
Submitted:
24 January 2023
Posted:
25 January 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
More than 600 Healthcare workers died due to COVID-19 infection until January 2022 in Ecuador. Even though the COVID-19 vaccines are safe, local, and systemic reactions were reported among physicians. This study aims to analyze the Adverse events (AEs) of COVID-19 vaccines with an emphasis on homologous and heterologous booster doses. An electronic survey was performed in Quito- Ecuador, directed to physicians who were vaccinated with the three doses of COVID-19 vaccines. 210 participants were analyzed after administering any doses of the vaccines. At least one AE was identified in 60.0% (126/210) of the sample after the first dose, 52.40% (110/210) after the second dose, and 75.2% (158/210) after the booster dose. The most frequent AEs were localized pain, myalgia, headache, and fever. At least one drug was used in 44.3% of the population after the first dose, 37.1% after the second dose, and 63.8% in the booster dose. Heterol-ogous booster produces more AEs compared with homologous booster (80.1% vs. 53.8%), and 77.3% of participants reported that interfered with daily activities. Similar studies agree that reactogenicity occurs mainly with heterologous vaccination compared to ho-mologous vaccination. This situation affected physicians’ performance in daily activities and led them to use medication for the symptoms
Keywords:
COVID-19 Vaccines
; BNT162 Vaccine
; ChAdOx1 nCoV-19
; Side Effects and Adverse Reactions
; Booster Immunizations
; COVID-19
; SARS-CoV-2
1. Introduction
The COVID-19 pandemic has produced 568,773,510 cases and 6,381,643 deaths worldwide (1). Healthcare workers (HCWs) are defined as paid or unpaid persons engaged in actions whose primary intent is to enhance health (2). Among the first line HCWs, physicians are one of the most affected groups by COVID-19 infections and the one with the highest mortality (3), for instance, more than 600 physicians died due to COVID-19 infection until January 2022 in Ecuador (4). For this reason, the World Health Organization (WHO) established that physicians were a priority in the administration of vaccines including the booster dose (5).
In Ecuador, 946,487 people were diagnosed with COVID-19(1), the most affected province is Pichincha (6), and Quito, the capital of Ecuador, is the city with the highest number of confirmed cases (7).
A booster dose is the response of the Public Health Systems to the emergence of new SARS-CoV-2 variants (8) and the decay of neutralizing antibodies in people fully vaccinated after 3-6 months (9,10). The National Vaccination Campaign achieved full vaccination of 83.84% of the population and 39.98% got a booster dose(11). The Ministry of Health (MoH) managed the administration of four COVID-19 vaccines: the mRNA Pfizer/BioNTech-Comirnaty, the non-replicating viral vector Oxford/AstraZeneca-Vaxzevria, and CanSino-Convidencia, and the inactivated virus vaccine Sinovac-CoronaVac.
The 56.39% of the total booster doses were primarily administered with Oxford/AstraZeneca-Vaxzevria, 34.78% with Pfizer/BioNTech-Comirnaty, 2.09% with CanSino-Convidencia, and 6.72% with Sinovac-CoronaVac(11).
Even though the COVID-19 vaccines are safe(12), few local and systemic reactions were reported after the first and second doses of vaccination(13) and after the application of a heterologous booster dose among HCWs(14). Regarding the homologous versus heterologous booster, the latter demonstrated a slightly higher rate of adverse events in HCW(15).
This study aims to analyze the adverse events of COVID-19 with an emphasis on homologous and heterologous booster doses in physicians that received three approved vaccines in Ecuador.
2. Materials and Methods
This article was written following the STROBE initiative for the reporting of observational studies (16).
Study Design and Ethical conditions: The present cross-sectional study was approved by the Independent Ethics Committee SOLCA-NUCLEO QUITO with the number OBS.21.202 and during its development, all the norms of Good Clinical Practice and Helsinki principles (17) were compiled to maintain the participant's safety and assure the quality of data obtained.
2.1. Settings, data source, and participants
An open and anonymous electronic survey (27 questions and 6 different screens) was performed in the city of Quito-Ecuador directed to the medical volunteer participants who were vaccinated with the 3 doses of the following vaccines against COVID-19: Oxford/AstraZeneca-Vaxzevria, Pfizer/BioNTech-Comirnaty or Sinovac-CoronaVac (greater than 7 days from the third dose). The instrument was published on different online media and social networks using platforms followed by physicians to delimit the sample; obtaining data from February 15 to April 01 of 2022 through the Google formulary application after individual authorization through the acceptance of electronic Informed Consent. To deal with the risk of duplicated responses, the email address was requested and if duplicated files were identified then the oldest one was eliminated.
2.2. Measurement of variables
Outcome measures: The results were obtained through the different responses to the questions asked during the development of the survey, keeping as dependent variables the development of any adverse event, the use of 1 or more medications, and the affectation of daily activities 7 days after any dose of vaccination against COVID-19.
The outcome adverse event was evaluated through the closed question "Did you present any subsequent adverse event in the 7 days following the administration of the COVID-19 vaccine?", in each dose administered (3 doses) dichotomizing the answer in Yes/No; in case of an affirmative answer, the type of adverse event was requested through the following non-exclusive question "If yes. Which of the following adverse events occurred during the first 7 days post-vaccination?", awaiting confirmation or denial of the following adverse events: localized pain, localized edema, localized erythema, localized pruritus, thermal elevation, diarrhea, nausea, vomiting, myalgia, arthralgia, headache and the development of other types of adverse events (obtained from the U.S Food and Drug Administration (FDA)(18)).
