
Submitted:
19 April 2025
Posted:
21 April 2025
You are already at the latest version
Abstract
Background: Aortic stenosis (AS) is the most common valvular heart disease, associated with poor outcomes if left untreated. Current guidelines recommend that transcatheter aortic valve implantation (TAVI) procedures be performed in hospitals with an on-site cardiac surgery unit due to potential complications requiring surgical intervention. This study aims to evaluate the feasibility and clinical outcomes of implementing a TAVI program at a cardiology department without an on-site cardiac surgery department, in collaboration with a remote hospital for surgical backup.
Methods: The TAVI program involved pre- and post-procedural evaluations conducted at Meir Medical Center (Kfar Saba, Israel) with a remote surgical team available. The study population included 149 consecutive patients with severe aortic stenosis treated at the Meir valve clinic between November 2019 and December 2023. Procedures were performed by the center's interventional cardiology team.
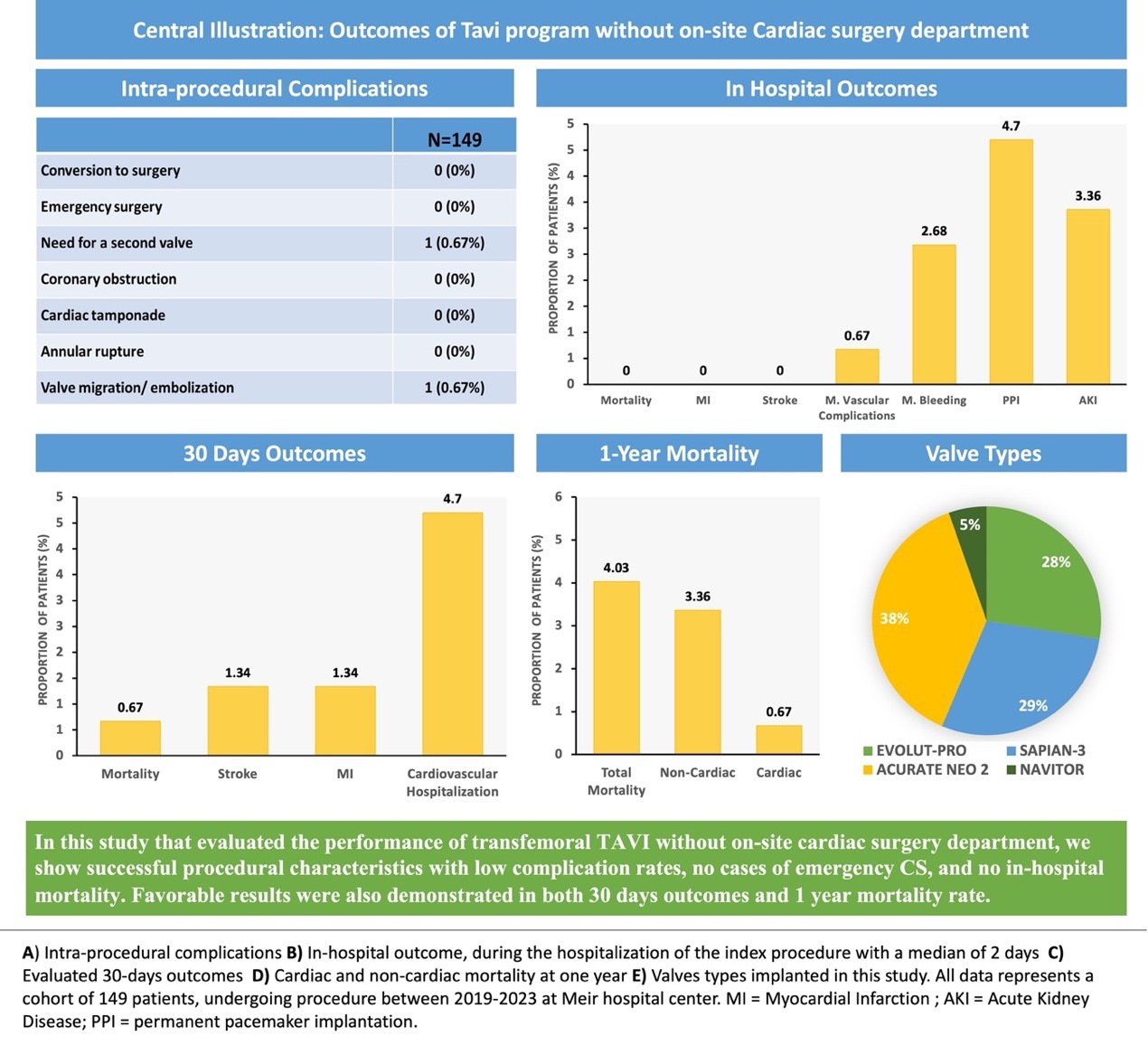
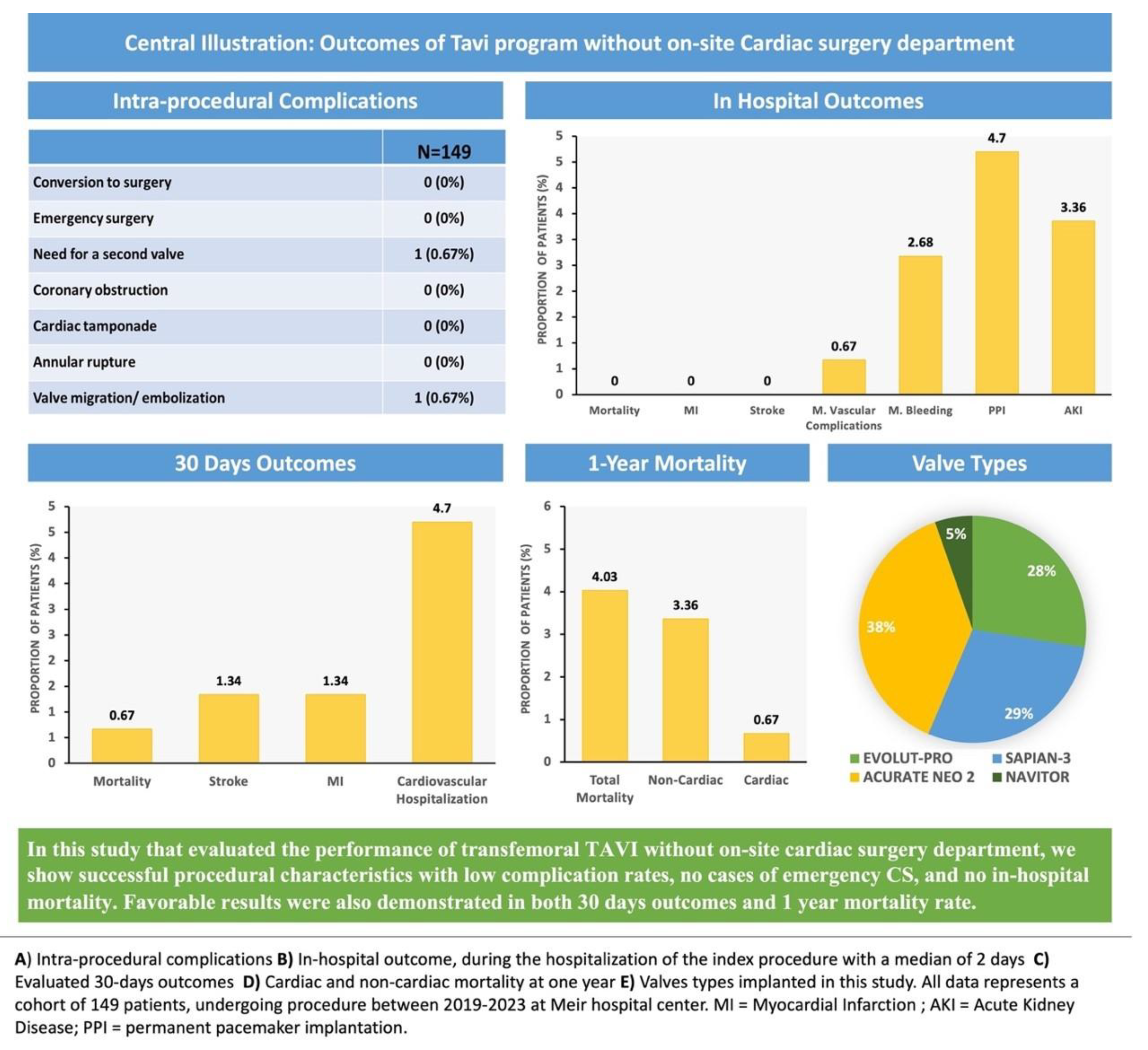
Results: The mean age of the 149 patients was 80 ± 6 years, and 75 (50%) were female. The average STS score was 4.3 and the EuroSCORE II was 3.1. Among the patients, 68 (45%) were classified as New York Heart Association (NYHA) class III-IV. Valve types used included Acurate-neo 2 (57 patients, 38%), Sapien-3 (43 patients, 28%), Evolut-PRO (41 patients, 27%), and Navitor (7 patients, 4%). There were no cases of moderate to severe paravalvular leak, no elevated post-implantation gradients, and no need for urgent cardiac surgery. One case of valve embolization was successfully managed percutaneously during the procedure. In-hospital follow-up revealed no deaths and only one major vascular complication. At one-year follow-up, six patients had died, with only one death attributed to cardiac causes.
