
Submitted:
03 February 2023
Posted:
10 February 2023
You are already at the latest version
Abstract
Introduction. The main task of the study was to measure the workload of nurses in the care of a patient with a developmental defect–congenital diaphragmatic hernia (CDH)–in the neonatal intensive care unit, which was evaluated on the basis of standardized tools Therapeutic Intervention Scoring System (TISS–28), Nine Equivalents of Nursing Manpower use Score (NEMS) and Nursing activities Score (NAS). Methods. Retrospective study. The workload was measured using TISS–28, NEMS and NAS tools. Descriptive statistics were used to analyze the data, and a single-sample test was used to verify the research hypotheses. Results. The sample consisted of medical records of 33 patients; 592 observations were analyzed. Studies prove the need for research on the workload of nurses in neonatal intensive care units. A patient with CDH should receive nursing care as required. Conclusion. It is necessary to implement a model for measuring the workload of nurses in neonatal intensive care units, taking into account the evaluation of work and its optimization.
Keywords:
nurse
; workload
; staff workload
; nursing intensive care
; nursing activities score
1. Introduction
1.1. Workload of Nurses
The number of nurses is not only a cost, but a concrete benefit to GDP (Gross Domestic Product) [1] and an opportunity to achieve the United Union Sustainable Development Goals (SDGs). It also affects patient safety as well as the quality of nursing care and costs, or missed care–as an effect of nursing workload [2,3]. The research results indicate that the high workload of nurses has a negative impact on the results of patient treatment. Therefore, it is proposed to increase the nursing staff or reduce the number of patients assigned to care for one nurse. The weak point of the available studies is the omission of the influence of contextual factors on the work of nurses and the degree of workload [4,5] and ignoring the impact of contextual factors and workload. Measurement of workload based on the characteristics of the profession is useful in human resources planning, prevention of staff turnover, resignation from work and shortage of personnel, or retirement in general [4,5].
The specificity of ICU (Intensive care unit) is the impact of new technologies on care. They change the health status of critically ill patients, increase the number of co-existing diseases and increase the number of procedures performed. This increases the need for care and workload, as well as the need for specific competencies [6,7]. It is considered that the workload of the nurse consists of the time of performing activities directly and indirectly related to the care of the patient. The proportions between these actions may change due to the variability of the patient's clinical condition [8]. The workload of nurses is the sum of all the needs that must be met in relation to the needs of the patient and their family, but also organizational, administrative, as well as educational work [9].
Many concepts of systems for measuring the workload of nurses have been developed [5,10]. These criteria can be determined by measuring workload basing on: (1) the type of hospital unit (unit level), (2) the professional role (work Level), (3) the number and health status of patients (patient level) and (4) the specific situation (situation level) [4,5].
The measurement of workload at the ward level (unit level) is based on a comparison of the number of patients to the number of nurses (nurse-to-patient ratio), used to compare wards in the context of patient outcomes in wards with similar specifics (benchmarking). Direct patient care is under analysis, excluding administrative actions [4,5].
The second category of workload measurement (work level), based on the characteristics of the profession, makes it possible to compare the consequences of workload depending on the scope of the professional role or specialization performed. This type of measurement determines the impact of workload on occupational burnout and the functioning of intensive care nurses. Load measures, referring to the characteristics of the profession, combine the consequences of performing various nursing roles, such as stress and job dissatisfaction.
Another category of measurement of nurses’ workload (patient level) assumes that the main determinant of workload is the patient's clinical condition and therapeutic variables (e.g. Therapeutic Intervention Scoring System) [4,5,11].
The last, previously indicated category of workload measurement is the situational concept of measuring the workload of a nurse. This measurement takes into account the time of day and night, the number of hours, the number of patients assigned to the nurse's care, as well as the health status of patients, and the broadly understood working environment. The situational measurement concept is based on a subjective assessment of the load experienced by the nurse and their individual projection of the microsystem of work, focusing on the analysis of the impact of contextual factors that increase the load versus facilitating the work of the nurse [4,5,11].
The world's first nurses workload analysis in ICU was based on objective assessments of patients’ clinical condition, level of demand for nursing care, nursing workload, and the optimal level of Human Resource Management, and was conducted in 1970 [12].
In the following years, research tools were developed, such as: Therapeutic Intervention Scoring System 57 (TISS–57) followed by TISS–28, OMEGA, Time Oriented Score System (TOSS), Nine Equivalents of Nursing Manpower Use Score (NEMS), Nursing Activities Score (NAS), which were validated in subsequent studies [12,13]. They have many limitations and focus mainly on measuring the intensity of work or actions performed in a certain period of time [14]. Without exhausting the problem of the workload in the intensive care unit [12,15,16]. Relatively few studies have been conducted in pediatric intensive care units [17,18].
1.2. Nursing Care for a Patient with Congenital Diaphragmatic Hernia
Congenital hernia of the diaphragm (CDH, Congenital Diaphragmatic Hernia) occurs between 3 and 8 weeks of embryonic life and is a birth defect, the essence of which is a loss in the diaphragm with a displacement of the viscera to the chest and pulmonary hypoplasia. Pulmonary hypoplasia occurs on both sides, with a greater severity on the side of the defect. The morphologically and functionally determined propensity to pulmonary hypertension is the consequence of underdevelopment of pulmonary tissue and defects of pulmonary vessels. Pulmonary hypertension is characterized by increased vascular resistance in the pulmonary circulation and right-left blood leakage, leading to impaired oxidation of the body [19]. Defects of hernias are divided into two types, Bochdalek hernia, i.e. posterior-lateral and Morgagni hernia aka parasternal hernia. Bochdalek hernia is a defect in which the opening in the diaphragm is located on the left side (which occurs more often, accounting for about 84% of all diaphragmatic hernias). Morgagni hernia is located on the right side of the diaphragm and accounts for about 13% of all diaphragmatic hernias. Bilateral hernia also occurs and accounts for 3% of all diaphragmatic hernias [20].
In Poland, the percentage of deaths of newborns with congenital malformations is 37,1% live births (Q00–Q99) [21]. Overall survival of neonates with CDH is estimated at about 60% [22]. The survival rate of newborns with CDH in centers providing optimal diagnostics and pre-and postnatal care increases to 90% [23,24,25].
ECMO (Extra Corporeal Membrane Oxygenation) is the extra corporal oxidation of blood by a membrane oxygen exchanger, and is an invasive [26] method of respiratory and/or cardiovascular support. Initiation of ECMO therapy improved survival of newborns with CDH [27] postponing surgery, which should be performed after, and not during ECMO therapy, especially in newborns from the high risk group [28].
Cooperation of (1) the doctor responsible for the diagnostic and therapeutic process, (2) the nurse who exclusively cares for the patient, and (3) the perfusionist during ECMO therapy is mandatory.
