
Submitted:
11 January 2023
Posted:
16 January 2023
You are already at the latest version
Abstract
Cognitive impairment in older adults is associated with poor gait performance, physical decline, falls and poor quality of life. This paper analyzes the feasibility and efficacy of a tango-based in-tervention in older people with cognitive impairment living in nursing homes. A multicenter study, with pre and post-test, was carried out. Intervention attendance, well-being, physical abilities (Short Physical Performance Battery), walking performance, functional capacities (Katz Index), and quality of life (Quality of Life in Alzheimer’s Disease) were assessed. Fifty-four participants (84.9 ± 6.7 years, Mini Mental State Examination 14.5 ± 7.4) completed the protocol. Intervention attendance was 92%, and the mean subjective well-being after each session was 4.5 ± 0.5 (on a five-point scale). Statistically significant improvement was found in the quality of life (p = 0.030). Non statistically significant changes were found in walking performance, physical abilities, or in functional capacities. The study shows feasibility and suggests evidence for the effects of Tango therapy on well-being and quality of life. Further studies are necessary to contrast these findings and to verify the role of Tango interventions as a holistic approach to prevent functional decline in older people with cognitive impairment.
Keywords:
older adults
; cognitive impairment
; tango-therapy
; quality of life
; well-being
; physical performance
; walking performances
; abilities of daily living
; dance movement therapy
; arts with therapeutic intent
1. Introduction
Cognitive impairment, even at an early stage is associated with gait disorders, poor physical function and a high risk of falling [1]. It has been shown that cognitive impairment is a common condition in people living in nursing homes, and this place of residence has been highly linked to physical inactivity, greater risk of sarcopenia [2], cognitive decline [3] poor quality of life (QoL) and depression [4].
The impoverished environment of long-term-care institutions could be an accelerating factor of the decline [5]. This is why, to prevent the deterioration, it is necessary to provide enriched interventions, involving multisensorial activities [6], attentional tasks, strength and dynamic balance exercises that promote immediate and working memories and praxis [7]. Music and dance are used as a non-drug therapy and have been shown to be effective for different conditions, like mental illnesses [8], Parkinson’s disease [9] and other neurological conditions [10]. Dance could be a promising intervention, particularly useful for people who find verbal communication difficult or impossible [11]. Dance is a social and cultural experience. People come together and create a specific community atmosphere and share an aesthetic space [12]. Dance may improve QoL by simultaneously engaging the sensory systems and by stimulating physical, emotional, and cognitive functions [13].
Tango may be particularly helpful for improving mobility, motor–cognitive function, and gait in older adults [14]. Its regular practice can have a positive impact on cognitive abilities, as it requires sustained attention, spatiotemporal awareness, and use of memory [15]. Studies on tango as a therapy in Parkinson's disease have shown its effectiveness particularly in ameliorating QoL, as well as improving psychomotor and cognitive functions [16]. Tango offers an enriched environment: via the different senses, touch, smell, and hearing, the participant experiences being part of a group. After a while, the music and dancing can activate memories and create a sense of familiarity [17].
Motorically, tango is a moderate-intensity exercise [18] in which static and dynamic postural control is stimulated [19]. Tango is a dance based on walking [20]: support polygon, anticipation, transfer of body weight, varying length of the steps, speed, and changes of rhythm are all elements that must be coordinated to succeed in a harmonious process. From these characteristics, tango appears to be an excellent tool for the rehabilitation of balance and gait [21], as well as for the prevention of functional decline [22].
Few of the previous studies on the effect of dance on older people include institutionalized people of advanced age and suffering from moderate-severe cognitive impairment [23,24,25]. The objective of this study was to analyze the feasibility and the efficiency of tango-interventions in older adults living in nursing homes.
2. Materials and Methods
This multicenter study, with pre and post-intervention assessment, was carried out in eight nursing homes, between October 2021 and March 2022 in France, during the COVID-19 crisis. The absence of a control group was due to the difficulty of implementing a control intervention, and to the ethical issues that are inherent to a passive control group.
2.1. Participants
The participants were all over 65 years old, independent in ambulation with or without a walking aid. They had agreed to participate and lived permanently in one of the nursing homes where therapeutic tango interventions were implemented. The exclusion criteria were medical contraindication, limited life expectancy and bedridden persons. The study exit criteria were withdrawal from the participation agreement; participation in less than 50% of tango-sessions; psychiatric state, pathologies and care no longer allowing for the continuation of the study; death.
2.2. Ethics
The study was explained to the participants, caregivers and families, and information forms were distributed. Participants were enrolled in the study after consent was obtained from both the person with dementia and their legal proxy.
2.3. Intervention
The interventions were implemented by ABB Reportages1, and were carried out by nursing staff who had previously received training in therapeutic tango at the University of Burgundy2. Participants attended a 1-hour tango session, once a week for twelve weeks. A dance movement therapist and a musician accompanied the interventions twice a month. An overview of tango therapeutic session content is shown in Table 1. While the music choice varied slightly depending on the choice of the facilitators, some songs were frequently used for group singing (Table 2). Depending on the exercise, the musician played milonga, waltz or tango to assist in the task.
2.4. Outcome Measures
One member of staff at each center was instructed to perform the assessments in collaboration with the main investigator. The participants were assessed before and upon completion of the intervention. The subjective feeling of well-being, however, was evaluated after each session.
Intervention attendance was recorded, and was calculated as: ([number of dance sessions attended/total number of dance sessions] x 100).
The subjective feeling of instantaneous well-being was assessed after each session through a visual analog scale of well-being named EVIBE (Échelle d’évaluation instantanée de bien-être, Scale of instantaneous well-being) [26]. On a graduated ruler from 1 to 5, the participants positioned their feeling of well-being in response to the question “How do you feel now?”. Answer "1" corresponded to the weakest feeling of well-being and answer "5" to the strongest feeling of well-being. This scale has been validated in older people with severe dementia. The result of the test–retest reliability with a 10-minute interval was satisfactory (Cohen's kappa coefficient = 0.52, p > 0.001) and there was a significant correlation with Quality of Life Alzheimer's Disease (Qol-AD) (r = 0.54, p < 0.001).
