Neuroimage. 2024, 291, 120408. [Google Scholar]
- Keng SL, Smoski MJ, Robins CJ. Effects of mindfulness on psychological health: a review of empirical studies. Clin Psychol Rev. 2011, 31, 1041–1056. [Google Scholar] [CrossRef]
- Van den Bergh O, Witthöft M, Petersen S, Brown RJ. Symptoms and the body: Taking the inferential leap. Neurosci Biobehav Rev. 2017, 74, 185–203. [Google Scholar] [CrossRef] [PubMed]
- Rathore M, Verma M, Nirwan M, Trivedi S, Pai V. Functional connectivity of prefrontal cortex in various meditation techniques: a mini-review. Int J Yoga, 15. [CrossRef]
- Craske, M.G.; Treanor, M.; Conway, C.C.; Zbozinek, T.; Vervliet, B. Maximizing Exposure Therapy: An Inhibitory Learning Approach. Behav. Res. Ther. 2014, 58, 10–23. [Google Scholar] [CrossRef]
- Gatzounis, R.; den Hollander, M.; Meulders, A. Optimizing Long-Term Outcomes of Exposure for Chronic Primary Pain from the Lens of Learning Theory. J. Pain 2021, 22, 1315–1327. [Google Scholar] [CrossRef]
- Knowles, K.A.; Olatunji, B.O. Enhancing Inhibitory Learning: The Utility of Variability in Exposure. Cogn. Behav. Pract. 2019, 26, 186–200. [Google Scholar] [CrossRef]
- Flatscher, J.; Pavez Loriè, E.; Mittermayr, R.; Meznik, P.; Slezak, P.; Redl, H.; Slezak, C. Pulsed Electromagnetic Fields (PEMF)—Physiological Response and Its Potential in Trauma Treatment. Int. J. Mol. Sci. 2023, 24, 11239. [Google Scholar] [CrossRef]
- Hu, H.; Yang, W.; Zeng, Q.; Chen, W.; Zhu, Y.; Liu, W.; Wang, S.; Wang, B.; Shao, Z.; Zhang, Y. Promising Application of Pulsed Electromagnetic Fields (PEMFs) in Musculoskeletal Disorders. Biomed. Pharmacother. 2020, 131, 110767. [Google Scholar] [CrossRef] [PubMed]
- Tran, M.T.D.; Skovbjerg, S.; Arendt-Nielsen, L.; Bech, P.; Lunde, M.; Elberling, J. Two of Three Patients with Multiple Chemical Sensitivity Had Less Symptoms and Secondary Hyperalgesia after Transcranially Applied Pulsed Electromagnetic Fields. Scand. J. Pain 2014, 5, 104–109. [Google Scholar] [CrossRef] [PubMed]
- Van Thriel, C.; Kiesswetter, E.; Schäper, M.; Juran, S.A.; Blaszkewicz, M.; Kleinbeck, S. Odor annoyance of environmental chemicals: Sensory and cognitive influences. J. Toxicol. Environ. Health A 2008, 71, 776–785. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
PRISMA 2020 flow diagram.
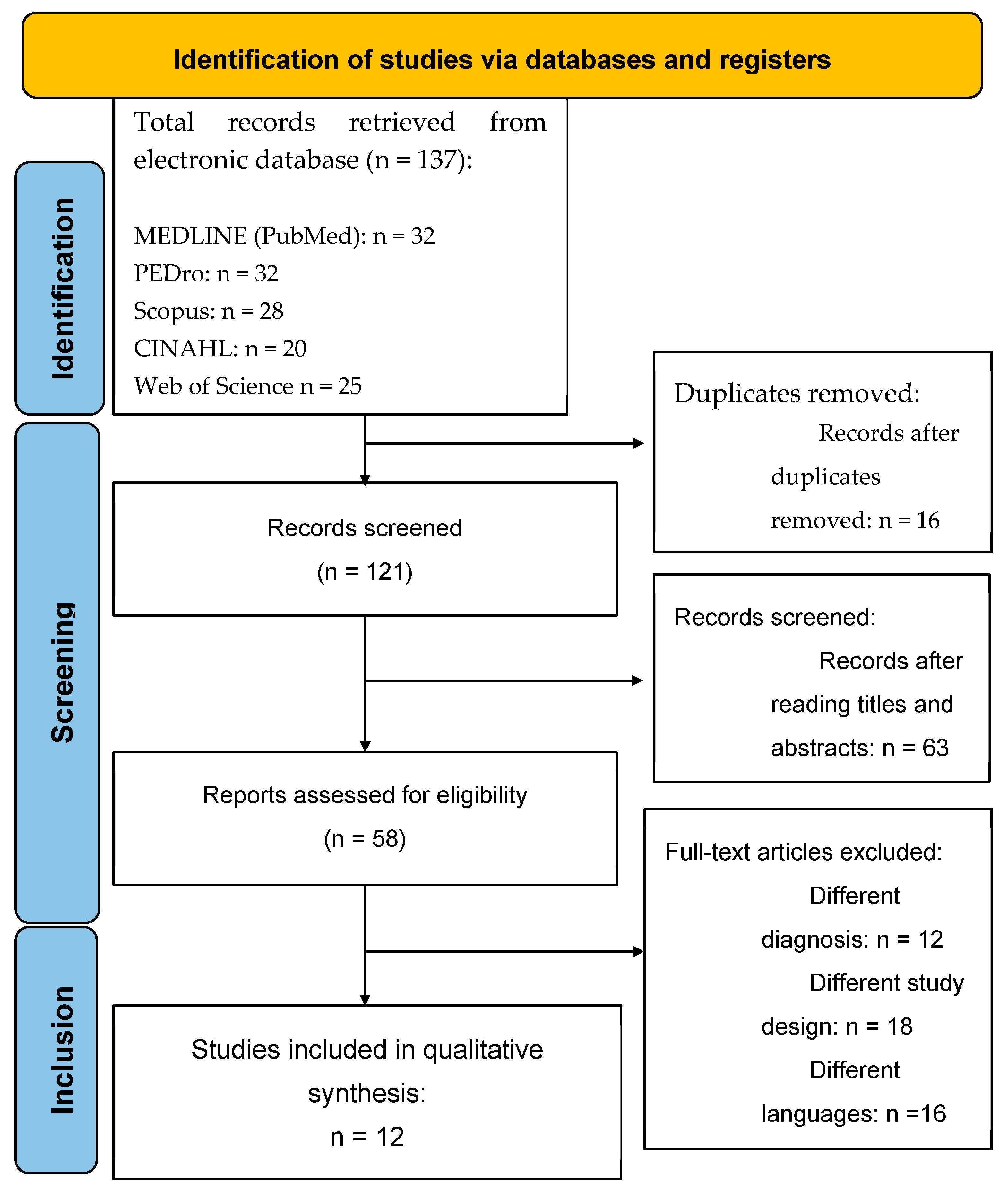
Figure 2.
Risk of bias assessment for the included studies. The bar chart illustrates the overall distribution of risk of bias across all included studies, categorized by each domain of the Cochrane Risk of Bias 2.0 tool. Colors indicate the proportion of studies rated as low risk (green), some concerns (yellow), or high risk (red) within each domain and for the overall bias judgment.
Figure 2.
Risk of bias assessment for the included studies. The bar chart illustrates the overall distribution of risk of bias across all included studies, categorized by each domain of the Cochrane Risk of Bias 2.0 tool. Colors indicate the proportion of studies rated as low risk (green), some concerns (yellow), or high risk (red) within each domain and for the overall bias judgment.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



