
Submitted:
30 January 2023
Posted:
02 February 2023
You are already at the latest version
Abstract
(1)Background: Among new anti-angiogenetic agents being developed and everchanging guidelines indications, the question of benefits/safety ratio remains unclear. (2)Methods: we have conducted a systematic review and meta-analysis of 25 randomized controlled trials (15487 patients), evaluating overall survival – OS, progression free survival– PFS and toxicity (grade ≥3 adverse effects, type and number of all adverse effects. (3)Results: analysis showed improvement of pooled-PFS (HR 0.72, 95%CI 0.66–0.78, I2 = 77%, P<0.00001) regardless of treatment settings (first-line - HR 0.83, 95%CI 0.77-0.90, P<0.00001, recurrent cancer – HR 0.61, 95%CI 0.54-0.68, P<0.00001 or maintenance – HR 0.82, 95%CI 0.67-1.00, P=0.04) and type of anti-angiogenetic drug used (VEGF inhibitors, VEGF-R inhibitors or angiopoietin inhibitors). Improved OS was also observed (HR 0.95, 95%CI 0.91–0.99, P=0.02). OS benefits were only observed in recurrent platinum-sensitive or platinum-resistant cancers. Grade≥3 adverse effects were increased across all trials. Anti-angiogenetic therapy increased the risk of hypertension, infection, thromboembolic/ hemorrhagic events, gastro-intestinal perforations but not the risk of wound related issues, anemia or posterior leukoencephalopathy syndrome. (4)Conclusions: Although angiogenesis inhibitors improve PFS, there is little to no OS benefits. Given the high risk of severe adverse reactions a careful selection of patients is required for obtaining the best results possible.
Keywords:
angiogenesis inhibitors
; VEGF inhibitors
; ovarian cancer
; progression-free survival
; overall sur-vival
; toxicity
; systematic review
; meta-analysis
; randomized controlled trials
; FDA approval of cancer drugs
1. Introduction
Significant improvements have been made in the management of ovarian cancer, but this disease continues to have a huge burden on health care especially in countries with a low human development index. According to GLOBOCAN 2020 statistics, ovarian cancer remains the 3rd in incidence and the 2nd cause of death among the genital neoplasms. In central and eastern Europe, ovarian cancer has the highest incidence rate in the World (10,7/100.000) and a mortality rate of 5,6/100.000[1]. In present, the guidelines promote a combination of cytoreductive surgery and combination chemotherapy of platinum agents and taxanes. Although most patients will experience remission under therapy, 80% will relapse within 18 months[2]. The relapse is usually diagnosed in advanced stages, despite the initial response to platinum-based chemotherapy, and is showing increased chemo-resistance, leading in most cases to death[3,4]. Thus, new agents like angiogenesis inhibitors and PARP inhibitors were introduced as treatment options. Regardless of initial factors that leads to the neoplastic transformation of cells, due to the increased metabolic need and secondary tissular hypoxia, cancers require neo-angiogenesis for their progressive growth and metastasis, cancer cells being able stimulate nearby normal cells to produce angiogenesis signaling molecules[5,6,7]. The angiogenesis in solid tumors is a well-known fact and targeting the pathways that regulate angiogenesis was suggested as potential therapeutic approach[8,9]. After the initial paper by Folkman in 1971[8] that shifted the therapeutic paradigm from targeting the tumor cell to an anti-angiogenetic approach, a new field of study in oncology emerged. Over the years numerous discoveries have been made regarding the identification of angiogenetic factors, the regulation of the tumoral angiogenesis process and the development of new drugs that could interfere with pathological tumor-related vessel formation. After the establishment of VEGF as the key mediator in pathological angiogenesis[10] targeting the VEGF/VEGF-R signaling axis has become the pivot of research in the development of antiangiogenetic agents. Clinical trials (number ranging in the thousand) demonstrated the benefits of the anti-angiogenesis drugs. Numerous molecules have been developed and have received regulatory approval for cancer therapy[11,12,13,14] and secondary for the treatment of ocular neovascular diseases which share molecular pathways with cancer neo-angiogenesis[13,15,16,17,18,19,20]. These therapies are credited with improved progression-free survival (PFS) and over-all survival (OS), but those results are inconstant. Due to the high costs, but also the frequency and severity of therapy-specific adverse effects, in low-income countries there is a tendency for careful consideration of efficacy-safety ratio. In Romania, these therapies are fully refunded through national health care programs, and as a result, in the Oncology Institute of Bucharest, around 50 patients with ovarian cancers are treated each year with anti-angiogenesis drugs. Although we observed improved survival, some patients experience severe adverse reactions and extreme alterations of QoL leading us to the conclusion that more in depth analysis of security profiles are warranted. In Romania, we see no reduction of incidence for ovarian cancer[21], thus the therapeutic options for these cases continues to be of concern.
The aim of this study is to provide a comprehensive review of efficacy-safety ratio of angiogenesis-inhibitors based therapies in ovarian cancer, thus providing a better evaluation and selection tool for clinicians.
2. Materials and Methods
2.1. Search Strategy
A systematic literature search, according to PRISMA guidelines[22], was performed in multiple international databases - PubMed, Web of Science, Embase, Cochrane Library and ASCO and ESMO abstract database, from establishment up to May 1st, 2022. The following combinations of search terms was used: (1) (ovar or ovarian or ovary) and (neoplasm or cancer or carcinoma or malignant or tumor or tumor); (2) vascular endothelial growth factor, angiogenesis inhibitor, VEGF, VEGFR, VEGF-R, anti-VEGF, VEGF-target, anti-angiogenic, anti-angiogenesis, antiangiogenetic; (3) bevacizumab, avastin, cediranib, AZD2171, recentin, aflibercept, VEGF trap, AVE0005, zaltrap, sorafenib, nexavar, pazopanib, Votrient, trebananib, AMG386, nintedanib, BIBF 1120, tyrosine kinases inhibitors, TIE, AXL, FLT, sunitinib, SU11248.
2.2. Study Selection
References were prepared by using Mendeley Reference Manager [23] After removing duplicate records an extensive title and abstract screening process was performed and records with irrelevant focus were removed.
Inclusion criteria were adult patients with confirmed ovarian cancer regardless of histology, regardless of treatment settings (first-line, recurrence or maintenance), receiving anti-angiogenetic drugs. The experimental arm needed to be compared to standard chemotherapy or placebo, with PFS and/or OS being reported by hazard ratio with 95%CI. PFS, OS and adverse effects were our outcomes of interest, but we did not limit the inclusion if a study didn’t report all three. The study design of trials included were Phase II/III randomized controlled. Non-randomized controlled studies or Phase I trials were also excluded due to the fact that were not considered high-quality statistical data. Book chapters, reviews and case-reports were also excluded for the same reason. Studies using cyclophosphamide as control arm were excluded due to the fact that the superiority of carboplatin/paclitaxel over cyclophosphamide regimens was long-time established by prior trials[24].
Population, Intervention, Comparator, Outcomes and Study designs (PICOS) structure shown in Table 1 was used for considering studies for the review[25].
The remaining articles were obtained as full text and were independently reviewed by two investigators, and discrepancies were discussed between all authors. The literature search flow chart is presented in Figure 1.
2.3. Data Extraction
From each trial selected the following data was retained: name of first author, year of clinical trial, study phase, patient selection criteria, drug regimens on experimental and controlled arms of study, sample size, different bias factors, and outcomes intended for use in meta-analysis (progression-free survival, overall survival and adverse events – type, total number of events, number and type of grade 3 or higher adverse events).
2.4. Risk of Bias Assessment
Risk of bias was assessed on six domains used by the Cochrane Collaboration’s tool[26]: selection bias (random sequence generation and allocation concealment), performance bias, detection bias, attrition bias, reporting bias, and other sources of bias. Details of bias risk is presented in Figure 2a,b. Risk was categorized as low, high or unclear.
2.5. Statistical Analysis
Pooled hazard-ratios (HRs) for overall survival (OS) and progression-free survival (PFS) were calculated in RevMan 5.4.1 software[27]. Risk ratios (RR) for adverse events were also calculated with 95% CI. I2 statistic was used in order to see the statistical heterogeneity of the studies. When a high heterogeneity between studies was observed we used a random model for statistical analysis. For I2<40% we used a fixed model.
3. Results
3.1. Literature Search
After the literature review, we identified n=9754 records concerning the utilization of antiangiogenetic therapies for ovarian cancer. Another 54 additional records were found after reference review. Duplicate records (n=2183) were removed and after title and abstract screening 7514 records were excluded: irrelevant focus (n=5127), non-randomized controlled/ Phase I studies (n=443), reviews or case reports (n=1908), other reasons (n=39). The remaining 119 records were obtained as full text articles and assessed. Another 95 studies were excluded due to lacking of outcomes of interest or being previous versions or exploratory outcomes of studies already included. In the end 25 randomized controlled trials (RCTs) were included.
3.2. Studies Characteristics
A total of 15487 patients met the inclusion criteria (adults with confirmed ovarian cancer, with therapies including anti-angiogenetic agents and compared to other drug regimens without such agents or placebo). The 25 RCTs have a publication date between 2011 and 2021, and they evaluated 7 inhibitors of angiogenesis (bevacizumab – 7, pazopanib – 5, trebananib – 4, nintedanib – 3, sorafenib – 2, cediranib – 2, aflibercept – 1). In the 2019 Tewari study there were 2 experimental arms which were both included in our study, the difference being in the maintenance therapy (1 arm using bevacizumab - BEVm, 1 arm using placebo - PLm). A similar situation was encountered in the Ledermann 2016 study, but we did not use separately the experimental arms due to the lack of hazard ratios for PFS and OS between the control and PLm arms of the study. The general characteristics, the references and the summary of outcomes from the included trial are listed in Table 2 and Table 3.
3.3. Progression-free Survival and Overall Survival
In our study the anti-angiogenetic regimens were credited with a significant improvement of PFS when compared to control arm (HR 0.72, 95% CI 0.66–0.78, I2 = 77%, P < 0.00001). The Z-test for overall effect was significant (Z=7,29; P < 0.00001). Improved OS was also observed, but the results had a lower P value (HR 0.95, 95% CI 0.91–0.99, I2 = 0, P=0.02). Improvement of progression was observed in all patients, regardless of treatment settings: first-line (HR 0.83, 95% CI 0.77-0.90, P<0.00001), recurrent cancer (HR 0.61, 95% CI 0.54-0.68, P<0.00001) or maintenance (HR 0.82, 95% CI 0.67-1.00, P=0.04). For the recurrent cancers, the PFS improvement affected both platinum-sensitive and platinum-resistant tumors (HR 0.58, 95% CI 0.49-0.69, P<0,00001, respectively HR 0.56, 95% CI 0.42-0.75, P<0,00001) - Figure 3. When analyzing the OS in different treatment setting, the results were more heterogenic – significant improvements were observed in recurrent cancers (both in P-S R and P-R R – HR 0.88, 95% CI 0.79-0.99, P=0,03, respectively HR 0.78, 95% CI 0.65-0.94, P=0.01). However, when employed as first-line or maintenance therapy, no improvement was observed – Figure 4.
Different action mechanisms of the antiangiogenetic drugs may have different effects. We tried to establish that by evaluating PFS and OS for 3 distinct action mechanisms – VEGF inhibitors (bevacizumab, aflibercept), VEGF-R inhibitors (pazopanib, cediranib, nintedanib, sorafenib) and angiopoietin inhibitors (trebananib). All three groups experienced improvements on PFS: VEGF inhibitors – HR 0.66, 95% CI 0.56–0.79, P < 0.00001; VEGF-R inhibitors HR 0.74, 95% CI 0.66–0.83, P < 0.0001; angiopoietin inhibitors HR 0.82, 95% CI 0.69–0.99, P = 0.04 – Figure 5. No significant differences in OS between subgroups and control groups were observed however – Figure 6.
In order to evaluate the impact of heterogeneity in PFS/OS results we performed a sensitivity analysis, by visual inspection of comparison-adjusted funnel plot of 25 included RCTs. We found no evidence of asymmetry in the funnel plot, indicating absence of publication bias.
3.4. Adverse Events
We analyzed the adverse effects reported for the included studies. For the Karlan and Tewari studies which included two experimental arms, the safety analyses were done by comparing the two experimental arms together with the control arm. Our analysis included 31 adverse events that are considered to be associated with anti-angiogenetic therapy for which RR were calculated (Supplementary Materials – Figures S1-S31). Hypertension was found to have a higher risk for the patients on angiogenesis inhibitors (RR 3.64, 95% CI 1.76-7.50, P=0,0005, I2=99%). Similar results were found for hemorrhagic events (RR 1.94, 95% CI 1.00-3.76, P=0.05, I2=77%) and for thromboembolic events (RR 1.47, 95% CI 1.12-1.92, P=0.006, I2=2%). However, only arterial thromboembolism was statistically linked to the anti-angiogenetic therapy (RR 2.13, 95% CI 1.41-3.23, P=0.0004, I2=17%). Same is not true for venous thromboembolism (RR 1.14, 95% CI 0.82-1.57, P=0.44, I2=43%). Significant increased risk was also seen for proteinuria (RR 4.52, 95% CI 2.12-9.62, P<0.00001, I2=87%), gastro-intestinal perforations (RR 2.86, 95% CI 1.36-6.04, P=0.006, I2=0%), infections (RR 1.28, 95% CI 1.07-1.53, P=0.008, I2=0%), ascites (RR 2.06, 95% CI 1.65-2.57, P<0.00001, I2=35%), neutropenia (RR 1.27, 95% CI 1.09-1.48, P=0.002, I2=92%), leucopenia (RR 1.21, 95% CI 1.05-1.39, P=0.009, I2=59%), thrombocytopenia (RR 1.98, 95% CI 1.56-2.52, P<0.00001, I2=86%), nausea (RR 1.27, 95% CI 1.12-1.45, P=0.0002, I2=79%), vomiting (RR 1.28, 95% CI 1.10-1.51, P=0.002, I2=57%), diarrhea (RR 2.05, 95% CI 1.60-2.62, P<0.00001, I2=91%), fatigue (RR 1.14, 95% CI 1.02-1.28, P=0.03, I2=83%), dyspnea (RR 1.20, 95% CI 1.05-1.37, P=0.008, I=0%), hypomagnesemia (RR 1.63, 95% CI 1.15-2.32, P=0.006, I2=46%), hypokalemia (RR 1.87, 95% CI 1.53-2.28, P<0.00001, I2=0%), headache (RR 1.63, 95% CI 1.36-1.95, P<0.00001, I2=58%), abdominal pain (RR 1.12, 95% CI 1.04-1.22, P=0.005, I2=11%). No significant correlations were seen between the following symptoms and the anti-angiogenetic therapy: reversible posterior leukoencephalopathy syndrome (RR 1.57, 95% CI 0.31-7.81, P=0.58, I2=0%), pyrexia (RR 0.88, 95% CI 0.73-1.08, P=0.22, I2=4%), wound related issues (RR 1.36, 95% CI 0.92-2.01, P=0.12, I2=12%), anemia (RR 0.94, 95% CI 0.82-1.07, P=0.33, I2=76%), anorexia (RR 1.54, 95% CI 0.96-2.49, P=0.07, I2=85%), constipation (RR 0.99, 95% CI 0.87-1.14, P=0.93, I2=45%), alopecia (RR 0.98, 95% CI 0.92-1.03, P=0.43, I2=11%), rash (RR 1.16, 95% CI 0.89-1.52, P=0.27, I=78%), back pain (RR 0.89, 95% CI 0.66-1.20, P=0.45, I2=60%), pain (RR 1.02, 95% CI 0.85-1.22, P=0.85, I2=66%). Grade 3 or higher adverse effects risk was increased in the therapeutic arms of our study (RR 1.43, 95% CI 1.20-1.72, P<0.00001) – Figure 7.