The use of medication was requested through the closed question "Was any medication administered for these side effects?", at each dose placed obtaining Yes/No answers; in case of an affirmative answer, it was requested to describe which medications were used through the use of the excluding question: Paracetamol, Ibuprofen, Diclofenac, Etoricoxib, and other medications. This qualitative variable was subclassified as the number of drugs used during the 7 days following each dose of the COVID-19 vaccine (None, 1 drug, 2 drugs, 3 or more drugs).
The affectation of daily activities during the 7 days after the administration of each dose of the COVID-19 vaccine was classified as an ordinal qualitative variable and assessed through a Likert-type scale with 4 options requested through the following question "Indicate the relationship between your daily activities and the adverse events present on a scale of 1 to 4", obtaining, as a result, the options: 1) Does not interfere with your daily activities and no treatment is administered; 2) Interferes with daily activities and/or required pharmacological treatment; 3) Impedes the performance of daily activities and required treatment; 4) Was hospitalized.
Individual measures: Participants were asked for sociodemographic information related to their date of birth (for age calculation), sex (male, female), and place of work; this last variable was classified as public, private, or no work. Dates of vaccination and the name of the vaccine applied were also required for each dose; these variables were classified according to the number of doses (first dose, second dose, third dose) and administered vaccine (Oxford/AstraZeneca-Vaxzevria, Pfizer/BioNTech-Comirnaty or Sinovac-CoronaVac). The third dose was subclassified concerning the type of vaccine into homologous (defined as administration of the same vaccine in all three doses) and heterologous (placement of a different vaccine in any dose).
2.3. Biases
As the study requires retrospective data, the risk of memory bias is latent, and it was managed by placing the download link of the vaccination certificate of the MoH of Ecuador and the request based on mixed questions that counted as options for different adverse events that help to remember the events that occurred.
2.4. Statistical analysis
To calculate the sample size, the finite universe formula was used with a sampling error of 5%, a confidence interval of 95%, and an expected proportion of 82.1% for a population of 11,730 physicians of Quito-Ecuador, with a loss of 10%, a sample of 250 participants was obtained. In this project using a non-probabilistic sampling studies snowball.
In case of missing data, the mean of each variable was placed to avoid loss of information. The descriptive analysis for qualitative variables was expressed with frequency tables; for qualitative variables, summary measures such as mean, median, standard deviation, and interquartile range were used and presented according to the type of distribution of each variable. For the bivariate analysis, measures of association were applied with a parametric test (chi2 and Student's t-tests) and nonparametric test (Mann Whitney U), and risk measures (Odds Ratio) with their respective 95% confidence intervals, using the presence or absence of adverse events as the dependent variable. Statistical analysis was performed with the Statistical Package for the Social Sciences version 26 program® (SPSS; IBM Corp., Armonk, NY).
3. Results
225 participants gave their consent to participate in the study, obtaining a recruitment and completion rate of 100%; 15 research subjects were excluded, 13 for being non-medical professionals, and 2 for receiving another type of vaccine. A total of 210 participants were analyzed with 630 vaccines administered divided into 3 doses (Figure 1). The 65.7% (138/210) are women; the participants present average age of 32 years (RIQ: 11.25) and for the 630 doses administered, 47.3% were Pfizer/BioNTech-Comirnaty, the 39.0% Oxford/AstraZeneca-Vaxzevria and the 13.7% Sinovac-CoronaVac). Table 1 describes the characteristics of the participants; no missing data were identified during the analysis.
3.1. Doses administered
It has been identified that 62.5% (394/630) of the doses administered presented at least one adverse event during the 7 days after the administration of any dose of the vaccine, with a frequency of 60.0% (126/210) after the first dose, 52.40% (110/210) and in the second dose 75.2% (158/210) after the third dose. The most frequent adverse event reported was localized pain in 49.5% (312/630) followed by myalgia in 28.3% (178/630), headache in 24.9% (157/630), and thermal elevation with a frequency of 21.6% (136/630). Concerning the use of medications, 48.4% (305/630) of the participants reported having used at least one medication for the management of adverse events, 44.3% (93/210) after the first dose, 37.1% (78/210) after the second dose and 63.8% (134/210) in the third dose applied; of the participants who reported at least one adverse event, the 44.7% (176/391) reported that their daily activities were affected and/or required pharmacological treatment. The characteristics of each dose are described in Table 2.
3.2. Vaccine administered
About the vaccine administered it becomes evident that 74.8% (184/246) of the participants that were given Oxford/AstraZeneca-Vaxzevria presented adverse events, with a mean of 3.4 (SD=2.0) adverse events. In the group of participants administered with Pfizer/BioNTech-Comirnaty, a frequency of 59.1% (176/298) with a mean of 2.4 (SD=1.6) adverse events were identified, and in the Sinovac-CoronaVac group, 39.5% (34/86) presented at least one adverse event with a mean of 1.8 (SD=1.2) (Figure 2). Concerning the use of medication, 63.0% (155/246) of the Oxford/AstraZeneca-Vaxzevria group reported using a medication, compared to 42.3% (126/298) of the Pfizer/BioNTech-Comirnaty group and 27.9% (24/86) of the participants inoculated with Sinovac-CoronaVac. The characteristics of adverse events, the use of medication, and the relationship with daily activities are described in Table 3. In Appendix A Table A1 descriptive characteristics of adverse events with the doses and the vaccine.
