Submitted:
23 January 2023
Posted:
31 January 2023
You are already at the latest version
Abstract
Dietary fiber has been associated with health benefits, therefore, the availability of validated tools to assess food consumption associated with high-fiber foods would allow the quantification of the intake of this functional nutrient, the identification of risk groups and target populations, and the development of public policies and/or programs aimed at improving the health of the population. In this study, a fiber intake short food frequency questionnaire (FFQ) was translated into Spanish and its content validity was determined by a group of experts, to subsequently conduct a pilot test including 198 subjects aged 36+12.5 years, residing in Chile (46 men and 150 women), with the purpose of quantifying dietary fiber intake. The global assessment of the FFQ revealed a validity coefficient of 0.98+0.02; after the application of the pilot, mean dietary fiber intake in adult Chilean residents was of 13 g per day, with similar results to those found in the National Food Consumption Survey 2010 (12.5 g per day in men, and 11.5 g in women). The FFQ is a quick and valid tool to classify people on the basis of their habitual dietary fiber intake.
Keywords:
Dietary fiber
; food frequency questionnaire
; questionnaire screening
; validation
1. Introduction
Several definitions of dietary fiber (DF) have been proposed over time, based primarily on physiological aspects or on the methods used for its analysis, as defined by the AOAC (Association of Agricultural Official Chemists) [1]. DF includes a diverse range of complex carbohydrates that play a critical role in public health, since this is an under-consumed nutrient when compared to the recommended intake in most countries worldwide [2]. While the codex alimentarius states that dietary fibre means carbohydrate polymers with ten or more monomeric units, which are not hydrolysed by the endogenous enzymes in the small intestine of humans and belong to the categories (a) edible carbohydrate polymers naturally occurring in the food as consumed, (b) carbohydrate polymers, which have been obtained from food raw material by physical, enzymatic or chemical means and which have been shown to have a physiological effect of benefit to health as demonstrated by generally accepted scientific evidence to competent authorities, and (c) synthetic carbohydrate polymers which have been shown to have a physiological effect of benefit to health as demonstrated by generally accepted scientific evidence to competent authorities [3]. On the other hand, FD can be classified into soluble FD (SDF) and insoluble FD (IDF) according to its ability to hydrate in water [4]. The food sources of SDF are apples, pears, citrus fruits, carrots, broccoli, peas, cucumber, celery and wheat bran [5]. SDF forms colloid solutions in the intestine, slows digestion and causes a prolonged feeling of satiety, while FDI accelerates intestinal transit, increasing stool volume, acting as a bulking agent and laxative and its food sources are nuts, legumes, whole wheat, barley and tubers [6]. Considering the above, DF is related to the promotion of mitigating effects on cholesterol and glucose levels [7,8], the latter being related to the onset of type 2 diabetes [9,10], obesity, colon cancer [11,12], and cardiovascular diseases [13,14]; it takes part in all the functions of the digestive system, from mastication to the evacuation of feces [15], and in general, health benefits provided by DF include improvements in gut health (increase in fecal loading, softening of feces, decrease of fecal pH, and fermentation) [16], glycemic and insulinemic control, cholesterol reduction (total cholesterol and LDL-cholesterol) [9], weight control (reduction of caloric intake and increase in satiety) [17], and an effect on the metabolic function of the different microbial species that colonize the gastrointestinal tract, to improve human health and potentially prevent or treat diseases in general [18]. The beneficial effects associated with FD consumption are shown in Figure 1. Generally speaking, the daily intake of DF should be in the range of 18-38 g per day for adult subjects [15], nevertheless, DF intake does not exceed 20 g per day at the global level [19]. Against this background, the Scientific Advisory Committee on Nutrition in the UK recommended in 2015 to increase the intake to 30 g per day, however, only 9% of adults in the United Kingdom managed to reach this objective [20], while in the United States, according to data from the National Health and Nutrition Examination Survey (NHANES) 2009-2010, mean fiber intake was of 16.2 g per day, representing an increase of approximately 1 g per day with respect to the 15.1 g per day reported in the 2001-2002 survey; nevertheless, this intake continues to fall well short of the recommendations [19].
In Chile, there is scant information available regarding food consumption, specially on the quantification of fiber intake. The epidemiological profile of the country has changed dramatically in recent decades [21], implying significant modifications in the dietary profile; these changes need to be addressed. Last data correspond to those collected by the National Food Consumption Survey 2010 (ENCA, as its acronym in Spanish), that reported a low consumption of foods that contain protective nutrients, such as DF, showing an average intake of 12.5 g per day in men, and 11.5 g per day in women [21], which is below the recommendations suggested by the Joint FAO/WHO Expert Committee, whose advice indicates an average intake of 25 g per day [14]. In this regard, the availability of validated tools to assess food consumption, particularly that associated with the intake of high-fiber foods, would allow the quantification of the intake of this functional nutrient, the identification of risk groups and target populations, and the development of public policies and/or programs aimed at improving the health of the population.
The objective of this research was (a) to adapt and validate the content of a dietary fiber intake short food frequency questionnaire through an assessment by experts; (b) to perform a pilot test of the dietary fiber intake short food frequency questionnaire in adults residing in Chile.
2. Materials and Methods
2.1. Food Frequency Questionnaire to assess Dietary Fiber and Scoring Sheet
In the year 2022, we conducted the pilot phase of an observational study for the validation of the dietary fiber intake short food frequency questionnaire (DF-FFQ) developed by Healey et al. (2016), who authorized its use for the performance of the present study [22]; the questionnaire was implemented as an online instrument, because compared with traditional methods, online dietary assessment methods can be used to target specific geographical population groups, can be accessed remotely, and can be designed to be easy to complete [23]. The questionnaire includes 59 foods that contain fiber classified in 5 food groups (fruits, vegetables, bread-cereals, dried fruits, and pulses), with consumption frequencies ranging from “never” to “6 or more times per day” (Supplementary Materials S1). Considering the high consumption of bread in the country [21], it was decided to subdivide the cereal food group, estimating fiber intake independently from bread consumption. In addition, in order to reduce reporting bias related to food serving size, representative images of each food group were added, according to the Atlas Fotográfico de Preparaciones Típicas Chilenas [Photographic Atlas of Typical Chilean Preparations] [24]. The included food groups are presented in Figure 2.
Fiber content was calculated using the Table of Chemical Composition of Chilean Food [25] and a scoring sheet, which was similar to the original version, was developed to quantify the amount of dietary fiber consumed by each participant (Supplementary Materials S2). The total intake of dietary fiber of an individual was calculated as the sum of the average amount of fiber consumed of each food group in relation to the number of consumed servings.
2.2. Content Validity of Food the DF-FFQ
The initial step in the process of validation of the instrument consisted of following the internationally suggested guidelines [26], that consider the translation of the questionnaire from the source language (English) to its Spanish version, with the translation being performed by a certified translator (Figure 3).
Subsequently, the instrument was presented to a commission of expert judges, composed by 6 scholars (dietitian-nutritionists) who work in the field of nutrition and food science on the basis of their professional experience, specialty and academic degree [27]. Experts were separately applied a closed-question survey to evaluate the adequacy and pertinence of the Spanish-translated version; the survey was based on a Likert-type scale including five alternatives (1 = strongly disagree; 2 = disagree; 3 = undecided; 4 = agree; 5 = strongly agree) (Supplementary materials S3). Among the criteria examined were clarity of wording, clarity of instructions, adequate language, whether it measures what it intends, and the extent to which it fulfills its stated purpose. They were also given the opportunity of adding comments and/or suggestions, as in open-ended questions. Items that did not meet the minimum standards were reconsidered for modification or elimination. From this step, the final version of the DF-FFQ (Dietary Fiber Food Frequency Questionnaire) was obtained.
