
Submitted:
24 December 2023
Posted:
26 December 2023
You are already at the latest version
Abstract
background: The Islamic Republic of Iran has been under sanctions since 1979. These sanctions were further reinforced between the years 2005 and 2012. This study utilizes available data from Iran post-sanctions to review the impact of economic sanctions on both the mental health and the quality of life of Iranian citizens.Methods: A comprehensive scoping review was conducted to identify studies examining the impact of sanctions on health in Iran. Searches were initiated in 2012 using PubMed/Medline, Embase, Web of Science, Scopus, and the Scientific Information Database (Iranian Database) with keywords such as sanctions, implications, mental health, quality of life, civilian mental health, and Iran. Subsequent to the screening process, secondary reports and letters to the editor were excluded. Only original studies—those collecting data via observation, interviews, surveys, experiments, or literature reviews—were retained for analysis. In addition to these search strategies, reference scanning was undertaken to identify additional articles pertinent to the scope of the current study. This thorough approach facilitated the discovery of relevant and significant articles exploring the effects of sanctions against Iran on the mental health and overall well-being of its civilian population. Following the search, duplicate articles were meticulously identified and removed by the authors. Data were subsequently extracted and summarized, focusing on study characteristics and the observed effects of sanctions on civilian mental health and quality of life in Iran.Result: Out of 165 items identified in the preliminary search, ten articles met the inclusion criteria. These selected articles highlighted the pronounced effects of sanctions on various health-related domains.Conclusion: Since 2012, Iran has been subject to intensified sanctions. There is evidence to suggest that the economic sanctions, imposed by Western nations, and have exerted a negative and detrimental impact on the health of individual Iranians.
Keywords:
Iran sanctions
; Post-sanctions data
; Mental health in Iran
; Sanctions implications
; Economic sanctions effects
; Western nations sanctions
Introduction
Trade sanctions are strict foreign policy measures that governmental bodies impose by curbing economic ties with another country with the intent to pressure them to accede. These economic sanctions are meant to avert war or other violent means to gain submission. Economic relations encompass trade and financial agreements. Hence, sanctions disrupt economic networks, either fully or in part, including air, communications, postal, rail, radio, sea, and telegraphic sectors, as well as lead to declining international relations. UN members must discuss these aspects with the Security Council [1]. In an attempt to make one country resolve or reconsider conflicting policy decisions, another country may compel them through these sanctions, for instance, to restrain nuclear development. Post-Cold War, sanctions are meant as another less violent yet deadly substitute for war. Although these sanctions are levied on governments to modify policies, those affected most are the target country’s common people. Mortality and suffering are a result of imposed sanctions and humanitarian efforts themselves cannot pacify those who belong to the lower strata. Thus, sanctions’ influence on the macroeconomic and political aspects has always been a contentious issue. As Iran’s nuclear activities came under scrutiny beginning in 2003, because of its unclear objectives, the country was asked to cease its enrichment and reprocessing activities and research. However, in 2006, given that the IAEA believed that the responses on Iran’s part were unsatisfactory, the case of Iran was brought to the UN Security Council, which also did not find the trust-building attempt satisfactory. Iran questioned the Council’s sanction proposals related to its nuclear activities in 2007, and no economic sanctions were implemented apart from those in the military and nuclear industry. However, some countries decided to proceed with coercive diplomacy and imposed economic sanctions in 2012 [1,2].
Post-sanctions Iran’s revenues plummeted, currency devaluated, with added surge in inflation and unemployment. These aspects fiddled with the civilians’ right basic requirements of standard life including nutritious food, healthcare and medicine [1]. Apart from lower medicine supply there are many factors which dwindles health and health services; namely water, sanitation, infrastructure, electrical supply, ambulance services and hospital set up. Diminished civilian health is also found to be as a result of limited access to imported raw materials and machines for production purposes. Effectiveness of humanitarian immunity is more theory than practicable to sustain health and health services. Other than weakened physical and medical infrastructure sanction imposed restricted state cash flow impacts maintenance and administrative costs roil the provision of better services and sub-optimal reflex to medical emergencies. Demotivation creeps in people with the deteriorating quantity and quality of health services who might consider abandoning these services. Embargo wrecks havoc on employment and livelihoods forcing civilians to opt for alternative social and economic activities. This paper attempts to investigate the detrimental effect of western sanctions to Iran its impact on health, mental health and quality of life [3]. This paper discussed about economic sanctions and violations that it incurs. Economic sanctions and the consequences on health, medical care and food security in Iran, its repercussions on mental health and quality of life of the inhabitants are presented.
METHOD
The current research paper address a systematic review based on the published studies that examined the implications of Iran Sanctions on Civilian Mental Health and Quality of life. In order to report the methods and results, the model of Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) was employed as a research strategy. However, a protocol for this systematic review was not registered in any protocol registries.
Research Study Eligibility Criteria
Published research studies exclusively that examined implications of Iran Sanctions on Civilian Mental Health and Quality of life were carefully included in this review for systematic analysis. The study eligibility criteria for presented was delineated by including all research papers existing and accessible, be it, based on experiments, surveys, observation, interviews, whether quantitative or qualitative. However, letters to the editors, commentaries, and short communications were debarred from the review and analysis.
