
Submitted:
31 December 2022
Posted:
09 January 2023
You are already at the latest version
Abstract
Japan is experiencing a super-aging society faster than is anywhere else worldwide. Consequently, extending healthy life expectancy is an urgent social issue. To understand diet that supports the extension of healthy life expectancy, we studied the relationships among quality of life (QOL: SF-36 questionnaire), physical activity (number of steps and activity calculated using an accelerometer), physical function (muscle strength, movement function, agility, static balance, dynamic balance, and walking function) and dietary intake among 469 older adults living in the Tokyo metropolitan area (65–75 years old, men/women = 166/303) from February 23, 2017, to March 31, 2018. There was a significant positive association between physical QOL and steps, moderate-intensity activity, and high-intensity activity (p < 0.05), and a significant positive association (p < 0.05) between physical activity and movement, static balance, and walking functions, but no association with muscle strength. These three body functions were significantly positively correlated with intake of vegetables, seeds, fruits, and milk, and with magnesium, potassium, vitamin B6, and the dietary fibre/carbohydrate ratio and composition ratios (p < 0.05). Balancing food and nutrition may improve QOL in older adults through increased physical function and physical activity. Future verification of interventions is needed.
Keywords:
quality of life
; physical activity
; physical function
; food and nutrition
; older Japanese adults
1. Introduction
Japan is experiencing a super-aging society at a faster rate than is anywhere else worldwide: approximately 28.4% of the total population is aged 65 years and over, and more than 18 million people are aged 75 years and over [1]. In such a social situation, there is a need to respond to the decrease in the working-age population (15–65 years old) and the increased burden of nursing care. In addition, from a medical perspective, reducing the burden of nursing care by extending healthy life expectancy is an urgent issue. Thus, a national health promotion program, Health Japan 21 (the second term), was formulated [2], given that metabolic syndrome and locomotive syndrome were observed as a response to cardiovascular diseases and decreased physical function due to aging.
Concerning abdominal fat, the accumulation of visceral fat is a higher risk factor for metabolic syndrome than is subcutaneous fat [3]. Thus, we have focused on visceral fat accumulation [4], which is key to the diagnostic criteria for metabolic syndrome, and we have examined the relationship between diet and lifestyle. In a previous study [5], we confirmed that dietary quality, quantity, time, night meals, fast eating, and inactivity are related to visceral fat accumulation. Among these factors, improving dietary quality might suppress visceral fat accumulation. Further examination revealed that the dietary composition of protein (kcal)/lipid (kcal) = 1.0, dietary fibre (g)/carbohydrate (g) > 0.063, and ω3 (mg)/lipid (g) > 0.054 may reduce the accumulation of visceral fat. In an additional clinical intervention study, these dietary compositions were shown to reduce visceral fat accumulation (the SMART WASYOKU® cuisine) [6].
The relationships among physical function, frailty, degree of care required, and lifestyle in older Japanese adults have been reported in several regions of Japan [7,8,9]. Cohort studies have reported the relationship between physical activity and dietary content based on qualitative measurement [10,11,12,13,14], where either diet or physical activity or function was evaluated using a qualitative assessment method. In particular, many dietary surveys adopted a food frequency questionnaire, the weakness of which is low quantitative accuracy [15]. Consequently, no research studies have performed quantitative assessments of dietary content, physical activity, and function. Therefore, we conducted a cross-sectional study among older Japanese adults to quantitatively evaluate the relationships among physical activity, physical function, and dietary content.
2. Materials and Methods
2.1. Participants
This study was conducted between February 23, 2017, and March 31, 2018. A cross-sectional study was conducted with 473 men and women aged between 65 and 75 years who were living in the suburban areas of west Tokyo. Based on multiple linear regression analysis of 36 items (characteristics, quality of life, physical activity, physical functions, and food intake), we aimed to include at least 360 subjects, namely 10 times the number of items [12]. We explained the examination to the participants at a briefing session and obtained their written informed consent to participate in the research. After excluding four people who did not participate in the measurements, 469 people who completed the study were included in the analysis (Figure 1).
This study procedure was approved by two ethics committees (Waseda University's Ethical Review Committee on Human Research and Kao Corporation's Institute of Biological Sciences Research Ethics Review Committee) and implemented in accordance with the Declaration of Helsinki (UMIN000026007).
2.2. Questionnaire survey
After agreeing to participate in the examination at the briefing session, the following questionnaire survey was administered and collected on the day of the measurement meeting: the Medical Outcomes Study 36-Item Short-Form Health Survey (SF-36), which assesses quality of life (QOL), and inquiries about physical conditions and medical history; the International Physical Activity Questionnaire (Japanese version), which confirms physical activity; and dietary and lifestyle questionnaires. For the SF-36, the following three dimensions were calculated from the scores of eight subscales, using specific standardized algorithms: physical component summary (PCS), mental component summary (MCS), and role–social component summary (RCS) [13].
2.3. Dietary survey
Photo recording was adopted as a quantitative assessment method. Participants took photographs of all meals, including snacks, for 3 days [5]. In addition, a description of all meals was prepared. Meal content was analysed by two independent dietitians skilled in meal photo analysis. Based on the results, the estimated intake of nutrients and foods was calculated based on the Standard Tables of Food Composition in Japan, using the residual method to adjust for total energy intake [16].