3.3. Group vaccine
In the group of participants with heterologous reinforcement, it is evident that 80.1% (137/171) presented at least 1 adverse event, compared to 53.8% (21/39) of the homologous group; they also report that 70.2% (120/171) report the use of medication for the control of adverse events in the heterologous group compared to 35.9% (14/39) of the homologous group. The characteristics of adverse events, medication use, and their relationship with daily activities are described in Table 4.
3.4. Factors related to the occurrence of adverse events.
In the bivariate analysis, it was identified that 62.5% (394/630) of the participants developed some adverse event, where being female (OR: 1.76 (1.25 -2.46)), receiving the third dose (OR: 2.36 (1.64-3. 42)), the Oxford/AstraZeneca vaccine (OR: 2.45 (1.79-3.49)) and a heterologous vaccine (OR: 3.63 (2.31-5.69)) increased the probability of presenting an adverse event, Table 5 describes these results.
4. Discussion
During the first year of the pandemic, scientists worldwide developed safe and effective vaccines to reduce hospitalization and deaths associated with COVID-19. However, due to the limited availability of vaccine doses, vaccination was prioritized for HCWs and was the best strategy to control deaths and diseases in this population(19). It is essential to describe the characteristics of the local and systemic AEs presented by the HCW and to analyze their relationship with the degree of affectation in the performance of daily activities after full or booster immunization and thus improve vaccination plans in the future.
Our study shows a high prevalence of local and systemic adverse events (62.5%), in medical personnel after 7 days of administration of the approved vaccines in Ecuador, describing a higher frequency after administration of the third dose (75.2%), compared to the first and second doses (60.0% and 52.4%, respectively). Of these adverse events, the great majority did not interfere or slightly interfered with daily activities, showing that they were mild to moderate, despite this, 48.4% of the participants administered some medication to control the side effects. Regarding the most frequent side effects, localized pain at the injection site (local event), myalgia, and headache (systemic events) were reported. Likewise, it was identified that being a woman, receiving an mRNA vaccine, Oxford/AstraZeneca-Vaxzevria, the third dose of any vaccine, and the heterologous vaccine as a booster increased the risk of presenting adverse events.
Naito T. et al.(20) conducted a study with HCWs in Japan with a population that received Pfizer/BioNTech-Comirnaty and Moderna vaccines. They reported similar frequencies of adverse reactions during the first eight days after the second and third vaccination. Also, they found that the incidence of adverse reactions was significantly higher in heterologous vaccination compared to homologous vaccination (20), which is consistent with our results.
In a German study performed by Nachtigall et al. (21), in health workers, the most reported local adverse event during the first eight days, at any vaccination dose, was pain at the injection site (50.2%), followed by malaise (30.1%). Homologous vaccination produced fewer adverse events (49.4%) than heterologous vaccination (81.4%) (21), similar to our results.
In Thailand, a prospective study was performed in HCWs, where the most common systemic adverse events after the Sinovac-CoronaVac / Oxford/AstraZeneca-Vaxzevria booster dose included myalgia, headache, and fever (37%, 34%, and 34%). The AE prevalence was significantly lower for individuals in the Oxford/AstraZeneca-Vaxzevria group after the CoronaVac booster. The most common symptoms observed in this group were headache, myalgia, and fatigue (13%, 11%, and 9%, respectively), and the local reaction was 14%, in comparison with de 17% of the other group (22), similar our results showed previously.
Concerning the vaccine type, Oxford/AstraZeneca-Vaxzevria vaccine showed the highest risk of adverse events (OR 2.45, CI 95% 1.73 - 3.49, p < 0.001) with similar results in several other studies (27,28). On the other hand, a systematic review and meta-analysis performed by Kouhpayeh and Ansari reported that inactivated vaccines such as Sinovac-CoronaVac have no relationship with systemic adverse events (RR 1.13, CI 95% 0.79 – 1.61) (29) as in our study where Sinovac-CoronaVac showed the least risk for AE (OR 0.33, 95% CI 0.20 - 0.53, p < 0.001).
Our study cohort consisted of physicians, and therefore in terms of age distribution, most participants were of working age; this may constrain the generalizability of our results, especially for the elder age groups. Further analysis including nurses, paramedics, and laboratory staff, should be performed to generalize our results to the Healthcare workers group.
5. Conclusion
This study presents the descriptive characteristics of local and systemic adverse events in medical personnel from Quito who were immunized with Oxford/AstraZeneca-Vaxzevria, Pfizer/BioNTech-Comirnaty, and Sinovac-CoronaVac during the National Vaccination Campaign in Ecuador. This study compares the symptoms described most frequently by the participants in the different doses and in the group that received homologous and heterologous vaccination. In addition, the relationship between vaccination and daily activities performance is analyzed, with the requirement of pharmacological treatment to alleviate the reported symptoms. People who received the Vaxzevria vaccine had more adverse events (74.8%) compared to those who received Comirnaty (59.1%) and CoronaVac (39.5%). The highest degree of adverse events occurs with heterologous vaccination compared to homologous immunization (80.1% vs. 53.8%), coinciding with other international results. All the vaccines used by medical personnel produced local and systemic adverse events from the first dose to the booster dose during the first seven days, and the booster dose presented a higher prevalence of adverse events. This situation led to the use of medication for the symptoms presented and affected the performance of physicians' daily activities during the pandemic.
Supplementary Materials
Not applicable.