Conclusions: This study demonstrates that the transfemoral TAVI procedure can be safely and effectively performed in a cardiology department without an on-site cardiac surgery unit, provided there is collaboration with a remote surgical center. These findings suggest that expanding TAVI programs to centers without on-site cardiac surgery could increase access to this life-saving treatment for aortic stenosis.
Keywords:
aortic stenosis
; transcatheter aortic valve implantation
; on-site cardiac surgery
; remote surgical backup
Central Illustration – Graphical Abstract
Introduction
Aortic stenosis is a common yet serious valve disease, leading to significant morbidity and mortality if left untreated. Since transcatheter aortic valve implantation (TAVI) was introduced in 2002, the management of valvular heart disease has been revolutionized. The development of TAVI offers a less invasive option than traditional surgery and has demonstrated good outcomes for patients globally. The procedure has continuously evolved, with improvements leading to simplification and a significant reduction in complication rates according to recent studies [1,2,3]. One notable advancement is the move toward early discharge, with some patients even leaving the hospital on the same day as the procedure [4].
Despite its beneficial value, TAVI still carries a potential risk for major complications such as annular rupture, coronary artery obstruction, valve embolization, tamponade, and aortic dissection. However, the incidence of these complications remains low, ranging from 0.9 to 1.6 % according to various studies [5,6]. The rising demand for TAVI has resulted in prolonged waiting times, which in turn leads to an increase in mortality, hospitalizations for heart failure, and urgent procedures. The mortality rate of AS patients awaiting TAVI ranges from 2% to 10% [7,8]. Giving the rising demand for TAVI and the associated morbidity and mortality among patients on waiting lists, there is a need to enhance the capacity of experienced teams to treat this population. Current guidelines [9] recommend that TAVI procedures be performed at centers with on-site cardiovascular surgical capabilities, based on the assumption that surgical backup is beneficial in case of complications requiring emergency cardiac surgery (CS). Although catastrophic complications are rare (<0.7%), they can be life-threatening, with a 30-day mortality rate of 45% to 70%. A meta-analysis of 9,251 patients collected during the first decade of TAVI procedures found that the incidence of emergency CS during transarterial TAVI was around 1.1±1.1% [11]. The evolution of transfemoral TAVI has been marked by significant advancements, including the development of new generation valves, improved procedural planning, better complication prediction, and refined implantation techniques. These improvements have made the procedure much safer. Recent data show that the incidence of emergency CS is extremely low, at 0.4% to 0.7% [1,2]. These findings support the feasibility of performing selected TAVI procedures without on-site cardiac surgery, potentially reducing waiting time risks. The goal of this study is to evaluate the feasibility, safety, and outcomes of performing a TAVI program in a cardiology department without an on-site CS department, in collaboration with a remote hospital that has surgical backup.
Methods
Study Selection, Data Abstraction, and Validity Assessment and Analysis
This study included consecutive aortic stenosis patients treated at the valve clinic of Meir Medical Center (Kfar Saba, Israel) who underwent TAVI between November 2019 and December 2023. All patients were evaluated by a multidisciplinary heart team, including an interventional cardiologist, cardiothoracic surgeon, and cardiac imaging specialist, to determine their eligibility for TAVI. Assessments included clinical evaluations, complete echocardiography, and ECG-gated computerized tomography (CT) scans for annular measurements, calcium scores, and vascular access evaluations, in accordance with current guidelines.
