
Submitted:
08 January 2023
Posted:
10 January 2023
You are already at the latest version
Abstract
The objective of this quantitative study was to examine the impact of selected factors on the level and state of public health in local self-government units in 2021, with the consideration of data from 2020 and 2019. This survey included 77 out of 145 local self-government units in the Republic of Serbia and examined six dimensions defined by the Law on Public Health: social care for the public health of the city/municipality in regard to the physical, mental, and social health of the population; health promotion and disease prevention; the environment and health; working environments and population health; the organization and functioning of the health system; and actions in emergency situations. The results of the Pearson correlation showed that there were statistically significant correlations between the effectiveness of the realized program budget and microbiologically defective drinking water samples from the so-called village water supply systems, defective samples of drinking water from public taps, unsatisfactory analyses of wastewater samples, the total number of air samples on an annual level for PM25s, and the number of mandated fines issued. The results of the logistic regression model showed that the local self-government units that received assistance from the Permanent Conference of Cities and Municipalities were 5.6 times more likely to perform analyses of their health status. Furthermore, we determined that the units of local self-governments that appointed a coordinator of the health council identified vulnerable groups in the analysis of the state of health four and a half times more often. In contrast, the units of local self-governments that prepared health status analyses could be used to identify vulnerable groups to a six times greater extent within the framework of the health status analysis. The results showed that in improving the state of public health at the local level, it is necessary to provide systematic institutional support to cities and municipalities in exercising their responsibilities. Based on these results, recommendations were made for the further development of support, i.e., the planning of further activities aimed at strengthening the capacity of the health councils and local self-government units in this area.
Keywords:
public health
; local self-government
; institutional support
; longitudinal research
; Serbia
1. Introduction
The health of the nation is the most valuable resource of any country and is essential for the sustainable economic and social development of every individual, family, and community [1,2,3]. Provided through the coordinated efforts and well-informed decisions made by societies, organizations (both public and private), communities, and people, public health refers to the science and art of avoiding disease, extending life, and promoting health [4,5]. The goals of public health are aimed at prolonging life and improving health through the organized efforts of society and providing conditions in which people can be healthy, and these goals are primarily aimed at the population as a whole [6]. Creating resilient, adaptable communities and supportive environments is one of the goals of the “Health 2020” police framework developed by the World Health Organization (WHO), of which Serbia is also a signatory. Resilient communities are those that react proactively to new or unwanted situations; prepare for economic, social, and environmental changes; and cope well with crises and difficulties [7,8]. Health promotion and disease prevention include the adoption, implementation, and evaluation of health promotion programs in cooperation with public health actors in the community, based on risk analysis and the health needs of the population [9]. Health education and promotion in the community are carried out through campaigns promoting healthy lifestyles and preservation and improvement of the environment and the work environment [10,11,12], as well as advocacy for organizational changes in the environment and the creation of an environment that supports healthy choices [13,14,15,16,17].
In Serbia, health councils are responsible for providing social care for public health at the level of local self-government units according to the Law on Public Health (“Official Gazette of the RS”, No. 15/16) and the Law on Patients’ Rights (“Official Gazette of the RS”, No. 45/13). The intersectoral composition of the council enables a comprehensive approach to meeting health needs, supported by a wide network of partners at the local community level. Through its advisory role, the council provides support in the process of strategic planning, the selection of priorities for financing programs related to health in the local community, as well as the coordination of the activities of other services and administrations of local self-government units related to health (communal activities, education, social protection, environment, sport, traffic, youth office, employment, urban planning, etc.). The Law on Health Care (“Official Gazette of RS”, No. 25/19, article 13) prescribes the competencies of local self-government units, and the founding rights have been returned to the Republic of Serbia. The monitoring and analysis of capacities and resources in the health system (personnel, equipment, space), the financing of healthcare, the coverage of the population with regard to health services, as well as ensuring the implementation of established priorities in healthcare in the territories of local self-government units are the responsibilities of the health councils and advisers for the protection of the rights of patients. According to the abovementioned law, the areas of action in regard to public health are (1) the physical, mental, and social health of the population; (2) health promotion and disease prevention; (3) environment and population health; (4) working environment and population health; (5) the organization and functioning of the healthcare system; (6) the handling of crisis and emergency situations.
The Standing Conference of Towns and Municipalities implemented a series of activities aimed at achieving the key interests of local self-governments, which are defined in the strategic and program documents of the Standing Conference of Towns and Municipalities, as well as through the actions of its organs and bodies. Given that this is a continuous process, it is necessary to continuously monitor the situation on the ground, and adjust the methods and scope of support provided to local self-government units in this area according to the assessed situation. One of the activities carried out as part of this monitoring process is the analysis of the state of public health at the local level, which is conducted using an electronic database containing information on the implementation of the responsibilities of local self-government units in the field of public health. In this study, we analyzed the situation in the areas of public health at the local level in 2021 and performed a comparative analysis with the situation in 2019–2021, as well as the implementation of the competences of local self-government units in the areas of public health.
The first assessment of the state of public health in local self-government units was conducted during the period of January–May 2020 for 2019. The analysis of the state of public health at the local level for 2019 provided the starting point for the regular monitoring and evaluation of indicators in the field of public health and health improvement at the local level.
Literature Review
The major challenges involved in analyzing the field of public health include the emphasis on populations rather than individuals, multi-component interventions, qualitative as well as quantitative approaches, the emphasis on implementation processes, and the complexity and long-term nature of interventions and outcomes [18]. Public health interventions [18,19,20] are highly cost-saving and cuts to public health budgets in high-income countries generate billions of pounds’ worth of additional costs to health services and the wider economy [21]. State policymakers and taxpayers continue to have serious concerns about the rising cost of healthcare [22]. The United States spent about one-fifth of its GDP, or USD 3 trillion, on its healthcare system in 2013, which was by far the highest amount spent by any country [23]. Around the world, various public health interventions are being implemented, including smoking cessation programs [24], home blood-pressure monitoring for the diagnosis and treatment of hypertension [25], workplace health promotion for firefighters [26], health promotion programs for hospital staff [27], the implementation of speed cameras in urban settings [28], intensive early education programs for socioeconomically deprived families [29], social service interventions [30,31], and income support services for older adults [32].
Wilkinson and Pickett [33] found that people’s health was better in countries with less inequality in incomes. Furthermore, Lewis [34] found that good governance is important in ensuring effective healthcare delivery, and that returns to investments in health are low in cases where governance issues are not addressed. Bara, Van den Heuvel [35] suggest that future reforms in Romania should encourage the free choice of physicians, the autonomy of the primary healthcare system, and increasing financial resources for the healthcare system. China needs to reorganize its public health system and the demand side of the public health system, particularly in regard to reducing the financial barriers to public health services [36]. Kawachi [37] found that better social engagement, collective efficacy, and trust are associated with better health outcomes. In a 2003 poll conducted in Germany, 89 percent of participants reported being in good health, with 10 percent reporting a sickness and 1 percent reporting an accident-related injury. Ninety-three percent of young children were deemed healthy. The proportion of healthy persons was highest among those between the ages of 10 and 20 (96%) and lowest among those between the ages of 60 and 75 (72%), who also had the highest proportion of sick (27%) and damaged (1.1%) people, respectively, as well as injured people (1.1%) [38]. In Italy, the majority of national and local taxes (97%) and patient co-payments go toward funding public healthcare. Private spending in 2001 was 21.4 billion euros, or 2.1 percent of GDP, and was mostly funded by personal funds. The majority of ambulatory specialist treatments and private hospital care for childbirth and minor surgery were covered by the 15% of Italians who have private health insurance [39].
For professionals such as nurses, doctors, dietitians, educators, and social workers, public health program designers and practitioners must offer training across sectors. They also need to check public health mass communication messages for stereotyping, blaming, and inaccuracy [40]. Anugwom [41] found that effective legislation, substantial funding, gender inclusivity, increased research, the assessment and evaluation of routine needs, the setting of needs-driven priorities, and the development of the capacity of health promotions to target marginalized and vulnerable members of society are just a few of the ways that health promotion in the continent can be strengthened. A more widespread adoption of evidence-based tactics has been advised in order to accomplish state and national goals for improved population health [42,43,44]. The development of healthy public policies, requirements to ensure that environments are supportive of health, the significance of personal skills, community action, and the challenge of reorienting health services are five key action areas that mutually reinforce one another with the aim of improving the health of populations [45]. Prevention campaigns should systematically incorporate and respond to the existing beliefs and emotions of at-risk populations, as well as the perceived barriers in the message design process, to effectively promote changes in behavior [46,47].
The objective of this study was to examine the state of public health in local self-government units, that is, to carry out assessments of the built capacities of public health actors in the community. Apart from this basic objective, in this work we had the following additional objectives.
- − This research will serve the Ministry of Health by providing a “baseline” for the regular monitoring and evaluation of indicators in the field of public health and health improvement at the local level, as well as the capacity of cities and municipalities to implement their responsibilities.
- − We aimed to test the electronic data collection model as a regular tool for monitoring and evaluating health improvement at the local level;
- − To create an electronic database for the monitoring of the effects of public health programs in all areas of public health during future periods/years, with the ability to monitor data for local self-government units and as a whole;
- − To test the selected indicators for each area of public health as parameters for monitoring the effects of the activities undertaken by various actors in local self-government units;
- − To evaluate the effects of the past activities in strengthening the capacities of local self-government units in the field of public health and in mapping their future activities;
- − To evaluate the cooperation of health councils and public health institutes, as well as other partners and actors related to public health in the community;
- − To propose measures and recommendations for the targeting of support, that is, planning further activities aimed at strengthening the capacity of the health council and local self-government units in general in this area, based on observations about what type of support local self-government units recognize as the most necessary; and
- − To make proposals to improve the tools used to collect and process sub-data.
2. Materials and Methods
This study was an examination of the impact of selected factors on the level and state of public health in local self-government units in 2021, with the consideration of data from 2020 and 2019. The goal of this scientific study was to provide a scientific explanation of the way in which these factors influenced the state of public health in local self-government units. On the basis of the research conducted, we have made recommendations for the further development of support, i.e., planning further activities aimed at strengthening the capacity of the health council and the local self-government units in general in this area, based on observations of what type of support the local self-government units recognized as the most necessary. We have also made a proposal for the improvement of the very tools that were used to collect and process the data. The social implications of the research are reflected in the creation of preconditions for the improvement of public health at the local level.
2.1. Study Area
This survey included 77 local governments in the Republic of Serbia (Figure 1): Ada (78), Aleksinac (113), Aranđelovac (55), Bač (144), Bačka Palanka (145), Batočina (125), Bečej (74), Beograd (145,146,147), Blace (97), Boljevac (117), Bor (178), Bujanovac (167), Ćićevac (103), Dimitrovgrad (173), Gadžin Han (121), Inđija (73), Ivanjica (9), Kanjiža (188), Kragujevac (57), Kruševac (102), Kula (37), Kuršumlija (95), Lajkovac (41), Lapovo (123), Mali Iđoš (39), Malo Crniće (133), Medveđa (92), Niš (112), Nova Varoš (1), Novi Bečej (77), Novi Pazar (13), Novi Sad (34), Odžaci (143), Bojnik (106), Pećinci (46), Plandište (181), Požarevac (131), Ražanj (114), Šabac (27), Smederevo (70), Smederevska Palanka (60), Sokobanja (116), Sombor (141), Srbobran (36), Subotica (189), Topola (54), Trstenik (99), Ub (42), Užice (152), Varvarin (104), Velika Plana (127), Veliko Gradište (134), Zrenjanin (80), Bela Crkva (179), Vladičin Han (119), Zaječar (175), Kikinda (185), Kosjerić (24), Ljubovija (190), Opovo (69), Paraćin (115), Ruma (29), Svilajnac (128), Smederevo (70), Titel (76), and Šid (146). In terms of regions, local self-governments from Vojvodina (32.5%) and Šumadija and Western Serbia (32.5%) participated the most, and those from Belgrade participated the least (7.8%) (Figure 1). A complete table of all Serbian municipalities (with IDs) is shown in the Supplementary Materials.
2.2. Sample
In terms of regions, the study covered 32.6% of local self-governments from Vojvodina, 32.4% from Šumadija, 27.3% from Southern and Eastern Serbia, and 7.8% from Belgrade. Table 1 shows the cities and municipalities that submitted questionnaires in electronic form by region.
The degree of development of local self-government units is an important indicator of the economic development of municipalities. It is determined by applying basic and corrective indicators. The basic indicator is the sum of the total amount of wages and pensions in the local self-government units and the budget income of the local self-government units, expressed per capita, after excluding the funds received from other bodies in order to eliminate the consequences of extraordinary circumstances. Corrective indicators are demographic decline or growth, the unemployment rate and the level of education. On the basis of the regulation regarding the establishment of a unified list reflecting the development of regions and local self-government units, they were classified into four groups.
- Group I consisted of local self-government units of which the level of development was above the national average.
- Group II consisted of local self-government units of which the level of development was in the range of 80% to 100% of the national average.
- Group III consisted of insufficiently developed local self-government units of which the level of development was in the range of 60% to 80% of the national average.
- Group IV consisted of extremely underdeveloped local self-government units of which the level of development was below 60% of the national average. Within this group were local self-government units classified as devastated areas, of which the level of development was below 50% of the national average. In relation to development, the survey included the highest number of local self-government units from category III (32.5%), then from category II (23.4%), and an equal number from categories I and IV (22.1%) (Figure 2).
Concerning the functional role of the person who filled out the questionnaire, the majority were Heads of the OU/GU (41.6%), followed by heads of departments (13%), heads of the Administration for Social Activities (6.5%), city administration employees (4.2%) and council members (2.6%). In the process of filling out the questionnaire, other functional roles were also reported (coordinator of the health council; employees on the legalization of facilities; presidents of the assembly and the health council, an associate in the field of public health, a social and healthcare advisor, an advisor for the protection of patients’ rights, an advisor for environmental protection and ecology, the head of the department for social activities, head of the department for the protection of veterans/disabled people, head of the department for social activities, etc.). In relation to the number of employees in local self-government units, the sample mostly included units with 31 to 60 employees (32.5%), followed those with more than 131 (27.3%), those with 61 to 100 employees (19.5%), and those with 1–30 and 101–130 employees (10.4%). Individually, most respondents were employed in the municipality of Novi Sad (1395).
2.3. Questionnaire Design
In order to realize the research objectives, a survey questionnaire entitled State of public health at the local level for the year 2021 was used. It is important to point out that previous versions of the questionnaire were used in research on the state of public health at the local level in the period from 2019 to 2020. Before the study was carried out, a group of experts analyzed all the questions in detail and made suggestions for its improvement in accordance with changes in the socio-economic and political environment, as well as recommendations for improving the questionnaire on the basis of previous research. The questionnaire consisted of a general and a special part, with six units:
(a) Basic data on local self-government units (5 questions);
(b) Social care for the public health of the city/municipality regarding the physical, mental, and social health of the population (27 questions);
(v) Social care for the public health of the city/municipality in the area of health promotion and disease prevention in 2021 (6 questions);
(g) Social care for the public health of the city/municipality in the field of the environment and health in 2021 (42 questions);
(d) Social care for the public health of the city/municipality in the area of working environments and population health in 2021 (6 questions);
(f) Social care for the public health of the city/municipality in relation to the organization and functioning of the health system (15 questions);
(e) Social care for the public health of the city/municipality in the field of dealing with emergency and crisis situations (15 questions) and two final questions related to the necessary engagement of the Union of Towns and Municipalities of Serbia by the surveyed local self-government units and the assessment of their cooperation so far.
The State of public health at the local level for the year 2021 questionnaire was constructed in such a way as to include all areas of public health based on the available knowledge concerning the previous activities of local self-government units in the process of assuming responsibility, as well as taking into account the capacities of local self-government units. The questionnaire primarily dealt with health councils and their development, as well as the monitoring of activities in the previous period. The structured questionnaire was developed using closed-ended five-point Likert scale questions (where 1 indicates strong disagreement and 5 indicates strong agreement). Based on the consensus of the expert team, additional data for analysis were obtained from the official databases of the Institute of Statistics of the Republic of Serbia (demographic statistics for the year 2020), from IJZS “Dr. Milan Jovanović Batut” (health statistics for the year 2020), and from the Decision on local self-government units budgets database (2019–2022). In this way, a large number of questions were avoided, and we ensured that the same source of data was used according to the same methodology, as well as the same cut-off year. A questionnaire, created and placed in Google Forms, was used as a tool.
With the support of SCTM and the Ministry of Health, a joint letter of invitation was drawn up for the representatives of municipalities and cities to participate in the third research in the series. SCTM invited all municipalities and cities via e-mail to participate in the survey on the state of public health in the Republic of Serbia. An invitation letter, instructions for filling in the questionnaire, a link to the questionnaire in electronic form, a Word version of the questionnaire, and the deadline for the submission of answers (April 22) were sent via e-mail. We suggested that the person filling out the questionnaire should be the head of the city/municipal administration. The study did not include local self-government units from the regions of Kosovo or Metohija. The e-mail also contained the contacts of people for professional support regarding the content of the questionnaire and the process of completing the questionnaire electronically.
In the instructions, it is proposed that different administrations/services or departments should participate in filling out the questionnaire. The part of the questionnaire related to social care for public health in relation to the physical, mental, and social health of the population and social care for public health in relation to health promotion and disease prevention should be filled in by employees of social services, health or health advice professionals. The part of the questionnaire related to social concern for public health in the field of the environment should be filled out by employees of environmental services and communal activities. The part of the questionnaire related to social concern for public health in relation to working environments should be filled out by employees of occupational health and safety services and inspection services. The part of the questionnaire related to social care for public health in relation to the organization and functioning of the health system should filled out by employees who work in relation to health and social activities. Finally, the part of the questionnaire related to social care for public health in the area of dealing with emergency and crisis situations should be filled out by employees who work in relation to social and health activities and the Headquarters for Emergency Situations. The research protocol was approved by the committees of the Institutional Review Board, University of Belgrade, the Institutional Review Board of Scientific-Professional Society for Disaster Risk Management, and the International Institute for Disaster Research (protocol code 002/2021, 14 March 2022).
2.4. Analyses
In the program for statistical data processing (SPSS), all the data obtained from the survey were sorted and classified. Using descriptive statistical analysis, the distributions of answers to the questions were determined. In the logical regression model, five independent variables were used (formed council, appointed coordinator, public health plan, received assistance from the Standing Conference of Towns and Municipalities, and having a rights protection advisor) that had statistical significance (p < 0.05). For more detailed analyses, T-tests, Pearson’s correlation, and chi-squared tests were used. The assumptions underlying the analyses, such as the assumption of normality, linearity, multicollinearity and homogeneity of variance, were not violated [48]. Additional data sets from the Institute for Statistics of the Republic of Serbia were used to test the correct selection of public health program priorities in local governments, as well as to examine the availability of healthcare. The mentioned statistical analysis was performed using IBM SPSS Statistics, Version 26. Previous investigations of the residual scattering diagram revealed that the assumptions of normality (normal probability P-P plot and scatterplot), linearity, multicollinearity (r = 0.81), and variance homogeneity were not violated. The internal consistency of Likert scales was good, with a Cronbach’s alpha of 0.82.
