
Submitted:
04 February 2023
Posted:
06 February 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Cardiac complications of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection have been well-identified since the beginning of the current coronavirus disease 2019 (COVID-19) pandemic. Such conditions can occur of various etiologies, such as respiratory failure and hypoxemia, direct cardiac tissue damage due to viral replication, indirect myocarditis as systemic inflammation, and the interaction of different medications. Recently, with the start of the COVID-19 vaccination programs, COVID-19 vaccine-associated cardiac adverse events (AEs) have emerged and are increasingly being reported. Although these AEs are usually mild and self-limited, they can sometimes cause severe, catastrophic outcomes. This review compares the pathophysiology, diagnosis, and treatment of the de novo SARS-CoV-2 infection-related and COVID-19 vaccine-related myocarditis and pericarditis.
Keywords:
SARS-CoV-2
; COVID-19
; Vaccines
; Myocarditis
; Pericarditis
1. Introduction
Early studies on coronavirus disease 2019 (COVID-19) caused by SARS-CoV-2 infection reported cardiac involvement in nearly 30% of the patients [1]. Later studies have shown that the rate of cardiac involvement in COVID-19 patients is higher than previously thought. A multinational study on unselected COVID-19 patients demonstrated that 55% had an abnormality in echocardiographic examination [2]. Another study showed that 78% of unselected COVID-19 patients had cardiac involvement in cardiac magnetic resonance imaging (CMR) [3]. Some studies have also investigated the incidence of cardiac manifestations in COVID-19 patients. It was shown that heart failure, myocardial injury, and arrhythmia were the most common cardiac complications of COVID-19 patients [4]. Another study on COVID-19 patients reported that myocardial injury, arrhythmia, heart failure, and acute coronary syndrome are, respectively most common cardiac complications, and myocardial injury and heart failure are the most frequent cardiovascular complications in non-survivors and are significantly higher in non-survivors than survivors [5].
Cardiac injury can be a result of various etiologies, such as respiratory failure and hypoxemia, direct cardiac tissue damage due to viral replication, indirect myocarditis as of systemic inflammation, and the interaction of medications, of which a well-known example could be the interaction of hydroxychloroquine and azithromycin, both abundantly used at the beginning of the pandemic. Recently, with the start of the anti-severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) vaccination program, vaccine-associated cardiac events have emerged and are increasingly being reported. Here, we discuss de novo SARS-CoV-2 infection-related and vaccine-related cardiac injuries.
2. Myocarditis
2.1. COVID-related myocarditis
Covid-19 manifestations can vary, ranging from asymptomatic to life-threatening conditions. A case series study of 187 patients demonstrated that myocardial injury, indicated by elevated troponin T levels, is significantly associated with disease severity and fatal outcome in COVID-19 patients [6]. Although the risk of myocarditis in patients infected with COVID-19 was 11 times higher than in the general population [7], the prevalence of myocarditis following COVID-19 is rare, and several studies have reported different rates varying from 0.005% to 5% [8,9]. However, it was speculated that the number of cases of myocarditis related to the COVID-19 infection is underestimated due to the lack of enough imaging studies on COVID-19 patients [10] and because almost of myocarditis-associated COVID-19 cases are mild and presented with typical COVID-19 presentation without specific manifestations related to the myocarditis [11].
Recently, SARS-CoV-2 infection has been a leading cause of myocarditis, resulting in growing numbers of acute cardiac injury cases worldwide. The pathophysiologic mechanism of myocarditis in the context of COVID-19 can result from either direct viral invasion of cardiomyocytes or indirect heart tissue damage as a result of cytokine storm, microvascular disease, hypoxia-induced excessive intracellular calcium leading to cardiac myocyte apoptosis, or angiotensin-converting enzyme 2 (ACE2)-mediated loss of protective cardiovascular effects on target organs [12,13], all leading to increased vascular permeability and the resultant myocardial edema (Figure 1 and Figure 2).
Like any other complications, myocarditis can occur alongside or following other typical COVID-19 manifestations [14,15] or may represent the infection’s presenting or sole manifestations without fever, cough, or other respiratory involvements [16,17]. Moreover, it can appear as a Kawasaki-like disease in SARS-CoV-2-infected pediatric patients, known as the multisystem inflammatory syndrome in children (MIS-C). A multisystem inflammatory syndrome is a rare and severe clinical condition linked to COVID-19 that can appear in children (MIS-C) and adults (MIS-A). MIS-C can present with cardiac manifestations and other organ involvements, leading to recurrent hospitalization [18].
Fever and enhancement of the level of inflammatory markers are an example of common features of MIS-C and myocarditis. The similarities between myocarditis and MIS-C induced by COVID-19 proposed the common underlying mechanism. However, some differences were observed between myocarditis and MIS-C. In this regard, myocarditis and MIS-C are developed in two different age groups, whereas MIS-C is present in older children, and myocarditis is related in adult patients. Besides, myocarditis is an acute presentation of COVID-19 that can emerge simultaneously or shortly after the appearance of COVID-19, but MIS-C is a present lately when the IgG test was positive for SARS-CoV-2 [19,20].
Myocarditis related to COVID-19 can present either indolently or sub-clinically such that it is only detected at autopsy or in a fulminant manner with significant life-threatening arrhythmias and hemodynamic instability [21,22]. However, most COVID-19-related myocarditis cases are mild and present with mild non-specific manifestations like chest pain, fatigue, and dyspnea, which is similar between COVID-19 patients with and without myocarditis [23]. Early studies have reported myocarditis only in hospitalized COVID-19 patients, but further studies have shown that myocarditis can be present even in post-covid athletes, whereas myocarditis and CMR abnormality was significantly lower in athletes than non-athletes [24].
Takotsubo (stress) cardiomyopathy (TTC) has been a prevalent cardiac manifestation of various infections, including COVID-19, defined as a regional wall motion abnormality presenting with transient apical ballooning in the setting of emotional or physical stressors, leading to various arrhythmias. Presentations of myocarditis vary from mild symptoms, such as palpitation, fever, chest pain, and weakness, to more severe manifestations, such as cardiogenic shock or significant arrhythmias, leading to sudden cardiac death.
It was demonstrated that tachycardia, dyspnea, shock, and fever are the most frequent clinical manifestations of myocarditis associated with COVID-19 and were estimated to be present in 76%, 74%, 53%, and 37% of patients, respectively [25]. Additionally, although comorbidities do not accompany most myocarditis-associated COVID-19 patients, hypertension (41%) and diabetes (17%) are the most commonly reported comorbidities [25].
Myocarditis is suspected in any patient presenting with compatible symptoms, including acute chest pain, new-onset or worsening at rest or exercise dyspnea, unexplained fatigue, palpitation, arrhythmias, syncope, and cardiogenic shock. It could be confirmed by an electrocardiographic, laboratory, imaging, and histopathologic finding [26,27]. Diagnostic criteria for detecting COVID-19-related myocarditis do not differ from myocarditis of other etiologies. However, a de novo severe SARS-CoV-2 infection can cause chest pain, dyspnea of exertion, or increased NT-proBNP and troponin levels due to supply-demand mismatch, even without actual cardiac damage. Thus, the distinction between these conditions is vital [28,29]. The cardiac damage of myocarditis in COVID-19 patients can be detected by ECG or troponin elevation. It is important to note that the absence of cardiac troponin elevation does not rule out myocarditis, and diagnosis of myocarditis can be confirmed by echocardiography, CMR, cardiac catheterization, and endomyocardial biopsy (EMB), respectively [25]. It is important to note that the American Heart Association (AHA) recommends using at least one imaging modality, like CMR and echocardiography, to confirm the diagnosis of myocarditis-associated COVID-19 [30]. Although CMR provides more high-quality images than echocardiography and is the paramount non-invasive diagnostic tool (31), it has some limitations and makes it unavailable for all COVID-19 patients. However, cardiac CT and ECG can be considered in the absence of CMR and as a suitable alternative to the CMR [23]. Therefore, it can conclude that although CMR imaging is the imaging modality of choice for the diagnosis of myocarditis, primarily when an EMB cannot be performed, and EMB is the decisive diagnostic tool [23], we should choose the safest diagnostic tool firstly in the work-up of covid-related myocarditis. Nevertheless, the diagnosis of some of the reported cases of myocarditis has been based on clinical, laboratory, and electrocardiography findings due to the unavailability of echocardiography and CMR in some institutions.
Positron-emission tomography (PET) scan is another useful imaging modality in diagnosing active inflammatory states, such as myocarditis, via assessing the amount of glucose uptake. It was recognized that PET/CT is associated with some advantages compared to CMR and can provide a quantity of inflammation. Therefore, PET/CT is indicated for intensive observation of disease progression and response to treatment [31]. There was any study that assessed the sensitivity and specificity of PET scan for myocarditis following COVID-19 infection, but previous studies have shown that PET/CT scan has a 74% and 97% sensitivity and specificity, respectively [32]. Eighty-seven percent accuracy was attributed to the PET/CT versus CMR, which revealed that PET/CT is a practical choice when the CMR is unavailable or cannot be performed [32]. Moreover, PET/CT scan is helpful in myocarditis patients when the diagnosis is suspected, and the accuracy of CMR is insufficient.
