Submitted:
13 January 2023
Posted:
16 January 2023
Read the latest preprint version here
Preprints on COVID-19 and SARS-CoV-2
Abstract
Hospitals are under pressure from society to improve the efficiency of their bed management processes. Among the various effects of inefficiency, the lack of beds to meet the demand stands out, which has increased significantly due to COVID-19, aggravating the overcrowding of emergency departments. Effective management of hospital production capacity includes bed management processes, which can be improved in order to leverage hospital performance. Thus, this study sought to understand how bed management works and identify the main factors that influence its management. The study was performed through a case study, with data collected from semi-structured interviews and bibliographic research, which were triangulated. Thematic content analysis of the case and cross-analysis were performed. As a result, the main factors that influence bed management were identified: communication between teams and units; definition of performance goals; decisions shared between units; occupation and discharge planning by the teams; length of stay; nurses; and COVID-19. The greatest difficulties in the management process are related to these factors.
Keywords:
Bed management
; Emergency Department
; Overcrowding
; Efficiency
; Hospital management
1. Introduction
Bed management (BM) aims to improve bed availability throughout the hospital. One of the most dangerous preliminary scenarios in the hospital system is overcrowding. Overcrowding in the emergency department (ED) is a problem that generates several implications for BM, which is deemed one of a hospital's most critical processes (Landa et al., 2018). In addition, overcrowding is understood by several authors as a worldwide concern (Borges et al., 2020; He et al., 2019). The Emergency Nurses Association (ENA) and the American College of Emergency Physicians (ACEP) state overcrowding, in this case, occurs when the demand for emergency services exceeds the capacity of human and material resources available to meet them (ACEP, 2019; ENA, 2006).
According to Landa et al. (2018) and He et al. (2019), the volume of patients in the ED of hospitals is highly unpredictable. Health professionals need actual real-time information on the arrival and departure of patients and judicious medical record forecasts, as this helps to improve efficiency in managing the bed availability index and reduce the waiting time for new patient admissions (Raffa, 2017; Raffa et al., 2017a).
Tampubolon & Pujiyanto (2018) report that overcrowding continues to grow and requires continuous interventions to minimize this problem. Thus, it is relevant to reassess the factors that insist on generating overcrowding in the ED, whilst these factors are deemed by these authors as a threat to an entire health system and patient safety.
As the problem of overcrowding has worsened in recent years, the COVID-19 pandemic has highlighted the urgency of it being effectively addressed. The pandemic stretched hospital care capacity, requiring hospitals to be more efficient in managing beds to meet demands, with the shortest length of hospital stay necessary for patient recovery (Noronha et al., 2020).
According to monitoring reports from the Brazillian COVID-19 Observatory, organized by the Oswaldo Cruz Foundation (Fiocruz), regarding the standard recommendations by the World Health Organization (WHO), the occupancy rate of hospital beds in Brazil has been growing steadfastly. In the first half of July 2020, the COVID-19 Intensive Care Unit (ICU) bed occupancy rate for adults in the Brazillian Unified Health System (UHS) was on critical alert (equal to or greater than 80%) in three states and the Federal District (FD). A few months later, in the first half of March 2021, the state of critical alert reached eighteen states and the FD (Fiocruz, 2021), being the peak of the entire COVID-19 pandemic in Brazil recorded so far.
In hospitals, decision-making processes by bed managers depend fundamentally on indicators (qualitative and quantitative) and tools (information technology systems) that rely on human and material resource planning. However, these organizations are characterized by departmentalized structures (Raffa, 2017). Thus, fragmentation takes commonplace in the daily basis of decision-making which, in turn, does not approach the interactions of the inpatient units in a systemic way, thus resulting in a lack of collaborative management, which ultimately implies problems such as difficulty in integration and coordination, and even overlapping decisions (Raffa, 2017).
In this sense, regarding managerial decisions, He et al. (2019) state that for a BM model to be efficient, the units as a whole must be taken into account. The sectors are part of a larger system, the hospital, and their different information must be included to generate more assertive decisions regarding the hospital beds. In other words, the adage “think global, act local” applies here. Along these lines, BM is considered a complex process in hospitals (He et al., 2019; Raffa et al., 2017c).
In an attempt to best meet the demand due to COVID-19, it was imperative to increase the overall efficiency of EDs. In the view of Landa et al. (2018), the growing demand for beds in EDs should not only be addressed at a strategic level, increasing the absolute number of beds, as this can not be done indefinitely. Rather, these authors suggest that the solution must also be found jointly at the tactical and operational levels.
Against this background, we start from the premise that problems related to the management of hospital beds can be found throughout all levels of planning (strategic, tactical, and operational), such as in the scheduling of bed occupancy (Machado & Machado, 2019; Raffa et al., 2017c), in the autonomy of the manager over the beds (Borges et al., 2020; Oliveira & Bittencourt, 2020; Raffa, 2017), in the patient flow process (Tampubolon & Pujiyanto, 2018), or the communication process (Borges et al., 2020; Machado & Machado, 2019; Raffa, 2017; Souza et al., 2020; Werner, 2017). Thus, thoroughly recognising the problems in managing emergency beds can be the first measure to seek changes in the management process at all levels.
A comprehensive analysis of hospital processes is essential to establish better policies, develop decision support tools and contribute to the overall improvement of the hospital system's performance (He et al., 2019). Landa et al. (2018) report that there are few studies related to managers' decisions on BM, including at the operational and tactical levels, which is why they deemed it relevant to research how daily bed allocation decisions are made. Thus, bed managers can shed light on measures to reduce inefficiency and to improve care. Managing hospital beds is invariably complex, regardless of hospital units. However, it may be even more difficult to act in EDs, due to the nature of caring for patients who need within a short period of time acute care. In light of all the above, understanding the perception of bed managers is relevant to identifying and implementing improvements in the management of beds in organizations.
With this in mind, the research question of this study is the following: how do health professionals manage beds in an ED? To answer this question, two organizations were investigated – one public and the other private, both large and highly complex in the city of Porto Alegre. This study aims to identify the factors that influence the management of emergency beds based on an in-depth qualitative analysis.
To achieve this objective, we surveyed the perception of bed managers regarding their work-as-done, factors, bottlenecks, and difficulties in the management of hospital emergency beds. Nevertheless, it was considered that individuals have limited rationality in the decision-making process (Melo & Fucidji, 2016). Finally, recommendations are suggested to hospital BM, taking into account their constraints (material and human).
This research is outlined as follows, after this section of the introduction, the remainder is section two, presenting the theoretical framework for this research. Then, the methodological procedures are explained in the third section. Subsequently, in the fourth section, the results and discussions are addressed. Afterward, considerations are weighed in the fifth section, and the bibliographical references are presented at the end.
2. Literature Review
In order to provide a theoretical basis for this research, articles related to the management of hospital emergency beds in Brazil were researched based on qualitative research approaches to the problem. The search was carried out in the scientific research base of Google Scholar, including the last six years, and using the keywords: “management of emergency beds” with the respective Boolean operators OR “management of beds” (which is a broader term but a valid term for beds of inpatient care) AND “hospitals” AND Brazil.
The search results showed a number of 45 articles. Subsequently, the abstracts were read, excluding 10 articles that dealt with bed management with different approaches regarding the research, for example, the application of information technologies in BM, hospital indicators among others. Also excluded were 22 publications from conferences, theses, or dissertations from the portfolio of studies selected for this research.
2.1. Management of Beds in Emergency Departments and Inpatient Care Units
Table 1 summarises the theoretical analysis of the articles that guided this study on ED BM. Next, the challenges and solutions for BM in hospital emergencies pointed out by the authors of the aforementioned articles are presented.
Through a systematic review of the literature, Raffa, Malik, & Pinochet (2017b) found just a few studies analyzing the variables that affected the management of hospital beds and identified which variables in the internal environment are important in BM. In line with Machado & Machado (2019), whose work identified the reasons that interfere with discharge and BM through an integrative review.
Rocha et al. (2018) evaluated the web-based implementation of electronic Kanban in inpatient beds. The Kanban-based tool, accessed via the web by a BM team, proved to be effective in reducing patients' LOS. Meanwhile, Mattos et al. (2019) selected 13 articles for an integrative review on the use of Kanban in health management. Such an effort found two main areas emerging from the literature, the quality of health care and patient flow.
As well as, Silva et al. (2021) carried out a bibliographic review on the implementation of Kanban in BM and presented the main factors that made this implementation difficult. Namely, top management with no interest in adopting the tool, few people in the implementation team, lack of knowledge to implement Kanban, manual control systems that delay the flow of information, and resistance from health professionals.
Matos & Bastos (2018) investigated how the interaction of sectors can contribute to the management of hospital beds. The main challenges found in the literature were the need for knowledge in the areas of public health policies, information systems, planning, and strategy. In addition, they highlighted the main advantages of managing hospital beds properly. In opposition to Wasgen et al. (2019), who proposed three measures for the whole hospital BM through a theoretical model, in which they suggested agility in cleaning the beds, medical discharge plans, and the creation of waiting for spaces after medical discharge to improve BM.
Souza et al. (2020) described the operational aspects of BM in a hospital in Jequitinhonha. Supported by interviews with health professionals, using the content analysis technique to categorize the textual bodies of the analysis. As well as Oliveira & Bittencourt (2020) evaluated indicators and presented the perception of health professionals from the Inpatient Management Center (NGINT) of a public hospital in the Federal District through semi-structured interviews. In the interviews, the following themes emerged: human resources, decision autonomy, recognition of NGINT's work, and work tools (information system). In the same year, Oliveira et al. (2020) conducted action research with a multidisciplinary team of nine people in an ED to implement the Kanban.
