Submitted:
15 February 2023
Posted:
16 February 2023
Read the latest preprint version here
Abstract
Immune checkpoint inhibition therapy (ICIT) is an emerging field in oncology especially opening new horizons to chemotherapy refractory patients. This paper provides deep insight into immune related adverse events (irAEs) posing a major challenge and drawback to ICIT, and presents right management strategies for very complex complications. Moreover, a non-linear mathematical approach to measure the ICIT success rate and a strategy to overcome or to delay the progression after initial good response to ICIT in a subset of patients are presented, respectively.
Keywords:
Oncology
; Immune Checkpoint Inhibition
; PD-1
; PD-L1
; CTLA-4
; Immune Related Adverse Events
; Immunotherapy
; Tumor Plasticity
; Tumor Microenvironment
Introduction
Immunology and oncology as two distinct fields are strongly linked since a very coincidental case, when in 1904 a cervical cancer patient had to receive rabies vaccine (high risk neural tissue vaccine at that time) due to a dog bite, which subsequently led to complete tumor regression [1]. Immune checkpoint inhibition therapy (ICIT) is a novel emerging field in immunotherapy providing great assistance to a subset of patients in achieving long term remission when applied either as a monotherapy or in combination with other ICIT types or treatment options such as chemotherapy. The classical tenet of cancer immunoediting focusses on the immune system and defines the so called elimination, equilibrium and escape stages suggesting that the cancer pathogenesis involves the dysfunction of the immune system, which leads to the escape of tumor cells from immune detection [2]. ICIT releases the brakes on the immune system and thus restores T cell responses on tumor cells. However, it is exactly this boost in T cell reactivity that can cause immune related adverse events (irAEs) in any tissue, which will be discussed in further sections providing a deep insight into this complex problem. Furthermore, the challenge of progression after initial good response in a subset of patients will be addressed with a strategy inspired by the mechanisms of brain plasticity.
Applicatıon and Mechanisms of ICIT
The revolutionary emerging ICIT has many applications in oncology including but not limited to classical Hodgkin lymphoma (cHL), gastric cancer, head and neck squamous cell carcinoma (HNSCC), hepatocellular carcinoma (HCC), melanoma, microsatellite instability in colorectal cancer (MSI CRC), non-small cell lung cancer (NSCLC), ovarian cancer, renal cell carcinoma (RCC), small cell lung cancer, triple-negative breast cancer (TNB) and urothelial cancer, each with different response rates ranging between 15 – 65%, with MSI CRC and cHL having the highest, small cell lung cancer and ovarian cancer presenting the lowest response rates [3,4,5]. It is also worth noting that several ICIT drugs have been approved by the US Food and Drug Administration (FDA) as first line treatment such as ipilimumab, nivolumab and pembrolizumab for metastatic melanoma, pembrolizumab (either as single agent or in combination with pemetrexed/carboplatin) for metastatic non-small cell lung cancer (mNSCLC), and avelumab for metastatic merkel cell carcinoma. Currently, there are seven ICIT drugs approved by FDA and one pending approval: Two cytotoxic T lymphocyte associated protein 4 (CTLA-4) inhibitors (ipilimumab and tremelimumab (pending)), three programmed cell death protein 1 (PD-1) inhibitors (nivolumab, pembrolizumab and cemiplimab), and three programmed cell death ligand 1 (PD-L1) inhibitors (atezolimumab, durvalumab and avelumab).
ICIT is based on inhibition of negative co-stimulatory signalling on T cells through CTLA-4, PD-1 or PD-L1. At the lymph node the interaction between the dendritic cell and T cell involves the release of antigen information to T cell through the communication of major histocompatibility complex (MHC) molecules with the T cell receptor (TCR) [6]. At the same time, B7, which is a type of integral membrane protein, is paired with CD28, which is a T cell co-stimulatory receptor, to produce a co-inhibitory signal to enhance or decrease the activity of a MHC-TCR signal between the dendritic cell and the T cell. Apart from these two signals, as an additional third signal cytokines can also contribute to T cell activation. The B7-CD28 signal pair additionally triggers the T cell to produce CTLA-4, which also binds to B7 downregulating the B7-CD28 signalling and suppressing the T cell activation [7,8]. Hence, CTLA-4 inhibition is believed to restore tumor directed T cell responses [9].
On the other hand, PD-1 plays a vital role in inhibiting immune responses and its involvement within the tumor microenvironment (TME) reduces cytokine secretion such as interferon gamma (IFN-γ), interleukin-2 (IL-2) and tumor necrosis factor alpha (TNF-α) via interaction with CD28 co-stimulatory signalling pathway [10]. PD-L1 can combine with PD-1 to reduce the proliferation of PD-1 positive cells, inhibit their cytokine secretion and induce apoptosis, and moreover can also attenuate the host immune response to tumor cells, thus restricting tumor cell killing [10,11]. Therefore, PD-1/PD-L1 inhibition promotes an effective immune response against cancer cells.
Furthermore, I want to emphasize that currently several next generation drugs are under investigation, which target lymphocyte activation gene-3 (LAG-3), T cell immunoglobulin and mucin-domain containing-3 (TIM-3), T cell immunoglobulin and immunoreceptor tyrosine-based inhibitory motif (ITIM) domain (TIGIT), V-domain Ig suppressor of T cell activation (VISTA), or B7-H3 protein receptor inhibition [12].
The Bottlenecks of ICIT, the Complexity and Effective Management
Although ICIT is a novel emerging promising and successful type of therapy, as mentioned earlier, it also has its drawbacks and bottlenecks, the major one being the so called irAEs that pose a great complex challenge on the entire course of therapy. Before moving deeper into this subject, I want to remind the community about the golden rules of medicine, i.e. that it is not mathematics, everything should be considered in a case- and person-specific manner, and that even in the same person all parameters continuously alter in dynamic adaptive manner in the real time. Hence, the following should be interpreted nothing else than as indicative factors, however based on quite strong knowledge.
As ICIT stimulates the immune system, it may anytime come to an overstimulation and any kind of autoimmune reaction can manifest itself, whereas theoretically any organ/tissue system can be affected by this boost in T cell reactivity. Interestingly, different checkpoint inhibitors have a different frequency of manifestation related to irAEs. Generally, CTLA-4 inhibition is related to higher irAE incidents than PD-1/PD-L1 inhibition. Furthermore, application of ICIT in combination with other options and/or in higher doses is rather associated with more frequent and more severe irAEs [13,14].
One has to be very careful by presenting the onset frequency of irAEs, as the numbers vary widely in the literature each based on different study models with their own limitations [15,16,17,18,19,20,21,22,23,24,25,26,27]. Apart from this, as also stated above, combination therapy yields different frequency, timing and risk duration results compared to ICIT applied as monotherapy.
I provide in Table 1 a general view about selected irAEs with respect to each organ/tissue system and their mostly observed onset frequency details. I strongly repeat that the information in Table 1 shall only be interpreted as some level of indication without any mathematical precision, and further corresponds to monotherapy cases only. Moreover, irAEs associated with ICIT are not limited to the ones presented in Table 1, as it does not necessarily provide a complete list, but rather mentions some selected pathologies.
We can clearly observe from Table 1 that the gastrointestinal and dermatologic irAEs are the most frequently experienced types followed by the endocrine system related complications.
It shall be noted that by presenting the approximate onset frequency for irAEs in Table 1, I did not consider the specific agent (with the exception of three irAEs where different checkpoint inhibitors yield quite different results), administered dose, underlying malignancy, disease stage, any existing comorbidity, gender difference, whether ICIT rechallenge was involved, whether a biopsy was made, and most importantly what the so called common terminology criteria for adverse events (CTCAE) grading of the irAEs was. I only provided a general indicative view.
The same is going to be valid for the next two tables, in which I will present approximate timing of some selected irAEs and related CTCAE grading peak in monotherapy and combination therapy applications, and approximate onset frequency of irAEs with respect to organ/tissue systems in a CTLA-4/PD-1 combination therapy scenario, respectively [14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30].
Please note that the weeks in Table 2 refer to weeks after the initial infusion. CTCAE peak time states the timing with the highest CTCAE grading risk of the corresponding irAEs. Damping time denotes the timing when the onset risk of the corresponding irAEs is nullified or the CTCAE grading equals to zero, and an infinite value demonstrates that the onset risk with the highest CTCAE grading remains uniform throughout the entire duration of the ICIT and a considerable undefined time afterwards.
In Table 3, again the weeks refer to weeks after the initial infusion and the damping time is as explained for Table 2 above. The frequency peak denotes the peak incidence percentage at the corresponding week. As mentioned previously, the provided numbers are just indicative figures without any mathematical precision. Moreover, I occasionally notice ideal Gaussian distribution curves in graphical representations in some literature that try to demonstrate similar information. This is totally unrealistic and absurd, as medical dynamics can never correspond to ideal mathematical representations, and furthermore as already stated above, such parameters never reflect the complete real world complexity.
Pathogenesis of irAEs, Management Burden and Strategies
As explained, the major drawbacks of ICIT are the irAEs, which unfortunately may lead to fulminant and fatal outcomes in a subset of patients, while many others need to suspend the therapy temporarily or discontinue permanently. The most fatal irAEs with highest toxicity grades are colitis, pneumonitis, myocarditis, hepatitis and encephalitis [21,31]. Moreover, in general terms, we usually observe more fatal outcomes in combination scenarios, precisely spoken CTLA-4 inhibition with PD-1 or PD-L1 inhibition, than monotherapy applications, whereas the fatality rates in descending order would yield ICIT with CTLA-4, PD-L1 and PD-1 inhibition, respectively.
Now, all current management strategies with respect to general consensus are based on immunosuppressive methodology using corticosteroids, which however is nothing else than symptomatic therapy far from considering the etiology of the irAEs. We need to understand well the precise pathogenesis, i.e. the molecular and cellular events that lead to the onset of the irAEs, in order to develop effective management strategies preventing most of the fatal outcomes and enabling most patients to continue with this promising antineoplastic regimen and benefit from it. It shall be noted that each checkpoint inhibitor has a different pathogenesis route involving the irAEs.
If we now try to give deep insight into various complex etiological considerations of irAEs, we may observe the following: In a CTLA-4 inhibition scenario, lack of CD4+CD25+ T regulatory (Treg) cells downregulated due to an antibody to CTLA-4 may initiate dysregulation of gastrointestinal mucosal immunity that may lead to colitis [32,33]. ICIT may assist the migration of T cell effectors into the kidneys by providing a permissive environment and thus initiate an inflammatory response that may lead to acute tubulointerstitial nephritis (ATIN) [34]. Furthermore, ICIT may induce reactivation of drug-specific T cells primed by nephrotoxic drugs [14,35]. Hypophysitis induced by CTLA-4 inhibition may be caused by direct binding of the monoclonal antibody to the CTLA-4 antigens present in the pituitary gland [36]. A patient’s histological autopsy details, who died from myocarditis induced by PD-1 inhibition, demonstrated a predominantly CD8+ T cell infiltrate, together with some CD4+ T cells and sparsely distributed B cells [37], i.e. denoting a loss of self tolerance. PD-1 or PD-L1 inhibition triggers a significant production of C5a, which is a potent anaphylatoxin, which may lead to glomerular inflammation [38]. CTLA-4 inhibition increases lymphocyte counts with an increased expression of T helper cell 1 (Th1) associated markers, which potentially may lead to a sarcoidosis-like reaction [39], or alternatively an increase in the number and function of Th17 cells could play a role in the development of sarcoid granulomas [40]. Furthermore, PD-1 inhibition may amplify the effects of Th17.1 cells to cause sarcoidosis [41]. A fatal encephalitis case induced by PD-1 inhibition suggests that cytotoxic CD4+ and CD8+ T cells are the culprits in the pathogenesis by infiltrating into central nervous system (CNS) [21]. For irAEs leading to hyper- or hypothyroidism induced by PD-1/PD-L1 inhibition a possible mechanism could be the disruption of the interaction between the PD-1 on the T cells and PD-L1/2 on the thyrocytes leading to T cell activation against the thyroid [42]. ICIT induced thrombocytopenia may involve the activation of CD4+ helper T cells and CD8+ cytotoxic T cells resulting in the damage to hematopoietic stem cells, and moreover reduced thrombocyte count may be influenced by a circulating immune response [43]. With respect to ICIT induced hepatitis, a possible pathogenesis mechanism could be that the secretion of TNF-α during the arrival of massive numbers of activated CD8+ T cells in the liver can cause hepatotoxicity and lead to bystander hepatitis, which is linked to Kupffer cells, whose activation is associated with hepatic damage and whose phagocytosis of apoptotic bodies leads to hepatocyte injury [44].
Interestingly, some research data suggest that irAEs may be correlated with improved survival rates in ICIT. Such a strong correlation can especially be observed by certain types of dermatologic irAEs [45,46]. Higher grade colitis also led to improved survival in a study [47]. Moreover, the incidence of hypophysitis may positively predict survival in melanoma patients treated with ipilimumab [48].
By providing rigorous novel management algorithms for some selected irAEs, in order to dramatically reduce the general exposure of the patient to corticosteroids and in order to be more effective in general terms, I will occasionally go beyond the general consensus considerations recommended by Society for Immunotherapy of Cancer, American Society of Clinical Oncology, National Comprehensive Cancer Network and European Society for Medical Oncology, and introduce some concepts that can be regarded as out of box compared to conventional approaches [49,50,51,52,53,54].
Let us start with Figure 1 by representing the general management approach in block diagrams, where corresponding blocks will be demonstrated in details in subsequent figures.
The information stage can be represented very straightforward in Figure 2 below.
Firstly, the oncologist should give deep insight into various aspects of ICIT including irAEs, and must acquire knowledge about the toxicity spectrum of checkpoint inhibitors. He/she must identify possible irAE signs and symptoms for specific organ systems and must be able to differentiate these from complications of chemotherapy in case of a combination scenario with a cytotoxic approach, but also from exacerbation of any preexisting autoimmune disease, which shall be discussed with the patient during the briefing stage along with any other preexisting comorbidity. The oncologist must form a team with the patient including an organ specialist for various scenarios and an immunologist. Moreover, a fast and efficient communication is extremely crucial, and the patient must be animated to watch out for possible symptoms and contact the team members quickly for an evaluation.
