
Submitted:
03 January 2023
Posted:
05 January 2023
You are already at the latest version
Abstract
Abstract: Vulvovaginal candidiasis (VVC) is a mucous membrane infection, with an increased rate of antifungal resistance of Candida species. The in vitro efficacy of farnesol alone or in combination with traditional antifungals, against resistant Candida strains recovered from women with VVC was assessed. In this study, 80 Candida isolats were identified by multi-plex PCR. Antifungal sus-ceptibility of amphotericin B (AMB), fluconazole (FLU), itraconazole (ITZ), voriconazole (VOR), clotrimazole (CTZ) and farnesol was tested by M27-A3/S4 broth micro dilution method. The combinations of farnesol with each antifungal were calculated based on the fractional inhibitor concentration index (FICI). C. glabrata was the predominant species (48.75%) isolated from vaginal discharges, followed by C. albicans (43.75%), C. parapsilosis (3.75%), mixed infection of C. albicans and C. glabrata (2.5%), C. albicans and C. parapsilosis (1%). C. albicans and C. glabrata isolates had lower susceptibility to FLU (31.4% and 23.0%, respectively) and CTZ (37.1% and 33.3%, respectively). Importantly, there was ‟synergismˮ between farnesol-FLU and farnesol-ITZ against C. albicans and C. parapsilosis (FICI= 0.5 and 0.35, respectively), reverting the original azole resistant profile. These findings indicate that farnesol is able to revert to the resistance profile of azole by enhancing the activity of FLU and ITZ in resistant isolates, which is a promising result.
Keywords:
vulvovaginal candidiasis
; farnesol
; azoles
; resistance
1. Introduction
Vulvovaginal candidiasis (VVC) is a major mucous membrane infection of the lower genital tract among women, associated to an increased rate of antifungal resistance of Candida specie the causative agent of vulvovaginal candidiasis (VVC) Furthermore, some women have severe or long-term daily symptoms, that do not respond to topical or oral antifungal therapy, which has been defined as Recurrent Vulvovaginal Candidiasis (RVVC) [1,2,3,4]. Globally, it is estimated that RVVC infects approximately 138 million women annually. In developing countries such as Iran, the prevalence of RVVC is > 4,300 cases per 100,000 women [5,6]. For instance, a recent study by Arastehfar et al., has estimated that Iran is among the countries with the highest rate RVVC, whereas C. albicans and C. glabrata are the most common agents of these infections [7]. Recently, the prevalence of VVC infections has significantly increased, which may be owned to the extensive use of azoles for both prophylactic and therapeutic purposes [8]. Azoles are the first-choice drugs for the initial treatment of VVC, but the long-term use of fluconazole have resulted in the development of multidrug resistance (MDR) and recurrent infections, which is a critical healthcare problem. Due to some limitations related to the availability of certain antifungal drugs, inefficient treatment, high toxicity, low tolerability, and drug interaction, the search for new compounds with antifungal properties is an urgent necessity to overcome the drug resistance phenomenon [9]. Farnesol (C15H26O), a sesquiterpene alcohol that was first described as a quorum-sensing molecule produced in C. albicans, has attracted highly considerable attention regarding its antimicrobial properties [10,11,12]. This substance found in essential oils has different pharmacological activities such as antitumor and antioxidant as well as antimicrobial effect [13]. Some studies have reported that farnesol inhibits hyphae formation, has antioxidant effects, also inhibiting drug transporters. Moreover, previously published data proposed that farnesol has in vitro synergistic effects with various antifungals like nystatin, itraconazole and fluconazole [14,15]. Furthermore, this signaling molecule was observed to inhibit biofilm formation and in combination with certain antifungals, farnesol can serve as an adjuvant in therapy of candidiasis [16].
For this purpose, combination antifungal therapy is considered as a promising strategy, that might increase the effectiveness of common antifungal agents, mitigating the emergence of antifungal resistance among clinical isolates [17,18]. The present study attempted to determine the pattern of antifungal susceptibility of Candida isolates recovered from VVC cases. Achieving desired statistical significance for a given hypothesis about synergistic effect of farnesol on the antifungal susceptibility of Candida clinical isolates collected from VVC, differing in susceptibility were collected and involved in this study. Interestingly, for the possible future application of this quorum-sensing molecule, it was necessary to examine its cytotoxicity on cell line, specifically in order to explore the concentration of farnesol effective in combination with antifungal agents.
2. Materials and Methods
2.1. Sample Collection
80 Candida isolates recovered from 150 women with VVC attended at the obstetrics and gynecology department affiliated to the Birjand University of Medical Sciences (Birjand, Iran) in the period from December 2018 to March 2019.This study was approved by ethics committee of the Iran University of Medical Sciences, Iran(no.1399.921). All participants signed a written consent form before participating in the study.
2.2. Identification of Isolates
2.2.1. Conventional Methods
All isolates were examined for direct examination to detect yeasts and pseudohyphae, and then cultured on Sabouraud dextrose agar (SDA, Merck, Darmstadt, Germany) for viability and purity. After recovery, the primary identification was carried out using conventional methods, such as germ tube test, chlamydospore formation (cornmeal agar test), and CHROM agar Candida medium (CHROMagar™, Sigma-Aldrich, St. Louis, MO, USA) (48 h at 35°C) [19].
2.2.2. Molecular Assay
Multiplex PCR assay, designed by species-specific primers, was applied in order to identify the Candida species. [20]. Genomic DNA was extracted using acetyl trimethylammonium bromide-based method described previously [21]. Species-specific primers [20] were used in this study (Table 1). PCR products were analyzed on 2% agarose gel electrophoresis and checked visually by Gel Doc (Gel Doc XR+, BioRad, BioRad, CA, USA). The identification of Candida species was performed by comparison of the size of the fragments with references’ band profiles. Species with failed identification in the first multiplex PCR were further tested by the second multiplex PCR and, in case of negative results, isolates were checked by a third multiplex.
