
Submitted:
08 February 2023
Posted:
09 February 2023
You are already at the latest version
Abstract
The aims of this study are to determine the oral health status of a rare sample of 19th-century migrant settlers to South Australia, how oral conditions may have influenced their general health, and how the oral health of this group compares with contemporaneous samples in Australia, New Zealand, and Britain. Dentitions of 18 adults and 22 subadults were investigated using non-destructive methods (micro-CT, macroscopic, radiographic). Extensive carious lesions were identified in 17 adults and 4 subadults, from this group 1 subadult and 16 adults had antemortem tooth loss. Sixteen adults showed evidence of periodontal disease. Enamel hypoplastic (EH) defects were identified in 14 adults and 9 subadults. Many individuals with dental defects also had skeletal signs of co-morbidities. South Australian individuals had the same percentage of carious lesions as the British sample (53%), more than other historic Australian samples, but less than a contemporary New Zealand sample. Over 50% of individuals from all the historic cemeteries had EH defects suggesting systemic health insults during dental development were common during the 19th century. The overall oral health of the South Australian settlers was poor but, in some categories, (tooth wear, periapical abscess, periodontal disease), better than the other historic samples.
Keywords:
Oral Health
; Systemic Health
; Colonial Dental Health
1. Introduction
A skeletal sample of 19th-century migrant settlers to South Australia was investigated to understand their health status. There are few collections of skeletal remains from early migrants to Australia. The majority of the individuals from this South Australian sample were buried in the first three decades after the establishment of the colony in 1836. Skeletal abnormalities in these individuals have been examined and the findings in relation to the general health have been published [1,2]. The dentoalveolar complexes of these skeletons were investigated in this study, to expand understanding of the health status in relation to dental and oral health.
Tooth enamel does not remodel in life [3,4]. Dentine can remodel but very slowly as a result of the aging process and/or due to dental caries or trauma [3,4]. Therefore, health insults that occur during dental development in utero and postnatally until young adulthood [5,6] can cause enamel and dentine defects such as enamel hypoplasia and interglobular dentine that remain throughout life [4]. This makes dentition an excellent model for the investigation of an individual’s health history compared with bones, which remodel during life in response to changes in the forces acting on them [7]. Skeletal abnormalities that result from a health insult in early life, may alter or change with the remodelling of the bone.
The presence of carious lesions, morphological changes to the alveolar bone, including its loss, and antemortem tooth loss due to extraction, disease, or trauma are all valuable sources of evidence. As a result of teeth being in direct contact with their environment, patterns of tooth wear from attrition, abrasion, and erosion can provide information regarding diet, lifestyle choices, oral hygiene, the use of teeth in daily activities, and the environment of the individual. Cultural practices affecting the oral environment may also leave their mark on dentition, for example, pipe mouthpieces or pins and nails habitually held between teeth by some tradespeople. The status of the oral health of this group of early settlers could also give an indication of the degree to which they had access to the available dental services [8].
The relationship between poor oral health and systemic ill health has been investigated [9,10,11]. Periodontal disease has links to many systemic illnesses, such as atherosclerotic cardiovascular disease [12,13,14,15], Type 2 diabetes [9,16], and bacterial pneumonia [17,18]. Considering the oral health of the St Mary’s Cemetery sample, together with any skeletal signs of disease to indicate co-morbidities [1,2] should provide the clearest possible insight into the health of these individuals.
Therefore, the aims of this study were to investigate 1) the oral health status of the individuals buried at the ‘free ground’ of St Mary’s Anglican Church Cemetery, 2) how these oral conditions may have influenced their general health and, 3) how the oral health status of these colonial South Australian settlers compared with other historic samples in Australia, New Zealand, and Britain.
2. Materials and Methods
2.1. Materials—The Archaeological Sample
The 70 individuals in this sample were buried between 1847 and 1927, in an area of the cemetery set aside for people who had no funds to pay for their interment. The burial register for St Mary’s Anglican Church lists interments in this section of the cemetery as either in the ‘free ground’, the ‘common ground’, or no burial location was recorded. Burials in the free ground were paid for by the South Australian Government. Leased buried plots in the main section of the cemetery were numbered and paid for by the deceased or their family, and gravestone memorials [1]. A higher number of migrant settlers from this parish (82%) were interred in the free ground area between 1847 and 1880 compared with in leased plots [1]. This was during a period of political instability and two economic depressions for the new colony. No gravestones were erected in the free ground to identify the buried individuals; thus each excavated skeleton was assigned a site code and number (e.g., St Mary’s Burial/number 58 = SMB 58). No other sections of the cemetery have been excavated. Relevant aspects concerning the excavation of this sample and the macroscopic skeletal abnormalities have been published [1,2,19,20]. Determination of the sex of each individual and an estimation of the age range at death, from the skeletal remains and macroscopic examination of tooth eruption, were recorded immediately after the excavation of each skeleton [19].
2.1.1. The Archaeological Sample—Dentitions
The skeletal remains of 40 individuals, where dentitions were preserved in a suitable state were selected for the study. This sample consisted of 18 adults (13 male and 5 female) and 22 subadults from the St Mary’s Cemetery skeletal collection (total n = 70). The maxillary and mandibular bones of the remaining 30 individuals were highly fragmented
The specimens investigated comprised dentitions in situ within the dentoalveolar complex of the skull and lose teeth that had been displaced post-mortem. A dental inventory (number and type of teeth present), an estimation of the age range (assessment of the skeletal remains and dentitions), and the sex of each individual are presented in Table S1.
2.1.2. The Archaeological Sample—Ethics
The excavation of the free ground section of St Mary’s Anglican Church Cemetery occurred upon the request of the Parish as they wished to re-use the area. Approval for the study of the skeletal remains was also granted by St Mary’s Parish and Flinders University Social and Behavioural Research Ethics Committee (SBREC project number 8169). Destructive analysis was not permitted during the investigation of this sample as they are of a rare historical nature.
2.2. Methods
Large Volume and Small Volume (LV or SV Micro-CT) scanning systems, macroscopic examination, and standard dental radiographs were used for the investigation of the structures of the dentoalveolar complexes of the selected human skulls from the St Mary’s skeletal collection.
2.2.1. Large Volume Micro-CT
This technique allowed the examination of ‘large ‘specimens such as dentitions that remain in situ within the skull that require minimal handling. This method provides rapid data acquisition at a high resolution of both external and internal structures [21]. The dentoalveolar complexes in situ within the skulls of six individuals (2 adults, SMB 66B, SMB 73; 2 subadults, SMB 04A, SMB 52B, and 2 infants SMB 58, SMB 82) were scanned using the Nikon XT H 225 ST cabinet Micro-CT scanning system [22]. The pixel/voxel size (spatial resolution) used for each scan was different as these are relative to the size of the specimen. The settings used for each complete skull, cranium, or mandible alone are presented, with additional scanning information, in Table S2.
2.2.2. Small Volume Micro-CT
Teeth that had been displaced post-mortem from 21 individuals (N=41 teeth) (Table S3) were investigated. The number of teeth and tooth types that were available for each individual varied. Individual tooth specimens were scanned using the desktop Bruker SkyScan 1276 [23], at a pixel size of 9.0 µm. Information regarding the SV Micro-CT scan settings is presented in Table S3.
2.2.3. Macroscopic Examination
Visual investigation of the structures of the dentoalveolar complexes was conducted in a dry laboratory with the aid of a table magnifying glass with enhanced lighting. A periodontal probe with incremental markings was used for measurements [24]. The Fédération Dentaire Internationale (FDI) - World Dental Federation notation system [25,26] was used in this study to accurately record and distinguish between permanent and primary teeth.
2.2.4. Standard Dental Radiographs
Panoramic extraoral radiographs (crania and mandibles were imaged separately), and periapical intraoral radiographs were taken using Planmeca X-ray equipment [27]. Details of the radiographic equipment and the settings used are available in the supplementary material as Appendix 1. Dental radiographs can only identify severe cases of interglobular dentine (IGD) or enamel hypoplastic defects (EH), therefore these categories were not scored on those.
2.2.5. Scoring: Dental and Alveolar Bone Health Categories
The following dental and alveolar health categories were scored: Dental inventory, dental age, tooth wear, presence of carious lesions, periodontal disease, enamel hypoplastic (EH) defects, and interglobular dentine (IGD). The identification criteria and scoring systems used for the above categories are listed in Table 1. Teeth with more wear could be suggestive of an older adult. Therefore, 11 adults from the St Mary’s sample with permanent molars remaining in situ were scored using Miles’s (1962) [28] tooth wear system for archaeological specimens. This system assesses the functional age of each molar and predicts the age of the subject [28]. To determine the extent of general tooth wear Molnar’s (1971) [29] system was also used for all individuals in the sample.
Avizo 9 data visualisation software [30] was used for image analysis of the reconstructed LV & SV Micro-CT scan data sets. The software (Avizo 9), provides digitally reconstructed radiographs (DRR) from the LV and SV Micro-CT scans, which were compared to the dental radiographs. The category of radiolucency of caries (Table 1), was scored on both the dental radiographs and the DRR. This software was used to manipulate the bone density threshold levels of specimens (i.e., reduce the density of the alveolar bone) to reveal developing teeth.
Alveolar bone loss, which was suggestive of periodontal disease, was scored using a measurement from the cementoenamel junction (CEJ) on a tooth to the crest of the alveolar bone [24]. This measurement was taken along the midline of the tooth on the labial/buccal and lingual/palatal surfaces. An increase in the distance measurement from the CEJ to the crest of the alveolar bone suggests that bone loss had occurred. Measurements of 4 mm or above are included in this analysis.
St Mary’s sample were examined for evidence of calculus deposits. Adult SMB 84 is edentulous (with dentures) and not included in this analysis. The presence and location of the calculus on the tooth (enamel or root), and the severity of the deposits (small/ slight, medium, or large/considerable) were scored following the criteria set out by Connell and Rauxloh (2003) [31]; and Powers (2012) [32] from the Museum of London Human Osteology Method Statement. These systems are developed from that of Brothwell (1963) [33].
It is difficult to differentiate areas of staining on the tooth that could be caused by the burial environment and/or taphonomic changes from developmental enamel opacities and/or variations in the mineralisation of the enamel [34,35,36]. Therefore, enamel opacities (hypo-mineralisation defects) were not investigated.

Table 1.
Categories for scoring dental and alveolar bone health.
| Categories to be Investigated | Criteria for Identification: | Scoring Systems: | References: |
|---|---|---|---|
|
Dental Inventory |
Total number of teeth in situ. Antemortem tooth loss: evidence of alveolar tissue healing. Post-mortem tooth loss: open socket and no evidence of bone healing |
Data were recorded on a visual chart representing the primary/ permanent teeth – using the FDI (ISO 3950) notation system. i) tooth type present, ii) location of healed alveoli, iii) open socket – location in the alveolar process |
[25,26,37,38,39,40] |
|
Dental age range |
Erupted tooth types present, semi-erupted and developing teeth in alveolar bones Tooth wear – adult molars only |
The London Atlas of tooth eruption and development was used with dental radiographs to identify the stage of eruption and tooth development (0-23.5 years). Adult age range: Assessment of the functional age of each molar and the predicted age of the subject based on tooth wear scores set out by Miles (1962). |
[5,6,28] |
|
Tooth wear |
Evidence of enamel loss and/or exposure of dentine on the occlusal surface of the teeth | Category of tooth wear selected from Molnar’s (1971) and Miles’s (1962) criteria charts. | [28,29] |
|
Carious lesions (caries - cavity) |
1) Evidence of decay: a) present on enamel surface only, b) involving enamel & dentine, c) decay involving the enamel dentine & the pulp. 2) Identify changes in radiolucency/ density of the tooth |
Score: i) tooth type affected (FDI), ii) location of the carious lesion in relation to the CEJ, iii) ICDAS/ICCMS category of radiolucency- using dental radiographs & DRRs. Select a category from a visual chart. | [41] |
|
Periodontal disease |
i) Evidence of alveolar bone loss ii) Evidence of morphological changes of the margins of the contours of the alveolar bone of the posterior teeth (buccal surface only) |
i) Measurement taken from the CEJ to the crest of the alveolar bone on the midline of the crown surface (labial/buccal & lingual/palatal). ii) Alveolar bone status: Graded 0-4 using Ogden’s (2008) system, by inspection of the margins of the alveolar bone surrounding the posterior teeth. |
[42,43,44] |
|
Enamel hypoplastic defects (EH) |
Evidence of lines or pits in the surfaces of the enamel | Scored using an adaptation of the Enamel Defect Index (EDI): i) type of EH defect/s, ii) number of EH defects on the enamel surface, iii) location of EH defect/s - measurement of the distance of the defect/s in relation to the CEJ. | [45,46] |
| Interglobular dentine (IGD) | Evidence of changes in the density of the dentine structure | Record: the presence of IGD as Yes/No (Micro-CT only) | [47,48] |
Notes: CEJ = Cemento-enamel Junction, FDI = Fédération Dentaire Internationale/ World Dental Federation notation system, DRR = Digitally Reconstructed Radiographs using Avizo 9 software [30], ICDAS/ICCMS = International Caries Detection and Assessment System/ International Caries Classification and Management System.
2.2.6. Scoring: Evaluation of Intra and Inter-Operator Variations
Intra-Operator Variation
The primary operator (AG) macroscopically examined and scored the images of teeth and alveolar tissues on dental radiographs, and on 2D and 3D images taken from the LV and SV Micro-CT scans using the Avizo 9 software [30]. A second data scoring session was carried out using the same specimens two weeks later for the evaluation of the intra-operator variability.
Inter-Operator Variation
Operators were trained and calibration sessions were carried out two weeks before these inter-operators independently scored the dental and alveolar bone health categories (Data S1 and Tables S4 and S5).
2.2.7. Statistical Analysis
All analyses were performed using Stata v17 computer software [49]. Assessments of the intra-operator and inter-operator reliability were made using Gwet’s Agreement Coefficient (AC1), weighted Gwet’s Agreement Coefficient (AC2), and Intraclass Correlation Coefficient (ICC) using a two-way random-effects model for absolute agreement, for binary and nominal scale data, ordinal scale data and continuous data, respectively. Results are presented as AC1/AC2 with a 95% confidence interval (CI) and percentage agreement for non-continuous data; ICC with 95% CI for continuous data. Interpretation of AC1 and AC2 was <0 poor agreement; 0 – 0.2 slight agreement; 0.21 – 0.4 fair agreement; 0.41 – 0.6 moderate agreement; 0.61 – 0.8 substantial agreement; >0.8 almost perfect agreement [50]. Interpretation of ICC values was <0.50 poor agreement; 0.50-0.75 moderate agreement; 0.75-0.90 good agreement; >0.90 excellent agreement [51].
2.3. Comparison of Historic Dental Samples from Australian, New Zealand, and British Cemeteries
Findings from the investigation of the dental and alveolar bone health categories for the St Mary’s Cemetery sample were compared with data from two colonial Australian samples, Cadia Cemetery, NSW, 1864-1927 (N=109) [52], and Old Sydney Burial Ground (OSBG), NSW, 1792-1820 (N=10) [53]. Dental findings from Cadia Cemetery have not been previously published therefore, permission was granted by the copyright holder, Newcrest Mining Ltd, and Dr. Edward Higginbotham and Associates Pty Ltd, the consultant archaeologist. St Mary’s findings were also compared with published data from St John’s Burial Ground, Milton, Otago, New Zealand, (1860-1926) (N= 7) [54], and a British sample from the Cross Bones Burial Ground, Southwark, London, UK (1800-1853) (N=83) [55]. The category of tooth wear for each cemetery was scored using different systems, therefore, only scores that represented ‘moderate to heavy’ tooth wear was compared.