The baseline tests [4,29], are detailed in Figure 3 with a special focus on blood analyses. Low dose chest computerized tomography (LDCCT) and electrocardiogram (ECG) are performed to obtain a baseline reference. Urinalysis is very straightforward and is especially done to look for proteinuria. Attention must be given to include free thyroxine (fT4) in the thyroid gland test, as only testing for the thyroid stimulating hormone (TSH) could yield misleading results. TSH and fT4 together would give a clearer picture as shown in Table 4 below.
I would also add blood cancer biomarkers to the baseline analyses in order to follow the evolution of those values with respect to the initial reference during the ICIT. Although this can be set regarding the underlying malignancy, I would highly recommend to test for the carcinoembryonic antigen (CEA) and cancer antigen 19-9 (CA 19-9) at least.
Although tests for baseline biomarkers as shown in Figure 4 (not to confuse with the test for blood biomarkers represented in Figure 3) are never mentioned in the general consensus among baseline checks, I recommend these, as they are predictive for the response to ICIT and therefore may be helpful in the appropriate selection of ICIT.
Figure 5 below shows the management algorithm for colitis/diarrhea as a frequent gastrointestinal irAE in ICIT.
It shall be noted that the management approach in Figure 5 is quite different than general consensus strategies. The rationale of my vitamin recommendation here is based on the possible pathogenesis of ICIT induced colitis that may result due to downregulation of Treg cells. Hence, higher levels of vitamin D3 leads to increase the number and/or function of Treg cells, whereas vitamin B3 promotes colonic Treg generation and maintains colon homeostasis, and vitamin B9 metabolism maintains gut Treg survival and restricts intestinal inflammation. This way, I hope to achieve a faster and more efficient resolution to grade 0-1 reducing the risk of intensive exposure to corticosteroids.
Moreover, it shall also be noted that the grades specified in the management algorithm in Figure 5 and in all other subsequent management approaches in the following figures, are simply referring to CTCAE grading schemes.
Furthermore, I also introduced the recommendation of the transplantation of faecal microbiota from healthy unrelated donors, if the continuous deterioration led to an imminent hemodynamic collapse. It is worth to keep in mind that such decisions must be taken rapidly to prevent fatal outcomes, when the conditions demand the application. And, the rationale for unrelated donors is simply to avoid potential shared genetic and environmental determinants of the gastrointestinal microbiota.
Needless to mention that it is also very important to rule out other etiologies that may also be responsible for diarrhea. This ruling out other etiologies consideration is of course also valid for other irAEs.
For grade 3 or 4 cases, it would make no sense to rechallenge the ICIT after a possible resolution or improvement to grade 0-1 due to high recurrence risk. Hence, unlike general consensus, my recommendation is a permanent discontinuation in such cases.
The management strategy for dermatitis, which is the most common dermatologic irAE, is represented in Figure 6.
Dermatologic irAEs mostly manifest as reticular and erythematous skin rash and are mostly located across the extremities and the trunk. Grade 1 and 2 cases mostly do not pose an insurmountable problem and can be easily managed to full resolution with topical corticosteroids. Dermatologic irAEs mostly do not severely affect the course of ICIT.
Figure 7a demonstrates the management algorithms for two common endocrine toxicities, i.e. hypothyroidism and hyperthyroidism. Table 4 already states the importance of combinative TSH and fT4 testing for accurate diagnosis. And in Figure 7b, hypophysitis and Addison’s disease as other endocrine irAEs are handled.
It shall be noted that hypophysitis presents with low TSH and low fT4, and laboratory testing of morning cortisol, adrenocorticotropic hormone (ACTH), luteinizing hormone (LH), follicle stimulating hormone (FSH) and growth hormone (GH) define the diagnosis. Moreover, Addison’s disease may mimic sepsis, which shall be ruled out.
Management of hepatitis as an irAE is presented in Figure 8.
My rationale to introduce here infliximab right as a first step for grade 2 case is again based on the possible pathogenesis of ICIT induced hepatitis such that I try here to inhibit massive secretion of TNF-α, and thus to reduce hepatotoxicity, to avoid intensive exposure to corticosteroids, and to achieve a faster improvement or resolution. Although the use of anti TNF-α inhibitors is generally not recommended due to sparse reports of adverse events, evidence is limited [56].
Figure 9 below deals with neurotoxicity in general terms.
ICIT induced neurologic toxicities are rare but potentially fatal including severe encephalitis cases [21]. I would also recommend considering galantamine in severe cases to significantly decrease CD4+ T cell activity. Pneumonitis management is shown in Figure 10.
Although pneumonitis is rare among irAEs, it can be life threatening. Imaging typically shows ground glass opacities or patchy nodular infiltrates, particularly in lower lobes.
In Figure 11 below management approach of renal toxicities is demonstrated.
It is worth noting that ICIT induced renal failure typically presents without any clinical features at the beginning. However later rising creatinine values can be detected, and with progression, symptoms such as oliguria, edema, anuria and electrolyte abnormalities can occur.
And Figure 12 represents management algorithm for thrombocytopenia, whose presenting signs and symptoms include bleeding such as petechiae, purpura, epistaxis, hemorrhage, and fatigue.
It shall be noted that bone marrow biopsy is not recommended in the absence of other accompanying cytopenias. However, if it was performed, a bone marrow biopsy would reveal increased megakaryocytes, referring to platelet destruction rather than decreased platelet production [57].
I want to emphasize that preexisting autoimmune disorders are not a contraindication to ICIT, which can safely be applied to such patients. Only a subset of patients would experience exacerbation of the preexisting disorder, and only a subset would develop de novo irAEs [58,59,60].
Furthermore, I would not recommend to administer corticosteroids as a premedication in the infusions prior to ICIT in order to prevent or address any possible irAE. Corticosteroids, as far as they are unavoidable to be used in the management of the irAEs, do not limit or alter the efficacy of the ICIT [61]. To manage some corticosteroid side effects, H2 blockers such as nizatidine, cimetidine, etc. and clotrimazole can be used.
Cancer Pain Management throughout ICIT
A subset of patients that start ICIT may well be under considerable progression and suffer from remarkable cancer pain, which is unfortunately up to now still an insufficiently addressed domain. Let us first illustrate the standard pain management approach in Figure 13 below.
Considering that such patients mentioned above may experience a long term stabilization or a slow smooth progression with ICIT, a simultaneous cancer pain management approach will definitely be necessary. Here, the problem will be that some of the drugs including nonsteroidal anti-inflammatory drugs (NSAIDs), corticosteroids, acetaminophen and opioids have an interaction with ICIT agents involving pharmacodynamics and pharmacokinetics [62,63,64]. Table 5 presents class and type of drugs used in cancer pain management.
It shall also be noted that in addition to the drug scheme shown in the above table several adjuvant analgesic medications such as antidepressants, anticonvulsants and bisphosphonates are also used in cancer pain management posing again risk of interaction with ICIT drugs. Another important consideration should be to avoid neurodestructive and irreversible procedures such as cordotomy as much as possible and to apply such approaches as ultima ratio, as, even with metastatic involvement, such subset of patients would survive for extended periods of time and the goal should be on one hand to sustain the quality of life and mobility of the patient as much and as long as possible, and on the other hand not to depress intellectual and cognitive spheres.
Discussion
Although the rate of fulminant and fatal outcomes related to irAEs is considerably low, apart from fatalities, many patients experience either temporary suspension or permanent discontinuation of ICIT posing them into risk of missing possible therapy benefits. However, for the time being let us forget the irAEs and consider the possible response patterns of ICIT as illustrated in Figure 14 below:
It shall be noted that by providing the indicative response curves I did not consider the rates and duration of regression and progression such that the slope and length of curves and timing of events can be different than the ones I presented above in Figure 14.
Exactly as inventing fast, effective and sparing management strategies for irAEs in order to offer the patients the benefits of ICIT as long as possible, it is equally of utmost importance to differentiate between pseudoprogression and real progression in order to avoid unjustified premature discontinuation of ICIT, as the pseudoprogression phenomenon always leads to a noticeable regression with a certain delay. We have to understand the mechanisms that occur, while the immune system primes for an antineoplastic response. Furthermore, after a possible initial progression, if the patient is symptomatically doing well, ICIT shall be continued for at least ≥ 3 more cycles to confirm the response pattern or to observe a delayed stabilization or regression. If there is still a progression, then we can talk of the so called innate resistance.
A subset of patients progress after initial good response. A problem would be that the inhibition of one immune checkpoint may trigger a compensational reaction such that other immune checkpoint receptors in the TME would be upregulated.
Now, let us consider the possible scenarios after having achieved full remission and having remained in this state for a considerable long time and either finishing the planned ICIT regimen, or discontinuing ICIT because of any other reason. This optimum response pattern is highlighted with green color in the above illustration. We obviously have two options: Either we will observe a progression, whose exact timing, speed and severity will be depending on case- and person-specific factors, or we will observe a very long or even near lifelong continued remission. This is possible, because after case- and person-specific sufficient enough long exposure to hostile mechanisms of neoplasms in the molecular and cellular level, the immune system develops, readjusts and reprograms its tactical strength decoding the evasion strategies of tumors and totally defeating them with a superior combativeness. Hence, ICIT plays here a crucial and vital role in supplying the patient with the required boost and this necessary sufficient time for the evolution and readjustment of the immune system.
Furthermore, the ICIT success rate can be assessed and predicted by a non-linear mathematical model considering especially the following parameters (but not only limited to them) and associated person-specific dynamic weighting for them:
- How soon the regression starts after the initial infusion
- What the rate of regression is
- How soon the remission is reached after the initial infusion
- The general personal immune strength
- The compatibility of baseline biomarkers with the ICIT
- Number of days without any irAE after the initial infusion
It shall be a recursive model, in which the mentioned weights would continuously change in dynamic adaptive manner in the real time. However, the development of such a non-linear mathematical model requires exhaustive work and rigorous analysis of large data sets involving correlations between states, parameters and time of events.
We can observe in literature that several assessment schemes have been proposed for the so called hyperprogression [65,66,67,68]. However, they are mostly based on nothing else than personal opinions and not on rigorous past research leading to a general realistic consideration. There is no correct or wrong in such assessments.
In view of this, instead of introducing the above mentioned non-linear rigorous mathematical model for the assessment of the ICIT success rate, to which I would dedicate another full paper on its own, I will suggest and provide here a much simpler and smoother mathematical approach for the ICIT success rate calling it “Hendekli assessment model for ICIT success rate”, and an algorithm in Table 7 for a fast, efficient and simple decision analysis that could be used at any arbitrary stage to assess the therapy impact and further steps to be taken. I want to emphasize here very strongly that the success is not only based on stabilization, regression and remission, but even a relatively slow smooth progression should also be regarded as a certain level of achievement, if otherwise without ICIT there would be a much faster, aggressive and more severe progression.
Hence, let us formulate the ICIT success rate measured in percentage with the following equation:
where and for any arbitrary stage and equiprobable assumption is set for the initial measurement stage , i.e. .
Furthermore, in Equation (1) denote ICIT success rate, timing of regression start, regression rate, timing of remission start, personal immune strength score, baseline biomarker compatibility, time without toxicity or irAEs, and associated person-specific dynamic weightings, respectively. The parameter scoring can be set and calculated as explained in Table 6.
I want to emphasize that the weightings will remain same whose corresponding parameters scored between 59 – 41 in the previous assessment stage and that obviously the constraint must always be kept for any arbitrary assessment stage . Furthermore, the scoring for the parameters are done once at the initial stage and remain constant throughout the whole further assessment stages.

Table 7.
ICIT decision analysis algorithm for any arbitrary therapy stage.
| Step# | Description of Step |
|---|---|
| 1 | ICIT continues |
| 2 | Check whether the patient is psychologically doing well and GO TO step 3 if YES, otherwise WITHHOLD ICIT until improvement |
| 3 | Check whether the patient is symptomatically doing well and GO TO step 4 if YES, otherwise WITHHOLD ICIT until improvement |
| 4 | Check whether the patient has developed any irAE or toxicity and GO TO step 5 if NO, otherwise REFER to management algorithms presented in the previous section |
| 5 | Check whether MRNn+1 > MRNn (n є ℕ) and GO TO step 6 if NO, otherwise DISCONTINUE ICIT permanently |
| 6 | Check whether NTn+1 > NTn+2 (n є ℕ) and GO TO step 7 if NO, otherwise DISCONTINUE ICIT permanently |
| 7 | Check whether VTn+1 > 1.15xVTn (n є ℕ) and GO TO step 8 if NO, otherwise DISCONTINUE ICIT permanently |
| 8 | CONTINUE ICIT |
| 9 | GO TO step 1 and MAKE n=n+1 |
ICIT: Immune checkpoint inhibition therapy. irAE: Immune related adverse event. MRNn: Number of metastatic regions at analysis stage n. NTn: Number of existing tumors at analysis stage n. VTn: Existing tumor volumes at analysis stage n. ℕ: Natural numbers.
It shall be noted that in Table 7 above n=1 obviously denotes the baseline analysis stage with respect to MRN, NT and VT. Furthermore, any existing tumor volume is compared with the volume of the same lesion in the previous analysis stage. Hence, ICIT should be continued, as long as in an arbitrary analysis stage we do not observe an additional further metastatic region, more than two additional tumors and more than 15% increase in existing tumor volumes compared to previous analysis stage, in addition to satisfaction of other constraints as explained in Table 7.
