
Submitted:
12 February 2023
Posted:
14 February 2023
You are already at the latest version
Abstract
Abstract: (1) Background: We hypothesized measuring the extent of brain overwork can extrapolate the burden of mental distress. This study aimed to develop a scale that measures mental distress and validate it in the general population. (2) Methods: In this population-based cross-sectional study, we recruited a total of 739 adults aged 16-65 years from 64 sampling centers of a clinical cohort across Mongolia to validate a 10-item self-report questionnaire. Internal consistency was measured using the McDonald’s ω. Test-retest reliability was analyzed using intraclass correlation coefficients. Construct and convergent validities were examined using the principal component analysis (PCA) and confirmatory factor analysis (CFA). Hospital Anxiety and Depression Scale (HADS) and the abbreviated version of the World Health Organization Quality of Life (WHOQOL-BREF) were used to evaluate the criterion validity. (3) Results: Among the participants, 70.9% were women, 22% held a bachelor's degree or higher, 38.8% were employed, and 66% were married. The overall McDonald’s ω coefficient was 0.861 demonstrating evidence of excellent internal consistency. The total intraclass correlation coefficient of the test-retest analysis was 0.75, indicating moderate external reliability. PCA and CFA established a three-domain structure that provided an excellent fit to the data (RMSEA=0.033, TLI=0.984, CFI=0.989, χ2=58, p=0.003). This 10-item scale, the Brain Overwork Scale (BOS-10), determines mental distress in three dimensions: Excessive Thinking, Hypersensitivity, and Restless Behavior. All items had higher item-total correlations with their corresponding domain than the other domains, and correlations between the domain scores ranged from 0.547–0.615. The BOS-10 correlated with the HADS, whereas it was inversely correlated with the WHOQOL-BREF. (4) Conclusions: The results suggest that the BOS-10 is a valid and reliable instrument for assessing mental distress in the general population. The current findings also demonstrate that the BOS-10 is quantitative, simple, and applicable for large-group testing.
Keywords:
health psychology
; mental distress
; stress
; population
; psychometric property
; validation
; Mongolia
1. Introduction
The number of entities that determine the diagnosis of a disease or an abnormal condition was nearly 55,000 on the tenth revision of the International Classification of Diseases (ICD-10) and jumped up to 85,000 by its current revision (ICD-11) [1]. In accordance with recent advances in medicine, life expectancy, quality of life, and overall public health across the globe have been improved. Public awareness of mental health raises gradually. However, the prevalence of mental disorders has significantly increased in recent decades worldwide [2]. One in eight people in the world has been diagnosed with a mental disorder. One in five people who were not diagnosed with psychiatric or neurological disorders may have mental distress or mental health problems. Mental distress decreases the quality of life, causes disability, and increases mortality [3,4,5]. Therefore, mental distress is an important public health burden and needs early detection and intervention.
There are several strongly validated questionnaires to assess mental distress, such as the Hospital Anxiety and Depression Scale (HADS), the Center for Epidemiologic Studies Depression Scale (CES-D), and the State-Trait Anxiety Inventory (STAI) [6,7,8]. These instruments detect psychological symptoms of mental distress, such as depressive mood, loss of interest, fatigue, diminished energy, and anxiety. Thus, they are useful for identifying mental disorders, accordingly. However, some people deny any emotional or behavioral symptoms or do not readily express their emotional state in questionnaires. Particularly, people with alexithymia do not easily recognize their mental distress [9]. Therefore, questionnaires that detect psychiatric symptoms using emotional words may not work for such people.
Furthermore, some people complain of mainly physical symptoms and deny mental symptoms. They are usually referred to non-psychiatric wards and end up with a diagnosis such as a condition with unknown origin, medically unexplained symptoms, or a functional somatic syndrome because their subjective symptoms cannot be explained by conventional medical examinations and tests. Common characteristics of those patients are that they recover after antidepressants and anxiolytics. This suggests that the etiopathology of mental distress is associated with chronic stress-induced dysfunctions of brain activity [10,11,12]. Taken together, identifying mental distress is often complicated and there is no screening tool that particularly identifies both physical and mental symptoms of mental distress in people without any clinical diagnosis.
