Submitted:
19 February 2026
Posted:
20 February 2026
You are already at the latest version
Abstract
Diffuse large B-cell lymphoma (DLBCL) is molecularly heterogeneous; genotype-directed first-line therapy may improve outcomes. We conducted a single-center, prospective, non-randomized interventional study evaluating a molecularly adapted R-CHOP-X strategy with two-year follow-up. Between February 2023 and the data cut-off (September 16, 2025), 43 adults with newly diagnosed DLBCL (excluding high-grade B-cell lymphoma, primary immune-privileged, and primary mediastinal large B-cell lymphomas) underwent tumor genotyping using LymphGen after targeted sequencing: an initial cohort had Sanger sequencing of a 19-gene panel (n = 35) and a second cohort an expanded 60-gene panel (n = 8). All patients received one cycle of R-CHOP followed by five cycles of R-CHOP-X, with the additional agent (vorinostat, acalabrutinib, decitabine, or lenalidomide) selected according to molecular subtype. Response assessment followed Lugano criteria; adverse events were recorded per NCI CTCAE v5.0. The overall response rate was 100% (n = 43); complete response among patients completing therapy (n = 35) was 100%. At two years, overall survival was 92% (95% CI 83%–100%) and progression-free survival was 94% (95% CI 86%–100%); two early relapses occurred. These findings indicate that molecularly adapted R-CHOP-X is feasible and associated with high response rates and favorable two-year survival and warrant validation in larger randomized clinical trials.
Keywords:
diffuse large B-cell lymphoma
; molecularly adapted therapy
; R-CHOP-X
; LymphGen
; targeted sequencing
; personalized medicine
; progression-free survival
; overall survival
Introduction
It is now well established that diffuse large B-cell lymphoma (DLBCL) comprises a biologically and clinically heterogeneous group of aggressive B-cell neoplasms. DLBCL is characterized by distinct molecular mechanisms of lymphomagenesis, variable prognosis, differential therapeutic sensitivity, and divergent clinical outcomes [1]. This heterogeneity is reflected not only in recent revisions of hematolymphoid tumor classifications - the 5th edition of the WHO classification [2] and the International Consensus Classification (ICC, 2022)[3] - but also in contemporary molecular stratification frameworks for DLBCL. Systems such as HMRN [4], LymphGen [5], and DLBclass [6] provide detailed genetic segregation of patients and carry direct prognostic and therapeutic implications for understanding lymphomagenesis, risk assessment, prediction of treatment response, and clinical outcome. It is important to emphasize that DLBCL is distinguished not only by molecular heterogeneity but also by its potentially curable nature. Accordingly, the primary objective of antitumor therapy remains the achievement of definitive cure for patients with this aggressive B-cell malignancy [7].
Despite progress in diagnostics and therapy, DLBCL remains a major unresolved challenge in oncohematology, both scientifically and clinically. This is largely attributable to the high incidence of early relapse, the frequency of primary refractory disease, and substantial disease-related mortality.
Therapeutic management of newly diagnosed DLBCL remains a subject of debate. Currently, several conceptually distinct treatment strategies coexist: risk-adapted approach, which select optimal immunochemotherapy based on progression risk strata; response-adapted approach, which optimize treatment according to dynamic assessments of therapeutic response; molecularly agnostic approach, which apply uniform therapy irrespective of tumor molecular characteristics; and molecularly oriented (targeted) approach, which aim to interrupt key aberrant signaling cascades of lymphomagenesis based on the tumor’s biological profile [8,9].
Notwithstanding this heterogeneity, the leading treatment paradigm for newly diagnosed DLBCL remains molecularly agnostic therapy - principally the programmed immunochemotherapy (ICT) regimen R-CHOP, which is endorsed by national and international clinical guidelines [10,11,12]. Nonetheless, most experts consider the outcomes achieved with this regimen to be suboptimal, motivating the search for innovative strategies to improve first-line treatment efficacy in de novo DLBCL.
A molecularly oriented strategy, grounded in tumor-specific molecular biomarkers, represents a promising and forward-looking solution for first-line therapy. This rationale is supported by several international studies and clinical observations demonstrating successful application of such an approach [13,14,15].
Thus, investigating the effectiveness of differentiated therapy for newly diagnosed DLBCL is a timely and clinically relevant objective.
Materials and Methods
This study represents a continuation of a single-center, prospective, non-randomized interventional clinical trial aimed at personalizing first-line therapy for DLBCL based on mutational profiling.
DLBCL diagnosis was confirmed by immunomorphological examination of tumor biopsy specimens in accordance with the criteria of the revised WHO classification of hematolymphoid neoplasms (2022) [2].
The clinical trial excluded patients with high-grade B-cell lymphoma, primary large B-cell lymphoma of immune-privileged sites (testis, central nervous system, vitreoretinal), and primary mediastinal (thymic) large B-cell lymphoma.
To exclude high-grade B-cell lymphoma, fluorescence in situ hybridization (FISH) was performed to detect rearrangements of the c-MYC, BCL2, and BCL6 genes.
DLBCL genotyping was performed according to the LymphGen classification.
