
Submitted:
31 January 2023
Posted:
02 February 2023
You are already at the latest version
Abstract
Introduction The Pericapsular Nerve Group (PENG) block is a novel technique that allows for analgesia of the anterior hip capsule via the articular branches of the accessory obturator nerve and femoral nerve, which have a significant role in the innervation of the hip capsule. PENG blockade is effective in both adult and pediatric patients. However, there are no studies in the available literature on patients under five years of age. Herein, we describe our experience with two pediatric patients with hip dysplasia. Purpose This study aimed to evaluate the analgesic effect of the pericapsular nerves group (PENG) in small children undergoing hip surgery. Patients and methods This study included two patients, aged 2 and 4 years old, who qualified for hip surgery. General or spinal anesthesia with the addition of a PENG block was performed. During the procedure, the basic hemodynamic parameters were monitored. After the surgery, the patients received 15mg/kg-1 iv paracetamol every 6 hours to prevent rebound pain. The pain was assessed using the FALCC score. The 15mg/kg-1 metamizole was administered if the FLACC score was 3. In the FLACC score 4, the application of 0,2mg/kg-1 Nalpain was ordered. Results The patient's hemodynamic parameters were stable and within normal range. FLACC scores from all patients ranged from 0 and 3 in the first 24 h period. One patient required metamizole 12 hours after surgery. No evidence of block complications was observed. Conclusions This case series showed that PENG block provided adequate postoperative analgesia and assured opioid-free pain management. However, we are convinced that future randomized, controlled trials are needed in this field.
Keywords:
pain
; myelomeningocele
; paralytic dislocation of the hip
; congenital dislocation of the hip
; Dega transiliac osteotomy
Introduction
The use of local anesthesia for perioperative analgesia in hip surgery is a widespread practice that has been shown to reduce pain, perioperative complications, and postoperative opioid use [1]. In pediatric anesthesia, regional techniques are the mainstay of perioperative analgesia, either alone or as part of a multimodal analgesia strategy. Perioperative pain management is paramount after pediatric hip surgery. Inadequate analgesia can lead to patient and parent dissatisfaction, longer recovery, and extended hospital stays [2]. Local anesthesia is beneficial because it provides adequate pain relief while reducing opioid side effects [3,4].
Neural axis technology reduces pain scores in pediatric patients undergoing hip replacement surgery. However, positioning requirements, bilateral sensory and motor block, and urinary retention limit their use. Caudal and lumbar plexus blocks are the most common regional blocs, which are advanced techniques. However, many anesthesiologists are reluctant to use this occlusion because of the risk of complications such as colonic and renal puncture and total obstruction [5]. Our institutional practice includes the administration of spinal anesthesia with propofol sedation or general anesthesia with propofol and remifentanil, both regimens combined with an epidural catheter for children undergoing unilateral or bilateral hip surgery. This type of anesthesia effectively blocks nerves that innervate the hip. However, sometimes the analgesia is insufficient due to epidural catheter dislodgement or migration [6]. The use of an epidural catheter is also limited due to the need for continuous hemodynamic monitoring during postoperative analgesia [7].
Pericapsular Nerve Group (PENG) block was first described in 2018 by Girón-Arango et al. [8] for perioperative analgesia in hip fracture patients. This block was confirmed by a cadaveric dye study [9] that exhibited the pericapsular spread targeting only the sensory branches of the anterior hip capsule with a motor-sparing effect. PENG block extensively blocks innervation of the anterior hip capsule. This advanced ultrasound-guided technology numbs the obturator, paraobturator, and capsular sensory branches of the femoral nerve [9,10].
Unfortunately, there are no studies in the available literature on patients under five years of age. Therefore, we present the utilization of the PENG block for perioperative pain management in 2 pediatric patients undergoing unilateral surgery for pediatric hip dysplasia.
Material and Methods
Written informed consent was obtained from the parent for this scientific contribution.
Patients admitted to the W. Dega Orthopedic and Rehabilitation Clinical Hospital of Poznan University of Medical Sciences with a hip pathology as a part of a multidisciplinary care pathway
Upon discussion with the surgical team, the goals of care included a 2-day admission for postoperative pain control and complete avoidance of motor blockade. In addition, we offered a PENG block for postoperative pain management instead epidural catheter. In both cases, after the induction of anesthesia, the PENG block was performed (Figure 1 and Figure 2).