The procedure was performed in a hospital affiliated with our healthcare organization (Clalit Health System). This facility is equipped solely with a cardiac operating room; however, it lacks a dedicated cardiac surgery department and specialized surgical staff. TAVI procedures were conducted with cardiac surgical backup provided by a remote team, which was available to arrive at the hospital if needed.
The procedures were conducted by experienced operators and staff using transfemoral access under local anesthesia and mild sedation. Device selection and sizing were determined by the heart team based on multidetector computed tomography (MDCT) and echocardiography results. A successful TAVI procedure was defined by the Valve Academic Research Consortium 2 (VARC 2) criteria [12], including correct valve placement, proper valve function, and the absence of major complications.
Patients were monitored post-procedurally at our hospital, and those with stable conditions were discharged following routine follow-up protocols. Data were collected on baseline characteristics, procedural outcomes, immediate post-operative results, complications, and 1-year mortality. Follow-up visits were conducted at the TAVI outpatient clinic one month after the procedure. Data on 30-day outcomes were gathered from follow-up visits and rehospitalization records.
Study Endpoints
The study’s endpoints were based on the Valve Academic Research Consortium-2 (VARC-2) criteria [12]. The primary endpoint was device success, defined by the absence of procedural mortality, accurate valve placement, and the absence of significant valve gradients or regurgitation. Secondary endpoints included cardiovascular death, all-cause mortality, and early safety measures such as stroke, bleeding, and vascular complications at 30 days and 1 year. Valve safety was assessed by evaluating valve degeneration, dysfunction, endocarditis, thrombosis, thromboembolic events, and bleeding events related to valve therapy.
Statistical Analysis
A retrospective analysis was performed on the patients who underwent TAVI between November 2019 and December 2023. Demographic and clinical baseline characteristics, as well as procedural parameters, were presented as absolute numbers and percentages. Continuous variables were expressed as mean and standard deviation or as median and interquartile range. Statistical analyses were conducted using SPSS/PC statistical software. The study was approved by an ethics committee and adhered to the principles outlined in the Declaration of Helsinki.
Results
The baseline characteristics are detailed in Table 1. The study population consisted of 149 patients with a mean age of 80.5±6.4 years, of which 50% were female. The mean STS score was 4.3 ± 2.9, the mean EuroSCORE II was 3.1 ± 2.2, and 45.6% of patients were in a NYHA functional class III-IV. A significant proportion (55%) of patients had a history of coronary artery disease (CAD), 28% had chronic kidney disease (CKD), and 17% had peripheral vascular disease (PVD). About half (45%) of the study population had diabetes, a quarter (25%) had atrial fibrillation (AF), and the minority (7%) had a permanent pacemaker before the procedure.
In pre-procedural echocardiography (Table 1), the mean aortic gradient was 46.9±15.5mmhg, and the mean calculated aortic valve area was 0.75±0.15 cm^2. The pre-procedural CT Analysis showed a mean calcium score of 2065±610 and a mean Annular Perimeter of 76.8±6.5. All TAVI procedures were carried out under local anesthesia and mild sedation. All procedures were performed with trans-femoral access. Among the valve types used in this study, Acurate neo 2 was the most common (38%), followed by Sapian-3 (29%), Evolut-PRO (28%), and Nvitor (5%) (Figure 1). Few (4.7%) patients received TAVI in a bioprosthetic valve (Table 2). The hemostasis for the large bore access site was predominantly achieved using Prostyle and Angioseal (57%), and the rest was Prostyle alone (14%) or Manta (28%). During the procedure, no cases of emergency surgery, annular rupture, coronary obstruction, or tamponade were observed (Table 2). We had one case of valve embolization to the thoracic aorta that was resolved percutaneously with implantation of another valve in the aortic position.