4. Discussion
4.1. Interpretation of Results
Our study demonstrated that anti-angiogenetic drugs can significantly improve PFS in ovarian cancer patients and increase the risk of common adverse events of all grades. The benefits regarding OS are more uncertain, being observed only in specific types of patients and tumors. We observed contradictory results for OS – pooled OS for all trials showed a significant improvement of survival favoring the angiogenesis inhibitors, but could not find a significant improvement when studying different treatment setting or types of anti-angiogenetic drugs separately. None of the therapeutic categories (VEGF blockade, VEGF-R inhibitors and angiopoietin inhibitors) were associated with improved OS. As first line therapy, we could prove no significant correlation with improved OS, possible reasons for this being: (1) most cases of ovarian cancer that benefit from first line chemotherapy are advanced (among the 6 trials included studying first-line therapy only one enrolled stage I-II cases[28]); (2) Three of the 25 RCTs [29,30,31] allowed patients in the control arm to receive anti-angiogenetic salvage therapy after disease progression tush diminishing the OS differential between experimental and control arms; (3) High-risk ovarian cancer is more likely to have a maximal response when treated with anti-angiogenesis agents as first-line.
The ICON7 trial[28]considered high-risk cancers as stage IV FIGO, inoperable cancer, or sub-optimally resected (> 1cm residual disease) stage III FIGO. The TRINOVA 3[53] GOG-0218[51], and the AGO-OVAR 12[49] shared the same definition for high-risk tumors. However, the OS between these trials were unconcording: ICON7 showed that bevacizumab in high-risk tumors is associated with improved OS (HR0.78, 95%CI 0.63–0.97, P=0.01)[28]. On the contrary, AGO-OVAR 12 showed that improved OS is obtain in standard chemotherapy rather than in nintedanib treated group (HR 1.14, 95%CI 0.89–1.45)[49]. GOG-0218 trial showed that advanced high-risk disease favored the concurrent use of bevacizumab with chemotherapy followed by bevacizumab maintenance arm (HR 0.72, 95% CI 0.53–0.97)[51]. The 2022 network meta-analysis by Helali et al. supported the use of bevacizumab, concurrently with chemotherapy, followed by bevacizumab maintenance until progression for chemo-naïve disease was associated with the highest probability of OS and PFS [54]. More over the same network meta-analysis ranked the effects of different anti-angiogenetic agents in high-risk chemo-naïve disease (Bevacizumab concurrent + maintenance > Nintedanib concurrent + maintenance > Tebananib concurrent + maintenance > Standard of care chemotherapy Carboplatin/ Paclitaxel). All mentioned trials showed no OS benefit favoring the usage of anti-angiogenetic agents in non-high-risk chemo-naïve disease. OS in the non-high-risk chemotherapy-naïve cancers can vary, thus making it difficult to propose any clinical recommendations for the usage of angiogenesis inhibitors in this disease setting, but most studies infer a probable lack of efficacy of angiogenesis inhibitors when used in the chemo-naive non-high-risk ovarian carcinoma[54].
In recurrent treatment settings, our study proved the benefits of anti-angiogenesis agents for both platinum-sensitive and platinum-resistant disease. For these categories both PFS and OS were improved, so angiogenesis inhibitors can be a treatment option for these patients. Helali et al.[54] ranked the angiogenesis inhibitors by probability of benefit in recurrent epithelial ovarian cancer. For platinum-resistant group they found that the concurrent chemotherapy and pazopanib has the best chance of improving OS, followed by combination chemotherapy with sorafenib. For platinum-sensitive group they found that the addition of anti-angiogenetic drugs to standard chemotherapy does not improve OS, but the association of bevacizumab or cediranib to chemotherapy in maintenance stage can improve PFS. Helali et al. also suggested that PARP inhibitors in addition to chemotherapy are the best option for platinum-sensitive recurrent disease[54]. Other studies suggested that PARP inhibitors in combination with antiangiogenetic agents may be a better therapeutic option than monotherapy with antiangiogenetic agents in platinum-sensitive cancers [55]
When analyzing the OS benefit of antiangiogenetic drugs used as maintenance therapy, we found no improvements.
The OS benefits are difficult to evaluate due to the fact that most trials included did not reported OS based on PFI (platinum free interval) and also the low sample size in some studies (MITO 11[47], TRIAS[33]) may influence results.
The results of our study suggest that PFS is not a viable surrogate evaluation of response for OS. The FDA approval process of various cancer drugs for solid tumors use surrogate endpoints (PFS) rather than clinical outcomes (OS). The definition of FDA for clinical outcomes is a direct measure of benefit of an intervention in a trial. A predictive substitute for clinical outcomes is called a surrogate endpoint. PFS is the most commonly used surrogate endpoint for OS for solid cancer[56,57], and its use is growing every day. The FDA has approved many cancer drugs based on surrogate endpoint data. Among those receiving regulatory approval, 57% of cancer drugs did not demonstrate an OS benefit[58]. Given the results of our study we consider that the usage of a surrogate endpoint for clinical outcomes (PFS) in the process of drug approval may need to be reconsidered, as PFS proved not to be a reliable substitute for OS. The suboptimal predictive value of PFS as a surrogate for OS was highlighted by several different articles and studies [54,59,60,61].
The absence of predictive biomarkers for anti-angiogenic agent therapy response makes it difficult to do a proper selection of patient categories that benefit most from anti-angiogenetic drugs. A series of markers have been suggested as response predictors: high Ang1/low Tie2 serum values was associated with improved PFS in experimental bevacizumab arm of ICON 7 patients[62]. The ICON 7 trial also validated the gene signature proposed by Gourley et al. in order to identify the angiogenic molecular subtypes of ovarian tumors[63]. In the serum samples from ICON 7 trial, Collinson et al.[64] identified several biomarkers predictive for response: fms-like tyrosine kinase-4 (FLT4), mesothelin, and α1-acid glycoprotein (AGP). This resulted in identifying a subgroup of patients likely to benefit from antiangiogenetic therapy, patients with a positive signature profile had a median PFS improved by 5,5 months (p=0.001). The GOG-218 trial was the source of a number of articles identifying several potential predictors for response to anti-angiogenetic therapy: plasmatic concentrations of VEGF and VEGF-R2 [65], tumor VEGF-A expression[66], micro-vessel density (MVD)[67], IL-6 levels[68]. Although the identification of these predictive biomarkers is encouraging, they need to be validated by more extensive trials in order to be incorporated into guideline recommendation for practicians. Oxidative stress related genes and factors have also been suggested to play an important role in ovarian cancer as a predictive factor for response to angiogenesis inhibitors therapy in ovarian cancer[69,70,71]. It is known that the OS affects chemoresistance through specific point mutations of key redox enzymes[72]. Oxidative stress factors have been identified in circulation among ovarian cancer patients[73]. However, the role of oxidative stress related prediction of response to therapy factors still needs to be investigated by trials.
Since for advanced ovarian cancer the treatment is mostly palliative in nature, and in the context of the myriad of potentially severe adverse effects and dubitable OS benefits, the question of quality of life (QoL) in patients treated with anti-angiogenetic agents should be an important indicator of therapeutic success. In present there are very few studies focusing on QoL in patients treated with angiogenesis inhibitors [74,75]. This aspect needs to be evaluated further by clinical trials. Our study demonstrated that some adverse effects that can significantly affect the QoL are more frequent when angiogenesis inhibitors are used. The anti-angiogenetic agents are associated with higher incidence of gastro-intestinal perforations, infections, thromboembolic and hemorrhagic events.
When debating the efficacity-toxicity ratio of angiogenesis inhibitors, one more concern is the cross results when employed in conjunction with other another class of targeted therapies like poly-(ADP-ribose) polymerase (PARP) inhibitors, especially since an ever-increasing number of trials have been published testing this therapeutic combination. This combination of drugs has a reported synergic effect, since angiogenesis inhibitors lead to hypoxia, which has been shown to induce homologous recombination repair deficiency (HRD) through the downregulation of homologous recombination repair genes. This effect result in an increased sensitivity of tumor cells to PARP inhibitors[76,77,78]. Liu et al.[43] showed a significant improvement of PFS when treating the recurrent platinum-sensitive ovarian cancer with cediranib combined with olaparib, when compared to olaparib monotherapy. The combination also increases the OS in patients without germline BRCA1/2 mutation. There is also data that suggested an improvement of PFS after the addition of olaparib in the maintenance phase in patients with advanced ovarian cancer which have received standard first-line therapy including bevacizumab – Phase II study conducted by Ray-Coquard in 2019[55]. This combination of angiogenesis inhibitors with PARP inhibitors can represent a new direction for future research. Another small Phase I study (Lorusso et al. from 2020) focused on the association between bevacizumab and a different PARP inhibitor (rucaparib) and found no safety concerns about the combination[79]. The randomized Phase II study MITO 25 will investigate further maintenance rucaparib with/without bevacizumab in patients with newly diagnosed stage III-IV ovarian cancer[80]. Mirza et al.[81] published a Phase I study on the combination of niraparib and bevacizumab in platinum-sensitive epithelial ovarian cancer which showed no safety concerns.
Anti-angiogenetic therapies, although constantly improving PFS, show suboptimal clinical effect[82,83]. This may be explained by the triggering of selective survival of hypoxic cells in the center of tumoral mass[7]. Moreover, the disruption of a given angiogenic pathway may provoke compensatory reactions through compensatory secretion of alternative angiogenic factors[84,85,86,87,88,89,90], leading to resistance to single-target therapeutic approaches. We, therefore see an unmet need for novel strategies in order to compensate for the shortcomings of current therapeutic modalities by employing concurrent therapies that target multiple angiogenetic pathways.
4.2. Comparison with Other Studies
In our study consists of 25 RCTs thus being the largest and more recent meta-analysis and systematic review done on the subject of anti-angiogenetic drugs and their usage in ovarian cancer, including 15487 patients. Over time a number of systematic review and meta-analysis demonstrating the outcome variabilities were performed on angiogenesis inhibitor randomized controlled trials[54,91,92,93,94,95,96,97,98,99,100,101]. One of the latest (Guo)[92] included 22 RCTs published between 2011 and 2019, with 11254 patients meeting the inclusion criteria. Our study included 3 other studies (Burger, du Bois 2014, du Bois 2016). Helali et al.[54] although included 23 RCTs focused on epithelial ovarian cancer omitting studies like Liu and Lederman 2016[42,43] included in our study, in which the sample included serous or endometrioid histology. They included the Matulonis 2019 (KEYNOTE 100) study[102] on the effects of pembrolizumab (a PD-1 inhibitor) in ovarian cancer, which we consider outside of the scope of this paper. The Hall et al. 2020[103] study was not included due to the fact that cyclophosphamide was used as treatment line rather than carboplatin/paclitaxel - the superiority of carboplatin/paclitaxel of over cisplatin/cyclophosphamide has been demonstrated by previous trial[24] and the usage of cyclophosphamide may falsely alter the PFS results in favor of anti-angiogenetic drugs.
Angiogenesis inhibitors are associated with an increased PFS over all patient groups and all categories of drugs used, results similar to previous studies. In our study the OS was only improved by the studied therapy for recurrent ovarian cancer, not influencing cases in first line or maintenance settings. The improved OS observed in other studies when using VEGF inhibitors or angiopoietin inhibitors was not observed in our study.
Most of previous meta-analysis regarding angiogenesis inhibitors in ovarian cancer patients, focused on survival parameters, toxicity being ignored. For a better understanding of the efficacy-safety ratio of angiogenesis inhibitors, we also analyzed the therapy-specific adverse effects. By calculating the RR for 31 therapy-specific we observed increased risk for hypertension, hemorrhagic and thromboembolic events, proteinuria, gastro-intestinal perforations, infections, ascites, neutropenia, leucopenia, thrombocytopenia, nausea, vomiting, diarrhea, fatigue, dyspnea, hypomagnesemia, hypokalemia, headache, abdominal pain. For all grade ≥ 3 adverse events, the risk was higher in angiogenesis inhibitors groups. There were no significant increased risks found in the following adverse events: venous thromboembolism, anemia, pyrexia, anorexia, rash, pain, back pain. Two of the adverse effects specific to the angiogenesis inhibitors (wound related issues and reversible posterior leukoencephalopathy syndrome were found not to be significantly associated with the therapy in our study.
4.3. Strengths and Limitations
The strengths of this study are the broad inclusion of 15487 patients treated with seven different angiogenesis inhibitors which allowed us to perform a comprehensive analysis of survival parameters (PFS, OS) and therapy-specific toxicity. To the best of our knowledge this is the largest meta-analysis on the usage of anti-angiogenetic drugs in ovarian cancer to this date. The RCTs included enrolled all stages of ovarian cancer and different treatment settings, thus allowing us to evaluate the role of the anti-angiogenetic therapy as first-line, as maintenance or as secondary therapy for recurrent disease. Furthermore, the subgroup analyses of different mechanism anti-angiogenetic drugs, may allow to make prediction on the type of anti-angiogenetic therapy more likely to obtain the maximum benefit. As a side effect of the broad inclusion criteria regardless of tumor type, stage of disease, drug regimens, number of previous lines of therapy, response to previous therapy, duration of follow-up and so on, the heterogeneity was increased, giving raise to the possibility of different results when focusing on more narrow patient types or more specific drug regimens (our study included VEGF- blockade, VEGF-R inhibitors and angiopoietin inhibitors). The high heterogeneity across studies is the most important limitation of our analysis. Another limitation of our study is the fact that our meta-analysis is based on published data, rather than on actual patient data. Also, some of the studies included had an increased risk of bias due to issues with randomization or blinding.