2.4. Physiological indicators
Height (cm), weight (kg), body mass index (BMI, kg/m2), abdominal circumference (cm), visceral fat area (cm2, EW-FA90; Panasonic Corporation, Osaka, Japan), body temperature (℃), and blood pressure (mmHg) were measured.
2.5. Physical activity
The amount of physical activity and the number of walking steps were measured while the individual performed their usual activities, using an accelerometer (Lifecorder EX; Suzuken Co. Ltd., Nagoya, Japan) placed on the participant’s waist at all times while awake, except during swimming or bathing. The criteria for analysis were as follows: wearing of the accelerometer on their waist for a total duration of ≥4 days including weekdays and holidays, for ≥10 hours/day [17,18,19]. Exercise intensity was defined as follows: micro-exercise: <1.8, low intensity: 1.8–3.0, moderate intensity: 3.0–6.0, and high intensity: ≥6.0 (unit: metabolic equivalents) [20].
2.6. Physical functions
2.6.1. Muscle strength
For grip strength, the average value measured on each arm was determined. To determine knee extension muscle strength, one ankle was fixed with a belt, and a sensor detected the muscle strength when the participant extended the other side’s knee while the experimenter supported the upper knee of the fixed side. The average value measured for each side was adopted, adjusted for body weight.
2.6.2. Movement function
2.6.3. Agility function
The open–close stepping test was used. In the test, the inside and outside of the tape wire were opened and closed at the same time at intervals of 30 cm, and a step was taken. The number of times this could be stepped in 20 seconds was measured.
The participant sat in a chair with no armrests, with both feet placed in the centre of a simple measurement sheet (30 × 30 cm). The participants’ hands were used to hold both sides of the chair. As soon as the experimenter signalled the participant to start, the participant opened their legs and spread their feet as quickly as possible, touching the floor beside the sheet with the forefoot or the entire sole of the foot, and then quickly returned their feet and legs to the original position. This series of actions constituted one repetition; the experimenter counted how many repetitions the subjects could perform in 20 seconds [24].
2.6.4. Balance function
The one-leg standing test with eyes open (OLS test) was used to assess sedentary balance. The ability of the participant to stand on one leg with eyes open was measured for up to 120 seconds, in accordance with the procedures for physical tests for older adults designed by the Ministry of Education, Culture, Sports, Science and Technology [25].
The functional reach test was used to assess movement balance. The participant extended their arms as far forward as possible in the horizontal plane while keeping both their heels in contact with the ground. The score was obtained by measuring the distance between the start and end positions of the fingertips [26].
2.6.5. Walking function
The timed up and go test (TUG test) was used to assess walking function. The participant was instructed to move from a seated position in an armless chair to a standing position, walk 3 meters at their fastest safe pace, turn around, walk back to the chair, and sit down. They were allowed two attempts. The times taken to execute the motion series were averaged [27,28].
2.7. Blood analysis
Participants were asked to refrain from eating or drinking after 9:00 pm before the measurement day. Consequently, they fasted overnight for more than 12 hours, and blood samples were collected. The levels of the following variables were measured: items related to glucose and lipid metabolism (glucose, insulin, HbA1c, triglycerides, free fatty acids, total cholesterol, high-density, and low-density lipoprotein cholesterol), blood counts (white and red blood cell counts, platelet count, haemoglobin, haematocrit), minerals (sodium, potassium, chloride, calcium, magnesium, inorganic phosphorus, and iron), and liver and kidney function (aspartate aminotransferase, alanine aminotransferase, alkaline phosphatase, gamma-glutamyl transferase, creatine kinase, amylase, uric acid, urea nitrogen and creatinine).
2.8. Statistical analysis
All statistical analyses were performed using SPSS (version 24.0 for Windows; SPSS, Inc., Armonk, NY, USA). The relationships between QOL–physical activity and physical activity–physical function were analysed using multiple regression, adjusting for sex, age, and BMI. Foods and nutrients related to physical function were extracted using multiple regression analysis with a forward selection method by forced entry of sex, age, and BMI.
3. Results
The characteristics of the participants (n = 469) are shown in Table 1. Systolic blood pressure was more than 140 mmHg in both sexes, and the mean values of other characteristics were in the normal range, even though visceral fat accumulation was observed in men (Table 1).
The average number of steps per day was 7931 and 6962 in men and women, respectively (Table 2); there was no significant difference between the sexes. These values were higher than the average values among Japanese individuals of a similar age (6311 steps in men/5438 steps in women, at 65–74 years old) [29]. Grip strength and the OLS test in both sexes were lower than the Japanese averages for each age group.
The PCS, MCS, and RCS were calculated based on the responses provided to the SF-36. The relationships between these component summaries and physical activity were examined using multiple regression analysis. The PCS was significantly positively associated with the number of steps and moderate- and high-intensity exercise. Similar associations were found between MCS and moderate-intensity exercise, RCS, and the number of steps (Table 3).
In addition, the relationship between physical activity and physical function was similarly analysed. The number of steps was significantly associated with the results of the two-step (locomotive function), OLS (sedentary balance function), and TUG tests (walking function) (Table 4). Similar associations were found between moderate-intensity exercise and the two-step test, high-intensity exercise, and the OLS test.