3. Results and Discussion
The study’s findings are presented in relation to the following dimensions.
-
Results of descriptive statistical analyses:
- (a) Social care for the public health of the city/municipality in relation to the physical, mental, and social health of the population;
- (b) Social care for the public health of the city/municipality in relation to health promotion and disease prevention in 2021 (social activities and health);
- (v) Social care for the public health of the city/municipality in relation to the environment and health in 2021 (environment, communal activities);
- (g) Social care for the public health of the city/municipality in relation to working environments and population health in 2021 (safety and health at work, inspection work);
- (d) Social concern for the public health of the city/municipality in relation to the organization and functioning of the health system (healthcare, social activity);
- (đ) Social care for the public health of the city/municipality in relation to dealing with emergency situations (social activities, health, Headquarters for Emergency Situations);
- 2.
- Correlation analyses of variables affecting public health in Serbia;
- 3.
- Predictors of the state of public health in Serbia.
- 1.
- Results of descriptive statistical analyses
(a) Social care for the public health of the city/municipality in relation to the physical, mental, and social health of the population
Our analysis showed that most local self-government units had a local action plan for youth (49.4%), followed by a slightly lower proportion having a local action plan for Roma and the City/Municipal Social Protection Strategy (42.9%) and the third-highest proportion of units having a local action plan for waste management 40.3%. A small proportion (1.3%) of local self-government units had a local action plan for the prevention of HIV/AIDS, the improvement of mental health, and preventing the abuse of psychoactive substances (Table 2).
A comparative analysis of the strategic documents adopted at the local self-government unit level (strategies, plans, and local action plans) with the previous two years of research showed an increase in the participation of local self-government units with the increased adoption of the following planning documents: public health plans, local action plans for Roma, social protection strategies and programs, and local action plans for the disabled (Table 3).
In further analyses, we determined that over 61.5% of local self-government units committed over 95% of their planned budgets for program activities in the field of public health, whereas 10.3% committed up to 70% (Table 4).
(b) Social care for the public health of the city/municipality in relation to health promotion and disease prevention in 2021 (social activities and health)
The second segment of the questionnaire included questions related to social care for the public health of the city/municipality in the domain of health promotion and disease prevention in 2021 (social activities and health). The results of the examination of the extent of local self-government units’ participation in public health promotion campaigns indicated that a relatively high level of participation (74%) has been realized so far. In the framework of public health promotion campaigns, Health Centers (89.7%) and Civil Society Organizations (63.8%) appeared as partners to the greatest extent. In addition, the roles of partners in these campaigns were assumed by the competent institutes for public health (34.5%), hospitals (15.5%), the Red Cross (10.2%), and IJZS Batut (6.9%). The implemented campaigns/promotions were mostly conducted in the domains of preventive examinations (77.6%) and immunization (63.8%), followed by screening examinations (55.2%), the prevention of infectious diseases (48.3%), smoking reduction (43.1%), physical activities (39.7%), violence prevention (41.4%), reproductive health (39.7%), prevention of the abuse of psychoactive substances (32.8%), breastfeeding (31%), and nutrition (29.3%). Mental health promotion campaigns were implemented to the smallest extent (24.1%) (Table 5).
In terms of the ways in which local self-government units participate in the abovementioned campaigns/promotions, we identified providing space (65.3%), participation through media support (64%), and personal participation by the representatives of local self-government units (57.3%) as the leading forms of participation. In addition, printing materials (21.3%) was identified as a way of participating in campaigns, and transportation (10.7%) and daily wages (2.7%) were reported to a lesser degree. Furthermore, in 42 local self-governments (54.5%), during COVID-19, cooperation between the council and the Headquarters for Emergency Situations was realized, which was manifested to the greatest extent in the area of population information (65.2%); immunization organization (58.7%); cooperation with the Red Cross (56.5%); and assistance in the procurement, storage, or distribution of protective equipment (34.8%). With a much smaller percentage, the council’s cooperation with the Headquarters was achieved through contact with donors (8.7%), participation in the recruitment of volunteers (23.9%), and the attendance of representatives of the Headquarters at the council to provide recommendations regarding pest control in the city (2.2%) (Table 5).
We observed a decline in the participation of local self-government units in campaigns promoting healthy lifestyles during the observed three years (Figure 3). Nevertheless, the surveyed local self-government units strengthened their cooperation with health centers, civil society organizations, and the competent institutions for public health in their activities related to the promotion of healthy lifestyles (Figure 4).
Compared to the previous year, the campaigns were on a larger scale for all topics except the abuse of psychoactive substances (Figure 5).
Health councils and local self-government units supported partners in implementing health promotion activities in the community somewhat more modestly compared to the previous year.
(v) Social care for the public health of the city/municipality in the field of the environment and health in 2021 (environment, communal activities)
When analyzing social concern for the public health of the city/municipality in the area of the environment and health in 2021 (environment, communal activities), we determined that in a large number of local governments (57.6%) no analyses of environmental indicators were available. Furthermore, for 88.3% of local governments, the health council did not issue proposals for improving the environment. Furthermore, several local self-government units reported having a drinking water factory and a water treatment plant (57.1%); sanitary protection zones for water supply sources (77.9%); constructed maps/schemes of the water supply system, sources and distribution networks (66.2%); and having a Water Network Reconstruction Plan (72.7%). In contrast, 66.2% of local governments did not report owning a wastewater treatment plant (Table 10).
For a large number of local governments, asbestos pipes were not present in the water supply network (64.9%), nor were lead pipes (89.6%). Concerning the control of drinking water samples from so-called rural water supply systems (small water supply systems that supplied more than five households in rural areas), our analyses indicated that 43 local governments (55.8%) reported regularly implementing control measures, whereas for 34 local governments (44.4%) this is not the case. A similar situation was observed with regard to the control of samples for drinking from public fountains with their own source of water, such as captured springs and drilled and artesian wells. At the same time, the volume of microbiologically defective drinking water samples from the JKP/JP water supply system was 4.48%, with physico-chemically defective drinking water samples from the JKP/JP water supply system (18.39%) and village water supply systems (16.28%) being the most frequently represented. In addition, microbiologically defective drinking water samples from rural water supply systems were reported for 6.36% of self-government units, microbiologically defective drinking water samples from public taps with their own source of water for 9.3%, physicochemically defective drinking water samples from public fountains with their own source of water for 10.89%, physico-chemically defective drinking water samples from rural schools for 11.53%, along with microbiologically defective water samples for drinking from village schools. Unsatisfactory analyses of wastewater samples in the territories of local self-governments were recorded for 28.65% of self-government units (Table 10).
Furthermore, a register of septic tanks and collection tanks was established in only four out of the total of 77 local communities included in the sample. Regarding air quality, it was reported that control was carried out by 65 (45.5%) local governments, and local air quality monitoring networks were present to the greatest extent (26%). The most common of these consisted of measuring stations for the monitoring of sulfur dioxide and soot concentrations. Furthermore, at the level of local self-government units, the total number of permanent meters for monitoring nitrogen dioxide levels was 0.34 on average, for the measurement of suspended PM10–0.21 and PM25–0.19 particles. From all permanent measuring stations, an average of 114 SO2 samples, 109 soot samples, 117 NO2 samples, 104 PM10 samples, and 49.36 PM25 samples were collected annually within the local self-government units. The total number of days in a year when the concentrations of measured pollutants in the air were higher than the permitted amount is 2.66 for sulfur dioxide, 5.70 for soot, 2.97 for nitrogen dioxide, 11.42 for PM10 particles, and 8.41 for PM25 particles. During 2021, an average of 25.09% of individual solid fuel burning stoves, which are one of the leading polluters, were extinguished, whereas, during the same year, afforestation was carried out on an area of 10,346 hectares within the local self-government units. Studies in the field of climate change and environmental protection have for decades appealed to the primary role of the government in encouraging the implementation of various measures involving renewable energy (Table 10).
The results of this study indicate that during 2021, in 19 local communities (25.3%), subsidies were adopted for the thermal insulation of public buildings (schools, kindergartens, cultural institutions, sports facilities, etc.); 31 local communities (41.3%) adopted subsidies for the thermal insulation of residential buildings, 24 local communities (32%) adopted subsidies for gas/pellet boiler houses; and 6 local communities (8%) highlighted the construction of traffic bypasses as incentive measures for renewable energy sources. The procurement of electric vehicles for public transport was not implemented in any of the investigated local self-government units. The largest number of local communities (72.7%) reported having a municipal waste dump on their territory, which was located more than 1000 m (48.1%) from the settlement, i.e., residential buildings. In 2021, the total number of landfills among local self-government units was 9.05 on average.
In addition to the anaerobic digestion of organic matter and recycling, sanitary landfills/bioreactor landfills are used in developed countries, which are accompanied by a lower risk of environmental pollution compared to the usual types of landfill. Among the examined local government units, the total number of sanitary landfills in 2021 was 0.31 on average, whereas the number of wild controlled landfills was many times higher (11.68), as well as the number of wild uncontrolled landfills, which was on average 10.32. Estimates indicate that there are about 10 sanitary landfills and over 120 municipal landfills at the national level, which do not even meet the minimum standards in terms of environmental protection, whereas the number of illegal landfills in the immediate vicinity of settlements and watercourses is over 2170. Septic and collection pits that are regularly emptied in a professional manner, that is, by licensed companies on the territory of local self-government units were reported by 9.41% of units. The results then indicated that 80.5% of local communities carried out disinfection, disinsection, and pest control of public areas and buildings. Regarding mosquito disinsection, the average number of local self-government units level was four. Further analysis revealed that in the territories of more than half of the local self-government units, over 91% of households were connected to the water supply system of the public utility company. For 37.7% of local self-government units, the number of households connected to the sewage system was up to 1000 connections, whereas 1% of the total number of households were connected to district heating in the territories of 55.8% of the surveyed local self-government units during 2021 (Table 6).
In the three years of the study period, the availability of analyses of environmental indicators to health councils did not increase, nor did their participation in proposals for environmental improvement (Table 7).
In 2020, a total of 2056 public water pipes and water facilities were controlled by local governments in 25 areas of the territory of the Republic of Serbia. Out of the total number, 156 public water supply systems in urban areas, 827 public water supply systems in rural areas, and 1073 water facilities were controlled. A total of 92,250 samples of drinking water were tested for their physical and chemical properties, of which 16.5% were defective. A total of 94,256 drinking water samples were tested for their microbiological properties, of which 5.4% were defective. Of the total number of controlled public water supply systems in urban areas in the Republic of Serbia in 2020, 13.5% of water supply systems exhibited both physico-chemical and microbiological defects, whereas 68.6% of water supply systems were found to be correct, that is, less than 5% of samples were microbiologically defective and less than 20% were physically and chemically defective on an annual basis.
The physical and chemical correctness was tested on a total of 68,565 samples of drinking water from public water supply systems in urban areas, of which 7.0% were defective. The most common parameters of physical and chemical defects were increased turbidity and color; increased concentrations of iron, manganese, ammonia, nitrates, and nitrites; and increased consumption of potassium permanganate. Sixty-nine thousand, eight hundred and seventy-seven samples of drinking water from the public water supply systems of urban areas were tested for microbiological correctness, of which 2.2% were defective. The most common causes of microbiological defects were an increased number of aerobic mesophilic and total coliform bacteria, as well as the presence of coliform bacteria. In 2020, not a single water epidemic was registered in the Republic of Serbia.
A comparative analysis of indicators of care for the population’s water supply, with the provision of healthy drinking water in the surveyed local self-government units (2019–2021), showed progress. The percentage of local self-government units with beverage factories, with prepared maps of water supply systems (sources and distribution networks) increased, whereas the percentage of local self-government units with asbestos and lead water pipes decreased, and the percentage of local self-government units with a plan for the reconstruction of a water network and with wastewater treatment plants increased (Table 8).
According to the WHO estimates for the European region, environmental factors contribute to at least 15% of mortality in the region, with their distribution and exposure varying between and within countries. Children, pregnant women, and the elderly are especially sensitive to the influence of risk factors from the environment. Most of the pollutants that negatively affect the quality of water, air, soil, and food originate from human activities: industry, energy production and consumption, traffic, agriculture, household activities, inadequate waste disposal, etc.
According to the WHO assessment, air pollution is the most significant risk factor in the environment and at the United Nations High-Level meeting on CNH, held in September 2018, it was included as the fifth risk factor for CNH. In addition to its connection with cardiovascular and respiratory diseases, the connection between air pollution and other diseases, such as diabetes, developmental neurological disorders in children, and neurological diseases in adults, has been proven. Furthermore, chronic exposure to suspended particles, as the dominant air pollutant in the Republic of Serbia, increases the risk of developing lung cancer.
Systematic monitoring of air quality (immission) is performed by measuring and recording the values of individual indicators within the national and local networks of measuring stations. Data obtained from monitoring carried out by public health institutions and other institutions are presented here. The indicator values for 2020 showed that sulfur dioxide was monitored in 48 settlements at 100 measuring points during 2020. The settlements least polluted by sulfur dioxide in 2020 were Gornji Milanovac, Kragujevac, and Čačak. The settlements most polluted by sulfur dioxide in 2020 were Bor, Elemir, and Zrenjanin. During 2020, carbon black was monitored in 40 settlements at 75 measuring points. The settlements that were the least polluted by this pollutant in 2020 were Senta, Kikinda, and Bor. The most polluted settlements in terms of the presence of soot were Zrenjanin and Elemir. Specific polluting substances during 2020 were monitored in 41 settlements at 127 measuring points. The average annual values of ammonia immission were reported only for Zrenjanin (2.92 μg/m3), Pančevo (8.76 μg/m3), and Šabac (35.80 μg/m3). The mean annual value of nitrogen dioxide immission, which reported only in Smederevo, exceeded the allowed mean annual threshold value for populated places of 40.0 μg/m3. The mean annual values for PM10 were above the allowed mean annual value of 40 μg/m3 in Belgrade m.m. Rakovica (40.50 μg/m3), Veliki Crljeni (44.02 μg/m3), Vranovo (49.30 μg/m3), Kraljevo (48.08 μg/m3), Niš (50.62 μg/m3), Požarevac (46.30 μg/m3), Ralji (50.00 μg/m3), Ćuprija (42.75 μg/m3), Užice (45.80 μg/m3), Čačka (46.21 μg/m3), and Šabac (41.20 μg/m3).
Preventive disinfection, disinsection, and deratization simply refer to the systematic implementation of appropriate measures of hygienic and epidemiological protection of the population in order to prevent the occurrence of infectious diseases. Preventive disinfection and the destruction of the causative agents of infectious diseases in the external environment are carried out in order to reduce their number to a level that is harmless to human health. The preventive disinfection of premises, equipment, and accessories is carried out in facilities for the production, storage, and circulation of foodstuffs and raw materials; means of public transport; the facilities of health organizations and social welfare organizations; facilities used for collective stays by children and youth; etc. Preventive disinsection is the destruction of insects (cockroaches, flies, mosquitoes, and ticks), which are possible carriers of infectious diseases, in public buildings and on public surfaces. Preventive extermination is the destruction of harmful rodents, which are sources and carriers of infectious diseases, in order to maintain their number at a level which poses no danger to human health in public buildings and on public surfaces.
The preventive disinfection of premises, equipment, accessories, and means of transportation is carried out daily. Preventive disinsection and pest control is carried out twice a year, and more often if necessary. The suppression of mosquitoes and ticks is carried out according to their population dynamics in coordination with their biodevelopment. In the case of epidemiological indications, disinfection, disinsection, and pest control measures are carried out by order of the administrative body responsible for sanitary inspections, and upon the proposals of the epidemiological services of the competent institutes for public health. The percentage of local self-government units that performed DDD in 2021 was 10 percentage points lower compared to 2020 (80.5%—2021; 90%—2020).
(g) Social care for the public health of the city/municipality in relation to the working environment and the health of the population in 2021 (safety and health at work, inspection work)
The public health importance of a healthy and safe working environment in Serbia is great because the largest contingent of the working population is 20–64 years old and makes up 60% of the population of Serbia. The working population is exposed to the specific conditions of their working environment for at least 40 h per week. In the sample of local self-government units included in this study, on average, 292 were employed per 1000 inhabitants. The lowest employment rate, observed in the municipality of Bujanovac, was 158, and the highest was 816, in the municipality of Topola. The average number of employees per 1000 inhabitants in the Republic of Serbia in 2020 was 321. The average number of employees per 1000 inhabitants in the sample of municipalities obtained from previous reports was 270 for 2019 and 282 for 2020.
The specific characteristics of local governments (urban/rural, industry/agriculture, etc.) determine which public health interventions they carry out in relation to the working environments and health of the population. Local self-government units must be informed about the economic infrastructure (number of employees, structure of jobs) in their territory, the associated risks and potentials, and partnerships with inspection officials and occupational health and safety and occupational medicine services is necessary.
As part of the analysis of social care for the public health of cities/municipalities in relation to the working environments and the health of the population in 2021 (safety and health at work, inspection duties), we determined that there was a large amount of data missing related to employee injuries that occurred in the territories of local self-government units (76.6%) and the systems for monitoring work injuries and occupational diseases (77.9%). In contrast, the procurement of individual protective equipment was at a satisfactory level; with 69 local governments (92%) stating that they had protective masks, 57 local governments (76%) having gloves, and 71 (94.7%) having disinfectants. In terms of the number of reports made to the labor inspection authority regarding safety and security at work, most local self-governments (71.8%) did not have access to this information (Table 9).
Information on monitoring data related to workplace injuries and occupational diseases is no longer available to health councils (Table 10).

Table 10.
Comparative analysis of selected variables related to the monitoring of workplace injuries in local government units, 2019–2021.
Table 10.