Since Selye postulated his stress theory based on his surprising findings that nonspecific response of the body to any demand results in adrenal hyperactivity, lymphatic atrophy, and peptic ulcer (called as a classic triad), the effects of stress on brain functions are well recognized. He distinguished acute stress from chronic stress or response to chronically applied stressors, termed as “general adaptation syndrome”, by introducing a basic concept of the hypothalamic-pituitary-adrenocortical axis as a main mediator that influence brain activity to maintain the homeostasis in response to any challenges [13]. At present, a diversity of stress mediators in addition to the corticotropin-releasing hormone response, including but not limited to the catecholaminergic pathway or sympathetic-adrenomedullary axis, the acetylcholinergic pathway or parasympathetic nervous system, and a recently emerging neuroimmune pathway was established [14,15,16]. However, so far, a direct biomarker that determines how strongly the nervous system copes with mental distress does not exist. Thus, untangling the fundamental problem of how psychological stress can produce various mental and somatic symptoms or even diseases has not been well described yet. Therefore, we hypothesized that chronic stress might cause restless overwork of brain activity. Any psychological event that induces mental distress may be associated with cognitive, emotional, and behavioral alterations. To cope with mental distress, brain activity increases, particularly the sympathetic nervous system is activated. If not solved, it causes exhaustion or overwork of the brain activity and eventually results in mental disorders. Aging, alexithymia, alexisomia, and other predispositions make vulnerable to mental overwork and further complications leading to diseases, both mental and physical disorders. In accordance with our hypothesis, previous studies suggested that people who have recurrent mental symptoms have typical characteristics of neuroticism, including a symptom called “thinking too much” [17,18]. We proposed that mental distress can be characterized by subjective symptoms of excessive thinking, hypersensitivity, restless behavior, social withdrawal, and minor problems in daily life, which constitute an abnormal condition called brain overwork syndrome.
This study aimed to develop a novel tool for assessing mental distress that could be useful for both clinicians and the public. The objectives of this study were (1) to develop a novel scale that measures brain overwork symptoms; (2) to determine the psychometric properties of the novel scale in the general population.
2. Materials and Methods
2.1. Development of a novel inventory for detecting mental distress
Our conceptual framework was aimed to outline the symptoms that describe the severity of mental distress in association with brain overwork symptoms. As shown in the supplement figure, chronic psychosocial stressors cause mental distress or an abnormal condition that is characterized by excessive thinking, hypersensitivity, restless behavior, social withdrawal, and minor problems in daily life (Figure S1). These five dimensions were described by 37 items and constitute the brain overwork syndrome; thus, we called this new questionnaire as the Brain Overwork Scale (BOS). To minimize the self-report and social desirability bias, we developed these items with a preference for items focusing on behavioral characteristics instead of emotional characteristics (mood changes). The 37 items consisted of statements of agreement measured on a 5-point Likert scale (Table S1). BOS was administered to the participants of the cohort described below. After data collection, items that scored a factor loading lower than 0.4 on a single domain with the principal component analysis (PCA) with varimax rotation were eliminated. Furthermore, items with more than 10% of missing responses which might be unintelligible to participants were removed. Remained 10 items built the final version of BOS (BOS-10) that was further examined for its psychometric properties.
2.2. Study population
This cross-sectional study was conducted as a part of a nationwide population-based cohort study that investigated brain-related disorders in the general population of Mongolia. To cover a full representative population, we included two residency locations (urban and rural area), resulting in the desired sample size of 770. Considering a response rate of 80%, 924 individuals who fulfilled the inclusion criteria were invited to participate in the study. Mongolian citizens who lived in the geopolitical units for at least six months and who were not diagnosed with any disease were considered to meet the inclusion criteria. The subjects were recruited from 64 sampling centers, including 30 centers of 8 districts in Ulaanbaatar and 34 centers of 4 rural regions in Mongolia.
Among the invited individuals, a total of 915 participants signed the informed consent to participate. Out of them, 109 participants declined to participate, and 67 were excluded due to incomplete survey data. The remaining 739 subjects were enrolled for the final analysis.
2.3. Data collection
The data collection started on September 7 and the preliminary dataset was extracted on January 19, 2021. The study was conducted in the official language (Mongolian). Based on a pilot test using the draft version of the BOS questionnaire, the expert committee reviewed the adaptation process and finalized the BOS-10. All participants completed tablet-based questionnaires addressing their demographics and the BOS questionnaire. A total of 366 participants completed the BOS questionnaire again within two weeks of the initial administration to assess test-retest reliability. All field study members completed a data collection training program prior to the study.
2.4. Instruments
The Hospital Anxiety and Depression Scale (HADS) and the abbreviated version of the World Health Organization Quality of Life (WHOQOL-BREF) were used to evaluate the criterion validity of the BOS. The HADS is a 14-item self-report questionnaire widely used to evaluate the severity of anxiety and depression symptoms in the past week [6]. Among 14 items, seven of them are for anxiety (HADS-A subscale) and the remaining seven are for depression (HADS-D subscale) formulated in a readily understandable language. The Mongolian version of the HADS demonstrated evidence of good validity and reliability for the general population [19]. Each item is rated on 4-point scale for a total score between 0 and 21 for each subscale. The ranges of scores for cases on each subscale are 0–7 or normal, 8–10 or mild abnormality, 11–14 or moderate abnormality, and 15–21 or severe abnormality.