Further, the relationships among the results of the aforementioned physical function measurement tests (two-step, OLS, and TUG) and food intake were examined. Vegetable intake was associated with extension of the standing time (OLS test; p = 0.028), while cereal and meat intakes were related to shorter standing times (p = 0.012 and p = 0.009, respectively; Table 5). Vegetable and milk intakes were associated with faster movement (TUG test; p = 0.001 and p = 0.033, respectively); however, cereal intake was associated with a delay in movement (p = 0.031). Vegetable, seed, fruit, and beverage intakes were associated with longer strides (two-step test; p = 0.019, p = 0.004, p = 0.028, and p = 0.040, respectively), while egg intake was associated with shorter strides (p = 0.020). With respect to nutrients, magnesium (Mg) intake was positively related to the results of the OLS test, potassium (K) intake was positively related to the results of the TUG test, vitamin B6 (VB6) intake was positively related to the results of the two-step test, and the dietary fibre intake/carbohydrate intake ratio (Fib/C) was positively related to the results of all three tests.
4. Discussion
We conducted a study of the quantitative relationships among diet, physical functions, and physical activity in older Japanese adults. The intake of Mg, K, VB6, fibre, and foods that include these nutrients (i.e., vegetables, fruits, and seeds) was positively correlated with physical functions (i.e., movement, balance, and walking functions). Physical activity, positively related to these physical functions, might result in improved physical QOL.
The average values of items other than systolic blood pressure were within the diagnostic criteria for metabolic syndrome (Table 1) [30]. A higher average number of steps than those of Japanese individuals of similar age of both sexes suggested that the participants in this study lived active daily lives; however, their physical functions, such as muscle strength and balance, might not have been superior to those of other individuals of the same age (Table 2).
Physical activity, comprising steps, moderate-intensity exercise, and high-intensity exercise, was significantly positively associated with PCS. This finding is consistent with that of a previous report describing the relationship of PCS with the number of steps and exercise intensity [31]. Similar associations were found between MCS and moderate-intensity exercise and between RCS and number of steps. These results suggest that QOL is related to number of steps, moderate-intensity exercise, and high-intensity exercise.
The physical functions that were significantly associated with the number of steps were sedentary balance (OLS test), walking function (TUG test), and mobility (two-step test). Moderate- and high-intensity exercise was significantly related to mobility and sedentary balance, respectively. Thus, a significant association was found between physical activity (number of steps, moderate-intensity exercise and high-intensity exercise) and physical functions (sedentary balance, walking function, and mobility), while it appears that physical functions, such as muscle strength and agility, were not associated with physical activity. A high level of daily physical activity is reportedly related to high mobility function but not to muscle strength [32]. The results of the present study are generally consistent with those of the aforementioned report. Therefore, improvement of mobility function, not muscle strength, may be important to support physical activity in older adults.
Seed intake was positively associated with mobility (Table 5). Milk and fruit intakes were positively related to walking function and mobility, respectively. Vegetable intake was positively associated with all three physical functions; however, cereal intake was negatively related to sedentary balance and walking function. Egg intake was negatively associated with mobility. Mg intake was positively related to sedentary balance, K intake was positively related to walking function, VB6 intake was positively related to mobility, and Fib/C was positively related to all three physical functions.
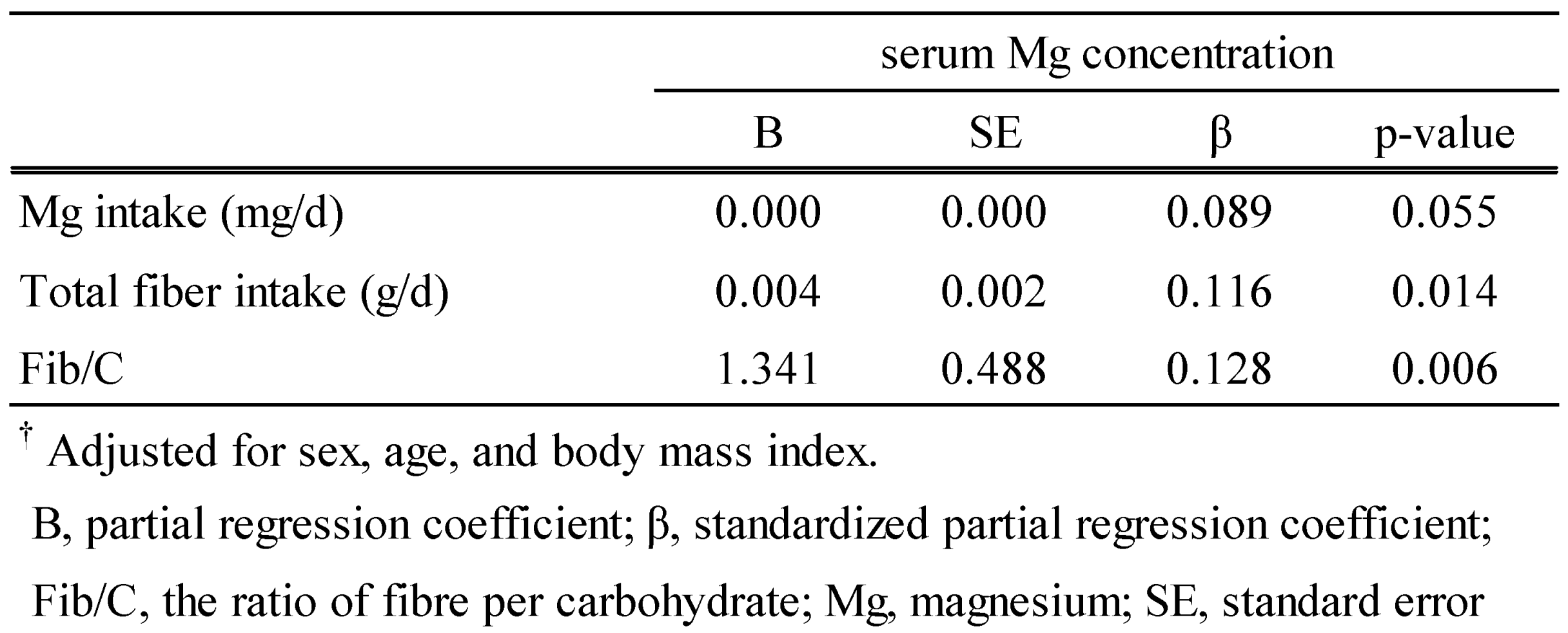
