
Submitted:
16 January 2023
Posted:
31 January 2023
You are already at the latest version
Abstract
Epithelial ovarian cancer is an aggressive disease of the female reproductive system and a leading cause of cancer death in women. Standard of care includes surgery and platinum-based chemotherapy yet patients continue to experience a high rate of recurrence and metastasis. Hyperthermic intraperitoneal chemotherapy (HIPEC) treatment in highly selective patients extends overall survival by nearly 12 months. The clinical studies are highly supportive of the use of HIPEC in the treatment of ovarian cancer though the therapeutic approach is limited to academic medical centers. The mechanism underlying HIPEC benefit remains unknown. The efficacy of HIPEC therapy is impacted by several procedural and patient/tumor factors including the timing of surgery, platinum sensitivity, and molecular profiling such as homologous recombination deficiency. The present review aims to provide insight into the mechanistic benefit of HIPEC treatment with a focus on how hyperthermia activates the immune response, induces DNA damage and impairs DNA damage repair pathways, and has a synergistic effect with chemotherapy, with the ultimate outcome of increasing chemosensitivity. Identifying the points of fragility unmasked by HIPEC may provide the key pathways that could be the basis of new therapeutic strategies for ovarian cancer patients.
Keywords:
hyperthermia
; ovarian cancer
; immunity
; chemotherapy
; HIPEC
1. Introduction
Epithelial ovarian, fallopian tube, and primary peritoneal cancers (EOC) are a leading cause of cancer death in women, highlighting the critical clinical need for therapeutic development [1]. The majority (80%) of EOC patients present with advanced stage (III-IV) disease and have a poor prognosis (5-year cancer stage-specific survival 42% and 26%, respectively). Standard of care treatment for advanced EOC involves a combination of debulking surgery and chemotherapy. Hyperthermia has been utilized in cancer treatment for centuries and continues in modern medicine [2]. The therapeutic strategy known as hyperthermic intraperitoneal chemotherapy (HIPEC) in EOC patients at time of interval debulking surgery (IDS) shows promise as patients experience an extension in overall survival (OS) of nearly 12 months compared to patients undergoing interval debulking surgery (IDS) alone [3]. While this, represents the most significant extension of overall survival in EOC patients in over a decade [3], HIPEC mechanisms of action have yet to be understood, thereby limiting further optimization of HIPEC for patients with advanced EOC. Mishra et al. reviewed the history of HIPEC including its adoption in ovarian cancer treatment [2]. Our review focuses on the clinical evidence in support of HIPEC benefit in ovarian cancer followed by an analysis of the mechanisms underlying the benefit of hyperthermia in combination with chemotherapy in cancer.
2. Hyperthermia in Cancer Therapy – The Clinical Picture
2.1. Ovarian Cancer
Epithelial ovarian cancer (EOC) is an aggressive disease of the female reproductive system, often arising from the fallopian tubes, involving the surface lining (epithelial tissue) of the ovaries. 1 in 78 women will experience ovarian cancer in their lifetime [4]. It is expected that more than 22,000 new cases will be reported annually, of which 14,000 will succumb to the disease [5]. EOC has the highest mortality rate than any other gynecological cancer with a case to death ratio equivalent to lung cancer [6]. Nearly 80% of patients present in late stage (III-IV) thus resulting in poor prognosis [5]. A combination of cytotoxic platinum-paclitaxel based chemotherapy and debulking surgery remain the standard of care for advance EOC. While standard treatments have shown initial beneficial outcomes, 70% of patients with advanced disease will experience recurrence within five years, ultimately ending in mortality [7]. In patients for whom upfront or primary debulking surgery (PDS) is not feasible, neoadjuvant chemotherapy (NACT) followed by interval debulking surgery (IDS) and postoperative chemotherapy allows for initial reduction of disease burden to optimize patients for surgical resection. Randomized clinical trials report no significant difference in progression-free survival (PFS) and overall survival (OS) with this approach compared to primary debulking surgery followed by adjuvant chemotherapy [8]. Despite several new chemotherapy agents demonstrating efficacy against EOC, minimal strides have been made to improve patient OS [8]. The need for new clinical therapeutic strategies is crucial in fighting this disease.
Hyperthermic intraperitoneal chemotherapy (HIPEC) is a novel approach in treating advanced EOC, prolonging overall survival of patients. HIPEC treatment involves abdominal perfusion of heated chemotherapy via catheter insertion at the time of cytoreductive surgery (Figure 1). Perfusion machines maintain a constant infusion temperature through the abdominal cavity. Van Driel and colleagues performed a phase 3 randomized controlled trial (OVHIPEC-1) to test the benefits of HIPEC on newly diagnosed EOC patients, comparing results to treatment without HIPEC [3]. Patients with extensive disease who were not ideal candidates for primary debulking surgery (PDS) or patients with residual tumor after PDS were referred for NACT with or without HIPEC as study participants. Three cycles of NACT were completed prior to entry into the trial. Cytoreductive surgery was completed with or without intraoperative administration of HIPEC using perfusion of cisplatin heated to 40⁰C for 90 minutes via an open abdomen technique. Following surgery, patients in both groups received an additional three cycles of chemotherapy. Results revealed patients receiving HIPEC had an extended OS by nearly 12 months, with no increased rate of adverse effects [3].
To answer the question of whether HIPEC extends patient survival regardless of timing of cytoreductive surgery, a single-blinded randomized study was performed including patients with stage III or IV ovarian cancer planned for either PDS or IDS [9]. Patients randomized to the HIPEC arm received cisplatin heated to 41.5oC for 90 minutes using the closed perfusion Belmont Hyperthermia Pump System. The results reveal an extended PFS and OS in the HIPEC cohort, with an OS increase of 8.2 months in HIPEC patients. Further exploration into any differences between HIPEC at time of PDS or IDS revealed an increase of PFS and OS in the patients receiving HIPEC after IDS, by 2 and 13 months respectively. Notably, HIPEC at time of PDS did not extend patient OS and PFS (Table 1). Consistent with Van Driel, these results indicate that HIPEC at time of IDS prolonged patient survival and improved time to recurrence, providing further evidence of the benefit of HIPEC on extending patient survival against EOC [9].
The standard of care for advanced EOC includes cytotoxic platinum and paclitaxel-based chemotherapy. In cases of HIPEC, however, single-agent platinum-based chemotherapies, particularly cisplatin or carboplatin, can be used [13]. Several studies have outlined variations in the efficacy of treatment based on the type of chemotherapy utilized in HIPEC. A recent prospective analysis found that PFS was significantly increased with paclitaxel/cisplatin-based HIPEC compared to single-agent cisplatin-based HIPEC [10]. These preliminary findings suggest that the combination of both chemotherapies may be superior to cisplatin alone. Overall survival data is not yet mature. Along the same line, though carboplatin and cisplatin have similar mechanisms of action [13], they can result in different patient outcomes. Zivanovic et al demonstrated that carboplatin and cisplatin had similar safety profiles in the use of HIPEC for treatment of recurrent ovarian cancer during secondary cytoreductive surgery [11]. Nevertheless, HIPEC with carboplatin at the time of IDS was not superior to IDS alone in terms of clinical outcomes in this study. These results illustrate that platinum-based HIPEC chemotherapy regimens have varying efficacies, particularly when used alone and when used with additional chemotherapeutic agents. Numerous types and regimens of chemotherapy are also available for other malignancies, as discussed below in HIPEC in Peritoneal Cancers.
While the majority of EOC patients initially respond to platinum-based therapy, they often become platinum resistant (PR) over time, defined as experiencing a disease recurrence within six months of platinum-based therapy [12]. The determination of platinum resistance confers poor prognosis for patients as remaining therapeutic options have limited efficacy. Several studies have suggested that PR patients receiving HIPEC had no alteration in survival rate after HIPEC compared to that of platinum sensitive (PS) patients [13,14]. More recently, a retrospective study compared PFS and OS in platinum sensitive and platinum resistant EOC patients after CRS and HIPEC to determine if CRS with HIPEC in PR patients can overcome PR treatment disadvantages [15]. Patients showed an improved treatment-free interval (TFI) when treated with a combination of HIPEC and secondary CRS, regardless of platinum sensitivity. PS patients had an improved survival to a higher degree than that of the PR patients. Complete tumor resection resulted in significantly increased PFS in PS patients. Study limitations included the low number of PR patients and lack of complete resection in nearly half the PR patients. Results suggested that the combination of CRS and HIPEC in PR patients extends the TFI and thus this combination could be a treatment option for patients with PR EOC [15].
