
Submitted:
20 January 2023
Posted:
24 January 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
During the COVID-19 pandemic, the high prevalence of comorbidities in Mexico, as well as the disparities between public and private health subsystems, substantially contributed to the severe impact it had in the country. The objective of this study was to evaluate and compare risk factors present at admission for mortality of hospitalized patients with COVID-19. A 2-year retrospective cohort study of hospitalized adult patients with COVID-19 was conducted at a private tertiary care center. The study population consisted of 1,258 patients with a median age of 56 ± 16.5 years, of whom 1,093 recovered (86.8%) and 165 died (13.1%). In the univariate analysis, older age (p <0.001), comorbidities such as hypertension (p <0.001) and diabetes (p <0.001), signs and symptoms of respiratory distress, and markers of acute inflammatory response were significantly more frequent in non-survivors. The multivariate analysis showed that older age (p <0.001), the presence of cyanosis (p 0.005) and previous myocardial infarction (p 0.032) were independent predictors for mortality. In the studied cohort, risk factors present at admission associated with an increased risk of death were older age, cyanosis and a previous myocardial infarction, which can be used as valuable predictors for patients’ outcomes. To our knowledge, this is the first study analyzing predictors of mortality in COVID-19 patients attended on a private tertiary hospital in Mexico.
Keywords:
COVID-19
; Cohort
; Mortality
; Mexico
1. Introduction
Two years after being declared a global pandemic by the World Health Organization (WHO) on March 11th, 2020, the coronavirus disease-2019 (COVID-19), caused by the severe acute respiratory syndrome coronavirus-2 (SARS-COV-2), has caused more than 449,000,000 cases and 6.6 million deaths [1,2]. COVID-19 is transmitted primarily through large respiratory droplets, presenting with a wide array of clinical manifestations which range from asymptomatic, mild respiratory, and extrapulmonary disease, to life-threatening respiratory failure, multi-organic failure, and death [1,3,4].
Due to the magnitude of the pandemic and the current absence of effective curative treatment, several studies have reported clinical and epidemiological characteristics of their respective populations, which can be used as a proxy for the prediction of patients’ outcomes [1,3,12–21,4,22–27,5–11]. Currently, risk factors related to worse clinical outcomes and mortality include older age, male sex, obesity, comorbidities such as diabetes, hypertension, and heart failure, and laboratory features compatible with an inflammatory state [1,2,21,28,29,3,4,5,10,14–16,19].
Latin America and the Caribbean (LAC) has arguably been one of the most impacted areas by the pandemic, having had five of the region’s countries among the 20 with the highest number of both reported cases and deaths [30,31]. The pandemic has had a very elevated socioeconomic impact on the region, especially affecting vulnerable populations, such as groups with a high poverty index or lack of formal employment [5,31], as well as with preexisting comorbidities, exacerbated by deficiencies of the health institutions in the most vulnerable countries [32], with most of these being unable to guarantee public health care to a considerable percentage of the population. As a response to the lack of complete public coverage, the health systems in countries such as Mexico are forced to heavily rely on private spending [32,33,34].
The country has experienced six waves of disease, resulting in more than 7.2 million cases and 331,407 deaths to date [35]. Despite not having the highest mortality rate of LAC, Mexico currently stands as the fifth country with the most deaths worldwide [35]. The alarming mortality, correlated with the aforementioned risk factors [5,7,36,37], can also be associated with the differences among healthcare institutions; evidence suggests that the lack of homogeneity among available resources, infrastructure, quality of care, and standardized protocols may have resulted in a higher probability of dying from COVID-19 for patients treated in a public healthcare facility, than those treated in a private institution [5,38,39,40]. Considering this, it becomes necessary to have an understanding of the statistical behavior of the pandemic in public and private institutions separately, which would in turn present a complete overview of its interaction within two different healthcare environments, as well as the corresponding socioeconomic implications, such as inequalities in healthcare access and possible cultural disparities for marginalized groups, which continue to impact the evolution of the pandemic in Mexico.
In this study, the findings from a 2-year retrospective large cohort study from a private tertiary care center in Guadalajara, Mexico, are reported. This study aimed to describe and compare clinical characteristics, laboratory and radiological findings, and mortality among adult patients hospitalized with COVID-19.
2. Materials and Methods
2.1. Study Design
A retrospective cohort study was conducted at San Javier Hospital (SJH), a private tertiary care center located in Guadalajara, Jalisco, Mexico. Adult patients hospitalized with COVID-19 from April 4th, 2020, to March 3rd, 2022, confirmed by RT-PCR of nasopharyngeal swab with the Berlin protocol were included. The present study was conducted in accordance with the Declaration of Helsinki and was approved by the research ethics committee of the SJH with the register number 002-08-2022-MLZ. Due to the study’s observational and retrospective nature, no informed consent was required. Decisions regarding diagnostic approach, treatment, and follow-up were the responsibility of the attending physician, with consideration that during the pandemic different medical treatments were used based on the best scientific information available at each moment.
2.2. Data Collection
Epidemiological data were retrieved from the electronic medical record (TASY) of primary and secondary evaluations performed by first-contact physicians at the respiratory care unit. Additional clinical, outcome and laboratory information was obtained from the medical record reported by the assigned attending doctor. Initial laboratory tests were defined as the first results available, typically within 24 hours of hospital admission [8], including complete blood count, liver panel, basic metabolic panel, C-reactive protein (CRP), D-dimer, Troponin I, among others.
2.3. Definitions and Outcomes
The primary outcome was in-hospital mortality, without a set timeframe for it to occur. The cause of death was retrieved according to the data reported in the electronic medical record, as determined by the attending doctor.
Co-morbidities were defined as follows: chronic obstructive pulmonary disease (COPD) as a diagnosis of postbronchodilator FEV1/FVC ratio of <0.70 [41]; asthma as established by the Global Initiative for Asthma 2020 [42]; Chronic Kidney Disease (CKD) as a glomerular filtration rate below 60 mL/min for more than three months [43]; diabetes according to the guidelines of American Diabetes Association [44]; hypertension as systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg [45]; and immunosuppression as neutropenia (less than 500 neutrophils), with active malignant disease, asplenia, or under immunosuppressive treatment (prednisone >20mg/day or other immunosuppressive drugs for at least 30 days) [5,6].
Definitions for causes of death include: acute respiratory distress syndrome (ARDS) according to the Berlin definition [5,9] septic shock according to 2016 Third International Consensus Definition for Sepsis and Septic Shock [46]; and myocardial infarction following the guidelines of the Fourth Universal Definition of Myocardial Infarction [47].