Physical performances were measured by the Short Physical Performance Battery (SPPB) with three evaluation criteria: balance, walking speed and sit to stand [27]. Specifically, during the balance test, the subject had to maintain each of three distinct positions for 10 seconds (feet together, semi-tandem and tandem). The failure of a step was the condition to start the second test, in which the subject walked 4 meters two consecutive times. The best score was retained. Finally, the time taken to complete the fastest 5 chair lifts without the help of the upper limbs was evaluated. At the end of the three tests, a score of a maximum of 12 points could be obtained. Walking performances were assessed based on the participants’ need of walking aids (without aids, canes or crutches, rollator).
Functional capacities were assessed with the Katz Index [28], consisting of a questionnaire assessing abilities in six activities of daily living (ADL): personal hygiene care, dressing, toilet use, locomotion, continence and eating. For each domain, the answer varies between: 1 (complete independence), 0.5 (partial independence) or 0 (absolute dependence). In total, an index of zero to six is obtained, where zero indicates the highest degree of dependence.
QoL was assessed using the QoL-AD French version [29]. This questionnaire was administered directly to the participant, up to a severe stage of the disease, and to the main caregiver. The participant and caregiver ratings were combined into a weighted composite score: (2 × patient score + 1 × caregiver score)/3. Thus, the answers provided by the patient remain preponderant in this model. The QoL-AD comprises 13 items (physical health, energy, mood, living situation, memory, family, marriage, friends, self, ability to carry out daily tasks, ability to do things for fun, money and life as a whole). Response options include 1(poor), 2(fair), 3(good) and 4 (excellent), for a total score of 13–52, with higher scores indicating better QoL.
2.5. Statistical Analysis
The relative frequencies of the qualitative variables were calculated. For quantitative variables, the mean and standard deviation (SD) were calculated with 95% confidence intervals (95% CI). Quantitative outcome measures taken before and after intervention were compared by paired t-test or Wilcoxon Signed-Ranked Test. A McNemar's-Bowker test was used to compare categorical variables before and after the intervention. Spearman's correlation coefficient was applied to verify the relationship between quantitative variables. The alpha-level was set to p<.05. Statistical analysis was done with SPSS version 25 from IBM.
3. Results
3.1. Sample Characteristic
As shown in Figure 1, out of 102 people screened for eligibility, 74 were recruited from 8 different nursing homes for a 12-week tango intervention, according to predefined inclusion criteria. Fifty-four participants completed the intervention program and were therefore eligible for statistical analyses. Reasons for dropout were change of care structure (n = 1), a deterioration in their state of health (n = 4), death (n = 1) and the absence to more than 50% of the sessions (n = 14). The present sample comprised multi-morbid older adults, with 40% showing moderate to severe disability, and almost 70 % presenting moderate to severe dementia. No significant differences in baseline characteristics were found between dropouts and those participants who completed the intervention. The mean age was 84.9 ± 6.7 years old and the average score of their Mini Mental State Examination (MMSE) was 14.5 ± 7.4. The main characteristics of these participants are shown in Table 3.
3.2. Feasibility
During this study, 67 sessions were carried out among the 8 nursing homes, with an average per center of 8.7 ± 1.6 sessions. Each participant completed an average of 8 ± 1.7 sessions. The average attendance was 92% and the subjective feeling of well-being after sessions measured with EVIBE was 4.5 ± 0.5 (on a five-point-scale).
3.3. Outcomes
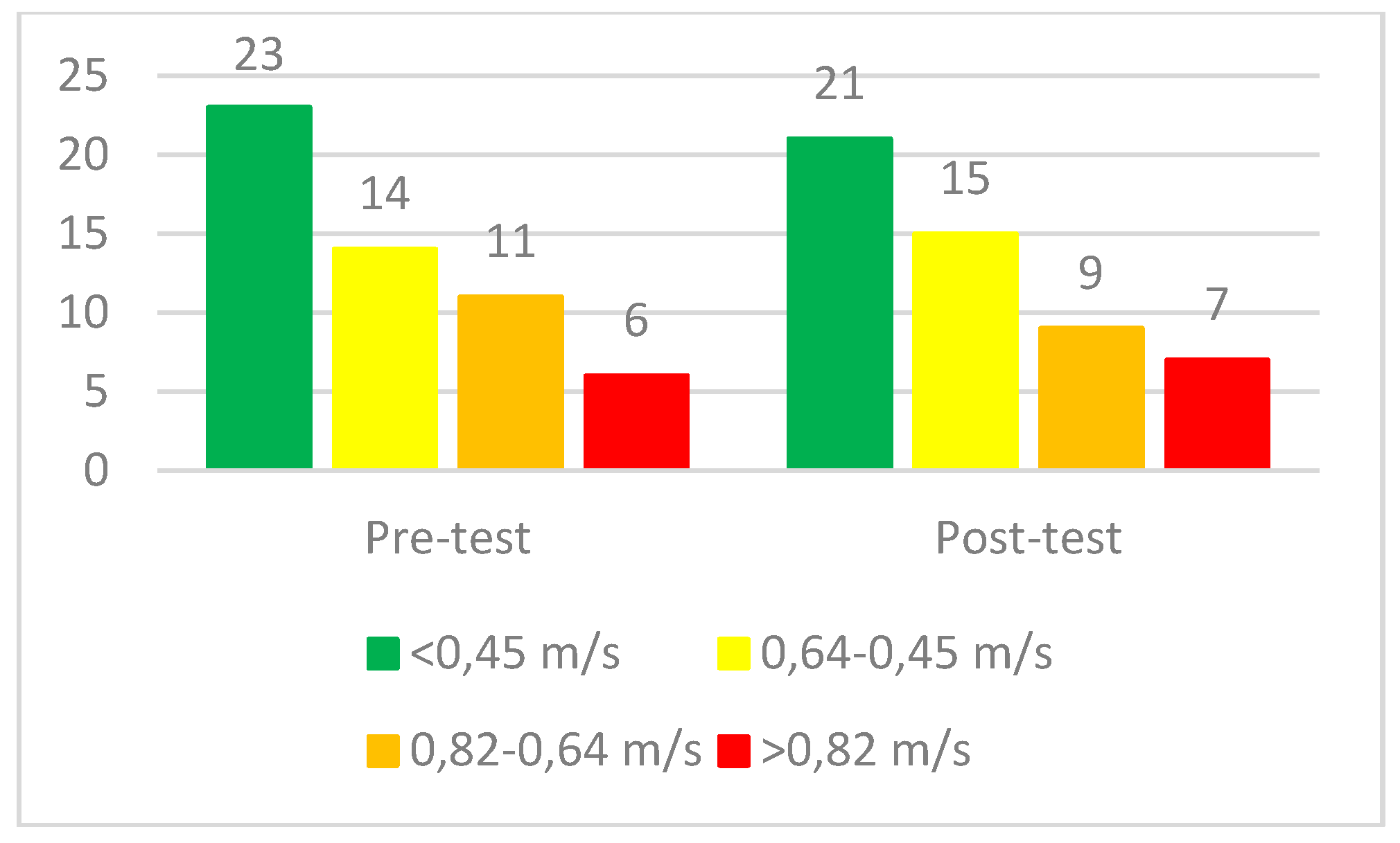
The main results are presented in Table 4. A statistically significant improvement in the QoL was noted (p = 0.030). No statistically significant changes were found in participants' physical performances or ability to perform ADLs. That is to say, there was a small improvement in the SPPB, especially in the full tandem balance test, but also a small decrease in functional abilities. There were also no statistically significant changes in walking performance, as can be seen in Figures 2 (Walking assistance devices) and 3 (Four Meters Gait Speed Test).