A content validity index (CVI): I-CVI—(item-level content validity index); acceptable limit >0.80 and S-CVI/Ave—scale-level with universal agreement method; acceptable limit >0.80 [28,29]. In addition with used the method proposed by Hernández-Nieto 2002 [30] [30], where each item of the instrument was verified by calculating the individual mean value (acceptable limit >0.80), based on the following formula CVC (Content Validity Coefficient):
where Mx represents the mean of the element in the score given by the experts, Vmáx the maximum score that the item could reach and Pei the error assigned to each item.
CVC = (Mx/Vmáx) - Pei
2.3. Determination of Dietary Fiber Intake Using the FFQ and Ethical Aspects
With respect to the application of the pilot test of the Spanish version of the questionnaire, participants consisted of adults aged 18 years and older, residents of Chile and with Internet access; the test was carried out from April to August 2022. All subjects who presented a condition that hinders the consumption of food sources with high fiber content were excluded from the study (severe liver disease; kidney failure; gastric cancer and colon cancer; diagnosis of food allergies and food intolerance; celiac disease; Crohn disease; ulcerative colitis; pregnancy; and/or having a disease that causes a disruption in consumption patterns). The research team used a non-probabilistic sampling method, issuing an open call to community members through virtual/social platforms. The recruitment process considered the initial screening and obtaining the informed consent. A total of 198 participants were recruited, whose sociodemographic [sex (men or women), age (years), occupation (dependent worker, freelance worker, student, unemployed, housekeeper or retired), place of residence (urban or rural)] and nutritional variables [weight (kg), height (m), Body Mass Index (kg/m2)]; in addition, subjects were applied a FFQ to assess dietary fiber intake. The research was developed following the Declaration of Helsinki [31] regarding work involving human beings, and the CIOMS Guidelines [32] were also considered. The protocol of this study was approved by the Scientific Ethics Committee of the Universidad San Sebastian (No. 5-22). All participants were fully informed and expressed their willingness to participate by signing the informed consent form.
2.4. Statistical Analysis
Statistical analysis was performed with the IBM SPSS Statistics V21 software. The validation of the survey content was verified for each item of the questionnaire, indicating the percentage of agreement among the expert judges, with a preset level of S-CVI/Ave, S-CVI/UA and CVC= 0.80 deemed acceptable. Descriptive statistics for quantitative variables were described with average and standard deviation, while categorical variables were described with frequencies and percentages. Variables were tested for normality using the Kolmogorov Smirnov test, and the Mann-Whitney test was used to evaluate differences between groups. A p value of <0.05 was considered statistically significant for all tests.
3. Results
Global assessment of the questionnaire demonstrated that the validity coefficient reached values higher than 0.8; specifically, I-CVI and S-CVI/Ave averaged 0.92 and 0.97 respect. Additionally, adequacy averaged a CVC of 0.98, whereas pertinence averaged an adequacy CVC of 0.95, with no need to modify a particular item, nevertheless, it was decided to split the “cereals and bread" group up, since considering the high consumption of bread among the Chilean population, it is worthy of a separate categorization. Detailed values for each item are shown in Table 1. Based on the opinions provided by external judges in the open-ended questions, the quality of some representative images of food items and their respective serving size were modified, to facilitate greater understanding of the questionnaire.
The questionnaire was applied to 198 participants residing in the national territory. The sociodemographic variables and nutritional status are shown in Table 2. Mean age of the population was 36.0 + 12.5 years, most of the subjects were Chilean citizens (94.2%), predominantly females (72.5%), concentrated mostly in the regions of Biobio, Maule, and Valparaíso, specifically in urban areas (85%), with respect to rural areas, which only reached 10.6%. The occupation of the participants, in decreasing order, corresponded to dependent worker (45.9%), students (26.1%) and independent worker (10.1%). When analyzing overall data, it is observed that 64.6% of the surveyed population had excess weight, with 37.9% classified as overweight, and 26% classified as obesity (Table 2); specifically, 19.5% had class I obesity, 6.2% class II obesity, and 1% class III obesity (data not shown).
The mean dietary fiber intake values were 12.3+6.9 g/d for the total population (Table 3). Average fiber intake and intake by food groups according to age, sex, residence, occupation, and BMI category is shown in Table 4. When comparing fiber intake by food groups and by age groups, a significant difference was observed in the cereals group (p<0.001), with a higher consumption in people aged 15-29 years (2.87 g/d), versus >30 years of age (1.33 g/d), while for the sex variable, a statistically significant difference was only observed in the amount of fiber contributed by bread (p=0.013), being men those who consume it in greater quantity, surpassing women in 1.44 g/d of total fiber. Likewise, fiber intake according to age and occupation is statistically different only in the cereal group, while when comparing with the nutritional status, a difference is observed in the fruit, bread and cereal groups, with a lower consumption of fiber in the participants with obesity, with respect to those with deficient nutritional status.
The contribution to total fiber intake by age, sex, residence, occupation and BMI category for each food group is shown in Figure 4; When analyzing each variable individually, it is observed that fiber intake from bread consumption is predominant, followed in most cases by cereals. Overall, it was observed a greater contribution to total fiber intake from bread (35.2%) and cereals (15.5%), while dried fruits (10.3%) and fruits (10.3%) were the items that contributed the least to total intake.
4. Discussion
To our knowledge, currently there are no short questionnaires for the quantification of dietary fiber intake in the Chilean population, which makes it difficult to classify users based on their dietary fiber intake and their association with different health events, whose etiology is partly related to the lower or higher intake of such food component.
This pilot study was intended to adapt the process of validation of the content of a dietary fiber intake short food frequency questionnaire, which was adapted from a previously validated English version [22], through an assessment by experts and the subsequent implementation of a pilot test with adults residing in Chile.
Content validity is one of the most important types of validity to ensure congruence between study objective and data collection instrument, therefore it is a common starting point for questionnaire validation [33]. As Lynn (1986) pointed out, researchers calculate two types of CVI [34]. The first involves content validity of the items individually (I-CVI), while the second involves content validity of the overall scale (S-CVI-Ave) [29]. Our results indicate that the DF-FFQ was considered by experts to have excellent clarity and relevance. The I-CVI, and S-CVI-Ave values were above the minimum standard of 0.80, and the CVC for most items were rated as excellent in both adequacy and pertinence. Participants found the questionnaire to be acceptable and understandable, demonstrating the content validity of the questionnaire, with minor modifications suggested by the external judges, such as specifying serving size of some food items.
Considering that in Chile there are no known short questionnaires for the quantification of dietary fiber intake, the performance of a pilot study is an essential step in the research process to quantify the intake of this nutrient in the population living in national territory, since it allows to evaluate the methodologic and procedural aspects of a larger scale future study, therefore, its planning, implementation and dissemination must be rigorously conducted in accordance with guidelines proposed for pilot studies [35,36]. Moreover, the publication of this study is relevant, since its scope is to identify the adequacy of the instrument, and therefore achieving a greater degree of representativeness in the development of a future research including a larger sample size.
A number of 198 people residing in Chile participated in the pilot study, 94% of whom are Chilean citizens living in urban areas, with the Biobio, Maule, Valparaiso and Metropolitan regions being reported as the most representative, which is in line with data on population density published in Chile [37]. The sample consisted predominantly of women, who represented the 72.5% of the total population, similar to what was observed in other studies on dietary intake [22,38], and is consistent with the demographic distribution of the country, where women represent more than half of the population [37].