2.3. Antifungal Susceptibility Testing (AFST)
Antifungal susceptibility of Candida isolates was performed against amphotericin B (AMB), itraconazole (ITZ), voriconazole (VOR), fluconazole (FLU), and clotrimazole (CTZ) (Sigma-Aldrich, Oakville, Canada) using the broth micro dilution method according to Clinical and Laboratory Standards Institute (CLSI M27-A3/S4)guideline [22]. Working dilutions were prepared by using RPMI-1640 medium (Roswell Park Memorial Institute; Sigma Chemical Co., St. Louis, MO, USA) in the concentration ranging from 0.016 to16 μg/mL for AMB, ITZ, VOR, and CTZ whereas FLU was prepared at concentrations ranging from 0.063 to 64 μg/mL were prepared in 96-well flat-bottom microtitre plates (NuncTM, Thermo Fisher Scientific, Illkirch-Graffenstaden, France) and 0.5 x 103 to 2.5 x 103 CFU/mL of each Candida isolates were inoculated each well. The plates incubated at 35°C for 24 h. C. albicans (ATCC10231), C. parapsilosis (ATCC 22019) and C. glabrata (ATCC2001) were used as quality control strains for each testing run. The MIC50 for antifungal was defined as the minimum concentration of drugs to inhibit 50% of fungal growth, while for AMB the concentration of drug that inhibited the 100% of growth was considered as MIC. C. albicans isolates were categorized as susceptible and resistance to FLU; MIC ≥8 μg/mL was considered resistance, MIC ≤2 μg/mL was considered susceptible, and MIC=4 μg/mL was dose-dependent susceptibility. Similarly, the isolates were categorized for other azoles; MIC ≤0.12 μg/mL was susceptible, MIC ≥1 μg/mL was resistant. Regarding to AMB; MIC ≤2 μg/mL was considered susceptible, and MIC ≥2 μg/mL was considered resistant. All tests were performed in three independent experiments and repeated at least three times.
2.4. Antifungal Activity of Farnesol
The activity of farnesol (Sigma-Aldrich, Klongton, Klongtoey , Thailand) on the cell proliferation Candida isolates as previously reported with a minor modification [23]. Farnesol as diluted with methanol when used to obtain a stock solution at a concentration of 30mM. To achieve this, 10µl of farnesol was added to 1 ml 10% methanol. Afterwards, the farnesol stock solution adjusted to a concentration of 300µ. For the in vitro proliferation assay, 103 yeast cells per ml were inoculated in yeast nitrogen base (YNB) medium supplemented with farnesol at different final concentration (5, 10, 20, 50, 100, 150 and 300 µM), employed 96 well-plates and farnesol-free as negative control and AmB for positive control. Cultures were allowed incubation at 32 0C for 24 hours. After this period, rate of growth was determined by measuring the optical dencity (OD) absorption at 630 nm by using ELISA reader (star sate, Germany). Minimum inhibitory concentration (MIC) for farnesol was defined compare to farnesol-free control.
2.5. Combination Study
Combinations of farnesol and classical antifungal (FLU, AMB, ITZ, VOR and CTZ) were tested against resistant isolates based on CLSI (M27-A3/S4) protocol. The fractional inhibitory concentration index (FICI) calculated in order to assess drug interaction [24]. FIC values were obtained by dividing the MIC value of the drug combination by the MIC value of each drug alone. The FICI method was defined using the following equation:
FICI = FIC (A) + FIC (B) = (MIC A combination/MIC A alone) + (MIC B combination/MIC of B alone).
Farnesol and antifungal interactions were classified as (synergism) FICI ≤ 0.5, antagonism (FICI > 4.0, and indifferent (0.5 < FICI ≤ 4.0).
2.6. Cytotoxcity Assay
In order to assess the cytotoxicity effect of farnesol on SW48 cell line, the cytotoxcity assay was carried out according to the Bio vision protocol [25]. In brief, the SW48 cell line were seeded (1 x 106 cell/mL) in the 96-well microtiter plate containing RPMI-1640, supplemented by Fetal Bovine Serum 10% (FBS, Sigma-Aldrich, St. Louis, MO, USA) incubated at 37 °C, CO2 5%, 90% humidity. Then, mammalian cells were treated with 300 µM of farnesol. Untreated cells were considered as control group. After 24 h, cells were harvested, washed and 5 x 105cells/mL of cells were transferred to a tube and re-suspended in 100 μL of binding buffer. Then, 5 μL of FITC-conjugated Annexin V (Annexin V-FITC) and 5 μL of propidium iodide (PI) were added, followed by incubation (15 min at room temperature, dark room) and at last directly analyzed by flow cytometer (Calibur, Becton Dickinson, Franklin Lakes, NJ, USA).
3. Results
Three species of Candida were identified in CHROM agar Candida and PCR. C. glabrata was the predominant species (n=39; 48.75%), followed by C. albicans (n=35; 43.75%) and C. parapsilosis (n=3; 3.75%). In addition, two mixed infections were detected including C. albicans and C. glabrata (n=2; 2.5%), C. albicans and C. parapsilosis (n=1; 1%) (Figure 1).
Regarding the susceptibility pattern of Candida species, the highest resistance rate was detected against FLU (65%), and followed by CTZ (66%), particularly related to C. albicans (65.7%) and C. glabrata (71.8%). Importantly, all C. albicans isolates were susceptible to AMB and all three C. parapsilosis were susceptible to ITZ (Table 2). For the isolates of C. albicans, the MIC values of FLU, ITZ, VOR, and CTZ were interpreted based on clinical breakpoints (CBP), while AMB MIC values were evaluated based on epidemiological cut-off values (ECV).
The results showed that the MIC of farnesol ranged from 150 to 300 µM for all isolates and the MIC concentration range for AMB was 4-0.06 µg/mL, for FLU 64-0.125 µg/mL, for ITZ 4-0.06 µg/mL, and VOR 6-0.125 µg/mL (Table 3). Interestingly, the synergistic effect was observed in combination of farnesol with FLU and ITZ against C. albicans and C. parapsilosis isolates (FICI: 0.5 and 0.35, 0.25 respectively), and also in combination of VOR and AMB with farnesol against C. parapsilosis (FICI: 0.5 and 0.35 respectively). In contrast, C. glabrata isolates showed no synergistic effect with antifungal drugs. Moreover, MIC value of drugs in combination with farnesol noticeably decreased in the species, FLU from 8-64 reached to 2-8 µg/mL, ITZ (from 1-8 to 1-4 µg/mL), and VOR (from 16-2 to 1-4 µg/mL), and AMB (from 2 to 1 µg/mL). Besides, The combination of CTZ with farnesol has not shown any effect. The results were shown in Table 3.
To evaluate the cytotoxicity effect farnesol on cells, we carried out a flowcytometry assay. Our result showed that farnesol could not significantly increase apoptosis in cell line. So Plots A (untreated cells (without farnesol) as control group) and B (Treated cells with farnesol) didn’t have significantly different from each other (p> 0.05). At 300 µM, farnesol did not show any cytotoxicity effects on the SW48 cell line (Figure 2).
