Submitted:
04 February 2026
Posted:
05 February 2026
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Background :Post-acute sequelae of COVID-19 (PASC) in children present persistent symptoms that impair quality of life. Vitamin D’s immunomodulatory and microbiome-modulating properties suggest its potential to alleviate PASC symptoms. This study evaluated the efficacy of Vitamin D3 supplementation in alleviating symptom severity and to explore associated immunological and microbiome alterations in children with PASC. Methods: In a double-blind randomized controlled clinical trial, 33 children with PASC were assigned to receive 2,000 IU/day of oral vitamin D (Group A, n=21) or placebo (Group B, n=12) for 6 months. Serum 25-hydroxyvitamin D [25(OH)D] levels, symptom severity (Children’s Somatic Symptom Inventory-24, CSSI-24), immune cytokines, and checkpoint proteins were assessed at baseline (M0) and 6 months (M6). Nasal and rectal microbiota were analyzed using 16S rRNA sequencing to evaluate composition and predict functional pathways. Results: Serum 25(OH)D increased significantly in Group A compared with Group B (p < 0.01). Group A demonstrated significant reductions in CSSI-24 scores (p < 0.05), with improvements in neuropsychiatric, respiratory and cardiovascular symptoms. Pro-inflammatory cytokines including IFN-γ (FDR = 0.01) and MIP-1α (FDR = 0.0004) decreased, while checkpoint proteins TIM-3 and HVEM increased (both FDR < 0.05). Nasal microbiota in Group A at M6 showed increased richness and enrichment of Sphingomonas, Paenibacillus, Ralstonia, and Sphingobium, with functional pathways related to xenobiotic metabolism altered after supplementation. Coprobacillus abundance in rectal samples positively correlated with 25(OH)D levels and negatively with IFN-γ (p = 0.02). Pooling participants from both time points across group A indicated that higher 25(OH)D levels were associated with lower symptom scores. Conclusions: Vitamin D3 supplementation improved symptom severity, modulated immune responses, and altered microbiota profiles in children with PASC. These findings support Vitamin D3 as a potential adjunctive therapy for pediatric PASC and highlight host–microbe–immune interactions as therapeutic targets.
Keywords:
post-acute sequelae of COVID-19
; vitamin D
; pediatric
; microbiome
; inflammation
; immune modulation
Background
Post-acute sequelae ofCOVID-19 (PASC) refers to symptoms persisting beyond four weeks after acute severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection, often driven by persistent inflammation and microbial dysbiosis, and affecting multiple organ systems [1]. In children, PASC can impact physical, cognitive, and emotional development [2,3], reducing quality of life and school performance [4]. The lack of effective treatments highlights the urgent need for safe and accessible interventions. This study investigates the therapeutic potential of Vitamin D3 supplementation, a cost-effective and widely available option [5,6], to alleviate pediatric PASC by modulating immune responses and microbiome composition. By addressing these mechanisms, this research aims to fill a critical gap in pediatric PASC management and improve long-term outcomes.
Vitamin D3 exerts broad immunomodulatory effects by regulating pro-inflammatory cytokines, inducing antimicrobial peptides, and modulating T-cell responses [7,8]. It also shapes gut and respiratory microbiota essential for immune homeostasis [9,10]. Given that microbial dysbiosis contributes to prolonged inflammation in PASC [11,12], Vitamin D3 may help restore microbial balance and alleviate symptoms. With its excellent safety profile and accessibility, Vitamin D3 represents a promising strategy to correct immune and microbial dysregulation in pediatric PASC.
Despite increasing awareness of pediatric PASC, therapeutic options remain limited, with most studies focusing on adults or supportive care [13,14]. Vitamin D3 has been shown to reduce disease severity in acute COVID-19, lower pro-inflammatory cytokines such as IL-6 and TNF-α, and improve immune regulation in respiratory infections [15,16,17,18]. Low serum 25-hydroxyvitamin D [25(OH)D] levels are associated with greater COVID-19 severity and delayed recovery [18,19]. Vitamin D3 supplementation also enhances gut microbial diversity, enriching beneficial taxa such as Bifidobacterium and Lactobacillus [20,21]. However, its role in pediatric PASC remains underexplored, and no randomized controlled trials have examined its effects on symptom burden, immune responses, or microbiota in this population [22,23,24].
We therefore conducted a randomized, double-blind, placebo-controlled trial of Vitamin D3 supplementation (2,000 IU/day for six months) in 33 children with PASC. The primary objectives were to: (1) assess changes in serum 25(OH)D levels and symptom severity using the Children’s Somatic Symptom Inventory-24 (CSSI-24); (2) examine alterations in systemic immune cytokines and checkpoint proteins; and (3) characterize shifts in nasal and rectal microbiota composition and function. This study aims to provide mechanistic insights into Vitamin D3’s immuno-microbial modulation in pediatric PASC and support its use as an adjunctive therapy for long-term recovery.
Methods
Study Design and Participant Recruitment
This study was a randomized, double-blind, placebo-controlled trial nested within the prospective DISCOVER (Diagnosis and Support for COVID Children to Enhance Recovery) cohort, conducted at China Medical University Children’s Hospital (CMUCH), Taiwan [25]. Children younger than 18 years with confirmed COVID-19 (via RT-PCR or rapid antigen test) and persistent PASC symptoms beyond 4 weeks were enrolled. Exclusion criteria included prior use of antibiotics, systemic corticosteroids, or immunosuppressive agents within the preceding month. Participants were consecutively recruited from the outpatient clinic between November 1, 2022, and December 31, 2023, and randomly assigned in a 1:1 ratio to receive either Group A (Vitamin D3) or Group B (placebo) for six months. The intervention, Vitamin D3 (TWHK Biotech Co., Ltd., Taiwan), was an oil-based, colorless, odorless oral drop containing 500 IU per drop. Participants took four drops (2,000 IU/day) each morning. The placebo was an identical medium-chain triglyceride (MCT) oil formulation without Vitamin D3. Both formulations were identical in appearance, taste, and packaging. Randomization was based on odd- and even-numbered medical records, assigning participants to Group A or Group B, and both investigators and participants were blinded to group allocation. Clinical assessments and sample collections were performed at baseline (Month 0, M0) and after six months (Month 6, M6). Primary outcomes included changes in serum 25(OH)D concentrations and symptom severity measured by the CSSI-24, a 24-item self-report tool for evaluating physical symptoms in children. The questionnaire was administered with assistance from trained pediatric nurses or guardians to ensure comprehension. For children under 9 years, responses were provided primarily by parents or guardians based on observed symptoms. Secondary outcomes assessed included immune cytokine and checkpoint protein levels, as well as nasal and rectal microbiota composition.
Clinical Assessments
Symptom severity was evaluated using the CSSI-24 [26] and a structured questionnaire capturing demographics and persistent symptoms at M0 and M6. The CSSI-24 assessed neuropsychiatric, respiratory, cardiovascular, musculoskeletal, and gastrointestinal symptoms. Additional clinical data, including vaccination status and medical history, were collected via standardized forms.
Sample Collection and Processing
Blood, nasal swab (NS), and rectal swab (RS) samples were collected at M0 and M6 by trained pediatric specialists (Figure 1). Serum 25(OH)D concentrations were measured using a chemiluminescence immunoassay (Diasorin XL, Siemens, Germany). Circulating immune cytokines and checkpoint proteins were quantified using MILLIPLEX® HSTCMAG28SPMX21 and HCKP111KPX17 panels, respectively (Merck Millipore, Burlington, MA, USA). For microbiota analysis, NS samples were collected by inserting sterile swabs 1–2 cm into the nasal cavity and rotating gently 3–5 times. RS samples were obtained by inserting swabs 1–2 cm into the anal sphincter with similar rotation. Swabs were immediately placed in sterile DNA/RNA Shield tubes (Zymo Research, Irvine, CA, USA) and stored at -80°C until processing.
16S rRNA Gene Sequencing
Microbial DNA was extracted from NS and RS samples using the ZymoBIOMICS DNA Microprep Kit (Zymo Research) following the manufacturer’s instructions. Samples with DNA concentrations below 0.1 ng/µL were excluded. The V3–V4 hypervariable regions of the bacterial 16S rRNA gene were amplified using primers with Illumina overhang adapters [27] and KAPA HiFi DNA Polymerase (Roche, Switzerland). PCR conditions included 25 cycles, yielding amplicons of~550 bp, verified by 2% agarose gel electrophoresis. Amplicons were purified using AMPure XP beads (0.8×; Beckman Coulter, Brea, CA, USA). Dual-index barcodes were added using the Nextera XT Index Kit v2 (Illumina, San Diego, CA, USA), followed by additional bead purification (0.5× and 1×). Indexed libraries were quantified, normalized, pooled, and sequenced on the Illumina MiSeq platform using the MiSeq Reagent Kit v3 (2 × 250 bp paired-end reads).
Statistical Analysis
Demographic, clinical, and immune data were summarized using counts, percentages, means (standard deviation), or medians (range) as appropriate. Within-group changes (M0 vs. M6) were analyzed using paired t-tests or Wilcoxon signed-rank tests, while between-group comparisons used unpaired t-tests or Mann-Whitney U tests. Symptom differences at M6 were assessed using Chi-square tests, and within-group symptom changes were evaluated with McNemar’s test. Raw p-values were corrected for multiple testing via controlling false discovery rate (FDR). Microbiome alpha diversity (richness, Shannon index) and beta diversity (based on UniFrac distances) were analyzed, with statistical significance tested using Mann-Whitney U (between groups) and Wilcoxon signed-rank (within groups) tests. Differential abundance was assessed with ANCOM and MaAsLin2, and functional predictions were generated using PICRUSt2. All analyses were performed using SAS (version 9.4), R (version 4.3.2), and GraphPad Prism (version 10, San Diego, CA, USA). Ap-value <0.05 was considered statistically significant.
