
Submitted:
31 December 2022
Posted:
05 January 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Mental health could worsen in children and adolescents with autism spectrum disorder during the Covid19 pandemic. In addition, their parents could be more at risk for an increase in anxiety and depression symptomatology. This study aims to understand the adaptation and the psychosocial well-being in a sample of 16 males aged 10-21 years old with Asperger syndrome after the quarantine for Covid19 when they return to school and partially to their activities in September 2020, The approach adopted is multi-informant with a battery of questionnaires on psychological health and adaptation given by a secure online web data Qualtrics both to adolescents and also to their parents. Paralleling matched peers with typically development were assessed adopting the same methodology. The results evidenced several difficulties in Asperger’s psychological health, especially in anxiety and socialization. Also adaptation is put in crisis, even if they reported a good comprehension and adoption of the behaviors anti-Covid19. Parents of children with Asperger reported similar psychological difficulties and general health than those of the group of children typically developing. Some clinical indications could be discussed for psychologists who follow children and adolescents with Asperger.
Keywords:
Asperger
; Atypically development
; Covid19
; Children
; Adolescents
; typically development
; Parents
; Adaptation
; Well-being
; Multi-informant
1. Introduction
Autism spectrum disorder (ASD) is a neurodevelopmental disorder characterized by deficits in social communication and social interaction, in addition to restricted and repetitive patterns of behavior and interests. In 2013, the Diagnostic and Statistical Manual of Mental Disorders, 5th (DSM-5) [1] created the umbrella diagnosis of ASD, consolidating four previously separate disorders: autistic disorder, Asperger syndrome (AS), childhood disintegrative disorder, and pervasive developmental disorder not otherwise specified. Unlike previous versions, in DSM-5 more importance is placed on what is a developmentally oriented classification of childhood mental pathology, paying attention to the neurobiological etiology underlying these disorders. In this new classification, Asperger’s Syndrome (AS) is inserted into the Level 1 autism spectrum disorder, without intellectual impairment of the associated language [2]. The characteristics of the subjects with this syndrome are: having special interests, reporting difficulties in social communication and social interaction, having an Intelligent Quotient > 70, having an early and formal language development, but lack of pragmatics of communication. Recently, data from the American Centers for Disease Control (CDC) indicate at 8 years a prevalence of 1 out of 134 children [3], i.e., about 0.75%.
The World Health Organization (WHO) declared the new coronavirus (COVID-19) outbreak a global pandemic on 11 March 2020. It is a public health emergency of international concern and poses a challenge to psychological resilience [4]. It is necessary to understand the psychological impact that the epidemic itself and relative quarantine have on the entire population, especially children and young people with disabilities. The COVID-19 pandemic has led families to adapt their lives, including social isolation and work from home. The consequences of this outbreak on mental health are several. Change in routine is often a significant challenge for children with ASD [5], and for that reason, families with children with ASD could be a vulnerable group to develop anxiety and mental abnormalities during quarantine and isolation. Children with autism spectrum disorder (ASD) often experience changing routines as a major challenge. For that reason, the need for adaptation during the COVID-19 pandemic may have brought great problems to families with children with this pathology. Children with ASD are at high risk for psychiatric problems during the COVID-19 pandemic, and the degree of understanding of the child of COVID-19, COVID-19 illness in the family, low family income, and depression and anxiety symptoms in parents increase the risk of poor mental health during the pandemic [6]. The results of recent studies showed a potential important psychological impact of the COVID-19 pandemic not only in children with neurodevelopmental disorders, but also in their caregivers, especially anxiety symptoms [7]. Parents of children with ASD had lower levels of resilience and more symptoms of anxiety and depression than parents of children typically developing [8].
The strict domestic quarantine policies adopted to control the transmission of COVID-19 could have adverse psychological effects and could exacerbate preexisting conditions such as depression and anxiety, especially in people with mental disorders [9]. Lockdown and boredom can reveal a susceptibility to unhealthy behaviour.
During quarantine, in addition to sociodemographic factors, the factors that seem to affect the worst psychological impact are: the duration of quarantine [10,11]; the fear of being infected and of being able to infect others [12,13]; boredom and frustration caused by the loss of daily routine and the reduction of physical and social contacts [11,14]; the lack of basic necessities (food, water, clothes) [15,16]; the scarce and inadequate information [14,17].
The numerous changes in the daily life of every single citizen with the lockdown have mainly been: school attendance, social and family relationships, also of children and young people both normal and with pervasive developmental disorders who have had to become aware of the health emergency.
In the adolescent population, some consequences in their health could be: sedentary behavior that increases proportionally to Covid19 screen exposure [18], decreased physical activity time [18], increased insomnia and sleep-related problems [19] and increased difficulty falling asleep and sudden awakening episodes [20]. Also, from the point of view of psychic and psychological problems, adolescents seem to have been influenced by anxiety symptoms, and some studies show some influence on the anxiety levels of suicidal thoughts.
Research Questions
Our interest focuses on the entire family unit of adolescents with Asperger’s syndrome who, like their peers, have had to adapt to quarantine especially to distance learning, but also to online rehabilitation activities during the period of isolation. There are limited studies on this population, for this reason, it is important to have a picture of their perceptions about risk and preventive or protective behaviors both during quarantine retrospectively and in school reintegration and social life.
The research questions are the following:
H1) Do children and young people with Asperger syndrome have a good understanding of the risk of COVID-19 and of the preventive measures to contain it?
H2) What were the possible psychological consequences, in children with Asperger’s and in their parents during quarantine?
H3) What have been the main difficulties for children and young people with Asperger’s syndrome in returning to school and resuming social life since September 2020?
H4) Could the high parental stress experienced during the lockdown have influenced in the long term the emotional and behavioral difficulties their children have experienced with returning to school and everyday life since September 2020?
2. Materials and Methods
2.1. Procedures
After obtaining the consent of the Ethics Committee in Psychology (Protocol 3814, University of Padua) on 1 November 2020, participants were recruited. It is necessary to distinguish the recruitment of families with children with Asperger’s syndrome from families with children with neurotypical development, aged between 9 and 20 years. The first group was reached through a letter of presentation of the project to the President of the Asperger Veneto Regional Association and by the collaboration of Dr. Guidi as head of the center of the province of Padua. The control group was recruited using a snowball procedure. The clinic and the control group signed the informed consent form before filling in the protect online questionnaires on the Qualtrics platform.
2.2. Participants
Sixteen school-age children aged 10 to 20 years with Asperger’s syndrome attended school were recruited (M=14; SD=3.62); while young adults were not included in this study. At the same time, neurotypically developing peers (M=14.07, SD=3.31) of the same sex, region and age as close as possible were also recruited.
Table 1 shows the characteristics of the participants.
2.3. Instruments
The methodological approach of this study is mixed (explanatory sequential design) in which the quantitative analysis is deepened by the qualitative one; and multiinformant (involvement of parents and their children and young people).
2.3.1. Perceived risk questionnaire
It is an ad hoc questionnaire, divided into two age groups (10-14 years and 15-20 years), with 42 statements on contagion, risks and knowledge of behaviors both adopted in the past, during the quarantine, and promoted today in the post -isolation, to which they were asked to answer with true or false. Statements were divided into four subscales: information, mode of transmission, symptoms, and behavior.