The patients were kept supine during the focal block. A low-frequency linear transducer (2–5 MHz) was placed in a transverse plane along the left inferior anterior iliac spine (AIIS) to identify the iliopsoas muscle, femoral artery (FA), and femoral nerve. The probe was then rotated counterclockwise to align with the pubic ramus to visualize the AIIS, iliopsoas prominence (IPE), FA, iliopsoas, and iliopsoas notch. Under direct vision, a 22-gauge 50 mm echo needle was advanced in the lateral-medial plane between the psoas tendon and the pubic ramus until the needle touched the IPE. The needle was withdrawn, and after negative aspiration, 0,2% ropivacaine was injected in incremental doses. Preparation and surgical positioning allowed for maximal time for block onset.
The basic hemodynamic parameters were monitored during the procedure and the first 24 hours postoperatively. After the surgery, the patients received 15mg/kg-1 iv paracetamol every 6 hours to prevent rebound pain. The pain was measured every 2 hours in a FLACC score. The 15mg/kg-1 metamizole was administered if the FLACC score was 3. In the FLACC score ≥4, the application of 0,2mg/kg-1 Nalpain was ordered. The evidence of block complications, like mobility disorders, bleeding, neuropathy, or systemic toxicity from local anesthetic deposition, was observed. Muscle weakness or mobility of the hip joint was difficult to observe due to the plaster cast.
1st Case Report
A 4-year-old, 14,3kg, the boy with developmental dysplasia due to myelomeningocele, and paralytic dislocation of the left hip joint, with no other co-morbidities (table 1). He was walking independently and did not require urine catheterization. Apart from the primary disease, he was not hospitalized. The boy did not take the medications permanently. He had no drug allergies and no history of convulsions. Due to his primary disease, he was under the care of an orthopedic, rehabilitation, and urological clinic. In June 2020, he underwent surgery for meningomyelocele, and in October 2020, he had an Achilles tenotomy on the left side. The course of the procedures and anesthesia without complications. His neurological development was expected according to age. He has qualified for Dega transiliac osteotomy with femoral subtrochanteric osteotomy combined with Mustard iliopsoas transfer. The ASA physical status classification was 3. An hour before the planned surgery, 7,5mg Midazolam p.o. and 4mg Dexamethasone i.v., were administered. In addition, 200mg of Paracetamol was given intravenously before surgery. General anesthesia was performed with a continuous infusion of propofol and remifentanil in doses, ensuring BIS within 40-60 limits and airway potency was maintained using a laryngeal mask. The lung-sparing mechanical ventilation with Air/O2 mixture was used, under the control of SpO2 >94% and pCO2, within the 35-45 mmHg range (Getinge, FlowC, Maquet Critical Care AB, Sweden). After the induction of general anesthesia, the PENG block was performed with 7,5mL of 0,2% Ropivacaine (Table 1). During the procedure, the hemodynamic parameters (MX550, Philips Medizin Systeme Beoblingen GmbH Hewlett-Packard-Str. 2, Germany) and the remifentanil dosage were monitored. Paracetamol was administered every six hours after surgery.
In the first 24 hours, postoperatively patient’s hemodynamic parameters were stable and within the normal range according to age. After the surgery, the pain was measured every 2 hours in a FLACC score. The 15mg/kg-1 metamizole was administered if the FLACC score was 3. In the FLACC score ≥4, the application of 0,2mg/kg-1 Nalpain was ordered. There was no evidence of block complications, like mobility disorders, bleeding, neuropathy, or systemic toxicity from local anesthetic deposition. Muscle weakness or mobility of the hip joint was difficult to observe due to the plaster cast. However, parents and caregivers did not observe any mobility or sensory disturbances.