A clinical study proved that 18F-2-fluoro-2-deoxy-D-glucose PET/CT scan (FDG-PET/CT) might help enhance the specificity and sensitivity of the myocarditis diagnosis and reduce the requirement of EMB, providing supplementary data for classification post-discharge risk. This illuminates that using FDG-PET/CT with or without CMR can significantly increase the accuracy of the diagnosis of myocarditis [33]. Besides, combining CMR and PET/CT scans and using contemporary PET/CT-CMR imaging is associated with complementary value and provides a more accurate diagnostic tool [34] (Figure 3).
Currently, the revised 2018 Lake Louise criteria (LLC) are used for myocarditis confirmation (Table 1) [35,36]. Nonetheless, CMR is not recommended in unstable patients with severe heart failure, cardiogenic shock, or high-grade AV block, and a PET scan can be performed instead, as it takes only seconds rather than hours to scan the patient. Thus, an EMB should be obtained in these patients by taking precautionary measures to avoid getting infected. However, EMB findings cannot differentiate between SARS-CoV-2-associated myocarditis, and other causes since interstitial mononuclear inflammatory infiltrate accompanied by myocyte degeneration and nonischemic necrosis are the prominent findings in the histopathological assessment, rather than evidence of direct myocardial viral invasion [37,38]. Additionally, studies denoted that CMR is central in diagnosing most myocarditis patients, and EMB is conducted in a small proportion of studies [39]. Therefore, despite the need for a positive SARS-CoV-2 reverse transcriptase-polymerase chain reaction (RT-PCR) test result for COVID-19 proof, other virological tests should also be performed to exclude other etiologies since COVID-19 per se is not a cardiotropic virus and other cardiotropic viruses, such as enteroviruses, or parvovirus B19, can cause myocarditis more commonly.
Moreover, the treatment of non-viral myocarditis relies on immunosuppressive therapy. In contrast, no definitive treatment is introduced for myocarditis in the SARS-CoV-2 infection-related cases, and treatment options are variable. Antiviral agents, high-dose corticosteroids, immunosuppressive agents, and intravenous immunoglobulin (IVIG) are recommended treatment options for myocarditis-associated COVID-19, particularly if the patient has the COVID-19 cytokine storm syndrome (COVID-CSS) [40,41]. Although several therapeutic approaches are established for managing myocarditis-associated COVID-19, most cases are resolved spontaneously, and supportive therapy is sufficient [25]. However, corticosteroids are the most frequent drug prescribed for treating myocarditis in COVID-19 patients [42]. It is essential to note that although there is a belief that systemic corticosteroids may lead to diminished viral clearance and increased risk of sepsis in the settings of COVID-19, the benefits of systemic immunosuppression in this setting often outweighs the disadvantages and is considered an effective therapy for myocarditis-related to the COVID-19 [25].
Furthermore, recombinant interleukin-1 receptor antagonists, such as anakinra, have also been used to treat COVID-related myocarditis. It was also demonstrated that IVIG could substantially reduce myocarditis mortality and enhance the left ventricle’s cardiac output [43]. Likewise, the mixed-use of IVIG/corticosteroid successfully treated COVID-19-related myocarditis [44]. Supportive measures, including inotropes, vasopressors, mechanical ventilation, and mechanical hemodynamic support (i.e., intra-arterial balloon pump, temporary left ventricular support devices, and ECMO), should also be considered for severe cases of cardiogenic shock. Nevertheless, supportive and guideline-directed therapies for heart failure are still the mainstay of myocarditis treatment [45,46].
The prognosis of SARS-CoV-2 infection-associated myocarditis is unpredictable since a minority of these patients develop heart failure due to dilated cardiomyopathy (DCM) and systolic dysfunction. Nevertheless, it was estimated that the overall mortality rate was about 14% [25]. Besides, it is essential to note that the mortality rate is higher in COVID-19 patients with myocarditis than in COVID-19 patients without myocarditis [47]. There is the possibility of developing more severe complications, such as cardioembolic stroke following myocarditis, implicating the need to carefully manage any suspected case of COVID-19-associated myocarditis according to current guidelines for heart failure and dysrhythmia.
3. COVID-19 vaccine-associated myocarditis
Several COVID-19 vaccines have been generated worldwide and implanted advantages to the health of communities. However, vaccines are associated with complications and are considered a potential risk factor for several adverse events. Most adverse events following COVID-19 vaccination are minor in severity, including local reactions such as injection site pain and induration, systemic manifestations such as myalgia, fever and chills, and coryza-like symptoms. Although it is rare, cardiac complications of COVID-19 vaccines are not excepted, and it was observed that COVID-19 vaccination could lead to acute myocarditis. Large population studies on individuals who received vaccines documented a rate of 2.13 to 5.34 per 100,000 persons and a 1.8 risk ratio of myocarditis in vaccinated compared to unvaccinated persons.
Moreover, the rate of myocarditis following COVID-19 vaccination in persons younger than 30 years and young males was 12.2 and 10.7 per 100,000, which shows young men are more susceptible than other groups of sex and age [48]. US Vaccine Adverse Event Reporting System (VAERS) stated that from December 2020 to August 2021, 1626 patients experienced myocarditis induced by the COVID-19 vaccine, most of which occurred after the second dose of the vaccine. The median age was 21, with a male predominance in sex and the median interval between vaccination and symptoms initiation was 2 days [49]. However, studies have shown that COVID-19 vaccine-induced myocarditis is mild in 95% and 98.6% of adults and children, respectively and the clinical symptoms were resolved rapidly [50,51].
This unfavorable consequence was previously demonstrated for other vaccines, such as the smallpox vaccine [52,53]. This complication has been reported more commonly in younger males aged between 12 to 30 years who received COVID-19 mRNA vaccines [54,55]. The exact pathophysiology of myocarditis following COVID-19 vaccination is still unknown. However, hypersensitivity reaction, genetic predisposition, sex-specific factors, and molecular mimicry are some potential mechanisms responsible for myocarditis after COVID-19 vaccination [56]. Therefore, evidence supports hyperimmunity as the underlying mechanism, similar to other drugs- and vaccine-associated myocarditis cases. Additionally, it was shown that specific alleles of human leukocyte antigen (HLA) are correlated with unfavorable reactions to some of the medications and vaccines [57,58]. Since a small proportion of individuals who received the COVID-19 vaccine demonstrated myocarditis, it can be assumed that such specific alleles of HLA play a vital role in developing myocarditis following COVID-19 vaccine administration [59].
Up to now, few COVID-19 vaccine-associated cases of cardiac complications, including myocarditis, have been reported. However, most reported cases have occurred following the second dose of the vaccines. Moreover, these vaccine-induced AEs have been reported following mRNA (Moderna or Pfizer/BioNTech) and adenoviral vector (Johnson & Johnson) vaccines [55,60,61,62]. Although the risk of developing myocarditis following COVID-19 vaccination is much lower than infection to SARS-Cov-2, the risk of vaccine-induced myocarditis increases following sequential administration of further vaccine doses [7,63]. Nonetheless, the Centers for Disease Control and Prevention (CDC) guidelines still indicate safety assurance for receiving these COVID-19 vaccines based on benefit-risk assessment in adolescents and young adults. Regarding the immunological basis of such complications, it should be noted that manifestations of vaccine-induced myocarditis can occur as soon as 2 to 3 days after COVID-19 vaccination [64]. It was suggested that a longer interval between doses of vaccines could reduce the risk of myocarditis.
It is vital to note that diagnostic evaluation, preferably CMR, is indicated in any SARS-CoV-2-infected or -vaccinated individual presenting with evidence of myocardial injury with viral or autoimmune etiologies. Physicians and healthcare workers should generally consider myocarditis in vaccinated individuals presenting with severe acute chest pain and abnormal electrocardiogram results. In this condition, cardiac enzymes, electrocardiography (ECG), and echocardiography are mandated, and if indicated, a CMR can also be performed (Figure 3). Notably, a systematic review of the COVID-19 vaccine-induced myocarditis showed that all patients underwent CMR, and CMR finding related to the myocarditis was evident in 89% of patients [65]. One must be careful not to immediately attribute all cardiac events to the vaccine, and other etiologies must be excluded [64]. It is necessary to rule out a de novo SARS-CoV-2 infection, leading to cardiac sequelae. According to the CDC recommendation, a diagnosis of COVID-19 vaccine-induced myocarditis is made by the following criteria: 1) the presence or deterioration of clinical manifestations, 2) confirming the diagnosis by histological examination, CMR, or either by elevation of troponin level exceed to the upper limit, 3) and the absence of any other cause for clinical and para-clinical findings [66].
In conditions where a viral prodrome has been observed, or if a coincident positive SARS-CoV-2 RT-PCR test result is available, the cardiac event is more likely to be attributed to the infection rather than the vaccine. However, the after-vaccine effects can mimic the viral infection’s prodromal symptoms, making it difficult to differentiate between these entities. It should also be noted that a negative serology test (anti-SARS-CoV-2 antibodies) cannot conclusively rule out the possibility of a de novo infection. Again, it should be emphasized that vaccine-related myocarditis is a diagnosis made by exclusion of other possible causes [66], and defining a causal association between myocarditis and vaccination is usually tricky, necessitating thorough evaluation of the patient, e.g., to rule out ischemic injury, autoimmune, and other potential infectious causes of myocarditis. Nonetheless, a useful paraclinical indicator of the potential role of vaccines in triggering myocarditis is an increase in the numbers of a specific subset of natural killer (NK) cells and some autoantibodies [64].
