
Submitted:
26 January 2023
Posted:
26 January 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Abstract Background COVID-19 vaccination program among Adults in India is one of the highly successful vaccination drives globally. Indian children aged 15–18 years old became eligible for COVID-19 vaccination on 3rd January, 2022 followed by 12-14 years old children on 16th March, 2022. As parents are primary decision-makers for their children, we aimed to assess parents' perceptions and intentions regarding COVID-19 vaccination for children in India. Aim To assess parental perceptions and intention to get COVID-19 vaccination for their children (aged<18 years), Materials and Methods A cross-sectional anonymous web-based survey was designed. Healthcare workers of a tertiary care institute in Eastern U.P. having any children aged <18 years were the study population. They were recruited through snowball sampling and were sent the study questionnaire in Google form through email and WhatsApp. Cross-tabulation was performed by parents' intention to vaccinate their children against COVID-19 virus with socio-demographic characteristics and their risk perception toward COVID-19, trust in the healthcare system, and their history of vaccine hesitancy behavior routine childhood immunization. Bi-variate analysis was performed to find out the predictors of child vaccination intention among the parents. Results A total of 388 healthcare workers parents (HCWPs) having A child < 18 years of age completed the survey. Mean age of the parents were 40.28 ±11.34 years with majority(97.0%) completing recommended 2 doses of COVIID-19 vaccine. Around 91% of the parents agreed that COVID-19 vaccines are important for child’s health whereas about 89% agreed to the statement that COVID-19 vaccines are effective. A total 356 (91.7%) participants were willing to vaccinate their child against COVID-19, 91.3% of them liked to do so as soon as possible. The factors significantly associated with the stated likelihood of child vaccination among the participants were younger age, female gender, urban residence, absence of any chronic illness, lower monthly income, history of COVID-19 in child and the child/children completed with routine childhood vaccines. Parental concerns mainly centered around vaccine need, safety and side effects. Conclusion The healthcare worker parents(HCWPs) have good knowledge and positive attitude towards COVID-19 vaccination for children. Around 92% of them were willing to vaccinate their children with COVID vaccine currently, which implies very low vaccine hesitancy among the HCWPs . Further longitudinal studies are required to be conducted to assess the trend of parental acceptance of COVID vaccine.
Keywords:
Parents
; Healthcare workers
; Children
; C0VID-19 vaccine
; Perception
; Intention
; Attitude
1. Introduction
Globally, there have been more than 650 million confirmed cases of COVID-19, including 6.6~million deaths, reported to World Health Organization (WHO) as of December 23. 2022 [1]. India reported around 44 million confirmed cases and 0.5 million deaths due to COVID-19 as of December 23, 2022 [2]. An effective strategy to combat the morbidity and mortality due to COVID-19 and to achieve higher population levels of immunity is development of an effective and safe vaccine for all populations, including children and adolescents. As per the available evidence, children infected with COVID-19 present with mild symptoms and are at lower risk of hospitalization and life-threatening complications due to COVID-19 [3]. Numerous public health authorities, including the WHO and United States’ Centers for Disease Control and Prevention (CDC), advocate COVID-19 vaccine for children [4,5]. Although severe COVID-19 disease is rare in children and adolescents, vaccination of adolescents aged 12–18 years has been found to be associated with a reduction in hospitalization COVID-19 [6,7] and risk of Multi-system Inflammatory Syndrome (MIS-C) [7,8,9] in this age group. A safe and effective COVID-19 vaccine will have both direct and indirect benefits [10]. COVID-19 vaccination is likely to provide many benefits simultaneously, such as reducing severe illness in children, resulting in fewer illnesses in families, normalizing the economy, opening schools, reducing inequalities and reducing stress.
Since early days of the pandemic, a large number of vaccines were being developed globally [11]. In India, 3 vaccines i.e. Bharat Biotech’s Covaxin, Cadila’s Zycov-D, and Biological E Limited’s Corbevax have been granted emergency use authorization by the Drugs Controller General of India (DCGI) for children in different age-groups [12]. In India, vaccination of children aged 15-18 years, was started from January 3, 2022 with Covaxin [13].
Despite the success of adult COVID-19 vaccination globally, implementation of childhood immunization against COVID-19 is faced with difficulties and is proving to be a big challenge for policymakers and healthcare managers. Including an effective and safe vaccine for children and a high level of vaccine acceptance among the parents or caregivers is also a key factor for global immunization success.WHO recommends that COVID-19 vaccines that have undergone clinical trials in children and adolescent are safe and effective in preventing disease in children and adolescents [5].
However, the success of any vaccination program depends on the acceptance of vaccines by the target population and is important for achieving herd immunity to halt the pandemic. WHO defines vaccine hesitancy as a delay in the acceptance or refusal of vaccination despite the availability of vaccination services. The WHO has designated it as one of the most critical challenges to public health at all times [14,15]. Vaccine hesitant individuals may accept some of the vaccines while rejecting others, delay vaccinations, or accept vaccinations but have concerns [16]. The causes of vaccine hesitancy vary across different countries and across the same country which signifies the complex and context-specific nature of vaccine hesitancy and the factors influencing it and highlights the importance of locally identifying the pertinent contributory factors of vaccine hesitancy and designing tailored interventions to tackle these [17].
Parents have the right to decide whether or not their children should be vaccinated against COVID-19. Therefore, it is important to understand parents’ perceptions including attitude and willingness to get their children the COVID-19 vaccine. Studies from different countries around the globe show variable parental acceptance for the COVID 19 vaccination for children with most of them reporting lower rate of acceptance [18,19,20,21,22,23,24,25,26,27,28]. In United States, it was less than 50%, to as low as 6.7% in South Korea whereas in UAE and China, it was as high as 75.1% and 92.7% respectively [19,22,23,24]. A recent systematic review assessing barriers and facilitators of COVID-19 vaccination among children found that parents around the globe are hesitant to vaccinate their kids against COVID-19 and the spectrum of factors associated with vaccine hesitancy and uptake varies across the globe.The review concluded that local context is inevitable to take into account while developing programs to reduce vaccine hesitancy [29]. As the decision of vaccinating children lies with their parents or guardians, it is important to study their acceptance of and attitudes toward the COVID-19 vaccine and the factors that determine vaccine acceptance and hesitancy.