Search Stratagem and Information Sources
The period for carrying out search as well as the target information sources were outlined for the present review. The duration of search period was limited and confined to January 2012 onwards as there has been an intensification in sanctions in Iran from 2005 to 2012. Therefore, it appears to be an appropriate period for reviewing the effects of sanctions, based on published information. Thus, using these demarcations for the present study the published articles and information was explored. The information sought was limited to only one language i.e. English and Persian and the data bases used for the search were also the ones providing the research information in only English language. The databases selected for present study search included Web of Science, Scopus, Pubmed, PubMed Central, Embase, Medline and Scientific Information Database (Iranian Database). The information search was conducted in January 2019 and restructured in June 2020 with the intent of acquiring all the suitable and relevant publications published after 2012. For making the most effective use of information search specific words were selected as key words to be used for search in the data bases. a situation or resource. The keywords comprised: “Iran“, “Sanctions”, “implications”, “mental health”, “quality of life” and “civilian mental health”. The search stratagem was wide-ranging in order to be as inclusive as probable. The information search was made via the text words plus the controlled vocabulary. Additional research was also carried out on Google Scholar with the same keywords to locate more publications and not to miss out any significant information. In addition to these search strategies, to locate further publications with reference to the scope of present study a reference scanning was also conducted. This complete stratagem assisted in accessing the suitable and noteworthy articles published regarding the implications of Iran sanctions on civilian mental health and quality of life. After search, the duplicates were deleted carefully by the authors. Afterwards, the research studies were crosschecked by two independent reviewers.
Identification of Sources of Evidence
Each suitable identified research study was verified by the authors independently. At the outset the titles and abstracts were examine for significance and relevance. Consequently, the full-length studies were examined to settle that which research study was appropriate for inclusion in the review (based on the inclusion criteria).
Quality assessment
A quality assessment tool was utilized for the quality assessment of each selected article which measured three facets, 1) study plan and design, 2) sample characteristics, and 3) data collection tools. Each facet was rated on a rating scale of 0–3, where a high score denoted a high methodological quality (Table 1).
Data Analysis
An extraction strategy was designed as a form to sift the information concerning the aims and objectives, and methodology of the research, data analysis, and results. After extraction of the required data, the findings of eligible studies were synthesized. (Figure 1)
No Sample Involvement
The present study was a review based study in which there was no public or patient involvement. Neither any sample was requested to make statements on the study design and nor was consulted to develop patient related outcomes or interpretation of the findings. Patients were not asked to play a part in the inscribing or editing of this research paper for readability or precision.
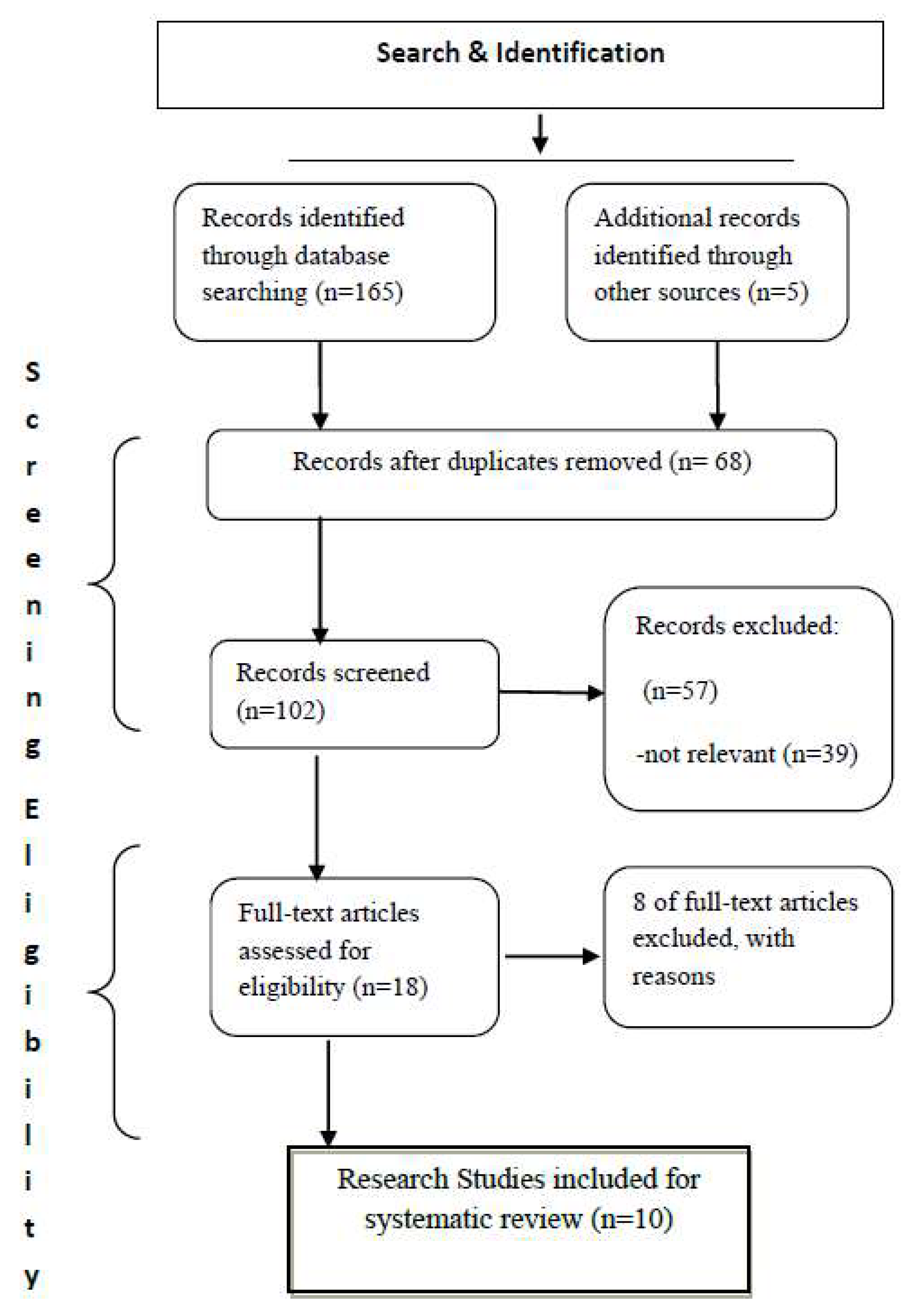
We retrieved 165 records; records were excluded due to duplication. During the initial stage, 102 references, including letters to the editor and articles addressing the effect of sanctions on areas other than health, were excluded on examination of the title and abstract. In the next stage, 18 articles were chosen for full-text reading, out of which 10 studies were included. The flow chart in figure 1 illustrates our selection process. The characteristics of included studies are demonstrated in Table 1.