4. Discussion
VVC and especially RVVC, the most mucosal infections of the genital tract, proposed one of the major concerning of women heath worldwide [26]. In this study, C. glabrata assigned the highest percentage of species isolated from women suffering from VVC, followed by C. albicans and C. parapsilosis, which was in agreement some similar studies isolated C. glabrata, as the most causative agent in infected cases [27,28]. In recent decades, we have seen a change in the prevalence of Candida species in candidiasis infections. As it has been reported in previous epidemiological studies, Candida albicans is the dominant species in infections. In the present study, Candida glabrata has replaced Candida albicans in terms of prevalence. On the other hand, in the studied population, other species of Candida, including Candida parapsilopsis, have been detected in limited numbers or in the form of mixed infection with Candida albicans.
As expected, and according to AFST findings in this work, Candida isolates showed different pattern of susceptibility to azoles. C. albicans and C. glabrata revealed a high rate of resistance to FLU followed by CTZ, whereas approximately only 10% of C. glabrata isolates were resistant to AMB. In general, Candida isolates showed lower MIC against ITZ and AMB compared with FLU and VOR. Many studies have highlighted the resistance to azole drugs in Candida species recovered from VVC, particularly to FLU [2,3,4,29]. Similarly, some related reports over the world, directed different range of azole resistance among Candida species. For instance, in a work by Bitew et al., 17.2% of Candida krusei isolated from vaginal tract were resistant to FLU [30]. Indeed, Arastehfar et al. showed the high rate of FLU resistant and FLU tolerant phenotypes in C. albicans strains recovered from Iranian women suffering from VVC and RVVC [7]. Likewise, similar studies reported the high percentage of C. albicans (81.5%) and C. glabrata (83.5%) recovered from Iranian pregnant women were FLU resistant [31].
Despite being the a first-line azole drug to treatment of VVC, FLU susceptibility has significantly decreased in the last decades, due to various mechanisms of resistance [22]. As a result, the search for efficient agents antifungal with minimum side effects and low toxicity is highly recommended [32]. Besides, the efficacy of conventional drugs is often undesirable due to their high toxicity, low tolerability, or narrow spectrum of action [15]. Hence, the abovementioned issues have encouraged researchers to explore novel antifungal agents, even though combination therapies to overcome therapeutic failure of VVC in women infected with resistant Candida species which led to recurrent VVC as well as economic burden in health care system. Some of which, farnesol a molecule synthesized by C. albicans via enzymatic dephosphorylation of farnesyl pyrophosphate [33] - has gained considerations as a promising antifungal agent in the recent decades. Farnesol exogenously inhibits the conidiation and germination of Aspergillus niger and Fusarium graminearum, and also induces apoptotic-like programmed cell death in Aspergillus flavus, Aspergillus nidulans and Fusarium graminearum[12,33,34,35,36], besides it has a capability to down regulated of genes expression in C. albicans which is related to hyphae formation and pathogenesis (HWP1 & SAP6) [37]. Farnesol has also shown to inhibit the biofilm formation against resistant strains of C. albicans [38,39]. Because of the noticeable inhibitory effects of farnesol on fungal cells as well as antifungal activity [14,40], we tested combination of farnesol with four common antifungal against 80 clinical isolates of Candida species recovered from VVC in vitro. Our finding showed that regarding combination of farnesol-FLU and farnesol-ITZ to resistant clinical isolates of C. albicans and C. parapsilopsis, which showed high MIC for those drugs (used alone). These results are expected considering the drug resistance pattern of these two Candida species and comparison with previous studies. For example in a study in 2020, farnesol in combination with antifungal drugs significantly decreased biofilm formation of 3 C. auris strains and one standard C. albicans [41]. Another study, also showed the inhibitory effect of farnesol as a promising molecule on biofilm formation at the beginning stage in 6 isolates of C. albians from dentures and C. albicans ATCC10231 [42]. Morever ,Decanis et al. showed farnesol was able significantly decrease Sap2 secretion, down regulated sap4-6 mRNA expression and changed yeast to hyphae morphogenesis in C.albicans strain [43]. In addition, remarkable synergism effects were detected for the combinations of farnesol-VOR and farnesol-AMB against C. parapsilopsis isolates, which clearly emphasize the potential importance of farnesol as an effective antifungal agent. On the other side, indifferent interactions were observed in combination of farnesol with all antifungals with C. glabrata isolates. According to the drug sensitivity pattern of C. galabrata, these isolates have shown resistance to AMB in some cases. Therefore, this high suffering of drug resistance has been attributed to the no synergy. Rodrigues et al. have also tried combining two common antifungal drugs (AMB and posaconazole), and the FICI showed that the combination did not bring a clear advantage for this species [44]. Also, in agreement with our results, other studies notably confirmed the antifungal effects of farnesol against Candida species. For example, Cordeiro et al. indicated farnesol ranged from 4.68 to 150 µM concentration significantly reduced MICs of antifungal (FLU, ITZ, AMB, and caspofungin) against drug-resistant Candida species [24]. In a study conducted by Xia et al. it has been reported a synergistic effect between farnesol and FLU / 5-flurocytosine, as it reduced the capacity for biofilm in the presence of farnesol [40]. Liposomal farnesol potentiated the action of FLU against C. albicans and C. tropicalis, but the association of unconjugated farnesol with fluconazole resulted in antagonistic effects [45]. Additionally, Katragkou et al. found that synergistic or additive interaction between farnesol and FLU, AMB, and micafungin related to C. albicans biofilms [14]. In 2011 were presented findings, that farnesol at a nontoxic concentration synergized with azoles and this interaction led to reactive oxygen species accumulation (apoptosis) and influenced drug extrusion resulting in shift of MIC [46]. Later, beside of many other roles, farnesol is able to modulate activity of ABC efflux transporters what can result in changes in susceptibility profile to azoles in C. albicans (2 standard strains C. albicans resistant and sensitive to FLU)or C. auris isolates resistant to FLU [47,48]. According to the mechanism of action of farnesol and its derivatives on the fungal cells, the exogenous farnesol leads to alterations in the cell membrane by inhibiting the synthesis of ergosterol [10] which is the possible mechanism of farnesol in combination therapy. The azole drugs inhibit the biosynthesis of ergosterol by blocking the action of cytochrome P450-depending enzyme 14-alpha-demethylase, resulting in the disruption of plasma membrane that explain the synergistic effect of farnesol and azoles in our study [49]. So, the farnesol inhibition of the ergosterol biosynthetic pathway might decrease the levels of the intermediates. Hence, its combination with VCZ may result in an indifferent interaction. Farnesol also shows anti-neoplastic activity by down regulation of cell proliferation and enhancement of apoptosis in some human cancer cell lines such as breast cancer, lung cancer, and multiple myeloma with some known mechanism [38,42]. Although farnesol has apoptotic influences and chromosomal damage in cancer cell lines such as lung cancer A549 cell line, colon adenocarcinoma (Caco-2) cell line in certain concentrations, it has no apoptotic effect on healthy human lung epithelial BEAS-2B cell line [51]. In line with these conclusions, our flow cytometry findings indicate that farnesol has no apoptosis activity in SW48 cell line, indicating to be a safe agent for mammalian cells for future studies with the purpose of antifungal agent. Because of cells exposed to cytotoxic compounds may undergo necrosis (uncontrolled cell death), apoptosis (programmed cell death), autophagy, or stop actively growing and dividing to decrease cell proliferation. We used apoptosis assay (PI/ Annexin) by flow cytometry to show the effect of farnesol on SW48 as a normal cell line. In agreement with our finding, in a study by Cernakova et al .in 2018,while farnesol at 200µM effectively reduced yeast to hyphae transition in dual biofilm of C.albicans and Streptococcus .mutans ,it did not exhibit cytotoxicity effect on larve Galleria mellonella [52].