Results
Participant Characteristics
Atotal of 33 children with PASC were enrolled from the DISCOVER cohort at CMUCH. Participants were randomized to receive Vitamin D3 supplementation (Group A, n = 21) or placebo (Group B, n = 12) (Figure 1). Minor group imbalance occurred because some participants withdrew mid-trial after symptom improvement or loss to follow-up. Baseline characteristics, including mean age (9 ± 3.36 years vs. 9 ± 3.53 years), sex distribution (42.86% vs. 41.67% female), and vaccination rates (80.95% vs. 83.33%), were comparable between Group A and Group B (Table 1). At baseline, Group A had significantly lower serum 25(OH)D levels compared to Group B (18.13 ± 4.99 ng/mL vs. 24.9 ± 4.56 ng/mL; p < 0.01) (Figure 2A, left).
Impact of Vitamin D3 Supplementation on Serum 25(OH)D Levels and Symptom
Severity
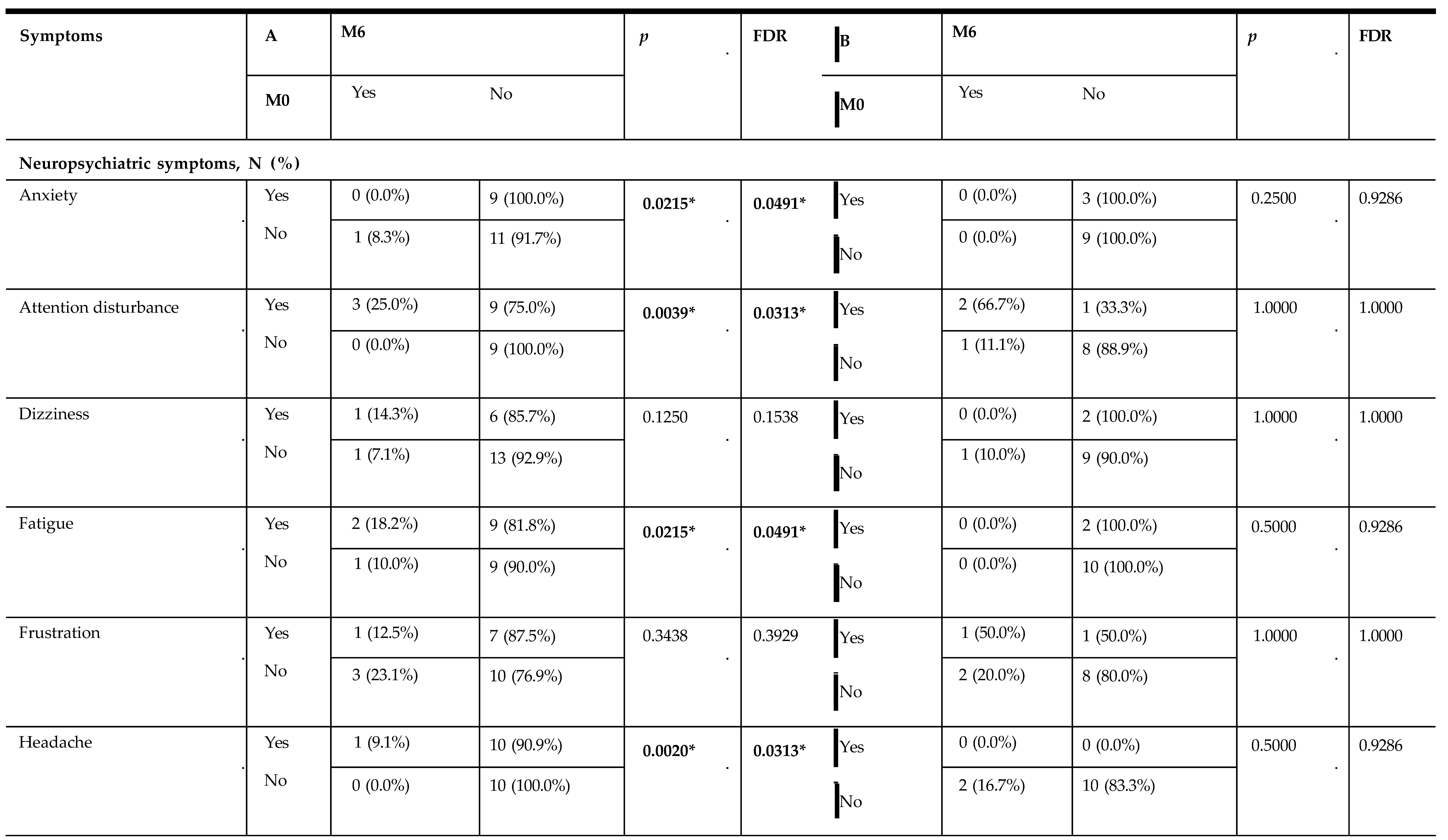
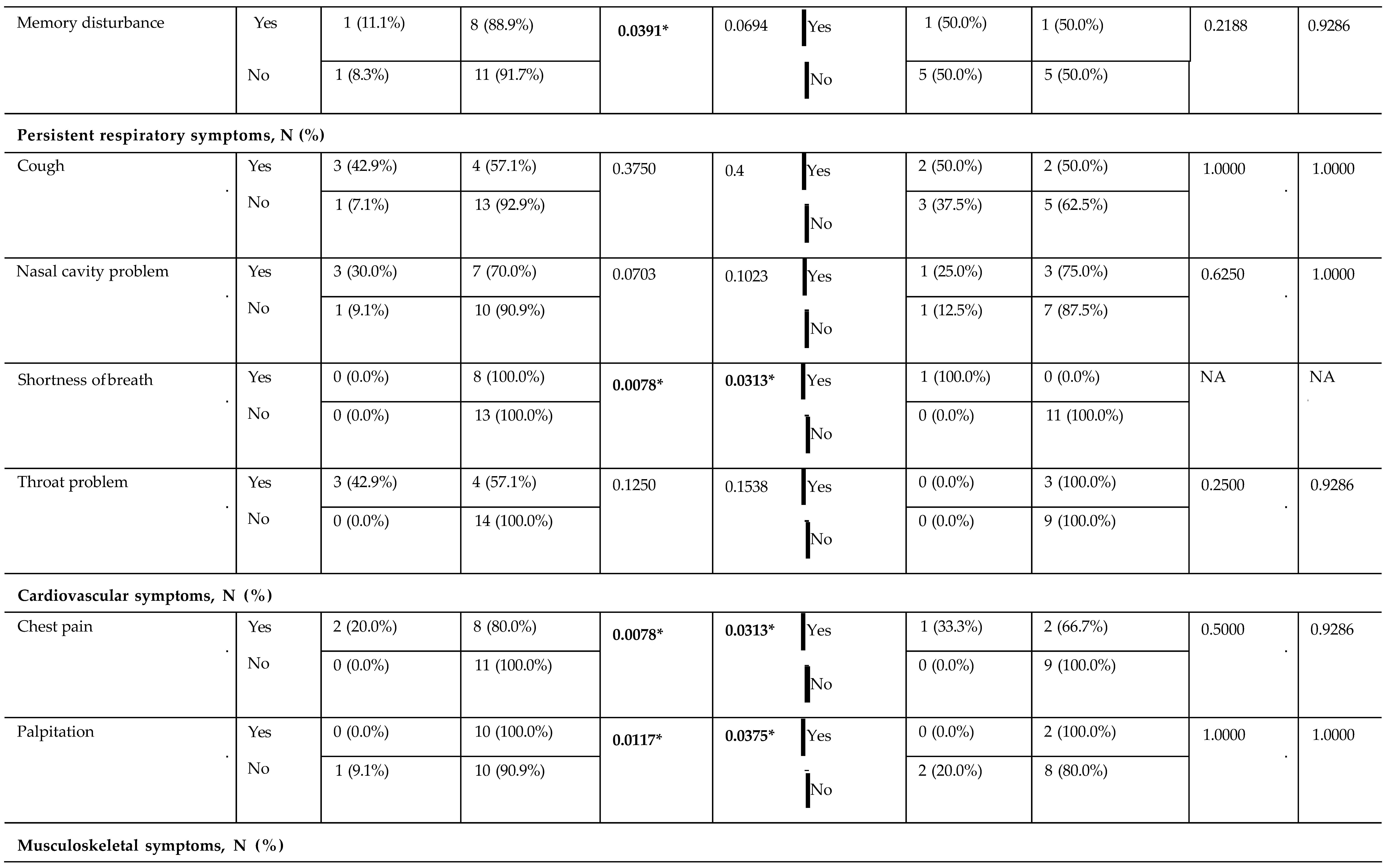
After six months supplementation, although the difference in serum 25(OH)D between Group A and Group B was no longer significant (27.35 ± 8.81 ng/mL vs. 29.41 ± 6.16 ng/mL; Figure 2A, right), both groups showed significant increases in 25(OH)D levels compared to their own baseline (p < 0.01 for both; Figure 2B). The increments of Group A were significantly higher than those of Group B (Figure 2C). Symptom severity, assessed by the CSSI-24, decreased significantly in Group A (p < 0.05), with no notable change in Group B (Figure 2D–F). Group A showed significant improvements in neuropsychiatric (e.g., anxiety, FDR = 0.05; attention disturbance, FDR = 0.03; fatigue, FDR = 0.05; headache, FDR = 0.03), respiratory symptoms (e.g., shortness of breath, FDR = 0.03), and cardiovascular (e.g., chest pain, FDR = 0.03; palpitation, FDR = 0.04) compared to Group B (Table 2).