The average discharge time was 2.1 ± 1.7 days, with the majority of patients discharged within a median time of two days. Clinical outcomes are detailed in Table 3 and Figure 2. No cases of in-hospital mortality, periprocedural MI, or stroke were reported during the study period. We identified one case (0.6%) of a major vascular event, specifically a pseudoaneurysm in the groin, complicated by significant bleeding. This was managed conservatively without surgical intervention. Additionally, there were two cases of major bleeding events: one involved upper gastrointestinal bleeding treated endoscopically with blood transfusion, and the other was a hematoma in the groin managed conservatively with blood transfusion. In total, there were three cases (2%) of major bleeding events observed, and there were no instances of mortality among these patients during the one-year follow-up period. Seven (4.7%) patients required new pacemaker Implantation. Post procedural mean aortic gradient was 11±6 mmHg, and no cases of significant peri-valvular leak (PVL) were observed in post-procedural echocardiography (Table 3).
During the first 30 days following the procedure, one patient died from a non-cardiac cause, two patients (1.3%) had stroke, and 7 patients (4.7%) were hospitalized duo to a cardiovascular cause (Table 3). Six patients died during the first year of follow-up, with only one due to a cardiac cause. Among the non-cardiac deaths, one patient died from pneumonia, one from pancreatic cancer, another from sepsis, a fourth from renal disease, and another from an unknown cause (Table 3).
Discussion
In this study, we examined a cohort of 149 patients with symptomatic severe aortic valve stenosis who underwent transfemoral TAVI, following a structured program. This program included heart team discussions, TAVI procedures performed at a center without cardiac surgical unit on-site but with remote surgical backup. Our study demonstrated encouraging outcomes, with no cases of emergency cardiac surgery, low complication rates, and successful procedural characteristics. We observed no instances of moderate to severe paravalvular leaks, only one major vascular complication, and no in-hospital mortality. During the entire follow-up period, only one patient died from a cardiac-related cause. These results highlight the efficacy and safety of our TAVI program, even in the absence of an on-site cardiac surgery department.
Despite the increasing maturity of TAVI, it remains a procedure with the potential for life-threatening complications [13]. Earlier studies conducted about a decade ago reported the need for emergent cardiac surgery in 1-5% of cases [14,15], whereas more recent studies show this requirement in less than 1% of cases [1,2,16]. This rate is expected to decline further with advancements in operator experience, procedural planning, and the development of repositionable TAVI systems and improved valve designs. In our study, no cases required conversion to cardiac surgery during or after the procedure.
A large German study (AQUA) [16] compared the outcomes of transfemoral TAVI at hospitals with and without on-site cardiac surgery departments. Patients undergoing TAVI at hospitals without cardiac surgery were older and had more comorbidities. However, the incidence of severe intraprocedural complications (such as annular rupture, aortic dissection, coronary obstruction, and device embolization) was rare (<1%) and actually lower in patients treated at hospitals without on-site cardiac surgery departments. In a separate analysis by Eggebrecht et al. [16] of more than 1,000 TAVI patients treated at hospitals without on-site cardiac surgery, it was shown that the heart teams at these non-CS sites selected patients similarly to those at CS sites. Procedural outcomes regarding in-hospital complications and mortality did not differ statistically between institutions with and without on-site cardiac surgery departments. In accordance with those studies and with our results, a recent Meta-analysis showed that outcomes of patients undergoing TAVI at institutions without on-site CS are similar to centers with CS department on-site [17].
In our study, there were no in-hospital deaths or major complications. However, as mentioned, one major procedural complication with a potential need for urgent surgery was observed and treated percutaneously during the index procedure. This underscores the importance of highly experienced and skilled TAVI teams, especially when on-site cardiac surgery is unavailable.
Over time, there has been a consistent reduction in the length of hospital stays following TAVI, regardless of patient’s surgical risk. Early discharge protocols, such as those outlined in the Vancouver 3M and FAST-TAVI registries, are expected to further reduce hospital stays following TAVI [18,19]. The (R-) EXPRESS program has demonstrated the feasibility of early discharge, either to home or a referral hospital, while maintaining safety and optimizing TAVI programs. This program reported a median length of stay of two days [20]. Similarly, our study revealed a median length of stay of two days.