Author Contributions
Conceptualization, J.R., L.F., and N.F.; methodology, J.R., L.F. and N.F.; software, J.R., L.F. and N.F.; validation, J.R., L.F., M.J. and N.F.; formal analysis, J.R., T.O. and C.M.; investigation, J.R., L.F., and G.G.; resources, J.R., L.F., G.G. and M.J.; data curation, J.R. and M.J.; writing—original draft preparation, J.R., L.F., and N.F.; writing—review and editing, J.R., L.F., T.O., C.M, M.J., G.G., and N.F.; supervision, J.R., and L.F; project administration, J.R., L.F., and N.F.; funding acquisition, G.G.
Funding
Not applicable.
Institutional Review Board Statement
This study was approved by the Independent Ethics Committee SOLCA-NUCLEO QUITO with the number OBS.21.202 and during its development, all the norms of Good Clinical Practice and Helsinki principles were compiled to maintain the participant's safety and assure the quality of data obtained.
Informed Consent Statement
Electronic informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to maintaining privacy data of the participants such as e-mail addresses.
Acknowledgments
ANID - MILENIO - NCS2021_013.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A
Table A1 descriptive characteristics of adverse events in relation to the dose and vaccine.

Table A1.
Descriptive characteristics of adverse events in relation to the dose and vaccine.
| First Dose (n=210) | Second Dose (n=210) | Third Dose (n=210) | ||||||
|---|---|---|---|---|---|---|---|---|
| Oxford/AstraZeneca-Vaxzevria n (%) | Pfizer/BioNTech-Comirnaty n (%) |
Sinovac-CoronaVac n (%) |
Oxford/AstraZeneca-Vaxzevria n (%) | Pfizer/BioNTech-Comirnaty n (%) |
Sinovac-CoronaVac n (%) |
Oxford/AstraZeneca-Vaxzevria n (%) | Pfizer/BioNTech-Comirnaty n (%) |
|
| N | 32 (100.0) | 135 (100.0) | 43 (100.0) | 32 (100.0) | 135 (100.0) | 43 (100.0) | 182 (100.0) | 28 (100.0) |
| Adverse Events | 25 (78.1) | 84 (62.2) | 17 (39.5) | 17 (53.1) | 76 (56.3) | 17 (39.5) | 142 (78.0) | 16 (57.1) |
| Pain | 18 (56.3) | 74 (54.8) | 15 (34.9) | 11 (34.4) | 64 (47.4) | 16 (37.2) | 100 (54.9) | 14 (50.0) |
| Edema | 2 (6.3) | 7 (5.2) | 2 (4.7) | 0 (0.0) | 3 (2.2) | 2 (4.7) | 21 (11.5) | 3 (10.7) |
| Erythema | 2 (6.3) | 11 (8.1) | 1 (2.3) | 0 (0.0) | 3 (2.2) | 3 (7.0) | 14 (7.7) | 2 (7.1) |
| Pruritus | 1 (3.1) | 9 (6.7) | 1 (2.3) | 3 (9.4) | 6 (4.4) | 2 (4.7) | 14 (7.7) | 3 (10.7) |
| Thermal elevation | 9 (28.1) | 19 (14.1) | 2 (4.7) | 1 (3.1) | 16 (11.9) | 2 (4.7) | 81 (44.5) | 6 (21.4) |
| Diarrhea | 2 (6.3) | 2 (1.5) | 0 (0.0) | 0 (0.0) | 2 (1.5) | 0 (0.0) | 12 (6.6) | 2 (7.1) |
| Nausea | 2 (6.3) | 2 (1.5) | 0 (0.0) | 1 (3.1) | 5 (3.7) | 0 (0.0) | 15 (8.2) | 0 (0.0) |
| Vomiting | 1 (3.1) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (0.7) | 0 (0.0) | 2 (1.1) | 0 (0.0) |
| Myalgia | 14 (43.8) | 29 (21.5) | 2 (4.7) | 7 (21.9) | 26 (19.3) | 3 (7.0) | 90 (49.5) | 7 (25.0) |
| Arthralgia | 12 (37.5) | 17 (12.6) | 0 (0.0) | 5 (15.6) | 11 (8.1) | 1 (2.3) | 61 (33.5) | 4 (14.3) |
| Headache | 12 (37.5) | 24 (17.8) | 7 (16.3) | 5 (15.6) | 22 (16.3) | 3 (7.0) | 77 (42.3) | 7 (25.0) |
| Other types of adverse events |
5 (15.6) | 16 (11.9) | 0 (0.0) | 2 (6.3) | 5 (3.7) | 0 (0.0) | 20 (11.0) | 3 (10.7) |
References
- WHO. WHO Coronavirus (COVID-19) Dashboard | WHO Coronavirus (COVID-19) Dashboard With Vaccination Data. Available online: https://covid19.who.int/ (accessed on 20 April 2022).
- WHO. The World Health Report. 2006: Working Together for Health; World Health Organization, 2006. [Google Scholar]
- Bandyopadhyay, S.; Baticulon, R.E.; Kadhum, M.; Alser, M.; Ojuka, D.K.; Badereddin, Y.; et al. Infection and mortality of healthcare workers worldwide from COVID-19: a systematic review. BMJ Glob Health 2020, 5, 3097. [Google Scholar] [CrossRef] [PubMed]
- La Federación Médica reporta decesos de profesionales de la salud por ómicron. Ecuavisa. 2022. Available online: https://www.ecuavisa.com/noticias/ecuador/la-federacion-medica-reporta-decesos-de-profesionales-de-la-salud-por-omicron-DJ1281757 (accessed on 28 July 2022).