Nasal and Rectal Microbiota Diversity and Composition
No significant differences of alpha diversity in nasal or rectal microbiota were observed between groups or within groups at baseline or overtime, except richness index for nasal microbiota at M6, which was significantly higher in Group A compared to Group B (p = 0.04; Additional file 1: Figure S1). Beta diversity analysis revealed no significant differences in nasal or rectal microbiota composition between groups or within groups over time (Additional file 1: Figure S2).
Differential Abundance and Functional Changes in Nasal Microbiota
To explore whether these compositional changes translated into functional alterations, we next performed differential abundance and pathway prediction analyses.
Differential abundance analysis by ANCOM identified Sphingomonas, Paenibacillus, and Ralstonia as enriched genera in Group A’s nasal microbiota at M6 (Figure 3A). MaAsLin2 analysis revealed a significant negative association between serum 25(OH)D levels and Sphingobium abundance in nasal samples (FDR = 0.13; Figure 3B). PICRUSt2 functional prediction indicated reductions in pathways related to xenobiotic degradation—including drug metabolism (p = 0.02), polyketide sugar unit biosynthesis (p = 0.04), and ethylbenzene (p = 0.04) and xylene degradation (p = 0.05). These associations, although were not significant different after multiple-testing correction, suggest that Vitamin D3 supplementation may influence microbial pathways linked to environmental chemical processing and host–microbe interactions.
Differential Abundance and Functional Changes in Rectal Microbiota
In the rectal microbiota, MaAsLin2 analysis of rectal microbiota in Group A showed associations between genera such as Negativicoccus, Agathobaculum, and Cutibacterium with age, and a positive association between Coprobacillus and 25(OH)D levels (FDR = 0.25; Figure 4A). Functional prediction with PICRUSt2 revealed an enrichment of several metabolic pathways at M6 compared to M0, including chloroalkane (p = 0.02), limonene (p < 0.001), and styrene degradation (p < 0.01; Figure 4B). Although these findings did not have significant differences after multiple-testing correction, paired-sample analyses showed trends toward increased activity in limonene (FDR = 0.058) and styrene degradation (FDR = 0.19) pathways after supplementation (Figure 4C).
Immunomodulatory Outcomes
In Group A, notable decreases were observed in pro-inflammatory cytokines at M6, specifically IFN-γ (FDR = 0.01) and MIP-1α (FDR = 0.0004; Additional file 1: Table S1). Additionally, significant increases were detected in immune checkpoint proteins, such as TIM-3 (FDR = 0.01) and HVEM (FDR = 0.01), at M6 (Additional file 1: Table S2). In contrast, Group B exhibited no significant alterations in either cytokine levels or immune checkpoint proteins. To explore possible microbial mediators connecting Vitamin D3 supplementation to host immunity, MaAsLin2 revealed a negative correlation between Coprobacillus abundance and circulating IFN-γ levels (p = 0.02), indicating a potential microbial contribution to the suppression of inflammatory signals.
Influence of Serum 25(OH)D on Symptom Burden
To investigate the relationship between serum 25(OH)D concentrations and the burden of PASC symptoms, we aggregated data from all participants across different time points to examine the link between serum 25(OH)D levels and CSSI-24 symptom severity scores. At the initial assessment (M0), elevated serum 25(OH)D levels showed a negative correlation with CSSI-24 scores (n = 30, p = 0.04; Figure 5A), though this relationship was not evident at Month 6 (M6; Figure 5B). When data from both time points (M0 and M6) were combined, the negative association persisted only among children receiving Vitamin D3 supplementation (Group A, n = 40, p = 0.04; Figure 5C), but was not observed in the placebo group (Group B, n = 20; Figure 5D). These results imply that Vitamin D3 supplementation may strengthen the inverse link between serum 25(OH)D status and PASC symptom burden, highlighting its possible effectiveness in reducing ongoing symptoms.
Serum 25(OH)D Categories and Microbial Composition
We divided all samples into three tertiles based on serum 25(OH)D concentrations: low (< 20.9 ng/mL), intermediate (20.9–27.6 ng/mL), and high (≥ 27.6 ng/mL), ensuring approximately equal patient distribution across the groups. CSSI-24 scores were significantly elevated in both the low and high 25(OH)D tertiles compared with the intermediate tertiles (Figure 6A). Analysis of alpha diversity revealed no significant variations in richness index for nasal or rectal microbiota; however, the intermediate 25(OH)D tertiles exhibited significantly greater Shannon index values for nasal microbiota compared to the low (p = 0.01) and high (p = 0.03) tertiles (Figure 6B–C). Beta diversity assessment using unweighted and weighted UniFrac distances showed no clear separation based on 25(OH)D status (Figure 6D–E). Given that alpha diversity differences were confined to nasal samples, we conducted a differential abundance analysis for this region, which revealed a higher prevalence of Proteobacteria in the nasal microbiota of the intermediate 25(OH)D tertiles relative to the combined low and high tertiles (Figure 6F). Taken together, these observations indicate that serum 25(OH)D levels are linked to clinical symptom severity in pediatric PASC and may also influence the relative abundance of specific microbes in the nasal and rectal regions.
Discussion
PASC in children remains a critical yet underexplored area, with limited evidence-based interventions tailored to pediatric populations. Previous research has predominantly focused on acute COVID-19 or adult PASC, leaving significant gaps in understanding the unique symptomology and pathophysiology in children [2,28]. The therapeutic potential of vitamin D in pediatric PASC has not been adequately investigated, with no prior randomized controlled trials (RCTs) evaluating its effects on symptom severity, immune regulation, or microbiome composition in this group [18]. Key uncertainties include the mechanisms linking Vitamin D3 to microbial dysbiosis and persistent inflammation in PASC, as well as optimal dosing, duration, and long-term effects in children [19,20]. Moreover, the interplay between Vitamin D3, microbiome dysbiosis, and immune dysregulation in PASC has not been systematically examined, despite evidence linking microbial imbalances to prolonged inflammation in post-viral syndromes [12,29]. This study addresses these gaps by providing evidence from an RCT on Vitamin D3 supplementation’s impact on symptoms, immune profiles, and nasal and rectal microbiota in pediatric PASC patients.
Our study is the first randomized controlled trial to investigate Vitamin D3 supplementation in pediatric PASC, providing evidence through a double-blind, placebo-controlled design. We demonstrated that 6 months of Vitamin D3 supplementation (2,000 IU/day) significantly alleviated PASC symptoms in children, as evidenced by the reduced CSSI-24 scores (p < 0.01), with notable improvements in neuropsychiatric, respiratory, cardiovascular, and gastrointestinal symptoms. In contrast, children taking placebo also showed an increase in 25(OH)D level after six months; however, no significant improvement in the symptoms was observed. Moreover, we found that the increase in serum 25(OH)D level likely contributed to symptoms relived by enhancing immunomodulatory effects and microbiota changes in nasal and gut cavities. Vitamin D3 supplementation (Group A) significantly increased serum 25(OH)D levels and was associated with shifts in nasal microbiota diversity, enrichment of specific taxa, and enhanced metabolic pathways. Rectal microbiota remained stable overall, but Coprobacillus abundance increased and correlated positively with 25(OH)D levels. Immunologically, supplementation reduced pro-inflammatory cytokines and elevated immune checkpoint proteins. Notably, the inverse association between Coprobacillus and IFN-γ suggests a microbial contribution to the observed attenuation of inflammatory responses, supporting Vitamin D3’s potential role in alleviating PASC symptoms.
The significant reduction in PASC symptom severity in children with Vitamin D3 supplementation established immunomodulatory properties, including suppression of pro-inflammatory cytokines and enhancement of immune regulation [7,8]. The substantial increase in 25(OH)D levels likely drove these effects by modulating T-cell responses and reducing chronic inflammation, a hallmark of PASC [1]. The observed decreases in IFN-γ and MIP-1α, coupled with increased immune checkpoint proteins (TIM-3 and HVEM), suggest that Vitamin D3 promotes a balanced immune response, potentially mitigating neuroinflammation and cardiovascular stress, which are linked to symptoms such as anxiety, headache, and chest pain [30,31]. The enrichment of Sphingomonas and Paenibacillus in nasal microbiota, alongside enhanced xenobiotic degradation pathways, indicates that Vitamin D3 fosters anti-inflammatory microbial communities and enhances mucosal defense against environmental toxins, potentially improving respiratory health [32,33]. In the gut, the positive correlation between Coprobacillus and 25(OH)D levels, and its negative association with IFN-γ, supports a gut-immune axis where Vitamin D3 promotes anti-inflammatory taxa, possibly via short-chain fatty acid production [34]. These site-specific microbial shifts suggest that Vitamin D3’s therapeutic effects are mediated by a synergistic interplay of increased 25(OH)D levels, microbial modulation, and reduced systemic inflammation [35].