2.4. Statistical Analysis
According to their distribution and type, variables are summarized as mean and standard deviation, or median with ranges and percentages (%), as appropriate. Characteristics at admission were compared between survivors at discharge versus non-survivors using a chi-squared test or Fisher’s exact test if qualitative, and a t-student test or ANOVA if quantitative with normal distribution. After the univariate analysis, mortality risk factors were analyzed by Cox regression analysis to determine explicative and predictive variables, considering a two-tailed p<0.05 as statistically significant. The statistical software used was SPSS 24.0 (SPSS Inc. Chicago, IL).
3. Results
In the study period, spanning from April 4th, 2020, to March 3rd, 2022, 1,377 patients were admitted under the diagnosis of confirmed SARS-CoV-2 pneumonia, 119 of which were excluded due to inter-hospital transfer or voluntary discharge against medical advice. The study population consisted of 1,258 patients, of whom 1,093 recovered (86.8%) and 165 died (13.1%). The mean length of stay was 12.2 ± 13.7 days, being significantly higher in those patients who died compared to survivors. In total, 243 (19.3%) of patients were admitted to the Intensive Care Unit (ICU), and 200 (15.9%) were mechanically ventilated (MV). A significant association was observed between the need for MV and ICU admission for in-hospital death. Among survivors, 86 (7.8%) received mechanical ventilation, and 107 (9.7%) were managed in the ICU. Figure 1 shows patient distribution regarding the number of hospital admissions, hospital discharges, ICU admissions, and in-hospital deaths during the study period. Similar to the observed in the general population, three waves of disease are denoted in the figure during the study period, reaching the peak of hospital admissions in December 2020, August 2021, and January 2022.
Demographical characteristics of patients at admission are shown in Table 1. The median age was 56.2 ± 16.5 years, being 68.3 ± 14.2 years for non-survivors and 54.4 ± 16.0 for survivors. Both groups had a predominance of male sex and a high frequency of comorbidities such as overweight and obesity, diabetes mellitus, and arterial hypertension. Hypertension, diabetes mellitus, COPD, immunosuppression, cancer, chronic kidney disease (CKD), and previous myocardial infarction were comorbidities significantly more observed in non-survivors. The use of angiotensin receptor blockers (ARB) or ACE inhibitors (ACEI) also showed differences between both groups. The presence of lung imaging findings (either by CT scan or chest X ray) compatible with COVID-19 was around 90% in both groups, showing no statistical difference.
Table 2 shows the results of clinical evaluation at admission. The mean time from symptom onset to hospitalization was 9.2 ± 5.2 days, showing a statistical difference in patients who died compared to survivors. Dyspnea, cough, malaise, and fever were the most frequently reported symptoms; dyspnea was the only symptom more frequent in non-survivors, while anosmia and odynophagia presented more frequently in those who survived. Median values of heart rate, respiratory rate, percent oxygen saturation, and presence of cyanosis were also more frequent in non-survivors, as well as a Glasgow Coma Scale <15.
Comparisons of laboratory findings on admission are shown in Table 3. Markers of acute inflammatory response, such as PCR, LDH, leukocytosis, absolute neutrophilic count, neutrophil/lymphocyte ratio, and D-dimer were remarkably altered in patients who died. Serum concentrations of urea, albumin, and ALT were also significantly higher in non-survivors than in survivors.
Causes of death in our cohort are summarized in Supplementary Table 1. The most common cause was multi-organic failure (42.4%), followed by ARDS (33.9%) and septic shock (10.9%). Other causes included unstable bradycardia, pulmonary embolism, myocardial infarction, and hypovolemic shock, which were much less common.
Finally, in the multivariate analysis (Table 4), variables that independently predicted mortality identified by cox regression analysis showed that older age (> 60yo), cyanosis and previous myocardial infarction significant predictors of mortality.
4. Discussion
To our knowledge, this is the first large cohort study of COVID-19 in-hospital mortality and associated risk factors of patients attended exclusively in a private hospital in Mexico, and one of the few in Latin America and LAC. In 2021, LAC was the region with the highest number of COVID-19 deaths and deaths per 1000 population, representing 28.8% of global reported deaths, while having only 8.4% of its population [48]. In our cohort, in-hospital overall mortality was 13.1%, which contrasts with the mortality reported by other hospitals in this country (22-53%) [5–7,9,10], as well as some of the cohorts in other LAC countries [12,25].
The significantly lower mortality rate found in our cohort can be explained by several factors, namely the fact that our hospital belongs to the private health subsystem, in contrast to other Mexican cohorts that belong to public health services [5–7,9,10]. Márquez-González et al. [11], Carrillo-Vega et al. [49], and Salinas-Escudero et al. [50] analyzed the national database to identify risk factors for hospitalization and death in the Mexican population, showing a lower patient survival rate among those hospitalized in public than those in private institutions. This problem is prevalent among health systems in most LAC countries which, while also varying between countries, all have in common the lack of universal public health regimes, relying instead heavily on private subsystems and, in most cases, considerable out-of-pocket expenses [32,51,52,53]. De Oliveira et al. [12], in their cohort study of a private healthcare network in Brazil, also reported a considerably lower mortality rate compared to other cohorts from the public subsystem in Brazil and other parts of the world. Besides age, which was also lower than the reported mean in other studies, they attributed the disparities between private and public hospitals as a possible factor involved in this difference. Mexican health system’s highly heterogeneous organization and quality of care have allowed discrepancies in healthcare to persist to date. The system of care is divided into four main subsystems (private health care providers, as well as Instituto Mexicano del Seguro Social (IMSS), Instituto de Seguridad y Servicios Sociales para los Trabajadores del Estado (ISSSTE), and Secretaría de Salud (SS) as public institutions), all of which remain fragmented and incapable of delivering universal care [32,33,34,38,54]. Public institutions represent the health services with the highest demand, as they are more affordable, which puts them at a higher risk of exceeding their capacity, causing health services saturation and increasing mortality [49].
Other factor to consider for the difference in mortality rate is that, while many Mexican cohorts analyzed the first months of the pandemic, our study spanned over a 2-year period. Thus, the evolution of the clinical knowledge about COVID-19, a lesser degree of bed-saturation and overcrowding of critical areas, and the effect of vaccines over the last months of our studied period most likely contributed to a decrease in in-hospital mortality.