- WHO. Access and allocation: how will there be fair and equitable allocation of limited supplies? 2021. Available online: https://www.who.int/news-room/feature-stories/detail/access-and-allocation-how-will-there-be-fair-and-equitable-allocation-of-limited-supplies (accessed on 26 July 2022).
- Ministerio de Salud Pública. Situación Epidemiológica Nacional COVID-19, Ecuador. 2022. Available online: https://www.salud.gob.ec/wp-content/uploads/2022/01/10.1.2022-epi.pdf (accessed on 28 July 2022).
- COE provincial de Pichincha. Situación cantonal por COVID-19. Distrito Metropolitano de Quito. 2021. Available online: https://coe-pichincha.senescyt.gob.ec/situacion-cantones-pichincha/ (accessed on 28 July 2022).
- Wang, P.; Nair, M.S.; Liu, L.; Iketani, S.; Luo, Y.; Guo, Y.; et al. Antibody resistance of SARS-CoV-2 variants B.1.351 and B.1.1.7. Nature 2021, 593, 130–135. Available online: https://www.nature.com/articles/s41586-021-03398-2. [CrossRef] [PubMed]
- Wall, E.C.; Wu, M.; Harvey, R.; Kelly, G.; Warchal, S.; Sawyer, C.; et al. Neutralising antibody activity against SARS-CoV-2 VOCs B.1.617.2 and B.1.351 by BNT162b2 vaccination. The Lancet 2021, 397, 2331–3. Available online: http://ees.elsevier.com/thelancet/www.thelancet.com (accessed on 21 April 2022). [CrossRef] [PubMed]
- Khoury, D.S.; Cromer, D.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; et al. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection. Nature Medicine 2021, 27, 1205–11. Available online: https://www.nature.com/articles/s41591-021-01377-8 (accessed on 21 April 2022). [CrossRef] [PubMed]
- Ministerio de Salud Pública. Vacunómetro COVID-19. 2022. Available online: https://app.powerbi.com/view?r=eyJrIjoiYTkzNTFkMmUtZmUzNi00NDcwLTg0MDEtNjFkNzhhZTg5ZWYyIiwidCI6IjcwNjIyMGRiLTliMjktNGU5MS1hODI1LTI1NmIwNmQyNjlmMyJ9&pageName=ReportSection (accessed on 26 July 2022).
- CDC. Selected Adverse Events Reported after COVID-19 Vaccination|CDC. Vaccines. 2022. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/safety/adverse-events.html (accessed on 21 April 2022).
- Nohl, A.; Brune, B.; Weichert, V.; Standl, F.; Stang, A.; Dudda, M. COVID-19: Vaccination Side Effects and Sick Leave in Frontline Healthcare-Workers-A Web-Based Survey in Germany. 2022. [Google Scholar] [CrossRef] [PubMed]
- Kitro, A.; Sirikul, W.; Thongkum, W.; Soponpong, S.; Yasamut, U.; Kiratipaisarl, W.; et al. Dynamic of anti-spike receptor binding domain (RBD) levels and short-term adverse events following a heterologous booster dose of BNT162b2 after two doses of CoronaVac in Thai health care workers. [CrossRef] [PubMed]
- Hillus, D.; Schwarz, T.; Tober-Lau, P.; Vanshylla, K.; Hastor, H.; Thibeault, C.; et al. Safety, reactogenicity, and immunogenicity of homologous and heterologous prime-boost immunisation with ChAdOx1 nCoV-19 and BNT162b2: a prospective cohort study. Lancet Respir Med. 2021, 9, 1255–1265. Available online: http://www.thelancet.com/article/S221326002100357X/fulltext (accessed on 21 April 2022). [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol. 2008, 61, 344–9. Available online: http://www.jclinepi.com/article/S0895435607004362/fulltext (accessed on 27 December 2022). [CrossRef] [PubMed]
- Helsinki Statement. WMA Declaration of Helsinki—Ethical Principles for Medical Research Involving Human Subjects. the 64th WMA General Assembly, Fortaleza, Brazil, October 2013; Available online: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/ (accessed on 15 December 2022).
- Food and Drug Administration. Toxicity Grading Scale for Healthy Adult and Adolescent Volunteers Enrolled in Preventive Vaccine Clinical Trials | FDA. Center for Biologics Evaluation and Research, editor. 2007, p. 1. Available online: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/toxicity-grading-scale-healthy-adult-and-adolescent-volunteers-enrolled-preventive-vaccine-clinical (accessed on 19 April 2022).
- Organización Panamericana de la Salud. Introducción de la vacuna contra la COVID-19: Orientaciones para determinar los grupos prioritarios y elaborar la microplanificación. 2021. Available online: https://www.campusvirtualsp.org/es (accessed on 27 December 2022).