Two other studies used the content analysis technique. In the first work, Borges et al. (2020) conducted 32 interviews with health professionals working in the management of hospital beds. As a result, three categories were raised from these interviews. The first refers to structuring services, highlighting professional qualifications, difficulties, and facilities. The second category concerns the work environment and process, such as autonomy, support services, decision-making, and nurses' activities in managing hospital beds. The third category refers to the results of the nurse's performance in the management of hospital beds concerning occupancy rate indicators and LOS of the patient, among others. In the second study, Fogaça et al. (2021) interviewed 17 nurses, from which three main categories emerged: (i) the profile of the BM team; (ii) the role of nurses in BM; and (iii) difficulties and potentialities in BM processes. Furthermore, an ethnographic study of nurses in the management of beds in the department during COVID-19 was carried out by Alonso et al. (2022).
2.2. The Importance of Bed Management
To achieve a high level of performance, a hospital organization needs to minimize the costs of providing services, maximizing production capacity with the appropriate sizing of human resources, materials utilized, and pertinent infrastructure (Landa et al., 2018; Raffa et al., 2017b). One of the strategies to minimize costs is accurately monitoring the flow of patients admitted to the hospital. The role of the bed manager is to report and coordinate, in real-time, the volume of patients who demand beds and the occupancy rates, synchronized with discharge forecasts, that is, to balance the supply of beds with the demand for beds in the ED (Landa et al., 2018).
Machado & Machado (2019) discussed hospital BM and the internal variables that affect this management. According to the authors, bed managers in hospital organizations are key elements, given their perceptions regarding the influencing factors in BM (Oliveira & Bittencourt, 2020). BM is a complex activity that interferes with hospital management and affects hospital performance as a whole. It involves all levels of the hierarchical structure, from operational to strategic activities, covering elements involving the patient and related to the hospital bed (Borges et al., 2020; Machado & Machado, 2019).
The importance of studying BM in Brazilian organizations also stems from the scarcity of published research. Oliveira & Bittencourt (2020), Raffa et al. (2017b), Souza et al. (2020), and Wasgen et al. (2019) consider that, despite the importance of BM for hospitals, there are a small number of articles available in journals. For these authors, there is a lack of empirical studies on the management of hospital beds in Brazil. In this sense, Machado & Machado (2019) found, through an integrative review study, that the number of publications on BM and hospital discharge in the country is insufficient. Additionally, Wasgen et al. (2019) state that there is a shortage of qualitative empirical studies on BM.
Essentially, BM is a process of adjustment between the demand and supply of hospital beds. Its objective is to provide access in accordance with the demand, reducing the number of unattended patients due to the lack of hospital beds (D'Aquino, 2017; Souza et al., 2020). So, BM should contribute to increasing hospital bed availability, and thereby, it is a strategy to mitigate the problem of hospital overcrowding.
The size of a hospital is determined by the number of beds, which, in turn, is one of the determinants of the hospital's capacity to provide care (D'Aquino, 2017). From this perspective, BM is considered a central component in hospitals, as it defines the operational capacity and, ultimately, the flexibility of these organizations. Thus, it is essential to continuously improve BM policies in order to achieve strategic organizational objectives and goals (Raffa et al., 2017b).
3. Methodological Procedures
In this section, we depicted the methodological procedures carried out for this research, which can be classified as objective, exploratory, and, as to the purpose, descriptive (Richardson, 2009). Data were collected and analyzed using a qualitative approach, using the technique of in-depth semi-structured interviews, and the method used was content analysis (Bardin, 2011). The operationalization of this research occurred through a case study.
3.1. Case study Selection and Characterization
In the first half of March 2021, the metropolitan region of Porto Alegre (the capital city of the state of Rio Grande do Sul) faced the second wave of COVID-19, with an occupancy rate of ICU beds equal to 117.43% (SMS, 2021), this overcrowding crisis reached several areas of hospitals, including EDs, with crowds that made it impossible to care for some patients. The case studies selected in this analysis refer to two of the largest hospitals (i.e., number of beds), one public and one private, located in Rio Grande do Sul.
Hospital A is a large public university hospital. It mainly serves patients from the Unified Health System (SUS), with an operational capacity of more than 1000 beds, the majority (+75%) being offered to the SUS. The average occupancy rate of the hospital is 95%, with peaks of demand often reported that generate an imbalance between the demand and supply of hospital beds. Hospital A is recognized by the Brazilian Ministry of Health as one of the best public hospitals in the country in the high complexity category, offering a wide range of specialties. It also has international recognition for its scientific production and health researchers' training.
Hospital B, which is private, has a team that works exclusively in BM, recognized as the hospital bed center. In contrast, Hospital A, which is public, does not have a unit dedicated solely to managing EDs beds since this function is assigned to the three EDs managers, who also act as physicians on duty. Hospital B is also considered of excellence by the Brazilian Ministry of Health, obtaining several international recognitions related to quality, as raised in an institutional presentation carried out before the interviews by Hospital B's consultancy representative.
Hospitals have different profiles regarding the services offered to their patients, with Hospital B recognized for the quality of care, justified by the number of awards. In contrast, Hospital A is recognized for its strong performance in scientific research, in addition to having been internationally accredited. Table 2 presents the characterization of the studied hospitals.
3.2. Data Collection
Data collection was performed through in-depth interviews. In order to conduct the interviews, a semi-structured script was used (see Appendix A). The content analysis method proposed by Bardin (2011) was used for data processing. The interviews were carried out from April to May 2021 with professionals who work with BM at Hospitals A and B.
The interviews were conducted via videoconference (Google Meet ®) on dates suggested by the managers. Right at the beginning of each interview, permission was formally requested to record them, which was granted. The researchers were not authorized to identify the hospitals or the subjects (managers). Six interviews were carried out, of which the interviewees are characterized according to Table 3. The sample purposely chose professionals from the hospital management areas of hospitals A and B.
Regarding the characterization of the interviewees, the managers and coordinators are responsible for their units; some play more than one role in the hospital. Each has at least eight years of experience in hospitals and extensive experience in their areas of expertise. In addition, participants have a direct relationship with hospital BM. Participants were mostly female. The interviews were recorded and fully transcribed using Microsoft Word®. Subsequently, a floating reading of the textual corpus was carried out, and the material was edited to correct spelling errors. The corpus of interviews comprised a total of 28 pages, single-spaced and in 12-point font.
Data from primary sources (interviews) were triangulated (Yin, 2014) using theoretical propositions (literature review). The content analysis followed the sequence indicated by Bardin (2011): (i) pre-analysis, (ii) analytical description, (iii) referential interpretation as a thematic analysis within the case, followed by (iv) cross-analysis, which consists of a thematic analysis between the cases, highlighting convergences and divergences between the contents (Creswell & Creswell, 2018).
4. Results
In this section, the results are shown in Table 4, classified into dimensions, and categorized by hospital BM factors by means of an analysis of interviews. Subsequently, the results relate the findings of the present study with the reviewed literature.
The review of the literature made it possible to identify the current and frequent factors that influence BM in hospital emergencies in Brazil. It is worth remembering that the studies found are in the Brazilian context since the BM problems of the Brazilian reality present some differences from what is observed in hospitals in developed countries. The themes that emerged from the literature and interviews were identified and grouped in Table 4. They were: family and patient; communication; length of stay (LOS); discharge planning by the team; performance goals; decisions shared between units; occupation planning; human resources; and COVID-19. For contextualization purposes, four dimensions were classified according to La Forgia & Couttolenc (2009): processes, resource management, structural characteristics of the provision of care services, and hospital demand.
4.1. Textual Analysis and Triangulation of Factors for BM
In order to identify the main themes addressed in the interviews, a survey of the most frequent words in the corpus of interviews was carried out. According to Camargo and Justo (2013), the word cloud is a basic text visualization technique that organizes and groups words according to their frequency and enables quick identification of keywords in a textual corpus. Thus, to build a word cloud with the interview data, the Voyant Tools ® software was used (Sinclair & Rockwell, 2016). Figure 1 shows the word cloud generated based on these transcripts. Thus, it can be seen that the words highlighted by the interviewees were: pacientes—patients (309); emergência—emergency (174); leitos—beds (172); hospital (103); alta—discharge (54); tempo—time (49); COVID-19 (40); demanda—demand (40); equipe—team (36); internação—hospitalization (32); pandemia—pandemic (29); gestão de leitos—bed management (27); UTI—ICU (24); altas—discharges (23); fluxo—flow(22) and so on. The predominant hospital units in the interviewees' statements were emergency, intensive care unit (ICU), and ward, as evidenced by the word cloud (Figure 1).
The uncertainty of the arrival rate at the ED reported at different times in the interviews shows the concern of managers about forecasting demand, as the data reveal a high variability and consequently make it difficult to plan the demand for beds in the ED. All interviewees mentioned that the historical average and experiences from previous periods (seasonality of demand, i.e., periods with greater or lesser demand) are the only information for decision-making related to planning resources in the short, medium, and long term. In this context, to assist in the decision-making process, hospitals could incorporate simulation models, machine learning algorithms, or statistical models to help forecast demand with better accuracy (He et al., 2019).
In line with Figure 1, COVID-19, lack of demand forecast, and hospital discharge are some of the problems faced in the management of emergency beds. The words patient and flow also appear as the most and least frequent, respectively. Corroborating with several studies that consider patient prioritization and care flows in the management of hospital beds (He et al., 2019). The terms pandemic and COVID-19 were important for BM, as they ultimately reveal that this external variable influenced emergency department activities in the period investigated by this study.
Table 5 presents the triangulation of the most important factors for BM in the studied emergencies, qualitatively compared with the literature on BM. According to Table 5, the factors with the highest incidence for BM in EDs are: “pLOS” (cited by 4 interviewees and 8 articles); “discharge planning by the team” (cited by 3 respondents and 8 articles); “bed occupancy planning” (cited by 2 interviewees and 10 studies); “family or patient resistance” (cited by 3 interviewees and 4 articles); “performance goals” (cited by all respondents and 2 articles); “communication failures” (cited by 2 interviewees and 8 articles); “decisions shared between units” (cited by 5 interviewees and 2 articles); “nurses” (cited by 4 interviewees and 6 articles); and “COVID-19” (cited by 5 respondents and 2 articles). In addition, the factors “bed management policies” and “manager autonomy” did not converge with the opinions of most respondents.