2nd Case Report
A 22-month-old, 18kg girl with congenital hip joint dislocation with no other co-morbidities. She was walking independently and was not hospitalized apart from the primary disease. The girl did not take the medications permanently. She had no drug allergies and no history of convulsions. She was under the care of an orthopedic and rehabilitation due to her primary disease. In August 2022, she underwent hip arthrography, closed repositioning of the hip, and placement of a tooth cast. In September 2020, chronic instability of the left hip joint and burns in the places of skin folds in the groin was found in the operating room conditions. The plaster cast was removed, and it was decided that surgery was necessary. After seven days, an open reposition of the hip joint with K-wire stabilization was performed. In October 2020, the K-wire was removed, and in November, the plaster cast was cut through, and a Frejka pillow was adjusted. The course of the procedures and anesthesia without complications. His neurological development was expected according to age. The girl was qualified for transiliac osteotomy with femoral subtrochanteric osteotomy. The ASA physical status classification was 2 (Table 1). An hour before the planned surgery, 7,5mg Midazolam p.o. and 4mg Dexamethasone i.v. were given. In addition, 250mg of Paracetamol was given intravenously before surgery. Sedation was performed with continuous propofol infusion at a dose of 5mg/kg/hour. Spontaneous ventilation was maintained with an oxygen mask 2L/min. Spinal anesthesia (L3/4, PAJUNK, sprotte needle 27G, 70mm) with 1,5 ml of 0,5% heavy spinal Bupivacaine. After the spinal anesthesia, the PENG block was performed with 5mL of 0,2% Ropivacaine (Table 1). Paracetamol was administered every six hours after surgery to prevent rebound pain.
In the first 24 hours, postoperatively patient’s hemodynamic parameters (MX550, Philips Medizin Systeme Beoblingen GmbH Hewlett-Packard-Str. 2, Germany) were stable and within the normal range. After the surgery, the pain was measured every 2 hours in a FLACC score. The 15mg/kg-1 metamizole was administered if the FLACC score was 3. In the FLACC score ≥4, the application of 0,2mg/kg-1 Nalpain was ordered. There was no evidence of block complications, like mobility disorders, bleeding, neuropathy, or systemic toxicity from local anesthetic deposition. Muscle weakness or mobility of the hip joint was difficult to observe due to the plaster cast. However, parents and caregivers did not observe any mobility or sensory disturbances.
Results
The patient’s hemodynamic parameters were stable and within normal range. During the surgery, both patients did not require extra doses of opioids. The time of the procedure was 105 and 75 minutes, the difference was due to the technique of the surgery, and the blood loss was 200ml and 170ml (Table 2).
Postoperatively, the patients appeared comfortable with numeric pain scores of 2/3 of 10. Paracetamol was administered every six hours. Over the night, both patients did not require breakthrough opioids or muscle relaxants. After 12 hours postoperatively, 200mg of metamizole iv was administered to the male patient due to a 3 in FLACC score. Later, FLACC and subjective pain scores were 0-1/10 for the next 24 hours, and the parents did not report poor pain control (Table 2). On the first postoperative day, the patients could participate in physical therapy.
The patients were discharged on the evening of day one with as-needed diazepam for muscle spasms and acetaminophen-opioid preparation for pain control. There was no evidence of block complications, like mobility disorders, bleeding, neuropathy, or systemic toxicity from large-volume local anesthetic deposition [11].
Discussion
Effective management and control of intraoperative and postoperative pain are essential in perioperative hip disease to minimize opioid use and its side effects. In our facility, most pediatric hip surgeries are performed under spinal anesthesia and propofol sedation [12], with preserved spontaneous ventilation. However, the 4-year-old boy had general anesthesia due to the myelomeningocele [13,14]. In addition, spinal and epidural anesthesia is inappropriate for patients with spinal malformations [15].
One of the difficulties in controlling hip pain using adequate topical analgesia is the complex innervation of the joint by multiple nerves. The most common local anesthesia and analgesia techniques for hip surgery are the lumbar plexus block, lumbar epidurals, femoral nerve blocks, sciatic nerve blocks, fascia iliac blocks, and pericapsular injections. However, they may provide only partial analgesia or lower extremity weakness, hypotension, and related side effects, especially in patients with congenital and acquired musculoskeletal system defects [15].