3. Results
3.1. Reproducibility—Standard Statistical Analysis
Due to the small sample size, many tests for intra-operator and inter-operator achieved perfect agreement resulting in all summary ranges including perfect or excellent agreement [50,51]. For the inventory and tooth wear measurements, the inter-operator agreement was better when using the Macroscopic or Radiographic techniques (poor to perfect - Macroscopic) and substantial to perfect (Radiographic) compared with fair to perfect (LV Micro-CT); and moderate to perfect (both Macroscopic and Radiographic) compared fair to perfect (LV Micro-CT); for inventory and tooth wear, respectively). For alveolar status, the inter-operator agreement was the same for both LV Micro-CT and Macroscopic. The LV Micro-CT method achieved the same level of agreement for all other measures when assessing both inter- and intra-operator as the other techniques. The Macroscopic method also had an almost perfect agreement. It should be noted though that the percentage agreement was very similar, between 81 and 100% agreement for LV Micro-CT and 88 to 100% agreement for Macroscopic.
A summary of the tests of intra- and inter-operator reliability for each of the methods investigated is presented in Table S4. A written summary with information on this statistical analysis follows Table S4. Additional data and the raw data can be found in Table S5 and Data_S1_Gurr et al. 2022_RAW DATA_S1_EXCEL_, respectively.
3.2. Dental Inventory
A full dental inventory for each individual is presented in Table S1. Thirty-nine of the 40 individuals had dentitions in situ. The total number of teeth present for the sample (N=40), was 518 (175 primary and 343 permanent teeth). Eight adults, each had less than 10 teeth present (Table S1). One adult female, SMB 84, was edentulous and had a full set of vulcanite dentures with porcelain teeth (Figure 1). The setup/ fabrication of the dentures suggests that they were well made.
3.2.1. Dental Age Range
The estimated dental age range for each individual is presented in Table S1. The dental age range of the majority of individuals was similar to that assigned from the skeletal assessment (Anson, 2004). The dental age ranges of the two subadults (SMB 28, SMB 70) were different from the skeletal age range (Table S1). Subadult SMB 28: the dental age range was 15.5 -16.5 years (+/= 1 year) compared with the 12-13 years skeletal age range. The skeletal age was based on the incomplete fusion of the epiphyseal plates at the elbow [19]. Radiographically, there was no evidence of the mandibular third molars developing, and the alveolar tissue in this area was fragmented. The developing crowns of these molars were loose and had separated from the jaw. Subadult SMB 70: dental age range was 11.5 -12.5 years (+/- 1 year), compared with the 8-9 years skeletal age range.
3.3. Tooth Wear
In scoring tooth wear a higher category implies more wear [28,29]. The functional age of the permanent molars of 11 adults was scored to estimate the age range of each individual [28] (Table S6). Some of the age ranges predicted by Miles’s (1962) system [28] were different from the age ranges assigned to the individuals from the evidence of skeletal changes/ maturity and dental eruption. Molnar’s (1971) [29] system provided general tooth wear scores for each tooth present in all of the individuals in the sample (Tables S7a–S7c). The individuals with higher categories of tooth wear (categories 4-8) [29] were all adults (Table S7a). Analysis of the distribution of tooth wear for the different tooth types (i.e., incisors, canines, premolars, etc.) showed that more anterior teeth (central and lateral incisors, and canines) were scored with category 4 and 5 tooth wear compared with premolars and molars (Table 2). The canine teeth of the St Mary’s adults were the only anterior teeth to be scored with category 5 tooth wear along with the molars (Table 2).
Three adult males (SMB 59, SMB 72, SMB 78), showed patterns of tooth wear that suggest they had smoked a pipe for an extended period of time. The opposing upper and lower teeth for example, the maxillary and mandibular canines and first premolars had a semi-circular pattern of tooth wear suggesting these teeth could have gripped a pipe (Figure 2).
3.4. Carious Lesions
Seventeen adults and 4 subadults (Table 3) had evidence of carious lesions on their dentitions (N= 21/40 - 53%). Seven individuals from this group had more than 60% of their teeth affected by caries (Table 3). The majority of the carious lesions were seen on the permanent teeth, except for the primary teeth of subadults SMB 19 (FDI tooth numbers 55 & 83), and SMB 70 (FDI tooth numbers 53 & 63). The total number and percentage of teeth affected by carious lesions are presented in Table 3. A greater number of lesions were located on the CEJ (46%) than above (42%), or below the CEJ (12%) (Table S8a), and a greater number of carious lesions was located on the mesial (29%) and distal (25%) surfaces of the teeth than on the occlusal (14%), the labial/buccal (21%), and the lingual/palatal (11%) surfaces (Table S8a). The extent of the carious lesions (e.g. how many involved the enamel only, the enamel and the dentine, or were extensive and approaching the pulp chamber) are presented in (Table S8b). The majority of carious lesions observed in the St Mary’s sample involved the enamel only and had not extended to involve the dentine or pulp (Table S8b).
A large carious lesion was identified on the mesial/ occlusal surface of the lower right permanent first molar (M1), of subadult SMB 79 (Figure 3A). Resorption of the alveolar bone surrounding this tooth exposed the majority of the buccal roots (Figure 3B). A localised periapical cavity was present with a circular hole (fistula) in the alveolar bone (3 mm in diameter), on the buccal surface, inferior to the mesial root of the M1 (Figure 3B,C). Evidence of changes in the texture of the alveolar bone surface (porosity) around this fistula was seen (Figure 3B). Radiographs showed the carious lesion had involved the enamel, dentine, and pulp of this tooth. The X-ray image also shows the extent and depth of the periapical cavity around the distal root of the M1 and the ‘opening’ in the alveolar bone adjacent to the apex of the mesial root (Figure 3C).
3.5. Periodontal Disease
3.5.1. Alveolar Bone Loss
N = 9/40 adults (7 males: SMB 06, SMB 23, SMB 57, SMB 63, SMB 68, SMB 73, SMB 78, and 2 females: SMB 53C, SMB 66B), age range 30 to 49 years had a distance measurement from the CEJ to the crest of the alveolar bone of 4 mm or over (up to 10 mm), on three or more teeth suggesting evidence of periodontal disease. Adult SMB 73, had 9 teeth with a distance measurement ranging from 6 mm to 10 mm (other affected teeth measured from 4 to 5 mm). Two adults (SMB 14, SMB 85, both male, age range 40-59 years), only had two teeth remaining having lost the majority of their teeth in life (antemortem). These teeth showed extensive horizontal alveolar bone loss (6 -7mm per tooth). The female with the dentures (SMB 84) (Figure 1) had complete resorption of alveolar processes.
3.5.2. Alveolar Bone Status
Ogden’s (2008) [42] system of assessment: Grade 0 = unable to score i.e., alveolar is missing, Grade 1 = no disease to Grade 4 = severe periodontitis. The higher grades (3 and 4) suggestive of evidence of periodontal disease are shown here.
Grade 3 – N=3 adults (males, SMB 72, SMB 73, SMB 83), age range 30-59 years.
Grade 4 – N=8 adults (7 males, SMB 06, SMB 09, SMB 23, SMB 57, SMB 63, SMB 68, SMB 85, and 1 female, SMB 66B), age range 30-39 years.
The buccal contours of the alveolar margins of the posterior teeth for adult SMB 06 (age 40-49 years), had the highest number of areas scored at grade 4. The remaining areas of alveolar bone for this individual were scored from grade 1 to 3, suggesting extensive periodontal disease.
3.5.3. Calculus
Calculus (calcified plaque) deposits were observed on the remaining dentitions of 11 of the 17 adults from the St Mary’s sample, the full results per tooth are presented in Table S9. A total of 240 teeth were examined with 79 teeth (33%) being affected by calculus (Table 4 and Table S9). The calculus deposits observed were small (slight) to medium amounts (Table S9). Five adults from the group of 11 had between 68% and 100% of their teeth affected by calculus (Table S9). The location of the calculus was predominantly on the enamel surface (60/79 teeth) (Table S9).
3.6. Enamel Hypoplasia (EH)
Fourteen adults and 10 subadults showed evidence of one or more enamel hypoplastic defects on one or more of their teeth (Table 5a and Table S10), representing over half of the total sample (N=24/40 - 60%). Four adults and 4 subadults had EH defects on 60% or more of their teeth (Table 5a). Adult SMB 73, had the highest percentage of teeth affected by EH defects (Table 5a). More canine teeth were affected by EH defects than the incisors, premolars or molars for both primary and permanent dentition (Table 5a and Table S10). This was followed by the central and lateral incisors. The permanent third molars were the least affected tooth type (Table 5b). Large Volume Micro-CT scans identified EH defects on the erupted primary teeth and the developing permanent teeth of infant SMB 58 (Figure 4) (Table 5a). This infant also had evidence of EH defects on 4 primary canines, 4 primary second molars, and 16 permanent teeth (central and lateral incisors, canines, and first molars), either starting to erupt or developing within the alveolae of the maxilla and mandible (Figure 4) (Table 5 and Table S9). Details of the number of EH defects per tooth per individual are presented in Table S10.
Table 5a.
Number and percentage of Enamel Hypoplastic (EH) defects identified in the individuals from the St Mary’s sample antemortem tooth loss.
Table 5a.
Number and percentage of Enamel Hypoplastic (EH) defects identified in the individuals from the St Mary’s sample antemortem tooth loss.
| St Mary’s ID |
Age Range (Skeletal & Eruption Findings) (Years) |
Sex | Total Number of Teeth Present |
Permanent and/or Primary Dentition |
Tooth Type/s Affected by EH Defects FDI Notation |
Total Number of Teeth with EH Defects |
Percentage of Teeth Affected by EH Defects |
Type of EH Defect/s Present |
|---|---|---|---|---|---|---|---|---|
| SMB 58 | 0-2 | U | 11 | All primary teeth | 51, 52, 54, 61, 62, 72, 74, 84 | 8 | 72% | Linear & pits |
| SMB 11 | 0-2 | U | 19 | primary | 53, 63, 73, 83 | 4 | 21% | Pits |
| SMB 04A | 3-5 | U | 19 | primary | 71, 72, 81, 82 | 4 | 21% | Pits |
| SMB 35 | 6-9 | U | 11 | primary | 63 | 1 | 9% | Pits |
| SMB 19 | 6-9 | U | 22 |
Mixed 7 primary 15 Permanent |
12, 13, 14, 15, 21, 22, 42, 83 | 8 | 36% | Linear & pit |
| SMB 51 | 10-15 | U | 16 | 1 primary 15 Permanent |
12, 13, 14, 16, 22, 23 24, 25, 26, 34, 36 | 11 | 69% | Linear & pit |
| SMB 52B | 10-15 | U | 17 | 2 primary 15 permanent |
11, 12, 13, 16, 21, 23, 26, 31,32, 33, 36, 14, 42, 43 | 14 | 82% | Linear & pit |
|
SMB 70 |
10-15 | U | 8 | 2 primary 6 Permanent |
53, 21, 63, 26 | 4 | 50% | Linear & Pits |
| SMB 28 | 10-15 | U | 26 | All Permanent | 11, 12, 15, 16, 22, 23, 25, 26, 27, 31, 32, 33, 34, 35, 41, 42, 43, 44, 45, 47 | 20 | 77% | Linear & pit |
| SMB 79 | 16-19 | U | 25 | Permanent | 13, 23, 27, 33,43 | 5 | 20% | Linear & pit |
| SMB 05 | 20-29 | F | 6 | Permanent | 41, 42 | 2 | 33% | Linear |
| SMB 53C | 30-39 | F | 9 | Permanent | 11, 13, 14, 21, 23 | 5 | 56% | Linear & pit |
| SMB 66B | 30-39 | F | 17 | permanent | 14, 17, 21, 23, 27, 34, 44, 45 | 8 | 47% | Pits |
| SMB 73 | 30-39 | M | 19 | Permanent | 11, 12, 13, 16, 21, 23, 25, 31, 32, 33, 34, 41, 42 ,43, 44 | 15 | 79% | Linear & pits |
| SMB 06 | 40-49 | M | 24 | Permanent | 12, 31, 32, 41, 42 | 5 | 21% | Linear |
| SMB 09 | 40-49 | M | 22 | Permanent | 12, 13, 21, 22, 23, 32, 33, 43 | 8 | 36% | Linear & pit |
| SMB 57 | 40-49 | M | 25 | Permanent | 11, 12, 13, 14, 27, 32, 33, 35, 42, 43 | 10 | 40% | Linear & pit |
| SMB 72 | 40-49 | M | 29 | Permanent | 12, 13, 23, 24, 38, 43, 48 | 7 | 24% | Pits |
| SMB 83 | 40-49 | M | 16 | Permanent | 13, 21, 23, 27, 28, 33, 34, 42, 43 | 9 | 56% | Linear & pit |
| SMB 85 | 40-49 | M | 2 | Permanent | 33 | 1 | 50% | Linear & pit2 |
| SMB 23 | 50-59 | M | 21 | Permanent | 17, 18, 21, 31, 32, 33, 41, 42, 43 | 9 | 43% | Linear & pit |
| SMB 59 | 50-59 | M | 15 | Permanent | 11, 12, 13, 21, 22, 23, 35, 38, 41, 42, 44, 46 | 12 | 80% | Linear & pit |
| SMB 63 | 50-59 | M | 3 | Permanent | 32, 43 | 2 | 67% | Pits |
| SMB 68 | 50-59 | M | 19 | Permanent | 14, 23, 35, 43, 44, 45 | 6 | 42% | Pits |
Notes: M = male, F = female, U = undetermined sex. EH = Enamel hypoplastic defects. *A tooth may have more than one EH defect. FDI = Fédération Dentaire Internationale tooth identification notation system.
Table 5b.
The different tooth types affected by enamel hypoplastic defects in the St Mary’s Cemetery sample.
Table 5b.
The different tooth types affected by enamel hypoplastic defects in the St Mary’s Cemetery sample.
| Tooth Type | Number of Primary Teeth with EH Defects |
Number of permanent Teeth with EH Defects |
Total Number of Each Tooth Type |
|---|---|---|---|
| Cent. Incisor | 4 | 32 | 36 |
| Lat. Incisor | 5 | 29 | 34 |
| Canine | 8 | 44 | 52 |
| P1 | n/a | 18 | 18 |
| P2 | n/a | 12 | 12 |
| M1 | 3 | 10 | 13 |
| M2 | 0 | 8 | 8 |
| M3 | n/a | 5 | 5 |
| Total | 20 | 158 |
Notes: EH = Enamel hypoplastic defects. Cent. = central, Lat. = lateral, P1 = first premolar, P2 = second premolar, M1= first molar, M2 = second molar, M3 = third permanent molar.
3.7. Interglobular Dentine (IGD)
Two individuals (adult, SMB 73, infant, SMB 58), of the six individuals that were scanned using the LV Micro-CT system, showed areas of IGD. This mineralisation defect in the dentine was seen in all of the erupted and developing primary teeth of infant SMB 58, and of the permanent dentition within the alveolae (developing maxillary and mandibular teeth listed above) (Figure 5). Individual SMB 73, had IGD in 17 of his 19 permanent teeth. Three individuals (adults, SMB 63, 73, subadult, SMB 70), from the 21 individuals who had one or more loose teeth scanned using the Small Volume Micro-CT system (Table S3), showed IGD.
3.8. Comorbidities, and Signs of Skeletal and Dental Changes
Twenty-five individuals from the St Mary’s dental sample of 40, had poor oral health. Their oral health findings are presented in Table 6. From this group, one infant, five subadults, and 7 adults (N=13/25) also had skeletal signs of one or more co-morbidities and/or signs of skeletal abnormalities and/ or evidence of dental changes including indicators of lifestyle habits (Table 6). Some co-morbidities are only evident in the soft tissue [9,12,13,14,15,16], and could not be identified in the skeletons of this sample. Seven adults had evidence of skeletal abnormalities such as Schmorl’s nodes and vertebral osteophytes (Table 6) [1,2] and three adult males had dental changes due to tooth wear (pipe notch) which indicate smoking and an increased risk of poor oral health.