Table 1.
Summery of the included studies.
| ID | Authors | Relevant Findings | Humanitarian Effects | score | ||
|---|---|---|---|---|---|---|
| Healthcare | Medicine | Determinants of Health | ||||
| 1 | Gorji [4] | Economic sanctions against Iran influenced all branches of Iranian economy and affected vulnerable patient. Unavailability of medicine and raw materials for domestic pharmaceutical companies and medical equipment for hospitals and unaffordability of medicines were big challenges of Iran during sanction’s period.- The weakened medical infrastructure decreased the ability of the health system to provide services even in medical emergencies.- Establishing uniform operational criteria and definitions for exemptions of medicine and medical products from sanctions in the future sanction regimes is necessary | * | * | high | |
| 2 | International Institute for Peace Justice and Human Rights [5] | Sanctions on Iran have had destructive effects on healthcare system, Iranian’s lives and quality of life. Because of sanctions on banking system, import of medicines has become difficult. These are violations of the basic human rights | * | * | * | meduim |
| 3 | Shahabi, Fazlalizadeh, Stedman, Chuang, Shariftabrizi & Ram [6] | Iran's NCCP has substantial deficits, including a serious shortage of medicines for cancer care. Sanctions exempted medicines and food, but lead to disruption of health services through complications in shipment or lack of foreign currencies | * | high | ||
| 4 | Zare, Trujillo, Leidman & Buttorff [7] | Income elasticity is lowest for the poorest Iranians in urban and rural areasEconomic sanctions on Iran have the potential to disrupt government-subsidized healthcare services | * | meduim | ||
| 5 | Deilamizade & Esmizade [8] | Because of economic sanctions, the price of goods and services including drugs has increased in Iran. Major changes in the drug use patterns and an increase in use-related harms of drug are expected in near future. | * | meduim | ||
| 6 | Massoumi & Koduri [9] | Sanctions caused limitations in the import of medicines (pharmaceutical ingredients and finished products) and access to patented ones. The quality of substituted medicines was not satisfactory while these scare medicines were not affordable for some groups of patients. | * | high | ||
| 7 | Ahmadi & Meskarpour-Amiri [10] | Study of targeted countries by sanctions including Iran showed that through limiting access to minimum basic needs, economic sanctions can threaten public health especially health of the mothers and children of poor families. Reduction of target countries’ revenues can lead to reduction of government capacity to finance healthcare system and increase of the share of households in healthcare costs and adversely affect access to healthcare services. | * | high | ||
| 8 | Farzanegan, Mohammadikhabbazan & Sadeghi [11] | Iranian economy and households are affected enormously by economic sanctions. The welfare of all income groups of households in urban and rural areas has declined. | * | meduim | ||
| 9 | Sha'bani, Mahkoei & Ghorbani [12] | Socio-economic status of Iranians is influenced adversely by the sanctions in recent years. Iran is facing a great deal of different challenges such as unemployment, inflation and depression, immigration, and marriage problem, brain drain and economic downturn. | * | high | ||
| 10 | Marzban [13] | Since the economy of Iran is dependent to oil revenues, the sanctions resulted in decrease of Iranians’ welfare. | * | meduim | ||
Results
In order to synchronize foreign policies of governments, firm actions in the form of economic sanctions have long been employed by western countries. Those countries that tend to have independent views and policies are made to undergo economic adversity to fall in line. But the hardest hit by these coercive actions are the ordinary citizens who have to endure immense difficulty with social and economic issues not to mention the human rights violations.
Sliding toward a deep recession
Due to its ongoing nuclear initiatives in recent years, Iran’s economy has suffered greatly from the global community’s sanctions. In 2015, President Hassan Rouhani made a pact with the United States and five other superpower nations to minimize its nuclear activities in exchange for a reduction of the sanctions imposed on Iran [14,15,16].
Economic sanctions’ effect on Iran
Drugs and raw materials
Essentially, the sanctions against Iran’s existing nuclear activities had detrimental effects on the Iranian people’s health, affecting their limited access to medicines and declining health services. It has left approximately six million people seeking various treatments for a long list of illnesses. As a result of the imposed sanctions, Iran’s pharma sector cannot meet its domestic needs, causing some difficulties in producing generic drugs and resulting in importing low-quality medicines and other raw materials abroad without ensuring their potency. In Setayesh and Tim’s (2016) study, it was noted that the increasing economic sanctions took a major toll on Iran’s medical shortages, which severely affected the living conditions of Iranian patients and their human right to good health [17].
Impact of sanctions and psychological warfare on the mental health and quality of life of Iranians
In 2018, Kokabisaghi assessed the effects of economic sanctions on Iranians’ right to health by using a human rights impact assessment tool (HRIA) in his systematic review. The International Community of Nations is well able to predict the humanitarian effects of sanctions and could have chosen any one of the many available and necessary means to prevent such humanitarian distress. Furthermore, Iran should have used any mandatory means to protect people from the adverse effects of the sanctions [1]; now, after the fact, they must focus on alleviation of their negative impact. Nevertheless, some of the effects, like disability and death, cannot be changed. In the future, when sanctions are considered, decision makers should establish an international convention to mitigate such impacts on targeted countries’ populations [1].