The factors shown in Table 5 are linked in different ways throughout the patient's journey in the ED. For example, it is common to have non-clinical factors that increase the length of time patients use beds (Raffa et al. 2017c). The pLOS in the EDs was associated with the various difficulties faced by families in vacating the bed. This agrees with the findings of Bryan et al. (2006) on the perceptions of bed managers that the family's resistance can be one of the main factors that interfere with the patient's pLOS. The multidisciplinary team needs to promote care guidelines for patiente and family members, thus enabling better self-care conditions for the patient (Fontana, Chesani, & Menezes, 2017; Fontana, Chesani, & Nalin, 2017; Suzuki et al., 2011). Other examples are the performance targets of the EDs not being achieved due to a lack of communication between the units and teams, with consequences in both hospitals associated with the difficulties shown concerning hospital discharge planning, as well as the prolonged occupation of patients who would be able to be discharged, among other influence relationships of the observed categories. Therefore, it is estimated that any improvement in any of these variables can trigger a positive effect on the availability of emergency beds.
Identifying the decisive factors in the BM process in EDs is essential to guide managers, health administrators, researchers, and other stakeholders to carry out effective interventions that can reduce overcrowding, promote beneficial organizational changes, such as discourage departmentalization and organizational silos, and can even bring improvements to patient and family satisfaction with care, as well as the optimized use of resources.
5. Discussion
In this section, the discussions are organized into subsections representing the main factors related to BM in EDs from the analysis of interviews and relating these findings to the reviewed literature.
5.1. Family or Patient
It refers to family members and patients as factors that interfere with the LOS of the patient in the ED. During the interviews, it was identified that at Hospital B, the needs of patients and their families could influence hospital discharge due to the lack of follow-up and understanding of the discharge plan by the patient and family. In addition, resistance to releasing the bed by family members increases the LOS, reducing the bed turnover capacity of the ED at Hospital B. The resistance of the patient and/or family member to releasing the bed is a problem that frequently occurs in hospitals (D'Aquino, 2017; He et al., 2019; Machado & Machado, 2019; Silva et al., 2014). One of the reasons that lead a family to resist removing the patient from the hospital (completing the hospital discharge process) is the social conditions in which the family and the patient live, as there are difficulties related to care after hospital discharge, which is one of the main reasons for delays in hospital discharge (Silva et al., 2014). Also, regarding the LOS, Werner (2017) and He et al. (2019) state that the delay in hospital discharge may be associated with the patient's willingness to complete the hospital discharge process, thus having a negative effect on new admissions and resulting in potential congestion in the upstream units.
5.2. Communication
It refers to aspects of communication between sectors and within each department carried out among its employees. Lack of communication is one of several factors that make managing beds in EDs a complex task (He et al., 2019; Werner, 2017). Several studies have raised communication inefficiency as an important category for BM (Borges et al., 2020; Fontana, Chesani, & Menezes, 2017; Machado & Machado, 2019; Raffa et al., 2017c; Souza et al., 2020).
In Hospital A, a lack of communication between the supervising physician and the assistant physician was observed. Communication between the departments' teams occurs with some failures related to the transfer of patients from the ED to the wards, as reported by the informants in Table 4. This communication process between the teams interferes with hospital discharge, resulting in a longer LOS.
Failure in communication is identified as the main barrier to freeing up beds in hospital emergencies in the literature, as it can influence everything from delays in completing discharge to patient safety (Souza et al., 2020; Wasgen et al., 2019 ; Werner, 2017). Machado & Machado (2019) argue that the lack of communication and integration between interdisciplinary teams generated a significant increase in the average LOS of the patient, constituting a variable that affects BM.
5.3. Lenght of Stay
Regarding the LOS of the patient, the results indicated that, frequently, the patient occupies the bed longer than necessary for non-clinical reasons. Suzuki et al. (2011), Silva et al. (2014), and He et al. (2019) argue that unnecessary stay is a concern for hospitals, as it generates increased operating costs, in addition to exposing the patient to risks related to a hospital infection, depression or loss of physical conditioning, these being all unnecessary risks.
The overcrowding of the ED is a problem caused, to some extent, by the unnecessary occupation of hospitalized patients who would be able to be discharged. Thus, the bed is invariably vacated when the ED is under pressure from incoming patients. For instance, in Hospital B (see Table 4), where in practice, patient admissions to the ED are predominantly pushed and not pulled by the inpatient sector. In this context, He et al. (2019) consider that the performance of each sector can affect downstream or upstream units, and patient transfers between units can critically change the availability of emergency beds.
5.4. Discharge Planning by the Team
Hospital discharge planning is carried out with limitations arising from postponed clinical decisions due to the absence of the supervising physician, who validates the clinical decision of the resident physician at Hospital A, as shown in Table 4. In fact, the delay in the discharge process of hospitalization was identified as a problem in both Hospitals A and B. Adwok (2014) states that delayed discharge can lead to patient dissatisfaction. Thus, this implies one more aggravating factor in the management of the ED as a whole.
Predicting hospital discharge is also a difficulty encountered. The physician's lack of communication with the family regarding the patient's discharge generates delays in the availability of beds. The discharge plan should be established upon patient admission and identify the actual care needs over the LOS (Wasgen et al., 2019).
5.5. Performance Goals
At Hospital A, the goals are not known by the entire team, although there is a work of sharing goals by the medical manager (A2). Whereas Hospital B already has its goals known and pursued by all teams. This data was observed in the interviewees' speeches; when they are not meeting the goal, an action plan is established to improve bed vacancy time. Thus, at Hospital B, it was found that there is a practice of disclosing the goals achieved by the command center to the multidisciplinary teams of each unit. In this sense, in order to achieve efficient BM in EDs, it is essential to share and commit to the goals established by the organization, thus enabling the optimization of resources (Raffa, 2017).
The hospital's command center, coordinated by interviewee B1, organizes and controls all performance indicators and targets. After installing this command center, there was an increase in efficiency concerning hospital goals. However, the goal of vacating emergency beds was not being achieved due to a change in the profile of patients due to the demands for the treatment of COVID-19. Raffa et al. (2017c) and Raffa (2017) state that the achievement of goals is relevant for the management of these beds since when goals are being achieved, surgeries are canceled less frequently, with a faster turnover of beds, for example. And the average LOS will be within the expected range. Still, regarding the goals, the command center (from Hospital B) monitors and coordinates the goals of all sectors. Respondents B1, B2, B3, and B4 reported efficiency improvements after implementing the center.
5.6. Decisions Shared Between Units
The hospital EDs have different management policies and hold at least one meeting daily, in the morning, with the teams of each hospital unit to discuss the potential barriers of the day and decide on the expected discharges, thus trying to discharge all patients by noon (He et al., 2019). This model was adopted in the ED of Hospital A, where a huddle meeting is held with the multidisciplinary team scheduled for mid-morning with an average duration of 25 minutes to discuss the flow of patients in each intra-unit, their evolution, potential transfers between emergency units or another hospital unit, as well as other demands related to patient health care.
In the case of Hospital B, the ED participates in a meeting in which the decision-making processes related to daily bottlenecks are discussed by those responsible for each unit together with the hospital bed command center. According to the verbalization made by interviewee B1: “A daily meeting is held with all managers who request beds. In this meeting, the priorities of the day are raised, with the coordinators of the ICU, ED and maternity and pediatrics wards.”. In the same sense, reinforced interviewee B2 “Since we started to create the BM committee (command center), which meets every day in the morning, we can see where the hospital's bottlenecks are”. This is how the decision-making process takes shape concerning the transfer of patients between units and the occupation of beds at Hospital B. Therefore, decisions related to BM are a process shared by the command center with the managers of all units in this hospital.
5.7. Bed Occupancy Planning
As for bed occupancy planning in the ED of Hospital A, the difficulty is that other departments have difficulties in cooperating and integrating information, especially in real-time. This was observed based on the statement of interviewee A1: “We have no idea of the number of vacant beds. We have to be prepared not to have any beds. If it eventually does, great, but it's something I don't know how to determine. So I can't predict. These are decisions that do not depend on the ED, as I am not aware of the patients who are hospitalized in the wards. I do not know how many discharges are being generated in other departments. Other teams are responsible. We have lost this contact; if they were discharged from the hospital, the beds are made available to the ED (...) in the hospital things are quite departmentalized. As I described before, I request beds from the wards, but I have no autonomy over the occupation of these beds (...) the teams work a lot in their specialties without realizing how their work affects the ED.".
Therefore, management does not know about ward beds to relocate patients from the ED there and make more beds available. They do not see the availability of beds in the wards in real-time. This finding is corroborated by He et al. (2019) and Raffa (2017), which highlight the departmentalized organizational structure of hospitals as the cause of some of the difficulties in managing beds, such as difficulties in collaboration between the different units.
Hospital B has difficulties managing discharges since they do not occur before noon, even in periods of high hospital occupancy rates. In this sense, actions are needed to minimize this situation, which is caused by the absence of the attending physician at the right time. This scenario can be considered a bottleneck for BM, as it substantially delays the discharge process by hours, increasing the bed occupancy time. The absence of a hospital discharge team to speed up this process, which could still be carried out in the morning, was also indicated as a difficulty by the interviewees. Indeed, both hospitals, during the pandemic, worked with an average hospital occupancy rate exceeding the recommended standard, above 85%, and the WHO recommendation is not to exceed this percentage in order to be able to receive patients in the ED (He et al., 2019). According to Jones (2009), the average occupancy rate of the entire hospital should not exceed 85% to maintain quality care, as well as the average LOS in the ED, within the range of 3 to 5 days.