Our stratification of patients by serum 25(OH)D levels revealed that those in the middle range (20.9–27.6 ng/mL) had the lowest CSSI-24 scores. This finding suggests that both insufficient and excessive 25(OH)D levels may be linked to greater symptom severity, underscoring the importance of maintaining an optimal range in pediatric PASC. From a microbiological perspective, 25(OH)D status was associated with changes in nasal, but not rectal, microbial diversity, indicating a compartment-specific effect. In particular, the enrichment of Proteobacteria in the nasal microbiota of the intermediate 25(OH)D tertiles, which coincided with lower symptom scores, raises the possibility that Vitamin D3 exerts local immunoregulatory effects through selective microbial modulation. Collectively, these results support that Vitamin D3 contributes to PASC recovery not only via systemic immunomodulation but also by shaping the microbiota. While causality cannot yet be inferred, the findings highlight the therapeutic potential of Vitamin D3 supplementation as an adjunctive strategy in pediatric PASC. Future studies with larger cohorts and mechanistic approaches will be needed to validate these associations and clarify microbiota-mediated pathways underlying Vitamin D3’s effects.
These findings support Vitamin D3 supplementation as a safe, cost-effective, and accessible adjunctive therapy for pediatric PASC. The broad symptom relief across neuropsychiatric, respiratory, and cardiovascular domains suggests its potential to improve quality of life in affected children. The immunomodulatory effects, evidenced by reduced pro-inflammatory cytokines and elevated immune checkpoint proteins, highlight Vitamin D3’s ability to address the chronic inflammatory state of PASC [15]. The modulation of nasal and gut microbiota further supports its role in restoring microbial homeostasis, which may contribute to sustained recovery [10]. Clinicians could consider Vitamin D3 supplementation (e.g., 2,000 IU/day) for pediatric PASC patients, particularly those with low baseline 25(OH)D levels, as part of a comprehensive management strategy. However, individualized dosing based on baseline 25(OH)D status, age, and symptom profile should be explored to optimize efficacy. These results also advocate for routine screening of 25(OH)D levels in children with PASC to identify those who may benefit most from supplementation [22]. The limitation of this study includes the small sample size (n = 33) limits statistical power and generalizability, particularly for detecting subtle microbiome changes. The six-month duration may not capture long-term effects or optimal dosing strategies. Baseline differences in 25(OH)D levels between groups could influence outcomes, despite statistical adjustments. The study did not account for dietary or environmental factors (e.g., sunlight exposure) that may affect Vitamin D3 metabolism or microbiome composition [17]. Additionally, the lack of mechanistic studies on specific microbial metabolites limits the understanding of how Vitamin D3 influences the gut-immune axis [21]. Larger, multicenter trials are needed to validate these findings and explore optimal dosing, duration, and patient-specific factors (e.g., baseline 25(OH)D status, genetic polymorphisms). Additionally, integrating multi-omics approaches (e.g., metabolomics, transcriptomics) could provide deeper insights into Vitamin D3’s role in PASC recovery.
In conclusion, this RCT study provides robust evidence that Vitamin D3 supplementation (2,000 IU/day for 6 months) effectively reduces PASC symptoms in children by increasing 25(OH)D levels, modulating nasal and gut microbiota, and attenuating systemic inflammation. These findings highlight Vitamin D3’s potential as a multifaceted therapeutic agent in pediatric PASC, addressing critical gaps in treatment options. The interplay between Vitamin D3, microbial composition, and immune regulation underscores the importance of a holistic approach to PASC management. Further research is essential to optimize clinical applications and elucidate underlying mechanisms, paving the way for targeted therapies in pediatric PASC.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Additional file 1: Figure S1. Alpha diversity analysis of nasal (NS) and rectal (RS) microbiota before and after intervention in pediatric PASC patients. Figure S2. Beta diversity of nasal (NS) and rectal (RS) microbiota before and after intervention in pediatric PASC patients. Table S1. Associations of serum 25(OH)D levels with immune cytokines at M0 versus M6 in Group A and Group B assessed by paired t-test. Table S2. Associations of serum 25(OH)D levels with immune checkpoint proteins at M0 versus M6 in Group A and Group B assessed by paired t-test.
Funding
This study was supported by funding from the National Science and Technology Council, Taiwan (grant No. NSTC 113-2314-B-039-057-, NSTC 114-2314-B-039-, NSTC 113-2320-B-006-048-, NSTC 114-2320-B-006-037-, NSTC 114-2622-M039-001-, NSTC 114-2321-B-182-005 -) and from the China Medical University Hospital, Taichung, Taiwan (grant No. DMR-114-024, and DMR-114-109).
Authors’ contributions
PCC, YLH, LSHW, and JYW designed the study. YLH, MHH, and YSH performed clinical data collections. PCC and YLH coordinated and supervised data collection. TL and YCC analyzed the microbiome data. PCC, YHC, CYL, XLL, HJT, and LSHW analyzed the clinical data. PCC wrote the initial draft of the manuscript. TL, LSHW, and JYW reviewed and revised the manuscript. WSK, HFK, and SDW provided critical assessments during the revision process leading to the final submitted manuscript. All authors have reviewed and approved the final version of this manuscript.
Availability of data and materials
Additional information: ClinicalTrials.gov Identifier: NCT05633472 https://www.clinicaltrials.gov/study/NCT05633472 Data of this study are available from the corresponding author upon reasonable request. The data are not publicly available due to privacy or ethical restrictions.
Ethical Approval and Consent to participate
The study protocol was approved by the Institutional Review Board of China Medical University Hospital (CMUH) (Approval No. CMUH111-REC2-122) in accordance with the Declaration of Helsinki and was registered at ClinicalTrials.gov (NCT05633472; registered on November 30, 2022). Written informed consent was obtained from all participants or their legal guardians prior to enrollment.
Competing interests
Dr. Jiu-Yao Wang reported grants from National Science and Technology Council and from the China Medical University Hospital during the conduct of the study. Dr. Pei- Chi Chen reported grants from National Science and Technology Council outside the submitted work. Dr. Tsunglin Liu, Dr. Wen-Shuo Kuo, Dr. Hui-Ju Tsai, and Dr. Lawrence Shih-Hsin Wu reported grants from National Science and Technology Council during the conduct of the study. The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication. No other disclosures were reported.
Abbreviations
| 25(OH)D | 25-hydroxyvitamin D |
| CSSI-24 | Children’s Somatic Symptom Inventory-24, |
| FDR | false discovery rate |
| MCT | medium-chain triglyceride |
| NS | nasal swab |
| PASC | Post-acute sequelae ofCOVID-19 |
| RCTs | randomized controlled trials |
| RS | rectal swab |
| SARS-CoV-2 | severe acute respiratory syndrome coronavirus 2 |
References
- Phetsouphanh, C; Darley, DR; Wilson, DB; Howe, A; Munier, CML; Patel, SK; et al. Immunological dysfunction persists for 8 months following initial mild-to-moderate SARS-CoV-2 infection. Nat Immunol;PubMed 2022, 23(2), 210–6. [Google Scholar] [CrossRef] [PubMed]
- Stephenson, T; Shafran, R; Ladhani, SN. Long COVID in children and adolescents. Curr Opin Infect Dis. 2022, 35(5), 461–7. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Davis, HE; Assaf, GS; McCorkell, L; Wei, H; Low, RJ; Re'em, Y; et al. Characterizing long COVID in an international cohort: 7 months of symptoms and their impact. EClinicalMedicine 2021, 38, 101019. [Google Scholar] [CrossRef] [PubMed Central]
- Meo MOS, AlHusseini N, Ibrahim DI, Meo MZS, Ahsan F, Tamim H, et al. Clinical manifestations of Long-COVID: an observational perspective. Front Med (Lausanne). 2025;12:1523817. PubMed PMID: 40177288. Pubmed Central PMCID: PMC11961443. Epub 20250319. eng.
- Holick MF. Vitamin D deficiency. N Engl J Med. 2007 Jul 19;357(3):266-81. PubMed PMID: 17634462. eng. 3).
- Martineau, AR; Jolliffe, DA; Hooper, RL; Greenberg, L; Aloia, JF; Bergman, P; et al. Vitamin D supplementation to prevent acute respiratory tract infections: systematic review and meta-analysis of individual participant data. Bmj 2017, 356, i6583. [Google Scholar] [CrossRef] [PubMed Central]
- Martens PJ, Gysemans C, Verstuyf A, Mathieu AC. Vitamin D's Effect on Immune Function. Nutrients. 2020 Apr 28;12(5). PubMed PMID: 32353972. Pubmed Central PMCID: PMC7281985. Epub 20200428. eng.
- Cantorna, MT; McDaniel, K; Bora, S; Chen, J; James, J. Vitamin D, immune regulation, the microbiota, and inflammatory bowel disease. Exp Biol Med (Maywood) 2014, 239(11), 1524–30. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ooi, JH; Chen, J; Cantorna, MT. Vitamin D regulation of immune function in the gut: why do T cells have vitamin D receptors? Mol Aspects Med 2012, 33(1), 77–82. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bellerba F, Muzio V, Gnagnarella P, Facciotti F, Chiocca S, Bossi P, et al. The Association between Vitamin D and Gut Microbiota: A Systematic Review of Human Studies. Nutrients. 2021 Sep 26;13(10). PubMed PMID: 34684379. Pubmed Central PMCID: PMC8540279. Epub 20210926. eng.