Economic Sanctions
The expanded global market major super powers post-Cold War did not opt for military engagements. To urge nations to comply in an attempt to achieve peace and block civil or overseas war, the United Nations and other countries prefer to impose economic sanctions rather than engage in military intervention. The consequence of this action is an obstacle to the sanctioned country’s economic development and affects the entire population’s welfare. Some of the sanctions’ coercive foreign policy measures include countries having to face revoking political relations, and adverse influences on the economy and communications. Further, the countries are targeted by limiting import or export trade activities, freezing bank accounts, restricting travel, elevating tariff rates, and other pressure tactics that influence the economy immensely [18].
Compared to a war’s irreversible repercussions, economic sanctions appear to be a milder option. However, the very intention to preserve human rights that the target country is expected to uphold is violated once sanctions are imposed, as the civilians residing in the sanction-imposed areas suffer drastic adverse effects on their health. Human rights violations that follow the imposition of economic sanctions inevitably include the rights to: people’s life, liberty, and security, freedom of opinion and expression, adequate food, the highest possible standard of physical and mental health, provision of medical assistance and healthcare, adequate clothing and housing, adequate environmental conditions, adequate standard of living that can ensure health and well-being, education, work and to just and favourable work conditions, social security, and the right to participate in government [19].
The basic fabric International human rights which pledged to safeguard and honour basic human needs are shredded once a country is subjected to sanctions dissolving the very the spirit of the International Covenant. further more to political and civil rights, the 1948 Universal Declaration of Human Rights refers to an individual’s right to better living standards and seek optimal health and well-being; inclusive of food security and medical care [20]. Lately, in 1976, the International Covenant on Economic, Social, and Cultural Rights extended support towards achieving best standard of physical and mental health; and asked for all countries participation in attaining the prevention, treatment, and disease control and proper delivery of medical care [21]. A balance between maintaining law and human right protection is always expected by international law. In times bereft of war it is mandatory to maintain provision of civilians and medical supplies, chances of contagious diseases and epidemics could be deflected by giving adequate access to medical centers, hospitals, and other public health infrastructure. These parameters are acceptable even at times of economic sanctions and war [21].
Humanitarian efforts are most of the time excluded from the range of sanctions. But how can this be possible if foreign currency is made unavailable, bank accounts are not allowed to function, or cross-border transactions are not allowed? Stringency in terms of trade, export licenses retrieval, or transportation surveillance make access to food and medicine difficult. Clinically, this refers to promoting the highest standards of medical care for individual patients. Physicians must concentrate on their expertise and duty and try to diffuse any possible tension emanating from government policy decisions. Health is an amalgamation of mental, physical, and social well-being, and there is a fundamental association between conserving human rights and the promotion of health. Higher socioeconomic status and better health status are often interlinked [21].
Generally, several countries worldwide are undergoing enormous psychosocial stresses and issues; this has affected people’s psychological well-being and has created a lack of primary physical and mental healthcare requisites. The existence of psychological well-being and a lack of mental illness provides endurance to everyday stress and plays active role within the social precincts of the community where an individual resides. Mental and behavioral disorders are major forms of diseases. The total estimated rise in mental and neurological disorders from 1990 to 2020 is expected to be 15%. Mental disorders are one of the leading causes of disability and early mortality. Previous retrospective clinical data records and epidemiological studies have shown statistically the preponderance of the total number of mental disorders. Presently, advanced screening questionnaires and standard clinical interviews are employed for more accuracy in the estimation. According to the WHO 2001, mental and behavioral disorders are the most frequent, with 25% affected during their lifetime. The 2013 NSDUH data showed the 12-month prevalence of mental illness was 18.5% in those ≥18 years [22].
Iran’s mental health facilities
Even though spacious mentally ill shelters existed in Iran since 1940 they were not in workable conditions. The transition came about in the 1950s and 60s when psychiatric hospitals and departments came about in the 1950s and improved services were rendered to psychiatric patients. 1983 saw the establishment of improved primary health-care system but after Iran-Iraq war concerns mental health problems shot up. In 1986, although there was increased incidence of mental disorders it had low capacity to respond, mostly in rural areas. To tackle this issue the first National Programme on Mental Health was developed in Iran to cater to the underprivileged, deprived, and at-risk populations and provide access to primary mental health-care facilities. It was pledged that a mental health was made available to all Iranians by the year 2000 the primary health-care system was employed as the primary delivery platform for its execution. Four categories of mental disorders were selected and were asked to see the general physicians and follow up these patients based on the instructions. After 15 years mental health facilities were functioning in rural health centres in 2005. The programme saw increased implementation and awareness but this was not matched with the outcomes, physician skills, supply of psychiatric medications, and outcomes of the treatment. Industrialization and urbanization, added up the number of cases but mental health programme was unprepared to take it up [23].
Iran embargoes and mental health
Based on the present state of events patients tend to be anxious about the future. This feature culminates into multiple forms of anxiety disorder in which these individuals dwell on feelings of extreme anxiety and fear. Elevated personal, social and economic liability precipitate to anxiety disorders [24]. It is common for anxiety disorders to be associated with other psychological conditions especially major depressive disorder [25].