5.8. Nurses
In line with the textual corpus of respondents A1, A2, B1, B4, and B5 and the literature reviewed on the role of nurses in BM, it was verified that this health professional performs a key role in BM, as they determine the flows of patients, and thus, are seen as a “facilitator” in the BM process. In general, nurses are recognized as crucial for more efficient management. These professionals perform functions at different stages in EDs: patient admission, sharing information with managers, transfers, and hospital discharge, among others.
Suzuki et al. (2011) concluded that the nurse has a key role in identifying the needs of patients, providing care guidance to the family, as well as the entire hospital discharge planning. Borges et al. (2020) analyzed the performance of nurses in BM, and the results revealed that they are fundamental professionals to integrate management, allocate patients, and improve LOS and communication between units.
Souza et al. (2020) emphasized nurses as essential for implementing and collaborating in BM, through their role as facilitators of operational work processes. Alonso et al. (2022) identified the main challenges nurses face in managing beds during the COVID-19 pandemic, in the dimensions of structure and processes, where the main challenges nurses face are found. Since such challenges are generated by inadequate infrastructure and the lack of establishing contingency plans for health crises, which amplify the challenges in BM.
6. Final Considerations
The research objective was to understand how BM works in EDs based on the perception of professionals working in decision-making processes, as well as to identify the main factors that influence this management. With regard to functioning, it is observed that managers decide based on a limited amount of information, which can characterize limited rationality in the decision-making process of managing emergency beds.
The relevant factors for emergency BM in the studied hospitals were seen in Table 4, where it was verified that most of the factors identified in the literature and highlighted by the interviewees refer to the internal environment related to resource management practices and processes, such as communication between unit teams; awareness and achievement of goals; decisions shared between units; occupancy and discharge planning by the teams; pLOS; nurses, with the exception of COVID-19, which is related to the external environment. Therefore, it is possible to observe the distinction of influence of environments, in terms of internal factors prevailing over external factors, for management purposes. To the best of our knowledge, this is the first study on hospital emergencies in Rio Grande do Sul state (Brazil) identifying the main factors which influence BM and presenting its downsides in the Brazilian context. Additionally, tips are provided (in Table 5) to mitigate such reported difficulties.
As management recommendations, it is suggested to promote care guidelines for family members, sharing performance goals among employees and even making indicators available from other intra-hospital units, develop awareness programs to involve the multidisciplinary team, make hospital occupancy rate available to emergency managers in real-time and monitor indicators more effectively as well as coordinating the integration and collaboration between the other intra-hospital units and the ED.
As limitations, it was seen that the most important factors for BM in the studied EDs are related to the internal environments in both organizations. However, the relationships between these factors are not explored. For example, what effects does each have on the other? Despite these relationships being important, as there are negative or positive influences between the variables, this study did not address them. Therefore, in light of the results presented, several opportunities for improvement were found, and consequently, they should be studied on how to implement them. Thus, it is recommended that future studies investigate appropriate techniques and tools to plan the implementation of strategies addressed to each identified factor.
Appendix A

Table A1.
Semi-structured interview script.
| Questions |
|---|
| 1. Please tell us briefly about your career experience so far. What is your current job? How long have you been in this role? What are your functions and main activities? 2. How do you plan the number of beds to meet the emergency demand? 3. How does decision-making occur in emergency bed management? Do you consider that there is any inefficiency in this process? What is missing for this process to be efficient? 4. How do you predict the volume of patients? Do you use any method to predict the arrival of patients? If yes, what is the method, and how is it applied? What are the advantages and disadvantages of this method? 5. What are the main difficulties in bed management? Are there bottlenecks (factors that delay) or facilitators (factors that benefit) in this process? Name the ones that occur most often and that you remember. For each bottleneck indicated, what actions are taken to reduce its effects? 6. Regarding bed management in your emergency service, which management components are not automatable and create a demand for the manager's decision? 7. Can you anticipate future occupancy in the short term? If so, how and for how long? If not, why? 8. Is there any document (report) that identifies the seasonality of the emergency department's attendance in recent years? If so, can we have access? 9. In the context of bed management in the ED, is there anything you would like to highlight? Any final thoughts? |
Source: Authors.
References
- Adwok, J. (2014). Application of Brim’s and Simon’s Sequential Decision Theories in Healthcare Administration. Journal of Biology, Agriculture and Healthcare, 4(14), 23–32.
- Alonso, C. da S., De Souza Pires Silva, D. E., Da Cruz Costa, F., Esmério Pimentel, F., Vieira Novaes, J. A., & Cabral de Castro e Silva, R. R. (2022). Desafios enfrentados por enfermeiros na gestão de leitos hospitalares durante a pandemia por COVID-19. Nursing (São Paulo), 25(291), 8342–8351. [CrossRef]
- American College of Emergency Physicians – ACEP. (2019). Crowding. Policy statement. Annals of Emergency Medicine, 61(6), 726–727. https://www.acep.org/patient-care/policy-statements/crowding/.
- BARDIN, L. Análise de conteúdo. São Paulo: edições 70, 2016. 280p. ISBN: 978-85-62938-04-7.
- Borges, F., Bernardino, E., Stegani, M. M., & Tonini, N. S. (2020). Performance of nurses in the bed management service of a teaching hospital. Revista Brasileira de Nursing, 73(4), 1–8. [CrossRef]
- Bryan, K., Gage, H., & Gilbert, K. (2006). Delayed transfers of older people from hospital: Causes and policy implications. Health Policy, 76(2), 194–201. [CrossRef]
- Camargo, B. V., & Justo, A. M. (2013). IRAMUTEQ: Um software gratuito para análise de dados textuais. Temas Em Psicologia, 21(2), 513–518. [CrossRef]
- Creswell, J. W., & Creswell, J. D. (2018). Research Design: Qualitative, Quantitative, and Mixed Methods Approaches (5th ed.). Sage publications.
- D’Aquino, S. F. (2017). Proposta de modelo de referência para o processo de gestão de leitos hospitalares. [Masters dissertation, Universidade Federal de Santa Catarina]. Repositório Institucional da UFSC. https://repositorio.ufsc.br/xmlui/handle/123456789/183604.
- Emergency Nurses Association – ENA. (2006). Emergency nurses association position statement: Crowding in the emergency department. Journal of Emergency Nursing, 32(1), 42–47. [CrossRef]
- Fiocruz. (2021). Observatório COVID-19 aponta maior colapso sanitário e hospitalar da história do Brasil. Fundação Oswaldo Cruz (Fiocruz). https://portal.fiocruz.br/sites/portal.fiocruz.br/files/documentos/boletim_extraordinario_2021-marco-16-red-red-red.pdf.
- Fogaça, C. S., Braga, L. A. S., Peres de Carvalho, E. M., & Göttems, L. B. D. (2021). Atuação do enfermeiro no gerenciamento dos leitos hospitalares na percepção dos profissionais de enfermagem. New Trends in Qualitative Research, 8, 528–537. [CrossRef]
- Fontana, G., Chesani, F. H., & Menezes, M. (2017). As significações dos profissionais da saúde sobre o processo de alta hospitalar. Health & Social Change, 8(2), 86–95.
- Fontana, G., Chesani, F. H., & Nalin, F. (2017). Percepções dos profissionais da saúde sobre o processo de alta hospitalar. Revista Da UNIFEBE, 1(21), 138–156.
- He, L., Chalil Madathil, S., Oberoi, A., Servis, G., & Khasawneh, M. T. (2019). A systematic review of research design and modeling techniques in inpatient bed management. Computers and Industrial Engineering, 127(October 2018), 451–466. [CrossRef]
- Jones, R. (2009). Emergency admissions and hospital beds. British Journal of Health Care Management, 15(6), 289–296. [CrossRef]
- La Forgia, G. M., & Couttolenc, B. F. (2009). Desempenho hospitalar no Brasil: em busca da excelência (1st ed.). Singular. https://pesquisa.bvsalud.org/portal/resource/pt/lil-695495.
- Landa, P., Sonnessa, M., Tànfani, E., & Testi, A. (2018). Multiobjective bed management considering emergency and elective patient flows. International Transactions in Operational Research, 25(1), 91–110. [CrossRef]
- Machado, D. de C., & Machado, A. C. A. (2019). A otimização do processo de gerenciamento de leitos e alta hospitalar. Revista Saúde Coletiva, 9(50), 1866–1872.
- Matos, F. de, & Bastos, C. M. de A. M. (2022). A interação dos setores no processo de gestão de leitos hospitalares. Scientia Academicus, 3(1), 2–16.
- Mattos, C. M., Farias de Oliveira, M. F. de O., Alves Vilar, A. M., Silvino, Z. R., Silvino, Z. R., & Andrade, M. (2019). A aplicação do Kanban como ferramenta de gestão em serviços de saúde: revisão integrativa. Nursing (São Paulo), 22(254), 3031–3038. [CrossRef]
- Melo, T. M., & Fucidji, J. R. (2016). Racionalidade limitada e a tomada de decisão em sistemas complexos. Revista de Economia Política, 36(3), 622–645. [CrossRef]
- Noronha, K. de S. V. M., Guedes, G. R., Turra, C. M., Andrade, M. V., Botega, L., Nogueira, D., Calazans, J. A., Carvalho, L., Servo, L., & Ferreira, M. F. (2020). Pandemia por COVID-19 no Brasil: análise da demanda e da oferta de leitos hospitalares e equipamentos de ventilação assistida segundo diferentes cenários. Cadernos de Saúde Pública, 36(6), 1–17. [CrossRef]
- Oliveira, B. D. P., & Bittencourt, R. J. (2020). Avaliação por triangulação de métodos de um núcleo de gestão de leitos em um hospital público do Distrito Federal. Revista de Gestão Em Sistemas de Saúde, 9(3), 406–432. [CrossRef]
- Oliveira, I. S. de, Lima, E. de F. A., Silva, R. I. C. da, Figueiredo, K. C., Dias, I. C. B., & Primo, C. C. (2020). Gerenciamento de leitos na urgência e emergência utilizando o kanban. Research, Society and Development, 9(10), e1329108354. [CrossRef]
- OPAS. (2021). Folha informativa sobre COVID-19. Organização Pan-Americana Da Saúde (OPAS). https://www.paho.org/pt/COVID-1919.