3.9. Comparison of Historic Dental Samples from Australian, New Zealand, and British Cemeteries
3.9.1. Demographic Profiles
For the Australian, New Zealand, and British samples compared with St Mary’s Cemetery sample are presented in Table 7a,b. There were differences and similarities between the samples. Examples a, a) No subadults were included in the dental sample from the Old Sydney Burial Ground (OSBG), NSW, or the St John’s Burial Ground, NZ, (Table 7a). b) The percentage of subadults in St Mary’s, SA; Cadia, NSW, Cross Bones, UK cemeteries was similar. St Mary’s and Cadia cemeteries had a slightly higher percentage of subadults (55% and 67% respectively), than adults compared with the Cross Bones Burial Ground (Table 8a,b).
Table 7a.
Demographic profiles of the subadults from St Mary’s Cemetery, SA, Cadia Cemetery, NSW, Old Sydney Burial Ground, NSW, St Johns Burial Ground, NZ, and Cross Bones Burial Ground, UK.
Table 7a.
Demographic profiles of the subadults from St Mary’s Cemetery, SA, Cadia Cemetery, NSW, Old Sydney Burial Ground, NSW, St Johns Burial Ground, NZ, and Cross Bones Burial Ground, UK.
|
Cemetery: |
Total Dental Sample/ Total Sample Size |
Total Number of Subadults in Dental Sample | Preterm < 37 Weeks |
Foetal 40 Weeks Post- Partum |
Infant 0-11 Months |
Subadult 1-5 Years |
Subadult 6-11 Years |
Adolescent 12-17 Years |
Subadult of Unknown Age |
|
|---|---|---|---|---|---|---|---|---|---|---|
|
St Mary’s Cemetery (SA) 1847-1927 |
40/70 |
22/40 55% |
0 | 0 | 4 | 10 | 6 | 2 | 0 | |
|
Cadia Cemetery (NSW)1864-1927 |
109/111 |
73/109 67% |
0 | 15 | 25 | 17 | 3 | 4 | 9 | |
|
Old Sydney Burial Ground (NSW)1792-1820 |
10/10 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
|
St John’s Burial Ground (NZ)1860-1926 |
7/27 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
|
Cross Bones Burial Ground (UK)1800-1853 |
83/147 |
39/79 47% |
0 | 0 | 8 | 26 | 2 | 1 | 2 |
Table 7b.
Demographic profiles of the adults from St Mary’s Cemetery, SA, Cadia Cemetery, NSW, Old Sydney Burial Ground, NSW, St Johns Burial Ground, NZ, and Cross Bones Burial Ground, UK.
Table 7b.
Demographic profiles of the adults from St Mary’s Cemetery, SA, Cadia Cemetery, NSW, Old Sydney Burial Ground, NSW, St Johns Burial Ground, NZ, and Cross Bones Burial Ground, UK.
|
Cemetery: |
Total Dental Sample/ Total Sample Size |
Total Number of Adults | Age Group 18-22 Years |
Young Adult 23-35 Years |
Middle Adult 35-50 Years |
Old Adult 50+ Years |
Adults of Unknown Age |
Adult Male |
Adult Female | Adults of Unknown Sex |
||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
St Mary’s Cemetery (SA)1847-1927 |
40/70 |
18/40 45% |
1 | 3 | 8 | 6 | 0 | 13 | 5 | 0 | ||
|
Cadia Cemetery (NSW)1864-1927 |
109/111 |
36/109 33% |
0 | 7 | 18 | 10 | 1 | 23 | 14 | 0 | ||
|
Old Sydney Burial Ground (NSW)1792-1820 |
10/10 |
10/10 100% |
N/A | N/A | N/A | N/A | 10 | 0 | 4 | 6 | ||
|
St John’s Burial Ground (NZ)1860-1926 |
7/27 |
7/7 100% |
0 | 0 | 4 | 4 | 2 | 4 | 3 | 3 | ||
|
Cross Bones Burial Ground (UK)1800-1853 |
83/147 |
44/83 53% |
3 | 4 | 18 | 14 | 5 | 12 | 27 | 5 |
Table 7a. Demographic profiles of the subadults from St Mary’s Cemetery, SA, Cadia Cemetery, NSW, Old Sydney Burial Ground, NSW, St Johns Burial Ground, NZ, and Cross Bones Burial Ground, UK.
Table 7b. Demographic profiles of the adults from St Mary’s Cemetery, SA, Cadia Cemetery, NSW, Old Sydney Burial Ground, NSW, St Johns Burial Ground, NZ, and Cross Bones Burial Ground, UK.
3.9.2. Dental and Alveolar Bone Health Categories
A summary of the scores for the five oral health categories of St Mary’s sample were compared with those of Cadia Cemetery, Old Sydney Burial Ground (OSBG), St John’s, and Cross Bones burial grounds (Table 8). All of the individuals from St John’s were scored with ‘moderate to high’ tooth wear compared with 60% from OSBG, and 35% of individuals from St Mary’s (Table 8). Evidence of ‘pipe facets’ associated with long-term pipe smoking was seen in all seven of the New Zealand adults (sex unknown), 2 adult females from the OSBG sample, and 3 adult males from St Mary’s (Figure 2). No information was available for the category of tooth wear from the Cadia or Cross Bones cemeteries.
St Mary’s and Cross Bones had the same percentage of individuals with carious lesions present (53%) (Table 8). Cadia Cemetery had the smallest percentage of individuals with caries present and St John’s had the highest (Table 8). Periodontal disease was identified in more individuals from St John’s, NZ, (100% of the sample), and Cross Bones, UK, (58%), than in the St Mary’s sample (23%) (Table 8). Data for this category were not available from Cadia Cemetery, or the OSBG, in NSW.
Evidence of one or more periapical lesion was seen in 18% of individuals from the Cross Bones Burial Ground compared with 5% and 3% of people from the Cadia and St Mary’s samples respectively (Table 8). St John’s and the OSBG did not have data for this category. Enamel Hypoplastic (EH) defects were identified in individuals from 4 of the 5 cemeteries (Table 8). Cadia Cemetery did not have specific data for this category. Statistical analyses carried out for the comparison of St Mary’s findings with other samples used the standard error and confidence interval for each percentage.
Table 8.
Comparison of findings for the oral health categories investigated between the St Mary’s Cemetery sample and other 19th-century Australian, New Zealand, and British cemetery samples. The results presented in Table 8 are the number of individuals affected/ number of individuals in the total sample for each cemetery, i.e., St Mary’s n =/ N = followed by the percentage of affected individuals from that cemetery.
Table 8.
Comparison of findings for the oral health categories investigated between the St Mary’s Cemetery sample and other 19th-century Australian, New Zealand, and British cemetery samples. The results presented in Table 8 are the number of individuals affected/ number of individuals in the total sample for each cemetery, i.e., St Mary’s n =/ N = followed by the percentage of affected individuals from that cemetery.
|
Cemetery: |
Sample Size (Total Number of Individuals) N = |
Dental and Alveolar Bone Health Categories Scored | ||||
|---|---|---|---|---|---|---|
| Tooth Wear ‡ Moderate to Heavy | Carious Lesions Present |
Periodontal Disease Interdental Alveolar Resorption |
Periapical abscess Present |
Enamel hypoplastic defects Present |
||
|
St Mary’s Cemetery (SA) 1847-1927 |
40 | 14/40 35% |
21/40 53% |
9/40 23% |
1/40 3% |
24/40 60% |
|
Cadia Cemetery (NSW) 1864-1927 |
109 | Results not available | 32/109 29% |
Results not available |
5/109 5% |
Results not available |
|
Old Sydney Burial Ground (NSW) 1792-1820 |
10 | 6/10 60% |
4/10 40% |
Results not available |
Results not available | 7/10 70% |
|
St John’s Burial Ground (NZ) 1860-1926 |
7 | 7/7 100% |
6/7 86% |
7/7 100% |
5/7 71% |
6/7 86% |
|
Cross Bones Burial Ground (UK) 1800-1853 |
83 | Results not available | 44/83 53% |
42/83 51% |
15/83 18% |
48/83 58% |
NOTES: Tooth wear scores =-‡‘moderate to heavy’- This term was used as each skeletal sample used a different system to score tooth wear. i.e., St Mary’s sample: Tooth wear was scored using Molnar’s (1971) [29] system: moderate to heavy = Category 5 and above, Cadia Cemetery scored using Smith’s (1984) [57] system: moderate to heavy wear = Category 5 and above, Old Sydney Burial Ground scored using Littleton & Frohlich (1993) [58] and Scott’s (1979) [59] systems: moderate to heavy wear = Category 7 or above, Cross Bones Burial Ground scored for tooth wear using Buikstra and Ubelaker (1994) [60]: moderate to heavy wear = Category 5 and above. SA= South Australia, NSW = New South Wales, NZ = New Zealand, UK = United Kingdom.
4. Discussion
4.1. Multiple Methods for Additional Data
The validity and reproducibility of methods used here, for the investigation of bone and dental samples using LV and SV Micro-CT systems had been established [21]. The methods used in this study are non-invasive, as required for rare archaeological specimens such as the St Mary’s sample. The 2D and 3D high-resolution images were produced from the reconstructed LV and SV Micro-CT scan data sets. These provided information that could not be obtained by the standard macroscopic and radiological investigations (Figure 5) [21]. For large specimens such as the dentoalveolar complex in situ within the human skull where minimal handling is required, the LV Micro-CT scanner is ideal. The SV Micro-CT is suitable for small specimens like isolated individual teeth. The resolution of the Micro-CT scanning systems depends on the size of the specimen, i.e. smaller the specimen higher the available resolution and vice versa.
4.2. Aim 1—The Oral Health Status of St Mary’s Cemetery Sample
There is a greater precision available for infants and subadults in assessing dental age based on the eruption and development of teeth [5,6] than for adults. Dental age and skeletal age are two different parameters that often do not coincide in an individual. For two subadults (SMB 28, SMB 70) the dental age range estimated by the London Atlas [5,6] using dental radiographs showed some variation from the assigned skeletal age range (Table S1). These subadults all had co-morbidities (Table 6), which could have affected the timing of their dental development and eruption [61,62,63].
Verma et al, (2022) [28,64] reviewed multiple methods that can be used for the determination of the age of adults using dentition. Many of these methods, however, are destructive. The non-invasive methods set out by Miles (1962) and Molnar (1971) [29] and others like them such as Smith (1984) [57], Littleton and Frochlich (1993) [58] and Scott (1979) [59] assess and score tooth wear (attrition) on the incisal/ occlusal surface. These studies can give an indication of both the functional age of the teeth and a predicted age for the individual [28] and the severity of tooth wear [29]. Since tooth wear increases with age, older individuals, in general, will have had more wear. However, differences that were seen in the dental age, of the investigated adults from St Mary’s, using Miles’s (1962) [28] system compared with their skeletal age range (Table S6), could be due to loss of molars in life. Scoring of the functional age of a tooth from tooth wear will be affected if it does not have an opposing molar and will affect the predicted age given for an individual.
The tooth wear scores for all tooth types [29] for the St Mary’s sample showed that various teeth (i.e., central and/or lateral incisors and/or canines) had different degrees of wear (Table 2). This may have resulted from differences in diet and/or specific habits and/or the presence or absence of opposing teeth due to antemortem tooth loss. A specific example of the sort of diet that the St Mary’s individuals may have had comes from a 19th-century coroner’s report of a man who fell under the wheels of a bullock cart. The “deceased was sitting on the load, which consisted of tea/ sugar and other stores” [65] after an annual trip to the City of Adelaide. A witness to the accident described, “there was about a ton and a half in the dray”, enough supplies for the extended family [65].
4.2.1. Dental Pathologies
Loss of teeth in previous generations may have occurred due to poor oral health, such as extensive caries and/or periodontal disease [42,66]. In addition, due to the high cost of dental treatment, some people may have opted for the extraction of teeth in place of preventative and restorative dental treatments [67]. In some cultures, and social classes, the tradition of removing a future bride’s teeth and replacing them with dentures as a prenuptial gift was practiced [68,69]. This voluntary edentulism was to prevent the burden of costly dental treatments for the new husband’s family. One adult female (SMB 84) was buried at St Mary’s ‘free ground’ area with a full set of vulcanite and porcelain dentures (Figure 1). The background of this individual was unknown but appears to have had a downturn in their economic status before death, as the burial was at the expense of the South Australian Government.
Carious lesions were identified in more than half of the individuals from the St Mary’s sample (N=21/40 - Table 3), the majority of whom were adults (N=17/21 - Table 3). Taking into account antemortem tooth loss that was mainly due to caries, notwithstanding non-clinical reasons, more teeth/ individuals in this sample would have been affected. Most of the carious lesions were located above or on the cementoenamel junction (CEJ), rather than below (Table S8). A ‘build-up’ of dental plaque [3,38], at the interproximal area of the teeth, may explain why a greater number of carious lesions were recorded on the mesial and distal surfaces of the teeth remaining in the jaw for the St Mary’s individuals (Table S8). Extensive carious lesions on other surfaces of the tooth such as the occlusal surface may have resulted in its extraction. Calculus deposits seen on the tooth enamel at these locations for many adults from St Mary’s (Table 4 and Table S9) indicate the accumulation of plaque that had contained caries-producing bacteria and then was calcified [66,70]. A cariogenic diet high in carbohydrates and sugars, such as the consumption of bread made of refined flour and tea with sugar [71,72,73,74,75]. Inclusion of such dietary factors as described in the afore mentioned 1859 Coroner’s report [65], could have resulted in the high incidence of caries in St Mary’s sample. The ‘Adelaide Commercial Report’ for July 1853, published in a local newspaper [76] states that “business was exceedingly flat…for all description of goods, both colonial and imported, but tea, sugar and brandy were the exceptions, all of which are in demand at full rates”.
A lack of knowledge and understanding of the effects of diet on oral hygiene [77,78] and the poor availability and/or affordability of dental services [8], could have also contributed to the poor oral health of several individuals from St Mary’s. The periapical cavity (Figure 3) [79], surrounding the roots of the lower right first permanent molar of subadult SMB 79, with an opening in the buccal surface of the alveolar bone would have arisen from a large carious lesion that extended into the pulp of the tooth.
The 11 adults (N-11/18 adults in sample) with horizontal bone loss (4 mm or more) from the CEJ to the crest of the alveolar bone and the 12 adults with morphological changes in the alveolar bone (grade 3 or above) [42] suffered from periodontal disease. Six individuals (SMB 14, SMB 53C, SMB 61, SMB 63, SMB 78, SMB 85), with higher scores for these categories, also had extreme antemortem tooth loss (Table 4), which is often seen with advanced periodontal disease.
Lifestyle habits such as smoking (Figure 2), have been linked to an increased risk of periodontal disease [80,81,82,83,84]. New migrants to the colony were encouraged to take up tobacco smoking, by advising them that “if they were in the bush, hungry, thirsty or tired” smoking would remedy the situation [85]. Tooth wear patterns indicating long-term pipe smoking were seen in three adult males (SMB 59, SMB 72, SMB 78) from the St Mary’s sample. Two of these individuals also had evidence of periodontal disease (Table 6).
4.2.2. Developmental Dental Defects
Extensive evidence of enamel hypoplastic (EH) defects was seen on the dentitions of 14 adults and 10 subadults (N=24/40) (60%) (Table 5a and Table S10). Eight individuals (4 adults, 4 subadults), from this group, had EH defects on more than 60% of their teeth, with some teeth having multiple defects (Table 5a and Table S10). The presence of multiple EH defects on the teeth indicates that the individuals suffered repeated chronic health insults, which affected the developing teeth [5,6]. Recovery from these episodes of ill health, in the colony, during the voyage, or before migration did occur as many of the individuals with EH defects in the St Mary’s sample were adults (Table 5a and Table S10). The canine teeth, of these individuals, were more affected by EH defects compared with the incisors, premolars or molars (Table 5b and Table S10), suggesting that many health insults occurred in childhood, during the development of the primary and/or permanent canines, rather than young adulthood [5,6].