Epidemiologic studies have indicated that a major proportion of Iranians suffer from mental disorders and psychological conditions. Prevalence of mental disorders is only next to that of unintentional injuries with respect to preponderance of disease in Iran, which is almost 16% of the overall burden of diseases [26]. In Iran, psychological disorders estimate 10.8% of the total population, out of which anxiety disorders is frequent with 8.4% [27]. It is the aftermath of low socioeconomic status, illiteracy; low level of education, unemployment translates into people with inferior socioeconomic status and poorer health indices [28].
In accordance to a survey performed in 1999, 21% of the Iranian population ≥ 15 years suffered from mental disorders. The preponderance of mental disorders as per the prevalence of mental disorders GHQ-28 ranged from 21% to 34.2%. Out of every 4 citizen at least one suffered from a mental disorder. The second survey conducted in (2001), showed a frequency of 17.0% as assessed by SADS. in the third nationwide survey of mental disorders, While GHQ-28 and the CIDI enumeration in 2011 yielded a 22.7% presence of mental health. These variable outcomes were due to statistical population, scoring methods and dynamics of social, economic, and political situation of Iran. An upswing of mental illness is evident from the Iranian studies 21% in 1999 to 23.44% in 2017 [22].
The outcomes of a 12 months national MHS conducted by employing Composite International Diagnostic Interview CIDI diagnostic tool in 2011 revealed anxiety disorders to be 15.6%. All types of anxiety disorders exhibited increased prevalence of anxiety disorders in females (19.4%) relative to males (12%). As per the study generalized anxiety disorder (5.2%), obsessive-compulsive disorder (5.1%) and social phobia (3.2%) were the frequent forms of anxiety disorders [29].
Female sex has a higher propensity towards anxiety related disorders. This could be attributable to environmental factors, genetics [30], female sex hormones and related cycles [31,32]. Greater fear response and penchant for safety is prominent in females as opposed to males; the difference is reflected through imaging studies in the presence of anterior cingulated cortex in females [33]. Poor health is directly proportional to socioeconomic factors like inadequate education, low income, stress, unhealthy lifestyle and occupational conditions [34]. Illiteracy and poor education underrate people [35], apart from this limited accessibility to mental health services, social support and health care services are also expected [36,37]. Poverty, unemployment and incarceration are often linked to being uneducated [36]. Poor education does not directly correlate to mental health problems if social solidarity is at one’s disposal [38]. It is very clear that unemployment accelerates the development and aggravation of psychiatric disorders [39,40]. Negative impact of psychosocial and work functioning, increased fatigue and sleep disturbance, limited physical health, suicide attempts, global cognitive impairment and social disability are consequences of generalized anxiety disorder [41].
Mental health in children and adolescents
The incidence of anxiety disorders is varied based on the different regions of Iran. In pre-pubescent children, the preponderance of anxiety disorders is 2.6% to 41.2%, and Zarafshan et al presented a grimmer picture of 6.8% to 85% of Iranian children and adolescents being afflicted with such disorders. Bandar Abbes city was the area with the highest frequency of anxiety disorders, but this needs further evaluation. Separation anxiety disorder frequency ranged between 0.7% to 15.7% among Iranian children and adolescents. Generalized anxiety disorder ranged from 0.54% to 12.8%, with an exception in Abhor, where generalized anxiety disorder was 20%. OCD ranged from 1% to 11.9% among Iranian children and adolescents, while the incidence of social phobias was as high as 8% to 23.5% among this populations. Overall, this high prevalence of social phobia among Iranian children and adolescents needs to be considered. Specific phobias were found to be 1.6% and 3%, and the frequency rate of panic disorder was 1% and 1.2% for agoraphobia, which is slightly higher than two studies reporting the. Across all the reports, anxiety disorders were almost double for females relative to males [42].
Quality of Life in Iran
Although it is not easy to define quality of life medically, Qol presents several different nuances and meanings that include psychological, social and emotional, functional capacity, life satisfaction, and social support parameters. In the absence of a definitive definition, all non-medical aspects of diseases are enlisted under the term of Qol [43]. A good quality of life is synonymous with the state of being in control; having the autonomy and ability to choose; having a pleasant self-image; feeling a sense of belonging; being hopeful and positive; and participating in sensible and fun tasks. On the contrary, severe mentally unhealthy individuals exist mostly in the state of ill-being. Those with mental issues might experience a poor quality of life, as they live with such mental health difficulties as feelings of suffering and uncontrolled behavior; a lack of choice and autonomy; poor self-esteem and confidence; a sense of not being part of society; diminished activity; and a sense of hopelessness and dejection with life in general [44].
Subjective well-being is associated with actual affective state, which can oscillate swiftly. Social participation tends to disrupt well-being easily, although it may largely be a gradual process. Environmental living conditions, either material or social, can also interrupt functioning. As depression progresses, individuals’ subjective well-being diminishes, although the person may be continuing with day-to-day social activity. Even if functioning is hampered in certain cases, material living conditions and social support may remain unchanged. While in some instances, once social participation has dwindled because of an extended period of the disease, and while environmental assets, both material and social, have diminished as well, a patient may regain psychological well-being rather quickly, but not sufficiently to perform social roles. Even if at all environmental living conditions were to be gained [45].
A complex time issue may exist if one’s expectations are inconsistent with what is at hand. QoL is high if the disparity between expectations and achievements are narrow. From this perspective, the complexity increases with respect to each individual’s priority, whether a better life at present or better conditions in the future. The disparity must be lower. Among multiple escapes, such as tranquilizers or alcohol, fast-acting psychotropics can provide short-term relief from the constant mental conflict that the individual is experiencing. Therefore, it may naturally transition into substance abuse, which may cause the gap to widen, and this dependence indicates reduced psychological well-being, a waning of social presence, and deteriorating living conditions, both environmental and social. In the rampant administration of first-generation narcoleptics, patients had to choose between two options: the use of narcoleptics reduced the frequency of recurrence, although serious side effects ensued and patients had to weigh the advantages and disadvantages between bearing the costs and side effects or enduring them for future good outcomes. This scenario could be changed through the use of novel atypical antipsychotics [42].