The median age in our study was 56.2 ± 16.5, similar to other large cohorts in our country [5–7,9,10]. As previously established, age has been reported as one of the most important risk factors in most countries, being associated with a higher mortality, extended hospital and ICU times [11,13,55]. In our study, age was identified as a risk factor for mortality; non-survivors’ age, was, in average, 14 years older than survivors, which remained as an independent mortality risk factor after multivariate analysis. This may be explained by contributing factors such as age-related physiological changes, impaired immune function, and preexisting illnesses [25,27,55,56]. At this point in the pandemic, older age is well established as a strong predictor of severity and mortality in patients with COVID-19, which prompts early referral of older individuals for inpatient care [18,26,28,57]. Although it did not represent a risk factor for mortality, two-thirds of our inpatients were male, which is consistent with the findings of other studies [23,24].
Several comorbidities and preexisting conditions have been classified as risk factors for mortality in the current evidence, many of which present with a high prevalence in LAC, and specifically the Mexican population [5,9,55]. Hypertension is one of the comorbidities that has most commonly been associated with increased mortality in COVID-19 patients, though the exact mechanism remains unclear [6,9,17,18,55,57,58]. Its prevalence in our cohort was similar to the national (31%) and to that of other LAC countries [4,5,9], showing an increased risk of in-hospital death. The use of ACEI/ARBS represented a significant difference between both groups. Although mediated by a possible mechanism by which RAAS blockers may increase ACE2 expression, potentially increasing the risk of SARS-CoV-2 infection, the effect of ARB or ACEI use on disease severity is still controversial [6,9].
Diabetes, which had a prevalence higher than the national (13.7%) [5], was significantly associated with an increased risk of in-hospital death. As with hypertension, diabetes has also shown an association with COVID-19 severity and mortality [3,26,55,56,58], with many proposed mechanisms including reduced resistance to viral infections as a consequence of a sustained low level of immunity, as well as vascular and heart damage due to longstanding disease [56].
Overweight and obesity showed no difference between the two groups. Though it has been consistently associated with increased disease severity in COVID-19 patients in some studies, the association remains unclear, with mixed results among bibliography [9,12,25]. A meta-analysis conducted by Mesas et al. [58] showed that increased mortality was present only in studies with fewer chronic or critical patients, by which BMI served as a prominent prognostic factor in studies with these conditions, which was not the case in our study.
Different studies have documented other comorbidities, such as COPD [19,55,56,58,59], immunosuppression [3,19,56,59], cancer [17,55,56,58], chronic kidney disease [19,24,27,50,58], and previous myocardial infarction [3,27] as risks factors for mortality, all of which were significantly more frequent in the mortality group of our cohort.
The clinical characteristics at admission more prevalent in the non-survival group included signs and symptoms of respiratory distress such as dyspnea, increased respiratory rate, oxygen saturation, and the presence of cyanosis, consistent with previous findings of other studies [13,29,55,57,58]. Other symptoms, however, have been associated with a more favorable prognosis [9,13], which in our cohort were anosmia and odynophagia. qSOFA [1,5,9,16], MuLBSTA Score [1,5], Charlson Comorbidity Index [1,5,21], and National Early Warning Score [1,5], all of which have been reported as useful predictive scales in COVID-19 patients, predicted mortality in the univariate analysis of our cohort.
In our study, 19.3% of patients received care in the ICU and 15.9% were MV. ICU and MV mortality were 55.9% and 57%, respectively, similar to other Mexican [5,7–9] and global [12,27] cohorts. Both ICU admission and the need for MV were significantly more frequent in non-survivors, which has been commonly reported amongst many cohorts, highlighting the importance of ICU management and MV as predictors of death in patients hospitalized due to COVID-19 [9–12,27].
Laboratory findings that were more prevalent in the mortality group included changes in blood cell counts, such as increased leukocytes and neutrophils and an altered neutrophil-to-lymphocyte ratio, as well as markers of acute inflammatory response, including increased CRP, LDH, and increased D-Dimer. These have all been associated with an aggravated course of disease [9,14,16,24,25,55,56]. Other laboratory parameters altered in this group included urea, ALT, and albumin, which have also been reported in literature as valuable predictors [4,9,14,16,24,25,29,55,58,60].
In the multivariate analysis, older age, the presence of cyanosis and previous myocardial infarction were the main predictors for mortality, consistent with the findings amongst other cohorts. In one study, age was found to be a main determinant of COVID-19 related in-hospital mortality, independent of other pre-existing comorbidities [61]. In another study, done in the city where the present study was conducted, age, along with other factors, was also found to be a mortality predictor [9]. The presence of cyanosis was also an important predictor while, interestingly, oxygen saturation was not. In other studies, cyanosis has been recognized as a risk factor in univariate analyses; nonetheless, in our cohort, in both the univariate and multivariate analyses it was found to be strongly linked to in-hospital mortality [25]. Finally, the history of previous myocardial infarction was also an important predictor, consistent with previous studies that have associated the presence of CV disease, including myocardial infarction, with poorer outcomes [3,19,62]. Similar to the results of our cohort, one study also reported myocardial infarction as a predictor of mortality in the multivariate analysis [63].
Regarding the limitations of this study, its retrospective nature makes it prone to under documentation of many clinical variables, limiting the researchers’ capacity to obtain comprehensive data due to incomplete medical records. Social determinants of the study population, such as median household income, were not assessed. Due to the changing nature of the pandemic, along with the evolution of the understanding of the disease, clinical practice improvements were implemented, with the evaluation of such changes exceeding the scope of this study [12]. Finally, we excluded patients that did not have the entire course of disease in our institution, such as those discharged against medical advice or because of inter-hospital transfer, as we were therefore unable to assess their evolution. Despite these limitations, the size and duration of this study allowed us to provide with a reasonably complete overview of the pandemic as it presented in our hospital [64].
Our study gains relevance as the socioeconomic impact of COVID-19 continues to impact the population of our country, worsening socioeconomic inequality: while non-vulnerable groups are given the option of more reliable services and quality according to their economic situation, the more marginalized populations are left with no choice but attempting to receive care in saturated, underfunded, often uncoordinated public health subsystems [65]. These disparities further heighten inequalities especially affecting vulnerable groups, including indigenous communities, migrants, people in overcrowded living conditions, informal workers, people with disabilities, and older adults, even more so in the cases that also involve chronic diseases, which are also correlated to those same vulnerabilities [5,37,48,52,53,65,66]. While this is not limited to Mexico or LAC, as the syndemic relationship between social inequalities, chronic diseases, and COVID-19 has been reported at an international level [67], the conditions of the region regarding public and private subsystems, low public spending in healthcare, infrastructure, and other health-related policies all have had a considerably higher socioeconomic impact of the pandemic in LAC [32].