Limited access to, or the affordability of, health services could have extended an illness. Infant SMB 58 and subadult SMB 70, both showed extensive enamel hypoplastic defects on both the primary and permanent dentition [19,56,86,87] (Table 5a and Table S10). The location of the EH defects on erupted primary and developing permanent teeth of infant SMB 58 (Figure 4) (Table 5a and Table S10), suggests that this infant suffered health insults around the time of birth and postnatally [4]. The pattern of enamel defects seen on the primary teeth of SMB 58 matches those found by Fearne et al., (1990) [88] in low birth weight children.
Dentine, like enamel, could be affected by health insults during dental development. Areas of defective mineralisation in the dentine are referred to as Interglobular Dentine (IGD) [4]. Such defects can occur in the same tooth, in addition to EH defects [1,89,90]. Furthermore, these internal dentine defects can be seen at a similar level to the external EH defect (Fig.5) [1,91], suggesting that the same systemic health insult caused both defects. Areas of IGD and EH defects at a similar level in the tooth were seen in 4 individuals (1 infant SMB 58, 1 subadult SMB 70, and 2 adults SMB 63 and SMB 73 (Table 6 and Figure 4 and Figure 5). No one in the St Mary’s sample was observed with IGD alone. The clinical manifestations of dental defects are related to the severity and duration of the health insult and the degree of the host’s response [92].
4.3. Aim 2: Oral Health Conditions and General Health Status
Evaluation of the oral health findings together with information regarding general health from the skeletal evidence for St Mary’s sample [1,2] provided additional insight into the overall health and lives of these early colonists. Seven adults from this sample had less than 10 teeth present, while four individuals in this group (SMB 14, SMB 63, SMB 78, SMB 85), had just two to four teeth each (Table 3, Table 6 and Table S1). This antemortem tooth loss indicates that their masticatory function was substantially reduced. Dental clinicians have indicated that “20 teeth, with nine to ten pairs of contacting units are necessary to maintain adequate masticatory efficiency” [93]. Therefore, many of the adults in St Mary’s sample would not have had a sufficient number of teeth to maintain adequate masticatory efficiency required for good general health and wellbeing [94].
Seven of the St Mary’s adults had evidence of vertebral osteophytes, eburnation of the vertebral articular facets and other joints of the body (Table 6) [2]. These changes to the bones due to joint disease could have limited their dexterity and the ability to maintain good oral hygiene [10]. It has been established that there is a relationship between poor oral health and systemic disease [9,11,12,13,14,16,17,95,96]. Individuals from St Mary’s showed extensive evidence of poor oral health such as carious lesions, periodontal disease, and antemortem tooth loss (Table 3, Table 6 and Table S1), which would have affected their general health.
The St Mary’s adults with extensive periodontal disease did not show evidence of pathological manifestations associated with systemic disease on their skeletons (Table 6). A lack of skeletal signs of chronic ill health near the time of death does not necessarily indicate an absence of co-morbidities, or indeed a sign of previous good general health. The extensive dental disease seen in many of St Mary’s individuals could have increased the severity of some systemic health conditions such as atherosclerotic cardiovascular disease [12,13,14,15]. This cardiovascular disease only affects the soft tissues of the body and does not leave pathological manifestations on the skeleton [12,13,14,15]. While others, e.g. diabetes mellitus can involve the skeleton [97,98,99]. However, the signs in the skeletal material may not be pathognomic, allowing identification of the specific aetiology.
Some chronic health insults suffered during development, for example, nutritional deficiencies, and/or infectious diseases such as treponemal disease (Syphilis – congenital or acquired) and/ or tuberculosis could produce dental defects (i.e., EH and IGD), as well as skeletal manifestations [1,100,101,102,103]. Twelve individuals from St Mary’s had both developmental dental defects and skeletal signs of a co-morbidity present (Table 6). The presence of specific EH defects on subadult SMB 70, (dental age 11.5-12.5 years +/- 1 year) and IGD, together with evidence of the involvement of the skeleton, including an “osteoblastic lesion on the cranial vault”, pathological changes to the clavicle, ribs, and vertebrae (Table 6) [56], indicated that this subadult had suffered from congenital syphilis, tuberculosis, and mercurial toxicity [19,56,87]. This is an example of the multiple interactions between factors in oral health and in general health which are components in a multilevel complex interactive network that operated throughout the lives of these individuals.
4.4. Aim 3: St Mary’s Oral Health Findings Compared with Australian, New Zealand, and a British Historic Sample
Individuals from the 19th century Cadia Cemetery, NSW, Australia [52], and St John’s Burial Ground, Milton, Otago, New Zealand, [54], represented contemporary communities (Table 7) that could have had similar lifestyles and occupations (agricultural and industrial – mining, etc.), to the individuals buried at the St Mary’s Cemetery ‘free ground’ (Table 7). Individuals interred at the Old Sydney Burial Ground (OSBG), NSW, [53], were not contemporaries of the St Mary’s sample (Table 7) and could have come from different backgrounds i.e., convicts or serving as sailors compared with free settlers in South Australia. They could have also lived in different environmental conditions. However, as previously stated, there are only a few colonial Australian skeletal samples, and it was thought a worthwhile comparison. Cross Bones Burial Ground, London, UK, [55], (Table 7) was used for the poorest people in the 19th century Southwark community [104]. Individuals interred here did not have the money to pay for a burial or a headstone memorial, similar to those buried in the unmarked ‘free ground’ section at St Mary’s Church Cemetery.
The outcome of the comparison of data between these historic cemeteries for five oral health categories found similarities and differences. Information on tooth wear was limited to the OSBG, and St John’s samples. Compared with these samples there seems to be only a small number of individuals from St Mary’s with ‘moderate to high’ wear on the occlusal surfaces of the dentition (Table 8). This may be due to a difference in diet i.e., the individuals from NSW and NZ probably had a more abrasive diet. However, the numbers in the OSBG and St John’s samples are small and therefore when statistics were applied there was considerable overlap of confidence levels and no statistical significance.
Similarities were seen between St Mary’s and Cross Bones Burial Ground (UK) for the categories of carious lesions and enamel hypoplastic (EH) defects (Table 8). In relation to developmental enamel defects, both St John’s and OSBG cemeteries had more individuals with EH present than St Mary’s or Cross Bones cemeteries (Table 8). Brook and Smith (1998) [105] investigated developmental defects in a 20th-century sample of East London school children. They found that 14.6% of the sample had enamel hypoplasia [105], which is markedly lower than any of the historic cemeteries compared in this study.
The same percentage of individuals with carious lesions (53%) for St Mary’s and Cross Bones (Table 8), could suggest that the background of the early settlers to South Australia was similar to those buried at Cross Bones and they continued with their oral hygiene and dietary habits.
Periodontal disease had a higher frequency in the British and New Zealand samples than St Mary’s (Table 8). The individuals from St John’s were all adults compared with St Mary’s, which had a higher number of subadults (Table 7a). Cross Bones had a similar percentage of subadults to St Mary’s sample, suggesting that many of the St Mary’s individuals maintained a better standard of oral hygiene than individuals from the British sample.
In summary, considering the limitations of sample sizes and variations in the presentation and availability of data for analysis, the oral health of many individuals in the comparison samples was poor (Table 8), which would have affected their general health. The seven individuals from St John’s Cemetery sample, NZ, appear to have had the worst oral health compared with data from the other historic samples, but the small sample size from this cemetery could have biased these findings (Table 8). The oral health of individuals from St Mary’s was poor but was better than the other cemetery samples for many of the oral health categories scored in this study (Table 8).
4.5. Limitations of This Study
The use of multiple non-invasive methods allowed detailed data to be collected. While the LV Micro-CT technique is ideal for high-resolution analysis of dentition in situ within archaeological human skull samples [21] the cost of this micro-CT system limited the number of individuals from the St Mary’s sample that were scanned. The number of isolated individual tooth samples available for SV Micro-CT scanning from the St Mary’s sample was also a limitation. As this equipment only scans small objects, teeth have to be separate from the jaw and destructive analysis was prohibited. The SV Micro-CT scanning method was included in this study even though the information obtained from an individual tooth is restricted. This data cannot infer the overall oral or general health of a person, but it can provide information on external and internal developmental defects.
Miles’s (1962) [28] acknowledges that the method of assessing the functional age of a tooth by tooth wear patterns, and thereby predicting the age of the subject has limitations. The individuals studied [28] were derived from a different population (Anglo Saxon). These people could have had a different diet and a different caries rate to the 19th-century group as they would have had less processed sugar. A lower caries rate meant less antemortem tooth loss and so they could have retained their permanent teeth longer compared with the adults from the St Mary’s sample. A limitation that could have affected the results of the presence, location, and severity of calculus deposits [31,32,33] on the dentitions of the St Mary’s adults was due to the partial removal of calculus from some of these skulls for previous studies [106].
5. Conclusions
The overall oral health of the settlers buried at the St Mary’s Cemetery ‘free ground’ area was poor. Their inability to consume adequate amounts of nutritious foods due to extensive antemortem tooth loss would have exacerbated co-morbidities and impacted their general health. The oral health of St Mary’s settlers in relation to categories of tooth wear, periodontal disease, and periapical abscess was better than individuals from the comparison Australian, New Zealand, and British Cemeteries. St Mary’s sample had similar findings for caries and enamel hypoplasia to the Cross Bones Burial Ground in London, suggesting that little improvement had occurred since arriving in the new colony. A high percentage of individuals from four of the five historic cemeteries (St Mary’s, Old Sydney Burial Ground, NSW, St John’s, NZ, and Cross Bones Burial Ground, UK), had enamel hypoplastic defects. This indicates that these individuals had suffered systemic health insults during dental development, which could have been commonplace during the 19th century.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Supplementary Data S1: Gurr. 2022_RAW DATA_Statistical Analysis_EXCEL; Supplementary Table S1: St Mary’s Cemetery - Dental inventory; Supplementary Table S2: Large Volume Micro-CT - Scan settings for in situ dentition; Supplementary Table S3: Small Volume Micro-CT- Scan settings for individual teeth; Supplementary Table S4: Statistical Analysis Summary; Supplementary Table S5: Additional information - Statistical Analysis of intra- and inter-operator reliability; Supplementary Table S6: Assessment of the functional age of each molar and the predicted age of the subject based on tooth wear scores set out by Miles (1962) - St Mary’s Cemetery adult sample; Supplementary Table S7a: Summary of findings for St Mary’s Cemetery adults using Molnar’s (1971) categories of tooth wear; Supplementary Table S7b: Molnar’s (1971) Category of tooth wear assigned to the maxillary dentition of the adults from the St Mary’s sample; Supplementary Table S7c: Molnar’s (1971) Category of tooth wear assigned to the mandibular dentition of the adults from the St Mary’s sample; Supplementary Table S8a: St Mary’s Cemetery Sample. Location of carious lesions on the surface/s of the teeth; Supplementary Table S8b: St Mary’s Cemetery Sample. Number of carious lesions involving either the enamel only, the enamel and dentine, or the enamel, dentine and pulp; Supplementary Table S9: Dental calculus – an indication of the number, and percentage of teeth affected by calculus with the location and severity of the deposit for the adults of the St Mary’s Cemetery sample; Supplementary Table S10: Enamel Hypoplastic Defects _ St Mary Cemetery Sample.
Author Contributions
Conceptualization: A.G and A.H.B, methodology: A.G, D.L, and A.H.B, Software: A.G and D.L, validation: A.G, M.H, and A.H.B. Formal Analysis: A.G, M.H, and A.H.B, Investigation:, A.G, D.L, L.R, and A.H.B, resources: M.H, J.K, and A.H.B, data curation: A.G and D.L, Writing-original draft preparation and review and editing, A.G, M.H, J.K, L.R, D.L, and A.H.B. Supervision, M.H, J.K, and A.H.B, project administration: A.G. Funding acquisition, A.H.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the University of Adelaide, Adelaide Dental School RIBG, and the Paul Kwok Lee Bequest Research Fund.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are openly available in * requested preprint to MDPI at [doi], reference number.
Acknowledgments
Fr. William Deng, of St Mary’s Anglican Church, provided access to the St Mary’s skeletal sample and the parish records. The facilities and the scientific and technical assistance of the Australian Microscopy & Microanalysis Research Facility at Adelaide Microscopy, University of Adelaide are acknowledged, in particular, Dr. Agatha Labrinidis who provided assistance with the Bruker SkyScan 1276 Micro-CT scanning system. Associate Professor Egon Perilli from the Medical Device Research Institute, College of Science and Engineering, Flinders University, shared his expertise regarding the Large Volume Micro-CT system. Flinders Microscopy and Microanalysis (FMMA), provided access to the new Nikon XT H 225 ST Micro-CT scanning system. The Australian Research Council (LE180100136) provided a funding contribution for the procurement of the Large Volume Micro-CT system.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A
Appendix 1
Standard Dental Radiographs - Summary of Equipment and Settings Used
Intraoral periapical and/or bitewing radiographs were taken using Planmeca X-ray equipment [27] with Phosphor Storage Plates (PSP) as the detectors with the following exposure settings: Tube voltage:70 kV; Tube current: 6mA, with an exposure time of 0.32 seconds. Panoramic extraoral dental radiographs were taken using orthopantomogram (OPG) X-ray equipment to rotate around the maxillary and mandibular dentitions if the maxilla and/or mandible were complete enough to use this equipment. The X-ray source used was a Kavo Pan eXam Plus. The tube type for this equipment was: a stationary anode; 65kV; Tube current: 15 mA, with an exposure time of up to 16.4 seconds.
References
- Gurr, A.; Kumaratilake, J.; Brook, A.H.; Ioannou, S.; Pate, F.D.; Henneberg, M. Health effects of European colonization: An investigation of skeletal remains from 19th to early 20th century migrant settlers in South Australia. PloS one 2022, 17, e0265878-e0265878. [CrossRef]
- Gurr, A.; Brook, A.H.; Kumaratilake, J.; Anson, T.J.; Pate, F.D.; Henneberg, M. Was it worth migrating to the new British industrial colony of South Australia? Evidence from skeletal pathologies and historic records of a sample of 19th-century settlers. International journal of paleopathology 2022, 37, 41-52. [CrossRef]
- Atkinson, M.E.; White, F.H. Principles of Anatomy and Oral Anatomy for Dental Students; Churchill Livingstone: Edinburgh, 1992.
- Nanci, A. Ten Cate's Oral Histology : Development, Structure, and Function; Saint Louis: Elsevier: Saint Louis, 2012.
- AlQahtani, S. The london atlas: developing an atlas of tooth development and testing its quality and performance measures. 2012.
- AlQahtani, S.J.; Hector, M.P.; Liversidge, H.M. Brief communication: The London atlas of human tooth development and eruption. American Journal of Physical Anthropology 2010, 142, 481-490. [CrossRef]
- Kenkre, J.S.; Bassett, J.H.D. The bone remodelling cycle. Annals of Clinical Biochemistry 2018, 55, 308-327. [CrossRef]
- Chapman, A.W. History of dentistry in South Australia 1836-1936. 1937.