Mg is found in vegetables and seeds; K is found in vegetables and fruits; VB6 is found in meat, fish, and seeds; and fibre is found in vegetables and fruits. Mg is involved in muscle relaxation and contraction [33], and its supplementation reportedly improves physical function [34]. K is reportedly involved in neurotransmission and muscle contraction, and it has been recently reported that VB6 intake is associated with agility and mobility [35]. In addition, Mg, K, and VB6 intakes were reported to be positively associated with physical activity [36]. Fibre intake, which has an unknown relationship with physical functions, was suggested to be associated with physical activity [37]. Fibre reportedly affects the absorption of various nutrients. The absorption of K and VB6 is primarily due to passive transport; therefore, the effect of fibre intake is unknown. Conversely, the enhancing effect of fibre on Mg absorption through active transportation has been reviewed at the level of animal experiments and clinical trials [38]. It was confirmed that Fib/C, not Mg intake, was significantly positively related to the blood Mg concentration based on multiple regression analysis (Table 6). Thus, fibre intake might indirectly affect physical function by increasing Mg absorption.
Based on the results of this study, we elucidated the quantitative relationships among physical activity, physical function, and food intake in older Japanese adults living in urban areas. Several limitations of the present study should be considered. First, this study was conducted following a cross-sectional design. Long-term observational studies are needed to examine the diets that promote a high quality of life through improving physical function and activity. Second, the participants were living in urban areas. Third, from the comparison with the national average of steps in individuals of the same age, the participants seemed to be relatively active. Thus, it is necessary to study participants who live in rural areas and who participate in other activities.
In conclusion, we found significant relationships among intake of foods and nutrients, physical functions, physical activity, and physical QOL. The intake of certain foods and nutrients was positively correlated with physical functions. Physical activity, positively related to these physical functions, might result in improved physical QOL among older Japanese adults. In the future, we aim to conduct a clinical trial using nutrients and/or foods recognized from this study as possible intervention targets. Thus, we will propose a diet that supports movement and activities of the older adult population.
Author Contributions
The examination plan was prepared by all authors. T.F., K.F., and M.M. were in charge of the operation of the examination. T.F. analysed the data and drafted the paper. All authors considered the results and confirmed the contents of the paper.
Funding
This research was funded by Kao Corporation, registered number 818-20161118.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, approved by Waseda University's Ethical Review Committee on Human Research and Kao Corporation's Institute of Biological Sciences Research Ethics Review Committee (UMIN000026007 registered on 6 Feb 2017).
Informed Consent Statement
Informed consent was obtained from all participants involved in the study.
Data Availability Statement
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Conflicts of Interest
T.F. and H.T. are employees of Kao Corporation.
References
- Cabinet Office; Government of Japan. Annual Report on the Ageing Society [Summary] FY2020. Available online: https://www8.cao.go.jp/kourei/english/annualreport/2020/pdf/2020.pdf. (accessed on 31 Dec 2022).
- Yokoyama, T. National health promotion measures in Japan: Health Japan 21 (the second term). J Natl Inst Public Health. 2020, 69, 14–24. [Google Scholar]
- Wajchenberg, B.L. Subcutaneous and visceral adipose tissue: Their relation to the metabolic syndrome. Endocr Rev. 2000, 21, 697–738. [Google Scholar] [CrossRef] [PubMed]
- Hiuge-Shimizu, A.; Kishida, K.; Funahashi, T.; Ishizaka, Y.; Oka, R.; Okada, M.; Suzuki, S.; Takaya, N.; Nakagawa, T.; Fukui, T.; et al. Absolute value of visceral fat area measured on computed tomography scans and obesity-related cardiovascular risk factors in large-scale Japanese general population (the VACATION-J study). Ann Med. 2012, 44, 82–92. [Google Scholar] [CrossRef] [PubMed]
- Takase, H.; Sakane, N.; Morimoto, T.; Uchida, T.; Mori, K.; Katashima, M.; Katsuragi, Y. Development of a dietary factor assessment tool for evaluating associations between visceral fat accumulation and major nutrients in Japanese adults. J Obes. 2019, 2019, 9497861. [Google Scholar] [CrossRef] [PubMed]
- Sakane, N.; Osaki, N.; Takase, H.; Suzuki, J.; Suzukamo, C.; Nirengi, S.; Suganuma, A.; Shimotoyodome, A. The study of metabolic improvement by nutritional intervention controlling endogenous GIP (Mini Egg study): a randomized, cross-over study. Nutr J. 2019, 18, 52. [Google Scholar] [CrossRef] [PubMed]
- Kumagai, S.; Watanabe, S.; Shibata, H.; Amano, H.; Fujiwara, Y.; Shinkai, S.; Yoshida, H.; Suzuki, T.; Yukawa, H.; Yasumura, S.; et al. Effects of dietary variety on declines in high-level functional capacity in elderly people living in a community. [Nihon Koshu Eisei Zasshi] Jpn J Public Health. 2003, 50, 1117–1124, (Only abstract in English). [Google Scholar]