On the other hand, the MRI can sometimes differentiate between vaccine-induced myocarditis and virus-associated MIS-C-related cardiac involvement. For example, late gadolinium enhancement with patchy subepicardial and mid-wall enhancement in the anterior, lateral, and inferior walls, as demonstrated in the revised 2018 Lake Louise criteria, are indicative of the former, while diffuse myocardial edema without evidence of late gadolinium enhancement described by Blondiaux et al. can be suggestive for the latter [67,68].
There is no perspective or clinical trial study on treating the myocarditis-associated COVID-19 vaccine. Regardless of its etiology, NSAIDs, steroids, intravenous immunoglobulin, and colchicine are treatment options for myocarditis. It was shown that NSAIDs, colchicine, and steroids are the most frequent medications used to manage COVID-19 vaccine-induced myocarditis [65]. Regarding COVID-19 vaccine-induced myocarditis in pediatrics, NSAIDs were recommended as a first-line treatment option. Besides, IVIG and corticosteroids are recommended only in severe cases and should be avoided in cases that experienced clinical amelioration 48 hours after initiation of clinical manifestation or prescription of NSAIDs [69]. Additionally, some studies have reported that aspirin, beta-blocker, and ACE inhibitors are also used to treat these patients, and β-blockers and ACE inhibitors should be prescribed in cases with left ventricular systolic dysfunction [64].
3. Pericarditis
4. COVID-19 vaccine-associated myocarditis
Pericarditis may occur following COVID-19 vaccination, both as new-onset pericarditis or a recurrent flare in patients with prior episodes. This phenomenon is rarely associated with other vaccines, except following meningococcal and live vaccines, such as the smallpox vaccine [83,84,85]. On the other hand, recurrent pericarditis had previously been reported after influenza vaccination. This complication occurs most frequently in the setting of underlying auto-inflammatory diseases but can also manifest as a new (previously undiagnosed) autoimmune disorder, such as adult-onset Still’s disease [86,87]. Like virus-induced pericarditis, it usually occurs as myopericarditis but can also occur as an isolated disease [74,88,89].
Moreover, pericarditis has been reported as an adverse event following SARS-CoV-2 vaccination in patients undergoing dialysis. Pericarditis following Pfizer-BioNTech, Moderna, Johnson & Johnson, and AstraZeneca COVID-19 Vaccines has been reported. Like myocarditis, pericarditis associated with COVID-19 vaccination has been most commonly reported following the second vaccine dose, and it has been more commonly reported in adolescents and younger individuals. The mechanism of vaccine-induced pericarditis, like most other vaccine-related complications, seems to be a hyper-immune response. The manifestations, diagnostic approach, and treatment of vaccine-associated pericarditis are the same as the pericarditis resulting from the infection. This, again, emphasizes that other potential causes of pericarditis should be excluded before attributing this condition to the vaccines. So far, outcomes of myopericarditis following COVID-19 vaccination appear to be favorable. Nonetheless, there is a probability of life-threatening arrhythmias, effusive pericarditis, and tamponade associated with a worse prognosis.
4. Conclusions
Clinicians should be aware that cardiac involvement, particularly myocarditis and pericarditis, may manifest in patients, usually occurring 2-4 days after COVID-19 vaccination. This review has emphasized that such rare vaccine-induced adverse events would not change the highly favorable risk-benefit ratio of COVID-19 vaccination, even in patients with underlying heart disease or cardiomyopathy. However, despite limited data, CDC recommends that patients with a history of previous severe adverse events following a COVID-19 vaccine, such as myocarditis/pericarditis after mRNA vaccines or thrombosis with thrombocytopenia syndrome (TTS) after adenoviral vector vaccines, may defer receiving a subsequent dose. Finally, additional surveillance of such adverse events after COVID-19 vaccination will help identify specific patients at increased risk of developing such catastrophic events and, if so, whether additional precautions are necessary.
Author Contributions
Z.M.A.: Data collection and writing the manuscript. J.J.L.: Writing the manuscript and contributed substantial revisions to the manuscript’s content. M.A.H.: Writing the manuscript and contributed substantial revisions to the manuscript’s content. M.A.T.M.: Writing the manuscript and contributed substantial revisions to the manuscript’s content. A.B.: Data collection and writing the manuscript. E.R.: Data collection and writing the manuscript. R.H.: Illustration and writing the manuscript. EH: Data collection and writing the manuscript. T.T.S.: Contributed substantial revisions to the manuscript’s content. A.A.: Data collection and writing the manuscript. M.B.: Data collection, helped with manuscript writing, and contributed substantial revisions to the manuscript’s content. S.E: Design of the research study, helped with manuscript writing, and supervision.
Data Availability Statement
Data sharing is not applicable to this article as no new data were created or analyzed in this study.
Acknowledgments
The authors would like to thank the clinical research development center of Imam Reza Hospital, Kermanshah University of Medical Sciences, for their kind support. All figures are Created with BioRender.com.
Conflict of Interest Disclosure
Terence T. Sio reports that he provides strategic and scientific recommendations as a member of the Advisory Board and speaker for Novocure, Inc. and also as a member of the Advisory Board to Galera Therapeutics, which are not in any way associated with the content or disease site as presented in this manuscript. All other authors have no relevant financial interests to be declared.
References
- Guo, T.; Fan, Y.; Chen, M.; Wu, X.; Zhang, L.; He, T.; Wang, H.; Wan, J.; Wang, X.; Lu, Z. Cardiovascular Implications of Fatal Outcomes of Patients With Coronavirus Disease 2019 (COVID-19). JAMA Cardiol 2020, 5, 811–818. [Google Scholar] [CrossRef] [PubMed]
- Dweck, M.R.; Bularga, A.; Hahn, R.T.; Bing, R.; Lee, K.K.; Chapman, A.R.; White, A.; Salvo, G.D.; Sade, L.E.; Pearce, K. Global evaluation of echocardiography in patients with COVID-19. European Heart Journal-Cardiovascular Imaging 2020, 21, 949–958. [Google Scholar] [CrossRef] [PubMed]
- Puntmann, V.O.; Carerj, M.L.; Wieters, I.; Fahim, M.; Arendt, C.; Hoffmann, J.; Shchendrygina, A.; Escher, F.; Vasa-Nicotera, M.; Zeiher, A.M.; et al. Outcomes of Cardiovascular Magnetic Resonance Imaging in Patients Recently Recovered From Coronavirus Disease 2019 (COVID-19). JAMA Cardiology 2020, 5, 1265–1273. [Google Scholar] [CrossRef] [PubMed]
- Sahranavard, M.; Rezayat, A.A.; Bidary, M.Z.; Omranzadeh, A.; Rohani, F.; Farahani, R.H.; Hazrati, E.; Mousavi, S.H.; Ardalan, M.A.; Soleiman-Meigooni, S. Cardiac complications in COVID-19: a systematic review and meta-analysis. Archives of Iranian medicine 2021, 24, 152. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.-H.; Zhao, L.; Yang, X.-C.; Wang, P. Cardiovascular complications of SARS-CoV-2 infection (COVID-19): a systematic review and meta-analysis. Reviews in cardiovascular medicine 2021, 22, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Guo, T.; Fan, Y.; Chen, M.; Wu, X.; Zhang, L.; He, T.; Wang, H.; Wan, J.; Wang, X.; Lu, Z. Cardiovascular Implications of Fatal Outcomes of Patients With Coronavirus Disease 2019 (COVID-19). JAMA Cardiology 2020, 5, 811–818. [Google Scholar] [CrossRef] [PubMed]