There have been very few studies from India and none from the state of Uttar Pradesh (U.P.), the largest state of India by population, assessing parent’s willingness of COVID-19 vaccine for their children. Further, there is a dire need to devise strategies to address vaccine hesitancy among parents through the identification of attributing factors. Our study objectives were to assess the perception and willingness of Healthcare Workers to have their children a COVID-19 vaccine and to identify parental concerns about the vaccines. Additionally, we also explored the factors associated with willingness for vaccine uptake by the parents. The study was conducted at a time when the government health authorities are implementing vaccination for children aged 12 to 17 years in the country. The findings would be helpful in designing and implementing newer health interventions aimed at increasing parental acceptance of the COVID-19 vaccine, as well as filling in any existing knowledge gaps.
2. Material and Methods
2.1. Study Design & Population
This cross-sectional web based survey was conducted from 1st October, 2022 to 30th November 2022.The study population were the healthcare workers (HCWs), of BRD Medical College & Hospital, a tertiary care hospital in Gorakhpur, Eastern U.P., who were parents of any child below the age of 18 years. The healthcare workers were of both genders, working in the institute and directly or indirectly involved in the patient care.
2.2. Sample Size and sampling strategy
Assuming the maximum variability, which is equal to 50% (p = 0.5) and taking 95% confidence level with ±5% relative precision, the calculation for required sample size was as follows:
So, using the formula n = z2pq/(pl)2, and putting in values as, p = 0.5 and hence q = 1 − 0.5 = 0.5; l = 0.05; z =1.96, the sample size came as 384. However, we intended to take around 400.
Snow ball sampling technique was used to recruit the participants. The directory of all healthcare workers was obtained from the Medical Superintendent’s office and the survey link was shared with the potential participants through WhatsApp and email.
2.3. Study tools
A draft of the questionnaire was prepared based on a review of the relevant literature and reviewed by subject experts. The draft questionnaire was then pilot tested on 50 participants and was adjusted for accuracy and clarity. The consistency and stability of the final questionnaire was tested using Cronbach’s alpha which was 0.82 denoting good internal consistency.The data of the piloted study were not included in the final analysis.
Socio-demographic Measures The questionnaire has detailed information about the sociodemographic characteristics of study participants, including participant’s age, sex, education level, place of residence, monthly income, occupation, and social status in the community.
Parents confidence in COVID 19 vaccine Participants were required to answer ten questions related to their confidence in COVID-19 vaccines on a five-point Likert scale (1 = Strongly disagree, 2 = disagree, 3 = Neither agree nor disagree, 4 = Agree, 5 = Strongly agree). All questions were framed such that options 1 and 2 were regarded to denote as hesitancy and 3, 4 and 5 as non-hesitancy in our study. Vaccination in general was changed to COVID-19 Vaccination in the original oxford vaccination hesitancy scale (VHS) [30] and all the negative statements were converted to positive ones.
Intent to Vaccinate the Child The survey asked, “Do you intend to vaccinate your child (ren) for COVID-19 if not vaccinated yet?”. The responses were captured in a 3-point Likert scale (Yes, No, and Not sure). We coded “Yes” as “Willing to get a COVID-19 vaccine for their child;” all others were labeled as “non-willing or hesitant”. Those who have already got their children vaccinated with one or two dose of COVID vaccine were also labelled as “Willing”
2.4. Data Collection
The link of the Google form containing the survey questionnaire was distributed online through email and WhatsApp to the HCW-parents and comprised of mainly closed ended questions designed to meet the study objectives. The questionnaire was prepared both in English and Hindi language in the Google forms. The questionnaire was translated from English to Hindi (local language) by a bilingual person to enable an easy understanding of the questions and avoid any questionnaire bias. The questionnaire comprised of three sections; the first included the participants’ socio-demographic characteristics, such as age, sex, and place of residence. The second part included questions assessing the attitude of parents towards COVID-19 vaccines for children using the modified VHS scale. The third part consisted of questions assessing the perspectives of parents towards COVID-19 vaccines for children.
2.4. Ethical Considerations
The survey questionnaire started with a brief explanation of the study objectives and intent and a reminder to participants that their participation is entirely voluntary. Electronic informed consent was obtained from all the participants before filling out the survey forms. The confidentiality of data was well-preserved throughout the study by keeping it anonymous and asking the participants to select honest answers and options.The study This study protocol was approved by the institutional Ethical Committee (IEC) of BRD Medical College, Gorakhpur, Uttar Pradesh, India vide letter no.- BRD/IEC/221/2022 dated 21/09/22
2.5. Statistical Analysis
The responses received in Google forms were extracted into excel sheets. Data was analyzed using Statistical Package for Social Sciences, version 23.0 (SPSS, Inc., Chicago, IL, USA). Information related to parent’s perspectives and their experiences towards COVID-19 vaccine were presented in descriptive statistics like, frequency and percentage. Pearson’s chi-square test/ Fischer exact test were used to find the association between willingness of participants to get their child/children vaccinated as a dependent variable and related variables such as socio-demographic characteristics, COVID-19 infection and vaccination history of participants’ etc. as independent variables. p-value of less than 0.05 was considered as statistically significant.
3. Results
A total of 388 healthcare workers parents (HCWPs) having a child < 18 years of age completed the survey and constituted our study participants during the study period. Around half of them were aged 30-39 years (46.4%), 60.8% were females, 88.6% were Hindu by religion, 97.9% were currently married, 54.6% were educated to graduate level or higher, 42.3% were OPD/Ward/Lab/Sanitary attendants, 70.1% had monthly income <50,000/- INR, 91.7% were not suffering from any chronic illness, 49.5% had a history of lab confirmed COVID-19 diagnosis and 96.9% of them had received 2 or more doses of COVID-19. Primary source of information with regard to COVID19 vaccines was workplace in 54.6% participants followed by traditional media (25.8%) such as Newspaper, Television, and Radio. Around half (48.5%) of the participants were having only 1 children below 18 years of age with majority of children being in the age-group of 12-17 years (51.5%) and males (57.5%). A total of 10.3% of the participants gave a history of COVID-19 infection in their child/children and 88.7% of them informed that their child/children is/are up-to-date with respect to the routine mandatory vaccines. Their detailed characteristics are depicted in Table 1.
Vaccine Hesitancy Scale (VHS)—Attitude towards the Importance of Vaccinating Children against COVID-19
All the ten statements of VHS, modified as per the context of COVID-19 vaccines for children, were incorporated to measure the adequacy of attitudes regarding the COVID-19 vaccine among the parents.