The WHOQOL-BREF was developed by the WHOQOL group in 1996 [20]. It contains 24 items, and each item is measured on a five-point Likert scale. This questionnaire determines the quality of life (QOL) with four domains: physical QOL, psychological QOL, social relationships, and environmental QOL. The score of each domain consists of a mean score of items in which a higher score indicates a better QOL of that aspect. Two additional single items measure the overall perception of QOL and general health. The Mongolian version of the WHOQOL-BREF had good reliability and validity for assessing QOL in the general population of Mongolia [21].
2.5. Statistical analysis
The study characteristics were expressed as means with a standard deviation for normally distributed variables, and as numbers with percentages in cases of categorical data. The reliability of the questionnaire was assessed by McDonald’s omega (excellent≥0.9, good≥0.8, acceptable≥0.7) for internal consistency. A test-retest procedure was performed at a 2-week interval using the intraclass correlation coefficient (ICC). ICC values of <0.5, 0.5 to 0.7, 0.7 to 0.9, and >0.9 were considered to have poor, moderate, good, and excellent test-retest reliability, respectively [22]. Validity was evaluated by the principal component analysis (PCA) with varimax rotation. Factor analysis suitability was examined by the Bartlett test of sphericity (p<0.001) and Kaiser-Meye-Olkin (KMO) test of sampling adequacy (p>0.65), followed by determining the number of relevant factors via eigenvalue analysis. The factors with eigenvalues >1 was assumed to be meaningful and retained for rotation [23]. A factor loading of 0.4 was established as the lower bound for a variable to be included in the respective factor structure. Confirmatory factor analysis (CFA) was performed to assess the BOS 3-factor model fit using the following criteria for the structural equation modeling: the Tucker-Lewis index (TLI), and the comparative fit index (CFI) close to 0.90 or above, the root mean square error of approximation (RMSEA < 0.05). To assess convergent validity, Spearman’s rank correlations were calculated with the HADS and WHOQOL-BREF. The Spearman’s rank correlations of 0.19–0.29 were considered weak, 0.30–0.49 moderate, and >0.5 strong. All data analysis was performed using JAMOVI v. 2.2.5, except for the ICC and CFA, which was performed using IBM SPSS v.21 and Amos v.26. Statistical significance was set at P<0.05, and all tests were two-tailed.
2.6. Ethics approval and consent to participate
All procedures performed in this study were done so in accordance with the ethical standards of the institutional and/or national research committee and the 1964 Helsinki Declaration and its later amendments. The design and methods were reviewed and approved by the ethics committee at the Mongolian National University of Medical Sciences, Ulaanbaatar, Mongolia (number: MNUMS 20/03-05). This study was not a trial and did not require registration. Written informed consent was obtained from all participants.
3. Results
3.1. Demographics and response distributions
This study comprised 739 participants aged 16–65 years with a mean age and standard deviation of 37.42 ± 14.7 years (Table 1).
Among them, 524 (70.9%) were females, 593 (80.2%) were residents out of the Ulaanbaatar city, 488 (66%) were married, and 411 (55.6%) graduated high school or below, 287 (38.8%) were employed, and 500 (67.7%) had low income.
Table 2 presents the distribution of responses for each BOS item in three domains.
The response distributions were skewed toward better conditions indicating floor effects(>29%), but responses to items in excessive thinking tended to have none. A full range of responses to all items had no ceiling effects.
3.2. Reliability
Item analyses included inspecting means, standard deviations, item-to-total correlations, Cronbach’s α and McDonald’s ω to determine internal consistency (Table 3).
McDonald’s ω coefficients of the Mongolian version of the BOS questionnaire were as follows: overall BOS, 0.861; excessive thinking domain, 0.908; hypersensitivity domain, 0.909; and restless behavior domain, 0.889. The overall Cronbach’s α coefficient of the BOS questionnaire was 0.859. The component scores of each item were significantly correlated with the rest, which were 0.520–0.628.
ICC was calculated using a three-factor mixed-effects model with a 95% CI to determine external reliability (Table 4).
A test-retest study was carried out on 366 participants, with an interval of 16 ± 2.3 days between two time points. Participants were aged 16 to 29, and the mean age was 21.55 ± 1.94; 194 (53%) were females. Results from ICC analyses showed that the total score of BOS was 0.75, which indicates moderate reliability. The ICC values of the domains were: excessive thinking domain, 0.73; hypersensitivity, 0.69; restless behavior domain, 0.65.
3.3. Validity
PCA using the varimax rotation method for 10 items of data identified three components with eigenvalue greater than 1, as presented by the scree plot in Figure 1.