2. Materials and Methods
2.1. Study Design
The main task of the study was to measure the workload of nurses in the care of a patient with a developmental defect–congenital diaphragmatic hernia (CDH)–in the neonatal intensive care unit, which was evaluated on the basis of standardized tools Therapeutic Intervention Scoring System (TISS–28), Nine Equivalents of Nursing Manpower use Score (NEMS) and Nursing activities Score (NAS). The retrospective study was conducted from January 1, 2017 to December 31, 2017 in the Clinic of Intensive Care and Congenital Malformations of Newborns and Infants.
2.2. Participants
The sample consisted of medical records of 33 patients, basing on which 592 observations were analyzed. The indication for childbirth in the III° reference center was a prenatal congenital defect, i.e. hernia of the diaphragm (Q79. 0 according to ICD–10). 30 patients were diagnosed with left–sided malformation and three with right–sided malformation. Median relative to the clinical status of patients, based on Apgar scale, was 6/6/6/6.
Among the newborns studied, 19 were male and 14 were female. Surgical procedure was performed on 25 patients. Of these, 20 surgeries were performed on day duty and 5 on night duty. Of the 25 patients who underwent surgery, implementation of the extracorporeal circulation procedure was decided in 15. Ten patients were disqualified from the procedure. 8 patients were not qualified for surgery and implementation of the ECMO procedure. Among the group of 33 newborns, 27 patients died, 5 patients were discharged home (for whom the ECMO procedure was not implemented), and one patient was discharged to an external medical facility (ECMO procedure implemented).
2.3. Instruments
Standardized tools TISS–28, NEMS and NAS were used to measure workload. Further analysis took into account the accepted model of nurse work, which is expressed as nurse-to-patient ratio of 1:2 or 1:1. A Nurse-to-patient ratio of 1:2 ** means that one nurse takes care of two patients. These patients undergo the following procedures, which for the purpose of research are marked with numbers from (1) to (14). These are: (1) invasive mechanical ventilation or non-invasive mechanical ventilation (1.1), central intravenous access (2), arterial access (3), continuous heparin infusion (3.1), parenteral nutrition (4), continuous infusion pharmacotherapy (5), antibiotic and fractionated pharmacotherapy (6), additional fluid therapy (7), monitoring of bladder catheter diuresis (8) or monitoring diuresis with a scale (8.1), intragastric tube feeding (9), monitoring and control of pain (10), monitoring and control of vital signs (11), patient care management (12), patient comfort (13), specialist procedures (14). Nurse-to-patient ratio 1:1* means that one nurse takes care of one patient who is undergoing procedures as above. (1)–(14).
2.4. Data Collection
TISS–28 and NEMS were used to measure the workload. They were applied in accordance with the methodology indicated by the authors. Implemented nurses interventions were analyzed (separately for day and night duty). Work pattern in the hospital word consists of two shifts, which last from 7:00 to 19:00 and from 19:00 to 7: 00 (12 h). The TISS–28 and NEMS were standardized into an 8–hour work pattern. For the purpose of this work, the measurement was performed once every 12 hours of the nurse's work. Documented medical procedures were referred to the tools, gaining a sum of points. Then the points from two shifts (24 h) were added up and divided into 3 shifts (3 shifts x 8h) to obtain an average of 8 hours of nurse work.
The second stage of the study was extended to the measurement and analysis of medical records, which were listed in the first part of the study. Paper documents were analyzed: (1) medical history, (2) daily observation card of the patient, (3) study card, (4) patient pain observation card, (5) central tract observation card, (6) arterial tract observation card, (7) peripheral tract observation card, (8) operating site observation card, (9) observation card of catheter in the bladder, (10) doctor's order card, (11) book of nurse reports. Nursing intervention analysis was summed up with 24 hours of nurse work according to the NAS methodology for direct patient care within 24 hours using Microsoft Excel and analyzed using the Statistica 13.3.721.1. 64-bit (pl) program.
The obtained results (TISS–28, NEMS and NAS) were then converted to the same–hourly–unit of comparison. The test results were then converted into hours (according to the guidelines for each tool). For TISS–28 the average nurse workload for the analyzed hospitalization days (expressed in minutes) was multiplied by 3, and the result was divided by 60’according to the methodology of the tool [29,30]. Calculations using TISS–28 omit the conversion of the average result into minutes (multiplied by 10.6’) because the collected data was expressed and analyzed in a minute record. For the NEMS tool, the average (expressed in points) of day and night duty was multiplied by 10.6’. The result in minutes was multiplied by 3, followed by the result being divided by 60’[14,29,30].
Rating in NAS is expressed in points. Each point means 14.4 minutes of nursing care, and 100 points means that the patient needed 100% of the nurse's time in the last 24 hours [31]. Therefore, the average results obtained from the NAS tool were multiplied by 14.4 minutes. Then the result was divided into 60’ [30,32]. The results obtained determined a nurse's average workload over 24 hours of work.
2.5. Data Analysis
The data was collected using Microsoft Excel and analyzed using Statistica 13.3.721.1. 64-bit (pl) program.
The obtained results determined the average workload of a nurse during 24 hours of work, which made it possible to compare the results obtained from three research tools (TISS–28, NEMS, NAS). Descriptive statistics were used to analyze the data, and a single-sample test was used to verify the research hypotheses.
2.6. Purpose and Research Hypotheses
In order to assess the need for nursing care of a patient with CDH, six research hypotheses were put forward:
- 1.
- H0 The workload of a nurse in the care of a patient with congenital diaphragmatic hernia, determined on the basis of TISS–28, is higher than 46 points.
- 2.
- H0 The workload of a nurse in the care of a patient with congenital diaphragmatic hernia, determined on the basis of NEMS, is higher than 46 points.
- 3.
- H0 The workload of a nurse in the care of a patient with congenital diaphragmatic hernia, determined on the basis of NAS, is higher than 100 points.
- 4.
- H0 The ratio of nursing care for a patient with congenital diaphragmatic hernia of 1:2 is sufficient.
- 5.
- H0 There is a correlation of results for TISS–28 & NEMS and TISS–28 & NAS.
- 6.
- H0 There is a correlation of results for NEMS and NAS.
3. Results
3.1. The Workload of a Nurse in the Care of a Patient with CDH in the Neonatal Intensive Care Unit on the Basis of TISS–28
To assess the workload of a nurse in the care of a patient with congenital diaphragmatic hernia, TISS–28 was used. The maximum workload must not exceed 46 points1 [27,33]. The average workload of a nurse for the analyzed hospitalization days was multiplied by 3, and the result was divided into 60 [29]. When calculating for TISS–28 the step of converting the average result into minutes by multiplying by 10.6 minutes was omitted, since the collected results were expressed and analyzed in a minute record. Descriptive statistics were used to analyze the data and the results of the analysis are shown in Table 1. The analysis of the results was carried out for the patient's hospitalization rates expressed in Table 2 (No.) from (1) to (9), i.e.: (1) day of patient admission to the ward, (2) day of surgery, (3) day of start of extracorporeal circulation, (4) first day of extracorporeal circulation, (5) last day of extracorporeal circulation, (6) day of end of therapy ECMO, (7) date of death of the patient.