- Raj, ST; Bruce, AW; Anbalagan, M; Srinivasan, H; Chinnappan, S; Rajagopal, M; et al. COVID-19 influenced gut dysbiosis, post-acute sequelae, immune regulation, and therapeutic regimens. Front Cell Infect Microbiol. 2024, 14, 1384939. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Liu, Q; Mak, JWY; Su, Q; Yeoh, YK; Lui, GC; Ng, SSS; et al. Gut microbiota dynamics in a prospective cohort of patients with post-acute COVID-19 syndrome. Gut;PubMed 2022, 71(3), 544–52. [Google Scholar] [CrossRef] [PubMed]
- Nalbandian, A; Sehgal, K; Gupta, A; Madhavan, MV; McGroder, C; Stevens, JS; et al. Post-acute COVID-19 syndrome. Nat Med 2021, 27(4), 601–15. [Google Scholar] [CrossRef] [PubMed Central]
- Yong, SJ. Long COVID or post-COVID-19 syndrome: putative pathophysiology, risk factors, and treatments. Infect Dis (Lond) 2021, 53(10), 737–54. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Entrenas Castillo M, Entrenas Costa LM, Vaquero Barrios JM, Alcalá Díaz JF, López Miranda J, Bouillon R, et al. "Effect of calcifediol treatment and best available therapy versus best available therapy on intensive care unit admission and mortality among patients hospitalized for COVID-19: A pilot randomized clinical study". J Steroid Biochem Mol Biol. 2020 Oct;203:105751. PubMed PMID: 32871238. Pubmed Central PMCID: PMC7456194. Epub 20200829. eng.
- Quesada-Gomez, JM; Entrenas-Castillo, M; Bouillon, R. Vitamin D receptor stimulation to reduce acute respiratory distress syndrome (ARDS) in patients with coronavirus SARS-CoV-2 infections: Revised Ms SBMB 2020_166. J Steroid Biochem Mol Biol. 2020, 202, 105719. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Baktash, V; Hosack, T; Patel, N; Shah, S; Kandiah, P; Van den Abbeele, K; et al. Vitamin D status and outcomes for hospitalised older patients with COVID-19. Postgrad Med J 2021, 97(1149), 442–7. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kaufman, HW; Niles, JK; Kroll, MH; Bi, C; Holick, MF. SARS-CoV-2 positivity rates associated with circulating 25-hydroxyvitamin D levels. PLoS One PubMed. 2020, 15(9), e0239252. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mercola, J; Grant, WB; Wagner, CL. Evidence Regarding Vitamin D and Risk of COVID-19 and Its Severity. Nutrients;PubMed 2020, 12(11). [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Singh P, Rawat A, Alwakeel M, Sharif E, Al Khodor S. The potential role of vitamin D supplementation as a gut microbiota modifier in healthy individuals. Sci Rep. 2020 Dec 10;10(1):21641. PubMed PMID: 33303854. Pubmed Central PMCID: PMC7729960. Epub 20201210. eng.
- Akimbekov, NS; Digel, I; Sherelkhan, DK; Lutfor, AB; Razzaque, MS. Vitamin D and the Host-Gut Microbiome: A Brief Overview. Acta Histochem Cytochem PubMed. 2020, 53(3), 33–42. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kenny G, Townsend L, Savinelli S, Mallon PWG. Long COVID: Clinical characteristics, proposed pathogenesis and potential therapeutic targets. Front Mol Biosci. 2023;10:1157651. PubMed PMID: 37179568. Pubmed Central PMCID: PMC10171433. Epub 20230426. eng.
- Giannos, P; Prokopidis, K. Gut dysbiosis and long COVID-19: Feeling gutted. J Med Virol. 2022, 94(7), 2917–8. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Álvarez-Santacruz, C; Tyrkalska, SD; Candel, S. The Microbiota in Long COVID. Int J Mol Sci.;PubMed 2024, 25(2). [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hsu, YL; Chen, PC; Tsai, YF; Wei, CH; Wu, LS; Hsieh, KS; et al. Clinical Features and Vaccination Effects among Children with Post-Acute Sequelae of COVID-19 in Taiwan. Vaccines (Basel);PubMed 2024, 12(8). [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Walker, LS; Beck, JE; Garber, J; Lambert, W. Children's Somatization Inventory: psychometric properties of the revised form (CSI-24). J Pediatr Psychol.;PubMed 2009, 34(4), 430–40. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Pichler, M; Coskun, Ö K; Ortega-Arbulú, AS; Conci, N; Wörheide, G; Vargas, S; et al. A 16S rRNA gene sequencing and analysis protocol for the Illumina MiniSeq platform. Microbiologyopen 2018, 7(6), e00611. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Rao, S; Gross, RS; Mohandas, S; Stein, CR; Case, A; Dreyer, B; et al. Postacute Sequelae of SARS-CoV-2 in Children. In Pediatrics;PubMed; Pubmed Central, 1 Mar 2024; 3, p. 153. [Google Scholar] [PubMed] [PubMed Central]
- Guo, C; Yi, B; Wu, J; Lu, J. The microbiome in post-acute infection syndrome (PAIS). Comput Struct Biotechnol J 2023, 21, 3904–11. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wykes MN, Lewin SR. Immune checkpoint blockade in infectious diseases. Nat Rev Immunol. 2018 Feb;18(2):91-104. PubMed PMID: 28990586. Pubmed Central PMCID: PMC5991909. Epub 20171009. eng.
- Cătălina, GR; Gheorman, V; Gheorman, V; Forțofoiu, MC. The Role of Neuroinflammation in the Comorbidity of Psychiatric Disorders and Internal Diseases. In Healthcare (Basel);PubMed; Pubmed Central, 7 Apr 2025; 7, p. 13. [Google Scholar] [PubMed] [PubMed Central]
- Durack, J; Lynch, SV; Nariya, S; Bhakta, NR; Beigelman, A; Castro, M; et al. Features of the bronchial bacterial microbiome associated with atopy, asthma, and responsiveness to inhaled corticosteroid treatment. J Allergy Clin Immunol. 2017, 140(1), 63–75. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Torres-Sánchez, A; Ruiz-Rodríguez, A; Ortiz, P; Moreno, MA; Ampatzoglou, A; Gruszecka-Kosowska, A; et al. Exploring Next Generation Probiotics for Metabolic and Microbiota Dysbiosis Linked to Xenobiotic Exposure: Holistic Approach. Int J Mol Sci;PubMed 2022, 23(21). [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Louis, P; Flint, HJ. Formation of propionate and butyrate by the human colonic microbiota. Environ Microbiol 2017, 19(1), 29–41. [Google Scholar] [CrossRef] [PubMed]
- Ullah, H. Gut-vitamin D interplay: key to mitigating immunosenescence and promoting healthy ageing. Immun Ageing 2025, 22(1), 20. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
Figure 1.
Double-blind randomized controlled trial (RCT) design for Vitamin D3 intervention in pediatric PASC patients.
Figure 1.
Double-blind randomized controlled trial (RCT) design for Vitamin D3 intervention in pediatric PASC patients.
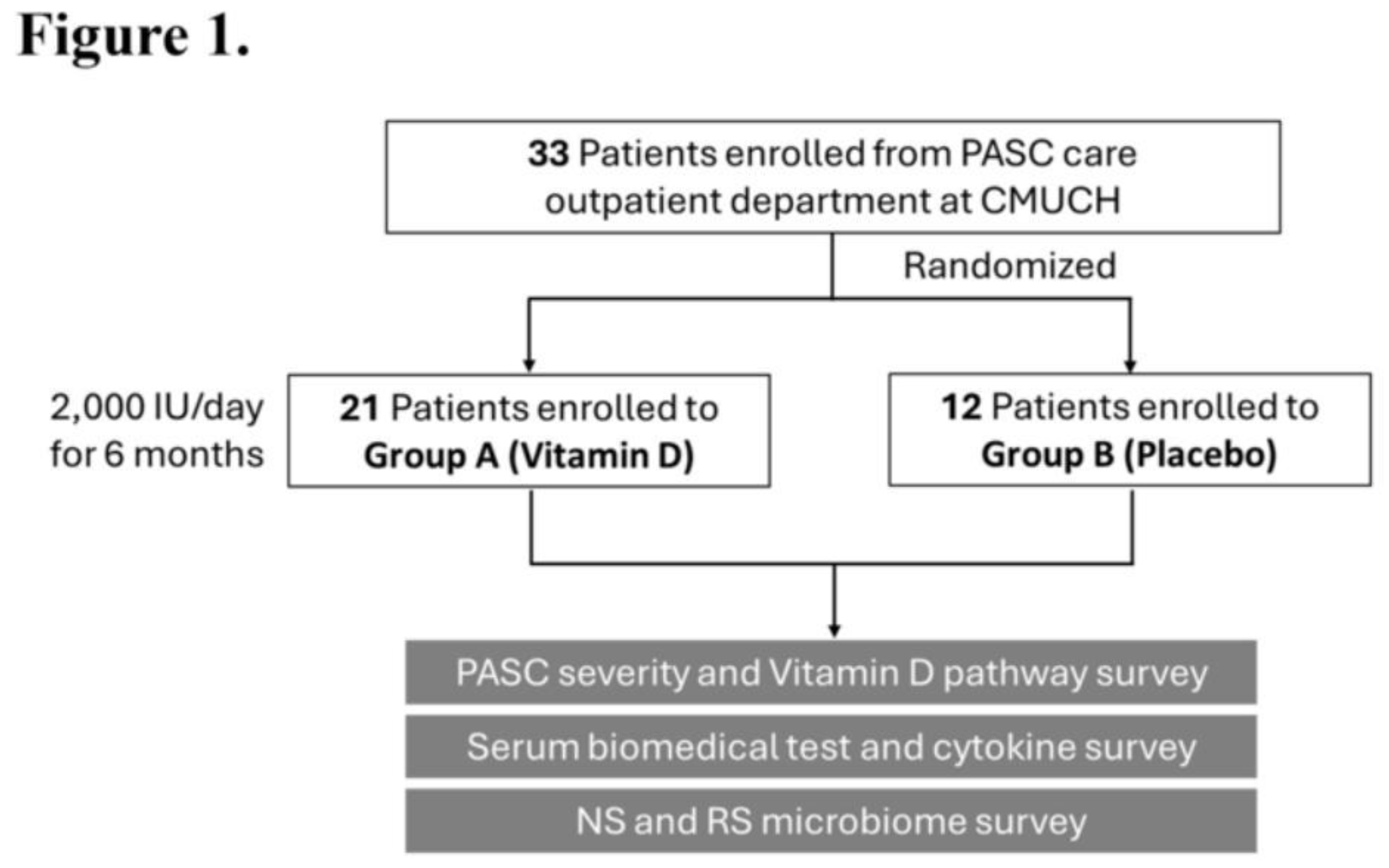
Figure 2.
