
Submitted:
24 April 2025
Posted:
25 April 2025
You are already at the latest version
Abstract
Background/Objectives: We have defined severe postpartum hemorrhage (PPH) complicated with hematuria as clinical disseminated intravascular coagulation (DIC) and reported a methodology, using artificial intelligence, for developing the boundary criterion for predicting hematuria on the fibrinogen–fibrin/fibrinogen degradation products (FDP) plane: a positive FDP–fibrinogen/3–60 (mg/dL) value indicates hematuria, otherwise, non-hematuria. We aimed to validate this criterion using severe placental abruption (PA), as the criterion was developed using PPH except for PA, and to examine the coagulation–fibrinolytic system activation in clinical DIC. Methods: Of 17,285 deliveries assessed, 13 had severe PA without hematuria, 18 severe PPH without hematuria, and three severe PPH with hematuria, i.e., clinical DIC. Cases were obtained from nine national perinatal centers in Japan between August 2020 and June 2024. We calculated the values for 13 severe PA cases using the criterion and compared the laboratory tests for coagulation–fibrinolytic activation including thrombin–antithrombin complex (TAT) and plasmin-α2–plasmin inhibitor complex (PIC) among the three groups. Results: The calculated values using the criterion for the 13 PA without hematuria were all negative. In clinical DIC cases, fibrinogen (median, 62 mg/dL) was lower, and FDP (median, 96 mg/dL), TAT (median, 120 ng/mL ), and PIC (median, 28.4 μg/mL) were significantly higher than in the other two groups. Conclusions: The criterion accurately diagnosed all PA without clinical hematuria as non-hematuria. The coagulation–fibrinolysis test results demonstrated the validity of considering cases with hematuria as clinical DIC. The criterion appears useful for diagnosing clinical DIC during delivery.
Keywords:
disseminated intravascular coagulation
; fibrinogen
; fibrin/fibrinogen degradation products
; macroscopic hematuria
; placental abruption
; plasmin-α2–plasmin inhibitor complex
; postpartum hemorrhage
; thrombin–antithrombin complex
1. Introduction
Disseminated intravascular coagulation (DIC) is a life-threatening condition, and which means that an appropriate diagnosis is extremely important in order to provide early treatment, thus, proper diagnostic criteria play a key role. The International Society of Thrombosis and Haemostasis (ISTH) [1], Japanese Association for Acute Medicine [2], and Japanese Society on Thrombosis and Hemostasis [3], have respectively established three diagnostic criteria for DIC in the non-pregnant state. Enhanced coagulation activation is a major pathophysiology in DIC, regardless of the underlying disease. However, the degree of fibrinolytic activation differs depending on the underlying disease, which is an important factor in characterizing DIC [4,5]. Suppressed-fibrinolytic-type DIC is typically seen in sepsis [4,5]. However, enhanced-fibrinolytic-type DIC seen in acute promyelocytic leukemia and obstetrical DIC including placental abruption (PA), amniotic fluid embolism (AFE), and postpartum hemorrhage (PPH) [4,5,6,7,8], is characterized by marked fibrinolytic activation. In such activation, fibrinogen levels decrease and fibrin/fibrinogen degradation products (FDP) levels increase [9,10,11]. Seen through clinical findings, hematuria is an important symptom reflecting marked fibrinolytic activation in human [12,13,14] and animal models [4]. DIC, if severe enough, also can cause organ dysfunction [1] and cases of PPH with hematuria also could be assumed to be organ dysfunction [15]. Considering the above, the occurrence of hematuria associated with PPH as clinical DIC requires defining.
For DIC diagnosis in obstetrics, the pregnancy-modified ISTH DIC score was developed in 2014 [16] and the new Japanese diagnostic criteria (tentative version) for obstetrical DIC were released in 2022 [17]. However, international consensus has yet to be reached [8]. In our previous study, among 13,368 total deliveries, 23 patients with PPH with > 2,000 mL of blood loss and fibrinogen <170 mg/dL were observed, including three patients with PPH with hematuria, in whom fibrinogen greatly decreased and FDP greatly increased, showing highly abnormal values on the fibrinogen–FDP plane compared with the non-hematuria cases [15]. These clinical and laboratory findings indicated that cases with hematuria might be diagnosed as clinical DIC. Miyagi et al. [15] used artificial intelligence to develop boundary formula for predicting hematuria dividing the fibrinogen–FDP plane: a positive FDP–fibrinogen/3–60 (mg/dL) value indicates hematuria, otherwise it is non-hematuria. This formula can also be considered as a criterion for predicting clinical DIC.
PA is a typical obstetrical condition that cause DIC, with only severe forms thought to be associated with DIC [10,13,18]. Although the cohort data used to develop the boundary criterion for predicting hematuria proposed by Miyagi et al. [15], included a considerable number of PA cases, the criterion’s feasibility in PA cases remains unconfirmed. Therefore, in this study, we aimed to validate the criterion using severe cases of PA with fibrinogen < 170 mg/dL, which was the threshold criterion for coagulation system failure [19]. There is also value in understanding the pathophysiology of other severe obstetrical conditions, except for DIC, to characterize the abnormalities observed during DIC. Thus, we compared the laboratory tests values for coagulation–fibrinolytic activation in cases of severe PA with or without hematuria and severe PPH with or without hematuria to clarify the characteristics of the coagulation–fibrinolytic profile in conditions related to acute hemorrhage and/or coagulopathy during delivery.
2. Materials and Methods
2.1. Design and Study Population
This was a multicenter prospective case series study of women who gave birth at any of the nine National Hospital Organization (NHO) perinatal centers in Japan between August 2020 and June 2024. Inclusion criteria were: (1) > 2,000 mL of blood loss within 24 hours of delivery, except for PA; (2) clinically diagnosed with PA irrespective of blood loss; (3) any mode of delivery, vaginal or cesarean section (C/S); (4) singleton or multiple pregnancies; and (5) delivery after 22 weeks of gestation. Our rationale for inclusion criteria 1 and 3 was that it is unusual to develop coagulopathy when blood loss is ≤ 2,000 mL [20]. Women with bleeding > 2,000 mL at delivery, regardless of delivery mode, also are defined by the Royal College of Obstetrics and Gynaecologists as having severe PPH [21]. The exclusion criteria were women with medical complications that could cause coagulopathy and women taking medications that affect the coagulation system, such as aspirin.
Because we developed criterion for predicting hematuria using PPH cases with fibrinogen < 170 mg/dL, the criterion for coagulation system failure [19], this study also included both PPH and PA cases with fibrinogen < 170 mg/dL. We then classified the included PPH and PA cases into those with or without hematuria.
2.2. Clinical Data and Laboratory Tests
During vaginal delivery, blood loss was weighed using the blood-soaked pad and/or from direct blood collection using a collector bag placed under the woman’s buttocks. During cesarean delivery, blood-soaked surgical pads were weighed and/or blood volume aspirated from the surgical field with a suction tube was determined in milliliters. Measured blood loss was standardized in milliliters (mL), because one gram approximately equals the weight of 1 mL. Obstetrical management, blood products transfusion, and determination of the cause of bleeding were performed at the discretion of the attending physicians at each center, and a hematuria case in this study was defined as one that a physician diagnosed as macroscopic hematuria (MH).
The attending physicians obtained blood samples when deemed clinically necessary, regardless of blood loss. Hemoglobin, platelet count, prothrombin time-international normalized ratio, fibrinogen, FDP, and D-dimer were measured in each center’s laboratory for clinical management. The levels of thrombin–antithrombin complex (TAT), a sensitive molecular marker of coagulation activation [22], and plasmin-α2–plasmin inhibitor complex (PIC), a sensitive marker of fibrinolytic activation [22], were also measured in the SRL INC. (Tokyo, Japan) laboratories for this study. Working ranges for the FDP and TAT assay were ≤ 96 mg/dL and ≤ 120 ng/mL, respectively. We used Data from the first measurement after delivery for each patient for analysis. Data used in this study were fully deidentified.