Geriatric people do not enjoy complete mental health condition. Measures have to be taken by family members, society, and government alike in keeping them occupied, old age pension scheme or elderly self-help set will ensure them to lead a contentful life. Evidence have accepted the fact that not having financial independence have detrimental effects on the mental and physical health of geriatric people [45].
Immediate attention with regards to Iran’s fragile health insurance system and limited health finance is called for. It is emphasized for providing improved quality of care, to counter non-communicable diseases associated medical errors, and induced demand must be addressed within the health-care provision in Iran’s health care domain. For financial risk protection measures alterations in health-care provision, integrating the family physician and home care facilities, better quality of care, and implementing national guidelines [23].
Psychiatric disorders and traumatic injuries in Iran
Psychiatric issues and injuries are bi-directionally associated. The worldwide incidence of deaths due to injury is 10%. Injury-related disability-adjusted life years (DALY) have increased in the last 20 years, and injury is featured among the leading attributes contributing to disability rates. Similarly, psychiatric disorders and major public health problems are linked with high disability rates. Importantly, unipolar depressive disorder is the largest reason of YLD and its impact on DALY rates increased in 2030. In Iran, injuries leading to mental disorders are linked with the highest disability rates amongst all age brackets and sexes, leading to 16% and 28% of DALY, respectively. Mental issues related to injuries, irrespective of the injury or organ damage, have been elucidated on a large scale. These issues are a result of anxiety disorders such as post-traumatic stress disorder (PTSD), mood issues due to major depressive disorder (MDD) and alcohol abuse. On the contrary, maladaptive coping mechanisms and psychopathology is the main reason in the people with a background of psychopathology. Mental illness is also a reason behind higher rates of injuries. Children and adolescents also demonstrate these behaviors. The injured population reflects increased rates of having previously experienced mental illness. Traumatic brain injury (TBI) also seemed to be common among psychiatric patients. Cognitive impairment, decreased concentration and drowsiness due to medicines could be the reason for these aspects. Therefore, the association between injuries with mental and behavioral disorders among the general public was evaluated [46].
Psychological features and drug use in Iran
The interlink between psychological features and drug abuse was longitudinally assessed from preschool through 18 years of age. Among the adolescents who tried drugs, those who used marijuana were found to be the best-adjusted. Interpersonal estrangement, inadequate impulse control, and apparent emotional distress were observed more frequently in adolescents who abused drugs than those who had never tried drugs. Meanwhile, children’s earliest impressions primarily consist of their interactions with their parents; this determines their psychological health and influences the variation between drug addicts, experimenters, and those who refrain from drug use. Unfortunately, today the psychological reasons underlying drug use have not been sufficiently investigated; rather, treatment concentrates on the symptoms. Evidence indicates that drug abuse is itself merely a symptom and not related to personal or social maladjustment, and that it is primarily influenced by an individual’s personality traits and development [47]. Deilamizade (2015) assessed drug abusers in drop-in centers (n = 23) and at-home treatment facilities (n = 25) in Tehran. The outcomes indicate that when the cost of drugs is high, users opt for cheaper drugs, which can negatively impact their health. Even the mode of administration, such as needle sharing, is more harmful under such circumstances, and money for drugs may be retrieved from illegal sources. Embargoes have caused a continual decline in the economic status of Iranians since 2006, which intensified in 2010 and 2011. These economic embargoes also increased the cost of drugs, among other items. Consequently, they have altered drug use trends and intensified harm caused by drug abuse, which as a result is estimated to rise in the future [8].
Suicide in Iran
The interaction between demographic, social, and cultural factors has contributed to suicide in Iran, which is an essential public health issue. The global incidence of suicides was 804,000, as per the WHO, in 2012 alone. It is predicted that by 2020, 1.53 million individuals will succumb to suicide. Although Islamic countries have traditionally had low suicide rates, suicide statistics have shown an upward trend lately. Iran currently has suicide rates of 5.3 per 100 000 individuals (3·6 in women and 7·0 in men). Suicide is a direct consequence of domestic disputes (32%), matrimonial issues (26%), financial limitations (12%), and academic challenges (5%). Various factors contribute to the prevalence of suicide, such as genetics, mental illness, familial conflicts, political and socio-economic conditions, and geography. Urban lifestyles bring added stress with higher suicide rates in cities compared to rural areas. Drug use and self-immolation are common modes of committing suicide in Iran. Providing life skills training and psychological support for youth, increasing household income, and offering pre-marriage counseling could help to reduce the nation’s suicide rate [48].
Conclusion
There is unanimity regarding the role of population health in achieving sustained economic growth of a country; similarly, having a healthier population is a result of economic growth. Any attempt to curb the economy through sanctions does not independently hamper the country’s financial wellbeing; rather, it has a tremendous per capita impact, which naturally extends to the overall physical and mental wellbeing of the citizens in places where sanctions are imposed. This is to say nothing of the brazen disruption of human rights stemming from sanctions, which is equivalent to that of war-ridden countries. the repercussions of imposing those sanctions should have been considered beforehand and thus possibly averted. A willingness to consider the impact of sanctions on the targeted country, in this case Iran, is a way to safeguard the interests and welfare of each and every individual dwelling there. Irreversible damage, like disability and mortality, cannot be corrected; thus, preventing the negative impact of sanctions is a more pragmatic strategy. Embargoes have severe implications for the indigenous population and calculated execution is expected.