- Cullinan, M.P.; Ford, P.J.; Seymour, G.J. Periodontal disease and systemic health: current status. Australian dental journal 2009, 54, S62-S69. [CrossRef]
- Tavares, M.D.M.D.M.P.H.; Lindefjeld Calabi, K.A.D.M.D.; San Martin, L.D.D.S.P.M. Systemic Diseases and Oral Health. The Dental clinics of North America 2014, 58, 797-814. [CrossRef]
- Varoni, E.M.; Rimondini, L. Oral Microbiome, Oral Health and Systemic Health: A Multidirectional Link. Biomedicines 2022, 10, 186. [CrossRef]
- Beukers, N.G.F.M.; van der Heijden, G.J.M.G.; van Wijk, A.J.; Loos, B.G. Periodontitis is an independent risk indicator for atherosclerotic cardiovascular diseases among 60 174 participants in a large dental school in the Netherlands. Journal of epidemiology and community health (1979) 2017, 71, 37-42. [CrossRef]
- Desvarieux, M.; Demmer, R.T.; Rundek, T.; Boden-Albala, B.; Jacobs, D.R.; Papapanou, P.N.; Sacco, R.L. Relationship Between Periodontal Disease, Tooth Loss, and Carotid Artery Plaque: The Oral Infections and Vascular Disease Epidemiology Study (INVEST). Stroke (1970) 2003, 34, 2120-2125. [CrossRef]
- Elter, J.R.; Champagne, C.M.E.; Offenbacher, S.; Beck, J.D. Relationship of Periodontal Disease and Tooth Loss to Prevalence of Coronary Heart Disease. Journal of periodontology (1970) 2004, 75, 782-790. [CrossRef]
- Friedewald, V.E.; Kornman, K.S.; Beck, J.D.; Genco, R.; Goldfine, A.; Libby, P.; Offenbacher, S.; Ridker, P.M.; Van Dyke, T.E.; Roberts, W.C. The American Journal of Cardiology and Journal of Periodontology Editors' Consensus: Periodontitis and Atherosclerotic Cardiovascular Disease. Journal of periodontology (1970) 2009, 80, 1021-1032. [CrossRef]
- Borgnakke, W.S.; Yl€ostalo, P.V.; Taylor, G.W.; Genco, R.J. Effect of periodontal disease on diabetes: systematic review of epidemiologic observational evidence. Journal of periodontology (1970) 2013, 84, S135-S152. [CrossRef]
- Iwasaki, M.; Taylor, G.W.; Awano, S.; Yoshida, A.; Kataoka, S.; Ansai, T.; Nakamura, H. Periodontal disease and pneumonia mortality in haemodialysis patients: A 7-year cohort study. Journal of clinical periodontology 2018, 45, 38-45. [CrossRef]
- Scannapieco, F.A.; Mylotte, J.M. Relationships Between Periodontal Disease and Bacterial Pneumonia. Journal of periodontology (1970) 1996, 67, 1114-1122. [CrossRef]
- Anson, T.J. The bioarchaeology of the St. Mary's free ground burials : reconstruction of colonial South Australian lifeways. Thesis (Ph.D.)--University of Adelaide, Dept. of Anatomical Sciences, 2004., 2004.
- F. Donald. Pate; Teghan. Lucas; Tim. J. Anson; Maciej. Henneberg. Bioarchaeology of a mid-late 19th century anglican community : St Mary's cemetery, Adelaide, South Australia. Acta Palaeomedica: International Journal of Palaeloe Medicine 2021, 2. [CrossRef]
- Gurr, A.; Higgins, D.; Henneberg, M.; Kumaratilake, J.; O’Donnell, M.B.; McKinnon, M.; Hall, K.A.; Brook, A.H. Investigating the dentoalveolar complex in archaeological human skull specimens: additional findings with Large Volume Micro-CT compared to standard methods. International journal of osteoarchaeology 2023. [CrossRef]
- Nikon Metrology. Products: X-ray and CT Technology: X-ray and CT systems: 225kV and 320kV CT inspection and metrology. Available online: https://www.nikonmetrology.com/de/roentgen-und-ct-technik/x-ray-ct-syteme-225kv-und-320kv-ct-inspektion-und-messtechnik (accessed on 20.06.).
- Bruker. Position, Scan, Reconstruct and Analyze. Available online: https://www.bruker.com/en/products-and-solutions/microscopes/3d-x-ray-microscopes/skyscan-1272.html (accessed on 22.06.).
- Al-Mutairi, R.; Liversidge, H.; Gillam, D.G. Prevalence of Moderate to Severe Periodontitis in an 18-19th Century Sample-St. Bride's Lower Churchyard (London, UK). Dentistry journal 2022, 10, 56. [CrossRef]
- FDI World Dental Federation. FDI Two-Digit Notation. Available online: http://www.fdiworldental.org/resources/5_0notation.html (accessed on 22.06).
- Leatherman, G. Two-digit system of designating teeth—FDI submission. Australian dental journal 1971, 16, 394-394. [CrossRef]
- Planmeca. Intraoral X-ray unit. Available online: https://www.planmeca.com/imaging/intraoral-imaging/intraoral-x-ray-unit/ (accessed on 10.06).
- Miles, A.E.W. Assessment of the Ages of a Population of Anglo-Saxons from Their Dentitions1. Proceedings of the Royal Society of Medicine 1962, 55, 881-886.
- Molnar, S. Human tooth wear, tooth function and cultural variability. American Journal of Physical Anthropology 1971, 34, 175-189. [CrossRef]
- ThermoFisher Scientific. 3D Visulaization & Analysis Software: Amiro-Avizo. Available online: https://www.thermofisher.com/au/en/home/industrial/electron-microscopy/electron-microscopy-instruments-workflow-solutions/3d-visualization-analysis-software.html (accessed on.
- Connell, B.; Rauxloh, P. A Rapid Method for Recording Human Skeletal Data; Museum of London: London, 2003.
- Powers, N. Human Osteology Method Statement; Museum of London: London, 2012.
- Brothwell, D.R. Digging up bones : the excavation, treatment and study of the human skeletal remains; British Museum Natural History: London, 1963.
- Efremov, J.A. Taphonomy: New Branch of Paleontology. American Geologist 1940, 74, 81-93, doi:http://www.astro.spbu.ru/staff/serg/interests/literature/efremov/taphartthumb.html..
- Garot, E.; Couture-Veschambre, C.; Manton, D.; Beauval, C.; Rouas, P. Analytical evidence of enamel hypomineralisation on permanent and primary molars amongst past populations. Scientific reports 2017, 7, 1712-1710. [CrossRef]
- Garot, E.; Couture-Veschambre, C.; Manton, D.; Bekvalac, J.; Rouas, P. Differential diagnoses of enamel hypomineralisation in an archaeological context: A postmedieval skeletal collection reassessment. International journal of osteoarchaeology 2019, 29, 747-759. [CrossRef]
- Araújo, M.G.; Silva, C.O.; Misawa, M.; Sukekava, F. Alveolar socket healing: what can we learn? Periodontology 2000 2015, 68, 122-134. [CrossRef]
- Hillson, S. Dental Anthropology; Cambridge University Press: Cambridge, 1996.
- International Organisation for Standardization; American National Standard; American Dental Association. Specification No. 3950. Designation System for Teeth and Areas of the Oral Cavity. Available online: https://webstore.ansi.org/preview-pages/ADA/preview_ISO+ANSI+ADA+Specification+No.+3950-2010.pdf (accessed on 22.06).
- Kinaston, R.; Willis, A.; Miszkiewicz, J.J.; Tromp, M.; Oxenham, M.F. The Dentition: Development, Disturbances, Disease, Diet, and Chemistry. In Ortner's Identification of Paleopathological Conditions in Human Skeletal Remains, Third ed.; Buikstra, J.E., Ed.; Academic Press: London, 2019.
- Pitts, N.B.; Ekstrand, K.R. International Caries Detection and Assessment System (ICDAS) and its International Caries Classification and Management System (ICCMS) - methods for staging of the caries process and enabling dentists to manage caries. Community dentistry and oral epidemiology 2013, 41, e41-e52. [CrossRef]
- Ogden, A.R.; Pinhasi, R.; White, W.J. Gross enamel hypoplasia in molars from subadults in a 16th-18th century London graveyard. American journal of physical anthropology 2007, 133, 957-966. [CrossRef]
- Perschbacher, S. Periodontal Diseases. In Oral Radiology: Prinicplas and Interpretations, White, S.C., Pharoah, M.J., Eds.; Elsvier: St Louis, 2014; pp. 299-313.
- Riga, A.; Begni, C.; Sala, S.; Erriu, S.; Gori, S.; Moggi-Cecchi, J.; Mori, T.; Dori, I. Is root exposure a good marker of periodontal disease? Bulletin of the International Association of Paleodontology 2021, 15, 21-30.
- Brook, A.H.; Elcock, C.; Hallonsten, A.L.; Poulsen, S.; Andreasen, J.; Koch, G.; Yeung, C.A.; Dosanjh, T. The development of a new index to measure enamel defects. In Dental Morphology, Brook, A.H., Ed.; Sheffield Academic Press: Sheffield, 2001; pp. 59-66.
- Elcock, C.; Lath, D.L.; Luty, J.D.; Gallagher, M.G.; Abdellatif, A.; Bäckman, B.; Brook, A.H. The new Enamel Defects Index: testing and expansion. European journal of oral sciences 2006, 114 Suppl 1, 35.
- Colombo, A.; Ortenzio, L.; Bertrand, B.; Coqueugniot, H.; KnüSel, C.J.; Kahlon, B.; Brickley, M. Micro-computed tomography of teeth as an alternative way to detect and analyse vitamin D deficiency. Journal of Archaeological Science: Reports 2019, 23, 390-395. [CrossRef]
- Veselka, B.; Brickley, M.B.; D'Ortenzio, L.; Kahlon, B.; Hoogland, M.L.P.; Waters-Rist, A.L. Micro-CT assessment of dental mineralization defects indicative of vitamin D deficiency in two 17th-19th century Dutch communities. Am J Phys Anthropol 2019, 1-10. [CrossRef]
- StataCorp LLC. Stata, Home: Products: New in Stata. Available online: https://www.stata.com/new-in-stata/ (accessed on 02.12.2022).
- Landis, J.R.; Koch, G.G. The Measurement of Observer Agreement for Categorical Data. Biometrics 1977, 33, 159-174. [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. Journal of chiropractic medicine 2016, 15, 155-163. [CrossRef]
- Higginbotham, E.; Associates Pty Ltd. Report on the excavation of the Cadia Cemetery, Cadia Road, Cadia, NSW, 1997-1998; 2002 2002.
- Donlon, D.; Griffin, R.; Casey, M. The Old Sydney Burial Ground: clues from the dentition about the ancestry, health and diet of the first British settlers of Australia. Australasian historical archaeology : journal of the Australasian Society for Historical Archaeology 2017, 35, 43-53.
- Buckley, H.R.; Roberts, P.; Kinaston, R.; Petchey, P.; King, C.; Domett, K.; Snoddy, A.M.; Matisoo-Smith, E. Living and dying on the edge of the Empire: a bioarchaeological examination of Otago's early European settlers. Journal of the Royal Society of New Zealand 2020, ahead-of-print, 1-27. [CrossRef]
- WORD database. Museum of London. Available online: https://www.museumoflondon.org.uk/collections/other-collection-databases-and-libraries/centre-human-bioarchaeology/osteological-database/post-medieval-cemeteries/post-medieval-cemetery-data (accessed on 23/09/2022).
- Ioannou, S.; Henneberg, M.; Henneberg, R.J.; Anson, T. Diagnosis of Mercurial Teeth in a Possible Case of Congenital Syphilis and Tuberculosis in a 19th Century Child Skeleton. Journal of Anthropology (2010) 2015, 2015, 1-11. [CrossRef]
- Smith, B.H. Patterns of molar wear in hunter–gatherers and agriculturalists. American Journal of Physical Anthropology 1984, 63, 39-56. [CrossRef]
- Littleton, J.; Frohlich, B. Fish-eaters and farmers: Dental pathology in the Arabian Gulf. American journal of physical anthropology 1993, 92, 427-447. [CrossRef]
- Scott, E.C. Dental wear scoring technique. American journal of physical anthropology 1979, 51, 213-217. [CrossRef]
- Buikstra, J.E.; Ubelaker, D.H.; Haas, J.; Aftandilian, D.; Field Museum of Natural, H. Standards for data collection from human skeletal remains : proceedings of a seminar at the Field Museum of Natural History, organized by Jonathan Haas / volume editors, Jane E. Buikstra and Douglas H. Ubelaker, assistant editor, David Aftandilian ; contributions by D. Aftandilian ... [et al.]; Fayetteville, Ark. : Arkansas Archeological Survey: Fayetteville, Ark., 1994.
- Atar, M.; Körperich, E.J. Systemic disorders and their influence on the development of dental hard tissues: A literature review. Journal of Dentistry 2010, 38, 296-306. [CrossRef]
- Seow, K. A study of the development of the permanent dentition of very low birth weight children. American Academy of Pediatric Dentistry 1996, 18.
- Seow, W.K. The effect of medical therapy on dentin formation in vitamin D-resistant rickets. Pediatric dentistry 1991, 13, 97-102.
- Verma, M.; Verma, N.; Sharma, R.; Sharma, A. Dental age estimation methods in adult dentitions: An overview. Journal of Forensic Dental Sciences 2019, 11, 57-63. [CrossRef]
- The South Australia Register. Dreadful Accident- Coroner’s Inquest. The South Australian Register March 3 1859 1859, p. 4.
- Selwitz, R.H.D.; Ismail, A.I.D.; Pitts, N.B.B.D.S. Dental caries. The Lancet (British edition) 2007, 369, 51-59. [CrossRef]
- Broers, D.L.M.; Dubois, L.; de Lange, J.; Welie, J.V.M.; Brands, W.G.; Bruers, J.J.M.; de Jongh, A. Financial, psychological, or cultural reasons for extracting healthy or restorable teeth. The Journal of the American Dental Association (1939) 2022, 153, 761-768.e763. [CrossRef]
- Gordon, S.C.; Kaste, L.M.; Barasch, A.; Safford, M.M.; Foong, W.C.; ElGeneidy, A. Prenuptial Dental Extractions in Acadian Women: First Report of a Cultural Tradition. Journal of women's health (Larchmont, N.Y. 2002) 2011, 20, 1813-1818. [CrossRef]
- Russell, S.L.; Gordon, S.; Lukacs, J.R.; Kaste, L.M. Sex/Gender differences in tooth loss and edentulism: historical perspectives, biological factors, and sociologic reasons. The Dental clinics of North America 2013, 57, 317-337. [CrossRef]
- Johnson, N.W.; Colman, G. Dental Caries. In A Comprehensive Guide to Clinical Dentistry, Rowe, A.H.R., Ed.; Class Publishing: London, 1989; pp. 112-159.
- Drummond, J.C.; Wilbraham, A. The Englishman's food : a history of five centuries of English diet, Rev. / with a new chapter by Dorothy Hollingsworth ; and a preface by Norman C. Wright. ed.; Jonathan Cape: London, 1958.
- Holloway, P.J.; Moore, W.J. The role of sugar in the aetiology of dental caries: 1. Sugar and the antiquity of dental caries. Journal of dentistry 1983, 11, 189-190. [CrossRef]
- Mant, M.; Roberts, C. Diet and Dental Caries in Post-Medieval London. International journal of historical archaeology 2015, 19, 188-207. [CrossRef]
- Miller, I. A Dangerous Revolutionary Force Amongst Us: Conceptualizing Working-Class Tea Drinking in the British Isles, c. 1860-1900. Cultural and social history 2013, 10, 419-438. [CrossRef]
- Peter, G. Black poison or beneficial beverage?: Tea consumption in colonial Australia. Journal of Australian colonial history 2015, 17, 23-44. [CrossRef]
- Wilkinson, J. Adelaide Commercial Report. South Australian Register 16th July 1853, p. 2.