2.3.2. Cantrill’s self-anchoring ladder of life satisfaction
It is a tool for measuring people’s attitudes toward their life and its components in various respects [21]. Participants are presented with three visual scales numbered 0-10 and told the following statement: “Could you please indicate, on a scale from 1 to 10, where 1 represents the worst possible life and 10 the best”:
1- What level would you have been at about a year ago when you started school in September 2019.
2- At what level would you have placed yourself during quarantine.
3- At what level do you position yourself at the moment.
Of the following scales, three levels of life satisfaction were defined: low (0–6), medium (7–8), and high (9–10). In particular, as regards the first two statements, the students are asked to remember a moment of life from the more remote (first statement) and more recent (second statement) past.
2.3.3. The SAFA battery
The SAFA battery is a self-administration diagnostic tool, it is adapted to three age groups: 8-10 years, 11-13 years, 14-19 years [22]. This favors the reliability of the instrument in relation to age.
The instruments scales, which present a textbook internal consistency index (α of Cronbach) in general higher than .80 (very good), can also be administered individually, this allowed us to use only the subscales for the study: "Anxiety", “Depression” and “Obsessions”; for a total of 110 items for the younger age group and 144 items for the remaining two age groups. All participants were asked to respond with a true, false, or somewhere in between statement.
2.3.4. The Adaptive Behavior Assessment System II (ABAS-II)
It is a scale for assessing children’s daily living skills compiled by parents [23]. For our study, having a group of participants who are not yet workers, we did not take into consideration the "Work" subscale; while of the remaining 9 subscales of the three conceptual, practical, and social domains; we administered: the entire subscales of the practical domain ("Self-care", "Home/school life", "Use of the environment", "Health and safety") and the social domain ("Leisure", "Socialisation") and, finally, only one of the three subscales of the conceptual domain: "Self-control"; for a total of 164 items.
Parents were asked to respond on a 4-point scale, ’0-Not able, 1-Never able, 2-Sometimes able, 3-Always able”; finally, to avoid causing confusion in the participants, we excluded the possibility of choosing the answer ’I suppose’, even in the face of the physical absence of the administrator who could not have helped the parents with the compilation.
2.3.5. Center for Epidemiological Studies-Depression (CES-D)
It is a self-assessment scale on depression, measured by 20 items (of which four reverse items) on a 4-point scale (0-"Never very rarely (less than a day)", 1-"Occasionally (1 or 2 days)”, 2-“ Very often (3 or 4 days)”, 3-“ Frequently, all the time (5 to 7 days)”); with clinical cut-off equal to 16 [24]. Specifically, a total score between 0 and 9 indicates the absence of depressive symptoms and mild symptoms with a score between 10 and 15, however, it becomes relevant to identify moderate depressive symptoms (score between 16 and 24) or severe symptoms when the total score is greater than or equal to 25. Cronbach’s alpha of.85 is excellent evidence of the high reliability of the tool’s content.
2.3.6. General Anxiety Disorder-7 (GAD-7)
It is a self-administered questionnaire used as a screening tool and as an assessment of the interference of symptoms of generalized anxiety disorder, in retrospective mode, consisting of 7 items [25]. There are 4 levels of presence/frequency of symptoms during the last two weeks (a score is then assigned to each level). Never present (0 pts), Present a few days (1 pt), Present more than half of the days (2 pts), Present almost every day (3 pts). The final scores of 5, 10, and 15 correspond to the cut-off points to define mild anxiety disorder, moderate anxiety disorder, and severe anxiety disorder, respectively. Finally, Cronbach’s alpha of.80 shows a good test of reliability of the instrument’s content.
2.3.7. General Health Questionnaire (GH12)
Participants were asked to complete the General Health Questionnaire (GH12), a validated questionnaire of 12 items assessing quality of life. The GH12 [26,27] provides a reliable, valid and brief assessment of quality of life. The 12-item self-rated questionnaire measures physical health, psychological health, social relationships, and the environment during the past two weeks. Each item is rated on a 4-point Likert scale (“less than usual”, “no more than usual”, “rather more than usual”, “much more than usual”), referring to the past 2 weeks, with a range of total scores from 0 to 36. Higher scores indicate a more problematic situation and there are different cut-offs to consider: Scores ≥ 15 are viewed as “problematic” and scores ≥ 19 as “very problematic”. An example item is: ’Able to concentrate’. Overall, the higher total scores on the GHQ indicate a higher psychological discomfort experienced by the respondents and vice versa. GH12 has good to excellent reliability psychometric properties and performed well in preliminary validity tests that were also carried out in the Italian population [28,29]. Furthermore, the tool was recently used with adults during lockdown [30], proving to be valid and reliable (α=.80).
2.4. Statistical analysis plan
To answer the research hypotheses, statistical analyzes were performed using IBM SPSS Statistics 27 statistical software. Initially, descriptive statistical analyses of the sociodemographic variables of the entire group of participating children and their parents were carried out separately.
Precisely, given the small number of participants, it was decided to use nonparametric analyses with the aim of obtaining statistically more robust results. In particular, the Wilcoxon ranks test for paired and dependent samples, the Mann-Whitney test with two independent samples, the two-way Spearman correlation, a repeated measures ANOVA and the Chi-square test were used.
3. Results
3.1. Knolewdge typically and Asperger adolescents about Coronavirus and anti-COVID rules
Paired-sample Wilcoxon tests were run to see the possible differences between right and wrong answers in the two groups. The mean ranks within the groups were significant, both for the clinical group Z = -3.50, p<0.001 and for the control group Z = -3.43, p = 0.001. The entire group of participants analyzed the answers, on average, correctly to a greater number of questions.
On the other hand, the comparison between the means of the ranks of the two paired samples of correct answers between groups appears to be insignificant Z = -1.89, p = 0.85. Thus, we demonstrate how the boys in both groups respond correctly on average to the same number of questions on the COVID-19 test
3.2. Possible psychological consequences in children with Asperger’s and in their parents during quarantine
First, a paired sample Wilcoxon test was performed to identify possible differences in perceptions of life between the two groups. The two groups didn’t show differences in their life perception scores (Z=.13, p=.90), showing an insufficient one in 53.3% of cases, a sufficient one in 26.7% and very good in 20% of cases.
In the clinical group, on a statistical level, no significant differences emerged between the scores attributed to one’s own life between T1 and T2 (Z=-1.44, p=.15); between T1 and T3 (Z=-.99, p=.32); and between T2 and T3 (Z=-1.21, p=.23). While for neurotypical children, no significant differences emerged between the scores attributed to one’s life between T1 and T3 (Z=-1.59, p=.113); instead we find significant differences between T1 and T2 (Z=-2.12, p=.034) and between T2 and T3 (Z=-2.29, p=.022). These results, related to the neurotypical group, were investigated using repeated measures ANOVA, in which the data did not satisfy the sphericity hypothesis of the Mauchly sphericity test [W(2)=.61, p=. 04], thus using the Greenhouse-Geisser correction criteria, a significant difference emerged between the three Cantrill scales in the different time periods investigated [F (1.44) = 5.47, p = 0.020], which can be observed in Figure 1.
