
Submitted:
25 January 2023
Posted:
28 January 2023
You are already at the latest version
Abstract
Polyacetylene phytochemicals are emerging as potentially responsible for the chemoprotective effects of consuming apiaceous vegetables. There is some evidence suggesting that polyacetylenes impact carcinogenesis by influencing a wide variety of signalling pathways, which are important in regulating inflammation, apoptosis, cell cycle regulation, etc. Studies have shown a correlation between human dietary intake of polyacetylene-rich vegetables with reduced risk of inflammation and cancer. Polyacetylene supplementation can influence cell growth, gene expression, and immunological responses, and reduce tumour number in rat and mouse models. Cancer chemoprevention by dietary polyacetylenes involves several mechanisms, including effects on inflammatory cytokines, the NF-κB pathway, antioxidant response elements, UPR pathway, growth factor signalling, cell cycle progression, and apoptosis. This review summarises the published research on falcarinol-type polyacetylene compounds and their mechanisms of action regarding cancer chemoprevention and treatment, and also identifies some gaps in our current understanding of the health benefits of these polyacetylenes.
Keywords:
polyacetylenes
; phytochemicals
; anti-inflammatory
; anticancer.
1. Introduction
Numerous studies have indicated the beneficial impact of eating vegetables and fruits on human health in preventing chronic diseases including cancer, which is one of the major causes of death around the world [1]. Polyacetylenes are a class of chemicals defined by the presence of two or more carbon-carbon triple bonds in the carbonic skeleton [2]. Falcarinol-type polyacetylenes (PA) are biologically active compounds widely found in plants in the Apiaceae family, such as carrots, celery and parsley, and the Araliaceae family, such as ginseng. Carrot is the main dietary source of polyacetylenic oxylipins, including falcarinol (FaOH), falcarindiol (FaDOH) and falcarindiol 3-acetate (FaDOH3Ac) (Figure 1), with FaOH serving as the intermediate metabolite of polyacetylene, from which the other forms are generated [3,4,5]. Carrots have been studied for their nutritional value, in addition to their disease-curative effects, for almost 90 years [6]. Carrot is a rich source of the vitamin A precursor β -carotene and also provides some potentially beneficial dietary fibre. Carrot also contains important phytochemicals including carotenoids, phenolics, polyacetylenes, isocoumarins, terpenes and sesquiterpenes, many of which have been extensively investigated for potential therapeutic properties against a wide range of diseases including cancer, cardiovascular disease, diabetes, anaemia, colitis, ocular diseases and obesity [7]. Ginseng is rich in polyacetylenes; in addition to falcarinol (also called panaxynol) they include panaxydiol and panaxydol (Figure 1) [8], which also have anti-inflammatory, antioxidant, and anti-cancer properties [9,10,11].
β -carotene was initially believed to be protective against multiple chronic diseases, particularly cardiovascular disease, and cancer of the lung; gastrointestinal tract; and pancreas, in addition to cataracts and age-related macular degeneration [12,13,14]. However, meta-analyses of subsequent intervention studies ruled out a role of β -carotene in suppressing lung cancer development, since dietary supplementation with purified beta-carotene failed to reduce lung cancer incidence and even increased the risk of lung cancer [15]. Thus, other bioactive substances such as polyacetylenes (FaOH and FaDOH) could be responsible for the health benefits of carrot [16] with evidence supporting that polyacetylene compounds improve human health by stimulating anti-cancer and anti-inflammatory mechanisms [3].
Recent research suggested that the anti-cancer role of certain foods might be attributed to their anti-inflammatory function. Root vegetables, and particularly purple carrots, are promising research subjects in this respect. By reducing the levels of proinflammatory cytokines including TNF-α and IL-6, purple carrots reduced intestinal inflammation in colitic mice [17]. The anti-inflammatory properties of purple carrots was suggested to be due to the high levels of anthocyanin pigments [17]; however, another study showed that polyacetylenes, not anthocyanins, are responsible for the anti-inflammatory bioactivity of purple carrots [18].
Several studies have examined the dietary compounds in the context of cancer chemoprevention. Several phytochemicals have shown potent cancer-preventive properties [19]. Phytochemicals have been the main sources of lead structures for conventional drugs for cure of cancer. It is estimated that approximately 60% of most effective anti-tumour and anti-infection drugs already on the market or under clinical investigations are compounds derived from natural products [20]. This review focuses on possible mechanisms of action of polyacetylenes in inflammation and cancer, with emphasis on various pathways involved including growth factor signalling, inflammatory processes, oxidative stress, cell cycle progression, and apoptosis. We will also discuss the potential polyacetylene components known to modulate one or more of these pathways to contribute toward treatment or prevention of inflammation and cancers.
2. Polyacetylenes and Inflammation
2.1. Chronic Inflammation Disease and Cancer
Chronic inflammation is recognized as a leading promoting factor of many diseases including carcinogenesis [21], which continues to be the leading cause of mortality and disability around the world [22,23]. Inflammation was proposed as the seventh hallmark of cancer in 2009 [24]. Cancer and inflammation are linked by intrinsic and extrinsic pathways. Intrinsically, oncogenes regulate the inflammatory microenvironment, whereas extrinsically, the inflammatory microenvironment promotes the growth and spread of cancer [25]. Many of the cell types involved in chronic inflammation can be found in tumours, both in the surrounding stroma and within the tumour itself. Many neoplasms, including some of epithelial origin, contain a significant inflammatory cell component [26]. Multiple studies on human clinical samples reveal that inflammation influences epithelial cell turnover [27,28]. Significantly, human susceptibility to breast, liver, large bowel, bladder, prostate, gastric mucosa, ovary, and skin carcinoma are increased when proliferation occurs in the context of chronic inflammation [27,28,29,30,31,32].
Chronic inflammation is linked to approximately 25% of all human cancers and increases cancer risks [33] by stimulating angiogenesis and cell proliferation, inducing gene mutations and/or inhibiting apoptosis [33]. Chronic inflammation can develop from acute inflammation if the irritant persists, although in most cases the response is chronic from the start. Chronic inflammation is characterized by the infiltration of injured tissue by mononuclear cells such as macrophages, lymphocytes, and plasma cells, as well as tissue destruction and attempts at repair [26]. Helicobacter pylori infections in gastric cancer, human papillomavirus infections in cervical cancer, hepatitis B or C infections in hepatocellular carcinoma, and inflammatory bowel disease in colorectal cancer (CRC) are common causes of chronic inflammation associated with cancer development [34,35]. Inflammation also causes epigenetic changes that are linked to cancer development. Natural polyacetylenes from numerous food and medicinal plants and their derivatives exerted multiple bioactivities, including anti-inflammatory properties [36]. Polyacetylene components can impact the inflammation through several known and unknown pathways.
2.1.1. Inhibition of Nuclear Factor kappa B (NF-κB) Pathways
NF-κB is a transcription factor that regulates the expression of many genes involved in the regulation of inflammation and autoimmune diseases [37,38]. Moreover, NF-κB plays a significant role in inflammation-induced cancers, as NF-κB is one of the major inflammatory pathways that are triggered by, for example, infections causing chronic inflammation [34,35,39]. Cellular immunity, inflammation, and stress are all regulated by NF-κB signalling, as are cell differentiation, proliferation, and apoptosis (Figure 2) [40,41]. Both solid and hematologic malignancies frequently modify the NF-κB pathway in ways that promote tumour cell proliferation and survival [42,43,44].