- Raffa, C. (2017). Análise das variáveis do ambiente interno para o gerenciamento de leitos em organizações hospitalares privadas. [Doctoral thesis, Fundação Getulio Vargas - Escola de Administração de Empresas de São Paulo]. http://hdl.handle.net/10438/18070.
- Raffa, C., Malik, A. M., & Pinochet, L. H. C. (2017a). A Tecnologia da informação no apoio À Gestão De Leitos: Um Estudo Multicaso Em Hospitais Privados. Revista Administração Em Diálogo, 19(3), 1–23. [CrossRef]
- Raffa, C., Malik, A. M., & Pinochet, L. H. C. (2017b). Análise das variáveis do ambiente Interno no gerenciamento de leitos em organizações hospitalares privadas: aplicação do software Nvivo. Revista de Administração Hospitalar e Inovação Em Saúde, 14(4), 20–39. [CrossRef]
- Raffa, C., Malik, A. M., & Pinochet, L. H. C. (2017c). O desafio de mapear variáveis na gestão de leitos em organizações hospitalares privadas. Revista de Gestão Em Sistemas de Saúde, 6(2), 124–141. [CrossRef]
- Richardson, R. J. (2009). Pesquisa social: métodos e técnicas (J. A. de S. Peres (ed.); 3rd ed.). Atlas.
- Rocha, H. A. L., Santos, A. K. L. da C., Alcântara, A. C. de C., Lima, C. S. S. da C., Rocha, S. G. M. O., Cardoso, R. M., & Cremonin, J. R. (2018). Bed management team with Kanban web-based application. International Journal for Quality in Health Care, 30(9), 708–714. [CrossRef]
- Silva, T. G. E., Silva, M. F. S. B. da, Vieira, L. C. N., Pimentel, C. A., & Musetti, M. A. (2021). Contribuições do kanban eletrônico e tradicional para a gerenciamento de leitos hospitalares. Revista Produção Online, 21(3), 818–836. [CrossRef]
- Silva, S. A. da, Valácio, R. A., Botelho, F. C., & Amaral, C. F. S. (2014). Fatores de atraso na alta hospitalar em hospitais de ensino. Revista de Saúde Pública, 48(2), 314–321. [CrossRef]
- Sinclair, S., & Rockwell, G. (2016). Voyant Tools. GitHub. http://voyant-tools.org/.
- SMS. (2021). Painel Diário COVID-19. Secretaria Municipal de Saúde (SMS) da Prefeitura Municipal de Porto Alegre. Painel Diário Coronavírus Secretaria Municipal de Saúde (SMS) Da Prefeitura Municipal de Porto Alegre. http://lproweb.procempa.com.br/pmpa/prefpoa/sms/usu_doc/painelcovi15marco.pdf.
- Souza, D. M., Vasconcelos, B. F., Viana, D. M. S., Ribeiro, L. da C. C., & Lima, A. M. D. J. (2020). Gestão de leitos em um hospital polo da região ampliada de saúde Jequitinhonha: aspectos organizacionais e operacionais do processo de trabalho. Journal of Health & Biological Sciences, 8(1), 1–5. [CrossRef]
- Suzuki, V. F., Carmona, E. V., & Lima, M. H. M. (2011). Planejamento da alta hospitalar do paciente diabético: construção de uma proposta. Revista da Escola de Nursing da USP, 45(2), 527–532. [CrossRef]
- Tampubolon, L., & Pujiyanto. (2018). Bed management strategy for overcrowding at the emergency department: A systematic review. KnE Life Sciences, 4(9), 50–59. [CrossRef]
- Wasgen, A. M., Terres, M. da S., & Machado, B. F. H. (2019). O impacto do gerenciamento de leitos na gestão hospitalar. Revista Hospitalidade, 16(2), 31–49. [CrossRef]
- Werner, S. M. (2017). Proposta de um modelo de gestão para alta hospitalar baseado na abordagem Lean. [Masters dissertation, Universidade Federal de Santa Catarina]. https://repositorio.ufsc.br/xmlui/handle/123456789/179794.
- Yin, R. K. (2014). Case study research design and methods (5th ed.). Sage publications.
Figure 1.
Word cloud from interviews. Source: Created by the authors using Voyant Tools ® software (Sinclair & Rockwell, 2016)
Figure 1.
Word cloud from interviews. Source: Created by the authors using Voyant Tools ® software (Sinclair & Rockwell, 2016)
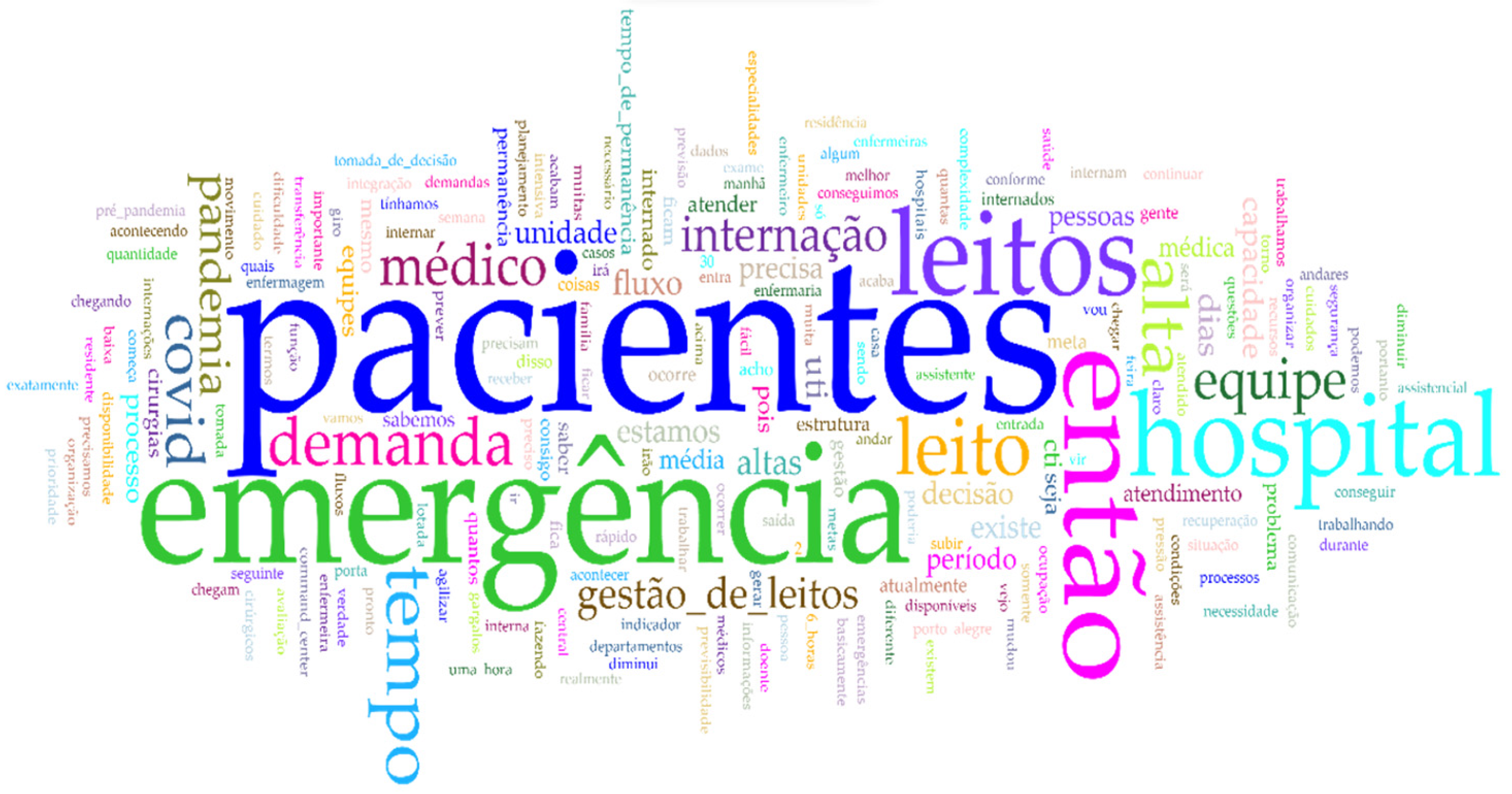
Table 1.
