
Submitted:
19 April 2025
Posted:
21 April 2025
You are already at the latest version
Abstract
Exposure to HIV-related stigma and mental health problems have been reported in HIV-positive individuals. However, there are gaps regarding the involvement of mediating variables that attenuate the effect. The objective of the study was to analyze the role of social support as a mediator in the relationship between HIV-associated stigma and mental health in HIV-positive individuals. A total of 303 HIV-positive adults from Trujillo (Peru), selected by non-probabilistic convenience sampling, participated in the study. The Macro PROCESS program for SPSS was used for data analysis. Among the results, it was found that stigma exerts an indirect effect on the mental health of HIV carriers, through social support (β = -0.05, SE=0.02; 95% CI [-0.09; -0.02]). However, it exerts no direct effect (β = -0.08; p=0.21). It is concluded that social support fully mediates the relationship between HIV-linked stigma and mental health in adults with HIV-positive status. Limitations and implications of the study are discussed.
Keywords:
HIV seroprevalence
; mediation analysis
; human health
1. Introduction
HIV/AIDS disease continues to be a global health challenge affecting large numbers of people [1] and is considered one of the top ten health threats [2]. There are 39 million people living with HIV worldwide and more than half a million have died of AIDS-related causes [3]. In the Latin American region, the average rate of new diagnoses of HIV infection is 3.6 per 100,000 inhabitants, with homosexual men, men who have sex with men, transgender women and sex workers being more affected [4].
Despite reports of lower mortality and greater access to timely diagnosis, prevention and treatment [3], AIDS continues to generate health and economic impact [5]. Moreover, the Covid-19 pandemic caused, in recent years, care for HIV carriers to be interrupted and threatened [3]. Health care for this population group was affected, at all levels of care [6,7,8,9], including mental health [10].
People living with HIV face significant barriers that affect their quality of life [11,12,13,14,15,16] and psychological well-being [17,18,19,20,21]. For this reason, the mental health of people with HIV is a critical aspect that deserves attention [22], as it can influence treatment adherence [23,24] and health-related decision making [25].
One of the factors that has been shown to have a significant impact on the lives of HIV carriers is the stigma associated with this disease [19,26,27,28,29,30]. HIV stigma is considered to be that social disapproval characterized by labeling, rejecting and/or discriminating against people only because of their HIV-positive status [31]. From the perspective in which people experience the stigma, there are three main forms: a) enacted stigma, referring to the perception of past or present experiences of prejudice and discrimination, b) anticipated stigma, which is the degree to which people expect to have future experiences of prejudice and rejection; and c) internalized stigma, where one adopts negative beliefs and feelings to oneself related to one’s HIV status [32].
The HIV-related stigma has four dimensions. The first is linked to experiences of discrimination and rejection when others know about the condition. The second is related to the concern about disclosing one’s HIV status. The third comprises the negative self-image. Finally, the fourth dimension is dominated by the concern of popular opinion about HIV infection [33]. This is corroborated by scientific evidence showing the stigma expressed in forms of rejection and discrimination [18,34,35,36,37]. So too, negative internalization of discriminatory and prejudicial experiences can lead to self-stigmatization [38] with profound consequences on the quality of life [39] and mental health of affected individuals [40,41].
To counteract the stigmatizing nature of HIV in people who suffer from it, social support is important [42,43]. This is understood as the perception and belief of feeling loved and appreciated by the social groups to which an individual belongs, whether family, friends and others they consider important in their lives [44]. It plays a relevant role in providing support [45] and contributing to the recovery of physical and emotional health [46,47,48,49]. It is a protective factor in a variety of health contexts [50,51,52], improves self-management, and prevents the emergence of risky behaviors [53].
In the field of mental health, depressive symptoms are more likely to manifest in people with HIV/AIDS who have low social support than those who do [54,55]. Social support has also been found to be inversely related to suicidal ideation [56], while it has a direct relationship with self-esteem [57]. In addition, social support contributes to the improvement of mental health in gay and HIV-positive men, indirectly promoting their quality of life [58].
Among the studies conducted on social support in people with HIV, its negative relationship with perceived stigma has been reported [59]. Another research found that both variables are associated with depressive symptoms in HIV-positive pregnant women [60]. Also, quality of life was associated with social support and stigma in people living with HIV in India [61].
Regarding the mediating role of social support, it has been able to explain the relationship between assertiveness in coping with difficult experiences and immune response in HIV-positive individuals in India [62]. Also, it has had a mediating effect between HIV self-stigma and depression in men who have sex with men [63]. Another study found social support to be a mediator between disease stigma and medical mistrust because of sexual orientation in gay, bisexual, and men who have sex with men [64]. These findings highlight the need to continue to explore its influence on the mental health of people with HIV.
While the presence of stigma and its link to mental health in people with HIV has been the subject of previous research [28,40,65,66,67] significant questions remain as to how this relationship develops and whether interactions with their social support networks would be a mediator that can attenuate or exacerbate the impact on the relationship. Therefore, the main objective of this study is to analyze the role of social support as a mediator in the relationship between HIV-associated stigma and the mental health of HIV carriers.
The theoretical perspective assumed is based on health psychology and takes as a reference the biopsychosocial model that points out not only the presence of the biological factor as a determinant of health problems, but also considers relevant the psychological, social and cultural aspects that contribute to the approach to a disease [68]. This model focuses on the person and their biological composition within a personal (personality, experiences, expectations, etc.) and temporal (period of life and illness) context. The person manifests their behavior within a social context where interactions are full of meanings, leading to decision making and evaluation of their quality of life based on their social interactions [69].
The assumed theoretical model explains the presence of psychological problems related to HIV infection that contribute to increased stigmatization and rejection of HIV carriers [70,71]. However, good accompaniment and acceptance by social support networks increase optimism, hope and motivation for better decision making related to their health [17].
The findings of the present study seek to contribute to the identification of effective intervention strategies that improve the quality of life of people affected by HIV by understanding social support as a variable that explains the process of the relationship between the stigma and mental health.
2. Materials and Methods
2.1. Participantes and Procedure
The sample participants met the following inclusion criteria: being over 18 years old and having been diagnosed with HIV for at least one year. Participants were contacted through the psychologist of a public hospital in the city of Trujillo, Peru. Permission was requested from the hospital authorities for data collection and participants gave their informed consent.
The sample composition took into account the recommendations for structural equations [72], using the Soper software (2020) [73]. The observed power was estimated with the following parameters for the sample calculation: an effect size d Cohen = 0.2, a desired statistical power of 0.8 and a probability level of 0.05. An upper sample size of 303 participants was reached.