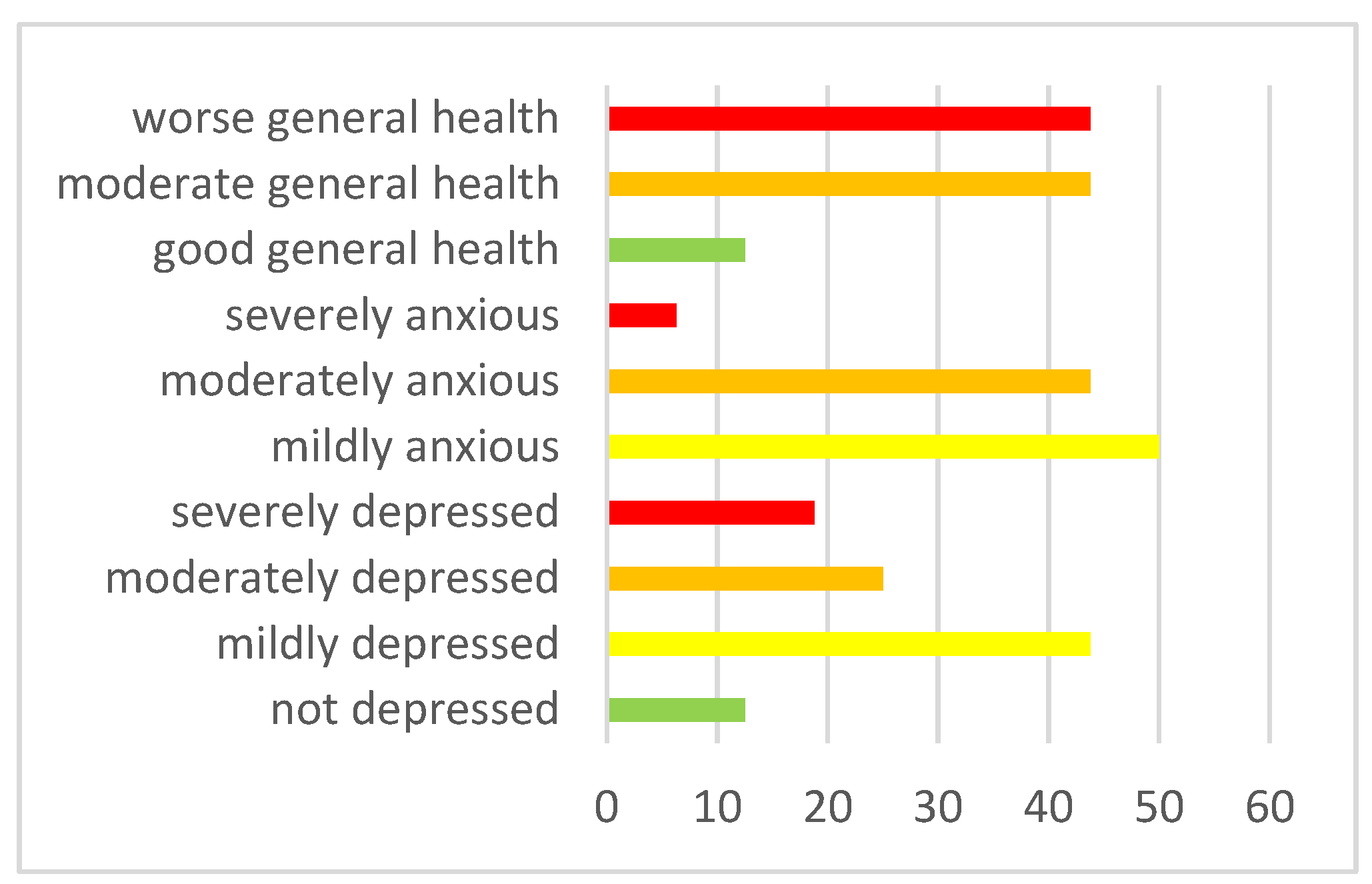
Then, the Wilcoxon rank test was run on paired samples to understand whether parents with Asperger’s children experienced the same stress and worsening of well-being as parents with neurotypical children. <this was followed, because there were no significant differences in depression (Z=-.347, p=.729), anxiety (Z=-.918, p=.359) and well-being (Z=-1.06, p=.291) between the two groups of parents (clinical and control). See Figure 2a for the clinic group and Figure 2b for the control group.
Figure 2a. Parents symptomatology in the clinic group.
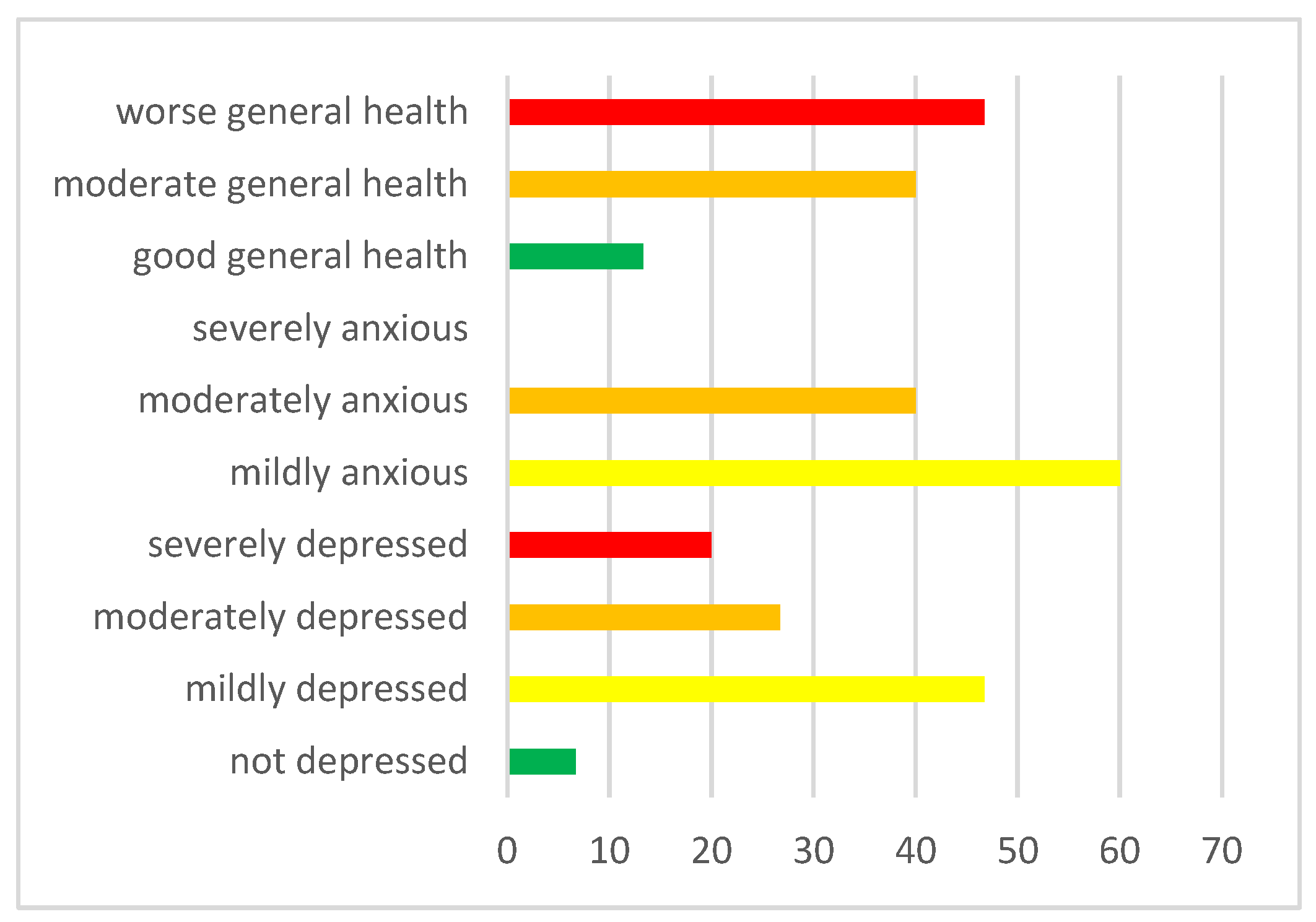
Figure 2b. Parental symptomatology in the control group.