Comparative analysis of selected variables related to the monitoring of workplace injuries in local government units, 2019–2021.
| Variable | 2019 | 2020 | 2021 | |
|---|---|---|---|---|
| Possession of data on injuries to employees that occurred on the territories of local self-government units | Yes | 38.7 | 45 | 20.8 |
| No | 48.4 | 55 | 76.6 | |
| Not sure | 12.9 | |||
| Existence of a system for monitoring workplace injuries and occupational diseases | Yes | 21.5 | 33.3 | 19.5 |
| No | 60.2 | 66.7 | 77.9 | |
The inspection and supervision of the implementation of the Law on Safety and Health at Work is carried out by the labor inspector as an administrative body within the Ministry of Labour, Employment, Veterans and Social Affairs. Based on the Work Report of the Ministry of Labour, Employment, Veterans and Social Affairs for 2020 (the latest one available on its website) among employers’ reports on workplace injuries and occupational diseases in 2020 (10,295 in total), 11 fatal injuries were recorded, 1226 serious injuries occurred at work, 435 serious injuries occurred during arrival or departure from work, and 8623 minor injuries occurred. The largest numbers of injuries at work were recorded in the processing industry (17.5%) and in health and social protection (13.1%). The largest number of injuries were reported by employers employing more than 500 employees (45.1%), as well as by employers with 50–249 employees (25.4%). Separating injuries at work by gender, men (63.9%) were injured more frequently than women. The largest number of work-related injuries occurred among employees aged between 46 and 55 (30%), as well as among employees aged between 36 and 45 (21.8%). By qualification level, the most frequently injured were persons with a medium level of education (third and fourth degree) (61.6%). By location, injuries most often occurred in production plants, factories, and workshops (25.8%) and in open spaces (15.3%). The largest number of injuries at work occurred during movement (40.6%); due to slipping, tripping, and falling; and when working on machines due to the loss of control (11.1%). The largest number of injuries at work, sorted by type of injury, were caused by bone fractures (70.5%).
Certain occupational risks, such as injuries, noise, carcinogenic agents, airborne particles, and ergonomic risks, represent a significant part of the burden of chronic diseases, being associated with 37% of all cases of back pain, 16% of cases of hearing loss, 13% of chronic obstructive diseases, 11% of asthma cases, 8% of injuries, 9% of lung cancer cases, 2% of leukemia, and 8% of depression. Economically active people, on average, spend about one third of their time at work. Employment and working conditions have a strong impact on health equity. Good working conditions can provide social protection and status, opportunities for personal development, and protection from physical and psychosocial hazards. They can also improve the social relations and self-esteem of employees and lead to positive health effects. The health of workers is a basic prerequisite for household income, productivity, and economic development. Therefore, restoring and maintaining working capacity is an important function of health services.
Health hazards in the workplace, such as heat, noise, dust, dangerous chemicals, unsafe machinery, and psychological stress, cause occupational diseases and can exacerbate other health problems. Health is also affected by people’s employment conditions, their profession, and their position in the workplace hierarchy. People who work under stress or with insecure employment conditions are likely to smoke more, exercise less, and consume an unhealthy diet. In addition to general healthcare, all workers—and especially those in high-risk occupations—need health services to assess and reduce their exposure to occupational risks, as well as medical surveillance for the early detection of occupational diseases and injuries at work. Chronic respiratory diseases, musculoskeletal disorders, noise-induced hearing loss, and skin problems are the most common occupational diseases. However, only one third of countries have programs to address these issues.
Non-communicable diseases related to work (occupational diseases), as well as cardiovascular diseases and depression caused by occupational stress, lead to an increase in the rate of long-term illnesses and absence from work. Occupational diseases include occupational cancer, chronic bronchitis, and asthma caused by workplace air pollution and radiation. The reform of the health system in the first decade of the 21st century in Serbia devastated the existing network of services for the healthcare of workers in institutions in the Network Plan, and private health institutions play the leading role in the preventive examinations of the working population, performing periodic and systematic examinations specific to the workplaces of employees.
(d) Social care for the public health of the city/municipality in relation to the organization and functioning of the health system (healthcare, social activity)
The results of our research in the field of social care for the public health of cities/municipalities in relation to the organization and functioning of the health system (healthcare, social activity) indicated that in 85.7% of local communities, the founding rights of the Health Center were transferred to the Ministry of Health/APV. Furthermore, in 70 (90.9%) local communities, there was an Advisor for the Protection of Patients’ Rights, who in most cass (70.1%) had an official ID card issued by the Ministry of Health and performed a wider range of tasks (84.4%), whereas for the protection of patients’ rights, the majority (85.7%) did not receive a salary supplement. The working hours of Counselors in most communities (37.7%) were not strictly determined, whereas a separate room in which Counselors received patients were reported in 34 (44.2%) local communities. In most local self-government units (83.3%), there was one executor in charge of protecting the rights of patients. Further results indicated the existence of public transport from surrounding towns to the center of the local community in 68.8% of communities (Table 11).
Emergency medical assistance, as a separate organizational unit, was available in a little more than half of the examined local communities (53.2%), whereas the number of health centers in the local self-government units reached up to five (89.8%), and the number of clinics reached up to 10 (73.97%). Local self-government units participated in most communities (85.7%) in the organization of special COVID clinics, i.e., temporary hospitals. In addition to this form of assistance, they participated to a significant extent in the provision of additional facilities/spaces for testing and examination points (60.3%), the procurement of personal protective equipment for health institutions (55.7%), and the provision of disinfectants (66.7%). In addition, 22 local governments (34.9%) provided assistance in financing additional staff, 38 local governments (28.6%) participated in providing transportation for patients and healthcare workers, whereas 13 local governments (20.6%) ensured the procurement of ambulances for health institutions (Table 11).
In order to analyze the availability of healthcare, a new category of variable for local self-government units was introduced according to population density per square kilometer. The categorization process was carried out in accordance with the rulebook on conditions for the performance of healthcare activities in healthcare institutions and other forms of healthcare (“Official Gazette of RS”, no. 43/06, 112/09, 50/10, 79/11, 10/12—Dr. Rulebook, 119/12—Dr. Rulebook, 22/13 and 16/18), with the establishment of three categories: municipalities with up to 25 inhabitants per square kilometer, municipalities with a population density of 26 to 40 inhabitants per square kilometer, and municipalities with more than 40 inhabitants per square kilometer. The criterion was chosen in accordance with the norms for the teams of general medical services in health centers, which, are standardized according to the population density at 1200, 1400, and 1600 inhabitants per team.
According to the estimates of the Institute of Statistics of the Republic of Serbia, 6,899,126 people live in Serbia. Of this total, 3,381,047 inhabitants, or 49%, lived in the 77 local governments that formed the basis of the current study. Serbia has a total of 6158 settlements, and in our survey local governments worked in participation with a total of 1944 settlements, that is, one third of the total number of settlements (32.3%). The average population density in Serbia is 78 inhabitants per square kilometer, i.e., the average is 95 inhabitants per square kilometer in our sample. In the survey, seven local governments had less than 25 inhabitants per square kilometer, and municipalities with a population density of 26 to 40 inhabitants per square kilometer were represented by 15 local self-government units. The other 55 cities/municipalities had more than 40 inhabitants per square kilometer (Table 12).
According to the official data, a total of 3676 doctors provided healthcare for the adult population over the age of 19 in the Republic of Serbia in 2020, i.e., the number of adult residents per doctor in this service was 1512. For each doctor providing health service for women in the Republic of Serbia, there are 5843 women over the age of 15. In 2020, a total of 1272 doctors provided health services for children (662) and for school children and youth (610). There were 1045 children aged 0–19 for each doctor providing these services in the Republic of Serbia.
Analyzing the two sets of data, regarding the number of residents per doctor (the total number of doctors of all specialties at all levels) and the number of residents within certain age groups per selected doctor, there was insufficient provision of doctors in all primary healthcare services in all local self-government units. The coverage of women during the first trimester of pregnancy, with the provision of modern healthcare, in the Republic of Serbia in 2020 was 71.77%. In one fifth of local self-government units (21%), less than half of pregnant women did not receive this service at the health center regardless of universal health insurance during pregnancy.
The right and scope of health insurance provides for five visits to a midwife and healthcare for the newborn during the first month, and more if necessary (by order of a pediatrician). On average, visiting nurses in the RS made three visits to each newborn. In 49 local self-government units (64.4%), complete coverage was not realized with all five visits.
In 2020, the coverage of complementary vaccination against diphtheria, tetanus, whooping cough, polio, and hemophilus influenza type B (pentavalent) in the first year of life was 91.7%. Only half of local self-government units (38) achieved the target coverage of children with this vaccine, i.e., 95% or more. The percentage of children who were vaccinated against measles in the first 18 months in the RS for 2020 was 78.1%. Only in 20 local self-government units, i.e., one quarter (26%), was the target coverage of 95% or more achieved.
(đ) Social concern for the public health of the city/municipality in relation to dealing with emergency situations (social activities, health, emergency headquarters)
Emergency situations—defined as a state of increased risks, threats, or consequences which require special measures, forces, and means for their elimination or reduction and an increased work regime conducted by competent authorities—often represent a great burden for public health at the local and national level. Strengthening emergency prevention measures through the development of appropriate assessments and plans for responding in such situations and the implementation of continuous education and training is a prerequisite for effective disaster risk management. The importance of this type of prevention, however, was not recognized by a large proportion of the local self-governments examined. This was indicated by the absence of local plans for taking care of the health of the population in emergency situations in 60 local governments (20.8%), as well as the insufficient scope of implementation of exercises and education in the field of first aid (57.1%). In contrast, protection and rescue plans had been developed in 40 local governments (51.9%), whereas in 26 local governments (33.8%) the drafting process was underway (Table 13).
Concerning the exercises and education programs implemented in relation to providing first aid, with an average of 1.56 such programs reported by each self-government unit, the Red Cross was the most commonly reported organizer (39%), followed by the Ministry of the Interior (19.5%), local self-government units themselves (12.2%), and civil society organizations (4.9%). Cooperation between the Headquarters for Emergency Situations and local self-government units was achieved in the most cases by health institutions (90.7%), the Ministry of the Interior (82.7%), the Red Cross (74.7%), and sanitary inspection officials (66.7%), whereas it was implemented in fewer self-government units in coordination with health councils (36%) and communal police (38.7%). During COVID-19, a “call center” for immunization was organized in 56 local governments (76.6%), whereas a professional/operational team for immunization was formed in a significantly smaller percentage of local government areas (42.9%).
Vulnerable categories of the population, such as children, the elderly, people with disabilities, and others, face special challenges during emergencies in terms of their mobility and their access to information and other resources. The registration of these groups for immunization was carried out in most cases through the call center (69.3%), the local community (53.3%), and engaged volunteers (49.3%) and to a lesser extent through the Center for Social Work (22.7%). Furthermore, seven local governments (9.3%) did not implement special activities targeting vulnerable population groups (Table 17). In most local self-governments (61%), no transportation for the population for the purpose of immunization was organized, and the total number of points available for people to receive immunizations was 3.11 on average. On the Likert scale, local self-government units rated their cooperation with health institutions as very highly developed (66.2%).
During the three years of the study period, the efforts of local self-government units to develop local plans for the care of the population in crisis and emergency situations, as well as the local rescue plans for emergency situations, did not exhibit a significant improvement compared with the preceding years (Table 14).
- Correlation analysis of variables from the field of public health in Serbia
The results of the chi-squared tests showed that there was a statistically significant relationship between the establishment of a council for public health and the following variables: having a Work Plan for 2022 (p = 0.000); having a public health plan (p = 0.000); the participation of a Standing Conference of Towns and Municipalities in the process of making the plan (p = 0.000); the process of making a plan with the help of institutions/institutes (p = 0.000); having a representative of the institute for public health (p = 0.000); the attendance of meetings by representatives (p = 0.000); the availability of analyses of the state of health of local self-government units (3 years) (p = 0.000); the identification of vulnerable groups (p = 0.000); the performing of public health risk assessments by local self-government units (p = 0.002); the availability of inspection reports (p = 0.000); the implementation of campaigns promoting healthy lifestyles (p = 0.000); different methods of supporting campaigns (p = 0.000); the cooperation of the council with the Headquarters for Emergency Situations (p = 0.000); the availability of analyses of environmental indicators (p = 0.000); the awareness of suggestions for improving environmental indicators (p = 0.000); the existence of zones of sanitary protection of the water supply (p = 0.000); the creation of a map/diagram of the water supply system (p = 0.000); the availability of a water network reconstruction plan (p = 0.000); having a wastewater treatment plant (p = 0.000); having a register of septic tanks and collecting pits (p = 0.000); performing air control measures (p = 0.000); having a municipal waste dump (p = 0.000); access to data on employee injuries (p = 0.000); having a system for monitoring work injuries (p = 0.000); having an adviser for the protection of patient rights (p = 0.000); having a local emergency healthcare plan (p = 0.000); having a protection and rescue plan (p = 0.000); and conducting exercises and education in the area of providing first aid (p = 0.000). No statistically significant correlation was found with the other variables (Table 15).
Further analysis showed that local self-government units that had formed a Health council had not adopted a Work Plan for 2022 in 71.6% of cases. Of the total number of local self-government units that had formed a health council, 49.3% had not adopted a Public Health Plan, 16.4% had started the drafting process, and 6% had such a plan underway in the parliamentary process. Then, we determined that 53.7% of local self-government units pointed out that the Standing Conference of Towns and Municipalities helped them in the process of making plans, whereas 46.3% pointed out that they did not receive such help. Furthermore, 52.2% of local self-government units did not report that they had used the help of the competent institute in the process of creating their public health plan. It is important to point out that we determined that only 26.9% of local self-government units that had formed a council did not have a representative of the institute for public health. On the other hand, 71.6% of local self-government units had a representative of institute in the council.
In the majority of local self-government units that had formed a council (44.8%), the competent institute for public health had not prepared an analysis of the health status of the local self-government units in the three years of the study period, whereas in 13.4% of cases it was in the process of being prepared. It is interesting to point out that in 52.2% of cases, local self-government units did not identify vulnerable groups in the analysis of the health status of the city/municipality. The results showed that in 83.6% of local self-government units that have formed a council, risk assessment studies for local self-government units health had not been prepared, whereas, on the other hand, in 49.3% of local self-government units, inspection reports for 2021 were not available.
In the further analysis of the obtained results, we determined that of local self-government units that had formed a council, the majority (76.1%) participated in health promotion campaigns. In addition, we determined that local self-government units that had formed a council provided support to the greatest extent (33%) by providing space, transportation, and media support. Furthermore, the majority of local self-government units with established councils (61.2%) cooperated with the Headquarters for Emergency Situations. Moreover, many of them (56.7%) pointed out that no analyses of environmental indicators were available and an even greater proportion (89.6%) did not give recommendations for the improvement of such indicators. Furthermore, we determined that local self-government units that had formed a council, in most cases (74.6%), had established certain sanitary protection zones in regard to their water supply; they had a map/diagram of their water supply system (68.5%).
On the contrary, among local self-government units that had not formed a council, most units (80%) had a plan for the reconstruction of the water supply network and they reported having wastewater treatment facilities to a greater extent (40%) than units that had formed a council. Several of these units reported having an advisor for the protection of patients’ rights (92.5%), having a developed plan for the protection and rescue of the population (55.2%), and had conducted exercises and education in the field of first aid (43.3%). On the other hand, local self-government units that had formed a council had to a slightly greater extent (4.5%) established a register of septic and collecting pits, performed air control measures (47.8%); had access to data on employee injuries (20%), had a system for monitoring injuries (22%), and had a local plan for taking care of the health of the population in emergency situations (40%).
The results of the chi-squared test showed that there was a statistically significant relationship between the development categories of local self-government units and the following variables: having a Work Plan for 2022 (p = 0.000); having a public health plan (p = 0.000); receiving help from the Standing Conference of Towns and Municipalities in the process of making the plan (p = 0.000); the type of help provided by the Standing Conference in the process of creating a plan (p = 0.000); the creation of a public health plan (p = 0.000); having a representative of the institute on the council (p = 0.000); the attendance of meetings by representatives (p = 0.000); the availability of analyses of the state of health of local self-government units (3 years) (p = 0.000); having identified vulnerable groups (p = 0.000); the availability of local self-government units’ public health risk assessments (p = 0.000); the availablility of inspection reports (p = 0.000); instituting campaigns promoting healthy lifestyles (p = 0.001); cooperation of the council with the Headquarters for Emergency Situations (p = 0.000); the availability of analyses of environmental indicators (p = 0.000); making suggestions for improving environmental indicators (p = 0.000); having zones of sanitary protection of the water supply (p = 0.000); having a map/diagram of the water supply system (p = 0.000); having a water network reconstruction plan (p = 0.000); having a wastewater treatment plant (p = 0.000); having a register of septic tanks and collecting pits (p = 0.000); performing air control measures (p = 0.000); having a municipal waste dump (p = 0.000); the availability of data on employee injuries (p = 0.000); having a system for monitoring work injuries (p = 0.000); having an adviser for the protection of patient rights (p = 0.000); having a local emergency healthcare plan (p = 0.000); having a protection and rescue plan (p = 0.000); and conducting exercises and education in the area of providing first aid (p = 0.000). No statistically significant correlation was found with the other variables (Table 16).
Further analyses showed that the local self-government units belonging to the fourth category of development in the largest number of cases (88.2%) had not adopted a work plan for 2022. In contrast, local self-government units belonging to the second category of development had most often (33%) adopted such a document. Furthermore, we determined that local self-government units in the second category of development had adopted a public health plan to the greatest extent (38.9%). In the same category of local self-government units, respondents pointed out most frequently (66.7%) that the Standing Conference of Towns and Municipalities helped them in the process of developing the plan, whereas this was noted the least (58.3%) by local self-government units belonging to the third category of development. Local self-government units in the third category of development pointed out to the greatest extent (33.6%) that the Standing Conference of Towns and Municipalities provided them with assistance in the form of training, professional support, and the use of manuals for the development of a public health plan.
The largest proportion (66.7%) of local self-government units from the second category developed a public health plan with the help of the competent institution. On the other hand, this was reported in the smallest number of cases (23.5%) by local self-government units from the fourth category of development. In addition, we determined that local self-government units from the fourth category of development, in most cases (76.5%), had a representative of the competent institution/institute on the health council, whereas local self-government units from the third category reported this the least (66.7%). Furthermore, local self-government units from the second category of development reported to the greatest extent (72.2%) that representatives of institutions regularly attended sessions, whereas those in the III category of development reported this the least (33.3%).
Most local self-government units from the second category of development (51%) had conducted an analysis of the health status of local self-government units for the previous 3 years. In local self-government units from the first category of development, to the greatest extent (70.6%)m vulnerable groups were identified within the analysis of the health status of local self-government units. In the largest number of cases, local self-government units from the fourth category of development (94.1%) did not have access to a public health risk assessment of local self-government units. Moreover, we determined that local self-government units from the third category (33.3%) most often emphasized that they had inspection reports available for the year 2021.
In further analyses of the obtained results, we determined that local self-government units from the first category participated to the greatest extent (94.4%) in health promotion campaigns, whereas local self-government units from the fourth category participated the least (58.8%). In addition, local self-government units in that category emphasized to the greatest extent (61.1%) that analyses of environmental indicators were available to them, whereas local self-government units from the fourth category (23.5%) emphasized this the least. To the greatest extent, proposals for improving the analysis of environmental indicators were given by local self-government units from the second category of development (27.8%), whereas local self-government units from the first category of development (5.6%) reported this the least. Sanitary protection zones had been determined to the greatest extent (88.9%) by local self-government units from the second category of development, whereas local self-government units from the first category of development reported this the least (61.1%).