It has been demonstrated that homologous recombination related (HRR) mutations extend EOC patient PFS and OS [16]. Homologous recombination (HR) is a double stranded DNA repair mechanism in which damaged chromosomes are repaired and cells are protected from chromosomal aberrations. Disruptions in this pathway result in homologous recombination deficiency (HRD), which impair a cells ability to repair the DNA damaged by chemotherapy [17]. The process of HR includes several mediator genes including BRCA1 and BRCA2, however these are also among the most mutated HR genes and commonly present in ovarian cancer [18]. Mutations in BRCA1/2 increases the lifetime risk of ovarian cancer development by 40% [19]. Studies show EOC patients with a BRCA mutation have increased chemosensitivity, specifically to platinum-based therapeutics. BRCA mutational status similarly impacts EOC patient response to HIPEC treatment, as hyperthermia impairs the BRCA protein function [20,21,22,23]. An exploratory analysis of the OVHIPEC-1 trial performed by Koole et al found that patients without BRCA mutations had increased benefit from HIPEC when compared to those with BRCA mutations [21]. The researchers evaluated tissue samples and tumor DNA from 200 patients with stage III ovarian cancer originally enrolled in the trial and categorized them by BRCA status and HRD status based on copy number variation profile. This study found no significant survival benefit to HIPEC among patients with BRCA mutations. Similarly, patients with HRD or BRCA wild type tumors also appear to benefit more from HIPEC than those without HRD. HRD classification may play and increasing role in selecting optimal patients for HIPEC therapy.
The reduction of recurrence seen from HIPEC treatment is promising as the majority of patients with advanced disease experience recurrence within five years [22]. Patients with recurrent disease report a significant impact on their overall quality of life compared to that of women without recurrence, including daily pain, increased emotional burden, activity limitations, and issues concentrating [23]. A single institution cohort study of advanced or recurrent EOC patients receiving cytoreductive surgery (CRS) and HIPEC was analyzed to identify patterns of recurrence (pelvic, upper abdominal, or extraperitoneal) and whether there exists an association between location of recurrence and patient survival [24]. Results revealed half of the patients analyzed had recurrence outside the peritoneal cavity after HIPEC following CRS. Recurrence location did not impact PFS or OS in HIPEC patients. As HIPEC in ovarian cancer therapy specifically targets the peritoneal cavity, this pattern of spread suggests that HIPEC maintains local control of EOC and may reduce recurrence within the peritoneal cavity [24].
Skepticism surrounds HIPEC as it is perceived to be highly toxic, causing complications [25]. Current HIPEC trials have not reported any adverse effects yet further analysis into patient’s quality of life post-HIPEC is necessary for continuation of HIPEC as a safe therapeutic. In a phase-III randomized trial, patients diagnosed with advance stage EOC were assessed for any alterations in their health-related quality of life after CRS with and without HIPEC [26]. The study followed patients from before randomization into the trial through 12 months post-treatment including analysis after several rounds of adjuvant chemotherapy. Patient health-related quality of life was assessed via questionnaires at various time points. In patients receiving HIPEC during CRS, no impairment in health-related quality of life was observed. A secondary analysis of PFS and OS confirmed that HIPEC patients after interval CRS had both an extended PFS and OS, consistent with previous findings [3,9].
In summary, an extension in patient survival and reduction in recurrence rate is evident, yet the mechanistic benefit of HIPEC in advanced EOC remains unknown. Studies are highly supportive of the use of HIPEC in treatment of advanced EOC and indicate the extension of patient survival (Table 1). Based on existing data, the efficacy of HIPEC can be impacted by procedural factors, such as timing of surgery in the patient’s treatment course and type of chemotherapy utilized. As previously outlined, different chemotherapy regimens may have altered efficacy when used alone vs in combination with other agents. Similarly, platinum sensitivity is a patient-related factor that affects the utility of HIPEC therapy. Molecular tumor-related factors, including deficiencies in homologous recombination and BRCA status, further influence how patients respond to HIPEC therapy. Additional research evaluating the mechanistic benefits of HIPEC is warranted.
2.1. HIPEC in Peritoneal Cancers
Peritoneal carcinomatosis (PC) is characterized by malignancy on the peritoneal surface and refers to any primary cancer that has spread to the abdominal cavity. Gastrointestinal and gynecologic cancers are among the most common to result in PC. A diagnosis of PC is likely fatal and is most often treated with palliative care [27]. A retrospective study of advance stage gastric cancer patients with or without PC aimed to determine survival benefit of HIPEC. In patients receiving CRS and HIPEC, a 6.2 month increase in OS was seen compared to patients given palliative chemotherapy. Patient PC status did not show difference in survival after CRS and HIPEC. Although survival was extended by over six months, all patients experienced recurrence and ultimately succumbed to disease [27].
Pancreatic cancer is among the non-gynecological cancers often presenting with peritoneal carcinomatosis with an average survival of about three months. A combination of CRS and HIPEC is the standard of care for colorectal cancers with peritoneal carcinomatosis. A retrospective study of pancreatic cancer patients with confirmed PC aimed to determine survival benefit of HIPEC [28]. Four of six patients enrolled in the study had an extended RFS of greater than 12 months. Results indicate HIPEC may have OS benefit in pancreatic carcinomas if in combination with complete cytoreduction [28].
Mucinous adenocarcinoma is a rare subtype of advanced stage colorectal cancer (CRC) and exhibits poor response to chemotherapy [29]. HIPEC at time of CRS in metastatic CRC has been reported, though limited data suggests benefits of mucinous CRC. A retrospective analysis of CRC patients diagnosed with peritoneal metastases with or without primary mucinous CRC was conducted to determine HIPEC survival benefit [30]. Patient peritoneal metastases included synchronous and metachronous. Historically, patients with synchronous metastases have a more advanced stage of primary disease with advanced tumor and nodules at diagnosis, compared to that of patients with metachronous metastases [31]. Results reveal HIPEC at time of CRS is beneficial in both mucinous and non-mucinous CRC in patients with metachronous peritoneal metastases. However, mucinous CRC patients with synchronous peritoneal metastases had a significantly worsened survival after treatment with CRS and HIPEC with a median survival decrease of 22.4 months. The use of HIPEC in mucinous synchronous patients is not supported, yet showed favorable benefit in CRC with metachronous metastases [30].

Table 1.
Summary of clinical findings indicating HIPEC survival benefit.
| Author | Year | Study Type | N | Study Details | OS Benefit | PFS Benefit | RFS Benefit |
|---|---|---|---|---|---|---|---|
| Lim et al | 2022 | Single-Blind Randomized | 184 | HIPEC + interval CRS after NACT in ovarian cancer | 13.6 months | 2 months | N/A |
| Ghirardi et al | 2022 | Retrospective | 70 | HIPEC + BRCA mutational status in EOC | No difference between BRCA status | No difference between BRCA status | N/A |
| Herold et al | 2022 | Retrospective | 218 | CRS + HIPEC in mucinous CRC | Could not be determined | Could not be determined | Could not be determined |
| Costales et al | 2021 | Retrospective | 48 | PS vs PR EOC patients given HIPEC after CRS | median 26.9 months in PR patients | N/A | 11.2 months in PS patients |
| Van Driel et al | 2018 | Open-Label Randomized | 245 | Interval CRS ± HIPEC for EOC | 11.8 months | N/A | 3.5 months |
| Tentes et al | 2018 | Retrospective | 6 | CRS + HIPEC for PC | N/A | N/A | >12 months |
| Boerner et al | 2016 | Retrospective | 38 | CRS + HIPEC for gastric cancer + PC | 6.2 months | N/A | N/A |
| Safra et al | 2014 | Case-Control Study | 27 | CRS ± HIPEC ± BRCA mutation in EOC | Not reached at time of analysis (70% patients alive) | 9 months, no difference in BRCA status | N/A |
3. Animal Models of HIPEC
An important aspect in elucidating the mechanistic benefit of HIPEC is the development of an animal model to effectively recapitulate clinical HIPEC. Helderman et al. reviewed the current in vivo HIPEC models including the challenges and clinical relevance of each experimental design [32]. Current study designs involve invasive murine models emulating the human surgical technique. Murine models involve either an open or closed perfusion pump system (Figure 2). The open (coliseum) perfusion system involves exposure of the abdominal cavity via a vertical midline laparotomy, securing skin to a ring stand, while maintaining sterility. The closed perfusion system involves the introduction of double inflow and outflow catheters through the upper and lower quadrants of the abdomen. Constant temperature is ideally maintained through study duration. Coliseum and closed perfusion systems have shown success in mimicking clinical HIPEC, although neither method of perfusion is without complication. Coliseum perfusion is beneficial as intraoperative organ manipulation is feasible and several studies report total animal survival using the coliseum system; however, reported heat loss limits total clinical recapitulation [33,34]. Simultaneous studies utilizing the closed perfusion system reported a multitude of complications including organ suction into outflow catheters, perfusate leakage, and blood loss at catheter insertion sites [33,34]. Closed and open perfusion systems both allow for one animal treatment at a time, limiting study cohorts to very few animals. Studies report no animal deaths prior to study endpoint, though most studies follow animals for only days post-HIPEC [35]. Miailhe et al sought to develop a less-invasive ovarian cancer HIPEC mouse model while limiting complications observed in previous reports [36]. Ten tumor-bearing mice were utilized in a closed perfusion system, in which inflow and outflow catheters were placed at specific locations. A single inflow catheter into the left hypochondria and a single outflow catheter into the left iliac fossa were introduced. Twelve minutes of 43oC oxaliplatin was infused while mice were kept under constant general anesthesia. All animals survived the duration of treatment with no reported complications. Study limitations include one mouse treatment at a time and the inability to manually stir the perfusate in the abdomen as is possible in the coliseum system. A key component in clinical HIPEC is the combination of CRS prior to HIPEC treatment. The lack of debulking primary tumor in the animals prior to heat is a major study limitation. This improved model of HIPEC showed limited morbidity as only one mouse died prior to study endpoint [36]. The need for a functional non-invasive animal model for total recapitulation of clinical HIPEC remains, though success in current modalities have reported HIPEC benefit in murine models.