The single-shot PENG block has recently been described in the cadaveric study [16,17] and in the literature for perioperative analgesia in hip surgery by blocking the articular branches of the femoral nerve (FN), accessory obturator nerve (AON), and obturator nerve (ON) [8,18,19,20].
The technical simplicity of imaging in traction-fixed patients and no need for multiple punctures made this blockage ideal for the young pediatric patient [10]. Unfortunately, there are no studies regarding PENG block in patients younger than five years old, like in our case report.
Similar to our study, the pediatric case reports of older children showed the opioid-sparing effect of PENG block in the first 24 hours postoperatively [8,18,19]. In our study, parents and caregivers did not observe muscle weakness, as reported in other studies [9,21,22], which is of particular importance in the case of children with myelomeningocele and other neuromuscular, neurodegenerative or other congenital nerve diseases [23].
A significant drawback of single-shot peripheral nerve blocks is the limited time window of analgesic effect. In addition, the possibility of rebound hyperalgesia after a single-shot nerve block from 12 at 24h has been described [24,25]. In our study, children were given acetaminophen before surgery to avoid rebound pain.
Several additives, such as dexamethasone and alpha-2-adrenergic receptor agonists, have been shown to prolong analgesia following peripheral nerve blocks with single doses and give the potential extent for pain beyond the provision of a single-shot nerve block [26]. Therefore, in our study, we decided to use dexamethasone with the best-proven effectiveness [27,28].
Also, some studies [29,30,31] have reported that few patients experience pain in the lateral femoral cutaneous nerve region after hip surgery. However, we did not observe it in our study.
In 2021, Morrison et al. [32] published a systematic review of studies describing PENG blockade in adults and pediatrics to treat hip pain caused by either fracture or surgery. They found 20 studies that met the inclusion criteria for both the PENG blockade alone and the PENG blockade in combination with other topical analgesic techniques. They concluded that PENG blockade is a promising topical analgesic technique. We achieved similar results in terms of analgesic efficacy and reduced opioid consumption.
Conclusions
Consistent with the literature, our experience demonstrated exercise-preserving and opioid-sparing analgesia using PENG blocks in patients under five. Therefore, we settled on a safe and well-tolerated pediatric range of ropivacaine 0,3-0,5mL 0,2% Ropivacaine [2]. We recognize that the efficacy of PENG blocks has yet to be demonstrated in prospective clinical trials in the pediatric population. Nevertheless, our observations were encouraging, but future studies of PENG efficacy and safety in the pediatric population are warranted.
Supplementary
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Figure 1. Sonoanatomy of PENG. Figure 2. PENG block. Table 1. Characteristics of Patients. Table 2. Surgery and postoperative course.
Author Contributions
Conceptualization M.D. and T.R. Methodology M.D., M.G., A.G.-W., and T.R. Software M.D., M.G. and K.W.-T. Formal Analysis M.D., A.G.-W., T.R. and G.K. Investigation M.D. and T.R. Resources M.D. and K.W.-T. Data Curation M.D. and K.W.-T. Writing- Orginal Draft Preparation M.D. Writing- Review & Editing M.D., K.W.-T., T.R., and G.K. Visualization M.D., M.G., A.G.-W., T.R. and K.W.-T. Supervision G.K. Project Administration G.K.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
Not applicable.
Conflicts of Interest
The author reports no conflicts of interest in this work.
References
- Guay J, Parker MJ, Griffiths R, Kopp SL. Peripheral nerve blocks for hip fractures: a Cochrane review. Anesth Analg. 2018, 126, 1695–704. [Google Scholar] [CrossRef] [PubMed]
- Cettler M, Zielińska M, Rosada-Kurasińska J, Kubica-Cielińska A, Jarosz K, Bartkowska-Śniatkowska A. Guidelines for treatment of acute pain in children–the consensus statement of the Section of Paediatric Anaesthesiology and Intensive Therapy of the Polish Society of Anaesthesiology and Intensive Therapy. Anaesthesiol Intensive Ther. 2022, 54, 197–218. [Google Scholar] [CrossRef] [PubMed]
- Kumar K, Kirksey MA, Duong S, Wu CL. A review of opioid-sparing modalities in perioperative pain management: methods to decrease opioid use postoperatively. Anesth Analg. 2017, 125, 1749–60. [Google Scholar] [CrossRef] [PubMed]
- Kulkarni VA, Kephart DT, Ball MA, Tumber S, Davidson LT, Davids JR. Neuraxial anesthesia for post-operative pain control after hip surgery in children with cerebral palsy and pre-existing intrathecal baclofen pumps. J Pediatr Rehabil Med. 2022, (Preprint):1–11.