Vitamin D3 supplementation improves serum 25(OH)D levels and reduces symptom severity in pediatric PASC patients. Comparison of baseline (M0) and 6-month (M6) serum (A) 25(OH)D levels and (D) CSSI-24 symptom severity scores between Group A (Vitamin D3) and Group B (placebo). Paired longitudinal changes in (B) 25(OH)D levels and (E) CSSI-24 scores within each group from M0 to M6. Net changes (M6–M0) in (C) serum 25(OH)D levels and (F) CSSI-24 scores. Statistical comparisons were performed using paired and unpaired tests as appropriate. *p ≤ 0.05, **p ≤ 0.01.
Figure 2.
Vitamin D3 supplementation improves serum 25(OH)D levels and reduces symptom severity in pediatric PASC patients. Comparison of baseline (M0) and 6-month (M6) serum (A) 25(OH)D levels and (D) CSSI-24 symptom severity scores between Group A (Vitamin D3) and Group B (placebo). Paired longitudinal changes in (B) 25(OH)D levels and (E) CSSI-24 scores within each group from M0 to M6. Net changes (M6–M0) in (C) serum 25(OH)D levels and (F) CSSI-24 scores. Statistical comparisons were performed using paired and unpaired tests as appropriate. *p ≤ 0.05, **p ≤ 0.01.
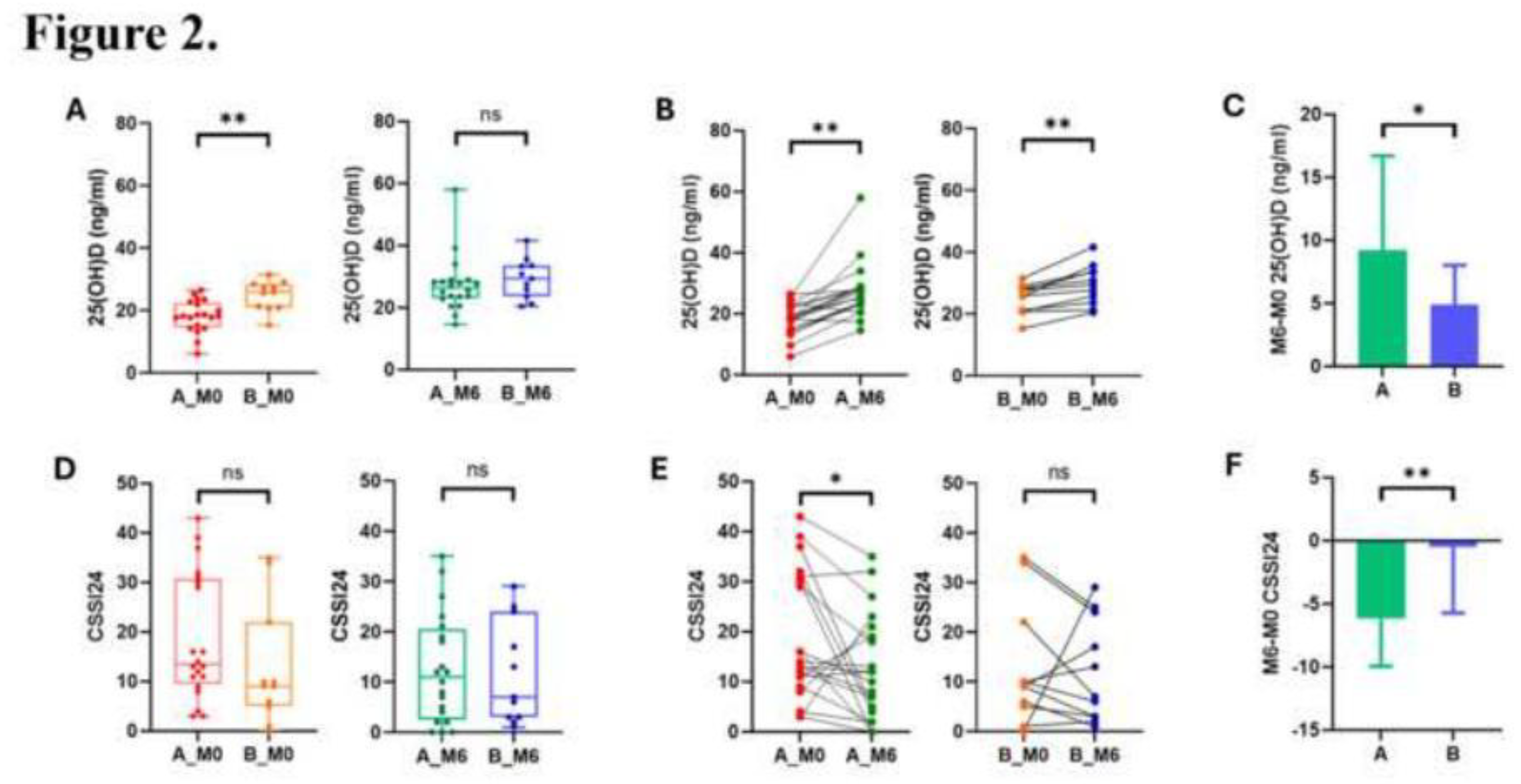
Figure 3.
Differential abundance and predicted functional pathways of nasal microbiota in Group A following vitamin D supplementation. (A) ANCOM analysis comparing nasal samples at baseline (M0) and after 6 months (M6). (B) MaAsLin2 multivariable association analysis incorporating serum 25(OH)D level, age, and sex as fixed effects, and participant ID as a random effect. (C) PICRUSt2-based functional prediction of metabolic pathways from 16S rRNA gene data comparing M0 and M6 samples. The 95% confidence intervals reflect differences in pathway abundance between time points (M0–M6).
Figure 3.
Differential abundance and predicted functional pathways of nasal microbiota in Group A following vitamin D supplementation. (A) ANCOM analysis comparing nasal samples at baseline (M0) and after 6 months (M6). (B) MaAsLin2 multivariable association analysis incorporating serum 25(OH)D level, age, and sex as fixed effects, and participant ID as a random effect. (C) PICRUSt2-based functional prediction of metabolic pathways from 16S rRNA gene data comparing M0 and M6 samples. The 95% confidence intervals reflect differences in pathway abundance between time points (M0–M6).