PCA using the varimax rotation method for 10 items of data identified three components with eigenvalue greater than 1.
The three components account for 22.9%, 20.3%, and 20% of variance, resulting in 63.2% of the total variance (Table 5).
The KMO value was 0.908 and Bartlett’s test of sphericity was significant (P<0.001), which indicate that the data set was adequately sampled and that factor analysis of the data was appropriate.
We tested the three-component model including 10 items to evaluate how well the three domains were combined to identify the underlying construct of BOS using CFA. Figure 2 presents the factor correlations and loading.
The model had excellent fit indices (RMSEA=0.0332, CFI=0.989, TLI=984) and a test for exact fit showed a significant difference (χ2=58.1, p=0.003). The arrows in Figure 2 are the factor loadings, representing direct effects of the indicators on the latent BOS. The value ranged from 0.74–0.76 for the correlation coefficients between the domains and from 0.62–0.73 for the standardized regression weights. The squared multiple correlations were 0.43–0.53, whereas the measurement errors were represented from e1 to e10.
To determine convergent validity, we analyzed the correlation of each item with its corresponding domain (corrected item-total correlations) and inter-item correlations between the domains (Table 6).
Each item was strongly correlated (≥0.4) with its corresponding domain than the other domains. There was no item correlated more strongly with another domain than with its corresponding domain. Therefore, 10 out of 10 items (100%) met the criterion for item convergence. These results supported the three-domain structure.
To determine criterion validity, we calculated the correlations of the BOS total score and domain scores with the HADS and WHOQOL-BREF total score and domain scores (Table 7).
The BOS total score correlated with the HADS scores (Anxiety r=0.429, p<0.001; Depression r=0.288, p<0.001), which indicates that BOS identifies anxiety and depression. In contrast, the total BOS scores inversely correlated with the WHOQOL-BREF domain scores (physical health: r=-0.396, p<0.001; psychological health r=-0.277, p<0.001; Social relations r=-0.161, p<0.001; environmental health r=-0.323, p<0.001), which suggests that BOS indicates poor QOL. Each BOS domains had the similar results in the correlation to HADS and WHOQOL-BREF, an only exception was the restless behavior domain of BOS did not correlate with the social relationship domain of WHOQOL-BREF.
4. Discussion
We developed a new self-assessment scale, the BOS, which is presented as a reliable instrument for screening mental distress in the general population. The results indicate that the BOS has excellent internal consistency and moderate external reliability. Explorative PCA obtained three constructs including 10 items which was confirmed by CFA indicating good construct validity. These three dimensions, including Excessive Thinking (ET), Hypersensitivity (H), and Restless Behavior (RB), constitute the final version of the BOS (BOS-10) that have been shown to be a valid measure of the severity of mental distress in healthy subjects with no diagnosis. The results of criterion validity suggest that the BOS-10 scores estimate the severity of mental distress, particularly anxiety and depression. The BOS-10 total score and subscale scores were moderately associated with anxiety, whereas only H showed relatively strong correlation with depression. The BOS-10 also depicts a decreased quality of life. The results suggest that the BOS-10 scores indicate a decrease in physical, psychological, social and environmental health, except RB.
Out of five main dimensions we initially hypothesized in our conceptual framework, ET, H, and RB were confirmed by PCA and CFA. ET is the core symptom of the brain overwork syndrome that reflects exhaustion of brain activity due to rumination thinking. We carefully selected the items for ET based on clinical observations. Also, previous studies indicated that people with symptoms such as “thinking too much”, “too much thinking” or “too much use of brain” complain that they feel unrelated to what their world is right now within their neurotic mind indicating brain activity was affected with neuroticism and hypersensitivity [17,18,24,25]. Many studies indicated that life events, childhood maltreatment, negative feedback from parents, and family history of psychiatric diseases were related to the establishment of rumination thinking, which might be a critical pathology of depression and anxiety disorders [26,27]. Furthermore, it’s suggested that rumination thinking is associated with neuroticism and physical diseases, such as diabetes, arthritis, stomach/gallbladder diseases, and chronic cough, in many clinical investigations [28,29,30,31]. On the other hand, some patients tend to pay exert attention to subtle thoughts that might be associated with past psychological events or future worries. Therefore, we proposed to use excessive thinking as it covers not only rumination but also obsessive thinking.
Although hypersensitivity is associated with abnormal reactions to physical stimuli such as drug, light, or noise, we used this symptom to describe an abnormal condition when someone gets highly sensitive to psychological stimuli such as, communication problems, eyesight, or voice. Hypersensitivity might be associated with mental fatigue or brain fatigue that results in mental disorders, including chronic fatigue syndrome, depressive disorders, or suicide [32,33].