5. Conclusions
Our study showed that anti-angiogenetic agents can improve the PFS in ovarian cancer regardless of treatment setting or type of drug used (VEGF inhibitors, VEGF-R inhibitors or angiopoietin inhibitors), thus being an option in treatment of ovarian cancer. Second, due to the fact that OS improvements are only seen in high-risk chemo-naive cancers and in recurrent disease, we believe that the usage of angiogenesis inhibitors needs to be administrated with prudence outside of these setting and after careful consideration of each case prognostic and response factors. Thirdly, we consider that further studies are required in order to better understand which categories benefit the most from angiogenesis inhibitors, and which are only subjected to the risk of adverse effects and diminished QoL. The need for identifying and validating biomarkers accurately predicting the response to therapy is a good future direction for study. Fourthly, for the platinum-sensitive recurrent disease the role of concurrent therapy with angiogenetic and PARP inhibitors needs to be explored further. And last: we consider that the usage of a surrogate endpoint for clinical outcomes (PFS) in the process of drug approval may need to be reconsidered as PFS proved not to be a viable substitute for OS.
Supplementary Materials
The following supporting information on the statistical analysis of therapy-specific adverse effects can be downloaded at www.mdpi.com/link: Figure S1: Hypertension; Figure S2: Hemorrhagic events; Figure S3: Thrombosis and embolism; Figure S4: Arterial thromboembolism; Figure S5: Venous thromboembolism; Figure S6: Proteinuria; Figure S7: Reversible posterior leukoencephalopathy syndrome; Figure S8: Gastrointestinal perforation; Figure S9: Infection; Figure S10: Pyrexia; Figure S11: Wound related issues; Figure S12: Ascites; Figure S13: Neutropenia; Figure S14: Anemia; Figure S15: Leucopenia; Figure S16: Thrombocytopenia; Figure S17: Nausea; Figure S18: Vomiting; Figure S19: Anorexia; Figure S20: Diarrhea; Figure S21: Constipation; Figure S22: Fatigue; Figure S23: Dyspnea; Figure S24: Alopecia; Figure S25: Rash; Figure S26: Hypomagnesemia; Figure S27: Hypokalemia; Figure S28: Pain; Figure S29: Headache; Figure S30: Abdominal pain; Figure S31: Back pain.
Author Contributions
Conceptualization, C.E. and R.V.; methodology, C.E. and R.V.; software, L.D.; validation, G.M. and T.B.; formal analysis, C.C., I.S.O. and S.L.; data curation, I.S.O, C.C. and G.L.; writing—original draft preparation, C.E. and R.V.; writing—review and editing, C.E. and R.V.; visualization, C.E., T.B. and L.D.; supervision, S.L., S.D.C. and G.L.; project administration, C.E. and R.V. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable. This article does not contain any studies with human participants or animals performed by any of the authors.
Informed Consent Statement
Not applicable. This article does not contain any studies with human participants or animals performed by any of the authors.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Ovary-Fact-Sheet.Pdf. 2020. https://gco.iarc.fr/today/data/factsheets/cancers/25-Ovary-fact-sheet.pdf (accessed on 28 January 2023).
- Luvero, D.; Milani, A.; Ledermann, J.A. Treatment Options in Recurrent Ovarian Cancer: Latest Evidence and Clinical Potential. Ther Adv Med Oncol 2014, 6, 229–239. [CrossRef]
- Matulonis, U.A.; Sood, A.K.; Fallowfield, L.; Howitt, B.E.; Sehouli, J.; Karlan, B.Y. Ovarian Cancer. Nat Rev Dis Primers 2016, 2, 16061. [CrossRef]
- Jayson, G.C.; Kohn, E.C.; Kitchener, H.C.; Ledermann, J.A. Ovarian Cancer. Lancet 2014, 384, 1376–1388. [CrossRef]
- Sherwood, L.M.; Parris, E.E.; Folkman, J. Tumor Angiogenesis: Therapeutic Implications. https://doi.org/10.1056/NEJM197111182852108 2010, 285, 1182–1186. [CrossRef]
- Folkman, J. Tumor Angiogenesis: Therapeutic Implications. New England Journal of Medicine 1971, 285, 1182–1186. [CrossRef]
- Jászai, J.; Schmidt, M.H.H. Trends and Challenges in Tumor Anti-Angiogenic Therapies. Cells 2019, 8. [CrossRef]
- Folkman, J. Tumor Angiogenesis: Therapeutic Implications. N Engl J Med 1971, 285, 1182–1186. [CrossRef]
- Akaza, H.; Nakagawa, M.; Tsuruo, T.; Saijo, N.; Sone, S.; Yamamoto, N.; Kakeji, Y.; Nakamura, S.; Kurebayashi, J.; Isonishi, S.; et al. Anti-Angiogenesis: New Concept for Therapy of Solid Tumors. Ann Surg 1972, 175, 409–416. [CrossRef]
- Carmeliet, P. VEGF as a Key Mediator of Angiogenesis in Cancer. Oncology 2005, 69, 4–10. [CrossRef]
- Dancey, J.; Sausville, E.A. Issues and Progress with Protein Kinase Inhibitors for Cancer Treatment. Nature Reviews Drug Discovery 2003 2:4 2003, 2, 296–313. [CrossRef]
- Ferrara, N. VEGF and the Quest for Tumour Angiogenesis Factors. Nat. Rev. Cancer 2002, 2, 795–803. [CrossRef]
- Ferrara, N.; Adamis, A.P. Ten Years of Anti-Vascular Endothelial Growth Factor Therapy. Nature Reviews Drug Discovery 2016 15:6 2016, 15, 385–403. [CrossRef]
- Olsson, A.K.; Dimberg, A.; Kreuger, J.; Claesson-Welsh, L. VEGF Receptor Signalling ? In Control of Vascular Function. Nature Reviews Molecular Cell Biology 2006 7:5 2006, 7, 359–371. [CrossRef]
- Elman, M.J.; Aiello, L.P.; Network, D.R.C.R.; al., et Randomized Trial Evaluating Ranibizumab plus Prompt or Deferred Laser or Triamcinolone plus Prompt Laser for Diabetic Macular Edema. Ophthalmology 2010, 117, 1064-1077 e35.
- Martin, D.F.; Maguire, M.G.; Group, C.R.; al., et Ranibizumab and Bevacizumab for Neovascular Age-Related Macular Degeneration. N Engl J Med 2011, 364, 1897–1908.
- Nguyen, Q.D.; Brown, D.M.; Marcus, D.M.; al., et Ranibizumab for Diabetic Macular Edema: Results from 2 Phase III Randomized Trials: RISE and RIDE. Ophthalmology 2012, 119, 789–801.
- Heier, J.S.; Brown, D.M.; Chong, V.; al., et Intravitreal Aflibercept (VEGF Trap-Eye) in Wet Age-Related Macular Degeneration. Ophthalmology 2012, 119, 2537–2548.
- Brown, D.M.; Campochiaro, P.A.; Bhisitkul, R.B.; al., et Sustained Benefits from Ranibizumab for Macular Edema Following Branch Retinal Vein Occlusion: 12-Month Outcomes of a Phase III Study. Ophthalmology 2011, 118, 1594–1602.
- Miller, J.W. The Harvard Angiogenesis Story. Surv Ophthalmol 2014, 59, 361–364. [CrossRef]
- Turcan, N.; Baros, A.; Zugravu, C.; Mergeanu, M.; Sajin, M.; Andreescu, C.V.; Frincu, F.; Carp-Veliscu, A.; Edu, A.; Mehedintu, C.; et al. Trend of Incidence in the Last Five Years of Breast, Cervical, Ovarian and Uterine Cancer in the Main Hospital in Romania. Romanian Journal of Medical Practice 2021, 16, 62–68. [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. The BMJ 2021, 372. [CrossRef]
- Mendeley Reference Manager | Mendeley Available online: https://www.mendeley.com/reference-management/reference-manager (accessed on 28 January 2023).
- McGuire, W.P.; Hoskins, W.J.; Brady, M.F.; Kucera, P.R.; Partridge, E.E.; Look, K.Y.; Clarke-Pearson, D.L.; Davidson, M. Cyclophosphamide and Cisplatin Compared with Paclitaxel and Cisplatin in Patients with Stage III and Stage IV Ovarian Cancer. New England Journal of Medicine 1996, 334, 1–6. [CrossRef]
- Amir-Behghadami, M.; Janati, A. Population, Intervention, Comparison, Outcomes and Study (PICOS) Design as a Framework to Formulate Eligibility Criteria in Systematic Reviews. Emergency Medicine Journal 2020, 37, 387. [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2011, 343. [CrossRef]
- 27. RevMan | Cochrane Training Available online: https://training.cochrane.org/online-learning/core-software/revman (accessed on 24 January 2023).
- Oza, A.M.; Cook, A.D.; Pfisterer, J.; Embleton, A.; Ledermann, J.A.; Pujade-Lauraine, E.; Kristensen, G.; Carey, M.S.; Beale, P.; Cervantes, A.; et al. Standard Chemotherapy with or without Bevacizumab for Women with Newly Diagnosed Ovarian Cancer (ICON7): Overall Survival Results of a Phase 3 Randomised Trial. Lancet Oncol 2015, 16, 928–936.
- Aghajanian, C.; Goff, B.; Nycum, L.R.; Wang, Y. v.; Husain, A.; Blank, S. v. Final Overall Survival and Safety Analysis of OCEANS, a Phase 3 Trial of Chemotherapy with or without Bevacizumab in Patients with Platinum-Sensitive Recurrent Ovarian Cancer. Gynecol Oncol 2015, 139, 10–16. [CrossRef]
- Gotlieb, W.H.; Amant, F.; Advani, S.; Goswami, C.; Hirte, H.; Provencher, D.; Somani, N.; Yamada, D.; Tamby, J.-F.; Vergote, I. Intravenous Afl Ibercept for Treatment of Recurrent Symptomatic Malignant Ascites in Patients with Advanced Ovarian Cancer: A Phase 2, Randomised, Double-Blind, Placebo-Controlled Study. Lancet Oncology 2012, 13, 154–162.
- Karlan, B.Y.; Oza, A.M.; Richardson, G.E.; Provencher, D.M.; Hansen, V.L.; Buck, M.; Chambers, S.K.; Ghatage, P.; Pippitt, C.H.; Brown, J. v.; et al. Randomized, Double-Blind, Placebo-Controlled Phase II Study of AMG 386 Combined with Weekly Paclitaxel in Patients with Recurrent Ovarian Cancer. Journal of Clinical Oncology 2012, 30, 362–371. [CrossRef]
- Burger, R.A.; Brady, M.F.; Bookman, M.A.; Fleming, G.F.; Monk, B.J.; Huang, H.; Mannel, R.S.; Homesley, H.D.; Fowler, J.; Greer, B.E.; et al. Incorporation of Bevacizumab in the Primary Treatment of Ovarian Cancer. New England Journal of Medicine 2011, 365, 2473–2483.
- Chekerov, R.; Hilpert, F.; Mahner, S.; El-Balat, A.; Harter, P.; de Gregorio, N.; Fridrich, C.; Markmann, S.; Potenberg, J.; Lorenz, R.; et al. Sorafenib plus Topotecan versus Placebo plus Topotecan for Platinum-Resistant Ovarian Cancer (TRIAS): A Multicentre, Randomised, Double-Blind, Placebo-Controlled, Phase 2 Trial. Lancet Oncol 2018, 19, 1247–1258.
- Coleman, R.L.; Brady, M.F.; Herzog, T.J.; Sabbatini, P.; Armstrong, D.K.; Walker, J.L.; Kim, B.G.; Fujiwara, K.; Tewari, K.S.; O’Malley, D.M.; et al. Bevacizumab and Paclitaxel–Carboplatin Chemotherapy and Secondary Cytoreduction in Recurrent, Platinum-Sensitive Ovarian Cancer (NRG Oncology/Gynecologic Oncology Group Study GOG-0213): A Multicentre, Open-Label, Randomised, Phase 3 Trial. Lancet Oncol 2017, 18, 779–791.
- du Bois, A.; Floquet, A.; Kim, J.W.; Rau, J.; del Campo, J.M.; Friedlander, M.; Pignata, S.; Fujiwara, K.; Vergote, I.; Colombo, N.; et al. Incorporation of Pazopanib in Maintenance Therapy of Ovarian Cancer. Journal of Clinical Oncology 2014, 32, 3374–3381. [CrossRef]
- Bois, A. du; Kristensen, G.; Ray-Coquard, I.; Reuss, A.; Pignata, S.; Colombo, N.; Denison, U.; Vergote, I.; del Campo, J.M.; Ottevanger, P.; et al. Standard First-Line Chemotherapy with or without Nintedanib for Advanced Ovarian Cancer (AGO-OVAR 12): A Randomised, Double-Blind, Placebo-Controlled Phase 3 Trial. Lancet Oncol 2016, 17, 78–89.
- Gore, M.; Hackshaw, A.; Brady, W.E.; Penson, R.T.; Zaino, R.; McCluggage, W.G.; Ganesan, R.; Wilkinson, N.; Perren, T.; Montes, A.; et al. An International, Phase III Randomized Trial in Patients with Mucinous Epithelial Ovarian Cancer (MEOC/GOG 0241) with Long-Term Follow-up: And Experience of Conducting a Clinical Trial in a Rare Gynecological Tumor. Gynecol Oncol 2019, 153, 541–548. [CrossRef]
- Herzog, T.J.; Scambia, G.; Kim, B.G.; Lhommé, C.; Markowska, J.; Ray-Coquard, I.; Sehouli, J.; Colombo, N.; Shan, M.; Petrenciuc, O.; et al. A Randomized Phase II Trial of Maintenance Therapy with Sorafenib in Front-Line Ovarian Carcinoma. Gynecol Oncol 2013, 130, 25–30. [CrossRef]
- Kim, J.W.; Mahner, S.; Wu, L.Y.; Shoji, T.; Kim, B.G.; Zhu, J.Q.; Takano, T.; Park, S.Y.; Kong, B.H.; Wu, Q.; et al. Pazopanib Maintenance Therapy in East Asian Women with Advanced Epithelial Ovarian Cancer: Results from AGO-OVAR16 and an East Asian Study. International Journal of Gynecological Cancer 2018, 28, 2–10. [CrossRef]
- Ledermann, J.A.; Hackshaw, A.; Kaye, S.; Jayson, G.; Gabra, H.; McNeish, I.; Earl, H.; Perren, T.; Gore, M.; Persic, M.; et al. Randomized Phase II Placebo-Controlled Trial of Maintenance Therapy Using the Oral Triple Angiokinase Inhibitor BIBF 1120 after Chemotherapy for Relapsed Ovarian Cancer. Journal of Clinical Oncology 2011, 29, 3798–3804. [CrossRef]
- Ledermann, J.A.; Embleton-Thirsk, A.C.; Perren, T.J.; Jayson, G.C.; Rustin, G.J.S.; Kaye, S.B.; Hirte, H.; Oza, A.; Vaughan, M.; Friedlander, M.; et al. Cediranib in Addition to Chemotherapy for Women with Relapsed Platinum-Sensitive Ovarian Cancer (ICON6): Overall Survival Results of a Phase III Randomised Trial. ESMO Open 2021, 6. [CrossRef]
- Ledermann, J.A.; Embleton, A.C.; Raja, F.; Perren, T.J.; Jayson, G.C.; Rustin, G.J.S.; Kaye, S.B.; Hirte, H.; Eisenhauer, E.; Vaughan, M.; et al. Cediranib in Patients with Relapsed Platinum-Sensitive Ovarian Cancer (ICON6): A Randomised, Double-Blind, Placebo-Controlled Phase 3 Trial. The Lancet 2016, 387, 1066–1074. [CrossRef]
- Liu, J.F.; Barry, W.T.; Birrer, M.; Lee, J.M.; Buckanovich, R.J.; Fleming, G.F.; Rimel, B.J.; Buss, M.K.; Nattam, S.R.; Hurteau, J.; et al. Overall Survival and Updated Progression-Free Survival Outcomes in a Randomized Phase II Study of Combination Cediranib and Olaparib versus Olaparib in Relapsed Platinum-Sensitive Ovarian Cancer. Annals of Oncology 2019, 30, 551–557. [CrossRef]
- Marth, C.; Vergote, I.; Scambia, G.; Oberaigner, W.; Clamp, A.; Berger, R.; Kurzeder, C.; Colombo, N.; Vuylsteke, P.; Lorusso, D.; et al. ENGOT-Ov-6/TRINOVA-2: Randomised, Double-Blind, Phase 3 Study of Pegylated Liposomal Doxorubicin plus Trebananib or Placebo in Women with Recurrent Partially Platinum-Sensitive or Resistant Ovarian Cancer. Eur J Cancer 2017, 70, 111–121. [CrossRef]
- Monk, B.J.; Poveda, A.; Vergote, I.; Raspagliesi, F.; Fujiwara, K.; Bae, D.S.; Oaknin, A.; Ray-Coquard, I.; Provencher, D.M.; Karlan, B.Y.; et al. Final Results of a Phase 3 Study of Trebananib plus Weekly Paclitaxel in Recurrent Ovarian Cancer (TRINOVA-1): Long-Term Survival, Impact of Ascites, and Progression-Free Survival-2. Gynecol Oncol 2016, 143, 27–34. [CrossRef]
- Pignata, S.; Lorusso, D.; Joly, F.; Gallo, C.; Colombo, N.; Sessa, C.; Bamias, A.; Salutari, V.; Selle, F.; Frezzini, S.; et al. Carboplatin-Based Doublet plus Bevacizumab beyond Progression versus Carboplatin-Based Doublet Alone in Patients with Platinum-Sensitive Ovarian Cancer: A Randomised, Phase 3 Trial; 2021; Vol. 22.