- Patone, M.; Mei, X.W.; Handunnetthi, L.; Dixon, S.; Zaccardi, F.; Shankar-Hari, M.; Watkinson, P.; Khunti, K.; Harnden, A.; Coupland, C.A.C.; et al. Risk of Myocarditis After Sequential Doses of COVID-19 Vaccine and SARS-CoV-2 Infection by Age and Sex. Circulation 2022, 146, 743–754. [Google Scholar] [CrossRef]
- Tuvali, O.; Tshori, S.; Derazne, E.; Hannuna, R.R.; Afek, A.; Haberman, D.; Sella, G.; George, J. The Incidence of Myocarditis and Pericarditis in Post COVID-19 Unvaccinated Patients—A Large Population-Based Study. Journal of Clinical Medicine 2022, 11, 2219. [Google Scholar]
- Buckley, B.J.R.; Harrison, S.L.; Fazio-Eynullayeva, E.; Underhill, P.; Lane, D.A.; Lip, G.Y.H. Prevalence and clinical outcomes of myocarditis and pericarditis in 718,365 COVID-19 patients. Eur J Clin Invest 2021, 51, e13679. [Google Scholar] [CrossRef]
- Atri, L.; Morgan, M.; Harrell, S.; AlJaroudi, W.; Berman, A.E. Role of cardiac magnetic resonance imaging in the diagnosis and management of COVID-19 related myocarditis: clinical and imaging considerations. World Journal of Radiology 2021, 13, 283. [Google Scholar] [CrossRef]
- Siripanthong, B.; Nazarian, S.; Muser, D.; Deo, R.; Santangeli, P.; Khanji, M.Y.; Cooper, L.T., Jr.; Chahal, C.A.A. Recognizing COVID-19-related myocarditis: The possible pathophysiology and proposed guideline for diagnosis and management. Heart rhythm 2020, 17, 1463–1471. [Google Scholar] [CrossRef] [PubMed]
- Das, B.B. SARS-CoV-2 Myocarditis in a High School Athlete after COVID-19 and Its Implications for Clearance for Sports. Children (Basel) 2021, 8, 427. [Google Scholar] [CrossRef] [PubMed]
- Cardiology, E.S.o. ESC Guidance for the Diagnosis and Management of CV Disease during the COVID-19 Pandemic; 10 June 2020. [Google Scholar]
- Doyen, D.; Moceri, P.; Ducreux, D.; Dellamonica, J. Myocarditis in a patient with COVID-19: a cause of raised troponin and ECG changes. Lancet 2020, 395, 1516. [Google Scholar] [CrossRef] [PubMed]
- Sardari, A.; Tabarsi, P.; Borhany, H.; Mohiaddin, R.; Houshmand, G. Myocarditis detected after COVID-19 recovery. Eur Heart J Cardiovasc Imaging 2021, 22, 131–132. [Google Scholar] [CrossRef] [PubMed]
- Paul, J.F.; Charles, P.; Richaud, C.; Caussin, C.; Diakov, C. Myocarditis revealing COVID-19 infection in a young patient. Eur Heart J Cardiovasc Imaging 2020, 21, 776. [Google Scholar] [CrossRef] [PubMed]
- Fischer, Q.; Brillat-Savarin, N.; Ducrocq, G.; Ou, P. Case report of an isolated myocarditis due to COVID-19 infection in a paediatric patient. European Heart Journal: Case Reports 2020, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- Most, Z.M.; Hendren, N.; Drazner, M.H.; Perl, T.M. Striking Similarities of Multisystem Inflammatory Syndrome in Children and a Myocarditis-Like Syndrome in Adults. Circulation 2021, 143, 4–6. [Google Scholar] [CrossRef]
- Noval Rivas, M.; Porritt, R.A.; Cheng, M.H.; Bahar, I.; Arditi, M. Multisystem Inflammatory Syndrome in Children and Long COVID: The SARS-CoV-2 Viral Superantigen Hypothesis. Frontiers in Immunology 2022, 13. [Google Scholar] [CrossRef]
- Patel, T.; Kelleman, M.; West, Z.; Peter, A.; Dove, M.; Butto, A.; Oster, M.E. Comparison of Multisystem Inflammatory Syndrome in Children-Related Myocarditis, Classic Viral Myocarditis, and COVID-19 Vaccine-Related Myocarditis in Children. J Am Heart Assoc 2022, 11, e024393. [Google Scholar] [CrossRef]
- Inciardi, R.M.; Lupi, L.; Zaccone, G.; Italia, L.; Raffo, M.; Tomasoni, D.; Cani, D.S.; Cerini, M.; Farina, D.; Gavazzi, E.; et al. Cardiac Involvement in a Patient With Coronavirus Disease 2019 (COVID-19). JAMA Cardiol 2020, 5, 819–824. [Google Scholar] [CrossRef]
- Zeng, J.H.; Liu, Y.X.; Yuan, J.; Wang, F.X.; Wu, W.B.; Li, J.X.; Wang, L.F.; Gao, H.; Wang, Y.; Dong, C.F.; et al. First case of COVID-19 complicated with fulminant myocarditis: a case report and insights. Infection 2020, 48, 773–777. [Google Scholar] [CrossRef] [PubMed]
- Siripanthong, B.; Nazarian, S.; Muser, D.; Deo, R.; Santangeli, P.; Khanji, M.Y.; Cooper Jr, L.T.; Chahal, C.A.A. Recognizing COVID-19–related myocarditis: The possible pathophysiology and proposed guideline for diagnosis and management. Heart rhythm 2020, 17, 1463–1471. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.Y.; Han, K.; Suh, Y.J. Prevalence of abnormal cardiovascular magnetic resonance findings in recovered patients from COVID-19: a systematic review and meta-analysis. Journal of Cardiovascular Magnetic Resonance 2021, 23, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Haussner, W.; DeRosa, A.P.; Haussner, D.; Tran, J.; Torres-Lavoro, J.; Kamler, J.; Shah, K. COVID-19 associated myocarditis: A systematic review. Am J Emerg Med 2022, 51, 150–155. [Google Scholar] [CrossRef]
- Mele, D.; Flamigni, F.; Rapezzi, C.; Ferrari, R. Myocarditis in COVID-19 patients: current problems. Intern Emerg Med 2021, 16, 1123–1129. [Google Scholar] [CrossRef] [PubMed]
- Lagana, N.; Cei, M.; Evangelista, I.; Cerutti, S.; Colombo, A.; Conte, L.; Mormina, E.; Rotiroti, G.; Versace, A.G.; Porta, C.; et al. Suspected myocarditis in patients with COVID-19: A multicenter case series. Medicine (Baltimore) 2021, 100, e24552. [Google Scholar] [CrossRef] [PubMed]
- Rivara, M.B.; Bajwa, E.K.; Januzzi, J.L.; Gong, M.N.; Thompson, B.T.; Christiani, D.C. Prognostic significance of elevated cardiac troponin-T levels in acute respiratory distress syndrome patients. PLoS One 2012, 7, e40515. [Google Scholar] [CrossRef] [PubMed]
- Imazio, M.; Klingel, K.; Kindermann, I.; Brucato, A.; De Rosa, F.G.; Adler, Y.; De Ferrari, G.M. COVID-19 pandemic and troponin: indirect myocardial injury, myocardial inflammation or myocarditis? Heart 2020, 106, 1127–1131. [Google Scholar] [CrossRef] [PubMed]
- Kociol, R.D.; Cooper, L.T.; Fang, J.C.; Moslehi, J.J.; Pang, P.S.; Sabe, M.A.; Shah, R.V.; Sims, D.B.; Thiene, G.; Vardeny, O. Recognition and initial management of fulminant myocarditis: a scientific statement from the American Heart Association. Circulation 2020, 141, e69–e92. [Google Scholar] [CrossRef]
- Adeboye, A.; Alkhatib, D.; Butt, A.; Yedlapati, N.; Garg, N. A Review of the Role of Imaging Modalities in the Evaluation of Viral Myocarditis with a Special Focus on COVID-19-Related Myocarditis. Diagnostics (Basel) 2022, 12, 549. [Google Scholar] [CrossRef]
- Nensa, F.; Kloth, J.; Tezgah, E.; Poeppel, T.D.; Heusch, P.; Goebel, J.; Nassenstein, K.; Schlosser, T. Feasibility of FDG-PET in myocarditis: Comparison to CMR using integrated PET/MRI. Journal of Nuclear Cardiology 2018, 25, 785–794. [Google Scholar] [CrossRef] [PubMed]
- Ozieranski, K.; Tyminska, A.; Kobylecka, M.; Caforio, A.L.P.; Sobic-Saranovic, D.; Ristic, A.D.; Maksimovic, R.; Seferovic, P.M.; Marcolongo, R.; Krolicki, L.; et al. Positron emission tomography in clinically suspected myocarditis - STREAM study design. Int J Cardiol 2021, 332, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Lawal, I.; Sathekge, M. F-18 FDG PET/CT imaging of cardiac and vascular inflammation and infection. British Medical Bulletin 2016, 120, 55–74. [Google Scholar] [CrossRef] [PubMed]
- Luetkens, J.A.; Faron, A.; Isaak, A.; Dabir, D.; Kuetting, D.; Feisst, A.; Schmeel, F.C.; Sprinkart, A.M.; Thomas, D. Comparison of Original and 2018 Lake Louise Criteria for Diagnosis of Acute Myocarditis: Results of a Validation Cohort. Radiol Cardiothorac Imaging 2019, 1, e190010. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, V.M.; Schulz-Menger, J.; Holmvang, G.; Kramer, C.M.; Carbone, I.; Sechtem, U.; Kindermann, I.; Gutberlet, M.; Cooper, L.T.; Liu, P.; et al. Cardiovascular Magnetic Resonance in Nonischemic Myocardial Inflammation: Expert Recommendations. J Am Coll Cardiol 2018, 72, 3158–3176. [Google Scholar] [CrossRef] [PubMed]