- Kobayashi, S.; Asakura, K.; Suga, H.; Sasaki, S.; Three-generation Study of Women on Diets and Health Study Group. High protein intake is associated with low prevalence of frailty among old Japanese women: A multicenter cross-sectional study. Nutr J. 2013, 12, 164. [Google Scholar] [CrossRef] [PubMed]
- Tomata, Y.; Watanabe, T.; Sugawara, Y.; Chou, W.T.; Kakizaki, M.; Tsuji, I. Dietary patterns and incident functional disability in elderly Japanese: The Ohsaki Cohort 2006 Study. J Gerontol A Biol Sci Med Sci. 2014, 69, 843–851. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, A.; Watanabe, T.; Watanabe, R.; Nakaji, K.; Mitsuda, H.; Inoue, S.; Yamaoka, C.; Nishimuta, M.; Miyazaki, H. Actual food group and nutrient intake by independent-living elderly individuals as assessed via meal weighing method—general components, minerals, vitamins, fatty acids, amino acids and carbohydrates. J Integr Study Diet Habits. 2015, 72, 221–229, (Only abstract in English). [Google Scholar]
- Yokoyama, Y.; Kitamura, A.; Seino, S.; Kim, H.; Obuchi, S.; Kawai, H.; Hirano, H.; Watanabe, Y.; Motokawa, K.; Narita, M.; et al. Association of nutrient-derived dietary patterns with sarcopenia and its components in community-dwelling older Japanese: a cross-sectional study. Nutr J. 2021, 20, 7. [Google Scholar] [CrossRef]
- Peduzzi, P.; Concato, J.; Feinstein, A.R.; Holford, T.R. Importance of events per independent variable in proportional hazards regression analysis. II. Accuracy and precision of regression estimates. J Clin Epidemiol. 1995, 48, 1503–1510. [Google Scholar] [CrossRef] [PubMed]
- Fukuhara, S.; Bito, S.; Green, J.; Hsiao, A.; Kurokawa, K. Translation, adaptation, and validation of the SF-36 Health Survey for use in Japan. J Clin Epidemiol. 1998, 51, 1037–1044. [Google Scholar] [CrossRef] [PubMed]
- Granic, A.; Sayer, A.A.; Robinson, S.M. Dietary patterns, skeletal muscle health, and sarcopenia in older adults. Nutrients. 2019, 11, 745. [Google Scholar] [CrossRef] [PubMed]
- Coates, J.; Colaiezzi, B.; Fiedler, J.L.; Wirth, J.; Lividini, K.; Rogers, B. A program needs-driven approach to selecting dietary assessment methods for decision-making in food fortification programs. Food Nutr Bull. 2012, 33(3_suppl), S146–S156. [Google Scholar] [CrossRef] [PubMed]
- Willett, W.; Stampfer, M.J. Total energy intake: Implications for epidemiologic analyses. Am J Epidemiol. 1986, 124, 17–27. [Google Scholar] [CrossRef] [PubMed]
- Kidokoro, T.; Tanaka, H.; Naoi, K.; Ueno, K.; Yanaoka, T.; Kashiwabara, K.; Miyashita, M. Factors associated with achieving physical activity guideline in Japanese adolescents. Jpn J Phys Fit Sports Med. 2016, 65, 383–392. [Google Scholar] [CrossRef]
- Mâsse, L.C.; Fuemmeler, B.F.; Anderson, C.B.; Matthews, C.E.; Trost, S.G.; Catellier, D.J.; Treuth, M. Accelerometer data reduction: a comparison of four reduction algorithms on select outcome variables. Med Sci Sports Exerc. 2005, 37, S544–S554. [Google Scholar] [CrossRef]
- Troiano, R.P.; Berrigan, D.; Dodd, K.W.; Mâsse, L.C.; Tilert, T.; McDowell, M. Physical activity in the United States measured by accelerometer. Med Sci Sports Exerc. 2008, 40, 181–188. [Google Scholar] [CrossRef]
- Kumahara, H.; Schutz, Y.; Ayabe, M.; Yoshioka, M.; Yoshitake, Y.; Shindo, M.; Ishii, K.; Tanaka, H. The use of uniaxial accelerometry for the assessment of physical-activity-related energy expenditure: a validation study against whole-body indirect calorimetry. Br J Nutr. 2004, 91, 235–243. [Google Scholar] [CrossRef]
- Seichi, A.; Hoshino, Y.; Doi, T.; Akai, M.; Tobimatsu, Y.; Iwaya, T. Development of a screening tool for risk of locomotive syndrome in the elderly: the 25-question Geriatric Locomotive Function Scale. J Orthop Sci. 2012, 17, 163–172. [Google Scholar] [CrossRef]
- Muranaga, S.; Hirano, K. Development of a convenient way to predict ability to walk, using a two-step test. J Showa Med Assoc. 2003, 63, 301–308, (Only abstract in English). [Google Scholar]
- Muranaga, S. Evaluation of the muscular strength of the lower extremities using the standing movement and clinical application. J Showa Med Assoc. 2001, 61, 362–367, (Only abstract in English). [Google Scholar]
- Kobayashi, K.; Hiiragi, Y.; Maruyama, H. Development of the “10-second open-close stepping test” (OCS-10) and fundamental study of its measurement values through a comparison of healthy young people and community-dwelling elderly. J Phys Ther Sci. 2012, 24, 747–749. [Google Scholar] [CrossRef]
- Ministry of Education, Culture, Sports, Science and Technology. New physical fitness tests. Available online: https://www.mext.go.jp/a_menu/sports/stamina/03040901.htm (accessed on 31 Dec 2022). (in Japanese).