Patients in the first group underwent Sanger targeted sequencing of a 19-gene panel: MYD88, CD79B, TNFAIP3, EP300, PIM1, STAT6, NOTCH1, EZH2, CREBBP, TET2, NOTCH2, BTG1, CD70, TNFRSF14, DTX1, MPEG1, MTOR, TBL1XR1, and TP53. The results convincingly demonstrated both the rationale and effectiveness of this diagnostic method for determining the genotype of DLBCL.
Since preliminary sequencing yielded encouraging results but revealed a high proportion of unclassified genotypes, we subsequently expanded the targeted lymphoid gene panel. Patients in the second group underwent whole-exome sequencing of a 60-gene panel: ARID1A, B2M, BTG1, BTG2, CCND3, CD70, CD79B, CIITA, CREBBP, DDX3X, DTX1, DUSP2, EP300, EZH2, FAS, GNA13, IRF4, IRF8, KMT2D, MPEG1, MYD88, NOTCH1, NOTCH2, PIM1, PRDM1, SGK1, SOCS1, STAT3, STAT6, TBL1XR1, TET2, TNFAIP3, TNFRSF14, TP53, ZFP36L1, MTOR, NFKBIA, ETV6, ACTG1, OSBPL10, C-MYC, BCL2, BCL6, FOXO1, ATM, CD79A, PIK3CD, PTEN, CD5, CD58, CDKN2A, CDKN2B, ASXL1, KRAS, EPHB1, BCL10, PRKCB, PLCG2, CARD11, and MEF2B.
Initial staging was performed according to the Ann Arbor classification, modified by the Lugano 2014 criteria, including PET/CT and unilateral bone-marrow trephine biopsy [16]. If baseline PET/CT was not feasible due to disease severity, contrast-enhanced whole-body CT was performed at the onset.
The first and second cohorts included 35 and 8 patients, respectively, all with newly diagnosed DLBCL.