NF-κB, a key factor in the inflammatory process, provides a mechanistic link between inflammation and cancer and the components of this pathway are targets for chemoprevention, particularly in CRC [45]. There are two major signalling pathways for NF-κB activation, which are the canonical and the non-canonical NF-κB signalling pathways. The canonical pathway activates NF-κB1 p50, RELA and c-REL, which are also called canonical NF-κB family members. The non-canonical NF-κB pathway, on the other hand, selectively activates p100-sequestered NF-κB members, mostly NF-κB2 p52 and RELB, which are also called non-canonical NF-κB family members [46]. LPS and proinflammatory cytokines, among other pathogenic substances, activate NF-κB through degrading Inhibitor of κB (IκBs) [47] to release the common subunit P65 (RELA). In order to trigger the transcription of these genes, activated NF-κB travels into the nucleus and attaches to its associated DNA motifs. When activated, NF-κB p65 subunit binds to promoter regions of genes involved in inflammation, leading to the production of IL-6, IL-1β, and TNF-α [48].
The carrot polyacetylenes, particularly (FaOH and FaDOH), the most abundant polyacetylenes in carrot, have been shown to reduce inflammation [3,49], in part by inhibiting the transcription factor NF-κB [50]. Mice fed a diet containing FaOH were less likely to develop severe inflammation after being exposed to LPS [5]. FaOH from ginseng significantly reduced the LPS induced TNF-α and IL-6 in cultured BV-2 microglia cells and murine serum [47]. It has been demonstrated that FaOH and FaDOH purified from carrots have preventative effects on colorectal precancerous lesions in azoxymethane (AOM)-induced rats. Biopsies of neoplastic tissue were analysed for gene expression and the results showed that FaOH and FaDOH inhibited NF-κB and the downstream inflammatory markers TNF-α, IL-6, and COX-2 [51]. A recent study has shown that FaOH from Radix Saposhnikoviae (dried roots of Saposhnikovia divaricata, Apiaceae), inhibited LPS-induced NF-κB p65 activation and IκB-α phosphorylation in BV-2 microglia cells [47]. Treatment using FaOH from the roots of Heracleum moellendorffii inhibited LPS-induced NF-κB signalling activation by inhibiting IκB-α degradation and nuclear accumulation of p65 [52] on RAW264.7 cells. In addition, FaDOH reduced level of LPS/IFNγ-induced NF-κB, IKK-α and IKK-β activation on rat primary astrocytes [50].
Prostaglandin (PG) synthesis is a hallmark of inflammation. Two enzymes, cyclooxygenase (COX) 1 and 2, catalyse the first step of PG synthesis, but COX-2 is the major one that responds to inflammatory signal to produce PG at inflammatory sites [53]. However, COX-2 can be suppressed by inhibiting the NF-kB translocation pathway (Figure 2) [54]. COX-2 expressions in healthy tissues are low, but can quickly increase in response to growth factors, cytokines, and signals promoting tumour invasion, metastasis, aberrant proliferation, and angiogenesis [55]. Many malignancies, including colorectal [56], bladder [57], breast [58], lung [59], pancreatic [60], prostate [60], and head and neck cancer [61], have been shown to be associated with elevated levels of COX-2. Mechanistically, COX-2 promotes carcinogenesis through the creation of prostaglandins (PGs), which suppress apoptosis and stimulate the development of blood vessels in tumour tissue which help sustaining tumour cell viability and growth [34,62], suggesting that anti-inflammatory drugs targeting COX-2 might be beneficiary in the treatment of many types of cancer.
It has been demonstrated that polyacetylenes modulate inflammation via suppressing COX-2, whose expression depends on NF-κB activation by inflammation [63]. FaOH inhibited LPS-induced COX-2 expression in RAW264.7 cells thus blocking PGE2 overproduction [52]. FaOH isolated from American ginseng effectively reduced the severity of colitis in mice treated with Dextran Sulfate Sodium (DSS). FaOH treatment prior to DSS did not prevent colitis in mice but FaOH decreased COX-2 expression level effectively when colitis was induced with DSS for one week then followed by FaOH treatment, suggesting that the polyacetylene component does have a therapeutic effect on colitis [8]. Moreover, in azoxymethane (AOM)-induced rats colorectal cancer model, FaOH and FaDOH downregulated COX-2 in precancerous lesions of colorectal cancer (CRC) [51] and also reduced the number of malignant tumour foci.
2.2. Oxidative Stress
2.2.1. Inhibition of Nitric oxide synthase (NOS) and Pro-inflammatory Cytokines Pathways
Nitric oxide (NO) is essential in a number of physiological functions, such as host defence, where it prevents the spread of disease-causing microbes within cells by stifling their reproduction [64]. The upregulation of NO expression in response to cytokines or pathogen-derived chemicals is a crucial part of the host's defence against many different types of intracellular pathogens. It has been shown that many different cell types produce the enzyme NOS, which catalyses the synthesis of NO, at high levels in a number of different tumour types [65]. Inflammation induces a specific form of NOS, inducible isoform of Nitric Oxide Synthase (iNOS), via activating iNOS gene transcription (Figure 2) [66]. iNOS is involved in complex immunomodulatory and antitumor mechanisms, which have been shown to kill bacteria, viruses, and parasites [67].
A considerable amount of literature has been published on the role of polyacetylenes on iNOS expression in inflammation. Studies have demonstrated panaxydiol and panaxydol extracted from American ginseng inhibited iNOS expression in ANA-1 mФ macrophage cells polarized to M1 [8] and LPS-induced iNOS expression in macrophages [68,69] leading to colitis suppression [8]. Moreover, FaDOH was tested on rat primary astrocytes for its impact on LPS/IFN-γ -induced iNOS expression. FaDOH blocked 80% of LPS/IFN-γ -induced iNOS by reducing iNOS protein and mRNA in a dose-dependent manner. FaDOH was shown to suppress iNOS expression and inhibited IKK, JAK, NF-κB, and Stat1 [50].
Another study showed dose-dependent reduction of nitric oxide production in macrophage cells, where treatment with an extract of purple carrots containing polyacetylenes significantly reduced iNOS activity and iNOS expression in macrophage cells [18]. Polyacetylenes reduced nitric oxide production in macrophage cells without cytotoxicity [18]. In vivo, purple carrots also inhibited inflammation in colitic mice and reduced colonic mRNA expression of iNOS [17]. FaOH from Heracleum moellendorffii roots has been tested on RAW264.7 cells and found to inhibit LPS-induced overexpression iNOS [52]. FaOH and other polyacetylenes from American ginseng such as panaxydiol have suppressive effect of iNOS expression in macrophages treated with LPS [69].
2.2.2. Reactive Oxygen Species (ROS) Pathways
Oxidative stress is described as an imbalance between the generation of free radicals and reactive metabolites, also known as oxidants or reactive oxygen species (ROS), and their removal by protective mechanisms, also known as antioxidants. Electron transfer is involved in oxidative and antioxidative processes, which influence the redox state of cells and the organism. The altered redox state stimulates or inhibits the activities of various signal proteins, which have the effect on cell fate [70,71]. It has been demonstrated that polyacetylenes promote apoptosis preferentially in cancer cells mediated ROS stress. A study has analysed ROS production in MCF-7 cells after treating with panaxydol. The increase of the ROS levels starts at 10–20 min after panaxydol treatment. The role of NADPH oxidase was investigated in order to determine the source of ROS after panaxydol treatment. The creation of reactive oxygen species (ROS) by NADPH oxidase appeared to take precedence, while ROS production in the mitochondria was secondary but also necessary, suggesting that NADPH oxidase generates ROS in the presence of panaxydol. Different cell lines have been tested to check whether the induction of apoptosis by panaxydol occurred preferentially in cancer cells. Indeed, panaxydol induced apoptosis only in cancer cells [72].