A single-sample test was used to verify the first research hypothesis (Table 2).
3.3. The Workload of a Nurse in the Care of a Patient with Congenital Diaphragmatic Hernia on the Basis of NEMS
To evaluate the work of a nurse in the care of a patient with CDH the neonatal intensive care unit NEMS was used, the results are shown in Table 3. Average NEMS results (expressed in hours) in the analyzed periods of hospitalization, described below, denoting according to the scheme used from (1)–(7), column 1 (No.(1)-(7)). Day of hospitalization: (1) admission of the patient to the ward, (2) surgery, (3) entry into ECMO, (4) 1 (first) day ECMO, (5) last day ECMO, (6) exit ECMO, (7) death of the patient. The point range of this scale ranges from 0 to 63 points. However, the maximum workload of a nurse may not exceed 46 points during nursing duty (8 h) [34].
For NEMS, the average (expressed in points) from day and night duty was multiplied by 10.6 minutes (thus obtaining a result in minutes), the result expressed in minutes was multiplied by 3, then the result was divided into 60 [29]. The results are shown in Table 3.
A single-sample test was used to verify test hypothesis number two (Table 4).
3.4. The Workload of a Nurse in the Care of a Patient with Congenital Diaphragmatic Hernia on the Basis of NAS
To assess the workload of a nurse in the care of a patient with CDH the intensive care unit was used NAS using the model NAS/24h [16] at various times of hospitalization. The results are shown in Table 5. Average results (expressed in hours) obtained with NAS in the individual analyzed periods of hospitalization, denoted according to the scheme used in (1)–(7), column 1 (No.) are described below. Day of hospitalization: (1) admission of the patient to the ward, (2) surgical procedure, (3) entry into ECMO, (4) 1 (first) day ECMO, (5) last day ECMO, (6) exit ECMO, (7) death of the patient (Table 5).
A single-sample test was used to verify the third research hypothesis (Table 6).
3.5. Demand for Nursing Care for a Patient with Congenital Diaphragmatic Hernia on the Basis of TISS–28, NEMS and NAS
In order to analyze the need of a patient with CDH for nursing care, the average working time (Table 1, Table 3 and Table 5) was converted into points. The results were plotted and analyzed according to the NEMS recommendation (Figure 1), taking into account the accepted categorization of the patient in accordance with the recommendations of the Swiss Society of Intensive Care [2].
4. Discussion
The main task of the research was to determine a CDH patient's need for nursing care. The task was accomplished by using three standardized research tools TISS–28, NEMS and NAS in intensive care units. The research hypotheses tested were confirmed. Converting 46 points TISS–28 into a daily workload of a nurse, a result of 24h38 was obtained, the 24h38 work threshold was adopted as the maximum allowable, and exceeding this threshold was determined as exceeding the maximum allowable workload. It was observed that in six out of seven days of hospitalization, the average 24–hour workload of a nurse was more than half of the measures exceeding the maximum load (Table 1. No. 1: M=24h5, SD±3.69, Me=25.2; No. 2: M=27h1, SD±3.22, Me=27.5; No. 3: M=29h4, SD±2.00, Me=29.7; No. 4: M=26h1, SD±1.75, Me=25.9; No. 6: M=27h8, SD±1.86, Me=27.8; No. 7: M=26h7, SD±1.92, Me=26.5). It should be noted that during the last day of extracorporeal circulation (5), 47% of the measurements did not exceed the permissible maximum workload (Table 1. No. 5: M=20.4; SD±7.45; Me=22.0) but the result was close to the maximum. Based on a comparison of the average measures in the study group, it is concluded that the workload during six days of hospitalization of a patient exceeded 46 points. As a result of the study, no basis was found to reject the hypothesis ‘The nursing workload during congenital diaphragmatic hernia patient care, determined on the basis of TISS-28is higher than 46 points’.
Results of analysis of measurement averages of a nursing workload during CDH patient care (acc. to NEMS) show a high workload. It was noted that during 6 hospitalization days of a CDH patient the average daily working time of a nurse exceeded 20 hours (Table 3. No. 2 M=22h6, SD±2.71, Me=23.3; No. 3 M=23h6, SD±1.76, Me=23.3; No. 4 M=20h7, SD±1.22, Me=20.7; No. 6 M=23h1, SD±2.05, Me=23.6; No. 7 M=21h6, SD±1.60, Me=20.7). On the first day of a patient's hospitalization, the average daily nursing workload was less than 20 hours (Table 3. No. 1 M=19.0; SD±2.82; Me=20.7). The results were interpreted against a scale of maximum scale = 46 points, which was equivalent to a 24h38 nurse's work. The data analysis showed that all the average scores were below the permissible maximum (46 points NEMS). On this basis, the hypothesis: ‘The workload of a nurse in the care of a patient with congenital diaphragmatic hernia, basing on NEMS is higher than 46 points ’was rejected.
According to NEMS it was found that the highest workload was at the time of the onset of extracorporeal circulation ECMO (Table 3. No. 3 M=23.6; SD±1.76; Me=26.5). A similar result was achieved using the tool TISS-28 (Table 1. No. 3 M=29h4, SD±2.00, Me=29.7).
According to the methodology of NAS , the workload of the nurse must not exceed 100 points [35]. It is proved that the average results of measuring the workload of a nurse in the care of a patient with CDH, ranged from 22h5 to 27h1 NAS. The equivalent of 100 points is 24 hours of work, which is the upper limit of the maximum allowable workload. Analyzing the average working time of the nurse, it was found that the maximum workload was exceeded in the first three days of the hospital stay (Figure 2). Table 5. No. 1 M=25.6, SD±1.90; No. 2 Me=26.2; M=26.2, SD±1.94, No. 3 Me=26.8; M=27.1, SD±0.77, Me=27.3). On the first day of ECMO, the maximum allowable workload was reached (Table 5. No. 4 M=24.0, SD±2.96, Me=24.8). In the last three days 5–7 (Table 5. No. 5–7) workload was lower, but close to 24 hours of work.
In the first three days of hospitalization, no grounds to reject the hypothesis were found. However, this hypothesis was rejected for the patient's hospitalization days 5–7 (Table 5. No. 5–7) hospitalization of the patient.