Our biggest challenge is to address the problem of progression after initial good response in a subset of patients, which is also highlighted in red color in Figure 14 above. I would not even call this as an acquired resistance, but as the impact of tumor plasticity. This response pattern can in fact be regarded as the duality of the pseudoprogression, just with different time windows involving the opposite trend. As mentioned above, there is also the problem of compensational reaction upregulating other immune checkpoint receptors in the TME. Hence, shall we perhaps apply multiple simultaneous ICIT to the patient? I would not recommend this, because on one hand this would not only dramatically increase the risk of irAEs both in frequency and severity, but also on the other hand would not stop this compensational process in the TME. Now, let me refer to neurology and give an example to brain plasticity: Among Parkinson patients under levodopa treatment, we occasionally observe that the drug stops showing any beneficial effect after a certain person-specific time following the initial good response. Such patients can mostly be helped by implanting deep brain electrodes applying electrical stimulation. Hence, referring back to our challenge, here the bottleneck is simply that we apply a continuous monotonous stimulation to the TME such that it develops a loss of sensitivity to this stimulation and the cancer cells activate evasion strategies. Indeed, we can especially observe a loss of sensitivity to the IFN-γ signalling pathway. IFN-γ is released by antigen specific T cells upon activation through their TCR and is involved in mediating antitumor responses. I do suggest to create a so called tumor microenvironment cytokine secretion manipulation (TMECSM), i.e. to transform the TME into a chaotic state by application of temporary and periodical electrical and/or magnetic field stimulation to the TME in order to prevent the loss of sensitivity problem and immune evasion mechanisms. I will deeply consider this strategy in a further paper, but just as a short information, we know convincingly well that both electrical and magnetic field stimulation induce a decrease in IFN-γ secretion by mitogenic activated T cells [69,70]. On the other hand, immune checkpoint inhibition leads to continuous exposure of cancer cells to IFN-γ released by antigen specific T cells. Hence, by the strategy I propose, we can temporarily (for the duration of the suggested electrical and/or magnetic field stimulation and a certain time afterwards) and periodically limit cancer cells from dealing too much with the IFN-γ signalling pathway and discovering its defects, while still performing our task of immune checkpoint inhibition. Although this strategy may sound somewhat controversial, I want to emphasize that the key here is to limit the continuous monotonous stimulation and thus to temporarily decrease the exposure of cancer cells to IFN-γ with the target of taking away the opportunity from them to find a weakness in the IFN-γ signalling pathway to develop insensitivity. I repeat: The temporary pause or relief from the continuous monotonous stimulation aims to block the loss of sensitivity, whereas this pause would be repeated periodically during the entire course of the ICIT once progression started. Many questions that should be investigated would be how to exactly localize the suggested stimulation (electrical field would be applied in a non- or minimally invasive manner, while the magnetic one in totally non-invasive way), what to do in case of multiple solid tumors, how to decide about the precise case- and person-specific duration and intensity of the stimulation, which all I hope to address in a further detailed paper.
One could logicall ask why we are then simply not suspending ICIT for a while to give a relief from the stimulation. If this option was applied, then the full absence of ICIT would also affect other components in the otherwise running signalling pathway in the presence of ICIT. Hence, a careful balance is very crucial. In my proposed method above, ICIT is not suspended and administered simultaneously within the plan.
Conclusions
In this paper, I tried to provide a comprehensive and deep understanding of ICIT and related irAEs with corresponding effective management approaches. Moreover, I presented a strategy against the progression after initial good response in ICIT considering the plasticity mechanisms in the TME.
irAEs are the major drawbacks of ICIT, and we have to understand well the exact pathogenesis in each specific case why such irAEs manifest throughout the course of the ICIT. Effective management strategies must be based on this knowledge.
Furthermore, equally as important as introducing rigorous effective management startegies going out of the box and addressing events in the TME including tumor plasticity, it is also very crucial to give deep insight into tumor cachexia, unfortunately a very neglected and underestimated phenomenon in cancer, and to illuminate its exact pathogenesis in order to be able to develop strategies to combat it efficiently. Breaking the refractory cachexia chain reaction starting from anorexia and mostly accompanying diarrhea going up to anemia and final act of hemodynamic collapse is the key to combat neoplastic premature mortality.
Hence, the key tactics are giving sufficient time to the immune system of the patient for a readjustment and reprogramming, which is a phenomenon that I observed among human rabies survivors, and further addressing cachexia and hemodynamic collapse, which certainly should be based on combinative strategies involving continuous monitoring of some parameters through biosensors such as body fat, muscle volume, extracellular water ratio, vitamin D status, electrolyte levels, etc. and application of artificial intelligence with well established machine learning methods for detection and prediction of cachexia deterioration.
In this novel emerging promising field, we need more research, more efforts, more investigation and, even if in the first moment they may sound controversial in the application, we also urgently need more courageous experiments to illuminate the still obscure areas, all for the sake of patients. Courage and heroic attempts going beyond standard algoritms and consensus decisions are the key to introduce groundbreaking beneficial concepts to the patients.
Funding
None
IRB Approval
Not applicable
Clinical Trials
Not applicable
Patient Consent
Not applicable
Conflicts of Interest
None
References
- Mahoney DJ, Stojdl DF, Laird G (2014) Virus therapy for cancer. Sci Am 311(5):54-9. [CrossRef]
- Schreiber RD, Old LJ, Smyth MJ (2011) Cancer immunoediting: integrating immunity’s roles in cancer suppression and promotion. Science 331(6024):1565-70. [CrossRef]
- Postow MA, Callahan MK, Wolchok JD (2015) Immune checkpoint blockade in cancer therapy. J Clin Oncol 33:1974–82. [CrossRef]
- Champiat S, Lambotte O, Barreau E et al (2016) Management of immune checkpoint blockade dysimmune toxicities: a collaborative position paper. Ann Oncol 27(4):559-74. [CrossRef]
- Chiou VL, Burotto M (2015) Pseudoprogression and immune-related response in solid tumors. J Clin Oncol 33(31):3541-3. [CrossRef]
- Abril-Rodriguez G, Ribas A (2017) SnapShot: immune checkpoint inhibitors. Cancer Cell 31(6):848-848.e1. [CrossRef]
- Linsley PS, Wallace PM, Johnson J et al (1992) Immunosuppression in vivo by a soluble form of the CTLA-4 T cell activation molecule. Science 257(5071):792-5. [CrossRef]
- Egen JG, Allison JP (2002) Cytotoxic T lymphocyte antigen-4 accumulation in the immunological synapse is regulated by TCR signal strength. Immunity 16(1):23-35. [CrossRef]
- Leach DR, Krummel MF, Allison JP (1996) Enhancement of antitumor immunity by CTLA-4 blockade. Science 271(5256):1734-6. [CrossRef]
- Han Y, Liu D, Li L (2020) PD-1/PD-L1 pathway: current researches in cancer. Am J Cancer Res 10(3):727-42.
- Dong H, Zhu G, Tamada K, Chen L (1999) B7-H1, a third member of the B7 family, co-stimulates T-cell proliferation and interleukin-10 secretion. Nat Med 5(12):1365-9. [CrossRef]
- Mohsenzadegan M, Bavandpour P, Nowroozi MR et al (2021) The potential of T cell immunoglobulin and mucin-domain containing-3 (Tim-3) in designing novel immunotherapy for bladder cancer. Endocr Metab Immune Disord Drug Targets (12):2131-46. [CrossRef]
- Sprangers B (2019) Pembrolizumab-related renal toxicities: diagnosis first, treatment later. Clin Kidney J 12(1):78-80. [CrossRef]
- Cortazar FB, Marrone KA, Troxell ML et al (2016) Clinicopathological features of acute kidney injury associated with immune checkpoint inhibitors. Kidney Int 90(3):638-47. [CrossRef]
- Hanna RM, Selamet U, Bui P et al (2018) Acute kidney injury after pembrolizumab-induced adrenalitis and adrenal insufficiency. Case Rep Nephrol Dial 8(2):171-77. [CrossRef]
- Dumoulin DW, Visser S, Cornelissen R et al (2020) Renal toxicity from pemetrexed and pembrolizumab in the era of combination therapy in patients with metastatic nonsquamous cell NSCLC. J Thorac Oncol 15(9):1472-83. [CrossRef]
- Izzedine H, Mathian A, Champiat S et al (2019) Renal toxicities associated with pembrolizumab. Clin Kidney J 12(1):81-8. [CrossRef]
- Warner BM, Baer AN, Lipson EJ et al (2019) Sicca syndrome associated with immune checkpoint inhibitor therapy. Oncologist 24(9):1259-69. [CrossRef]
- Som A, Mandaliya R, Alsaadi D et al (2019) Immune checkpoint inhibitor-induced colitis: a comprehensive review. World J Clin Cases 7(4):405-18. [CrossRef]
- El Sabbagh R, Azar NS, Eid AA, Azar ST (2020) Thyroid dysfunctions due to immune checkpoint inhibitors: a review. Int J Gen Med 13:1003-9. [CrossRef]
- Johnson DB, McDonnell WJ, Gonzalez-Ericsson PI et al (2019) A case report of clonal EBV-like memory CD4+ T cell activation in fatal checkpoint inhibitor-induced encephalitis. Nat Med 25(8):1243-50. [CrossRef]
- Liu X, Liang X, Liang J, Li Y, Wang J (2020) Immune thrombocytopenia induced by immune checkpoint inhibitors in solid cancer: case report and literature review. Front Oncol 10:530478. [CrossRef]
- Salinas N, Nowak E, Etienne M et al (2021) Causes of pruritus in patients treated with immune checkpoint inhibitors for melanomas or skin carcinomas. Front Med (Lausanne) 8:632683. [CrossRef]
- Ghoraba H, Or C, Karaca I et al (20229 Immunotherapy-induced retinopathy mimicking cancer associated retinopathy. Am J Ophthalmol Case Rep 26:101449. [CrossRef]
- Takatsuki K, Yanagihara T, Egashira A et al (2021) A rare case of pembrolizumab-induced dermatomyositis in a patient with cancer of unknown primary origin. Am J Case Rep 22:e930286. [CrossRef]
- Rai M, Go M (2020) Nivolumab induced adrenal insufficiency: rare side-effect of a new anti-cancer therapy - immune-checkpoint inhibitors. Cureus 12(4):e7625. [CrossRef]
- Hercun J, Vincent C, Bilodeau M, Lapierre P (2022) Immune-mediated hepatitis during immune checkpoint inhibitor cancer immunotherapy: lessons from autoimmune hepatitis and liver immunology. Front Immunol 13:907591. [CrossRef]
- Weber JS, Kähler KC, Hauschild A (2012) Management of immune-related adverse events and kinetics of response with ipilimumab. J Clin Oncol 30(21):2691-7. [CrossRef]
- Hassel JC, Heinzerling L, Aberle J et al (2017) Combined immune checkpoint blockade (anti-PD-1/anti-CTLA-4): evaluation and management of adverse drug reactions. Cancer Treat Rev 57:36-49. [CrossRef]
- Martins F, Sofiya L, Sykiotis GP et al (2019) Adverse effects of immune-checkpoint inhibitors: epidemiology, management and surveillance. Nat Rev Clin Oncol 16(9):563-80. [CrossRef]
- Wang DY, Salem JE, Cohen JV et al (2018) Fatal toxic effects associated with immune checkpoint inhibitors: a systematic review and meta-analysis. JAMA Oncol 4(12):1721-28. Erratum in: JAMA Oncol 4(12):1792. [CrossRef]
- Oble DA, Mino-Kenudson M, Goldsmith J et al (2008) Alpha-CTLA-4 mAb-associated panenteritis: a histologic and immunohistochemical analysis. Am J Surg Pathol 32(8):1130-7. [CrossRef]
- Read S, Malmström V, Powrie F (2000) Cytotoxic T lymphocyte-associated antigen 4 plays an essential role in the function of CD25(+)CD4(+) regulatory cells that control intestinal inflammation. J Exp Med 192(2):295-302. [CrossRef]
- Troxell ML, Higgins JP, Kambham N (2016) Antineoplastic treatment and renal injury: an update on renal pathology due to cytotoxic and targeted therapies. Adv Anat Pathol 23(5):310-29. [CrossRef]
- Shirali AC, Perazella MA, Gettinger S (2016) Association of acute interstitial nephritis with programmed cell death 1 inhibitor therapy in lung cancer patients. Am J Kidney Dis 68(2):287-91. [CrossRef]
- Caturegli P, Di Dalmazi G, Lombardi M et al (2016) Hypophysitis secondary to cytotoxic T-lymphocyte-associated protein 4 blockade: insights into pathogenesis from an autopsy series. Am J Pathol 186(12):3225-35. [CrossRef]
- Matson DR, Accola MA, Rehrauer WM, Corliss RF (2018) Fatal myocarditis following treatment with the PD-1 inhibitor nivolumab. J Forensic Sci 63(3):954-57. [CrossRef]
- Zha H, Han X, Zhu Y et al (2017) Blocking C5aR signaling promotes the anti-tumor efficacy of PD-1/PD-L1 blockade. Oncoimmunology 6(10):e1349587. [CrossRef]
- Moller DR (1999) Cells and cytokines involved in the pathogenesis of sarcoidosis. Sarcoidosis Vasc Diffuse Lung Dis 16(1):24-31.
