
Submitted:
06 February 2023
Posted:
08 February 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
The long-term laboratory aspects of the effects of COVID-19 on liver function are still not well understood. Therefore, this study aimed to evaluate the hepatic clinical-laboratory profile of patients with up to 20 months of long-term COVID-19. A total of 243 patients of both sexes aged 18 years or older hospitalised in the acute phase of COVID-19 were included in this study. Liver function analysis was performed. Changes were identified in the mean levels of alanine aminotransferase (ALT), aspartate aminotransferase (AST), lactate dehydrogenase (LDH), gamma-glutamyl transferase (GGT), and ferritin. Inflammatory markers such as ferritin > 300 U/L were observed in the group that presented more changes in liver function markers (ALT, AST, and GGT). Age ≥ 60 years, male sex, AST > 25 U/L, and GGT ≥ 50 or 32 U/L were associated with ALT > 29 U/L. There was a correlation between ALT and AST, LDH, GGT, and ferritin. Our findings suggest that ALT and AST levels may be elevated in patients with long-term COVID, especially in those hospitalised in the acute phase. In addition, ALT > 29 U/L was associated with other markers of liver injury, such as LDH, GGT, and ferritin.
Keywords:
COVID-19
; post COVID
; liver
; aspartate aminotransferase
; risk factors
Introduction
A significant proportion of patients who survived the acute phase of infection of coronavirus disease 2019 reported the continuation or onset of symptoms after 4 or more weeks of the initial infection [1,2]. Such symptoms include fatigue, loss of smell and taste, muscle and joint pain, tachycardia, unexplained drop or increase in pressure, and shortness of breath, among others [3,4,5,6].
Liver damage may be associated with COVID-19 due to direct injury of the viral infection to the liver cells [7], delayed resolution of inflammation, and viral persistence [8]. A preliminary study suggested that angiotensin-converting enzyme 2 (ACE2) expression is enriched in cholangiocytes and that severe acute respiratory syndrome coronavirus 2 can bind directly to ACE-positive cholangiocytes, thereby deregulating liver function [9,10]. Cholangiopathy has been reported in three cases of long-term COVID-19 in hospitalised patients who showed worsening liver markers over the length of hospital stay and developed new cholangiopathy [11]. Patients with long-term COVID demonstrated persistently increased levels of activated CD14+CD16+ monocytes, plasmacytoid dendritic cells, and type I (IFN-β) and III (IFN-λ1) interferon levels compared with that of control individuals 8 months after infection [12].
Some studies have reported changes in serum markers in long-term COVID, including inflammatory (C-reactive protein) and liver markers (alanine aminotransferase [ALT] and aspartate aminotransferase [AST]) [13,14,15,16]. Patients who develop lung lesions (ALT and AST) are associated with worse clinical outcomes, such as liver fibrosis and heart disease [17]. Thus, this study aimed to analysed serum markers of liver damage in patients with up to 20 months of long-term COVID-19.
Results
The study participants were composed of female individuals, non-smokers, with more than 6 months of long-term COVID, who were not hospitalised, and whose average age was approximately 50 years. Fatigue and dyspnoea were symptoms of long-term COVID that affected more than 70% of patients, and the most recurrent comorbidity was arterial hypertension (Table 1).
In patients hospitalised in the acute phase of COVID-19, high mean levels of ALT (P = 0,0182), AST (P = 0,0042), GGT in men (P = 0,0024), and ferritin in both sexes (P = 0,0235; P = 0,0048) were observed. Levels above the reference values were observed for AST (P = 0,0063), LDH (P = 0,0024), and ferritin in males (P = 0,0350). As for the length of time with COVID, the ≤ 6 months group had high mean levels of GGT (P = 0,0013) and ferritin (P = 0,0056) in males. In the ≤ 6 months group, levels above the reference values were observed for GGT (P = 0,0192) and ferritin in males (P = 0,0084), and total bilirubin (P = 0,0370). In the ALT > 29 U/L group, higher mean levels of AST (P < 0,0001), LDH (P = 0,0269), GGT (P = 0,0004 and P < 0,0001), and ferritin were observed in both sexes (P = 0,0239 and P = 0.0148). We observed even higher levels of AST (P < 0,0001) and GGT in males and females (P = 0,0006 and P < 0,0001, respectively) compared with that of the group with ALT levels < 29 U/L (Table 2).
As for the stratification by groups of inflammatory markers (Table 3), we identified high mean levels of ALP (P = 0.0092) and GGT in males (P = 0,0345), in addition to a tendency for ALP >190 µg/L (P = 0,0689). In male patients with ESR > 30 mm/h, we observed a higher occurrence of ALT > 29 U/L (P = 0.0370). For females with ESR > 30 mm/hr, we observed a greater tendency towards high mean levels of total bilirubin (P = 0,0755) and indirect bilirubin (P = 0,0537). For male patients with ferritin > 300 ng/mL, we found elevated mean levels of ALT (P = 0,0104), AST (0,0064), and ALP (P = 0,0164), and higher AST levels > 25 U/L (P = 0,0233). In female patients with ferritin levels > 300 ng/mL, high mean AST level (P = 0,0491) was observed.
Age ≥ 60 years (P = 0,0214), male sex (P = 0,0274), AST > 25 U/L (P < 0,0001), and GGT ≥ 50 or 32 U/L (P = 0,0019) were associated with ALT > 29 U/L. AST level > 25 U/L was associated with ALT level > 29 U/L (P < 0,0001) (Table 4).
Correlation analysis was performed between ALT and AST (P < 0,0001, r = 0.670), LDH (P = 0,0149, r = 0,1560), GGT (P < 0,0001, r = 0,4144), and ferritin (P = 0,0006, r = 0.2180) levels in the general study population (Figure 1). In hospitalised patients, there was a correlation between ALT and AST (P < 0,0001, r = 0,7502), ALP (P = 0,0036, r = 0,3088), and GGT (P < 0,0001, r = 0,4772). The other correlations are shown in Figure 2.
Discussion
In this study, patients with long-term COVID symptoms that lasted up to 20 months were admitted. Alterations were identified in the average levels of ALT, AST, LDH, GGT, and ferritin. The elevation of ferritin, a group of inflammatory markers, was related to the increase in the levels of other liver markers, and ESR was above the reference values in all groups in this study. In addition, we observed that age > 60 years, male sex, and AST and GGT levels above the reference values were more associated with ALT > 29 U/L. The high correlation between ALT and AST levels also suggests a high risk of liver damage.
An et al. [18] also reported elevated levels of ALT, GGT, and ALP 14 days after hospital discharge within 2 months of the initial infection. According to Gameil et al. [19], ALT, AST, GGT, and ALP levels may be elevated 3 months after the resolution of COVID-19. Such altered markers are the result of direct damage caused by the virus to hepatocytes and a systemic inflammatory process already documented in hospitalised patients whose levels of IFN-λ, interleukin (IL)-6, IL-10, and IL-2 are found to be high [20].
Patients with severe COVID-19 have elevated levels of AST, ALT, and GGT [21] and reduced albumin levels [22]. In the findings of our study, the mean albumin levels were within normal limits.
AST has also been used as a liver marker. Because it is produced in the muscle, and patients with long-term COVID have fatigue and muscle weakness as the most frequent symptoms, the elevation of this marker is questionable as to its hepatic origin [23]. However, the correlation and association between ALT and AST identified in our study suggest that true liver injury is the predominant source of aminotransferase elevation.
Bende et al. [17] identified liver stiffness and viscosity in patients with post-COVID-19 syndrome, whose rates were significantly higher in those with lung injury in the acute phase and developed exacerbated clinical manifestations. Liver viscosity appears to be associated with the degree of inflammation and hepatic steatosis [24].