Figure 2.
Walking assistance devices before and after 3-month tango intervention.
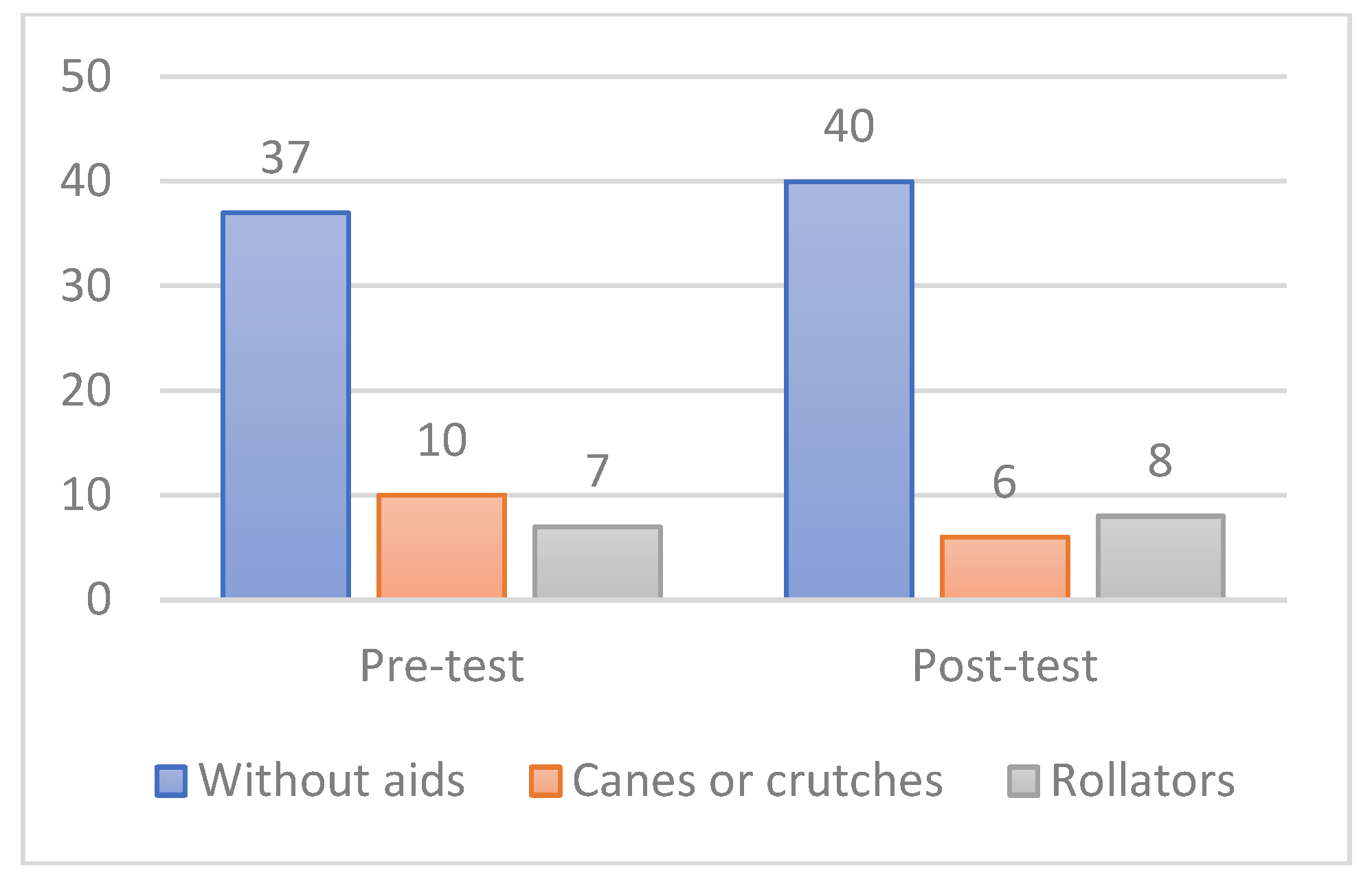
Figure 3.
Four Meters Gait Speed Test Subscore (n).
4. Discussion
The objective of this study was to analyze the feasibility and efficacy of a tango-based intervention in nursing homes. The results demonstrate that tango interventions are both feasible and highly appreciated among the participants. The participation rate and the average of immediate well-being after each session show high acceptance. Moreover, tango-interventions were effective in improving QoL and maintaining physical and functional capacities. These results are remarkable, especially considering the deterioration in older adults caused by lockdown and other restrictions imposed to contain the COVID-19 [30].