Further considerations focus on evaluation of the 1:2 ratio of nursing care. It should be emphasized that the purpose of this work was to develop a model for determining the need for nursing care, not making recommendations. The assessment of the nursing care ratio was carried out on the basis of the results obtained from TISS-28, NEMS and NAS by category of care by NEMS [36]. As a result, it was found that a patient generated a need for care >30 points of NEMS. Patient qualification for nurse-to-patient ratio (1A) (nurse-to-patient ratio >1: patient), the highest on the NEMS scale, in six days of hospitalization (No. 1–4 and 6–7 Figure 1) means that the patient required more comprehensive nursing care. On the fifth day of hospitalization (No. 5 Figure 1) for category 1B (30 points), nursing care demand met the required care criteria (1:1). Basing on the analyzed data, it was found that the nurse-to-patient ratio of 1:2 was insufficient for the full period of hospitalization. The ‘nurse-to-patient ratio of 1:2 is sufficient’ hypothesis was then rejected. It should be noted that in the six days of hospitalization of the patient in CDH total number of points in NEMS was higher than 30, but lower than 46 (Table 3 and Graph 1. No. 2, 3, 6 and 7). The total points ranged from 40 to 44 NEMS.
The workload of a nurse caring for a patient with congenital diaphragmatic hernia ranged from 38 to 54 TISS-28 points, which qualified the patient for Category III in the full period of hospitalization (Table 1. No. 1–7).
According to NAS (maximum of 100 nurse workload points) a nurse-to-patient ratio of 1:1 and >1:1 was distinguished. During hospitalization (Table 5. No. 1–3) the average workload of the nurse exceeded 100 points. This meant that the patient required more comprehensive nursing care, that is more than one nurse. During hospitalization (Table 5 and Figure 1 No. 4–7) the need for care did not require a second nurse, i.e. a nurse-to-patient ratio of 1:1 was sufficient. Rejection of the hypothesis ‘Nurse-to-patient ratio of 1:2 is sufficient’ occurred.
Research shows the need to change the model of care used in the clinic. Our own research shows that patients with CDH required a high level of complexity in nursing care, which generated increased workload and, in some cases, the need to involve an additional nurse. Lack of adequate number of nurses may result in missed care and reduce patient and occupational safety [28,29,37,38,41,42,43,44,45]. International research groups, and networks such as The RANCARE Consortium and Missed Care Study Group, collaborate on the concept and phenomenon of missed nursing care. They demonstrate the need to conduct research on the issue of omission and loss of nursing care in relation to medical personnel, working conditions, patient safety and the relationship between these elements [40].
The results of the studies conducted in the analyzed intensive care unit proved that work planning deviated from the recommendations of The Minister Of Health [46], which stems from a shortage of nurses in the labor market (6.2/100 000 population) [47]. It should be noted that the regulation of the Minister of Health [48] determines the average time of direct nursing services in a category III patient for only 300 minutes per day (5 h). However, in our own study, it was proved that the minimum average working time of a nurse, in the case of CDH patient was 20h4 according to TISS-28 (Table 1. Me=22.0; SD±7.45 No. 5 Table 1), NEMS = 15h7 (Me=18.4; SD±7.08 No. 5 Table 3) and NAS = 22h5 (Me=21.3; SD±3.27 No. 5 Table 5). Nursing staff are key to ensuring resilience in ICU [49]. This is one of the key elements necessary to prepare organization in response to crisis [50,51,52].
Correlation tests were performed on the results obtained for the applied research tools. The tools are divided into three comparative groups TISS–28 & NEMS, NEMS & NAS and TISS–28 & NAS. The highest correlation value for TISS–28 & NEMS was shown. A smaller correlation was found when comparing TISS–28 & NAS. The statistical significance of the correlation has been proven for TISS–28 & NEMS (of moderate strength and very weak strength). TISS–28 & NAS correlation was shown as average strength. The results of the analysis did not give grounds to reject the hypothesis ‘there is a correlation of results for TISS–28 & NEMS and TISS–28 & NAS’. However, no correlation of results was found for NEMS & NAS, which led to the rejection of the research hypothesis: ‘There is a correlation of results for NEMS and NAS’.
5. Conclusions
As a result of the analysis, the following conclusions were drawn for the practice:
- 1.
- A nurse-to-patient ratio >1:1 is recommended over a patient with CDH from the first day of hospitalization.
- 2.
- A patient with CDH should receive the care they need, so it is recommended to use standardized tools of TISS–28, NEMS and NAS to measure the workload of nurses.
- 3.
- Use of TISS–28, NEMS and NAS tools can help to increase the level of patient safety in ICU.
- 4.
- Development of a model for the use of TISS–28, NEMS and NAS tools to measure the workload in neonatal intensive care units is the goal of further research.
- 5.
- It is necessary to implement a model for measuring the workload of nurses in neonatal intensive care units, taking into account the evaluation of work and its optimization.
6. Limitations
Limitations in the conducted research should be mentioned. The first major limitation was the disease unit. The study was conducted in one neonatal intensive care unit, in the main reference center of the third stage of surgical treatment of congenital malformations, therefore the results of the analyzes should be interpreted with caution in relation to other groups of patients. Another limitation of the study was the fact that the tools used in the development of the field by experts were dedicated to adult patients and may not reflect practice in the pediatric intensive care unit, especially in the neonatal intensive care unit. In many studies TISS–28 and NEMS have been criticized for failing to take into account both direct and indirect nursing interventions, such as hygiene, as well as the psychological support of the patient's family and the nurse's managerial tasks. The answer to these aspects is NAS which is becoming increasingly used in intensive care units. In order to verify patient safety and occupational safety, as well as to evaluate the use of measurements of these tools, studies on the workload of nurses working in pediatric and neonatal intensive care units are recommended.
The conducted study provided a lot of valuable information on the workload of a nurse in the care over a patient with congenital diaphragmatic hernia, the organization of work, the number of interventions performed, the continuity of highly specialized procedures conducted. This study proves the need for research on the workload of nurses in neonatal intensive care units. The analyses from the measurements will be able to serve as an introduction to the discussion regarding the determination of optimal indicators of care.