- Winter, G.B. Sugar and Dental Caries. British Medical Journal 1964, 2, 1595-1595. [CrossRef]
- Moynihan, P.; Petersen, P.E. Diet, nutrition and the prevention of dental diseases. Public health nutrition 2004, 7, 201-226. [CrossRef]
- Dias, G.; Tayles, N. 'Abscess cavity'-a misnomer. International journal of osteoarchaeology 1997, 7, 548-554. [CrossRef]
- Albandar, J.M.; Streckfus, C.F.; Adesanya, M.R.; Winn, D.M. Cigar, Pipe, and Cigarette Smoking as Risk Factors for Periodontal Disease and Tooth Loss. Journal of periodontology (1970) 2000, 71, 1874-1881. [CrossRef]
- Arno, A.; Schei, O.; Lovdal, A.; Wæehaug, J. Alveolar Bone Loss as a Function of Tobacco Consumption. Acta odontologica Scandinavica 1959, 17, 3-10. [CrossRef]
- Johnson, G.K. Position Paper: Tobacco Use and the Periodontal Patient. Journal of periodontology (1970) 1999, 70, 1419-1427. [CrossRef]
- Krall, E.A.; Garvey, A.J.; Garcia, R.I. ALVEOLAR BONE LOSS AND TOOTH LOSS IN MALE CIGAR AND PIPE SMOKERS. The Journal of the American Dental Association (1939) 1999, 130, 57-64. [CrossRef]
- Rivera-Hidalgo, F. Smoking and periodontal disease. Periodontology 2000 2003, 32, 50-58. [CrossRef]
- Wilkinson, G.B. South Australia, its advantages and its resources : being a description of that colony, and a manual of information for emigrants / by George Blakiston Wilkinson; London : J. Murray: London, 1848.
- Ioannou, S.; Henneberg, M. Dental signs attributed to congenital syphilis and its treatments in the Hamann-Todd Skeletal Collection. Anthropological review (Poznań, Poland) 2017, 80, 449-465. [CrossRef]
- Ioannou, S.; Sassani, S.; Henneberg, M.; Henneberg, R.J. Diagnosing congenital syphilis using Hutchinson's method: Differentiating between syphilitic, mercurial, and syphilitic-mercurial dental defects. American Journal of Physical Anthropology 2016, 159, 617-629. [CrossRef]
- Fearne, J.M.; Bryan, E.M.; Elliman, A.M.; Brook, A.H.; Williams, D.M. Enamel defects in the primary dentition of children born weighing less than 2000 g. British dental journal 1990, 168, 433-437. [CrossRef]
- Nikiforuk, G.; Fraser, D. Etiology of Enamel Hypoplasia and Interglobular Dentin: The Roles of Hypocalcemia and Hypophosphatemia. Metabolic Bone Disease and Related Research 1979, 2, 17-23. [CrossRef]
- Jump, E.B. Changes within the mandible and teeth in a case of rickets. American journal of orthodontics and oral surgery 1939, 25, 484-490. [CrossRef]
- Brook, A.H.; Smith, J.M. Hypoplastic enamel defects and environmental stress in a homogeneous Romano-British population. Eur. J. Oral Sci. 2006, 114, 370-374.
- Winter, G.B.; Brook, A.H. Enamel Hypoplasia and Anomalies of the Enamel. Dental Clinics of North America 1975, 19, 3-24. [CrossRef]
- Gotfredsen, K.; Walls, A.W.G. What dentition assures oral function? Clinical oral implants research 2007, 18, 34-45. [CrossRef]
- Seraj, Z.; Al-Najjar, D.; Akl, M.; Aladle, N.; Altijani, Y.; Zaki, A.; Al Kawas, S. The Effect of Number of Teeth and Chewing Ability on Cognitive Function of Elderly in UAE: A Pilot Study. International journal of dentistry 2017, 2017, 5732748-5732746. [CrossRef]
- Friedewald, V.E.M.D.; Kornman, K.S.D.D.S.P.; Beck, J.D.P.; Genco, R.D.D.S.P.; Goldfine, A.M.D.; Libby, P.M.D.; Offenbacher, S.D.D.S.P.M.; Ridker, P.M.M.D.M.P.H.; Van Dyke, T.E.D.D.S.P.; Roberts, W.C.M.D. The American Journal of Cardiology and Journal of Periodontology Editors' Consensus: Periodontitis and Atherosclerotic Cardiovascular Disease. The American journal of cardiology 2009, 104, 59-68. [CrossRef]
- Scannapieco, F.A.; Torres, G.; Levine, M.J. Salivary alpha-amylase: role in dental plaque and caries formation. Critical reviews in oral biology and medicine 1993, 4, 301-307. [CrossRef]
- Farr, J.N.; Khosla, S. Determinants of bone strength and quality in diabetes mellitus in humans. Bone (New York, N.Y.) 2015, 82, 28-34. [CrossRef]
- Vilaca, T.; Schini, M.; Harnan, S.; Sutton, A.; Poku, E.; Allen, I.E.; Cummings, S.R.; Eastell, R. The risk of hip and non-vertebral fractures in type 1 and type 2 diabetes: A systematic review and meta-analysis update. Bone (New York, N.Y.) 2020, 137, 115457-115457. [CrossRef]
- Carnevale, V.; Romagnoli, E.; D'Erasmo, E. Skeletal involvement in patients with diabetes mellitus. Diabetes/metabolism research and reviews 2004, 20, 196-204. [CrossRef]
- Baker, B.J.; Crane-Kramer, G.; Dee, M.W.; Gregoricka, L.A.; Henneberg, M.; Lee, C.; Lukehart, S.A.; Mabey, D.C.; Roberts, C.A.; Stodder, A.L.W.; et al. Advancing the understanding of treponemal disease in the past and present. American Journal of Physical Anthropology 2020, 171, 5-41. [CrossRef]
- Brickley, M.B.; Ives, R.; Mays, S. The Bioarchaeology of Metabolic Bone Disease; Elsevier Science & Technology: San Diego, 2020.
- Buckberry, J.; Crane-Kramer, G. The dark satanic mills: Evaluating patterns of health in England during the industrial revolution. International journal of paleopathology 2022, 39, 93-108. [CrossRef]
- Steyn, M.; Van der Merwe, L.; Meyer, A. Infectious diseases and nutritional deficiencies in early industrialized South Africa. International Journal of Paleopathology 2021.
- Nally, C. Cross Bones Graveyard: Excavating the Prostitute in Neo-Victorian Popular Culture. Journal of Victorian Culture : JVC 2018, 23, 247-261. [CrossRef]
- Brook, A.H.; Smith, J.M. The Aetiology of Developmental Defects of Enamel: A Prevalence and Family Study in East London, U.K. Connective Tissue Research 1998, 39, 151-156. [CrossRef]
- Skelly, E.J. Processes of Industrialisation Influencing the Human Oral Microbiome. 2019.
Figure 1.
SMB 84 - adult female (age range 50-59 yrs.). Vulcanite base dentures with porcelain teeth. Images show dentures in situ and removed from the maxilla and mandible. (A) Anterior view of the edentulous maxilla and mandible. (B) Left lateral view of the ‘well-made’ dentures with a class one occlusion in the jaw. (C,D) The vulcanite dentures with porcelain teeth – the maxillary denture shows a shield shape suction area on the superior surfaceof the plate. © Angela Gurr.
Figure 1.
SMB 84 - adult female (age range 50-59 yrs.). Vulcanite base dentures with porcelain teeth. Images show dentures in situ and removed from the maxilla and mandible. (A) Anterior view of the edentulous maxilla and mandible. (B) Left lateral view of the ‘well-made’ dentures with a class one occlusion in the jaw. (C,D) The vulcanite dentures with porcelain teeth – the maxillary denture shows a shield shape suction area on the superior surfaceof the plate. © Angela Gurr.
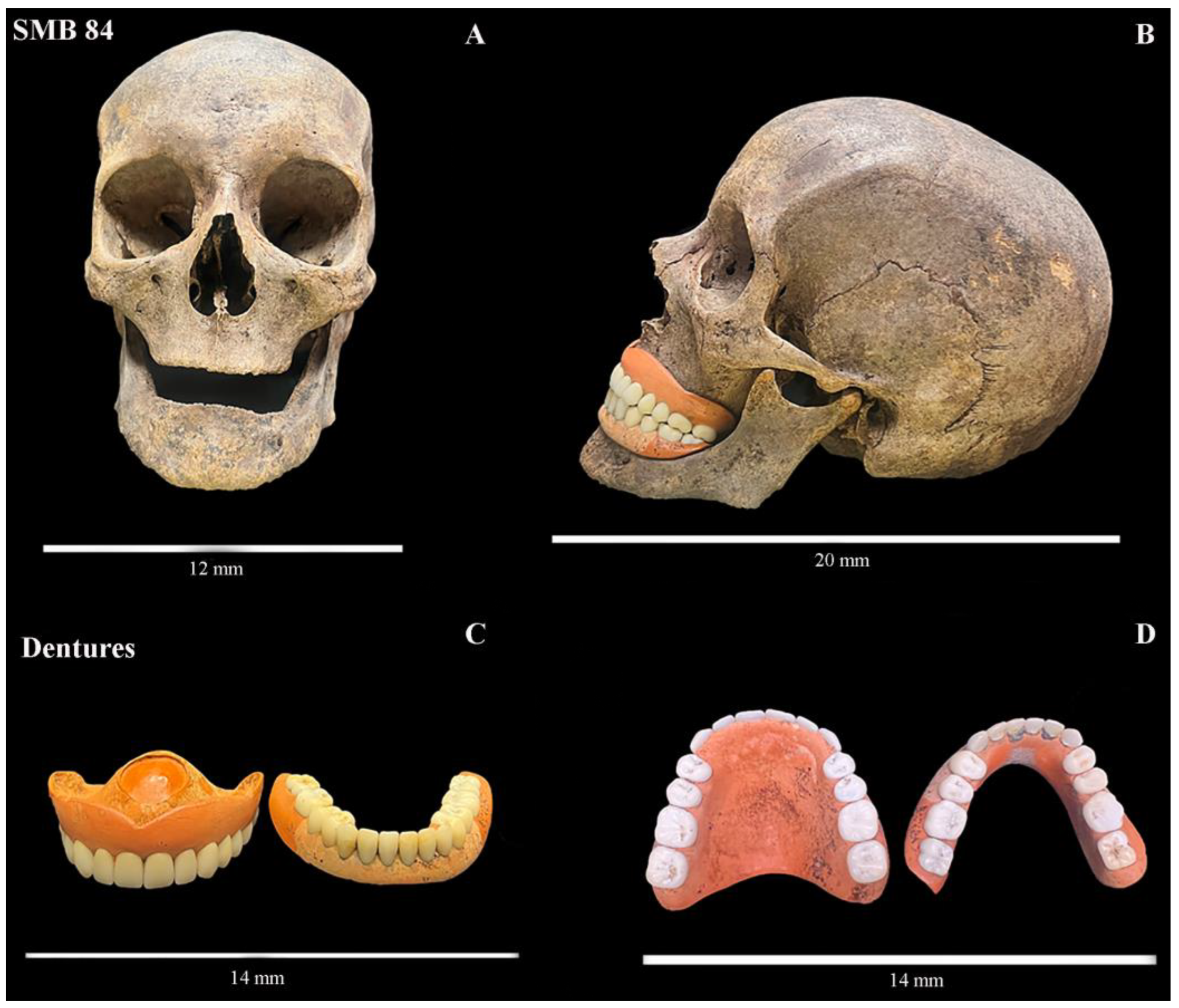
Figure 2.
SMB 72. Adult male (age range 40-49 yrs.). (A) Left lateral view of the dentition in-situ in the skull. Yellow circle highlights a pattern of tooth wear often referred to as a ‘pipe notch’. The teeth have become worn from the movement of and holding a smoking pipe between the teeth over an extended period of time. (B) A close-up view of the left maxillary and mandibular permanent lateral incisors and canines opposing each other. The yellow circle shows a clear semi-circular tooth wear pattern. © Angela Gurr.
Figure 2.
SMB 72. Adult male (age range 40-49 yrs.). (A) Left lateral view of the dentition in-situ in the skull. Yellow circle highlights a pattern of tooth wear often referred to as a ‘pipe notch’. The teeth have become worn from the movement of and holding a smoking pipe between the teeth over an extended period of time. (B) A close-up view of the left maxillary and mandibular permanent lateral incisors and canines opposing each other. The yellow circle shows a clear semi-circular tooth wear pattern. © Angela Gurr.
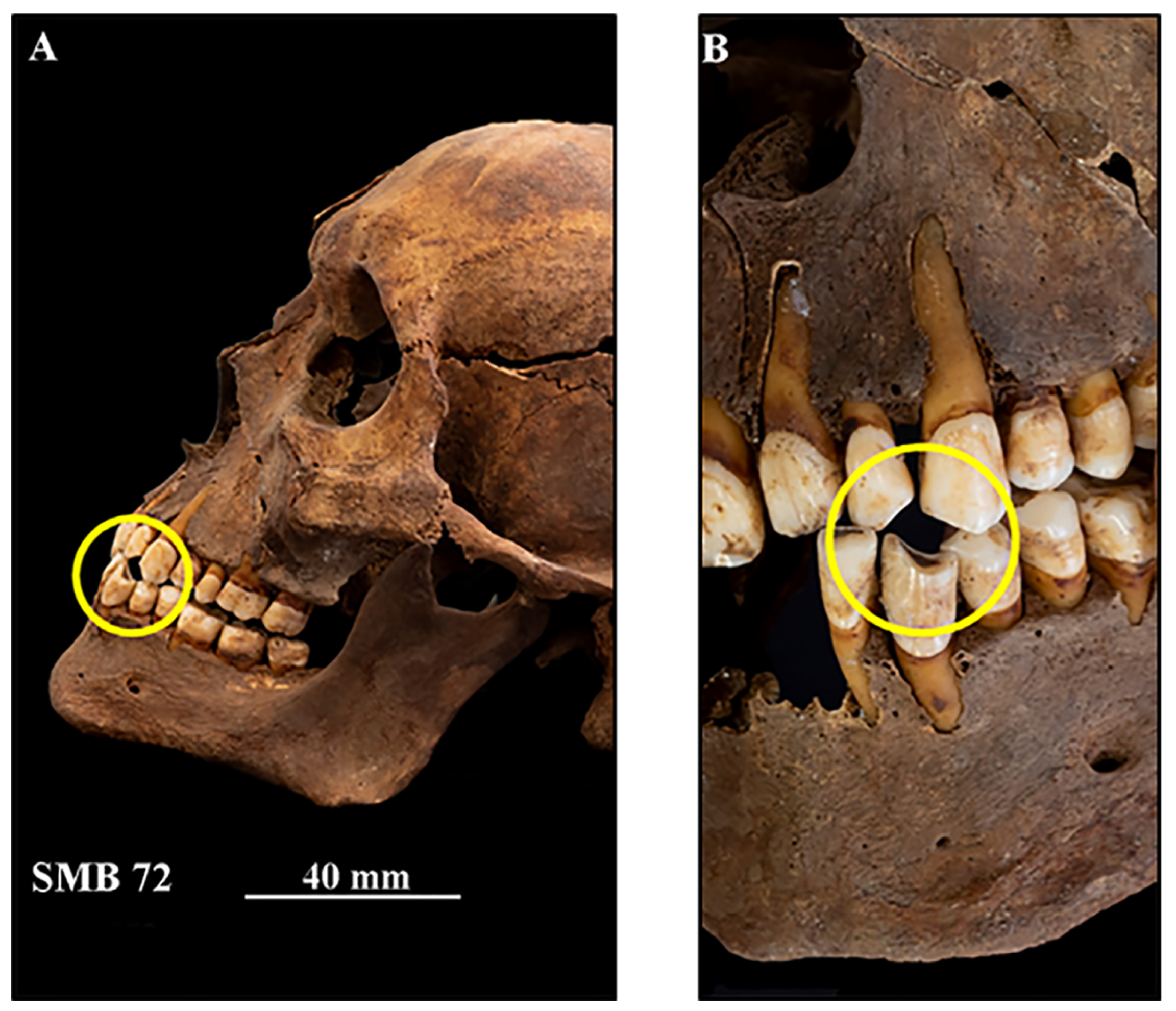
Figure 3.