Studies using primarily rats and mice have reported the HIPEC procedure is possible in animal models, though limited data exists on the mechanistic benefits HIPEC provides. HIPEC perfusion in colorectal tumor bearing rats resulted in significantly reduced tumor load in the HIPEC group compared to that of the control and chemotherapeutic only groups [37]. HIPEC targeting ovarian cancer stem-like cells (CSCs) showed significant therapeutic effect in immunocompetent mice compared to that of immunodeficient mice [38]. CSCs are a subpopulation of cancer cells exhibiting chemoresistance, thus CSCs may be enriched by chemotherapy [39]. Using the coliseum perfusion system, IP hyperthermia (heated PBS) was infused into the peritoneal cavity for 20 minutes, maintaining a constant temperature. An IP injection of chemotherapeutics was administered immediately after hyperthermia treatment in the treatment group. Mice were then kept under a heat lamp until awake from anesthesia. Results reveal the combination of chemotherapy and IP hyperthermia showed antitumor effects as tumor size was significantly decreased after treatment compared to that of hyperthermia and control groups. Enhancement of antitumor effects was related to the enrichment of chemotherapy by hyperthermia thus reducing the proportion of CSCs in immunocompetent mice. Hyperthermia overcame the chemoresistance, reducing the CSC proportion, in presence of immune system [38].
3.1. Summary of Pre-Clinical Findings and Challenges
Challenges in the study of HIPEC in murine models include the difficulty recapitulating the clinical HIPEC setting. Clinical HIPEC involves several rounds of neoadjuvant chemotherapy followed by interval debulking surgery and a 90-minute heated chemotherapy pumped through the peritoneal cavity. In reported murine HIPEC models, study cohorts are very small due to the nature of the procedure not allowing for multiple animals to be treated simultaneously. Procedure complications have been reported in nearly all cases, including organ suction into outflow catheters, bleeding, and heat loss. Though clinical HIPEC is not completely without complication, heat loss during murine HIPEC poses a major limitation as constant heat is the main premise of HIPEC treatment. The closed perfusion system is a promising model to mimic clinical HIPEC and has successfully shown HIPEC efficacy in reducing murine tumor burden [37,38,39,40,41]. Studies report the use of heated PBS as an IP hyperthermia, though analysis of heated chemotherapeutics would more closely follow human HIPEC. The current unmet need in the current murine models is the low throughput to permit larger cohorts to investigate the impact of the immune system more robustly in HIPEC benefit.
4. Mechanisms of Hyperthermia with or without Chemotherapy
4.1. Heat Shock Response
Stressful conditions including heat shock and tumor presence increase synthesis of a family of intracellular heat shock proteins (HSPs) [42]. These molecular chaperones are expressed in all cells and are critical for a multitude of functions including protein folding, promotion of immune response, and enhancement of signal pathways essential for cell survival [43,44]. The release of intracellular HSPs in response to heat is dependent on heat shock transcription factor 1 (HSF1), which upon activation by stressors binds to heat shock gene promotors. These extracellular HSPs express pro-immunity function and have been shown to promote antitumor immunity [45]. Extracellular HSPs promote maturation of dendritic cells (DCs) thus activating the innate immune system [46]. In response to heat shock (42-45oC), HSPs are released from cells and bind to peptides forming HSP-peptide complexes [47]. The HSP-peptide complexes shuttle antigenic peptides into the major histocompatibility complex (MHC) class I pathway of antigen-presenting cells (APCs) [42] (Figure 3). The MHC-I APC peptide complex binds to the T cell antigen receptor (TCR) on the surface of T cells, leading to stimulation of the adaptive immune response via activation of CD8+ T cells. CD8+ T cells have shown significant anticancer effects as they produce cytokines targeting tumor tissue.
The picture of the role of HSPs is complex as many cancers exhibit overexpression of Hsp70 and Hsp90, known to be is associated with tumor promotion [48]. Due to involvement in multidrug resistance, metastasis, and tumor progression, Hsp90 has been identified as a target for anticancer therapy [48]. Inhibition of Hsp90 stimulates dissociation of HSF1 from Hsp90, activating the heat shock response, with increased expression of heat shock response genes. Simultaneous inhibition of HSF1 is suggested to improve Hsp90 inhibitor anticancer activity due to the HSF1 target genes containing drug resistance and antiapoptotic properties [48]. Inactivation of Hsp90 increases antitumor immune response thus making Hsp90 inhibitors a promising cancer therapeutic.
5. Hyperthermia Impact on the Immune System
A fever response is a key component to the presence of infection and inflammation and plays a vital role in immune activation, increasing pathogen defense mechanisms [49]. Although HSPs are induced via heat shock, febrile temperatures (38-41oC) are sufficient to promote HSP production [49]. Clinical results reveal antitumor immunity in the presence of hyperthermia via HSP production and activation of antigen presenting cells (APCs), resulting in lymphocyte trafficking to the tumor site [50]. Hyperthermia generates the release of HSP-peptide complexes and increases tumor antigens. Febrile temperatures are associated with activation of circulating neutrophils which are then recruited to local and distant sites such as tumors, though once temperatures surpass febrile range neutrophil function will be impaired [49]. Adaptive immune response is heightened during hyperthermia in that NK cells are recruited to the tumor sites under febrile temperatures with enhanced cytotoxicity [49]. The elevated cytotoxicity in NK cells can be linked to increased Hsp70, heat shock protein present in major cellular components, and decreased MHC-I expression by the tumor cells. Tumor cells have upregulated HSP production in response to heat resulting in enhanced antigen-specific cytotoxic T lymphocyte production [49].
The immune system is comprised of two components, innate and adaptive immunity, which work to prevent and limit invasion of unhealthy cells. Innate immune response is the immediate defense mechanism and provides a general response to foreign substances. Adaptive immune response is a slower, highly specific response that is long-lasting. Immune cells stem from precursor cells found in bone marrow. Myeloid progenitor stem cells are precursors for innate immune cells and include neutrophils, monocytes, DCs, and macrophages. Lymphoid progenitor stem cells are precursors for adaptive immune cells and include B cells, T cells, and natural killer (NK) cells, broadly categorized as lymphocytes. Antigens are foreign substances unrecognizable by the body, thus activating an immune response. Tumors possess a set of specific antigens recognizable by the immune system. APCs at tumor sites uptake the antigens and can create an immune response by activating lymphocytes. Cytotoxic lymphocytes then target tumor cells for destruction. Hyperthermia has the ability to improve this process by generation of HSPs and activation of APCs, heightening the immune response [50].