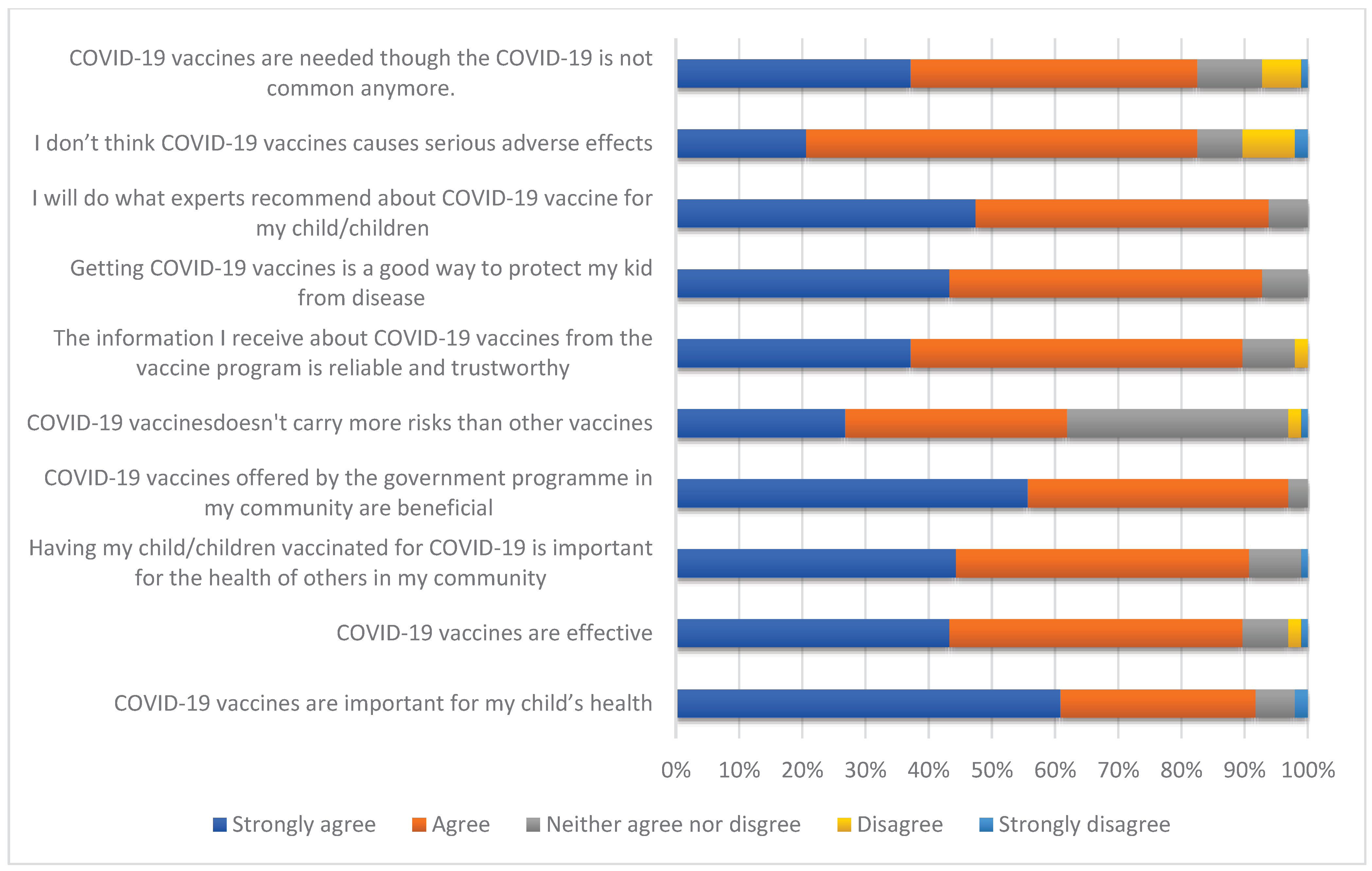
More than 60% of parents have shown agreement with all the ten statements depicting positive attitude with more than 80% of the parents showing agreement with 9 out of the 10 statements, indicating that parents are aware of the COVID-19 vaccine’s importance and benefits in children. More than 90% of parents stated that they would follow the experts’ recommendations regarding vaccinating their children with COVID-19 vaccine.Nearly 90% of parents agreed that they trust and rely on information from the vaccine program regarding COVID-19 vaccination in children and a similar percentage of parents agreed that the COVID-19 vaccines were effective. Conversely, around 40% of parents have displayed their disagreement on the statement “COVID-19 vaccines doesn’t carry more risks than other vaccines” and around 20% of them displaying disagreement with the statements “I don’t think COVID-19 vaccines causes serious adverse effects” and “COVID-19 vaccines are needed though the COVID-19 is not common anymore”, which denotes the vaccine hesitancy among them.
Figure 1.
-Parental attitude towards importance of vaccinating their children with COVID-19 vaccine.
Figure 1.
-Parental attitude towards importance of vaccinating their children with COVID-19 vaccine.
A total of 356 (91.7%) participants showed willing to vaccinate their child with COVID-19 vaccines, 16(4.1%) refused for the same and remaining 16 (4.1%) were undecided regarding vaccinating their children. Out of the 356 participants showing willingness, 320(89.9%) intended to get their child vaccinated as soon as possible whereas 36 (10.1%) told that they would do as after some time only (Figure 2).
On bivariate analysis, the factors found to be significantly associated with the stated willingness for getting their children vaccinated with COVID-19 vaccine among the participants were younger age (18-39 years), female gender, currently married status, urban residence, lower monthly income(<10,000 INR), absence of any chronic illness in participant, history of any child testing positive for COVID-19 and history of completing immunization of the child/children with mandatory childhood vaccines.

Table 3.
Association of socio-demographic and medical characteristics of the participants and their children with their willingness to vaccinate their children with COVID-19 vaccine (n=388).
Table 3.