SMB 79, subadult (dental age range 15.5-16.5 years (+/-1 year) – skeletal assessment age range 16-18 yrs.). (A,B) Yellow circle shows caries in the mesial occlusal surface of the lower right permanent first molar (M1- FDI number 46). Yellow arrows indicate the periapical cavity and opening in the buccal surface of the alveolar bone. (C) Periapical dental radiograph of the mandible – yellow arrows show the extent of the cavity surrounding the roots of the M1 molar, and the ‘opening’ in the alveolar bone adjacent to the apex of the mesial root. The yellow circle highlights caries that extended to involve the pulp. © Angela Gurr.
Figure 3.
SMB 79, subadult (dental age range 15.5-16.5 years (+/-1 year) – skeletal assessment age range 16-18 yrs.). (A,B) Yellow circle shows caries in the mesial occlusal surface of the lower right permanent first molar (M1- FDI number 46). Yellow arrows indicate the periapical cavity and opening in the buccal surface of the alveolar bone. (C) Periapical dental radiograph of the mandible – yellow arrows show the extent of the cavity surrounding the roots of the M1 molar, and the ‘opening’ in the alveolar bone adjacent to the apex of the mesial root. The yellow circle highlights caries that extended to involve the pulp. © Angela Gurr.
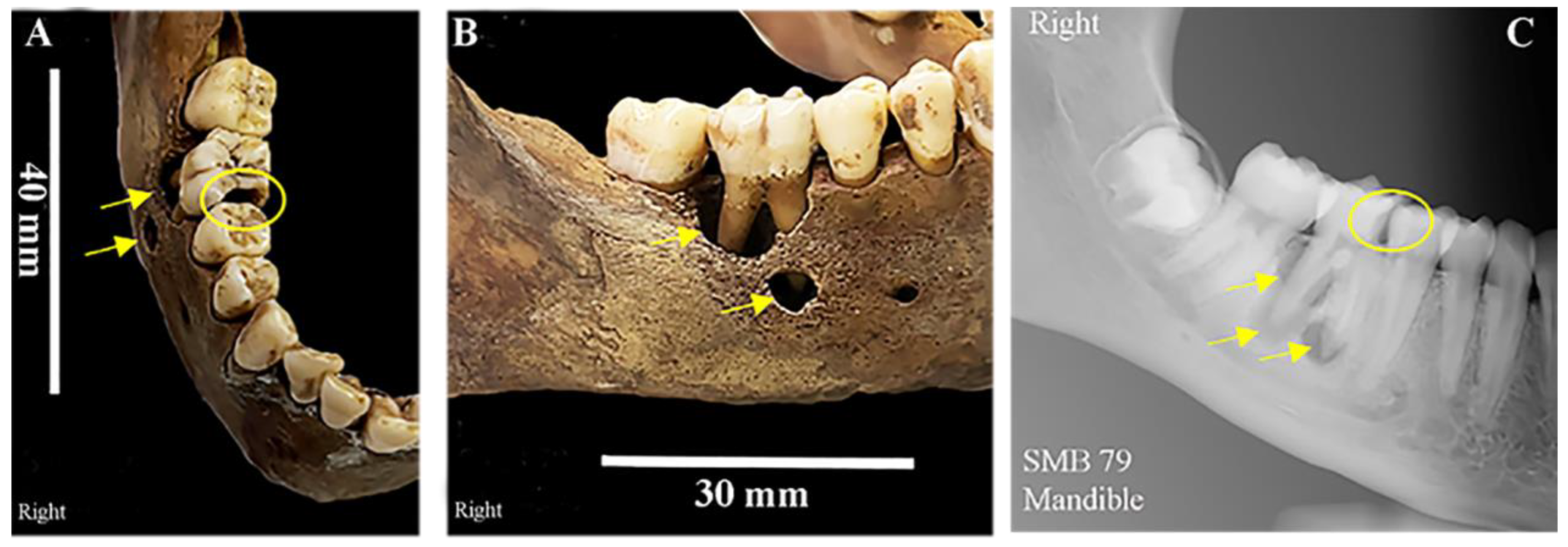
Figure 4.
SMB 58 – Infant (dental age range 1-1.5 +/-3 months, skeletal assessment age range 0-2. years of age). (Cranium - Large Volume Micro-CT scanned at 35µm/pixel & mandible at 21µm/pixel, Table S2). (A,B,D) Created using Avizo 9 software [30], the bone density threshold level was manipulated/ reduced to reveal the denser structures of the developing teeth within the alveolar bone. (A) Buccal view of the semi-erupted upper right primary canine, and primary second molar, the first primary molar was lost post-mortem. Yellow circles show teeth affected by enamel hypoplastic defects, including the developing crown of the permanent upper right first molar within the alveolar bone. (B) Lingual/palatal view of the upper left primary first and second molars, and the crown of the permanent first molar within the alveola. Yellow arrows highlight enamel hypoplastic defects. (C) lateral view of the mandibular primary dentition. Yellow arrows indicate some enamel hypoplastic defects on the primary canine, first molar, and erupting second molar. (D) As with image B, the bone density threshold level was changed to show the developing teeth within the alveola –yellow arrows enamel hypoplastic defects the erupted primary teeth, semi-erupted primary second molar and the cusps of the developing crown of the permanent first molar. © Angela Gurr.
Figure 4.
SMB 58 – Infant (dental age range 1-1.5 +/-3 months, skeletal assessment age range 0-2. years of age). (Cranium - Large Volume Micro-CT scanned at 35µm/pixel & mandible at 21µm/pixel, Table S2). (A,B,D) Created using Avizo 9 software [30], the bone density threshold level was manipulated/ reduced to reveal the denser structures of the developing teeth within the alveolar bone. (A) Buccal view of the semi-erupted upper right primary canine, and primary second molar, the first primary molar was lost post-mortem. Yellow circles show teeth affected by enamel hypoplastic defects, including the developing crown of the permanent upper right first molar within the alveolar bone. (B) Lingual/palatal view of the upper left primary first and second molars, and the crown of the permanent first molar within the alveola. Yellow arrows highlight enamel hypoplastic defects. (C) lateral view of the mandibular primary dentition. Yellow arrows indicate some enamel hypoplastic defects on the primary canine, first molar, and erupting second molar. (D) As with image B, the bone density threshold level was changed to show the developing teeth within the alveola –yellow arrows enamel hypoplastic defects the erupted primary teeth, semi-erupted primary second molar and the cusps of the developing crown of the permanent first molar. © Angela Gurr.
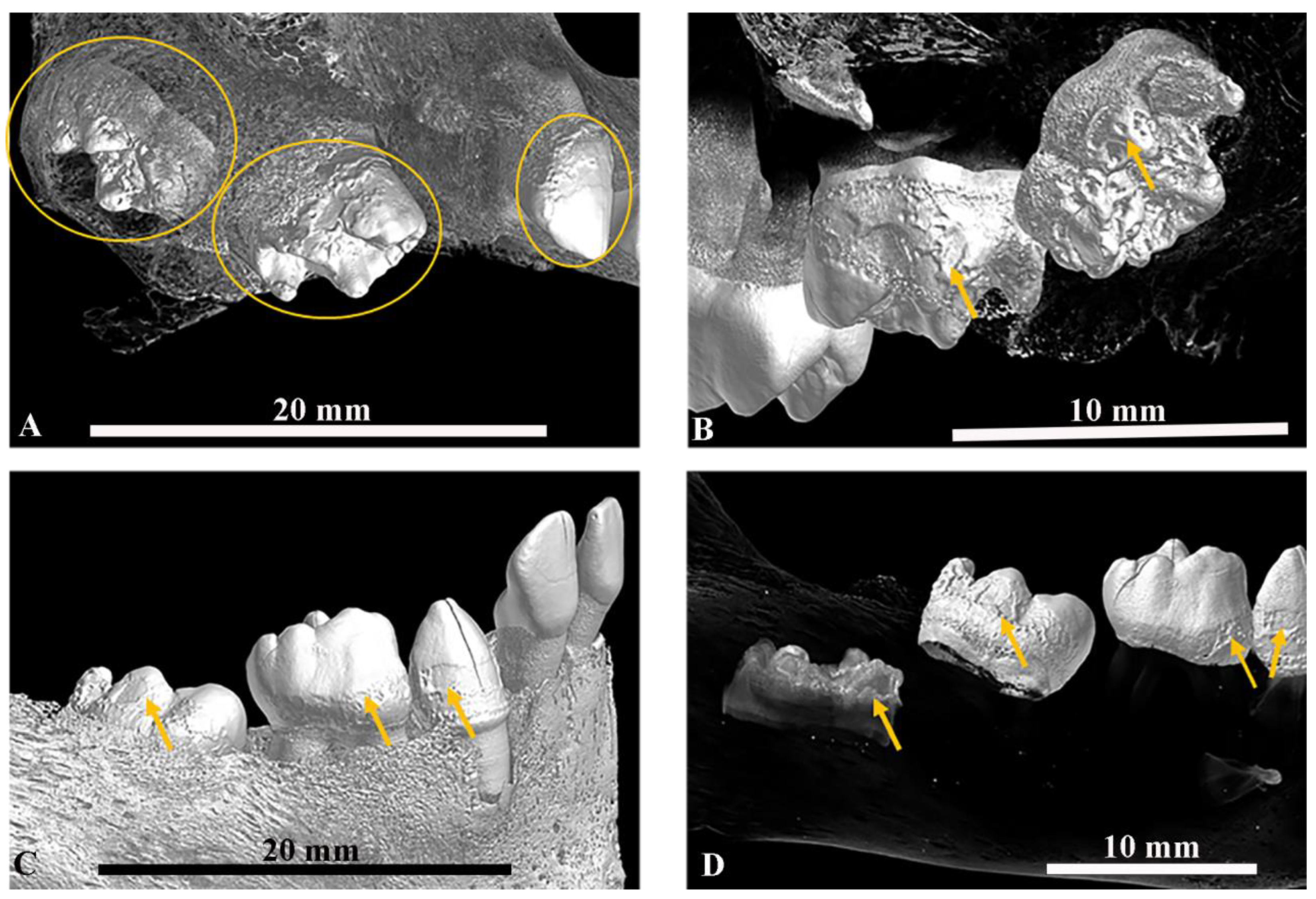
Figure 5.
(A–D) SMB 58 – infant (dental age range 1-1.5 +/-3 months, skeletal age range 0-2 years of age). Large Volume (LV) Micro-CT scanned at 21µm/pixel- (Table S2). (A) Superior/posterior view of the mandible and primary teeth. The left side of the jaw and teeth are shown in 3D and the right side is a 2D LV micro-CT slice of the teeth - yellow lines show interglobular dentine (IGD). (B) Lateral view of the mandibular primary dentition – red lines show enamel hypoplastic (EH) defects. (C,D) Sagittal slices from LV micro-CT scans of the mandibular dentition (Image C - FDI tooth numbers 83 & 84, Image D – FDI teeth 84 & 85). Yellow lines show areas of IGD in the internal structure of the teeth and the red lines show EH defects on the external structures of the teeth. (E,F) SMB 73- adult male, (skeletal age range: 30-39 years). Individual tooth samples scanned with the Small Volume (SV) Micro-CT system at 9µm/pixel- (Table S3). (E) FDI tooth number 16 and (F) FDI tooth number 23. Both images - yellow lines show areas of IGD and red lines show EH defects in the teeth and at a similar level. All images were created using Avizo software [30] Volren or Orthoslice functions from reconstructed L V and SV Micro-CT scan data. © Angela Gurr.
Figure 5.
(A–D) SMB 58 – infant (dental age range 1-1.5 +/-3 months, skeletal age range 0-2 years of age). Large Volume (LV) Micro-CT scanned at 21µm/pixel- (Table S2). (A) Superior/posterior view of the mandible and primary teeth. The left side of the jaw and teeth are shown in 3D and the right side is a 2D LV micro-CT slice of the teeth - yellow lines show interglobular dentine (IGD). (B) Lateral view of the mandibular primary dentition – red lines show enamel hypoplastic (EH) defects. (C,D) Sagittal slices from LV micro-CT scans of the mandibular dentition (Image C - FDI tooth numbers 83 & 84, Image D – FDI teeth 84 & 85). Yellow lines show areas of IGD in the internal structure of the teeth and the red lines show EH defects on the external structures of the teeth. (E,F) SMB 73- adult male, (skeletal age range: 30-39 years). Individual tooth samples scanned with the Small Volume (SV) Micro-CT system at 9µm/pixel- (Table S3). (E) FDI tooth number 16 and (F) FDI tooth number 23. Both images - yellow lines show areas of IGD and red lines show EH defects in the teeth and at a similar level. All images were created using Avizo software [30] Volren or Orthoslice functions from reconstructed L V and SV Micro-CT scan data. © Angela Gurr.
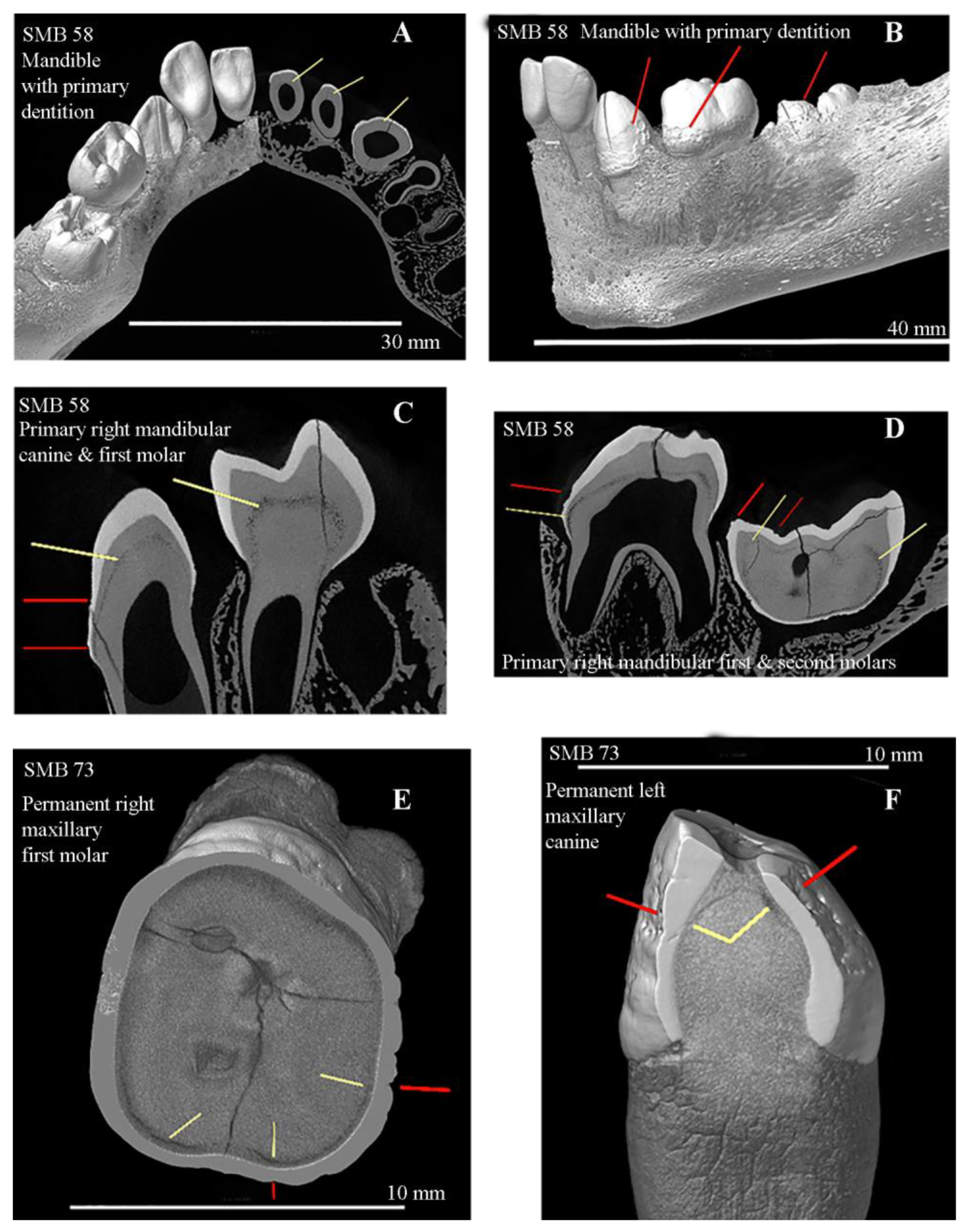
Table 2.