- Naito, T.; Tsuchida, N.; Kusunoki, S.; Kaneko, Y.; Tobita, M.; Hori, S.; et al. Reactogenicity and immunogenicity of BNT162b2 or mRNA-1273 COVID-19 booster vaccinations after two doses of BNT162b2 among healthcare workers in Japan: a prospective observational study. Expert Rev Vaccines 2022, 21, 1319–1229. [Google Scholar] [CrossRef] [PubMed]
- Nachtigall, I.; Bonsignore, M.; Hohenstein, S.; Bollmann, A.; Günther, R.; Kodde, C.; et al. Effect of gender, age and vaccine on reactogenicity and incapacity to work after COVID-19 vaccination: a survey among health care workers. BMC Infect Dis. 2022, 22, 1–13. Available online: https://bmcinfectdis.biomedcentral.com/articles/10.1186/s12879-022-07284-8 (accessed on 27 December 2022). [CrossRef]
- Cohen, G.; Jungsomsri, P.; Sangwongwanich, J.; Tawinprai, K.; Siripongboonsitti, T.; Porntharukchareon, T.; et al. Immunogenicity and reactogenicity after heterologous prime-boost vaccination with CoronaVac and ChAdox1 nCov-19 (AZD1222). vaccines 2022, 18. [Google Scholar] [CrossRef]
- Kadali, R.A.K.; Janagama, R.; Peruru, S.; Malayala, S.v. Side effects of BNT162b2 mRNA COVID-19 vaccine: A randomized, cross-sectional study with detailed self-reported symptoms from healthcare workers. International Journal of Infectious Diseases. 2021, 106, 376–381. Available online: http://www.ijidonline.com/article/S1201971221003581/fulltext (accessed on 27 December 2022). [CrossRef] [PubMed]
- Bae, S.; Lee, Y.W.; Lim, S.Y.; Lee, J.H.; Lim, J.S.; Lee, S.; et al. Adverse Reactions Following the First Dose of ChAdOx1 nCoV-19 Vaccine and BNT162b2 Vaccine for Healthcare Workers in South Korea. J Korean Med Sci. 2021, 36, 1–9 Available online:. [Google Scholar] [CrossRef] [PubMed]
- Beatty, A.L.; Peyser, N.D.; Butcher, X.E.; Cocohoba, J.M.; Lin, F.; Olgin, J.E.; et al. Analysis of COVID-19 Vaccine Type and Adverse Effects Following Vaccination. JAMA Netw Open. 2021, 4. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, D.C.; Dao, T.L.; Truong, T.M.D.; Nguyen, T.H.; Phan, T.N.; Nguyen, H.M.; et al. Short-Term Adverse Effects Immediately after the Start of COVID-19 Booster Vaccination in Vietnam. Vaccines 2022, 10. [Google Scholar] [CrossRef] [PubMed]
- Alqahtani, S.; Jokhdar, H.; Al-Tawfiq, J.A.; Al-Otaibi, S.; Assiri, A.; Almudarra, S.; et al. Adverse events following administration of COVID-19 vaccines in Saudi Arabia. Sci. Rep. 2022, 12. [Google Scholar] [CrossRef] [PubMed]
- Montano, D. Frequency and Associations of Adverse Reactions of COVID-19 Vaccines Reported to Pharmacovigilance Systems in the European Union and the United States. Front Public Health. 2022, 9. [Google Scholar] [CrossRef] [PubMed]
- Kouhpayeh, H.; Ansari, H. Adverse events following COVID-19 vaccination: A systematic review and meta-analysis. Int Immunopharmacol. 2022, 109. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Summary of participants.
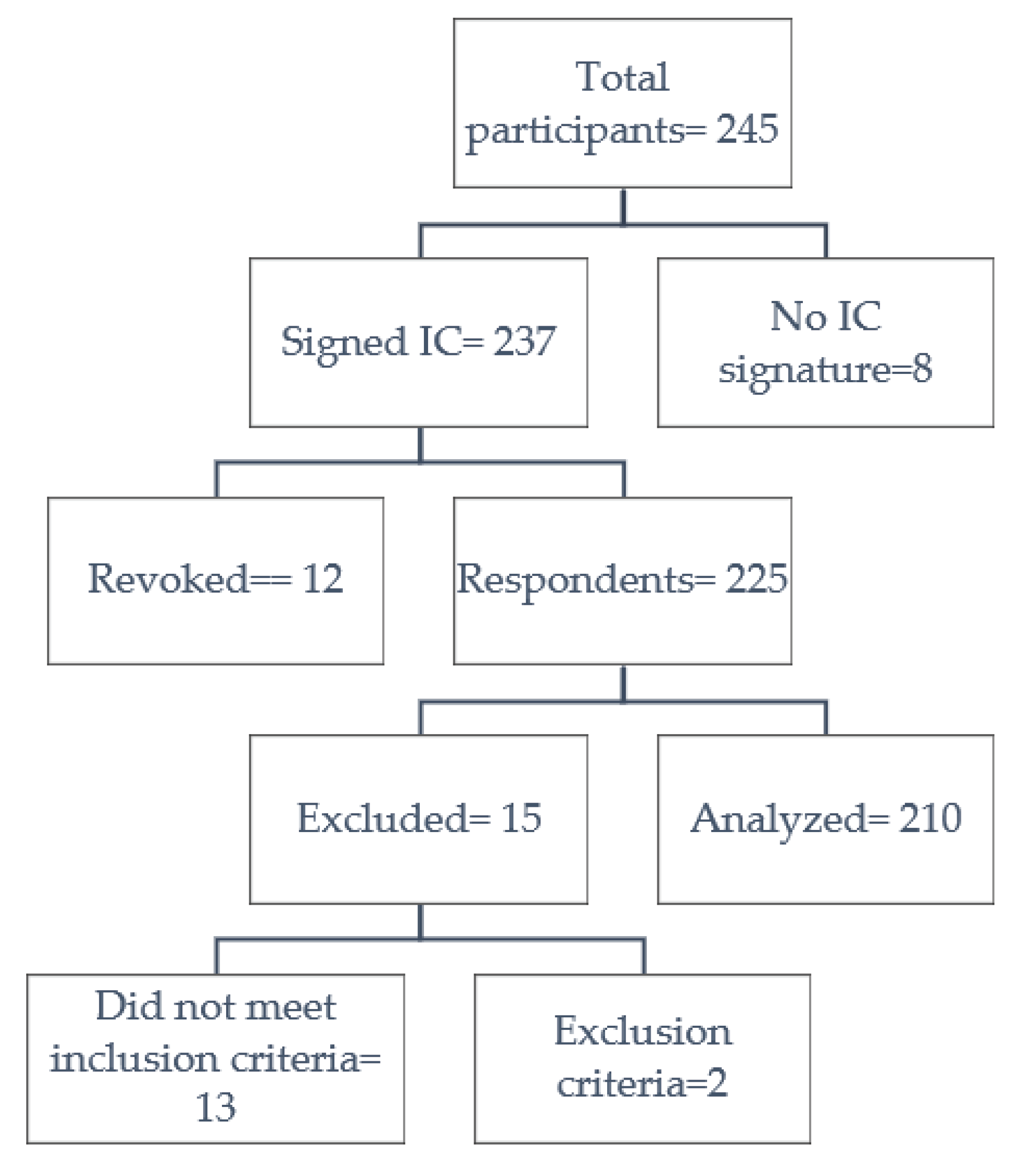
Table 1.