- Sala, S.; Peretto, G.; Gramegna, M.; Palmisano, A.; Villatore, A.; Vignale, D.; De Cobelli, F.; Tresoldi, M.; Cappelletti, A.M.; Basso, C. Acute myocarditis presenting as a reverse Tako-Tsubo syndrome in a patient with SARS-CoV-2 respiratory infection. European heart journal 2020, 41, 1861–1862. [Google Scholar] [CrossRef] [PubMed]
- Rose, N.R. Viral myocarditis. Curr Opin Rheumatol 2016, 28, 383–389. [Google Scholar] [CrossRef]
- Italia, L.; Tomasoni, D.; Bisegna, S.; Pancaldi, E.; Stretti, L.; Adamo, M.; Metra, M. COVID-19 and heart failure: from epidemiology during the pandemic to myocardial injury, myocarditis, and heart failure sequelae. Front Cardiovasc Med 2021, 867. [Google Scholar] [CrossRef] [PubMed]
- Shi, S.; Qin, M.; Shen, B.; Cai, Y.; Liu, T.; Yang, F.; Gong, W.; Liu, X.; Liang, J.; Zhao, Q.; et al. Association of Cardiac Injury With Mortality in Hospitalized Patients With COVID-19 in Wuhan, China. JAMA Cardiol 2020, 5, 802–810. [Google Scholar] [CrossRef]
- Russell, C.D.; Millar, J.E.; Baillie, J.K. Clinical evidence does not support corticosteroid treatment for 2019-nCoV lung injury. The Lancet 2020, 395, 473–475. [Google Scholar] [CrossRef]
- Sawalha, K.; Abozenah, M.; Kadado, A.J.; Battisha, A.; Al-Akchar, M.; Salerno, C.; Hernandez-Montfort, J.; Islam, A.M. Systematic Review of COVID-19 Related Myocarditis: Insights on Management and Outcome. Cardiovasc Revasc Med 2021, 23, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Sun, Y.; Su, G.; Li, Y.; Shuai, X. Intravenous immunoglobulin therapy for acute myocarditis in children and adults a meta-analysis. International heart journal 2019, 60, 359–365. [Google Scholar] [CrossRef] [PubMed]
- Hu, H.; Ma, F.; Wei, X.; Fang, Y. Coronavirus fulminant myocarditis treated with glucocorticoid and human immunoglobulin. European heart journal 2021, 42, 206–206. [Google Scholar] [CrossRef] [PubMed]
- Pirzada, A.; Mokhtar, A.T.; Moeller, A.D. COVID-19 and myocarditis: what do we know so far? CJC open 2020, 2, 278–285. [Google Scholar] [CrossRef] [PubMed]
- Agdamag, A.C.C.; Edmiston, J.B.; Charpentier, V.; Chowdhury, M.; Fraser, M.; Maharaj, V.R.; Francis, G.S.; Alexy, T. Update on COVID-19 Myocarditis. Medicina (Kaunas) 2020, 56, 678. [Google Scholar] [CrossRef] [PubMed]
- Buckley, B.J.R.; Harrison, S.L.; Fazio-Eynullayeva, E.; Underhill, P.; Lane, D.A.; Lip, G.Y.H. Prevalence and clinical outcomes of myocarditis and pericarditis in 718,365 COVID-19 patients. European Journal of Clinical Investigation 2021, 51, e13679. [Google Scholar] [CrossRef] [PubMed]
- Mevorach, D.; Anis, E.; Cedar, N.; Bromberg, M.; Haas, E.J.; Nadir, E.; Olsha-Castell, S.; Arad, D.; Hasin, T.; Levi, N. Myocarditis after BNT162b2 mRNA vaccine against Covid-19 in Israel. New England Journal of Medicine 2021, 385, 2140–2149. [Google Scholar] [CrossRef] [PubMed]
- Oster, M.E.; Shay, D.K.; Su, J.R.; Gee, J.; Creech, C.B.; Broder, K.R.; Edwards, K.; Soslow, J.H.; Dendy, J.M.; Schlaudecker, E.; et al. Myocarditis Cases Reported After mRNA-Based COVID-19 Vaccination in the US From December 2020 to August 2021. JAMA 2022, 327, 331–340. [Google Scholar] [CrossRef]
- Truong, D.T.; Dionne, A.; Muniz, J.C.; McHugh, K.E.; Portman, M.A.; Lambert, L.M.; Thacker, D.; Elias, M.D.; Li, J.S.; Toro-Salazar, O.H.; et al. Clinically Suspected Myocarditis Temporally Related to COVID-19 Vaccination in Adolescents and Young Adults: Suspected Myocarditis After COVID-19 Vaccination. Circulation 2022, 145, 345–356. [Google Scholar] [CrossRef]
- Mevorach, D.; Anis, E.; Cedar, N.; Bromberg, M.; Haas, E.J.; Nadir, E.; Olsha-Castell, S.; Arad, D.; Hasin, T.; Levi, N.; et al. Myocarditis after BNT162b2 mRNA Vaccine against Covid-19 in Israel. New England Journal of Medicine 2021, 385, 2140–2149. [Google Scholar] [CrossRef]
- Eckart, R.E.; Love, S.S.; Atwood, J.E.; Arness, M.K.; Cassimatis, D.C.; Campbell, C.L.; Boyd, S.Y.; Murphy, J.G.; Swerdlow, D.L.; Collins, L.C.; et al. Incidence and follow-up of inflammatory cardiac complications after smallpox vaccination. J Am Coll Cardiol 2004, 44, 201–205. [Google Scholar] [CrossRef] [PubMed]
- Dudley, M.Z.; Halsey, N.A.; Omer, S.B.; Orenstein, W.A.; O'Leary, S.T.; Limaye, R.J.; Salmon, D.A. The state of vaccine safety science: systematic reviews of the evidence. Lancet Infect Dis 2020, 20, e80–e89. [Google Scholar] [CrossRef] [PubMed]
- Oster, M.E. Overview of Myocarditis and Pericarditis: ACIP COVID-19 Vaccines Work Group; Centers for Disease Control and Prevention: CDC COVID-19 Vaccine Task Force, June 23 2021. [Google Scholar]
- Mevorach, D.; Anis, E.; Cedar, N.; Bromberg, M.; Haas, E.J.; Nadir, E.; Olsha-Castell, S.; Arad, D.; Hasin, T.; Levi, N.; et al. Myocarditis after BNT162b2 mRNA Vaccine against Covid-19 in Israel. N Engl J Med 2021. [Google Scholar] [CrossRef] [PubMed]
- Heymans, S.; Cooper, L.T. Myocarditis after COVID-19 mRNA vaccination: clinical observations and potential mechanisms. Nature Reviews Cardiology 2022, 19, 75–77. [Google Scholar] [CrossRef]
- Mitchell, L.A.; Tingle, A.J.; MacWilliam, L.; Horne, C.; Keown, P.; Gaur, L.K.; Nepom, G.T. HLA-DR class II associations with rubella vaccine-induced joint manifestations. Journal of Infectious Diseases 1998, 177, 5–12. [Google Scholar] [CrossRef] [PubMed]
- Stasiak, M.; Zawadzka-Starczewska, K.; Lewiński, A. Significance of HLA Haplotypes in Two Patients with Subacute Thyroiditis Triggered by mRNA-Based COVID-19 Vaccine. Vaccines 2022, 10, 280. [Google Scholar] [CrossRef] [PubMed]
- Bolze, A.; Mogensen, T.H.; Zhang, S.-Y.; Abel, L.; Andreakos, E.; Arkin, L.M.; Borghesi, A.; Brodin, P.; Hagin, D.; Novelli, G. Decoding the Human Genetic and Immunological Basis of COVID-19 mRNA Vaccine-Induced Myocarditis. Journal of Clinical Immunology 2022, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Marshall, M.; Ferguson, I.D.; Lewis, P.; Jaggi, P.; Gagliardo, C.; Collins, J.S.; Shaughnessya, R.; Carona, R.; Fuss, C.; Corbin, K.J.E. Symptomatic acute myocarditis in seven adolescents following Pfizer-BioNTech COVID-19 vaccination. Pediatrics 2021, 2. [Google Scholar]
- Rosner, C.M.; Genovese, L.; Tehrani, B.N.; Atkins, M.; Bakhshi, H.; Chaudhri, S.; Damluji, A.A.; de Lemos, J.A.; Desai, S.S.; Emaminia, A.; et al. Myocarditis Temporally Associated With COVID-19 Vaccination. Circulation 2021, 144, 502–505. [Google Scholar] [CrossRef]
- Albert, E.; Aurigemma, G.; Saucedo, J.; Gerson, D.S. Myocarditis following COVID-19 vaccination. Radiol Case Rep 2021, 16, 2142–2145. [Google Scholar] [CrossRef]
- Voleti, N.; Reddy, S.P.; Ssentongo, P. Myocarditis in SARS-CoV-2 infection vs. COVID-19 vaccination: A systematic review and meta-analysis. Front Cardiovasc Med 2022, 9, 951314–951314. [Google Scholar] [CrossRef] [PubMed]
- Bozkurt, B.; Kamat, I.; Hotez, P.J. Myocarditis With COVID-19 mRNA Vaccines. Circulation 2021, 144, 471–484. [Google Scholar] [CrossRef]
- Khan, Z.; Pabani, U.K.; Gul, A.; Muhammad, S.A.; Yousif, Y.; Abumedian, M.; Elmahdi, O.; Gupta, A. COVID-19 Vaccine-Induced Myocarditis: A Systemic Review and Literature Search. Cureus 2022, 14, e27408–e27408. [Google Scholar] [CrossRef] [PubMed]
- Dooling, K.; Marin, M.; Wallace, M.; McClung, N.; Chamberland, M.; Lee, G.M.; Talbot, H.K.; Romero, J.R.; Bell, B.P.; Oliver, S.E. The Advisory Committee on Immunization Practices' Updated Interim Recommendation for Allocation of COVID-19 Vaccine - United States, December 2020. MMWR Morb Mortal Wkly Rep 2021, 69, 1657–1660. [Google Scholar] [CrossRef]