FaOH and FaDOH from carrot were tested for their effects on the oxidative stress responses of primary myotube cultures. The effects of 100μM H2O2 on the intracellular formation of ROS, transcription of the antioxidative enzyme, cytosolic glutathione peroxidase (cGPx), the heat shock proteins (HSP) HSP70 and heme oxygenase 1 (HO1) were studied after 24 h treatment with FaOH and FaDOH at a wide range of concentrations. At intermediate concentrations, under which only moderately cytotoxic were shown, intracellular ROS formation was slightly enhanced by polyacetylenes. In addition, polyacetylenes increased transcription of cGPx and decreased the transcription of HSP70 and HO1. The enhanced cGPx transcription may have decreased the need for the HSPs protective properties as an adaptive response to the elevated ROS production. However, ROS production was significantly reduced with higher doses of polyacetylenes (causing substantial cytoxicity), and the reducing in transcription of HSP70 and HO1 decreased to a less extent while induction of cGPx was marginally reduced, showing a necessity for the HSPs protective and repairing functions [73].
Transcription factor Nrf2 (also known as nuclear factor erythroid 2-like 2) regulates the expression of numerous antioxidant, anti-inflammatory, and cytoprotective factors, including heme oxygenase-1 (Hmox1, HO-1) and NADPH:quinone oxidoreductase-1 (Nqo1). S-alkylation of the protein Keap1, which normally inhibits Nrf2, is induced by FaDOH, as reported in [74]. Moreover, nuclear accumulation of Nrf2 and expression of HO-1 were both enhanced in LPS-stimulated RAW264.7 cells by FaOH from Heracleum moellendorffii roots [52]. FaOH also inhibited the inflammatory factor level and reduced the nitric oxide production in BV-2 microglia. FaOH also reduced levels of LPS induced oxidative stress in BV-2 microglia [47]. HO-1 has been linked to redox-regulated gene expression. Chemical and physical stimuli that produce ROS either directly or indirectly cause the expression of HO-1 to respond [75]. A one-week study looked at the effects of FaOH (5 mg/kg twice per day in CB57BL/6 mice) pretreatment on acute intestinal and systemic inflammation. FaOH effectively increased HO-1 mRNA and protein levels in both the mouse liver and intestine and reduced the levels of the plasma chemokine eotaxin and the myeloid inflammatory cell growth factor GM-CSF, both of which are involved in the recruitment and maintenance of first-responder immune cells [76].
2.3. Unfolded Protein Response (UPR) Pathways
The endoplasmic reticulum (ER) stress response, also known as unfolded protein response (UPR), is a cellular process that is activated by a number of conditions that disrupt protein folding in the ER. The UPR is an evolutionarily conserved adaptive mechanism in eukaryotic cells that aims to clear unfolded proteins and restore ER protein homeostasis. When ER stress is irreversible, cellular functions deteriorate, often leading to cell death (Figure 2) [77]. There is mounting evidence that ER stress plays a significant role in the development and progression of numerous diseases, including cancer and inflammation [77,78]. FaDOH-induced cell death is mediated via endoplasmic reticulum (ER) stress induction and activation of the unfolded protein response (UPR).
Reducing the extent of ER stress by overexpressing the ER chaperone protein glucose-regulated protein 78 (GRP78) or by knocking down components of the UPR pathway decreased FaDOH-induced apoptosis. In contrast, raising the level of ER stress by inhibiting GRP78 enhanced the apoptosis triggered by FaDOH [79]. In addition, ER stress mediates panaxydol-induced apoptosis in MCF-7 cells [80]. Another study investigated the effect of a sub-toxic dose 5μM of FaDOH in a series of experiments, and found that this increased the lipid content and number of lipid droplets (LDs) in human mesenchymal stem cells (hMSCs) and enhanced PPARγ2 expression in human colon adenocarcinoma cells. The activation of PPARγ can enhance ABCA1 expression [81]. FaDOH treatment shows upregulation of ABCA1 in colon neoplastic rat tissue, suggesting a function for this transporter in the redistribution of lipids and enhanced creation of LDs in cancer cells, which may result in endoplasmic reticulum (ER) stress and cancer cell death [81].
3. Cancer
3.1. In vitro
3.1.1. Anti-Proliferative Activity
Polyacetylenes derived from different plants exhibit potent cytotoxicity against a variety of cancer cells. These biologically active molecules engage directly or indirectly in biological processes, including cellular cycle arrest, HIF-1 (hypoxia-inducible factor-1 alpha) activation, and signal transducer and transcriptional factor 3 (STAT3) suppression.
The anti-proliferative effects of FaOH isolated from carrots was initially shown in 2003. In addition, FaOH-type polyacetylenes has been shown to be cytotoxic against human pancreatic carcinoma cells in vitro by modulating the expression of the genes involved in apoptosis, cell cycle, stress response, and death receptors [82,83].
Treatment of leukaemia cell lines with carrot extract or isolated FaOH or FaDOH inhibited the cell cycle progression, suggesting that carrots cause cell cycle arrest (G0/G1) in leukaemia cell lines [84]. Moreover, cytotoxicity of FaOH, FaDOH and panaxydiol isolated from the dichloromethane extract of root celery were tested for their potential impact in a number of human cancer and leukaemia cell lines. All polyacetylenes examined exhibited moderate cytotoxicity against leukaemia, lymphoma, and myeloma cell lines. Although FaOH had significantly more activity against the lymphocytic leukaemia cells than FaDOH and panaxydiol [85]. In other studies, FaDOH also had less cytotoxic activity than FaOH and FaDOH3Ac [84,86].
3.1.2. Pro-apoptosis Activity
Cancer prevention and treatment depend on the use of a variety of bioactive compounds that inhibit the early stages of cellular transformation required for the development of the neoplastic phenotype, such as initiating autophagy, apoptosis, or other forms of cell death such as oncosis or necrosis [87]. Apoptosis dysfunction is a major contributor to cancer development and progression. Tumour cells' ability to avoid apoptosis can play a significant role in their resistance to traditional therapies.
FaOH has been studied on human pancreatic ductal adenocarcinoma cell lines and found to regulate genes related to pro-apoptosis, anti-apoptosis, apoptosis, cell cycle, stress-related, and death receptors. FaOH suppressed pro-apoptosis genes (BAD, HTRA-2), anti-apoptosis genes (Livin, XIAP), cell cycle controller (Phospho-p53 at animo acids serine 15, 46 and 392 (S15, S46 & S392), stress-related genes (Clusterin, Hsp60) and death receptor gene (TNFR1, TNFSF1A). In addition, FaOH increased cell cycle checkpoint phosphorylation (Phospho-Rad17 (S635)) and induced stress-related genes (HO-1, HMXO1, HP32, Hsp27). Furthermore, FaOH-type and other polyacetylene components are potent inhibitors of pancreatic cancer cell proliferation [82].
Tumour recurrence and drug resistance are both facilitated by cancer stem-like cells (CSCs) [88]. Hsp90 is known to enhance cancer cell survival and ability to acquire anti-cancer drug resistance; overexpression of Hsp90 has been reported in numerous human malignancies to be associated with poor prognosis [89,90]. An in vivo study showed that orally administered FaOH significantly suppressed the proliferation of lung cancer in a mouse model without overt symptoms of toxicity at concentrations of 50 mg/kg body weight [88], which would correspond to a human dose of 4 mg/kg [91]. FaOH inhibited carcinogenesis both in vitro and in vivo by inhibiting the function and viability of cancer stem-like cells of non-small-cell lung cancer by triggering apoptosis without enhancing Hsp70 expression. Moreover, FaOH, at the low dose of 1 µM, induced apoptosis in cancer stem-like cells [88].
3.1.3. Gut microbiota composition
A study aimed to investigate whether antibacterial effects of FaOH and FaDOH may be a mechanism of action in the antineoplastic property of FaOH and FaDOH. They tested the effect of FaOH and FaDOH on gut microbiota composition in the AOM induced rat colorectal cancer model. Rats treated with AOM were fed either a normal rat diet or diet enriched with FaOH and FaDOH. Analysis of cecum faecal samples revealed a significant change in the gut microbiota among the groups. FaOH and FaDOH, which have been found to suppress the growth of neoplastic tumours in the colon in a rat colon cancer model, modify the composition of low abundant gut microbiota GM members such as Lactobacillus reuteri and high prevalence of Turicibacter, which is also correlated with a reduction in the number of macroscopic sites of neoplasms. Thus, this study has demonstrated that modifications in the gut microbiota may play a significant role in the colon-protective action of FaOH and FaDOH against neoplastic transformation [92].