3.3. Main psychological difficulties for children and young people with Asperger syndrome with returning to school and resuming social life since September 2020
The Wilcoxon rank test for paired samples was calculated. The aim was to evaluate the presence of a significant difference in anxiety, depression, and obsession scores between the clinic and control groups.
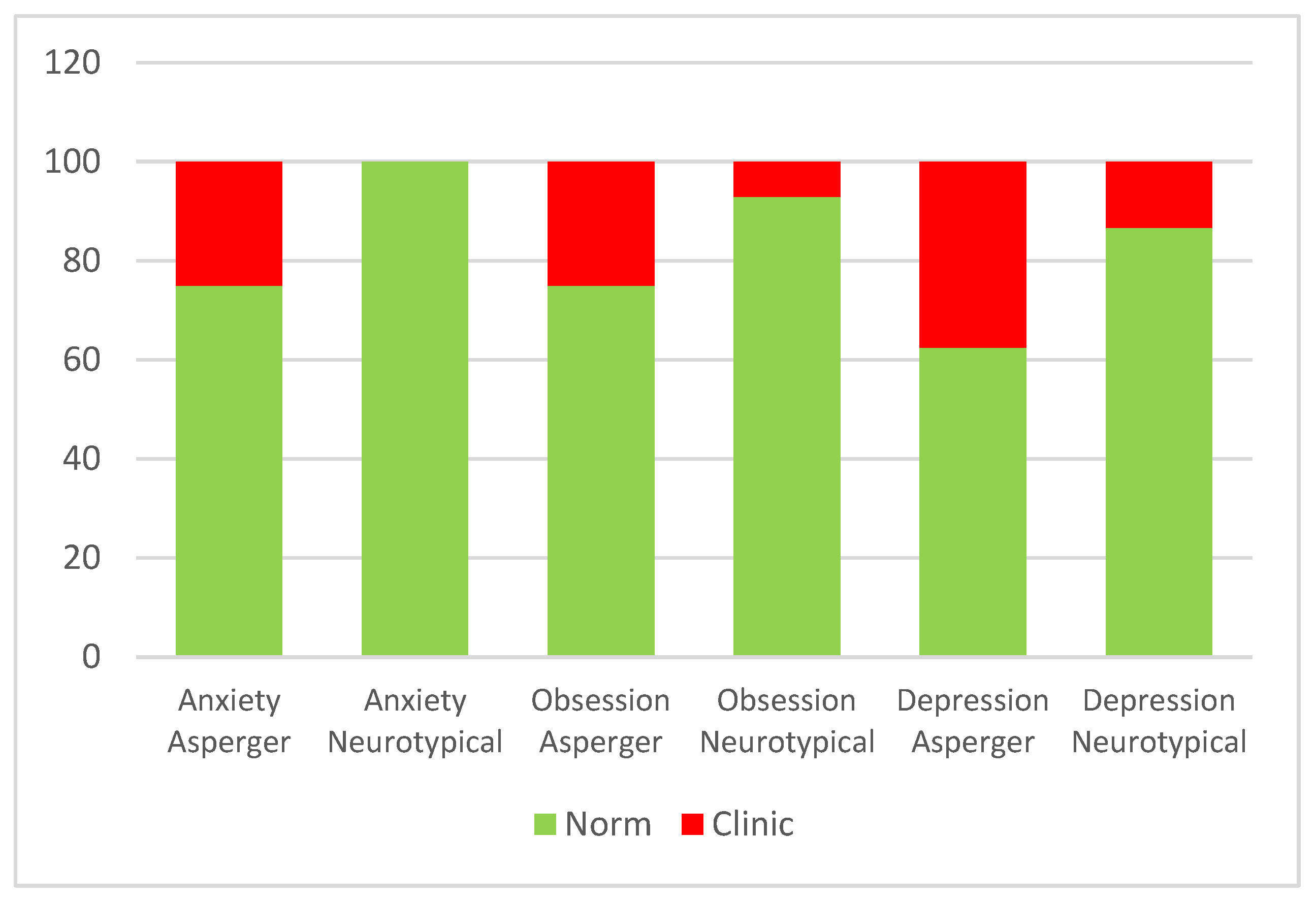
The comparison between the rank means of the two matched samples was significant only for the SAFA subscale related to anxiety (Z = -2.59, p = 0.01), where neurotypical adolescents reported, on average, higher scores (Mean = 8.12) compared to the control group (Mean = 7.25). Figure 3 shows the placement at the normal or clinical level for both groups on all SAFA scales.
Figure 3.
Placement at the normal or clinical level for both groups on all SAFA scales.