Restless behavior covers those symptoms associated with resistance to stress, by the general adaptation syndrome perspective. Those people who have excessive thinking tend to move fast and to be occupied with time. Such people usually think too much and often hurry up in daily works.
This new tool might be helpful to detect mental distress in individuals who are difficult to assess with conventional questionnaires. The BOS is structured of items with simple and concrete expressions that are easily recalled from diverse daily life perspectives. Therefore, it might be useful to identify patients who have alexithymia and alexisomia. Alexithymia is a personality trait characterized by difficulties in the awareness and expression of own emotions. Sifneos introduced the term and indicated alexithymia is associated with psychosomatic diseases including ulcerative colitis and asthma [9]. In clinical practice, many patients complain of physical symptoms that cannot be clearly explained even with appropriate medical examinations, and were usually diagnosed as having medically unexplained symptoms (MUS) or functional somatic syndrome (FSS). Those patients tend to show alexithymia traits including difficulty in identifying emotions, describing feelings to others, and externally-oriented thinking. Previous literature has shown that patients with alexithymia express their mental distress as relatively strong physical symptoms [12]. Moreover, alexisomia is characterized by personality traits of difficulties in identifying and expressing somatic sensations, meaning that patients have no words to describe their bodily states [32,35]. Patients with alexisomia tend to have difficulties to express their mental and somatic symptoms making them hard to understand by clinicians. Taken together, patients with alexithymia or alexisomia are thought to have difficulty to aware and describe their feelings and troubles. The BOS is composed of items made easy to understand for subjects with alexithymia and alexisomia. In clinical settings, this tool might be useful for assessing mental distress in patients with MUS and FSS.
Currently, it is not fully understood how mental distress causes psychiatric disorders. Recent in vivo studies have demonstrated that psychological stress impairs brain structures, such as the hippocampus, extended amygdala, and midbrain raphe, and leads to memory impairment, maladaptive behaviors, and vulnerability to psychosocial stress [36,37,38]. For example, repeated stress exposures decrease spinogenesis and spine stability in the dorsal CA1 pyramidal neurons of the hippocampus in mice, indicating cognitive deficits [36]. In clinical studies, oxidative stress, neuroinflammation, and maladjustment of the gut microbiota might be involved in the pathophysiology of stress-related disorders [32]. Taken together, this study provided a new tool that measures different dimensions of mental distress distinct from anxiety or depression and validated it in a nonclinical population.
This study has several methodological limitations and shortcomings. First, as participants were recruited from the general population of Mongolia, the three-dimensional structure of the BOS-10 is only appropriate for the particular study population. It’s recommended to use the 37-item version of BOS with 5 dimensions if tested in a different population. We had to eliminate two dimensions, including social withdrawal and minor problems in daily life symptoms, out of the 37-item version for the BOS-10. Those dimensions were supposed to detect subjects who avoid asking for help from others and try to do everything themselves not to bother others. However, these characteristics were not typical of Mongolian adults, of whom half are nomadic herders in the countryside. Moreover, nomadic people live close to nature and are relatively free from intensive digital media use, in contrast to urban dwellers. Second, although construct, convergent, and criterion validities were assessed, this study did not examine the discriminant validity. Furthermore, as a cross-sectional study, it did not provide information regarding the persistence of mental distress over time.
To improve the validity of the instrument, future studies should compare with other relevant measurement tools. To further determine the sensitivity and specificity of the instrument, the assessment need to be conducted bot in clinical and nonclinical settings using a longitudinal design. Clinical studies are needed to explain the pathophysiological mechanisms underlying the brain overwork syndrome.
5. Conclusions
The results suggest that the BOS-10 is a valid and reliable instrument for assessing mental distress in the general population of Mongolia. The current findings demonstrated evidence of excellent internal consistency, moderate external reliability, and a three-domain structure for the BOS-10.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Figure S1: Conceptual framework of the Brain Overwork Syndrome. Table S1: Descriptive statistics of the 37-item Brain Overwork Scale (BOS-37)
Author Contributions
T.H. conceived and B.L. contributed to the concept. T.H. and B.L. completed interpretation of data, data analysis, drafting the manuscript, and revision of the manuscript. E.T., E.B., G.T. contributed to data collection and the interpretation of data. V.V., and J.C. contributed to developing items and drafting the manuscript. T.J contributed to the revision of the manuscript. All authors critically reviewed the manuscript and approved the final version.
Funding
This research was funded by The Mongolian Coro-Heart Society for Health and Education —Grant Number 2020MN1. The APC was funded by the same grant.