Regarding DF intake, average intake was of 12,3 g per day, falling well short of intake recommendation of this nutrient, that should be in the range of 18-38 g per day for adult subjects [15], which is associated with health benefits such as cardiovascular health [39], blood glucose levels [8], gastrointestinal health [16], and obesity and weight managent [40]. According to data previously published by the National Food Survey in Chile, the low consumption of total fiber is maintained [21], a situation similar to other countries with insufficient consumption such as Brazil (15.7 g/d)[41], Argentina (9.3 g/d)[42], Mexico (16 to 18 g/d) [43] or the United States (18.3 g/d) [44], while studies in European countries such as Sweden and Norway established a total fiber intake of 19.6 g/d and 24.0 g/d, respectively [45].
With respect to fiber intake, according to age range, the results of the National Diet and Nutrition Survey in the United Kingdom (2014) and the Australian National Survey (2017) have shown that the intake of this nutrient increases with age, with a marked decrease after the age of 65 years [45,46]. However, in this research, the highest fiber intake was observed in the population aged 15-29 years, with a decrease of approximately 4 grams in the intake of the population aged 30 years or older, which can be explained by differences in the classification of age groups, since there was no subclassification between adults and older adults.
On the other hand, our results show a significantly higher intake in the male population, probably explained by the higher consumption of bread and cereals in this population, which represent the food sources with the highest contribution to the total intake of this nutrient, a situation that is repeated when compared with other studies in which a higher average daily intake has been identified in men (17.3 g/d) than in women (14.9 g/d) [47]. Likewise, Brazilian researchers have affirmed that rural households had a higher fiber intake than urban ones [41], as observed in our research, which can be explained by the lower industrialization of food available in rural areas [48].
Participants in this study with an underweight body mass index (BMI) had an average total fiber intake of 24.2 g/d, while those participants with obesity reported an intake of 11.1 g/d. Therefore, it was shown that those with higher BMI consumed significantly less fiber. Several studies have shown that individuals with a higher total fiber intake experience less annual weight gain [49].
Another relevant finding reported in these preliminary results showed that bread made the greatest contribution to DF intake, representing 34.3% of total fiber intake.
This result is in accordance with the bread consumption pattern observed in Chile [21], since according to data reported by the Federación Nacional de Industriales Panaderos [National Federation of Bakers, FECHIPAN, as its Spanish acronym] Chile is the second largest consumer of bread worldwide after Turkey with a consumption of 98 kilograms per capita [50]. Bread consumption is a deeply rooted habit in Chile. Studies carried out by the Oficina de Estudios y Políticas Agrarias [Office of Agrarian Studies and Policies, ODEPA, as its Spanish acronym], which investigate the perceptions of Chilean consumers, indicate that bread is considered basic and indispensable. However, most consumers do not attribute nutritional benefits to bread. However, this food can be excellent for a balanced diet [51]. Given the plethora of scientific evidence that corroborate the multiple and varied health benefits of dietary fibre, and the risks associated with a diet that lacks fibre, the optimization of fibre within our diets represents an important public health strategy to improve both metabolic and overall health, and one of the possible strategies is to increase the fiber content of bread.
The survey showed a great practical relevance in the Chilean population, since the criterion to select food sources and the way of estimating dietary fiber contribution facilitate the use of the tool. This study has shown that the FFQ is a quick and valid tool to classify people based on their habitual dietary fiber intake. However, despite the success of the pilot test, results may not be generalized nationwide because of methodological limitations, particularly sample size (as it is a pilot study) and the concentration of responses, that corresponded mostly to the Biobio, Maule and Metropolitan regions, therefore, in the future it is expected the development of a stratified questionnaire to be applied at a national level, with the purpose of having a more accurate estimate of reality with respect to dietary fiber intake in the population residing in Chile.
5. Conclusions
This research showed that the Chilean population has a low consumption of dietary fiber, mainly among women and people with higher body mass index. In this sense, it is important to promote the consumption of fiber, through messages that guide to a better food selection, detailing the benefits it provides for the prevention of chronic diseases and the best quality of life of the population. Likewise, knowing the intake of nutrients and their dietary sources is crucial for the development of public health policies and behavioral change strategies to improve dietary intake.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. S1: Fiber intake questionnaire administered in native language (Spanish version). S2: Scoring sheet for the estimation of Dietary Fiber intake in the Chilean population. S3: Questionnaire for validation by expert judges (Spanish version).
Author Contributions
Conceptualization, F.F., J.B.E., and C.G.; methodology, F.F., J.B.E. and C.G.; software, C.G.; validation, F.F., J.B.E. and C.G.; formal analysis, C.G.; investigation, F.F. J.B.E. and C.G.; resources, F.F. and J.B.E.; data curation, C.G.; writing—original draft preparation, F.F., J.B.E., and C.G.; writing—review and editing, F.F., J.B.E. and C.G.; visualization, F.F., J.B.E. and C.G.; supervision, F.F., J.B.E. and C.G.; project administration, F.F. and B.J.E.; funding acquisition, F.F. and B.J.E. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the project VRIDIDR20/02. Vice Rectory for Research and Doctoral programs. University San Sebastian, Chile.
Informed Consent Statement
Written informed consent has been obtained from the patients to publish this paper.
Data Availability Statement
Not applicable.