5. Conclusions
Mortality in hospitalized patients with COVID-19 in this private tertiary care center was 13.1%. Older age, the presence of cyanosis and a previous myocardial infarction were the most significant independent risk factors for mortality in our 2-year cohort. To our knowledge, this is the first study analyzing predictors of mortality in COVID-19 patients attended on a private tertiary hospital in Mexico. Considering the significant disparities in the quality of care that exist between the private and public health subsystems in Mexico, our results gain special significance, as they contribute to a more complete overview of the health care system and its interaction with the pandemic.
Supplementary Materials
Supplementary Table 1. Causes of death.
Author Contributions
Conceptualization, M.L.-Z., J.E.M.-C. and L.R.G.-L.; methodology, M.L.-Z. and C.A.L.-P.; validation, M.L.-Z.; formal analysis, C.A.L.-P.; investigation, C.A.L.-P., F.J.S.C.-P., R.B.M.-G., R.V.-G., X.F.-M., D.G.M.-S., J.A.G.-B., A.N.-M., M.F.-G., C.G.-R., E.D.V.-M.; data curation, C.A.L.-P., A.U.L.-P. and F.J.S.C.-P.; writing—original draft preparation, C.A.L.-P., A.U.L.-P. and F.J.S.C.-P. ; writing—review and editing, C.A.L.-P., A.U.L.-P. and F.J.S.C.-P.; visualization, C.A.L.-P. and F.J.S.C.-P.; supervision, C.A.L.-P., J.E.M.-C. and L.R.G.-L.; project administration, M.L.-Z.; funding acquisition, L.R.G.-L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The present study was conducted in accordance with the Declaration of Helsinki and was approved by the research ethics committee of the San Javier Hospital with the register number 002-08-2022-MLZ.
Informed Consent Statement
Due to the retrospective nature of the present study, patient consent was waived. No personal information about the patients involved nor any data that can be associated to a particular subject has been shown.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
The authors are deeply grateful to all healthcare workers and allied personnel for their resilience and relentless work during the COVID-19 pandemic.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Ortiz-Brizuela, E.; Villanueva-Reza, M.; González-Lara, M.F.; Tamez-Torres, K.M.; Román-Montes, C.M.; Díaz-Mejía, B.A.; Pérez-García, E.; Olivas-Martínez, A.; Rajme-López, S.; Martinez-Guerra, B.A.; et al. Clinical and Epidemiological Characteristics of Patients Diagnosed With Covid-19 in a Tertiary Care Center in Mexico City: A Prospective Cohort Study. Rev. Invest. Clin. 2020, 72, 165–177. [Google Scholar] [CrossRef]
- Martos Pérez, F.; Luque del Pino, J.; Jiménez García, N.; Mora Ruiz, E.; Asencio Méndez, C.; García Jiménez, J.M.; Navarro Romero, F.; Núñez Rodríguez, M.V. Comorbilidad y Factores Pronósticos Al Ingreso En Una Cohorte COVID-19 de Un Hospital General. Rev. Clínica Española 2021, 221, 529–535. [Google Scholar] [CrossRef] [PubMed]
- Tartof, S.Y.; Qian, L.; Hong, V.; Wei, R.; Nadjafi, R.F.; Fischer, H.; Li, Z.; Shaw, S.F.; Caparosa, S.L.; Nau, C.L.; et al. Obesity and Mortality among Patients Diagnosed with COVID-19: Results from an Integrated Health Care Organization. Ann. Intern. Med. 2020, 173, 773–781. [Google Scholar] [CrossRef] [PubMed]
- Mendizabal, M.; Pi, F.; Ridruejo, E.; Anders, M.; Silveyra, M.D.; Torre, A.; Montes, P.; Urzúa, A.; Pages, J.; Toro, L.G.; et al. Since January 2020 Elsevier Has Created a COVID-19 Resource Centre with Free Information in English and Mandarin on the Novel Coronavirus COVID- 19 . The COVID-19 Resource Centre Is Hosted on Elsevier Connect , the Company ’ s Public News and Information . 2020.
- Brill, S.E.; Jarvis, H.C.; Ozcan, E.; Burns, T.L.P.; Warraich, R.A.; Amani, L.J.; Jaffer, A.; Paget, S.; Sivaramakrishnan, A.; Creer, D.D. COVID-19: A Retrospective Cohort Study with Focus on the over-80s and Hospital-Onset Disease. BMC Med. 2020, 18, 1–9. [CrossRef]
- Álvarez-Arroyo, L.; Carrera-Hueso, F.J.; El-Qutob, D.; Robustillo-Villarino, M.; Girona-Sanz, A.M.; Pin-Godos, M.T.; Sánchez-Monzó, P.; Martínez-Gonzálbez, R.; Cepeda-Madrigal, S.; Martínez-Martínez, F. Estudio Descriptivo de Una Cohorte de Pacientes Con COVID-19 Hospitalizados En España. Gac. México 2021, 157, 80–87. [CrossRef]
- Marcela Vélez, C. COVID-19 and Vaccination in Latin America and the Caribbean: Challenges, Needs and Opportunities 2021, 1–88.
- The Covid-19 Pandemic in Latin America and the Caribbean. Popul. Dev. Rev. 2022, 48, 263–266. [CrossRef]
- Interventions, R. Revue Interventions Économiques Latin American Health Regimes in the Face of the Pandemic Revue Interventions Économiques Papers in Political Economy Latin American Health Regimes in the Face of the Pandemic Les Régimes de Santé Latino-Américains Face à L. 2022. [CrossRef]
- Estudios de La OCDE Sobre Los Sistemas de Salud: México 2016; 2016. ISBN 9789264230491.