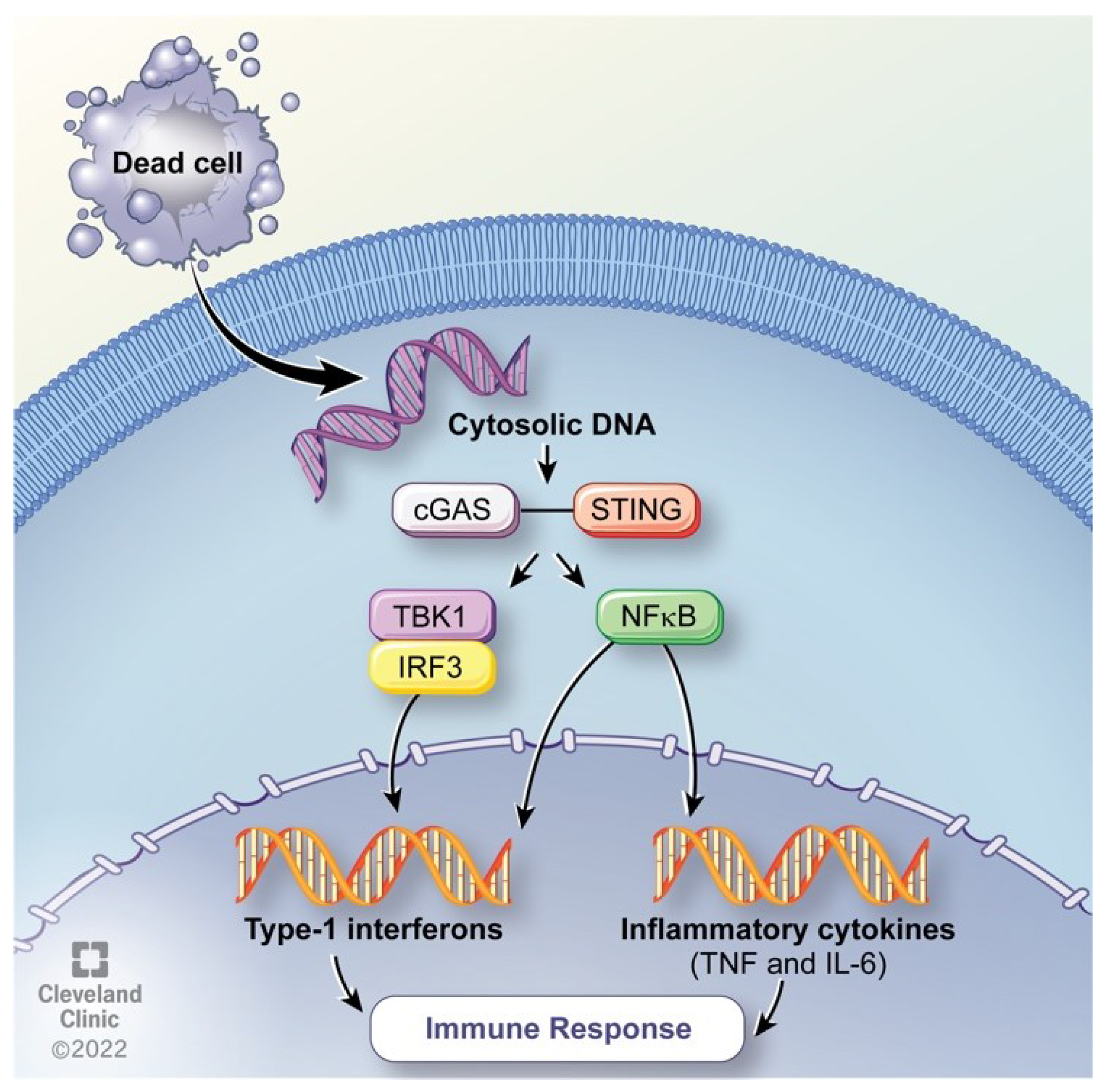
The cGAS-STING pathway is an innate immune system component [51] (Figure 4). Hyperthermia has been shown to promote the cGAS-STING pathway in macrophage like cells [52]. Cyclic GMP-AMP synthase (cGAS) is a protein coding gene which detects cytosolic DNA and activates the Stimulator of Interferon Genes (STING) pathway with a downstream effect of cytokine activation [53]. DNA is typically localized to the nucleus allowing for control of specialized functions including DNA damage repair and replication [54]. DNA crossing the plasma membrane must translocate across the cytoplasm for nuclear entry through the nuclear envelope [55]. DNA found in the cytoplasm therefore is a trigger for immune response activation, as the body recognizes cytosolic DNA as viral entry [56]. Cytosolic DNA is detected resulting in the expression of inflammatory genes, activating defense mechanisms. The cGAS-STING pathway has been discovered to play a vital role in detecting DNA in response to immune defense mechanisms [57]. cGAS interacts with double-stranded DNA (dsDNA) causing DNA ligands to bind with cGAS. Ligand binding induces conformational changes which allow for the catalyzation of ATP and GTP into cyclic GMP-AMP (cGAMP). cGAMP is a second messenger which binds to the surface receptor on the endoplasmic reticulum (ER), activating the Stimulator of Interferon Genes (STING) [58]. STING translocates from the ER to the ER-Golgi intermediate compartments at which TANK binding kinase-1 (TBK1) and interferon regulatory factor 3 (IRF3) are recruited. IRF3 translocates from the Golgi to the nucleus where transcription takes place resulting in expression of immune stimulated genes and type 1 interferons. Additionally, STING activates IKB kinase. IKB phosphorylates, mediating the activation of nuclear factor kappa B (NF-KB) activated inflammatory genes including Interleukin 6 (IL-6) and tumor necrosis factor (TNF) [58]. Activation of inflammatory genes elicits an immune response thus hyperthermia is implicated in promotion of immunity.
6. Hyperthermia Impact on Genome Instability
The hallmarks of cancer include genome instability and mutation. Heat causes DNA and protein damage and inhibits cell cycle progression, triggering apoptosis [59]. Hyperthermia induces DNA damage and in combination with chemotherapy has a synergistic effect with chemotherapy increasing sensitivity to chemotherapeutics [60]. Increased chemosensitivity has been attributed to impaired DNA damage repair mechanisms. Chemotherapy alone induces DNA damage thus in combination with heat, HR is impaired, increasing cancer cell death. To elucidate the effect of hyperthermia on HR, HR proficient mouse embryonic stem (ES) cells were radiosensitized at normothermic and hyperthermic temperatures and compared to that of HR deficient ES cells [61]. Quantification of genes showed HR-mediated gene targeting had significantly reduced efficiency in ES cells incubated at an elevated temperature. Results suggest hyperthermia inactivates HR repair mechanism [61] leaving cells reliant on other repair mechanisms such as Poly(ADP-ribose) polymerase-mediated DNA repair.
Poly(ADP-ribose) polymerase (PARP) is a family of proteins involved in DNA repair that when inhibited increases chemotherapy cytotoxicity [62]. PARP enzymes detect single-stranded DNA breaks and bind to the DNA-binding domain. This binding allows for synthesis and transfer of poly(ADP) ribose to acceptor proteins, thus recruiting repair proteins to the site of damaged DNA [58]. Poly(ADP) ribose is involved in repair of both single-stranded and double-stranded DNA breaks [58]. PARP1 is an enzyme involved in repair of single stranded DNA breaks, making PARP1 inhibitors prominent in cancer therapy. BRCA is a HR mediator gene commonly mutated in ovarian cancer. A mutation in BRCA wouldn’t allow for tumor suppression protein release. Hyperthermia on tumor cells resulted in BRCA degradation and HR inhibition [61]. Synergy between hyperthermia and chemotherapy may increase HIPEC benefit for BRCA positive patients via inhibition of PARP-1 dependent DNA replication [63]. The degradation of BRCA induces increased sensitivity of tumor cells to PARP-1 inhibitors [61]. The studies indicate hyperthermia causes HR proficient tumors to become sensitive to PARP-1 inhibitors, enhanced by HSP inhibition [61]. The combination of PARP-1 and HSP inhibition with HR inactivation via hyperthermia may be a promising therapeutic in cancer treatment.
7. Clinical Correlates on Immune and DNA Repair Activity in HIPEC
Hyperthermia induces an immune response with a downregulation of DNA repair pathways, allowing for tumor suppression. To analyze transcriptomic profile changes induced by HIPEC, pre- and post-HIPEC tumor samples were collected from ovarian cancer patients and compared to normal tissue [64]. HIPEC was given with carboplatin to the four patients included. Samples were analyzed using RNA sequencing. HIPEC induced upregulation of HSPs in tumor tissue with expression changes of Hsp90, Hsp70, Hsp40, and Hsp60 in both normal and tumor tissue. HIPEC with carboplatin induces increased immune related gene expression in normal tissue with increased protein folding in tumor tissue. Results support a combination of HIPEC with HSP inhibitors may provide increased therapeutic benefit as some HSPs inhibit protein misfolding thus promote tumor survival [64].
Tumors of EOC patients receiving HIPEC were collected for whole-transcriptomic analysis to elucidate HIPEC induced molecular changes [65]. Tumor samples from advanced stage EOC patients undergoing HIPEC were harvested before and after the procedure. Whole-transcriptomic sequencing, differential gene expression analysis, and gene enrichment analysis were performed. HIPEC induced upregulation of TNFα via the NF-KB pathway [65]. NF-KB is known to be activated through the cGAS-STING pathway and enhanced via hyperthermia [52]. Notably, HIPEC tumors had increased T cell activation as indicated by elevated expression of programmed cell death protein 1 (PD-1), a protein found on the surface of T cells and has a role in immune regulation. PD-1 expression was significantly increased in CD8+ T cells in the post-HIPEC tumor microenvironment. Elevated PD-1 expression post-HIPEC was correlated with improved patient PFS. Post-HIPEC tumors showed an upregulation of immune-related pathways and a downregulation of HR [65]. This analysis references in vitro analyses as preclinical data validation for comparison to human specimens, posing a major limitation of the analyses [65]. Significant elevation in CD8+ T cells, NK cells, and B lymphocyte cells has been observed 30 days after the HIPEC procedure via analysis of peripheral blood in patients with peritoneal metastasis [66]. Results are consistent with other studies showing stimulation of adaptive and innate immune response and inhibition of DNA repair mechanisms via HIPEC.
8. Conclusions and Prospects of Future Therapeutic Strategy
Advance stage EOC causes more deaths in women than any other gynecological malignancies. Although the standard of care shows initial benefit in treating disease, most patients experience reoccurrence and will ultimately succumb to the disease, indicating a critical need for improved therapy. HIPEC in the treatment of EOC shows significant extension in patient overall survival. Mechanistic insights as to how HIPEC improves patient overall survival provides the opportunity for clinical therapeutic advancement. Hyperthermia induces a multitude of effects making thermotherapy a promising aspect of cancer treatment. Heat activates an immune response, impairs DNA damage repair while inducing DNA damage, and has a synergistic effect with chemotherapy making cancer cells more sensitive to chemotherapeutics. Therapies reliant on DNA damage need also consider inhibition of DNA repair mechanisms. In parallel, heat induces synthesis of HSPs triggering innate and adaptive immunity via activation of cytotoxic T cells, DCs, and NK cells. Future therapeutic strategies need to include hyperthermic activation of the cGAS-STING pathway, apparently a key component in HIPEC efficacy. Increased cGAS-STING expression would promote increased activation of inflammatory genes leading to increased immune response and targeting the tumor for destruction. Additionally, simultaneous inhibition of Hsp90 and PARP-1 via hyperthermia could sensitize tumors to HR inactivation, impairing tumor cell repair mechanisms. A question for the field is why HIPEC treated tumors recur. Future studies need to address mechanisms and identify therapeutics to prolong efficacy perhaps by targeting immune surveillance. Animal models have exhibited significant improvement in tumor burden following HIPEC, yet none have reported mechanisms of benefit. HIPEC efficacy is ostensibly reliant on immune system involvement. Studies to elucidate the role of the immune system in HIPEC would provide a starting point to explaining the mechanistic benefit of HIPEC, which could be translated into clinical medicine.