Acknowledgments
We would like to thank the Universidad San Sebastián, Vice Rectors office fot university outreach [VCM, as its Spanish acronym] and National Federation of Bakers, [FECHIPAN, as its Spanish acronym] for their support during the execution of the project.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Institute of Medicine (US). Panel on the Definition of Dietary Fiber and the Standing Committee on the Scientific Evaluation of Dietary Reference Intakes. Dietary Reference Intakes Proposed Definition of Dietary Fiber; 2001; ISBN 0309075645. [Google Scholar]
- Millen, B.E.; Abrams, S.; Adams-campbell, L.; Anderson, C.A.M.; Brenna, J.T.; Campbell, W.W.; Clinton, S.; Hu, F.; Nelson, M.; Neuhouser, M.L.; et al. The 2015 Dietary Guidelines Advisory Committee Scienti Fi c Report : Development and Major Conclusions. Adv Nutr. 2016, 7, 438–444. [Google Scholar] [CrossRef] [PubMed]
- Jones, J.M. Dietary Fiber Future Directions: Integrating New Definitions and Findings to Inform Nutrition Research and Communication. Adv. Nutr. 2013, 4, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Vilcanqui-Pérez, F.; Vílchez-Perales, C. Dietary Fiber: New Definitions, Functional Properties and Health Benefits. Review. Arch. Latinoam. Nutr. 2017, 67, 146–156. [Google Scholar]
- Xue, Y.; Cui, L.; Qi, J.; Ojo, O.; Du, X.; Liu, Y.; Wang, X. The Effect of Dietary Fiber (Oat Bran) Supplement on Blood Pressure in Patients with Essential Hypertension: A Randomized Controlled Trial. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 2458–2470. [Google Scholar] [CrossRef] [PubMed]
- Ionită-Mîndrican, C.-B.; Ziani, K.; Mititelu, M.; Oprea, E.; Neacs, S.M.; Morosan, E.; Dumitrescu, D.-E.; Rosca, A.C.; Drăgănescu, D.; Negrei, C. Therapeutic Benefits and Dietary Restrictions of Fiber Intake: A State of the Art Review. Nutrients 2022, 14, 100–125. [Google Scholar] [CrossRef] [PubMed]
- Garcia, I.; Mendez, S.; Aguirre, N.; Sanchez, M.; Matias, D.; Perez, E. Increasing Consumption of Dietary Fiber Complementary to the Treatment of Metabolic Syndrome. Nutr. Hosp. 2018, 35, 582–587. [Google Scholar]
- Reynolds, A.N.; Akerman, A.P.; Mann, J. Dietary Fibre and Whole Grains in Diabetes Management: Systematic Review and Meta-Analyses. PLoS Med. 2020, 17, e1003053. [Google Scholar] [CrossRef] [PubMed]
- Hartley, L.; May, M.; Loveman, E.; Colquitt, J.; Rees, K. Dietary Fibre for the Prevention of Cardiovascular Disease. Ir. Med. J. 2016, 113. [Google Scholar] [CrossRef] [PubMed]
- Bae, I.Y.; Jun, Y.; Lee, S.; Lee, H.G. Characterization of Apple Dietary Fibers Influencing the in Vitro Starch Digestibility of Wheat Flour Gel. Food Sci. Technol. 2016, 65, 158–163. [Google Scholar] [CrossRef]
- Frost, G.; Sleeth, M.L.; Sahuri-Arisoylu, M.; Lizarbe, B.; Cerdan, S.; Brody, L.; Anastasovska, J.; Ghourab, S.; Hankir, M.; Zhang, S.; et al. The Short-Chain Fatty Acid Acetate Reduces Appetite via a Central Homeostatic Mechanism. Nat. Commun. 2014, 5, 1–11. [Google Scholar] [CrossRef]
- Song, Y.; Liu, M.; Yang, F.G.; Cui, L.H.; Lu, X.Y.; Chen, C. Dietary Fibre and the Risk of Colorectal Cancer: A Case-Control Study. Asian Pacific J. Cancer Prev. 2015, 16, 3747–3752. [Google Scholar] [CrossRef] [PubMed]
- Fu, L.; Zhang, G.; Qian, S.; Zhang, Q.; Tan, M. Associations between Dietary Fiber Intake and Cardiovascular Risk Factors: An Umbrella Review of Meta-Analyses of Randomized Controlled Trials. Front. Nutr. 2022, 9. [Google Scholar] [CrossRef] [PubMed]
- Barber, T.M.; Kabisch, S.; Pfei, A.F.H.; Weickert, M.O. The Health Benefits of Dietary Fibre. Nutrients 2020, 12, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Lattimer, J.M.; Haub, M.D. Effects of Dietary Fiber and Its Components on Metabolic Health. Nutrients 2010, 2, 1266–1289. [Google Scholar] [CrossRef] [PubMed]
- Gill, S.K.; Rossi, M.; Bajka, B.; Whelan, K. Dietary Fibre in Gastrointestinal Health and Disease. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 101–116. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Olendzki, B.C.; Wang, J.; Persuitte, G.M.; Li, W.; Fang, H.; Merriam, P.A.; Wedick, N.M.; Ockene, I.S.; Culver, A.L.; et al. Single-Component versus Multicomponent Dietary Goals for the Metabolic Syndrome: A Randomized Trial. Ann. Intern. Med. 2015, 162, 248–257. [Google Scholar] [CrossRef] [PubMed]
- Abreu y Abreu, A.T.; Milke-García, M.P.; Argüello-Arévalo, G.A.; Calderón-de la Barca, A.M.; Carmona-Sánchez, R.I.; Consuelo-Sánchez, A.; Coss-Adame, E.; García-Cedillo, M.F.; Hernández-Rosiles, V.; Icaza-Chávez, M.E.; et al. Dietary Fiber and the Microbiota: A Narrative Review by a Group of Experts from the Asociación Mexicana de Gastroenterología. Rev. Gastroenterol. Mex. 2021, 86, 287–304. [Google Scholar] [CrossRef]
- Reicks, M.; Jonnalagadda, S.; Albertson, A.M.; Joshi, N. Total Dietary Fiber Intakes in the US Population Are Related to Whole Grain Consumption: Results from the National Health and Nutrition Examination Survey 2009 to 2010. Nutr. Res. 2014, 34, 226–234. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, A.; Mann, J.; Cummings, J.; Winter, N.; Mete, E.; Te Morenga, L. Carbohydrate Quality and Human Health: A Series of Systematic Reviews and Meta-Analyses. Lancet 2019, 393, 434–445. [Google Scholar] [CrossRef]
- Department of Nutrition, School of Nutrition, School of Public Health and Microdata Center U of C. National Survey of Food Consumption - Final Report. 2014. 2014. Available online: http://www.minsal.cl.
- Healey, G.; Brough, L.; Murphy, R.; Hedderley, D.; Butts, C.; Coad, J. Validity and Reproducibility of a Habitual Dietary Fibre Intake Short Food Frequency Questionnaire. Nutrients 2016, 8, 3–9. [Google Scholar] [CrossRef]
- Beasley, J.M.; Davis, A.; Riley, W.T. Evaluation of a Web-Based, Pictorial Diet History Questionnaire. Public Health Nutr. 2009, 12, 651–659. [Google Scholar] [CrossRef]
- Cerda, R.; Barrero, C.; Arena, M.; Bascuñán, K.; Jiménez, C. Photographic Atlas of Typical Chilean Foods and Preparations. Univ. Chile 2010. Available online: http://www.repositoriodigital.minsal.cl.
- Gattás, V. Guide to the Nutritional Composition of Natural Foods, Industry and Typical Chilean Preparations.; Chile : University of Chile : INTA, Ed.; 2a. ed.; 2011. [Google Scholar]
- Beaton, D.; Bombardier, C.; Guillemin, F.; Bosi, M. Guidelines for the Process of Cross-Cultural Adaptation of Self-Report Measures. Acta Odontol. Scand. 2000, 24, 3186–3191. [Google Scholar] [CrossRef] [PubMed]
- Shanteau, J.; Weiss, D.J.; Thomas, R.P.; Pounds, J.C. Performance-Based Assessment of Expertise: How to Decide If Someone Is an Expert or Not. Eur. J. Oper. Res. 2002, 136, 253–263. [Google Scholar] [CrossRef]
- Goni, L.; Gil, M.; de la O, V.; Martínez-González, M.Á.; Eisenberg, D.M.; Pueyo-Garrigues, M.; Vasilj, M.; Gayoso, L.; Etxeberria, U.; Ruiz-Canela, M. Development and Validation of a New Home Cooking Frequency Questionnaire: A Pilot Study. Nutrients 2022, 14, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Yusoff, M.S.B. ABC of Content Validation and Content Validity Index Calculation. Educ. Med. J. 2019, 11, 49–54. [Google Scholar] [CrossRef]
- Hernández Nieto, R. Contributions to Statistical Analysis. Rev Venez Cienc Política. 2002, 23, 132–134. [Google Scholar]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. JAMA. 2013, 310, 2191–2194. [Google Scholar] [CrossRef]
- International Ethical Guidelines for Health-related Research Involving Humans, Fourth Edition. Geneva. Council for International Organizations of Medical Sciences (CIOMS). 2016.
- Terwee, C.B.; Bot, S.D.M.; de Boer, M.R.; van der Windt, D.A.W.M.; Knol, D.L.; Dekker, J.; Bouter, L.M.; de Vet, H.C.W. Quality Criteria Were Proposed for Measurement Properties of Health Status Questionnaires. J. Clin. Epidemiol. 2007, 60, 34–42. [Google Scholar] [CrossRef]
- Intan Suraya Noor Arzahan; Zaliha Ismail; Siti Munira Yasin Content Validity Of A Self-Reported Instrument For Safety And Health (S&H) Culture Practice In Paramedic Training Institute Using A Heterogeneous Expert Panel. Turkish J. Comput. Math. Educ. 2021, 12, 2464–2472.