- Liu Y, Ke X, Xiang G, Shen S, Mei W. A modification of ultrasound with nerve stimulation-guided lumbar plexus block in supine position for pediatric hip surgery. Pediatr Anesth. 2018, 28, 678–9. [Google Scholar] [CrossRef] [PubMed]
- Suksompong S, von Bormann S, von Bormann B. Regional catheters for postoperative pain control: Review and observational data. Anesthesiol Pain Med. 2020, 10(1).
- Arslantas MK. Problems with epidural catheter. In: Treatments, Mechanisms, and Adverse Reactions of Anesthetics and Analgesics. Elsevier; 2022. p. 273–80. Elsevier;
- Girón-Arango L, Peng PW, Chin KJ, Brull R, Perlas A. Pericapsular nerve group (PENG) block for hip fracture. Reg Anesth Pain Med. 2018, 43, 859–63. [Google Scholar]
- Tran J, Agur A, Peng P. Is pericapsular nerve group (PENG) block a true pericapsular block? Reg Anesth Pain Med. 2019, 44, 257–257.
- Yörükoğlu H, Cesur S, Aksu C, Kuş A. B432 Opioid sparing effect of PENG block in open reduction of pediatric developmental dysplasia of the hip: a case series. 2022. 2022.
- Berlioz BE, Bojaxhi E. PENG Regional Block. 2020. 2020.
- Mallory MD, Travers C, Cravero JP, Kamat PP, Tsze D, Hertzog JH. Pediatric Sedation/Anesthesia for MRI: Results from the Pediatric Sedation Research Consortium. J Magn Reson Imaging. 2022.
- Xu M, He Y, Du B. Pericapsular nerve group block for a child with spina malformation for hip surgery. J Pediatr Surg Case Rep. 2022, 86:102464.
- John A, Katari Y, Murthy V, Sahajananda H. Anesthetic Management of a Rare Case of Type 2 Arnold-Chiari Malformation with Hydrocephalus, Lumbar Myelomeningocele and Thoracolumbar Scoliosis. J Med Sci. 2019, 5, 14–6. [Google Scholar]
- Hopkins PM. Musculoskeletal disorders and anaesthesia. In: Hopkins PM, Hardman JG, Hopkins PM, Struys MMRF, editors. Oxford Textbook of Anaesthesia [Internet]. Oxford University Press; 2017 [cited 2023 Jan 27]. p. 0. [CrossRef]
- Short AJ, Barnett JJG, Gofeld M, Baig E, Lam K, Agur AM, et al. Anatomic study of innervation of the anterior hip capsule: implication for image-guided intervention. Reg Anesth Pain Med. 2018, 43, 186–92. [Google Scholar]
- Çiftçi B, Ahıskalıoğlu A, Altıntaş HM, Tekin B, Şakul BU, Alıcı HA. A possible mechanism of motor blockade of high volume pericapsular nerve group (PENG) block: A cadaveric study. J Clin Anesth. 2021.
- Orozco S, Muñoz D, Jaramillo S, Herrera AM. Pediatric use of Pericapsular nerve group (PENG) block for hip surgical procedures. J Clin Anesth. 2019, 57:143–4.
- Aksu C, Cesur S, Kuş A. Pericapsular nerve group (PENG) block for postoperative analgesia after open reduction of pediatric congenital dysplasia of the hip. J Clin Anesth. 2019, 61:109675–109675.
- Ueshima H, Otake H. RETRACTED: Pericapsular nerve group (PENG) block is effective for dislocation of the hip joint. J Clin Anesth. 2018, 52:83–83.