- Pignata, S.; Lorusso, D.; Scambia, G.; Sambataro, D.; Tamberi, S.; Cinieri, S.; Mosconi, A.M.; Orditura, M.; Brandes, A.A.; Arcangeli, V.; et al. Pazopanib plus Weekly Paclitaxel versus Weekly Paclitaxel Alone for Platinum-Resistant or Platinum-Refractory Advanced Ovarian Cancer (MITO 11): A Randomised, Open-Label, Phase 2 Trial. Lancet Oncol 2015, 16, 561–568.
- Pujade-Lauraine, E.; Hilpert, F.; Weber, B.; Reuss, A.; Poveda, A.; Kristensen, G.; Sorio, R.; Vergote, I.; Witteveen, P.; Bamias, A.; et al. Bevacizumab Combined with Chemotherapy for Platinum-Resistant Recurrent Ovarian Cancer: The AURELIA Open-Label Randomized Phase III Trial. Journal of Clinical Oncology 2014, 32, 1302–1308. [CrossRef]
- Ray-Coquard, I.; Cibula, D.; Mirza, M.R.; Reuss, A.; Ricci, C.; Colombo, N.; Koch, H.; Goffin, F.; González-Martin, A.; Ottevanger, P.B.; et al. Final Results from GCIG/ENGOT/AGO-OVAR 12, a Randomised Placebo-Controlled Phase III Trial of Nintedanib Combined with Chemotherapy for Newly Diagnosed Advanced Ovarian Cancer. Int J Cancer 2020, 146, 439–448. [CrossRef]
- 50. Richardson, D.L.; Sill, M.W.; Coleman, R.L.; Sood, A.K.; Pearl, M.L.; Kehoe, S.M.; Carney, M.E.; Hanjani, P.; van Le, L.; Zhou, X.C.; et al. Paclitaxel with and without Pazopanib for Persistent or Recurrent Ovarian Cancer: A Randomized Clinical Trial. In Proceedings of the JAMA Oncology; American Medical Association, February 1 2018; Vol. 4, pp. 196–202.
- Tewari, K.S.; Burger, R.A.; Enserro, D.; Norquist, B.M.; Swisher, E.M.; Brady, M.F.; Bookman, M.A.; Fleming, G.F.; Huang, H.; Homesley, H.D.; et al. Final Overall Survival of a Randomized Trial of Bevacizumab for Primary Treatment of Ovarian Cancer. J Clin Oncol 2019, 37, 2317–2328.
- Vergote, I.; du Bois, A.; Floquet, A.; Rau, J.; Kim, J.W.; del Campo, J.M.; Friedlander, M.; Pignata, S.; Fujiwara, K.; Colombo, N.; et al. Overall Survival Results of AGO-OVAR16: A Phase 3 Study of Maintenance Pazopanib versus Placebo in Women Who Have Not Progressed after First-Line Chemotherapy for Advanced Ovarian Cancer. Gynecol Oncol 2019, 155, 186–191. [CrossRef]
- Vergote, I.; Scambia, G.; O’Malley, D.; van Calster, B.; Park, S.Y.; del Campo, J.M.; Meier, W.; Bamias, A.; Colombo, N.; Wenham, R.M.; et al. Trebananib or Placebo plus Carboplatin and Paclitaxel as First-Line Treatment for Advanced Ovarian Cancer (TRINOVA-3/ENGOT-Ov2/GOG-3001): A Randomised, Double-Blind, Phase 3 Trial. Lancet Oncol 2019, 20, 862–876.
- Helali, A. el; Wong, C.H.L.; Choi, H.C.W.; Chan, W.W.L.; Dickson, N.; Siu, S.W.K.; Chan, K.K.; Ngan, H.Y.S.; Ngan, R.K.C.; Kennedy, R.D. A Comprehensive Systematic Review and Network Meta-Analysis: The Role of Anti-Angiogenic Agents in Advanced Epithelial Ovarian Cancer. Sci Rep 2022, 12. [CrossRef]
- Ray-Coquard, I.; Pautier, P.; Pignata, S.; Pérol, D.; González-Martín, A.; Berger, R.; Fujiwara, K.; Vergote, I.; Colombo, N.; Mäenpää, J.; et al. Olaparib plus Bevacizumab as First-Line Maintenance in Ovarian Cancer. New England Journal of Medicine 2019, 381, 2416–2428. [CrossRef]
- Kay, A.; Higgins, J.; Day, A.G.; Meyer, R.M.; Booth, C.M. Randomized Controlled Trials in the Era of Molecular Oncology: Methodology, Biomarkers, and End Points. Annals of Oncology 2012, 23, 1646–1651. [CrossRef]
- A Review of Studies Examining the Relationship between Progression-Free Survival and Overall Survival in Advanced or Metastatic Cancer [Internet] - PubMed Available online: https://pubmed.ncbi.nlm.nih.gov/28481488/ (accessed on 27 January 2023).
- Kim, C.; Prasad, V. Cancer Drugs Approved on the Basis of a Surrogate End Point and Subsequent Overall Survival: An Analysis of 5 Years of US Food and Drug Administration Approvals. JAMA Intern Med 2015, 175, 1992–1994. [CrossRef]
- Pasalic, D.; McGinnis, G.J.; Fuller, C.D.; Grossberg, A.J.; Verma, V.; Mainwaring, W.; Miller, A.B.; Lin, T.A.; Jethanandani, A.; Espinoza, A.F.; et al. Progression-Free Survival Is a Suboptimal Predictor for Overall Survival Among Metastatic Solid Tumor Clinical Trials. Eur J Cancer 2020, 136, 176. [CrossRef]
- Prasad, V.; Kim, C.; Burotto, M.; Vandross, A. The Strength of Association between Surrogate End Points and Survival in Oncology: A Systematic Review of Trial-Level Meta-Analyses. JAMA Intern Med 2015, 175, 1389–1398. [CrossRef]
- Paoletti, X.; Lewsley, L.A.; Daniele, G.; Cook, A.; Yanaihara, N.; Tinker, A.; Kristensen, G.; Ottevanger, P.B.; Aravantinos, G.; Miller, A.; et al. Assessment of Progression-Free Survival as a Surrogate End Point of Overall Survival in First-Line Treatment of Ovarian Cancer: A Systematic Review and Meta-Analysis. JAMA Netw Open 2020, 3. [CrossRef]
- Backen, A.; Renehan, A.G.; Clamp, A.R.; Berzuini, C.; Zhou, C.; Oza, A.; Bannoo, S.; Scherer, S.J.; Banks, R.E.; Dive, C.; et al. The Combination of Circulating Ang1 and Tie2 Levels Predict Progression Free Survival Advantage in Bevacizumab-Treated Ovarian Cancer Patients. Clin Cancer Res 2014, 20, 4549. [CrossRef]
- Gourley, C.; McCavigan, A.; Perren, T.; Paul, J.; Michie, C.O.; Churchman, M.; Williams, A.; McCluggage, W.G.; Parmar, M.; Kaplan, R.S.; et al. Molecular Subgroup of High-Grade Serous Ovarian Cancer (HGSOC) as a Predictor of Outcome Following Bevacizumab. Journal of Clinical Oncology 2014, 32, 5502–5502. [CrossRef]
- Collinson, F.; Hutchinson, M.; Craven, R.A.; Cairns, D.A.; Zougman, A.; Wind, T.C.; Gahir, N.; Messenger, M.P.; Jackson, S.; Thompson, D.; et al. Predicting Response to Bevacizumab in Ovarian Cancer: A Panel of Potential Biomarkers Informing Treatment Selection. Clin Cancer Res 2013, 19, 5227. [CrossRef]
- Jayson, G.C.; Kerbel, R.; Ellis, L.M.; Harris, A.L. Antiangiogenic Therapy in Oncology: Current Status and Future Directions. The Lancet 2016, 388, 518–529. [CrossRef]
- Birrer, M.J.; Choi, Y.; Brady, M.F.; Mannel, R.S.; Burger, R.A.; WEI, W.; Husain, A.; Bais, C. Retrospective Analysis of Candidate Predictive Tumor Biomarkers (BMs) for Efficacy in the GOG-0218 Trial Evaluating Front-Line Carboplatin–Paclitaxel (CP) ± Bevacizumab (BEV) for Epithelial Ovarian Cancer (EOC). Journal of Clinical Oncology 2015, 33, 5505–5505. [CrossRef]
- Bais, C.; Mueller, B.; Brady, M.F.; Mannel, R.S.; Burger, R.A.; Wei, W.; Marien, K.M.; Kockx, M.M.; Husain, A.; Birrer, M.J. Tumor Microvessel Density as a Potential Predictive Marker for Bevacizumab Benefit: GOG-0218 Biomarker Analyses. JNCI Journal of the National Cancer Institute 2017, 109. [CrossRef]
- Secord, A.A.; Burdett, K.B.; Owzar, K.; Tritchler, D.; Sibley, A.B.; Liu, Y.; Starr, M.D.; Chris Brady, J.; Lankes, H.A.; Hurwitz, H.I.; et al. Predictive Blood-Based Biomarkers in Patients with Epithelial Ovarian Cancer Treated with Carboplatin and Paclitaxel with or without Bevacizumab: Results from GOG-0218. Clinical Cancer Research 2020, 26, 1288–1296. [CrossRef]
- Liu, Q.; Yang, X.; Yin, Y.; Zhang, H.; Yin, F.; Guo, P.; Zhang, X.; Sun, C.; Li, S.; Han, Y.; et al. Identifying the Role of Oxidative Stress-Related Genes as Prognostic Biomarkers and Predicting the Response of Immunotherapy and Chemotherapy in Ovarian Cancer. Oxid Med Cell Longev 2022, 2022, 6575534. [CrossRef]
- Chaiswing, L.; Yarana, C.; st. Clair, W.; Tovmasyan, A.; Batinic-Haberle, I.; Spasojevic, I.; st. Clair, D. A Redox-Active Mn Porphyrin, MnTnBuOE-2-PyP5+, Synergizes with Carboplatin in Treatment of Chemoresistant Ovarian Cell Line. Oxid Med Cell Longev 2022, 2022. [CrossRef]
- Cecerska-Heryć, E.; Surowska, O.; Heryć, R.; Serwin, N.; Napiontek-Balińska, S.; Dołęgowska, B. Are Antioxidant Enzymes Essential Markers in the Diagnosis and Monitoring of Cancer Patients – A Review. Clin Biochem 2021, 93, 1–8. [CrossRef]
- Fletcher, N.M.; Belotte, J.; Saed, M.G.; Memaj, I.; Diamond, M.P.; Morris, R.T.; Saed, G.M. Specific Point Mutations in Key Redox Enzymes Are Associated with Chemoresistance in Epithelial Ovarian Cancer. Free Radic Biol Med 2017, 102, 122–132. [CrossRef]
- Senthil, K.; Aranganathan, S.; Nalini, N. Evidence of Oxidative Stress in the Circulation of Ovarian Cancer Patients. Clinica Chimica Acta 2004, 339, 27–32. [CrossRef]
- Friedlander, M.; Rau, J.; Lee, C.K.; Meier, W.; Lesoin, A.; Kim, J.W.; Poveda, A.; Buck, M.; Scambia, G.; Shimada, M.; et al. Quality of Life in Patients with Advanced Epithelial Ovarian Cancer (EOC) Randomized to Maintenance Pazopanib or Placebo after First-Line Chemotherapy in the AGO-OVAR 16 Trial. Measuring What Matters-Patient-Centered End Points in Trials of Maintenance Therapy. Annals of Oncology 2018, 29, 737–743. [CrossRef]
- Stark, D.; Nankivell, M.; Pujade-Lauraine, E.; Kristensen, G.; Elit, L.; Stockler, M.; Hilpert, F.; Cervantes, A.; Brown, J.; Lanceley, A.; et al. Standard Chemotherapy with or without Bevacizumab in Advanced Ovarian Cancer: Quality-of-Life Outcomes from the International Collaboration on Ovarian Neoplasms (ICON7) Phase 3 Randomised Trial. Lancet Oncol 2013, 14, 236–243.
- Bindra, R.S.; Schaffer, P.J.; Meng, A.; Woo, J.; Måseide, K.; Roth, M.E.; Lizardi, P.; Hedley, D.W.; Bristow, R.G.; Glazer, P.M. Down-Regulation of Rad51 and Decreased Homologous Recombination in Hypoxic Cancer Cells. Mol Cell Biol 2004, 24, 8504–8518. [CrossRef]
- Mirza, M.R.; Pignata, S.; Ledermann, J.A. Latest Clinical Evidence and Further Development of PARP Inhibitors in Ovarian Cancer. 2018.