The treatment protocol included one induction cycle of ICT with R-CHOP as bridge therapy pending receipt of molecular profiling results, followed by initiation of five induction cycles of R-CHOP-X (X - an additional antitumor agent). Depending on the identified genotype, patients received one of the agents designated as X: the first group received Vorinostat, Acalabrutinib, Decitabine, or Lenalidomide; the second group received Acalabrutinib, Decitabine, or Lenalidomide (Table 3 and Table 4).
Treatment response was evaluated according to the International Lugano Criteria [17]. Adverse events were recorded by type and severity in accordance with the National Cancer Institute Common Terminology Criteria for Adverse Events (NCI CTCAE), version 5.0 [18].
Statistical analysis was performed using R software, version 4.2.2 (https://www.r-project.org). The analysis comprised descriptive and inferential components. Categorical variables are presented as percentages. Quantitative variables are presented as means ± standard deviations.
Kaplan-Meier methodology was used to generate PFS and OS curves. OS was calculated as the time from therapy initiation to death from any cause, and was censored with the date of last available follow-up. PFS was calculated as the time from therapy initiation to disease progression, relapse, or death from any cause.
Results
Analysis of the study results was performed as of September 16, 2025. Clinical outcomes of patients with newly diagnosed DLBCL are presented in Table 5.
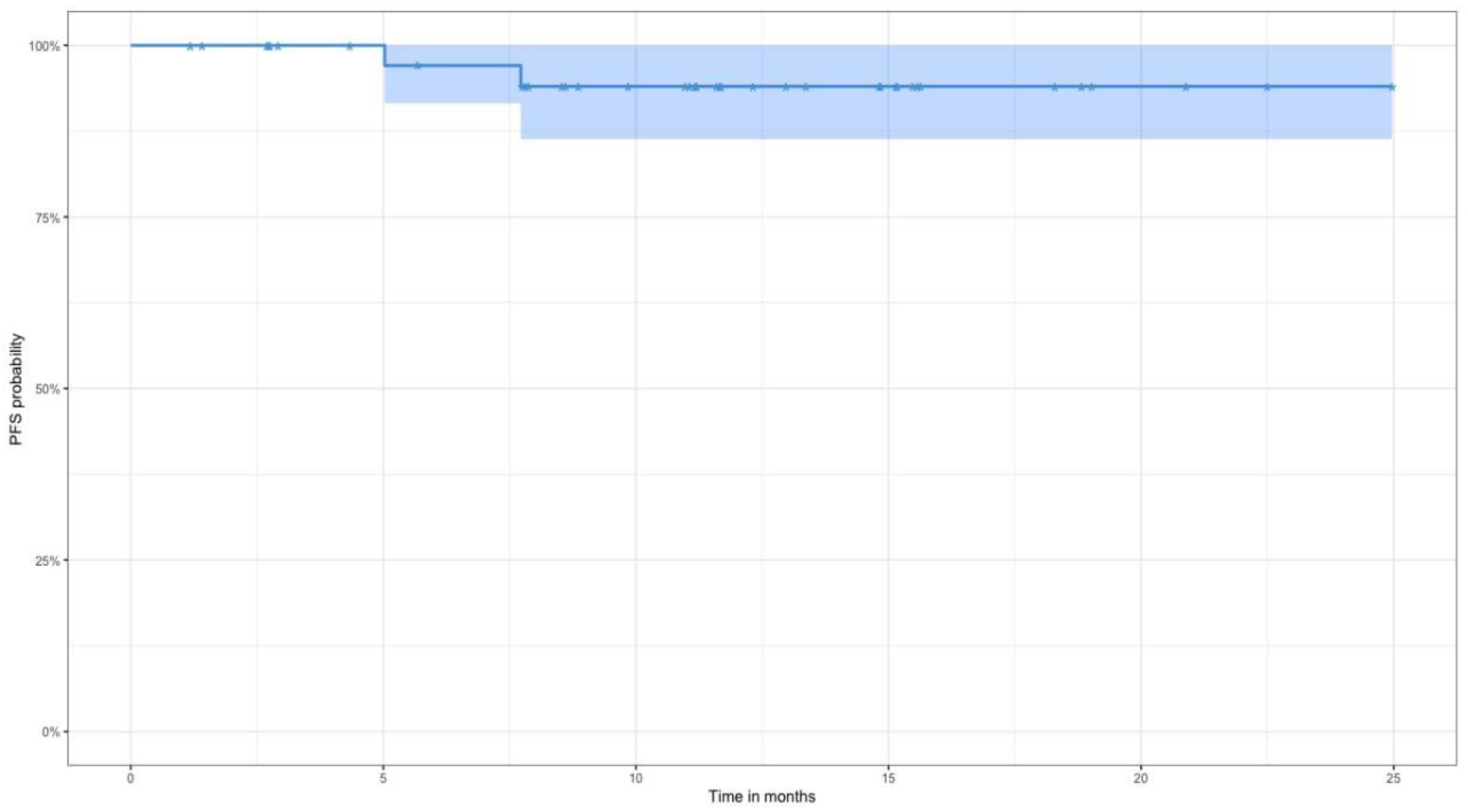
Table 2. year OS and PFS for all patients with newly diagnosed DLBCL are shown in Figure 1: 2-year OS was 92% (95% CI 83%–100%), PFS was 94% (95% CI 86%–100%). Two immunomorphologically confirmed early relapses were recorded.
Figure 1.
2-year overall survival values (n = 43).
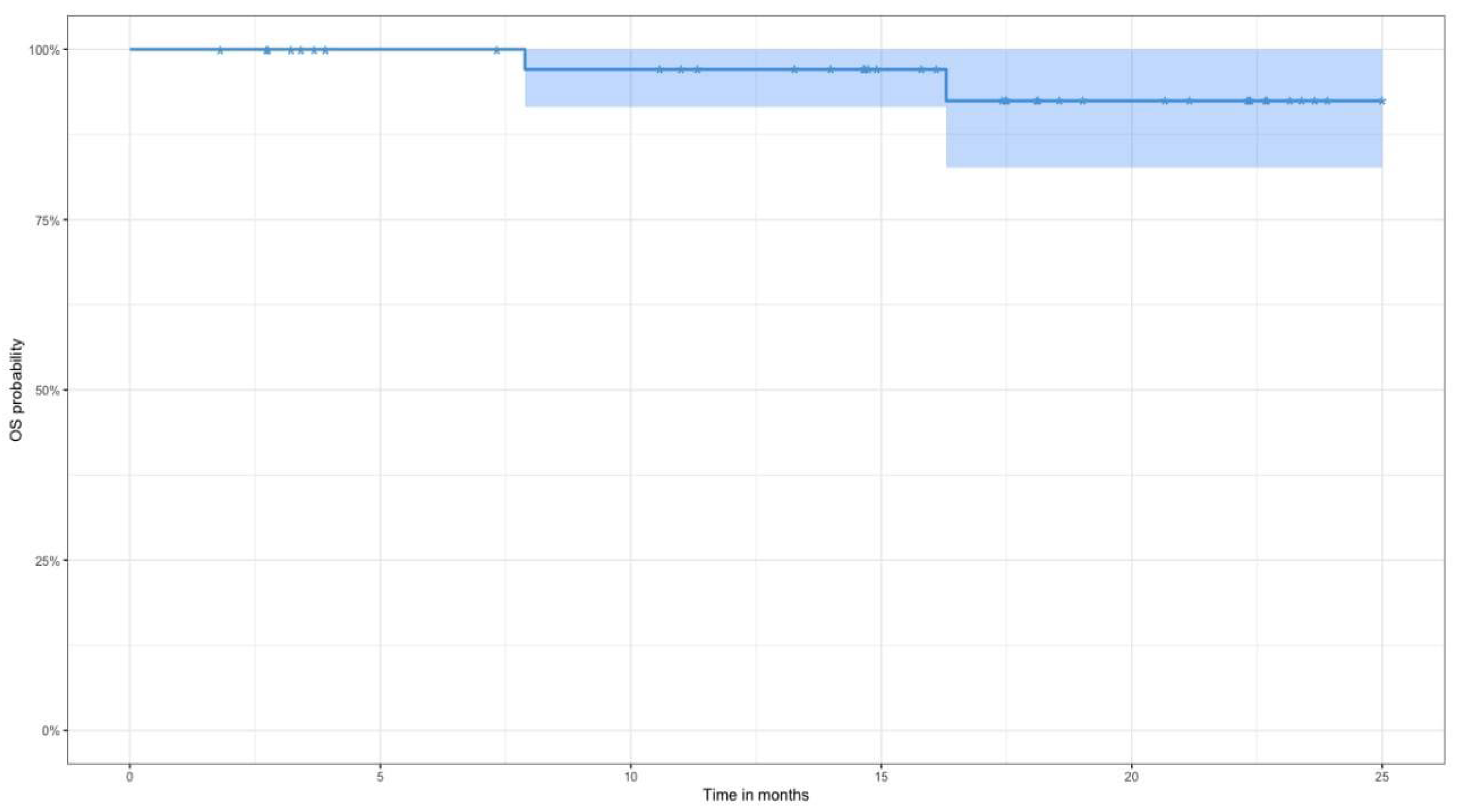
Figure 2.