- Duncan, P.W.; Weiner, D.K.; Chandler, J.; Studenski, S. Functional reach: a new clinical measure of balance. J Gerontol. 1990, 45, M192–M197. [Google Scholar] [CrossRef] [PubMed]
- Podsiadlo, D.; Richardson, S. The timed “UP & Go”: a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc. 1991, 39, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Boulgarides, L.K.; McGinty, S.M.; Willett, J.A.; Barnes, C.W. Use of clinical and impairment-based tests to predict falls by community-dwelling older adults. Phys Ther. 2003, 83, 328–339. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health Labour and Welfare. National health and nutrition survey 2017. Available online: https://www.mhlw.go.jp/content/000451760.pdf (accessed on 31 Dec 2022). (in Japanese).
- Arai, H.; Yamamoto, A.; Matsuzawa, Y.; Saito, Y.; Yamada, N.; Oikawa, S.; Mabuchi, H.; Teramoto, T.; Sasaki, J.; Nakaya, N.; et al. Prevalence of metabolic syndrome in the general Japanese population in 2000. J Atheroscler Thromb. 2006, 13, 202–208. [Google Scholar] [CrossRef] [PubMed]
- Vagetti, G.C.; Barbosa Filho, V.C.; Moreira, N.B.; Oliveira, Vd; Mazzardo, O. ; Campos, Wd. Association between physical activity and quality of life in the elderly: a systematic review, 2000–2012. Braz J Psychiatry. 2014, 36, 76–88. [Google Scholar] [CrossRef] [PubMed]
- Morie, M.; Reid, K.F.; Miciek, R.; Lajevardi, N.; Choong, K.; Krasnoff, J.B.; Storer, T.W.; Fielding, R.A.; Bhasin, S.; Lebrasseur, N.K. Habitual physical activity levels are associated with performance in measures of physical function and mobility in older men. J Am Geriatr Soc. 2010, 58, 1727–1733. [Google Scholar] [CrossRef]
- Bohl, C.H.; Volpe, S.L. Magnesium and exercise. Crit Rev Food Sci Nutr. 2002, 42, 533–563. [Google Scholar] [CrossRef]
- Veronese, N.; Berton, L.; Carraro, S.; Bolzetta, F.; De Rui, M.D.; Perissinotto, E.; Toffanello, E.D.; Bano, G.; Pizzato, S.; Miotto, F.; et al. Effect of oral magnesium supplementation on physical performance in healthy elderly women involved in a weekly exercise program: a randomized controlled trial. Am J Clin Nutr. 2014, 100, 974–981. [Google Scholar] [CrossRef] [PubMed]
- Struijk, E.A.; Lana, A.; Guallar-Castillón, P.; Rodríguez-Artalejo, F.; Lopez-Garcia, E. Intake of B vitamins and impairment in physical function in older adults. Clin Nutr. 2018, 37, 1271–1278. [Google Scholar] [CrossRef] [PubMed]
- Mendonça, N.; Hill, T.R.; Granic, A.; Davies, K.; Collerton, J.; Mathers, J.C.; Siervo, M.; Wrieden, W.L.; Seal, C.J.; Kirkwood, T.B.L.; et al. Micronutrient intake and food sources in the very old: analysis of the Newcastle 85+ Study. Br J Nutr. 2016, 116, 751–761. [Google Scholar] [CrossRef]
- Dukas, L.; Willett, W.C.; Giovannucci, E.L. Association between physical activity, fiber intake, and other lifestyle variables and constipation in a study of women. Am J Gastroenterol. 2003, 98, 1790–1796. [Google Scholar] [CrossRef] [PubMed]
- Adams, S.; Sello, C.T.; Qin, G.X.; Che, D.; Han, R. Does dietary fiber affect the levels of nutritional components after feed formulation? Fibers. 2018, 6, 29. [Google Scholar] [CrossRef]
Figure 1.
Flow chart of participants.

Table 1.