Among the limitations of this study, due to Iran's economic conditions, access to flow cytometry kits is very limited and this technique is expensive for us, so it was not possible to perform this test for farnesol/pharmacol. It is worthwhile mention that other related studies previously examined its antifungal activity against standard species of Candida with limited number that strongly highlight the importance of our current study in terms of statistical analysis to confirm farnesol efficacy. This study was conducted for the first time on Candida isolates from clinical samples, and the purpose of selecting drugs was to obtain a basic pattern for future studies and lead to practical solutions in similar populations.
5. Conclusions
Combination farnesol with commercial antifungal drugs might enhance the activity of fluconazole and itraconazole in resistant isolates with significant decrease of MIC, suggesting that it might be a promising antifungal agent. One point worth highlighting is the necessity to further studies to uncover the role of farnesol in the sterol biosynthesis and genes expression that contribute for the regulation of this pathway and how it interferes with cells.
Author Contributions
Conceptualization, M.R and F.N.; methodology, M.R.; software, M.F.; validation, M.R., F.N. and C.F.R.; formal analysis, M.R.,S.R.M.,M.F ; investigation, M.R.,F.N.; resources, M.R,F.N.; data curation, M.R.,F.N; writing—original draft preparation, M.R,M.F .; writing—review and editing, C.F.R,L.C and A.L.S..; visualization, F..N.; supervision, M.R.; project administration,F.N.; funding acquisition, M.R. All authors have read and agreed to the published version of the manuscript.
Funding
The Iran University of Medical Sciences supported this study with Grant-Project Number:9929918907.
Data Availability Statement
Not applicable.
Acknowledgments
All authors give thanks to Iran University of Medical Science (IUMS) for financial support with grant number9929918907.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Denning, D.W.; Bromley, M.J. How to Bolster the Antifungal Pipeline: Few Drugs Are Coming to Market, but Opportunities for Drug Development Exist. Science (80-. ). 2015, 347, 1414–1416. [Google Scholar] [CrossRef]
- Eckert L; Hawes S; Stevens c; Koutsky L; Eschenbach D; Holmes K Vulvovaginal Candidiasis: Clinical Manifestations, Risk Factors, Management Algorithm. Obs. Gynecol 1998, 92, 757–765. [CrossRef]
- Pirotta MV; Garland SM Genital Candida Species Detected in Samples from Women in Melbourne, Australia, before and after Treatment with Antibiotics. J. Clin. Microbiol 2006, 44, 3213–3217. [CrossRef]
- Guzel AB; Ilkit M; Burgut R; Urunsak IF; Ozgunen FT An Evaluation of Risk Factors in Pregnant Women with Candida Vaginitis and the Diagnostic Value of Simultaneous Vaginal and Rectal Sampling. Mycopathologia 2011, 172, 25–36. [CrossRef]
- Lema, VM. Recurrent Vulvo-Vaginal Candidiasis: Diagnostic and Management Challenges in a Developing Country Context. Obs. Gynecol Int J 2017, 7, 260. [Google Scholar] [CrossRef]
- Lírio J; Giraldo PC; Amaral RL; Sarmento ACA; Costa APF; Gonçalves AK Antifungal (Oral and Vaginal) Therapy for Recurrent Vulvovaginal Candidiasis: A Systematic Review Protocol. BMJ Open 2019, 9, e027489. [CrossRef]
- Arastehfar A; Kargar ML; Mohammadi SR; Roudbary M; Ghods N; Haghighi L; et al. A High Rate of Recurrent Vulvovaginal Candidiasis and Therapeutic Failure of Azole Derivatives among Iranian Women. Front. Microbiol. 2021, 12. [CrossRef]
- Li C; Xu Z; Liu S; Huang Y; Duan W; Wei X In Vivo Antifungal Activities of Farnesol Combined with Antifungal Drugs against Murine Oral Mucosal Candidiasis. Biofouling 2021, 37, 818–829. [CrossRef]
- Sobel J; Sobel R; et al. Current Treatment Options for Vulvovaginal Candidiasis Caused by Azole-Resistant Candida Species. Expert Opin. Pharmacother. 2018, 19, 971–977. [CrossRef]
- Jabra-Rizk MA; Shirtliff M; James C; Meiller T Effect of Farnesol on Candida Dubliniensis Biofilm Formation and Fluconazole Resistance. FEMS Yeast Res. 2006, 6, 1063–1073. [CrossRef]
- Brilhante RSN; de Lima RAC; Caetano EP; Leite JJG; Castelo-Branco DSCM; Riberio JF; et al. Effect of Farnesol on Growth, Ergosterol Biosynthesis, and Cell Permeability in Coccidioides Posadassi. Antimicrob Agent Chemother 2013, 57, 2167–2170. [CrossRef]
- Wang X; Wang Y; Zhou Y; Wei X Farnesol Induces Apoptosis-like Cell Death in the Pathogenic Funus Aspergillus Flavus. Mycologia 2014, 106, 881–888. [CrossRef]
- Delmondes, G.D.A.; Santiago Lemos, I.C.; Dias, D.D.Q.; Cunha, G.L. Da; Araújo, I.M.; Barbosa, R.; Coutinho, H.D.M.; Felipe, C.F.B.; Barbosa-Filho, J.M.; Lima, N.T.R. De; et al. Pharmacological Applications of Farnesol (C15H26O): A Patent Review. Expert Opin. Ther. Pat. 2020, 30, 227–234. [Google Scholar] [CrossRef]
- Katragkou, A.; Mccarthy, M.; Alexander, E.L.; Antachopoulos, C.; Meletiadis, J.; Jabra-rizk, M.A.; Petraitis, V.; Roilides, E.; Walsh, T.J. In Vitro Interactions between Farnesol and Fluconazole, Amphotericin b or Micafungin against Candida Albicans Biofilms. J. Antimicrob. Chemother. 2015, 70, 470–478. [Google Scholar] [CrossRef]
- Onder, S.; Oz, Y. In Vitro Effects of Farnesol Alone and in Combination with Antifungal Drugs against Aspergillus Clinical Isolates. Med. Mycol. J. 2021, 62, 5–10. [Google Scholar] [CrossRef]
- Bozó, A.; Domán, M.; Majoros, L.; Kardos, G.; Varga, I.; Kovács, R. The in Vitro and in Vivo Efficacy of Fluconazole in Combination with Farnesol against Candida Albicans Isolates Using a Murine Vulvovaginitis Model. J. Microbiol. 2016, 54, 753–760. [Google Scholar] [CrossRef]
- Spitzer M; Robbins N; Wright GD Combinatorial Strategies for Combating Invasive Fungal Infections. Virulence 2017, 8, 169–185. [CrossRef]
- Gong Y; Liu W; Huang X; Hao L; Li Y; Sun S Antifungal Activity and Potential Mechanism of N-Butylphthalide Alone and in Combination with Fluconazole against Candida Albicans. Front. Microbiol. 2019, 10, 1461.