The participants were recruited through non-probabilistic convenience sampling. The three questionnaires were administered over a period of 6 months. The ages of the participants ranged from 20 to 73 years and the greatest proportion of the respondents were women (73.6%). Details of the sociodemographic data are shown in Table 1.
2.2. Measurements
Sociodemographic data sheet. Collected sociodemographic data: age, sex, sexual orientation, employment status, educational level, marital status, history of drug and/or alcohol use, history of disease and time of HIV diagnosis.
HIV stigma (Wrigth et al. [74]). The original scale was composed of 40 items [33] and was later reduced to a 10-item version [74]. This scale has 4 Likert-type response options, from 1 = strongly disagree to 4 = strongly agree. The scale was translated into Spanish and validated in the Peruvian context by Ranjit et al. [75]. The translation into Spanish was done by two Peruvian native speakers and then back-translated into English. Likewise, the translated version was reviewed and discussed through a panel of researchers [75].
The psychometric evidence of the scale was developed through a confirmatory factor analysis, where the 10-item model did not have good fit indices. For this reason, two items that had factor loadings below .40 were eliminated. Therefore, the 3-factor model with 8 items showed satisfactory fit indices (X2 = 42.92; gl = 17; p<.001; RMSEA = .06; CFI = .98; TLI = .95). The reliability was calculated using Cronbach’s alpha coefficient and obtained values above .70 in the three factors.
Perception of Social Support Scale ([EPAS]; Vaux et al. [45]). The instrument is composed of 23 items and has four response options (strongly agree = 1; agree = 2; disagree = 3 and strongly disagree = 4) and the dimensions of: family, friends and others. The original psychometric properties report acceptable Cronbach’s alpha reliability coefficients (Family [α = .90]; friends [α = .80] and others [α = .94]). The scale has been validated in Latin American countries such as Mexico [76] and Chile [77].
Psychometric evidence in the Peruvian context was conducted by Manrique-Millones et al. [78] where by means of the confirmatory factor analysis it establishes the factor structure of 3 dimensions (BS-χ² (207) = 305.61, CFI = .98, RMSEA = .05). In addition, the reliability was obtained through the Jöreskog Rho coefficient, presenting acceptable values (.72 = others, .85 = friends and .92 = family).
Mental Health Inventory-5 (MHI-5). The instrument was created by Veit and Ware [79] in a general population [80]. It consists of 5 items and uses four response options (never = 1, sometimes = 2, many times = 3 and always = 4). The instrument assesses the presence of well-being and distress.
The psychometric evidence presents a two-dimensional structure with factorial solutions above .57. In addition, reliability was performed through the internal consistency Alpha Coefficient (α = .90). It is applicable in adult and adolescent general population [81].
2.2. Data Analysis
The statistical analysis was performed using the IBM SPSS Statistics version 25 statistical program. At the beginning, the sociodemographic data and descriptive measures of the study variables were analyzed. Subsequently, the reliability was estimated by means of the omega coefficient (ω) of all the measurement instruments. To consider the reliability acceptable, the value should exceed .70. Following this, the bivariate correlation measures among the variables of interest were used. Finally, a mediation model was tested with the Macro PROCESS program for SPSS [82].
For the mediation analysis, the indirect effect of the mediating variable was taken into account [83] and the statistical significance of the mediating variable obtained by bootstrapping 10 000 simulations was estimated. The confidence intervals at 95% were calculated and checked for the analysis of the indirect effect not to be on both sides of zero to be significant [82].
Finally, the correlations of the stigma, social support and mental health with the sociodemographic variables were performed, and the effect size was calculated with Spearman correlation statistics for numerical variables, biserial rank correlation for dichotomous and numerical variables, and Epsilon squared effect size for ordinal and numerical variables. For the interpretation of the magnitude of the correlations, the following values were considered: very small (r < 0.12), small (r < 0.24), moderate (r < 0.41) and large (r >= 0.41) [84].
3. Results
3.1. Descriptive Analysis
The findings evidence a moderate negative correlation of the stigma with social support (r = - .377, p< .001); a moderate positive correlation of social support with mental health (r = .293, p< .001); and a very small correlation of social support with mental health (r = - .175, p< .001). These correlations provide support for the mediation analysis (Table 2).
3.2. Mediational Analysis
Figure 1 presents the hierarchical linear regression analysis to explore the mediating role of social support. The stigma shows a negative direct effect on social support (β = -0.38; p<0.001). However, with mental health no direct effect is evident (β = -0.08; p=0.21). The mediating variable of social support shows a positive direct effect (β = 0.27; p<0.001) on mental health. Finally, the total effect is shown which refers to the sum of the direct and indirect effects of stigma and mental health, being direct and negative (β = -0.18; p=0.0023).
Table 3 shows the direct and indirect effects of the hypothetical model. It is seen that social support plays a mediating role in the relationship of the stigma and mental health (β = -0.05, SE=0.02; 95% CI [-0.09; -0.02]). These results suggested the complete mediation of social support in the relationship of the stigma with mental health.
Table 4 shows significant differences according to mental health (rbis = -0.265, p<0.01) obtaining a small effect size and with higher scores in the male sex than in the female sex. Finally, no correlations were found between stigma, social support and mental health with the other sociodemographic variables.
4. Discussion
Previous studies have documented the impact of HIV-related stigma on treatment adherence and quality of life. However, its relationship with mental health needs to be elucidated. Therefore, we aimed to analyze the role of social support as a mediator in the relationship between HIV-associated stigma and mental health in adults with HIV.
Social support has been found to fully mediate the relationship between HIV-associated stigma and mental health in HIV-positive adults. The disapproval, discrimination and social exclusion of people because of their HIV-positive status affects their mental health when they do not have a support network of significant people in their lives. In other words, social support plays a protective role in mental health by attenuating the impact of discrimination and rejection on people living with HIV.
The findings are similar to that of other previous studies. One of them reported that social support groups reduced the impact of HIV-associated stigma on quality of life in HIV-positive women [85]. Similarly, other research found an indirect effect between perceived stigma and depression, partially mediated by social support in HIV-positive men who have sex with other men [86]. The referenced antecedents point to social support as a buffer against the impact of stigma in people with HIV.
The beneficial effects of social support in HIV-positive patients are reaffirmed [59,60,61] by attenuating the impact of clinical problems [54,55,60]. The importance of the significant support network reduces the likelihood of assumption of risky behaviors [53] that could complicate the health of HIV-positive individuals and any sexual partners they may have.