2-year progression-free survival values (n = 43).
Discussion
From a molecular biology perspective, DLBCL is an extremely heterogeneous disease. In recent years, the focus of clinical research has shifted toward personalized medicine, and DLBCL treatment is following this trend. Implementation of molecular diagnostics aimed at identifying biomarkers introduces a new stage in the management of newly diagnosed DLBCL.
The present clinical study is a unique project that, for the first time in the Russian Federation, implemented a personalized molecularly oriented approach to first-line therapy for newly diagnosed DLBCL. The analysis encompassed clinical and molecular-biological characteristics of the patients, direct efficacy, toxicity, and two-year PFS and OS.
The complete metabolic response in the analyzed cohort among those who completed therapy (n=35) was 100%. Eight patients remain on treatment - the overall response rate is 100%. The two-year PFS and OS for the patients included in this work reached 94% and 92%, respectively, which is particularly important given the predominance of patients at high risk of early progression by IPI (3–5 points) in the studied cohort.
As noted above, several fundamentally different strategies exist for treating newly diagnosed DLBCL.
The primary clinical tool used in routine practice to stratify patients by risk is the IPI. According to IPI, patients are divided into low-risk (0–2 points) and high-risk (3–5 points) groups. Considering results from studies of risk-adapted approach, standard R-CHOP-21 is appropriate for patients at low risk of early progression, whereas Pola-R-CHP is recommended for high-risk DLBCL and, in some cases, planning of high-intensity induction therapy [19] may be considered.
Cellular therapies are actively entering frontline treatment for newly diagnosed DLBCL. Bispecific monoclonal antibodies directed against CD20xCD3 have demonstrated high efficacy in high-risk DLBCL as components of risk-adapted therapy. For example, Epcoritamab combined with R-CHOP in a phase Ib/II study in patients with high-risk DLBCL according to IPI showed high efficacy: overall and complete metabolic response rates were 100% and 76%, respectively [20]. A randomized phase III trial is currently ongoing to evaluate the efficacy and safety of adding Epcoritamab to R-CHOP in patients with high-risk DLBCL [21]. Similarly, the efficacy of another bispecific antibody, Glofitamab, in combination with Pola-R-CHP is under investigation in the context of risk-adapted therapy [22].
Another approach is the response-adapted therapy strategy. Previous attempts to implement response-adapted strategies using intensified antitumor immunochemotherapy did not demonstrate a proven survival benefit. In the PETAL trial, patients after two cycles of R-CHOP with a PET/CT-positive interim response (ΔSUVmax <66%) were randomized to two groups. The first one continued standard R-CHOP, while the second received a Burkitt-like intensified regimen. The results showed that therapy intensification did not improve survival but was associated with markedly increased toxicity [23]. Currently, the SAKK 38-19 study is evaluating whether adding Acalabrutinib to R-CHOP after two cycles in patients with a PET/CT-positive interim scan and/or lack of a molecular response can improve clinical outcomes [24].
First-line CAR-T cell therapy has demonstrated high antitumor activity in patients with high-risk large B-cell lymphoma. The ZUMA-12 study design combined criteria of both risk-adapted strategy (IPI ≥3) and response-adapted strategy (Deauville score 4–5 on interim PET/CT). The study enrolled 40 patients who received Axicabtagene Ciloleucel (axi-cel). Overall and complete response rates were 89% and 78%, respectively, while one-year PFS and OS were 74.6% and 90.6%. Median OS was 24.5 months [25]. A randomized phase III trial, ZUMA-23, is currently ongoing comparing axi-cel with standard therapy in high-risk patients (NCT05605899).
According to guideline recommendations, molecularly agnostic regimens, particularly R-CHOP - remain the standard of therapy for newly diagnosed DLBCL. However, effectiveness of R-CHOP is markedly reduced in molecularly unfavorable DLBCL subtypes [9]. The totality of clinical and biological evidence supports a shift from molecularly agnostic to molecularly directed strategies based on the tumor’s genetic architecture.
In recent years, several pivotal clinical trials have evaluated the efficacy of molecularly targeted chemoimmunotherapy. In the randomized REMoDL-B trial published in 2019, adding Bortezomib to standard R-CHOP did not confer a benefit in the studied cohort [26]. However, updated REMoDL-B results published in 2023 indicated that the Bortezomib plus R-CHOP combination was more effective in ABC-DLBCL [27].