Author Contributions
Conceptualization, O.H. and O.R.; resources, O.H., D.C., and O.R.; writing—original draft preparation, O.H.; writing—review and editing, O.H., D.C., A.D., R.D., O.R.; supervision, O.R. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Acknowledgments
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
All abbreviations were defined the first time they appeared in each article section. EOC: epithelial ovarian cancer; HIPEC: hyperthermic intraperitoneal chemotherapy; IDS: interval debulking surgery; OS: overall survival; PDS: primary debulking surgery; NACT: neoadjuvant chemotherapy; PFS: progression-free survival; CRS: cytoreductive surgery; PR: platinum resistant; PS: platinum sensitive; TFI: treatment-free interval; HRR: homologous recombination related; HR: homologous recombination; HRD: homologous recombination deficiency; WT: wild type/without mutation; PC: peritoneal carcinomatosis; CRC: colorectal cancer; CSC: cancer stem-like cell; HSP: heat shock protein; HSF1: heat shock transcription factor 1; DC: dendritic cell; MHC: major histocompatibility complex; APC: antigen-presenting cell; TCR: T cell antigen receptor; NK: natural killer; cGAS: cyclic GMP-AMP synthase; STING: stimulator of interferon genes; dsDNA: double-stranded DNA; cGAMP: cyclic GMP-AMP; ER: endoplasmic reticulum; TBK1: TANK binding kinase-1; IRF3: interferon regulatory factor 3; NF-κB: nuclear factor kappa B; IL-6: interleukin 6, ES: embryonic stem cells; PARP: poly(ADP-ribose) polymerase; PD-1: programmed cell death protein 1.
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA Cancer J Clin 2021, 71, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Mishra, M.; Singh, N.; Ghatage, P. Past, Present, and Future of Hyperthermic Intraperitoneal Chemotherapy (HIPEC) in Ovarian Cancer. Cureus 2021, 13, e15563. [Google Scholar] [CrossRef] [PubMed]
- van Driel, W.J.; Koole, S.; Schagen van Leeuwen, J.H.; Schreuder, H.W.R.; Hermans, R.H.M.; de Hingh, I.H.J.T.; van der Veldern, Jacobus, Arts; Massuger, L.F.A.G.; et al. Hyperthermic Intraperitoneal Chemotherapy in Ovarian Cancer. N Engl J Med 2018, 378, 230–240. [Google Scholar] [CrossRef] [PubMed]
- Clinic, C. Epithelial Ovarian Cancer, 2022.
- Torre, L.A.; Trabert, B.; DeSantis, C.E.; Miller, K.D.; Samimi, G.; Runowicz, C.D.; Gaudet, M.M.; Jemal, A.; Siegel, R.L. Ovarian cancer statistics, 2018. CA Cancer J Clin 2018, 68, 284–296. [Google Scholar] [CrossRef] [PubMed]
- Society, A.C. Cancer Statistics Center, http://cancerstatisticscenter.cancer.org (2022).
- Kurnit, K.C.; Fleming, G.F.; Lengyel, E. Updates and New Options in Advanced Epithelial Ovarian Cancer Treatment. Obstet Gynecol 2021, 137, 108–121. [Google Scholar] [CrossRef]
- Armstrong, D.K.; Alvarez, R.D.; Bakkum-Gamez, J.N.; Barroilhet, L.; Behbakht, K.; Berchuck, A.; Berek, J.S.; Chen, L.M.; Cristea, M.; DeRosa, M.; et al. NCCN Guidelines Insights: Ovarian Cancer, Version 1.2019. J Natl Compr Canc Netw 2019, 17, 896–909. [Google Scholar] [CrossRef]
- Lim, M.C.; Chang, S.J.; Park, B.; Yoo, H.J.; Yoo, C.W.; Nam, B.H.; Park, S.Y. Survival After Hyperthermic Intraperitoneal Chemotherapy and Primary or Interval Cytoreductive Surgery in Ovarian Cancer: A Randomized Clinical Trial. JAMA Surg 2022, 157, 374–383. [Google Scholar] [CrossRef]
- Chambers, C.; Horowitz, M.; Costales, A.; Yao, M.; Chichura, A.; Morton, M.; Gruner, M.; Rose, P.; Michener, C.; Debernardo, R. Cisplatin and paclitaxel are associated with improved progression-free survival compared to cisplatin alone during interval debulking surgery with hyperthermic intraperitoneal chemotherapy in women with advanced epithelial ovarian cancer. Science Direct 2021. [CrossRef]
- Dasari, S.; Tchounwou, P.B. Cisplatin in cancer therapy: molecular mechanisms of action. Eur J Pharmacol 2014, 740, 364–378. [Google Scholar] [CrossRef]
- Zivanovic, O. et al. Secondary Cytoreduction and Carboplatin Hyperthermic Intraperitoneal Chemotherapy for Platinum-Sensitive Recurrent Ovarian Cancer: An MSK Team Ovary Phase II Study. J Clin Oncol 2021, 39, 2594–2604. [CrossRef]
- Davis, A.; Tinker, A.V.; Friedlander, M. "Platinum resistant" ovarian cancer: what is it, who to treat and how to measure benefit? Gynecol Oncol 2014, 133, 624–631. [Google Scholar] [CrossRef] [PubMed]
- Spiliotis, J.; Halkia, E.; Lianos, E.; Kalantzi, N.; Grivas, A.; Efstathiou, E.; Giassas, S. Cytoreductive surgery and HIPEC in recurrent epithelial ovarian cancer: a prospective randomized phase III study. Ann Surg Oncol 2015, 22, 1570–1575. [Google Scholar] [CrossRef] [PubMed]
- Bakrin, N.; Bereder, J.M.; Decullier, E.; Classe, J.M.; Msika, S.; Lorimier, G.; Abboud, K.; Meeus, P.; Ferron, G.; Quenet, F.; et al. Peritoneal carcinomatosis treated with cytoreductive surgery and Hyperthermic Intraperitoneal Chemotherapy (HIPEC) for advanced ovarian carcinoma: a French multicentre retrospective cohort study of 566 patients. Eur J Surg Oncol 2013, 39, 1435–1443. [Google Scholar] [CrossRef] [PubMed]
- Costales, A.B.; Chambers, L.; Chichura, A.; Rose, P.G.; Mahdi, H.; Michener, C.M.; Yao, M.; Debernardo, R. Effect of platinum sensitivity on the efficacy of hyperthermic intraperitoneal chemotherapy (HIPEC) in recurrent epithelial ovarian cancer. J Gynecol Obstet Hum Reprod 2021, 50, 101844. [Google Scholar] [CrossRef]
- Norquist, B.M.; Brady, M.F.; Harrell, M.I.; Walsh, T.; Lee, M.K.; Gulsuner, S.; Bernards, S.S.; Casadei, S.; Burger, R.A.; Tewari, K.S.; et al. Mutations in Homologous Recombination Genes and Outcomes in Ovarian Carcinoma Patients in GOG 218: An NRG Oncology/Gynecologic Oncology Group Study. Clin Cancer Res 2018, 24, 777–783. [Google Scholar] [CrossRef] [PubMed]
- Qi, Y.; Zhang, Y.; Shi, Y.; Yao, S.; Dai, M.; Cai, H. Cytoreductive Surgery (CRS) Combined With Hyperthermic Intraperitoneal Chemotherapy (HIPEC) for Platinum-Sensitive Recurrence Epithelial Ovarian Cancer With HRR Mutation: A Phase III Randomized Clinical Trial. Technol Cancer Res Treat 2022, 21, 15330338221104565. [Google Scholar] [CrossRef] [PubMed]
- Toh, M.; Ngeow, J. Homologous Recombination Deficiency: Cancer Predispositions and Treatment Implications. The Oncologist 2021, 26, e1526–e1537. [Google Scholar] [CrossRef] [PubMed]