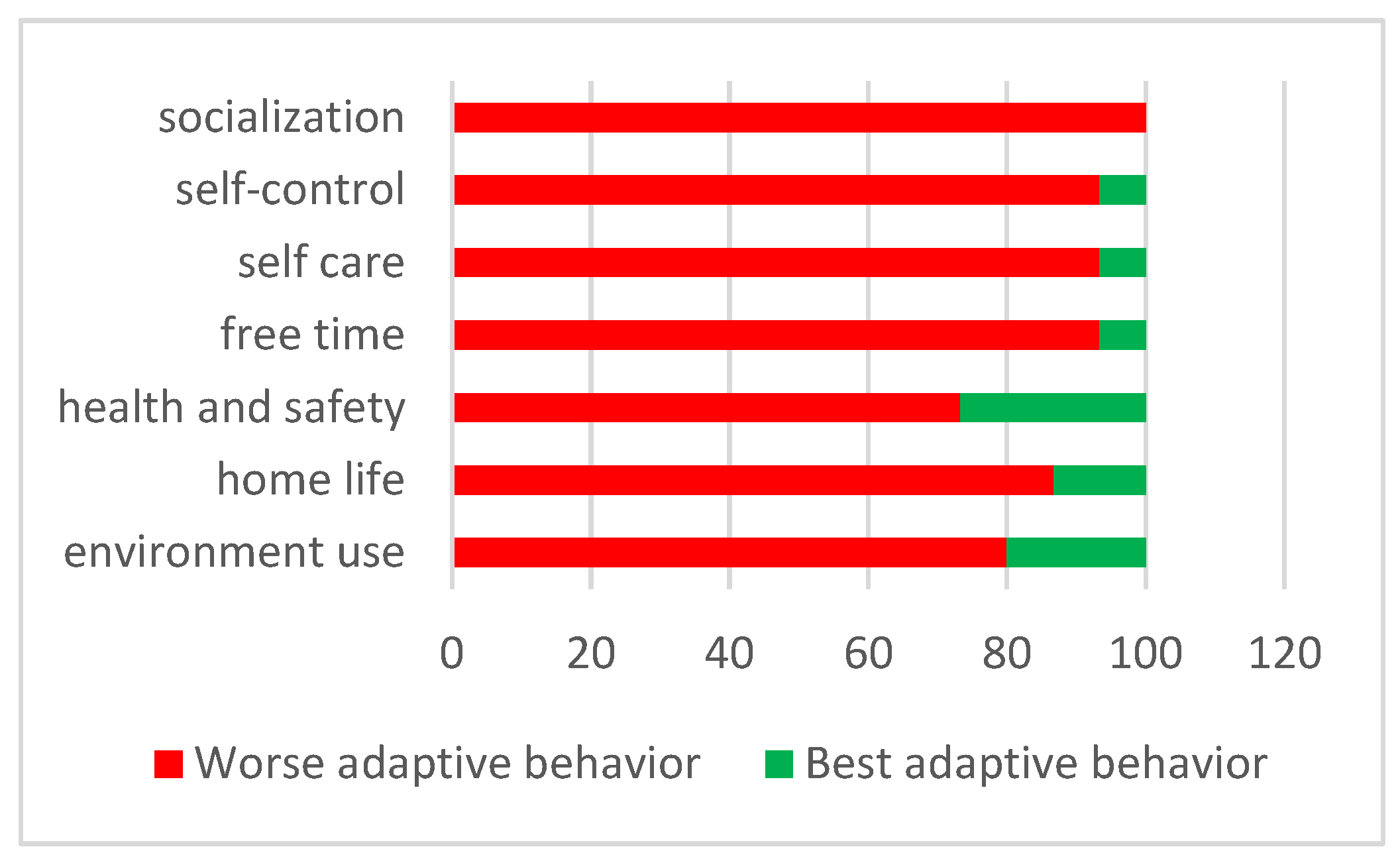
However, in terms of the adaptive behavior of Asperger’s children assessed by their parents, the worst adaptive behaviors were several, especially the area of socialization, evaluated by all parents as the area with the worst adaptive behavior (Figure 4).
Figure 4.
Placement in the worst or best adaptive behavior in ABAS-2 scores in the clinic group.
Only secondarily, a series of two paired samples Wicoxon test were run to analyze whether there was a significant difference in each adaptive behavior scale along the belonging on clinic or control group. Differences were found for the General Adaptive Composite GAC (Z = - 2.55; p = 0.01), Conceptual Composite CC (Z = - 2.13; p = 0.3), Social Composite SC (Z = - 3.11; p = 0.002) and Practical Composite PC (Z = - 2.36; p = 0.02).
The clinic group members had significantly lower averages in GAC (M=60.43; SD= 12.92) than the second group (M = 74.12; SD= 10.58), in CC (M= 55.22; SD= 5.33 versus M= 61.17; SD= 3.56), in SC (M=65.13; SD=11.03 versus M=83.38; SD=14.88) and in PC (M= 69.33; SD=20.22 versus M=87.25; SD=12.67).
3.4. The high parental stress experienced during the lockdown influenced the emotional and behavioral difficulties when children experienced the return to school and to everyday life since September 2020
For the Asperger group, a significant correlation was found between parental depression scores during lockdown and children’s anxiety subscale scores related to school return since September 2020 (r(13) = 0.56, p=.029). For the neurotypical group, a significant correlation was found between the questionnaire scores on the well-being perceived by their parents during quarantine and the scores related to the perception of life that adolescents themselves attribute to the "current moment" (r(13) = - 0.57, p = 0.02).
4. Discussion
What motivated this study was to try to give a greater voice to children and young people with Asperger syndrome (clinical population still little investigated from the point of view of the literature) with regard to their perceptions and evaluations at a retrospective level during the lockdown and their understanding of the anti-COVID rules. Above all, we wanted to investigate the long-term consequences associated with the resumption of everyday life. Furthermore, taking into consideration the entire family unit and comparing it with families with neurotypical children, the secondary aim would be, through a comparative analysis, to prepare ad hoc guidelines for parents and teachers on how to support and help children with Asperger’s, the behaviors to follow and the management of safe and secure behaviors in schools and in relationships with others; but also to give feedback to the operators of their centers of afference.
The psychologists of the center had underlined a notable characteristic of Asperger children, namely the diligent respect of rules and duties after they had been explained in a language they could understand. These explanations were given not only by the psychologists and parents, but also by the school, which assumed a fundamental role in the prompt provision of various information on COVID-19 and the support of adolescents. This feature had allowed hypothesizing an adequate knowledge and constant implementation of the anti-COVID rules confirmed by the results of the ad hoc questionnaire on perceived risk. In fact, the data confirm a good understanding and application of the regulations by the Asperger participants on the same level as their neurotypical peers, precisely out of a total of 42 questions both groups correctly answered on average 35 questions. In particular, the former correctly answered 83.6% of the questions, while the neurotypical peers 84.3%.
Regarding the second area of investigation, aimed at identifying the consequences, in terms of perceived stress, of family members of the population with Asperger’s during the quarantine; two research questions were analyzed separately. Our expectations, regarding the greater well-being of Asperger’s children in quarantine, were only partially confirmed. In fact, from their point of view, the perception of life in quarantine is estimated, like neurotypical peers, in 53.3% with an insufficient vote; this tends to fade in the post-quarantine period, however remaining higher in Asperger boys (33.3%) than in neurotypical (26.7%). In fact, adolescents in the experimental group on average, as those in the control group, perceived greater discomfort during quarantine, not benefiting as uniformly from social distancing as in those with neurological disorders [31]. Although more in line with our expectation relating to the third research question, which foresees greater difficulties for the clinical group from September 2020, Asperger’s children perceived their life more negatively than their neurotypical peers, precisely in the period of the resumption of daily activities such as, for example, school in attendance.
Although the perception of life during quarantine has an insufficient assessment for just over half of Asperger’s children, it is not excessively high since, at the individual and family level, functional strategies have been implemented to better deal with the pandemic situation. On the one hand, adolescents uniformly declared that they perceived benefits in terms of limiting travel and extracurricular activities by obtaining more time for themselves by focusing on their special interests; on the other hand, parents have tried to reconstitute stable and positive routines such as moments of family conviviality during meals, "virtual workouts" and activities games, becoming important protective factors for the entire family unit [32,33,34]. Furthermore, these new routines have made it possible to better regulate and discharge the emotionality of the children, thanks to the active and moderate participation of the parents themselves [35], but also to specifically reduce two anomalous behaviors of the children reported in the lockdown questionnaire, such as: irritable behavior and lack of appetite.
Parents of atypical development [36] reported, as parents of children with neurotypical development [35], negative effects in terms of increased stress and worsening mental health. This hypothesis was fully corroborated. In fact, in both groups, it was possible to highlight symptoms, although not excessively elevated, of anxiety and depression (higher frequency between mild and moderate), and in most parents a deterioration of well-being during quarantine. Furthermore, no significant differences were identified between the symptoms of the parents and the age groups of the children and also regarding the symptoms between the two groups of parents.