Association of socio-demographic and medical characteristics of the participants and their children with their willingness to vaccinate their children with COVID-19 vaccine (n=388).
| Variables | Willing to vaccine the child N(%) |
Not willing to vaccinate the child N(%) |
X2* -value | p-value |
|---|---|---|---|---|
|
Age-group ( in years) 18-39 ≥ 40 years |
176(95.7) 180(88.2) |
8(4.3) 24(11.8) |
7.03 |
0.008* |
|
Gender Male Female |
128(84.2) 228(96.6) |
24(15.8) 8(3.4) |
18.8 |
0.00001* |
|
Religion Hindu Non-Hindu |
316(91.7) 40(90.9) |
28(8.3) 4(9.1) |
0.004 |
0.83 |
|
Marital status Currently married Widowed/divorced/separated |
352(92.6) 4(50.0) |
28(7.4) 4(50.0) |
18.8 |
0.00001* |
|
Education level Below graduate Graduate and above |
164(93.2) 192(90.6) |
12(6.8) 20(9.4) |
0.86 |
0.35 |
|
Occupation Doctor Nurse/Technician/Others |
112(90.3) 244(92.4) |
12(9.7) 20(7.6) |
0.49 |
0.48 |
|
Place of residence Urban Rural |
216(94.7) 140(87.5) |
12(5.3) 20(12.5) |
6.5 |
0.01* |
|
Monthly income (in INR) <10,000 ≥ 10,000 |
156(95.1) 200(89.3) |
8(4.9) 24(11.7) |
4.26 |
0.03* |
|
Presence of any chronic illness in participant Yes No |
24(75.0) 332(93.2) |
8(25.0) 24(6.8) |
12.93 |
0.0003* |
|
History of Lab confirmed COVID-19 in participant Present Absent |
172(89.6) 184(93.9) |
20(11.4) 12(6.1) |
2.36 |
0.12 |
|
History of hospitalization due to COVID-19 Present Absent |
12(100.0) 344(91.5) |
0(0.0) 32(8.5) |
- |
0.7 |
|
Self COVID-19 vaccination status Taken 2 or more doses Taken 1 dose only/not vaccinated |
344(91.5) 12(100.0) |
32(8.5) 0(0.0) |
- |
0.7 |
|
History of any adverse event post COVID-19 vaccination Present Absent |
116(93.5) 240(90.9) |
8(6.5) 24(8.1) |
0.77 |
0.38 |
|
History of any child testing positive for COVID-19 Present Absent |
32(80.0) 324(93.1) |
8(20.0) 24(6.9) |
8.14 |
0.004* |
|
The child/ren up-to-date with routine childhood vaccines Yes No/Not sure |
320(93.0) 36(81.8) |
24(7.0) 8(18.2) |
6.47 |
0.01* |
*Statistically significant.
The reasons given by the participants who showed non willingness for their child vaccination against COVID-19 are listed in Figure 3. The common reasons given were that there is lesser risk of infection to my child as community has acquired immunity against COVID-19(50.0%), the epidemic of COVID-19 has gone now (37.5%), sub-clinical infections have already imparted considerable immunity to my child (37.0%), vaccine is not effective (25.0%) and concerns with the safety of vaccine in children (25.0%). A total of 4 (25.0%) participants gave no reason for their unwillingness.
4. Discussion
Vaccination is one of the most cost-effective scientific interventions which has been proven for controlling many infectious diseases and has also helped in eradicating some diseases. The most important ingredient in all vaccines is trust” [31], and their public acceptance is critical for containing or ending any pandemic [32]. COVID-19 vaccine is the most powerful tool that we have in combating the battle against the COVID-19 pandemic but vaccine hesitancy could be one of the greatest challenges in the battle against the COVID-19 by hindering the successful roll out of COVID-19 vaccination among children. The vaccine refusal or hesitancy is driven by diverse factors in different countries or community groups [33,34].
In our study, around 97% of Healthcare Worker Parents (HCWPs) had received the recommended 2-doses of COVID vaccines and around 75% of them had also taken the booster dose of the vaccine. Only around 3% of the participants were found to have self COVID-19 vaccine hesitancy as compared to 15 % of the health care workers in United States having hesitancy to receive the COVID-19 vaccine [35]. In contrast, in a pan India study conducted among general population in early 2021, more than a fifth were either unaware of the COVID vaccine (20.63 %), more than a fourth were not sure if they will get the vaccine (27%), and 10% indicated that they will refuse for the vaccination [36]. The reason for this could be the differences in study populations and time periods in the two studies. Our study was done among HCWs who are definitely having better knowledge and awareness of COVID-19 vaccines and the former study was conducted in the early phase of the COVID-19 vaccine roll out when apprehensions regarding the new COVID-19 vaccines were much higher.
Majority (91.7%) of the parents in our study were willing to get their children vaccinated with COVID vaccine with 83% of them intended to get their children vaccinated as soon possible. In contrast to this, a study by Padhy et al. [37] found only 33.5% of the Indian parents to be willing to get their child a COVID-19 vaccine. The later study was conducted before the introduction of COVID-19 for Children in India and their study participants were from the general population whereas our study was conducted after the rollout of COVID-19 vaccine for children and our study participants were healthcare workers only. In a study by Mohan et al. [38], majority of the parents (85%) reported acceptance of the COVID-19 vaccine for children. Similarly, in a study by Sarkar et al. [39] among the healthcare worker parents (HCWPs) from Southern India, 85.13% said they would vaccinate their children, 12.6 % said they wouldn’t and 2.2 % said they were not sure, similar to our findings. In the same study, 97% of the HCWPs had completed their COVID-19 vaccination schedule which is exactly same as found in our study. Another study by Himanshi et al. [40] found the prevalence of COVID-19 vaccine hesitancy for children among the healthcare professionals to be only 3.3%. It is clearly evident from these findings that healthcare workers have much lower COVID-19 vaccine hesitancy for children compared to the general population. In a study by Yilmaz et al. [27] from Turkey, the only characteristic of either parents or children found to affect the parents’ willingness for children to receive the COVID-19 vaccine was the parent being a healthcare worker. Vaccine hesitancy (VH) is highly context and time specific. A survey on COVID-19 vaccine acceptance across 23 countries from 29 June to 10 July 2022, found willingness to accept vaccination at 79.1%, up 5.2% from June 2021. However, hesitancy increased in eight countries, ranging from 1.0% (United Kingdom) to 21.1% (South Africa). Overall support for vaccinating children under 18 years of age increased slightly but declined among parents who were personally hesitant [41]. Similarly, in a study from China comparing parent’s COVID-19 VH before and after the rollout of childhood covid-19 vaccination, the prevalence of VH for children aged 3-11 years dropped from 25.9% to 17.4%, while such a prevalence of VH for children aged 12-17 years dropped from 26.0% to 3.5% [42].
Factors found to be significantly associated with willingness to have their children receive a COVID-19 vaccine in our study were: younger age of the parent (18-39 years), female parent, currently married status, urban residence, lower monthly income (<10,000 INR), absence of any chronic illness in the parent, history of any child testing positive for COVID-19 and the child/children being up-to-date with mandatory childhood vaccines. In the study by Padhy et al. [37], the stated likelihood of child vaccination was greater among parents who had a bachelor’s degree or higher education as well as among parents who intended to vaccinate themselves. However, in our study, parent’s level of education as well as parent’s COVID-19 vaccination status was not found to associated with their willingness for their child’s COVID vaccination. However, a study by Shati et.al. [43] from Western Saudi Arabia found younger parents to have lesser vaccine hesitancy as compared to the older ones, which was also observed in our study.