2.3. Validation of the Boundary Criterion for Predicting Hematuria and Comparison of Coagulation–Fibrinolytic Activation in Each Group
To validate the boundary criterion for predicting hematuria, we used the following formula to calculate the value for severe PA cases with fibrinogen <170 mg/dL; if the calculated value of the formula “FDP–fibrinogen/3–60 (mg/dL)” was positive, the case was diagnosed with hematuria; otherwise, non-hematuria [15]. We then examined whether the results obtained using the formula were consistent with the clinical hematuria complications in each case.
Additionally, to elucidate the characteristics of the coagulation–fibrinolytic system activation in severe PA cases with or without hematuria and severe PPH cases with or without hematuria, we compared fibrinogen, FDP, TAT, and PIC levels among these groups.
2.4. Data Analysi
All anonymized data from each center were analyzed at the NHO Okayama Medical Center. Continuous variables are reported with the median and range. Categorical variables are reported as counts with percentages. In Figure 3 and Figure 4, the boxes represent the 25th and 75th percentiles, and the whiskers are the maximum and minimum values. For comparison among the three groups, we used the Kruskal–Wallis test and χ2 test for the continuous and categorical variables, respectively. We used the Mann–Whitney test for the continuous variables for comparison between the two groups. We used GraphPad Prism 8.4.3 (GraphPad Software, San Diego, CA) for all analyses, with p < 0.05 set as the level of significance.
This study was approved by the NHO Central Research Ethics Committee (R1-1009002, February 7, 2020) and conducted with reference to the STROBE statement [23].
3. Results
During the study period, 159 cases of PPH with blood loss > 2,000 mL at delivery, except for PA, and 56 cases of PA regardless of blood loss at delivery, were enrolled from among 17,285 deliveries at all participating centers. Of these women, 131 with PPH and 40 with PA fulfilled the inclusion criteria, and were enrolled for final sample (Figure 1).
The boundary criterion for predicting hematuria was developed using data from August 2020 to September 2023 from the cohort data in this study [15]. Of the 107 PPH cases during the period, 23 with fibrinogen < 170 mg/dL were used to develop the criterion; these included two cases of PA with blood loss > 2,000 mL and with fibrinogen < 170 mg/dL. Because no cases with PPH with fibrinogen < 170 mg/dL were enrolled from September 2023 onward, this study had 21 cases of PPH except for PA, of which three had MH (MH group) and 18 did not (PPH group). Of 40 cases of PA, 13 cases with fibrinogen < 170 mg/dL were observed, none of which had MH (PA group) (Figure 1).
Table 1 shows the clinical characteristics in the three groups. Of 13 cases in the PA group, 12 underwent emergency C/S because of deterioration of fetal heart rate monitoring, such as recurrent late deceleration, severe prolonged deceleration, bradycardia, thus, both the Apgar score (median, 1 point) and umbilical arterial pH (median, 7.045) in the PA group were low. Two of three women in the MH group had complicated hypertensive disorders of pregnancy (one with mild gestational hypertension and one with mild preeclampsia) and underwent emergency C/S at 37 and 38 weeks of gestation, respectively, because of elevated blood pressure. Another one underwent elective C/S at 32 weeks of gestation because of fetal indication and was diagnosed with adherent placenta intraoperatively.
The calculated values using the boundary criterion formula for 13 cases in the PA group ranged from –108.91 to –5.87 (median, –73.34), all were negative, and all cases were diagnosed as non-hematuria. Therefore, when the (fibrinogen, FDP) coordinates of each case in the PA group (△) were plotted on the fibrinogen–FDP plane on which the boundary for predicting hematuria was shown as the solid line, all cases were under the boundary (Figure 2).
Table 2 shows the comparison of laboratory tests results and clinical data among the three groups. For the laboratory tests, there were significant differences for hemoglobin, prothrombin time–INR, fibrinogen, FDP, D-dimer, and PIC. Hemoglobin levels in the PPH group were lower (p < 0.01) than in the PA group. FDP and PIC levels in the PA group were higher (both p < 0.05) than in the PPH group, but D-dimer and TAT levels did not differ between the two groups. For the clinical data, there were significant differences for blood loss at initial blood sampling and total blood loss among the three groups, and both items in the PPH group were higher (p < 0.01, p < 0.0001) than in the PA group, but the administration volume of blood products and clear fluids did not differ between the two groups.
Fibrinogen levels differed (p < 0.05) among the three groups (Table 2), and those in the MH group were significantly lower than in the other two groups (Figure 3A). TAT and PIC were measured in 11 of 13 cases in the PA group. TAT levels did not differ (p = 0.054) among the three groups (Table 2); however, TAT levels, all at the upper limit of measurement, in the MH group were higher (p < 0.05) than in the PA group and tended to be higher (p = 0.065) than in the PPH group (Figure 3B). TAT levels did not differ between the PA and PPH groups.
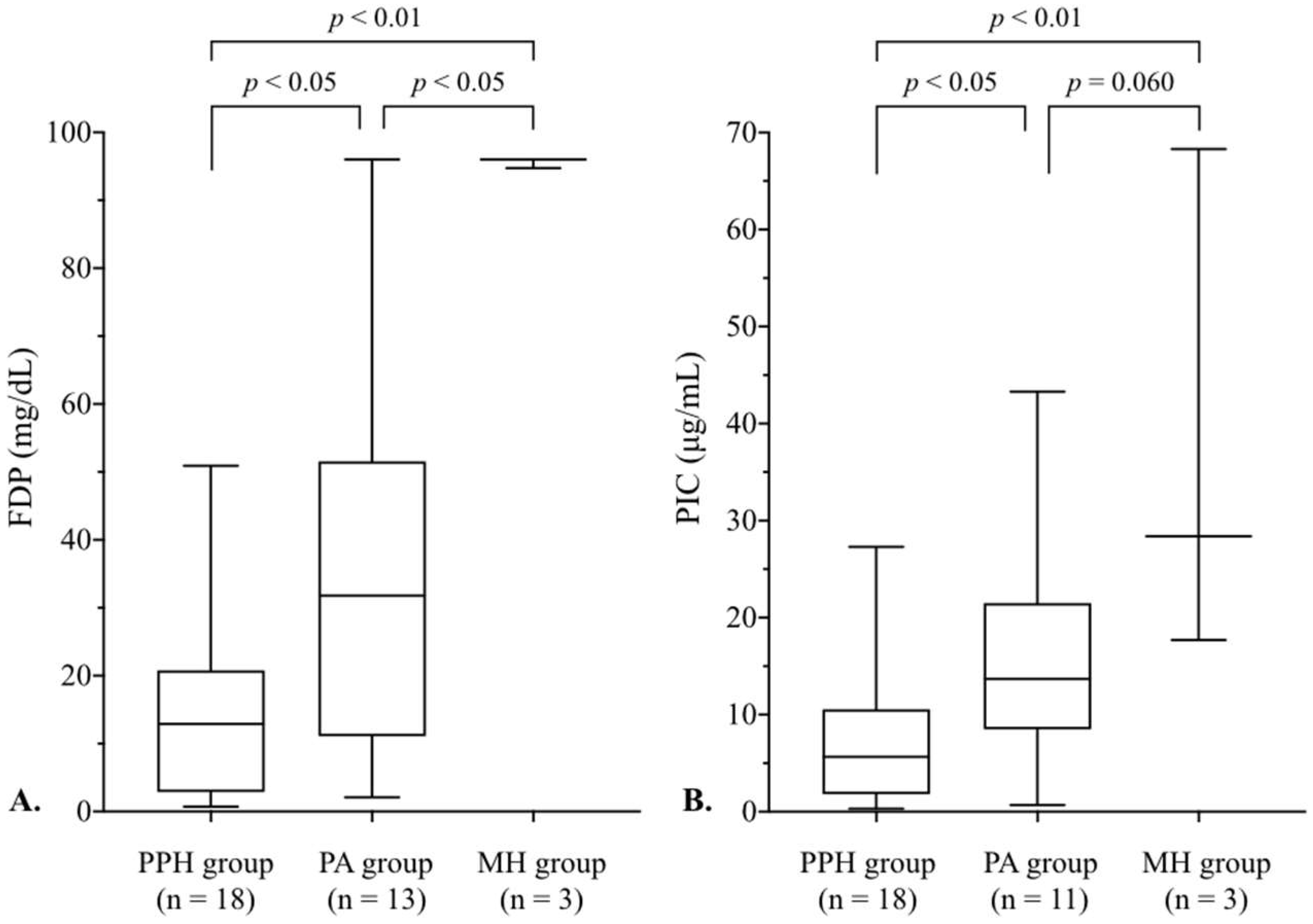
FDP and PIC levels differed (p < 0.01) among the three groups (Table 2). FDP levels in the MH group were significantly higher than in the other two groups, and those in the PA group were higher (p < 0.05) than in the PPH group (Figure 4A). PIC levels in the MH group were also higher than in the PPH group (p < 0.01) and tended to be higher (p = 0.060) than in the PA group (Figure 4 B). Additionally, PIC levels in the PA group were higher (p < 0.05) than in the PPH group.