3.1.4. Other Effects
FaOH stimulated differentiation of primary mammalian cells at concentrations as low as 0.004 to 0.4µM, whereas cytotoxic effects were observed at concentrations of > 4µM, [93]. Moreover, a study has evaluated polyacetylenes (FaOH and FaDOH) isolated from carrots in non-cancerous human intestinal epithelial cells (FHs 74 Int. cells) and intestinal cancer cells (CaCo-2). The growth-inhibition response was seen in concentrations above 1μg/mL (~4μM) with maximum inhibition at 20μg/mL(~80μM). The FaOH showed higher inhibitory potency in comparing with FaDOH. In addition, cancer cells treated with combinations of FaOH and FaDOH has showed a synergistic response for the inhibition of cell growth [94]. FaOH purified from carrots inhibited caspase-3 expression to prevent cell death and reduced basal DNA strand breakage in CaCo-2 cells. Thus, FaOH is either pro-survival or pro-death at a concentration dependent manner in CaCo-2 cells [95].
Polyacetylenes have other effects with relevance for cancer. Polyacetylenes can be used to heal or relieve symptoms by interacting with other foods or drugs. Cisplatin, which has nephrotoxicity as a side effect, is a therapeutic drug for various solid tumours. FaDOH has been found to attenuate cisplatin-induced injury and down-regulate mRNA levels of TNF-α, IL-1β and protein expression of p-NF-kB p65 in mice [96].
Another study has demonstrated the effects of FaOH, FaDOH, FaDOH3Ac, and falcarindiol 3,8-diacetate on breast cancer multidrug resistance protein (BCRP/ABCG2), a xenobiotic efflux transporter causing chemotherapy resistance in cancer. Polyacetylenes inhibited mitoxantrone efflux (an ABCG2 substrate) in HEK293 cells overexpressing ABCG2. In a vesicular transport assay, concentration-dependent inhibition of methotrexate (another ABCG2 substrate) uptake into ABCG2-overexpressing Sf9 insect cell membrane vesicles was observed. Polyacetylenes also inhibited baseline and sulfasalazine-stimulated vanadate-sensitive ATPase activities in ABCG2-overexpressing Sf9 insect cell membrane vesicles. This study suggested that polyacetylenes might mitigate multidrug resistance in chemotherapy. As ABCG2 may play a role in the absorption and disposition of polyacetylenes, there may be food-drug interactions between polyacetylene-rich foods and ABCG2 substrate drugs [97].
3.2. In vivo
In a prospective cohort study including 57,053 Danes, intake of 2–4 or more raw carrots each week (>32 g/day) was associated with a 17% reduced in risk of colorectal cancer compared to individuals with no intake of raw carrots [98]. Moreover, consumption of carrot powder reduced the growth of intestinal tumours in the ApcMin mouse colon cancer model [99]. A study examined colon preneoplastic lesions in AOM-treated rats fed carrots (10% freeze-dried carrot with a natural concentration of FaOH at 35 µg/g); FaOH (purified FaOH mixed at 3.5 µg/g in food); or control, for 18 weeks. Compared to the control group, the number and size of lesions decreased significantly in rats that received either one of the two experimental treatments, compared to the control group. The study found that carrots and FaOH can slow the growth of aberrant crypt foci (ACF) and tumours [100]. In a similar study, again using AOM-treated rats as a colon cancer model, feed containing a mixture of FaOH and FaDOH at concentrations 4 times higher than the previous study, significantly reduced the number of tumours >1mm, from 21 in controls to 12 in polyacetylene-treated rats [101]. An inverse correlation was found between higher intake of a combination of FaOH and FaDOH with multiplicity of colorectal neoplastic lesions [51]. These studies support the hypothesis that diets rich in FaOH and FaDOH can be a preventive treatment of colorectal cancer. A human dose of polyacetylenes corresponding to the 2017 rat experiment would be 24mg per day for a 70kg person, which could be provided by consuming 260g per day of the cultivated carrot cultivar ‘Nantes Empire’ [101].
Polyacetylenes from ginseng have shown selective tumour killing activities similar to chemotherapeutic agents. Panaxydol isolated from Panax ginseng inhibited tumour growth in mouse tumour models, including PC3 human prostate cancer xenograft and mouse renal carcinoma (Renca) cells. BALB/c nude mice bearing PC3 or Renca cells tumour were injected with panaxydol every two days for a course of three-weeks. Panaxydol inhibited growth of the PC3 xenograft dose-dependently, with complete suppression at 100 mg/kg. In addition, panaxydol also reduced Renca tumour size in dose-dependent manner, demonstrating that panaxydol has an anticancer effect in vivo [80].
4. Polyacetylene Toxicology
Polyacetylenes in high concentrations could have some toxic effects which may depend on cell sensitivity. In in vitro studies, FaOH has cytotoxic activity against several intestinal cell lines at the concentrations 4 µM [93] and 10 μM [94]. In addition, FaDOH has shown a toxic activity in human colon adenocarcinoma (HT-29) cells in concentrations >50µM, while it exhibited a toxic effect on human mesenchymal stem (hMSC) cells in concentrations >20µM [81]. In another study, FaDOH and panaxydol have shown toxicity at concentrations of 40μM [94]. In addition, FaOH showed neurotoxic effects at high concentration (LD50=100 mg/kg) when injected into mice [102] whereas FaDOH had no neurotoxic effects in rats when injected with similar concentrations (LD50 >200 mg/kg) [103]. Mammals have not been observed to be poisoned after voluntary consumption of falcarinol-type polyacetylenes in natural sources; this is probably related with the bitter taste of polyacetylenes, in particular FaDOH, which causes a bitter or burning sensation when occurring in concentrations >40µM [104], thus preventing the eating of unsafe amounts of vegetables with too high levels of these polyacetylenes. This contrasts with other types of polyacetylenes, such as oenanthotoxin found in the neurotoxic plant hemlock water-dropwort [105]. However, while the falcarinol-type polyacetylenes can also cause neurotoxic symptoms, this requires much higher concentrations than occur in edible plants, and therefore their presence in food plants is deemed harmless [106].
5. Conclusion
Many studies indicate that Apiaceae and Araliaceae food plants rich in polyacetylenes are important tools for cancer prevention. The findings reviewed here consistently support that polyacetylenes are anti-neoplastic natural phytochemicals with potential for advances into multiple applications in cancer prevention, treatment, and as lead compounds in the discovery of new anticancer drugs. These mechanisms of action attributed to polyacetylenes are similar to those of many other anticancer drugs, which include triggering cell cycle arrest, apoptosis, UPR and reducing inflammation but potentially with lower toxic side effects. The polyacetylene concentrations in widely consumed vegetables such as carrots are sufficiently high to potentially provide substantial chemo-preventive effect within the recommended vegetable & fruit intake of 400g per day, while at the same time sufficiently low to exclude concerns about toxicity from these dietary sources. Polyacetylenes have significant inhibitory effects on multiple cancer cell pathways reflecting their anti-proliferative and anti-tumorigenic properties.
Future studies are needed to determine the safe doses of polyacetylenes in humans, as a prerequisite for any non-food application, whether in food supplements or drugs. NF-κB pathways have been shown to be influenced by polyacetylene components, indicating their significance in terms of not only cancer prevention and treatment but also numerous other biological processes. However, future studies should focus on human intervention studies on biomarkers of inflammation in both NF-κB, UPR pathways, and other anti-cancer processes, to guide the optimisation of the implementation of affordable food-based cancer prevention programmes.