- Foulkes, W.D. BRCA1 and BRCA2: chemosensitivity, treatment outcomes and prognosis. Fam Cancer 2006, 5, 135–142. [Google Scholar] [CrossRef]
- Ghirardi, V.; De Felice, F.; D’Indinosante, M.; Bernardini, F.; Giudice, M.T.; Fagotti, A.; Scambia, G. Hyperthermic intraperitoneal chemotherapy (HIPEC) after primary debulking surgery in advanced epithelial ovarian cancer: Is BRCA mutational status making the difference? Cancer Treat Res Commun 2022, 31, 100518. [Google Scholar] [CrossRef] [PubMed]
- Koole, S.N.; Schouten, P.C.; Hauke, J.; Kluin, R.J.C.; Nederlof, P.; Richters, L.K.; Krebsbach, G.; Sikorska, K.; Alkemade, M.; Opdam, M.; et al. Effect of HIPEC according to HRD/BRCAwt genomic profile in stage III ovarian cancer: Results from the phase III OVHIPEC trial. Int J Cancer 2022, 151, 1394–1404. [Google Scholar] [CrossRef]
- Safra, T.; Grisaru, D.; Inbar, M.; Abu-Abeid, S.; Dayan, D.; Matceyevsky, D.; Weizman, A.; Klausner, J.M. Cytoreduction surgery with hyperthermic intraperitoneal chemotherapy in recurrent ovarian cancer improves progression-free survival, especially in BRCA-positive patients- a case-control study. J Surg Oncol 2014, 110, 661–665. [Google Scholar] [CrossRef] [PubMed]
- Colombo, N.; Lorusso, D.; Scollo, P. Impact of Recurrence of Ovarian Cancer on Quality of Life and Outlook for the Future. Int J Gynecol Cancer 2017, 27, 1134–1140. [Google Scholar] [CrossRef] [PubMed]
- Chambers, L.M.; Yao, M.; Morton, M.; Gruner, M.; Chichura, A.B.; Horowitz, M.; Costales, A.; Rose, P.G.; Michener, C.M.; Debernardo, R. Patterns of recurrence in women with advanced and recurrent epithelial ovarian cancer treated with cytoreductive surgery and hyperthermic intraperitoneal chemotherapy. Gynecol Oncol 2021, 161, 389–395. [Google Scholar] [CrossRef] [PubMed]
- Mehta, S.S.; Gelli, M.; Agarwal, D.; Goéré, D. Complications of Cytoreductive Surgery and HIPEC in the Treatment of Peritoneal Metastases. Indian J Surg Oncol 2016, 7, 225–229. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Lee, D.E.; Lee, Y.; Ha, H.I.; Chang, Y.J.; Chang, S.J.; Park, S.Y.; Lim, M.C. Quality of life outcomes from the randomized trial of hyperthermic intraperitoneal chemotherapy following cytoreductive surgery for primary ovarian cancer (KOV-HIPEC-01). J Gynecol Oncol 2022, 33, e54. [Google Scholar] [CrossRef] [PubMed]
- Boerner, T.; Graichen, A.; Jeiter, T.; Zemann, F.; Renner, P.; Marz, L.; Soeder, Y.; Schlitt, H.J.; Piso, P.; Dahlke, M.H. ; CRS-HIPEC Prolongs Survival but is Not Curative for Patients with Peritoneal Carcinomatosis of Gastric Cancer. Ann Surg Oncol 2016, 23, 3972–3977. [Google Scholar] [CrossRef] [PubMed]
- Tentes, A.A.; Pallas, N.; Karamveri, C.; Kyziridis, D.; Hristakis, C. Cytoreduction and HIPEC for peritoneal carcinomatosis of pancreatic cancer. J buon 2018, 23, 482–487. [Google Scholar]
- Luo, C.; Cen, S.; Ding, G.; Wu, W. Mucinous colorectal adenocarcinoma: clinical pathology and treatment options. Cancer Commun (Lond) 2019, 39, 13. [Google Scholar] [CrossRef] [PubMed]
- Herold, Z.; Acs, M.; Szasz, A.M.; Olasz, K.; Hussong, J.; Mayr, M.; Dank, M.; Piso, P. Patients with Metachronous Peritoneal Metastatic Mucinous Colorectal Adenocarcinoma Benefit More from Cytoreductive Surgery (CRS) and Hyperthermic Intraperitoneal Chemotherapy (HIPEC) than Their Synchronous Counterparts. Cancers 2022, 14, 3978. [Google Scholar] [CrossRef]
- Lurvink, R.J.; Bakkers, C.; Rijken, A.; van Erning, F.N.; Nienhuijs, S.W.; Burger, J.W.; Creemers, G.J.; Verhoef, C.; Lemmens, V.E.; De Hingh, I.H. Increase in the incidence of synchronous and metachronous peritoneal metastases in patients with colorectal cancer: A nationwide study. Eur J Surg Oncol 2021, 47, 1026–1033. [Google Scholar] [CrossRef]
- Helderman, R.; Loke, D.R.; Tanis, P.J.; Tuynman, J.B.; Ceelen, W.; de Hingh, I.H.; van der Speeten, K.; Franken, N.A.P.; Oei, A.L.; Kok, H.P.; Crezee, J. Preclinical In Vivo-Models to Investigate HIPEC; Current Methodologies and Challenges. Cancers (Basel) 2021, 13. [Google Scholar] [CrossRef] [PubMed]
- M. Peterson, E.M.-L.; B. McCarthy, B. Levi-Polyachenko. Survival Mouse Model of Intraperitoneal Perfusion Mimicking Hyperthermic Intraperitoneal Chemotherapy (HIPEC). Academic Surgical Congress (2018).
- McCabe-Lankford, E.; Peterson, M.; McCarthy, B.; Brown, A.J.; Terry, B.; Galarza-Paez, L.; Levi-Polyachenko, N. Murine Models of Intraperitoneal Perfusion for Disseminated Colorectal Cancer. J Surg Res 2019, 233, 310–322. [Google Scholar] [CrossRef] [PubMed]
- Liesenfeld, L.F.; Wagner, B.; Hillebrecht, H.C.; Brune, M.; Eckert, C.; Klose, J.; Schmidt, T.; Buchler, M.W.; Schneider, M. HIPEC-Induced Acute Kidney Injury: A Retrospective Clinical Study and Preclinical Model. Ann Surg Oncol 2022, 29, 139–151. [Google Scholar] [CrossRef] [PubMed]
- Miailhe, G.; Arfi, A.; Mirshahi, M.; Eveno, C.; Pocard, M.; Touboul, C. A new animal model for hyperthermic intraperitoneal chemotherapy (HIPEC) in tumor-bearing mice in the treatment of peritoneal carcinomatosis of ovarian origin. J Visc Surg 2018, 155, 183–189. [Google Scholar] [CrossRef] [PubMed]
- Pelz, J.O.; Doerfer, J.; Hohenberger, W.; Meyer, T. A new survival model for hyperthermic intraperitoneal chemotherapy (HIPEC) in tumor-bearing rats in the treatment of peritoneal carcinomatosis. BMC Cancer 2005, 5, 56. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.C.; Hsu, Y.T.; Chang, C.L. Hyperthermic intraperitoneal chemotherapy enhances antitumor effects on ovarian cancer through immune-mediated cancer stem cell targeting. Int J Hyperthermia 2021, 38, 1013–1022. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Lv, L.; Yang, K. Chemotherapy targeting cancer stem cells. Am J Cancer Res 2015, 5, 880–893. [Google Scholar] [PubMed]
- Wagner, B.R.; Adamus, A.L.; Sonnecken, D.; Vahdad, R.; Jank, P.; Denkert, C.; Mahnken, A.H.; Seitz, G. Establishment of a new valid animal model for the evaluation of hyperthermic intraperitoneal chemotherapy (HIPEC) in pediatric rhabdomyosarcoma. Pediatr Blood Cancer 2021, 68, e29202. [Google Scholar] [CrossRef] [PubMed]
- Graziosi, L.; Mencarelli, A.; Renga, B.; Santorelli, C.; Cantarella, F.; Bugiantella, W.; Cavazzoni, E.; Donini, A.; Fiorucci, S. Gene expression changes induced by HIPEC in a murine model of gastric cancer. In Vivo 2012, 26, 39–45. [Google Scholar]