- Narvaez, C.; Rivas, L.A.; Chavez, A. Modelos de Gestión de La Calidad En Instituciones Públicas de Salud En México. Rev. Innovaciones Negocios 2017, 12, 177–205. [Google Scholar] [CrossRef]
- Dong, E.; Du, H.; Gardner, L. An Interactive Web-Based Dashboard to Track COVID-19 in Real Time. Lancet Infect. Dis. 2020, 20, 533–534. [Google Scholar] [CrossRef]
- Ángeles Correa, M.G.; Villarreal Ríos, E.; Galicia Rodríguez, L.; Vargas Daza, E.R.; Frontana Vázquez, G.; Monrroy Amaro, S.J.; Ruiz Pinal, V.; Álvarez, J.D.; Beltrán, S.S. Enfermedades Crónicas Degenerativas Como Factor de Riesgo de Letalidad Por COVID-19 En México. Rev. Panam. Salud Pública 2022, 46, 1. [Google Scholar] [CrossRef]
- Campos-Nonato, I.; Hernández-Barrera, L.; Flores-Coria, A.; Gómez-Álvarez, E.; Barquera, S. Prevalence, Diagnosis and Control of Hypertension in Mexican Adults with Vulnerable Condition. Results of the Ensanut 100k. Salud Publica Mex. 2019, 61, 888–897. [Google Scholar] [CrossRef]
- García-Peña, C.; Bello-Chavolla, O.Y.; Castrejón-Pérez, R.C.; Jácome-Maldonado, L.D.; Lozano-Juárez, L.R. Variability in Case Fatality Rate Risk Due to Covid-19 According to Health Services Provider in Mexico City Hospitals. Salud Publica Mex. 2022, 64, 119–130. [Google Scholar] [CrossRef] [PubMed]
- Colchero, M.A.; Gómez, R.; Pineda-Antúnez, C.J.; Bautista-Arredondo, S. Health Care Utilization during the Covid-19 Pandemic in Mexico: The Cascade of Care. Salud Publica Mex. 2021, 63, 743–750. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Martínez, O.A.; Rodríguez-Brito, A. Vulnerability in Health and Social Capital: A Qualitative Analysis by Levels of Marginalization in Mexico. Int. J. Equity Health 2020, 19, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Halpin, D.M.G.; Criner, G.J.; Papi, A.; Singh, D.; Anzueto, A.; Martinez, F.J.; Agusti, A.A.; Vogelmeier, C.F. Global Initiative for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease. The 2020 GOLD Science Committee Report on COVID-19 and Chronic Obstructive Pulmonary Disease. Am. J. Respir. Crit. Care Med. 2021, 203, 24–36. [Google Scholar] [CrossRef] [PubMed]
- Reddel, H.K.; Bacharier, L.B.; Bateman, E.D.; Brightling, C.E.; Brusselle, G.G.; Buhl, R.; Cruz, A.A.; Duijts, L.; Drazen, J.M.; FitzGerald, J.M.; et al. Global Initiative for Asthma Strategy 2021: Executive Summary and Rationale for Key Changes. Eur. Respir. J. 2022, 59. [Google Scholar] [CrossRef]
- Levey, A.S.; Coresh, J. Chronic Kidney Disease. Lancet (London, England) 2012, 379, 165–180. [Google Scholar] [CrossRef]
- Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2020. Diabetes Care 2020, 43, S14–S31. [CrossRef]
- Unger, T.; Borghi, C.; Charchar, F.; Khan, N.A.; Poulter, N.R.; Prabhakaran, D.; Ramirez, A.; Schlaich, M.; Stergiou, G.S.; Tomaszewski, M.; et al. 2020 International Society of Hypertension Global Hypertension Practice Guidelines. Hypertens. (Dallas, Tex. 1979) 2020, 75, 1334–1357. [Google Scholar] [CrossRef]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D. Fourth Universal Definition of Myocardial Infarction (2018). J. Am. Coll. Cardiol. 2018, 72, 2231–2264. [Google Scholar] [CrossRef]
- ECLAC Social Panorama of Latin America 2021; 2007. ISBN 9789211218244.
- Carrillo-Vega, M.F.; Salinas-Escudero, G.; García-Peña, C.; Gutiérrez-Robledo, L.M.; Parra-Rodríguez, L. Early Estimation of the Risk Factors for Hospitalization and Mortality by COVID-19 in Mexico. PLoS One 2020, 15, 1–11. [Google Scholar] [CrossRef]
- Salinas-Escudero, G.; Carrillo-Vega, M.F.; Granados-García, V.; Martínez-Valverde, S.; Toledano-Toledano, F.; Garduño-Espinosa, J. A Survival Analysis of COVID-19 in the Mexican Population. BMC Public Health 2020, 20, 1–8. [Google Scholar] [CrossRef]
- ECLAC-PAHO Health and the Economy: A Convergence Needed to Address COVID-19 and Retake the Path of Sustainable Development in Latin America and the Caribbean. 2020.
- NU. CEPAL The Recovery Paradox in Latin America and the Caribbean Growth amid Persisting Structural Problems: Inequality, Poverty and Low Investment and Productivity. 2021, 40.
- ECLAC-PAHO COVID-19 Report: The Prolongation of the Health Crisis and Its Impact on Health, the Economy and Social Development. 2020, 37.
- Puig, A.; Pagán, J.A.; Wong, R. Assessing Quality across Healthcare Subsystems in Mexico. J. Ambul. Care Manage. 2009, 32, 123–131. [Google Scholar] [CrossRef]
- Shi, C.; Wang, L.; Ye, J.; Gu, Z.; Wang, S.; Xia, J.; Xie, Y.; Li, Q.; Xu, R.; Lin, N. Predictors of Mortality in Patients with Coronavirus Disease 2019: A Systematic Review and Meta-Analysis. BMC Infect. Dis. 2021, 21, 1–15. [Google Scholar] [CrossRef]
- Zhang, J.J.; Dong, X.; Liu, G.H.; Gao, Y.D. Risk and Protective Factors for COVID-19 Morbidity, Severity, and Mortality. Clin. Rev. Allergy Immunol. 2022. [Google Scholar] [CrossRef]
- Leidman, E.; Doocy, S.; Heymsfield, G.; Sebushishe, A.; Mbong, E.N.; Majer, J.; Bollemeijer, I. Risk Factors for Hospitalisation and Death from COVID-19: A Prospective Cohort Study in South Sudan and Eastern Democratic Republic of the Congo. BMJ Open 2022, 12, e060639. [Google Scholar] [CrossRef]
- Mesas, A.E.; Andrade, S.M. De; Sequı, I. Predictors of In-Hospital COVID-19 Mortality : A Comprehensive Systematic Review and Meta- Analysis Exploring Differences by Age , Sex and Health Conditions. 2020, 6, 1–23. [CrossRef]
- Toledo-tapia, R.; Mayoral-ortiz, A.; Tlecuitl-mendoza, N.; Toledo-tapia, M.; Ortega-aguirre, M.; Amaro-balderas, E. Influencia de Factores de Riesgo Sobre Mortalidad Por COVID-19. 2022, 60.