Institutional Review Board Statement
The design and methods were reviewed and approved by the ethics committee at the Mongolian National University of Medical Sciences, Ulaanbaatar, Mongolia (number: MNUMS 20/03-05). All procedures performed in this study were done so in accordance with the ethical standards of the institutional and/or national research committee and the 1964 Helsinki Declaration and its later amendments. This study was not a trial and did not require registration.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data sharing is not applicable.
Acknowledgements
We thank Ms. Kojima and Ms. Oda for their technical assistance in undertaking this study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Roser, M.; Ritchie, H.; Spooner, F.; Burden of disease. Our World in Data. Available online: https://ourworldindata.org/burden-of-disease/ (accessed on 11 January, 2023).
- GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- Global, regional, and national disability-adjusted life-years (DALYs) for 333 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1260–1344. [CrossRef] [PubMed]
- Kessler, R.C.; Berglund, P.; Demler, O.; Jin, R.; Merikangas, K.R.; Walters, E.E. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch. Gen. Psychiatry 2005, 62, 593–602. [Google Scholar] [CrossRef] [PubMed]
- Thapar, A.; Collishaw, S.; Pine, D.S.; Thapar, A.K. Depression in adolescence. Lancet 2012, 379, 1056–1067. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P.; Snaith, R.P. The hospital anxiety and depression scale. Acta. Psychiatrica. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef]
- Zung, W.W.; Richards, C.B.; Short, M.J. Self-rating depression scale in an outpatient clinic. Further validation of the SDS. Arch. Gen. Psychiatry 1965, 13, 508–515. [Google Scholar] [CrossRef]
- Smith, R.C. Response bias in the State-Trait Anxiety Inventory: detecting the exaggeration of stress. J. Psychol. 1974, 86, 241–246. [Google Scholar] [CrossRef]
- Sifneos, P.E. "The prevalence of 'alexithymic' characteristics in psychosomatic patients". Psychother. Psychosom. 1973, 22, 255–262. [Google Scholar] [CrossRef]
- Tack, M. Medically Unexplained Symptoms (MUS): Faults and Implications. Int. J. Environ. Res. Public Health 2019, 16, 1247. [Google Scholar] [CrossRef] [PubMed]
- Wessely, S.; Nimnuan, C.; Sharpe, M. Functional somatic syndromes: one or many? Lancet 1999, 354, 936–939. [Google Scholar] [CrossRef]
- Graver, C.J. Functional Somatic Syndrome: Assessment and Management. J. Am. Osteopath. Assoc. 2017, 117, 511–519. [Google Scholar] [CrossRef] [PubMed]
- Selye, H.A. Confusion and Controversy in the Stress Field. J. Human Stress 1975, 1, 37–44. [Google Scholar] [CrossRef] [PubMed]
- De Kloet, E.R.; Joels, M.; Holsboer, F. Stress and the brain: from adaptation to disease. Nat. Rev. Neurosci. 2005, 6, 463–475. [Google Scholar] [CrossRef] [PubMed]
- Joels, M.; Baram, T.Z. The neuro-symphony of stress. Nat. Rev. Neurosci. 2009, 10, 459–66. [Google Scholar] [CrossRef] [PubMed]
- Komaroff, A.L.; Lipkin., W.I.L. Insights from myalgic encephalomyelitis/chronic fatigue syndrome may help unravel the pathogenesis of postacute COVID-19 syndrome. Trends Mol. Med. 2021, 27, 895–906. [Google Scholar] [CrossRef] [PubMed]
- Kaiser, B.N.; Haroz, E.E.; Kohrt, B.A.; Bolton, P.A.; Bass, J.K.; Hinton, D.E. "Thinking too much": A systematic review of a common idiom of distress. Soc. Sci. Med. 2015, 147, 170–183. [Google Scholar] [CrossRef] [PubMed]
- Eisma, M.C.; de Lang, T.A.; Boelen, P.A. How thinking hurts: Rumination, worry, and avoidance processes in adjustment to bereavement. Clin. Psychol. Psychother. 2020, 27, 548–558. [Google Scholar] [CrossRef] [PubMed]
- Tumurbaatar, E.; Hiramoto, T.; Tumur-Ochir, G.; Jargalsaikhan, O.; Erkhembayar, R.; Jadamba, T.; Lkhagvasuren, B. Translation, reliability, and structural validity of the Hospital Anxiety and Depression Scale (HADS) in the general population of Mongolia. Neurosci. Res. Notes 2021, 4, 30–39. [Google Scholar] [CrossRef]