According to the findings of this study, tango-interventions are a beneficial strategy to improve QoL and to reduce the difference between the caregiver's and the participants' QoL perception. Consistently with prior surveys, we found that participants give better scores on their baseline QoL than caregivers [31,32,33]. One reason for this may be social representations of old age and a health culture that is more focused on health-related aspects than on overall QoL [34]. Then, the improvement in caregiver's perception after the intervention may be explained by a change in their gaze, through the relationship created during the tango sessions. The literature reports a positive change in group dynamics after a dance therapy-based intervention among residents and staff [35]. Tango could contribute to a positive work environment, directly impacting the caregiver's gaze on the patient [36]. However, further studies are necessary to understand the mechanisms of this relationship.
We found a significant improvement in the QoL-AD global score, which weights the answers provided by the participant and by the caregiver. This finding contrasts with other studies based on non-drug interventions. In a study with older adults with dementia living in a long term care facility, that evaluated the effects of a virtual-dance program, non-significant changes in QoL were observed [37]. Another similar investigation with older adults with cognitive impairment, living in a community dwelling, analyzed the impact of a dance intervention, without finding an effect on quality of life either [38].
By contrast, in our study, we found a significant improvement in QoL. One explanation may be that interventions based on tango focus on the work of emotions linked to interpersonal relationships [39]. One of the approaches presented by Cohen-Mansfield to frame non-drug interventions aimed at people with dementia is based precisely on relief of unmet needs, caused by sensory deprivation, boredom, or loneliness [40]. Tango interventions are rich in sensory stimuli, provide fun and feelings of connection.
Furthermore, in a more specific way, tango allows, through the movement of the body and the embrace (“abrazo”), a better awareness of one’s own axis and that of the other, thus promoting bodily, relational and emotional discoveries [17]. The maintenance of links and relationships with the caregivers, as well as access to meaningful activities, have been identified as factors that would exert an influence on the QoL of institutionalized older people [41]. All these factors present in the tango interventions could explain the improvement in QoL.
Regarding physical and functional capacities, no changes were observed. Tango interventions could have contributed to maintaining physical abilities during this period of harsh restrictions, representing a positive result. This study took place between October 2021 and March 2022, during the fifth epidemic wave of COVID-19. As has been highlighted by several studies, the measures applied to limit the spread of the virus had direct deleterious effects in the geriatric population, such as sarcopenia and depression, as well as indirect effects through the delay, or even the absence of care for diseases, such as cardiovascular diseases and neurodegenerative pathologies [42]. A study carried out after the first wave of COVID-19 among nursing home residents showed a significant functional, cognitive, and nutritional decline. This deterioration may have been produced by the lockdown itself because no differences were found between COVID-19 and non-COVID-19 patients [43].
Conversely, the participants in our study did not experience significant deterioration. Other studies with a control group that evaluated the effect of a dance-intervention in a similar population have shown a deterioration in the control group and a slowed down deterioration of functional status in the intervention group [44,45]. These findings provide evidence of a stabilization of physical and functional performance produced by dance interventions.
In addition, no changes were observed in gait performance. This result disagrees with other studies that applied tango in gait rehabilitation. In a controlled trial it was possible to observe an improvement in gait in older people after 20 sessions of tango [14]. Several studies in Parkinson’s disease have observed a significant improvement in gait immediately after a tango lesson [46] and after an adapted tango program [47].
In addition, a study examined the functional changes in the activity of the cerebral areas involved in a locomotor imagery task after one week of training consisting in performing basic tango steps. The results showed an expansion of active bilateral motor areas and a reduction of visuospatial activation in the posterior right brain, suggesting a decreased role of visual imagery processes after intervention in favor of motor-kinesthetic ones [48]. All these findings allow us to think that tango-interventions are a good way to prevent gait-disorders in older people with cognitive impairment. However, further studies are necessary to improve this promising method.
Therapeutic tango is an intervention inspired by the principles of Dance Movement Therapy and Rehabilitation of frail older people with dementia. Its objective is to provide alternative and complementary therapy to people living in nursing homes. From on-site spontaneous testimonies, it emerged that participants, caregivers and families intuitively perceived an impact on the well-being and on the neuromotor capacities. Staff-resident dynamics improved and relationships between residents were fostered. Walking, which tends to be slowed down with small steps, is transformed by the effect of the music. Despite this being basically an empirical finding, based on these spontaneous expressions, we postulate that tango may lead to faster results than traditional rehabilitation techniques.
Our study had several strengths. This is the first study analyzing the effectiveness of tango in older people living in nursing homes. It is necessary to highlight the characteristics of the participants, who were of a very advanced age, disabled and with a high rate of cognitive impairment. There are few studies on non-pharmacological therapies in similar populations [23,25,49,50] because research in this context presents several challenges and methodological issues. These include: ethics concerns, finding opportunities to conduct assessments, involvement of care-home staff and residents' families [51], recruitment and retention of participants [52]. Therefore, one of the strengths of this project is that it allowed to assess on older participants the effects of an intervention designed specifically for them, thus contributing to the evidence base for care of the older adults [53].
Our study also had some limitations. First, this study does not provide a control group. Tango could play a role, no longer improving, but maintaining physical and functional capacities. However, without a randomized controlled trial (RCT), this remains a hypothesis. In addition, probably the frequency of interventions was not enough to generate changes in physical performances. Finally, even if most studies used the SPPB to assess the physical performances in older adults with cognitive impairment, this may not be sensitive enough to measure outcomes, because minimal cognitive performance is required to understand instructions and respond appropriately. The lessons from these limitations have been incorporated into further projects of the research team: an RCT protocol, with a higher number of interventions (2 or 3 per week) and the technical implementation of assessment of spatiotemporal gait parameters.
5. Conclusions
Tango therapy has shown to be feasible and highly accepted to support wellbeing in older adults living in nursing homes. The results of this study suggest that tango-based interventions have a positive impact on participants' QoL, and especially in the caregivers' view of the participants’ QoL. Concerning physical abilities and walking performances, tango therapy could play a stabilizer role, but new studies are needed to establish this relationship. Tango therapy may involve older persons and be particularly beneficial for those with dementia. The results obtained here encourage us to continue searching for our work towards the understanding of the mechanisms that are set in motion through tango and its relationship with QoL and physical capacities of older adults with cognitive impairment. Tango therapy with its versatile sensory-motor possibilities may be just the intervention needed for older adults in nursing homes to prevent the decline and to foster joy and well-being.