- Blondiaux, E.; Parisot, P.; Redheuil, A.; Tzaroukian, L.; Levy, Y.; Sileo, C.; Schnuriger, A.; Lorrot, M.; Guedj, R.; Ducou le Pointe, H. Cardiac MRI in Children with Multisystem Inflammatory Syndrome Associated with COVID-19. Radiology 2020, 297, E283–E288. [Google Scholar] [CrossRef]
- Kafil, T.S.; Tzemos, N. Myocarditis in 2020: Advancements in Imaging and Clinical Management. JACC Case Rep 2020, 2, 178–179. [Google Scholar] [CrossRef] [PubMed]
- Sandeep, N.; Fairchok, M.P.; Hasbani, K. Myocarditis After COVID‐19 Vaccination in Pediatrics: A Proposed Pathway for Triage and Treatment. Journal of the American Heart Association 2022, 11, e026097. [Google Scholar] [CrossRef] [PubMed]
- Okor, I.; Sleem, A.; Zhang, A.; Kadakia, R.; Bob-Manuel, T.; Krim, S.R. Suspected COVID-19-Induced Myopericarditis. Ochsner J 2021, 21, 181–186. [Google Scholar] [CrossRef]
- Ghosh, S.; Panda, P.; Sharma, Y.P.; Handa, N. COVID-19 presenting as acute pericarditis. BMJ Case Reports 2022, 15, e243768. [Google Scholar] [CrossRef]
- Osman, W.A.M.; Ahmed, A.S.M.; Eljack, M.M.F.; Abbasher Hussien Mohamed Ahmed, K.; S. Haroun, M.; Abdelrahim Abdalla, Y. Acute pericarditis complicated with pericardial effusion as first presentation of COVID-19 in an adult sudanese patient: A case report. Clinical Case Reports 2022, 10, e05570. [Google Scholar] [CrossRef]
- Cairns, L.; Abed El Khaleq, Y.; Storrar, W.; Scheuermann-Freestone, M. COVID-19 myopericarditis with cardiac tamponade in the absence of respiratory symptoms: a case report. Journal of Medical Case Reports 2021, 15, 31. [Google Scholar] [CrossRef] [PubMed]
- Kariyanna, P.T.; Sabih, A.; Sutarjono, B.; Shah, K.; Peláez, A.V.; Lewis, J.; Yu, R.; Grewal, E.S.; Jayarangaiah, A.; Das, S. A Systematic Review of COVID-19 and Pericarditis. Cureus 2022, 14. [Google Scholar] [CrossRef] [PubMed]
- Adler, Y.; Charron, P.; Imazio, M.; Badano, L.; Barón-Esquivias, G.; Bogaert, J.; Brucato, A.; Gueret, P.; Klingel, K.; Lionis, C.; et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases: The Task Force for the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology (ESC)Endorsed by: The European Association for Cardio-Thoracic Surgery (EACTS). European Heart Journal 2015, 36, 2921–2964. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.; Lu, L.; Cao, W.; Li, T. Hypothesis for potential pathogenesis of SARS-CoV-2 infection–a review of immune changes in patients with viral pneumonia. Emerging Microbes & Infections 2020, 9, 727–732. [Google Scholar] [CrossRef] [PubMed]
- Kermani-Alghoraishi, M.; Pouramini, A.; Kafi, F.; Khosravi, A. Coronavirus disease 2019 (COVID-19) and severe pericardial effusion: from pathogenesis to management: a case report based systematic review. Current Problems in Cardiology 2021, 100933. [Google Scholar] [CrossRef] [PubMed]
- Lange, U.; Schumann, C.; Schmidt, K. Current aspects of colchicine therapy--classical indications and new therapeutic uses. European journal of medical research 2001, 6, 150–160. [Google Scholar]
- Molad, Y. Update on colchicine and its mechanism of action. Current rheumatology reports 2002, 4, 252–256. [Google Scholar] [CrossRef] [PubMed]
- Zhao, H.; Huang, S.; Huang, S.; Liu, F.; Shao, W.; Mei, K.; Ma, J.; Jiang, Y.; Wan, J.; Zhu, W.; et al. Prevalence of NSAID use among people with COVID-19 and the association with COVID-19-related outcomes: Systematic review and meta-analysis. British Journal of Clinical Pharmacology 2022, 88, 5113–5127. [Google Scholar] [CrossRef] [PubMed]
- Karadeniz, H.; Yamak, B.A.; Ozger, H.S.; Sezenoz, B.; Tufan, A.; Emmi, G. Anakinra for the Treatment of COVID-19-Associated Pericarditis: A Case Report. Cardiovasc Drugs Ther 2020, 34, 883–885. [Google Scholar] [CrossRef]
- Imazio, M.; Brucato, A.; Lazaros, G.; Andreis, A.; Scarsi, M.; Klein, A.; De Ferrari, G.M.; Adler, Y. Anti-inflammatory therapies for pericardial diseases in the COVID-19 pandemic: safety and potentiality. J Cardiovasc Med (Hagerstown) 2020, 21, 625–629. [Google Scholar] [CrossRef]
- Morgan, J.; Roper, M.H.; Sperling, L.; Schieber, R.A.; Heffelfinger, J.D.; Casey, C.G.; Miller, J.W.; Santibanez, S.; Herwaldt, B.; Hightower, P. Myocarditis, pericarditis, and dilated cardiomyopathy after smallpox vaccination among civilians in the United States, January–October 2003. Clinical infectious diseases 2008, 46, S242–S250. [Google Scholar] [CrossRef] [PubMed]
- Kuntz, J.; Crane, B.; Weinmann, S.; Naleway, A.L.; Vaccine Safety Datalink Investigator, T. Myocarditis and pericarditis are rare following live viral vaccinations in adults. Vaccine 2018, 36, 1524–1527. [Google Scholar] [CrossRef] [PubMed]
- Al-Ebrahim, E.K.; Algazzar, A.; Qutub, M. Reactive Pericarditis post Meningococcal Vaccine: First Case Report in the Literature. International Journal of Cardiovascular Sciences 2020, 34, 330–334. [Google Scholar] [CrossRef]
- Ishay, Y.; Kenig, A.; Tsemach-Toren, T.; Amer, R.; Rubin, L.; Hershkovitz, Y.; Kharouf, F. Autoimmune phenomena following SARS-CoV-2 vaccination. Int Immunopharmacol 2021, 99, 107970. [Google Scholar] [CrossRef] [PubMed]
- Leone, F.; Cerasuolo, P.G.; Bosello, S.L.; Verardi, L.; Fiori, E.; Cocciolillo, F.; Merlino, B.; Zoli, A.; D'Agostino, M.A. Adult-onset Still's disease following COVID-19 vaccination. Lancet Rheumatol 2021. [Google Scholar] [CrossRef] [PubMed]
- Tano, E.; San Martin, S.; Girgis, S.; Martinez-Fernandez, Y.; Sanchez Vegas, C. Perimyocarditis in Adolescents After Pfizer-BioNTech COVID-19 Vaccine. J Pediatric Infect Dis Soc 2021. [Google Scholar] [CrossRef]
- Gargano, J.W.; Wallace, M.; Hadler, S.C.; Langley, G.; Su, J.R.; Oster, M.E.; Broder, K.R.; Gee, J.; Weintraub, E.; Shimabukuro, T. Use of mRNA COVID-19 vaccine after reports of myocarditis among vaccine recipients: update from the Advisory Committee on Immunization Practices—United States, June 2021. Morbidity and Mortality Weekly Report 2021, 70, 977. [Google Scholar] [CrossRef]
Figure 1.
Summary of the possible mechanisms of SARS-CoV-2 infection-related myocarditis. After entering the body, the virus can exert its cardiotoxic effects via several different pathways. It can directly damage the heart after entering via the ACE2 receptors expressed on heart cells, or it can go to the lungs and act on the alveoli through the ACE2 receptors, causing an overgrowth of Ang II compared to Ang 1-7, increasing the risk of ARDS. When the virus spreads through the arteries, it activates platelets, causing DIC and microthrombosis, eventually leading to multiple organ failure. The SARS-CoV-2 virus also activates macrophages and increases cytokines, such as TGF-β, TNF-α, IL-1α/β, IL-6, IL-8, and MCP-1, by triggering diffuse alveolar damage, angiogenesis, endotheliitis, and thrombosis through NK cells, initiating cytokine storm and multi-organ failure, cytopenia, coronary artery involvement hyper-inflammation and increasing CRP, ferritin, LDH, transaminases, D-dimers, and fibrinogen levels. Coronary artery involvement could cause hyperinflation, cardiogenic shock, endocardial ischemia, and myocarditis. Elevated cytokine levels and the ACE2 receptor involvement with the SARS-CoV-2 virus cause ARDS, leading to acute pulmonary hypertension and hypoxia, eventually causing myocarditis. Abbreviations: ACE2, Angiotensin-converting enzyme 2; Ang II, Angiotensin II; Ang 1-7, Angiotensin 1-7; ARDS, Acute respiratory distress syndrome; DIC, disseminated intravascular coagulation; TGF-β, Transforming growth factor β; TNF-α, Tumor necrosis factor α; IL-1α/β, Interleukin 1α/β; IL-8, Interleukin 8; MCP-1, Monocyte chemoattractant protein 1; NK cell, Natural killer cell; CRP, C-reactive protein; LDH, Lactate dehydrogenase.
Figure 1.