- Thabane, L.; Ma, J.; Chu, R.; Cheng, J.; Ismaila, A.; Rios, L.P.; Robson, R.; Thabane, M.; Giangregorio, L.; Goldsmith, C.H. Pilot Study Article Need To Rename. BMC Med. Res. Methodol. 2010, 10, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Pearson, N.; Naylor, P.J.; Ashe, M.C.; Fernandez, M.; Yoong, S.L.; Wolfenden, L. Guidance for Conducting Feasibility and Pilot Studies for Implementation Trials. Pilot Feasibility Stud. 2020, 6, 1–12. [Google Scholar] [CrossRef]
- National Institute of Statistics of Chile (NIS). Annual Environment Report 2021. Available online: https://www.ine.gob.cl/.
- Soto-Equihua, E.R.; Ramírez-Silva, C.I.; Elton-Puente, J.E.; Chávez-Servín, J.L.; Gutiérrez-Lara, P.; Chávez-Alabat, E.F.; Caamaño, M. del C.; de la Torre-Carbot, K. Design and Validation of a Food Frequency Questionnaire to Evaluate the Consumption of Trans Fatty Acids in the Adult Population (FFQ-TFA). Int. J. Environ. Res. Public Health 2022, 19. [Google Scholar] [CrossRef]
- Nirmala Prasadi, V.P.; Joye, I.J. Dietary Fibre from Whole Grains and Their Benefits on Metabolic Health. Nutrients 2020, 12, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, A.; Clinchamps, M.; Pereira, B.; Courteix, D.; Lesourd, B.; Chapier, R.; Obert, P.; Vinet, A.; Walther, G.; Chaplais, E.; et al. Dietary Fibres and the Management of Obesity and Metabolic Syndrome: The Resolve Study. Nutrients 2020, 12, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Sardinha, A.N.; Canella, D.S.; Martins, A.P.B.; Claro, R.M.; Levy, R.B. Dietary Sources of Fiber Intake in Brazil. Appetite 2014, 79, 134–138. [Google Scholar] [CrossRef] [PubMed]
- National Ministry of Health. National Nutrition and Health Survey. Results Document 2007. Available online: http://www.msal.gob.ar/.
- Lopez-Salido, S.; Llanes-Canedo, C.; Housni, F.; Gonzalez-Flores, J. Analysis Of Dietary Fiber Awareness, Body Mass Index And Socioeconomic Status In The Mexican Population. Interciencia 2020, 45, 469–474. [Google Scholar]
- Centers for Disease Control and Prevention (CDC). National Center for Health Statistics (NCHS). National Health and Nutrition Examination Survey Data. Hyattsville, MD: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention. Available online: http://www.cdc.gov/nchs/nhanes/.
- Stephen, A.M.; Champ, M.M.J.; Cloran, S.J.; Fleith, M.; Van Lieshout, L.; Mejborn, H.; Burley, V.J. Dietary Fibre in Europe: Current State of Knowledge on Definitions, Sources, Recommendations, Intakes and Relationships to Health. 2017; Volume 30, ISBN 0954422417000. [Google Scholar]
- England, P.H. National Diet and Nutrition Survey Results from Years 1, 2, 3 and 4 (Combined) of the Rolling Programme (2008/2009 – 2011/2012); 2017; Volume 1. [Google Scholar]
- Fernstrand, A.M.; Bury, D.; Garssen, J.; Verster, J.C. Dietary Intake of Fibers: Differential Effects in Men and Women on Perceived General Health and Immune Functioning. Food Nutr. Res. 2017, 61. [Google Scholar] [CrossRef]
- Dhingra, D.; Michael, M.; Rajput, H.; Patil, R.T. Dietary Fibre in Foods: A Review. J. Food Sci. Technol. 2012, 49, 255–266. [Google Scholar] [CrossRef]
- Du, H.; Van Der A, D.L.; Boshuizen, H.C.; Forouhi, N.G.; Wareham, N.J.; Halkjær, J.; Tjønneland, A.; Overvad, K.; Jakobsen, M.U.; Boeing, H.; et al. Dietary Fiber and Subsequent Changes in Body Weight and Waist Circumference in European Men and Women. Am. J. Clin. Nutr. 2010, 91, 329–336. [Google Scholar] [CrossRef] [PubMed]
- National Federation of Bakers. Report bread consumption in Chile. 2020. Available online: http://www.fechipan.cl.
- Office of Agrarian Studies and Policies. Consumer perception of fruit and vegetable products, dairy, meat and bread. 2009. Available online: http://www.odepa.gob.cl.
Figure 1.
Benefits of dietary fiber consumption on human health. PYY: peptide YY; GLP1: Glucagon like peptide 1; SCFA: Short-chain fatty acid.
Figure 1.
Benefits of dietary fiber consumption on human health. PYY: peptide YY; GLP1: Glucagon like peptide 1; SCFA: Short-chain fatty acid.
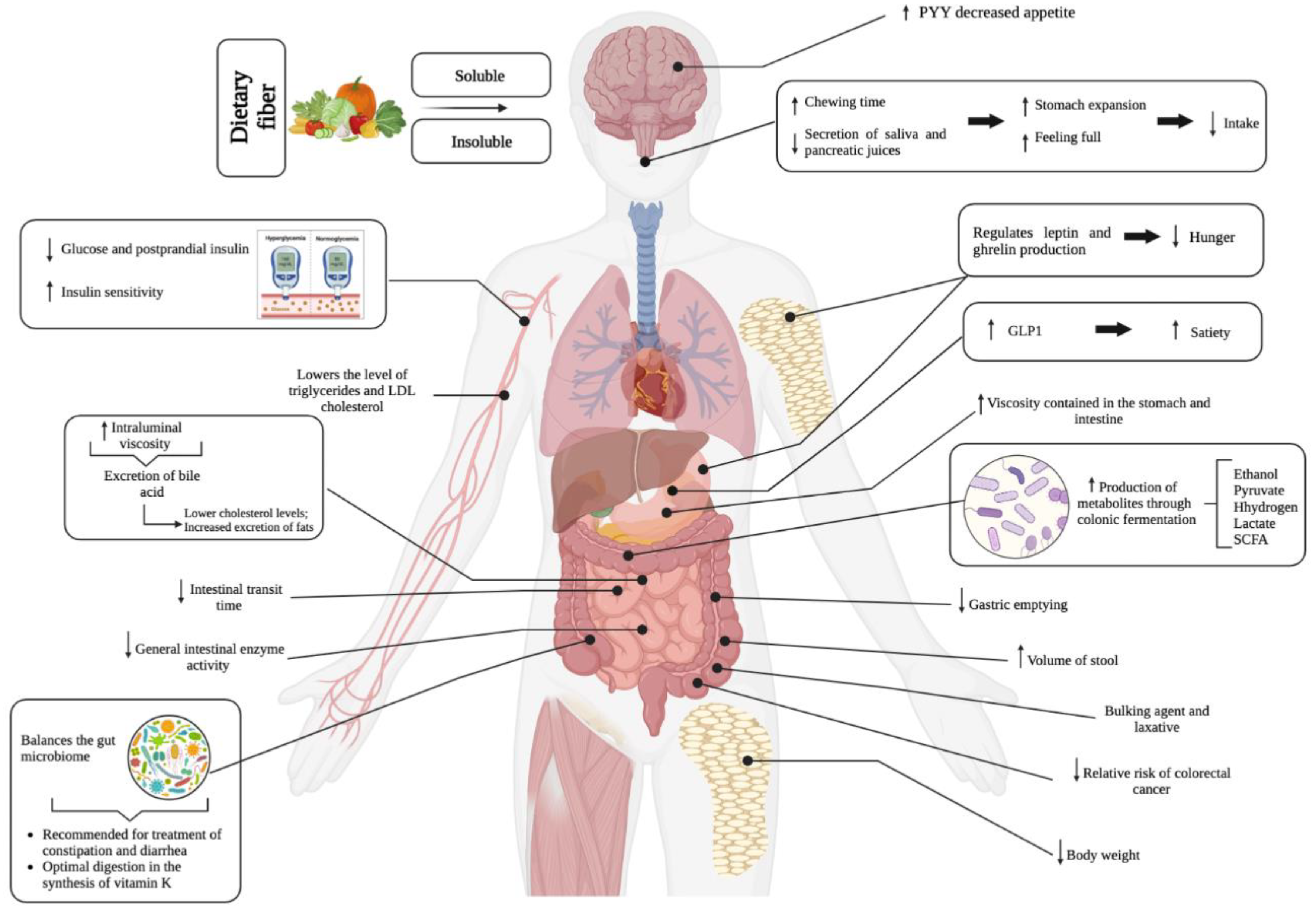
Figure 2.