Author Contributions
Conceptualization, L.B. and F.M.; methodology, L.B., A.P.C. and F.M.; validation, S.C.K. and F.M.; formal analysis, L.B. and A.P.C.; investigation, L.B. and C.C.; resources, F.M.; data curation, L.B.; writing—original draft preparation, L.B. and C.C.; writing—review and editing, L.B., C.C., A.P.C., S.C.K. and F.M.; visualization, F.M.; supervision, F.M.; project administration, F.M.; funding acquisition, F.M. All authors have read and agreed to the published version of the manuscript.
Funding
This study has been carried out in the context of a doctoral program financed by the Société de Gérontologie de l'Est and the Conférence des Financeurs de Paris.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Research Ethics Committee of the University of Burgundy (CERUBFC 2021-09-15-026).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
We thank the participants, the teams, and the directors of the various nursing homes for their participation and their confidence in the researchers. The collaboration with Anne Bramard Blagny of ABB Reportages has been fundamental for the implementation of this research. Our appreciation also goes to Quentin Guenebaut, Hugo Mascaro, Maélisse Crance and Romain Tissot for their supportive help with data collection and entry. Thanks to Fran Carter and Catalina Onofrei for their valuable English corrections.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Taylor, M.E.; Close, J.C.T. Dementia. In; 2018; pp. 303–321 ISBN 9780444639165.
- Landi, F.; Liperoti, R.; Fusco, D.; Mastropaolo, S.; Quattrociocchi, D.; Proia, A.; Russo, A.; Bernabei, R.; Onder, G. Prevalence and Risk Factors of Sarcopenia Among Nursing Home Older Residents. Journals Gerontol. Ser. A Biol. Sci. Med. Sci. 2012, 67A, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Colaço Harmand, M.; Meillon, C.; Rullier, L.; Avila-Funes, J.A.; Bergua, V.; Dartigues, J.F.; Amieva, H. Cognitive Decline after Entering a Nursing Home: A 22-Year Follow-up Study of Institutionalized and Noninstitutionalized Elderly People. J. Am. Med. Dir. Assoc. 2014, 15, 504–508. [Google Scholar] [CrossRef] [PubMed]
- De Medeiros, M.M.D.; Carletti, T.M.; Magno, M.B.; Maia, L.C.; Cavalcanti, Y.W.; Rodrigues-Garcia, R.C.M. Does the Institutionalization Influence Elderly’s Quality of Life? A Systematic Review and Meta-Analysis. BMC Geriatr. 2020, 20. [Google Scholar] [CrossRef] [PubMed]
- Volkers, K.M.; Scherder, E.J.A. Impoverished Environment, Cognition, Aging and Dementia. revneuro 2011, 22, 259–266. [Google Scholar] [CrossRef]
- Picanço-Diniz, C.; Galdino De Oliveira, T.C.; Cabral Soares, F.; Dias E Dias De Macedo, L.; Wanderley Picanco Diniz, D.L.; Valim Oliver Bento-Torres, N. Beneficial Effects of Multisensory and Cognitive Stimulation on Age-Related Cognitive Decline in Long-Term-Care Institutions. Clin. Interv. Aging 2014, 9, 309. [Google Scholar] [CrossRef] [PubMed]
- Manckoundia, P.; Mourey, F.; Pfitzenmeyer, P. Marche et Démences. Ann. Réadaptation Médecine Phys. 2008, 51, 692–700. [Google Scholar] [CrossRef] [PubMed]
- Kiepe, M.-S.; Stöckigt, B.; Keil, T. Effects of Dance Therapy and Ballroom Dances on Physical and Mental Illnesses: A Systematic Review. Arts Psychother. 2012, 39, 404–411. [Google Scholar] [CrossRef]
- Carapellotti, A.M.; Stevenson, R.; Doumas, M. The Efficacy of Dance for Improving Motor Impairments, Non-Motor Symptoms, and Quality of Life in Parkinson’s Disease: A Systematic Review and Meta-Analysis. PLoS One 2020, 15, e0236820. [Google Scholar] [CrossRef]
- Patterson, K.K.; Wong, J.S.; Prout, E.C.; Brooks, D. Dance for the Rehabilitation of Balance and Gait in Adults with Neurological Conditions Other than Parkinson’s Disease: A Systematic Review. Heliyon 2018, 4, e00584. [Google Scholar] [CrossRef]
- Odell-Miller, H.; Hughes, P.; Westacott, M.; Odell-Miller, H.; Hughes, P.; Westacott, M. An Investigation into the Effectiveness of the Arts Therapies for Adults with Continuing Mental Health Problems. Psychother. Res. 2006, 16, 122–139. [Google Scholar] [CrossRef]
- Koch, S.C.; Mergheim, K.; Raeke, J.; Machado, C.B.; Riegner, E.; Nolden, J.; Diermayr, G.; von Moreau, D.; Hillecke, T.K. The Embodied Self in Parkinson’s Disease: Feasibility of a Single Tango Intervention for Assessing Changes in Psychological Health Outcomes and Aesthetic Experience. Front. Neurosci. 2016, 10, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Goldstein-Levitas, N. Dance/Movement Therapy and Sensory Stimulation: A Holistic Approach to Dementia Care. Am. J. Danc. Ther. 2016, 38, 429–436. [Google Scholar] [CrossRef]
- Hackney, M.E.; Byers, C.; Butler, G.; Sweeney, M.; Rossbach, L.; Bozzorg, A. Adapted Tango Improves Mobility, Motor–Cognitive Function, and Gait but Not Cognition in Older Adults in Independent Living. J. Am. Geriatr. Soc. 2015, 63, 2105–2113. [Google Scholar] [CrossRef] [PubMed]
- McKee, K.E.; Hackney, M.E. The Effects of Adapted Tango on Spatial Cognition and Disease Severity in Parkinson’s Disease. J. Mot. Behav. 2013, 45, 519–529. [Google Scholar] [CrossRef] [PubMed]
- Lötzke, D.; Ostermann, T.; Büssing, A. Argentine Tango in Parkinson Disease – a Systematic Review and Meta-Analysis. BMC Neurol. 2015, 15, 226. [Google Scholar] [CrossRef] [PubMed]
- Joyal, F. Tango, Corps à Corps Culturel : Danser En Tandem Pour Mieux Vivre; Presses de l’Université de Quebec, Ed.; Collection Santé et Societé: Québec, 2009; ISBN 978-2-7605-2392-0.