Although ferritin was the only inflammatory marker with differences between the study groups, we observed that the mean ESR values were above the reference values in all groups, which could be explained by a probable residual systemic inflammatory response [19].
In hospitalised patients with COVID-19, liver markers demonstrate a correlation between ALT and AST levels; however, this relationship has not been identified between muscle degradation and inflammatory markers, which suggests that liver damage is directly caused by the presence of the virus in the tissue, whose mechanisms have not yet been fully elucidated [25]. In our study, there was a correlation between markers of muscle degradation (LDH) and inflammation (ferritin).
Alteration of liver markers without concomitant elevation of serum total bilirubin observed in acute and long COVID, as well as the elevated expression of ACE2 in cholangiocytes, suggests a persistent systemic inflammatory response in these patients [26]. ACE2-mediated direct viral invasion of hepatocytes, disrupted immune homeostasis, systemic inflammatory response, concomitant hypotension, pneumonia-associated hypoxia, cytokine storm with increased pro-inflammatory cytokines, and drug use suggest probable pathogenesis of liver injury in long-term COVID [27,28].
An et al. [18] highlighted that patients in serious conditions during acute COVID-19 used more drug therapies, such as oxygen inhalation, antiviral drugs, anti-infective drugs, vasoactive drugs, hormone therapy, immunoregulatory drugs, drugs to regulate the intestinal flora, and symptomatic treatment drugs. Most of these drugs have hepatotoxic effects and may cause liver damage in patients with long-term COVID [29,30].
In addition, reliable control groups are difficult to obtain because of the pandemic that affects many people. On the other hand, this study evaluates possible liver damage in patients with up to 20 months of long COVID, the first study in the literature, mainly in the Amazon Region.
Changes in liver function markers, such as ALT, AST, LDH, GGT, and ferritin, may be present in patients who have developed long-term COVID, especially those hospitalised during acute infection. This may be due to the direct injury caused by the virus to hepatocytes and a persistent systemic inflammatory process. Furthermore, the results of this study suggest that changes in markers of liver injury in patients with long-term COVID may persist for more than 1.5 years after the resolution of COVID-19. Finally, we suggest that new studies be carried out, especially those that allow monitoring the evolution of these patients for a longer time to identify whether such findings are indelible or transient, which represents one of the main gaps in current scientific knowledge.
Materials and Methods
Type of study and ethical aspects
This cross-sectional, quantitative, descriptive, and analytical observational study followed the criteria adopted by Strengthening the Reporting of Observational Studies in Epidemiology (STROBE). This study was approved by the Research Ethics Committee of the State University of Pará (opinion no. 4.252.664/2020), and all patients provided written consent to participate in the study.
Sampling and study population
The study participants were selected for convenience from the Long COVID-19 Program in the Brazilian Eastern Amazon between March 2020 and December 2021. A total of 448 adult patients of both sexes, aged 18 years, diagnosed with COVID-19 by reverse transcriptase polymerase chain reaction (RT-PCR) and who developed long-term COVID-19, were selected. Of these, 134 were excluded owing to incomplete data, non-collection of blood (n = 34), incomplete laboratory analysis (n = 35), and history of previous liver disease (n = 2). Thus, 243 patients were eligible for this study. For data comparison, patients were allocated into groups: i) long duration of COVID, ii) hospitalisation, iii) inflammatory markers, and iv) liver injury markers (Figure 3). The total, direct, and indirect bilirubin and albumin tests were performed in only 94 patients.
Clinical data
Data were collected through interviews and clinical evaluation of the study patients, such as sex, age, main symptoms presented, and presence of comorbidities, among others.
Liver function data
Blood samples were collected for biochemical and haematological analyses. Blood samples were stored in tubes containing clot activator and separator gel, using the serum for biochemical analysis; citrated samples to evaluate the prothrombin time (PT), which was subjected to centrifugation for 10 min at 3,000 RPM; and EDTA samples used in haematological analyses.
For all analyses, only blood serum was used (50 μL), except for the erythrocyte sedimentation rate (ESR), which used whole blood. Biochemical analysis of liver markers was performed using a semi-automatic biochemical analyser CDM 600 (Wiener Lab, Rosario, Argentina).
PT was evaluated using Humaclot Junior equipment (In Vitro Diagnóstica LTDA, Belo Horizonte, Brazil). Blood serum (25 μL of liquid PT) was used for the analysis, enabling visualisation of the test results after 1 min of reaction.
The ESR was determined using graduated pipettes, inserted directly into tubes with anticoagulant, maintained for 1 h, and then readings were taken on the descending scale of the tubes.
The following tests were included because of the following considerations: ALT, AST, LDH tests are considered serum markers of liver injury; bilirubin, alkaline phosphatase (ALP), and GGT, because they are commonly associated with cholestasis; albumin provides information related to liver capacity and synthesis; and PT, ferritin, C-reactive protein (CRP), and ESR because they are altered in inflammatory processes associated with liver damage.
Statistical analysis
The collected data were analysed using GraphPad Prism™ software version 8.4.3 (GraphPad Software, San Diego, USA). Data normality was assessed with the D'Agostino Pearson test using the mean and standard deviation for data description. For comparisons between groups, the Mann–Whitney and chi-square tests were used to compare variables without a normal distribution, while analysis of variance (ANOVA) was used for comparisons with a normal distribution. Multiple logistic regression analysis was used to verify the predictors and associations between different study variables. The linear correlation between hepatic and inflammatory markers was evaluated using Pearson's correlation coefficient. Statistical significance was set at P < 0.05.
Author Contributions
Conceptualization, I.C.L. and L.F.M.F; Methodology, I.C.L. and L.F.M.F; Validation, C.N.C.B., P.F.C.V., J.A.S.Q. and L.F.M.F.; Formal Analysis, I.C.L. and L.F.M.F; Investigation, I.C.L.; Resources, L.F.M.F; Data Curation, I.C.L., D.C.M. and J.H.E.U.; Writing – Original Draft Preparation, I.C.L. and L.F.M.F; Writing – Review & Editing, I.C.L., C.N.C.B., P.F.C.V., J.A.S.Q. and L.F.M.F.; Visualization, I.C.L. and L.F.M.F.; Supervision, C.N.C.B., P.F.C.V., J.A.S.Q. and L.F.M.F.; Project Administration, L.F.M.F.; Funding Acquisition, L.F.M.F. All authors have read and agreed to the published version of the manuscript.
Funding
Amazon Foundation for Research Support [FAPESPA #006/2020], Secretary of science, technology, and higher, professional and technological education [SECTET #09/2021], Higher Education Personnel Improvement Coordination – Brazil CAPES) – Finance Code [Notice n° 13/2020] and National Council for Scientific and Technological Development - Brazil [INCT: 406360/2022-7].
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of the State University of Pará (opinion no. 4.252.664/2020).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author, L.F.M.F. The data are not publicly available due to containing information that could compromise the privacy of research participants.
Acknowledgments
The authors would like to thank the support of Federal University of Pará for this publication through the PROPESP/UFPA (PAPQ - Programa de Apoio a Publicação Qualificada).
Conflicts of Interest
The authors have no conflicts of interest to declare.