Selected studies on hospital BM (2017-2022).
| Authors | Research objective | Title* | Research method | Main results |
|---|---|---|---|---|
| Raffa & Malik (2017b) | Identifying variables related to the internal environment relevant to bed management in hospital organisations | Analysis of internal environmental variables in bed management in private hospital organizations: application of NVivo software | Systematic literature review, case study, and content analysis | Concerning the resource management practices, the author highlighted: occupancy planning, decision autonomy, and the use of goals and indicators. Regarding structural characteristics of service delivery, the hospital structure, information technology, equipment, and human resources stand out. In respect of processes, there are discharge planning, formalization, and clinical and communication protocols, which are determinants for management. Regarding operationalization, the decision-making of physicians and nurses' management knowledge were also factors that impacted BM. These authors concluded that these are the relevant internal factors for the performance and efficiency of BM. However, policies were inadequate and could be improved to achieve the organization's strategies, highlighting that it constitutes a strategic resource in hospitals. |
| Matos & Bastos (2018) | Introducing the complexity of BM and the importance of inter-sector teams’ interaction in the BM process | The interaction of the sectors in the process of management of hospital Beds | Scoping review | Communication and interaction between sectors can contribute to improving the management of hospital beds. |
| Rocha et al. (2018) | Measuring the effectiveness of e-Kanban in managing beds in a high complexity, private and accredited hospital | Bed management team with Kanban web-based application | Intervention research | The use of the e-Kaban tool in the management of hospital beds enabled the systematic monitoring and evaluation of patients by the multidisciplinary team. Kanban is continuously accessed via tablets, cell phones, or computers, reducing overall LOS and increasing bed turnover without reducing the occupancy rate. Finally, there was a decrease in the waiting time for hospitalization in EDs. |
| Wasgen et al. (2019) | Creating a theoretical model for BM | The impact of bedside management on hospital management | Literature review | According to the authors, the hospitals that adopted the measures proposed by their theoretical model can optimize the LOS of patients and increase the number of patients seen. |
| Machado & Machado (2019) | Identifying the reasons that interfere with hospital discharge and that impact on BM | Optimization of the hospital bed and hospital discharge management process | Integrative review | The main reasons are factors such as hospital discharge, lack of communication, discharge planning by the team, family refusal to remove the patient from the bed, and the increase of the LOS. These authors concluded that greater integration and effective team communication added to patients' follow-up through therapeutic plans. Besides, it can facilitate a more assertive management process. |
| Mattos et al. (2019) | To analyze the recent scientific production on the application of the Kanban tool in the management of health services, assessing the evidence and discussing the results | The application of Kanban as a management tool in health services: An integrative review | Integrative review | In the area of health care quality: Kanban contributed to cost reduction, error reduction, more effective care flows, and multidisciplinary teams informed in real time about the patient's status. In the area of patient flow: Kanban helped the multidisciplinary team in the management of inpatient and emergency beds, facilitated the identification of processes that needed to be improved or eliminated, and reduced waiting times for hospitalization, increasing the turnover of hospital beds. |
| Borges et al. (2020) | Analyzing the performance of nurses in BM service of a public teaching hospital | Performance of nurses in the bed management service of a teaching hospital | Theme-based content analysis | The knowledge employed by the nurse is mainly in patient management and flow. The main competencies were also reported, e.g., communication, agility, and decision-making. The main difficulties in managing hospital beds reported were poor communication, the clinical profile of the admitted patient incompatible with the care unit's capacity to provide care, and the organizational culture. The facilitator in the management of reported hospital beds was the centralization of management attributed to nurses. However, a limited autonomy of nurses regarding the management of beds was identified. |
| Souza et al. (2020) | Describing the organizational and operational aspects of the BM process at a hospital in the Jequitinhonha Expanded Health Region | Management of beds in a pole hospital of the Jequitinhonha expanded health region: organizational and operational aspects of the work process | Content analysis | Five main factors found were: the organization of patient admission and discharge processes, communication, correct referral of the patient to the appropriate ward, the organization of hospital care, and the organization of surgeries. They also found that there were efficiency gains in permanence, occupancy, and turnover rates after implementing BM. These authors concluded that strategic planning of hospital beds is essential to improve the operational aspects of hospital beds. |
| Oliveira et al. (2020) | Describe the development of protocols and flowcharts for the implementation of kanban in the urgency and emergency sector | Beds management in the urgency and emergency using kanban | Action research and content analysis | The participants considered the action research an adequate method to select the Kanban that was later implemented in the management of ED beds. The benefits and challenges identified in the tool's implementation were the optimization of beds, higher turnover of beds, an increase in the number of visits, and an improvement in the quality of the service provided. However, the participants had difficulties demonstrating to the managers the benefits of managing the ED and BM. |
| Oliveira & Bittencourt (2020) | Evaluating through the structure, process, and results. Also, presenting the perception of NGINT professionals about its operation | Evaluation by triangulation of methods in a bed management center of a public hospital in the Federal District | Case study | The results showed that the lack of personnel and recognition of well-performed work is not uncommon. The NGINT does not have the autonomy to decide about the beds; Ultimately, the admission and discharge of inpatients are determined by physicians. In addition, NGINT was evaluated as middling, with the occupancy rate and the average LOS rate below the expected performance. The decision-making over the beds was centered on the physician, not on the NGINT. In this way, a governance problem was diagnosed. Thus, establishing NGINT's power over beds was a measure recommended by the authors, who concluded that the established power structure was compromising the decision-making process of BM. |
| Silva et al. (2021) | Introducing the different features of traditional Kanban and e-Kanban for hospital BM | Contributions of electronic and traditional kanban to hospital bed management | Bibliographic review | A lean maturity improves the patient's LOS and assists in managing hospital beds. |
| Fogaça et al. (2021) | Analysing nurses' perception of the work process in BM | Nurses’ performance in the management of hospital beds in the perception of nursing professionals | Content analysis | According to the nurses, knowledge in management, assistance, functioning of the hospital as a whole, and the interaction between the units are fundamental in the management of beds. The nurse's role reduces the average LOS, increasing bed turnover, reducing overcrowding in the emergency department, and improving communication and transparency in the use of resources. The main difficulties in managing hospital beds were the absence of beds in good working order to allocate patients, communication failures between the teams of inpatient units, lack of trained managers to work in the area of BM, and lack of knowledge of care unit teams of the importance of BM. The potentialities found were the nurses' abilities to streamline various BM processes, such as reducing the waiting time for inpatient surgeries, reducing the waiting time for outpatient procedures, speeding up the transfer to the inpatient units, and reducing the number of patients in the ED. |
| Alonso et al. (2022) | Reporting challenges faced by nurses in managing beds in a hospital inpatient unit during COVID-19 | Challenges faced by nurses in managing hospital beds during the COVID-19 pandemic | Ethnographic research | The authors identified the challenges, which include the need to increase social distancing, and sharing bathrooms in the wards. As the use of bathrooms was limited to confirmed or suspected cases, this led to a reduction in the availability of beds, an increase in beds for clinical stabilization, electrical adaptations, changes in bed profiles, cancellation or suspension of surgeries, and even effective communication between the multidisciplinary team when admitting patients. |
* Note: Translated to English. Source: Authors
Table 2.
Characterization of the hospitals selected for this study.
| Hospital (A) | Hospital (B) | |
|---|---|---|
| Nature | Public institution and university - Covenant | Membership - Philanthropic - Private |
| Dimension | Large | Large |
| Localization | Porto Alegre | Porto Alegre |
| Characteristics | High complexity services; Assistance in the social, educational, and professional areas | High complexity services; Assistance in the social, educational, and professional areas |
| Hospital beds | 59 total 46 adult 13 pediatric |
38 total 30 adult 8 pediatric |
| Patient profile | High Complexity | High Complexity |
| Accreditation | Collaborator for the quality of management and hospital care at the Brazilian Ministry of Health A3P Certificate from the Ministry of the Environment Joint Commission International (JCI) from 2013 to 2021 and academically linked to a federal university |
Hospital of Excellence by the Brazilian Ministry of Health ISO 9001:2015 3M – Black Diamond Joint Commission International Affiliation with Johns Hopkins University |
| Technology of Information |
Applications for hospital management (AGHUse), which is the hospital management support system itself | MV Soul Orquestra Sênior and Own System |
Source: Authors.
Table 3.
Characterization of the interviewees.
| Interviewee | (A1) | (A2) | (B1) | (B2) | (B3) | (B4) | (B5) |
| Hospital | Hospital A | Hospital A | Hospital B | Hospital B | Hospital B | Hospital B | Hospital B |
| Sex | ♀ | ♀ | ♀ | ♂ | ♂ | ♀ | ♀ |
| Bachelor | Nursing | Medicine | Nursing | Medicine | Nursing | Medicine | Nursing |
| Postgraduate studies | Master in nursing, and specializations in emergency and family health | Intensive medicine, residency in emergency medicine, and MBA in business management | Specializations in hospital management and best care practice management | Internal medicine residency | Master's in health sciences and specialization in risk management | Residency in intensive care, master's, doctorate in intensive care, and university professor | Master in nursing and specialization in neurology |
| Role | Nurse at the Internal Regulation Center - NIR | Medical manager and physician in the emergency | Hospital operations coordinator | Chief emergency service manager | Adult and pediatric emergency care coordinator | Medical head of the adult ICU | ICU nursing coordinator |
| Organization time and current role | Emergency nurse: 7 years, 2011-2018. Nurse at NIR: 3 years | Physician on duty: 8 years and 4 months. Medical manager: 4 years | Emergency supervisor: 21 years old Emergency coordinator: 9 years |
Physician on duty in the emergency: 10 years between 2000-2010 Chief manager: since 2013 |
Nurse in the emergency: 9 years Care coordinator: 4 years |
Intensive care physician: 18 years old. Medical head: 2 years | ICU nursing supervision: 2 years ICU nursing coordinator: 6 years |
| Total hospital time | 10 years | 12 years | 30 years | 18 years | 9 years | 20 years | 8 years |
Source: Authors.
Table 4.