Figure 3.
Comparison of fibrinogen and TAT levels among the three groups with fibrinogen < 170 mg/dL. Fibrinogen and TAT levels for each group are shown in box-and-whisker plots. Fibrinogen levels differed (p < 0.05) among the three groups, and fibrinogen levels in the MH group were significantly lower than those in the PPH and PA groups, respectively. TAT levels did not differ (p = 0.054) among the three groups; however, TAT levels in the MH group were higher (p < 0.05) than in the PA group. The differences among the three groups were analyzed using the Kruskal–Wallis test and those between the two groups were analyzed using the Mann–Whitney test. The PPH group indicates cases of PPH without MH except for PA, PA group is cases of PA without MH regardless of blood loss at delivery, and MH group is cases of PPH with MH except for PA. MH, macroscopic hematuria; PA, placental abruption; PPH, postpartum hemorrhage; TAT, thrombin–antithrombin complex.
Figure 3.
Comparison of fibrinogen and TAT levels among the three groups with fibrinogen < 170 mg/dL. Fibrinogen and TAT levels for each group are shown in box-and-whisker plots. Fibrinogen levels differed (p < 0.05) among the three groups, and fibrinogen levels in the MH group were significantly lower than those in the PPH and PA groups, respectively. TAT levels did not differ (p = 0.054) among the three groups; however, TAT levels in the MH group were higher (p < 0.05) than in the PA group. The differences among the three groups were analyzed using the Kruskal–Wallis test and those between the two groups were analyzed using the Mann–Whitney test. The PPH group indicates cases of PPH without MH except for PA, PA group is cases of PA without MH regardless of blood loss at delivery, and MH group is cases of PPH with MH except for PA. MH, macroscopic hematuria; PA, placental abruption; PPH, postpartum hemorrhage; TAT, thrombin–antithrombin complex.
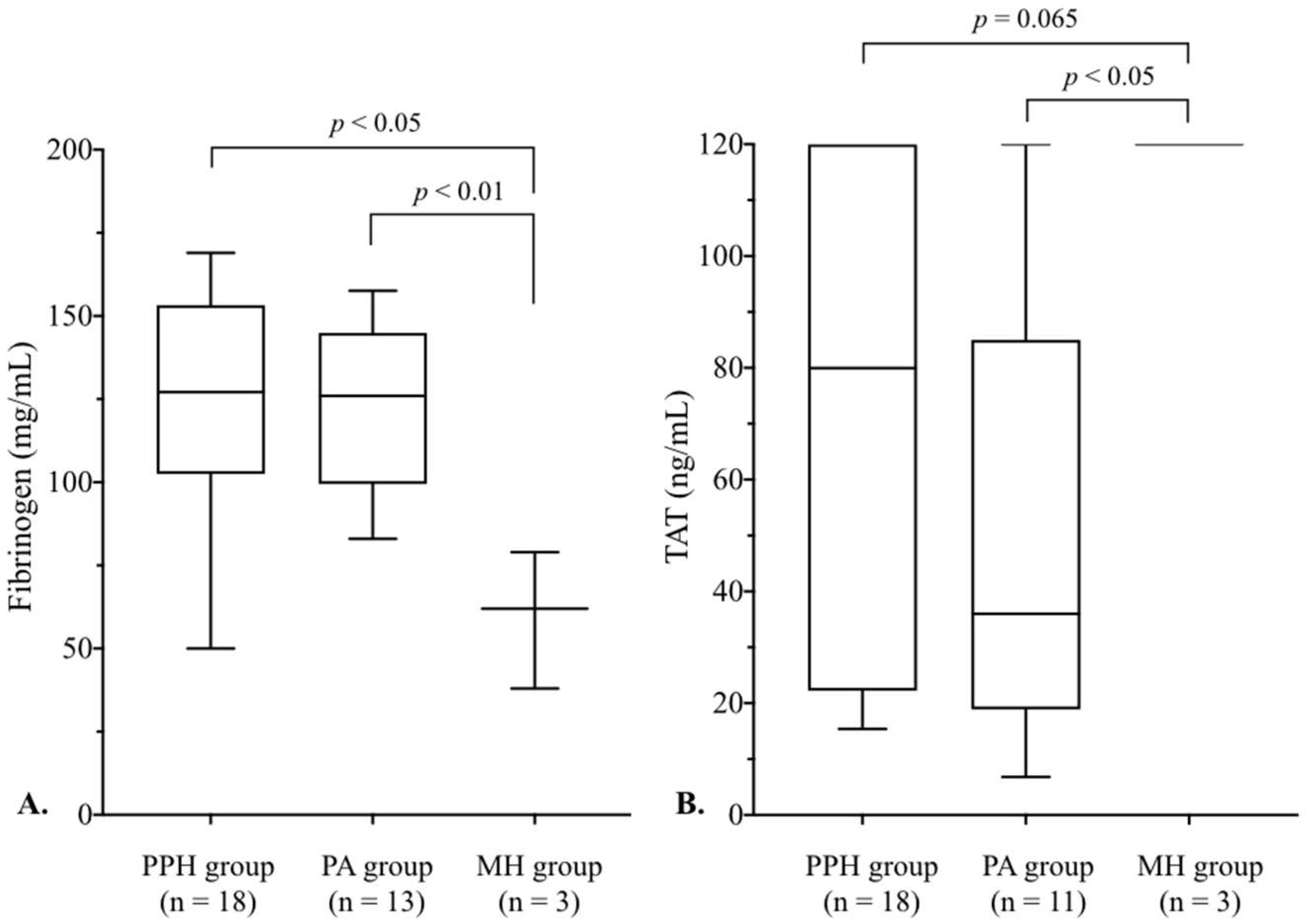
Figure 4.
Comparison of FDP and PIC levels among the three groups with fibrinogen < 170 mg/dL. FDP and PIC levels in each group are shown in box-and-whisker plots. FDP and PIC levels differed (p < 0.01) among the three groups. The differences among the three groups were analyzed using the Kruskal–Wallis test and those between the two groups were analyzed using the Mann–Whitney test. The PPH group indicates cases of PPH without MH except for PA, PA group is cases of PA without MH regardless of blood loss at delivery, and MH group is cases of PPH with MH except for PA. FDP, fibrin/fibrinogen degradation products; MH, macroscopic hematuria; PA, placental abruption; PIC, plasmin-α2–plasmin inhibitor complex; PPH, postpartum hemorrhage.
Figure 4.
Comparison of FDP and PIC levels among the three groups with fibrinogen < 170 mg/dL. FDP and PIC levels in each group are shown in box-and-whisker plots. FDP and PIC levels differed (p < 0.01) among the three groups. The differences among the three groups were analyzed using the Kruskal–Wallis test and those between the two groups were analyzed using the Mann–Whitney test. The PPH group indicates cases of PPH without MH except for PA, PA group is cases of PA without MH regardless of blood loss at delivery, and MH group is cases of PPH with MH except for PA. FDP, fibrin/fibrinogen degradation products; MH, macroscopic hematuria; PA, placental abruption; PIC, plasmin-α2–plasmin inhibitor complex; PPH, postpartum hemorrhage.