The randomized PHOENIX trial assessed the efficacy and safety of adding Ibrutinib, a Bruton’s tyrosinekinase inhibitor, to R-CHOP in patients with non-GCB DLBCL [28]. The trial did not meet its primary endpoint. A retrospective analysis that stratified patients by genetic subtype using the LymphGen algorithm, however, showed a survival benefit from Ibrutinib in younger patients with MCD- and N1 genotypes of DLBCL (3-year event-free survival for those genotypes was 100%). Preclinical data had predicted an improved response in MCD but not in N1 [29].
In the randomized phase II GUIDANCE-01 trial, the R-CHOP-X approach - where the choice of an additional antitumor agent was dictated by genetic subtype according to LymphGen - produced statistically and clinically meaningful improvements in both early and long-term outcomes versus R-CHOP [15]. Overall response rate was higher with R-CHOP-X compared with R-CHOP (92% vs 73%, p=0.005), and complete response rates were 88% versus 66% (p=0.003). Two-year PFS was 88% in the R-CHOP-X group versus 63% in the R-CHOP (p<0.001), and two-year OS was 94% versus 77% (p=0.001).
Two ongoing multicenter, prospective, randomized trials are currently evaluating the efficacy and safety of personalized treatment approaches for newly diagnosed DLBCL: GUIDANCE-02 and GUIDANCE-05.
In GUIDANCE-02, all patients received a single induction cycle of standard R-CHOP after diagnosis, followed by tumor stratification according to molecular subtype using the LymphPlex classification and subsequent 1:1 randomization to complete the remaining five cycles either as R-CHOP-X or standard R-CHOP. Within the R-CHOP-X group, patients with MCD-, BN2-, or N1- subtypes received the BTK inhibitor Orelabrutinib in combination with R-CHOP; patients with EZB-, ST2-, or NOS subtypes received the immunomodulatory agent Lenalidomide with R-CHOP; and patients harboring TP53 mutations received the hypomethylating agent Decitabine combined with R-CHOP. The trial enrolled 1100 patients across 58 centers in China.
GUIDANCE-05 enrolls patients aged 18-75 years with newly diagnosed DLBCL and a IPI score of 2-5 who demonstrate a ≥3-log reduction in circulating tumor DNA (ctDNA) after one cycle of Pola-R-CHP. Following tumor stratification by genetic subtype using LymphPlex, patients are randomized 1:1 to receive the subsequent five cycles as either Pola-R-CHP-X or standard Pola-R-CHP. Patients with MCD-, BN2-, or N1- subtypes will receive the BTK inhibitor Zanubrutinib in combination with Pola-R-CHP; those with EZB-MYC+/−, ST2-, or NOS subtypes will receive Lenalidomide with Pola-R-CHP; and patients with TP53 mutations will receive Decitabine with Pola-R-CHP. The primary endpoint of this study is PFS.
Taken together, these trials test the hypothesis that combining distinct therapeutic modalities can improve outcomes in patients with newly diagnosed DLBCL. The most promising strategy appears to be an integrated approach that couples molecularly-adapted therapy with response-adapted based on dynamic ctDNA monitoring.
Conclusion
Contemporary studies, including the present work, indicate that implementation of personalized therapy guided by the tumor mutational profile has the potential to substantially change the treatment paradigm for newly diagnosed DLBCL. This approach yields high antitumor efficacy and supports further optimization of therapy through precision-guided strategies.
Author Contributions
Conceptualization, M. Mingalimov, E. Baryakh and E. Misyurina; methodology, M. Mingalimov, E. Baryakh and E. Misyurina; validation, M. Mingalimov, E. Baryakh and E. Misyurina; formal analysis, M. Mingalimov and E. Baryakh; investigation, M. Mingalimov, E.Baryakh, A. Misyurin, L. Kesaeva, A. Mkrtchyan, M. Orlova, O. Kochneva, E. Zotina, G. Tyshkevich, M. Donskoy, T. Tolstykh, T. Chudnova, D. Ivanova, S. Andreev, D. Lebedev, L. Shimanovskaia, K.Tsurkina, V.Basova, N. Bekreneva, S. Rodnikov, I.Abramov, N.Bodunova; Resources, M. Mingalimov, E. Baryakh and the clinical research team; data curation, M. Mingalimov, E. Baryakh and E. Misyurina; writing - original draft Preparation, M. Mingalimov, E. Baryakh, E. Misyurina, M. Orlova and G. Tyshkevich; visualization, M. Mingalimov; supervision,E. Misyurina, E. Baryakh; writing - review & editing Preparation, M. Mingalimov, E. Baryakh, E. Misyurina and M. Orlova; project administration, E. Misyurina, E. Baryakh, S.Gadzhieva, T.Semina, I. Samsonova and M. Lysenko. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by the Ministry of Science and Higher Education of the Russian Federation.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and was approved by the d, Moscow Healthcare Department.