Excerpts from the interviews.
| Defining the main categories | ||
|---|---|---|
| Family and patient: It is a common problem with patients and family members not being able to complete the patient discharge process for a variety of reasons. The literature on BM frequently presents this difficulty in finishing healthcare assistance in hospital organizations (D'Aquino, 2017; He et al., 2019; Machado & Machado, 2019; Silva et al., 2014; Suzuki et al., 2011; Werner, 2017). | ||
| Communication: Communication between departments and teams is an important task in BM and is considered one of the main variables that can affect BM (Borges et al., 2020; D'Aquino, 2017; He et al., 2019; Machado & Machado, 2019; Raffa et al., 2017b; Souza et al., 2020; Werner, 2017). Effective communication is one of WHO's International Patient Safety Goals. | ||
| Prolonged length of stay (pLOS): Average LOS is the total number of days in bed divided by total admissions (Jones, 2009). It is the duration between admission and discharge of a patient. It is a widely used metric, one of the quality indicators related to BM (He et al., 2019). However, the literature shows that unnecessary stays often occur, usually for non-clinical reasons (D'Aquino, 2017; He et al., 2019; Machado & Machado, 2019; Raffa, 2017; Souza et al., 2020). | ||
| Discharge planning by the team: It is an interdisciplinary, complex process that involves identifying the needs of patients, providing guidance for family members, and coordinating those involved (Suzuki et al., 2011). | ||
| Performance goals: The literature shows that regardless of the type of organization, the goals need to be known by the teams for BM to occur in the best way. Raising awareness can streamline processes, remove bottlenecks, and improve BM. | ||
| Occupancy planning: This is an important stage of BM defined through the management policy adopted in hospitals. | ||
| Nurses: Nurses play a key role in BM. | ||
| COVID-19: It is an infectious disease caused by the new coronavirus SARS-CoV-2 (OPAS, 2021) that has changed the BM process due to patient needs, increased demand, and exclusive teams for care, among other unexpected developments. | ||
| Dimension | Category | Excerpt from the interview |
| Processes (internal environment) | Family and/or patient | Interviewee B1: The demand for care and the degree of dependence patients have on health care is also a problem affecting the delay in vacating beds. I think that the fear and anxiety of family members about taking the patient home demands more dedication from professionals when providing post-discharge guidance. |
| Interviewee B2: The main difficulty I see concerns the LOS of the patient in the hospital. I believe that patients could spend less time in the hospital but stay longer than they need to. It occurs because several forces make this happen, for example, issues of convenience for patients and their families. So sometimes, a chronic patient is admitted to the hospital, and everything conspires for him to remain admitted to the hospital. The family prefers it, and the patient prefers it, all because the care at the hospital is better than at home. | ||
| Interviewee B3: More often, the patient is asked to remain hospitalized at the request of the patient's family but also of the social organization or physician. The physician, to feel safe, prefers to release the patient to be discharged and go home with a prepared family to receive the patient. So, sometimes this can be a bottleneck, mainly because hospitalized patients need to leave with greater care, and the family has to structure itself better at home, with caregivers or someone helping at home. You know, it's not easy to care for a patient who has just been released at home. | ||
| Communication | Interviewee A2: I think this problem is also a cultural situation, you know. This is the way the hospital works. The resident physician comes here today, and he/she will discuss the decision the next day. It would be better if the resident could call the professor and discuss it over the phone or make a video call. But of course, this involves the work contract and the person's availability. Anyway, I think it could be done in other ways to speed up decision-making. Even more now, we are making video calls frequently. It has become part of our work routine. So we have many ways to make that decision on the same day. I don't know. Can you see the difference it makes? For example, if the resident examined the patient, and it will be discussed the next day at noon (12:00 am), if an examination is needed, the truth is, in fact, the resident could have already requested this examination in her/his first contact with the patient. So the next day, the exam would be ready with a diagnosis. | |
| Interviewee B2: As much as we have improved, patient transfer is still a problem. Sometimes the transfer situation of the patient admitted to the ED is already available. We have the bed ready and clean in the inpatient ward, but there is still takes time to transfer the patient and handover. Communication between the parties is still not quite as we would like. We want patients to be pulled and not pushed. Not that we had to push them, as a bed is ready to receive a new patient, but if the sector itself (hospital ward) already called and pulled and made us a movement so that it would be easier for the patient to leave the ED. However, often, we see that this does not happen. We have to push, which generates a period of idleness with an empty bed. | ||
| Resource management (internal environment) | Discharge planning by the team | Interviewee A2: The resident physician needs validation from a professor. The resident cannot make any clinical decision alone, so, for example, at the end of the afternoon, as the professor is not present in the hospital, the resident has no one to discuss and validate her/his decision with, so he/she will not make any decisions. Unless it's an emergency, if it's not an emergency and that's something that can wait until the next day, then your decision-making will be postponed until the morning of the next day. |
| Interviewee B1: The delay in discharge occurs mainly due to the lack of a discharge forecast, in which the family does not agree with the physician, so there is often a surprise when the patient is discharged. The family is not prepared to receive the patient. So this is a problem we work with daily due to the lack of predictability of hospital discharge. So, there is still an inefficiency related to the planning and predictability of discharge. This is an inefficiency that we see in the hospital very clearly. If I worked with predictability, I would have a much better bed turnover. | ||
| Interviewee B2: We have to think on a more systemic level and on a day-to-day basis to see where they are and what types of bottlenecks exist. At the same time, knowing what patients were not discharged but could have already been discharged from the hospital and trying to interfere with that. Although we cannot interfere in the physician's decision to discharge (...) When the ED is full, we start to put pressure on discharges to occur. Sometimes, we find patients who are not discharged early, and their discharges are necessary to free up beds, and the ED manages to vent and make the wheel turn as well. | ||
| Prolonged LOS (pLOS) | Interviewee A2: We have been doing a lot of work, especially within the ED and in the hospital, so that the time that the patient remains hospitalized is reduced as much as possible (...) Eventually, yes, the patient stays longer than he should have because he/she needs to take an exam or surgery was canceled. Many patients come from the interior of Porto Alegre to be treated at the ED, so it depends on the municipal ambulance to come and pick them up. So, these are times I think there is still room for improvement. Afterwards, there has also been this effort, in recent years, to reduce this situation of the patient staying longer than necessary. | |
| Interviewee B1: I believe that it happens that the patient stays in the hospital bed longer than necessary (...) Today we can see, even from the demand for care, patients stay in bed much longer than before the pandemic. | ||
| Interviewee B2: There are long-stay patients beyond the necessary time who end up occupying the bed for more days. And one more day that the patient is hospitalized unnecessarily is more one day that another patient is waiting in the ED. So, the permanence rate, this extended stay of hospitalized patients, has everything to do with overcrowding in the ED (...). It does happen that the patient unnecessarily occupies a space in the ED, as they no longer need to be in the ED (...). | ||
| Interviewee B3: The stay in the ED to later go to an inpatient unit occurs in a way that the patient stays longer than he should. | ||
| Interviewee A2: Concerning goals, I am sure the entire team is not clear about our BM goals. Although I work on this aspect by promoting goals among them, most of the team doesn't understand why this is necessary. | ||
| Interviewee B1: Our goal is that after medical discharge, the patient has one hour to vacate the bed. After this period, the nurse has to take action. The nurse's goal is for the bed to be vacated quickly, within one hour. The goal is known, as we hold monthly meetings with the teams responsible for beds and show the efficiency of each team. When we started with the command center, we had time to vacate (release) beds for more than three hours. Afterward, we had less than an hour to release the bed, but due to COVID-19, we are working with an average of one hour and twenty minutes (1h:20min). | ||
| Interviewee B2: There are indicators and targets for everything, from the moment the patients arrive at the door of the ED to the time they are seen, from registration to the nurse's care, when the physician sees them, then the time that it will take the physician to decide between discharge and hospitalization, the period of examinations and evaluations that we also seek to reduce, both the LOS of the patient in the ED and the effectiveness of our actions in the ED so that the patient has a feeling that they have been well taken care of and also to stay for less time and thus accommodate the other patients who arrive (...). So yes, those on the front line (at the end) do not conduct their actions directly based on goals, but everyone knows that there is an indirect demand for productivity, speed, and agility so that this wheel turns faster. | ||
| Interviewee B3: These days, teams are more focused on goals. Before, not so much, but when we started to share information between the units, through the command center, from then on, we started to have clearer and more established goals; the LOS of the patient in the ED waiting for a bed, the waiting time of the patient who entered the ED waiting for a bed in the destination unit, the time of transfer of the patient after getting a bed. We are currently working with a hospital bed forecast. It is interesting and a possibility that did not exist before. | ||
| Interviewee B4: I think that the whole team is well-prepared. We work as a multidisciplinary team, and everyone is very engaged. Of course, with all the changes caused by the pandemic, a lot of new people have entered. This creates a greater inconvenience since I don't think all the latest are well-engaged concerning goals. | ||
| Interviewee B5: The care team is part of the BM, making them aware of our bed planning and goals. | ||
| Decisions shared between units | Interviewee A2: There is a head of the entire ED and three medical managers, so we don't have a specific area, but we divide the tasks. | |
| Interviewee B1: Decision-making for BM is shared in the hospital. As I mentioned, we have the managers who participate in this meeting and make the decision together so that everyone sees the “problem” or the solution together. | ||
| Interviewee B2: We participate in the management of beds in the command center because patients leave the ED in two ways: discharge or hospitalization (...) The command center, which meets every morning, analyzes the main points of hospital bottlenecks. | ||
| Interviewee B3: Every day in the morning, at the central bed command meeting, there are representatives of all hospital units who meet to plan the workday and to check which are the sectors with the highest priority, departments with the highest pressure for beds that day, the departments that will demand more beds. (...) In the ED, we share information among the multidisciplinary team (...). We use admission criteria, discharge criteria, and transfer criteria. This is all discussed with the medical team, and then we share it with everyone. And the nurse's responsibility is to share the decisions taken in the ED with the bed center team (...). We monitor the resources and communicate and share with the bed center to show how the situation in the sector is, informing how the flow of patients is and if there is a need to relieve the burden on the sector. | ||