Lesser risk of COVID-19 in children and pandemic of COVID- 19 being over were the common reasons given by parents for their unwillingness for the child vaccination. In the study by Sarkar et al.[39], among the parents who were unwillingness for child vaccination, most parents felt COVID-19 is a mild illness in children and therefore do not require vaccination and the second most common cause was fear of adverse effects in their children, quite similar to our findings. In an another study from Turkey reported that fear of adverse effects of vaccines is a significant driver of vaccine hesitancy among the parents [44].
Strengths & Limitations
The major strength of our study is that it is one of the few studies from India assessing parental perception and acceptance for childhood COVID-19 vaccination and first study from Uttar Pradesh (U.P.) the largest state of country. It was carried out in the high risk population of health care workers who are parents (HCWPs). However, it has certain limitations. The cross-sectional design of the study should be interpreted carefully when describing overall prevalence of vaccine hesitancy among parents in India. As it was an online survey, our sample only represented individuals with smart phone and internet access with knowledge of mobile literacy. Therefore, it may not be representing all the healthcare workers. The another limitations being a single centre study and inability to collect responses from all participants, and under representation of certain category of healthcare workers such as nursing officers and technicians and over representation of attendants and doctors working at our institute. Although an attempt was made to sample the health care workers based on their proportion, we were not able to recruit the planned number of participants under each category. There may be a possibility of recall bias affecting the validity of our study results as most of the information concerning the medical history and routine vaccination status of child was obtained from the participants based on their memory.
Despite the above limitations, our study was conducted at a critical time, when the COVID-19 pandemic is supposedly becoming less intense day by day and people have authorities have become complacent. Our findings reminiscent of the fact that although willingness for Childhood COVID-19 vaccination among the HCWPs is high, it may not necessarily turn into action i.e. getting their children vaccinated and requires continuous campaigns to remove misconceptions of COVID-19 vaccination in Children. highlights the need for longitudinal studies to measure the acceptability of a COVID-19 vaccines at different intervals. Future studies are thus required to supplement our current findings to enhance vaccine uptake among children in India. Nevertheless, our study establishes the evidence towards parent’s hesitancy for getting their children vaccinated and this a immediate need to address their concerns in the coming months through targeted communication strategies.
5. Conclusions
Vaccine acceptance for COVID-19 vaccination of children in our population of health care worker parents (HCWPs) was found to satisfactory and much higher was compared to other previous studies. Majority of the HCWPs were having positive attitude towards the need and importance of COVID-19 vaccine in children, although concerns over the vaccine safety and its need were shown by some parents. Our study provides insight into determinants of vaccine acceptance, vaccine hesitancy, and trusted sources of information that may be helpful to develop targeted interventions to increase childhood COVID-19 vaccination. Further longitudinal studies to assess the trend of parental acceptance and need for timely interventions for improving the coverage of COVID-19 vaccines among children are needed.
References
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 23 December 2022).
- World Health Organization. Available online: https://covid19.who.int/region/searo/country/in (accessed on 23 December 2022).
- ` Delahoy MJ, Ujamaa D, Whitaker M, O’Halloran A, Anglin O, Burns E, et al. Hospitalizations associated with COVID-19 among children and adolescents—COVID-NET, 14 states, March 1, 2020–August 14, 2021. MMWR Morb. Mortal. Wkly Rep. 2021, 70, 1255–1260. [CrossRef] [PubMed]
- Interim statement on COVID-19 vaccination for children and adolescents. Available online: https://www.who.int/news/item/24-11-2021-interim-statement-on-covid-19-vaccination-for-children-and-adolescents (accessed on 23 December 2022).
- Centers for Disease Control and Prevention. COVID-19 Vaccination for Children. Available online: https://www.cdc.gov/vaccines/covid-19/planning/children.html (accessed on 23 December 2022).
- Ioannidis JPA. COVID-19 vaccination in children and university students. Eur J Clin Investig ation 2021, 51.
- Olson SM, Newhams MM, Halasa NB, Price AM, Boom JA, Sahni LC, et al. Effectiveness of BNT162b2 vaccine against critical Covid-19 in adolescents. N. Engl J Med. 2022, 386, 713–723. [Google Scholar] [CrossRef] [PubMed]
- Xue, F. Shen K. COVID-19 in children and the importance of COVID-19 vaccination. World J. Pediatr. 2021, 17, 462–466. [Google Scholar] [CrossRef] [PubMed]
- Zambrano LD, Newhams MM, Olson SM, Halasa NB, Price AM, Boom JA. Effectiveness of BNT162b2 (Pfizer-BioNTech) mRNA Vaccination Against Multisystem Inflammatory Syndrome in Children Among Persons Aged 12-18 Years - United States, July-December 2021. MMWR Morb Mortal Wkly Rep. 2022, 71, 52–58. [Google Scholar] [CrossRef] [PubMed]
- Klass P, Ratner AJ. Vaccinating children against covid-19 - the lessons of measles. N Engl J Med. 2021, 384, 589–591. [Google Scholar] [CrossRef]
- Lurie N, Saville M, Hatchett R, Halton J. Developing Covid-19 vaccines at pandemic speed. N Engl J Med. 2020, 382, 1969–1973. [Google Scholar] [CrossRef]
- 3 Vaccines Get Emergency Approval For Children. Available online: https://www.india.com/news/india/vaccine-for-kids-3-vaccines-get-emergency-approval-for-children-zycov-d-corbevax-covaxin-dcgi-green-signal-read-details-5358986/ (accessed on 23 December 2022).
- The Times of India. Beneficiaries in 15-18 yrs age group to start getting 2nd dose. Available online: https://timesofindia.indiatimes.com/india/beneficiaries-in-15-18-yrs-age-group-to-start-getting-2nd-dose-of-covid-vaccine-from-monday/articleshow/89229669.cms (accessed on 23 December 2022).
- MacDonald, N.E. SAGE Working Group on Vaccine Hesitancy Vaccine Hesitancy: Definition, Scope and Determinants. Vaccine. 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Ten Health Issues WHO Will Tackle This Year. Available online: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019 (accessed on 23 December 2023).