Authors' contributions
MT came up with the idea of the systematic review. Methodology was planned, designed, and initial search performed by MT, ST, FA. Duplicates were removed by MT. ST did title/abstract and full-text screening. MT and ST were all involved in data extraction, and writing the body of the manuscript.
Funding Sources
There was no funding provided by any agency of institute for the conduction of the present study.
Ethics approval and consent to participate
The present study was a review based study in which there was no public or patient involvement. Neither any sample was requested to make statements on the study design and nor was consulted to develop patient related outcomes or interpretation of the findings. Patients were not asked to play a part in the inscribing or editing of this research paper for readability or precision.
Consent for Publication
Not Pertinent.
Availability of data and materials
Not Pertinent.
Competing interests
The authors have no conflicts of interests.
Acknowledgement
The authors of the article would like to thank the cooperation and assistance of all those who helped us in this research.
References
- Kokabisaghi1, F. Assessment of the Effects of Economic Sanctions on Iranians’ Right to Health by Using Human Rights Impact Assessment Tool: A Systematic Review, Int J Health Policy Manag. 2018; 7(5): 374–393. [CrossRef]
- 2.U.S. Department of the Treasury. Sanctions Programs and Country Information. Accessed 10 oct 2019, Available From: https://www.treasury.gov/resource-center/sanctions/programs/pages/iran.aspx.
- Akbarpour N, Abbasi M. The Impact of the U.S. Economic Sanctions on Health in Cuba, October 2014, Available From: https://www.researchgate.net/publication/313116398.
- Gorji, A. Sanctions against Iran: The Impact on Health Services. Iran J Public Health. 2014;43(3):381-382. [PubMed]
- International Institute for Peace Justice and Human Rights. The impact of sanction on Iranian People Healthcare. Switzerland: International Institute for Peace, Justice and Human Rights; 2013.
- Shahabi S, Fazlalizadeh H, Stedman J, Chuang L, Shariftabrizi A, Ram R. The impact of international economic sanctions on Iranian cancer healthcare. Health Policy. 2015;119(10):1309-1318. [CrossRef]
- Zare H, Trujillo AJ, Leidman E, Buttorff C. Income elasticity of health expenditures in Iran. Health Policy Plan. 2013;28(6):665-679. [CrossRef]
- Deilamizade A, Esmizade S. Economic Sanctions Against Iran, and Drug Use in Tehran, Iran: A 2013 Pilot Study. Subst Use Misuse. 2015;50(7):859-868. [CrossRef]
- Massoumi RL, Koduri S. Adverse effects of political sanctions on the health care system in Iran. J Glob Health. 2015;5(2):020302. [CrossRef]
- Ahmadi AM, Meskarpour-Amiri M. The public health effects of economic sanctions as a global concern in 21th century: Why the economic sanctions is a cruel strategy. Journal Health Policy Sustainable Health. 2015;2(1):145-146.
- Farzanegan MR, Mohammadikhabbazan M, Sadeghi H. Effect of oil sanctions on the macroeconomic and household welfare in Iran: New evidence from a CGE model. Joint Discussion Paper Series in Economics; 2015.
- Sha'bani M, Mahkoei H, Ghorbani E. Investigating Socioeconomic Challenges of Iran During Sanctions. International Journal Resistive Economics. 2015;3(1):18-37.
- Marzban HO, A. The Impact of Economic Sanctions on Gross Domestic Product and Social Welfare for Iran: Generalized Stochastic Growth Model. Econ Res. 2015;20(63):37-69. [CrossRef]
- Six charts that show how hard US sanctions have hit Iran. [https://www.bbc.com › news › world-middle-east-48119109]. Accessed 2019.
- Dendrinou V, Chrysoloras N. EU, China, Russia Defy Trump With Plan to Keep Trading With Iran.[https://www.bloomberg.com/news/articles/2018-09-25/eu-defies-trump-with-plan-to-enable-continued-trade-with-iran]. Accessed 25 sep 2018.
- Sadeghi S. For Many Iranians, Staying In the Nuclear Deal No Longer Makes Sense. [https://foreignpolicy.com/2019/09/24/for-many-iranians-staying-in-the-nuclear-deal-no-longer-makes-sense/]. Accessed 24 sep 2019.
- Setayesh S, Mackey T. K. Addressing the impact of economic sanctions on Iranian drug shortages in the joint comprehensive plan of action: promoting access to medicines and health diplomacy. Globalization and health. 2016; 12(1): 31. [CrossRef]
- Garfield, R. The Impact of Economic Sanctions on Health and Well-being. Relief and Rehabilitation Network (RRN). London: Overseas Development Institute; 1999.
- Hoskins, E. Nutt S. The Humanitarian Impact of Economic Sanctions on Burundi. Occasional Paper 29, Watson, Institute for International Studies (Providence: Watson Institute); 1997.
- Human Rights Watch, Cuba's Repressive Machinery: Human Rights Forty Years After the Revolution, 1 June 1999, 2343, available at: https://www.refworld.org/docid/3ae6a85f0.html [accessed 22 July 2019].
- Morin K, Miles S.H. The Health Effects of Economic Sanctions and Embargoes: The Role of Health Professionals. Ethics and Human Rights Committee. Annals of Internal Medicine. 2000; 132(2):158-61. [CrossRef]
- Noorbala AA, Faghihzadeh S, Kamali K, Bagheri Yazdi SA, Hajebi A, Mousavi MT, Akhondzadeh S, Faghihzadeh E, Nouri B. Mental health survey of the adult population of Iran in 2015. Arch Iran Med. 2017; 128–134. [PubMed]
- Danaei G, et al. Iran in transition, The Lancet. 2019; 393(10184): 1984-2005. [CrossRef]
- Ipser JC, Stein DJ. A systematic review of the quality and impact of anxiety disorder meta-analyses. Current psychiatry reports. 2009; 11: 302-309. [CrossRef]
- Aina Y, Susman JL. Understanding comorbidity with depression and anxiety disorders. J Am Osteopath Assoc. 2006; 106(5 Suppl 2): S9–14.