- Bindra, R.S.; Gibson, S.L.; Meng, A.; Westermark, U.; Jasin, M.; Pierce, A.J.; Bristow, R.G.; Classon, M.K.; Glazer, P.M. Hypoxia-Induced down-Regulation of BRCA1 Expression by E2Fs. Cancer Res 2005, 65, 11597–11604. [CrossRef]
- Lorusso, D.; Maltese, G.; Sabatucci, I.; Cresta, S.; Matteo, C.; Ceruti, T.; D’Incalci, M.; Zucchetti, M.; Raspagliesi, F.; Sonetto, C.; et al. Phase I Study of Rucaparib in Combination with Bevacizumab in Ovarian Cancer Patients: Maximum Tolerated Dose and Pharmacokinetic Profile. Target Oncol 2021, 16, 59–68. [CrossRef]
- Carboplatin-Paclitaxel-Bevacizumab vs Carbo-Pacli-Beva-Rucaparib vs Carbo-Pacli-Ruca, Selected According to HRD Status, in Patients With Advanced Ovarian, Primary Peritoneal and Fallopian Tube Cancer, Preceded by a Phase I Dose Escalation Study on Ruca-Beva Combination - Full Text View - ClinicalTrials.Gov Available online: https://clinicaltrials.gov/ct2/show/NCT03462212 (accessed on 27 January 2023).
- Mirza, M.R.; Bergmann, T.K.; Mau-Sørensen, M.; Christensen, R. de P.; Åvall-Lundqvist, E.; Birrer, M.J.; Jørgensen, M.; Roed, H.; Malander, S.; Nielsen, F.; et al. A Phase I Study of the PARP Inhibitor Niraparib in Combination with Bevacizumab in Platinum-Sensitive Epithelial Ovarian Cancer: NSGO AVANOVA1/ENGOT-OV24. Cancer Chemother Pharmacol 2019, 84, 791–798. [CrossRef]
- Stapor, P.; Wang, X.; Goveia, J.; Moens, S.; Carmeliet, P. Angiogenesis Revisited - Role and Therapeutic Potential of Targeting Endothelial Metabolism. J Cell Sci 2014, 127, 4331–4341.
- de Bock, K.; Cauwenberghs, S.; Carmeliet, P. Vessel Abnormalization: Another Hallmark of Cancer?: Molecular Mechanisms and Therapeutic Implications. Curr Opin Genet Dev 2011, 21, 73–79. [CrossRef]
- Michaelsen, S.R.; Staberg, M.; Pedersen, H.; Jensen, K.E.; Majewski, W.; Broholm, H.; Nedergaard, M.K.; Meulengracht, C.; Urup, T.; Villingshøj, M.; et al. VEGF-C Sustains VEGFR2 Activation under Bevacizumab Therapy and Promotes Glioblastoma Maintenance. Neuro Oncol 2018, 20, 1462–1474. [CrossRef]
- Taylor, A.P.; Rodriguez, M.; Adams, K.; Goldenberg, D.M.; Blumenthal, R.D. Altered Tumor Vessel Maturation and Proliferation in Placenta Growth Factor-Producing Tumors: Potential Relationship to Post-Therapy Tumor Angiogenesis and Recurrence. Int J Cancer 2003, 105, 158–164. [CrossRef]
- Shojaei, F.; Wu, X.; Zhong, C.; Yu, L.; Liang, X.H.; Yao, J.; Blanchard, D.; Bais, C.; Peale, F. v.; van Bruggen, N.; et al. Bv8 Regulates Myeloid-Cell-Dependent Tumour Angiogenesis. Nature 2007 450:7171 2007, 450, 825–831. [CrossRef]
- Shojaei, F.; Wu, X.; Malik, A.K.; Zhong, C.; Baldwin, M.E.; Schanz, S.; Fuh, G.; Gerber, H.-P.; Ferrara, N. Tumor Refractoriness to Anti-VEGF Treatment Is Mediated by CD11b+Gr1+ Myeloid Cells. Nature Biotechnology 2007 25:8 2007, 25, 911–920. [CrossRef]
- Li, D.; Xie, K.; Ding, G.; Li, J.; Chen, K.; Li, H.; Qian, J.; Jiang, C.; Fang, J. Tumor Resistance to Anti-VEGF Therapy through up-Regulation of VEGF-C Expression. Cancer Lett 2014, 346, 45–52. [CrossRef]
- Crawford, Y.; Kasman, I.; Yu, L.; Zhong, C.; Wu, X.; Modrusan, Z.; Kaminker, J.; Ferrara, N. PDGF-C Mediates the Angiogenic and Tumorigenic Properties of Fibroblasts Associated with Tumors Refractory to Anti-VEGF Treatment. Cancer Cell 2009, 15, 21–34. [CrossRef]
- Casanovas, O.; Hicklin, D.J.; Bergers, G.; Hanahan, D. Drug Resistance by Evasion of Antiangiogenic Targeting of VEGF Signaling in Late-Stage Pancreatic Islet Tumors. Cancer Cell 2005, 8, 299–309. [CrossRef]
- Wang, H.; Xu, T.; Zheng, L.; Li, G. Angiogenesis Inhibitors for the Treatment of Ovarian Cancer: An Updated Systematic Review and Meta-Analysis of Randomized Controlled Trials. International Journal of Gynecological Cancer 2018, 28, 903–914.
- Guo, C.; Yan, C.; Qu, L.; Du, R.; Lin, J. The Efficacy and Toxicity of Angiogenesis Inhibitors for Ovarian Cancer: A Meta-Analysis of Randomized Controlled Trials. Arch Gynecol Obstet 2021, 303, 285–311. [CrossRef]
- Ye, Q.; Chen, H.L. Bevacizumab in the Treatment of Ovarian Cancer: A Meta-Analysis from Four Phase III Randomized Controlled Trials. Arch Gynecol Obstet 2013, 288, 655–666.
- Zhou, M.; Yu, P.; Qu, X.; Liu, Y.; Zhang, J. Phase III Trials of Standard Chemotherapy with or without Bevacizumab for Ovarian Cancer: A Meta-Analysis. PLoS One 2013, 8, e81858. [CrossRef]
- Li, X.; Zhu, S.; Hong, C.; Cai, H. Angiogenesis Inhibitors for Patients with Ovarian Cancer: A Meta-Analysis of 12 Randomized Controlled Trials. Curr Med Res Opin 2016, 32, 555–562. [CrossRef]
- Shen Wu, Y.; Shui, L.; Shen, D.; Chen, X. Bevacizumab Combined with Chemotherapy for Ovarian Cancer: An Updated Systematic Review and Meta-Analysis of Randomized Controlled Trials. Oncotarget 2017, 8, 10703–10713.
- Jiang, Y.; Sun, X.; Kong, B.; Jiang, J. Antiangiogenesis Therapy in Ovarian Cancer Patients: An Updated Meta-Analysis for 15 Randomized Controlled Trials. Medicine 2018, 97. [CrossRef]
- Li, J.; Li, S.; Chen, R.; Yu, H.; Lu, X. The Prognostic Significance of Anti-Angiogenesis Therapy in Ovarian Cancer: A Meta-Analysis. J Ovarian Res 2015, 8. [CrossRef]
- Marchetti, C.; de Felice, F.; Palaia, I.; Musella, A.; di Donato, V.; Gasparri, M.L.; Musio, D.; Muzii, L.; Tombolini, V.; Panici, P.B. Efficacy and Toxicity of Bevacizumab in Recurrent Ovarian Disease: An Update Meta-Analysis on Phase III Trials. Oncotarget 2016, 7, 13221. [CrossRef]
- Li, J.; Zhou, L.; Chen, X.; Ba, Y. Addition of Bevacizumab to Chemotherapy in Patients with Ovarian Cancer: A Systematic Review and Meta-Analysis of Randomized Trials. Clinical and Translational Oncology 2015, 17, 673–683.
- Wang, T.S.; Lei, W.; Cui, W.; Wen, P.; Guo, H.F.; Ding, S.G.; Yang, Y.P.; Xu, Y.Q.; Lv, S.W.; Zhu, Y.L. A Meta-Analysis of Bevacizumab Combined with Chemotherapy in the Treatment of Ovarian Cancer. Indian J Cancer 2014, 51 Suppl 3, e95–e98. [CrossRef]
- Matulonis, U.A.; Shapira-Frommer, R.; Santin, A.D.; Lisyanskaya, A.S.; Pignata, S.; Vergote, I.; Raspagliesi, F.; Sonke, G.S.; Birrer, M.; Provencher, D.M.; et al. Antitumor Activity and Safety of Pembrolizumab in Patients with Advanced Recurrent Ovarian Cancer: Results from the Phase II KEYNOTE-100 Study. Annals of Oncology 2019, 30, 1080–1087. [CrossRef]
- Hall, M.R.; Dehbi, H.M.; Banerjee, S.; Lord, R.; Clamp, A.; Ledermann, J.A.; Nicum, S.; Lilleywhite, R.; Bowen, R.; Michael, A.; et al. A Phase II Randomised, Placebo-Controlled Trial of Low Dose (Metronomic) Cyclophosphamide and Nintedanib (BIBF1120) in Advanced Ovarian, Fallopian Tube or Primary Peritoneal Cancer. Gynecol Oncol 2020, 159, 692–698. [CrossRef]
Figure 1.
Literature search flow diagram.
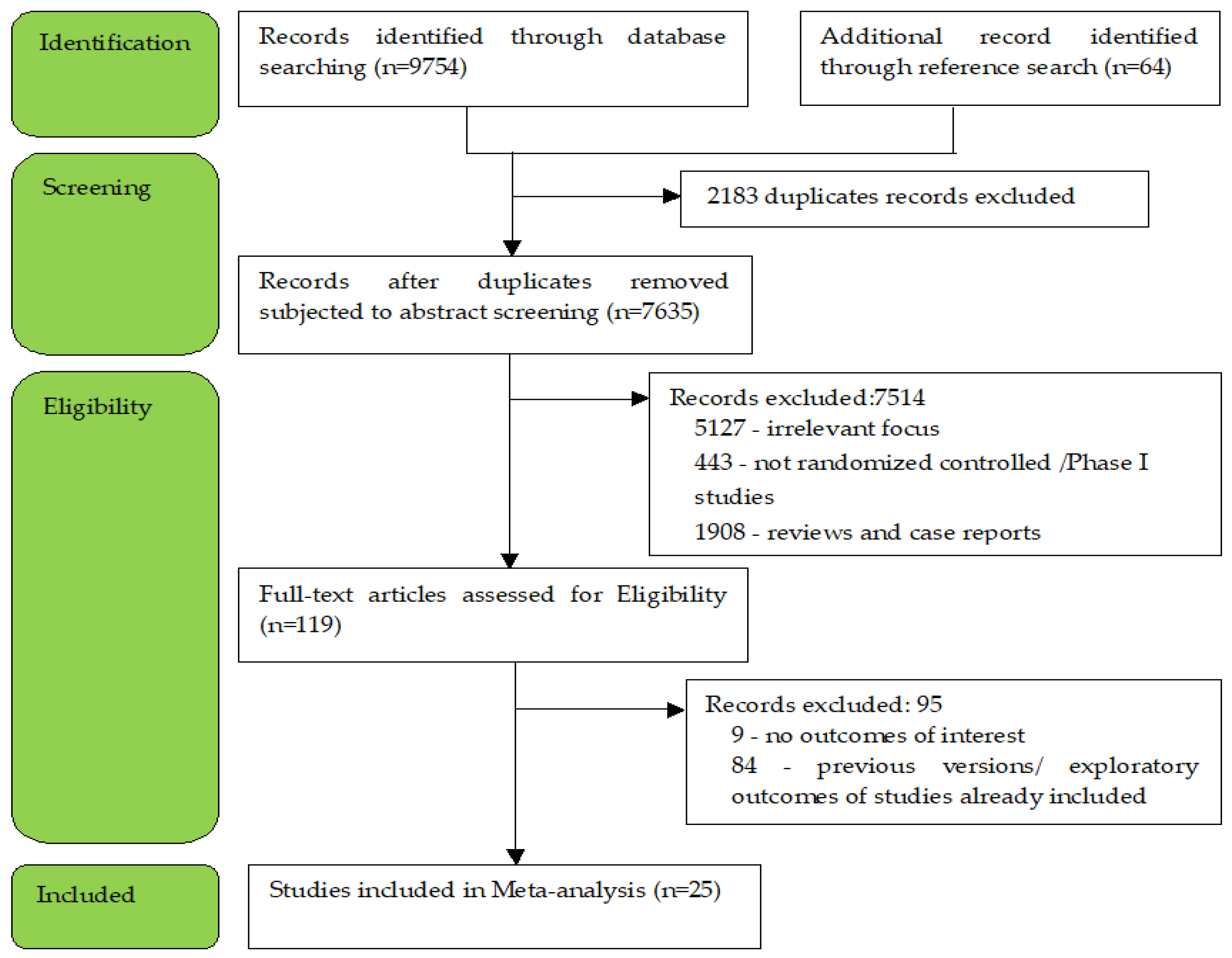
Figure 2.
Risk of bias graph: (a) Review of authors’ judgements about each risk of bias item presented as low risk (green), unclear risk (yellow) or high risk (red) for each included study; (b) Risk of bias summary across all included studies presented as a percentage.
Figure 2.
Risk of bias graph: (a) Review of authors’ judgements about each risk of bias item presented as low risk (green), unclear risk (yellow) or high risk (red) for each included study; (b) Risk of bias summary across all included studies presented as a percentage.