People just presenting the status of living with HIV experience greater mental health problems [87]. In addition, being part of a sexual minority may be associated with a higher prevalence of mental disorders [88]. In the case of this study, about half of the sample presented a non-heterosexual orientation. Added to this is the social stigma, which would be an aggravating factor in people living with HIV, not only because of its relationship with low access to health services and low adherence to treatment [89], but also because it is a barrier to the control of the spread of HIV [90].
Mental health problems are a critical aspect in HIV-positive patients that deserves attention [22,86,91], because of their negative influence on treatment adherence [23,24], and on health-related decision making [25]. Therefore, ensuring the well-being of people with HIV would also contribute to preventing the spread of the disease.
The absence of a direct effect between the HIV-related stigma and mental health found is in line with one study, which found that structural stigma does not directly influence the mental health of LGB people [92]. Other studies, in contrast, reported that the HIV-related stigma is associated with manifestations of the absence of mental health, such as the presence of depression [40,41,86].
The findings support the merits of social support and elucidate how HIV-related stigma has an indirect effect on the mental health of patients with HIV-positive status. However, the research contains limitations. Among them, the sample was drawn from hospital settings, which could constitute a bias by having included patients who are receiving their treatment. However, a variable that was not controlled for was continuity in treatment and their level of adherence. Therefore, these factors could be considered in future research.
Another limitation is having worked with a non-probabilistic sample, which affects the external validity of the study. Another limitation is the cross-sectional design which, not being longitudinal, contains causal inferences that are limited by the impossibility of observing the behavior of the variables over time. Not having considered as a moderating variable being part of the LGBTQ+ community is another limitation, because being part of it is associated with a higher prevalence of mental disorders [87]. In addition, self-report measures may contain some social desirability bias.
In practice, this study provides evidence for the need to integrate social support as a key factor in interventions for people with HIV. Promoting the development of emotional and community support programs can significantly strengthen the well-being of people living with HIV. In addition, the results suggest that health professionals should incorporate strategies to improve patients’ support networks, contributing to the reduction of stigma and promoting mental health in this vulnerable group.
As for future lines of research, it would be relevant to delve deeper into the different forms of social support and their differential impact, considering the quality of the support received. Also, to explore the effectiveness of specific interventions focused on social support to reduce the stigma. Finally, longitudinal studies could provide more information on the long-term effects of social support on the stigma and mental health of people with HIV.
5. Conclusions
The problem of social stigma associated with HIV raises the need for interventions [93,94] to preserve the mental health of those living with HIV and prevent the occurrence of mental health disorders and the consequences they generate in the spread of the disease. In addition, it is necessary that, within the prevention and intervention programs for this population, the social support network available to them should be strengthened or self-help groups should be formed.
Author Contributions
Conceptualization, H.S.C.E. and G.C.V.; methodology, H.S.C.E. and G.CH.V.; software, J.D.V.; validation, H.S.C.E. and G.CH.V.; formal analysis, H.S.C.E. and G.CH.V.; data curation, J.D.V.; writing—original,H.S.C.E., G.C.V., J.D.V., N.M.G.R., J.M.A, and J.C.P.; writing—review and editing, H.S.E., G.C.V. and J.C.P.; visualization, H.S.E. All authors have read and agreed to the published version of the Manuscript.
Funding
This research was funded by the Universidad Autónoma del Perú.
Institutional Review Board Statement
The study was conducted in accordance with the guidelines of the Declaration of Helsinki and was approved by the Ethics Committee of the Universidad Autónoma del Perú (N° 001A-2023-VRI-UA).
Informed Consent Statement
Informed consent was obtained from all the participants in the study.
Data Availability Statement
Following the policies of information transparency, the authors support open science and, therefore, make the database accessible to those who request it.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- World Health Organization. VIH y sida; WHO, 2023. Available online: https://www.who.int/es/news-room/fact-sheets/detail/hiv-aids.
- Pan American Health Organization. Cuáles son las 10 principales amenazas a la salud en 2019; PAHO/WHO, 2019. Available online: https://www.paho.org/es/noticias/17-1-2019-cuales-son-10-principales-amenazas-salud-2019.
- UNAIDS. Hoja informativa — Últimas estadísticas sobre el estado de la epidemia de sida; UNAIDS, 2022. Available online: https://www.unaids.org/es/resources/fact-sheet.
- Pan American Health Organization. Cuadro de indicadores básicos; PAHO/WHO, 2023. Available online: https://opendata.paho.org/en/core-indicators/core-indicators-dashboard.