The majority (77.8%) of local self-government units from the second category had a map/scheme of their water supply system, whereas the local self-government units from the third category (55.6%) reported this the least. Having a plan for the reconstruction of the water supply network was reported to the greatest extent (94.4%) by local self-government units from the second category, whereas local self-government units from the fourth category reported this the least. Wastewater treatment plants were mostly owned by local self-government units from the second category (66.7%), whereas local self-government units from the first category (33.3%) were the least likely to own them.
Registers of septic and collection pits were reported most often (5.9%) by local self-government units from the fourth category of development, whereas this was reported the least (0.5%) by local self-government units from the first category. Air control measures in local self-government units were carried out to the greatest extent (72.2%) by local self-government units from the second category, whereas these were carried out by the fewest local self-government units in the fourth category (17.6%). Data related to injuries of employees in the workplace were most frequently reported to be available (35.3%) to local self-government units from the fourth category, whereas this was reported the least by local self-government units from the second category (16.7%). A system for monitoring work injuries was available to the greatest extent (29.4%) to local self-government units from the fourth category, whereas local self-government units from the third category (8.3%) reported this the least. Advisors for the protection of patients’ rights were reported to the greatest extent (95.8%) by local self-government units from the third category. The existence of a local plan for taking care of the health of the population in emergency situations was most often reported (33.3%) by local self-government units from the third category, whereas local self-government units from the first category (16.7%) were the least likely to have such plans.
Having a plan for protection and rescue in emergency situations was reported to the greatest extent (58.3%) by local self-government units from the third category, whereas this was reported the least by local self-government units from the second category (44.4%). Practices and education in the field of providing first aid were most often provided by local self-government units from the first category (50%), whereas local self-government units from the second category (38.9%) reported the lowesrt amount of training. Furthermore, the results showed that local self-government units from the third category most often (62.5%) emphasized that the health council cooperated with the Headquarters for Emergency Situations, whereas local self-government units from category IV emphasized this the least (47.1%).
The results of the chi-squared test showed that there was a statistically significant relationship between the realized budget for program activities and the public health risk assessments of local self-government units (p = 0.005). In contrast, no statistically significant association with any other variables was found (Table 17). Based on the obtained results, it could be said that the budget is not a decisive factor for the success of the implementation or improvement of public health by local self-government units, bearing in mind that no statistically significant difference was determined on this basis (Table 22). Further analysis showed that local self-government units that implemented up to 70% of their program budget in the largest number of cases (87.5%) did not have access to public health risk assessments of local self-government units. In addition, we determined that local self-government units that realized up to 80% of their projected budget in 33.3% of cases had access to a public health risk assessment in the drafting procedure (Table 17).
Table 17.
Results of the chi-squared test of the percentage of realized budget and selected variables.
Table 17.
Results of the chi-squared test of the percentage of realized budget and selected variables.
| Variable | Sig. (2-Tailed) |
df | X2 |
|---|---|---|---|
| The council adopted a Work Plan for 2022 | 0.439 | 12 | 12.08 |
| The council adopted a public health plan | 0.355 | 16 | 17.47 |
| Received help from the Standing Conference of Towns and Municipalities in the process of developing the plan | 0.946 | 8 | 2.79 |
| Type of assistance received from the Standing Conference of Towns and Municipalities in the process of developing the plan | 0.277 | 16 | 18.83 |
| Drafting of a public health plan | 0.936 | 8 | 2.97 |
| Presence of a representative of the competent institution on the council | 0.749 | 12 | 8.45 |
| Attendance of representatives at sessions | 0.577 | 12 | 10.44 |
| Access to analyses of the state of health of local self-government units (3 years) | 0.160 | 12 | 16.73 |
| Having identified vulnerable groups | 0.686 | 8 | 5.65 |
| Access to public health risk assessments of local self-government units | 0.005 * | 12 | 26.70 |
| Availability of inspection reports | 0.232 | 21 | 26.17 |
| Instituting campaigns promoting healthy lifestyles | 0.904 | 8 | 3.43 |
| Means of supporting campaigns | 0.316 | 34 | 15.24 |
| Cooperation of the council with the Headquarters for Emergency Situations | 0.428 | 12 | 12.21 |
| Availability of analyzes of environmental indicators | 0.570 | 8 | 6.69 |
| Creation of proposals for improving life indicators | 0.946 | 8 | 2.80 |
| Having zones of sanitary protection for the water supply | 0.594 | 12 | 10.24 |
| Having a map/diagram of the water supply system | 0.644 | 20 | 17.13 |
| Having a plan for the reconstruction of the water supply network | 0.869 | 8 | 3.87 |
| Having a wastewater treatment plant | 0.769 | 8 | 4.89 |
| Having a register of septic and collecting pits | 0.377 | 12 | 12.88 |
| Performing air control measures | 0.601 | 8 | 6.41 |
| Having a municipal waste dump | 0.376 | 8 | 8.60 |
| Access to data on employee injuries | 0.648 | 8 | 5.99 |
| Having a system for monitoring work injuries | 0.626 | 8 | 6.19 |
| Having a counselor for the protection of patient rights | 0.622 | 8 | 6.22 |
| Having a local emergency healthcare plan | 0.800 | 8 | 4.59 |
| Having a protection and rescue plan | 0.995 | 12 | 3.09 |
| Conducting exercises and education in the field of first aid | 0.679 | 8 | 5.71 |
* p ≤ 0.05;
The results of the chi-squared test showed that there was a statistically significant relationship between the preparation of a public health risk assessment study of local self-government units and the following variables: the creation of a public health plan (p = 0.007); the identification of vulnerable groups (p = 0.008); instituting campaigns promoting healthy lifestyles (p = 0.004); the availability of analyses of environmental indicators (p = 0.003); making suggestions for improving indicators (p = 0.004); having a water network reconstruction plan (p = 0.003); having a wastewater treatment plant (p = 0.006); having a protection and rescue plan (p = 0.039); conducting exercises and education in the field of first aid (p = 0.000). In contrast, no statistically significant association with any other variables was found (Table 18).
Further analysis revealed that local self-government units that had reported preparing a public health risk assessment study to a greater extent (33%) had adopted a public health plan and to a greater extent had such plans in progress (50%). Such local self-government units reported more often (66.7%) that the Standing Conference of Towns and Municipalities helped them in the process of developing the plan and that the competent institution helped them in the process of developing a public health plan (64.8%). Moreover, we determined that the local self-government units that had prepared such an assessment more often (83.3%) performed an analysis of the health condition of the local self-government units for the previous three years. In addition, to a greater extent, they identified vulnerable groups in the area of local self-government units (87%).
In addition, such local self-government units were also more likely to participate in campaigns for the promotion of healthy lifestyles (83.3%), to report the availability of analyses of environmental indicators (82.3%), to give suggestions for improving indicators (33.3%), to have plans for the reconstruction of water supply networks (100%), to have wastewater treatment plants (34.3%), not to have plans for protection and rescue in disasters (52.4%), and to conduct exercises and education in the field of first aid (50%).
The results of the Pearson correlation analysis showed that there was a statistically significant correlation between the effectiveness of the realized program budget and the following variables: microbiologically defective samples of drinking water from the so-called village waterworks (r = 0.529, p ≤ 0.01), microbiologically defective samples of drinking water from public taps (r = 0.368, p ≤ 0.01), the percentage of unsatisfactory analyses of wastewater samples (r = 0.406, p ≤ 0.01), the total number of air samples on an annual level for PM25s (r = 0.365, p ≤ 0.01), and the number of mandated fines issued (r = 0.252, p ≤ 0.01). No statistically significant correlation was found with other variables (Table 19).
Judging by the obtained results, we determined that with the increase in the efficiency of the realized program budget, the number of microbiologically defective drinking water samples from the so-called village waterworks increased, as did those from public fountains, the number of unsatisfactory analyses of waste water samples, as well as the total number of air samples on an annual level for PM25s. In addition, with the increase in the efficiency of the implementation of the program budget, the number of mandated fines issued also increased.
The results of the T-tests showed that there was a statistically significant association between having a public health plan and the following variables: physical/chemical defective water samples in rural schools (p = 0.023), unsatisfactory analyses of waste water samples (p = 0.037), and septic and collection pits (p = 0.001). Further analyses showed that local self-government units that had a public health plan were more likely (M = 25.61) to report that they had physico-chemical defective water samples in their rural water supply systems, followed by unsatisfactory analyses of wastewater samples (M = 54.05). On the other hand, local self-government units that did not have a Public Health Plan were more likely (M = 9.62) to report that had have septic and collecting pits that were regularly maintained (Table 20 and Table 21).
- 3.
- Predictors of the state of public health in Serbia
In the first step of applying the logistic regression model, the combined impact of various factors was tested (with these factors including the availability of analyses of the health status of local self-government units, the identification of vulnerable groups, the availability of risk assessment studies, performing air control measures, having a register of septic and collection pits, having a local plan for healthcare in emergency situations, instituting health promotion campaigns, and access to data on employee injuries) in the predicted model (Table 22).
The first model, with the dependent variable analysis of the health status of local self-government units, indicated statistically significant results, with χ2 = 18.44, (5, N = 77) p ≤ 0.002, and explained between 21.1% (Cox and Snell) and 28.9% (Nagelkerke) of the variance. The results indicated that one variable had a unique statistical influence on the model (receiving help from the Standing Conference of Towns and Municipalities; p ≤ 0.05) and its probability quotient was 5.6. This shows that local self-government units that received assistance from the Standing Conference of Towns and Municipalities performed an analysis of the health status of local self-government units 5.6 times more often than other units did.
Next, we tested the model with the dependent variable of the identified vulnerable group and found that it was statistically significant, with χ2 = 36.85 (10, N = 77) p ≤ 0.000, and explained between 37% (Cox and Snell) and 50.6% (Nagelkerke) of the variance. The results indicated that two variables had a unique statistical influence on the model (appointed coordinator (p ≤ 0.05) and health status analysis (p ≤ 0.05)). In addition, we determined that the coefficient of probability for the appointed coordinator variable was 4.5, whereas for the analysis of the health status the coefficient was 6. This showed that the local self-government units that appointed a coordinator of the health council were four and a half times more likely to identify vulnerable groups within their analysis of the health status of the local self-government unit. In contrast, local self-government units that conducted health status analyses identified vulnerable groups six times more often within their analysis of the local self-government unit’s healthcare status (Table 22).
In the third model, with the dependent variable of the risk assessment study, it was determined that the results were not statistically significant, with χ2 = 4.66 (5, N = 77) p = 0.458. In addition, the results showed that the model (air control) was not statistically significant (χ2 = 5.66 (5, N = 77), p = 0.340) as was the case for the predictive model regarding the register of septic tanks and collection pits (χ2 = 6.51 (5, N = 77) p = 0.259); the model related to having a local plan for the provision of healthcare in emergency situations (χ2 = 2.99 (5, N = 77) p = 0.701), the model related to the implementation of campaigns (χ2 = 6.14 (5, N = 77) p = 0.293), as well as the model related to injuries to employees (χ2 = 10.34 (5, N = 77), p = 0.412) (Table 22).
Table 22.
Logistic regression analysis used to assess the predictive power of selected variables.
| Predictor Variable | Analysis of the Health Status of Local Self-Government Units | Identified Vulnerable Groups | Risk Assessment Studies | Air Control | Register of Septic and Collecting Pits | Local Emergency Care Plan | Health Promotion Campaigns | Data on Employee Injuries | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| B | SE | B | SE | B | SE | B | SE | B | SE | B | SE | B | SE | B | SE | |
| Council formed | 1.84 | 1.14 | 2.50 | 1.46 | −3.05 | 1.84 | 0.62 | 0.82 | 0.71 | 0.75 | 0.05 | 0.87 | 0.97 | 0.72 | −1.55 | 0.80 |
| Coordinator appointed | −0.15 | 0.561 | 1.52 | 0.65 | −2.18 | 1.50 | 0.54 | 0.54 | 0.40 | 0.49 | 0.77 | 0.60 | 0.54 | 0.58 | 0.27 | 0.61 |
| Public health plan | 0.30 | 0.62 | 1.22 | 0.72 | −0.99 | 1.65 | 0.56 | 0.67 | 0.78 | 0.59 | −0.21 | 0.69 | 0.64 | 0.76 | 1.02 | 0.71 |
| Received help from the Standing Conference of Towns and Municipalities | 1.73 | 0.60 | −0.063 | 0.74 | 0.29 | 1.47 | −1.37 | 0.67 | −0.50 | 0.53 | 0.58 | 0.65 | 0.44 | 0.59 | 0.032 | 0.69 |
| Adviser for the protection of rights | 1.05 | 1.20 | −1.85 | 1.10 | −0.87 | 1.92 | 0.65 | 032 | 0.95 | 0.91 | −0.63 | 0.93 | −0.73 | 0.98 | 20.34 | 0.97 |
4. Recommendations
The level of participation of local governments in health promotion campaigns in the community was satisfactory. After the decentralization process in 2005, local governments received the founding rights in relation to primary healthcare institutions. The health policy adopted at that time, described in the document Better Health for All in the Third Millennium and the series of activities undertaken in accordance with the action plan required the significant engagement, aside from the health sector, of a number of different actors associated with public health in the community. Numerous programs have strengthened the civil sector, including both citizens’ associations and patients’ associations. Through numerous projects, actors in the community were strengthened through the formation of a partnership with a common goal, creating conditions in their living and working environments designed to lead to the improvement and preservation of health and increase the quality of health services.
At the same time, the focus of health protection institutions at that time changed significantly to reflect a new, significantly broader concept of public health. From numerous projects supported by the international community, foundations of advisors arose for the protection of patients’ rights and the provision of health advice. During the past fifteen years, the involvement of these actors in the community has been strengthened, but we must certainly not neglect further work with young people who are just getting involved in the field of public health. Health centers, as providers of primary healthcare, are the strongest partners in local self-government units, and it is necessary to nurture and further improve these relationships by all means, as well as partnerships with experts from the Institute for Public Health.
Further steps in increasing the capacities of local governments and other public health actors in the community are as follows.
- − The presentation of research results and the distribution of analyses to interested parties and partners;
- − Providing support to local self-governments that are in the process of adopting and developing public health plans to help them complete the process;
- − Aim to complete the process of creating public health plans in 90% of local self-government units;
- − Organize training related to the development of public health programs (involving the selection of priorities, goals, change indicators, activities, and activity indicators, as well as budget preparation) for at least 50% of local self-government units which have not yet adopted public health programs;
- − Organize workshops for the development of public health program models in accordance with the rulebook on conditions for the implementation of public health in the area of the environment and population health, covering two topics per year: the monitoring and analysis of the state of the environment in relation to health impacts;
- − Monitoring and controling the quality and suitability of drinking water in relation to health and assessing its impact on the health of the population;
- − Monitoring and controling the healthiness of foodstuffs and items of general use;
- − Performing disinfection, disinsection, pest control, and monitoring for the presence of harmful organisms;
- − The control of sanitary and hygienic conditions in public facilities;
- − Providing opinions on documents for spatial and urban planning in relation to the health of the population;
- − Performing assessments of the risk to the health of the population based on the pollution source register (cadaster), and in connection with the risk factors from the environment, including the assessment of the epidemiological situation;
- − Providing support for local self-government units in the development of plans regarding the care of the population in emergency situations (50% in 4 years);
- − Organizing workshops for the development of public health programs in the field of promotion—the creation of successful campaigns and the provision of support for national programs;
- − The establishment of a mentoring model of local self-government units
- − The exchange of practices and experiences, providing support for the dissemination of successful program activities;
- − Facilitating intersectoral cooperation in local self-government units among public health actors, and building and strengthening the partnership between the public and civil sectors in the area of public health;
- − The creation of publications—providing guides/instructions;
- − Conducting continuous monitoring and evaluations;
- − In addition to supporting the development of public health plans, providing support for local self-governments in the development of mandatory local action plans related to public health, especially in the area of improving the vaccination coverage of children in the first and second years of life, including preventive examinations of pregnant women in the first trimester of pregnancy, full coverage visits to midwives and newborns by a patronage service, the improvement of mental health, and the prevention of HIV/AIDS and the abuse of psychoactive substances;
- − Although a large percentage of local governments have an institutionally provided advisor for the protection of patients’ rights, a small number of patients’ complaints indicated that it is necessary to empower citizens to exercise their rights guaranteed by law;
- − The analysis highlighted the importance of communication between partners and interested actors in relations to public health (healthcare facilities, public health institutes, inspection services, and the civil sector) and model workshops with the participation of all actors are recommended in further work; furthermore, so that the existing analysis can be applied to follow the progress of all local self-government units and so that we can accomplish the planned inclusion of local governments according to our priority areas, it would be desirable in the coming period to collect data from municipalities that were not included in this study through the competent public health institutes;
- − All activities should be coordinated with an action plan as part of the public health strategy. Given that this is a continuous process, it is necessary to monitor the situation on the ground continuously and, according to the assessed situation, to adjust the methods and scope of support provided to local self-government units in the area of public health.
Cities and municipalities, according to the competences derived from the Law on Local Self-Government (“Official Gazette of the RS”, no. 129/07, 83/14) perform many functions that are directly related to the protection of the environment and health. The Law on Public Health stipulates that local self-government units, as part of the social provision of healthcare, have the obligation to implement preventive measures for the preservation and improvement of the environment (water, air, soil, noise, vibrations, and ionizing and non-ionizing radiation), ensuring the conditions for supplying the population with healthy water for drinking and safe food and the disposal of waste materials, as well as activities related to sanitary, hygienic, and epidemiological surveillance. The tasks related to monitoring and supervision are carried out by the territorially competent public health institutes; they analyze the health status of the population through assessments of health risks related to the impact of the environment.
Public health enforcement in the area of dealing with emergency situations includes public health risk assessments and actions conducted according to the law that regulates this area (the Law on Disaster Risk Reduction and Emergency Management). Each unit of local self-government is obliged to prepare protection and rescue plans and plans for action in emergency situations, as well as to implement security measures and the exchange of information in emergency and crisis situations. A prerequisite for a good response and action is effective cooperation among all actors at the local level (communal services, health services, the army, police, water supply, traffic organizations, etc.). In the preparation and prevention stage, it is necessary to train the population to react effectively to different situations, through the preparation of shelters, first aid training, the timely printing and distribution of brochures on dealing with crisises and emergency situations and health protection, as well as providing verified and true information through the media regarding the current situation, as well as providing training for volunteers.