- Peidro, R.M.; Osses, J.; Caneva, J.; Briont, G.; Angelino, A.; Kerbage, S.; Garcia Ben, M.; Pesce, R. Tango: Modificaciones Cardiorrespiratorias Durante El Baile. Rev. Argent. Cardiol. 2002, 70, 358–363. [Google Scholar]
- Koh, Y.; Hur, Y.; Noh, G. Tango Posture and Stance: Functional Anatomical Analysis and Therapeutic Characteristics. J. Tango 2019, 1, 19–32. [Google Scholar] [CrossRef]
- Koh, Y.; Hur, Y.; Kim, I.S.; Ha, C.W.; Noh, G. Tango Gait for Tango Therapy: Functional Anatomical Characteristics of Tango Gait (‘Tango Gaitology’). J. Tango 2019, 1, 33–47. [Google Scholar] [CrossRef]
- Koh, Y.; Kim, I.C.S.; Noh, G. Tango Therapy: Current Status and the Next Perspective. J. Clin. Rev. Case Reports 2018, 3, 1–6. [Google Scholar] [CrossRef]
- McKinley, P.; Jacobson, A.; Leroux, A.; Bednarczyk, V.; Rossignol, M.; Fung, J. Effect of a Community-Based Argentine Tango Dance Program on Functional Balance and Confidence in Older Adults. J. Aging Phys. Act. 2008, 16, 435–453. [Google Scholar] [CrossRef]
- Guzmán-García, A.; Hughes, J.C.; James, I.A.; Rochester, L.; Guzman-Garcia, A.; Hughes, J.C.; James, I.A.; Rochester, L. Dancing as a Psychosocial Intervention in Care Homes: A Systematic Review of the Literature. Int. J. Geriatr. Psychiatry 2013, 28, 914–924. [Google Scholar] [CrossRef] [PubMed]
- Gomaa, Y.S.; Slade, S.C.; Tamplin, J.; Wittwer, J.E.; Gray, R.; Blackberry, I.; Morris, M.E. Therapeutic Dancing for Frail Older People in Residential Aged Care: A Thematic Analysis of Barriers and Facilitators to Implementation. Int. J. Aging Hum. Dev. 2020, 90, 403–422. [Google Scholar] [CrossRef] [PubMed]
- Bracco, L.; Poirier, G.; Pinto-Carral, A.; Mourey, F. Effect of Dance Therapy on the Physical Abilities of Older Adults with Dementia: A Systematic Review. Eur. J. Geriatr. Gerontol. 2021, 3, 134–142. [Google Scholar] [CrossRef]
- Delphin-Combe, F.; Dauphinot, V.; Denormandie, P.; Sanchez, S.; Hay, P.-E.; Moutet, C.; Krolak-Salmon, P. The Scale of Instantaneous Wellbeing: Validity in a Population with Major Neurocognitive Disorders. Gériatrie Psychol. Neuropsychiatr. du Viellissement 2018, 16, 329–334. [Google Scholar] [CrossRef] [PubMed]
- Treacy, D.; Hassett, L. The Short Physical Performance Battery. J. Physiother. 2018, 64, 61. [Google Scholar] [CrossRef] [PubMed]
- The Staff of The Benjamin Rose Hospital Multidisciplinary Study of Illness in Aged Persons. I. Methods and Preliminary Results. J. Chronic Dis. 1958, 7, 332–345. [CrossRef] [PubMed]
- Cousi, C.; Igier, V.; Quintard, B. French Cross-Cultural Adaptation and Validation of the Quality of Life-Alzheimer’s Disease Scale in Nursing Homes (QOL-AD NH). Health Qual. Life Outcomes 2021, 19, 219. [Google Scholar] [CrossRef] [PubMed]
- O’Caoimh, R.; O’Donovan, M.R.; Monahan, M.P.; Dalton O’Connor, C.; Buckley, C.; Kilty, C.; Fitzgerald, S.; Hartigan, I.; Cornally, N. Psychosocial Impact of COVID-19 Nursing Home Restrictions on Visitors of Residents With Cognitive Impairment: A Cross-Sectional Study as Part of the Engaging Remotely in Care (ERiC) Project. Front. Psychiatry 2020, 11. [Google Scholar] [CrossRef] [PubMed]
- Logsdon, R.G.; Gibbons, L.E.; McCurry, S.M.; Teri, L. Assessing Quality of Life in Older Adults with Cognitive Impairment. Psychosom. Med. 2002, 64, 510–519. [Google Scholar] [CrossRef]
- Conde-Sala, J.L.; Garre-Olmo, J.; Turró-Garriga, O.; López-Pousa, S.; Vilalta-Franch, J. Factors Related to Perceived Quality of Life in Patients with Alzheimer’s Disease: The Patient’s Perception Compared with That of Caregivers. Int. J. Geriatr. Psychiatry 2009, 24, 585–594. [Google Scholar] [CrossRef]
- Gómez-Gallego, M.; Gómez-Amor, J.; Gómez-García, J. Determinants of Quality of Life in Alzheimer’s Disease: Perspective of Patients, Informal Caregivers, and Professional Caregivers. Int. Psychogeriatrics 2012, 24, 1805–1815. [Google Scholar] [CrossRef]
- Baud Mermoud, V.; Morin, D. Regards Croisés Entre l’évaluation de La Qualité de Vie Perçue Par Le Résident Hébergé En Établissement Médico-Social et Par Le Soignant Référent. Rech. Soins Infirm. 2016, 126, 38–50. [Google Scholar] [CrossRef]
- Duignan, D.; Hedley, L.; Milverton, R. Exploring Dance as a Therapy for Symptoms and Social Interaction in a Dementia Care Unit. Nurs. Times 2009, 105, 19–22. [Google Scholar] [PubMed]