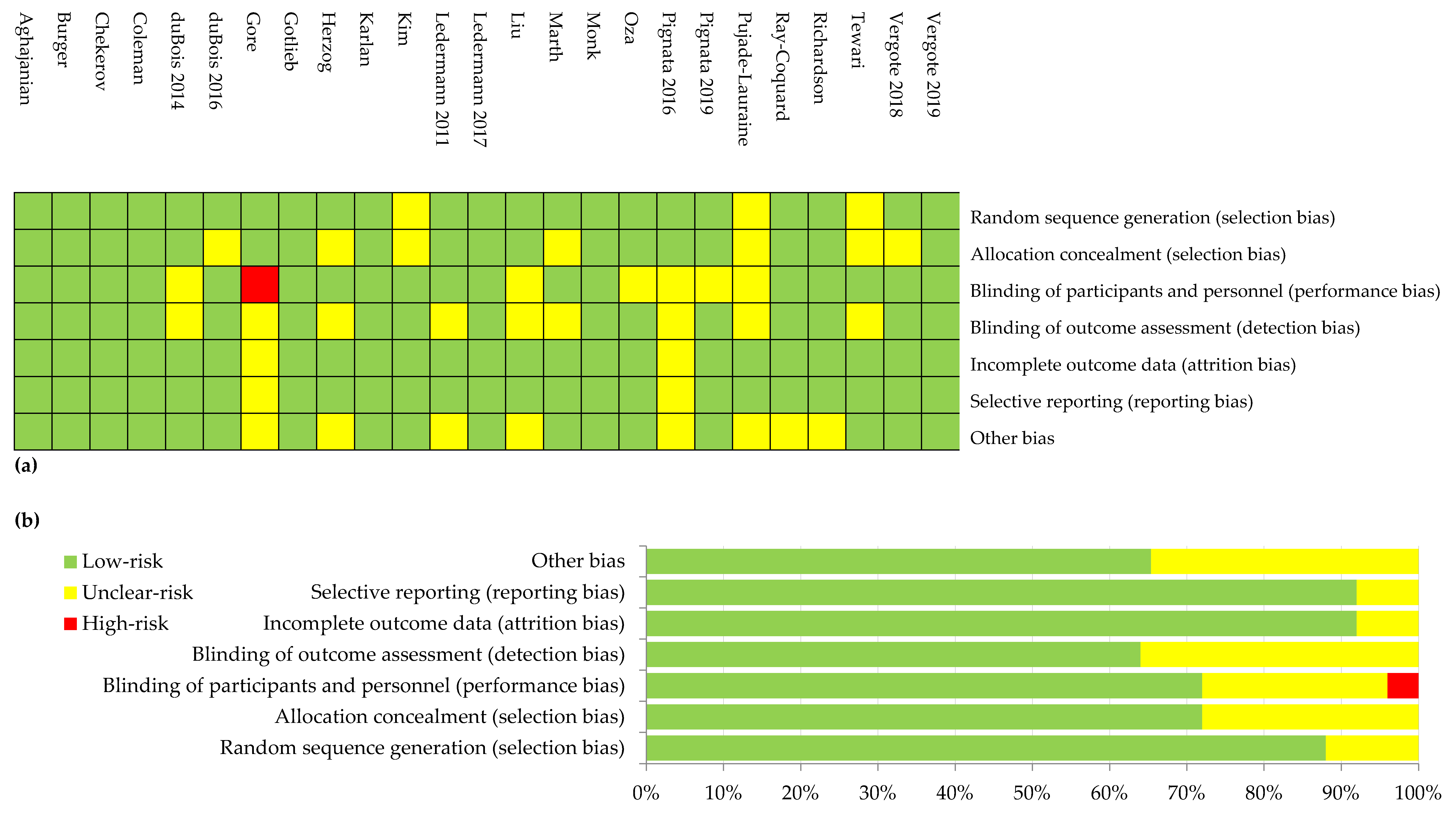
Figure 3.
Settings subgroup analysis of progression:(a) First-line; (b) Recurrent; (c) P-S R; (d) P-R R; (e) maintenance.
Figure 3.
Settings subgroup analysis of progression:(a) First-line; (b) Recurrent; (c) P-S R; (d) P-R R; (e) maintenance.
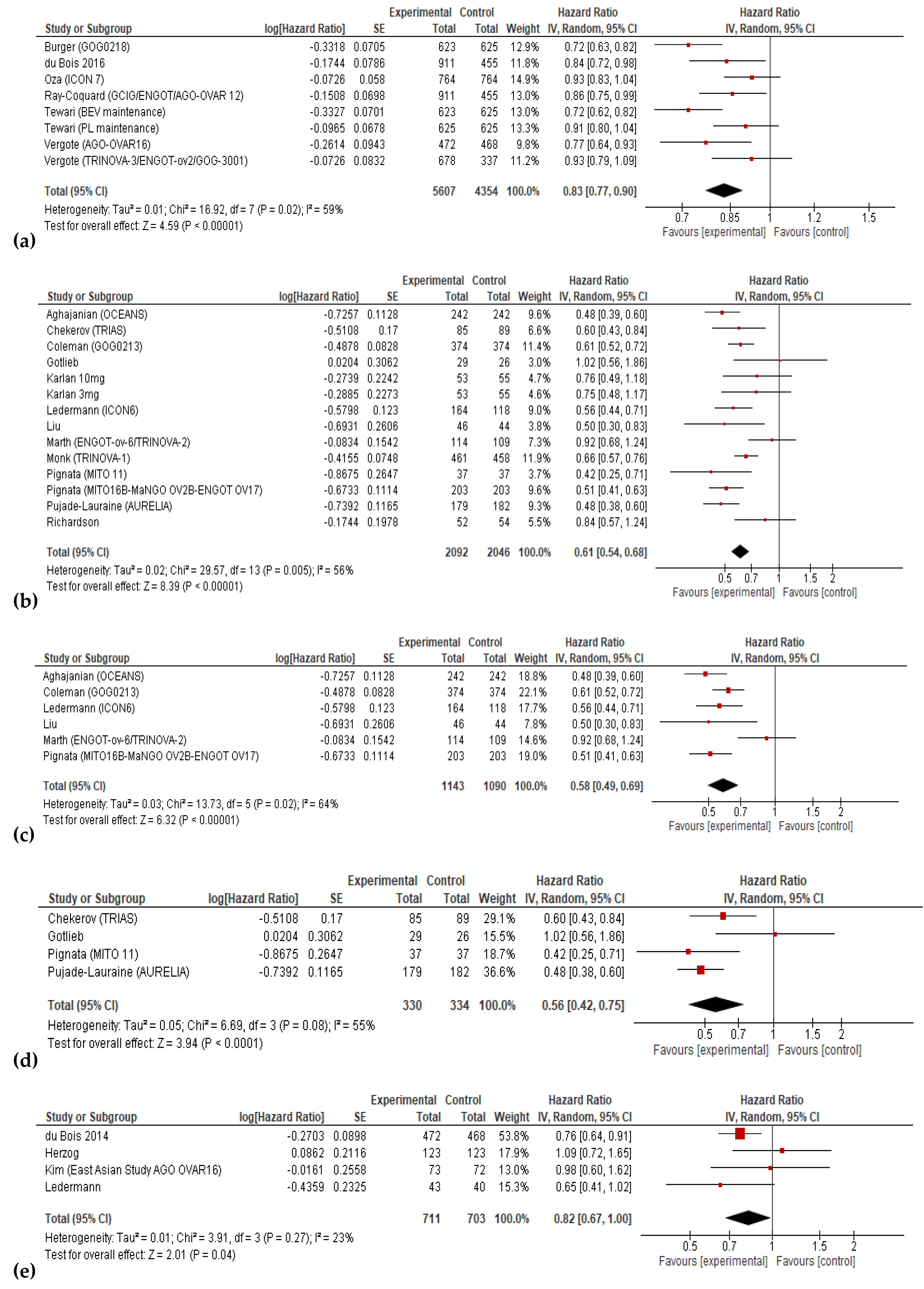
Figure 4.
Settings subgroup analysis of overall survival: (a) First-line; (b) Recurrent; (c) P-S R; (d) P-R R; (e) maintenance.
Figure 4.
Settings subgroup analysis of overall survival: (a) First-line; (b) Recurrent; (c) P-S R; (d) P-R R; (e) maintenance.
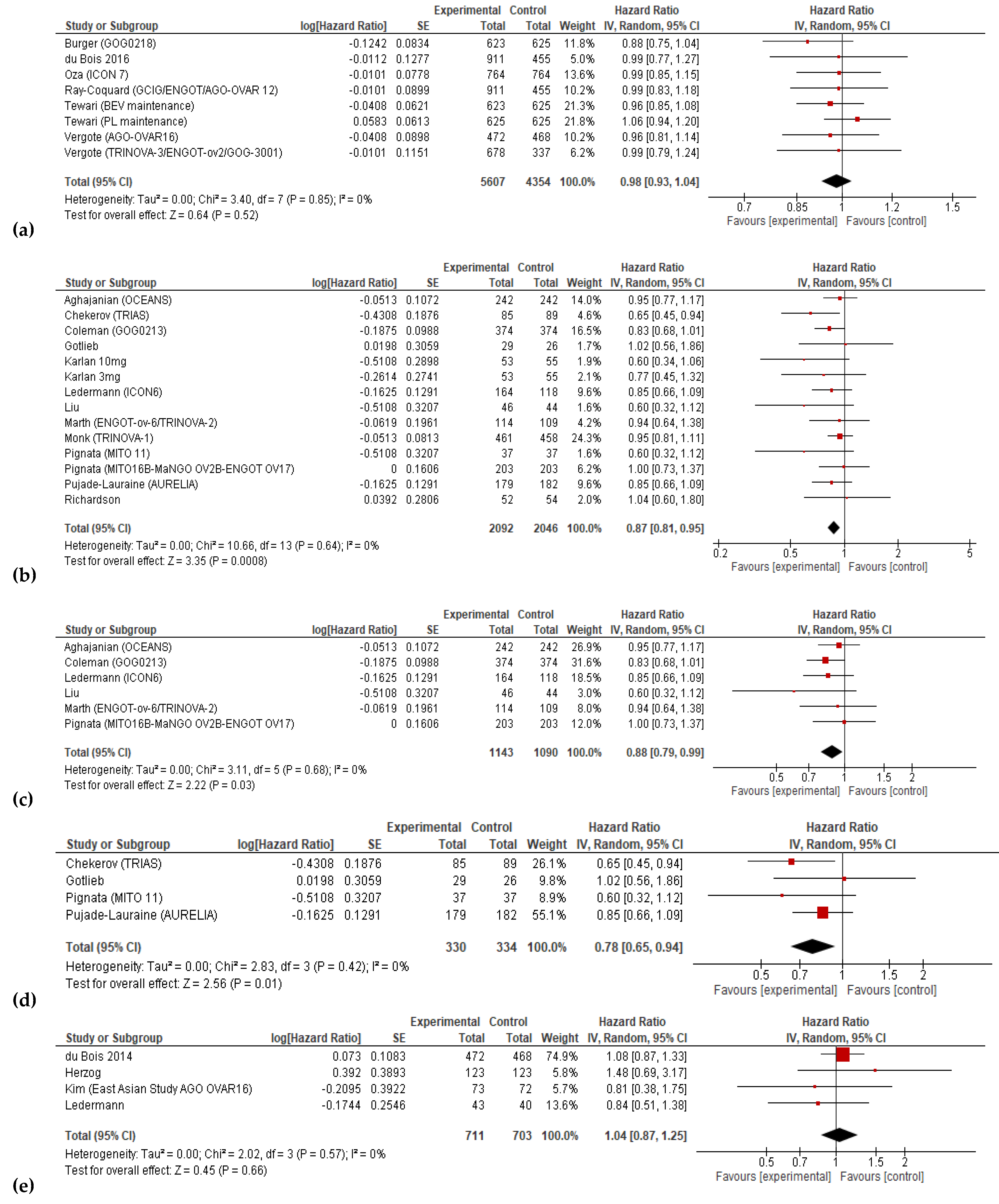
Figure 5.
Action-mechanisms subgroup analysis of progression: (a) VEGF inhibitors; (b) VEGF-R inhibitors; (c) angiopoietin inhibitors;.
Figure 5.
Action-mechanisms subgroup analysis of progression: (a) VEGF inhibitors; (b) VEGF-R inhibitors; (c) angiopoietin inhibitors;.
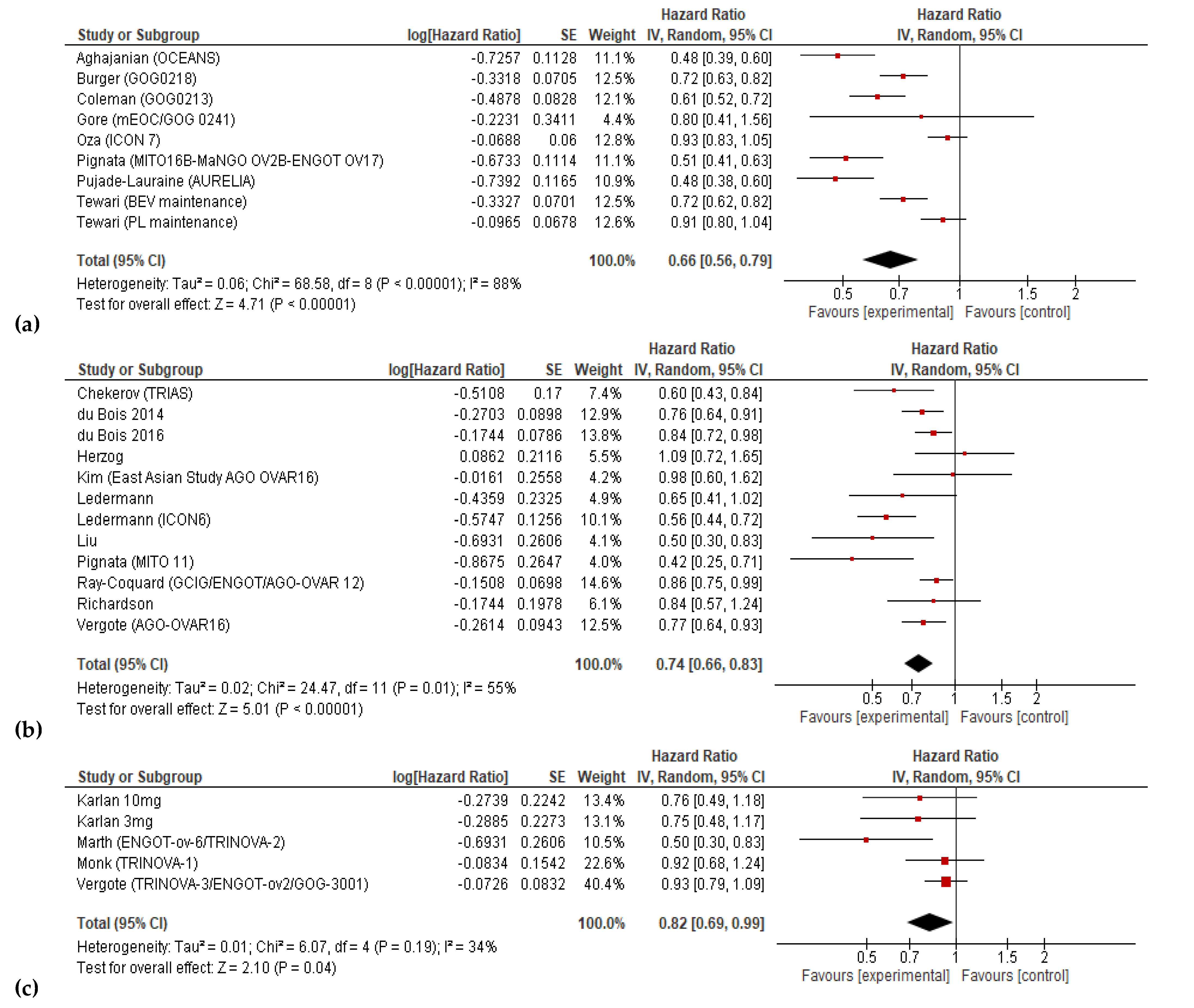
Figure 6.
Action-mechanisms subgroup analysis of overall survival: (a) VEGF inhibitors; (b) VEGF-R inhibitors; (c) angiopoietin inhibitors.
Figure 6.