The investigation of the third research area on the difficulties in Asperger’s children identified with the resumption of everyday life from September 2020) only partially confirmed our hypothesis. In fact, as already expressed above, children with Asperger syndrome evaluate their lives by referring to the present moment with an insufficient vote in 33% of children, while the remaining percentage has medium-high evaluations. This lack of homogeneity of response can be explained by the fact that Asperger’s children, while expressing, in most of the interviews, happiness in returning to school and in resuming activities in the center of reference, however, compared to their neurotypical peers, they constantly experience a high sense of uncertainty linked, albeit minimally, to having to get used to face-to-face activities and, moreover, to the possibility of returning to DaD and therefore in quarantine or of being able to contract COVID in the face of a still deep-rooted health emergency.
These concerns are revealed by the presence, in Asperger’s children, of depressive (37.5%) and anxious (25%) symptoms related to the possibility of returning to quarantine and obsessive (25%) symptoms related to the possibility of contracting the virus, which leads them to diligently implement, and also ask others to respect, all the anti-COVID rules (wash your hands, do not touch other people’s objects, then the mask or your eyes, etc.). Specifically, all three symptoms are higher than in the control group; especially anxiety does not appear to be clinical for the neurotypical sample; while in both groups, obsessive symptoms appear to be higher in boys between 15 and 20 years of age.
This symptomatology supports the results of studies conducted on neurotypical and neurological adolescents, in which direct effects of COVID related to anxiety, depression [37], and obsessions [31,38]; in the quarantine period and immediately after. It was hypothesized that these consequences could also be found in the long term, an aspect traced in our study with reference to the Asperger population and the period from September 2020.
The results obtained for the fourth and last research area confirmed partial cumulative effects of parental stress during quarantine and behavioral and emotional imbalance with return to school from September 2020, in the knowledge that parental stress had already negatively influenced their own children [20,35,39,40]. Specifically, it seems that in children with Asperger syndrome the greater depressive symptoms of the parent during quarantine, also due to the difficulties in reconciling work and support for the DaD, have a more negative influence on anxiety symptoms (albeit moderate) related to the return to daily life in children between the ages of 10 and 14. Probably, the guys from this age group, also in the face of a greater possibility of attending their own institutions in person more than older children, could perceive more anxiety related to a situation of returning to DaD and "locked up at home" by taking siblings as an example or rather older friends, compared to a greater "resignation" to the situation for the latter.
A narrative of an adolescent explains well this concept: ’We really wanted to go back to school, I was delighted to see everyone again, with a little fear that we might attack COVID’ - “At first I was intrigued about what it would be like to go back to school and I was dubious about what it would be like to do it with masks… it went well and I was happy!” - “I was delighted to go back to class; however, it took me some time to get used to the situation again. It has been a beautiful few months but we were all always anxious for the other risk of being able to return to DaD from one day to the next, as in reality then it happened!".
In neurotypical adolescents, a lower well-being perceived by parents during quarantine correlates with a lower evaluation that the boys themselves give to their lives in the current moment; in particular, it seems to be the older boys who express these evaluations, thus perceiving even greater effect of the well-being experienced in quarantine by their parents.
Strengths and Limits
One of the limitations of this research is certainly the number of participants and the gender and age characteristics of the sample, which do not make the results sufficiently generalizable. The sample made up of 16 Asperger’s children paired with neurotypically developed children must, however, take into account both the niche clinical population that we have tried to recruit in the project, and the historical context in which entire families have found themselves facing the overwhelming and disharmonious everyday life, which could have undermined the greater adherence to research.
An aspect of particular relevance is the fact that the participants are all males and there is little heterogeneity as regards their age and distribution in the three academic ranges (primary, lower secondary, and upper secondary schools). It would be interesting to extend the survey also to girls with Asperger syndrome, albeit of lesser diagnostic importance precisely because they are very often underdiagnosed and at the same time make the age groups of the participants more homogeneous.
A second important limitation was the large number of items to which the boys were subjected; specifically the application of three subscales of the SAFA (anxiety, depression, and obsessions) made it more difficult to maintain the attention of the participants and lengthened the time required to complete the questionnaire, especially for the adolescents in the experimental group.
Finally, the predominantly transversal data collection that refers in many respects to the present moment, integrated with specific questions and questionnaires in which they are asked to recall aspects related to the more remote past (September 2019) and more recent (during quarantine) has encountered considerable difficulties in the Asperger population regarding the temporal aspect of the past.
Despite these limitations, we can identify three strengths of the research: the first is related to the fact that the research itself is the first, to our knowledge, to investigate difficulties during quarantine but, above all, the long-term effects of the measures determined from the onset of the Coronavirus pandemic in Asperger children and teenagers and the perceived difficulties with returning to everyday life. A second merit is that we conducted the survey on families in Veneto, one of the most affected areas on the national territory, to highlight the consequences in a context in which there has been a greater incidence of COVID. With reference to the latter aspect, it would be interesting to be able to estimate the presence of differences that we could find in families with the same atypical population but in central-south regions of Italy.
Finally, a last and great advantage is highlighted by the use of the mixed and multi-informant approach. The first allowed us to delve into the narrowest niche of Paduan families, aspects more generally investigated through questionnaires, both as regards Asperger’s children and their parents; the second, through the involvement of significant family members, has allowed us to better enrich not only the individual but also the family picture.
In a future perspective, not too distant, it could be interesting to include support teachers in the study, with the aim not only of investigating their experiences in quarantine with the DaD and the fluctuating and partial recovery of the presence for most of the new academic year; but also of highlighting their role for Asperger’s children and highlighting aspects of greater management difficulty that could be supported by ad hoc guidelines.
Furthermore, for future studies, it would be more necessary to reduce the workload required for the recruited clinical and neurotypical population.
Finally, starting from our results, it could be interesting to investigate in the same group of participants one year from today whether and for how long the symptoms persist, making this study a starting point for a possible longitudinal study of the consequences of a pandemic that has marked, like a scar, the experience of each of us.
Authors Contributions
Conceptualization, M.T., M.G.; methodology, M.T. and L.T.; software, R.B.I., M. R.; formal analysis, M.T. and M.R.; investigation, M.R., M.G.; data curation, M.R., R.M.I.; writing - original draft preparation, M.T.; writing - review and editing, M.R., R.B.I., M.G.; project administration, M.G. All authors have read and agreed to the published version of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research did not receive external funding.
Conflicts of Interest
The authors declare that they have no conflict of interest.
References
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders, fifth edition (DSM-5). Washington, DC: American Psychiatric Association; 2013. 2013.
- Attwood, T. (2019, March). Guida completa alla Sindrome di Asperger. Edra.