Nowadays, while the complication rate mandating urgent surgery is lower than 0.5%. Therefore, we believe that the presence of on-site CS is not the primary safety concern [17]. Instead, the critical factors include thorough procedure planning, pre- and post-operative evaluations, and collaboration among the heart team. TAVI programs without on-site cardiac surgery should be done by an experienced centers with teams familiar with all stages of planning and performing the procedure and post-procedural care, including prompt recognition of postoperative cardiac and non-cardiac complications. When these conditions are met, the procedure can be performed safely, even without on-site CS. Implementing TAVI in centers without on-site cardiac surgery presents unique challenges but also opportunities for innovation in patient care. Our experience demonstrated that, with careful planning and collaboration, these challenges can be overcome, leading to outcomes comparable to those seen in centers with cardiac surgery departments.
Study Limitations
Our study has several notable limitations. First, there is a potential selection bias due to the early phase of our TAVI program. As this program was newly established at our hospital, the initial cases involved relatively uncomplicated patients to ensure procedural safety and optimize outcomes. However, we did not exclude any patients based on risk profile, and this study presents the first 150 consecutive patients treated at our center. Future studies with a broader and more complex patient population will be necessary to further validate our findings.
Additionally, this is a single-center, retrospective, non-randomized observational study, which may introduce biases. The distribution of different valve types used for TAVI could also influence outcomes, and we were unable to evaluate the impact of potential differences in valve selection on major complications, post-implantation paravalvular leak, or pacemaker rates. Lastly, our analysis is limited to evaluating in-hospital and 1-year outcomes, as we had no data regarding longer-term follow-up.
Conclusions
This study demonstrates favorable outcomes for patients undergoing transfemoral TAVI in institutions without an onsite cardiac surgery department, with strong safety profiles and without heightened risk to patients. Our successful TAVI program highlights the potential for similar models in other institutions. Nevertheless, research involving larger patient cohorts is warranted.
Trial identification number 0032-23-MMC
Funding
This research received no funding.
References
- Eggebrecht, H.; Vaqueirzo, B.; Moris, C.; et al. Incidence and outcomes of emergency cardiac surgery during transfemoral transcatheter aortic valve implantation (TAVI): insights from the European Registry on Emergent Cardiac Surgery during TAVI (EuRECS-TAVI). Eur Heart J 2018, 39, 676–684. [Google Scholar] [CrossRef] [PubMed]
- Auffret, V.; Lefevre, T.; Van Belle, E.; et al.; FRANCE TAVI Investigators Temporal Trends in Transcatheter Aortic Valve Replacement in France: FRANCE 2 to FRANCE TAVI. J Am Coll Cardiol. 2017, 70, 42–55. [Google Scholar] [CrossRef] [PubMed]
- Okuno, T.; Asami, M.; Heg, D.; et al. Impact of Left Ventricular Outflow Tract Calcification on Procedural Outcomes After Transcatheter Aortic Valve Replacement. JACC Cardiovasc Interv. 2020, 13, 1789–1799. [Google Scholar] [CrossRef] [PubMed]
- Zahid, S.; Rai, D.; Tanveer Ud Din, M.; et al. Same-Day Discharge After Transcatheter Aortic Valve Implantation: Insights from the Nationwide Readmission Database 2015 to 2019. J Am Heart Assoc. 2022, 11, e024746. [Google Scholar] [CrossRef] [PubMed]
- Scarsini, R.; De Maria, G.L.; Joseph, J.; et al. Impact of Complications During Transfemoral Transcatheter Aortic Valve Replacement: How Can They Be Avoided and Managed? J Am Heart Assoc. 2019, 8, e013801. [Google Scholar] [CrossRef] [PubMed]