- Rodrigues, C.F.; Boas, D.V.; Haynes, K.; Henriques, M. The MNN2 Gene Knockout Modulates the Antifungal Resistance of Biofilms of Candida Glabrata. Biomolecules 2018, 8. [Google Scholar] [CrossRef]
- Arastehfar A; Fang W; Pan W; Liao W; Yan L; Boekhout T Identification of Nine Cryptic Species of Candida Albicans, C. Glabrata, and C. Parapsilosis Complexes Using One-Step Multiplex PCR. BMC Infect. Dis. 2018, 18, 1–9.
- Nikoomanesh, F.; Roudbarmohammadi, S.; Khoobi, M.; Haghighi, F.; Roudbary, M. Design and Synthesis of Mucoadhesive Nanogel Containing Farnesol: Investigation of the Effect on HWP1, SAP6 and Rim101 Genes Expression of Candida Albicans in Vitro. Artif. Cells, Nanomedicine Biotechnol. 2019, 47, 64–72. [Google Scholar] [CrossRef]
- Whaley, S.G.; Berkow, E.L.; Rybak, J.M.; Nishimoto, A.T.; Barker, K.S.; Rogers, P.D. Azole Antifungal Resistance in Candida Albicans and Emerging Non-Albicans Candida Species. Front. Microbiol. 2017, 7, 2173. [Google Scholar] [CrossRef]
- Nikoomanesh F.; Roudbarmohammadi S.; Bashardoust B.; Zareei M. Effect of Farnesol on Responsive Gene Expressions in Hyphal Morphogenesis Transformation of Candida Albicans. Infect. Epidemiol. Microbiol. 2018, 4, 73–77.
- Cordeiro, R.A.; Teixeira, C.E.C.; Brilhante, R.S.N.; Castelo-Branco, D.S.C.M.; Paiva, M.A.N.; Giffoni Leite, J.J.; Lima, D.T.; Monteiro, A.J.; Sidrim, J.J.C.; Rocha, M.F.G. Minimum Inhibitory Concentrations of Amphotericin B, Azoles and Caspofungin against Candida Species Are Reduced by Farnesol. Med. Mycol. 2013, 51, 53–59. [Google Scholar] [CrossRef]
- Alipour R; Fatemi A; Alsahebfosul F; Andalib A; Pourazar A Autologous Plasma versus Fetal Calf Serum as a Supplement for the Culture of Neutrophils. BMC Res. Notes 2020, 13, 39. [CrossRef]
- Kumar, S.; Kumar, A.; Roudbary, M.; Mohammadi, R.; Černáková, L. Overview on the Infections Related to Rare Candida Species. Pathogens 2022, 11, 1–49. [Google Scholar] [CrossRef]
- Denning, D.W.; Kneale, M.; Rautemaa-Richardson, R.; Sobel, J.D. Global Burden of Recurrent Vulvovaginal Candidiasis. Lancet Infect Dis 2017, 1–9, in press. [Google Scholar]
- Roudbary M; Roudbarmohammadi SH; Bakhshi B; Farhadi Z; Nikoomanesh F Identification of Candida Species Isolated Form Iranian Women Eith Vaginal Candidasis by PCR-RFLP Method. Eur.J. Exp. Biol. 2013, 3, 365–369.
- Rodrigues CF, Gonçalves B, Rodrigues ME, Silva S, Azeredo J, H.M. The Effectiveness of Voriconazole in Therapy of Candida Glabrata’s Biofilms Oral Infections and Its Influence on the Matrix Composition and Gene Expression. Mycopathologia 2017, 182, 653–664. [CrossRef]
- Bitew, A.; Abebaw, Y. Vulvovaginal Candidiasis: Species Distribution of Candida and Their Antifungal Susceptibility Pattern. BMC Womens. Health 2018, 18, 1–10. [Google Scholar] [CrossRef]
- Mohammadi-Ghalehbin, B.; Javanpour Heravi, H.; Arzanlou, M.; Sarvi, M. Prevalence and Antibiotic Resistance Pattern of Candida Spp. Isolated from Pregnant Women Referred to Health Centers in Ardabil, Iran. J Ardabil Univ Med Sci 2017, 16, 409–421. [Google Scholar]
- Sustr, V.; Foessleitner, P.; Kiss, H.; Farr, A. Vulvovaginal Candidosis: Current Concepts, Challenges and Perspectives. J. Fungi 2020, 6, 1–14. [Google Scholar] [CrossRef]
- Hornby JM; Jensen EC; Lisec AD; Tasto JJ; Jahnke B; Shoemaker R; et al. Quorum Sensing in the Demorphic Fungus Candida Albicans Is Mediated by Farnesol. Appl Env. Microbiol 2001, 67, 2982–2992. [CrossRef]
- Lorek J; Poggeler S; Weide MR; Breves R; Bokmuhl DP Infeluence of Farnesol on the Morphogenesis of Aspergillus Niger. J Basic Microbiol 2008, 48, 99–103. [CrossRef]
- Semighini CP; Murray N; Harris SD Inhibition of Fusarium Graminearum Growth and Development by Farnesol. FEMS Microbiol. Lett. 2008, 279, 259–264. [CrossRef]
- Semighini CP; Honrry JM; Dumitru R; Nickerson KW; Harris SD Farnesol-Induced Apoptosis in Aspergillus Nidulans Reveals a Possible Mechanism for Antagonistic Interaction between Fungi. Mol Microbiol 2006, 59, 753–764. [CrossRef]
- Nikoomanesh F.; Roudbarmohammadi S.; Bashardoust B.; Zareei M . . Effect of Farnesol on Responsive Gene Expressions in Hyphal Morphogenesis Transformation of Candida Albicans. Infect. Epidemiol. Microbiol. 2018, 4, 73–77.