References
- Greenhalgh, T.; Knight, M.; A’Court, C.; Buxton, M.; Husain, L. Management of post-acute COVID-19 in primary care. Brit. Med. J. 2020, 370, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72 314 Cases From the Chinese Center for Disease Control and Prevention. JAMA. 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Carfì, A.; Bernabei, R.; Landi, F. Persistent Symptoms in Patients After Acute COVID-19. JAMA. 2020, 324, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Sudre, C.H.; Murray, B.; Varsavsky, T.; Graham, M.S.; Penfold, R.S.; Bowyer, R.C.; Pujol, J.C.; Klaser, K.; Antonelli, M.; Canas, L.S.; Molteni, E.; et al. Attributes and predictors of long COVID. Nat Med. 2021, 27, 626–631. [Google Scholar] [CrossRef] [PubMed]
- Halpin, S.J.; McIvor, C.; Whyatt, G.; Adams, A.; Harvey, O.; McLean, L.; Walshaw, C.; Kemp, S.; Corrado, J.; Singh, R.; et al. Postdischarge symptoms and rehabilitation needs in survivors of COVID-19 infection: A cross-sectional evaluation. J Med Virol. 2021, 93, 1013–1022. [Google Scholar] [CrossRef]
- Kamal, M.; Abo Omirah, M.; Hussein, A.; Saeed, H. Assessment and characterisation of post-COVID-19 manifestations. Int J Clin Pract. 2021, 75. [Google Scholar] [CrossRef] [PubMed]
- Schaefer, E.A.K.; Arvind, A.; Bloom, P.P.; Chung, R.T. Interrelationship Between Coronavirus Infection and Liver Disease. Clin Liver Dis (Hoboken). 2020, 21, 175–180. [Google Scholar] [CrossRef]
- Mehandru, S.; Merad, M. Pathological sequelae of long-haul COVID. Nat Immunol. 2022, 23, 194–202. [Google Scholar] [CrossRef]
- Saviano, A.; Wrensch, F.; Ghany, M.G.; Baumert, T.F. Liver Disease and Coronavirus Disease 2019: From Pathogenesis to Clinical Care. Hepatology 2021, 74, 1088–1100. [Google Scholar] [CrossRef]
- Xu, L.; Liu, J.; Lu, M.; Yang, D.; Zheng, X. Liver injury during highly pathogenic human coronavirus infections. Liver Int. 2020, 40, 998–1004. [Google Scholar] [CrossRef]
- Roth, N. C.; Kim, A.; Vitkovski, T.; Xia, J.; Ramirez, G.; Bernstein, D.; Crawford, J.M. Post-COVID-19 Cholangiopathy: A Novel Entity. Am J Gastroenterol. 2021, 116, 1077–1082. [Google Scholar] [CrossRef]
- Phetsouphanh, C.; Darley, D.R.; Wilson, D.B.; Howe, A.; Munier, C.M.L.; Patel, S.K.; Juno, J.A.; Burrell, L.M.; Kent, S.J.; Dore, G.J.; et al. Immunological dysfunction persists for 8 months following initial mild-to-moderate SARS-CoV-2 infection. Nat Immunol. 2022, 23, 210–216. [Google Scholar] [CrossRef] [PubMed]
- Al-Aly, Z.; Xie, Y.; Bowe, B. High-dimensional characterization of post-acute sequelae of COVID-19. Nature 2021, 594, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Higgins, V.; Sohaei, D.; Diamandis, E.P.; Prassas, I. COVID-19: from an acute to chronic disease? Potential long-term health consequences. Crit Rev Clin Lab Sci. 2021, 58, 297–310. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Leon, S.; Wegman-Ostrosky, T.; Perelman, C.; Sepulveda, R.; Rebolledo, P.A.; Cuapio, A.; Villapol, S. More than 50 long-term effects of COVID-19: a systematic review and meta-analysis. Sci Rep. 2021; 11. [Google Scholar] [CrossRef]
- Mandal, S.; Barnett, J.; Brill, S.E.; Brown, J.S.; Denneny, E.K.; Hare, S.S.; Heightman, M.; Hillman, T.E.; Jacob, J.; Jarvis, H.C.; et al. 'Long-COVID': a cross-sectional study of persisting symptoms, biomarker and imaging abnormalities following hospitalisation for COVID-19. Thorax. 2021, 76, 396–398. [Google Scholar] [CrossRef]
- Bende, F.; Tudoran, C.; Sporea, I.; Fofiu, R.; Bâldea, V.; Cotrău, R.; Popescu, A.; Sirli, R.; Ungureanu, B.S.; Tudoran, M. A Multidisciplinary Approach to Evaluate the Presence of Hepatic and Cardiac Abnormalities in Patients with Post-Acute COVID-19 Syndrome-A Pilot Study. J Clin Med. 2021, 6. [Google Scholar] [CrossRef]
- An, Y.W.; Song, S.; Li, W.X.; Chen, Y.X.; Hu, X.P.; Zhao, J.; Li, Z.W.; Jiang, G.Y.; Wang, C.; Wang, J.C.; et al. Liver function recovery of COVID-19 patients after discharge, a follow-up study. Int J Med Sci. 2021, 18, 176–186. [Google Scholar] [CrossRef]
- Gameil, M.A.; Marzouk, R.E.; Elsebaie, A.H.; Rozaik, S.E. Long-term clinical and biochemical residue after COVID-19 recovery. Egypt Liver J. 2021, 11. [Google Scholar] [CrossRef]
- Patterson, B.K.; Francisco, E.B.; Yogendra, R.; Long, E.; Pise, A.; Rodrigues, H.; Hall, E.; Herrera, M.; Parikh, P.; Guevara-Coto, J.; et al. Persistence of SARS CoV-2 S1 Protein in CD16+ Monocytes in Post-Acute Sequelae of COVID-19 (PASC) up to 15 Months Post-Infection. Front Immunol. 2022, 10, 746021. [Google Scholar] [CrossRef]
- Kumar-M, P.; Mishra, S.; Jha, D.K.; Shukla, J.; Choudhury, A.; Mohindra, R.; Mandavdhare, H.S.; Dutta, U.; Sharma, V. Coronavirus disease (COVID-19) and the liver: a comprehensive systematic review and meta-analysis. Hepatol Int. 2020, 14, 711–722. [Google Scholar] [CrossRef]
- Wu, Y.; Li, H.; Guo, X.; Yoshida, E.M.; Mendez-Sanchez, N.; Levi Sandri, G.B.; Teschke, R.; Romeiro, F.G.; Shukla, A.; Qi, X. Incidence, risk factors, and prognosis of abnormal liver biochemical tests in COVID-19 patients: a systematic review and meta-analysis. Hepatol Int. 2020, 14, 621–637. [Google Scholar] [CrossRef] [PubMed]
- Bloom, P.P.; Meyerowitz, E.A.; Reinus, Z.; Daidone, M.; Gustafson, J.; Kim, A.Y.; Schaefer, E.; Chung, R.T. Liver Biochemistries in Hospitalized Patients With COVID-19. Hepatology 2021, 73, 890–900. [Google Scholar] [CrossRef] [PubMed]
- Sugimoto, K.; Moriyasu, F.; Oshiro, H.; Takeuchi, H.; Yoshimasu, Y.; Kasai, Y.; Furuichi, Y.; Itoi, T. Viscoelasticity Measurement in Rat Livers Using Shear-Wave US Elastography. Ultrasound Med Biol. 2018, 44, 2018–2024. [Google Scholar] [CrossRef] [PubMed]
- Marjot, T.; Webb, G.J.; Barritt, A.S. 4th; Moon, A.M.; Stamataki, Z.; Wong, V.W.; Barnes, E. COVID-19 and liver disease: mechanistic and clinical perspectives. Nat Rev Gastroenterol Hepatol. 2021, 18, 348–364. [Google Scholar] [CrossRef]
- Fan, B.E.; Chong, V.C.L.; Chan, S.S.W.; Lim, G.H.; Lim, K.G.E.; Tan, G.B.; Mucheli, S.S.; Kuperan, P.; Ong, K.H. Hematologic parameters in patients with COVID-19 infection. Am J Hematol. 2020, 95, E131–E134. [Google Scholar] [CrossRef]
- Shi, H.; Han, X.; Jiang, N.; Cao, Y.; Alwalid, O.; Gu, J.; Fan, Y.; Zheng, C. Radiological findings from 81 patients with COVID-19 pneumonia in Wuhan, China: a descriptive study. Lancet Infect Dis. 2020, 20, 425–434. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.; Shi, L.; Wang, Y.; Zhang, J.; Huang, L.; Zhang, C.; Liu, S.; Zhao, P.; Liu, H.; Zhu, L.; et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir Med. 2020, 8, 420–422. [Google Scholar] [CrossRef] [PubMed]
- Boeckmans, J.; Rodrigues, R.M.; Demuyser, T.; Piérard, D.; Vanhaecke, T.; Rogiers, V. COVID-19 and drug-induced liver injury: a problem of plenty or a petty point? Arch Toxicol. 2020, 94, 1367–1369. [Google Scholar] [CrossRef]
- Olry, A.; Meunier, L.; Délire, B.; Larrey, D.; Horsmans, Y.; Le Louët, H. Drug-Induced Liver Injury and COVID-19 Infection: The Rules Remain the Same. Drug Saf. 2020, 43, 615–617. [Google Scholar] [CrossRef]
Figure 1.