Author Contributions
Investigation, Figure design, Writing—original draft preparation, Writing—review and editing, R.A.; Supervision, Writing—review and editing, L.H.; Supervision, Writing—review and editing, K.B. All authors have read and agreed to the published version of the manuscript.
Funding
This work was funded by Qassim University, Qassim, KSA. The funder had no role in data collection, data interpretation, or writing of the review.
Data Availability Statement
Data are contained within the article.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Wang, X., et al., Fruit and vegetable consumption and mortality from all causes, cardiovascular disease, and cancer: systematic review and dose-response meta-analysis of prospective cohort studies. Postgraduate Medical Journal, 2014. 349.
- Negri, R., Polyacetylenes from terrestrial plants and fungi: recent phytochemical and biological advances. Fitoterapia, 2015. 106: p. 92-109.
- Dawid, C., et al., Bioactive C17-polyacetylenes in carrots (Daucus carota L.): current knowledge and future perspectives. Journal of Agricultural and Food Chemistry, 2015. 63(42): p. 9211-9222.
- Hansen, L. and P.M. Boll, Polyacetylenes in Araliaceae: their chemistry, biosynthesis and biological significance. Phytochemistry, 1986. 25(2): p. 285-293.
- Stefanson, A. and M. Bakovic, Dietary polyacetylene falcarinol upregulated intestinal heme oxygenase-1 and modified plasma cytokine profile in late phase lipopolysaccharide-induced acute inflammation in CB57BL/6 mice. Nutrition Research, 2020. 80: p. 89-105.
- Moore, T., Vitamin A and carotene: The association of vitamin A activity with carotene in the carrot root. Biochemical Journal, 1929. 23(4): p. 803.
- Butnariu, M., Therapeutic Properties of Vegetable. Journal of Bioequivalence & Bioavailability, 2014. 6: p. e55.
- Chaparala, A., et al., Panaxynol, a bioactive component of American ginseng, targets macrophages and suppresses colitis in mice. Oncotarget, 2020. 11(22): p. 2026.
- Cambria, C., S. Sabir, and I.C. Shorter, Ginseng. 2019.
- Hong, H., D. Baatar, and S.G. Hwang, Anticancer activities of ginsenosides, the main active components of ginseng. Evidence-Based Complementary and Alternative Medicine, 2021. 2021.
- Yang, S., et al., Ginseng root extract attenuates inflammation by inhibiting the MAPK/NF-κB signaling pathway and activating autophagy and p62-Nrf2-Keap1 signaling in vitro and in vivo. Journal of Ethnopharmacology, 2022. 283: p. 114739.
- Mares-Perlman, J.A., et al., The body of evidence to support a protective role for lutein and zeaxanthin in delaying chronic disease. Overview. The Journal of Nutrition, 2002. 132(3): p. 518S-524S.
- Sommer, A. and K.S. Vyas, A global clinical view on vitamin A and carotenoids. The American Journal of Clinical Nutrition, 2012. 96(5): p. 1204S-1206S.
- Tapiero, H., D.M. Townsend, and K.D. Tew, The role of carotenoids in the prevention of human pathologies. Biomedicine & Pharmacotherapy, 2004. 58(2): p. 100-110.
- Kordiak, J., et al., Role of Beta-Carotene in Lung Cancer Primary Chemoprevention: A Systematic Review with Meta-Analysis and Meta-Regression. Nutrients, 2022. 14(7): p. 1361.
- Brandt, K., et al., Health promoting compounds in vegetables and fruits: A systematic approach for identifying plant components with impact on human health. Trends in Food Science & Technology, 2004. 15(7-8): p. 384-393.
- Kim, Y.-J., et al., Anti-colitic effect of purple carrot on dextran sulfate sodium (DSS)-induced colitis in C57BL/6J Mice. Preventive Nutrition and Food Science, 2018. 23(1): p. 77.
- Metzger, B.T., D.M. Barnes, and J.D. Reed, Purple carrot (Daucus carota L.) polyacetylenes decrease lipopolysaccharide-induced expression of inflammatory proteins in macrophage and endothelial cells. Journal of Agricultural and Food Chemistry, 2008. 56(10): p. 3554-3560.
- Benetou, V., A. Lagiou, and P. Lagiou, Chemoprevention of cancer: Current evidence and future prospects. F1000Research, 2015. 4(F1000 Faculty Rev).
- Wang, M.-W., X. Hao, and K. Chen, Biological screening of natural products and drug innovation in China. Philosophical Transactions of the Royal Society B: Biological Sciences, 2007. 362(1482): p. 1093-1105.
- Singh, N., et al., Inflammation and cancer. Annals of African Medicine, 2019. 18(3): p. 121.
- Prasad, S., B. Sung, and B.B. Aggarwal, Age-associated chronic diseases require age-old medicine: role of chronic inflammation. Preventive Medicine, 2012. 54: p. S29-S37.
- Nasef, N.A., S. Mehta, and L.R. Ferguson, Susceptibility to chronic inflammation: an update. Archives of Toxicology, 2017. 91(3): p. 1131-1141.
- Colotta, F., et al., Cancer-related inflammation, the seventh hallmark of cancer: links to genetic instability. Carcinogenesis, 2009. 30(7): p. 1073-1081.
- Raposo, T., et al., Inflammation and cancer: till death tears them apart. The Veterinary Journal, 2015. 205(2): p. 161-174.
- Macarthur, M., G.L. Hold, and E.M. El-Omar, Inflammation and Cancer II. Role of chronic inflammation and cytokine gene polymorphisms in the pathogenesis of gastrointestinal malignancy. American Journal of Physiology-Gastrointestinal and Liver Physiology, 2004. 286(4): p. G515-G520.
- De Marzo, A.M., et al., Proliferative inflammatory atrophy of the prostate: implications for prostatic carcinogenesis. The American journal of pathology, 1999. 155(6): p. 1985-1992.
- Kuper, H., H.O. Adami, and D. Trichopoulos, Infections as a major preventable cause of human cancer. Journal of internal medicine, 2001. 249(S741): p. 61-74.
- Scholl, S., et al., Anti-colony-stimulating factor-1 antibody staining in primary breast adenocarcinomas correlates with marked inflammatory cell infiltrates and prognosis. Journal of the National Cancer Institute, 1994. 86(2): p. 120-126.
- Ernst, P.B. and B.D. Gold, The disease spectrum of Helicobacter pylori: the immunopathogenesis of gastroduodenal ulcer and gastric cancer. Annual Review of Microbiology, 2000. 54: p. 615.
- Ness, R.B. and C. Cottreau, Possible role of ovarian epithelial inflammation in ovarian cancer. Journal of the National Cancer Institute, 1999. 91(17): p. 1459-1467.
- Bröcker, E., et al., Inflammatory cell infiltrates in human melanoma at different stages of tumor progression. International Journal of Cancer, 1988. 41(4): p. 562-567.
- Kundu, J.K. and Y.-J. Surh, Inflammation: gearing the journey to cancer. Mutation Research/Reviews in Mutation Research, 2008. 659(1-2): p. 15-30.
- Coussens, L.M. and Z. Werb, Inflammation and cancer. Nature, 2002. 420(6917): p. 860-867.
- Multhoff, G., M. Molls, and J. Radons, Chronic inflammation in cancer development. Frontiers in immunology, 2012. 2: p. 98.
- Christensen, L.P., Bioactive C17 and C18 acetylenic oxylipins from terrestrial plants as potential lead compounds for anticancer drug development. Molecules, 2020. 25(11): p. 2568.
- Spooner, R. and Ö. Yilmaz, The role of reactive-oxygen-species in microbial persistence and inflammation. International journal of molecular sciences, 2011. 12(1): p. 334-352.
- Kauppinen, A., et al., Antagonistic crosstalk between NF-κB and SIRT1 in the regulation of inflammation and metabolic disorders. Cellular signalling, 2013. 25(10): p. 1939-1948.