Sociodemographic characteristics and vaccine administered to participants.
| n (%) | ||
| General | 210 (100.0) | |
| Sex | Female | 138 (65.7) |
| Male | 72 (34.3) | |
| Age (Years) | Under 30 years of age | 88 (41.9) |
| 30 to 39 years old | 70 (33.3) | |
| 40 to 49 years old | 25 (11.9) | |
| 50 to 59 years old | 15 (7.1) | |
| Over 60 years old | 12 (5.7) | |
| Vaccine | Total | 630 (100.0) |
| Pfizer/BioNTech-Comirnaty | 298 (47.3) | |
| Oxford/AstraZeneca-Vaxzevria | 246 (39.0) | |
| Sinovac-CoronaVac | 86 (13.7) | |
Table 2.
Descriptive characteristics of adverse events, medication, and relationship with daily activities.
Table 2.
Descriptive characteristics of adverse events, medication, and relationship with daily activities.
| Total n (%) |
First Dose n (%) |
Second Dose n (%) | Third Dose n (%) |
|
|---|---|---|---|---|
| General | 630 (100.0) | 210 (33.3) | 210 (33.3) | 210 (33.4) |
| Adverse Events | 394 (62.5) | 126 (60.0) | 110 (52.4) | 158 (75.2) |
| Pain | 312 (49.5) | 107 (51.0) | 91 (43.3) | 114 (54.3) |
| Myalgia | 178 (28.3) | 45 (21.4) | 36 (17.1) | 97 (46.2) |
| Headache | 157 (24.9) | 43 (20.5) | 30 (14.3) | 84 (40.0) |
| Thermal elevation | 136 (21.6) | 30 (14.3) | 19 (9.0) | 87 (41.4) |
| Arthralgia | 111 (17.6) | 29 (13.8) | 17 (8.1) | 65 (31.0) |
| Edema | 40 (6.3) | 11 (5.2) | 5 (2.4) | 24 (11.4) |
| Pruritus | 39 (6.2) | 11 (5.2) | 11 (5.2) | 17 (8.1) |
| Erythema | 36 (5.7) | 14 (6.7) | 6 (2.9) | 16 (7.6) |
| Other types of adverse events | 100 (15.9) | 30 (3.6) | 16 (7.3) | 54 (25.8) |
| Use of medication | 305 (48.4) | 93 (44.3) | 78 (37.1) | 134 (63.8) |
| 1 drug | 243 (79.7) | 84 (90.3) | 68 (87.2) | 91 (67.9) |
| 2 drugs | 54 (17.7) | 6 (6.5) | 8 (10.3) | 40 (29.9) |
| 3 or more drugs | 8 (2.6) | 3 (3.2) | 2 (2.6) | 3 (2.2) |
| Daily Activities | 394 (100.0) | 126 (100.0) | 110 (100.0) | 158 (100.0) |
| Do not interfere with your daily activities and no treatment is administered | 158 (40.1) | 64 (50.8) | 56 (50.9) | 38 (24.1) |
| Interferes with daily activities and/or required pharmacological treatment. | 176 (44.7) | 55 (43.7) | 46 (41.8) | 75 (47.5) |
| Impedes the performance of daily activities and required treatment | 57 (14.5) | 7 (5.6) | 8 (7.3) | 42 (26.6) |
| Was hospitalized | 3(0.8) | 0 (0.0) | 0 (0.0) | 86 (1.9) |
Table 3.
Descriptive characteristics of adverse events, medication, and relationship to daily activities in relation to the vaccine.
Table 3.