Correlation between ALT and markers of liver function in the general study population. Belém/PA, 2020-2021. ALT: Alanine aminotransferase. AST: Aspartate aminotransferase. LDH: Lactic dehydrogenase. ALP: Alkaline phosphatase. GGT: Gamma-glutamyltransferase. (a): correlation between ALT and AST. (b): correlation between ALT and LDH. (c): correlation between ALT and ALP. (d): correlation between ALT and GGT. E: correlation between ALT and Ferritin.
Figure 1.
Correlation between ALT and markers of liver function in the general study population. Belém/PA, 2020-2021. ALT: Alanine aminotransferase. AST: Aspartate aminotransferase. LDH: Lactic dehydrogenase. ALP: Alkaline phosphatase. GGT: Gamma-glutamyltransferase. (a): correlation between ALT and AST. (b): correlation between ALT and LDH. (c): correlation between ALT and ALP. (d): correlation between ALT and GGT. E: correlation between ALT and Ferritin.
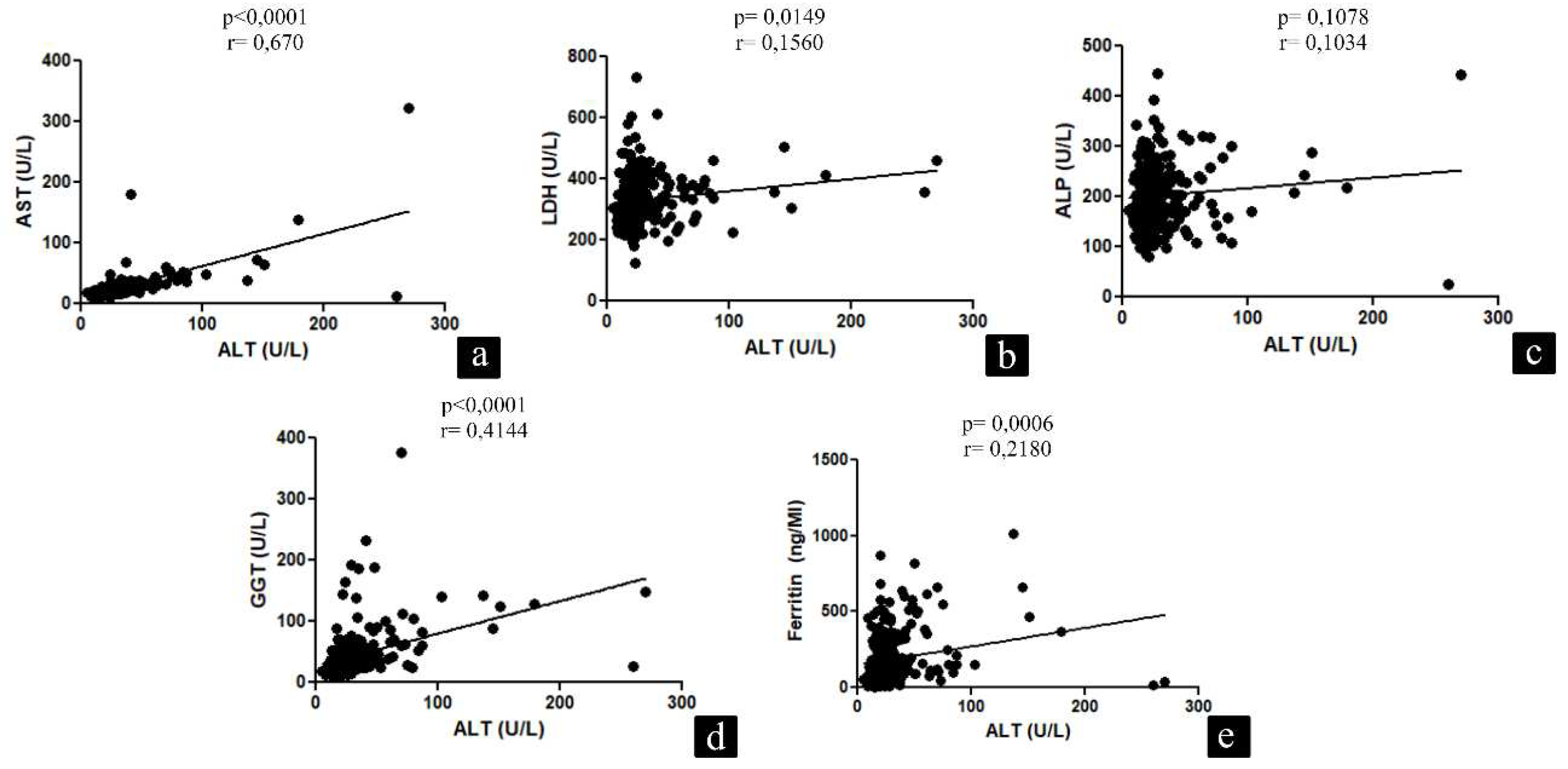
Figure 2.
Correlation between ALT and liver function markers in patients who were hospitalized during acute COVID-19. Belém/PA, 2020-2021. ALT: Alanine aminotransferase. AST: Aspartate aminotransferase. LDH: Lactic dehydrogenase. ALP: Alkaline phosphatase. GGT: Gamma-glutamyltransferase. (a): correlation between ALT and AST. (b): correlation between ALT and LDH. (c): correlation between ALT and ALP. (d): correlation between ALT and GGT. E: correlation between ALT and Ferritin.
Figure 2.
Correlation between ALT and liver function markers in patients who were hospitalized during acute COVID-19. Belém/PA, 2020-2021. ALT: Alanine aminotransferase. AST: Aspartate aminotransferase. LDH: Lactic dehydrogenase. ALP: Alkaline phosphatase. GGT: Gamma-glutamyltransferase. (a): correlation between ALT and AST. (b): correlation between ALT and LDH. (c): correlation between ALT and ALP. (d): correlation between ALT and GGT. E: correlation between ALT and Ferritin.