Representative images of each food group, according to the Photographic Atlas of Typical Chilean Preparations.
Figure 2.
Representative images of each food group, according to the Photographic Atlas of Typical Chilean Preparations.
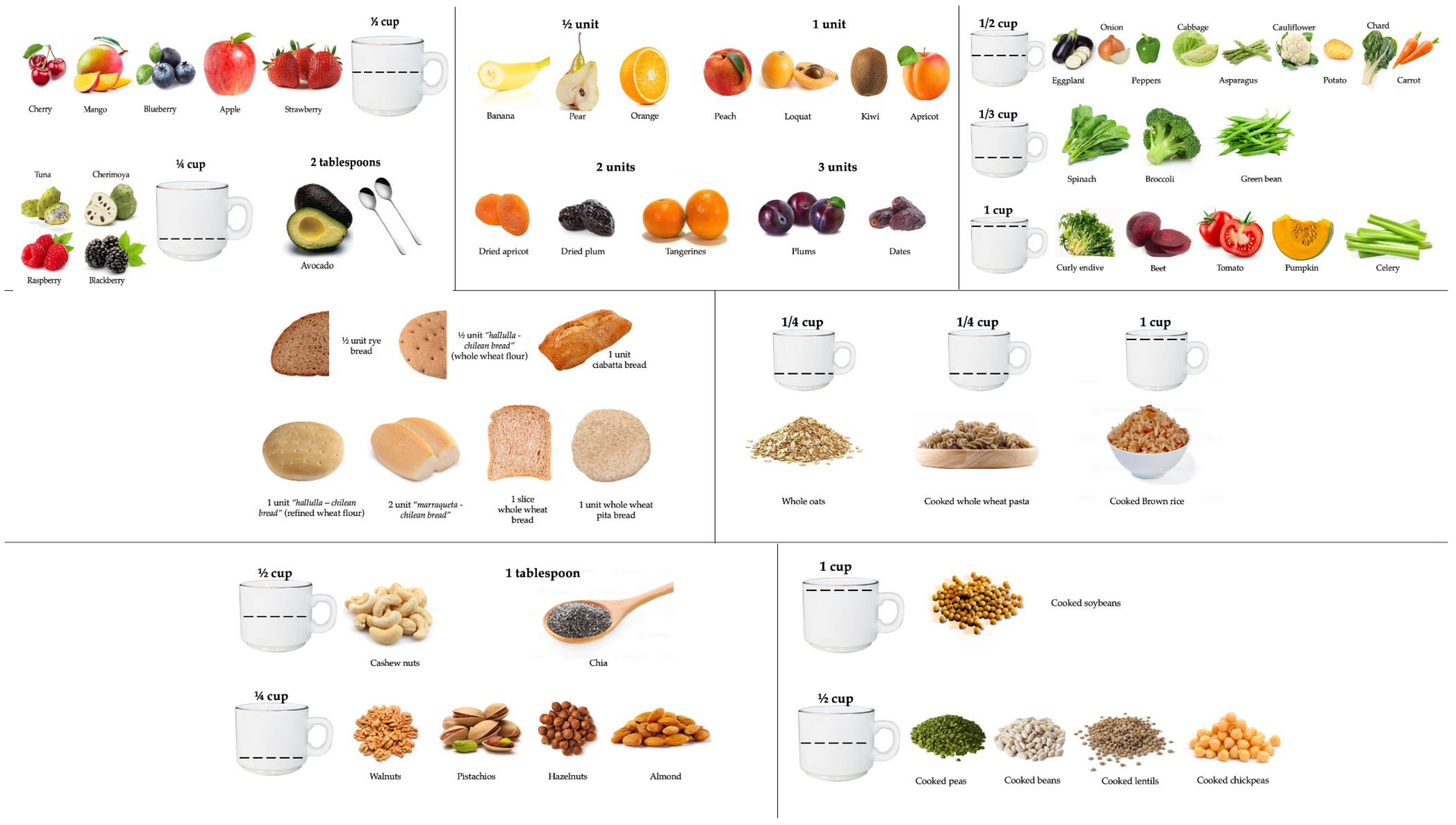
Figure 3.
Process of translation of the original questionnaire to its Spanish version.