| Interviewee B5: We also manage critical patients in the hospital. The care team is part of this BM, making them aware of our bed planning. So this management of beds is shared by many people. It is not just one person responsible. It is a whole team responsible for managing the beds, from senior management to the people who are here at the end, so we have this exchange for allowing us to have successful results. | ||
| Bed occupancy planning | Interviewee A2: The occupancy rate is very high, so a free bed is a rarity. As soon as the bed is vacated, another patient already occupies it. Here, it depends on hospitalized patients being discharged to, from there, assist new patients. Availability is something that varies a lot because sometimes there are days when the wards have more discharges, and there are days when there are no discharges, so it is something that we were unable to have an accurate forecast of the number of beds available. | |
| Interviewee B1: We work with clinical staff and have a predictive discharge before ten o'clock in the morning, so we encourage discharges of the day to occur until ten o'clock. This is, in fact, very difficult to manage, so at times of high occupancy, we call the physicians, it is an action we do, but the physicians have their lives outside the hospital where they work in offices until noon and come to discharge them later from noon. Then the physicians tell me, yes, I have discharges to give, but I will go to the hospital only afternoon. This is also an obstacle in the hospital because we do not have a discharge team, a medical team that performs discharges. It is the attending physician who performs discharges at the hospital. This physician is not a contractor. He is not available exactly when we need him because he has a job outside the hospital, which is a difficulty we have at the hospital. | ||
| structural characteristics of the provision of care services (internal environment) | Nurses | Interviewee A2: The nurse is a streamliner of flows. He controls the exams and conditions, as he has an overview of the patient's progress during the follow-up. For me, the nurse has a fundamental role in speeding up the process. The nurse coordinates the exchange of patients in the wards and ED. |
| Interviewee B1: In the bed command center, a nurse manages the entire flow of inputs and outputs. If I have a bed reserved for a patient in the ED, they ensure that the transfer happens as quickly as possible. If I have a discharged patient, the nurse's responsibility is for this patient to leave as soon as possible. The nurse's goal is for the bed to be vacated quickly, within one hour. | ||
| Interviewee B3: The nurse's role is not to allow the system as a whole to collapse. Because it is the nurse who manages the flow of patients within the ED. So the nurses must let me know, and I can see through the system. The nurse is an important link with BM because every time a patient is hospitalized, the nurse puts them in the BM queue. In the ED, we have units by specialties, so we deliver the patient to the necessary specialty for BM to be able to organize itself; if it takes too long to carry out this process, the demands will accumulate throughout the day, so the nurse already has to make the link with the bed center and notify them as soon as the patient is admitted. The bed center should then receive the patient's pathology, but it needs to be notified beforehand. So the nurse can make this whole flow rotate more easily. The nurse is a facilitator because when he/she sees that the system is about to collapse, he/she has to communicate with the coordination, so I (coordination) shoot for the rest of the hospital, and from that, we carry out measures that the hospital must take to not leave the ED overcrowded, as this is not good for the hospital nor for the patients who are admitted to the ED. | ||
| Interviewee B5: We were able to carry out an entire assessment of the total number of patients that we have today together with the medical team to see our discharges and move forward together with the distribution of beds, which can already be ready for admissions that we know that they come from the operating room according to the schedule, or we are constantly sharing information with physicians and nurses to be able to admit the patients scheduled for intensive care. | ||
| Hospital demand (external environment) | COVID-19 | Interviewee A2: The pandemic changed everything. I think it brought some good things, greater integration between the departments with the ED (...). For example, last month's ED (April/2021) had its worst moment, in which psychiatrists and other specialties were all on duty in the ED. This is not common. These physicians have their teams on other floors, but they have become aware of the situation. And they realized that if they took their time to discharge patients, more patients would stay in the ED in a situation where they saw how it works. This exchange of experiences was valid, as I believe it should impact the agility of the beds on the floors in the coming months. |
| Interviewee B2: We had two inflows to protect non-COVID-19 patients. Everything was already complicated with a single input and processing stream. We had to divide human resources, materials, and physical spaces during the pandemic. We operate with two input streams; one for patients with COVID-19 and the other for patients without COVID-19. All this because the professionals who care for both patients cannot mix to ensure the safety of the uninfected patient. Right now, for example, we continue to have a duplicate structure, but the demand for COVID-19 beds has decreased, but we don't know how long it should stay like this. We don't know, so we have to maintain the structure. The demand for COVID-19 has dropped, but we have to be prepared for an increase, so it is a challenge to continue maintaining this structure in duplicate and with all the variables that they have for both things, that is, they have duplicated the variables. So this is the biggest challenge of this isolation issue. It is to avoid the contagion of non-COVID-19 patients. | ||
| Interviewee B3: The pandemic came to change everything. Everything that worked until then currently has a different meaning. So BM had to update to the new reality of the pandemic (COVID-19), along with infection control, taking initiatives in BM in the flows of these patients. This is important, as there is a workflow for the suspected patient of COVID-19, another stream for patients who are confirmed with COVID-19, and a third stream of the patient who is no longer contagious and is not in the period of transmission of COVID-19 to other patients. | ||
| Interviewee B4: The pandemic influenced everything. For example, now I'm working here on WhatsApp it's 24/7. A lot of demand, number of extra beds, more teams, they are a huge problem because that's what I told you, there are a lot of people new, in all areas the hospital works with processes, with organization, with planning, and it has a way of working that needs to be maintained and must be maintained for the benefit and quality of care and care safety. So I'll tell you this, it's practically insane what happened and what's still happening. Of course, we have a whole structure with equipment and a technological park, but what makes the hospital work out are the people. So this had a huge impact not only on the nursing part but on the medical part as well. Previously, it was a door where 100 patients passed, and now it is passing about 500, and it has to pass because if it does not pass, it means death. Our objective here is mainly two: care safety, also for us, for the entire multidisciplinary team, and also that the patient is attended to and that they are not left without assistance when they come to the hospital. | ||
| Interviewee B5: New hires had an impact, and this view on the BM all the time for what has been happening is important. We are going through this pandemic period with some higher peaks, others more moderate, and others a little lighter. We are always reorganizing ourselves as necessary. | ||
Source: Adapted from La Forgia & Couttolenc (2009).
Table 5.
Factors for bed management in EDs.
| Factors | Problems | Solutions | Authors | Interviewees |
|---|---|---|---|---|
| Family or patient | Resistance to accepting discharge and leaving the hospital. | - Promote care guidelines for patient and family members, thus enabling better self-care conditions for the patient. | D’Aquino (2017), Fontana, Chesani, & Menezes (2017), Fontana, Chesani, & Nalin (2017), Werner (2017), Machado & Machado (2019) and He et al. (2019). | B1, B2 and B3. |
| Communication | Communication failures with other hospital units. | - In hospital systems, share the arrival and departure of patients in the units in real-time. This measure requires the sharing of information regarding the transfer of patients, occupancy rate, expected discharge, and average LOS. - Develop means of streamlining communication between supervising and assistant physicians to expedite discharges. |
D’Aquino (2017), Fontana et al. (2017), Werner (2017), Raffa (2017b), Machado & Machado (2019), He et al. (2019), Borges et al. (2020), Souza et al. (2020) and Alonso et al. (2022). | A1, A2 and B1. |
| Lenght of stay | pLOS. The patient occupies the bed longer than necessary. | - A team with hospital discharge autonomy for any time of the day on any day. - A team responsible for managing hospital beds as a whole, with exclusive dedication. - Technological support in order to efficiently map all processes related to BM. |
Jones (2009), Suzuki et al. (2011), Silva et al. (2014), D’Aquino (2017), Raffa et al. (2017a), Machado & Machado (2019), He et al. (2019), Wasgen et al. (2019), Oliveira & Bittencourt (2020) and Souza et al. (2020). | A1, A2, B1, B2 and B3. |
| Hospital discharge planning by the team | Delay in the hospital discharge process; overcrowding in the ED. | - Improve intra-hospital transfer prediction in the ED with real-time monitoring of bed availability in other units. - A dedicated cleaning team responsible for cleaning the released beds to speed up the availability of beds. |
Suzuki et al. (2011), D’Aquino (2017), Werner (2017), Raffa (2017b), Raffa et al. (2017b), Machado & Machado (2019), He et al. (2019) and Wasgen et al. (2019). | A1, A2, B1 and B2. |
| Performance goals | Goals are not known by the entire team or achieved. | - Promote awareness and engagement of the goals for the teams involved, as well as for those responsible for managing beds in general. - Accompany the goals on a daily basis and carry out an action plan in order to achieve them. |
Raffa (2017), Raffa et al. (2017a) and Raffa et al. (2017b). | A1, A2, B1, B2, B3, B4 and B5. |
| Decisions shared between units | Misaligned expectations; lack of team mentality; departmentalization; competition for resources; | - Decentralize the decision-making process. - Multidisciplinary meetings (huddles). |
Raffa et al. (2017a), Landa et al. (2018) and He et al. (2019). | A1, A2, B1, B2, B3 and B5. |
| Bed management policies | Management policies are not adequate for organizational needs. | - Collaboratively develop management policy changes to increase the efficiency of emergency BM. - Listen carefully to all stakeholders. |
Raffa (2017), Raffa et al. (2017b), He et al. (2019) and Borges et al. (2020). | A2 and B3. |
| Hospital bed occupancy planning | Difficulties in cooperation and information integration; difficulties in managing hospital discharges in periods of high occupancy rates; uncertainty about arrival rate; pressure to prioritize patients in overcrowded settings (Sophie's choices). | - Determine criteria for vacating prioritization and updating as soon as possible discharge planning; - Incorporating forecast models based on historical patient arrival data to aid and support planning. |
D’Aquino (2017), Raffa et al. (2017a), Raffa et al. (2017b), Raffa et al. (2017c), Machado & Machado (2019), He et al. (2019), Wasgen et al. (2019), Oliveira & Bittencourt (2020) and Souza et al. (2020). | A1 and B1. |
| Enfermeiros | Lack of autonomy related to ED hospital beds. | - Allow greater autonomy for nurses in the BM process in the ED. | Raffa (2017), Raffa et al. (2017a), Raffa et al. (2017b), Borges et al. (2020), Oliveira & Bittencourt (2020), Souza et al. (2020) and Alonso et al. (2022). | A1, A2, B1, B4 and B5. |
| COVID-19 | Unforeseen change in the BM process in the ED due to patient needs. Increased demand and need for dedicated teams for care. | - Promote diligent changes in the BM policy, adapting it to the demands of the pandemic. | Noronha et al. (2020) and Alonso et al. (2022). | A1, A2, B1, B2, B3, B4 and B5. |
Source: Authors
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