- Crusz, S.M. and F.R. Balkwill, Inflammation and cancer: advances and new agents. Nature Reviews Clinical Ocology, 2015. 12(10): p. 584-596.
- Song, W., et al., Translational significance for tumor metastasis of tumor-associated macrophages and epithelial–mesenchymal transition. Frontiers in Immunology, 2017. 8: p. 1106.
- Kwon, H.-J., et al., Stepwise phosphorylation of p65 promotes NF-κB activation and NK cell responses during target cell recognition. Nature Communications, 2016. 7(1): p. 1-15.
- Hayden, M.S. and S. Ghosh, Shared principles in NF-κB signaling. Cell, 2008. 132(3): p. 344-362.
- Sau, A., et al., Persistent activation of NF-κB in BRCA1-deficient mammary progenitors drives aberrant proliferation and accumulation of DNA damage. Cell Stem Cell, 2016. 19(1): p. 52-65.
- Salazar, L., et al., Fibroblast growth factor receptor 3 interacts with and activates TGFβ-activated kinase 1 tyrosine phosphorylation and NFκB signaling in multiple myeloma and bladder cancer. PLoS One, 2014. 9(1): p. e86470.
- Burstein, E. and E.R. Fearon, Colitis and cancer: a tale of inflammatory cells and their cytokines. The Journal of Clinical Investigation, 2008. 118(2): p. 464-467.
- Sun, S.-C., The non-canonical NF-κB pathway in immunity and inflammation. Nature Reviews Immunology, 2017. 17(9): p. 545-558.
- Zhao, Y., et al., Study on the antidepressant effect of panaxynol through the IκB-α/NF-κB signaling pathway to inhibit the excessive activation of BV-2 microglia. Biomedicine & Pharmacotherapy, 2021. 138: p. 111387.
- Chen, T., et al., The protective effect of CDDO-Me on lipopolysaccharide-induced acute lung injury in mice. International immunopharmacology, 2015. 25(1): p. 55-64.
- Kang, H., et al., Protective effect of the methanol extract from Cryptotaenia japonica Hassk. against lipopolysaccharide-induced inflammation in vitro and in vivo. BMC Complementary and Alternative Medicine, 2012. 12(1): p. 1-7.
- Shiao, Y.-J., et al., Falcarindiol impairs the expression of inducible nitric oxide synthase by abrogating the activation of IKK and JAK in rat primary astrocytes. British journal of pharmacology, 2005. 144(1): p. 42.
- Kobaek-Larsen, M., et al., Dietary polyacetylenic oxylipins falcarinol and falcarindiol prevent inflammation and colorectal neoplastic transformation: A mechanistic and dose-response study in a rat model. Nutrients, 2019. 11(9): p. 2223.
- Kim, H.N., et al., Heracleum moellendorffii roots inhibit the production of pro-inflammatory mediators through the inhibition of NF-κB and MAPK signaling, and activation of ROS/Nrf2/HO-1 signaling in LPS-stimulated RAW264. 7 cells. BMC complementary and alternative medicine, 2019. 19(1): p. 1-10.
- Yao, C. and S. Narumiya, Prostaglandin-cytokine crosstalk in chronic inflammation. British Journal of Pharmacology, 2019. 176(3): p. 337-354.
- Lee, S., et al., Anti-inflammatory function of arctiin by inhibiting COX-2 expression via NF-κB pathways. Journal of Inflammation, 2011. 8(1): p. 1-9.
- Nagaraju, G.P. and B.F. El-Rayes, Cyclooxygenase-2 in gastrointestinal malignancies. Cancer, 2019. 125(8): p. 1221-1227.
- Ghosh, N., et al., COX-2 as a target for cancer chemotherapy. Pharmacological Reports, 2010. 62(2): p. 233-244.
- Agrawal, U., et al., Overexpression of COX2 indicates poor survival in urothelial bladder cancer. Annals of Diagnostic Pathology, 2018. 34: p. 50-55.
- Harris, R.E., B.C. Casto, and Z.M. Harris, Cyclooxygenase-2 and the inflammogenesis of breast cancer. World Journal of Clinical Oncology, 2014. 5(4): p. 677.
- Petkova, D., et al., Overexpression of cyclooxygenase-2 in non-small cell lung cancer. Respiratory Medicine, 2004. 98(2): p. 164-172.
- Yip-Schneider, M.T., et al., Cyclooxygenase-2 expression in human pancreatic adenocarcinomas. Carcinogenesis, 2000. 21(2): p. 139-146.
- Saba, N.F., et al., Role of Cyclooxygenase-2 in Tumor Progression and Survival of Head and Neck Squamous Cell CarcinomaRole of COX-2 in Head and Neck Cancer. Cancer Prevention Research, 2009. 2(9): p. 823-829.
- Masferrer, J.L., et al., Antiangiogenic and Antitumor Activities of cyclooxygenase-2 inhibitors. Cancer Research, 2000. 60(5): p. 1306-1311.
- Shi, G., et al., Upregulation of cyclooxygenase-2 is associated with activation of the alternative nuclear factor kappa B signaling pathway in colonic adenocarcinoma. Am J Transl Res, 2015. 7(9): p. 1612-20.
- Bogdan, C., M. Röllinghoff, and A. Diefenbach, The role of nitric oxide in innate immunity. Immunological Reviews, 2000. 173: p. 17-26.
- Ekmekcioglu, S., E.A. Grimm, and J. Roszik, Targeting iNOS to increase efficacy of immunotherapies. Human Vaccines & Immunotherapeutics, 2017. 13(5): p. 1105-1108.
- Hausel, P., et al., Src-mediated phosphorylation regulates subcellular distribution and activity of human inducible nitric oxide synthase. Oncogene, 2006. 25(2): p. 198-206.
- Pautz, A., et al., Regulation of the expression of inducible nitric oxide synthase. Nitric Oxide, 2010. 23(2): p. 75-93.
- Ichikawa, T., et al., American ginseng preferentially suppresses STAT/iNOS signaling in activated macrophages. Journal of Ethnopharmacology, 2009. 125(1): p. 145-150.
- Qu, C., et al., Identifying panaxynol, a natural activator of nuclear factor erythroid-2 related factor 2 (Nrf2) from American ginseng as a suppressor of inflamed macrophage-induced cardiomyocyte hypertrophy. Journal of Ethnopharmacology, 2015. 168: p. 326-336.
- Ďuračková, Z., Some current insights into oxidative stress. Physiological research, 2010. 59(4).
- Scialo, F. and A. Sanz, Coenzyme Q redox signalling and longevity. Free Radical Biology and Medicine, 2021. 164: p. 187-205.
- Kim, J.Y., et al., Panaxydol induces apoptosis through an increased intracellular calcium level, activation of JNK and p38 MAPK and NADPH oxidase-dependent generation of reactive oxygen species. Apoptosis, 2011. 16(4): p. 347-358.
- Young, J.F., et al., The polyacetylenes falcarinol and falcarindiol affect stress responses in myotube cultures in a biphasic manner. Dose-Response, 2008. 6(3): p. dose-response. 08-008. Young.
- Ohnuma, T., et al., Activation of the Nrf2/ARE pathway via S-alkylation of cysteine 151 in the chemopreventive agent-sensor Keap1 protein by falcarindiol, a conjugated diacetylene compound. Toxicology and Applied Pharmacology, 2010. 244(1): p. 27-36.
- Chiang, S.K., S.E. Chen, and L.C. Chang, A Dual Role of Heme Oxygenase-1 in Cancer Cells. Int J Mol Sci, 2018. 20(1).
- Stefanson, A.L. and M. Bakovic, Falcarinol is a potent inducer of heme oxygenase-1 and was more effective than sulforaphane in attenuating intestinal inflammation at diet-achievable doses. Oxidative Medicine and Cellular Longevity, 2018. 2018.