Author Contributions
Conceptualization, P.S.-P. and D.K.; methodology, P.S.-P. and D.K.; software, P.S.-P.; validation, D.K., R.K. and M.M.; formal analysis, P.S.-P., D.K., R.Z. and R.K.; investigation, P.S.-P., M.B.; resources, P.S.-P., D.K. and M.B.; data curation, P.S.-P. and D.K.; writing—original draft preparation, P.S.-P.; writing—review and editing, D.K.; R.K., R.Z. and M.M.; visualization, P.S.-P. and D.K.; supervision, M.M., D.K., R.K.; project administration, D.K.; funding acquisition, R.Z. and M.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by the project “InterDoktorMen—Building new quality and effectiveness of education in the formula of doctorate studies for healthcare managers at the Health Sciences Faculty at the Medical University in Łódź’(POWR. 03.02.00-00-I027/16) and co-financed from European Union resources from the European Social Fund as a part of the Operational Programme Knowledge Education Development.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, according to polish law the ethical statement is available only for experiment. In accordance with the law on scientific research in force in Poland, the consent of the bioethics committee can be obtained only in the case of experimental research. The Bioethics Committee of the Medical University of Lodz does not consider applications that do not have such premises, or if a doctor is not part of the research project.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. The content of the questionnaire contained information about the consent
Data Availability Statement
Non-digital data supporting this study are curated by Dorota Kilanska.
Acknowledgments
The authors of the publication would like to thank head of the intensive care unit and treatment of congenital defects in newborns and infants Prof. Iwona Maroszyńska and ward nurse Aleksandra Matczak.
Conflicts of Interest
The authors declare no conflict of interest.
| 1. | By calculating 46 points per daily workload (46 points x 10.6 minutes x 3 / 60 = the result is the number of hours worked during 24 hours of work), a result of 24.38 h/24h hours during 24 hours of work of a nurse was obtained. |
References
- Amiri, A., & Solankallio-Vahteri, T. (2020). Analyzing economic feasibility for investing in nursing care: Evidence from panel data analysis in 35 OECD countries. 7(1), 13–20. [CrossRef]
- Griffiths, P., Recio-Saucedo, A., Dall’Ora, C., & Briggs, J. (2018). The association between nurse staffing and omissions in nursing care: A systematic review. 74(7), 1474–1487. [CrossRef]
- Wieczorek-Wojcik, B., Gaworska-Krzemińska, A., J Owczarek, A., & Kilańska, D. (2020). In-hospital mortality as the side effect of missed care. 28(8), 2240–2246. [CrossRef]
- Carayon, P., & P. Gurses, A. (2008). Nursing Workload and Patient Safety—A Human Factors Engineering Perspective.
- Cisek, M., Przewoźniak, L., Kózka, M., & Tomasz Brzostek, T. (2013). Obciążenie pracą podczas ostatniego dyżuru w opiniach pielęgniarek pracujących w szpitalach objętych projektem RN4CAST (T. 11).
- Yatsue Conishi, R. M., & Gaidzinski, R. R. (2007). Nursing activities score (NAS) como instrumento para medir carga de trabalho de enfermagem em UTI adulto. Rev Esc Enferm. 41(3), 346–354. [CrossRef]
- Sprung, C. L., Artigas, A., Kesecioglu, J., & Pezzi, A. (2012). The Eldicus prospective, observational study of triage decision making in European intensive care units. Part II: intensive care benefit for the elderly. 40(1), 132–138. [CrossRef]
- Panunto, M. R., & Guirardello, E. de B. (2012). Carga de trabalho de enfermagem em Unidade de Terapia Intensiva de um hospital de ensino. 25(1), 96–101. [CrossRef]
- Gonçalves, L. A., & Padilha, K. G. (b.d.). Fatores associados à carga de trabalho de enfermagem em Unidade de Terapia Intensiva. 41(4), 645–652. [CrossRef]
- Wiskow, C. (2006). Pomiar obciążenia pracą w określaniu potrzeb kadrowych. Przegląd piśmiennictwa. Opracowanie dla Międzynarodowej Rady Pielęgniarek. http://www.ptp.na1.pl/pliki/ICN/ICN_pomiar_obciazenia_praca_ 03_11_2009.pdf.
- Ball, J. E., Murrells, T., Rafferty, A. M., Morrow, E., & Griffiths, P. (2014). Care left undone’during nursing shifts: Associations with workload and perceived quality of care. 23(2), 116–125. [CrossRef]
- Guccione, A., Morena, A., Pezzi, A., & Iapichino, G. (2004). The assesment of nursing workload. 70(5), 411–416.
- Canabarro, S. T., Velozo, K. D. S., Eidt, O. R., Piva, J. P., & Garcia, P. C. R. (2010). Nine Equivalents of Nursing Manpower Use Score (NEMS): A study of its historical process. 31(3), 584–590. [CrossRef]
- Kelly Dayane Stochero Velozo, Pedro Celiny Ramos Garcia, Jefferson Pedro Piva, & Humberto Holmer Fiori,. (2017). Scores TISS–28 versus NEMS to size the nursing team in a pediatric intensive care unit. 15(4), 470–475. [CrossRef]
- Irimagawa, S., & Imamiya, S. (1993). Industrial hygienic study on nursing activities investigation on heart rate and energy expenditure of cranial nerves and ICU ward nurses. 65, 91–98.
- Debergh, D., Myny, D., Van Herzeele, I., Van Maele, G., & Reis Miranda, D. (2012). Measuring the nursing workload per shift in the ICU. 38(9), 1438–1444. [CrossRef]
- Campagner, A. O. M., Pedro Celiny Ramos Garcia, P. C. R., & Piva, J. P. (2014). Aplicação de escores para estimar carga de trabalho de enfermagem em unidade de terapia intensive pediátrica. 26(1), 36–43.
- Monroy, J. C., & Hurtado Pardos, B. (2002). Utilization of the nine equivalents of nursing manpower use score (NEMS) in a pediatric intensive care unit. 13(3), 107–112.
- Moore, K. L., Persaud, T. V. N., & Torchia, M. G. (2021). Embriologia i wady wrodzone. Od zapłodnienia do urodzenia. Urban & Partner.
- Bohosiewicz, J. (2013). Diagnostyka i terapia wad płodu aktualny stan wiedzy i praktyki (5. wyd., T. 67). Ann. Ac. Silea.
- Program kompleksowej terapii wewnątrzmacicznej w profilaktyce następstw i powikłań wad wrodzonych i chorób dziecka nienarodzonego – jako element poprawy stanu zdrowia dzieci nienarodzonych i noworodków na lata 2018–2020. (2018). Program Polityki Zdrowotnej Ministra Zdrowia ‘. https://www.gov.pl/attachment/85de995a-ab00-4df0-9dea-f32400311e9d.
- Bösenberg, A. T., & Brown, R. A. (2008). Management of congenital diaphragmatic hernia. Curr Opin Anaesthesiol 2008. 21(3), 323–331.