- Langer, N.B.; Hamid, N.B.; Nazif, T.M.; et al. Injuries to the Aorta, Aortic Annulus, and Left Ventricle During Transcatheter Aortic Valve Replacement: Management and Outcomes. Circ Cardiovasc Interv. 2017, 10, e004735. [Google Scholar] [CrossRef] [PubMed]
- Ali, N.; Faour, A.; Rawlins, J.; et al. ‘Valve for Life’: tackling the deficit in transcatheter treatment of heart valve disease in the UK. Open Heart. 2021, 8, e001547. [Google Scholar] [CrossRef] [PubMed]
- Elbaz-Greener, G.; Masih, S.; Fang, J.; et al. trends and clinical consequences of wait times for transcatheter aortic valve replacement: a population-based study. Circulation. 2018, 138, 483–493. [Google Scholar] [CrossRef] [PubMed]
- Vahanian A, Beyersdorf F, Praz F, et al. ; ESC/EACTS Scientific Document Group. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2022, 43, 561–632. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.K.; Schäfer, U.; Tchetche, D.; et al. Incidence and outcome of peri-procedural transcatheter heart valve embolization and migration: the TRAVEL registry (TranscatheteR HeArt Valve EmboLization and Migration). Eur Heart J. 2019, 40, 3156–3165. [Google Scholar] [CrossRef] [PubMed]
- Eggebrecht, H.; Schmermund, A.; Kahlert, P.; et al. Emergent cardiac surgery during transcatheter aortic valve implantation (TAVI): a weighted meta-analysis of 9,251 patients from 46 studies. EuroIntervention. 2013, 8, 1072–80. [Google Scholar] [CrossRef] [PubMed]
- Kappetein AP, Head SJ, Généreux P, et al. ; Valve Academic Research Consortium (VARC)-2. Updated standardized endpoint definitions for transcatheter aortic valve implantation: the Valve Academic Research Consortium-2 consensus document (VARC-2). Eur J Cardiothorac Surg. 2012, 42, S45–S60. [Google Scholar] [CrossRef] [PubMed]
- Mylotte, D.; Head, S.J.; Kappetein, A.P.; et al. TAVI at institutions without cardiovascular surgery departments: why? EuroIntervention. 2014, 10, 539–41. [Google Scholar] [CrossRef] [PubMed]
- Eggebrecht, H.; Mehta, R.H.; Kahlert, P.; et al. Emergent cardiac surgery during transcatheter aortic valve implantation (TAVI): insights from the Edwards SAPIEN Aortic Bioprosthesis European Outcome (SOURCE) registry. EuroIntervention. 2013. [Google Scholar] [CrossRef] [PubMed]
- Griese, D.P.; Reents, W.; Kerber, S.; et al. Emergency cardiac surgery during transfemoral and transapical transcatheter aortic valve implantation: incidence, reasons, management, and outcome of 411 patients from a single center. Catheter Cardiovasc Interv. 2013, 82, E726–E733. [Google Scholar] [CrossRef] [PubMed]
- Eggebrecht, H.; Bestehorn, M.; Haude, M.; et al. Outcomes of transfemoral transcatheter aortic valve implantation at hospitals with and without on-site cardiac surgery department: insights from the prospective German aortic valve replacement quality assurance registry (AQUA) in 17 919 patients. Eur Heart J. 2016, 37, 2240–2248. [Google Scholar] [CrossRef] [PubMed]
- Compagnone, M.; Dall’Ara, G.; Grotti, S.; et al. Transcatheter Aortic Valve Replacement Without On-Site Cardiac Surgery: Ready for Prime Time? JACC Cardiovasc Interv. 2023, 16, 3026–3030. [Google Scholar] [CrossRef] [PubMed]
- Wood, D.A.; Lauck, S.B.; Cairns, J.A.; et al. The Vancouver 3M (Multidisciplinary, Multimodality, But Minimalist) Clinical pathway facilitates safe next-day discharge home at low-, medium-, and high-volume transfemoral transcatheter aortic valve replacement centers: The 3M TAVR Study. JACC Cardiovasc Interv 2019, 12, 459–469. [Google Scholar] [CrossRef] [PubMed]
- Barbanti, M.; van Mourik, M.S.; Spence, M.S.; et al. Optimising patient discharge management after transfemoral transcatheter aortic valve implantation: the multicentre European FAST-TAVI trial. EuroIntervention 2019, 15, 147–154. [Google Scholar] [CrossRef] [PubMed]
- van Wiechen, M.P.; de Ronde-Tillmans, M.J.; Van Mieghem, N.M. Referring hospital involvement in early discharge post transcatheter aortic valve implantation: the TAVI (R-) EXPRES program. Mini-invasive Surg 2022, 6, 1. [Google Scholar] [CrossRef]

Table 1.