- Yu, H.; Wang, T.; Chen, Z. Blood Urea Nitrogen to Serum Albumin Ratio (BAR) Predicts Critical Illness in Patients with Coronavirus Disease 2019 (COVID-19). 2021.
- Henkens, M.T.H.M.; Raafs, A.G.; Verdonschot, J.A.J.; Linschoten, M.; van Smeden, M.; Wang, P.; van der Hooft, B.H.M.; Tieleman, R.; Janssen, M.L.F.; ter Bekke, R.M.A.; et al. Age Is the Main Determinant of COVID-19 Related in-Hospital Mortality with Minimal Impact of Pre-Existing Comorbidities, a Retrospective Cohort Study. BMC Geriatr. 2022, 22, 1–11. [Google Scholar] [CrossRef]
- Cordero, A.; Santos García-Gallego, C.; Bertomeu-González, V.; Fácila, L.; Rodríguez-Mañero, M.; Escribano, D.; Castellano, J.M.; Zuazola, P.; Núñez, J.; Badimón, J.J.; et al. Mortality Associated with Cardiovascular Disease in Patients with COVID-19. REC CardioClinics 2021, 56, 30–38. [Google Scholar] [CrossRef]
- Ranucci, M.; Parati, G.; Di Dedda, U.; Bussotti, M.; Agricola, E.; Menicanti, L.; Bombace, S.; De Martino, F.; Giovinazzo, S.; Zambon, A.; et al. When Outcomes Diverge: Age and Cardiovascular Risk as Determinants of Mortality and ICU Admission in COVID-19. J. Clin. Med. 2022, 11. [Google Scholar] [CrossRef]
- Rosso, F.; Tafurt, E.; Valle, F.; Icesi, U.; Cauca, V.; Valle, F.; Cauca, V. Downloaded from Https://Academic.Oup.Com/Ofid/Article/8/Supplement_1/S274/6450193 by Guest on 01 September 2022. 2021, 8, 2021.
- Ortiz-Hernández, L.; Pérez-Sastré, M.A. Social Inequalities in the Progression of COVID-19 in the Mexican Population. Rev. Panam. Salud Publica/Pan Am. J. Public Heal. 2020, 44, 1–8. [Google Scholar] [CrossRef]
- Marcela Vélez, C. COVID-19 and Vaccination in Latin America and the Caribbean: Challenges, Needs and Opportunities 2021, 1–88.
- Islam, N.; Lacey, B.; Shabnam, S.; Erzurumluoglu, A.M.; Dambha-Miller, H.; Chowell, G.; Kawachi, I.; Marmot, M. Social Inequality and the Syndemic of Chronic Disease and COVID-19: County-Level Analysis in the USA. J. Epidemiol. Community Health 2021, 75, 496–500. [Google Scholar] [CrossRef]
Figure 1.
Number of hospital discharges, in-hospital deaths, hospital admissions and ICU admissions from April 4th, 2020, to March 3rd, 2022.
Figure 1.
Number of hospital discharges, in-hospital deaths, hospital admissions and ICU admissions from April 4th, 2020, to March 3rd, 2022.
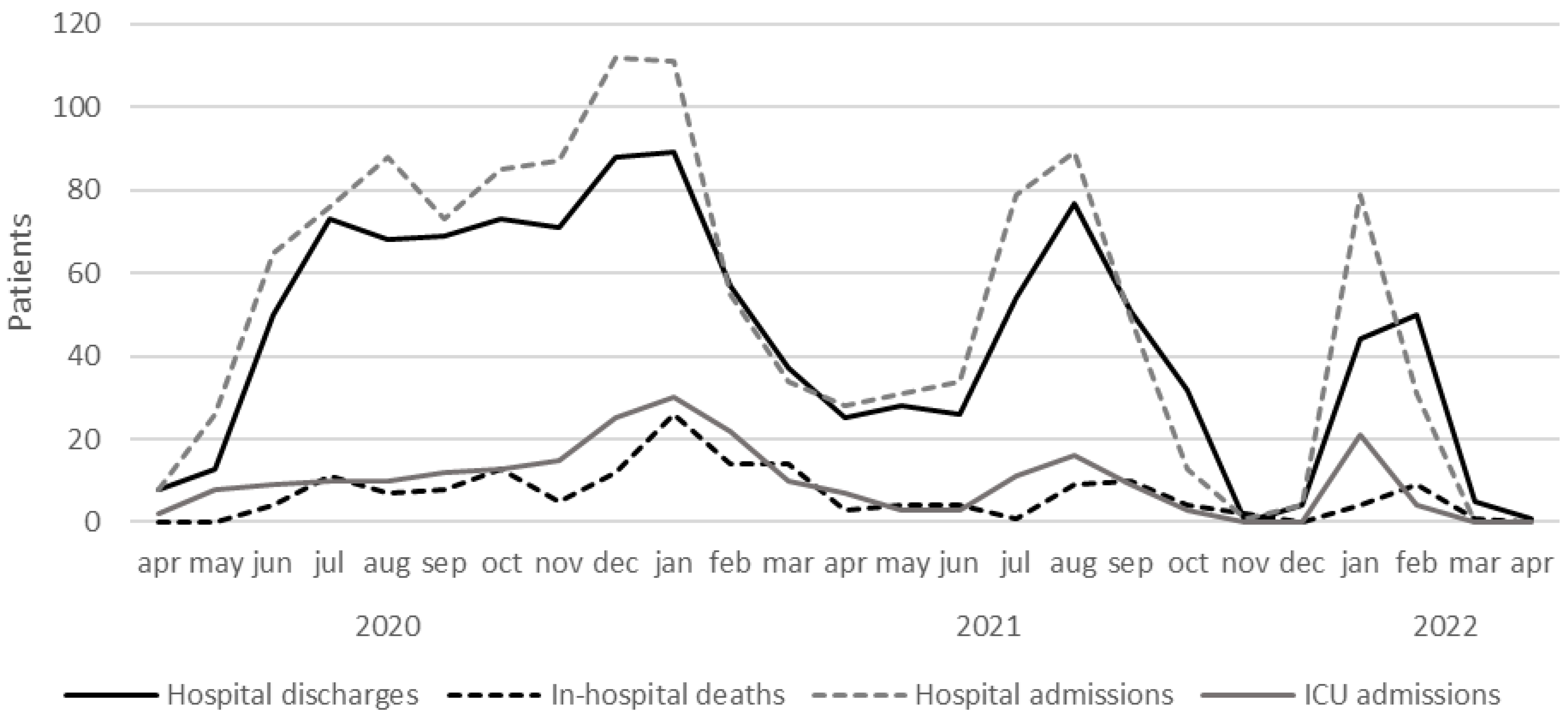

Table 1.