- Facco M, Cabrelle A, Teramo A et al (2011) Sarcoidosis is a Th1/Th17 multisystem disorder. Thorax 66(2):144-50. [CrossRef]
- Lomax AJ, McGuire HM, McNeil C et al (2017) Immunotherapy-induced sarcoidosis in patients with melanoma treated with PD-1 checkpoint inhibitors: case series and immunophenotypic analysis. Int J Rheum Dis 20(9):1277-85. [CrossRef]
- Yamauchi I, Sakane Y, Fukuda Y et al (2017) Clinical features of nivolumab-induced thyroiditis: a case series study. Thyroid 27(7):894-901. [CrossRef]
- Quirk SK, Shure AK, Agrawal DK (2015) Immune-mediated adverse events of anticytotoxic T lymphocyte-associated antigen 4 antibody therapy in metastatic melanoma. Transl Res 166(5):412-24. [CrossRef]
- Polakos NK, Cornejo JC, Murray DA et al (2006) Kupffer cell-dependent hepatitis occurs during influenza infection. Am J Pathol 168(4):1169-78; quiz 1404-5. [CrossRef]
- Teulings HE, Limpens J, Jansen SN et al (2015) Vitiligo-like depigmentation in patients with stage III-IV melanoma receiving immunotherapy and its association with survival: a systematic review and meta-analysis. J Clin Oncol 33(7):773-81. [CrossRef]
- Freeman-Keller M, Kim Y, Cronin H et al (2016) Nivolumab in resected and unresectable metastatic melanoma: characteristics of immune-related adverse events and association with outcomes. Clin Cancer Res 22(4):886-94. [CrossRef]
- Wang Y, Abu-Sbeih H, Mao E et al (2018) Endoscopic and histologic features of immune checkpoint inhibitor-related colitis. Inflamm Bowel Dis 24(8):1695-1705. [CrossRef]
- Faje AT, Sullivan R, Lawrence D et al (2014) Ipilimumab-induced hypophysitis: a detailed longitudinal analysis in a large cohort of patients with metastatic melanoma. J Clin Endocrinol Metab 99(11):4078-85. [CrossRef]
- Spain L, Diem S, Larkin J (2016) Management of toxicities of immune checkpoint inhibitors. Cancer Treat Rev 44:51-60. [CrossRef]
- González-Rodríguez E, Rodríguez-Abreu D; Spanish Group for Cancer Immuno-Biotherapy (GETICA) (2016) Immune checkpoint inhibitors: review and management of endocrine adverse events. Oncologist 21(7):804-16. [CrossRef]
- Kumar V, Chaudhary N, Garg M et al (2017) Current diagnosis and management of immune related adverse events (irAEs) induced by immune checkpoint inhibitor therapy. Front Pharmacol 8:49. [CrossRef]
- Friedman CF, Proverbs-Singh TA, Postow MA (2016) Treatment of the immune-related adverse effects of immune checkpoint inhibitors: a review. JAMA Oncol 2(10):1346-53. [CrossRef]
- Torino F, Barnabei A, De Vecchis L et al (2012) Hypophysitis induced by monoclonal antibodies to cytotoxic T lymphocyte antigen 4: challenges from a new cause of a rare disease. Oncologist 17(4):525-35. [CrossRef]
- Linardou H, Gogas H (2016) Toxicity management of immunotherapy for patients with metastatic melanoma. Ann Transl Med 4(14):272. [CrossRef]
- Weber JS, Yang JC, Atkins MB, Disis ML (2015) Toxicities of immunotherapy for the practitioner. J Clin Oncol 33(18):2092-9. [CrossRef]
- Zhang HC, Luo W, Wang Y (2019) Acute liver injury in the context of immune checkpoint inhibitor-related colitis treated with infliximab. J Immunother Cancer 7(1):47. [CrossRef]
- Calvo R (2019) Hematological side effects of immune checkpoint inhibitors: the example of immune-related thrombocytopenia. Front Pharmacol 10:454. [CrossRef]
- Menzies AM, Johnson DB, Ramanujam S et al (2017) Anti-PD-1 therapy in patients with advanced melanoma and preexisting autoimmune disorders or major toxicity with ipilimumab. Ann Oncol 28(2):368-76. [CrossRef]
- Johnson DB, Sullivan RJ, Ott PA et al (2016) Ipilimumab therapy in patients with advanced melanoma and preexisting autoimmune disorders. JAMA Oncol 2(2):234-40. [CrossRef]
- Abdel-Wahab N, Shah M, Lopez-Olivo MA, Suarez-Almazor ME (2018) Use of immune checkpoint inhibitors in the treatment of patients with cancer and preexisting autoimmune disease: a systematic review. Ann Intern Med 168(2):121-30. [CrossRef]
- Horvat TZ, Adel NG, Dang TO et al (2015) Immune-related adverse events, need for systemic immunosuppression, and effects on survival and time to treatment failure in patients with melanoma treated with ipilimumab at Memorial Sloan Kettering Cancer Center. J Clin Oncol 33(28):3193-8. [CrossRef]
- Bessede A, Marabelle A, Guégan JP et al (2022) Impact of acetaminophen on the efficacy of immunotherapy in cancer patients. Ann Oncol 33(9):909-15. [CrossRef]
- Lissoni P, Mandalà M, Brivio F (2000) Abrogation of the negative influence of opioids on IL-2 immunotherapy of renal cell cancer by melatonin. Eur Urol 38(1):115-8. [CrossRef]
- Prasetya RA, Metselaar-Albers M, Engels F (2021) Concomitant use of analgesics and immune checkpoint inhibitors in non-small cell lung cancer: a pharmacodynamics perspective. Eur J Pharmacol 906:174284. [CrossRef]
- Kato S, Goodman A, Walavalkar V et al (2017) Hyperprogressors after immunotherapy: analysis of genomic alterations associated with accelerated growth rate. Clin Cancer Res 23(15):4242-50. [CrossRef]
- Saâda-Bouzid E, Defaucheux C, Karabajakian A et al (2017) Hyperprogression during anti-PD-1/PD-L1 therapy in patients with recurrent and/or metastatic head and neck squamous cell carcinoma. Ann Oncol 28(7):1605-11. [CrossRef]
- Freixinos VR, Garcia A, Fasani R et al (2018) Immune profile and outcomes of patients (pts) with gynecological malignancies (GYN) enrolled in early phases immunotherapy (IO) trials. J Clin Oncol 36(15_suppl):5595. [CrossRef]
- Matos I, Martin-Liberal J, Hierro C et al (2018) Incidence and clinical implications of a new definition of hyperprogression (HPD) with immune checkpoint inhibitors (ICIs) in patients treated in phase 1 (Ph1) trials. J Clin Oncol 36(15_suppl):3032. [CrossRef]
- Arnold CE, Rajnicek AM, Hoare JI et al (2019) Physiological strength electric fields modulate human T cell activation and polarisation. Sci Rep 9(1):17604. [CrossRef]
- Salerno S, La Mendola C, La Manna MP et al (2009) Reversible effect of magnetic fields on human lymphocyte activation patterns: different sensitivity of naive and memory lymphocyte subsets. Radiat Res 172(4):444-50. [CrossRef]
Figure 1.
General management approach for ICIT and irAEs.
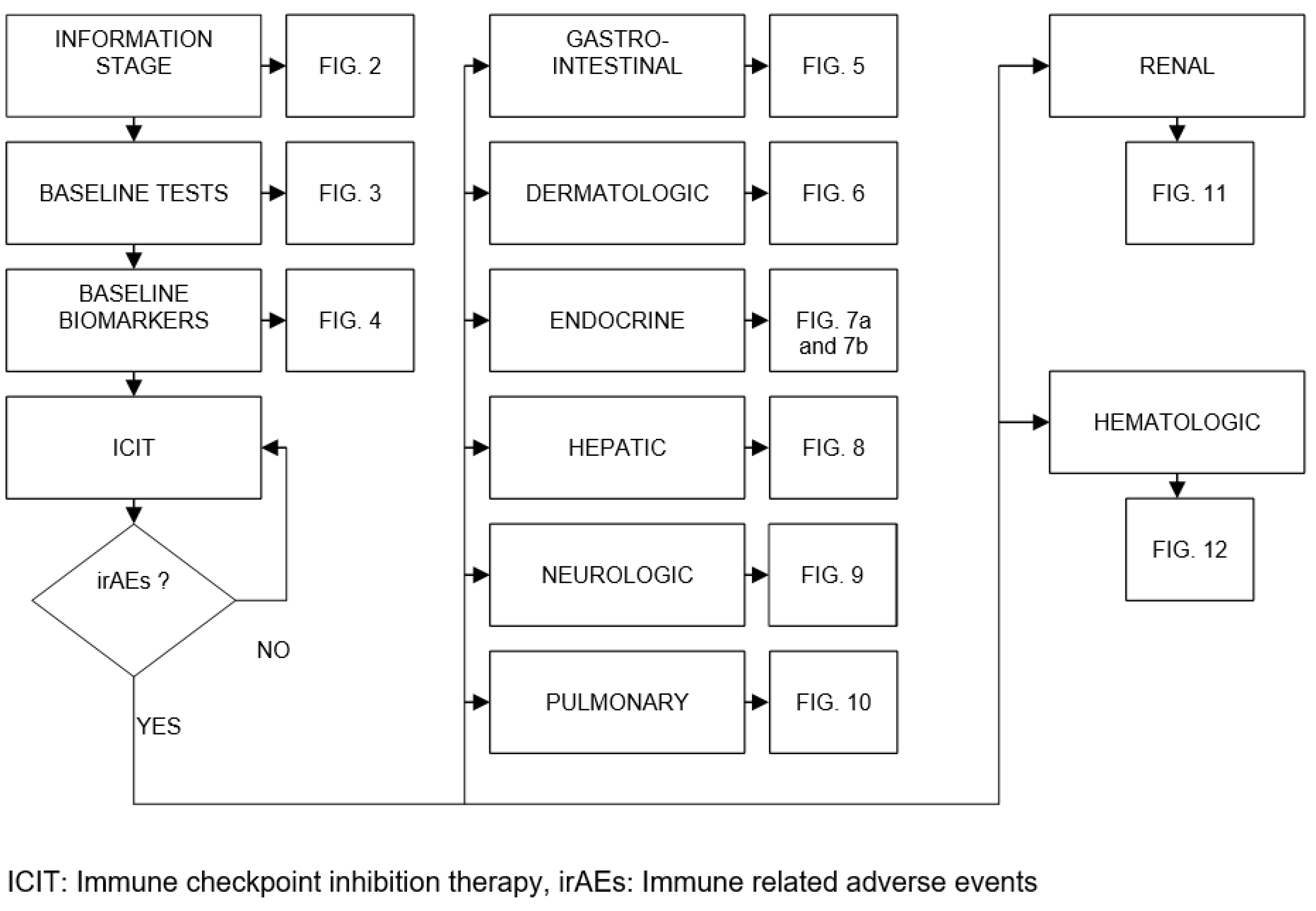
Figure 2.
Decomposition of the information stage.
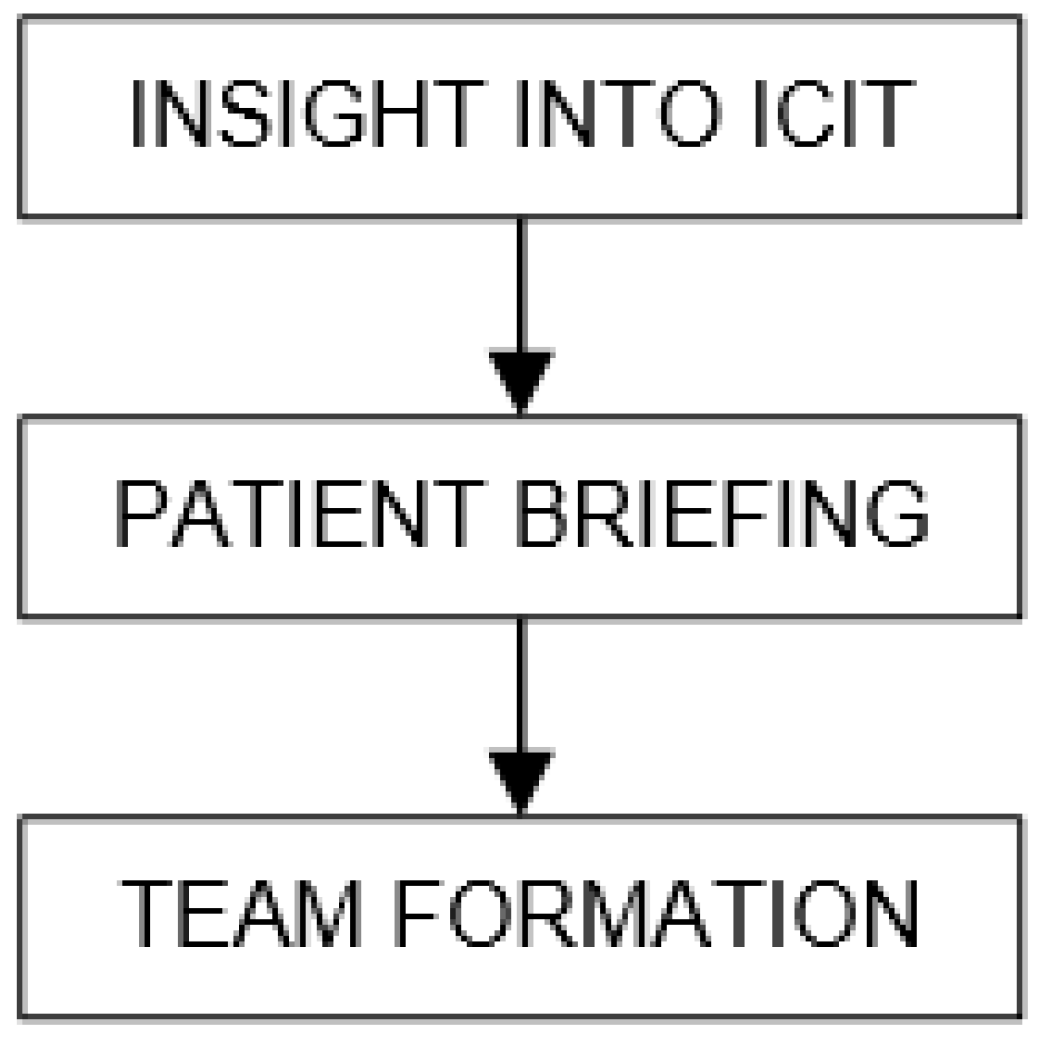
Figure 3.
Baseline tests details.