- Baio, J, Wiggins L, Christensen D.L., Maenner, M. J., Daniels, J., Warren, Z.,… & Durkin, M. S. (2018). Prevalence of Autism Spectrum Disorder Among Children Aged 8 Years — _Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2014. MMWR Surveillance Summaries, 67(No.SS-6):1–23. [CrossRef]
- Wang, C., Pan, R., Wan, X., Tan, Y., Xu, L., Xu, L., Ho, C. e, Ho, R. C. (2020). Immediate Psychological Responses and Associated Factors during the Initial Stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China. Environmental Research and Public Health, 17, 1-25. [CrossRef]
- Baumer N, Spence S. Evaluation and management of the child with autism spectrum disorder. Continuum (Minneap Minn) 2018; 24: 248-75. [CrossRef]
- Vasa, R. A., Singh, V., Holingue, C., Kalb, L. G., Jang, Y., & Keefer, A. (2021). Psychiatric problems during the COVID-19 pandemic in children with autism spectrum disorder. Autism Research, 14(10), 2113– 2119. [CrossRef]
- Amorim R, Catarino S, Miragaia P, Ferreras C, Viana V, Guardiano M. The impact of COVID-19 on children with autism spectrum disorder. Rev Neurol 2020; 71: 285-91. [CrossRef]
- Wang, L., Zhang, H., Shang, C., Liang, H., Liu, W., Han, B., Xia, W., Zou, M., & Sun, C. (2022). Mental health issues in parents of children with autism spectrum disorder: A multi-time-point study related to COVID-19 pandemic. Autism Research, 15(12), 2346– 2358. [CrossRef]
- Liu JJ, Bao Y, Huang X, Shi J, Lu L. Mental health considerations for children quarantined because of COVID-19. Lancet Child Adolesc Health 2020 May; 4:347–9. [CrossRef]
- Marjanovic, Z., Greenglass, E. R., Coffey, S. (2007). The relevance of psychosocial variables and working conditions in predicting nurses coping strategies during the SARS crisis: an online questionnaire survey. International Journal of Nursing Studies, 44, 991–98. [CrossRef]
- Reynolds, D. L., Garay, J. R., Deamond, S. L., Moran, M. K., Gold, W., Styra, R. (2008). Understanding, compliance and psychological impact of the SARS quarantine experience. Epidemiology and Infection, 136, 997–1007. [CrossRef]
- Bai, Y. Bai, Y., Lin, C. C., Lin, C.Y., Chen, J. Y., Chue, C. M., Chou, P. (2004). Survey of stress reactions among health care workers involved with the SARS outbreak. Psychiatric Service, 55, 1055–57. [CrossRef]
- Cava, M. A., Fay, K. E., Beanlands, H. J., McCay, E. A., Wignall, R. (2005). The experience of quarantine for individuals affected by SARS in Toronto. Public Health Nursing, 22, 398–406. [CrossRef]
- Robertson, E., Hershenfield, K., Grace, S. L., Stewart, D. E. (2004). The psychosocial effects of being quarantined following exposure to SARS: a qualitative study of Toronto health care workers. The Canadian Journal of Psychiatry, 49, 403–07. [CrossRef]
- Blendon, R. J., Benson, J. M., DesRoches, C. M., Raleig, E., Taylor-Clark, K. (2004). The public’s response to severe acute respiratory syndrome in Toronto and the United States. Clinical Infectious Dieasess, 38, 925–31. [CrossRef]
- Jeong, H., Yim, H. W., Song, Y. J., et al. (2016) Mental health status of people isolated due to Middle East respiratory syndrome. Epidemiology and Health, 38. [CrossRef]
- Di Giovanni, C., Conley, J., Chiu, D., Zaborski, J. (2004). Factors influencing compliance with quarantine in Toronto during the 2003 SARS outbreak. Biosecur Bioterror, 2, 265–72. [CrossRef]
- Xiang, M.; Zhang, Z.; Kuwahara, K. (2020) Impact of COVID-19 Pandemic on children and adolescents’ lifestyle behavior larger than expected. Prog. Cardiovasc. Dis. 2020. [CrossRef]
- Zhou, S-J.; Wang, L-L.; Yang, R.; Yang, X-J.; Zhang, L-G.; Guo, Z-C.; Chen, J-C.; Wang, J-Q.; Chen, J-X.; (2020) Sleep problems among Chinese adolescents and young adults during the coronavirus-2019 pandemic, Sleep Medicine 74, 39-47. [CrossRef]
- Uccella S, De Grandis E, De Carli F, D’Apruzzo M, Siri L, Preiti D, Di Profio S, Rebora S, Cimellaro P, Biolcati Rinaldi A, Venturino C, Petralia P, Ramenghi LA and Nobili L. (2021) Impact of the COVID-19 Outbreak on the Behavior of Families in Italy: A Focus on Children and Adolescents. Public health. [CrossRef]
- Cantril, H. (1965). The pattern of human concerns. New Brunswick, NJ: Rutgers University Press, p.22.
- Cianchetti, C. & Sannio Fancello G. (2001). SAFA: scale psichiatriche di autosomministrazione per fanciulli e adolescenti. Firenze O.S.
- Harrison, P. L., & Oakland, T., (2003). Adaptive behavior assessment system – Second Edition. Los Angeles: Pearson Education. Adattamento italiano a cura di Ferri Rosa, Orsini Arturo e Rea Monica (2014). Firenze: Giunti Psychometrics.
- Radloff, L.S. (1977). The CES-D Scale: A Self-Report Depression Scale for Research in the General Population. Applied Psychological MeasurementMisurazione psicologica applicata, 1, 385–401. 1. [CrossRef]
- Spitzer, R.L., Kroenke K., Williams J.B., Löwe B. (2006). A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006 May 22;166(10):1092-7. 22 May.
- Goldberg, D.P.; Gater, R.; Sartorius, N.; Ustun, T.B.; Piccinelli, M.; Gureje, O.; Rutter, C. The Validity of two Versions of the GHQ in the WHO Study of Mental Illness in General Health Care. Psychol. Med. 1997, 27, 191–197. [Google Scholar] [CrossRef]
- Goldberg, D.P. General Health Questionnaire (GHQ-12); NFER-Nelson: Windsor, UK, 1992. [Google Scholar]
- Politi, P.L.; Piccinelli, M.; Wilkinson, G. Reliability, validity and factor structure of the 12-item General Health Questionnaire among young males in Italy. Acta Psychiatr. Scand. 1994, 90, 432–437 2021. [Google Scholar] [CrossRef] [PubMed]
- Piccinelli, M.; Bisoffi, G.; Bon, M.G.; Cunico, L.; Tansella, M. Validity and test-retest reliability of the Italian version of the 12-item General Health Questionnaire in general practice: A comparison between three scoring methods. Compreh. Psychiat. 1993, 34, 198–205. [Google Scholar] [CrossRef]
- Bonichini, S., & Tremolada, M. (2021). Quality of Life and Symptoms of PTSD during the COVID-19. [CrossRef]
- Lockdown in Italy. International Journal of Environmental Research and Public Health, 18(8), 4385. [CrossRef]
- Conti, E., Sgandurra, G., De Nicola, G., Biagioni, T., Boldrini, S., Bonaventura, E., Buchignani, B., Della Vecchia, S., Falcone, F., Fedi, C., Gazzillo, M., Marinella, G., Mazzullo, C., Micomonaco, J., Pantalone, G., Salvati, A., Sesso, G., Simonelli, V., Tolomei, G., Troiano, I., Cioni, G., Masi, G., Muratori, F., Milone, A, & Battini, R. (2020). Behavioural and Emotional Changes during COVID-19 Lockdown in an Italian Paediatric Population with Neurologic and Psychiatric Disorders. Brain sciences, 10(12), 918. [CrossRef]
- Bates, L. C., Zieff, G., Stanford, K., Moore, J. B., Kerr, Z. Y., Hanson, E. D., Barone Gibbs, B., Kline, C. E., & Stoner, L. (2020). COVID-19 Impact on Behaviors across the 24-Hour Day in Children and Adolescents: Physical Activity, Sedentary Behavior, and Sleep. Children (Basel, Switzerland), 7(9), 138. [CrossRef]
- Masten, A.S., & Motti-Stefanidi, F. (2020). Multisystem Resilience for Children and Youth in Disaster: Reflections in the Context of COVID-19. Adversity and Resilience Science. 1. [CrossRef]
- Prime, H., Wade, M., & Browne, D. T. (2020). Risk and resilience in family well-being during the COVID-19 pandemic. The American psychologist, 75(5), 631–643. [CrossRef]
- Spinelli, M., Lionetti, F., Pastore, M., & Fasolo, M. (2020). Parents’ Stress and Children’s Psychological Problems in Families Facing the COVID-19 Outbreak in Italy. Frontiers in psychology, 11, 1713. [CrossRef]
- Montirosso, R., Mascheroni, E., Guida, E., Piazza, C., Sali, M. E., Molteni, M., & Reni, G. (2021). Stress symptoms and resilience factors in children with neurodevelopmental disabilities and their parents during the COVID-19 pandemic. Health Psychology, 40(7), 428–438. [CrossRef]
- Magson, N.R. Magson, N.R., Freeman, J.Y.A., Rapee, R.M., Richardson, C.E., Oarl, E.L, & Fardouly, J.(2020). Risk and Protective Factors for Prospective Changes in Adolescent Mental Health during the COVID-19 Pandemic. J Youth Adolescence 50, 44–57 (2021). 2021; 50. [Google Scholar] [CrossRef]
- Nearchou, F., Flinn, C., Niland, R., Subramaniam, S. S., & Hennessy, E. (2020). Exploring the Impact of COVID-19 on Mental Health Outcomes in Children and Adolescents: A Systematic Review. International journal of environmental research and public health, 17(22), 8479. [CrossRef]
- Orgilés, M., Morales, A., Delvecchio, E., Mazzeschi, C., & Espada, J. P. (2020). Immediate Psychological Effects of the COVID-19 Quarantine in Youth From Italy and Spain. Frontiers in psychology, 11, 579038. [CrossRef]
- Racine, N., Cooke, J. E., Eirich, R., Korczak, D. J., McArthur, B., & Madigan, S. (2020). Child and adolescent mental illness during COVID-19: A rapid review. Psychiatry research, 292, 113307. [CrossRef]
Figure 1.