- Arrighi, Y.; Ventelou, B. Epidemiological Transition and the Wealth of Nations: the Case of HIV/AIDS in a Microsimulation Model. Rev econ polit 2019, 129, 591–618. [Google Scholar] [CrossRef]
- Benade, M.; Long, L.; Rosen, S.; Meyer-Rath, G.; Tucker, J. M.; Miot, J. Reduction in initiations of HIV treatment in South Africa during the COVID pandemic. BMC Health Serv Res 2022, 22, 428. [Google Scholar] [CrossRef]
- Hogan, A. B.; Jewell, B. L.; Sherrard-Smith, E.; Vesga, J. F.; Watson, O. J.; Whittaker, C.; Hamlet, A.; Smith, J. A.; Winskill, P.; Verity, R.; et al. Potential impact of the COVID-19 pandemic on HIV, tuberculosis, and malaria in low-income and middle-income countries: a modelling study. Lancet Glob health 2020, 8, e1132–e1141. [Google Scholar] [CrossRef]
- Holmes, E. A.; O’Connor, R. C.; Perry, V. H.; Tracey, I.; Wessely, S.; Arseneault, L.; Ballard, C.; Christensen, H.; Cohen Silver, R.; Everall, I.; et al. Multidisciplinary research priorities for the COVID-19 pandemic: a call for action for mental health science. Lancet Psychiatry 2020, 7, 547–560. [Google Scholar] [CrossRef] [PubMed]
- Santos, G. M.; Hong, C.; Wilson, N.; Nutor, J. J.; Harris, O.; Garner, A.; Holloway, I.; Ayala, G.; Howell, S. Persistent disparities in COVID-19-associated impacts on HIV prevention and care among a global sample of sexual and gender minority individuals. Glob Public Health 2022, 17, 827–842. [Google Scholar] [CrossRef] [PubMed]
- Paredes, J.; Navarro, R.; Cabrera, D.; Diaz, M.; Mejia, F.; Caceres, C. Los desafíos en la continuidad de atención de personas viviendo con VIH en el Perú durante la pandemia de la COVID-19. Rev Peru Med Exp Salud Publica 2021, 38, 166–170. [Google Scholar] [CrossRef]
- da Silva, J.; Bunn, K.; Bertoni, R. F.; Neves, O. A.; Traebert, J. Quality of life of people living with HIV. AIDS Care 2013, 25, 71–76. [Google Scholar] [CrossRef]
- da Silva, J. G.; da Rocha Morgan, D. A.; Melo, F. C. M.; Dos Santos, I. K.; de Azevedo, K. P. M.; de Medeiros, H. J.; Knackfuss, M. I. Level of pain and quality of life of people living with HIV/AIDS pain and quality of life in HIV/AIDS. AIDS Care 2017, 29, 1041–1048. [Google Scholar] [CrossRef]
- Hipolito, R. L.; Oliveira, D. C.; Costa, T. L. D.; Marques, S. C.; Pereira, E. R.; Gomes, A. M. T. Quality of life of people living with HIV/AIDS: temporal, socio-demographic and perceived health relationship. Rev Latino-Am. Enfermagem 2017, 25, e2874. [Google Scholar] [CrossRef]
- Marques, S. C.; de Oliveira, D. C.; Cecilio, H. P. M.; Silva, C. P.; Sampaio, L. A.; da Silva, V. X. P. Evaluating the quality of life of people living with HIV/AIDS: integrative review/Avaliacao da qualidade de vida de pessoas vivendo com HIV/AIDS: revisao integrative/Evaluación de la calidad de vida de personas que viven con VIH/SIDA: revisión integradora. Enfermagem Uerj 2020, 28, e39144. [Google Scholar] [CrossRef]
- Reis, R. K.; Santos, C. B.; Gir, E. Quality of life among Brazilian women living with HIV/AIDS. AIDS Care 2011, 24, 626–634. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Z.; Li, X.; Qiao, S.; Zhou, Y.; Shen, Z. Social support, depression, and quality of life among people living with HIV in Guangxi, China. AIDS Care 2016, 29, 319–325. [Google Scholar] [CrossRef]
- Ammirati, R. J.; Lamis, D. A.; Campos, P. E.; Farber, E. W. Optimism, well-being, and perceived stigma in individuals living with HIV. AIDS Care 2015, 27, 926–933. [Google Scholar] [CrossRef]
- Fuster-Ruiz de Apodaca, M. J.; Molero, F.; Sansinenea, E.; Holgado, F.; Magallares, A.; Agirrezabal, A. Perceived discrimination, self-exclusion and well-being among people with HIV as a function of lipodystrophy symptoms. Anal. Psicol. 2018, 34, 7–15. [Google Scholar] [CrossRef]
- Porter, K. E.; Brennan-Ing, M.; Burr, J. A.; Dugan, E.; Karpiak, S. E. HIV Stigma and Older Men’s Psychological Well-Being: Do Coping Resources Differ for Gay/Bisexual and Straight Men? The journals of gerontology: Series B 2019, 74, 685–693. [CrossRef]
- Rzeszutek, M.; Gruszczyńska, E.; Pięta, M.; Malinowska, P. HIV/AIDS stigma and psychological well-being after 40 years of HIV/AIDS: a systematic review and meta-analysis. Eur. J. Psychotraumatol. 2021, 12, 1990527. [Google Scholar] [CrossRef]
- Rivera-Picón R, C.; Benavente-Cuesta, M. H.; Quevedo-Aguado, M. P.; Rodríguez-Muñoz, P. M. The Importance of Positive Psychological Factors among People Living with HIV: A Comparative Study. Behav. Sci. 2022, 12, 288. [Google Scholar] [CrossRef]
- Heslin, M.; Jewell, A.; Croxford, S.; Chau, C.; Smith, S.; Pittrof, R.; Covshoff, E.; Sullivan, A.; Delpech, V.; Brown, A.; et al. Prevalence of HIV in mental health service users: a retrospective cohort study. BMJ Open 2023, 13, e067337. [Google Scholar] [CrossRef]
- Da, W.; Li, X.; Qiao, S.; Zhou, Y.; Shen, Z. Antiretroviral therapy and mental health among people living with HIV/AIDS in China. Psychol, Health Med 2020, 25, 45–52. [CrossRef]
- Dow, D. E.; Turner, E. L.; Shayo, A. M.; Mmbaga, B.; Cunningham, C. K.; O’Donnell, K. Evaluating mental health difficulties and associated outcomes among HIV-positive adolescents in Tanzania. AIDS Care 2016, 28, 825–833. [Google Scholar] [CrossRef] [PubMed]
- Sikkema, K. J.; Watt, M. H.; Drabkin, A. S.; Meade, C. S.; Hansen, N. B.; Pence, B. W. Mental health treatment to reduce HIV transmission risk behavior: a positive prevention model. AIDS Behav 2010, 14, 252–262. [Google Scholar] [CrossRef]
- Anamaria, P. Informe final: índice de estigma y discriminación hacia las personas con VIH en Perú. Consorcio de organizaciones de personas con VIH en el Perú: Lima, Perú; 2018. https://plataformalac.org/wp-content/uploads/2019/03/MFOSC89SPa.pdf.