- Naghavi M, Abolhassani F, Pourmalek F, Lakeh M, Jafari N, Vaseghi S, Mahdavi Hezaveh N, Kazemeini H. The burden of disease and injury in Iran 2003. Popul Health Metr. 2009; 7:9. [CrossRef]
- Mohammadi MR, Davidian H, Noorbala AA, Malekafzali H, Naghavi HR, Pouretemad HR, et al. An epidemiological survey of psychiatric disorders in Iran. Clin Pract Epidemiol Ment Health. 2005; 1:16. [CrossRef]
- Marmot, M. The status syndrome: how social standing affects our health and longevity. New York: Owl Books; 2004.
- Hajebi A, Motevalian SA, Rahimi-Movaghar A, Sharifi V, Amin-Esmaeili M, Radgoodarzi R, Hefazi M. Major anxiety disorders in Iran: prevalence, sociodemographic correlates and service utilization, BMC Psychiatry. 2018; 18:261. [CrossRef]
- Kendler KS, Walters EE, Neale MC, Kessler RC, Heath AC, Eaves LJ. The structure of the genetic and environmental risk factors for six major psychiatric disorders in women. Phobia, generalized anxiety disorder, panic disorder, bulimia, major depression, and alcoholism. Arch Gen Psychiatry. 1995; 52(5): 374–83. [CrossRef]
- Shear, MK. Anxiety disorders in women: gender-related modulation of neurobiology and behavior. Semin Reprod Endocrinol. 1997; 15(1): 69–76. [CrossRef]
- Redmond, G. Mood disorders in the female patient. Int J Fertil Womens Med. 1997; 42(2): 67–72.
- Butler T, Pan H, Epstein J, Protopopescu X, Tuescher O, Goldstein M, et al. Fear-related activity in subgenual anterior cingulate differs between men and women. Neuroreport. 2005; 16(11): 1233–6. [CrossRef]
- World Health Organization. Closing the gap: policy into practice on social determinants of health: discussion paper. Rio de Janeiro: WHO; 2011.
- Luke, A. Critical literacy: foundational notes. Theory Pract. 2012; 51(1): 4–11. [CrossRef]
- Lincoln A, Espejo D, Johnson P, Paasche-Orlow M, Speckman JL, Webber TL, White RF. Limited literacy and psychiatric disorders among users of an urban safety-net hospital's mental health outpatient clinic. J Nerv Ment Dis. 2008; 196(9): 687–93. [CrossRef]
- Vijayalakshmi, P. Ramachandra, Reddemma K, math SB. Perceived human rights violation in persons with mental illness: role of education. Int J Soc Psychiatry. 2013; 59(4):351–64. [CrossRef]
- Lincoln A, Paasche-Orlow MK, Cheng DM, Lloyd-Travaglini C, Caruso C, Saitz R, Samet JH. Impact of health literacy on depressive symptoms and mental health-related: quality of life among adults with addiction. J Gen Intern Med. 2006; 21(8): 818–822. [CrossRef]
- Zhang S, Bhavsar V. Unemployment as a risk factor for mental illness: combining social and psychiatric literature. Adv Appl Sociol. 2013; 3(2): 131–136. [CrossRef]
- Paul KI, Moser K. Unemployment impairs mental health: meta-analysis. J Vocat Behav 2009; 74: 264–282. [CrossRef]
- Haller H, Cramer H, Lauche R, Gass F, Dobos GJ.The prevalence and burden of subthreshold generalized anxiety disorder: a systematic review. BMC Psychiatry. 2014; 14: 128. [CrossRef]
- Zarafshan H, Mohammadi M, Salmanian M, Prevalence of Anxiety Disorders among Children and Adolescents in Iran: A Systematic Review. Iranian Journal of Psychiatry. 2015; 10(1): 1-7. [PubMed]
- Katschnig H.Quality of life in mental disorders: challenges for research and clinical practice. World Psychiatry. 2006; 5(3): 139–145. [PubMed]
- Connell J, Brazier J, O’Cathain A, Lloyd-Jones M and Paisley S. Quality of life of people with mental health problems: a synthesis of qualitative research. Health and Quality of Life Outcomes. 2012; 10:138. [CrossRef]
- Datta, P.P, Gangopadhyay N, Sengupta B. Association of Psychological Morbidity with Socio-Demographic Characteristics among Elderly: A Cross-Sectional Study from Eastern India, International Journal of Medicine and Public Health. 2013; 3(2) :94-99. [CrossRef]
- Shadloo B, et al. Psychiatric Disorders Are Associated With an Increased Risk Of Injuries: Data From The Iranian Mental Health Survey (Iranmhs). Iran J Public Health. 2016; 45(5): 623–635. [PubMed]
- Shedler J, Block J. Adolescent drug use and psychological health: A longitudinal inquiry. American Psychologist. 1990; 45(5): 612-630. [CrossRef]
- Mirhashemi S, Motamedi A.H, Taghipour H, Danialet Z. Suicide in Iran. The Lancet. 2016; 387(10013): 29. [CrossRef]
Figure 1.
Screening process and selection of articles for Systematic Review according to the PRiSMA statement.
Figure 1.
Screening process and selection of articles for Systematic Review according to the PRiSMA statement.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