Estimated marginal means of Cantrill’s life perceptions in the neurotypical group.
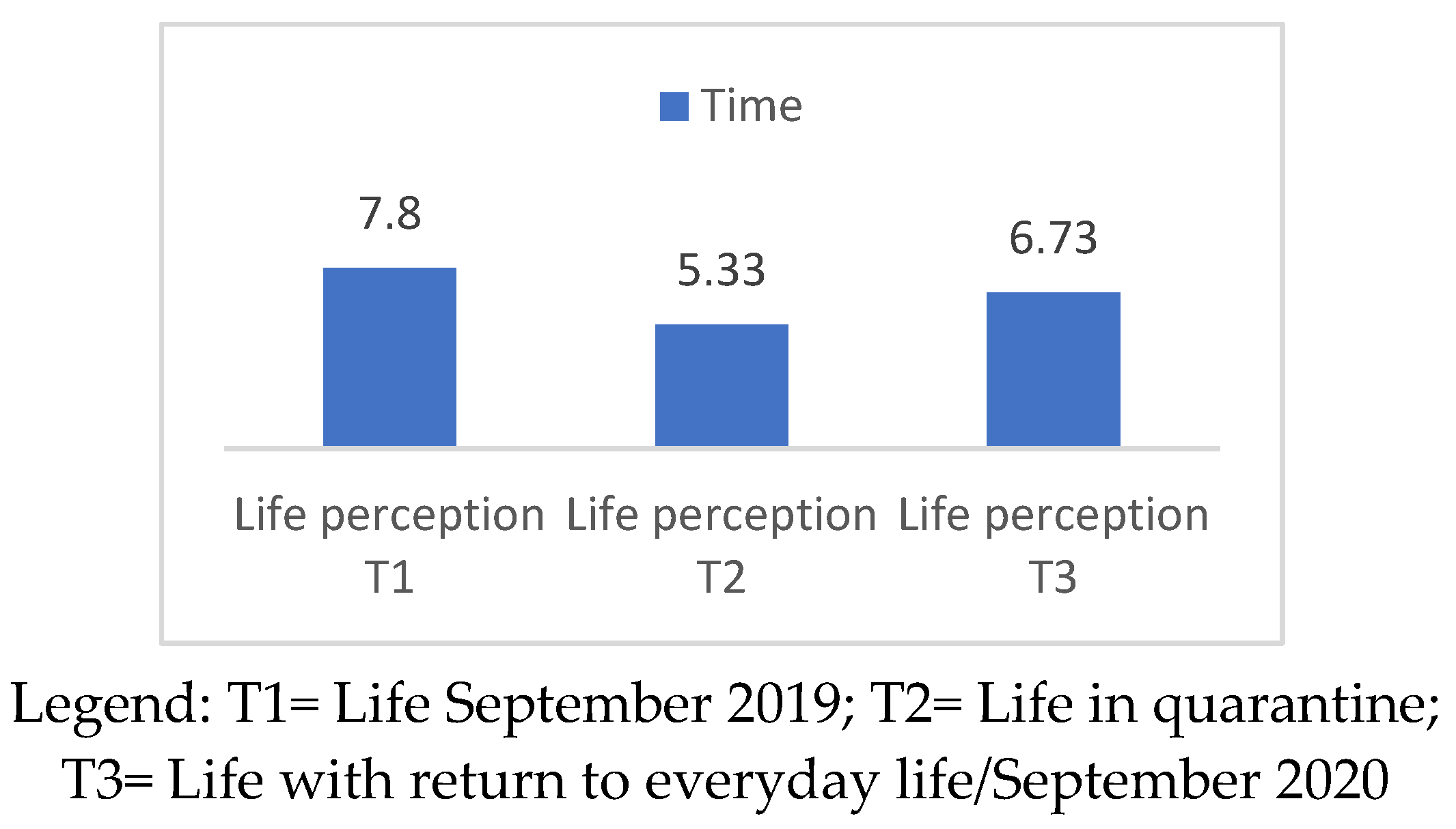

Table 1.
Sociodemographic characteristics of the participants.
| Asperger | Neuro Typical | ||||||
| Adolescents | Frequency | Mean | SD | Frequency | Mean | SD | |
| Gender | Male | 16 | 16 | ||||
| Age | 14 | 3.62 | 14.07 | 3.31 | |||
| Age groups | 10-14 yrs old 15-20 yrs old |
10 6 |
9 6 |
||||
| School | Primary | 3 | 3 | ||||
| Secondary first grade Secondary second grade |
6 7 |
5 7 |
|||||
| Support school | Yes No |
12 4 |
0 15 |
||||
| Parents | Frequency | Mean | SD | Frequency | Mean | SD | |
| Role | Father Mother |
4 11 |
4 12 |
||||
| Education | Primary/secondary school first grade | 0 | 0 | ||||
| Secondary second grade Yunior degree |
6 2 |
9 1 |
|||||
| Degree | 7 | 5 | |||||
| Master/Ph.D. | 3 | 1 | |||||
| Number of children | 1 2 3 4 5 |
4 8 2 0 1 |
4 9 2 1 0 |
||||
| Child with other disabilities | Yes No |
2 13 |
0 15 |
||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