Physiological characteristics of the older Japanese adults living in urban areas
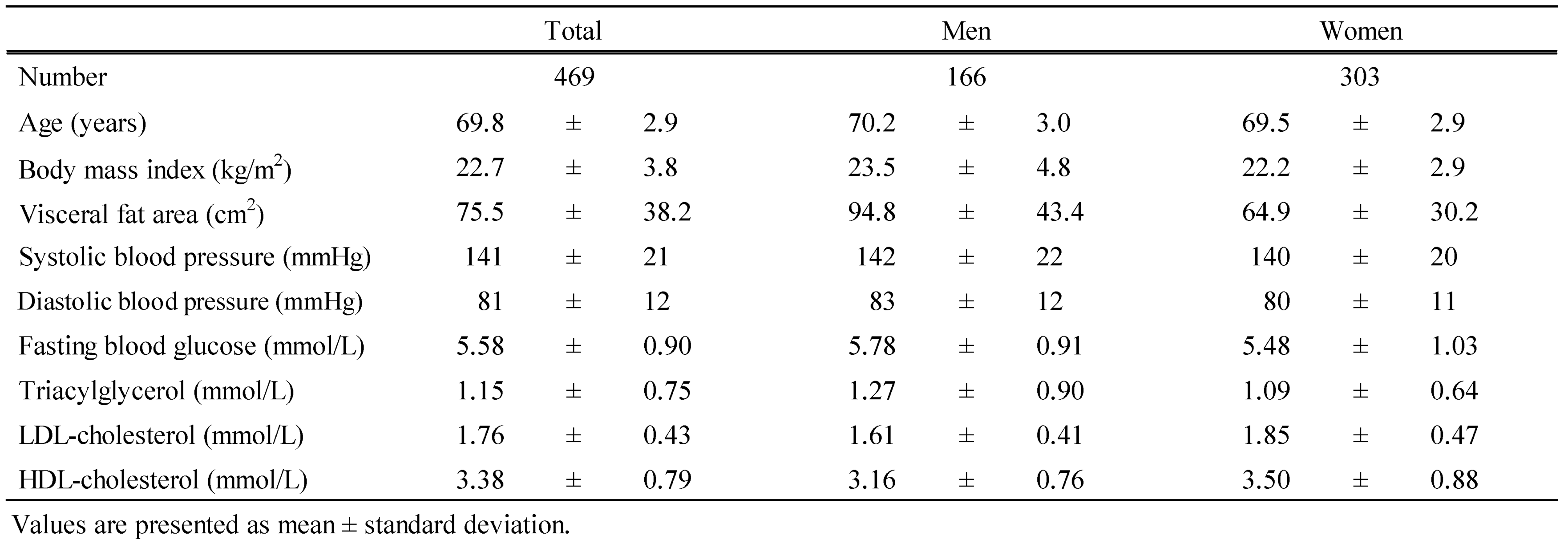 |
Table 2.
Comparison of physical functions between subjects with the national average
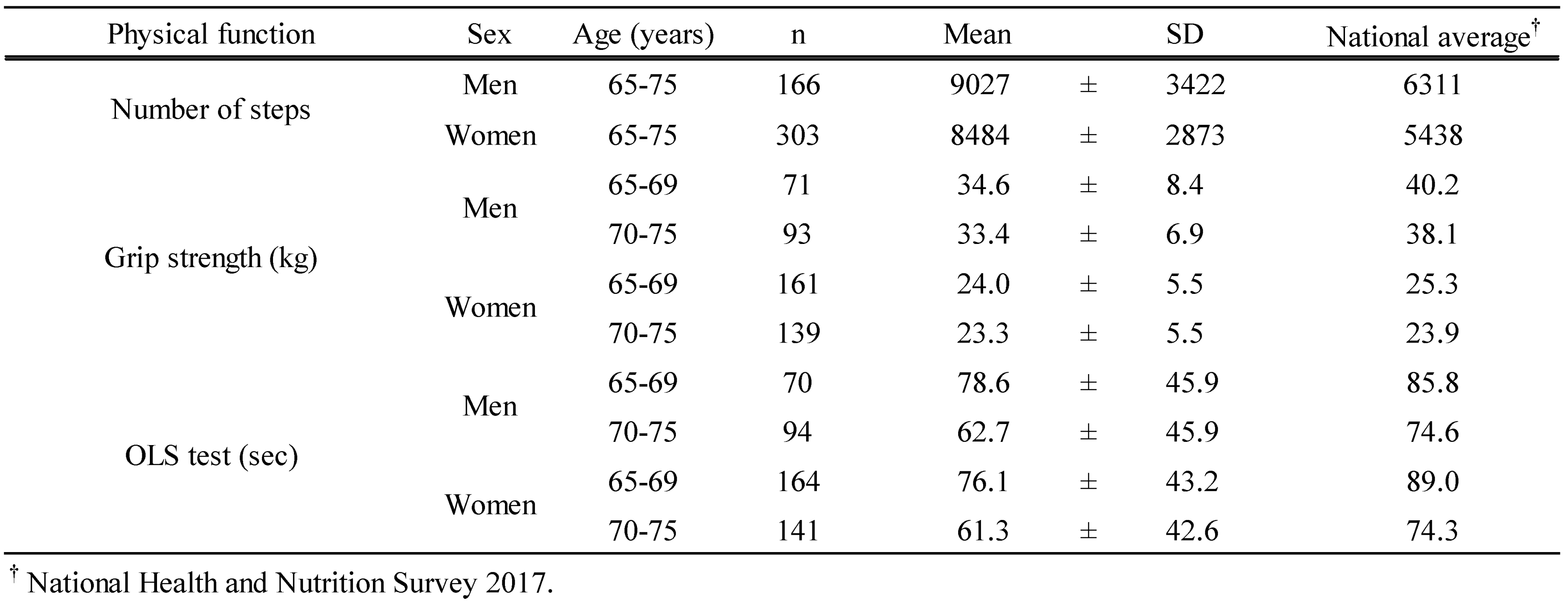 |
Table 3.
Results from multiple linear regression models adjusted for sex, age, and body mass index examining the association of QOLs with physical activities †
Table 3.