- Rossignol, T.; Logue, M.E.; Reynolds, K.; Grenon, M.; Lowndes, N.F.; Butler, G. Transcriptional Response of Candida Parapsilosis Following Exposure to Farnesol. Antimicrob. Agents Chemother. 2007, 51, 2304–2312. [Google Scholar] [CrossRef]
- Rodrigues, C.F.; Černáková, L. Farnesol and Tyrosol: Secondary Metabolites with a Crucial Quorum-Sensing Role in Candida Biofilm Development. Genes (Basel). 2020, 11. [Google Scholar] [CrossRef]
- Xia J; Qian F; Xu W; Zhang Z; Wei X In Vitro Inhibitory Effects of Farnesol and Interaction between Farnesol and Antifungals against Biofilm of C Andida Albicans Resistance Strains. Biofouling 2017, 33, 283–293. [CrossRef]
- Nagy F, Vitális E, Jakab Á, Borman AM, Forgács L, Tóth Z, Majoros L, K.R. In Vitro and in Vivo Effect of Exogenous Farnesol Exposure Against Candida Auris. Front Microbiol 2020, 20, 957. [CrossRef]
- Sebaa S, Boucherit-Otmani Z, C.P. Effects of Tyrosol and Farnesol on Candida Albicans Biofilm. Mol Med Rep 2019, 19, 3201–3209. [CrossRef]
- Décanis N, Tazi N, Correia A, Vilanova M, R.M. Farnesol, a Fungal Quorum-Sensing Molecule Triggers Candida Albicans Morphological Changes by Downregulating the Expression of Different Secreted Aspartyl Proteinase Genes. Open Microbiol J 2011, 5, 119–126. [CrossRef]
- Rodrigues, C.F.; Alves, D.F.; Henriques, M. Combination of Posaconazole and Amphotericin b in the Treatment of Candida Glabrata Biofilms. Microorganisms 2018, 6, 1–11. [Google Scholar] [CrossRef]
- Bezerra, C.F.; de Alencar Júnior, J.G.; de Lima Honorato, R.; dos Santos, A.T.L.; Pereira da Silva, J.C.; Gusmão da Silva, T.; Leal, A.L.A.B.; Rocha, J.E.; de Freitas, T.S.; Tavares Vieira, T.A.; et al. Antifungal Activity of Farnesol Incorporated in Liposomes and Associated with Fluconazole. Chem. Phys. Lipids 2020, 233, 33058818. [Google Scholar] [CrossRef] [PubMed]
- Sharma, M.; Prasad, R. The Quorum-Sensing Molecule Farnesol Is a Modulator of Drug Efflux Mediated by ABC Multidrug Transporters and Synergizes with Drugs in Candida Albicans. Antimicrob. Agents Chemother. 2011, 55, 4834–4843. [Google Scholar] [CrossRef] [PubMed]
- Černáková, L.; Dižová, S.; Gášková, D.; Jančíková, I.; Bujdáková, H. Impact of Farnesol as a Modulator of Efflux Pumps in a Fluconazole-Resistant Strain of Candida Albicans. Microb. Drug Resist. 2019, 25. [Google Scholar] [CrossRef] [PubMed]
- Dekkerová, J.; Černáková, L.; Kendra, S.; Borghi, E.; Ottaviano, E.; Willinger, B.; Bujdáková, H. Farnesol Boosts the Antifungal Effect of Fluconazole and Modulates Resistance in Candida Auris through Regulation of the CDR1 and ERG11 Genes. J. Fungi 2022, 8, 783. [Google Scholar] [CrossRef] [PubMed]
- Ghannoum MA; Rice LB Antifungal Agents: Mode of Action Mechnism of Resistance, and Correlation of These Mechanisms with Bacterial Resistance. Clin Microbiol Rev 1999, 12, 501–517. [CrossRef] [PubMed]
- Fana, Y.S.Y.Z.S.; Liuc, A.V.X. Clinical Characteristics and Antifungal Susceptibility of Candida Nivariensis from Vulvovaginal Candidiasis. 2019.
- Öztürk BY; Feyzullazade N; Dağ I; Şengel T The Investigation of in Vitro Effects of Farnesol at Different Cancer Cell Lines. Microsc. Res. Tech. 2022.
- Černáková L, Jordao L, B.H. Impact of Farnesol and Corsodyl ® on Candida Albicans Forming Dual Biofilm with Streptococcus Mutans. Oral Dis 2018, 24, 1126–1131. [CrossRef] [PubMed]
Figure 1.
Identification of prevalence of Candida species recovered from VVC patients.