4. Discussion
This study demonstrated that the boundary criterion formula for predicting hematuria on a fibrinogen–FDP plane – i.e., FDP–fibrinogen/3–60 (mg/dL), proposed by Miyagi et al. [15] – accurately diagnosed all cases of severe PA without clinical hematuria as non-hematuria cases. The types of coagulopathies associated with bleeding during delivery are classified as dilutional or consumptive, with the latter further divided into local consumptive and DIC [10]. Most consumptive coagulopathy associated with PPH results from local consumption of coagulation factors, such as fibrinogen, to form hemostatic clots in the placental vascular bed (e.g., in many PA cases), in blood vessels within the uterine muscle (e.g., in uterine atony), or in damaged vessels (e.g., in surgical or birth canal trauma) [10,24]. Most cases in the PPH and PA groups, both of which were non-DIC (Figure 2) corresponded to this condition. In some severe cases of the condition, fibrinogen levels considerably decreased and FDP levels considerably increased, though the coagulation–fibrinolytic system activation is considered to be localized to the uterus because these were non-DIC. DIC onset in obstetrics is not only related to the influx of massive tissue factors, a major initiator of the coagulation cascade, from damaged trophoblasts and damaged maternal decidua [25,26], but also to the involvement of the innate immune system [13,25], resulting in the systemic activation of coagulation with simultaneous activation of fibrinolysis. The cases in the MH group that were clinical DIC (Figure 2) corresponded to this condition, and in the group, by the time the attending physician requested a blood test, the fibrinogen and FDP levels were likely to already have reached the area for predicting hematuria due to the enhanced coagulation–fibrinolytic activation.
In the MH group, TAT levels were all at the upper limit of measurement, and PIC levels (median, 28.4 μg/mL) were extremely high compared with the other two severe obstetrical conditions (Figure 3 and 4). Additionally, PIC levels in this study were similarly high as those in recent reports [27], showing that median PIC values in clinically diagnosed AFE cases and PA cases with DIC were approximately 60 μg/mL and 10 μg/mL, respectively. As TAT and PIC is a molecular marker of thrombin generation and plasmin generation, respectively [22,28], these results illustrated the presence of enhanced coagulation–fibrinolytic activation, the main pathophysiology of enhanced-fibrinolytic-type DIC [4,5]. Moreover, FDP in the MH group was markedly elevated compared with the other two groups (Figure 4). D-dimer is a fibrin degradation product by plasmin, but FDP is a degradation product of fibrinogen and fibrin by plasmin. Therefore, extremely high FDP levels in the MH group reflected the enhanced fibrinogenolysis [28], resulting in a marked decrease in fibrinogen levels (Figure 3), consistent with the characteristics of laboratory tests in enhanced-fibrinolytic-type DIC [9,10,11]. Thus, these laboratory tests results including the TAT and PIC dynamics provided the rationale for considering cases with hematuria as clinical DIC.
The pathophysiology of DIC in sepsis is becoming clearer [7,29,30]. In septic DIC, common components of microbes and/or damage-associated molecular patterns (DAMPs) from damaged host cells by infection activate innate immune cells, such as monocytes. The activated immune cells then release inflammatory cytokines, which then systemically activate the coagulation system, leading to the development of DIC. During trauma, even though this is a non-infectious insult, DAMPs produced by post-traumatic cell damage can cause a systemic inflammatory syndrome through a mechanism similar to that of sepsis, leading to DIC [7,31]. In obstetrics, the development of DIC associated with AFE also involves the immune system [32]. Amniotic fluid contains components that function as DAMPs [33] and the immune system activated by these amniotic fluid components that enter the maternal circulation is involved in DIC onset [32]. In this study, all three cases with hematuria were delivered by C/S, and influx of amniotic fluid into the maternal circulation is an especially common phenomenon during C/S [32,34]. Additionally, in vitro data have shown that even a small amount of amniotic fluid can cause DIC [35,36]. Based on the above, the influx of amniotic fluid into the maternal circulation following C/S may have caused DIC in three cases in this study.
Regarding characteristics of the laboratory tests in the PA group, blood loss at the initial blood sampling in the PPH group (median, 2,598 mL) was greater (p < 0.01) than that in the PA group (median, 1,594 mL), and the dilutional factor contributed to a decrease in hemoglobin levels in the PPH group. However, fibrinogen levels were similarly low in both groups (Table 2, Figure 3A). Focusing on the coagulation and fibrinolysis system in the PA group, the TAT level did not differ from that in the PPH group (Figure 3B), but the fibrinolysis markers’ FDP and PIC levels were both significantly higher than in the PPH group (Figure 4), showing the highly activated fibrinolysis system in the PA group compared with the PPH group. Unlike PPH, which develops because of atony or birth canal injury without involvement of the immune system, disruption of immune processes in the decidua plays an important role in PA development, leading to a maternal immune response with the release of cytokines [26,37]. Considering that some severe PA cases develop enhanced-fibrinolytic-type DIC [10,13,18], PA may cause hyperfibrinolysis even if it does not progress to DIC, contributing to a low fibrinogen level despite minimal blood loss initially.
This study had several limitations. First, there was a low number (three) of hematuria cases, i.e., clinical DIC cases; however, a recent study of 151,678 deliveries in a solitary tertiary obstetrical hospital showed a much lower incidence of clinically diagnosed DIC, at 0.032%, for all deliveries [6]. A rough calculation of the incidence rate for this study was 0.017% (3/17,285), for a similar incidence rate, indicating this is an extremely rare condition. There also was an upper limit to the TAT and FDP measurements, and accurate coagulation–fibrinolytic activity in the MH group could not be determined, which may have led to underestimating the severity of coagulation–fibrinolytic disorders. In the future, samples showing upper measurement limits should be retested, such as by dilution. We also were unable to examine the detailed mechanism of coagulation–fibrinolytic system activation, as this study was not designed to measure proinflammatory cytokines such as tumor necrosis factor, interleukin (IL)-1 or IL-6 that activate the coagulation system [7], and factors that affect the fibrinolysis system, such as tissue plasminogen activator or plasminogen activator inhibitor type 1 [27].
5. Conclusions
This study of patients with severe PA without hematuria confirmed the accuracy of the hematuria prediction formula, “FDP–fibrinogen/3–60 (mg/dL)”, consisting of fibrinogen and FDP, which can be measured at many facilities with rapid results. Additionally, the results of coagulation–fibrinolysis tests including TAT and PIC demonstrated the validity of considering cases with hematuria as clinical DIC. If clinical data, such as hematuria and coagulation–fibrinolysis test results, are accumulated in the future and this formula’s validity is further confirmed, it should become a useful criterion for enabling early response to clinical DIC during delivery.
Author Contributions
Conceptualization, Y.M. and K.T. (Katsuhiko Tada); validation, K.T. (Katsuhiko Tada), Y.M., I.Y., K.T. (Keisuke Tsumura), I.E., M.S., N.T., K.Y., K.M., and K.K.; formal analysis, Y.M. and K.T. (Katsuhiko Tada); investigation, Y.M. and K.T. (Katsuhiko,Tada); resources, Y.M. and K.T. (Katsuhiko Tada); data curation, K.T. (Katsuhiko Tada), I.Y., K.T. (Keisuke Tsumura), I.E., M.S., N.T., K.Y., K.M., and K.K.; writing—original draft preparation, K.T. (Katsuhiko Tada) and Y.M.; writing—review and editing, Y.M. and K.T. (Katsuhiko Tada); visualization, K.T. (Katsuhiko Tada) and Y.M.; supervision, I.Y.; project administration, K.T. (Katsuhiko Tada); funding acquisition, K.T. (Katsuhiko Tada). All authors have read and agreed to the published version of the manuscript.
Funding
This study was funded by a grant from the National Hospital Organization (grant number: R1-1009002).