5. Conclusions
The results of the study can be considered relevant to the regular monitoring and evaluation of indicators in the field of public health and in regard to health improvement at the local level, as well as assessing the capacities of cities and municipalities to implement their given responsibilities. The survey comprehensively assessed self-government units’ competencies in all areas of public health. The results obtained from the analysis of the work of the health councils, the selected indicators for each area of public health, and the effects of the support of the Standing Conference of Towns and Municipalities and the representatives of the public health institutes provided clear guidelines for establishing effective monitoring systems, planning the activities of the actors involved (local self-government units, the Standing Conference of Towns and Municipalities, and public health institutes) and evaluating their effects.
The results confirmed the effectiveness of implementing health councils in the areas of promotion and prevention, as well as in the organization and functioning of the healthcare system. In future works, local self-government units should be supported in their choices of effective programs and priorities. Although a large percentage of local governments reported having an institutionally provided advisor for the protection of patients’ rights, a small number of patient complaints indicated that it is necessary to empower citizens to exercise their rights guaranteed by law.
Areas of public health that were identified as needing special support included the environment, workplace environments, and emergency situations. The environment is the most complex area and probably the most important because it includes the entire population in each local self-government area. First of all, it is necessary to conduct health risk assessments in each municipality and adopt special environmental improvement programs based on the unit’s priorities. In general, the most important issues identified was water—the provision of proper drinking water in cities and small village waterworks, the availability of proper water in public facilities, as well as providing solutions regarding wastewater for both communal and industrial facilities. The second most important issue was air pollution measurements, which must be conducted continuously and for specific pollutants, and which were provided in less than a third of the local self-government units.
It is necessary to help local self-governments to develop plans for the care of the population in crisis and emergency situations, because the occurrence of unwanted events (such as floods, mass migrations, chemical spills, and pandemics) is becoming more frequent. The results of this study showed that the participation of public health representatives in the councils resulted in the councils having better access to analyses of health status and indicators of various areas of public health. Establishing good communication between partners at the local level contributes to the improved effectiveness of the activities undertaken.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Figure S1. Locations of the study areas. Numbers refer to the IDs of the municipalities. Table S1. IDs of each municipality and the county to which it belongs in Serbia.
Author Contributions
J.T. and V.M.C. had the original idea for this study and developed the study design and questionnaire in collaboration with M.Ž.-Š.; N.Ć. and S.M. contributed to the dissemination of the questionnaire; V.M.C. analyzed and interpreted the data with J.T. and M.Ž.-Š.; V.M.C., J.T., and M.Ž.-Š. made special contributions by drafting the introduction; M.Ž.-Š. and S.M. drafted the discussion and J.T. drafted the conclusion; V.M.C., J.T., M.Ž.-Š., and N.Ć. critically reviewed the data analysis and contributed to the content when revising and finalizing the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Standing Conference of Towns and Municipalities, Scientific-Professional Society for Disaster Risk Management, Belgrade (https://upravljanje-rizicima.com/, accessed on 16 September 2021) and the International Institute for Disaster Research (https://upravljanje-rizicima.com/medjunarodni-institut-za-istrazivanje-katastrofa/, accessed on 16 September 2021), Belgrade, Serbia.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board of Scientific-Professional Society for Disaster Risk Management and International Institute for Disaster Research (protocol code 001/2022, 7 October 2022).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data is unavailable due to privacy.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Kim, K.; Moody, P.M. More resources better health? A cross-national perspective. Soc. Sci. Med. 1992, 34, 837–842. [Google Scholar] [CrossRef] [PubMed]
- Cvetković, V.; Dragašević, A.; Protić, D.; Janković, B.; Nikolić, N.; Milošević, P. Fire Safety Behavior Model for Residential Buildings: Implications for Disaster Risk Reduction. Int. J. Disaster Risk Reduct. 2022, 75, 102981. [Google Scholar] [CrossRef]
- Cvetković, V.; Nikolić, N.; Ocal, A.; Martinović, J.; Dragašević, A. A Predictive Model of Pandemic Disaster Fear Caused by Coronavirus (COVID-19): Implications for Decision-Makers. Int. J. Environ. Res. Public Health 2022, 19, 652. [Google Scholar] [CrossRef] [PubMed]
- Gatseva, P.D.; Argirova, M. Public Health: The Science of Promoting Health; Springer: Berlin/Heidelberg, Germany, 2011; Volume 19, pp. 205–206. [Google Scholar]
- Rocha, N.P.; Dias, A.; Santinha, G.; Rodrigues, M.; Queirós, A.; Rodrigues, C. Smart cities and public health: A systematic review. Procedia Comput. Sci. 2019, 164, 516–523. [Google Scholar] [CrossRef]
- Rosen, G. A History of Public Health, Revised Expanded ed.; Johns Hopkins University Press: Baltimore, MD, USA, 2015. [Google Scholar]
- Kirmayer, L.J.; Sehdev, M.; Whitley, R.; Dandeneau, S.F.; Isaac, C. Community resilience: Models, metaphors and measures. Int. J. Indig. Health 2009, 5, 62–117. [Google Scholar]
- Ocal, A.; Cvetković, V.; Baytiyeh, H.; Tedim, F.; Zečević, M. Public reactions to the disaster COVID-19: A comparative study in Italy, Lebanon, Portugal, and Serbia. Geomat. Nat. Hazards Risk 2020, 11, 1864–1885. [Google Scholar] [CrossRef]
- Li, W.; Yang, Y.; Liu, Z.-H.; Zhao, Y.-J.; Zhang, Q.; Zhang, L.; Cheung, T.; Xiang, Y.-T. Progression of mental health services during the COVID-19 outbreak in China. Int. J. Biol. Sci. 2020, 16, 1732. [Google Scholar] [CrossRef]
- Nutbeam, D. Health literacy as a public health goal: A challenge for contemporary health education and communication strategies into the 21st century. Health Promot. Int. 2000, 15, 259–267. [Google Scholar] [CrossRef]
- Cvetković, V. The relationship between educational level and citizen preparedness for responding to natural disasters. J. Geogr. Inst. “Jovan Cvijić” SASA 2016, 66, 237–253. [Google Scholar] [CrossRef]
- Cvetković, V.M.; Öcal, A.; Lyamzina, Y.; Noji, E.K.; Nikolić, N.; Milošević, G. Nuclear Power Risk Perception in Serbia: Fear of Exposure to Radiation vs. Social Benefits. Energies 2021, 14, 2464. [Google Scholar] [CrossRef]
- Doherty, T.M.; Del Giudice, G.; Maggi, S. Adult vaccination as part of a healthy lifestyle: Moving from medical intervention to health promotion. Ann. Med. 2019, 51, 128–140. [Google Scholar] [CrossRef]
- Harms-Ringdahl, L. Safety Analysis: Principles and Practice in Occupational Safety; CRC Press: Boca Raton, FL, USA, 2001. [Google Scholar]
- Mekonnen, M.M.; Hoekstra, A.Y. Four billion people facing severe water scarcity. Sci. Adv. 2016, 2, e1500323. [Google Scholar] [CrossRef] [PubMed]
- Cvetković, V.; Nikolić, N.; Nenadić, R.U.; Ocal, A.; Zečević, M. Preparedness and Preventive Behaviors for a Pandemic Disaster Caused by COVID-19 in Serbia. Int. J. Environ. Res. Public Health 2020, 17, 4124. [Google Scholar] [CrossRef]
- Cvetković, V.; Adem, O.; Aleksandar, I. Young adults’ fear of disasters: A case study of residents from Turkey, Serbia and Macedonia. Int. J. Disaster Risk Reduct. 2019, 35. [Google Scholar] [CrossRef]
- Jackson, N.; Waters, E. Criteria for the systematic review of health promotion and public health interventions. Health Promot. Int. 2005, 20, 367–374. [Google Scholar] [CrossRef] [PubMed]
- Glanz, K.; Bishop, D.B. The role of behavioral science theory in development and implementation of public health interventions. Annu. Rev. Public Health 2010, 31, 399–418. [Google Scholar] [CrossRef] [PubMed]
- Hartley, D.M.; Perencevich, E.N. Public health interventions for COVID-19: Emerging evidence and implications for an evolving public health crisis. JAMA 2020, 323, 1908–1909. [Google Scholar] [CrossRef] [PubMed]
- Masters, R.; Anwar, E.; Collins, B.; Cookson, R.; Capewell, S. Return on investment of public health interventions: A systematic review. J. Epidemiol. Community Health 2017, 71, 827–834. [Google Scholar] [CrossRef] [PubMed]
- Bradley, E.H.; Canavan, M.; Rogan, E.; Talbert-Slagle, K.; Ndumele, C.; Taylor, L.; Curry, L.A. Variation in health outcomes: The role of spending on social services, public health, and health care, 2000–2009. Health Aff. 2016, 35, 760–768. [Google Scholar] [CrossRef]
- Papanicolas, I.; Woskie, L.R.; Jha, A.K. Health care spending in the United States and other high-income countries. JAMA 2018, 319, 1024–1039. [Google Scholar] [CrossRef]
- Collins, S.R.; Rasmussen, P.W.; Doty, M.M.; Beutel, S. The Rise in Health Care Coverage and Affordability Since Health Reform Took Effect; The Commonwealth Fund: New York, NY, USA, 2015. [Google Scholar]
- Arrieta, A.; Woods, J.R.; Qiao, N.; Jay, S.J. Cost–benefit analysis of home blood pressure monitoring in hypertension diagnosis and treatment: An insurer perspective. Hypertension 2014, 64, 891–896. [Google Scholar] [CrossRef] [PubMed]
- Kuehl, K.S.; Elliot, D.L.; Goldberg, L.; Moe, E.L.; Perrier, E.; Smith, J. Economic benefit of the PHLAME wellness programme on firefighter injury. Occup. Med. 2013, 63, 203–209. [Google Scholar] [CrossRef] [PubMed]
- Long, D.A.; Sheehan, P. A case study of population health improvement at a Midwest regional hospital employer. Popul. Health Manag. 2010, 13, 163–173. [Google Scholar] [CrossRef] [PubMed]
- Mendivil, J.; García-Altés, A.; Pérez, K.; Marí-Dell’Olmo, M.; Tobías, A. Speed cameras in an urban setting: A cost–benefit analysis. Inj. Prev. 2012, 18, 75–80. [Google Scholar] [CrossRef]
- Reynolds, A.J.; Temple, J.A.; White, B.A.B.; Ou, S.R.; Robertson, D.L. Age 26 cost-benefit analysis of the child-parent center early education program. Child Dev. 2011, 82, 379–404. [Google Scholar] [CrossRef] [PubMed]
- Ludwig, J.; Sanbonmatsu, L.; Gennetian, L.; Adam, E.; Duncan, G.J.; Katz, L.F.; Kessler, R.C.; Kling, J.R.; Lindau, S.T.; Whitaker, R.C. Neighborhoods, obesity, and diabetes—A randomized social experiment. N. Engl. J. Med. 2011, 365, 1509–1519. [Google Scholar] [CrossRef] [PubMed]
- Frank, D.A.; Neault, N.B.; Skalicky, A.; Cook, J.T.; Wilson, J.D.; Levenson, S.; Meyers, A.F.; Heeren, T.; Cutts, D.B.; Casey, P.H. Heat or eat: The Low Income Home Energy Assistance Program and nutritional and health risks among children less than 3 years of age. Pediatrics 2006, 118, e1293–e1302. [Google Scholar] [CrossRef]
- Herd, P.; Schoeni, R.F.; House, J.S. Upstream solutions: Does the supplemental security income program reduce disability in the elderly? Milbank Q. 2008, 86, 5–45. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, R.; Pickett, K. The Spirit Level: Why Equality Is Better for Everyone; Penguin UK, 2010. [Google Scholar]
- Lewis, M. Governance and Corruption in Public Health Care Systems. SSRN Electron. J. 2006. [Google Scholar] [CrossRef]
- Bara, A.-C.; Van den Heuvel, W.J.A.; Maarse, J.A.M. Reforms of health care system in Romania. Croat. Med. J. 2002, 43, 446–452. [Google Scholar]
- Liu, Y. China’s public health-care system: Facing the challenges. Bull. World Health Organ. 2004, 82, 532–538. [Google Scholar]
- Kawachi, I. Social capital for health and human development. Development 2001, 44, 31–35. [Google Scholar] [CrossRef]
- Busse, R.; Riesberg, A.; World Health, O. Health Care Systems in Transition; SAGE Publications Inc.: Berlin, Germany, 2004. [Google Scholar]
- France, G.; Taroni, F.; Donatini, A. The Italian health-care system. Health Econ. 2005, 14, S187–S202. [Google Scholar] [CrossRef]
- MacLean, L.; Edwards, N.; Garrard, M.; Sims-Jones, N.; Clinton, K.; Ashley, L. Obesity, stigma and public health planning. Health Promot. Int. 2009, 24, 88–93. [Google Scholar] [CrossRef] [PubMed]
- Anugwom, E.E. Health promotion and its challenges to public health delivery system in Africa. In Public Health in Developing Countries-Challenges and Opportunities, IntechOpen; 2020. [Google Scholar]
- Brownson, R.C.; Fielding, J.E.; Maylahn, C.M. Evidence-based public health: A fundamental concept for public health practice. Annu. Rev. Public Health 2009, 30, 175–201. [Google Scholar] [CrossRef]
- Brownson, R.C.; Baker, E.A.; Deshpande, A.D.; Gillespie, K.N. Evidence-Based Public Health; Oxford University Press: Oxford, UK, 2017. [Google Scholar]
- Fielding, J.E.; Briss, P.A. Promoting evidence-based public health policy: Can we have better evidence and more action? Health Aff. 2006, 25, 969–978. [Google Scholar] [CrossRef]
- Kickbusch, I. The contribution of the World Health Organization to a new public health and health promotion. Am. J. Public Health 2003, 93, 383–388. [Google Scholar] [CrossRef] [PubMed]
- Cho, H.; Witte, K. Managing fear in public health campaigns: A theory-based formative evaluation process. Health Promot. Pract. 2005, 6, 482–490. [Google Scholar] [CrossRef]
- Boulware, L.E.; Cooper, L.A.; Ratner, L.E.; LaVeist, T.A.; Powe, N.R. Race and trust in the health care system. Public Health Rep. 2003, 118, 358. [Google Scholar] [CrossRef]
- Tabachnick, B.G.; Fidell, L.S.; Ullman, J.B. Using Multivariate Statistics; Pearson: Boston, MA, USA, 2007; Volume 5. [Google Scholar]
Figure 1.
Study areas.
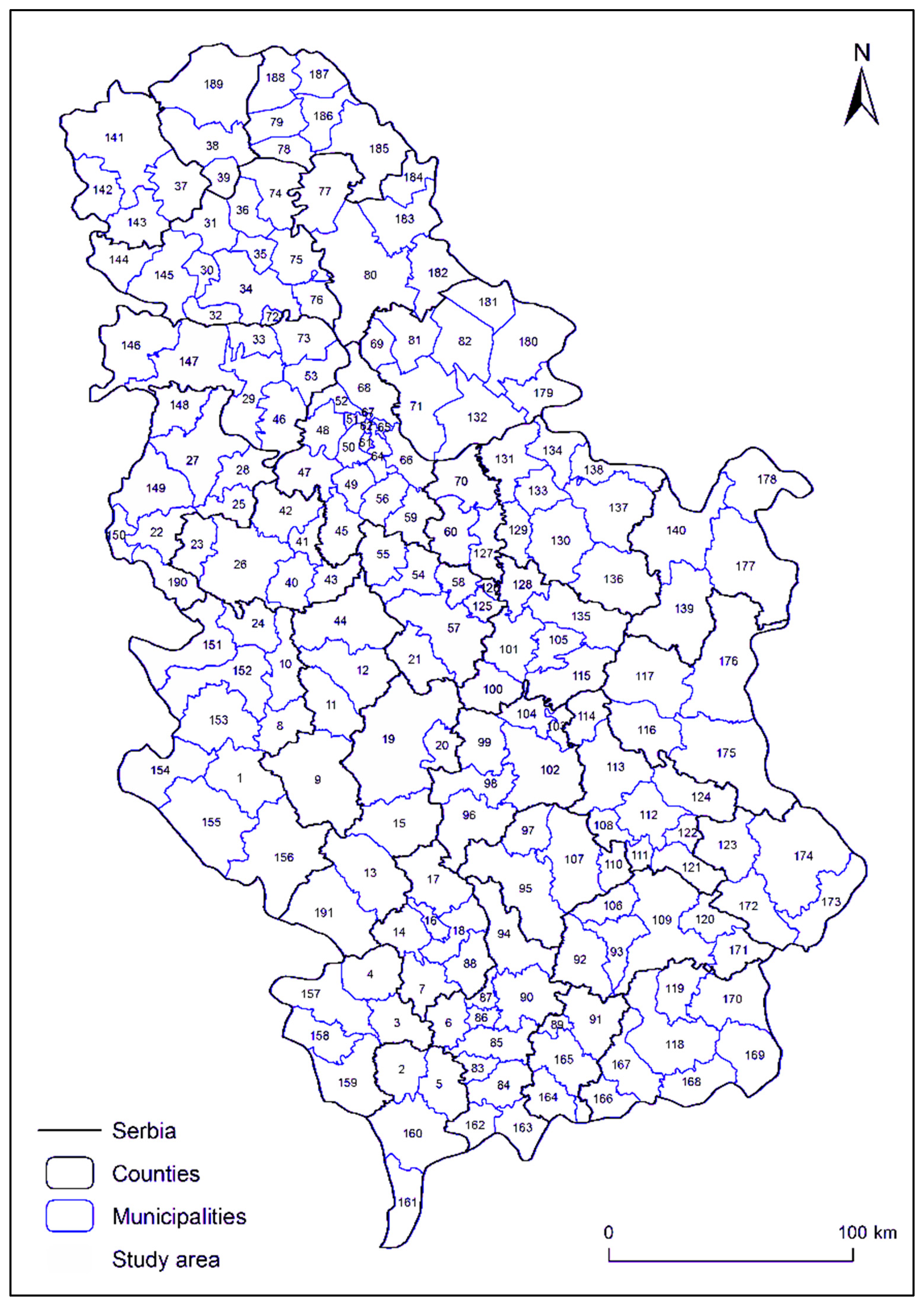
Figure 2.
Percentage distribution of the participation of local self-governments according to their category of development.
Figure 2.
Percentage distribution of the participation of local self-governments according to their category of development.