Results from multiple linear regression models adjusted for sex, age, and body mass index examining the association of QOLs with physical activities †
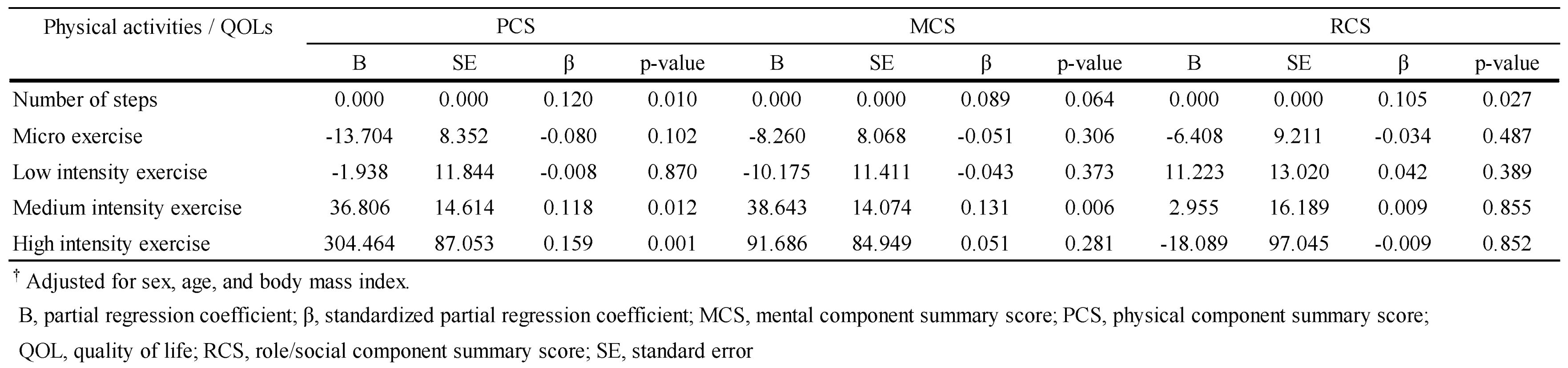 |
Table 4.
Results from multiple linear regression models adjusted for sex, age, and body mass index examining the association of physical activities with physical functions †.
Table 4.
Results from multiple linear regression models adjusted for sex, age, and body mass index examining the association of physical activities with physical functions †.
 |
Table 5.
Results from multiple linear regression models adjusted for sex, age, and body mass index examining the association of physical functions with food intake †
Table 5.
Results from multiple linear regression models adjusted for sex, age, and body mass index examining the association of physical functions with food intake †
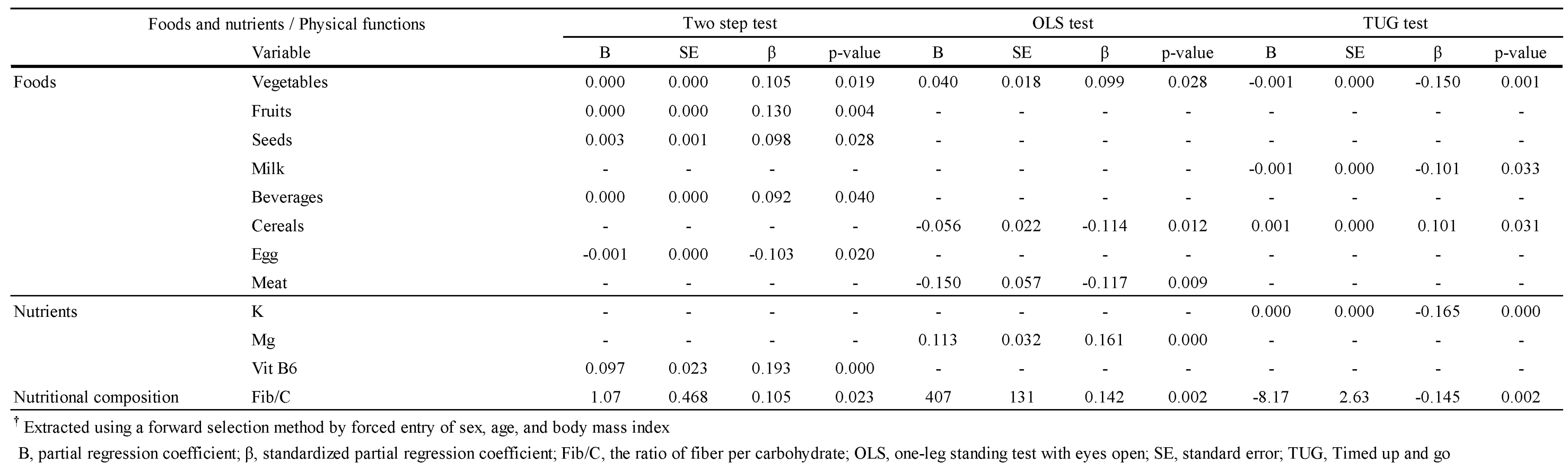 |
Table 6.
Results from multiple linear regression models adjusted for sex, age, and body mass index examining the association of serum Mg concentration with Mg intake, total fiber intake and Fib/C ratio †.
Table 6.
Results from multiple linear regression models adjusted for sex, age, and body mass index examining the association of serum Mg concentration with Mg intake, total fiber intake and Fib/C ratio †.
 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