Informed Consent Statement
Written informed consent was obtained from all participants.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
ABC activated B-cell-like
BTK Bruton tyrosine kinase
C-MYC cellular myelocytomatosis oncogene
CT computed tomography
DLBCL diffuse large B-cell lymphoma
DUSP2 dual specificity phosphatase 2
FISH fluorescence in situ hybridization
GCB germinal center B-cell-like
NOS not otherwise specified
OS overall survival
PFS progression-free survival
PET positron emission tomography
WES whole-exome sequencing
WHO World Health Organization
References
- Hilton, L.K.; Scott, D.W.; Morin, R.D. Biological heterogeneity in diffuse large B-cell lymphoma. Semin. Hematol. 2023, 60, 267–276. [Google Scholar] [CrossRef] [PubMed]
- Alaggio, R.; Amador, C.; Anagnostopoulos, I.; Attygalle, AD.; Araujo, IB.; De, O.; Berti, E.; Borges, A,M.; Boyer, D.; Calaminici, M. The 5th edition of the World Health Organization Classification of Haematolymphoid Tumours: Lymphoid Neoplasms. Leukemia 2022, 36(7), 1720–48. [Google Scholar] [CrossRef] [PubMed]
- Campo, E.; Jaffe, E.S.; Cook, J.R.; Quintanilla-Martinez, L.; Swerdlow, S.H.; Anderson, K.C.; Brousset, P.; Cerroni, L.; de Leval, L.; Dirnhofer, S.; et al. The International Consensus Classification of Mature Lymphoid Neoplasms: a report from the Clinical Advisory Committee. Blood 2022, 140, 1229–1253. [Google Scholar] [CrossRef] [PubMed]
- Lacy, S.E.; Barrans, S.L.; Beer, P.A.; Painter, D.; Smith, A.G.; Roman, E.; Cooke, S.L.; Ruiz, C.; Glover, P.; Van Hoppe, S.J.L.; et al. Targeted sequencing in DLBCL, molecular subtypes, and outcomes: a Haematological Malignancy Research Network report. Blood 2020, 135, 1759–1771. [Google Scholar] [CrossRef] [PubMed]
- Wright, G.W.; Huang, D.W.; Phelan, J.D.; Coulibaly, Z.A.; Roulland, S.; Young, R.M.; Wang, J.Q.; Schmitz, R.; Morin, R.D.; Tang, J.; et al. A Probabilistic Classification Tool for Genetic Subtypes of Diffuse Large B Cell Lymphoma with Therapeutic Implications. Cancer Cell 2020, 37, 551–568.e14. [Google Scholar] [CrossRef]
- Chapuy, B.; Wood, T.; Stewart, C.; Dunford, A.; Wienand, K.; Khan, S.J.; Serin, N.; Wang, M.; Calabretta, E.; Shimono, J.; et al. DLBclass: a probabilistic molecular classifier to guide clinical investigation and practice in diffuse large B-cell lymphoma. Blood 2025, 145, 2041–2055. [Google Scholar] [CrossRef]
- Shi, Y.; Xu, Y.; Shen, H.; Jin, J.; Tong, H.; Xie, W. Advances in biology, diagnosis and treatment of DLBCL. Ann. Hematol. 2024, 103, 3315–3334. [Google Scholar] [CrossRef]
- Vodicka, P.; Klener, P.; Trneny, M. Diffuse Large B-Cell Lymphoma (DLBCL): Early Patient Management and Emerging Treatment Options. OncoTargets Ther. 2022, ume 15, 1481–1501. [Google Scholar] [CrossRef]
- Dabrowska-Iwanicka, A.P.; Nowakowski, G.S. DLBCL: who is high risk and how should treatment be optimized? Blood 2024, 144, 2573–2582. [Google Scholar] [CrossRef]
- Thieblemont, C.; Da Silva, M.G.; Leppä, S.; Lenz, G.; Cottereau, A.; Fox, C.; Lopez-Guillermo, A.; Illidge, T.; Jurczak, W.; Eich, H.; et al. Large B-cell lymphoma (LBCL): EHA Clinical Practice Guidelines for diagnosis, treatment, and follow-up. HemaSphere 2025, 9, e70207. [Google Scholar] [CrossRef]
- Fox, C.P.; Chaganti, S.; McIlroy, G.; Barrington, S.F.; Burton, C.; Cwynarski, K.; Eyre, T.A.; Illidge, T.; Kalakonda, N.; Kuhnl, A.; et al. The management of newly diagnosed large B-cell lymphoma: A British Society for Haematology Guideline. Br. J. Haematol. 2024, 204, 1178–1192. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health of Russia. Clinical guidelines for the diagnosis and treatment of aggressive B cell lymphomas (КР129_3). Available online: https://cr.minzdrav.gov.ru/view_cr/129_3 (accessed on 12.04.2025).