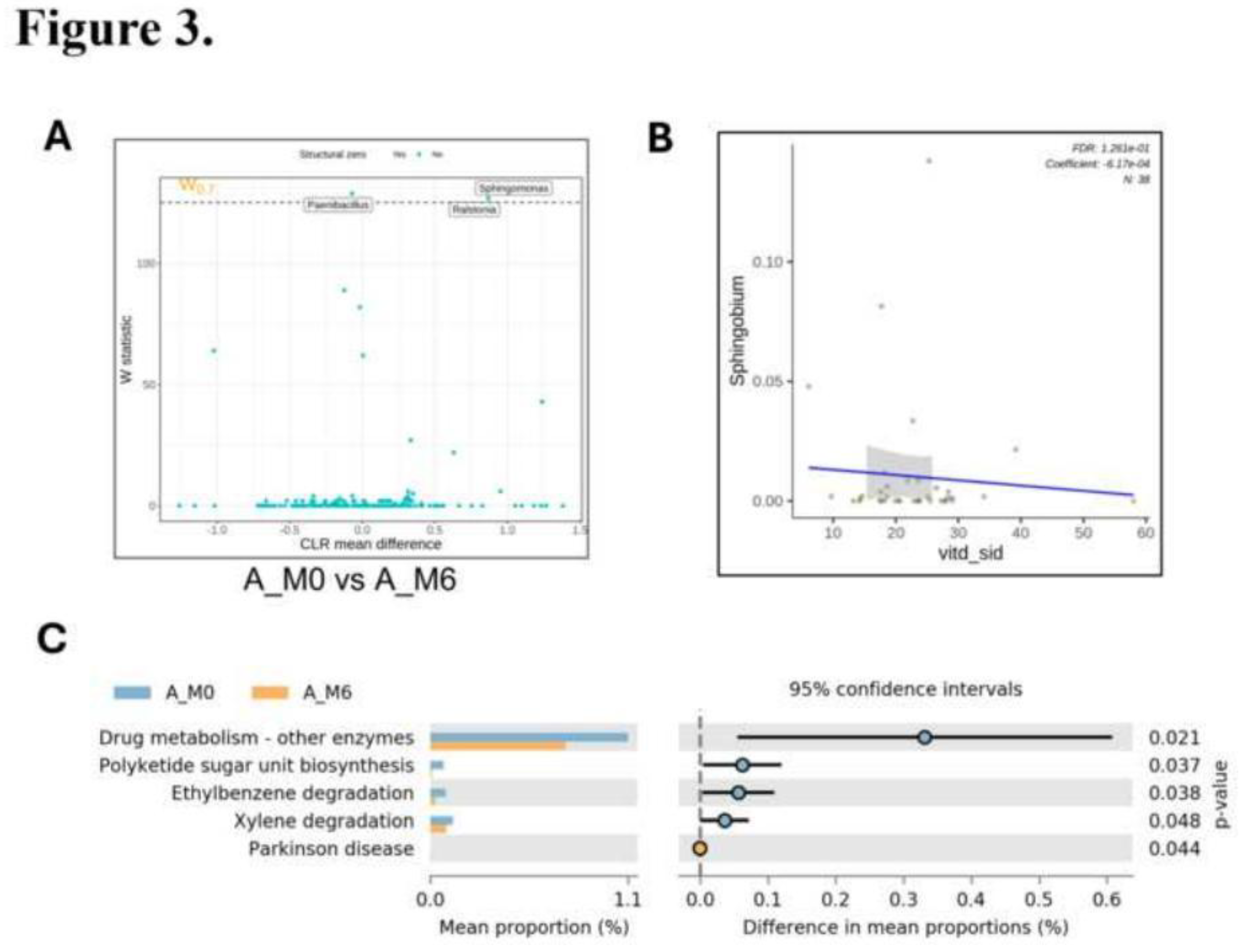
Figure 4.
Differential abundance and predicted functional pathways of rectal microbiota in Group A following Vitamin D3 supplementation. (A) MaAsLin2 multivariable association analysis incorporating serum 25(OH)D level, age, and sex as fixed effects, and participant ID as a random effect. (B) PICRUSt2-based functional prediction of metabolic pathways from 16S rRNA gene data comparing M0 and M6 samples. The 95% confidence intervals reflect differences in pathway abundance between time points (M0–M6). (C) Paired-sample analysis of predicted pathways to assess within-subject functional shifts over time.
Figure 4.
Differential abundance and predicted functional pathways of rectal microbiota in Group A following Vitamin D3 supplementation. (A) MaAsLin2 multivariable association analysis incorporating serum 25(OH)D level, age, and sex as fixed effects, and participant ID as a random effect. (B) PICRUSt2-based functional prediction of metabolic pathways from 16S rRNA gene data comparing M0 and M6 samples. The 95% confidence intervals reflect differences in pathway abundance between time points (M0–M6). (C) Paired-sample analysis of predicted pathways to assess within-subject functional shifts over time.
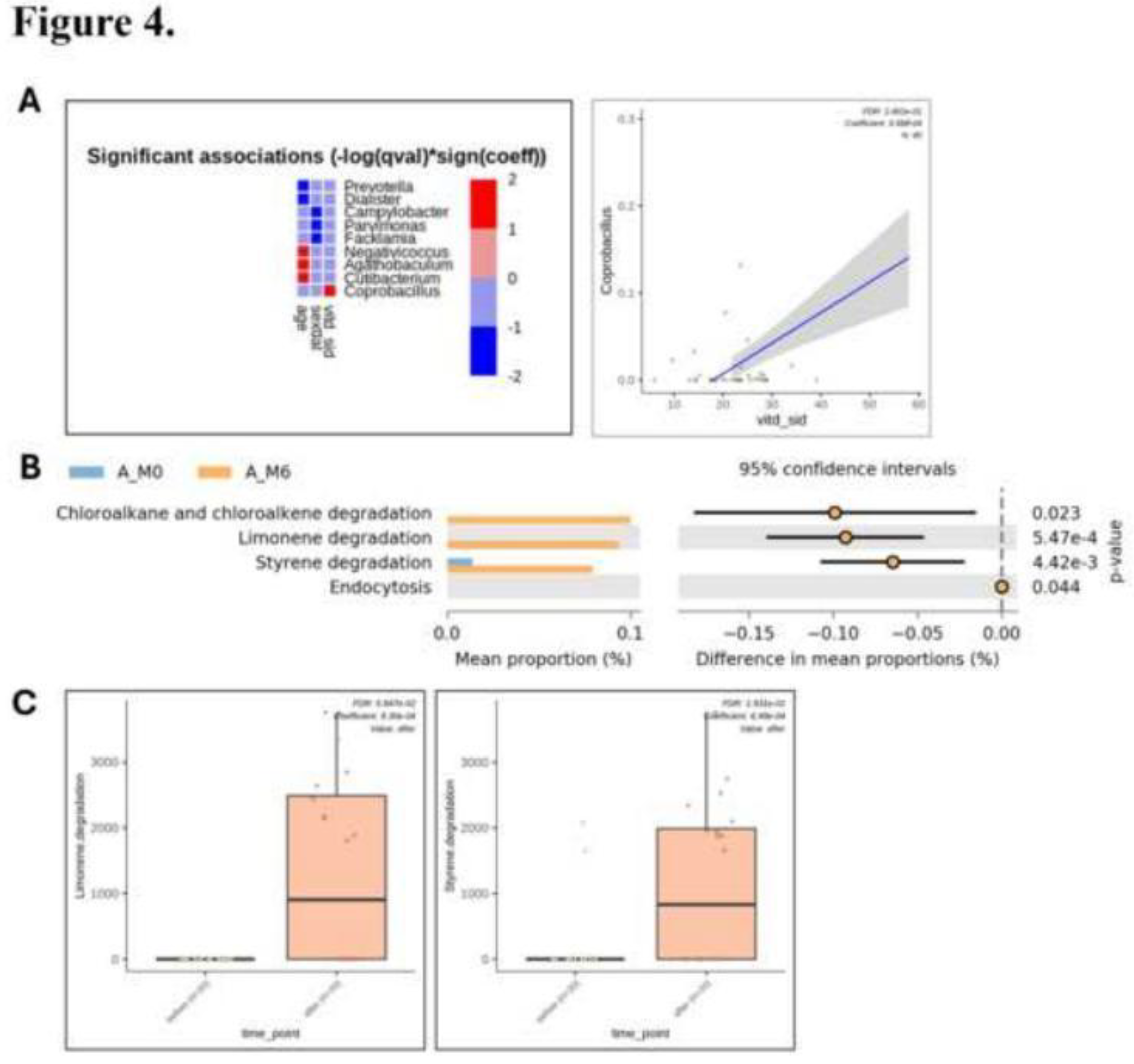
Figure 5.
Spearman’s correlation between serum 25(OH)D levels and CSSI-24 symptom severity scores in pediatric PASC patients. (A) Baseline (Month 0) correlation analysis pooling samples from both Group A (Vitamin D3) and Group B (placebo), n = 30. (B) Month 6 (M6) correlation analysis pooling samples from both groups, n = 30. (C) Combined analysis pooling samples from Group A across both time points (M0 and M6), n = 40. (D) Combined analysis pooling samples from Group B across both time points, n = 20. Each dot represents one participant, and red lines indicate the linear trend across the dataset.
Figure 5.
Spearman’s correlation between serum 25(OH)D levels and CSSI-24 symptom severity scores in pediatric PASC patients. (A) Baseline (Month 0) correlation analysis pooling samples from both Group A (Vitamin D3) and Group B (placebo), n = 30. (B) Month 6 (M6) correlation analysis pooling samples from both groups, n = 30. (C) Combined analysis pooling samples from Group A across both time points (M0 and M6), n = 40. (D) Combined analysis pooling samples from Group B across both time points, n = 20. Each dot represents one participant, and red lines indicate the linear trend across the dataset.