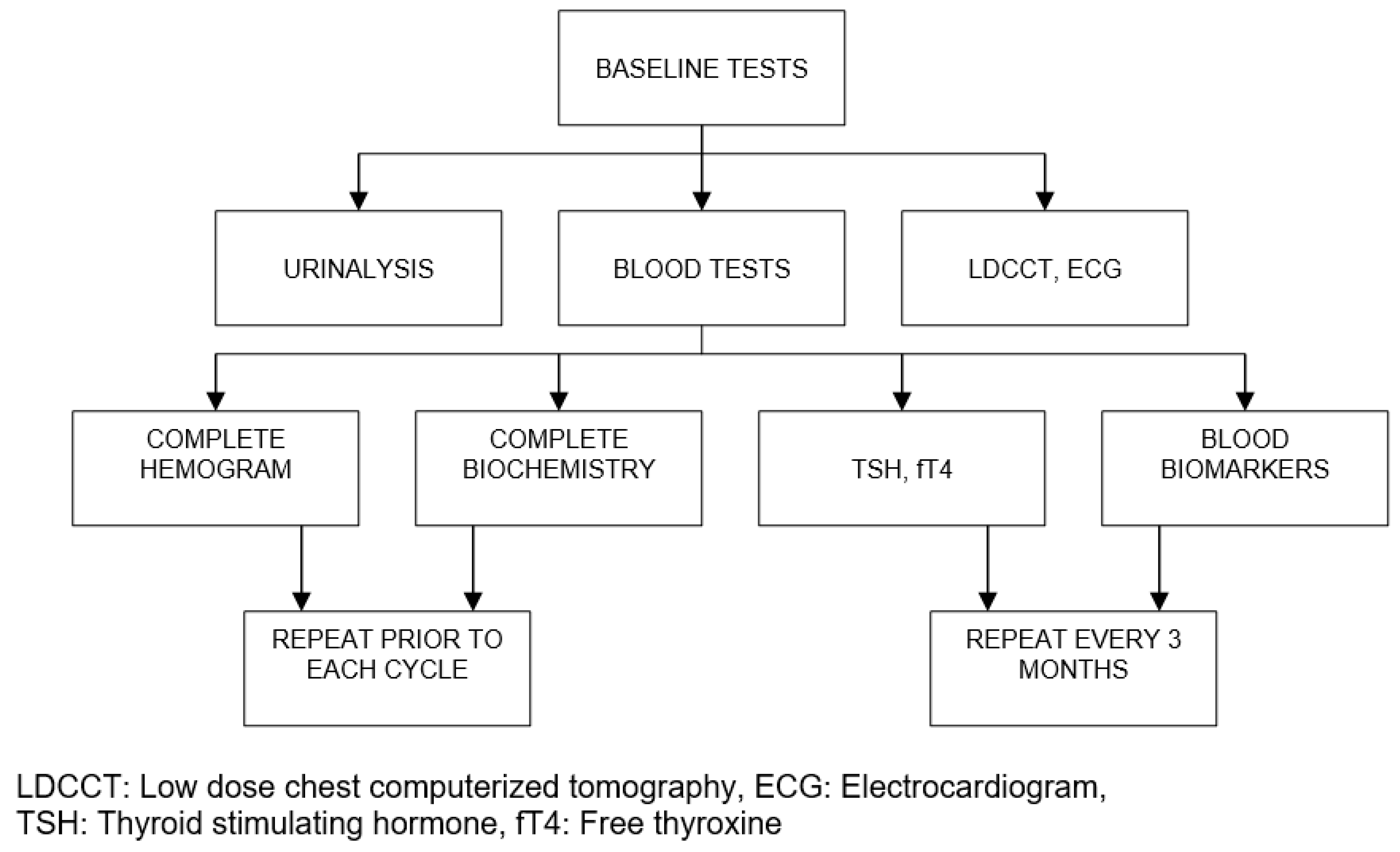
Figure 4.
List of baseline biomarkers.
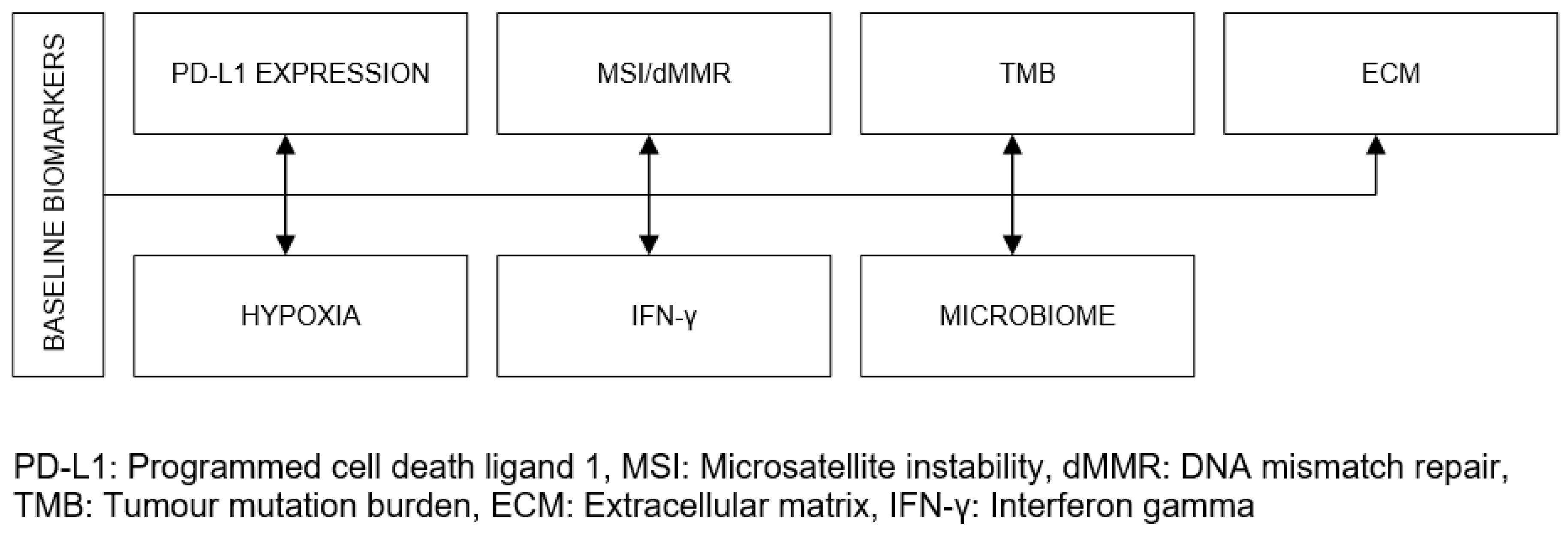
Figure 5.
Management algorithm for colitis/diarrhea.
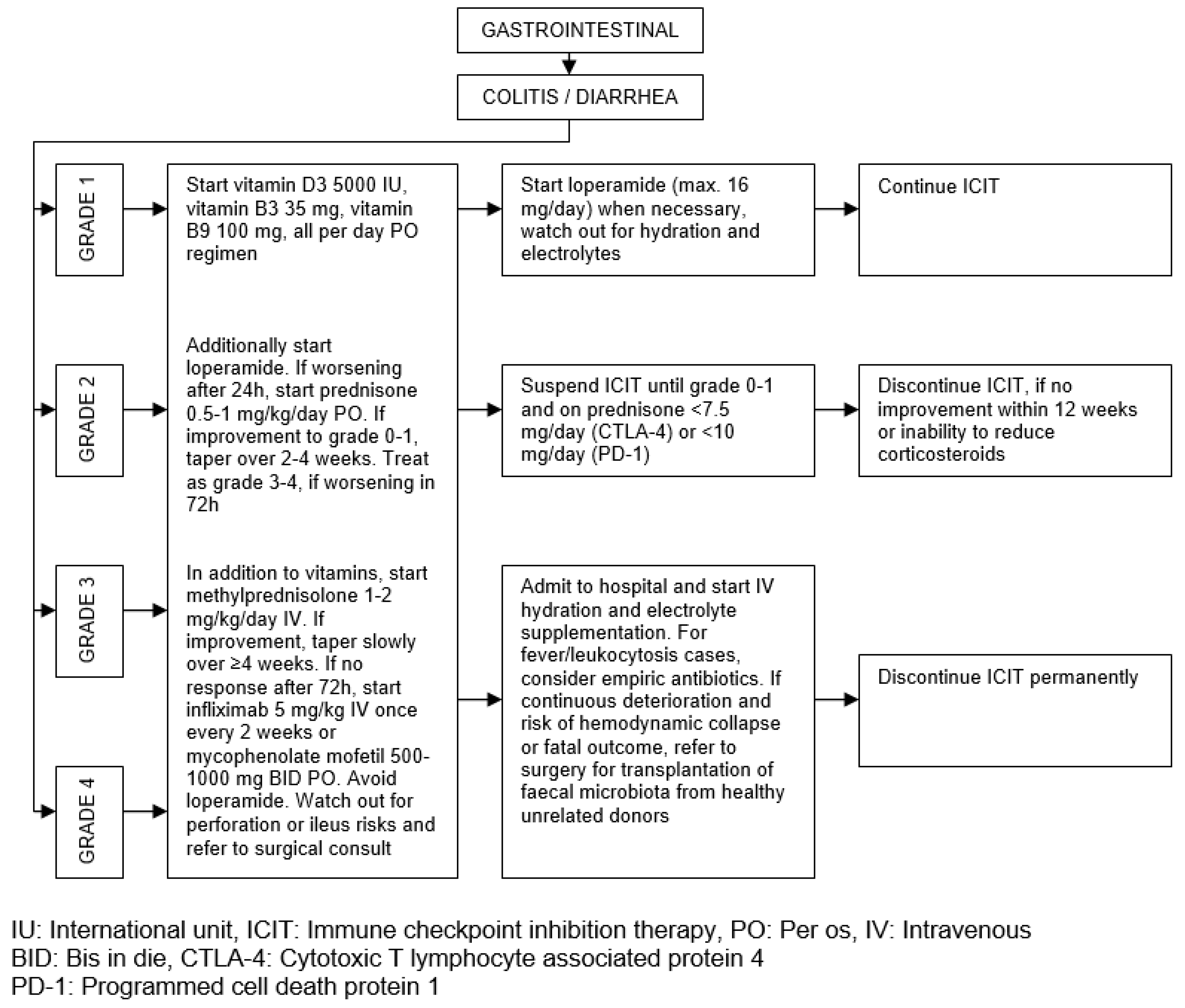
Figure 6.
Management approach for dermatitis.
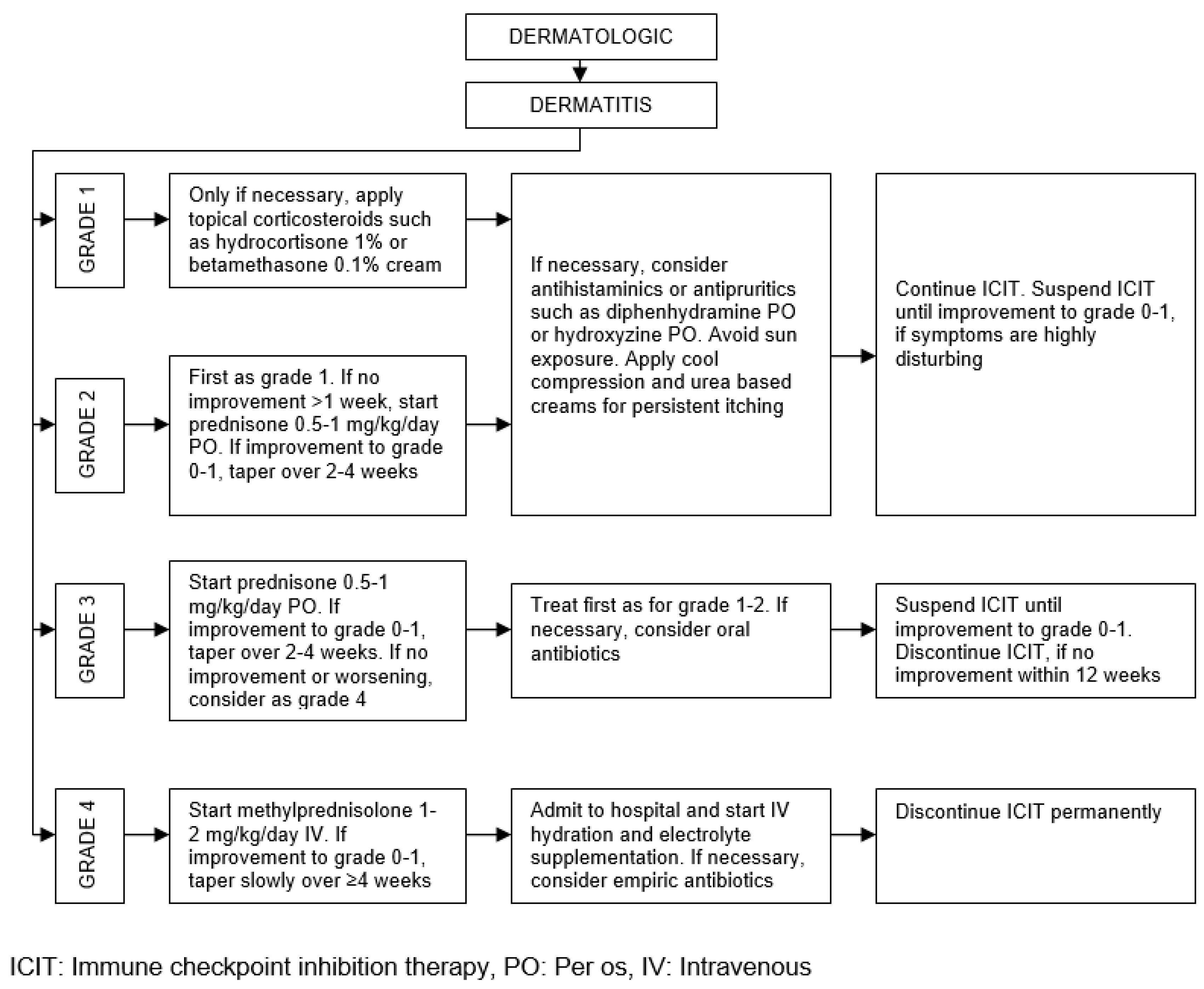
Figure 7.
(a) Management strategy for hypothyroidism and hyperthyroidism. (b) Management strategy for hypophysitis and Addison’s disease.
Figure 7.
(a) Management strategy for hypothyroidism and hyperthyroidism. (b) Management strategy for hypophysitis and Addison’s disease.