- Domek, GJ, O’Leary ST, Bull S, Bronsert M, Contreras-Roldan IL, Bolaños Ventura GA, et al. Measuring Vaccine Hesitancy: Field Testing the WHO SAGE Working Group on Vaccine Hesitancy Survey Tool in Guatemala. Vaccine. 2018, 35, 5273–5281. [Google Scholar]
- Dubé E, Gagnon D, Nickels E, Jeram, S, Schuster M. Mapping Vaccine Hesitancy—Country-Specific Characteristics of a Global Phenomenon. Vaccine. 2014, 32, 6649–6654. [Google Scholar] [CrossRef]
- Zhang KC, Fang Y, Cao H, Chen H, Hu T, Chen YQ, et al. Parental Acceptability of COVID-19 Vaccination for Children Under the Age of 18 Years: Cross-Sectional Online Survey. JMIR Pediatr Parent. 2020, 3, e24827. [Google Scholar] [CrossRef] [PubMed]
- Szilagyi PG, Shah MD, Delgado JR, Thomas K, Vizueta N, Cui Y, et al. Parents’ Intentions and Perceptions About COVID-19 Vaccination for Their Children: Results From a National Survey. Pediatrics. 2021, 148, e2021052335. [Google Scholar] [CrossRef] [PubMed]
- Humble RM, Sell H, Dubé E, MacDonald NE, Robinson J, Driedger SM, et al. Canadian parents’ perceptions of COVID-19 vaccination and intention to vaccinate their children: Results from a cross-sectional national survey. Vaccine. 2021, 39, 7669–7676. [Google Scholar] [CrossRef] [PubMed]
- Hammershaimb EA, Cole LD, Liang Y, Hendrich MA, Das D, Petrin R, et al. COVID-19 Vaccine Acceptance Among US Parents: A Nationally Representative Survey. J Pediatric Infect Dis Soc. 2022, 11, 361–370. [Google Scholar] [CrossRef] [PubMed]
- Lee M, Seo S, Choi S, Park JH, Kim S, Choe YJ, et al. Parental Acceptance of COVID-19 Vaccination for Children and Its Association With Information Sufficiency and Credibility in South Korea. JAMA Netw Open. 2022, 5, e2246624. [Google Scholar] [CrossRef] [PubMed]
- Hou Z, Song K, Wang Q, Zang S, Tu S, Chantler T, Larson HJ. Childhood COVID-19 vaccine acceptance and preference from caregivers and healthcare workers in China: A survey experiment. Prev Med. 2022, 161, 107138. [Google Scholar] [CrossRef] [PubMed]
- AlKetbi LMB, Al Hosani F, Al Memari S, et al. Parents’ views on the acceptability of a COVID-19 vaccine for their children: A cross-sectional study in Abu Dhabi-United Arab Emirates. Vaccine. 2022, 40, 5562–5568. [Google Scholar] [CrossRef] [PubMed]
- Li JB, Lau EYH, Chan DKC. Why do Hong Kong parents have low intention to vaccinate their children against COVID-19? testing health belief model and theory of planned behavior in a large-scale survey. Vaccine. 2022, 40, 2772–2780. [Google Scholar] [CrossRef]
- Bianco A, Della Polla G, Angelillo S, Pelullo CP, Licata F, Angelillo IF. Parental COVID-19 vaccine hesitancy: a cross-sectional survey in Italy. Expert Rev Vaccines. 2022, 21, 541–547. [Google Scholar] [CrossRef]
- Yılmaz, M, Sahin, MK. Parents’ willingness and attitudes concerning the COVID-19 vaccine: A cross-sectional study. Int J Clin Pract. 2021, 75, e14364. [Google Scholar]
- Mohammed AH, Hassan BAR, Wayyes AM, Gadhban AQ, Blebil A, Alhija SA, Darwish RM, Al-Zaabi AT, Othman G, Jaber AAS, Al Shouli BA, Dujaili J, Al-Ani OA, Muthanna FMS. Parental health beliefs, intention, and strategies about COVID-19 vaccine for their children: A cross-sectional analysis from five Arab countries in the Middle East. Vaccine. 2022, 40, 6549–6557. [Google Scholar] [CrossRef] [PubMed]
- Khan YH, Rasheed M, Mallhi TH, Salman M, Alzarea AI, Alanazi AS, Alotaibi NH, Khan SU, Alatawi AD, Butt MH, Alzarea SI, Alharbi KS, Alharthi SS, Algarni MA, Alahmari AK, Almalki ZS, Iqbal MS. Barriers and facilitators of childhood COVID-19 vaccination among parents: A systematic review. Front Pediatr. 2022, 10, 950406. [Google Scholar] [CrossRef] [PubMed]
- Xin Shen, Hao Dong, Jing Feng, Heng Jiang, Rowan Dowling, Zuxun Lu, Chuanzhu Lv & Yong Gan. Assessing the COVID-19 vaccine hesitancy in the Chinese adults using a generalized vaccine hesitancy survey instrument. Human Vaccines & Immunotherapeutics 2021, 17, 4005–4012. [Google Scholar]
- Boston, 677 Huntington Avenue; Ma 02115 +1495-1000 Barry, R. Bloom’s Faculty Website. Available online: https://www.hsph. harvard.edu/barry-bloom/.
- Orenstein WA, Ahmed R. Simply put: Vaccination saves lives. Proc Natl Acad Sci U S A. 2017, 114, 4031–4033. [Google Scholar] [CrossRef] [PubMed]
- Trogen B, Pirofski LA. Understanding vaccine hesitancy in COVID-19. Med (N Y). 2021, 2, 498–501. [Google Scholar]
- Razai M S, Chaudhry U A R, Doerholt K, Bauld L, Majeed A. Covid-19 vaccination hesitancy. BMJ 2021, 373, n1138. [Google Scholar]
- Toth-Manikowski SM, Swirsky ES, Gandhi R, Piscitello G. COVID-19 vaccination hesitancy among health care workers, communication, and policy-making. Am J Infect Control. 2022, 50, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Chandani S, Jani D, Sahu PK, Kataria U, Suryawanshi S, Khubchandani J, et al. COVID-19 vaccination hesitancy in India: State of the nation and priorities for research. Brain Behav Immun Health. 2021, 18, 100375. [Google Scholar] [CrossRef] [PubMed]
- Padhi BK, Satapathy P, Rajagopal V, Rustagi N, Vij J, Jain L, et al. Parents’ Perceptions and Intention to Vaccinate Their Children Against COVID-19: Results From a Cross-Sectional National Survey in India. Front. Med. 2022, 9, 806702. [Google Scholar] [CrossRef]
- Mohan R, Pandey V, Kumar A, Gangadevi P, Goel AD, Joseph J, et al. Acceptance and Attitude of Parents Regarding COVID-19 Vaccine for Children: A Cross-Sectional Study. Cureus. 2022, 14, e24518. [Google Scholar]
- Sarkar P, Chandrasekaran V, Gunasekaran D, Chinnakali P. COVID-19 vaccine hesitancy among health care worker-parents (HCWP) in Puducherry, India and its implications on their children: A cross sectional descriptive study. Vaccine. 2022, 40, 5821–5827. [Google Scholar] [CrossRef] [PubMed]
- Himanshi, KADAM KS, Uttarwar PU. COVID-19 VACCINE HESITANCY FOR CHILDREN IN PARENTS: A CROSS-SECTIONAL SURVEY AMONG HEALTH-CARE PROFESSIONALS IN INDIA. Asian Journal of Pharmaceutical and Clinical Research. 2022, 15, 41–45. [Google Scholar]
- Lazarus J, Wyka K, White T, Picchio C, Gostin L, Larson H, et al. A survey of COVID-19 vaccine acceptance across 23 countries in 2022. Nature Medicine 2023, 1–10.