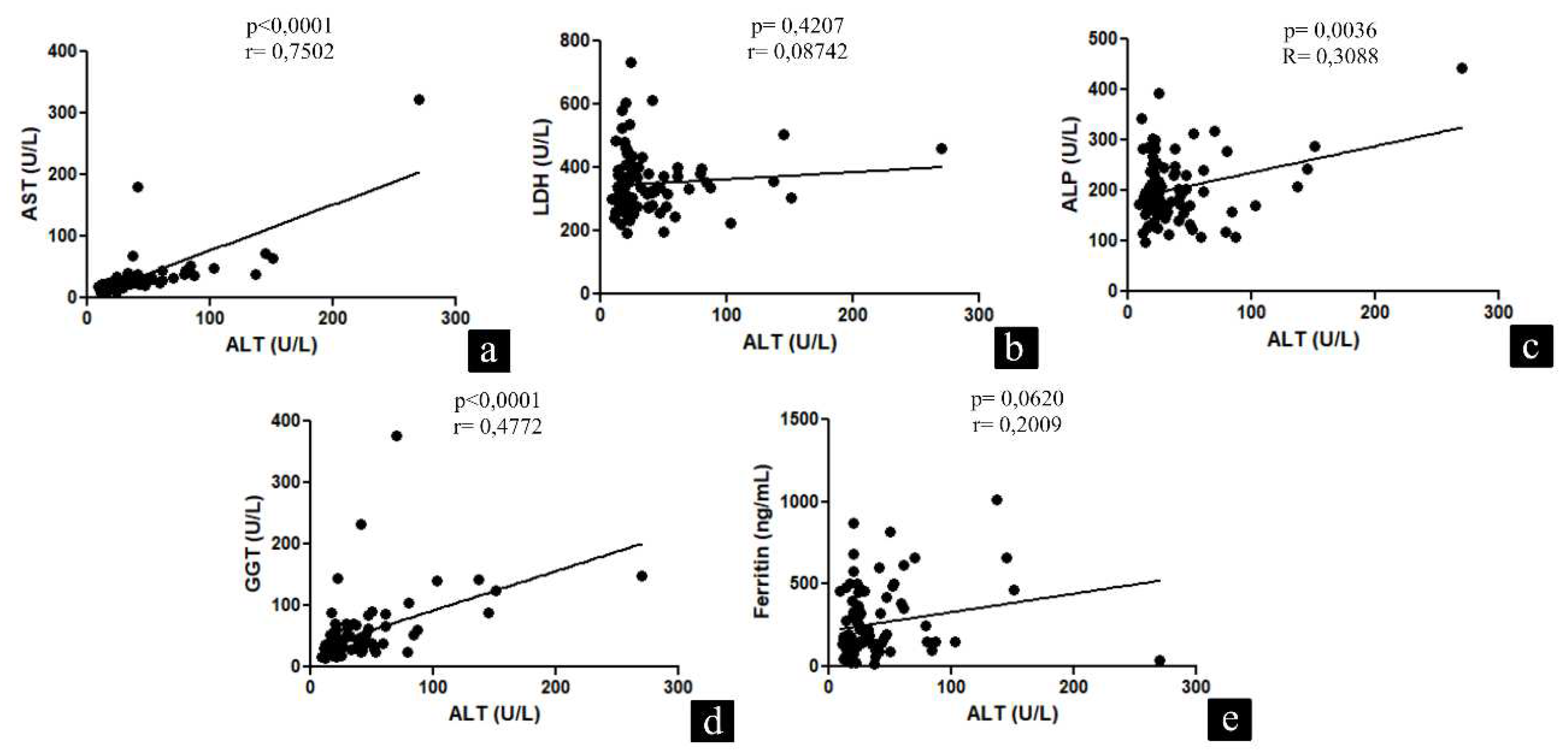
Figure 3.
Study patient recruitment flowchart. Belém/PA, 2020-2021.
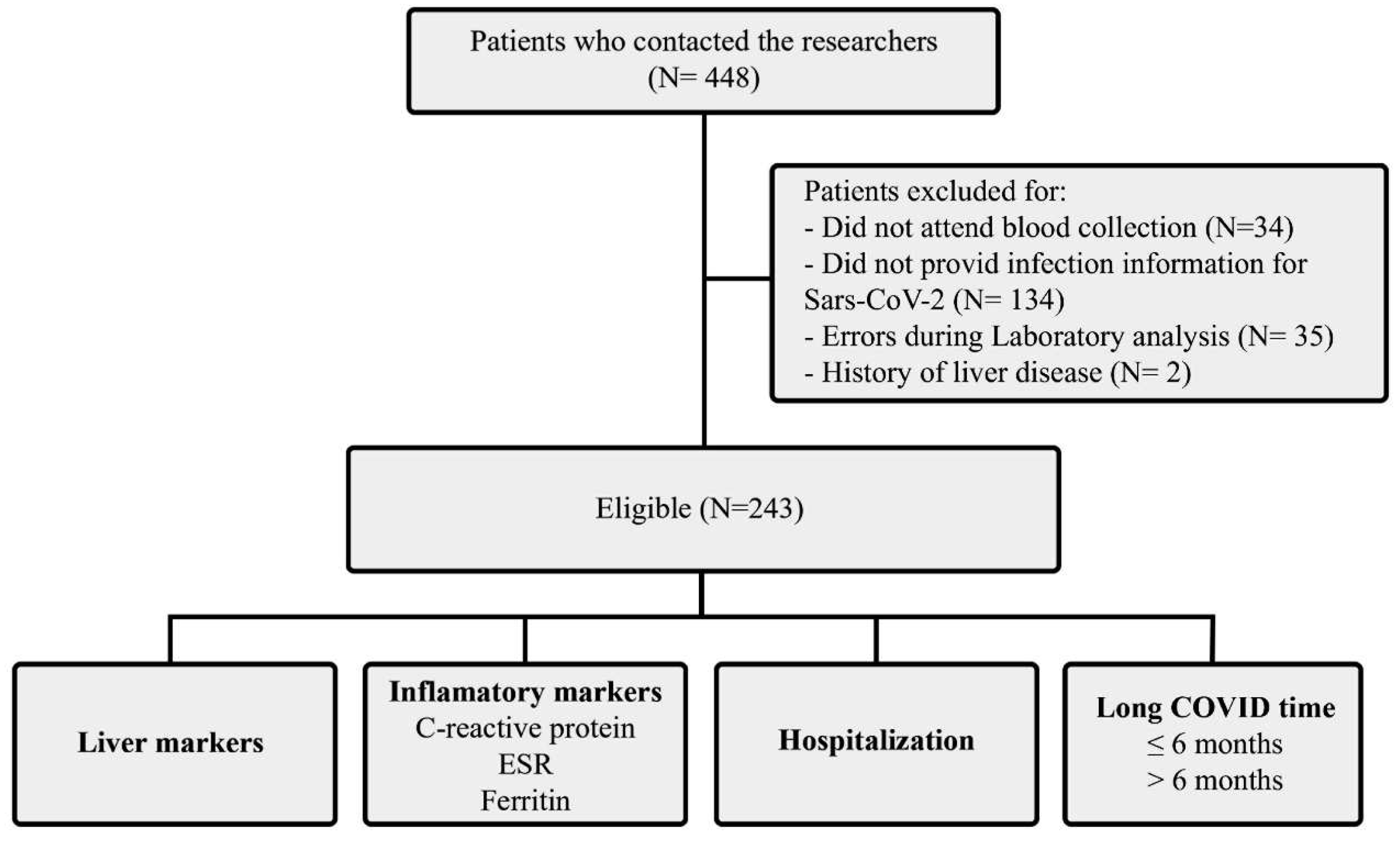

Table 1.
General data of the study patients. Belém/PA, 2020-2021. SD: Standard Deviation. DM: Diabetes Melittus.
Table 1.