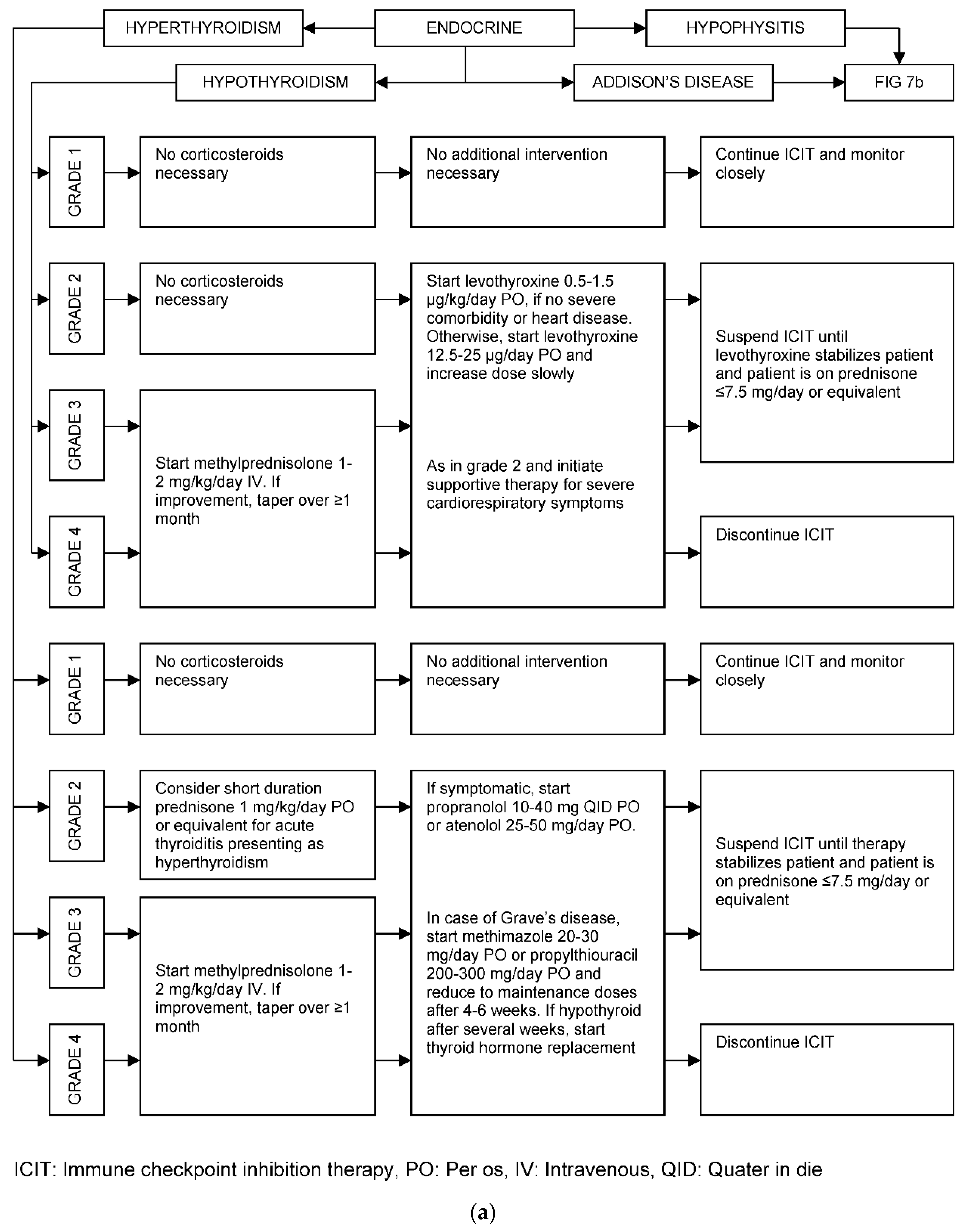
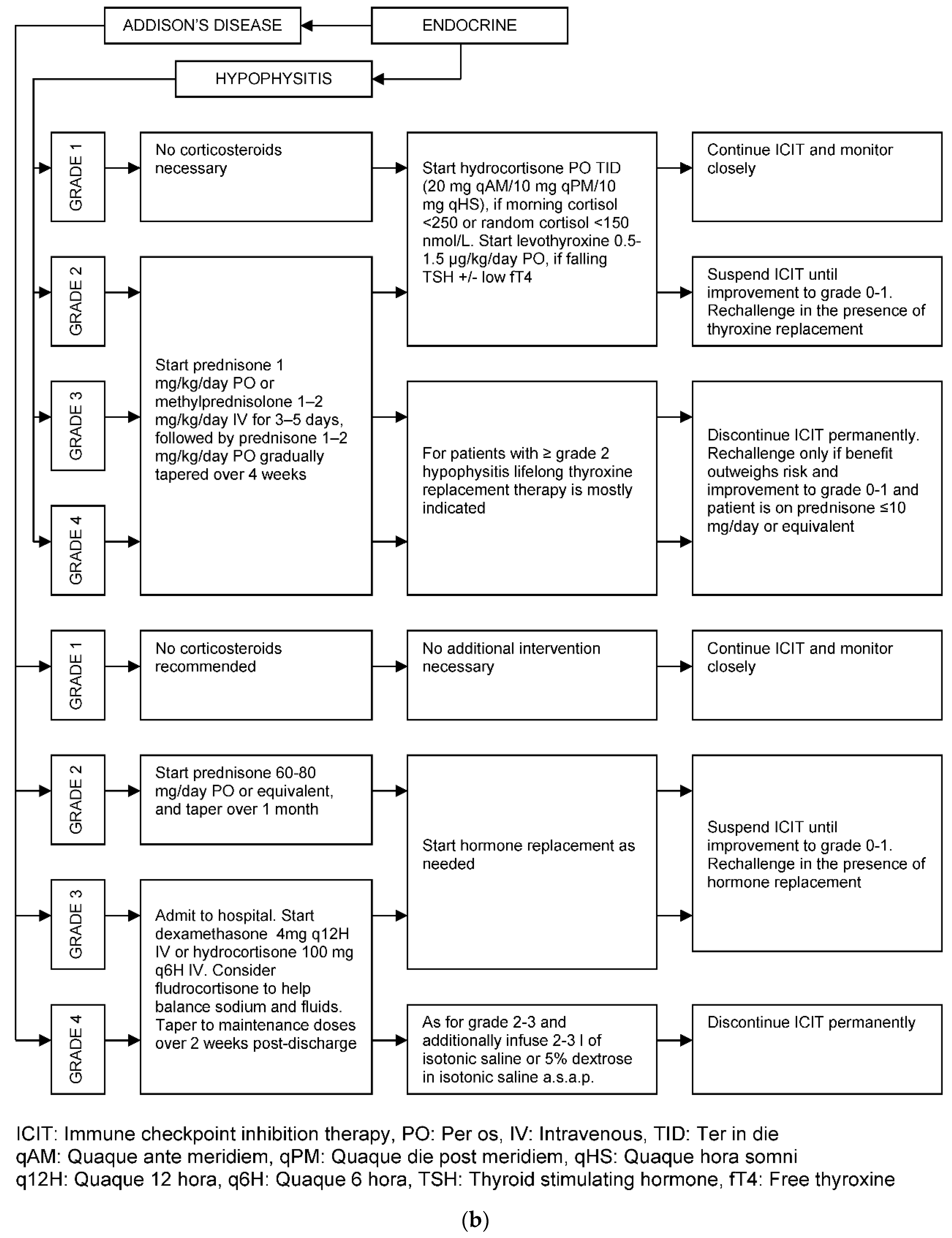
Figure 8.
Management algorithm for hepatitis.
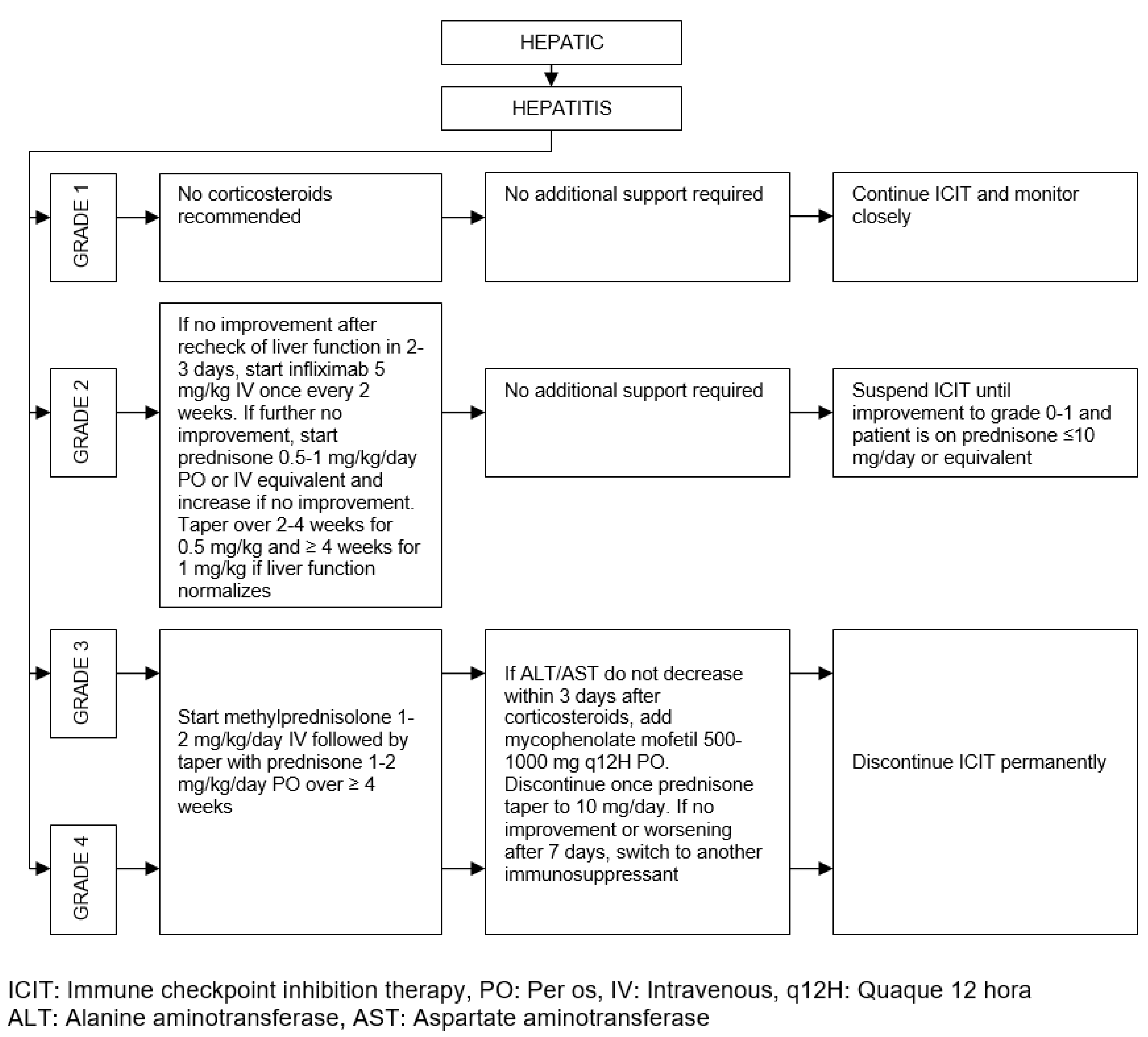
Figure 9.
General management approach for ICIT induced neurologic irAEs.
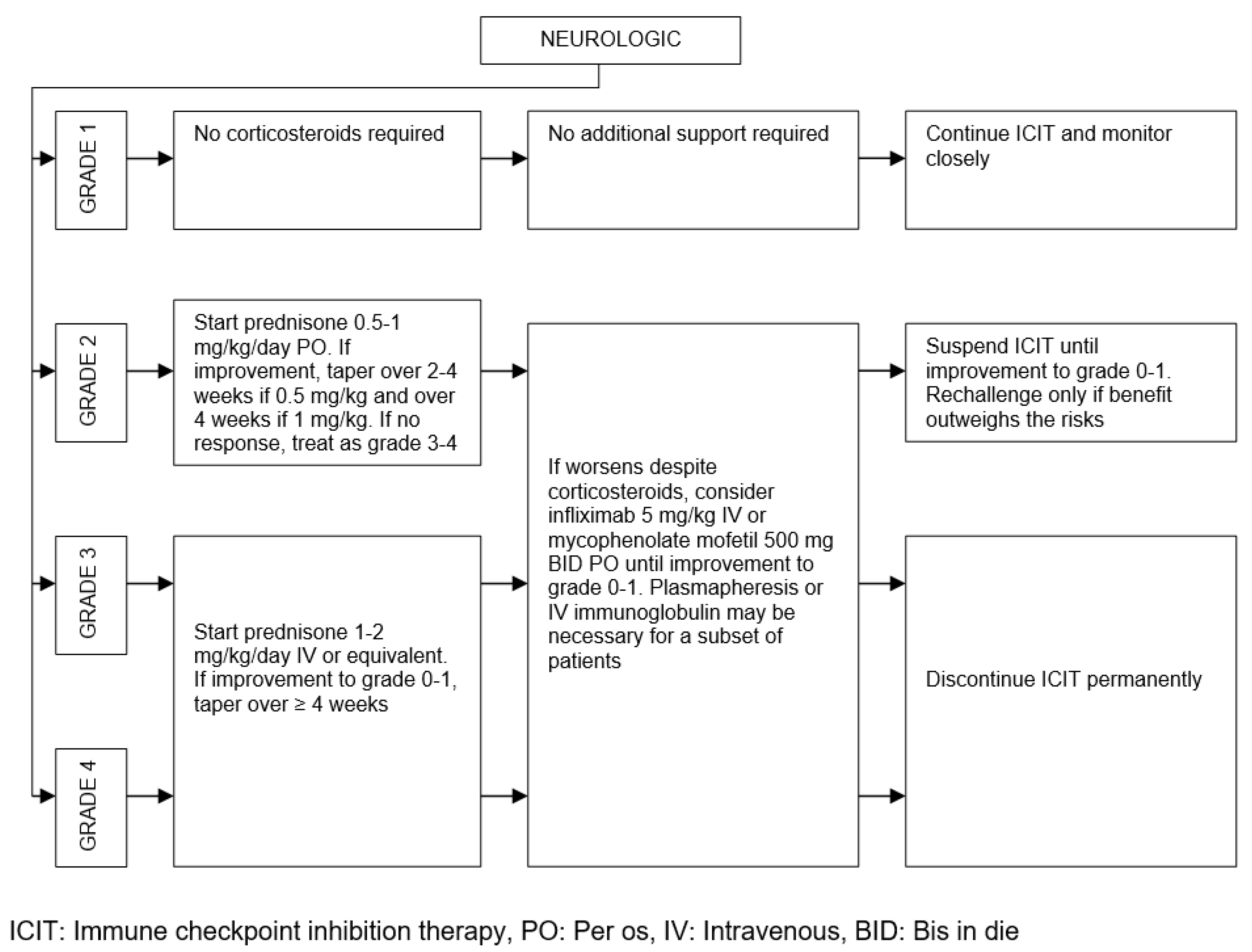
Figure 10.
Management algorithm for pneumonitis.