- World Health Organization. Development of the World Health Organization WHOQOL-BREF quality of life assessment. The WHOQOL Group. Psychol. Med. 1998, 28, 551–558. [Google Scholar] [CrossRef]
- Bat-Erdene, E.; Tumurbaatar, E.; Tumur-Ochir, G.; Jamiyandorj, O.; Jadamba, T.; Yamamoto, E.; Hamajima, N.; Oka, T.; Lkhagvasuren, B. Validation of the abbreviated version of the World Health Organization Quality of Life in Mongolia: a population-based cross-sectional study among adults in Ulaanbaatar. Nagoya J. Med. Sci. 2013, 85, 79–92. [Google Scholar]
- Koo, T.K.; Li, M.Y.A. Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef]
- Cattell, R.B. The Scree Test For The Number Of Factors. Multivariate Behav. Res. 1996, 1, 245–76. [Google Scholar] [CrossRef]
- Perkins, A.M.; Arnone, D.; Smallwood, J.; Mobbs, D. Thinking too much: self-generated thought as the engine of neuroticism. Trends Cogn. Sci. 2015, 19, 492–498. [Google Scholar] [CrossRef] [PubMed]
- Ehring, T. Thinking too much: rumination and psychopathology. World Psychiatry 2021, 20, 441–442. [Google Scholar] [CrossRef]
- Neeleman, J.; Bijl, R.; Ormel, J. Neuroticism, a central link between somatic and psychiatric morbidity: Path analysis of prospective data. Psychol. Med. 2004, 34, 521–531. [Google Scholar] [CrossRef]
- Weinstock, L.M.; Whisman, M.A. Neuroticism as a common feature of the depressive and anxiety disorders: A test of the revised integrative hierarchical model in a national sample. J. Abnorm. Psychol. 2006, 115, 68–74. [Google Scholar] [CrossRef]
- Neeleman, J.; Sytema, S.; Wadsworth, M. Propensity to psychiatric and somatic ill-health: Evidence from a birth cohort. Psychol. Med. 2002, 32, 793–803. [Google Scholar] [CrossRef] [PubMed]
- Goodwin, R.D.; Cox, B.J.; Clara, I. Neuroticism and physical disorders among adults in the community: Results from the National Comorbidity Survey. J. Behav. Med. 2006, 29, 229–238. [Google Scholar] [CrossRef]
- Rosmalen, J.G.; Neeleman, J.; Gans, R.O.; de Jong, P. The association between neuroticism and self-reported common somatic symptoms in a population cohort. J. Psychosom. Res. 2007, 62, 305–311. [Google Scholar] [CrossRef]
- Hulme, K.; Deary, V.; Dogan, S.; Parker, S.M. Psychological profile of individuals presenting with chronic cough. ERJ Open Res. 2017, 3, 00099–2016. [Google Scholar] [CrossRef]
- Oka, T.; Lkhagvasuren, B. Effects of practicing yoga on alexisomia: an open-label trial. Biopsychosoc. Med. 2022, 16, 14. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.L.; Cotler, J.; Terman, J.M.; Jason, L.A. Risk factors for suicide in chronic fatigue syndrome. Death Stud. 2022, 46, 738–744. [Google Scholar] [CrossRef] [PubMed]
- Kanbara, K.; Fukunaga, M. Links among emotional awareness, somatic awareness and autonomic homeostatic processing. Biopsychosoc. Med. 2016, 10, 16. [Google Scholar] [CrossRef] [PubMed]
- Oka, T. Shitsu-taikan-sho (alexisomia): a historical review and its clinical importance. Biopsychosoc. Med. 2020, 2020 14, 23. [Google Scholar] [CrossRef]
- Chenani, A.; Weston, G.; Ulivi, A.F.; Castello-Waldow, T.P.; Huettl, R.E.; Chen, A.; Attardo, A. Repeated stress exposure leads to structural synaptic instability prior to disorganization of hippocampal coding and impairments in learning. Transl. Psychiatry 2022, 12, 381. [Google Scholar] [CrossRef] [PubMed]
- Hu, P.; Liu, J.; Maita, I.; Kwok, C.; Gu, E.; Gergues, M.M.; Kelada, F.; Phan, M.; Zhou, J.N.; Swaab, D.F.; Pang, Z.P.; Lucassen, P.J.; Roepke, T.A.; Samuels, B.A. Chronic Stress Induces Maladaptive Behaviors by Activating Corticotropin-Releasing Hormone Signaling in the Mouse Oval Bed Nucleus of the Stria Terminalis. J. Neurosci. 2020, 40, 2519–2537. [Google Scholar] [CrossRef]
- Zou, W.J.; Song, Y.L.; Wu, M.Y.; Chen, X.T.; You, Q.L.; Yang, Q.; Luo, Z.Y.; Huang, L.; Kong, Y.; Feng, J.; Fang, D.X.; Li, X.W.; Yang, J.M.; Mei, L.; Gao, T.M. A discrete serotonergic circuit regulates vulnerability to social stress. Nat. Commun. 2020, 11, 4218. [Google Scholar] [CrossRef]
Figure 1.