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the National Hospital Organization (NHO) Central Research Ethics Committee (R1-1009002, February 7, 2020).
Informed Consent Statement
Written informed consent was obtained from all subjects involved in this study.
Data Availability Statement
The datasets generated during this study are available from the corresponding author upon reasonable request.
Acknowledgments
We thank the following clinicians who helped with recruiting of participants: Sachiyo Suga and Megumi Koga at NHO Nagasaki Medical Center, Makoto Nomiyama and Yuko Oshima at NHO Saga Hospital, Tomoya Mizunoe at NHO Kure Medical Center, Takashi Kodama and Takako Sadakane at NHO Higashihiroshima Medical Center, Yuka Maegawa and Ryoun Cho at NHO Mie Chuo Medical Center, and Aki Nagao at NHO Shikoku Medical Center for Children and Adults.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| AFE | Amniotic fluid embolism |
| C/S | Cesarean section |
| DAMPs | Damage-associated molecular patterns |
| DIC | Disseminated intravascular coagulation |
| FDP | Fibrin/fibrinogen degradation products |
| FFP | Fresh frozen plasma |
| HDP | Hypertensive disorders of pregnancy |
| INR | International normalized ratio |
| ISTH | International Society of Thrombosis and Haemostasis |
| MH | Macroscopic hematuria |
| NHO | National Hospital Organization |
| PA | Placental abruption |
| PIC | Plasmin-α2–plasmin inhibitor complex |
| PPH | Postpartum hemorrhage |
| RCC | Red cell concentrates |
| TAT | Thrombin–antithrombin complex |
References
- Taylor, Jr, F. B.; Toh, C.H.; Hoots, W.K.; Wada, H.; Levi, M.; Scientific Subcommittee on Disseminated Intravascular Coagulation (DIC) of the International Society on Thrombosis and Haemostasis (ISTH). Towards definition, clinical and laboratory criteria, and a scoring system for disseminated intravascular coagulation. Thromb. Haemost. 2001, 86, 1327–1330. [Google Scholar]
- Gando, S.; Saitoh, D.; Ogura, H.; Mayumi, T.; Koseki, K.; Ikeda, T.; Ishikura, H.; Iba, T.; Ueyama, M.; Eguchi, Y.; Ohtomo, Y.; Okamoto, K.; Japanese Association for Acute Medicine Disseminated Intravascular Coagulation (JAAM DIC) Study Group. Natural history of disseminated intravascular coagulation diagnosed based on the newly established diagnostic criteria for critically ill patients: results of a multicenter, prospective survey. Crit. Care. Med. 2008, 36, 145–150. [Google Scholar] [CrossRef] [PubMed]
- Wada, H.; Takahashi, H.; Uchiyama, T.; Eguchi, Y.; Okamoto, K.; Kawasugi, K.; Madoiwa, S.; Asakura, H.; DIC subcommittee of the Japanese Society on Thrombosis and Hemostasis. The approval of revised diagnostic criteria for DIC from the Japanese Society on Thrombosis and Hemostasis. Thromb. J. 2017, 15, 17. [Google Scholar] [PubMed]
- Asakura, H. Classifying types of disseminated intravascular coagulation: clinical and animal models. J. Intensive. Care. 2014, 2, 20. [Google Scholar]
- Asakura, H.; Takahashi, H.; Uchiyama, T.; Eguchi, Y.; Okamoto, K.; Kawasugi, K.; Madoiwa, S.; Wada, H.; DIC subcommittee of the Japanese Society on Thrombosis and Hemostasis. Proposal for new diagnostic criteria for DIC from the Japanese Society on Thrombosis and Hemostasis. Thromb. J. 2016, 14, 42. [Google Scholar] [CrossRef]
- Rattray, D.D.; O’Connell, C.M.; Basket, T.F. Acute disseminated intravascular coagulation in obstetrics: a tertiary centre population review (1980 to 2009). J. Obstet. Gynaecol. Can. 2012, 34, 341–347. [Google Scholar] [CrossRef]
- Gando, S.; Levi,M. ; Toh, C.H. Disseminated intravascular coagulation. Nat. Rev. Dis. Primers. 2016, 2, 16037. [Google Scholar]
- Erez, O.; Othman, M.; Rabinovich, A.; Leron, E.; Gotsch, F.; Thachil, J. DIC in pregnancy–pathophysiology, clinical characterristics, diagnostic scores, and treatment. J. Blood. Med. 2022, 13, 21–44. [Google Scholar] [CrossRef]
- Levi, M. Pathogenesis and management of peripartum coagulopathic calamities (disseminated intravascular coagulation and amniotic fluid embolism). Thromb. Res. 2013, 131, 32–34. [Google Scholar] [CrossRef]
- Collis, R.E.; Collins, P.W. Haemostatic management of obstetric haemorrhage. Anesthesia. 2015, 70, 78–86. [Google Scholar] [CrossRef]
- Collins, P.; Abdul-Kadir, R.; Thachil, J. Management of coagulopathy associated with postpartum hemorrhage: guidance from the SSC of the ISTH. J. Thromb. Haemost. 2016, 14, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Terao, T.; Maki, M.; Ikenoue, T. A prospective study in 38 patients with abruptio placentae of 70 cases complicated by DIC. Asia-Oceania. J. Obstet. Gynaecol. 1987, 13, 1–13. [Google Scholar] [CrossRef]
- Cunningham, F.G.; Nelson, D.B. Disseminated intravascular coagulation syndromes in obstetrics. Obstet. Gynecol. 2015, 126, 999–1011. [Google Scholar] [CrossRef] [PubMed]
- Society for Maternal-Fetal Medicine (SMFM). ; Pacheco, L.D.; Saade, G.; Hankins, G.D.V.; Clark, S.L. Amniotic fluid embolism: diagnosis and management. Am. J. Obstet. Gynecol. 2016, 215, B16–24. [Google Scholar] [CrossRef]
- Miyagi, Y.; Tada, K.; Yasuhi, I.; Tsumura, K.; Maegawa, Y.; Tanaka, N.; Mizunoe, T.; Emoto, I.; Maeda, K.; Kawakami, K.; and behalf of the Collaborative Research in National Hospital Organization Network Pediatric and Perinatal Group. A novel method for determining fibrin/fibrinogen degradation products and fibrinogen threshold criteria via artificial intelligence in massive hemorrhage during delivery with hematuria. J. Clin. Med. 2024, 13, 1826. [Google Scholar] [CrossRef] [PubMed]
- Erez, O.; Novack, L.; Beer-Weisel, R.; Dukler, D.; Press, F.; Zlotnik, A.; Than, NG.; Tomer, A.; Mazor, M. DIC score in pregnant women – A population based modification of the International Society on Thrombosis and Hemostasis score. PLoS. One. 2014, 11, 9, e93240. [Google Scholar] [CrossRef]
- Morikawa, M.; Kamiya, A.; Yoshida, A.; Nishibata, S.; Okada, H. Differences between Japanese new criteria and pregnancy-specific modified ISTH DIC scores for obstetrical DIC diagnosis. Int. J. Hematol. 2024, 119, 265–274. [Google Scholar] [CrossRef]
- Ananth, C.V.; Lavery, J.A.; Vintzileos, A.M.; Skupski, D.W.; Varmer, M.; Saade, G.; Biggio, J.; Williams, M.A.; Wapner, R.J.; Wright, J.D. Severe placental abruption: clinical definition and association with maternal complications. Am. J. Obstet. Gynecol. 2016, 214, 272, e1–272. [Google Scholar] [CrossRef]