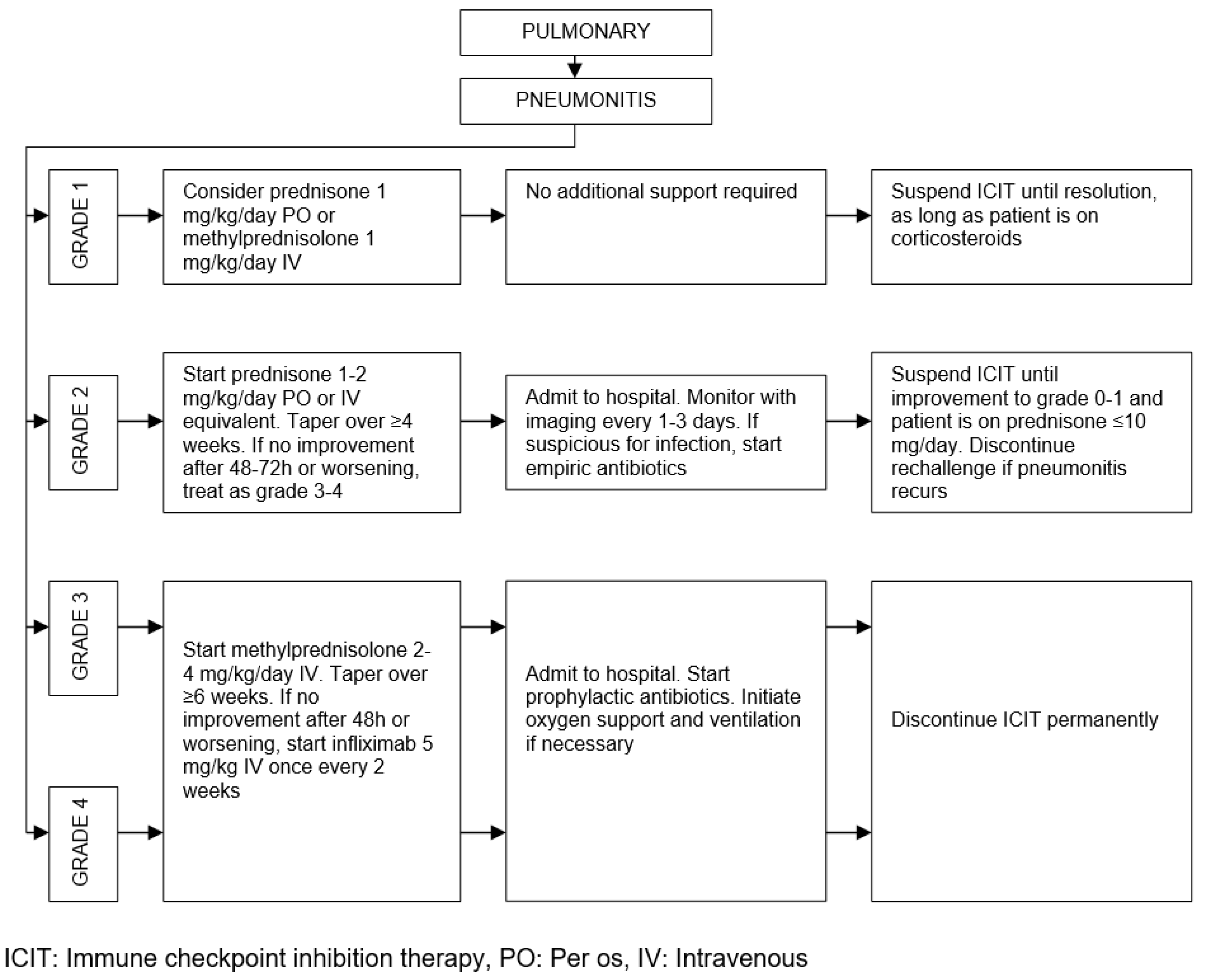
Figure 11.
Management algorithm for renal toxicities.
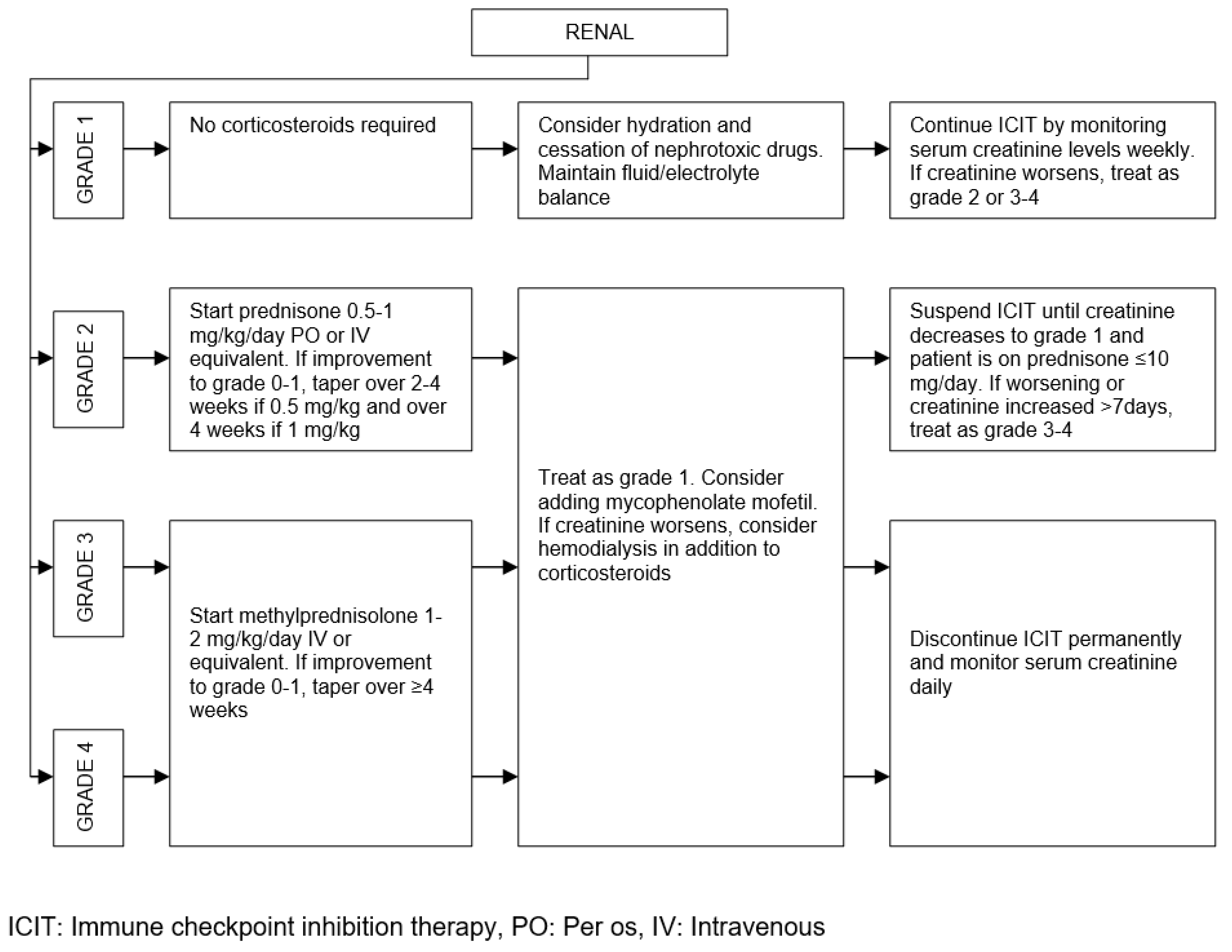
Figure 12.
Management strategy for thrombocytopenia.
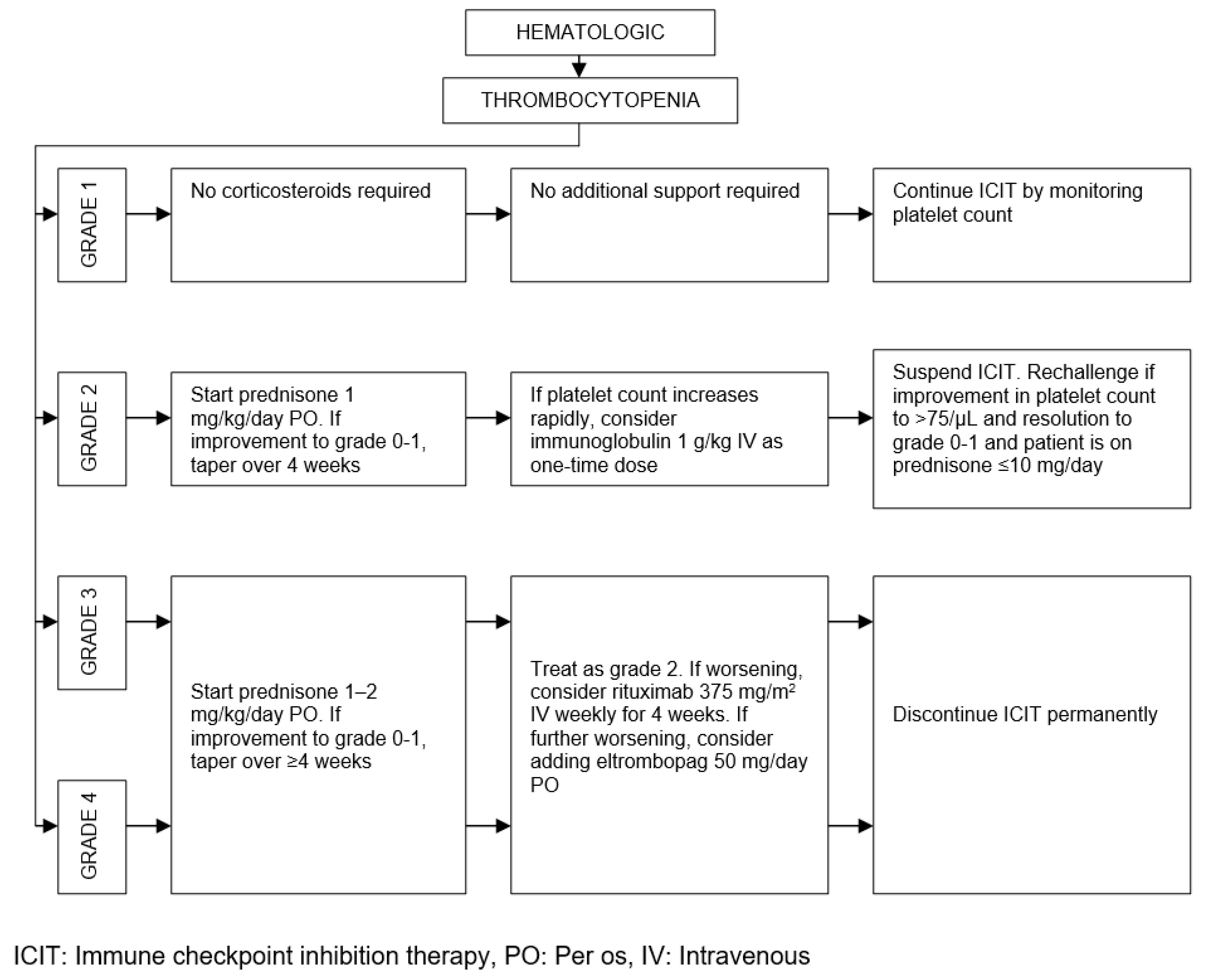
Figure 13.
Traditional cancer pain management strategy.
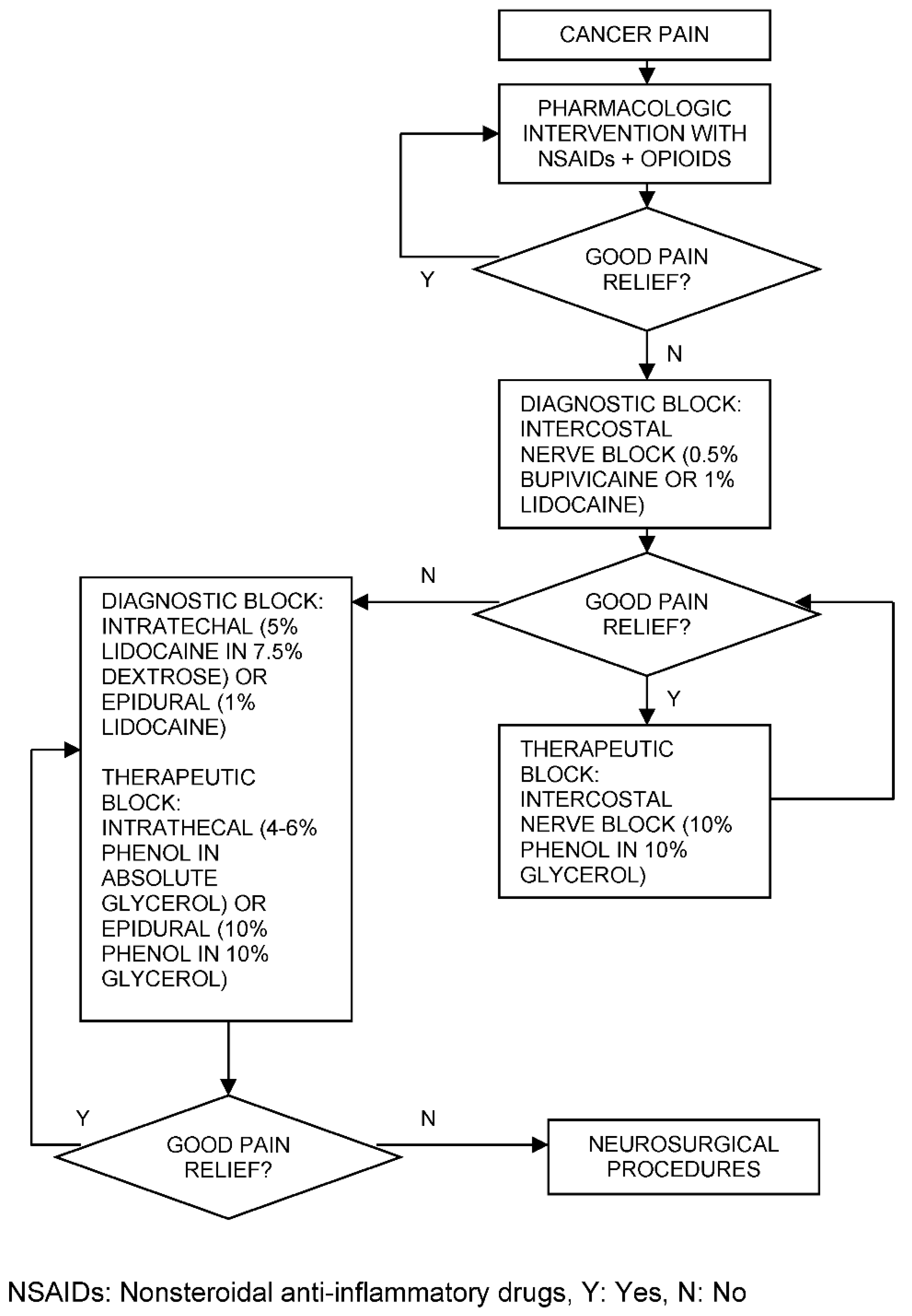
Figure 14.