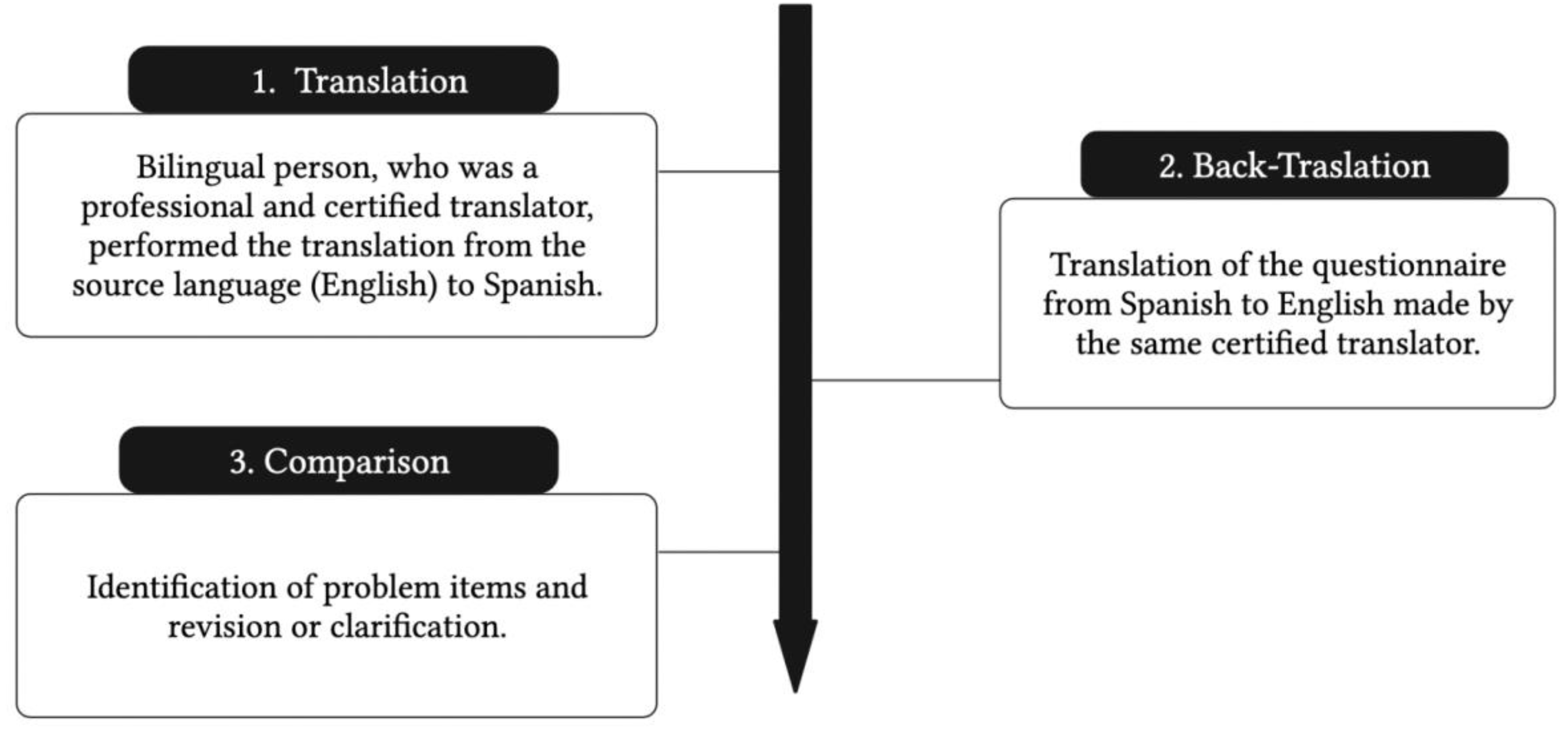
Figure 4.
Percentage contribution to fiber intake (%) by food group in (A) age; (B) sex; (C) residence; (D) occupation; (E) BMI classification.
Figure 4.
Percentage contribution to fiber intake (%) by food group in (A) age; (B) sex; (C) residence; (D) occupation; (E) BMI classification.
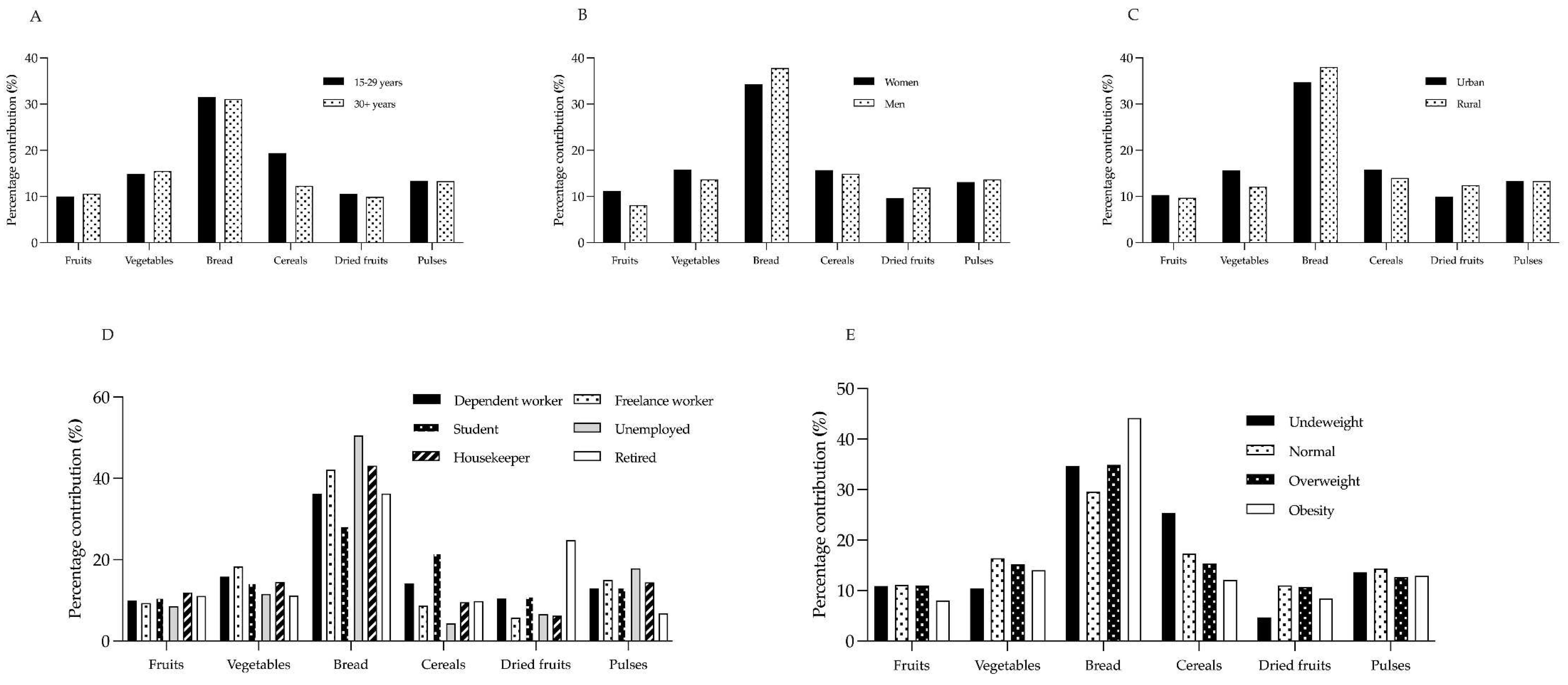

Table 1.
Mean, standard deviation, confidence interval, and validity coefficient for adequacy and pertinence of the DF-FFQ instrument.
Table 1.
Mean, standard deviation, confidence interval, and validity coefficient for adequacy and pertinence of the DF-FFQ instrument.
| Variable | Item | Mean | SD | 95% CI | CVC | S-CVI/Ave |
|---|---|---|---|---|---|---|
|
Adequacy |
1 | 4.9 | 0.15 | 4.73 - 5.06 | 0.98 | 1.00 |
| 2 | 5.0 | 0.00 | 5.00 - 5.00 | 1.00 | 1.00 | |
| 3 | 4.8 | 0.28 | 4.53 - 5.13 | 0.96 | 1.00 | |
| 4 | 4.9 | 0.20 | 4.70 - 5.13 | 0.98 | 1.00 | |
| 5 | 4.9 | 0.12 | 4.82 - 5.07 | 0.98 | 1.00 | |
| 6 - |
4.8 - |
0.40 - |
4.40 - 5.26 - |
0.96 0.98 |
1.00 1.00 |
|
|
Pertinence |
1 | 4.7 | 0.44 | 4.14 - 5.25 | 0.94 | 1.00 |
| 2 | 4.7 | 0.44 | 4.14 - 5.25 | 0.94 | 1.00 | |
| 3 | 4.5 | 0.86 | 3.42 - 5.57 | 0.90 | 0.80 | |
| 4 | 5.0 | 0.00 | 5.00 - 5.00 | 1.00 | 1.00 | |
| 5 | 4.9 | 0.22 | 4.62 - 5.17 | 0.98 | 1.00 | |
| 6 - |
4.7 - |
0.44 - |
4.14 - 5.25 - |
0.94 0.95 |
0.80 0.93 |
1 Item 1: Fruits; Item 2: Vegetables; Item 3: Bread; Item 4: Cereals; Item 5: Dried fruits; Item 6: Pulses; SD: standard deviation; 95% CI: 95% confidence interval; CVC: Content validity coefficient and S-CVI/Ave: scale-level content validity index based on the average method.