Comparisons of demographic and clinical characteristics of survivors and non-survivors at admission.
Table 1.
Comparisons of demographic and clinical characteristics of survivors and non-survivors at admission.
| Variable | Total n (%) |
Survivor n (%) |
Non-survivor n (%) |
P Value |
|---|---|---|---|---|
| Sex (Male/Female), n | 845/413 | 741/352 | 104/61 | 0.248 |
| ± S.D.) years | 56.2 ± 16.5 | 54.4 ± 16.0 | 68.3 ± 14.2 | <0.001 |
| BMI classification, % | ||||
| Underweight | 10 (0.8%) | 9 (0.8%) | 1 (0.6%) | |
| Normal BMI | 240 (19.1%) | 199 (18.4%) | 41 (24.8%) | |
| Overweight | 486 (38.6%) | 423 (38.3%) | 63 (38.2%) | 0.399 |
| Obesity grade I | 322 (25.6%) | 285 (26.1%) | 37 (22.4%) | |
| Obesity grade II | 114 (9.1%) | 103 (9.3%) | 11 (6.7%) | |
| Obesity grade III | 86 (6.8%) | 74 (7.0%) | 12 (7.3%) | |
| Hypertension (%) | 427 (33.9%) | 346 (31.7%) | 81 (49.1%) | <0.001 |
| Diabetes (%) | 270 (21.5%) | 216 (19.8%) | 54 (32.7%) | <0.001 |
| COPD (%) | 34 (2.7%) | 22 (2.0%) | 12 (7.3%) | 0.001 |
| Asma (%) | 27 (2.1%) | 25 (2.3%) | 2 (1.2%) | 0.422 |
| Immunosuppression (%) | 56 (4.5%) | 42 (3.8%) | 14 (8.5%) | 0.010 |
| Cancer (%) | 60 (4.8%) | 42 (3.8%) | 18 (10.9%) | <0.001 |
| HIV (%) | 2 (0.2%) | 2 (0.2%) | 0 (0%) | >0.999 |
| Previous stroke (%) | 16 (1.3%) | 11 (1.0%) | 5 (3.0%) | >0.999 |
| CKD (%) | 49 (3.9%) | 39 (3.6%) | 10 (6.1%) | 0.021 |
| Organ transplant recipient (%) | 16 (1.3%) | 14 (1.3%) | 2 (1.2%) | >0.999 |
| Chronic liver disease (%) | 9 (0.7%) | 8 (0.7%) | 1 (0.6%) | >0.999 |
| ACEI/ARA (%) | 283 (22.5%) | 234 (21.4%) | 49 (29.7%) | 0.021 |
| Previous myocardial infarction (%) | 35 (2.8%) | 23 (2.1%) | 12 (7.3%) | 0.001 |
| Depression (%) | 17 (1.4%) | 15 (1.4%) | 2 (1.2%) | 0.830 |
| Smoker (%) | ||||
| Never | 808 (64.2%) | 715 (65.4%) | 93 (56.4%) | |
| Unknown | 301 (23.9%) | 257 (23.5%) | 44 (26.7%) | 0.071 |
| Currently | 65 (5.2%) | 54 (4.9%) | 11 (6.7%) | |
| Former | 84 (6.7%) | 67 (6.1%) | 17 (10.3%) | |
| Alcohol use (%) | ||||
| Never | 805 (64.0%) | 700 (64.0%) | 105 (63.6%) | |
| Unknown | 330 (26.2%) | 279 (25.5%) | 51 (30.9%) | 0.114 |
| Currently | 109 (8.7%) | 102 (9.3%) | 7 (4.2%) | |
| Former | 14 (1.1%) | 12 (1.1%) | 2 (1.2%) | |
| COVID-19 pneumonia on imaging (%) | 1,133 (90.1%) | 981 (90.2) | 152 (92.1) | 0.480 |
| NIH severity scale (%) | ||||
| Critical | 64 (5.1%) | 26 (2.4%) | 38 (23.0%) | |
| Moderate | 90 (7.2%) | 85 (7.8%) | 5 (3.0%) | <0.001 |
| Severe | 1,104 (87.8%) | 982 (89.8%) | 122 (73.9%) | |
| ± S.D.) | 6.3 ± 3.3 | 6.0 ± 3.2 | 8.3 ± 3.6 | <0.001 |
| ± S.D.) | 2.1 ± 2.9 | 1.8 ± 3.0 | 3.5 ± 2.1 | <0.001 |
| qSOFA (%) n | ||||
| 0 | 354 (28.1%) | 329 (30.1%) | 25 (15.2%) | |
| 1 | 816 (64.9%) | 714 (65.3%) | 102 (61.8%) | <0.001 |
| 2 | 71 (5.6%) | 47 (4.3%) | 24 (14.5%) | |
| 3 | 17 (1.4%) | 3 (0.3%) | 14 (8.5%) | |
| ± S.D.) | 6.3 ± 2.5 | 6.1 ± 2.2 | 7.9 ± 3.1 | <0.001 |
Table 2.
Comparisons of signs and symptoms between non-survivors and survivors at admission.