- Earnshaw, V. A.; Lang, S. M.; Lippitt, M.; Jin, H.; Chaudoir, S. R. HIV Stigma and Physical Health Symptoms: Do Social Support, Adaptive Coping, and/or Identity Centrality Act as Resilience Resources? AIDS Behav 2015, 19, 41–49. [Google Scholar] [CrossRef]
- Mendonca, C. J.; Newton-John, T. R. O.; Alperstein, D. M.; Begley, K.; Hennessy, R. M.; Bulsara, S. M. Quality of Life of People Living with HIV in Australia: The Role of Stigma, Social Disconnection and Mental Health. AIDS Behavr 2023, 27, 545–557. [Google Scholar] [CrossRef] [PubMed]
- Nikus Fido, N.; Aman, M.; Brihnu, Z. HIV stigma and associated factors among antiretroviral treatment clients in Jimma town, Southwest Ethiopia. HIV/AIDS Res. Palliat. Care. 2016, 8, 183–193. [CrossRef]
- Shrestha, S.; Shibanuma, A.; Poudel, K. C.; Nanishi, K.; Koyama Abe, M.; Shakya, S. K.; Jimba, M. Perceived social support, coping, and stigma on the quality of life of people living with HIV in Nepal: a moderated mediation analysis. AIDS Care 2019, 31, 413–420. [Google Scholar] [CrossRef] [PubMed]
- Herek, G. M. (2002). Thinking about AIDS and stigma: A psychologist’s perspective. J Law Med Ethics 2002, 30, 594-607. [CrossRef]
- Earnshaw, V. A.; Chaudoir, S. R. From conceptualizing to measuring HIV stigma: a review of HIV stigma mechanism measures. AIDS behav 2009, 13, 1160–1177. [Google Scholar] [CrossRef]
- Berger, B. E.; Ferrans, C. E.; Lashley, F. R. Measuring stigma in people with HIV: Psychometric assessment of the HIV stigma scale. Res Nur Health. 2001, 24, 518–529. [Google Scholar] [CrossRef] [PubMed]
- Al Busthomy Rofi’I, A. Y.; Kurnia, A. D.; Bahrudin, M.; Waluyo, A.; Purwanto, H. Determinant factors correlated with discriminatory attitude towards people living with HIV in Indonesian population: demographic and health survey analysis. HIV AIDS Rev 2023, 22, 104–109. [Google Scholar] [CrossRef]
- Chaudhary, S.; Kakchapati, S. Social stigma, discrimination, and their determinants among people living with HIV and AIDS in Sudurpashchim Province, Nepal. HIV & AIDS Rev. 2022, 21, 230-238. [CrossRef]
- Rahman, M. M.; Lemin, A. S.; Pangarah, C. A. Factors affecting discrimination toward people with HIV/AIDS in Sarawak, Malaysia. HIV & AIDS Rev. 2020, 19, 49-55. [CrossRef]
- Tamayo-Zuluaga, B.; Macías-Gil, Y.; Cabrera-Orrego, R.; Henao-Pelaéz, J. N.; Cardona-Arias, J. A. Estigma social en la atención de personas con VIH/SIDA por estudiantes y profesionales de las áreas de la salud, Medellín, Colombia. Rev. Cienc. salud 2015, 13, 9–23. [Google Scholar] [CrossRef]
- Van der Kooij, Y. L.; Kupková, A.; den Daas, C.; van den Berk, G. E. L.; Kleene, M. J. T.; Jansen, H. S. E.; Elsenburg, L. J. M.; Schenk, L. G.; Verboon, P.; Brinkman, K.; et al. Role of Self-Stigma in Pathways from HIV-Related Stigma to Quality of Life Among People Living with HIV. AIDS Patient Care STDs 2021, 35, 231–238. [Google Scholar] [CrossRef]
- Nobre, N.; Pereira, M.; Roine, R. P.; Sutinen, J.; Sintonen, H. HIV-Related Self-Stigma and Health-Related Quality of Life of People Living With HIV in Finland. The Journal of the Association of Nurses in AIDS Care 2018, 29, 254–265. [Google Scholar] [CrossRef]
- Hong, C.; Ochoa, A. M.; Wilson, B. D. M.; Wu, E. S. C.; Thomas, D.; Holloway, I. W. The associations between HIV stigma and mental health symptoms, life satisfaction, and quality of life among Black sexual minority men with HIV. Qual Life Res 2023, 32, 1693–1702. [Google Scholar] [CrossRef]
- Mugo, C.; Kohler, P.; Kumar, M.; Badia, J.; Kibugi, J.; Wamalwa, D. C.; Kapogiannis, B.; Agot, K.; John-Stewart, G. C. Effect of HIV stigma on depressive symptoms, treatment adherence, and viral suppression among youth with HIV. AIDS 2023, 37, 813–821. [Google Scholar] [CrossRef]
- Rodríguez, L. M.; Lagos, M. G. Redes de apoyo en los procesos de stigma asociado al VIH en Nuevo León (México). Health and Addictions / Salud y Drogas 2022, 22, 40-54. [CrossRef]
- Wedajo, S.; Degu, G.; Deribew, A.; Ambaw, F. Social support, perceived stigma, and depression among PLHIV on second-line antiretroviral therapy using structural equation modeling in a multicenter study in Northeast Ethiopia. Int J Ment Health Syst 2022, 16, 27. [Google Scholar] [CrossRef] [PubMed]
- Cobb, S. Social support as a moderator of life stress. Psychosom. Med, 1976, 38, 300-314. https://psycnet.apa.org/doi/10.1097/00006842-197609000-00003.
- Vaux, A.; Phillips, J.; Holly, L.; Thomson, B.; Williams, D.; Stewart, D. The social support appraisals (SS-A) scale: Studies of reliability and validity. Am. J. Community Psychol. 1986, 14, 195-218. https://psycnet.apa.org/doi/10.1007/BF00911821.
- Cohen, S.; Syme, L. Social support and health; Academic Press: Florida, United States, 1985. [Google Scholar]
- Cohen, S.; Underwood, L.; Gottlieb, B. Social support measurement and intervention; Oxford University Press: Oxford, England, 2000. [Google Scholar]
- Vaux, A. Social support: theory, research, and intervention; Praeger publishers: New York, United States, 1988. [Google Scholar]
- Vaux, A.; Harrison, D. Support network characteristics associates with support satisfaction and perceived support. Am. J. Community Psychol. 1985, 13, 245–265. [Google Scholar] [CrossRef]
- Dinh, T. T. H.; Bonner, A. Exploring the relationships between health literacy, social support, self-efficacy and self-management in adults with multiple chronic diseases. BMC Health Serv Res 2023, 23, 923. [Google Scholar] [CrossRef] [PubMed]
- Held, M. L.; First, J. M.; Huslage, M. Effects of COVID-19, Discrimination, and Social Support on Latinx Adult Mental Health. J Immigrant Minority Health 2022, 24, 1446–1458. [Google Scholar] [CrossRef]
- Pan, W.; Zhao, Y.; Long, Y.; Wang, Y.; Ma, Y. The Effect of Perceived Social Support on the Mental Health of Homosexuals: The Mediating Role of Self-Efficacy. Int. J. Environ. Res. Public Health 2022, 19, 15524. [Google Scholar] [CrossRef] [PubMed]
- Wallace, D. D.; Pack, A.; Uhrig Castonguay, B.; Stewart, J. L.; Schalkoff, C.; Cherkur, S.; Schein, M.; Go, M.; Devadas, J.; Fisher, E. B.; et al. Validity of Social Support Scales Utilized Among HIV-Infected and HIV-Affected Populations: A Systematic Review. AIDS Behav 2019, 23, 2155–2175. [Google Scholar] [CrossRef]