- Mingalimov, M.A.; Baryakh, E.A.; Misyurin, A.V.; Kesaeva, L.A.; Mkrtchyan, A.S.; Misyurina, E.N.; Tolstykh, T.N.; Orlova, M.S.; Akhmadeeva, A.A.; Chudnova, T.S.; et al. Personalized genotype-directed antitumor therapy for newly diagnosed diffuse large B-cell lymphoma: efficacy and toxicity of the R-CHOP-X protocol in a single-center, non-randomized, prospective clinical trial (first results). Oncohematology 2024, 19, 84–92. [Google Scholar] [CrossRef]
- Mingalimov, M.A.; Baryakh, E.A.; Tolstykh, T.N.; Misyurin, A.V.; Kesaeva, L.A.; Mkrtchyan, A.S.; Kovrigina, A.M.; Misyurina, E.N.; Orlova, M.S.; Chudnova, T.S.; et al. Personalized Approach to Treatment of Newly Diagnosed Diffuse Large B-Cell Lymphoma Patients with Respect to Molecular Landscape: A Case Report and Literature Review. Clin. oncohematology 2025, 18, 177–183. [Google Scholar] [CrossRef]
- Zhang, M.-C.; Tian, S.; Fu, D.; Wang, L.; Cheng, S.; Yi, H.-M.; Jiang, X.-F.; Song, Q.; Zhao, Y.; He, Y.; et al. Genetic subtype-guided immunochemotherapy in diffuse large B cell lymphoma: The randomized GUIDANCE-01 trial. Cancer Cell 2023, 41, 1705–1716.e5. [Google Scholar] [CrossRef]
- Cheson, B.D.; Fisher, R.I.; Barrington, S.F.; Cavalli, F.; Schwartz, L.H.; Zucca, E.; Lister, T.A. Recommendations for initial evaluation, stag-ing, and response assessment of Hodgkin and non-Hodgkin lymphoma: The Lugano classification. J. Clin. Oncol. 2014, 32, 3059–3068. [Google Scholar] [CrossRef]
- Yoo, K.H. Staging and response assessment of lymphoma: a brief review of the Lugano classification and the role of FDG-PET/CT. BLOOD Res. 2022, 57, S75–S78. [Google Scholar] [CrossRef]
- Freites-Martinez, A.; Santana, N.; Arias-Santiago, S.; Viera, A. CTCAE versión 5.0. Evaluación de la gravedad de los eventos adversos dermatológicos de las terapias antineoplásicas. Actas Dermo-Sifiliograficas 2021, 112, 90–92. [Google Scholar] [CrossRef]
- Babicheva, LG; Poddubnaya, IV. Challenges and perspectives of first-line therapy in patients with diffuse B-cell lymphoma: A review. Journal of Modern Oncology (in Russian). 2023, 25(2), 178–184. [Google Scholar]
- Falchi, L.; Clausen, M.; Offner, F.; de Vos, S.; Brody, J.; Linton, K.M.; Snauwaert, S.; Cordoba, R.; Wu, J.; Bykhovski, I.; et al. Metabolic response rates of epcoritamab + R-CHOP in patients with previously untreated (1L) high-risk diffuse large B-cell lymphoma, including double-hit/triple-hit lymphoma: Updated EPCORE NHL-2 data. J. Clin. Oncol. 2023, 41, 7519–7519. [Google Scholar] [CrossRef]
- A study to evaluate change in disease activity in subcutaneous (sc) epcoritamab combined with intravenous and oral rituximab, cyclophosphamide, doxorubicin hydrochloride, vincristine and prednisone (R-CHOP) or R-CHOP in adult participants with newly diagnosed diffuse large B-cell lymphoma (DLBCL) (EPCORE DLBCL-2). ClinicalTrials.gov identifier: NCT05578976. Updated 14 Nov 2023. Accessed 17 Nov 2023. LINK (https://clinicaltrials.gov/study/NCT05578976).
- A phase II study of glofitamab + polatuzumab-R-CHP for patients with high-risk diffuse large B-cell lymphoma. ClinicalTrials.gov identifier: NCT05800366. 13 Sep 2023. Available online: https://clinicaltrials.gov/ct2/show/NCT05800366 (accessed on 17 Nov 2023).
- Dührsen, U.; Müller, S.; Hertenstein, B.; Thomssen, H.; Kotzerke, J.; Mesters, R.; Berdel, W.E.; Franzius, C.; Kroschinsky, F.; Weckesser, M.; et al. Positron Emission Tomography–Guided Therapy of Aggressive Non-Hodgkin Lymphomas (PETAL): A Multicenter, Randomized Phase III Trial; Annual Meeting of the German, Austrian, and Swiss Societies of Hematology and Medical Oncology. LOCATION OF CONFERENCE, COUNTRYDATE OF CONFERENCE; pp. 2024–2034.
- Assessing a ctDNA and PET-oriented therapy in patients with DLBCL. A multicenter, open-label, phase 2 trial. ClinicalTrials.gov identifier: NCT04604067. 18 Apr 2023. Available online: https://clinicaltrials.gov/ct2/show/NCT04604067 (accessed on 17 Nov 2023).