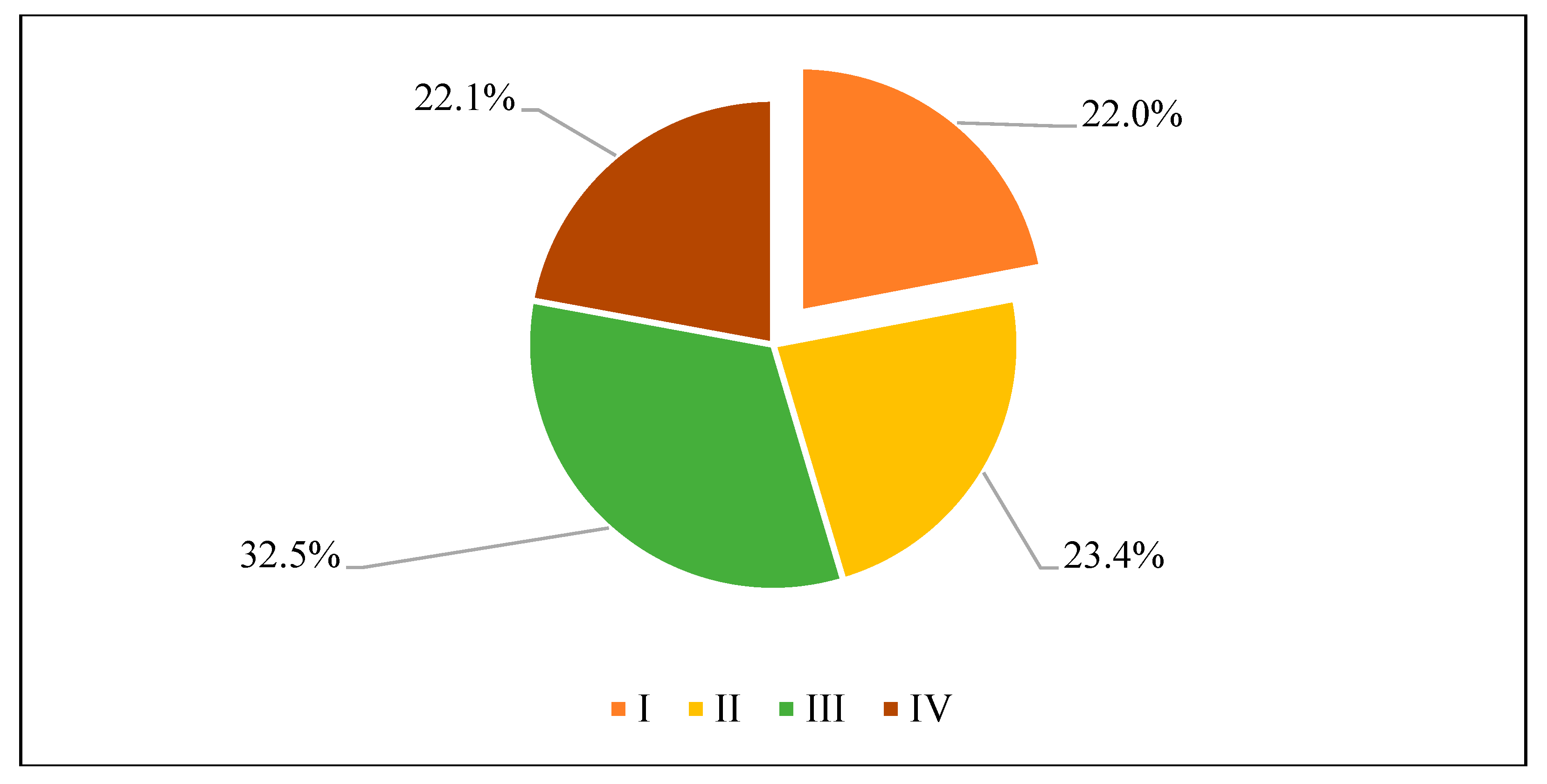
Figure 3.
Percentages of local governments that participated in the promotion of healthy lifestyles, 2019–2021.
Figure 3.
Percentages of local governments that participated in the promotion of healthy lifestyles, 2019–2021.
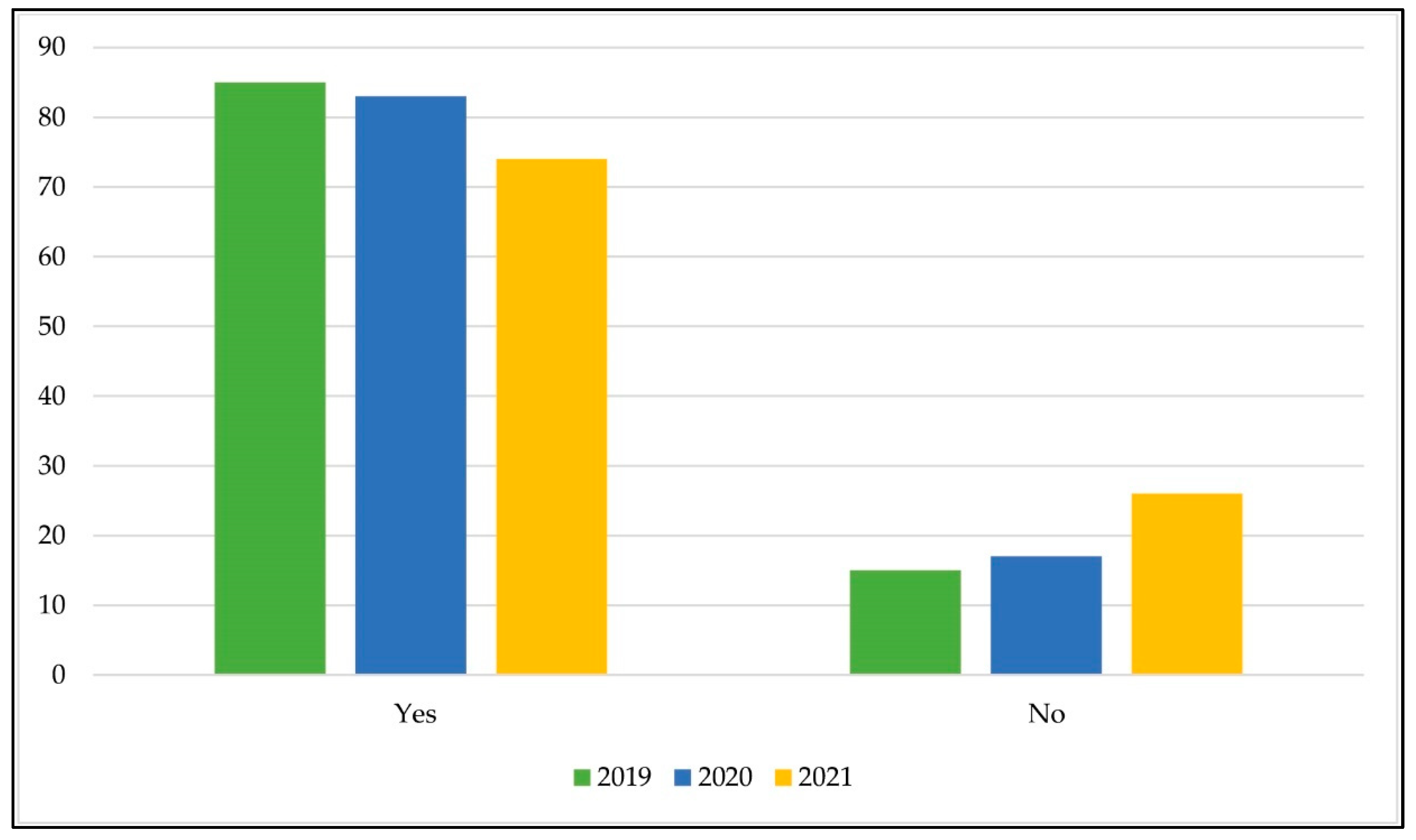
Figure 4.
Participation of local self-government partners in community campaigns, expressed as percentages, 2019–2021.
Figure 4.
Participation of local self-government partners in community campaigns, expressed as percentages, 2019–2021.
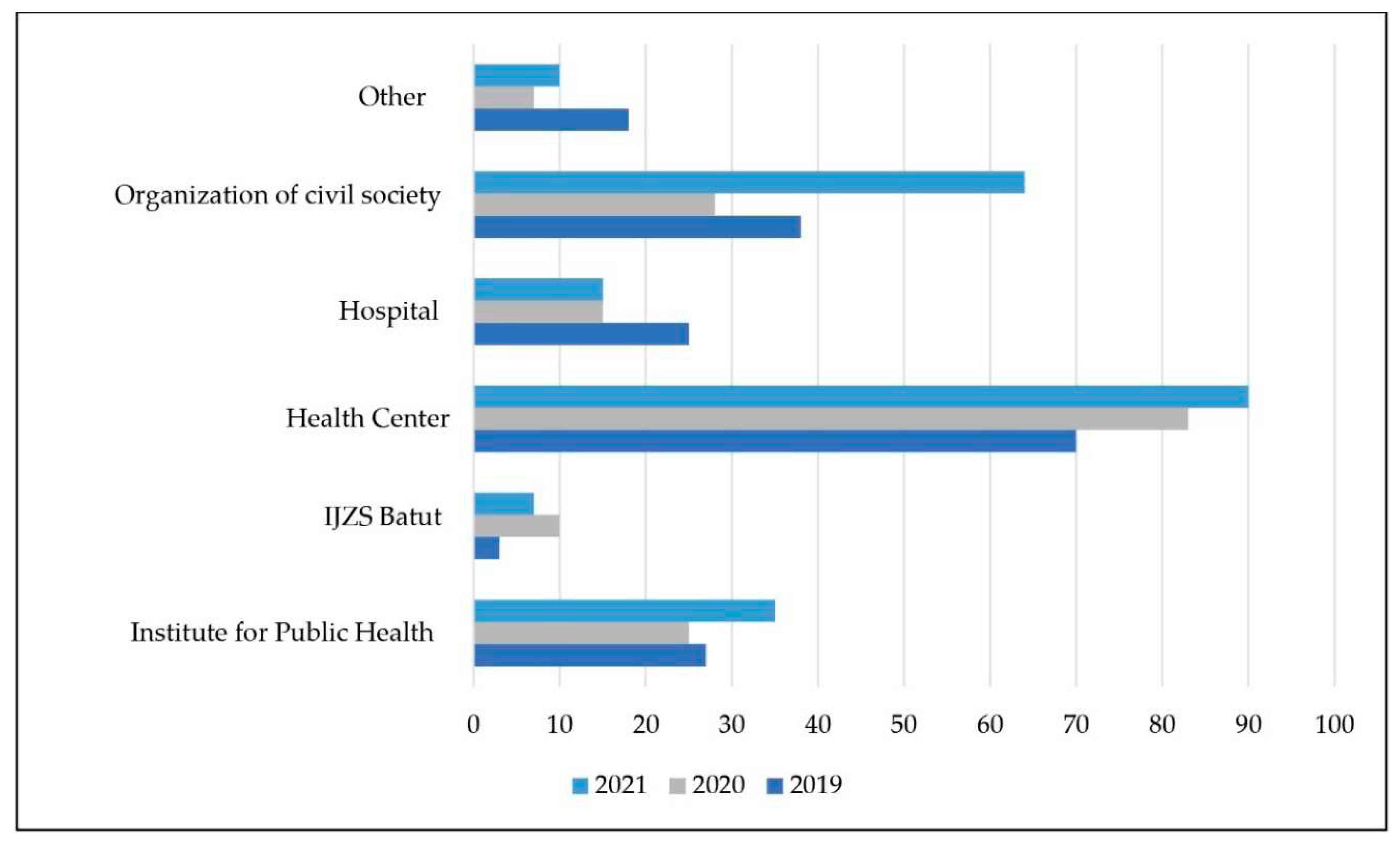
Figure 5.
Content participation in community campaigns/promotion, expressed as percentages, 2020–2021.
Figure 5.
Content participation in community campaigns/promotion, expressed as percentages, 2020–2021.
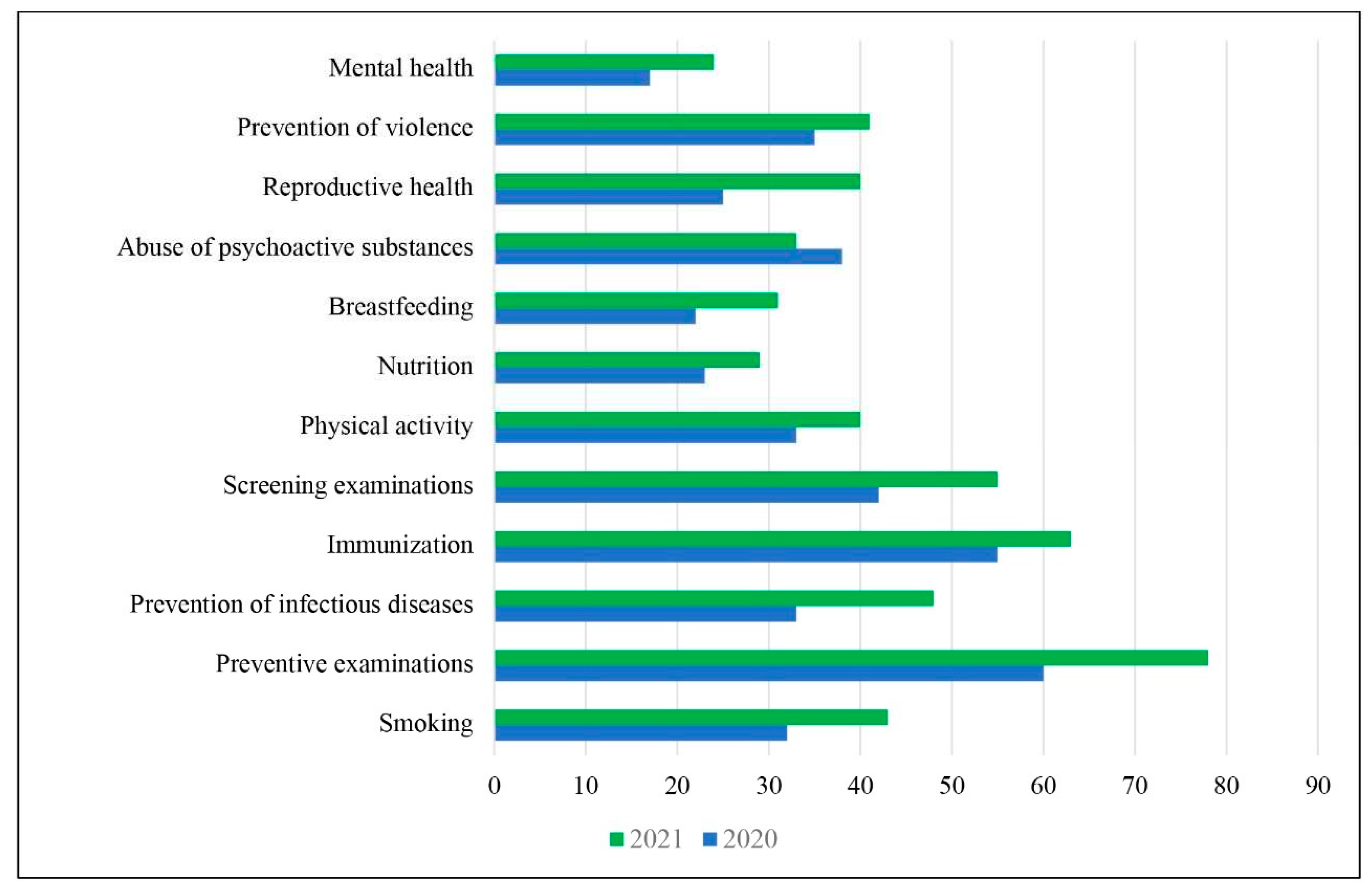
Table 1.
Cities and municipalities by region.
| City/Municipality by Region | |||
|---|---|---|---|
| Vojvodina | Beograd | Južna i Istočna Srbija | Šumadija i Zapadna Srbija |
| Sombor | Barajevo | Bor | Grad Užice |
| Kula | Zvezdara | Požarevac | Sevojno |
| Odžaci | Zemun | Veliko Gradište | Kosjerić |
| Bela Crkva | Mladenovac | Žabari | Nova Varoš |
| Opovo | Čukarica | Malo Crniće | Lajkovac |
| Plandište | Zaječar | Ub | |
| Novi Sad | Boljevac | Paraćin | |
| Bač | Sokobanja | Svilajnac | |
| Bačka Palanka | Bojnik | Kruševac | |
| Vrbas | Medveđa | Ćićevac | |
| Bečej | Crna Trava | Varvarin | |
| Srbobran | Niš–Niška Banja | Trstenik | |
| Titel | Aleksinac | Novi Pazar | |
| Sremski Karlovci | Gadžin Han | Raška | |
| Kikinda | Ražanj | Kragujevac | |
| Ada | Smederevo | Aranđelovac | |
| Kanjiža | Velika Plana | Batočina | |
| Subotica | Smederevska Palanka | Lapovo | |
| Mali Iđoš | Dimitrovgrad | Topola | |
| Zrenjanin | Bujanovac | Šabac | |
| Novi Bečej | Vladičin Han | Ljubovija | |
| Šid | Blace | Ivanjica | |
| Ruma | Kuršumlija | Lučani | |
| Pećinci | |||
| Inđija | |||
Table 2.
Distribution of planning documents reported among local self-government units.
| Planning Documents | Category | N | % |
|---|---|---|---|
| Public health plan | Yes | 26 | 33.8 |
| No | 51 | 66.2 | |
| Local action plan for young people | Yes | 38 | 49.4 |
| No | 39 | 50.6 | |
| Local action plan for environmental protection | Yes | 25 | 32.5 |
| No | 52 | 67.5 | |
| Local waste management action plan | Yes | 31 | 40.3 |
| No | 46 | 59.7 | |
| Local action plan for monitoring and improving air quality | Yes | 11 | 14.3 |
| No | 66 | 85.7 | |
| Local action plan for Roma | Yes | 33 | 42.9 |
| No | 44 | 57.1 | |
| City/municipality social protection strategy | Yes | 33 | 42.9 |
| No | 44 | 57.1 | |
| Program for the improvement of social protection | Yes | 14 | 18.2 |
| No | 63 | 81.8 | |
| Local action plan for the disabled | Yes | 7 | 9.1 |
| No | 70 | 90.9 | |
| Local action plan for HIV/AIDS prevention | Yes | 1 | 1.3 |
| No | 76 | 98.7 | |
| Local action plan for the improvement of mental health | Yes | 1 | 1.3 |
| No | 76 | 98.7 | |
| Local action plan for the prevention of abuse of psychoactive substances | Yes | 1 | 1.3 |
| No | 76 | 98.7 |
Table 3.