Descriptive characteristics of adverse events, medication, and relationship to daily activities in relation to the vaccine.
| Oxford/AstraZeneca-Vaxzevria n (%) |
Pfizer/BioNTech-Comirnaty n (%) |
Sinovac-CoronaVac n (%) |
|
|---|---|---|---|
| General | 246 (100.0) | 298 (100.0) | 86 (100.0) |
| Adverse Events | 184 (74.8) | 176 (59.1) | 34 (39.5) |
| Pain | 129 (52.4) | 152 (51.0) | 31 (36.0) |
| Myalgia | 111 (45.1) | 62 (20.8) | 5 (5.8) |
| Headache | 94 (38.2) | 53 (17.8) | 10 (11.6) |
| Thermal elevation | 91 (37.0) | 41 (13.8) | 4 (4.7) |
| Arthralgia | 78 (31.7) | 32 (10.7) | 1 (1.2) |
| Edema | 23 (9.30) | 13 (4.4) | 4 (4.7) |
| Pruritus | 18 (7.3) | 18 (6.0) | 3 (3.5) |
| Erythema | 16 (6.5) | 16 (5.4) | 4 (4.7) |
| Other types of adverse events | 62 (22.3) | 38 (12.7) | 0 (0.0) |
| Use of medication | 155 (63.0) | 126 (42.3) | 24 (27.9) |
| 1 drug | 111 (71.6) | 110 (87.3) | 22 (91.7) |
| 2 drugs | 40 (25.8) | 12 (9.5) | 2 (8.3) |
| 3 or more drugs | 4 (2.6) | 4 (3.2) | 0 (0.0) |
| Daily Activities | 184 (100.0) | 176 (100.0) | 34 (100.0) |
| Do not interfere with your daily activities and no treatment is administered | 54 (77.0) | 79 (44.9) | 25 (73.5) |
| Interferes with daily activities and/or required pharmacological treatment. | 88 (79.0) | 79 (44.9) | 9 (26.5) |
| Impedes the performance of daily activities and required treatment | 39 (18.0) | 18 (10.2) | 0 (0.0) |
| Was hospitalized | 3 (1.6) | 0 (0.0) | 0 (0.0) |
Table 4.
Adverse events after vaccination medication, and relationship to daily activities: Heterologous vs Homologous.
Table 4.
Adverse events after vaccination medication, and relationship to daily activities: Heterologous vs Homologous.
| Heterologous n (%) |
Homologous n (%) |
|
|---|---|---|
| General | 171 (100.0) | 39 (100.0) |
| Adverse Events | 137 (80.1) | 21 (53.8) |
| Pain | 97 (56.7) | 17 (43.6) |
| Myalgia | 89 (52.0) | 8 (20.5) |
| Thermal elevation | 80 (46.8) | 7 (17.9) |
| Headache | 78 (45.6) | 6 (15.4) |
| Arthralgia | 61 (35.7) | 4 (10.3) |
| Edema | 23 (13.5) | 1 (2.6) |
| Pruritus | 15 (8.80) | 2 (5.1) |
| Erythema | 14 (8.20) | 2 (5.1) |
| Other types of adverse events | 51 (29.9) | 3 (7.7) |
| Use of medication | 120 (70.2) | 14 (35.9) |
| 1 drug | 82 (68.3) | 9 (64.3) |
| 2 drugs | 35 (29.2) | 5 (35.7) |
| 3 or more drugs | 3 (2.5) | 0 (0.0) |
| Daily Activities | 137 (100.0) | 21 (100.0) |
| Do not interfere with your daily activities and no treatment is administered | 28 (20.4) | 10 (47.6) |
| Interferes with daily activities and/or required pharmacological treatment. | 68 (49.6) | 7 (33.3) |
| Impedes the performance of daily activities and required treatment | 38 (27.7) | 4 (19.0) |
| Was hospitalized | 3 (2.2) | 0 (0.0) |
Table 5.
Factors related to the development of adverse events.
| Total (n/%) |
Adverse Event No (n/%) |
Adverse Event Yes (n/%) |
p Value | OR (CI 95%) | |
|---|---|---|---|---|---|
| General | 630(100.0) | 236 (37.5) | 394 (62.5) | - | - |
| Sex | |||||
| Female | 414 (65.7) | 136 (57.6) | 278 (70.6) | 0.001 | 1.76 (1.25 – 2.46) |
| Age | |||||
| Over 32 years old | 522 (82.9) | 193 (81.8) | 329 (83.5) | 0.579 | 1.12 (0.73 - 1.72) |
| Doses administered | |||||
| First Dose | 210 (33.3) | 84 (35.6) | 126 (32.0) | 0.353 | 0.85 (0.60 - 1.19) |
| Second Dose | 210 (33.3) | 100 (42.4) | 110 (27.9) | < 0.001 | 0.52 (0.37 - 0.74) |
| Third Dose | 210 (33.3) | 52 (22.0) | 158 (40.1) | < 0.001 | 2.36 (1.64 - 3.42) |
| Vaccine | |||||
| Pfizer/BioNTech-Comirnaty | 298 (47.3) | 122 (51.7) | 176 (44.7) | 0.087 | 1.32 (0.95 – 1.83) |
| Oxford/AstraZeneca-Vaxzevria | 246 (39.0) | 62 (26.3) | 184 (46.7) | < 0.001 | 2.45 (1.73 - 3.49) |
| Sinovac-CoronaVac | 86 (13.7) | 52 (22.0) | 34 (8.6) | < 0.001 | 0.33 (0.20 - 0.53) |
| General | 420(100.0) | 152 (36.2) | 268 (63.8) | - | - |
| Group Vaccine | |||||
| Heterologous | 171 (40.7) |
34 (22.4) |
137 (51.1) |
< 0.001 | 3.63 (2.31 – 5.69) |
| Homologous | 249 (59.3) | 118 (77.6) | 131 (48.9) |
CI: Confidence Interval.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