| Variable | Total n (%) |
Survivor n (%) |
Non-survivor n (%) |
P value |
|---|---|---|---|---|
| Days onset symptom-admission (x ̅ ± S.D.) | 9.2 ± 5.2 | 9.1 ± 5.1 | 10.1 ± 6.1 | 0.027 |
| Length of stay, days (x ̅ ± S.D.) | 12.2 ± 13.7 | 10.6 ± 10.4 | 22.9 ± 24.5 | <0.001 |
| Heart rate (x ̅ ± S.D.) | 89.0 ± 19.2 | 88.6 ± 18.1 | 91.8 ± 24.9 | 0.043 |
| Respiratory rate (x ̅ ± S.D.) | 25.4 ± 7.3 | 25.2 ± 7.0 | 27.5 ± 8.7 | <0.001 |
| ± S.D.) | 82.1 ± 11.6 | 83.4 ± 10.2 | 74.0 ± 15.9 | <0.001 |
| Fever (%) n | 60.1% | 60.2% | 59.4% | 0.865 |
| AVPU score | ||||
| Alert | 1,196 (95.1%) | 1,066 (97.5%) | 130 (78.8%) | |
| Voice | 30 (2.4%) | 17 (1.6%) | 13 (7.9%) | <0.001 |
| Pain | 7 (0.6%) | 1 (0.1%) | 6 (3.6%) | |
| Unresponsive | 25 (2.0%) | 9 (0.8%) | 16 (9.7%) | |
| Cough (%) | 838 (66.6%) | 726 (66.4%) | 112 (67.9%) | 0.724 |
| Headache (%) | 538 (42.8%) | 478 (43.7%) | 60 (36.4%) | 0.077 |
| Dyspnea (%) | 1,041 (82.8%) | 892 (81.6%) | 149 (90.3%) | 0.008 |
| Diarrhea (%) | 252 (20.0%) | 224 (20.5%) | 28 (17.0%) | 0.300 |
| Chest pain (%) | 224 (17.8%) | 193 (17.7%) | 31 (18.8%) | 0.743 |
| Chills (%) | 309 (24.6%) | 275 (25.7%) | 34 (16.4%) | 0.210 |
| Odynophagia (%) | 308 (24.5%) | 281 (37.4) | 27 (29.7%) | 0.011 |
| Myalgias (%) | 458 (36.4%) | 409 (37.4%) | 49 (29.7%) | 0.057 |
| Arthralgias (%) | 406 (32.3%) | 357 (32.7%) | 49 (29.7%) | 0.476 |
| Malaise (%) | 880 (70.0%) | 769 (70.4%) | 111 (67.3%) | 0.466 |
| Rhinorrhea (%) | 151 (12.0%) | 135 (12.4%) | 16 (9.7%) | 0.370 |
| Vomiting (%) | 93 (7.4%) | 83 (7.6%) | 10 (6.1%) | 0.529 |
| Abdominal pain (%) | 77 (6.1%) | 64 (5.9%) | 13 (7.9%) | 0.382 |
| Conjunctivitis (%) | 22 (1.7%) | 20 (1.8%) | 2 (1.2%) | 0.757 |
| Cyanosis (%) | 101 (8.0%) | 71 (6.5%) | 30 (18.2%) | <0.001 |
| Anosmia (%) | 145 (11.5%) | 135 (12.4%) | 10 (6.1%) | 0.018 |
| Dysgeusia (%) | 129 (10.3%) | 118 (10.8%) | 11 (6.7%) | 0.129 |
| Glasgow Coma Scale <15 (%) | 77 (6.1%) | 43 (3.9%) | 34 (20.6) | <0.001 |
Table 3.
Comparisons of laboratory findings between non-survivors and survivors at admission.
| Variable | Total | Survivor | Non-survivor | P value |
|---|---|---|---|---|
| ± S.D.) | 44.1 ± 30.1 | 41.8 ± 26.8 | 59.3 ± 43.4 | <0.001 |
| ± S.D.) | 1.0 ± 1.1 | 1.0 ± 1.2 | 1.1 ± 0.8 | 0.489 |
| ± S.D.) | 0.7 ± 0.6 | 0.8 ± 0.6 | 0.8 ± 0.4 | 0.757 |
| ± S.D.) | 60.8 ± 57.8 | 60.0 ± 53.6 | 66.8 ± 82.3 | 0.242 |
| ± S.D.) | 60.9 ± 67.4 | 62.6 ± 69.9 | 48.2 ± 43.2 | 0.033 |
| ± S.D.) | 102.1 ± 61.4 | 101.4 ± 59.8 | 107.2 ± 72.2 | 0.349 |
| ± S.D.) | 3.6 ± 0.5 | 3.7 ± 0.5 | 3.3 ± 0.5 | <0.001 |
| ± S.D.) | 132.2 ± 101.3 | 128.4 ± 99.5 | 158.9 ± 110.1 | 0.001 |
| ± S.D.) | 9.9 ± 6.8 | 9.6 ± 6.8 | 12.0 ± 6.5 | <0.001 |
| ± S.D.) | 14.4 ± 2.2 | 14.5 ± 2.2 | 13.7 ± 2.4 | <0.001 |
| ± S.D.) | 431.8 ± 5674.5 | 456.7 ± 6092.0 | 269.0 ± 176.9 | 0.700 |
| ± S.D.) | 1285.1 ± 1089.6 | 1260.6 ± 905.3 | 1447.6 ± 1903.7 | 0.234 |
| ± S.D.) | 7173.3 ± 3960.6 | 6978.7± 3832.7 | 8535.34 ± 547.3 | <0.001 |
| ± S.D.) | 7.3 ± 6.3 | 6.8 ± 5.2 | 10.7 ± 10.4 | <0.001 |
| ± S.D.) | 1109.3 ± 2194.0 | 933.8 ± 1947.3 | 2342.0 ± 3214.6 | <0.001 |
| ± S.D.) | 213.0 ± 658.6 | 219.0 ± 699.8 | 179.5 ± 354.5 | 0.718 |
| ± S.D.) | 387.9 ± 212.2 | 371.6 ± 183.0 | 501.1 ± 334.0 | <0.001 |
| ± S.D.) | 422.5 ± 170.6 | 414.0 ± 162.2 | 490.5 ± 299.1 | 0.566 |
| ± S.D.) | 0.18 ± 3.4 | 0.0 ± 0.1 | 1.1 ± 9.0 | 0.291 |
| ± S.D.) | 7.4 ± 0.1 | 7.4 ± 0.1 | 7.4 ± 0.1 | 0.064 |
| ± S.D.) | 80.4 ± 40.1 | 79.0 ± 39.6 | 82.9 ± 41.2 | 0.555 |
| ± S.D.) | 42.4 ± 18.2 | 38.2 ± 12.7 | 49.9 ± 23.4 | 0.001 |
| ± S.D.) | 567.3 ± 5005.8 | 445.0 ± 4448.9 | 784.0 ± 5902.1 | 0.684 |
Table 4.
Results of the multivariate Cox’s regression analysis to predict mortality in patients with COVID-19.
Table 4.
Results of the multivariate Cox’s regression analysis to predict mortality in patients with COVID-19.
| Variable | Exp (B) | 95% CI | P Value |
|---|---|---|---|
| >60 years | 2.445 | 1.679-3.561 | <0.001 |
| Cyanosis | 1.825 | 1.195 to 2.787 | 0.005 |
| Previous myocardial infarction | 1.930 | 1.058 to 3.520 | 0.032 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