Action-mechanisms subgroup analysis of overall survival: (a) VEGF inhibitors; (b) VEGF-R inhibitors; (c) angiopoietin inhibitors.
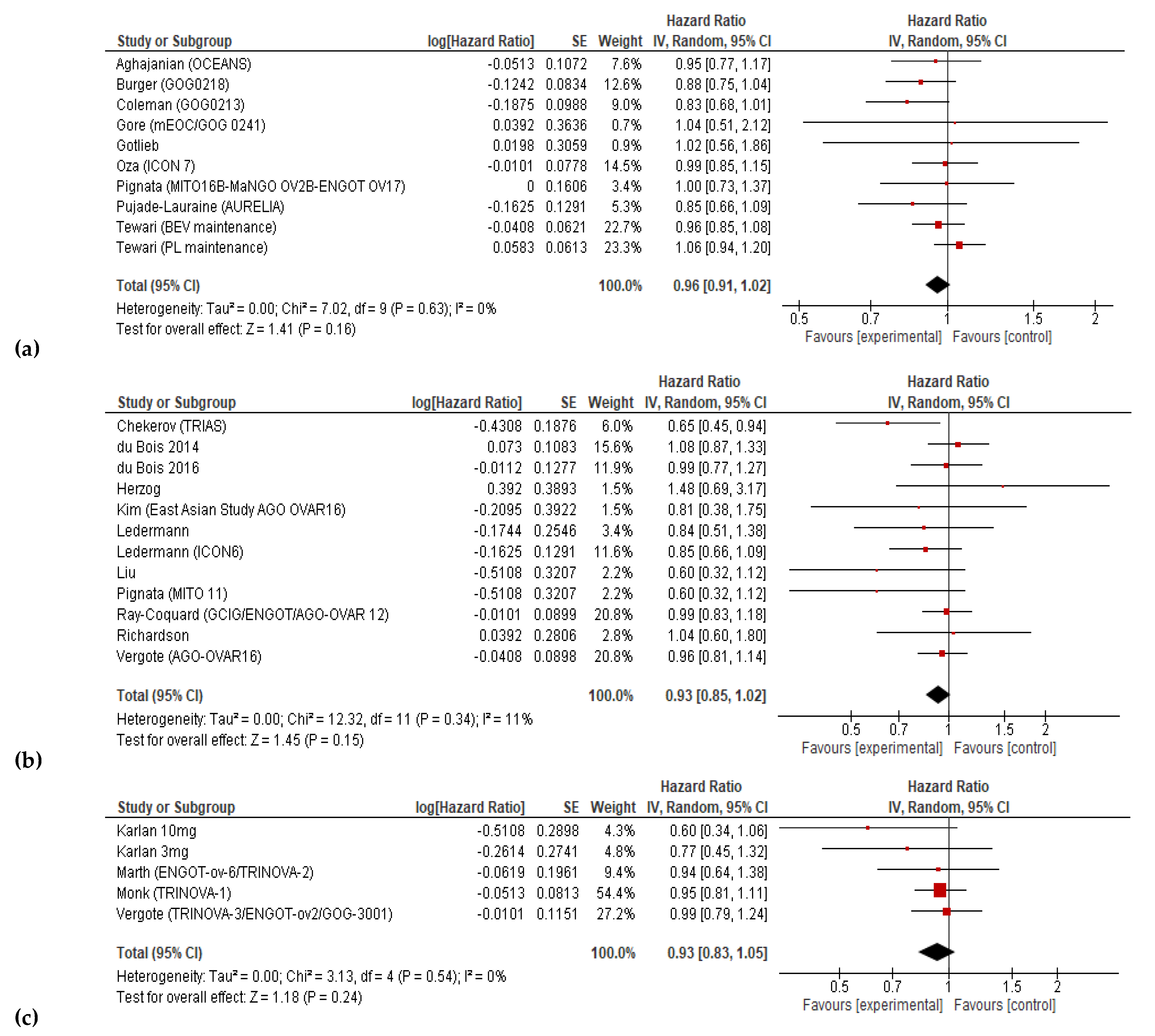
Figure 7.
Grade≥3 adverse effects associated with antiangiogenetic therapy.
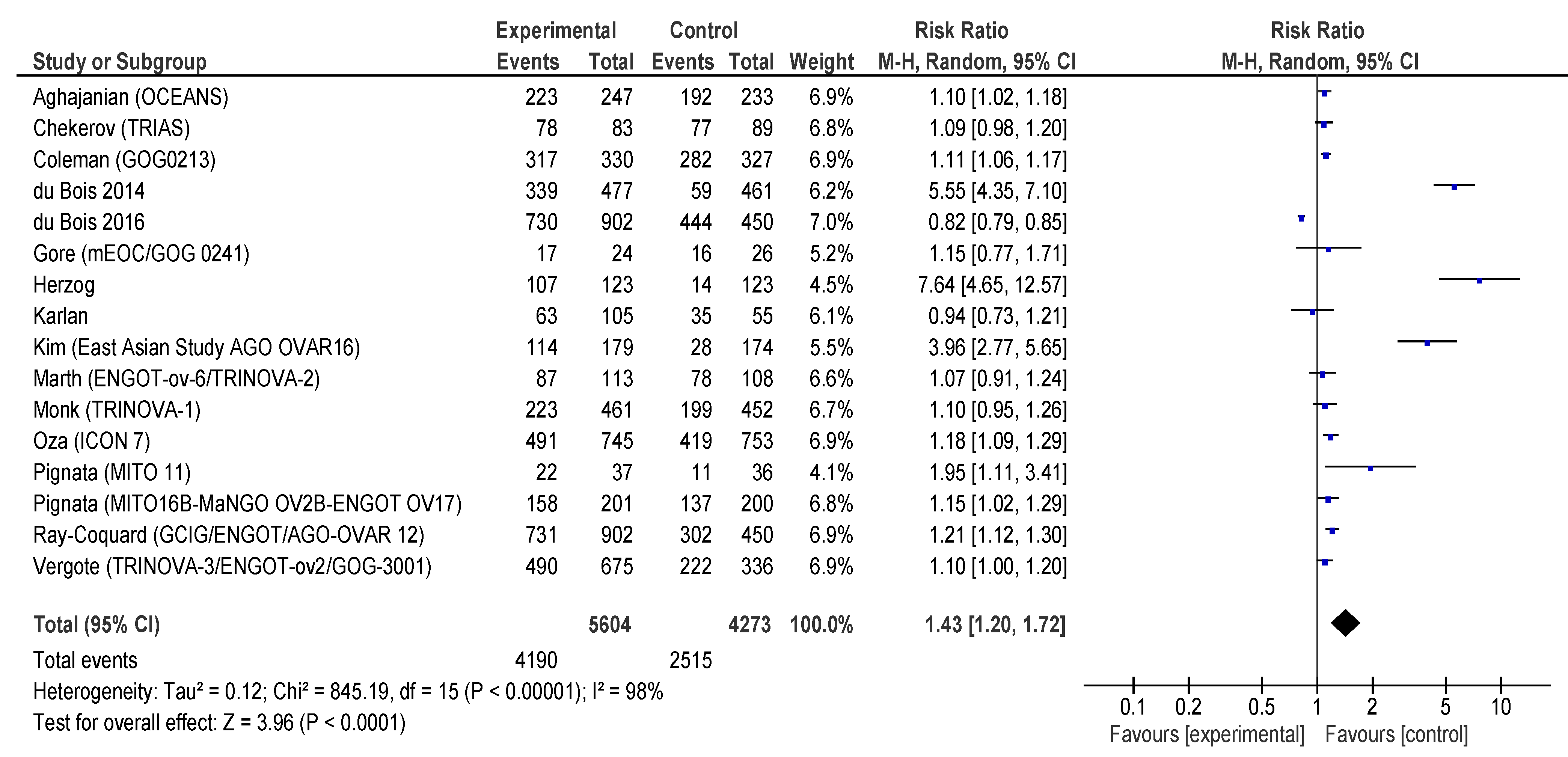

Table 1.
PICOS criteria for inclusion of trials.
| Parameter | Inclusion criteria |
|---|---|
| Participants | Adults with confirmed ovarian cancer |
| Intervention | Angiogenesis-inhibitor therapy |
| Comparison | Drug regimens without angiogenesis inhibitors |
| Outcomes | PFS (hazard-ratio [HR] and 95% confidence interval [CI]), OS (HR and 95% CI), adverse effects (toxicity) |
| Study design | Randomized-controlled trials |
Table 2.
General characteristics of included trials.
| Study (Reference/ Name/Phase) |
Drug | Subjects | Sample size (E/C) |
Angiogenesis inhibitors group treatment |
Control group treatment | Outcomes in meta-analysis |
|---|---|---|---|---|---|---|
| Aghajanian (OCEANS) Phase III[29] |
Bevacizumab | P-S R epithelial ovarian, fallopian tube, or primary peritoneal carcinoma ECOG PS 0–1 |
242/242 | Cycles 1–6: Gem (1000 mg/m2, days 1 and 8) + Carbo (AUC 4, day 1) + Bev (15 mg/kg on day 1,6–10 cycles of 21 days) Cycles 10 +: Bev(15 mg/kg) |
Cycles 1–6: Gem(1000mg/m2, days 1and 8) and Carbo (AUC 4, day 1) + PL (15 mg/kg on day 1,6–10 cycles of 21 days) Cycles 10 +:PL (15 mg/kg) |
PFS; OS; Toxicity |
| Burger Phase III [32] |
Bevacizumab | Newly diagnosed, FIGO stage III or IV epithelial ovarian, primary peritoneal or fallopian tube cancer GOG PS 0-2 |
625/623 | Cycles 1-6: Pac (175 mg/m2) +Carbo (AUC 6) +Bev (15 mg/kg),q3w Cycles 7-22:Bev(15 mg/kg), q3w |
Cycles1-6:Pac (175 mg/m2) + Carbo (AUC 6) +PL, q3w Cycles 7-22:PL,q3w |
PFS |
| Chekerov (TRIAS) Phase II[33] |
Sorafenib | P-R R ovarian, peritoneal, or fallopian tube cancers that had progressed during platinum therapy(platinum refractory)or within 6 months of completing primary, secondary, or tertiary platinum containing therapy ECOG PS 0–2 | 85/89 | Cycles 1–6: Top (1–25 mg/m2 on days 1–5) +Sorafenib(400 mg oral Bid on days 6–15, every 21 days) Cycles 6 +: Daily maintenance Sorafenib for up to 1 year |
Cycles 1–6: Top (1–25 mg/m2 on days 1–5) + PL(Bid on days 6–15, every 21 days) Cycles 6 +: Daily maintenance PL for up to1 year |
PFS; OS; Toxicity |
| Coleman (GOG-0213) Phase III[34] |
Bevacizumab | P-S R epithelial ovarian, fallopian tube or primary peritoneal cancer GOG PS 0–2 |
337/337 | Cycles 1–6: Pac(175 mg/m2)-Carbo[AUC 5]) 3-weekly + Bev (15 mg/kg, 3-weekly) Cycles 6 +: Bev (15 mg/kg, 3-weekly) |
Cycles 1–6: Pac-(175 mg/ m2) Carbo [AUC 5]) 3-weekly |
PFS; OS; Toxicity |
| du Bois 2014 Phase III [35] |
Pazopanib | FIGO stage II-IV epithelial ovarian, fallopian tube or primary peritoneal carcinoma who have not progressed after first line chemotherapy ECOG PS 0-1 |
472/468 | Maintenance Pazopanib(800 mg, orally, once daily for 104 weeks(24 months) |
Maintenance PL(800 mg, orally, once daily), for104 weeks (24 months). | PFS |
| du Bois 2016 Phase III [36] |
Nintedanib | Chemotherapy-naive, FIGO stage IIB-IV epithelial ovarian cancer, fallopian tube or primary peritoneal cancer ECOG PS 0-2 | 911/455 | Cycles1-6: Pac (175 mg/m2) +Carbo (AUC5 or6) + Nintedanib (200 mg twice a day, days 2-21), q3w followed by Nintedanib maintenance |
Cycles1-6:Pac (175 mg/m2) + Carbo (AUC5 or 6) +PL (200 mg, twice a day, days 2-21, q3w)followed byPL maintenance |
PFS |
| Gore (GOG-0241) Phase III [37] |
Bevacizumab | FIGO stage II–IV primary mEOC or recurrence after stage I disease | 24/26 | Pac(175 mg/m2) + Carbo(AUC5/6) + Bev (15 mg/kg, 3-weekly maintenance, 12cycles); Oxal(130 mg/m2) + Cape(850 mg/m2,Bid, days 1–14) + Bev(15 mg/kg, 3-weekly maintenance, 12 cycles) |
Pac(175 mg/m2) + Carbo(AUC 5/6); Oxal(130 mg/m2) + Cape(850 mg/m2,Bid, days 1–14) |
PFS; OS; Toxicity |
| Gotlieb (NCT003274444) Phase II[30] |
Aflibercept | Platinum-resistant, and Top resistant and/or PLD-resistant disease; Advanced ovarian cancer patients with recurrent symptomatic malignant ascites ECOG PS 0–2 |
26/29 | Aflibercept (4 mg/kg, every 2 weeks) | PL(4 mg/kg, every2 weeks) | OS; Toxicity |
| Herzog (NCT00791778) Phase II[38] |
Sorafenib | FIGO stage III–IV ovarian epithelial cancer or primary peritoneal cancer who have achieved a response after standard platinum/ taxane containing chemotherapy (first-line therapy)ECOG PS 0–1 |
123/123 | Sorafenib (400 mg orally Bid, every12 h) | PL(400 mg orally Bid, every 12 h) | PFS; OS; Toxicity |
| Karlan (10 mg/kg) (NCT00479817) Phase II[31] |
Trebananib (AMG 386) |
Recurrent epithelial ovarian (FIGO stage II-IV), fallopian tube or primary peritoneal cancer ECOG PS 0-1 | 53/55 |
Pac(80 mg/m2 once weekly, 3 weeks on/1 week off) + AMG 386 (10 mg/kg, every week) |
Pac(80 mg/m2once weekly, 3 weeks on/1 week off) + PL (10 mg/kg, every week) |
PFS; OS; Toxicity |
| Karlan (3 mg/kg) (NCT00479817) Phase II[31] |
Trebananib (AMG 386) |
FIGO stage II to IV recurrent epithelial ovarian, fallopian tube or primary peritoneal cancer ECOG PS 0–1 |
53/55 | Pac(80 mg/m2 once weekly, 3 weeks on/ 1 week off) + AMG 386 (3 mg/kg, once weekly) |
Pac(80 mg/m2once weekly, 3 weeks on/1 week off) + PL(3 mg/kg, once weekly) |
PFS; OS; Toxicity |
| Kim(East Asian Study) Phase III[39] |
Pazopanib | Advanced ovarian, fallopian tube or primary peritoneal carcinoma |
73/72 | Pazopanib 800 mg Qd for up to24 months | PL800 mg Qd for up to 24 months |
PFS; OS |
| Ledermann (NCT00710762) Phase II[40] |
Nintedanib (BIBF 1120) |
Advanced ovarian carcinoma, fallopian tube carcinoma or primary peritoneal cancer of serous type with recurrent disease and who responded to second-, third-,or fourth-line chemotherapy ECOG PS 0–1 |
43/40 | Cycles 1–9: BIBF 1120 (250 mg, Bid, 28-day cycles) |
Cycles 1–9: PL (250 mg, Bid, 28-day cycles) |
PFS; OS; Toxicity |
| Ledermann (ICON6) Phase III[41,42] |
Cediranib | P-S R epithelial ovarian cancer, primary peritoneal carcinomatosis or fallopian tube cancer after first-line platinum-based chemotherapy ECOG PS 0–1 |
164/118 | Platinum-based chemotherapy + Cediranib (20 mg, Qd) then maintenance Cediranib (20 mg, Qd) alone |
Platinum-based chemotherapy + PL(20 mg, Qd) then maintenance PL(20 mg, Qd)alone |
PFS; OS; Toxicity |
| Liu (NCT01116648) Phase II[43] |
Cediranib | P-S R ovarian cancer of high-grade serous or endometrioid histology or had a deleterious germline BRCA1/2mutation | 46/44 | Olaparib(200 mg, Bid) + Cediranib(30 mg daily) |
Olaparib(400 mg, Bid) | PFS; OS; Toxicity |
| Marth (TRINOVA-2) Phase III[44] |
Trebananib (AMG 386) |
P-R R epithelial ovarian, peritoneal or fallopian tube cancer ECOG PS 0–2 | 114/109 | PLD(50 mg/m2, every 4 weeks) + Trebananib (15 mg/kg, every week) |
PLD(50 mg/m2, every4 weeks) + PL(15 mg/kg, every week) |
PFS; OS; Toxicity |
| Monk (TRINOVA-1) Phase III[45] |
Trebananib (AMG 386) |
Recurrent partially platinum-sensitive or –resistant epithelial ovarian, primary peritoneal or fallopian tube cancer GOG PS 0–1 | 458/461 |
Pac(80 mg/m2 once weekly,3 weeks on/1 week off) + Trebananib(15 mg/ kg, every week) |
Pac(80 mg/m2 onceweekly,3 weeks on/1 week off) + PL(15 mg/kg, every week) | PFS; OS; Toxicity |
| Oza (ICON7) Phase III[28] |
Bevacizumab | FIGO stage I–IIA newly diagnosed high risk ovarian cancer or more FIGO stage IIB–IV ovarian epithelial, fallopian tube, or primary peritoneal cavity cancer ECOG PS 0-2 | 764/764 | Cycles 1–6: Pac(175 mg/m2) + Carbo AUC 5 or 6) 3-weekly + Bev (7.5 mg/ kg, 3-weekly) Cycles 7–18: Bev (7.5 mg/kg, 3-weekly) |
Cycles 1–6: Pac(175 mg/ m2) + Carbo AUC 5 or 6) 3-weekly |
PFS; OS; Toxicity |
| Pignata (MITO16b) Phase II[46] |