General data of the study patients. Belém/PA, 2020-2021. SD: Standard Deviation. DM: Diabetes Melittus.
| Variables | Patients |
|---|---|
| Women, n (%) | 182 (65,46) |
| Age (Mean ± SD, anos) | 49,55 ± 12,72 |
| Smoker/Ex-smoker | 82 (29,49) |
| Long COVID symptoms (n, %) | |
| Fatigue | 206 (74,10) |
| Dyspnoea | 201 (72,30) |
| Muscle weakness | 184 (66,18) |
| Muscle and joint pain | 177 (63,66) |
| loss of balance | 146 (52,51) |
| Insomnia | 135 (48,56) |
| Chest pain | 131 (47,12) |
| Cough | 110 (39,56) |
| Comorbidities (n, %) | |
| Comorbidities | 90 (32,37) |
| Respiratory disease | 42 (15,10) |
| DM | 22 (7,91) |
| Heart disease | 20 (7,19) |
| Kidney disease | 1 (0,35) |
| Hospital internment (n, %) | 101 (36,33) |
| Up to 30 days | 85 (30,57) |
| > 30 days | 16 (5,75) |
| Long COVID time (n, %) | |
| ≤ 6 months | 91 (32,73) |
| > 6 months | 187 (67,26) |
Table 2.
Comparison of liver function laboratory variables between hospitalization groups, post-COVID time, and ALT >29 U/L. Belém/PA, 2020-2021. *Male. **Women. *** Qualitative exam. ALT: Alanine aminotransferase. AST: Aspartate aminotransferase. LDH: Lactic dehydrogenase. TB: Total bilirubin. DB: Direct bilirubin. IB: Indirect bilirubin. ALP: Alkaline phosphatase. GGT: gamma-glutamyl transferase. CRP, C-reactive protein. PT: Prothrombin time. ESR: Erythrocyte sedimentation rate. Data are expressed as mean ± standard deviation (M ± SD) and as absolute and relative frequencies. ANOVA test (p<0.05#) Mann-Whitney test (p<0.05&). Chi-square test (p<0.05), and Fisher’s exact test (p<0.05'').
Table 2.
Comparison of liver function laboratory variables between hospitalization groups, post-COVID time, and ALT >29 U/L. Belém/PA, 2020-2021. *Male. **Women. *** Qualitative exam. ALT: Alanine aminotransferase. AST: Aspartate aminotransferase. LDH: Lactic dehydrogenase. TB: Total bilirubin. DB: Direct bilirubin. IB: Indirect bilirubin. ALP: Alkaline phosphatase. GGT: gamma-glutamyl transferase. CRP, C-reactive protein. PT: Prothrombin time. ESR: Erythrocyte sedimentation rate. Data are expressed as mean ± standard deviation (M ± SD) and as absolute and relative frequencies. ANOVA test (p<0.05#) Mann-Whitney test (p<0.05&). Chi-square test (p<0.05), and Fisher’s exact test (p<0.05'').
| Variables | Hospitalization | Long COVID time | ALT >29 U/L | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Yes | No | P value | ≤6 months | >6 months | P value | Yes | No | P value | |
| ALT, M ± SD | 37,68±37,84 | 27,73±26,42 | 0,0182& | 31,74±26,86 | 31,07±33,31 | 0,5740 | - | - | - |
| ALT >29 U/L, n. (%) | 33 (13,58) | 41 (16,87) | 0,0808 | 25 (10,28) | 49 (20,16) | 0,9674 | - | - | - |
| AST, M ± SD | 30,85±37,55 | 22,79±12,34 | 0,0042& | 23,37±9,79 | 26,80±29,43 | 0,7790 | 39,43 ±41,30 | 19,65±4,76 | < 0,0001& |
| AST >25 U/L, n. (%) | 32 (13,16) | 31 (12,75) | 0,0063’ | 21 (8,64) | 42 (17,28) | 0,9402 | 49 (20,16) | 14 (5,76) | < 0,0001’ |
| LDH, M ± SD | 348,01±97,94 | 322,23±66,78 | 0,1474 | 345,01±92,30 | 324,81±72,79 | 0,0873 | 343,11±70,56 | 326,36±83,64 | 0,0269& |
| LDH >460 U/L, n. (%) | 10 (4,11) | 3 (1,23) | 0,0024’’ | 7 (2,88) | 6 (2,47) | 0,1289 | 3 (1,23) | 10 (4,11) | 0,7594 |
| ALP, M ± SD | 203,10±64,25 | 201,74±62,18 | 0,8535 | 201,81±54,45 | 202,43±66,67 | 0,7035 | 206,32±67,17 | 200,44±60,91 | 0,4821 |
| ALP >190 µg/L, n. (%) | 46 (18,93) | 84 (34,56) | 0,9908 | 47 (19,34) | 83 (34,15) | 0,3110 | 42 (17,28) | 88 (36,21) | 0,5932 |
| GGT*, M ± SD | 60,15±61,14 | 37,07±21,46 | 0,0024& | 64,02±64,78 | 35,68±15,97 | 0,0013& | 69,60±68,45 | 35,04±14,03 | 0,0004& |
| GGT >50 µg/L, n. (%) | 17 (6,99) | 8 (3,29) | 0,1371 | 17 (6,99) | 8 (3,29) | 0,0192 | 18 (7,40) | 7 (2,88) | 0,0006’ |
| GGT**, M ± SD | 44,47±34,94 | 39,09±34,82 | 0,3912 | 37,02±26,60 | 44,30±36,46 | 0,5645 | 64,97±45,70 | 32,56±26,14 | < 0,0001& |
| GGT >32 µg/L, n. (%) | 19 (7,81) | 42 (17,28) | 0,3773 | 16(6,58) | 45 (18,51) | 0,9318 | 26 (10,70) | 35 (14,40) | < 0,0001’ |
| PT, M ± SD | 12,29±1,01 | 12,87±5,63 | 0,2142 | 12,35±1,18 | 12,82±5,50 | 0,4390 | 13,20±8,08 | 12,43±1,17 | 0,3034 |
| PT > 15 segundos, n. (%) | 1 (0,41) | 2 (0,82) | 1,0000 | 2 (0,82) | 1 (0,41) | 0,2528 | 1 (0,41) | 1 (0,41) | 0,2937 |
| Ferritin*, M ± SD | 338,11±229,71 | 226,72±155,61 | 0,0235& | 368,02±238,19 | 208,27±146,69 | 0,0056& | 352,28±236,85 | 239,32±166,66 | 0,0239 |
| Ferritin >300 ng/mL, n. (%) | 24 (9,87) | 11 (4,52) | 0,0350’ | 23 (9,46) | 13 (5,35) | 0,0084’ | 18 (7,40) | 17 (6,99) | 0,1904 |
| Ferritin **, M ± SD | 177,09±154,13 | 119,38±116,52 | 0,0048& | 122,92±110,85 | 175,07±167,44 | 0,2090 | 161,74±133,42 | 125,81±127,60 | 0,0148& |
| Ferritin >300 ng/mL, n. (%) | 6 (2,47) | 11 (4,52) | 0,3907 | 3 (1,23) | 14 (5,76) | 0,5628 | 6 (2,47) | 11 (4,52) | 0,3691 |
| CRP-positiva***, n. (%) | 10 (4,11) | 23 (9,46) | 0,6076 | 9 (3,70) | 24 (9,87) | 0,5867 | 11 (4,52) | 22 (9,05) | 0,8545 |
| ESR*, M ± SD | 35,22±23,63 | 33,10±28,35 | 0,3698 | 33,95±23,81 | 34,31±27,72 | 0,8629 | 30,71±21,07 | 36,75±28,64 | 0,5343 |
| ESR >20 mm, n. (%) | 31 (12,75) | 22 (9,05) | 0,3394 | 26 (10,69) | 27 (11,11) | 0,6856 | 22 (9,05) | 31 (12,75) | 0,8484 |
| ESR**, M ± SD | 41,16±28,33 | 43,93±25,24 | 0,4544 | 51,24±32,88 | 41,72±26,49 | 0,1343 | 48,66±33,94 | 41,42±22,77 | 0,4176 |
| ESR >30 mm, n. (%) | 25 (10,29) | 77 (31,68) | 0,5882 | 27 (11,11) | 75 (30,86) | 0,9403 | 28 (11,52) | 74 (30,45) | 0,3403 |
| TB, M ± SD | 0,46±0,23 | 0,47±0,21 | 0,7087 | 0,48±0,28 | 0,46±0,18 | 0,7587 | 0,47±0,25 | 0,47±0,21 | 0,7099 |
| TB >1.0 mg/dL | 2 (0,82) | 1 (0,41) | 0,5634 | 3 (1,23) | 0 | 0,0370’’ | 1 (0,41) | 2 (0,82) | 0,9756 |
| DB, M ± SD | 0,17±0,05 | 0,17±0,07 | 0,7317 | 0,17±0,07 | 0,17±0,06 | 0,8638 | 0,17±0,07 | 0,17±0,06 | 0,9341 |
| DB >0,2 mg/dL, n. (%) | 1 (0,41) | 7 (2,88) | 0,1369 | 3 (1,23) | 5 (2,05) | 0,9980 | 4 (1,64) | 4 (1,64) | 0,2326 |
| IB, M ± SD | 0,31±0,21 | 0,31±0,18 | 0,5453 | 0,3094±0,23 | 0,3145±0,17 | 0,3736 | 0,30±0,18 | 0,31±0,19 | 0,6345 |
| IB >0,8 mg/dL, n. (%) | 1 (0,41) | 1 (0,41) | 1,0000 | 2 (0,82) | 0 | 0,1135 | 0 | 2 (0,82) | 0,5772 |
| Albumin, M ± SD | 4,09±0,34 | 4,12±0,38 | 0,2321 | 3,9969±0,37 | 4,1677±0,35 | 0,6949 | 4,13±0,34 | 4,10±0,38 | 0,6542 |
| Albumin>4,8 g/dL, n. (%) | 0 | 0 | 1,0000 | 0 | 0 | 1,0000 | 0 | 0 | 1,0000 |
Table 3.