- de Buys Roessingh, A. S., & Dinh-Xuan, A. T. (2009). Congenital diaphragmatic hernia: Current status and review of the literature. 168(4), 393–406. [CrossRef]
- Logan, J., Rice, H., Goldberg, R., & Cotten, C. (2007). Congenital diaphragmatic hernia: A systematic review and summary of best-evidence practice strategies. 27(9), 535–549. [CrossRef]
- Deprest, J. A., Gratacos, E., Nicolaides, K., & Done, E. (2009). Changing perspectives on the perinatal management of isolated congenital diaphragmatic hernia in Europe. 36(2), 329–347. [CrossRef]
- Lango, R., Szkulmowski, Z., Maciejewski, D., & Kusza, K. (2009). Protokół zastosowania pozaustrojowej oksygenacji krwi (ECMO) w leczeniu ostrej niewydolności oddechowej. 51(4).
- Mugford, M., Elbourne, D., & Field, D. (2008). Extracorporeal membrane oxygenation for severe respiratory failure in newborn infants. 16(3), CD001340.
- Bryner, B. S., West, B. T., Hirschl, R. B., & Drongowski, R. A. (2009). Congenital diaphragmatic hernia requiring extracorporeal membrane oxygenation: Does timing of repair matter? 44(6), 1165–1171. [CrossRef]
- Ducci, A. J., Zanei, S. S. V., & Whitaker, I. Y. (2008). Nursing workload to verify nurse/patient ratio in a cardiology ICU. 42(4), 673–680.
- Velozo, K. D. S., Costa, C. A. D., Tonial, C. T., Crestani, F., Andrades, G. R. H., & Garcia, P. C. R. (2021). Comparison of nursing workload in a Pediatric Intensive Care Unit estimated by three instruments. 55. [CrossRef]
- Queijo, A., & Padilha, K. (2004). Instrumento de medida da carga de trabalho de enfermagem em Unidade de Terapia Intensiva: Nursing Activities Score (N.A.S). 23, 114–122.
- Castro MCN, Dell’Acqua MCQ, Corrente JE, Zornoff DCM, Arantes LF. (2009). Aplicativo informatizado com O nursing activities score: Instrumento para gerenciamento da assistência em unidade de terapia intensiva. Texto Contexto Enferm. 18(3), 577–585. [CrossRef]
- Katia Grillo Padilha, Regina M Cardoso Sousa, Miako Kimura, & Ana Maria Kazue Miyadahira. (2007). Padilha KG, Sousa RM, Kimura M, et al. Nursing workload in intensive care units: A study using the Therapeutic Intervention Scoring System–28 (TISS–28). [CrossRef]
- Cudak, E., & Dyk, D. (2007). Ocena nakładu pracy pielęgniarek na oddziale intensywnej terapii na podstawie skali Nine equivalents of nursing manpower use score (NEMS). 15(1), 7–12.
- Lucchini, A., Elli, S., De Felippis, C., Greco, C., Mulas, A., Ricucci, P., Fumagalli, R., & Foti, G. (2019). The evaluation of nursing workload within an Italian ECMO Centre: A retrospective observational study. 55. [CrossRef]
- Rothen, H. U., Küng, V., Ryser, D. H., Zürcher, R., & Regli, B. (1999). Validation of “nine equivalents of nursing manpower use score’on an independent data sample. 25, 606–611. [CrossRef]
- Uchmanowicz, I., & Gotlib, J. (2018). Czym jest racjonowanie opieki pielęgniarskiej? 7(2), 40–47.
- VanFosson, C. A., Jones, T. L., & Yoder, L. H. (2016). Unfinished Nursing Care: Am Important Performance Measure for Nursing Care. 64(2), 124–136. [CrossRef]
- Schubert, M., Ausserhofer, D., Desmedt, M., Schwendimann, R., Lesaffre, E., Li, B., & De Geest, S. (2019). Schubert M, Ausserhofer D, Desmedt M, et al. Levels and correlates of implicit rationing of nursing care in Swiss acute care hospitals – a cross sectional study. 50, 230–239. [CrossRef]
- Suhonen, R., & Scott, P. A. (2018). Missed care: A need for careful ethical discussion. 25(5), 549–551. [CrossRef]
- Gibbon, B., & Crane, J. (2018). The impact of ‘missed care’on the professional socialisation of nursing students: A qualitative research study. 66, 19–24. [CrossRef]
- Cho, S.-H., Kim, Y.-S., Yeon, K. N., You, S.-J., & Lee, I. D. (2015). Effects of increasing nurse staffing on missed nursing care. 62(2), 267–274. [CrossRef]
- Tubbs-Cooley, H. L., Mara, C. A., Carle, A. C., Mark, B. A., & Pickler, R. H. (2019). Association of Nurse Workload With Missed Nursing Care in the Neonatal Intensive Care Unit. 173(1), 44–51. [CrossRef]
- Kalisch, B. J., & Xie, B. (2014). Errors of Omission: Missed Nursing Care. 36(7).
- Carvalho de Oliveira, A., Garcia, P. C., & Nogueira, L. de S. (2016). Nursing workload and occurrence of adverse events in intensive care: A systematic review. 50(4), 679–689. [CrossRef]
- Obwieszczenie Ministra Zdrowia z dnia 18 stycznia 2022 r. W sprawie ogłoszenia jednolitego tekstu rozporządzenia Ministra Zdrowia w sprawie standardu organizacyjnego opieki zdrowotnej w dziedzinie anestezjologii i intensywnej terapii. (2022). MIN. ZDROWIA.
- WHO. (b.d.). STATE OF THE WORLD’S NURSING. Pobrano 8 grudzień 2022, z https://apps.who.int/nhwaportal/Sown/Files?name=POL.
- Rozporządzenie Ministra Zdrowia z dnia 28 grudnia 2012 r. W sprawie sposobu ustalania minimalnych norm zatrudnienia pielęgniarek i położnych w podmiotach leczniczych niebędących przedsiębiorcami. (2012). MIN. ZDROWIA.
- Borzuchowska, M., Kilańska, D., Kozłowski, R., Ilchev, P., Czapla, T., Marczewska, S., & Marczak, M. (2022). The Effectiveness of Healthcare System Resilience during the COVID–19 Pandemic: A Case Study (Nr 2022120242). Preprints. [CrossRef]
- Nurses: A force for change: Improving health systems’resilience. (b.d.). NTERNATIONAL NURSES DAY 2016. https://www.thder.org.tr/uploads/files/icn-2016.pdf.
- Building health systems resilience for universal health coverage and health security during the COVID–19 pandemic and beyond: WHO position paper. (b.d.). Pobrano 31 grudzień 2022, z https://www.who.int/publications-detail-redirect/WHO-UHL-PHC-SP-2021.01.
- COMMUNICATION FROM THE COMMISSION On effective, accessible and resilient health systems. (2014). EUROPEAN COMMISSION.
Figure 1.
Average nurse working hours chart for TISS–28, NEMS and NAS. Legend: Cat. – category of patients according to NEMS [36]
Figure 1.