- Zhou X, Wang S, Zhang K, Chen S, Chan PS, Fang Y, et al. Changes in Parents’ COVID-19 Vaccine Hesitancy for Children Aged 3-17 Years before and after the Rollout of the National Childhood COVID-19 Vaccination Program in China: Repeated Cross-Sectional Surveys. Vaccines (Basel). 2022, 10, 1478. [Google Scholar] [CrossRef] [PubMed]
- Shati AA, Al-Qahtani SM, Alsabaani AA, Mahmood SE, Alqahtani YA, AlQahtani, KM, et al. Perceptions of Parents towards COVID-19 Vaccination in Children, Aseer Region, Southwestern Saudi Arabia. Vaccines 2022, 10, 1222. [Google Scholar] [CrossRef]
- Yigit M, Ozkaya-Parlakay A, Senel E. Evaluation of COVID-19 Vaccine Refusal in Parents. Pediatr Infect Dis J. 2021, 40, e134–e136. [Google Scholar] [CrossRef]
Figure 2.
Willingness of the HCW parents to get their children vaccinated with COVID 19 vaccine (n=388).
Figure 2.
Willingness of the HCW parents to get their children vaccinated with COVID 19 vaccine (n=388).
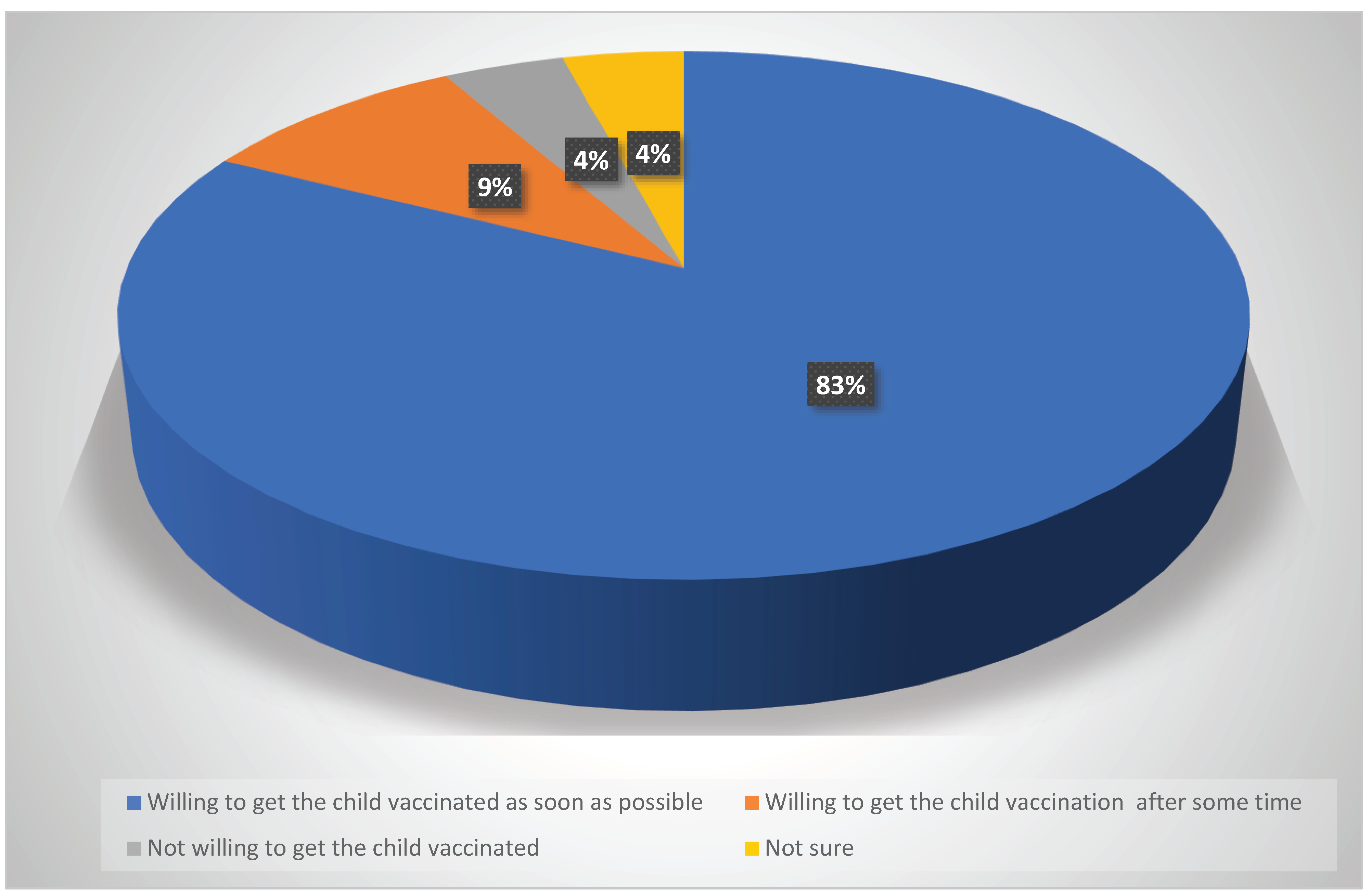
Figure 3.
Reasons given by the participants for their unwillingness for Child vaccination against COVID-19 (n=16).