- Sjögren, K.; Lindkvist, M.; Sandman, P.-O.; Zingmark, K.; Edvardsson, D. To What Extent Is the Work Environment of Staff Related to Person-Centred Care? A Cross-Sectional Study of Residential Aged Care. J. Clin. Nurs. 2015, 24, 1310–1319. [Google Scholar] [CrossRef]
- Brami, C.; Trivalle, C.; Maillot, P. Feasibility and Interest of Exergame Training for Alzheimer Patients in Long-Term Care [Faisabilité et Intérêt de l’entraînement En Exergames Pour Des Patients Alzheimer En SLD]. NPG Neurol. - Psychiatr. - Geriatr. 2018, 18, 235–244. [Google Scholar] [CrossRef]
- Charras, K.; Mabire, J.-B.; Bouaziz, N.; Deschamps, P.; Froget, B.; de Malherbe, A.; Rosa, S.; Aquino, J.-P. Dance Intervention for People with Dementia: Lessons Learned from a Small-Sample Crossover Explorative Study. Arts Psychother. 2020, 70, 101676. [Google Scholar] [CrossRef]
- Hackney, M.E.; Earhart, G.M. Recommendations for Implementing Tango Classes for Persons with Parkinson Disease. Phys. Ther. Fac. Publ. 2010, 6. [Google Scholar] [CrossRef] [PubMed]
- Cohen-Mansfield, J. Nonpharmacologic Interventions for Inappropriate Behaviors in Dementia: A Review, Summary, and Critique. Am. J. Geriatr. Psychiatry 2001, 9, 361–381. [Google Scholar] [CrossRef]
- Murphy, K.; Shea, E.O.; Cooney, A. Quality of Life for Older People Living in Long-Stay Settings in Ireland. J. Clin. Nurs. 2007, 16, 2167–2177. [Google Scholar] [CrossRef]
- Maamar, M.; Khibri, H.; Harmouche, H.; Ammouri, W.; Tazi-Mezalek, Z.; Adnaoui, M. Impact Du Confinement Sur La Santé Des Personnes Âgées Durant La Pandémie COVID-19. NPG Neurol. - Psychiatr. - Gériatrie 2020, 20, 322–325. [Google Scholar] [CrossRef]
- Pérez-Rodríguez, P.; Díaz de Bustamante, M.; Aparicio Mollá, S.; Arenas, M.C.; Jiménez-Armero, S.; Lacosta Esclapez, P.; González-Espinoza, L.; Bermejo Boixareu, C. Functional, Cognitive, and Nutritional Decline in 435 Elderly Nursing Home Residents after the First Wave of the COVID-19 Pandemic. Eur. Geriatr. Med. 2021, 12, 1137–1145. [Google Scholar] [CrossRef] [PubMed]
- Hokkanen, L.; Rantala, L.; Remes, A.M.; Harkonen, B.; Viramo, P.; Winblad, I. Dance/Movement Therapeutic Methods in Management of Dementia. J. Am. Geriatr. Soc. 2008, 56, 771–772. [Google Scholar] [CrossRef] [PubMed]
- Machacova, K.; Vankova, H.; Volicer, L.; Veleta, P.; Holmerova, I. Dance as Prevention of Late Life Functional Decline Among Nursing Home Residents. J. Appl. Gerontol. 2017, 36, 1453–1470. [Google Scholar] [CrossRef] [PubMed]
- Fontanesi, C.; DeSouza, J.F.X. Beauty That Moves: Dance for Parkinson’s Effects on Affect, Self-Efficacy, Gait Symmetry, and Dual Task Performance. Front. Psychol. 2021, 11. [Google Scholar] [CrossRef]
- Rios Romenets, S.; Anang, J.; Fereshtehnejad, S.-M.; Pelletier, A.; Postuma, R. Tango for Treatment of Motor and Non-Motor Manifestations in Parkinson’s Disease: A Randomized Control Study. Complement. Ther. Med. 2015, 23, 175–184. [Google Scholar] [CrossRef] [PubMed]
- Sacco, K.; Cauda, F.; Cerliani, L.; Mate, D.; Duca, S.; Geminiani, G.C. Motor Imagery of Walking Following Training in Locomotor Attention. The Effect of ‘the Tango Lesson’. Neuroimage 2006, 32, 1441–1449. [Google Scholar] [CrossRef]
- Karkou, V.; Meekums, B. Dance Movement Therapy for Dementia. Cochrane Database Syst. Rev. 2017, 2017, CD011022. [Google Scholar] [CrossRef] [PubMed]
- Mabire, J.-B.; Aquino, J.-P.; Charras, K. Dance Interventions for People with Dementia: Systematic Review and Practice Recommendations. Int. Psychogeriatrics 2019, 31, 977–987. [Google Scholar] [CrossRef] [PubMed]
- Hall, S.; Longhurst, S.; Higginson, I.J. Challenges to Conducting Research with Older People Living in Nursing Homes. BMC Geriatr. 2009, 9, 38. [Google Scholar] [CrossRef]
- Mody, L.; Miller, D.K.; McGloin, J.M.; Freeman, M.; Marcantonio, E.R.; Magaziner, J.; Studenski, S. Recruitment and Retention of Older Adults in Aging Research. J. Am. Geriatr. Soc. 2008, 56, 2340–2348. [Google Scholar] [CrossRef]
- Studenski, S. Challenges in Clinical Aging Research: Building the Evidence Base for Care of the Older Adult. J. Am. Geriatr. Soc. 2008, 56, 2351–2352. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Flowchart for enrollment, allocation and follow-up of participants.