- Wallin, R.P.; Lundqvist, A.; More, S.H.; von Bonin, A.; Kiessling, R.; Ljunggren, H.G. Heat-shock proteins as activators of the innate immune system. Trends Immunol 2002, 23, 130–135. [Google Scholar] [CrossRef]
- Dubey, A.; Prajapati, K.S.; Swamy, M.; Pachauri, V. Heat shock proteins: a therapeutic target worth to consider. Vet World 2015, 8, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Dubrez, L.; Causse, S.; Borges Bonan, N.; Dumétier, B.; Garrido, C. Heat-shock proteins: chaperoning DNA repair. Oncogene 2020, 39, 516–529. [Google Scholar] [CrossRef] [PubMed]
- Calderwood, S.K.; Gong, J.; Murshid, A. Extracellular HSPs: The Complicated Roles of Extracellular HSPs in Immunity. Front Immunol 2016, 7, 159. [Google Scholar] [CrossRef] [PubMed]
- Brenu, E.W.; Staines, D.R.; Tajouri, L.; Huth, T.; Ashton, K.J.; Marshall-Gradisnik, S.M. Heat shock proteins and regulatory T cells. Autoimmune Dis 2013, 2013, 813256. [Google Scholar] [CrossRef] [PubMed]
- Tsan, M.F.; Gao, B. Heat shock protein and innate immunity. Cell Mol Immunol 2004, 1, 274–279. [Google Scholar] [PubMed]
- Park, H.K.; Yoon, N.G.; Lee, J.E.; Hu, S.; Yoon, S.; Kim, S.Y.; Hong, J.H.; Nam, D.; Chae, Y.C.; Park, J.B.; Kang, B.H. Unleashing the full potential of Hsp90 inhibitors as cancer therapeutics through simultaneous inactivation of Hsp90, Grp94, and TRAP1. Exp Mol Med 2020, 52, 79–91. [Google Scholar] [CrossRef]
- Evans, S.S.; Repasky, E.A.; Fisher, D.T. Fever and the thermal regulation of immunity: the immune system feels the heat. Nat Rev Immunol 2015, 15, 335–349. [Google Scholar] [CrossRef] [PubMed]
- Skitzki, J.J.; Repasky, E.A.; Evans, S.S. Hyperthermia as an immunotherapy strategy for cancer. Curr Opin Investig Drugs 2009, 10, 550–558. [Google Scholar] [PubMed]
- Decout, A.; Katz, J.D.; Venkatraman, S.; Ablasser, A. The cGAS-STING pathway as a therapeutic target in inflammatory diseases. Nat Rev Immunol 2021, 21, 548–569. [Google Scholar] [CrossRef]
- Khan, I.U.; Brooks, G.; Guo, N.N.; Chen, J.; Guo, F. Fever-range hyperthermia promotes cGAS-STING pathway and synergizes DMXAA-induced antiviral immunity. Int J Hyperthermia 2021, 38, 30–37. [Google Scholar] [CrossRef]
- Hopfner, K.P.; Hornung, V. Molecular mechanisms and cellular functions of cGAS-STING signalling. Nat Rev Mol Cell Biol 2020, 21, 501–521. [Google Scholar] [CrossRef] [PubMed]
- Miller, K.N.; Victorelli, S.G.; Salmonowicz, H.; Dasgupta, N.; Liu, T.; Passos, J.F.; Adams, P.D. Cytoplasmic DNA: sources, sensing, and role in aging and disease. Cell 2021, 184, 5506–5526. [Google Scholar] [CrossRef]
- Bai, H.; Lester, G.M. S.; Petishnok, L.C.; Dean, D.A. Cytoplasmic transport and nuclear import of plasmid DNA. Biosci Rep 2017, 37. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.; Wu, J.; Du, F.; Chen, X.; Chen, Z.J. Cyclic GMP-AMP synthase is a cytosolic DNA sensor that activates the type I interferon pathway. Science 2013, 339, 786–791. [Google Scholar] [CrossRef] [PubMed]
- Motwani, M.; Pesiridis, S.; Fitzgerald, K.A. DNA sensing by the cGAS-STING pathway in health and disease. Nat Rev Genet 2019, 20, 657–674. [Google Scholar] [CrossRef] [PubMed]
- Kwon, J.; Bakhoum, S.F. The Cytosolic DNA-Sensing cGAS-STING Pathway in Cancer. Cancer Discov 2020, 10, 26–39. [Google Scholar] [CrossRef] [PubMed]
- Oei, A.L.; Vriend, L.E.; Crezee, J.; Franken, N.A.; Krawczyk, P.M. Effects of hyperthermia on DNA repair pathways: one treatment to inhibit them all. Radiat Oncol 2015, 10, 165. [Google Scholar] [CrossRef] [PubMed]
- Chang, M.; Hou, Z.; Wang, M.; Li, C.; Lin, J. Recent Advances in Hyperthermia Therapy-Based Synergistic Immunotherapy. Advanced Materials 2021, 33, 2004788. [Google Scholar] [CrossRef] [PubMed]
- Krawczyk, P.M.; Eppink, B.; Essers, J.; Stap, J.; Rodermond, H.; Odijk, H.; Zelensky, A.; van Bree, C.; Stalpers, L.J.; Buist, M.R.; et al. Mild hyperthermia inhibits homologous recombination, induces BRCA2 degradation, and sensitizes cancer cells to poly (ADP-ribose) polymerase-1 inhibition. Proc Natl Acad Sci U S A 2011, 108, 9851–9856. [Google Scholar] [CrossRef]
- Chen, A. PARP inhibitors: its role in treatment of cancer. Chin J Cancer 2011, 30, 463–471. [Google Scholar] [CrossRef]
- Schaaf, L.; Schwab, M.; Ulmer, C.; Heine, S.; Murdter, T.E.; Schmid, J.O.; Sauer, G.; Aulitzky, W.E.; van der Kuip, H. Hyperthermia Synergizes with Chemotherapy by Inhibiting PARP1-Dependent DNA Replication Arrest. Cancer Res 2016, 76, 2868–2875. [Google Scholar] [CrossRef] [PubMed]
- Moukarzel, L.A.; Ferrando, L.; Dopeso, H.; Stylianou, A.; Basili, T.; Pareja, F.; Da Cruz Paula, A.; Zoppoli, G.; Abu-Rustum, N.R.; Reis-Filho, J.S.; et al. Hyperthermic intraperitoneal chemotherapy (HIPEC) with carboplatin induces distinct transcriptomic changes in ovarian tumor and normal tissues. Gynecol Oncol 2022, 165, 239–247. [Google Scholar] [CrossRef] [PubMed]
- Dellinger, T.H.; Han, E.S.; Raoof, M.; Lee, B.; Wu, X.; Cho, H.; He, T.F.; Lee, P.; Razavi, M.; Liang, W.S.; et al. Hyperthermic Intraperitoneal Chemotherapy-Induced Molecular Changes in Humans Validate Preclinical Data in Ovarian Cancer. JCO Precis Oncol 2022, 6, e2100239. [Google Scholar] [CrossRef] [PubMed]
- Fiorentini, G.; Sarti, D.; Patriti, A.; Eugeni, E.; Guerra, F.; Masedu, F.; Mackay, A.R.; Guadagni, S. Immune response activation following hyperthermic intraperitoneal chemotherapy for peritoneal metastases: A pilot study. World J Clin Oncol 2020, 11, 397–404. [Google Scholar] [CrossRef]
Figure 1.
Hyperthermic Intraperitoneal Chemotherapy (HIPEC) treatment in a patient with primary ovarian cancer and peritoneal metastasis. HIPEC has shown an overall survival benefit of nearly 12 months and regression-free survival benefit of 3.5 months compared to standard of care alone.
Figure 1.
Hyperthermic Intraperitoneal Chemotherapy (HIPEC) treatment in a patient with primary ovarian cancer and peritoneal metastasis. HIPEC has shown an overall survival benefit of nearly 12 months and regression-free survival benefit of 3.5 months compared to standard of care alone.
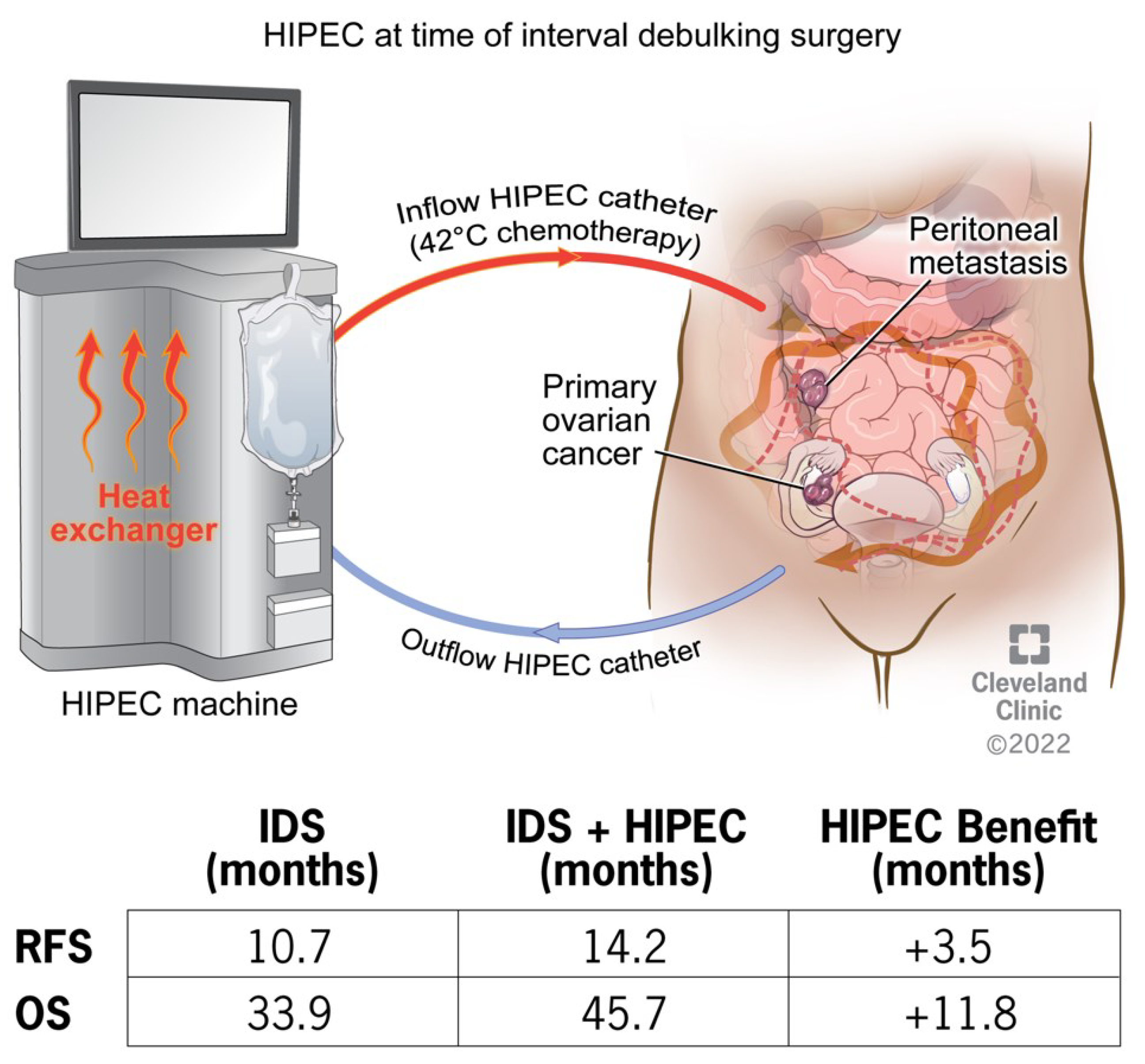
Figure 2.