Comparison of laboratory variables of liver function between groups related to inflammatory markers. Belém/PA, 2020-2021. *Male. **Women. *** Qualitative exam. ALT: Alanine aminotransferase. AST: Aspartate aminotransferase. LDH: Lactic dehydrogenase. TB: Total bilirubin. DB: Direct bilirubin. IB: Indirect bilirubin. ALP: Alkaline phosphatase. GGT: gamma-glutamyl transferase. CRP, C-reactive protein. PT: Prothrombin time. ESR: Erythrocyte sedimentation rate. Data are expressed as mean ± standard deviation (M ± SD) and as absolute and relative frequencies. ANOVA test (p<0.05#) Mann-Whitney test (p<0.05&). Chi-squared test (p<0.05') and Fisher’s exact test (p<0.05'').
Table 3.
Comparison of laboratory variables of liver function between groups related to inflammatory markers. Belém/PA, 2020-2021. *Male. **Women. *** Qualitative exam. ALT: Alanine aminotransferase. AST: Aspartate aminotransferase. LDH: Lactic dehydrogenase. TB: Total bilirubin. DB: Direct bilirubin. IB: Indirect bilirubin. ALP: Alkaline phosphatase. GGT: gamma-glutamyl transferase. CRP, C-reactive protein. PT: Prothrombin time. ESR: Erythrocyte sedimentation rate. Data are expressed as mean ± standard deviation (M ± SD) and as absolute and relative frequencies. ANOVA test (p<0.05#) Mann-Whitney test (p<0.05&). Chi-squared test (p<0.05') and Fisher’s exact test (p<0.05'').
| Variables | CRP*** | ESR (mm/h) * | ESR (mm/h) ** | Ferritin* (ng/mL) | Ferritin** (ng/mL) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| + | - | P value | > 20 | ≤20 | P value | >30 | ≤30 | P value | > 300 | ≤300 | P value | > 300 | ≤300 | P value | |
| ALT, M ± SD | 43,79±59,36 | 29,33±23,77 | 0,1145 | 35,04±23,19 | 42,58±41,21 | 0,7073 | 27,92±28,78 | 27,70±34,76 | 0,4037 | 49,48±41,58 | 29,49±16,52 | 0,0104& | 25,88±10,55 | 28,07±32,56 | 0,2520 |
| ALT >29 U/L n. (%) | 11 (4,52) | 63 (25,92) | 0,8545 | 22 (9,05) | 13 (5,35) | 0,0370’ | 28 (11,52) | 11 (4,52) | 0,3403 | 18 (7,40) | 17 (6,99) | 0,1904 | 6 (24,69) | 33 (13,58) | 0,3691 |
| AST, M ± SD | 32,33±52,94 | 24,63±16,53 | 0,9236 | 24,37±7,73 | 34,87±36,62 | 0,6597 | 26,00±31,27 | 21,30±6,77 | 0,3626 | 31,83±22,67 | 25,69±23,82 | 0,0064& | 24,06±6,25 | 24,34±26,83 | 0,0491& |
| AST >25 U/L n. (%) | 9 (3,70) | 54 (22,22) | 0,9811 | 18 (7,40) | 10 (4,11) | 0,9363 | 25 (10,29) | 10 (41,15) | 0,4139 | 17 (6,99) | 11 (4,52) | 0,0233’ | 4 (1,64) | 31 (12,75) | 0,9970 |
| LDH M ± SD | 332,06±81,41 | 331,37±80,10 | 0,8762 | 334,15±100,17 | 331,13±95,05 | 0,9078 | 333,13±70,74 | 326,16±67,18 | 0,4893 | 348,03±107,76 | 322,32±89,52 | 0,2968 | 343,76±72,56 | 329,06±69,06 | 0,4222 |
| LDH >460 U/L n. (%) | 2 (0,82) | 11 (4,52) | 0,9803 | 3 (1,23) | 4 (1,64) | 0,4148 | 3 (1,23) | 3 (1,23) | 4 (1,64) | 3 (1,23) | 1 (0,42) | 5 (2,06) | 0,4817 | ||
| ALP M ± SD | 232,97±84,13 | 197,40±57,53 | 0,0092& | 199,13±63,82 | 193,77±48,21 | 0,2808 | 210,38±68,42 | 195,12±57,88 | 0,3712 | 209,02±53,64 | 188,67±60,53 | 0,5312 | 225,41±59,24 | 202,46±65,49 | 0,1520 |
| ALP >190 µg/L | 23 (9,46) | 107 (44,03) | 0,0689 | 30 (12,34) | 16 (6,58) | 0,8287 | 54 (22,22) | 30 (12,34) | 0,8980 | 23 (9,46) | 23 (9,46) | 0,1383 | 11 (4,52) | 73 (30,04) | 0,4349 |
| GGT* M ± SD | 49,80±31,46 | 49,42±49,24 | 0,9774 | 52,24±57,38 | 44,64±26,30 | 0,8457 | - | - | - | 66,31±69,34 | 37,39±16,17 | 0,0164& | - | - | - |
| GGT >50 µg/L | 2 (0,82) | 23 (9,46) | 0,6297 | 16 (6,58) | 9 (3,70) | 0,8923 | - | - | - | 14 (5,76) | 11 (4,52) | 0,1356 | - | - | - |
| GGT** M ± SD | 46,25±33,47 | 39,29±35,11 | 0,0345& | - | - | - | 40,65±33,79 | 40,26±36,91 | 0,3522 | - | - | - | 56,70±53,14 | 38,57±31,67 | 0,1226 |
| GGT >32 µg/L | 15 (6,17) | 46 (18,93) | 0,1076 | - | - | - | 39 (16,05) | 22 (9,05) | 0,8980 | - | - | - | 9 (3,70) | 52 (21,40) | 0,2965 |
| PT M ± SD | 14,57±11,98 | 12,36±1,18 | 0,2444 | 12,33±1,27 | 12,66±0,99 | 0,3124 | 12,37±1,26 | 13,50±9,15 | 0,8224 | 12,42±1,35 | 12,47±1,06 | 0,6394 | 12,77±1,20 | 12,78±5,88 | 0,1465 |
| PT > 15 segundos | 1 (0,42) | 2 (0,82) | 0,3535 | 1 (0,42) | 0 | 1,0000 | 1 (0,42) | 1 (0,42) | 1,0000 | 1 (0,42) | 3 (1,23) | 0,6374 | 1 (0,42) | 2 (0,82) | 0,2883 |