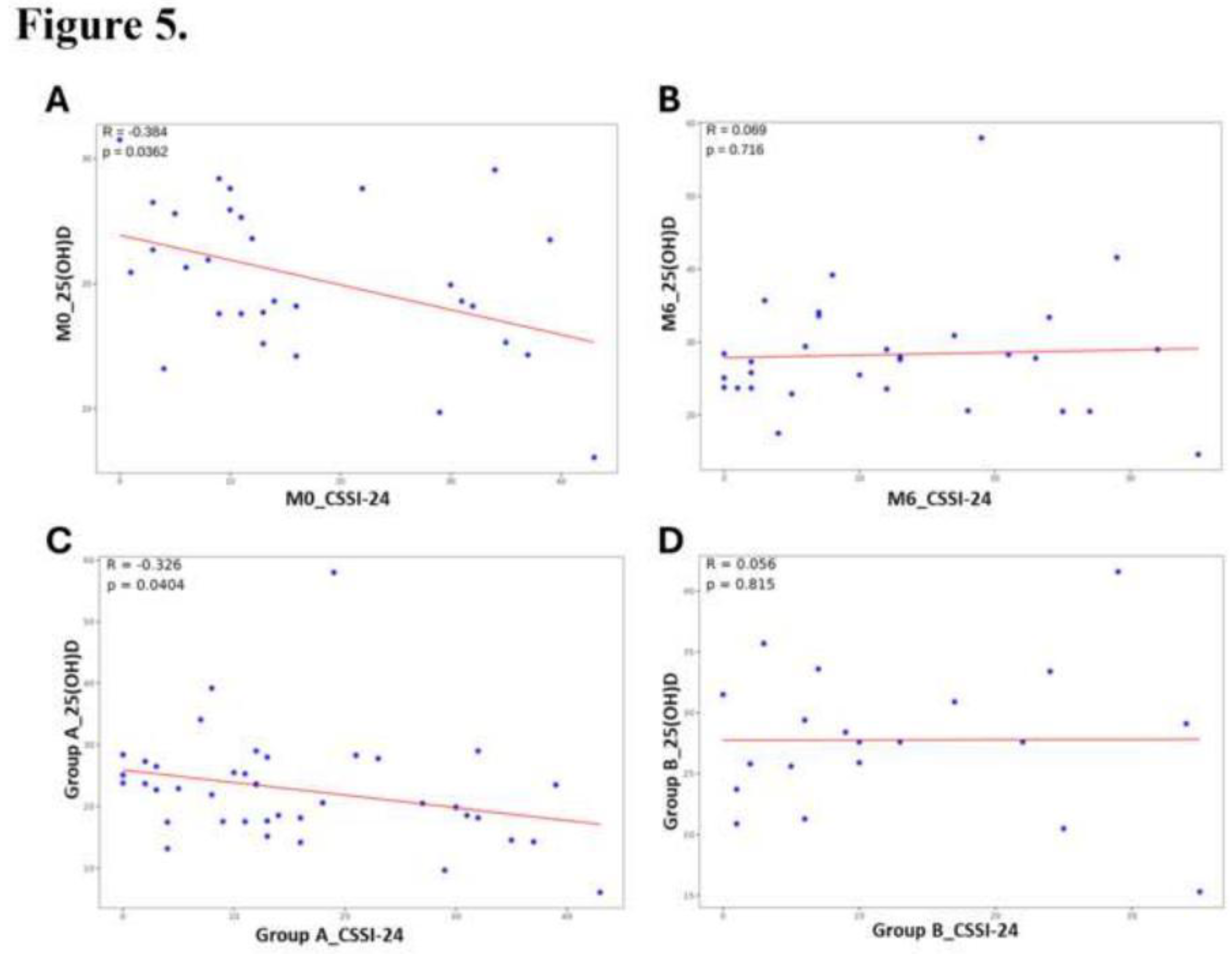
Figure 6.
Comparison of symptom severity and nasal (NS) and rectal (RS)microbiota in pediatric PASC patients stratified by serum 25(OH)D levels. (A) CSSI-24 symptom severity scores among three serum 25(OH)D tertiles: low (< 20.9 ng/mL), intermediate (20.9–27.6 ng/mL), and high (≥ 27.6 ng/mL). Alpha diversity indices (richness and Shannon index) of (B) NS and (C) RS microbiota across the three 25(OH)D tertiles. Beta diversity of (D) NS and (E) RS microbiota visualized by PCoA plots based on unweighted and weighted UniFrac distances. (F) Differential abundance analysis in NS samples comparing the intermediate tertiles to the combined high and low tertiles. Statistical significance was assessed using the Wilcoxon rank-sum test for (A–C), PERMANOVA for (D–E), and a general linear model for (F); *p ≤ 0.05, **p ≤ 0.01.
Figure 6.
Comparison of symptom severity and nasal (NS) and rectal (RS)microbiota in pediatric PASC patients stratified by serum 25(OH)D levels. (A) CSSI-24 symptom severity scores among three serum 25(OH)D tertiles: low (< 20.9 ng/mL), intermediate (20.9–27.6 ng/mL), and high (≥ 27.6 ng/mL). Alpha diversity indices (richness and Shannon index) of (B) NS and (C) RS microbiota across the three 25(OH)D tertiles. Beta diversity of (D) NS and (E) RS microbiota visualized by PCoA plots based on unweighted and weighted UniFrac distances. (F) Differential abundance analysis in NS samples comparing the intermediate tertiles to the combined high and low tertiles. Statistical significance was assessed using the Wilcoxon rank-sum test for (A–C), PERMANOVA for (D–E), and a general linear model for (F); *p ≤ 0.05, **p ≤ 0.01.
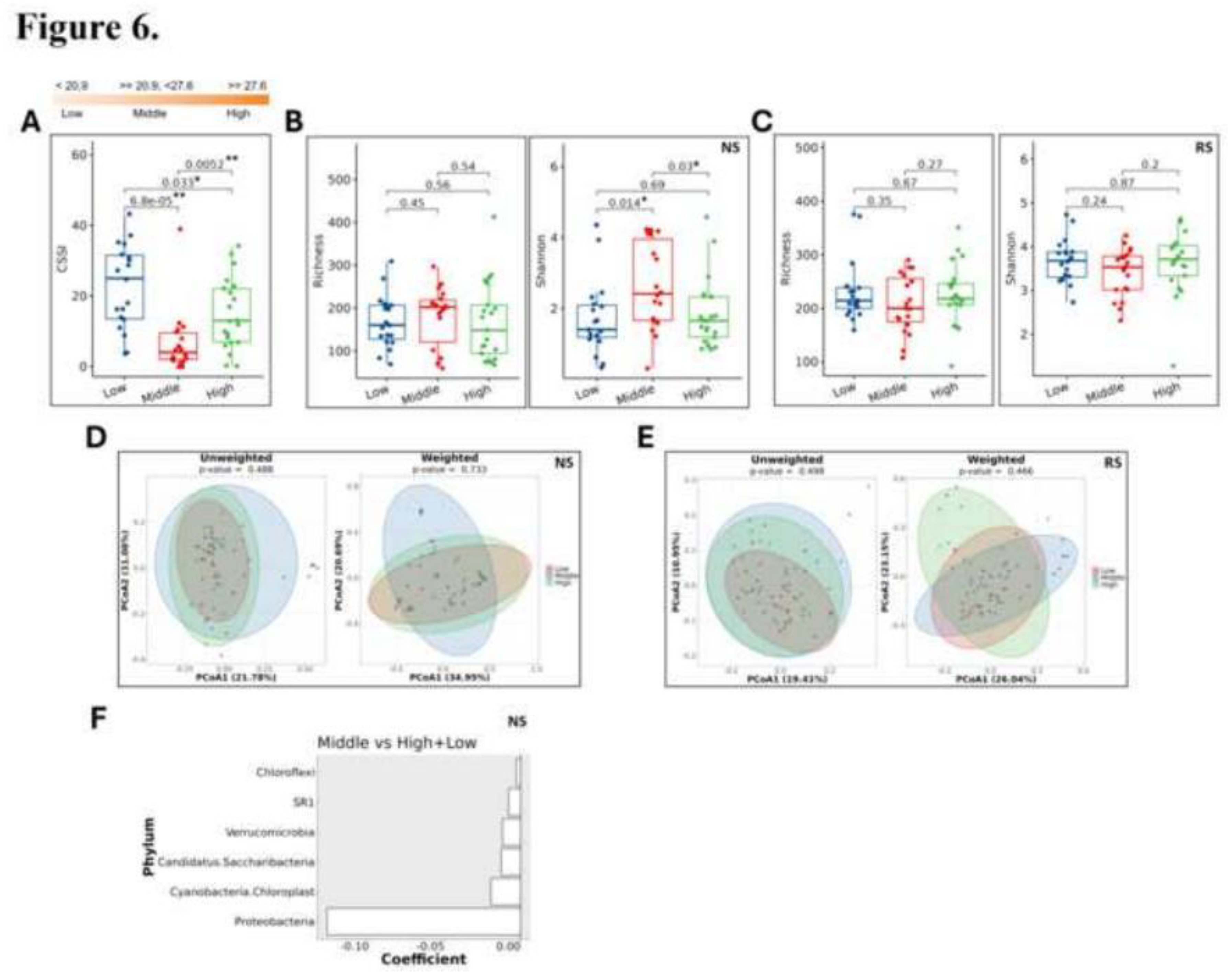

Table 1.
Demographic characteristics of the study population.
| Demographic characteristics | ||
| Age | A | B |
| mean ± SD (N) | 9±3.36 (21) | 9±3.53 (12) |
| Sex, N (%) | ||
| Female | 9 (42.86%) | 5 (41.67%) |
| Male | 12 (57.14%) | 7 (58.33%) |
| Vaccination, N (%) | 17 (80.95%) | 10 (83.33%) |
Table 2.
Group-wise comparison of PASC symptoms before and after 6-month Vitamin D3 or placebo intervention assessed by McNemar’s test.
Table 2.
Group-wise comparison of PASC symptoms before and after 6-month Vitamin D3 or placebo intervention assessed by McNemar’s test.
 |
 |
 |
Symptoms observed in fewer than six participants, including depression, lost fun, lack motivation, muscle pain, abdominal pain, diarrhea, at M0 in Group A were excluded from analysis. *p ≤ 0.05 and **p ≤ 0.01 are in bold.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