ICIT response patterns and decision strategies.
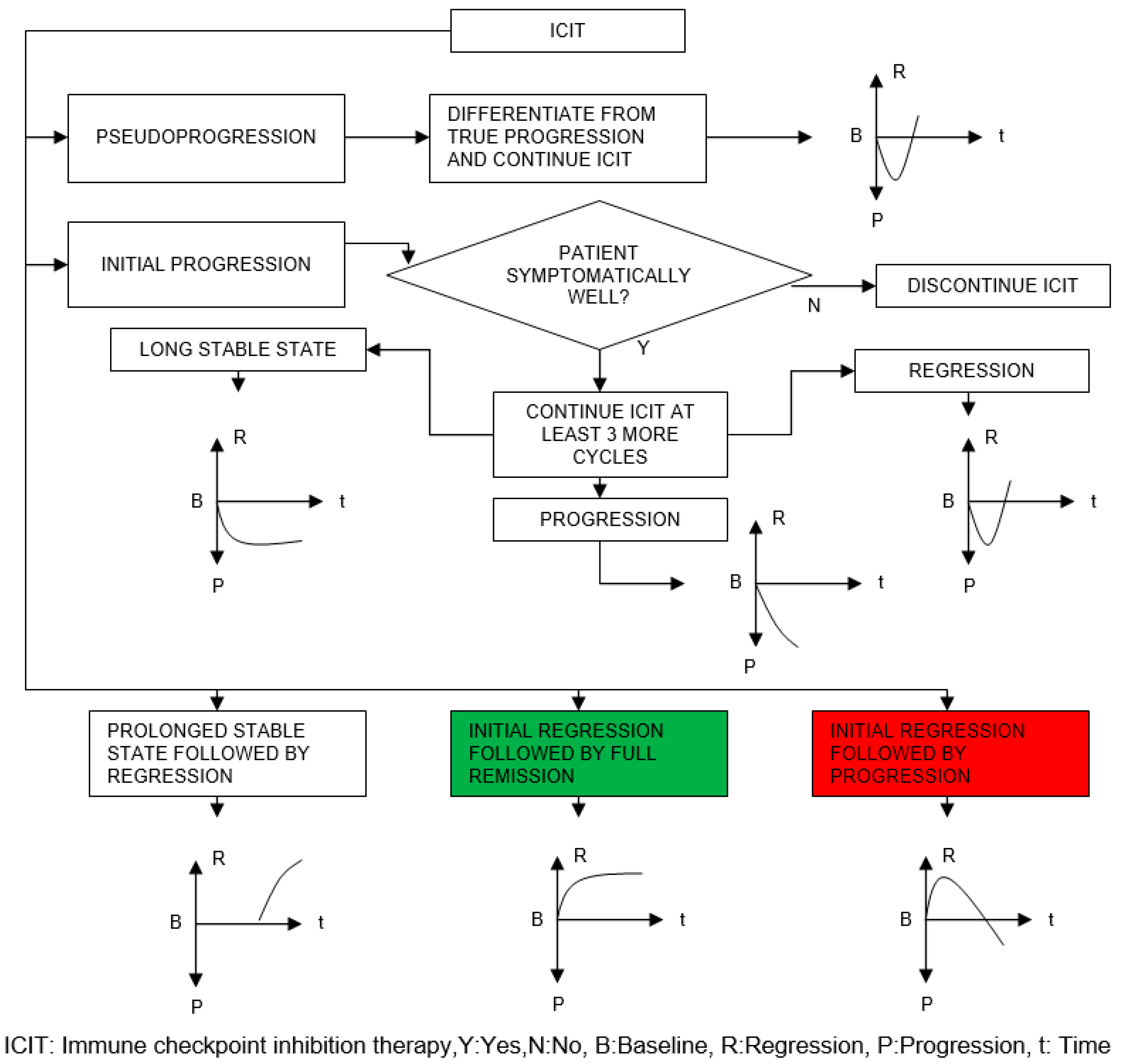
Table 1.
Selected irAEs with respect to organ/tissue systems and their onset frequency.
| Organ/Tissue System | irAEs | Approx. Onset Frequency (%) |
|---|---|---|
| Gastrointestinal | Oral mucositis | < 5 |
| Xerostomia | < 6 | |
| Gastritis | > 50 (PD-1), < 5 (PD-L1) | |
| Colitis | > 10 | |
| Ileitis | > 10 | |
| Hepatitis | 5 – 10 | |
| Pancreatitis | < 5 | |
| Dermatologic | Dermatitis | > 20 |
| Pruritus | 10 – 50 | |
| Stevens Johnson | < 5 | |
| Psoriasis | < 5 | |
| Vitiligo | 5 – 10 | |
| DRESS syndrome | < 4 | |
| Endocrine | Hypohysitis | 5 – 10 |
| Hyper-/hypothyroidism | < 10 | |
| Diabetes Mellitus | < 3 | |
| Addison's disease | 5 – 10 | |
| Pulmonary | Pleuritis | < 1 |
| Pneumonitis | < 5 | |
| Sarcoid-like granulomatosis | 5 – 7 (CTLA-4), < 0.5 (PD-L1) | |
| Neurologic | Encephalitis | < 5 |
| Meningitis | < 5 | |
| Guillain Barré | < 5 | |
| Neuropathy | < 5 | |
| Myasthenia gravis | < 5 | |
| Myelopathy | < 1 | |
| Optic neuritis | < 1 | |
| Cardiovascular | Myocarditis | < 5 |
| Pericarditis | < 3 | |
| Vasculitis | < 1 | |
| Hematologic | Thrombocytopenia | < 2 |
| Neutropenia | < 1 | |
| Hemolytic anemia | < 5 (CTLA-4), < 10 (PD-1) | |
| Pancytopenia | < 1 | |
| Renal | Acute interstitial nephritis | < 5 |
| Acute tubular injury | < 1 | |
| Glomerulonephritis | < 2 | |
| Musculoskeletal | Dermatomyositis | < 1 |
| Arthritis | < 4 | |
| Ocular | Retinitis | < 3 |
| Conjunctivitis | < 1 | |
| Uveitis | < 5 | |
| Scleritis | < 1 |
irAEs: Immune related adverse events. CTLA-4: Cytotoxic T lymphocyte associated protein 4. PD-1: Programmed cell death protein 1. PD-L1: Programmed cell death ligand 1. DRESS: Drug reaction with eosinophilia and systemic symptoms.
Table 2.
Approximate timing in weeks of selected irAEs in different scenarios.
| ICIT | irAEs | Onset Time (Week) |
CTCAE Peak (Week) |
Damping Time (Week) |
|---|---|---|---|---|
| CTLA-4 | Colitis | 4 – 5 | 6 | 10 |
| Hepatitis | 6 – 7 | 8 – 13 | 15 | |
| Pancreatitis | 3 – 9 | N/A | N/A | |
| Pruritus | ≈ 4 | ≈ 5 | ≈ 6 | |
| Hypohysitis | 6 – 7 | 8 | ∞ | |
| Addison's disease | 6 – 7 | 8 | ∞ | |
| Myasthenia gravis | 2 – 6 | 1 – 4 | N/A | |
| Acute interstitial nephritis | 2 – 12 | N/A | N/A | |
| PD-1 or PD-L1 | Colitis | 4 – 5 | 6 | 10 |
| Hepatitis | 6 – 7 | 8 – 14 | 15 | |
| Pancreatitis | 3 – 30 | N/A | N/A | |
| Pruritus | ≈ 4 | ≈ 5 | ≈ 6 | |
| Hypohysitis | 6 – 7 | 8 | ∞ | |
| Addison's disease | 6 – 7 | 8 | ∞ | |
| Pneumonitis | 10 – 11 | 12 | 22 | |
| Myasthenia gravis | 4 – 5 | N/A | N/A | |
| Acute interstitial nephritis | 12 – 72 | N/A | N/A | |
| CTLA-4 and PD-1 | Colitis | 3 – 4 | 5 | 10 |
| Hepatitis | 5 – 6 | 7 – 13 | 15 | |
| Pruritus | ≈ 2 | ≈ 4 | ≈ 5 | |
| Hypohysitis | ≈ 2 | 4 | ∞ | |
| Addison's disease | ≈ 2 | 4 | ∞ | |
| Pneumonitis | ≈ 5 | ≈ 7 | ≈ 11 | |
| Myasthenia gravis | 2 | N/A | N/A |
ICIT: Immune checkpoint inhibition therapy. irAEs: Immune related adverse events. CTCAE: Common terminology criteria for adverse events. CTLA-4: Cytotoxic T lymphocyte associated protein 4. PD-1: Programmed cell death protein 1. PD-L1: Programmed cell death ligand 1. N/A: Not available.
Table 3.
Approximate timing and frequency of irAEs for CTLA-4/PD-1 combination.
| ICIT | irAEs | Onset Time (Week) |
Frequency Peak (Week and %) |
Damping Time (Week) |
|
|---|---|---|---|---|---|
| CTLA-4 and PD-1 | Gastrointestinal | 0 – 1 | ≈ 5 | ≈ 46 | 6 – 8 |
| Dermatologic | 0 | ≈ 2 | ≈ 52 | 4 – 5 | |
| Endocrine | 2 – 3 | ≈ 10 | ≈ 9 | ≈ 18 | |
| Pulmonary | ≈ 1 | 5 – 6 | 25 | ≈ 10 | |
| Hepatic | 0 | 4 – 5 | 39 | ≈ 8 | |
| Renal | 1 | 5 – 6 | ≈ 5 | 10 | |
| Other | 2 | 10 | ≈ 2 | 18 | |
ICIT: Immune checkpoint inhibition therapy. irAEs: Immune related adverse events. CTLA-4: Cytotoxic T lymphocyte associated protein 4. PD-1: Programmed cell death protein 1.
Table 4.
TSH and fT4 effects in diagnosis.
| Diagnosis | TSH | fT4 |
|---|---|---|
| Primary hypothyroidism | High | Low |
| Subclinical hypothyroidism | High | Normal |
| Secondary hypothyroidism | Normal | Low |
| Primary hyperthyroidism | Low | High |
| Subclinical hyperthyroidism | Low | Normal |
TSH: Thyroid stimulating hormone, fT4: Free thyroxine.
Table 5.
Drugs in cancer pain management.
| Class | Type | Examples | Notes |
|---|---|---|---|
| Nonopioids | NSAIDs | Ibuprofen, aspirin, diflunisal, piroxicam, naproxen | Risk of renal failure in chronic use, not recommended in hemostatic disorders, risk of gastrointestinal bleeding |
| Acetaminophen | Paracetamol | Risk of hepatotoxicity in overdosage | |
| Weak opioids | Codeine | Oxycodone, hydrocodone, propoxyphene | Mostly in combination with NSAIDs or acetaminophen |
| Potent opioids with short half-life | MorphineFentanyl | Oxymorphone, hydromorphone, meperidine, pentazocine, butorphanol | Meperidine not recommended in patients with renal disease |
| Potent opioids with long half-life | MethadoneLevorphanol | Risk of withdrawal symptoms in physically dependent patients |
NSAIDs: Nonsteroidal anti-inflammatory drugs.
Table 6.
Definition of parameter scoring in the Hendekli ICIT success rate (%) model.
| Parameter | Definition of Scoring |
|---|---|
| Score with 100, if regression starts after the first initial infusion | |
| Score with 100 – 5x, if regression starts after the xth infusion where x=2,...,6 | |
| Score with 100 – 7y, if regression starts after the yth infusion where y=7,...,11 | |
| Score with 10, if regression starts beyond the 12th infusion | |
| Score with 0, if no regression is observed at the assessment stage | |
| Score with x, where x denotes tumor volume shrinkage in % | |
| Score with the average for multiple tumors, i.e. number of tumors | |
| Score with 100, if remission starts latest after the 3rd infusion | |
| Score with 100 – 10(x – 3), if remission starts after the xth infusion where x=4,...,11 | |
| Score with 10, if remission starts beyond the 12th infusion | |
| Score with 0, if no remission is observed at the assessment stage | |
| Score between 100 – 75, if there is no preexisting comorbidity and autoimmune disorder | |
| Score between 74 – 50, if there is only one preexisting comorbidity or autoimmune disorder | |
| Score between 49 – 0, if there is more than one preexisting comorbidity or autoimmune disorder | |
| Score with 100, if all of the baseline biomarkers in Figure 4 present compatibility with ICIT | |
| Score with 100 – 14(7 – x), if x of the baseline biomarkers in Figure 4 present compatibility with ICIT where x=1,...,6 | |
| Score with 0, if none of the baseline biomarkers in Figure 4 present compatibility with ICIT | |
| Score with 5, if there is no irAE after the first initial infusion | |
| Score with 5x, if there is no irAE after the xth infusion where x=2,...,20 | |
| Score with 0 when any irAE is observed at the assessment stage | |
| Increment each w with whose corresponding parameter scored between 100 – 60 in the previous assessment stage where denotes number of weightings to be incremented | |
| Decrement each w with whose corresponding parameter scored between 40 – 0 in the previous assessment stage where denotes number of weightings to be decremented |
ICIT: Immune checkpoint inhibition therapy. : Timing of regression start. : Regression rate. : Timing of remission start. : Personal immune strength score. : Baseline biomarker compatibility. : Time without toxicity or irAEs. : Person-specific dynamic weightings
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