- Mistry T, Sonawane KB, Kuppusamy E. PENG block: points to ponder. Reg Anesth Pain Med. 2019, 44, 423–4. [Google Scholar]
- Wyatt K, Zidane M, Liu C jy J. Utilization of a continuous pericapsular nerve group (PENG) block with an opioid-sparing repair of a femoral neck fracture in a pediatric patient. Case Rep Orthop. 2020, 2020.
- Cung S, Ritz ML, Masaracchia MM. Regional anesthesia in pediatric patients with preexisting neurological disease. Pediatr Anesth. 2021, 31, 522–30. [Google Scholar] [CrossRef] [PubMed]
- Nobre LV, Cunha GP, Sousa PCCB de, Takeda A, Ferraro LHC. Peripheral nerve block and rebound pain: literature review. Rev Bras Anestesiol. 2020, 69:587–93.
- Dada O, Gonzalez Zacarias A, Ongaigui C, Echeverria-Villalobos M, Kushelev M, Bergese SD, et al. Does rebound pain after peripheral nerve block for orthopedic surgery impact postoperative analgesia and opioid consumption? A narrative review. Int J Environ Res Public Health. 2019, 16, 3257. [Google Scholar] [CrossRef] [PubMed]
- Muñoz-Leyva F, Cubillos J, Chin KJ. Managing rebound pain after regional anesthesia. Korean J Anesthesiol. 2020, 73, 372–83. [Google Scholar] [CrossRef] [PubMed]
- Yang J, Cui Y, Cao R, Huang QH, Zhang QQ. Dexmedetomidine as an adjunct to peripheral nerve blocks in pediatric patients. World J Pediatr. 2022, 1–12. [Google Scholar]
- Zhu C, Zhang S, Gu Z, Tong Y, Wei R. Caudal and intravenous dexamethasone as an adjuvant to pediatric caudal block: A systematic review and meta-analysis. Pediatr Anesth. 2018, 28, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Girón-Arango L, Roqués V, Peng P. Reply To Dr Roy et al: Total postoperative analgesia for hip surgeries: PENG block with LFCN block. Reg Anesth Pain Med. 2019.
- Thallaj, A. Combined PENG and LFCN blocks for postoperative analgesia in hip surgery-A case report. Saudi J Anaesth. 2019, 13, 381. [Google Scholar] [CrossRef] [PubMed]