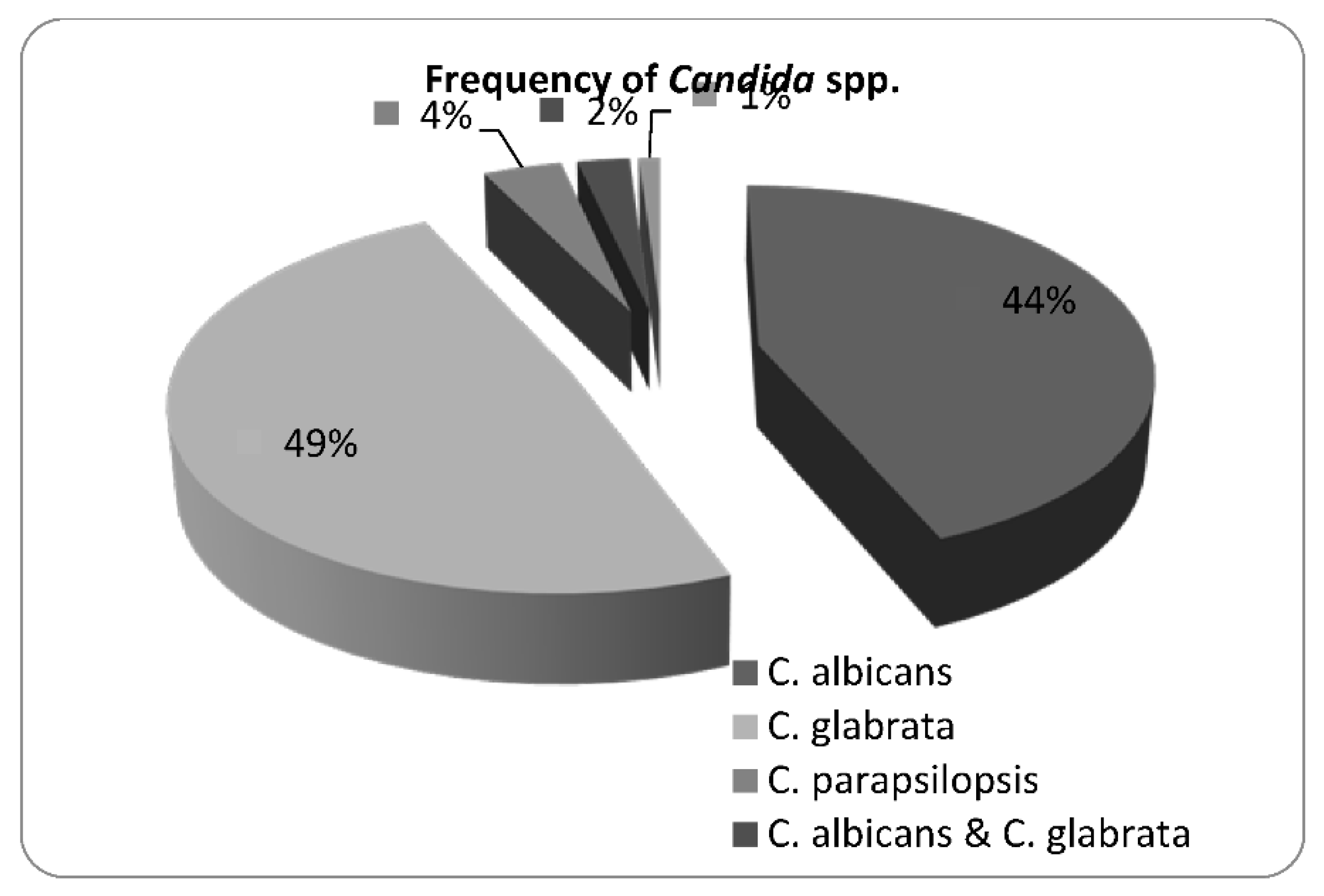
Figure 2.
Apoptosis assay of SW48 cell line staining by Annexin-V and propidium iodide (PI) when treated with 300μM farnesol. A: Untreated cells (without farnesol) as control group and B: Treated cells with farnesol. (Q1: Viable cells; Q2: Early apoptotic cells; Q3: Late apoptotic cells and Necrotic cells; Q4: Necrotic cells).
Figure 2.
Apoptosis assay of SW48 cell line staining by Annexin-V and propidium iodide (PI) when treated with 300μM farnesol. A: Untreated cells (without farnesol) as control group and B: Treated cells with farnesol. (Q1: Viable cells; Q2: Early apoptotic cells; Q3: Late apoptotic cells and Necrotic cells; Q4: Necrotic cells).
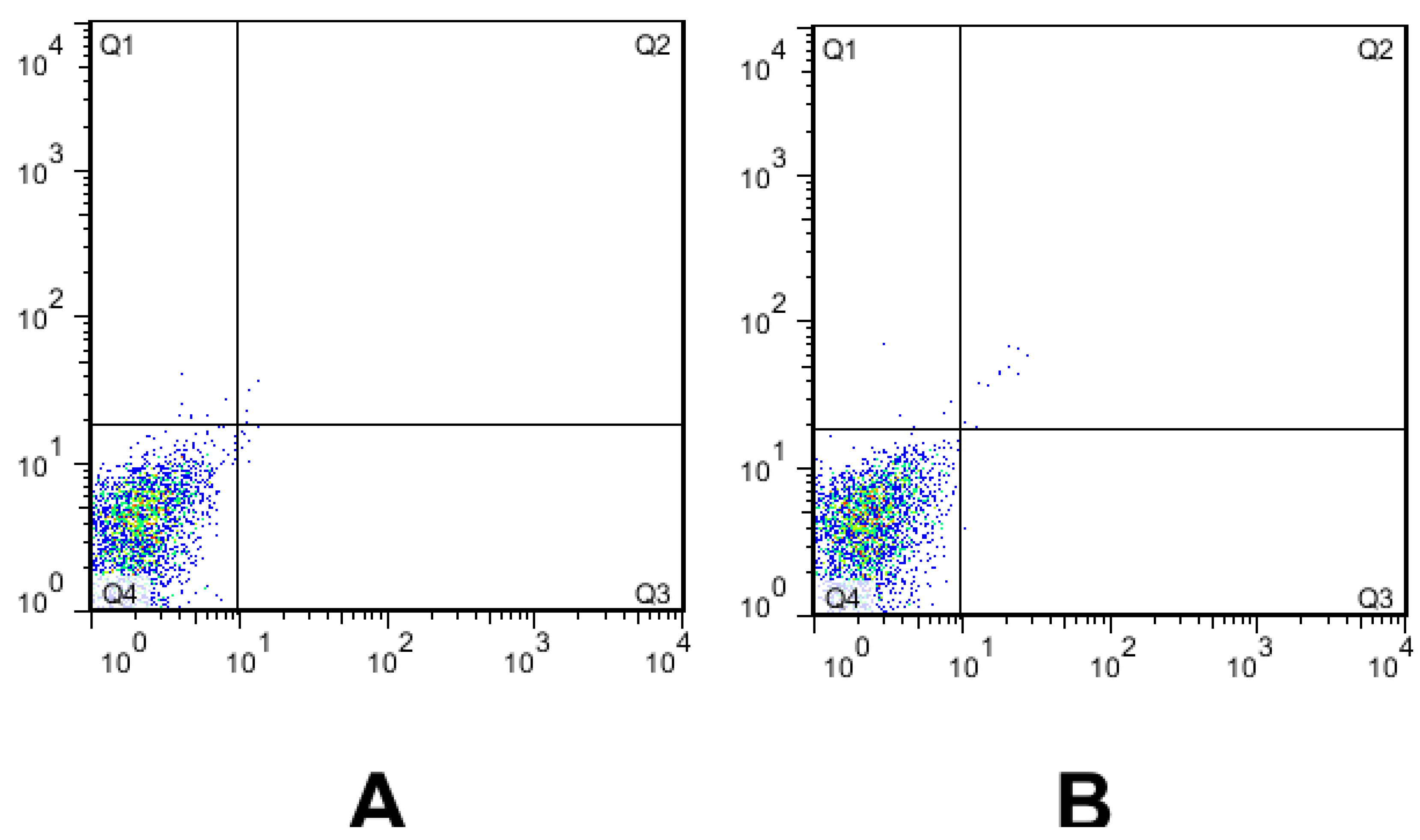

Table 1.