Percentages of local governments that adopted planning documents from 2019 to 2021.
| Planning Documents | 2019 | 2020 | 2021 |
|---|---|---|---|
| Public health plan | 23.4 | 25.0 | 33.8 |
| Local action plan for young people | No data | No data | 49.4 |
| Local action plan for environmental protection | No data | 26.7 | 32.5 |
| Local waste management action plan | No data | No data | 40.3 |
| Local action plan for monitoring and improving air quality | No data | No data | 14.3 |
| Local action plan for Roma | 41.5 | 40.0 | 42.9 |
| City/municipality social protection strategy | 33.0 | 31.7 | 42.9 |
| Program for the improvement of social protection | 24.5 | 15.0 | 18.2 |
| Local action plan for the disabled | 8.5 | 8.3 | 9.1 |
| Local action plan for HIV/AIDS prevention | 0.0 | 1.7 | 1.3 |
| Local action plan for the improvement of mental health | 8.5 | 3.3 | 1.3 |
| Local action plan for the prevention of abuse of psychoactive substances | 3.2 | 5.0 | 1.3 |
Table 4.
Effectiveness of public health plans, in terms of the commitment of local self-government units’ program budgets for program activities in the field of public health.
Table 4.
Effectiveness of public health plans, in terms of the commitment of local self-government units’ program budgets for program activities in the field of public health.
| Percentage of Realization | N | % |
|---|---|---|
| ≤70% | 8 | 10.3 |
| 71–80% | 6 | 7.8 |
| 81–90% | 10 | 12.8 |
| 91–95% | 6 | 7.6 |
| ≥95% | 48 | 61.5 |
Table 5.
Overview of the results regarding the descriptive statistics for variables related to social care for the public health of the city/municipality in the area of health promotion and disease prevention in 2021 (social activities and health).
Table 5.
Overview of the results regarding the descriptive statistics for variables related to social care for the public health of the city/municipality in the area of health promotion and disease prevention in 2021 (social activities and health).
| Variable | N | % | |
|---|---|---|---|
| Participation of local self-government units in public health promotion campaigns | Yes | 57 | 74 |
| No | 20 | 26 | |
| Partners in public health promotion campaigns | Community Health center | 52 | 89.7 |
| Civil society organizations | 37 | 63.8 | |
| Competent Institute for Public Health | 20 | 34.5 | |
| Hospitals | 9 | 15.5 | |
| IJS Batut | 4 | 6.9 | |
| Red Cross | 6 | 10.2 | |
| Realized campaigns/promotions | Preventive examinations | 45 | 77.6 |
| Immunization | 37 | 63.8 | |
| Screening examinations | 32 | 55.2 | |
| Prevention of infectious diseases | 28 | 48.3 | |
| Smoking reduction | 25 | 43.1 | |
| Physical activity | 23 | 39.7 | |
| Prevention of violence | 24 | 41.4 | |
| Reproductive health | 23 | 39.7 | |
| Prevention of the abuse of psychoactive substances | 19 | 32.8 | |
| Breastfeeding | 18 | 31 | |
| Nutrition | 17 | 29.3 | |
| Mental health | 14 | 24.1 | |
| Methods of participation by local self-government units in campaigns/promotions | Space | 49 | 65.3 |
| Media support | 48 | 64 | |
| Personal participation by representatives of local self-government units | 43 | 57.3 | |
| Printing materials | 16 | 21.3 | |
| Transportation | 8 | 10.7 | |
| Diaries | 2 | 2.7 | |
| Cooperation of the council with the Headquarters for Emergency Situations during COVID-19 | Yes | 42 | 54.5 |
| No | 35 | 45.5 | |
| The manner of the council’s cooperation with the Headquarters for Emergency Situations | Contact with donors | 4 | 8.7 |
| Assistance in the procurement, storage, or distribution of protective equipment | 16 | 34.8 | |
| Participation in the recruitment of volunteers | 11 | 23.9 | |
| Cooperation with the Red Cross | 26 | 56.5 | |
| Informing the population | 30 | 65.2 | |
| Organization of immunization | 27 | 58.7 | |
| Representatives of the Headquarters attended the council and gave recommendations for pest control in the city | 1 | 2.2 | |
Table 6.
Overview of the results of the descriptive statistics for environmental and health variables in 2021 (environment, communal activities).
Table 6.
Overview of the results of the descriptive statistics for environmental and health variables in 2021 (environment, communal activities).
| Variable | N | % | |
|---|---|---|---|
| Available analyses of environmental indicators | Yes | 33 | 42.9 |
| No | 44 | 57.1 | |
| The health council made proposals for the improvement of the environment | Yes | 9 | 11.7 |
| No | 68 | 88.3 | |
| Drinking water factory, water processing plant | Yes | 44 | 57.1 |
| No | 33 | 42.9 | |
| Possession of zones of sanitary protection of sources for water supply | Yes | 60 | 77.9 |
| No | 17 | 22.1 | |
| A map/diagram of the water supply system, sources, and distribution network was created | Yes | 51 | 66.2 |
| No | 16 | 20.8 | |
| In procedure | 10 | 13 | |
| Asbestos pipes in the water supply network | Yes | 27 | 35.1 |
| No | 50 | 64.9 | |
| Lead pipes in the water supply network | Yes | 8 | 10.4 |
| No | 69 | 89.6 | |
| Existence of a Water Network Reconstruction Plan | Yes | 56 | 72.7 |
| No | 21 | 27.3 | |
| Existence of wastewater treatment plants | Yes | 26 | 33.8 |
| No | 51 | 66.2 | |
| Control of drinking water samples from the so-called village waterworks | Yes | 43 | 55.8 |
| No | 34 | 44.4 | |
| Control of samples for drinking from public fountains with their own source of water | Yes | 48 | 62.3 |
| No | 29 | 37.7 | |
| A register of septic and collecting pits was established | Yes | 4 | 5.2 |
| No | 73 | 94.8 | |
| Performing air control measures | Yes | 65 | 45.5 |
| No | 41 | 53.2 | |
| Air quality monitoring station part | State monitoring networks | 4 | 5.2 |
| Local networks for monitoring | 20 | 26 | |
| Both | 12 | 15.6 | |
| Incentive measures for renewable energy in 2021 | Subsidies for thermal insulation of residential buildings | 31 | 41.3 |
| Subsidies for thermal insulation of public buildings (schools/kindergartens/cultural institutions/sports facilities/PE) | 19 | 25.3 | |
| Subsidies for gas/pellet boilers | 24 | 32 | |
| Procurement of electric vehicles for public transport | 0 | 0 | |
| Construction of traffic bypasses | 6 | 8 | |
| Municipal waste dump | Yes | 56 | 72.7 |
| No | 20 | 26 | |
| Landfill location | Less than 1000 m | 20 | 26 |
| More than 1000 m | 37 | 48.1 | |
| Disinfection, disinsection, and pest control of public areas and buildings | Yes | 62 | 80.5 |
| No | 13 | 16.9 | |
| Percentage of households connected to the water supply system of a public utility company (analysis of results) | Up to 30% | 3 | 3.9 |
| From 31 to 50% | 8 | 10.4 | |
| From 51% to 70% | 12 | 15.6 | |
| From 71% to 90% | 14 | 18.2 | |
| Over 91% | 40 | 51.9 | |
| Percentage of households connected to the water supply system | Up to 3000 connections | 27 | 35.1 |
| From 3001 to 5000 | 17 | 22.1 | |
| From 5001 to 10,000 | 9 | 11.7 | |
| From 10,001 to 20,000 | 12 | 15.6 | |
| From 20,001 to 50,000 | 10 | 13 | |
| Over 50,001 connections | 2 | 2.6 | |
| Percentage of households connected to the sewage system | Up to 1000 connections | 29 | 37.7 |
| From 1001 to 3000 | 15 | 19.5 | |
| From 3001 to 6000 | 12 | 15.6 | |
| From 6001 to 10,000 | 7 | 9.1 | |
| From 10,001 to 20,000 | 6 | 7.8 | |
| Over 20,001 connections | 8 | 10.4 | |
| Percentage of households connected to district heating | Up to 1% | 43 | 55.8 |
| Up to 5% | 9 | 11.7 | |
| Up to 10% | 6 | 7.8 | |
| Up to 25% | 10 | 13 | |
| Up to 50% | 5 | 6.5 | |
| Over 51% | 4 | 5.2 | |
| Percentage of microbiologically defective samples of drinking water from the PUK/JP water supply system | M = 4.48 | ||
| Percentage of physico-chemically defective samples of drinking water from the water supply system of PUK/JP | M = 18.39 | ||
| Percentage of microbiologically defective drinking water samples from the so-called rural waterworks (small waterworks that supply more than five households in rural areas) | M = 6.36 | ||
| Percentage of physically and chemically defective drinking water samples from the so-called rural waterworks (small waterworks that supply more than 5 households in rural areas) | M = 16.28 | ||
| Percentage of microbiologically defective samples of drinking water from public taps with their own source of water (e.g., captured spring, bore well, artesian well) | M = 9.3 | ||
| Percentage of physico-chemically defective samples of drinking water from public taps with their own source of water (e.g., captured spring, bore well, artesian well) | M = 10.89 | ||
| Percentage of microbiologically defective samples of drinking water from rural schools | M = 3.07 | ||
| Percentage of physico-chemically defective samples of drinking water from rural schools | M = 11.53 | ||
| Percentage of unsatisfactory analyses of wastewater samples | M = 28.65 | ||
| The percentage of septic and collecting pits that are regularly emptied in a professional manner, i.e., by PUK/JP and licensed companies | M = 9.41 | ||
| The number of permanent measuring points for air quality monitoring in local self-government units | S02 − M = 0.76 | ||
| Čađ − M = 0.71 | |||
| N02 − M = 0.34 | |||
| PM10 − M = 0.21 | |||
| PM25 − M = 0.19 | |||
| Number of air samples on an annual basis (from all permanent measuring points) | S02 − M = 114 | ||
| Čađ − M = 109 | |||
| N02 − M = 117 | |||
| PM10 − M = 104 | |||
| PM25 − M = 49.36 | |||
| The number of days in a year with a concentration of measured pollutants in the air higher than the permitted one | S02 − M = 2.66 | ||
| Čađ − M = 5.70 | |||
| N02 − M = 2.97 | |||
| PM10 − M = 11.42 | |||
| PM25 − M = 8.41 | |||
| The number of extinguished individual solid fuel burners in 2021 | M = 25.09 | ||
| Areas forested in local self-government units in 2021 | M = 10,346 ha | ||
| The number of landfills in local self-government units in 2021 | M = 9.05 | ||
| The number of sanitary landfills in local self-government units in 2021 | M = 0.31 | ||
| The number of wild controlled landfills in local self-government units in 2021 | M = 11.68 | ||
| The number of wild uncontrolled landfills in local self-government units in 2021 | M = 10.32 | ||
| Number of mosquito disinsections carried out | M = 4 | ||
Table 7.
Percentage of health councils with access to environmental indicator analyses and percentages of health councils that provided proposals for improving environmental indicators, 2019–2021.
Table 7.
Percentage of health councils with access to environmental indicator analyses and percentages of health councils that provided proposals for improving environmental indicators, 2019–2021.
| Variable | 2019 | 2020 | 2021 | |
| Available analyses of environmental indicators | Yes | 43.6 | 45.0 | 42.9 |
| No | 56.4 | 55.0 | 57.1 | |
| The health council made proposals for the improvement of the environment | Yes | 26.6 | 21.7 | 11.7 |
| No | 73.4 | 78.3 | 88.3 | |
Table 8.
Comparative analysis of selected variables (percentage of local self-government units that had a water plant, water system map, asbestos and lead pipes in their water supply networks, a water supply network reconstruction plan, or a wastewater treatment plant), 2019–2021.
Table 8.
Comparative analysis of selected variables (percentage of local self-government units that had a water plant, water system map, asbestos and lead pipes in their water supply networks, a water supply network reconstruction plan, or a wastewater treatment plant), 2019–2021.
| Variable | 2019 | 2020 | 2021 | |
|---|---|---|---|---|
| Drinking water factory, water processing plant | Yes | 47.9 | 48.3 | 57.1 |
| No | 52.1 | 51.7 | 42.9 | |
| A map/diagram of the water supply system, sources, and distribution network was created | Yes | 38.3 | 53.3 | 66.2 |
| No | 23.4 | 16.7 | 20.8 | |
| In procedure | 38.3 | 30.0 | 13 | |
| Asbestos pipes in the water supply network | Yes | 85.1 | 86.0 | 35.1 |
| No | 14.9 | 14.0 | 64.9 | |
| Lead pipes in the water supply network | Yes | / | 18.2 | 10.4 |
| No | / | 81.8 | 89.6 | |
| Existence of a Water Network Reconstruction Plan | Yes | 74.5 | 70.0 | 72.7 |
| No | 25.5 | 30.0 | 27.3 | |
| Existence of wastewater treatment plants | Yes | 26.6 | 30.0 | 33.8 |
| No | 73.4 | 70.0 | 66.2 | |
Table 9.
Overview of the results of descriptive statistics for variables related to the working environment and health of the population in 2021 (safety and health at work, inspection activities).
Table 9.
Overview of the results of descriptive statistics for variables related to the working environment and health of the population in 2021 (safety and health at work, inspection activities).
| Variable | N | % | |
|---|---|---|---|
| Possessed data on injuries to employees that occurred on the territories of local self-government units | Yes | 16 | 20.8 |
| No | 59 | 76.6 | |
| Existence of a system for monitoring workplace injuries and occupational diseases | Yes | 15 | 19.5 |
| No | 60 | 77.9 | |
| Procurement of individual protective equipment | Protective masks | 69 | 92 |
| Gloves | 57 | 76 | |
| Disinfectants | 71 | 94.7 | |
| Other protective means | 1 | 1.3 | |
| The number of reports to labor inspection authorities regarding safety and health protection at work | There were no applications | 12 | 5.4 |
| Up to 5 applications | 4 | 5.2 | |
| 37 applications | 1 | 1.3 | |
| 39 applications | 2 | 2.6 | |
| They have no access | 56 | 71.8 | |
Table 11.
Overview of the results of descriptive statistics for variables related to the organization and functioning of the health system (healthcare, social activity).
Table 11.
Overview of the results of descriptive statistics for variables related to the organization and functioning of the health system (healthcare, social activity).
| Variable | N | % | ||
|---|---|---|---|---|
| The founding rights of the Health Center were transferred to the Ministry of Health/APV | Yes | 66 | 85.7 | |
| No | 11 | 14.3 | ||
| Existence of an Adviser for the Protection of Patients’ Rights | Yes | 70 | 90.9 | |
| No | 6 | 7.8 | ||
| The counselor had an official identification card issued by the Ministry of Health | Yes | 54 | 70.1 | |
| No | 22 | 28.6 | ||
| Existence of a separate room where the Counselor received patients | Yes | 34 | 44.2 | |
| No | 41 | 53.2 | ||
| Certainty regarding the working hours of the advisor | No | 29 | 37.7 | |
| Yes | 23 | 29.9 | ||
| Optionally | 24 | 31.2 | ||
| The advisor only worked to protect the rights of patients | Yes | 5 | 6.5 | |
| No | 65 | 84.4 | ||
| Yes, within the service for the protection of patients’ rights | 5 | 6.5 | ||
| Employees who protected the rights of patients received a salary supplement for performing these tasks | Yes | 10 | 13 | |
| No | 66 | 85.7 | ||
| Public transport was available from surrounding towns to the center | Yes | 53 | 68.8 | |
| No | 16 | 20.8 | ||
| Partially | 8 | 10.4 | ||
| Emergency medical assistance was provided by a separate organizational unit | Yes | 41 | 53.2 | |
| No | 36 | 46.8 | ||
| Local self-government units participated in the organization of special COVID clinics/temporary hospitals | Yes | 66 | 85.7 | |
| No | 10 | 13 | ||
| Ways in which assistance was provided | Organization of temporary hospitals | 9 | 14.3 | |
| Financing of additional personnel | 22 | 34.9 | ||
| Provision of additional facilities/space for testing/examination points | 38 | 60.3 | ||
| Provided transportation for patients and healthcare workers | 18 | 28.6 | ||
| Procurement of ambulances for health institutions | 13 | 20.6 | ||
| Procurement of personal protective equipment for health institutions | 35 | 55.6 | ||
| Procurement of disinfectants | 42 | 66.7 | ||
| The total number of executors employed in protecting the rights of patients in local self-government units | Zero | 5 | 6.4 | |
| One | 65 | 83.3 | ||
| Two | 2 | 2.6 | ||
| The number of applications in 2021 made regarding the adviser for the protection of patients’ rights | M = 9.41 | |||
| Number of health centers in local self-government units | Zero | 0 | 0 | |
| Up to 5 | 44 | 89,8 | ||
| 6–10 | 3 | 6,12 | ||
| Over 11 | 2 | 4,08 | ||
| The number of clinics in local self-government units | Up to 10 | 54 | 73,97 | |
| 11–20 | 12 | 16,44 | ||
| 21–30 | 3 | 4,11 | ||
| Over 31 | 4 | 5,48 | ||
Table 12.
Number of inhabitants per doctor by region (RZS, 2019–2020).
| Region | Number of Inhabitants per Doctor | ||
|---|---|---|---|
| 2018 | 2019 | 2020 | |
| Beograd | 288 | 285 | 286 |
| Vojvodina | 397 | 445 | 399 |
| Šumadija i Zapadna Srbija | 389 | 388 | 371 |
| Južna i Istočna Srbija | 335 | 333 | 329 |
| Serbia | 349 | 349 | 343 |
Table 13.
Overview of the results of descriptive statistics for variables related to dealing with emergency situations (social activities, health, emergency headquarters) in 2021.
Table 13.
Overview of the results of descriptive statistics for variables related to dealing with emergency situations (social activities, health, emergency headquarters) in 2021.
| Variable | N | % | |
|---|---|---|---|
| Local plan for taking care of the health of the population in emergency situations | Yes | 16 | 20.8 |
| No | 60 | 79.2 | |
| Plan prepared for the protection and rescue of the population in emergency situations | Yes | 40 | 51.9 |
| No | 11 | 14.3 | |
| In procedure | 26 | 33.8 | |
| Exercises and training realized in the field of first aid | Yes | 33 | 42.9 |
| No | 44 | 57.1 | |
| Exercise organizer | Local self-government unit | 5 | 12.2 |
| Red Cross | 16 | 39 | |
| Organization of civil society | 2 | 4.9 | |
| MUP | 8 | 19.5 | |
| Cooperation of the Emergency Situations Headquarters with the local self-government units | Health council | 27 | 36 |
| Health institutions | 68 | 90.7 | |
| Sanitary inspection | 50 | 66.7 | |
| MUP | 62 | 82.7 | |
| Communal police | 29 | 38.7 | |
| Red Cross | 56 | 74.7 | |
| Organized a “call center” for immunization during COVID-19 | Yes | 56 | 76.6 |
| No | 17 | 22.1 | |
| Means of providing immunization for vulnerable groups | Call center | 52 | 69.3 |
| Through the local community | 40 | 53.3 | |
| Volunteers | 37 | 49.3 | |
| Through the Center for Social Work | 17 | 22.7 | |
| We do not have special activities towards vulnerable groups | 7 | 9.3 | |
| Professional operational team for immunization of COVID-19 formed | Yes | 33 | 42.9 |
| No | 43 | 55.8 | |
| Transportation of the population for immunization | Yes | 28 | 36.4 |
| No | 47 | 61 | |
| Cooperation with health institutions (Likert scale) | 1 | 0 | 0 |
| 2 | 0 | 0 | |
| 3 | 3 | 3.9 | |
| 4 | 20 | 26 | |
| 5 | 51 | 66.2 | |
| Number of first aid training programs related to responding in emergency and crisis situations | M = 1.56 | ||
| Number of mandated fines issued for violating the decisions of the crisis headquarters in 2021 | M = 29.6 | ||
| Number of media statements/campaigns on the topic of immunization against COVID-19 | M = 74.82 | ||
| Number of immunization points available in local self-government units | M = 3.11 | ||
Table 14.