- Talawar P, Tandon S, Tripathy D, Kaushal A. Combined pericapsular nerve group and lateral femoral cutaneous nerve blocks for surgical anaesthesia in hip arthroscopy. Indian J Anaesth. 2020, 64, 638. [Google Scholar] [CrossRef] [PubMed]
- Morrison C, Brown B, Lin DY, Jaarsma R, Kroon H. Analgesia and anesthesia using the pericapsular nerve group block in hip surgery and hip fracture: a scoping review. Reg Anesth Pain Med. 2021, 46, 169–75. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Sonoanatomy of PENG.

Figure 2.
Injection technique of PENG block.
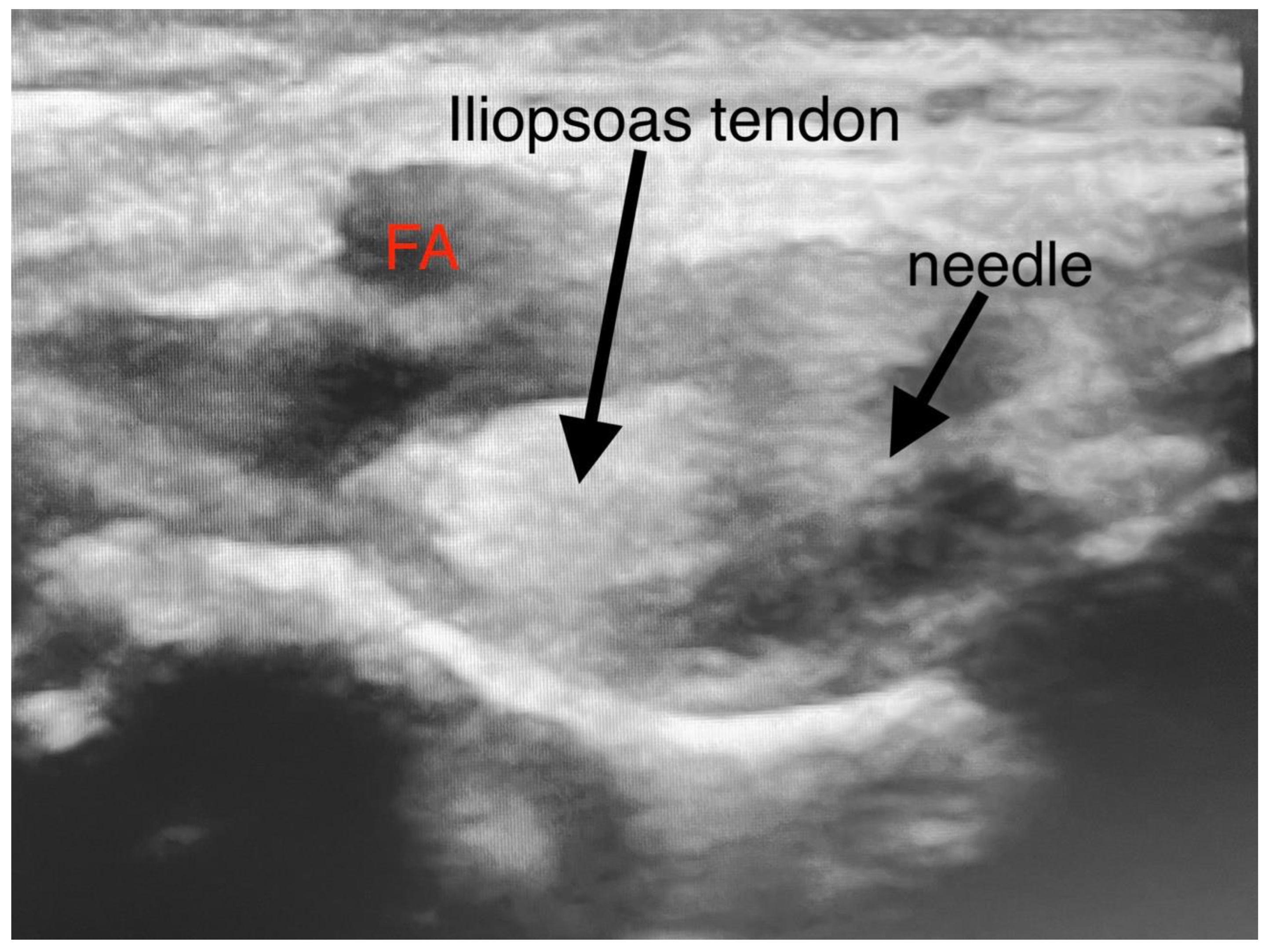

Table 1.
Characteristics of Patients.
| 1st | 2nd | |
| Sex | M | F |
| Age | 4 years | 22 months |
| Weight | 14,3 kg | 18kg |
| ASA | 3 | 2 |
| Comorbidities | myelomeningocele | obesity |
| Hip pathology | paralytic dislocation of the left hip joint | congenital dislocation of the left hip joint |
| Type of Surgery | Dega transiliac osteotomy with femoral subtrochanteric osteotomy combined with iliopsoas transfer, according to Mustard | Traniliac osteotomy with femoral subtrochanteric osteotomy |
| Type of Anesthesia | General anesthesia Propofol 0,2mg/kg/min Remifentanil 0,1ug/kg/min |
Spinal anesthesia 1,5mL heavy, spinal Bupivacaine Propofol 0,06mg/kg/min |
| Type and Volume of Local Anesthetic used for PENG block | 7,5mL of 0,2% ropivacaine | 5mL of 0,2% Ropivacaine |
Table 2.
Surgery and postoperative course.
| 1st | 2nd | |
| Total operating time | 105 minutes | 75 minutes |
| Complications | no | no |
| Estimated blood loss | 200ml | 170ml |
| Highest FLACC score | 3 | 2 |
| Pain medications | 200mg Paracetamol every 6 hours | 250mg Paracetamol every 6 hours |
| Interventional pain drugs | 200mg Metamizole iv. | no |
| Breakthrough opioids or muscle relaxants | no | no |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