| TB M ± SD | 0,45±0,21 | 0,47±0,22 | 0,8213 | 0,49±0,26 | 0,50±0,22 | 0,9049 | 0,42±0,19 | 0,52±0,22 | 0,0755 | 0,48±0,27 | 0,50±0,24 | 0,7357 | 0,41±0,19 | 0,46±0,21 | 0,4735 |
| TB >1.0 mg/dL | 0 | 3 (1,23) | 1,0000 | 1 (0,42) | 1 (0,42) | 1,0000 | 0 | 1 (0,42) | 0,3390 | 1 (0,42) | 1 (0,42) | 1,0000 | 0 | 1 (0,42) | 1,0000 |
| DB M ± SD | 0,16±0,06 | 0,17±0,06 | 0,4465 | 0,17±0,06 | 0,17±0,06 | 1,0000 | 0,16±0,06 | 0,18±0,07 | 0,4565 | 0,16±0,05 | 0,18±0,06 | 0,4773 | 0,14±0,05 | 0,17±0,07 | 0,3428 |
| DB >0,2 mg/dL | 1 (0,42) | 7 (2,88) | 1,0000 | 2 (0,82) | 1 (0,42) | 0,5508 | 3 (1,23) | 2 (0,82) | 0,9969 | 0 | 3 (1,23) | 0,5361 | 0 | 5 (2,06) | 0,5860 |
| IB M ± SD | 0,33±0,20 | 0,31±0,19 | 0,6692 | 0,31±0,21 | 0,32±0,19 | 0,7328 | 0,27±0,17 | 0,37±0,20 | 0,0537 | 0,32±0,25 | 0,31±0,19 | 0,7899 | 0,26±0,15 | 0,33±0,19 | 0,5066 |
| IB >0,8 mg/dL | 0 | 2 (0,82) | 1,0000 | 1 (0,42) | 1 (0,42) | 1,0000 | 0 | 0 | 1,0000 | 1 (0,42) | 1 (0,42) | 1,0000 | 0 | 0 | 1,0000 |
| Albumin M ± SD | 4,17±0,40 | 4,09±0,36 | 0,4643 | 4,01±0,34 | 4,13±0,37 | 0,2978 | 4,17±0,36 | 4,07±0,39 | 0,2630 | 4,03±0,41 | 4,06±0,34 | 0,6314 | 4,08±0,36 | 4,15±0,37 | 0,5909 |
| Albumin >4,8 g/dL | 0 | 0 | 1,0000 | 0 | 0 | 1,0000 | 0 | 0 | 1,0000 | 0 | 0 | 1,0000 | 0 | 0 | 1,0000 |
Table 4.
Factors associated with changes in liver injury markers, post-COVID time, symptoms and hospitalization in study patients. Belém/PA, 2020-2021. *Male. **Women. *** Qualitative exam. ALT: Alanine aminotransferase. AST: Aspartate aminotransferase. LDH: Lactic dehydrogenase. ALP: Alkaline phosphatase. GGT: gamma-glutamyl transferase. ESR: Erythrocyte sedimentation rate.
Table 4.
Factors associated with changes in liver injury markers, post-COVID time, symptoms and hospitalization in study patients. Belém/PA, 2020-2021. *Male. **Women. *** Qualitative exam. ALT: Alanine aminotransferase. AST: Aspartate aminotransferase. LDH: Lactic dehydrogenase. ALP: Alkaline phosphatase. GGT: gamma-glutamyl transferase. ESR: Erythrocyte sedimentation rate.
| Risk variables | ALT >29 U/L | AST >25 U/L | Ferritin >300 ng/mL | Long COVID time ≤6 | >5 long COVID symptoms | Hospitalization | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Odds ratio | P value | Odds ratio | P value | Odds ratio | P value | Odds ratio | P value | Odds ratio | P value | Odds ratio | P value | |
| Hospitalization, Yes | 0,8948 | 0,8025 | 2,1662 | 0,0807 | 1,7693 | 0,1495 | 2,4271 | 0,0059 | 1,9802 | 0,0542 | - | - |
| Long COVID time ≤6 | 0,7877 | 0,5933 | 0,6341 | 0,3236 | 1,5344 | 0,2711 | - | - | 2,8343 | 0,0042 | 2,4542 | 0,0052 |
| Age ≥60 years | 0,2855 | 0,0214 | 1,1367 | 0,8038 | 2,4342 | 0,0331 | 1,5585 | 0,2126 | 0,9407 | 0,8678 | 1,4307 | 0,3218 |
| Male | 2,6959 | 0,0274 | 0,9369 | 0,8878 | 4,8173 | < 0,0001 | 2,0594 | 0,0351 | 0,6988 | 0,3046 | 2,4365 | 0,0087 |
| >5 long COVID symptoms | 1,1528 | 0,7536 | 0,6118 | 0,2554 | 0,6997 | 0,3829 | 2,8768 | 0,0041 | - | - | 1,9906 | 0,0539 |
| ALT >29 U/L | - | - | 21,3046 | < 0,0001 | 1,7447 | 0,2720 | 0,8798 | 0,7707 | 1,0923 | 0,8321 | 0,8981 | 0,8054 |
| AST >25 U/L | 21,5317 | < 0,0001 | - | - | 1,2285 | 0,6807 | 0,7166 | 0,4531 | 0,6006 | 0,2344 | 2,2260 | 0,0670 |
| LDH ≥460 U/L | 0,2712 | 0,1577 | 5,4802 | 0,0266 | 1,3118 | 0,7063 | 1,2126 | 0,7673 | 2,0278 | 0,3957 | 4,6938 | 0,0370 |
| ALP ≥ 190 U/L | 0,7481 | 0,4745 | 1,0868 | 0,8380 | 1,9531 | 0,0852 | 1,3307 | 0,3638 | 0,7894 | 0,4398 | 0,7015 | 0,2669 |
| GGT ≥ 50 U/L* ou 32 U/L** | 3,5989 | 0,0019 | 1,9687 | 0,1094 | 1,5007 | 0,3431 | 1,3967 | 0,3401 | 1,7849 | 0,1055 | 1,2841 | 0,4755 |
| Ferritin ≥ 300 ng/mL | 1,6449 | 0,3357 | 1,3499 | 0,5338 | - | - | 1,5394 | 0,2654 | 0,6965 | 0,3639 | 1,9245 | 0,0966 |
| ESR ≥ 20 mm/h* ou 30 mm/h ** | 1,1198 | 0,7887 | 1,2075 | 0,6576 | 1,9377 | 0,1069 | 1,3981 | 0,3084 | 0,6022 | 0,1178 | 1,0869 | 0,8008 |
| Positive C-reactive protein *** | 1,2672 | 0,6725 | 0,8917 | 0,8434 | 0,4243 | 0,1865 | 0,7255 | 0,5023 | 1,1572 | 0,7462 | 0,9796 | 0,9651 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