Average nurse working hours chart for TISS–28, NEMS and NAS. Legend: Cat. – category of patients according to NEMS [36]
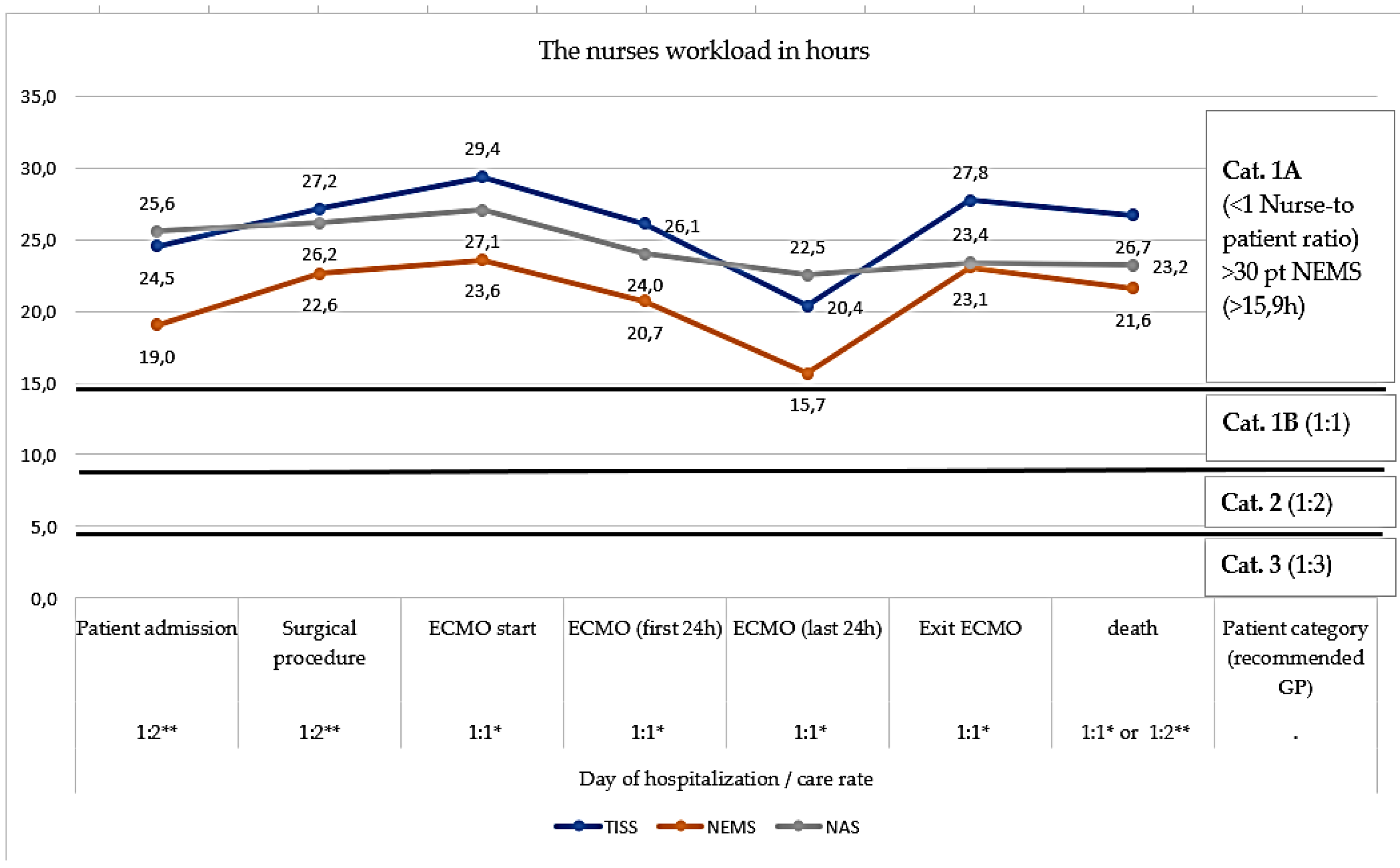

Table 1.
TISS–28 analysis of the daily workload of a nurse expressed in hours.
| No. | Variable | Nurse-to-patient ratio | Average number of working hours in 24 hours | SD | N | Min | Max | Me |
|---|---|---|---|---|---|---|---|---|
| (1) | Patient admission to the ward | 1:2** | 24.5 | 3.69 | 33 | 15.3 | 29.1 | 25.2 |
| (2) | Surgical procedure | 1:2** | 27.1 | 3.22 | 25 | 19.6 | 32.3 | 27.5 |
| (3) | Entry to ECMO | 1:1* | 29.4 | 2.00 | 15 | 25.9 | 33.4 | 29.7 |
| (4) | 1 day ECMO | 1:1* | 26.1 | 1.75 | 12 | 24.1 | 29.4 | 25.9 |
| (5) | Last day ECMO | 1:1* | 20.4 | 7.45 | 17 | 5.8 | 30.2 | 22.0 |
| (6) | exit ECMO | 1:1* | 27.8 | 1.86 | 12 | 23.8 | 30.7 | 27.8 |
| (7) | Patient's death | 1:1* or 1: 2** | 26.7 | 1.92 | 27 | 22.8 | 30.2 | 26.5 |
Legend: 1:1* = nurse-to-patient ratio one-to-one (1:1), means that the patient is cared for by one nurse; 1:2** = nurse-to-patient ratio one-to-two (1:2). It is understood as nursing care performed by one nurse on two patients requiring intensive care (mechanically ventilated patient) SD = standard deviation; ECMO—Extra Corporeal Membrane Oxygenation.
Table 2.
Test of averages against a fixed reference value for TISS–28.
| No. | Variable | Test of averages against a fixed reference value | |||||||
| Me | SD | N | S. E. | t | df | Cohen’s d | P | ||
| (1) | Patient admission to the ward | 19.0 | 2.82 | 33 | 0.49 | 6.41 | 32 | 1.12 | 0.000000 |
| (2) | Surgical procedure | 22.6 | 2.71 | 25 | 0.54 | 12.44 | 24 | 2.49 | 0.000000 |
| (3) | Entry to ECMO | 23.6 | 1.76 | 15 | 0.45 | 16.99 | 14 | 4.39 | 0.000000 |
| (4) | 1 day ECMO | 20.7 | 1.22 | 12 | 0.35 | 13.76 | 11 | 3.97 | 0.000000 |
| (5) | Last day ECMO | 15.7 | 7.08 | 16 | 1.77 | -0.14 | 15 | -0.04 | 0.890314 |
| (6) | exit ECMO | 23.1 | 2.05 | 12 | 0.59 | 12.15 | 11 | 3.51 | 0.000000 |
| (7) | Patient's death | 21.6 | 1.60 | 27 | 0.31 | 18.57 | 26 | 3.57 | 0.000000 |
Legend: 1:1* = nurse-to-patient ratio one-to-one (1:1), means that the patient is cared for by one nurse; 1:2** = nurse-to-patient ratio one-to-two (1:2). It is understood as nursing care performed by one nurse on two patients requiring intensive care (mechanically ventilated patient) SD = standard deviation; ECMO – Extra Corporeal Membrane Oxygenation.