- Nakimuli-Mpungu, E.; Musisi, S.; Katabira, E.; Nachega, J.; Bass, J. Prevalence and factors associated with depressive disorders in an HIV+ rural patient population in southern Uganda. J. Affect. Disord. 2011, 135, 160–167. [Google Scholar] [CrossRef]
- Weldesenbet, A. B.; Kebede, S. A.; Tusa, B. S. The Effect of Poor Social Support on Depression among HIV/AIDS Patients in Ethiopia: A Systematic Review and Meta-Analysis. Depress Res Treat 2020, 6633686. [Google Scholar] [CrossRef]
- Yu, Y.; Luo, B.; Qin, L.; Gong, H.; Chen, Y. Suicidal ideation of people living with HIV and its relations to depression, anxiety and social support. BMC Psychol 2023, 11, 159. [Google Scholar] [CrossRef]
- Wani, M. A. Apoyo social, autoestima y calidad de vida entre las personas que viven con el VIH / SIDA en Jammu y Cachemira, India. Anal. Psicol. 2020, 36, 232–241. [Google Scholar] [CrossRef]
- Shao, B.; Song, B.; Feng, S.; Lin, Y.; Du, J.; Shao, H.; Chi, Z.; Yang, Y.; Wang, F. The relationship of social support, mental health, and health-related quality of life in human immunodeficiency virus-positive men who have sex with men: From the analysis of canonical correlation and structural equation model: A cross-sectional study. Medicine 2018, 97, e11652. [Google Scholar] [CrossRef]
- Alemu, A.; Meskele, M.; Darebo, T. D.; Beyene Handiso, T.; Abebe, A.; Paulos, K. Perceived HIV Stigma and Associated Factors Among Adult ART Patients in Wolaita Zone, Southern Ethiopia. HIV/AIDS 2022, 14, 487–501. [CrossRef]
- Brittain, K.; Mellins, C. A.; Phillips, T.; Zerbe, A.; Abrams, E. J.; Myer, L.; Remien, R. H. Social Support, Stigma and Antenatal Depression Among HIV-Infected Pregnant Women in South Africa. AIDS Behav 2017, 21, 274–282. [Google Scholar] [CrossRef]
- Garrido-Hernansaiz, H.; Heylen, E.; Bharat, S.; Ramakrishna, J.; Ekstrand, M. L. Stigmas, symptom severity and perceived social support predict quality of life for PLHIV in urban Indian context. Health Qual Life Outcomes 2016, 14, 152. [Google Scholar] [CrossRef] [PubMed]
- Pandey, D.; Shrivastava, P. Mediation effect of social support on the association between hardiness and immune response. Asian J Psychiatr 2017, 26, 52–55. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Mo, P. K.; Wu, A. M.; Lau, J. T. Roles of Self-Stigma, Social Support, and Positive and Negative Affects as Determinants of Depressive Symptoms Among HIV Infected Men who have Sex with Men in China. AIDS Behav 2017, 21, 261–273. [Google Scholar] [CrossRef] [PubMed]
- Hill, M.; Truszczynski, N.; Newbold, J.; Coffman, R.; King, A.; Brown, M. J.; Radix, A.; Kershaw, T.; Kirklewski, S.; Sikkema, K.; et al. The mediating role of social support between HIV stigma and sexual orientation-based medical mistrust among newly HIV-diagnosed gay, bisexual, and other men who have sex with men. AIDS Care 2022, 35, 696–704. [Google Scholar] [CrossRef]
- Kim, K.; Jang, S.; Rim, H. D.; Kim, S. W.; Chang, H. H.; Woo, J. Attachment Insecurity and Stigma as Predictors of Depression and Anxiety in People Living With HIV. Psychiatry Investig 2023, 20, 418–429. [Google Scholar] [CrossRef]
- Liu, H.; Zhao, M.; Ren, J.; Qi, X.; Sun, H.; Qu, L.; Yan, C.; Zheng, T.; Wu, Q.; Cui, Y. Identifying factors associated with depression among men living with HIV/AIDS and undergoing antiretroviral therapy: a cross-sectional study in Heilongjiang, China. Health Qual Life Outcomes 2018, 16, 190. [Google Scholar] [CrossRef]
- Travaglini, L. E.; Himelhoch, S. S.; Fang, L. J. HIV Stigma and Its Relation to Mental, Physical and Social Health Among Black Women Living with HIV/AIDS. AIDS Behav 2018, 22, 3783–3794. [Google Scholar] [CrossRef]
- Engel, G. L. The need for a new medical model: a challenge for biomedicine. Science 1977, 196, 129–136. [Google Scholar] [CrossRef]
- Wade, D. T.; Halligan, P. W. The biopsychosocial model of illness: a model whose time has come. Clin. Rehabil. 2017, 31, 995–1004. [Google Scholar] [CrossRef]
- Ballester, R. Aportaciones desde la psicología al tratamiento de las personas con infección por VIH/SIDA. Revista de Psicopatología y Psicología Clínica 2005, 10, 53–69. [CrossRef]
- Cantú Guzmán, R.; Álvarez Bermúdez, J.; Torres López, E.; Sulvarán, O. M. Impacto psicosocial en personas que viven con VIH-sida en Monterrey, México. Psicología y Salud 2012, 22, 136–172. [Google Scholar] [CrossRef]
- Wolf, E. J.; Harrington, K. M.; Clark, S. L.; Miller, M. W. Sample size requirements for structural equation models: An evaluation of power, bias, and solution propriety. Educ Psychol Meas 2013, 73, 913–934. [Google Scholar] [CrossRef] [PubMed]
- Soper, D. S. A-priori Sample Size Calculator for Structural Equation Models. Free Statistics Calculators. 2020. http://www.danielsoper.com/statcalc.
- Wright, K.; Naar-King, S.; Lam, L.; Templin, T.; Frey, M. Stigma scale revised: reliability and validity of a brief measure of stigma for HIV+ youth. J Adolesc Helath. 2007, 40, 96–98. [Google Scholar] [CrossRef]
- Ranjit, Y. S.; Krishnan, A.; Earnshaw, V. A.; Weikum, D.; Ferro, E. G.; Sanchez, J.; Altice, F. L. Psychometric evaluation and validation of the HIV Stigma Scale in Spanish among men who have sex with men and transgender women. Stigma and Health 2021, 8, 437–444. [Google Scholar] [CrossRef] [PubMed]
- Nava Quiroz, C. N.; Bezies, R.; Vega, C. Z. Adaptación y validación de la escala de percepción de apoyo social de vaux. Liberabit 2015, 21, 49–58, http://www.scielo.org.pe/scielo.php?pid=S1729-48272015000100005&script=sci_arttext&tlng=pt. [Google Scholar]
- Cárdenas, M.; Barrientos, J.; Ricci, E. Estructura factorial de la escala de soporte social subjetivo: validación en una muestra de estudiantes universitarios chilenos. Act. Colom. Psicol. 2015, 18, 95–101. [Google Scholar] [CrossRef]
- Manrique-Millones, D. L. M.; Rivalles, R. M.; Lara, S. D.; Marín, C. P.; Pino, O. M. Apoyo social en educación superior: evidencias de validez y confiabilidad en el contexto peruano. Universitas Psychologica 2020, 19, 1-11. https://doi-org/1. 10.11144/Javeriana.upsy19.sshe.