- Miyagi, Y.; Tada, K.; Yasuhi, I.; Maekawa, Y.; Okura, N.; Kawakami, K.; Yamaguchi, K.; Ogawa, M.; Kodama, K.; Nomiyama, N.; Mizunoe, T.; Miyake, T. New method for determining fibrinogen and FDP threshold criteria by artificial intelligence in cases of massive hemorrhage during delivery. J. Obstet. Gynaecol. Res. 2020, 46, 256–265. [Google Scholar] [CrossRef]
- Wikkelsø, A.J.; Edwards, H.M.; Afshari, A.; Stensballe, J.; Langhoff-Roos, J.; Albrechtsen, C.; Ekelund, K.; Hanke, G.; Secher, E.L.; Sharif, H.F.; FIB-PPH Trial Group. Pre-emptive treatment with fibrinogen concentrate for postpartum haemorrhage: randomized controlled trial. Br. J. Anaesth. 2015, 114, 623–633. [Google Scholar] [CrossRef]
- Mavrides, E.; Allard, S.; Chandraharan, E.; Collins, P.; Green, L.; Hunt, B.J.; Riris, S.; Thomson, A.J.; on behalf of the Royal College of Obstetricians and Gynaecologists. Prevention and management of postpartum haemorrhage. BJOG. 2016, 124, e106–e149. [Google Scholar]
- Liu, Z; Liu, C. ; Zhong, M.; Yang, F.; Chen, H.; Kong, W.; Lv, P.; Chen, W.; Yao, Y.; Cao, Q.; Zhou, H. Changes in coagulation and fibrinolysis in post-cesarean section parturients treated with low molecular weight heparin. Clin. Appl. Thromb. Hemost. 2020, 26, 1–6. [Google Scholar]
- Von Elm, E.; Altman, D.G. : Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. STROBE Initiative. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. BMJ. 2007, 335, 806–808. [Google Scholar] [CrossRef] [PubMed]
- Allard, S.; Green, L.; Hunt, B.J. How we manage the haematologic aspects of major obstetric haemorrhage. Br. J. Haematol. 2014, 164, 177–188. [Google Scholar] [CrossRef]
- Erez, O.; Mastrolia, S.A.; Thachil, J. Disseminated intravascular coagulation in pregnancy: insights in pathophysiology, diagnosis and management. Am. J. Obstet. Gynecol. 2015, 213, 452–463. [Google Scholar] [CrossRef]
- Bączkowska, M.; Zgliczyńska, M.; Faryna, J.; Przytuła, E.; Nowakowski, B.; Ciebiera, M. Molecular changes on maternal-fetal interface in placental abruption–A systematic review. Int. J. Mol. Sci. 2021, 22, 6612. [Google Scholar] [CrossRef]
- Ide, R.; Oda, T.; Todo, Y.; Kawai, K.; Matsumoto, M.; NarumiM. ; Kohmura-Kobayashi, Y.; Furuta-Isomura, N.; Yaguchi, C.; Uchida, T.; Suzuki, K.; Kanayama, N.; Itoh, H.; Tamura, N. Comparative analysis of hyperfibrinolysis with activated coagulation between amniotic fluid embolism and severe placental abruption. Sci. Rep. 2024, 2, 14 (1), 272. [Google Scholar]
- Sawamura, A.; Hayakawa, M.; Gando, S.; Kubota, N.; Sugano, M.; Wada, T.; Katabami, K. Disseminated intravascular coagulation with a fibrinolytic phenotype at an early phase of trauma predicts mortality. Thromb. Res. 2009, 124, 608–613. [Google Scholar] [CrossRef]
- Ito, T. PAMPs and DAMPs as trigger for DIC. J. Intensive. Care. 2014, 2, 65. [Google Scholar] [CrossRef]
- Iba, T.; Levy, J.H. Sepsis-induced coagulopathy and disseminated intravascular coagulation. Anesthesiology. 2020, 132, 1238–1245. [Google Scholar] [CrossRef]
- Zhang, Q.; Raoof, M.; Chen, Y.; Sursal, T.; Junger, W.; Bohi, K.; Itagaki, K.; Hauser, C.J. Circulating mitochondrial DAMPs cause inflammatory responses to injury. Nature. 2010, 464, 104–107. [Google Scholar] [CrossRef] [PubMed]
- Yang, R.L.; Lang, M.Z.; Qiao, X.M. Immune storm and coagulation storm in the pathogenesis of amniotic fluid embolism. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 1796–1803. [Google Scholar] [PubMed]
- Romero, R.; Chaiworapongsa, T.; Alpay, S.Z.; Xu, Y.; Hussein, Y.; Dong, Z.; Kusanovic, J.P.; Kim, C.J.; Hassan, S.S. Damage-associated molecular patterns (DAMPs) in preterm labor with intact membranes and preterm PROM: a study of the alarmin HMGB1. J. Matern. Fetal. Neonatal. Med. 2011, 24, 1444–1455. [Google Scholar] [CrossRef] [PubMed]
- Leong, A.S.; Norman, J.E.; Smith, R. Vascular and myometrial changes in the human uterus at term. Reprod. Sci. 2008, 15, 59–65. [Google Scholar] [CrossRef]
- Hayami, H.; Ohama, S.; Sakurai, A.; Yamada, J.; Yamaguchi, O.; Koide, Y.; Okura, M. Effect of amniotic fluid on blood coagulation. Crit. Care. 2009, 13, 440. [Google Scholar] [CrossRef]
- Oda, T.; Tamura, M.; Shen, Y.; Kohmura-Kobayashi, Y.; Furuta-Isomura, N.; Yaguchi, C.; Uchida, T.; Suzuki, K.; Ito, H.; Kanayama, N. Amniotic fluid as potent activator of blood coagulation and platelet aggregation: Study with rotational thromboelastometry. Thromb. Res. 2018, 172, 142–149. [Google Scholar] [CrossRef]
- Tikkanen, M. Etiology, clinical manifestations, and prediction of placental abruption. Acta. Obstetrika. et. Gynecogica. 2010, 89, 732–740. [Google Scholar] [CrossRef]
Figure 1.
Flowchart of the study participants. Data were collected for women with > 2,000 mL of blood loss within 24 hours of delivery except for PA and women with clinically diagnosed PA regardless of blood loss. The boundary criterion for predicting hematuria was developed using severe cases of PPH with fibrinogen < 170 mg/dL [15]. Therefore, this study used PA cases with fibrinogen <170 mg/dL to validate the boundary criterion. The laboratory tests and clinical data were compared among the MH, PPH, and PA groups. The MH group indicates cases of PPH with MH except for PA, PPH group is cases of PPH without MH except for PA, and PA group is cases of PA without MH regardless of blood loss at delivery. MH, macroscopic hematuria; PA, placental abruption; PPH, postpartum hemorrhage.
Figure 1.
Flowchart of the study participants. Data were collected for women with > 2,000 mL of blood loss within 24 hours of delivery except for PA and women with clinically diagnosed PA regardless of blood loss. The boundary criterion for predicting hematuria was developed using severe cases of PPH with fibrinogen < 170 mg/dL [15]. Therefore, this study used PA cases with fibrinogen <170 mg/dL to validate the boundary criterion. The laboratory tests and clinical data were compared among the MH, PPH, and PA groups. The MH group indicates cases of PPH with MH except for PA, PPH group is cases of PPH without MH except for PA, and PA group is cases of PA without MH regardless of blood loss at delivery. MH, macroscopic hematuria; PA, placental abruption; PPH, postpartum hemorrhage.