Summary of the possible mechanisms of SARS-CoV-2 infection-related myocarditis. After entering the body, the virus can exert its cardiotoxic effects via several different pathways. It can directly damage the heart after entering via the ACE2 receptors expressed on heart cells, or it can go to the lungs and act on the alveoli through the ACE2 receptors, causing an overgrowth of Ang II compared to Ang 1-7, increasing the risk of ARDS. When the virus spreads through the arteries, it activates platelets, causing DIC and microthrombosis, eventually leading to multiple organ failure. The SARS-CoV-2 virus also activates macrophages and increases cytokines, such as TGF-β, TNF-α, IL-1α/β, IL-6, IL-8, and MCP-1, by triggering diffuse alveolar damage, angiogenesis, endotheliitis, and thrombosis through NK cells, initiating cytokine storm and multi-organ failure, cytopenia, coronary artery involvement hyper-inflammation and increasing CRP, ferritin, LDH, transaminases, D-dimers, and fibrinogen levels. Coronary artery involvement could cause hyperinflation, cardiogenic shock, endocardial ischemia, and myocarditis. Elevated cytokine levels and the ACE2 receptor involvement with the SARS-CoV-2 virus cause ARDS, leading to acute pulmonary hypertension and hypoxia, eventually causing myocarditis. Abbreviations: ACE2, Angiotensin-converting enzyme 2; Ang II, Angiotensin II; Ang 1-7, Angiotensin 1-7; ARDS, Acute respiratory distress syndrome; DIC, disseminated intravascular coagulation; TGF-β, Transforming growth factor β; TNF-α, Tumor necrosis factor α; IL-1α/β, Interleukin 1α/β; IL-8, Interleukin 8; MCP-1, Monocyte chemoattractant protein 1; NK cell, Natural killer cell; CRP, C-reactive protein; LDH, Lactate dehydrogenase.
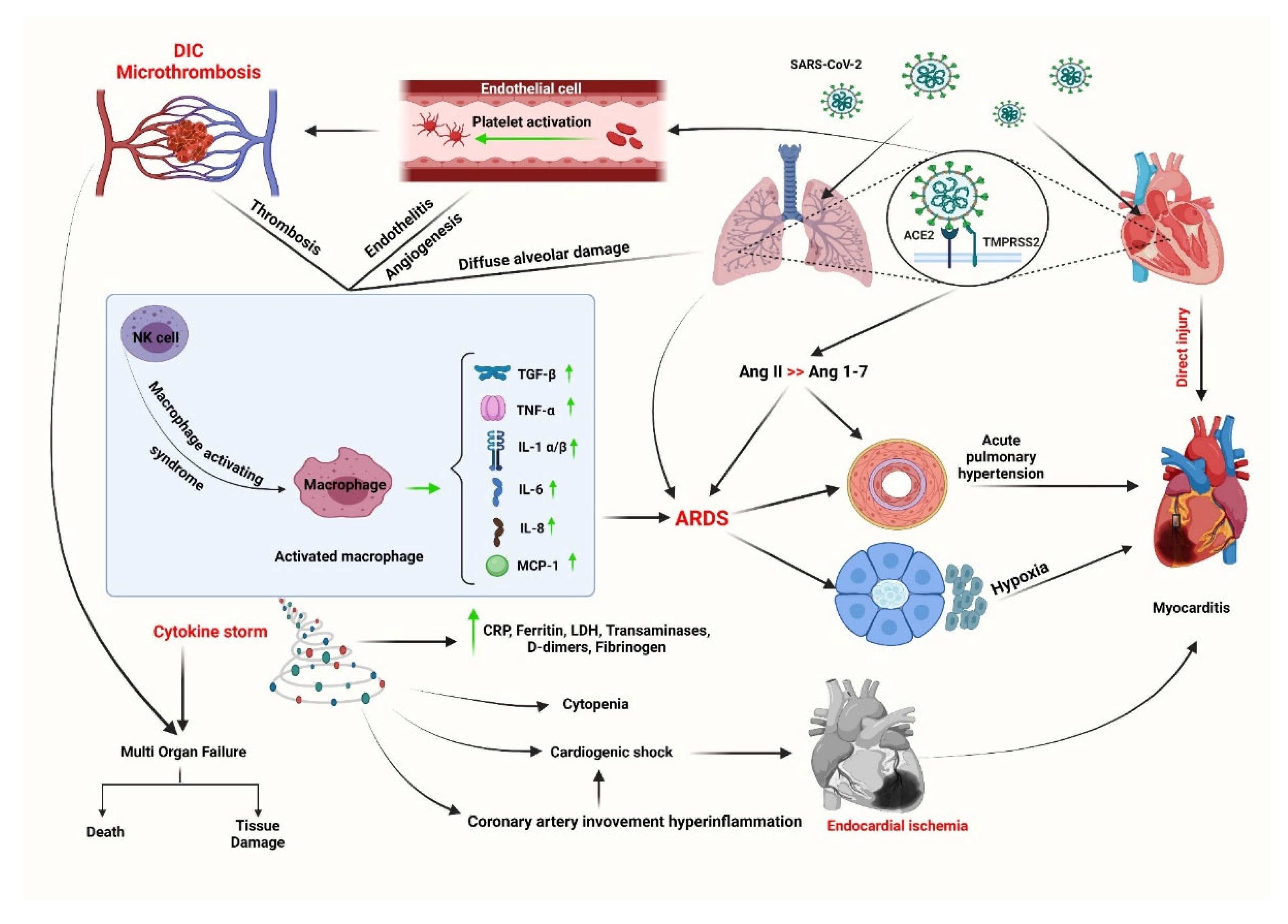
Figure 2.
Effect of SARS-CoV-2 on the renin-angiotensin system (RAS). During the RAS pathways, the enzyme renin actively converts angiotensinogen to Ang I, which produces Ang II under the influence of ACE1. Then, ACE2 breaks down Ang II, a pro-inflammatory agent, to Ang 1-7. Meanwhile, SARS-CoV-2 infection disrupts the balance between Ang II and Ang 1-7 by altering the ACE2 function, resulting in increased levels of Ang II and enhancing the risk of hypertension, cardiac fibrosis, thrombosis, and ARDS. Abbreviations: Ang I, Angiotensin I; Ang II, Angiotensin II; ACE1, Angiotensin-converting enzyme 1; ACE2, Angiotensin-converting enzyme 2; Ang 1-7, Angiotensin 1-7; ARDS, Acute respiratory distress syndrome.
Figure 2.
Effect of SARS-CoV-2 on the renin-angiotensin system (RAS). During the RAS pathways, the enzyme renin actively converts angiotensinogen to Ang I, which produces Ang II under the influence of ACE1. Then, ACE2 breaks down Ang II, a pro-inflammatory agent, to Ang 1-7. Meanwhile, SARS-CoV-2 infection disrupts the balance between Ang II and Ang 1-7 by altering the ACE2 function, resulting in increased levels of Ang II and enhancing the risk of hypertension, cardiac fibrosis, thrombosis, and ARDS. Abbreviations: Ang I, Angiotensin I; Ang II, Angiotensin II; ACE1, Angiotensin-converting enzyme 1; ACE2, Angiotensin-converting enzyme 2; Ang 1-7, Angiotensin 1-7; ARDS, Acute respiratory distress syndrome.
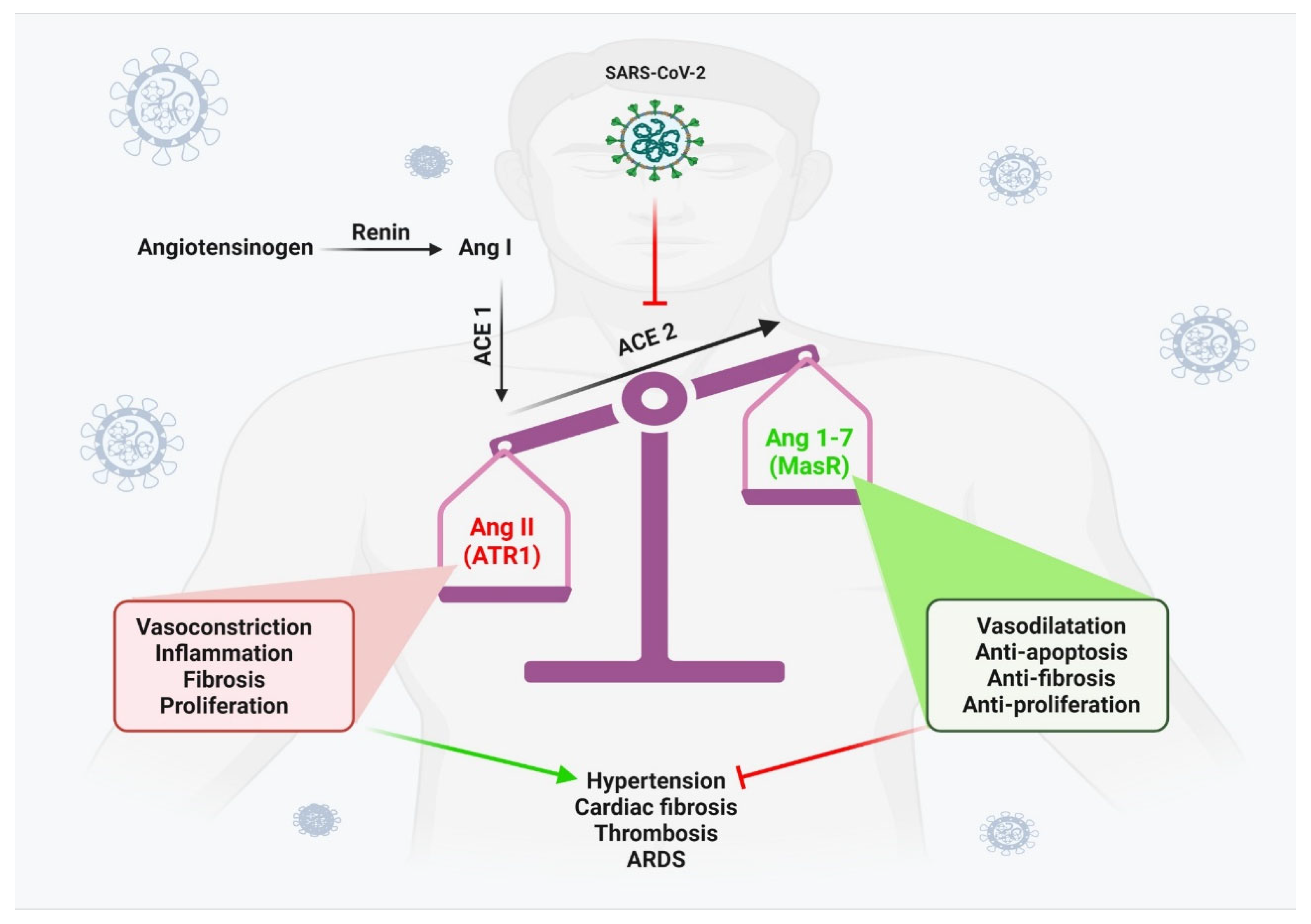
Figure 3.