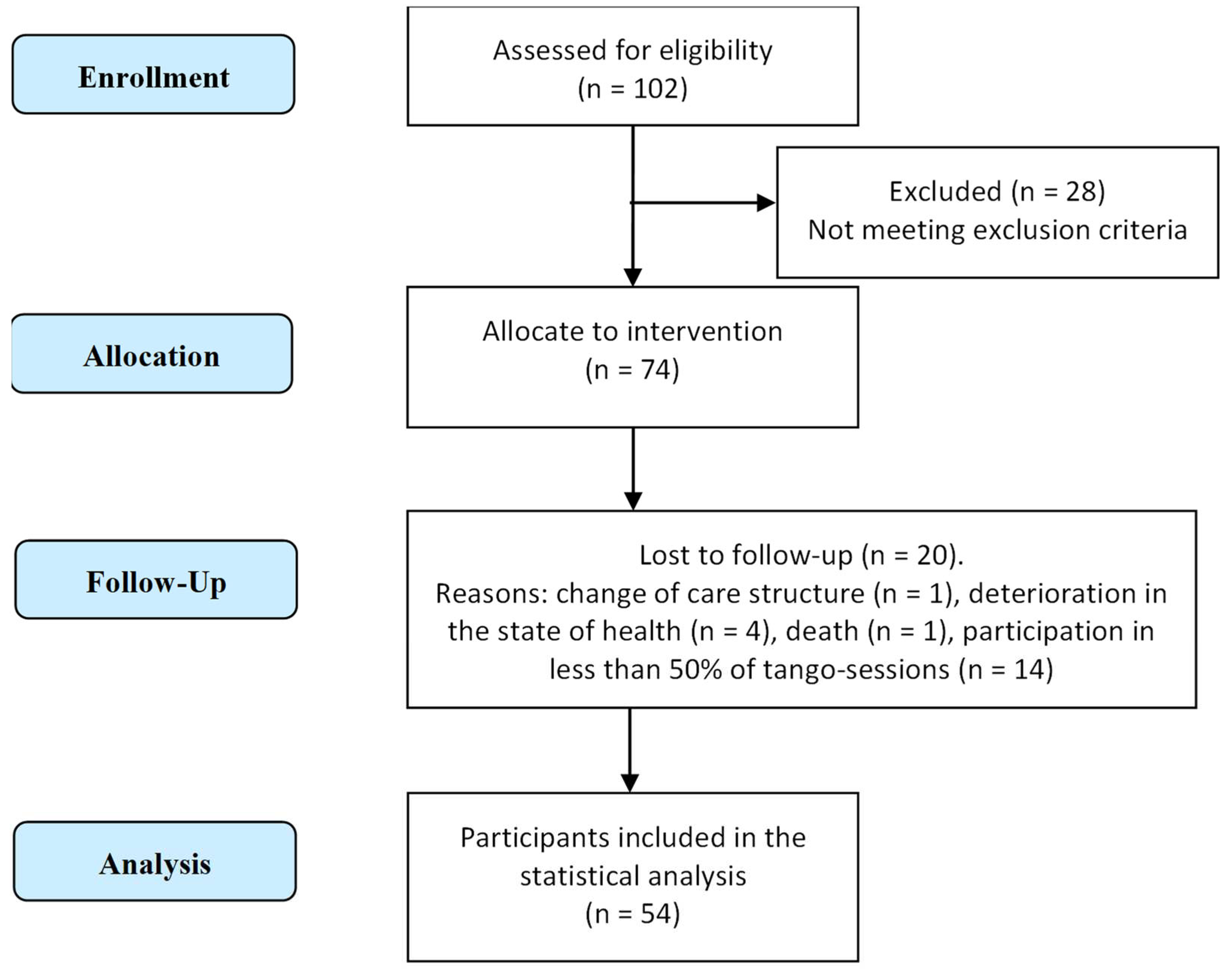

Table 1.
Overview of session content.
| Session Components | Activities |
|---|---|
| Pre-warm-up | Organizing the seating arrangement in the room, greeting the participants, engaging in small talk |
| Warm-up | Seated exercises to mobilize lower and upper limbs, head and trunk as well as singing to warm-up the voice and foster social connection |
| Main part | Different aspects of tango therapy were practiced. This could include technical aspects such as: foreword and backward walking, side-step, square, rectangle, as well as improvisation via spontaneous expression. The physical connection via ‘Abrazo’ (embrace) or other interactions were also an important aspect of the intervention. |
| Cool-down | Seated rituals such as singing and breathing exercises. |
| Social exchange | The sessions were frequently followed by coffee and cake, or participants still stayed around to talk with each other and facilitators. |
Table 2.
Songs frequently used.
| Song title | Artist |
|---|---|
| Le plus beau tango du monde | Tino Rossi |
| Paloma | Tino Rossi |
| Mon Amant de Saint Jean | Lucienne Delyle |
| Voulez-Vous Danser Grand'mère | Lina Margy |
| Vous Permettez Monsieur | Salvatore Adamo |
Table 3.
Baseline simple characteristic.
| Variables | Total (N=54) |
|---|---|
| Sex, females, n (%) | 42 (78) |
| Age (years), M ± SD | 84.9 ± 6.7 |
| Charlson Index, M ± SD | 5.6 ± 1.6 |
| MMSE, score (range 0–30) M ± SD | 14.5 ± 7.4 |
| Katz Index, score (range 0–6) M ± SD | 4.5 ± 1.3 |
M mean, SD standard deviation, MMSE mini-mental state examination.
Table 4.
Variables of physical abilities, functional capacities and quality of life before and after a 3-month tango intervention.
Table 4.
Variables of physical abilities, functional capacities and quality of life before and after a 3-month tango intervention.
| Variables | Pre-test M ± SD | Post-test M ± SD | p-value | |
|---|---|---|---|---|
| SPPB | Balance subscore (0-4) | 2,1 ± 0,9 | 2,3 ± 1 | 0,221 |
| Gait speed subscore (0-4) | 2 ± 1 | 2 ± 1,1 | 0,725 | |
| Sit to stand subscore (0-4) | 1,2 ± 1,2 | 1,2 ± 1,2 | 0,862 | |
| Total score (0-12 | 5,3 ± 2,4 | 5,4 ± 2,6 | 0,876 | |
| Katz Index, score (range 0–6) M ± SD | 4,5 ± 1,3 | 4,3 ± 1,2 | 0,253 | |
| QoL-AD, score (range 13–52) | Participant | 33,8 ± 5,4 | 34,3 ± 5,7 | 0,172 |
| Caregiver | 31,9 ± 4,5 | 33 ± 4,2 | 0,103 | |
| Weighted composite score | 33,1 ± 4,6 | 34 ± 4,5 | 0,030* | |
M mean, SD standard deviation, SPPB short physical performance battery, QoL-AD Quality of life in Alzheimer disease, * p < 0.05 based on paired t tests to test for differences between before and after intervention.
| 1 | To know more: http://www.abbreportages.fr/content/view/214/186/lang,english/ |
| 2 | To know more: https://sefca.u-bourgogne.fr/toute-lactualite/379-la-melodie-d-alzheimer.html?fbclid=IwAR0bu8hkfWfMJ39oRRZNGcI9aFG-HK4CTy9YucKr72Quwvb04P4ivC4TkEE |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