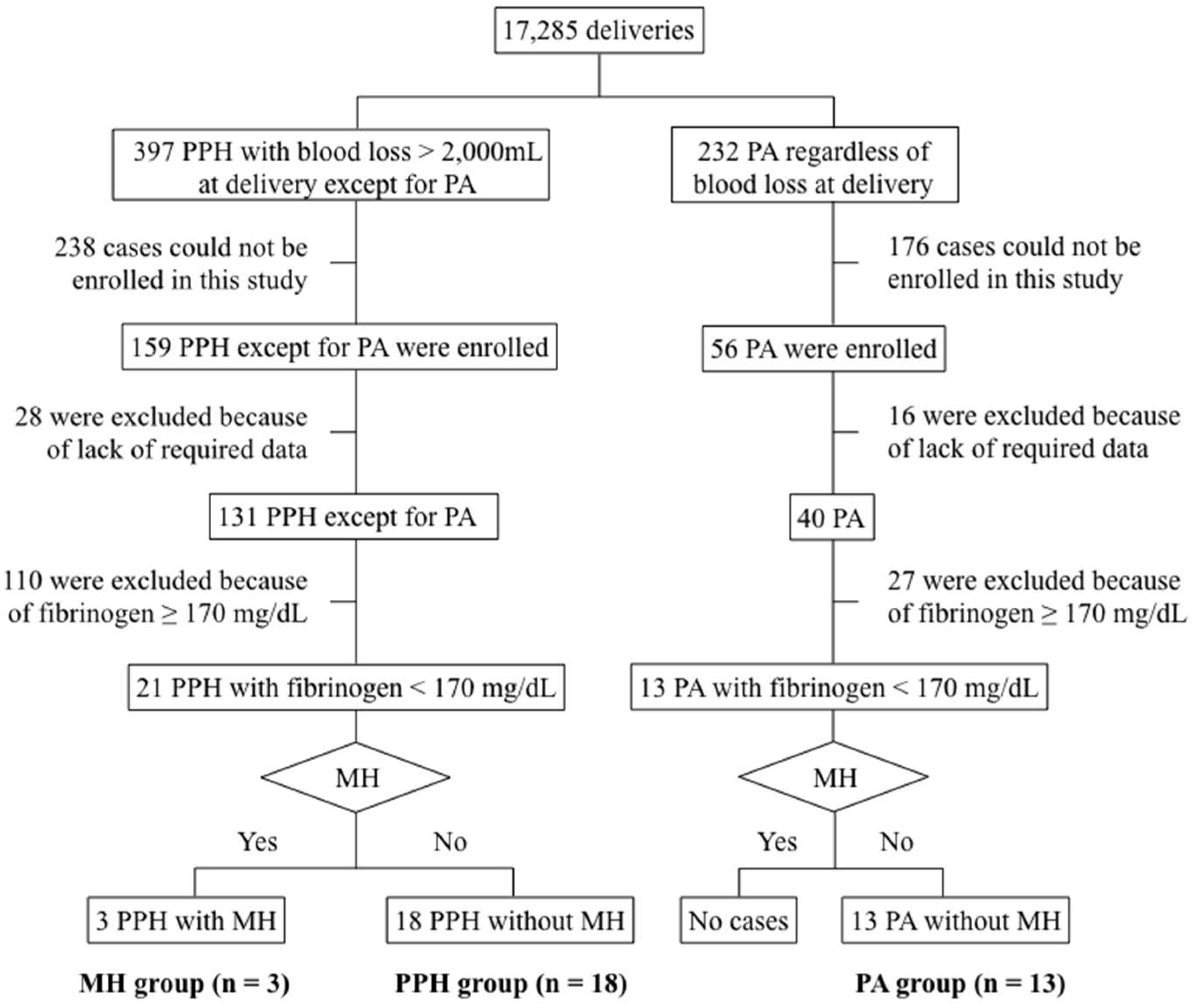
Figure 2.
Scatterplots of the cases in the MH (●), PPH (○), and PA groups (△) on the fibrinogen–FDP plane, respectively. The gray area indicates hematuria. The boundary was a straight line connecting (0, 60) and (108, 96) on the fibrinogen–FDP plane; a positive FDP–fibrinogen/3–60 (mg/dL) value indicates hematuria, otherwise, the case is non-hematuria [15]. The calculated values in 13 cases in the PA group (△) were negative, and all cases were under the boundary. All three cases in the MH group (●) that we considered as clinical DIC were over the boundary. The MH group indicates cases of PPH with MH except for PA, PPH group is cases of PPH without MH except for PA, and PA group is cases of PA without MH regardless of blood loss at delivery. FDP, fibrin/fibrinogen degradation products; MH, macroscopic hematuria; PA, placental abruption; PPH, postpartum hemorrhage.
Figure 2.
Scatterplots of the cases in the MH (●), PPH (○), and PA groups (△) on the fibrinogen–FDP plane, respectively. The gray area indicates hematuria. The boundary was a straight line connecting (0, 60) and (108, 96) on the fibrinogen–FDP plane; a positive FDP–fibrinogen/3–60 (mg/dL) value indicates hematuria, otherwise, the case is non-hematuria [15]. The calculated values in 13 cases in the PA group (△) were negative, and all cases were under the boundary. All three cases in the MH group (●) that we considered as clinical DIC were over the boundary. The MH group indicates cases of PPH with MH except for PA, PPH group is cases of PPH without MH except for PA, and PA group is cases of PA without MH regardless of blood loss at delivery. FDP, fibrin/fibrinogen degradation products; MH, macroscopic hematuria; PA, placental abruption; PPH, postpartum hemorrhage.
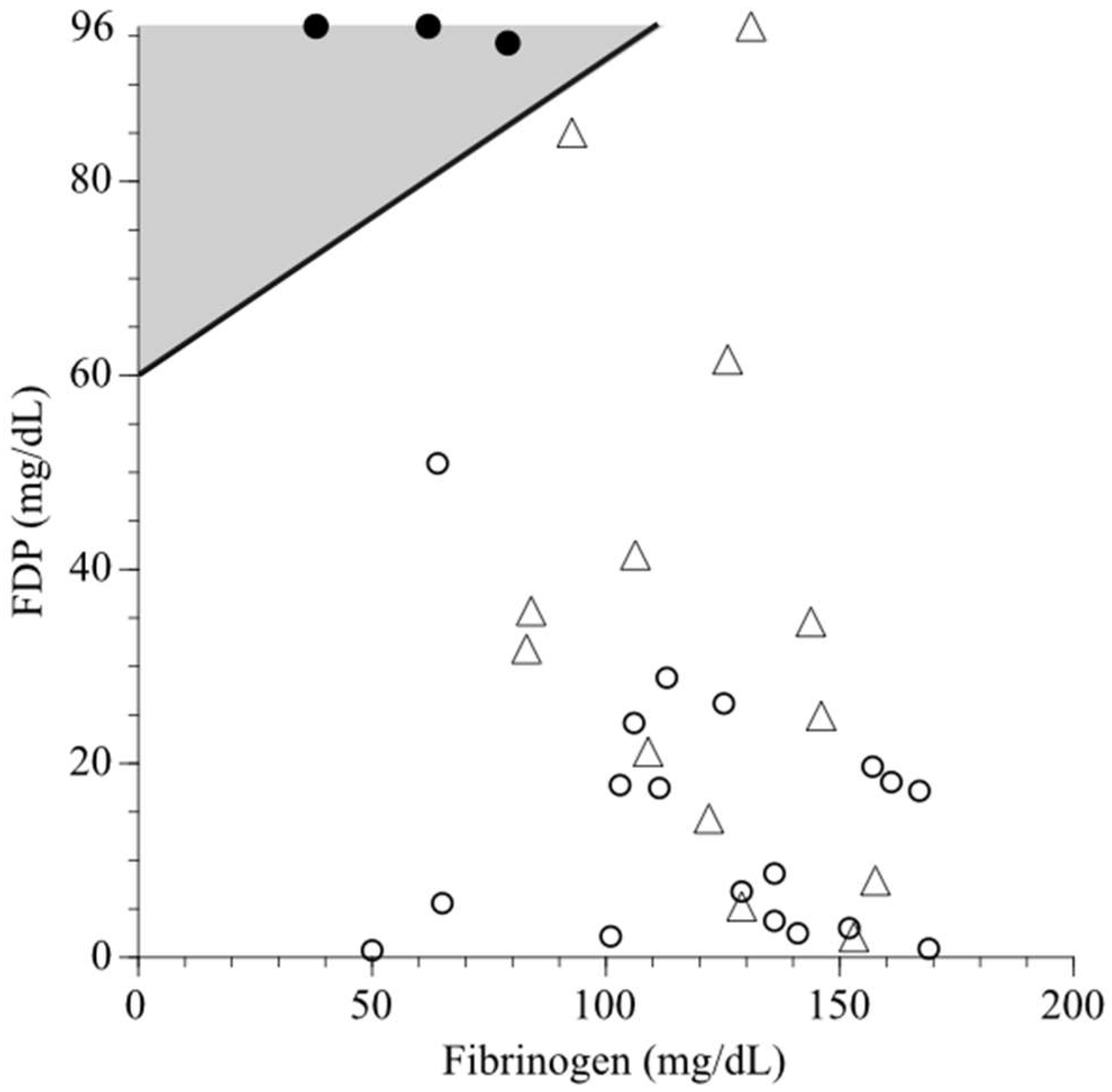

Table 1.