- Neelapu, S.S.; Dickinson, M.; Munoz, J.; Ulrickson, M.L.; Thieblemont, C.; Oluwole, O.O.; Herrera, A.F.; Ujjani, C.S.; Lin, Y.; Riedell, P.A.; et al. Axicabtagene ciloleucel as first-line therapy in high-risk large B-cell lymphoma: the phase 2 ZUMA-12 trial. Nat. Med. 2022, 28, 735–742. [Google Scholar] [CrossRef]
- Davies, A.; E Cummin, T.; Barrans, S.; Maishman, T.; Mamot, C.; Novak, U.; Caddy, J.; Stanton, L.; Kazmi-Stokes, S.; McMillan, A.; et al. Gene-expression profiling of bortezomib added to standard chemoimmunotherapy for diffuse large B-cell lymphoma (REMoDL-B): an open-label, randomised, phase 3 trial. Lancet Oncol. 2019, 20, 649–662. [Google Scholar] [CrossRef]
- Davies, A.J.; Barrans, S.; Stanton, L.; Caddy, J.; Wilding, S.; Saunders, G.; Mamot, C.; Novak, U.; McMillan, A.; Fields, P.; et al. Differential Efficacy From the Addition of Bortezomib to R-CHOP in Diffuse Large B-Cell Lymphoma According to the Molecular Subgroup in the REMoDL-B Study With a 5-Year Follow-Up. J. Clin. Oncol. 2023, 41, 2718–2723. [Google Scholar] [CrossRef]
- Younes, A.; Sehn, L.H.; Johnson, P.; Zinzani, P.L.; Hong, X.; Zhu, J.; Patti, C.; Belada, D.; Samoilova, O.; Suh, C.; et al. Randomized Phase III Trial of Ibrutinib and Rituximab Plus Cyclophosphamide, Doxorubicin, Vincristine, and Prednisone in Non–Germinal Center B-Cell Diffuse Large B-Cell Lymphoma. 60th Annual Meeting of the American-Society-of-Hematology (ASH); LOCATION OF CONFERENCE, COUNTRYDATE OF CONFERENCE; pp. 1285–1295.
- Wilson, W.H.; Wright, G.W.; Huang, D.W.; Hodkinson, B.; Balasubramanian, S.; Fan, Y.; Vermeulen, J.; Shreeve, M.; Staudt, L.M. Effect of ibrutinib with R-CHOP chemotherapy in genetic subtypes of DLBCL. Cancer Cell 2021, 39, 1643–1653.e3. [Google Scholar] [CrossRef]

Table 1.
Summary characteristics of patients (n = 35). .
| Parameters | Number of patients, n (%) |
| Age, median, range (years) | 63 (38-78) |
| ECOG performance status ≥ 2 | 24 (54) |
| Sex - male | 15 (43) |
| IPI 3-5 | 28 (80) |
| Stage by Ann Arbor (Lugano modification, 2014) II III-IV |
14 (40) 21 (60) |
| Immunophenotype GCB nonGCB |
11 (32) 24 (68) |
| Co-expression of c-MYC/BCL2 | 1 (3) |
| «Single-hit» | 2 (7) |
| LymphGen: MCD N1 BN2 EZB A53 ST2 NOS |
2 (6) 11 (31) 2 (6) 5 (14) 0 (0) 3 (9) 12 (34) |
Table 2.
Summary characteristics of patients (n = 8). .
| Parameters | Number of patients, n (%) |
|---|---|
| Age, median, range (years) | 58 (60-78) |
| ECOG performance status ≥ 2 |
1 (12) |
| Sex - male |
4 (50) |
| IPI 3-5 |
3 (38) |
| Stage by Ann Arbor (Lugano modification, 2014) II III-IV |
4 (50) 4 (50) |
| Immunophenotype GCB nonGCB |
3 (38) 5 (62) |
| Co-expression of c-MYC/BCL2 | 1 (12) |
| «Single-hit» | 0 |
| LymphGen: MCD N1 BN2 EZB A53 ST2 NOS |
1 (12) 1 (12) 0 (0) 2 (26) 1 (12) 2 (26) 1 (12) |
Table 3.
R-CHOP-X treatment regimen in the first patient group.
| Drug | Dosage and rout of adminisrtation | Days of administration | LymphGen genotype |
| Rituximab | 375 mg/m2, intravenously | 0 | - |
| Doxorubicin | 50 mg/m2, intravenously | 1 | - |
| Vincristine | 1.4 mg/m2, intravenously | 1 | - |
| Cyclophosphamide | 750 mg/m2, intravenously | 1 | - |
| Prednisone | 60 mg/m2, intravenously | 1-5 | - |
| Acalabrutinib | 100 mg twice daily, orally | 1-21 | MCD, N1, BN2 |
| Lenalidomide | 25 mg once daily, orally | 1-10 | ST2, NOS |
| Vorinostat | 400 mg once daily, orally | 1-9 | EZB |
| Decitabine | 10 mg/m2, intravenously | 1-5 | A53 |
Table 4.
R-CHOP-X treatment regimen in the second patient group.
| Drug | Dosage and rout of adminisrtation | Days of administration | LymphGen genotype |
|---|---|---|---|
| Rituximab | 375 mg/m2, intravenously | 0 | - |
| Doxorubicin | 50 mg/m2, intravenously | 1 | - |
| Vincristine | 1.4 mg/m2, intravenously | 1 | - |
| Cyclophosphamide | 750 mg/m2, intravenously | 1 | - |
| Prednisone | 60 mg/m2, intravenously | 1-5 | - |
| Acalabrutinib | 100 mg twice daily, orally | 1-21 | MCD, N1, BN2 |
| Lenalidomide | 25 mg once daily, orally | 1-10 | ST2, NOS |
| Decitabine | 10 mg/m2, intravenously | 1-5 | A53, EZB |
Table 5.
Outcomes of patients with newly diagnosed DLBCL, n (%).
| Outcome | Completed therapy (n = 35) | Ongoing therapy (n = 8) |
| Overall response | 35 (100) | 8 (100) |
| Complete response | 35 (100) | 8 (100) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