- Veit, C. T.; Ware, J. E. The structure of psychological distress and well-being in general populations. J Consult. Clin Psychol. 1983, 51, 730–742. [Google Scholar] [CrossRef]
- Berwick, D. M.; Murphy, J. M.; Goldman, P. A.; Ware Jr, J. E.; Barsky, A. J.; Weinstein, M. C. Performance of a five-item mental health screening test. Medical Care 1991, 169-176. https://www.jstor.org/stable/3766262.
- Merino-Soto, C.; Cuba-Canales, Y.; Rojas-Aquiño, L. Inventario de Salud Mental-5 (MHI-5) en adolescentes peruanos: estudio preliminar de validación. Rev. salud pública 2019, 21, 439–443. [Google Scholar] [CrossRef]
- Hayes, A. F. Partial, conditional, and moderated moderated mediation: Quantification, inference, and interpretation. Commun. Monogr. 2017, 85, 4–40. [Google Scholar] [CrossRef]
- Van Jaarsveld, D. D.; Walker, D. D.; Skarlicki, D. P. The role of job demands and emotional exhaustion in the relationship between customer and employee incivility. J Managet 2010, 36, 1486–1504. [Google Scholar] [CrossRef]
- Lovakov, A.; Agadullina, E. Empirically derived guidelines for effect size interpretation in social psychology. European Journal of Social Psychology 2021, 51, 485–504. [Google Scholar] [CrossRef]
- Logie, C. H.; Wang, Y.; Lacombe-Duncan, A.; Wagner, A. C.; Kaida, A.; Conway, T.; Webster, K.; de Pokomandy, A.; Loutfy, M. R. HIV-related stigma, racial discrimination, and gender discrimination: Pathways to physical and mental health-related quality of life among a national cohort of women living with HIV. Preventive Medicine 2018, 107, 36–44. [Google Scholar] [CrossRef]
- Yan, H.; Li, X.; Li, J.; Wang, W.; Yang, Y.; Yao, X.; Yang, N.; Li, S. Association between perceived HIV stigma, social support, resilience, self-esteem, and depressive symptoms among HIV-positive men who have sex with men (MSM) in Nanjing, China. AIDS Care 2019, 31, 1069–1076. [Google Scholar] [CrossRef]
- Orza, L.; Bewley, S.; Logie, C. H.; Crone, E. T.; Moroz, S.; Strachan, S.; Vazquez, M.; Welbourn, A. How does living with HIV impact on women’s mental health? Voices from a global survey. J Int AIDS Soc 2015, 18, 20289. [Google Scholar] [CrossRef] [PubMed]
- Meyer, I. H. Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: Conceptual issues and research evidence. Psychological Bulletin 2023, 129, 674–697. [Google Scholar] [CrossRef] [PubMed]
- Rueda, S.; Mitra, S.; Chen, S.; Gogolishvili, D.; Globerman, J.; Chambers, L.; Wilson, M.; Logie, C. H.; Shi, Q.; Morassaei, S.; et al. Examining the associations between HIV-related stigma and health outcomes in people living with HIV/AIDS: a series of meta-analyses. BMJ Open 2016, 6, e011453. [Google Scholar] [CrossRef] [PubMed]
- Gesesew, H. A.; Tesfay Gebremedhin, A.; Demissie, T. D.; Kerie, M. W.; Sudhakar, M.; Mwanri, L. Significant association between perceived HIV related stigma and late presentation for HIV/AIDS care in low and middle-income countries: A systematic review and meta-analysis. PloS One 2017, 12, e0173928. [Google Scholar] [CrossRef]
- Contreras Jara, B.; Cordero Álvarez, F.; Pino Morales, V.; Ávalos Blaser, J. Adherencias al tratamiento antiretroviral de la persona adulta viviendo con VIH/SIDA. Benessere – Revista de Enfermería 2021, 6, 1-11. [CrossRef]
- Song, H. Structural stigma and mental health among lesbian, gay, and bisexual adults: Policy protection and cultural acceptance. Soc. Sci. Med. 2025, 373, 117985. [Google Scholar] [CrossRef]
- Pollack, T. M.; Duong, H. T.; Nhat Vinh, D. T.; Phuong, D. T.; Thuy, D. H.; Nhung, V. T. T.; Uyen, N. K.; Linh, V. T.; Van Truong, N.; Le Ai, K. A.; Ninh, N. T.; Nguyen, A.; Canh, H. D.; Cosimi, L. A. Un diseño pretest-postest para evaluar la eficacia de una intervención para reducir el estigma y la discriminación relacionados con el VIH en entornos sanitarios de Vietnam. J Int AIDS Soc 2022, 25, e25932. [Google Scholar] [CrossRef]
- Stangl, A. L.; Lloyd, J. K.; Brady, L. M.; Holland, C. E.; Baral, S. A systematic review of interventions to reduce HIV-related stigma and discrimination from 2002 to 2013: how far have we come? J Int AIDS Soc 2013, 16, 18734. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
This is a figure. Schemes follow the same formatting.