Percentage of local self-governments that had a local plan for taking care of the health of the population in crisis and emergency situations and a prepared rescue plan for emergency situations, 2019–2021.
Table 14.
Percentage of local self-governments that had a local plan for taking care of the health of the population in crisis and emergency situations and a prepared rescue plan for emergency situations, 2019–2021.
| Variable | 2019 | 2020 | 2021 | |
|---|---|---|---|---|
| Local plan for taking care of the health of the population in emergency situations | Yes | 27.7 | 10.0 | 20.8 |
| No | 59.6 | 90.0 | 79.2 | |
| In process | 12.8 | |||
| Prepared plan for protection and rescue in emergency situations | Yes | 54.3 | 73.3 | 51.9 |
| No | 19.1 | 8.3 | 14.3 | |
| In process | 26.6 | 18.3 | 33.8 | |
Table 15.
Results of the chi-squared test regarding the relationship between the formation of a health council and selected variables.
Table 15.
Results of the chi-squared test regarding the relationship between the formation of a health council and selected variables.
| Variable | Sig. (2-Tailed) |
df | X2 |
|---|---|---|---|
| The adoption of a Work Plan for 2022 | 0.000 ** | 12 | 81.81 |
| The adoption of a Public Health Plan | 0.000 ** | 16 | 84.81 |
| Receiving help from the Standing Conference of Towns and Municipalities in the process of developing the plan | 0.000 ** | 8 | 81.01 |
| Type of assistance provided by the Standing Conference of Towns and Municipalities in the process of developing the plan | 0.000 ** | 16 | 54.40 |
| Drafting of a public health plan | 0.000 ** | 8 | 81.36 |
| Representative of the institute in the council | 0.000 ** | 12 | 86.83 |
| Attendance of representatives at sessions | 0.000 ** | 12 | 46.35 |
| Access to analyses of the state of health of local self-government units | 0.000 ** | 12 | 51.51 |
| Having identified vulnerable groups | 0.000 ** | 8 | 42.87 |
| Access to public health risk assessments of local self-government units | 0.002 * | 12 | 31.65 |
| Availability of inspection reports | 0.000 ** | 25 | 94.66 |
| Instituting campaigns promoting healthy lifestyles | 0.000 ** | 8 | 80.24 |
| Means of supporting campaigns | 0.000 ** | 28 | 196.44 |
| Cooperation with the Headquarters for Emergency Situations | 0.000 ** | 12 | 88.34 |
| Availability of analyses of environmental indicators | 0.000 ** | 8 | 80.521 |
| Making proposals for improving life indicators | 0.000 ** | 8 | 87.12 |
| Zones of sanitary protection for the water supply | 0.000 ** | 12 | 80.73 |
| Creation of a map/diagram of the water supply system was created | 0.000 ** | 20 | 85.04 |
| Having a plan for the reconstruction of the water supply network | 0.000 ** | 8 | 80.26 |
| Having a wastewater treatment plant | 0.000 ** | 8 | 80.24 |
| Having a register of septic and collecting pits | 0.000 ** | 8 | 39.05 |
| Performing air control measures | 0.000 ** | 8 | 43.51 |
| Having a municipal waste dump | 0.005* | 6 | 56.51 |
| Availability of data on employee injuries | 0.000 ** | 8 | 31–73 |
| Availability of a system for monitoring work injuries | 0.000 ** | 8 | 29.85 |
| Having a counselor for the protection of patient rights | 0.000 ** | 8 | 46.59 |
| Having a local emergency healthcare plan | 0.000 ** | 8 | 41.04 |
| Having a protection and rescue plan | 0.000 ** | 12 | 83.95 |
| Conducting exercises and education in the field of first aid | 0.000 ** | 8 | 79.90 |
* p ≤ 0.05; ** p ≤ 0.01.
Table 16.
Results of the chi-squared tests of the relationship between local self-government units’ development categories and selected variables.
Table 16.
Results of the chi-squared tests of the relationship between local self-government units’ development categories and selected variables.
| Variable | Sig. (2-Tailed) |
df | X2 |
|---|---|---|---|
| The council adopted a Work Plan for 2022 | 0.000 ** | 12 | 84.42 |
| The council adopted a public health plan | 0.000 ** | 16 | 86.53 |
| Received help from the Standing Conference of Towns and Municipalities in the process of developing the plan | 0.000 ** | 8 | 80.64 |
| Type of assistance received from the Standing Conference of Towns and Municipalities in the process of developing the plan | 0.000 ** | 16 | 50.69 |
| Drafting of a public health plan with help | 0.000 ** | 8 | 86.01 |
| Presence of a representative of the competent institution on the council | 0.000 ** | 12 | 82.25 |
| Attendance of representatives at sessions | 0.000 ** | 12 | 47.38 |
| Access to analyses of the state of health of local self-government units (3 years) | 0.000 ** | 12 | 47.75 |
| Having identified vulnerable groups | 0.000 ** | 8 | 54.84 |
| Access to public health risk assessments of local self-government units | 0.000 ** | 8 | 82.85 |
| Availability of inspection reports | 0.027 * | 12 | 23.05 |
| Instituting campaigns promoting healthy lifestyles | 0.001 ** | 8 | 84.54 |
| Means of supporting campaigns | 0.198 | 34 | 48.51 |
| Cooperation of the council with the Headquarters for Emergency Situations | 0.000 ** | 12 | 82.39 |
| Availability of analyses of environmental indicators | 0.000 ** | 8 | 83.14 |
| Creation of proposals for improving life indicators | 0.000 ** | 8 | 84.06 |
| Having zones of sanitary protection for the water supply | 0.000 ** | 12 | 85.42 |
| Having a map/diagram of the water supply system | 0.000 ** | 20 | 93.54 |
| Having a plan for the reconstruction of the water supply network | 0.000 ** | 8 | 87.48 |
| Having a wastewater treatment plant | 0.000 ** | 8 | 90.64 |
| Having a register of septic and collecting pits | 0.000 ** | 8 | 41.29 |
| Performing air control measures | 0.000 ** | 8 | 55.29 |
| Having a municipal waste dump | 0.000 ** | 7 | 67.29 |
| Access to data on employee injuries | 0.000 ** | 8 | 30.32 |
| Having a system for monitoring work injuries | 0.000 ** | 8 | 30.28 |
| Having a counselor for the protection of patient rights | 0.000 ** | 8 | 47.84 |
| Having a local emergency healthcare plan | 0.000 ** | 8 | .43.66 |
| Having a protection and rescue plan | 0.000 ** | 12 | 80.98 |
| Conducting exercises and education in the field of first aid | 0.000 ** | 8 | 78.53 |
* p ≤ 0.05; ** p ≤ 0.01.
Table 18.
Results of the chi-squared test of the relationship between having a prepared public health risk assessment study and selected variables.
Table 18.
Results of the chi-squared test of the relationship between having a prepared public health risk assessment study and selected variables.
| Variable | Sig. (2-Tailed) |
df | X2 |
|---|---|---|---|
| The council adopted a Work Plan for 2022 | 0.065 | 9 | 16.35 |
| The council adopted a public health plan | 0.031 * | 12 | 22.64 |
| Received help from the Standing Conference of Towns and Municipalities in the process of developing the plan | 0.012 * | 6 | 16.37 |
| Type of assistance received from the Standing Conference of Towns and Municipalities in the process of developing the plan | 0.147 | 12 | 17.06 |
| Drafting of a public health plan | 0.007 ** | 6 | 17.79 |
| Presence of a representative of the competent institution on the council | 0.051 | 9 | 16.85 |
| Attendance of representatives at sessions | 0.071 | 9 | 15.84 |
| Access to analyses of the state of health of local self-government units (3 years) | 0.052 | 9 | 13.42 |
| Having identified vulnerable groups | 0.008 ** | 6 | 17.40 |
| Access to public health risk assessments of local self-government units | 0.321 | 10 | 24.31 |
| Availability of inspection reports | 0.058 | 8 | 21.24 |
| Instituting campaigns promoting healthy lifestyles | 0.004 * | 6 | 18.92 |
| Means of supporting campaigns | 0.083 | 26 | 97.24 |
| Cooperation of the council with the Headquarters for Emergency Situations | 0.054 | 9 | 19.57 |
| Availability of analyses of environmental indicators | 0.003 * | 6 | 19.59 |
| Creation of proposals for improving life indicators | 0.004 * | 6 | 18.96 |
| Having zones of sanitary protection of the water supply | 0.073 | 9 | 15.72 |
| Having a map/diagram of the water supply system | 0.077 | 15 | 23.36 |
| Having a plan for the reconstruction of the water supply network | 0.003 * | 6 | 19.70 |
| Having a wastewater treatment plant | 0.006 * | 6 | 18.09 |
| Having a register of septic and collecting pits | 0.142 | 6 | 9.60 |
| Performing air control measures | 0.053 | 6 | 12.43 |
| Having a municipal waste dump | 0.061 | 6 | 10.53 |
| Access to data on employee injuries | 0.484 | 6 | 5.47 |
| Having a system for monitoring work injuries | 0.470 | 6 | 5.59 |
| Having a counselor for the protection of patient rights | 0.168 | 6 | 9.09 |
| Having a local emergency healthcare plan | 0.219 | 6 | 8.27 |
| Having a protection and rescue plan | 0.039 * | 9 | 17.68 |
| Conducting exercises and education in the field of first aid | 0.000 ** | 6 | 20.97 |
* p ≤ 0.05; ** p ≤ 0.01.
Table 19.
Results of Pearson’s correlation analysis of the relationship between the effectiveness of the realized program budget and the selected variables.
Table 19.
Results of Pearson’s correlation analysis of the relationship between the effectiveness of the realized program budget and the selected variables.
| Variable | r | Sig. |
|---|---|---|
| Number of employees in local self-government units | 0.270 * | 0.034 |
| Water supply network | −0.025 | 0.844 |
| Sewage network | 0.042 | 0.746 |
| Number of households connected to the water supply system | 0.133 | 0.302 |
| Microbiologically defective water samples | −0.049 | 0.739 |
| Physically and chemically correct samples | −0.082 | 0.570 |
| Microbiologically defective samples of drinking water from the so-called village waterworks | 0.529 ** | 0.000 ** |
| Physically and chemically defective samples of drinking water from the so-called village waterworks | −0.026 | 0.842 |
| Microbiologically defective samples of drinking water from public taps | 0.368 | 0.004 ** |
| Physical and chemical defective samples of drinking water from public taps | −0.012 | 0.930 |
| Percentage of unsatisfactory analyses of wastewater samples | 0.406 | 0.001 * |
| The percentage of septic and collecting pits that were regularly emptied in a professional manner | −0.018 | 0.893 |
| Number of permanent measuring points for air-quality monitoring in local self-government units | 0.078 | 0.546 |
| Total number of air samples per year for PM10s | 0.171 | 0.183 |
| Total number of air samples on an annual basis for PM25s | 0.365 | 0.004 ** |
| Number of landfills in local self-government units | 0.206 | 0.131 |
| Number of sanitary landfills in local self-government units | 0.232 | 0.095 |
| Number of wild controlled landfills in local self-government units | 0.001 | 0.997 |
| Number of wild, uncontrolled landfills in local self-government units | 0.112 | 0.447 |
| Number of mandated fines issued | 0.252 | 0.048 * |
| Number of mosquito disinsections undertaken | −0.111 | 0.578 |
* p ≤ 0.05; ** p ≤ 0.01.
Table 20.
T-test results of the relationship between having a public health plan and selected variables.
Table 20.
T-test results of the relationship between having a public health plan and selected variables.
| t-Test for Equality of Means | |||||||
|---|---|---|---|---|---|---|---|
| t | df | Sig. (2-Tailed) | Mean Difference | Std. Error Difference | 95% Confidence Interval of the Difference | ||
| Lower | Upper | ||||||
| Cooperation with health institutions in the process of immunization | 1.572 | 72 | 0.120 | 0.225 | 0.143 | −0.060 | 0.509 |
| Cooperation with the Standing Conference of Towns and Municipalities | 1.244 | 74 | 0.217 | 0.148 | 0.119 | −0.089 | 0.385 |
| Number of health centers in local self-government units | 1.760 | 72 | 0.083 | 2.111 | 1.199 | −0.280 | 4.501 |
| Number of clinics | 1.089 | 73 | 0.280 | 2.511 | 2.305 | −2.084 | 7.105 |
| Number of security guards | −0.140 | 70 | 0.889 | −0.012 | .082 | −0.176 | 0.153 |
| Number of applications for protection advisors | 1.648 | 69 | 0.104 | 15.789 | 9.580 | −3.322 | 34.901 |
| Number of public companies with a risk assessment act | 0.413 | 75 | 0.681 | 0.250 | 0.606 | −0.957 | 1.457 |
| The total number of enterprises in the local self-government unit | 0.911 | 72 | 0.365 | 0.635 | 0.697 | −0.755 | 2.025 |
| The number of extinguished individual fireplaces in the local self-government unit | 1.575 | 74 | 0.120 | 15.426 | 9.794 | −4.088 | 34.940 |
| Microbiologically defective water samples—village waterworks | 0.808 | 74 | 0.422 | 21.719 | 26.886 | −31.853 | 75.290 |
| Physico-chemical defective water samples—village waterworks | 1.635 | 66 | 0.107 | 7.716 | 4.720 | −1.709 | 17.140 |
| Microbiologically defective water samples—public taps | 1.428 | 72 | 0.158 | 12.321 | 8.627 | −4.876 | 29.518 |
| Physico-chemical defective water samples—public taps | 1.074 | 72 | 0.286 | 6.212 | 5.784 | −5.319 | 17.743 |
| Microbiologically defective water samples—village schools | 1.222 | 72 | 0.226 | 8.467 | 6.930 | −5.348 | 22.281 |
| Physical and chemical defective water samples—village schools | 2.329 | 72 | 0.023 * | 6.848 | 2.940 | 0.987 | 12.709 |
| Unsatisfactory analyses of wastewater samples | 2.121 | 72 | 0.037 * | 16.144 | 7.612 | 0.970 | 31.319 |
| Septic and collecting pits | 3.422 | 73 | 0.001 * | 34.632 | 10.120 | 14.462 | 54.802 |
| Microbiologically defective water samples—JKP/JP | −0.132 | 74 | 0.896 | −0.761 | 5.782 | −12.282 | 10.760 |
| Physical and chemical defective water samples—JKP/JP | −0.445 | 60 | 0.658 | −1.946 | 4.373 | −10.693 | 6.801 |
* p ≤ 0.05; ** p ≤ 0.01.
Table 21.
Results related to the mean values of the variables of significance for the T-test.
| Public Health Plan | N | Mean | Std. Deviation | Std. Error Mean | |
|---|---|---|---|---|---|
| Cooperation with health institutions in the process of immunization | Yes | 21 | 4.81 | 0.512 | 0.112 |
| No | 53 | 4.58 | 0.570 | 0.078 | |
| Cooperation with Standing Conference of Towns and Municipalities | Yes | 21 | 4.86 | 0.359 | 0.078 |
| No | 55 | 4.71 | 0.497 | 0.067 | |
| Number of health centers in local self-government units | Yes | 21 | 3.71 | 8.391 | 1.831 |
| No | 53 | 1.60 | 1.691 | 0.232 | |
| Number of clinics in the JLS | Yes | 21 | 10.71 | 7.907 | 1.725 |
| No | 54 | 8.20 | 9.331 | 1.270 | |
| Number of security guards | Yes | 20 | 0.95 | 0.394 | 0.088 |
| No | 52 | 0.96 | 0.277 | 0.038 | |
| Number of applications—protection advisor | Yes | 20 | 20.75 | 62.036 | 13.872 |
| No | 51 | 4.96 | 18.898 | 2.646 | |
| Number of public companies with a risk assessment act | Yes | 21 | 1.71 | 2.452 | 0.535 |
| No | 56 | 1.46 | 2.335 | 0.312 | |
| The total number of enterprises in the local self-government unit | Yes | 20 | 3.45 | 2.164 | 0.484 |
| No | 54 | 2.81 | 2.822 | 0.384 | |
| The number of extinguished individual fireplaces in the local self-government unit | Yes | 21 | 40.81 | 167.843 | 36.626 |
| No | 55 | 19.09 | 67.975 | 9.166 | |
| Microbiologically defective water samples—village waterworks | Yes | 17 | 12.15 | 22.310 | 5.411 |
| No | 51 | 4.43 | 14.688 | 2.057 | |
| Physico-chemical defective water samples—village waterworks | Yes | 18 | 25.61 | 40.866 | 9.632 |
| No | 56 | 13.29 | 28.475 | 3.805 | |
| Microbiologically defective water samples—public taps | Yes | 21 | 13.48 | 27.560 | 6.014 |
| No | 53 | 7.26 | 20.115 | 2.763 | |
| Physico-chemical defective water samples—public taps | Yes | 21 | 16.95 | 35.170 | 7.675 |
| No | 53 | 8.49 | 22.898 | 3.145 | |
| Microbiologically defective water samples—village schools | Yes | 19 | 8.16 | 19.797 | 4.542 |
| No | 55 | 1.31 | 5.669 | 0.764 | |
| Physical and chemical defective water samples—village schools | Yes | 19 | 23.53 | 40.464 | 9.283 |
| No | 55 | 7.38 | 23.350 | 3.148 | |
| Unsatisfactory analyses of waste water samples | Yes | 20 | 54.05 | 42.479 | 9.499 |
| No | 55 | 19.42 | 37.360 | 5.038 | |
| Septic and collecting pits | Yes | 21 | 8.86 | 17.033 | 3.717 |
| No | 55 | 9.62 | 24.264 | 3.272 | |
| Microbiologically defective water samples—JKP/JP | Yes | 16 | 3.03 | 3.380 | 0.845 |
| No | 46 | 4.98 | 17.286 | 2.549 | |
| Physical and chemical defective water samples—JKP/JP | Yes | 18 | 32.02 | 43.427 | 10.236 |
| No | 44 | 12.81 | 31.388 | 4.732 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