Figure 3.
Reasons given by the participants for their unwillingness for Child vaccination against COVID-19 (n=16).
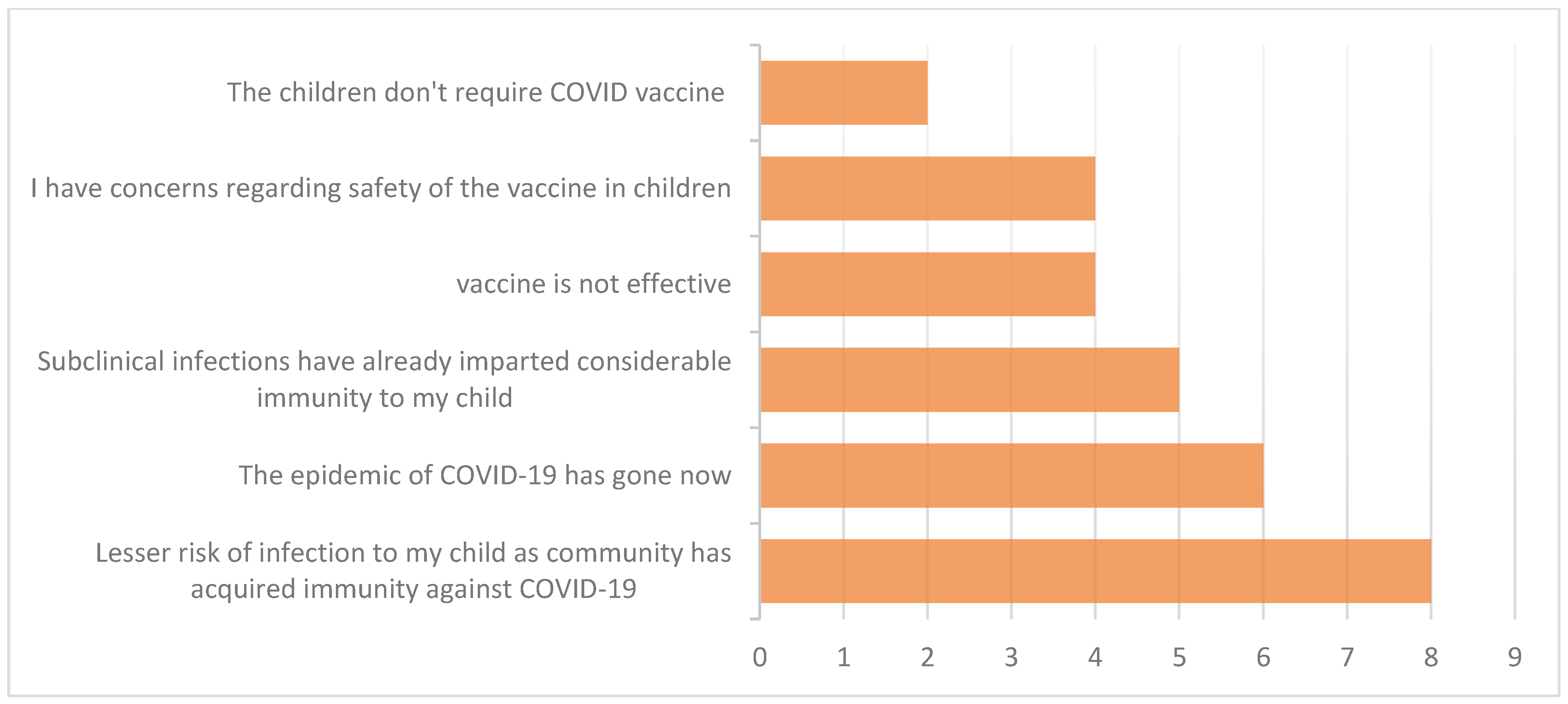
Table 1.
General characteristics of Healthcare workers-parents (HCWPs) and their children (n=388).
| Variables | Frequency (n) | Percentage (%) |
|---|---|---|
|
Age-groups( in years) 18-29 years 30-39 40-49 50-59 ≥ 60 |
04 180 172 24 08 |
1.0 46.4 44.3 6.3 2.0 |
|
Gender Male Female |
152 236 |
39.2 60.8 |
|
Religion Hindu Muslim Christian Others |
344 24 12 8 |
88.6 6.2 3.1 2.1 |
|
Marital status Currently married Widowed/Divorced/Separated |
380 08 |
97.9 2.1 |
|
Place of residence Urban Rural |
228 160 |
58.8 41.2 |
|
Highest level of Education Up to Matriculation Intermediate (10+2)/Diploma Graduate Postgraduate & Above |
156 20 108 104 |
40.2 5.1 26.8 27.8 |
|
Designation Doctor Nursing officer/Technician OPD/Ward/Lab/Sanitary attendant Security staff |
124 80 164 16 |
32.0 20.6 42.3 4.1 |
|
Monthly income(in INR) <10,000 10,000-49,999 50,000-99,999 ≥100,000 |
164 108 40 76 |
42.3 27.8 10.3 19.6 |
|
History of any chronic illness Present Absent |
32 356 |
91.7 8.3 |
|
History of Lab confirmed COVID-19 infection Yes No |
192 196 |
49.5 51.5 |
|
History of Hospitalization due to COVID-19 Yes No No history of COVID-19 |
12 180 196 |
6.3 43.2 51.5 |
|
COVID-19 Vaccination status Received 2 doses & 1 booster dose Received 2 doses Received 1 dose Not vaccinated |
292 84 8 4 |
75.3 21.6 2.1 1.0 |
|
History of any adverse event post COVID-19 vaccine Present Absent |
124 264 |
31.9 68.1 |
|
Primary source of information for COVID-19 vaccine Workplace Traditional media (TV, Radio, Newspaper) Social & Online Media Family & friends |
212 100 64 12 |
54.6 25.8 16.5 3.1 |
|
History of any child testing positive for COVID-19 Present Absent |
40 348 |
10.3 89.7 |
|
Distribution of participants by no. of child(<18 years) Have 1 child Have 2 child Have 3 child |
188 132 68 |
48.4 43.3 33.0 |
|
Age-groups of the children(in years) 12-17 <12 |
312 294 |
51.5 48.5 |
|
Gender of the children Male Female |
346 260 |
57.1 42.1 |
|
History of any child testing positive for COVID-19 Present Absent |
40 348 |
10.3 89.7 |
|
The child/children up-to-date with routine childhood vaccines Yes No/Not sure |
344 42 |
88.7 11.3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