Primers employed in the Multiplex PCR amplification.
| Candida species | Sequences (5' 3' ) 3' ) |
Amplicons |
|
C. albicans |
F-5'AGATTATTGCCATGCCCTGAG3' R5'CCATGTCGAACGTAGCGTATGC3' |
606bp |
| C. glabrata | F5'ACCGTGCTTGCCTCTACA3' R5'GACATCTGAGCCTCGTCTGA3' |
212bp |
| C. tropicalis | F5'AGAACAAGAAAACAGTGAAGCAA3' R5'CCATGTCGAACGTAGCGTATGC3 |
126bp |
| C. parapsiolosis | F5'TACACCAAGCGACTCAGC3' R5'ACCAGCTGCTTTGACTTG3' |
490bp |
| C. krusei | F5'GGCGTTGTCCATCCAATG3' R5'CAGGAGAATTGCTGTTCCC3' |
1159bp |
| C. dubliniensis | F5'GTCGGACATATACCTCCAACTC3' R5'CCATGTCGAACGTAGCGTAT3' |
718bp |
Table 2.
Antifungal susceptibility pattern of Candida species against Antifungal drugs (CLSI M27-A3/S4).
Table 2.
Antifungal susceptibility pattern of Candida species against Antifungal drugs (CLSI M27-A3/S4).
| Candida species | Antifungal drug | Sensitive(S) | Dose-dependent | Resistance(R) | |||
| n | % | n | % | n | % | ||
|
C. albicans n=35 |
FLU | 11 | 31.4 | 1 | 2.1 | 23 | 65.7 |
| ITZ | 18 | 51.4 | - | - | 17 | 48.5 | |
| VOR | 17 | 48.5 | - | - | 18 | 51.4 | |
| AMB | 35 | 100 | - | - | - | - | |
| CTZ | 13 | 37.1 | - | - | 22 | 62.8 | |
|
C. glabrata n=39 |
FLU | 9 | 23 | 2 | 5.1 | 28 | 71.8 |
| ITZ | 16 | 41 | - | - | 23 | 59 | |
| VOR | 14 | 35.9 | - | - | 25 | 64.1 | |
| AMB | 35 | 89.7 | - | - | 4 | 10.2 | |
| CTZ | 13 | 33.3 | - | - | 26 | 66.6 | |
|
C. parapsilosis n=3 |
FLU | 2 | 66.6 | - | - | 1 | 33.3 |
| ITZ | 3 | 100 | - | - | - | - | |
| VOR | 2 | 66.6 | - | - | 1 | 33.3 | |
| AMB | 1 | 33.3 | - | - | 2 | 66.6 | |
| CTZ | 1 | 33.3 | - | - | 2 | 66.6 | |
Table 3.
Minimum inhibitory concentrations (MICs) of farnesol and antifungals alone and in combinations with farnesol against Candida isolates.
Table 3.
Minimum inhibitory concentrations (MICs) of farnesol and antifungals alone and in combinations with farnesol against Candida isolates.
| Isolates | Median MIC values | Interaction analysis | ||||
| MIC alone | MIC in combination | Median FICI | Type of interaction | |||
| FLU (µg/L) | FAR (µM | FLU (µg/L) | FAR (µM) | |||
| C. albicans | 64(8-64) | 300 | 8(2-8) | 150 | 0.5 | Synergy |
| C. glabrata | 64(8-64) | 300 | 8(2-16) | 300 | 0.9 | Indifferent |
| C.parapsilosis | 32(8-32) | 300 | 4(2-8) | 150 | 0.35 | Synergy |
| ITRA (µg/L) | FAR (µM | ITRA (µg/L) | FAR (µM) | |||
| C. albicans | 8(1-8) | 300 | 4(1-8) | 150 | 0.5 | Synergy |
| C. glabrata | 8(2-8) | 300 | 8(2-8) | 300 | 1.01 | Indifferent |
| C.parapsilosis | 8(2-8) | 300 | 4(1-4) | 150 | 0.25 | Synergy |
| VOR(µg/L) | FAR (µM | VOR(µg/L) | FAR (µM) | |||
| C. albicans | 16(2-16) | 300 | 8(1-8) | 150 | 0.75 | Indifferent |
| C. glabrata | 16(2-16) | 300 | 8(2-16) | 300 | 0.75 | Indifferent |
| C.parapsilosis | 8(2-16) | 300 | 4(1-4) | 150 | 0.5 | Synergy |
| AmB (µg/L | FAR (µM | AmB(µg/L) | FAR (µM) | |||
| C. albicans | 2(0.031-2) | 300 | 2(0.031-2) | 150 | - | - |
| C. glabrata | 2(0.031-2) | 300 | 1(0.031-2) | 300 | 1.25 | Indifferent |
| C.parapsilosis | 2(0.031-2) | 300 | 1(0.031-2) | 150 | 0.35 | Synergy |
| CTZ(µg/L) | FAR (µM | CTZ(µg/L) | FAR (µM) | |||
| C. albicans | 16(2-16) | 300 | 4(1-4) | 150 | 1.75 | Indifferent |
| C. glabrata | 16(2-16) | 300 | 8(2-16) | 300 | 0.9 | Indifferent |
| C.parapsilosis | 8(2-16) | 300 | 2(0.5-4) | 150 | 1.25 | Indifferent |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