Table 2.
Descriptive analysis of sociodemographic variables and nutritional status (n=198).
| Variables | Participants (n) | Percentage (%) | |
|---|---|---|---|
| Age | 15 – 29 years > 30 years |
76 122 |
38.4 61.6 |
| Sex |
Men | 46 | 22.2 |
| Women | 150 | 72.5 | |
| Prefer not to answer | 2 | 1.0 | |
| Region | Antofagasta Region Valparaiso Region O'Higgins Region Maule Region Biobio Region Los Lagos Region Magallanes Region Metropolitan Region Ñuble Region |
1 30 1 36 101 1 1 23 3 |
0.5 14.5 0.5 17.4 48.8 0.5 0.5 11.1 1.4 |
| Residence | Urban Rural |
176 22 |
85.0 10.6 |
| Occupation | Dependent worker Freelance worker Student Unemployed Housekeeper Retired |
95 21 54 7 15 6 |
45.9 10.1 26.1 3.4 7.2 2.9 |
| BMI category | Underweight Normal Overweight Obesity |
3 68 74 52 |
1.5 34.5 37.6 26.4 |
2 BMI: Body Mass Index (kg/m2).
Table 3.
Description of total fiber intake (g/day) (n=196).
| Variable | Mean | SD | Minimum | Maximum |
|---|---|---|---|---|
Age
|
14.8 10.8 0.004* |
8.8 5.0 |
0.2 0.6 |
40.3 26.3 |
Sex
|
11.7 14.4 0.045* |
6.47 8.33 |
0.20 3.00 |
32.4 40.3 |
Residence
|
12.2 13.5 0.233 |
7.12 6.09 |
0.20 3.90 |
40.3 28.6 |
Occupation
|
11.4 10.6 15.6 12.2 9.93 10.8 0.181 |
5.35 5.24 9.65 6.48 4.67 4.57 |
0.60 3.00 0.20 3.50 0.80 5.00 |
26.3 26.2 40.3 21.9 17.4 18.2 |
BMI category
|
24.2 13.7 11.4 11.1 0.037* |
5.56 8.15 6.53 5.01 |
17.9 3.90 0.60 0.20 |
28.5 40.3 37.4 22.2 |
3 Data are presented as mean, standard deviation (SD), minimum and maximum. BMI: Body Mass Index (kg/m2). Comparisons between categories were performed with Mann-Whitney U test or Kruskal Wallis test as appropriate; (*) statistical significance <0.05.
Table 4.
Description of fiber intake (g/day) by food groups (n=196).
| Fruits | Vegetables | Bread | Cereals | Dried fruits | Pulses | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Range | Mean | SD | Range | Mean | SD | Range | Mean | SD | Range | Mean | SD | Range | Mean | SD | Range | |
|
Age 15-29 years >30 years p value |
1.48 1.15 0.153 |
1.43 1.19 |
0-5.2 0-5.2 |
2.21 1.67 0.06 |
1.83 1.47 |
0-8.4 0-7.0 |
4.66 4.12 0.173 |
2.87 2.81 |
0-11.2 0-11.2 |
2.87 1.33 <0.001* |
3.28 2.04 |
0-17.0 0-17.0 |
1.57 1.07 0.951 |
2.86 1.43 |
0-18.0 0-9.0 |
1.98 1.44 0.197 |
2.661.59 | 0-18.90-12.6 |
|
Sex Women Men p value |
1.31 1.16 0.628 |
1.32 1.23 |
0-5.2 0-5.2 |
1.85 1.97 0.484 |
1.66 1.58 |
0-8.4 0-7.0 |
4.01 5.45 0.013* |
2.59 3.31 |
0-11.2 0-11.2 |
1.84 2.15 0.332 |
2.63 2.93 |
0-17.0 0-17.0 |
1.13 1.71 0.442 |
1.58 3.28 |
0-9.0 0-18.0 |
1.53 1.97 0.054 |
2.042.10 | 0-18.90-12.6 |
|
Residence Urban Rural p value |
1.26 1.31 0.593 |
1.30 1.27 |
0-5.2 0-5.2 |
1.90 1.64 0.877 |
1.68 1.23 |
0-8.4 0.1-4.2 |
4.23 5.14 0.118 |
2.84 2.72 |
0-11.2 1.2-11.2 |
1.93 1.90 0.846 |
2.67 2.91 |
0-17.0 0-13.6 |
1.21 1.67 0.431 |
2.07 2.39 |
0-18.0 0-9.0 |
1.63 1.80 0.152 |
2.151.41 | 0-18.90-6.3 |
|
Occupation Dependent worker Freelance worker Student Unemployed Housekeeper Retired p value |
1.13 0.99 1.68 1.04 1.19 1.20 0.207 |
1.13 1.47 1.56 0.82 1.10 0.82 |
0-5.2 0.1-5.2 0-5.2 0-2.6 0-3.9 0.2-2.6 |
1.80 1.94 2.24 1.41 1.44 1.21 0.923 |
1.58 1.79 1.91 1.03 0.96 0.32 |
0.1-8.4 0.1-7.0 0-8.4 0.1-2.8 0-2.8 0.6-1.4 |
4.13 4.47 4.43 6.17 4.28 3.93 0.803 |
2.76 3.01 2.86 4.14 2.31 3.15 |
0-11.2 0-11.2 0-11.2 1.2-11.2 0.4-8.4 0-8.4 |
1.62 0.92 3.38 0.53 0.95 1.06 <0.001* |
2.39 1.01 3.51 0.68 1.31 1.35 |
0-17.0 0-3.4 0-17.0 0-1.5 0-3.4 0-3.4 |
1.18 0.61 1.73 0.80 0.62 2.68 0.284 |
1.54 0.75 3.16 0.89 0.80 3.22 |
0-9.0 0-2.4 0-18.0 0-2.4 0-3.0 0.2-9.0 |
1.48 1.60 2.06 2.18 1.43 0.74 0.331 |
1.651.473.100.871.100.24 | 0-12.60-6.30-18.90.9-2.70-2.70.4-0.9 |
|
BMI Underweight Normal Overweight Obesity p value |
2.66 1.53 1.26 0.89 0.041* |
2.50 1.38 1.31 0.93 |
0.2-5.2 0-5.2 0.1-5.2 0-3.9 |
2.53 2.25 1.74 1.56 0.245 |
2.68 1.91 1.46 1.33 |
0.6-5.6 0.2-8.4 0.1-7.0 0-7.0 |
8.40 4.06 3.98 4.91 0.069 |
2.80 2.27 2.72 3.44 |
5.6-11.2 0-11.2 0-11.2 0-11.2 |
6.16 2.38 1.75 1.35 0.021* |
4.38 2.87 2.90 1.58 |
1.5-10.2 0-17.0 0-17.0 0-6.8 |
1.14 1.52 1.22 0.94 0.181 |
1.62 2.67 1.77 1.70 |
0-3.0 0-18.0 0-9.0 0-9.0 |
3.30 1.96 1.45 1.44 0.459 |
2.743.041.391.03 | 0.9-6.30-18.90-6.30-2.7 |
4 Data are presented as mean, standard deviation (SD), minimum and maximum. Comparisons between categories were performed with Mann-Whitney U test or Kruskal Wallis test as appropriate; (*) statistical significance <0.05.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