Bevacizumab | FIGO stage IIIB-IV recurrent ovarian cancer patients relapsing at least 6 months after last dose of platinum, who had received Bev during first line treatment ECOG PS 0–2 | 203/203 | Cycles 1–6: platinum-based doublets Pac-Carbo/Carbo-Gem/Carbo-PLD + Bev m |
Cycles1–6: Platinum-based doublets Pac-Carbo/ Carbo-Gem/Carbo-PLD |
PFS; OS; Toxicity |
| Pignata (MITO11) Phase II [47] |
Pazopanib | Platinum-resistant or refractory ovarian cancer ECOG PS 0–1 |
37/37 | Pac(80 mg/m2 on days 1, 8 and 15 in every 28 days) + Pazopanib 800 mg daily |
Pac(80 mg/m2 on days 1, 8 and 15 every 28 days) |
PFS; OS; Toxicity |
| Pujade-Lauraine (AURELIA) Phase III[48] |
Bevacizumab | P-R R epithelial ovarian, fallopian tube or primary peritoneal cancer ECOG PS 0–2 |
182/179 | Cycles 1-PD: PLD (40 mg/m2,day 1q4w) or Pac (80 mg/m2,days 1, 8, 15, and22, q4w);or Top (4 mg/m2,days 1, 8, 15, q4w or 1.25 mg/m2, days 1-5, q3w);+Bev (10 mg/kg, every2 weeks or 15 mg/kg, every 3 weeks) |
Cycles 1-PD:PLD (40 mg/m2, day 1, q4w);Pac (80 mg/m2 on days 1, 8, 15and 22, q4w);or Top (4 mg/m2,days 1, 8, 15, q4w or1.25 mg/m2,days 1-5, q3w); |
PFS; OS; Toxicity |
| Ray-Coquard. (AGO-OVAR12) Phase III[49] |
Nintedanib (BIBF 1120) |
FIGO stage IIB–IV newly diagnosed advanced epithelial ovarian, fallopian tube or primary peritoneal cancer |
911/455 | Nintedanib (200 mg Bid on days2–21 every 21 days) + Pac(175 mg/m2)-Carbo(AUC 5 or 6day 1, every21 days for six cycles) |
PL(200 mg Bid on days 2–21 every21 days) + Pac (175 mg/m2)-Carbo (AUC 5 or 6) day 1, every 21 days for six cycles) |
PFS; OS; Toxicity |
| Richardson (NCT01468909) Phase II [50] | Pazopanib | Persistent or recurrent epithelial ovarian, fallopian tube, or primary peritoneal carcinoma GOG PS 0–1 |
52/54 | Pac(80 mg/m2 on days 1, 8 and 15 every 28 days) + Pazopanib 800 mg daily |
Pac(80 mg/m2 on days 1, 8 and 15 every 28 days) + PL 800 mg daily |
PFS; OS; Toxicity |
| Tewari (PLm) (GOG-0218) Phase III [51] |
Bevacizumab | Newly diagnosed ovarian, fallopian tube, or primary peritoneal carcinoma | 625/625 | Cycles 1–6: Pac(175 mg/m2) + Carbo(AUC 6) + Bev (15 mg/kg; cycle 2 +) every 21 days Cycles 7–22:PLm every 21 days |
Cycles 1–6: Pac(175 mg/ m2) + Carbo(AUC6) + PL (cycle 2 +)every 21 days Cycles 7–22:PLm every21 days |
PFS; OS; Toxicity |
| Tewari (BEVm) (GOG-0218) Phase III[51] |
Bevacizumab | Newly diagnosed ovarian, fallopian tube, or primary peritoneal carcinoma | 623/625 | Cycles 1–6: Pac(175 mg/m2) + Carbo(AUC 6) + Bev (15 mg/kg; cycle 2 +) every 21 days Cycles 7–22: Bev m (15 mg/kg) every 21 days |
Cycles 1–6: Pac(175 mg/ m2) + Carbo(AUC 6) PL (cycle 2 +)every21 days Cycles 7–22:PL every21 days |
PFS; OS; Toxicity |
| Vergote (AGO-OVAR16) Phase III [52] |
Pazopanib | Newly diagnosed advanced ovarian cancer | 472/468 | Pazopanib 800 mg Qd for up to24 months | PL 800 mg Qd for up to 24 months |
PFS; OS; Toxicity |
| Vergote (TRINOVA-3) Phase III [53] |
Trebananib (AMG 386) |
FIGO stage III–IV epithelial ovarian, primary peritoneal, or fallopian tube cancer ECOG PS 0–1 |
678/337 | Cycles 1–6:Pac(175 mg/m2)- Carbo([AUC 5/6] every3 weeks) + Trebananib (15 mg/kg) Cycles6+:Trebananib for up to 18 additional months |
Cycles 1–6:Pac (175 mg/m2)-Carbo([AUC5/6] every3 weeks) + PL (15 mg/kg) Cycles6+:PL for up to18 additional months |
PFS; OS; Toxicity |
* P-S R – platinum sensitive recurrent; ECOG - Eastern Cooperative Oncology Group; PS – Performance Status; Gem – gemcitabine; Carbo – carboplatin; AUC – area under curve; Bev – Bevacizumab; PL – placebo; PFS – progression free survival; OS – overall survival; FIGO - International Federation of Gynecology and Obstetrics; GOG gynecological oncology group; Pac- paclitaxel; q3w – every 3 weeks; P-R R – Platinum resistant recurrent; Top – topotecan; Bid - twice daily; mEOC – mucinous epithelial ovarian cancer; Oxal – oxaliplatin; Cape – Capecitabine; PLD – pegylated liposomal doxorubicin; Qd - once daily; Bid – twice a day; Bev-m bevacizumab maintenance therapy; PD - progressive disease; q4w – every 4 weeks; PLm – placebo maintenance.
Table 3.
Summary of outcomes of included trials.
| Study | Line | Size | Arms | PFS | OS | ||
|---|---|---|---|---|---|---|---|
| Median (months) | HR (95% CI) | Median (months) | HR (95% CI) | ||||
| Aghajanian |
P-S R | 484 | GC + PL + Bev(m) GC + PL |
12.4 8.4 |
0.484 (0.388–0.605) | 33.6 32.9 |
0.95 (0.77–1.77) |
| Burger | F | 1248 | TC + PL TC + Bev + Bev(m) |
10.3 14.1 |
0.717 (0.625-0.824) | 39.3 39.7 |
0.885 (0.750-1.040) |
| Chekerov |
P-R R | 174 | TOP + sorafenib + sorafenib(m) PL + PL(m) |
6.7 4.4 |
0.60 (0.43–0.83) | 17.1 10.1 |
0.65 (0.45–0.93) |
| Coleman |
P-S R | 674 | GC + PL + Bev(m) TC |
13.8 10.4 |
0.628 (0.534–0.739) | 42.2 37.3 |
0.829 (0.683-1.005) |
| Du Bois 2016 | F | 1366 | TC +nintedanib+nintedanib(m) TC + PL + PL(m) |
17.2 16.6 |
0.84 (0.72-0.98) | 34 32.8 |
0.99 (0.77-1.27) |
| Du Bois 2014 | M | 940 | Pazopanib PL |
17.9 12.3 |
0.77 (0.64-0.91) | NA | 1.08 (0.87-1.33) |
| Gore | F or R | 50 | TC/Oxal-Cape + Bev TC/Oxal-Cape |
18.1 8.8 |
0.80 (0.41–1.57) | 27.7 32.7 |
1.04 (0.51–2.10) |
| Gotlieb | R | 55 | Aflibercept PL |
6.3 w 7.3 w |
NA | 12.9 w 16.0 w |
1.02 (0.56–1.86) |
| Herzog | M | 246 | Sorafenib PL |
12.7 15.7 |
1.09 (0.72–1.63) | NA | 1.48 (0.69–3.23) |
| Karlan (10 mg/kg) |
R | 108 | Pac + trebananib Pac + PL |
7.2 4.6 |
0.76 (0.49–1.18) | 22.5 20.9 |
0.60 (0.34–1.06) |
| Karlan (3 mg/kg) |
R | 108 | Pac + trebananib Pac + PL |
5.7 4.6 |
0.75 (0.48–1.17) | 20.4 20.9 |
0.77 (0.45–1.31) |
| Kim | M | 145 | Pazopanib PL |
18.1 18.1 |
0.984 (0.596–1.626) | NA | 0.811 (0.376-1.751) |
| Ledermann |
P-S R | 282 | TC/GC/Carbo + cediranib +cediranib(m) TC/GC/Carbo + PL +PL(m) |
11.0 8.7 |
0.56 (0.44–0.72) | 27.3 19.9 |
0.85 (0.66–1.10) |
| Ledermann |
M | 83 | Nintedanib PL |
NA | 0.65 (0.41–1.02) | NA | 0.84 (0.51–1.39) |
| Liu | P-S R | 90 | Olaparib + cediranib Olaparib |
16.5 8.2 |
0.5 (0.3–0.83) | 44.2 33.3 |
0.64 (0.36–1.11) |
| Marth | P-S R | 223 | PLD + trebananib PLD + PL |
7.6 7.2 |
0.92 (0.68–1.24) | 19.4 17.0 |
0.94 (0.64–1.39) |
| Monk | R | 919 | Pac + Trebananib Pac + PL |
7.2 5.4 |
0.66 (0.57–0.77) | 19.3 18.3 |
0.95 (0.81–1.11) |
| Oza | F | 1528 | TC + Bev + Bev(m) TC |
19.9 17.5 |
0.93 (0.83–1.05) | 58.0 58.6 |
0.99 (0.85–1.14) |
| Pignata | P-R R | 73 | Pac + pazopanib Pac + PL |
6.35 3.49 |
0.42 (0.25–0.69) | 19.1 13.7 |
0.60 (0.32–1.13) |
| Pignata | P-S R | 406 | TC/GC/Carbo-PLD + Bev TC/GC/Carbo-PLD |
11.8 8.8 |
0.51 (0.41–0.64) | 26.7 27.1 |
1.00 (0.73–1.39) |
| Pujade-Lauraine |
P-R R | 361 | PLD/Pac/TOP + Bev PLD/Pac/TOP |
6.7 3.4 |
0.48 (0.38–0.60) | 16.6 13.3 |
0.85 (0.66–1.08) |
| Ray-Coquard |
F | 1366 | TC + nintedanib TC + PL |
17.6 16.6 |
0.86 (0.75–0.98) | 62.0 62.8 |
0.99 (0.83–1.17) |
| Richardson |
R | 106 | Pac + pazopanib Pac + PL |
7.5 6.2 |
0.84 (0.57–1.22) | 20.7 23.3 |
1.04 (0.60–1.79) |
| Tewari (PLm) | F | 1250 | TC + Bev + PL(m) TC + PL |
11.2 10.3 |
0.908 (0.795–1.040) | 40.8 41.1 |
1.06 (0.94–1.20) |
| Tewari (BEV-m) | F | 1248 | TC + Bev + Bev(m) TC + PL |
14.1 10.3 |
0.717 (0.625–0.824) | 43.4 41.1 |
0.96 (0.85–1.09) |
| Vergote |
F | 940 | Pazopanib PL |
17.9 12.3 |
0.77 (0.64–0.91) | 59.1 64.0 |
0.96 (0.805–1.145) |
| Vergote |
F | 1015 | TC + trebananib + trebananib(m) TC + PL + PL(m) |
15.9 15.0 |
0.93 (0.79–1.09) | 46.6 43.6 |
0.99 (0.79–1.25) |
F first line, R recurrent, P-R R platinum-resistant recurrent, P-S R platinum-sensitive recurrent, TC paclitaxel + carboplatin, Oxal oxaliplatin, Cape capecitabine, Bev bevacizumab, m maintenance therapy, PL placebo, GC Gemcitabine + Carboplatin, Carbo carboplatin, PLD pegylated liposomal doxorubicin, Pac paclitaxel, TOP topotecan, w weeks, NA not available M pure maintenance.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