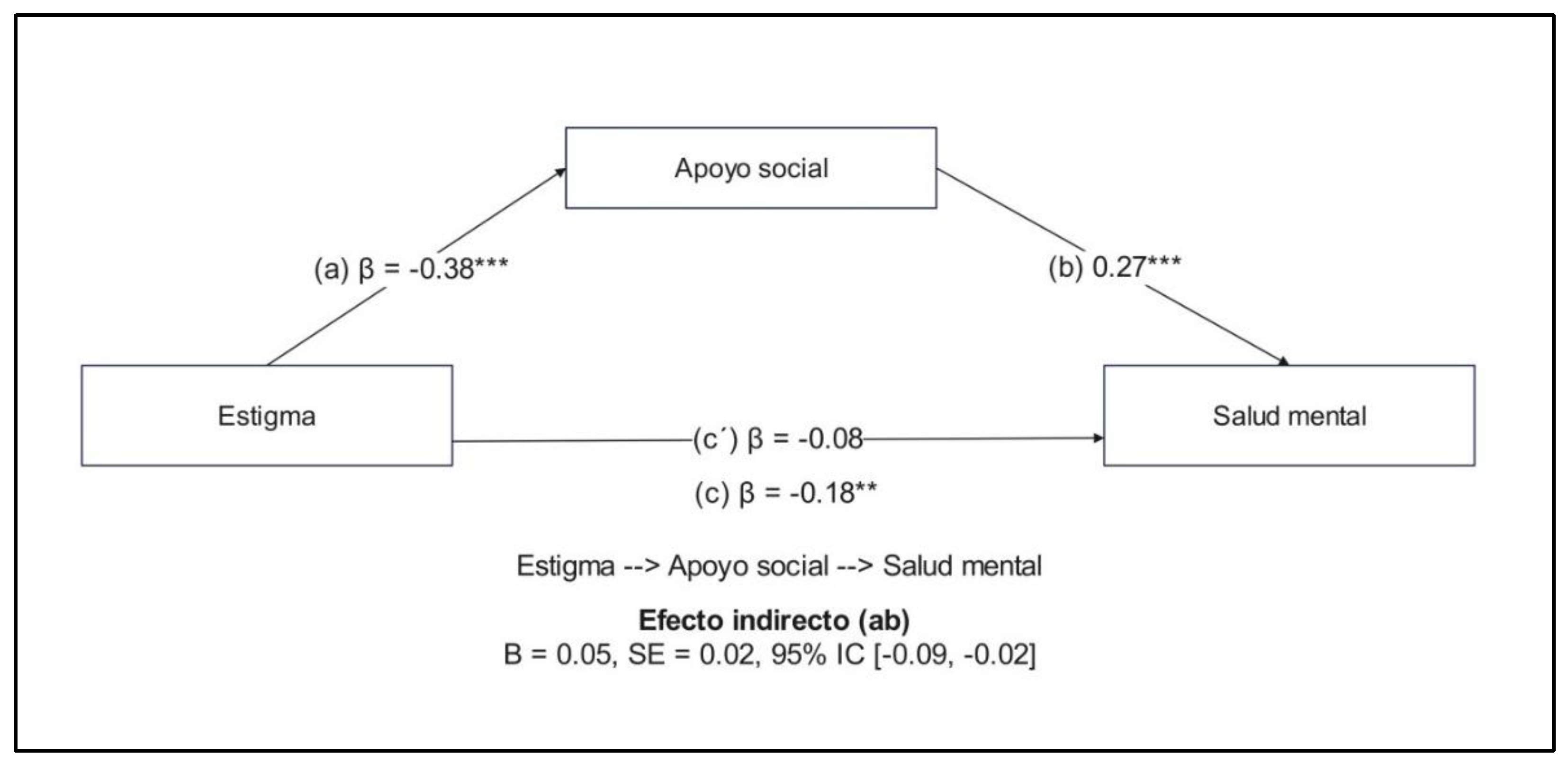

Table 1.
Sociodemographic data of the sample.
| Characteristics | (n=303) |
|---|---|
| Sex (%) | |
| Woman | 223 (73.6%) |
| Man | 80 (26.4%) |
| Sexual orientation (%) | |
| Heterosexual | 163 (53.8%) |
| Homosexual | 108 (35.6%) |
| Bisexual | 26 (8.6%) |
| Other | 6 (2.0%) |
| Age (M ± SD) | 40.55 ± 11.17 |
| Educational level (%) | |
| Primary school | 32 (10.6%) |
| Secondary school | 131 (43.2%) |
| Higher technical | 57 (18.8%) |
| Higher education | 83 (27.4%) |
| Marital status (%) | |
| Single | 190 (62.7%) |
| Married / live-in partner | 95 (31.4%) |
| Divorced / separated | 18 (5.9%) |
| Employment status (%) | |
| Employed | 231 (76.2%) |
| Unemployed | 57 (18.8%) |
| Student | 14 (4.6%) |
| Retired | 1 (0.3%) |
| Time of diagnosis (M ± SD) | 81.8 ± 129.34 |
Table 2.
Descriptive statistics and correlation analysis among variables.
| Variable | M | SD | Min | Max | 1 | 2 |
|---|---|---|---|---|---|---|
| 1. Stigma | 21.23 | 5.43 | 10 | 58 | - | |
| 2. Social support | 48.03 | 7.12 | 18 | 91 | -0.377** | - |
| 3. Mental health | 15.69 | 2.87 | 6 | 20 | -0.175** | 0.293** |
Note: M = Mean, SD = Standard deviation, Min = minimum value, Max = maximum value, *p<0.05; **p<0.01.
Table 3.
Direct and indirect effects of the stigma model and mental health mediated by social support.
Table 3.
Direct and indirect effects of the stigma model and mental health mediated by social support.
| Model routes | Estimated effect | SE | 95% CI | p |
|---|---|---|---|---|
| Direct effects | ||||
| Stigma --> Mental health | -0.08 | 0.03 | -0.10, 0.02 | 0.2094 |
| Stigma --> Social support | -0.38 | 0.02 | -0.63, -0.36 | <0.001*** |
| Social --> Mental health | 0.27 | 0.09 | 0.06, 0.15 | <0.001*** |
| Indirect effect | ||||
| Stigma --> Social support--> Mental health | -0.05 | 0.02 | -0.09, - 0.02 | <0.001*** |
| Total effect | -0.18 | 0.03 | -0.15, -0.03 | 0.0023** |
Note: EE = Standard error, 95% CI = 95% Confidence intervals 1000 bootstraps, p<0.001***, p<0.01**.
Table 4.
Stigma, social support and mental health according to sociodemographic variables.
| Variables | Stigma | Social support | Mental health |
|---|---|---|---|
| Sex | 0.073 b | 0.003 b | -0.265 b ** |
| Age | 0.011 a | -0.055 a | -0.025 a |
| Orientation | 0.001 c | 0.031 c | 0.003 c |
| Educational level | 0.047 c | 0.072 c | 0.009 c |
| Marital status | 0.003 c | 0.000 c | 0.004 c |
| Employment status | 0.025 c | 0.022 c | 0.024 c |
| Time of diagnosis | 0.021 a | -0.036 a | 0.002 a |
Note: aSpearman correlation, bRank-biserial correlation, cEpsilon squared effect size. * p<0.05; ** p<0.01.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