- Sano, R. and J.C. Reed, ER stress-induced cell death mechanisms. Biochimica et Biophysica Acta (BBA)-Molecular Cell Research, 2013. 1833(12): p. 3460-3470.
- Li, Y., et al., The role and therapeutic implication of endoplasmic reticulum stress in inflammatory cancer transformation. American Journal of Cancer Research, 2022. 12(5): p. 2277-2292.
- Jin, H., et al., The antitumor natural compound falcarindiol promotes cancer cell death by inducing endoplasmic reticulum stress. Cell Death & Disease, 2012. 3(8): p. e376-e376.
- Kim, H.S., et al., Panaxydol, a component of P anax ginseng, induces apoptosis in cancer cells through EGFR activation and ER stress and inhibits tumor growth in mouse models. International Journal of Cancer, 2016. 138(6): p. 1432-1441.
- Andersen, C.B., et al., Falcarindiol Purified From Carrots Leads to Elevated Levels of Lipid Droplets and Upregulation of Peroxisome Proliferator-Activated Receptor-γ Gene Expression in Cellular Models. Frontiers in Pharmacology, 2020. 11: p. 565524.
- Cheung, S.S., et al., Devil’s Club falcarinol-type polyacetylenes inhibit pancreatic cancer cell proliferation. Nutrition and Cancer, 2019. 71(2): p. 301-311.
- Xie, Q. and C. Wang, Polyacetylenes in herbal medicine: A comprehensive review of its occurrence, pharmacology, toxicology, and pharmacokinetics (2014–2021). Phytochemistry, 2022: p. 113288.
- Zaini, R., et al., Effects of bioactive compounds from carrots (Daucus carota L.), polyacetylenes, beta-carotene and lutein on human lymphoid leukaemia cells. Anti-Cancer Agents in Medicinal Chemistry (Formerly Current Medicinal Chemistry-Anti-Cancer Agents), 2012. 12(6): p. 640-652.
- Zidorn, C., et al., Polyacetylenes from the Apiaceae vegetables carrot, celery, fennel, parsley, and parsnip and their cytotoxic activities. Journal of Agricultural and Food Chemistry, 2005. 53(7): p. 2518-2523.
- Bernart, M.W., et al., Cytotoxic falcarinol oxylipins from Dendropanax arboreus. Journal of Natural Products, 1996. 59(8): p. 748-753.
- Sapienza, C. and J.-P. Issa, Diet, nutrition, and cancer epigenetics. Annual Review of Nutrition, 2016. 36: p. 665-681.
- Le, H.T., et al., Panaxynol, a natural Hsp90 inhibitor, effectively targets both lung cancer stem and non-stem cells. Cancer Letters, 2018. 412: p. 297-307.
- Chatterjee, S. and T.F. Burns, Targeting heat shock proteins in cancer: a promising therapeutic approach. International journal of molecular sciences, 2017. 18(9): p. 1978.
- Neckers, L. and P. Workman, Hsp90 molecular chaperone inhibitors: are we there yet? Clinical Cancer Research, 2012. 18(1): p. 64-76.
- Nair, A., M.A. Morsy, and S. Jacob, Dose translation between laboratory animals and human in preclinical and clinical phases of drug development. Drug Development Research, 2018. 79(8): p. 373-382.
- Kobaek-Larsen, M., et al., Effect of the dietary polyacetylenes falcarinol and falcarindiol on the gut microbiota composition in a rat model of colorectal cancer. BMC Research Notes, 2018. 11(1): p. 1-6.
- Hansen, S.L., S. Purup, and L.P. Christensen, Bioactivity of falcarinol and the influenceof processing and storage on its content in carrots (Daucus carota L). Journal of the Science of Food and Agriculture, 2003. 83(10): p. 1010-1017.
- Purup, S., E. Larsen, and L.P. Christensen, Differential effects of falcarinol and related aliphatic C17-polyacetylenes on intestinal cell proliferation. Journal of Agricultural and Food Chemistry, 2009. 57(18): p. 8290-8296.
- Young, J.F., et al., Biphasic effect of falcarinol on CaCo-2 cell proliferation, DNA damage, and apoptosis. Journal of Agricultural and Food Chemistry, 2007. 55(3): p. 618-623.
- Dolatpanah, M., et al., Falcarindiol attenuates cisplatin-induced nephrotoxicity through the modulation of NF-kB and Nrf2 signaling pathways in mice. 2022.
- Tan, K.W., et al., Dietary polyacetylenes of the falcarinol type are inhibitors of breast cancer resistance protein (BCRP/ABCG2). European Journal of Pharmacology, 2014. 723: p. 346-352.
- Deding, U., et al., Carrot intake and risk of colorectal cancer: A prospective cohort study of 57,053 Danes. Nutrients, 2020. 12(2): p. 332.
- Almqbel, M., C. Seal, and K. Brandt, Effects of carrot powder intake after weaning on tumours in APCMin mice. Proceedings of the Nutrition Society, 2017. 76(OCE4).
- Kobæk-Larsen, M., et al., Inhibitory effects of feeding with carrots or (−)-falcarinol on development of azoxymethane-induced preneoplastic lesions in the rat colon. Journal of Agricultural and Food Chemistry, 2005. 53(5): p. 1823-1827.
- Kobaek-Larsen, M., et al., Dietary polyacetylenes, falcarinol and falcarindiol, isolated from carrots prevents the formation of neoplastic lesions in the colon of azoxymethane-induced rats. Food & Function, 2017. 8(3): p. 964-974.
- Crosby, D. and N. Aharonson, The structure of carotatoxin, a natural toxicant from carrot. Tetrahedron, 1967. 23(1): p. 465-472.
- Uwai, K., et al., Exploring the structural basis of neurotoxicity in C17-polyacetylenes isolated from water hemlock. Journal of Medicinal Chemistry, 2000. 43(23): p. 4508-4515.
- Czepa, A. and T. Hofmann, Structural and sensory characterization of compounds contributing to the bitter off-taste of carrots (Daucus carota L.) and carrot puree. Journal of Agricultural and Food Chemistry, 2003. 51(13): p. 3865-3873.
- Downs, C., et al., A hemlock water dropwort curry: a case of multiple poisoning. Emerg Med J, 2002. 19(5): p. 472-3.
- Christensen, L., Bioactivity of Polyacetylenes in food plants: Bioactive Foods in Promoting Health (Chapter 20). 2010, Academic Press, .
Figure 1.
Chemical structures of (3R)-falcarinol (also known as panaxynol), (3R,8S)-falcarindiol, and (3R,8S)-falcarindiol 3-acetate, panaxydol, and panaxydiol.
Figure 1.
Chemical structures of (3R)-falcarinol (also known as panaxynol), (3R,8S)-falcarindiol, and (3R,8S)-falcarindiol 3-acetate, panaxydol, and panaxydiol.