Table 3.
Average NEMS results per day (results expressed in hours).
| No. | Clinical pathway | Nurse-to-patient ratio | Avg no of working hours in 24 hours | SD | Me | Min | Max | N |
|---|---|---|---|---|---|---|---|---|
| (1) | Patient admission to the ward | 1:2** | 19.0 | 2.82 | 20.7 | 14.3 | 23.3 | 33 |
| (2) | Surgical procedure | 1:2** | 22.6 | 2.71 | 23.3 | 17.0 | 29.7 | 25 |
| (3) | Entry to ECMO | 1:1* | 23.6 | 1.76 | 23.3 | 20.7 | 26.5 | 15 |
| (4) | 1 day ECMO | 1:1* | 20.7 | 1.22 | 20.7 | 18.0 | 22.3 | 12 |
| (5) | Last day in ECMO | 1:1* | 15.7 | 7.08 | 18.4 | 1.59 | 23.9 | 12 |
| (6) | exit ECMO | 1:1* | 23.1 | 2.05 | 23.6 | 20.1 | 26.5 | 12 |
| (7) | Patient's death | 1:2* * or 1:1* | 21.6 | 1.60 | 20.7 | 20.1 | 26.5 | 27 |
Legend: 1:1* = nurse-to-patient ratio one-to-one (1:1), means that the patient is cared for by one nurse; 1:2** = nurse-to-patient ratio one-to-two (1:2). It is understood as nursing care performed by one nurse on two patients requiring intensive care (mechanically ventilated patient); SD = standard deviation; ECMO – Extra Corporeal Membrane Oxygenation.
Table 4.
Test of averages against a fixed reference value for NEMS.
| Variable | Test of averages against a fixed reference value | ||||||||
| No. | M | SD | N | S. E. | t | df | Cohen's d | P | |
| (1) | Patient admission to the ward | 19.05 | 2.82 | 33 | 0.49 | -10.86 | 32 | -1.89 | 0.000000 |
| (2) | Surgical procedure | 22.64 | 2.71 | 25 | 0.54 | -3.21 | 24 | -0.64 | 0.003762 |
| (3) | Entry to ECMO | 23.60 | 1.76 | 15 | 0.45 | -1.71 | 14 | -0.44 | 0.108538 |
| (4) | 1 day ECMO | 20.74 | 1.22 | 12 | 0.35 | -10.36 | 11 | -2.99 | 0.000001 |
| (5) | Last day in ECMO | 15.65 | 7.08 | 16 | 1.77 | -4.93 | 15 | -1.23 | 0.000182 |
| (6) | exit ECMO | 23.10 | 2.05 | 12 | 0.592408 | -2.1621 | 11 | -0.62 | 0.053510 |
| (7) | Patient's death | 21.63 | 1.60 | 27 | 0.31 | -8.90 | 26 | -1.71 | 0.000000 |
Legend: 1:1* = nurse-to-patient ratio one-to-one (1:1), means that the patient is cared for by one nurse; 1:2** = nurse-to-patient ratio one-to-two (1:2). It is understood as nursing care performed by one nurse on two patients requiring intensive care (mechanically ventilated patient) SD = standard deviation. ECMO – Extra Corporeal Membrane Oxygenation.
Table 5.
Average NAS results over 24–hour work (results expressed in hours).
| No. | Variable | Nurse-to-patient ratio | Avg no of working hours in 24 hours | SD | Me | Min | Max | N |
|---|---|---|---|---|---|---|---|---|
| (1) | Patient admission to the ward | 1:2** | 25.6 | 1.90 | 26.2 | 17.4 | 28.9 | 33 |
| (2) | Surgical procedure | 1:2** | 26.2 | 1.94 | 26.8 | 19.7 | 28.9 | 25 |
| (3) | Entry to ECMO | 1:1* | 27.1 | 0.77 | 27.3 | 25.7 | 28.9 | 15 |
| (4) | 1 day ECMO | 1:1* | 24.0 | 2.96 | 24.8 | 19.6 | 29.0 | 12 |
| (5) | Last day in ECMO | 1:1* | 22.5 | 3.27 | 21.3 | 19.0 | 29.0 | 12 |
| (6) | exit ECMO | 1:1* | 23.4 | 4.25 | 24.0 | 15.0 | 29.6 | 12 |
| (7) | Patient's death | 1:2** or 1:1* | 23.2 | 4.82 | 23.7 | 13.1 | 29.6 | 27 |
Legend: 1:1* = nurse-to-patient ratio one-to-one (1:1), means that the patient is cared for by one nurse; 1:2** = nurse-to-patient ratio one-to-two (1:2). It is understood as nursing care performed by one nurse on two patients requiring intensive care (mechanically ventilated patient); SD = standard deviation; ECMO – Extra Corporeal Membrane Oxygenation.
Table 6.
Test of averages against a fixed reference value for NAS.
| Day of hospitalization | Test of averages against a fixed reference value | ||||||||
| No. | Avg | SD | N | SE. | T | df | Cohen's d | P | |
| (1) | Patient admission to the ward | 25.60 | 1.90 | 33 | 0.33 | 4.84 | 32 | 0.84 | 0.000032 |
| (2) | Surgical procedure | 26.16 | 1.94 | 25 | 0.39 | 5.59 | 24 | 1.12 | 0.000009 |
| (3) | Entry to ECMO | 27.10 | 0.77 | 15 | 0.20 | 15.53 | 14 | 4.01 | 0.000000 |
| (4) | 1 day ECMO | 24.00 | 2.96 | 12 | 0.86 | 0.00 | 11 | 0.00 | 0.996353 |
| (5) | Last day in ECMO | 22.53 | 3.27 | 12 | 0.95 | -1.56 | 11 | -0.45 | 0.146988 |
| (6) | exit ECMO | 23.39 | 4.25 | 12 | 1.23 | -0.49 | 11 | -0.14 | 0.629811 |
| (7) | Patient's death | 23.24 | 4.82 | 27 | 0.93 | -0.82 | 26 | -0.16 | 0.417825 |
Legend: 1:1* = nurse-to-patient ratio one-to-one (1:1), means that the patient is cared for by one nurse; 1:2** = nurse-to-patient ratio one-to-two (1:2). It is understood as nursing care performed by one nurse on two patients requiring intensive care (mechanically ventilated patient) SD = standard deviation. ECMO – Extra Corporeal Membrane Oxygenation.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