Characteristics of the Patients at Baseline.
| Variable | N=149 |
|---|---|
| Age (y) (mean ± SD) | 80.5±6.4 |
| Female no. (%) | 75 (50.3%) |
| Body-mass index (mean ± SD) | 28 ± 7.1 |
| STS score (mean ± SD) | 4.36 ± 2.96 |
| EuroSCORE II score (mean ± SD) | 3.16 ± 2.27 |
| NYHA class III/IV no. (%) | 68 (45.6%) |
| Previous myocardial infarction no. (%) (N=131) | 15 (11.4%) |
| Coronary artery disease no. (%) | 83 (55.7%) |
| Prior PCI no. (%) | 50 (33.5%) |
| Peripheral vascular disease (%) | 26 (17.45%) |
| Previous Valvular surgery no. (%) | 9 (6%) |
| Hypertension no. (%) | 125 (84%) |
| Previous stroke no. (%) | 20 (13.4%) |
| Diabetes Mellitus, no. (%) | 68 (45.6%) |
| Hyperlipidemia, no. (%) | 130 (87.2%) |
| Atrial fibrillation no. (%) | 38 (25.5%) |
| COPD no. (%) | 25 (16.8%) |
| CKD (eGFR <60 ml/min/1.73 m2) no. (%) | 41 (27.5%) |
| Anemia (Hg <10 mg/dl) no. | 76 (51%) |
| Permanent pacemaker no. (%) (N=134) | 10 (7.4%) |
| Echocardiographic data | |
| Aortic valve area, (cm^2) | 0.75±0.15 |
| Max Aortic-valve gradient, (mm Hg) | 75 ± 23.3 |
| Mean Aortic Gradient, (mm Hg) | 46.9 ± 15.5 |
| LVEF, % | 57.8 ± 9.9 |
| CT Analysis | |
| Calcium, Score (mean ± SD) Annular | 2065 ± 610 |
| Annular Perimeter (mean ± SD) | 76.85 ± 6.57 |
Table 2.
Procedural Characteristics and intra procedural complications.
| Variables | N=149 |
|---|---|
| Valve type | no. (%) |
| Evolut-PRO | 41 (27.5%) |
| Sapian-3 | 43 (28.8%) |
| Acurate neo 2 | 57 (38.2%) |
| Navitor | 8 (5.4%) |
| Valve in bioprosthetic valve (%) | 7 (4.7%) |
| Closure device* (valve access only) (%) | |
| Prostar / Proglide | 21 (14.1%) |
| Prostar / Proglide + Angioseal | 86 (57.7%) |
| Manta | 42 (28.2%) |
| Intra procedural complications | |
| Conversion to surgery | 0 (0%) |
| Emergent surgery | 0 (0%) |
| Need for a second valve | 1 (0.67%) |
| Coronary obstruction | 0 (0%) |
| Cardiac tamponade | 0 (0%) |
| Annular rupture | 0 (0%) |
| Valve migration/embolization | 1 (0.67%) |
Values are N(%).
Table 3.
In hospital, 30days and 1-year outcomes.
| In hospital outcomes | N=149 |
|---|---|
| In Hospital Death | 0 (0%) |
| Peri-procedural MI | 0 (0%) |
| Stroke | 0 (0%) |
| Major vascular complication | 1 (0.67%) |
| Major bleeding (Type 2 >=BARC 3) | 4 (2.68%) |
| Permanent pacemaker implantation | 7(4.7%) |
| Acute renal failure | 5 (3.36%) |
| Hemodialysis | 0 (0%) |
| Time to discharge (days, mean+/-SD) | 2.1 ± 1.7 |
| Echocardiographic finding – in hospital pos procedural evaluation | |
| Ejection fraction (mean+/-SD) | 60±8 |
| mean aortic-valve gradient, mm Hg (mean+/-SD) | 11.25±6.2 |
| Moderate or severe AR | 0 (0%) |
| 30 Days outcomes | |
| Mortality | 1/149 (0.67%) |
| Myocardial Infarction | 2/149 (1.34%) |
| Stroke | 2/149 (1.34%) |
| Cardiovascular hospitalization HALT Endocarditis Acute coronary syndrome Heart Failure |
7/149 (4.7%)1 (0.67%)1 (0.67%)2(1.34%)3(2%) |
| Non-cardiovascular Hospitalization | 14 (9.39%) |
| Mortality - 1 Year | |
| Total | 6/149 (4.0%) |
| Non-Cardiac | 5/149 (3.36%) |
| Cardiac | 1/149 (0.67%) |
Values are N(%) or mean ± SD.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