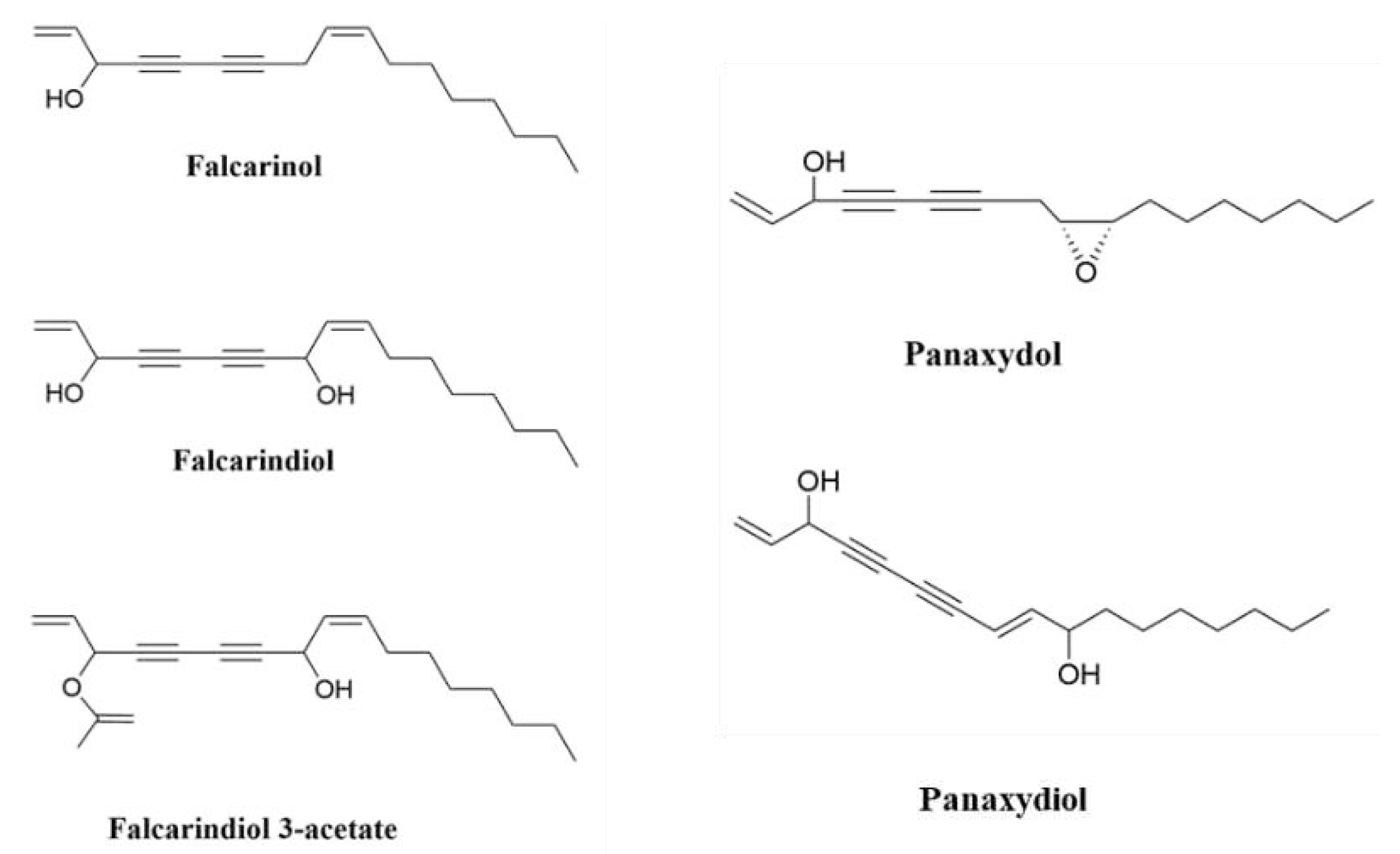
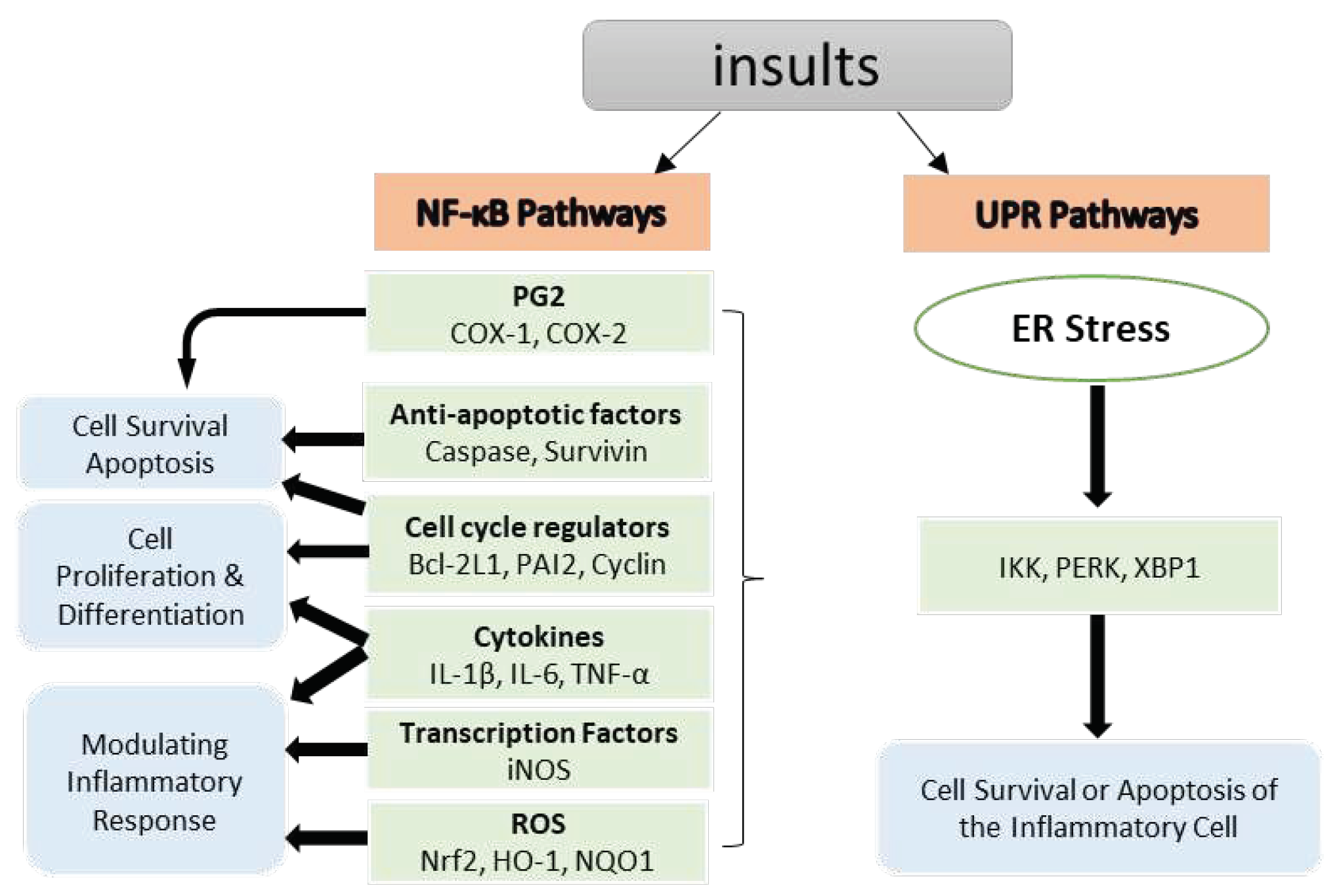
Figure 2.
NF-κB target genes implicated in the onset and progression of inflammation. NF-κB is a transcription factor that is inducible. After activation, it can regulate inflammation by activating the transcription of several genes. NF-κB regulates cell proliferation, apoptosis, and differentiation in addition to promoting the production of pro-inflammatory cytokines, and chemokines. Chronic endoplasmic reticulum (ER) stress results in an inflammatory unfolded protein response (UPR). Stress on the ER induces apoptosis by activating inflammation. This can be accomplished by stimulating IKK complex or XBP1 and PERK through a mediator. These trigger the release of pro-inflammatory molecules, hence accelerating cell death.
Figure 2.
NF-κB target genes implicated in the onset and progression of inflammation. NF-κB is a transcription factor that is inducible. After activation, it can regulate inflammation by activating the transcription of several genes. NF-κB regulates cell proliferation, apoptosis, and differentiation in addition to promoting the production of pro-inflammatory cytokines, and chemokines. Chronic endoplasmic reticulum (ER) stress results in an inflammatory unfolded protein response (UPR). Stress on the ER induces apoptosis by activating inflammation. This can be accomplished by stimulating IKK complex or XBP1 and PERK through a mediator. These trigger the release of pro-inflammatory molecules, hence accelerating cell death.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