Clinical characteristics of participants in the three groups. Apgar score and umbilical arterial pH values in the PA group were significantly lower than in the other two groups. Values are presented as median (range) or counts (%). The PPH group indicates cases of PPH without MH except for PA, PA group is cases of PA without MH regardless of blood loss at delivery and MH group is cases of PPH with MH except for PA.
Table 1.
Clinical characteristics of participants in the three groups. Apgar score and umbilical arterial pH values in the PA group were significantly lower than in the other two groups. Values are presented as median (range) or counts (%). The PPH group indicates cases of PPH without MH except for PA, PA group is cases of PA without MH regardless of blood loss at delivery and MH group is cases of PPH with MH except for PA.
| PPH group (n = 18) (PPH without MH) |
PA group (n = 13) (PA without MH) |
MH group (n = 3) (PPH with MH) |
p-value | |
|---|---|---|---|---|
| Maternal characteristics | ||||
| Age (years) | 37 (28–45) | 32 (22–45) | 32 (28–36) | 0.20 |
| Nulliparity (%) | 10 (56) | 3 (23) | 2 (67) | 0.14 |
| Body mass index at delivery (kg/m2) | 26.1 (20.7–28.1) | 27.6 (22.6–38.6) | 25.6 (20.6–28.6) | 0.12 |
| Gestational age at delivery (weeks) | 37.5 (28–41) | 35 (22–39) | 37 (32–38) | < 0.05 |
| HDP complicated | ||||
| Gestational hypertension (%) | 1 (6) | 1 (8) | 1 (33) | 0.29 |
| Preeclampsia (%) | 6 (33) | 6 (46) | 1 (33) | 0.76 |
| Neonatal characteristics | ||||
| Apgar score at 1 min | 8 (1–10) | 1 (0–8) | 8 (1–8) | < 0.001 |
| Umbilical arterial pH | 7.292 (7.051–7.351) | 7.045 (6.563–7.282) | 7.228 (7.225–7.296) | < 0.001 |
| Mode of delivery | ||||
| Cesarean section (%) | 9 (50) | 12 (92) | 3 (100) | < 0.05 |
| Instrumental vaginal (%) | 2 (11) | 0 (0) | 0 (0) | 0.39 |
| Multifetal pregnancy (%) | 4 (22) | 0 (0) | 1 (33) | 0.14 |
| Maternal transport (%) | 6 (33) | 5 (38) | 0 (0) | 0.44 |
| Causes of bleeding | ||||
| Uterine atony (%) | 8 (44) | 0 (0) | 0 (0) | – |
| Placenta previa (%) | 2 (33) | 0 (0) | 0 (0) | – |
| Adherent placenta (%) | 4 (33) | 0 (0) | 1 (33) | – |
| Surgical trauma (%) | 3 (17) | 0 (0) | 2 (67) | – |
| Others (%) | 1 (6) | 0 (0) | 0 (0) | – |
| PA (%) | 0 (0) | 13 (100) | 0 (0) | – |
HDP, hypertensive disorders of pregnancy; MH, macroscopic hematuria; PA, placental abruption; PPH, postpartum hemorrhage.
Table 2.
Comparison of laboratory tests and clinical data among the three groups. There were significant differences for hemoglobin, prothrombin time–INR, fibrinogen, FDP, D-dimer, PIC, blood loss at initial blood sampling, and total blood loss among the three groups. There were no differences in the time between delivery and initial blood sampling, the administration volume for clear fluids, RCC, and FFP. TAT and PIC were measured in 11 of 13 cases in the PA group. Values are presented as median (range) or counts (%). The PPH group indicates cases of PPH without MH except for PA, PA group is cases of PA without MH regardless of blood loss at delivery and MH group is cases of PPH with MH except for PA.
Table 2.
Comparison of laboratory tests and clinical data among the three groups. There were significant differences for hemoglobin, prothrombin time–INR, fibrinogen, FDP, D-dimer, PIC, blood loss at initial blood sampling, and total blood loss among the three groups. There were no differences in the time between delivery and initial blood sampling, the administration volume for clear fluids, RCC, and FFP. TAT and PIC were measured in 11 of 13 cases in the PA group. Values are presented as median (range) or counts (%). The PPH group indicates cases of PPH without MH except for PA, PA group is cases of PA without MH regardless of blood loss at delivery and MH group is cases of PPH with MH except for PA.
|
PPH group (n = 18) (PPH without MH) |
PA group (n = 13) (PA without MH) |
MH group (n = 3) (PPH with MH) |
p-value | |
| Hemoglobin (g/dL) | 6.75 (5–10.2) | 8.3 (4.9–11.3) | 7.5 (4.5–10.1) | < 0.05 |
| Platelet counts (×1000/μL) | 88 (39–147) | 120 (45–204) | 96 (76–144) | 0.31 |
| Prothrombin time–INR | 1.11 (0.96–10) | 1.1 (1.02–1.44) | 1.53 (1.46–1.84) | < 0.05 |
| Fibrinogen (mg/dL) | 127.1 (50–169) | 126 (83–158) | 62 (38–79) | < 0.05 |
| FDP (mg/dL) | 12.9 (0.72–50.93) | 31.8 (2.09–96) | 96 (94.73–96) | < 0.01 |
| D-dimer (mg/dL) | 2.875 (0.3–21.9) | 3.7 (0.65–26.69) | 42.55 (13.54–49.1) | < 0.05 |
| TAT (ng/mL) | 79.95 (15.4–120) | 36 (6.8–120), n=11 | 120 (120–120) | 0.054 |
| PIC (μg/mL) | 5.65 (0.3–27.3) | 13.7 (0.7–43.3), n=11 | 28.4 (17.7–68.3) | < 0.01 |
| Time between delivery and initial blood sampling (h) | 2.83 (1–14) | 2 (0.56–8) | 1.5 (1.3–4) | 0.30 |
| Blood loss at initial blood sampling (mL) | 2,598.5 (900–4,000) | 1,594 (404–4,294) | 2,215 (1,300–2,215) | < 0.05 |
| Total blood loss (mL) | 3,148 (2,015–5,294) | 1,856 (475–4,294) | 2,950 (2,700–3,801) | < 0.001 |
| Volume of clear fluids at initial blood sampling (mL) | 2,250 (100–4,000) | 1,500 (100–4,500) | 1,500 (500–2,000) | 0.25 |
| Total volume of clear fluids | 4,000 (2,500–8,000) | 3,000 (1,500–5,000) | 4,500 (3,500–5,500) | 0.13 |
| Volume of RCC at initial blood sampling (mL) | 0 (0–1,120) | 0 (0–2,240) | 0 (0–0) | 0.44 |
| Total volume of RCC (mL) | 840 (0–3,360) | 560 (0–2,520) | 1,120 (840–1,960) | 0.18 |
| Volume of FFP at initial blood sampling (mL) | 240 (0–1,200) | 480 (0–3,600) | 0 (0–0) | 0.42 |
| Total volume of FFP (mL) | 720 (0–4,800) | 960 (0–4,080) | 960 (720–1,920) | 0.72 |
FDP, fibrin/fibrinogen degradation products; FFP, fresh frozen plasma; INR, international normalized ratio; MH, macroscopic hematuria; PA, placental abruption; PIC, plasmin-α2–plasmin inhibitor complex; PPH, postpartum hemorrhage; RCC, red cell concentrates; TAT, thrombin–antithrombin complex.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