Established murine model of heated chemotherapy treatment. Visualization of the closed system and open (coliseum) system.
Figure 2.
Established murine model of heated chemotherapy treatment. Visualization of the closed system and open (coliseum) system.
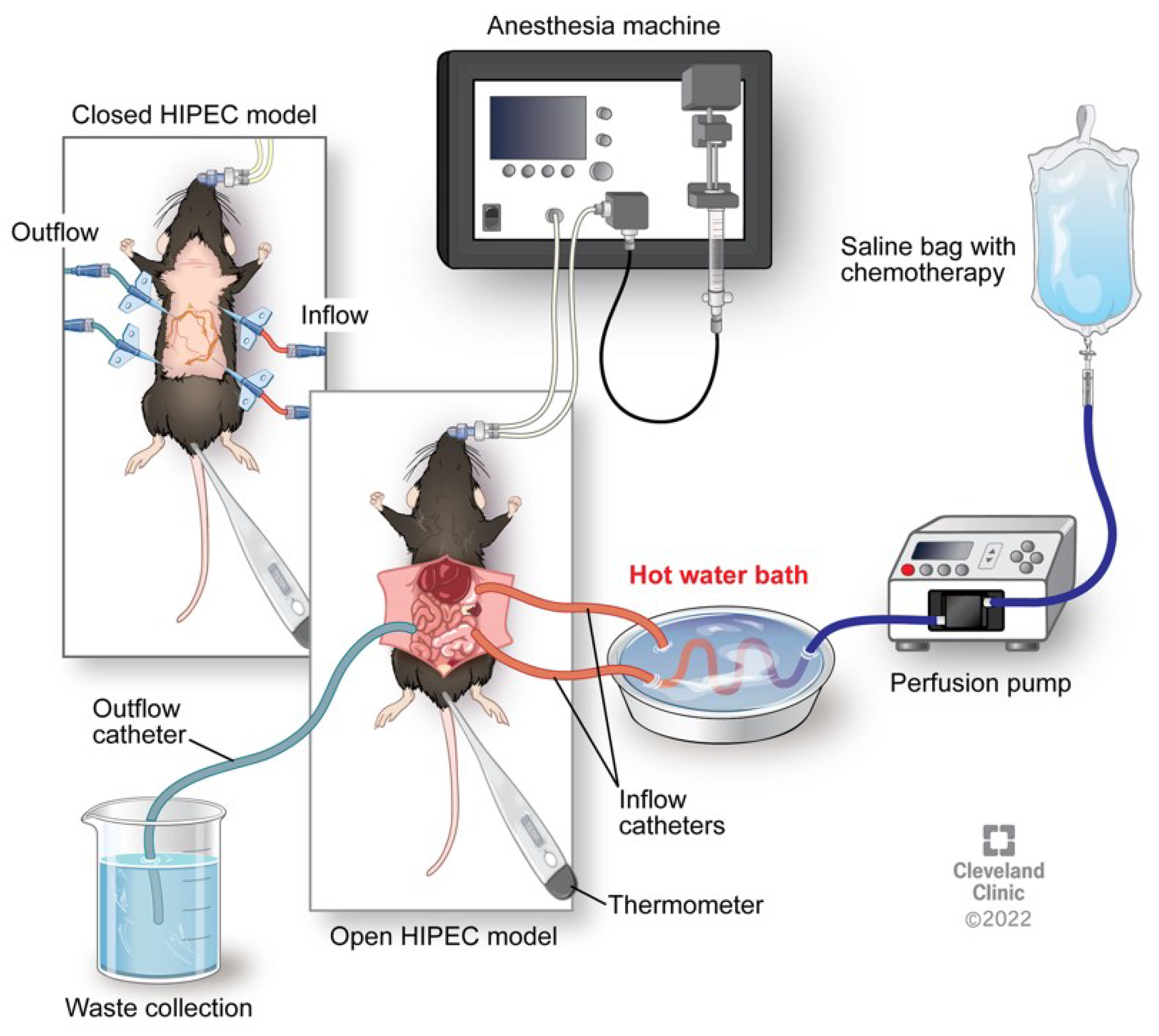
Figure 3.
Heat shock protein activation via hyperthermia with downstream cytokine activation, stimulating an immune response.
Figure 3.
Heat shock protein activation via hyperthermia with downstream cytokine activation, stimulating an immune response.
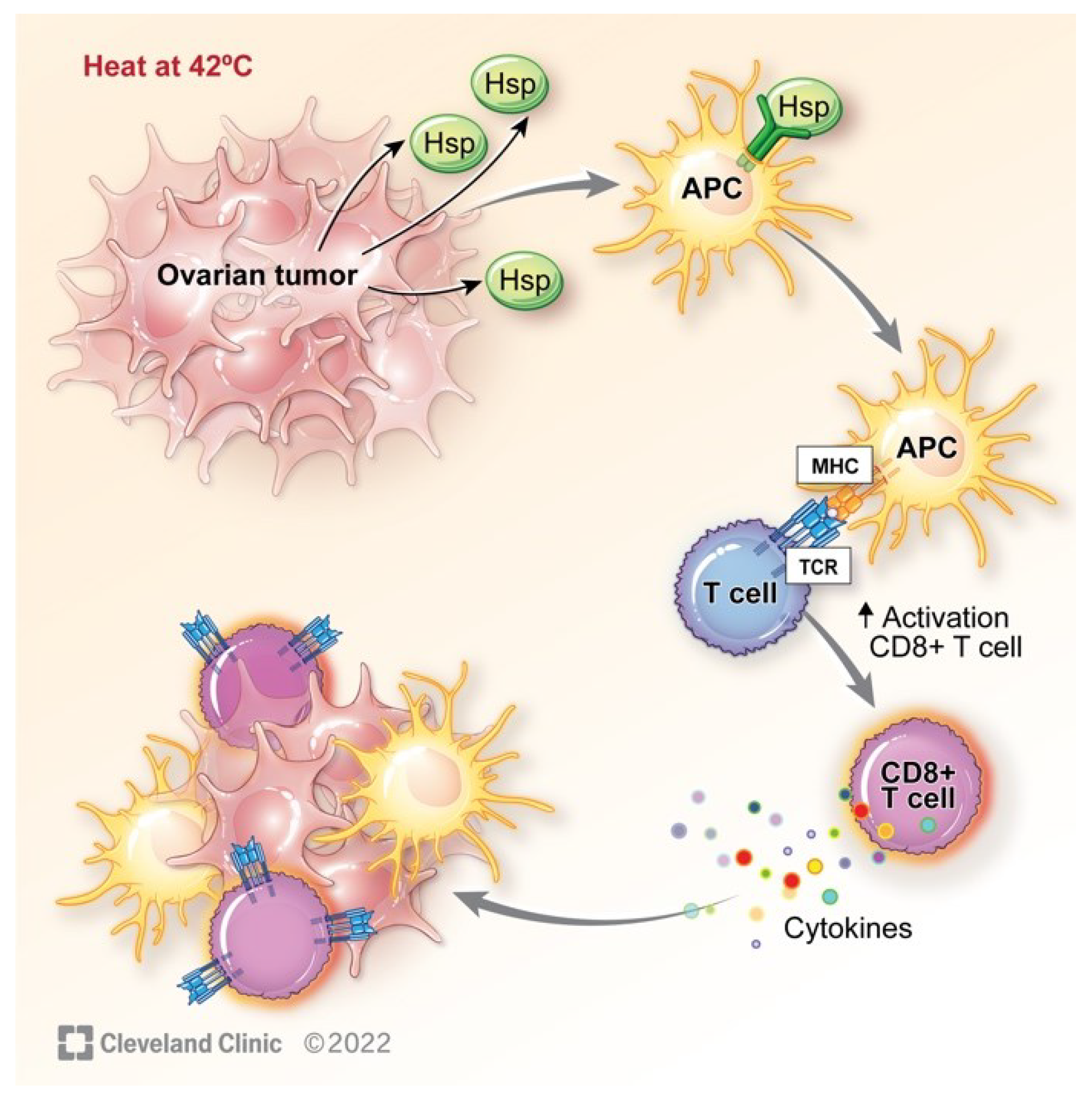
Figure 4.
cGAS-STING pathway activation via detection of cytosolic DNA.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