The number of each tooth type for each category of tooth wear scored [29] for the permanent dentition of the adults from the St Mary’s sample, with the number of each tooth type for each category of tooth wear scored [29].
| Type of Permanent Tooth | Number of Teeth with Cat. 4 |
Number of Teeth with Cat. 5 |
Number of Teeth with Cat. 6 |
Number of Teeth with Cat. 7 |
Number of Teeth with Cat. 8 |
Total Number of Each Tooth Type |
|---|---|---|---|---|---|---|
| Cent. Incisor | 13 | 13 | 0 | 0 | 0 | 26 |
| Lat Incisor | 22 | 18 | 0 | 0 | 0 | 40 |
| Canine | 16 | 14 | 3 | 0 | 0 | 33 |
| P1 | 8 | 6 | 0 | 1 | 0 | 15 |
| P2 | 9 | 1 | 2 | 1 | 0 | 13 |
| M1 | 7 | 1 | 4 | 0 | 0 | 12 |
| M2 | 7 | 3 | 3 | 1 | 0 | 14 |
| M3 | 1 | 1 | 3 | 0 | 1 | 6 |
|
Total |
||||||
| 83 | 57 | 15 | 3 | 0 | ||
Notes: Cent. = central, Lat. = lateral, P1 = first premolar, P2 = second premolar, M1 = first permanent molar, M2 = second permanent molar, M3 = third permanent molar. Cat. = category of tooth wear [29].
Table 3.
Number and percentage of carious lesions identified for individuals from the St Mary’s sample, with identification of teeth lost in life (antemortem).
Table 3.
Number and percentage of carious lesions identified for individuals from the St Mary’s sample, with identification of teeth lost in life (antemortem).
| St Mary’s ID |
Age Range |
Sex | Total Number of Teeth Present |
Permanent or Primary Dentition |
* Total Number of Teeth Affected by Carious Lesions |
Percentage of teeth Affected by carious Lesions |
Total Number of carious lesions Present |
** Antemortem Tooth Loss FDI Notation Number/s of Teeth Lost in Life |
|---|---|---|---|---|---|---|---|---|
| SMB 19 | 6-9 | U | 22 | 7 primary 15 Permanent |
2 | 9% | 3 | None |
| SMB 70 | 6-9 | U | 8 | 2 primary 6 Permanent |
2 | 25% | 3 | None |
| SMB 28 | 10-14 | U | 26 | Permanent | 1 | 4% | 2 | None |
| SMB 79 | 15-18 | U | 25 | Permanent | 8 | 32% | 13 | 36 |
| SMB 05 | 20-30 | F | 6 | Permanent | 4 | 67% | 8 | 11, 12, 13, 14, 15, 16, 18, 21, 22, 23, 24, 25, 26, 27,28, 36, 37, 38, 45, 46, 47, 48 |
| SMB 53C | 30-39 | F | 9 | Permanent | 8 | 89% | 12 | 15, 16, 17, 18, 24, 25, 27, 28, 31, 35, 36, 37, 38, 41, 44, 47, 48 |
| SMB 66B | 30-39 | F | 17 | Permanent | 11 | 65% | 16 | 11 (root only), 13, 16, 18, 26, 28, 36, 37, 38, 46, 47, 48 |
| SMB 73 | 30-39 | M | 19 | Permanent | 17 | 89% | 39 | 15, 17, 18, 24, 26, 27, 36, 37, 38, 46, 47, 48 |
| SMB 06 | 40-49 | M | 24 | Permanent | 12 | 50% | 19 | 28, 34, 35, 36, 38, 48 |
| SMB 09 | 1/21 | M | 22 | Permanent | 1 | 5% | 11 | 11, 27, 38 |
| SMB 57 | 40-49 | M | 25 | Permanent | 8 | 32% | 12 | 25, 28 |
| SMB 61 | 40-49 | F | 7 | Permanent | 4 | 57% | 5 | 11, 12, 15, 16, 17, 18, 21, 22, 24, 26, 27, 28, 334,35, 36, 37,38, 43, 45, 46, 47, 48 |
| SMB 72 | 40-49 | M | 29 | Permanent | 7 | 24% | 15 | None |
| SMB 78 | 40-49 | M | 4 | Permanent | 2 | 50% | 3 | 11, 12, 15, 16, 17, 18, 21, 22, 23, 24, 25, 26, 27, 28, 31, 32, 36, 37, 38, 41, 42, 43, 44, 45, 46, 47, 48 |
| SMB 83 | 40-49 | M | 16 | Permanent | 6 | 38% | 7 | 16, 18, 26, 36, 45, 46 |
| SMB 85 | 40-49 | M | 2 | Permanent | 1 | 50% | 1 | 11, 12, 13, 14, 15, 16, 17, 18, 23, 24, 25, 26, 27, 28, 31, 35, 36, 37, 38, 41, 43, 44, 45, 46, 47, 48 |
| SMB 14 | 50-59 | M | 2 | Permanent | 1 | 50% | 1 | 12, 14, 15, 16, 17, 18, 21, 22, 24, 25, 26, 27, 28, 34, 36, 37, 38, 46, 48 |
| SMB 23 | 50-59 | M | 21 | Permanent | 20 | 95% | 54 | 48 |
| SMB 59 | 50-59 | M | 15 | Permanent | 10 | 67% | 10 | 14, 15, 24, 25, 47 |
| SMB 63 | 50-59 | M | 3 | Permanent | 1 | 33% | 3 | 11, 12, 14, 15, 16, 17, 21, 22, 24, 25, 26, 27, 28, 35, 36, 37, 38, 41, 42, 44, 46, 47, 48 |
| SMB 68 | 50-59 | M | 19 | Permanent | 11 | 58% | 14 | 15, 16, 36, 41, 46 |
| TOTAL | 321 | 137 | 251 | |||||
Notes: F= Female, M= male, U= undetermined. * A tooth could have more than one carious lesion present. ** Antemortem tooth loss = evidence of healing or healed alveolar bone in the location of the absent tooth. FDI = Fédération Dentaire Internationale tooth identification notation system.
Table 4.
Calculus—the percentage of individuals and the number of teeth with calculus deposits.
|
Dental Pathology: Calculus |
Sample Size (Adults Only) N= |
Percentage of Individuals Affected | Number of Teeth Present | Number of Teeth with Calculus Deposits |
Percentage of Teeth with Calculus |
Mean Number of Teeth Affected |
| 17 | 65% | 240 | 79 | 33% | 7.2 | |
Table 6.
Key individuals from the St Mary’s Cemetery sample with a summary of their oral health findings. Many individuals had one or more skeletal signs of a co-morbidity, and/or signs of skeletal and dental changes.
Table 6.
Key individuals from the St Mary’s Cemetery sample with a summary of their oral health findings. Many individuals had one or more skeletal signs of a co-morbidity, and/or signs of skeletal and dental changes.
| St Mary’s Burial I/D |
Sex | Dental Age D = Skeletal Age S= (Years) |
Inventory Number of Teeth Present de= Deciduous P= Permanent |
Caries Number of Teeth Affected |
Periodontal Disease | EH Number of Teeth Affected † Max: |
IGD Number of Teeth Affected |
Co-Morbidities Signs of Skeletal & Dental Changes |
|
|---|---|---|---|---|---|---|---|---|---|
| Alveolar Bone Status Grade 1-4 Min.-Max |
Alveolar Bone Loss Number of Teeth Affected |
||||||||
| SMB 58 | U | D= 1-1.5 (+/- 3 mths) S= 0-2 |
10 de | 0 | 1 | 0 | 9/10 | 10/10 | i) Abnormal porosity of the cortical bones of the maxilla & mandible [1] |
| SMB 04A | U | D= 3.5-4.5 (+/- 6 mths) S= 2-4 |
19 de | 0 | 1 | 0 | 4/19 | 0 | i) Cribra orbitalia Type 3-4 [1] |
| SMB 19 | U | D=7.5-8.5 (+/-1 yr) S=5-9 |
7 de 12 P |
2/19 | 1-2 | 0 | 8/19 | 0 | i) Cribra orbitalia Type 3-4 [1] |
| SMB 70 | U | D=11.5-12.5 (+/- 1 yr) S=8-9 |
2 de 6 P |
6/8 | 1-2 | 0 | 4/8 | 2/2 | i) Congenital Syphilis, ii) TB, iii) mercury toxicity, iv) abnormal porosity in the cortical bones of the greater wing of sphenoid, maxilla, scapulae, pelvic bones, bilaterally. [1,19,56] |
| SMB 52 B | U | D=10.5-11.5 (+/- 1 yr) S=8-12 |
2 de 14 P |
0 | 1 | 1/16 | 14/15 | 0 | None seen |
| SMB 51 | U | D=10-11. (+/- 1 yr) S=8-12 |
14 de | 0 | 1-3 | 0 | 10/14 | 0 | None seen |
| SMB 28 | F | D=15.5-16.5 (+/- 1 yr) S=10-14 |
26 P | 1/26 | 1-4 | 0 | 20/26 | 0 | i)Cribra orbitalia Type 4 ii) Possible nutritional deficiency due to abnormal porosity of the cortical bones of the greater wing of the sphenoid, and alveolar tissue of the maxilla – bilaterally. [1] |
| SMB 79 | U | D=15-16 (+/- 1 yr) S=16-18 |
25 P | 13/25 | 1-2 | 0 | 5/25 | 0 | i) Spina bifida occulta ii) Evidence of a dental abscess (Figure 3.) |
| SMB 05 | F | D= over 23.5 S=20-29 |
6 P | 4/6 | 1-2 | 0 | 2/5 | 0 | None seen |
| SMB 53 C | F | D= over 23.5 S=30-39 |
9 P | 8/9 | 2-3 | 8/9 | 5/9 | 0 | i) Pitting of the external surface of the Occipital bone, ii) several vertebral osteophytes- [2] |
| SMB 66 B | F | D= over 23.5 S=30-39 |
17 P | 12/17 | 1-4 | 12/17 | 8/17 | 0 | None seen |
| SMB 73 | M | D= over 23.5 S=30-39 |
19 P | 17/19 | 1-3 | 15/19 | 18/19 | 7/19 | i) Torticollis, iii) Spina bifida occulta |
| SMB 06 | M | D= over 23.5 S=40-49 |
24 P | 12/24 | 1-4 | 22/24 | 5/24 | 0 | i) Posterior external surfaces of Parietal bones- uneven thickening, possible mild caries sicca. ii) Vertebral osteophytes & Schmorl’s nodes.[1,2,19] |
| SMB 09 | M | D= over 23.5 S=40-49 |
21 P | 11/21 | 2-4 | 6/21 | 8/21 | Not micro-CT scanned |
i) Spina bifida occulta |
| SMB 57 | M | D= over 23.5 S=40-49 |
25 P | 8/25 | 2-4 | 21/25 | 11/25 | Not micro-CT scanned |
i) Vertebral osteophytes [2] |
| SMB 61 | F | D= over 23.5 S=40-49 |
6 P | 4/6 | 2-3 | 3/6 | 0 | Not micro-CT scanned |
i) Spina bifida occulta |
| SMB 72 | M | D= over 23.5 S=40-49 |
31 P | 7/31 | 2-3 | 2/31 | 0 | 0 | i) Evidence of pipe smoker’s tooth wear pattern*. (Figure 2.). |
| SMB 78 | M | D= over 23.5 S=40-49 |
4 P | 2/4 | 0 | 4/4 | 0 | Not micro-CT scanned |
ii) Vertebral osteophytes, ii) bony growth 20 mm x 10 mm left fibular ossified haemorrhage [2] |
| SMB 83 | M | D= over 23.5 S=40-49 |
16 P | 6/16 | 1-3 | 0 | 9/16 | 0 | i) Spina bifida occulta, ii) Vertebral osteophytes, iii) Bony thickening mid-shaft femur 20 mm x 3 mm, healed trauma antemortem [2] |
| SMB 85 | M | D= over 23.5 S=40-49 |
2 P | 1/2 | 3-4 | 2/2 | 1/2 | 0 | i) Vertebral osteophytes ii) Eburnation of multiple vertebral facet joints. [2] |
| SMB 14 | M | D= over 23.5 S=50-59 |
2 P | 1/2 | 2-3 | 2/2 | 0 | Not micro-CT scanned |
i) Multiple vertebral osteophytes, ii) Eburnation of multiple vertebral facet joints, the joints of the ulna, trochlear, and olecranon (bilaterally), femoral head, acetabulum, talus (head), and the navicular [2] |
| SMB 23 | M | D= over 23.5 S=50-59 |
21 P | 20/21 | 3-4 | 10/21 | 9/21 | 0 | None seen |
| SMB 59 | M | D= over 23.5 S=50-59 |
16 P | 10/16 | 3-4 | 8/16 | 12/16 | Not micro-CT scanned |
i) Evidence of pipe smoker’s tooth wear pattern*. (Figure 2.). |
| SMB 63 | M | D= over 23.5 S=50-59 |
3 P | 3/3 | 4 | 3/5 | 2/3 | 1/1 | i) Spina bifida occulta, ii) Concaved maxillary sinus with signs of new bone growth. |
| SMB 68 | M | D= over 23.5 S=50-59 |
19 P | 11/19 | 2-4 | 15/19 | 8/19 | 0 | i) Eburnation of femoral head, acetabulum, talus and calcaneus.[2] |
Notes: D= Dental age range was estimated using the London Atlas of Human Tooth Development and Eruption [5,6]. S= skeletal age range estimated from the assessment of skeletal changes/maturity [19], U = undetermined sex; M = male; F = female. Periodontal disease includes i) Alveolar Bone Status – Ogden’s (2008) [42] screening system assigns a grade the condition of the buccal contours of the alveolar margins of the posterior teeth. A higher grade implies a more severe grade of periodontal disease. Graded 0 - 4 (0 = unable to score, 1 = no disease to 4 = severe periodontitis). Also, 2) horizontal alveolar bone loss measurements - the average distance measurement from the CEJ on a tooth to the crest of the alveolar bone that has not been affected by periodontal disease, is ~ 2 mm. The higher distance measurement over this point suggests that horizontal alveolar bone loss has occurred. Measurements of 4 mm & over are included in Table 4. EH = Enamel Hypoplasia: Category assigned to each tooth for the presence or absence of EH defects. Table 4 shows the maximum number of EH defects identified. IGD = Interglobular Dentine. A mineralisation defect in the dentine of the tooth. A category was assigned to each tooth for the presences of this defect. Pipe notch/ facet: a tooth wear pattern caused by a pipe stem held & moved between the maxillary and mandibular teeth – indicator of smoking.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