Myocarditis algorithm. Algorithm for manifestations and diagnosis of myocarditis due to SARS-CoV-2 infection or COVID-19 vaccination. Abbreviations: ECG, electrocardiogram; LVEF, left ventricular ejection fraction; RVEF, right ventricular ejection fraction; CK, Creatine kinase; BNP, B-type natriuretic peptide; NT-proBNP, N-terminal pro–B-type natriuretic peptide; CMR, cardiac magnetic resonance; LGE, late gadolinium enhancement; T2WI, T2-weighted; EGE, early gadolinium enhancement; ECV, extracellular volume fraction; EMB, endomyocardial biopsy; CRP, C-reactive protein; LLC, Lake Louise criteria; LV, left ventricular; RV, right ventricular. Adapted from “Myocarditis in Athletes Is a Challenge: Diagnosis, Risk Stratification, and Uncertainties,” by Eichhorn, C., Bière, L., Schnell, F., Schmied, C., Wilhelm, M., Kwong, R. Y., & Gräni, C., 2020, JACC. Cardiovascular imaging, 13(2 pt 1), p. 494–507. Copyright [2021] by Elsevier. Adapted with permission.
Figure 3.
Myocarditis algorithm. Algorithm for manifestations and diagnosis of myocarditis due to SARS-CoV-2 infection or COVID-19 vaccination. Abbreviations: ECG, electrocardiogram; LVEF, left ventricular ejection fraction; RVEF, right ventricular ejection fraction; CK, Creatine kinase; BNP, B-type natriuretic peptide; NT-proBNP, N-terminal pro–B-type natriuretic peptide; CMR, cardiac magnetic resonance; LGE, late gadolinium enhancement; T2WI, T2-weighted; EGE, early gadolinium enhancement; ECV, extracellular volume fraction; EMB, endomyocardial biopsy; CRP, C-reactive protein; LLC, Lake Louise criteria; LV, left ventricular; RV, right ventricular. Adapted from “Myocarditis in Athletes Is a Challenge: Diagnosis, Risk Stratification, and Uncertainties,” by Eichhorn, C., Bière, L., Schnell, F., Schmied, C., Wilhelm, M., Kwong, R. Y., & Gräni, C., 2020, JACC. Cardiovascular imaging, 13(2 pt 1), p. 494–507. Copyright [2021] by Elsevier. Adapted with permission.
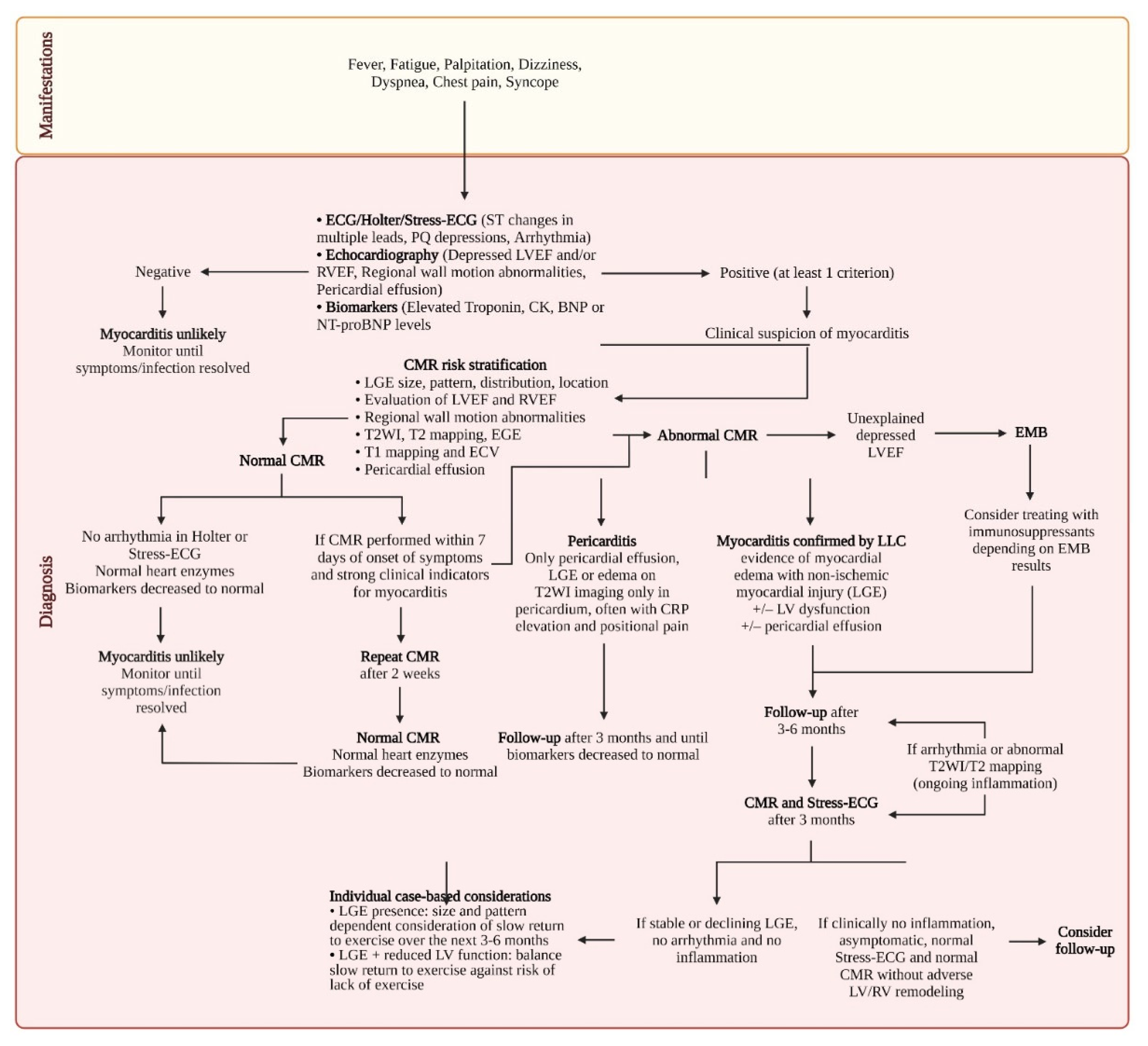

Table 1.
Updated Recommendations of CMR Criteria of Myocardial Inflammation.
| Updated Lake Louise Criteria (2 out of 2) |
Diagnostic Targets |
|---|---|
| Main criteria | |
| T2-based imaging | Myocardial edema |
| Regional* high T2 SI | |
| or | |
| Global T2 SI ratio ≥ 2.0† in T2WI CMR images | |
| or | |
| Regional or global increase in myocardial T2 relaxation time† | |
| T1-based imaging | ↑ T1: Edema (intra-or extracellular), hyperemia/capillary leak, necrosis, fibrosis LGE: Necrosis, fibrosis, (acute extracellular edema) ↑ ECV: Edema (extracellular), hyperemia/capillary leak, necrosis, fibrosis |
| Regional or global increase of native myocardial T1 relaxation time or ECV†, ‡ | |
| or | |
| Areas with high SI in a nonischemic distribution pattern in LGE images | |
| Supportive criteria | |
| Pericardial effusion in cine CMR images | Pericardial inflammation |
| or | |
| High signal intensity of the pericardium in LGE images, T1-mapping or T2-mapping | |
| or | |
| T1 mapping or T2 mapping | |
| Systolic LV wall motion abnormality in cine CMR images | LV dysfunction |
* “Regional” refers to an area of at least 10 contiguous pixels. †Published or local normal values, LV coverage, and proper analysis tools must be acknowledged. ‡T1 mapping is highly sensitive to detecting both acute and chronic forms of increased free water content within the myocardium, and thus, the Consensus Group recommends treating it as an alternative criterion to EGE. If paired with LGE to diagnose myocarditis, the areas of T1 abnormality should be beyond that of LGE imaging. Abbreviations: SI, Signal; T2WI, T2-weighted imaging; CMR, Cardiac magnetic resonance imaging; ECV, Extracellular volume; LGE, Late gadolinium enhancement; LV, Left ventricular. Adapted from “Cardiovascular Magnetic Resonance in Nonischemic Myocardial Inflammation,” by Ferreira, V. M., Schulz-Menger, J., Holmvang, G., Kramer, C. M., Carbone, I., Sechtem, U., Kindermann, I., Gutberlet, M., Cooper, L. T., Liu, P., & Friedrich, M. G., 2018, Journal of the American College of Cardiology, 72(24), p. 3158–3176. Copyright [2021] by Elsevier. Adapted with permission.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