Scree plot for 10 items of the BOS (n = 739).
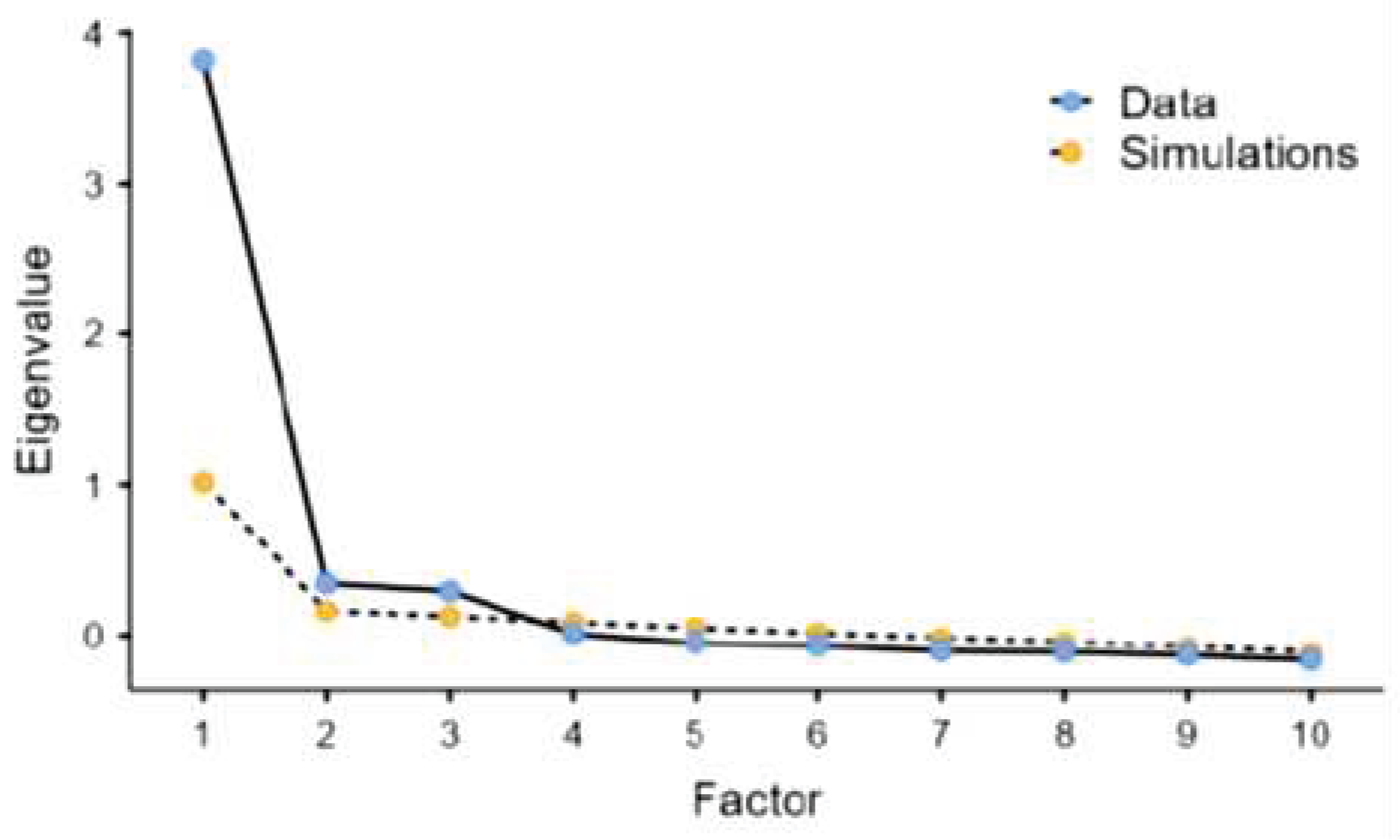
Figure 2.
Confirmatory factor analysis path diagram for the three domains of the BOS (n = 739).The model had excellent fit indices (RMSEA = 0.0332, CFI = 0.989, TLI = 0.984) and a test for exact fit showed a significant difference (χ2(32) = 58.1, p = 0.003). Ellipses represent subscales. Covariances of errors between items with similar content are shown.
Figure 2.
Confirmatory factor analysis path diagram for the three domains of the BOS (n = 739).The model had excellent fit indices (RMSEA = 0.0332, CFI = 0.989, TLI = 0.984) and a test for exact fit showed a significant difference (χ2(32) = 58.1, p = 0.003). Ellipses represent subscales. Covariances of errors between items with similar content are shown.
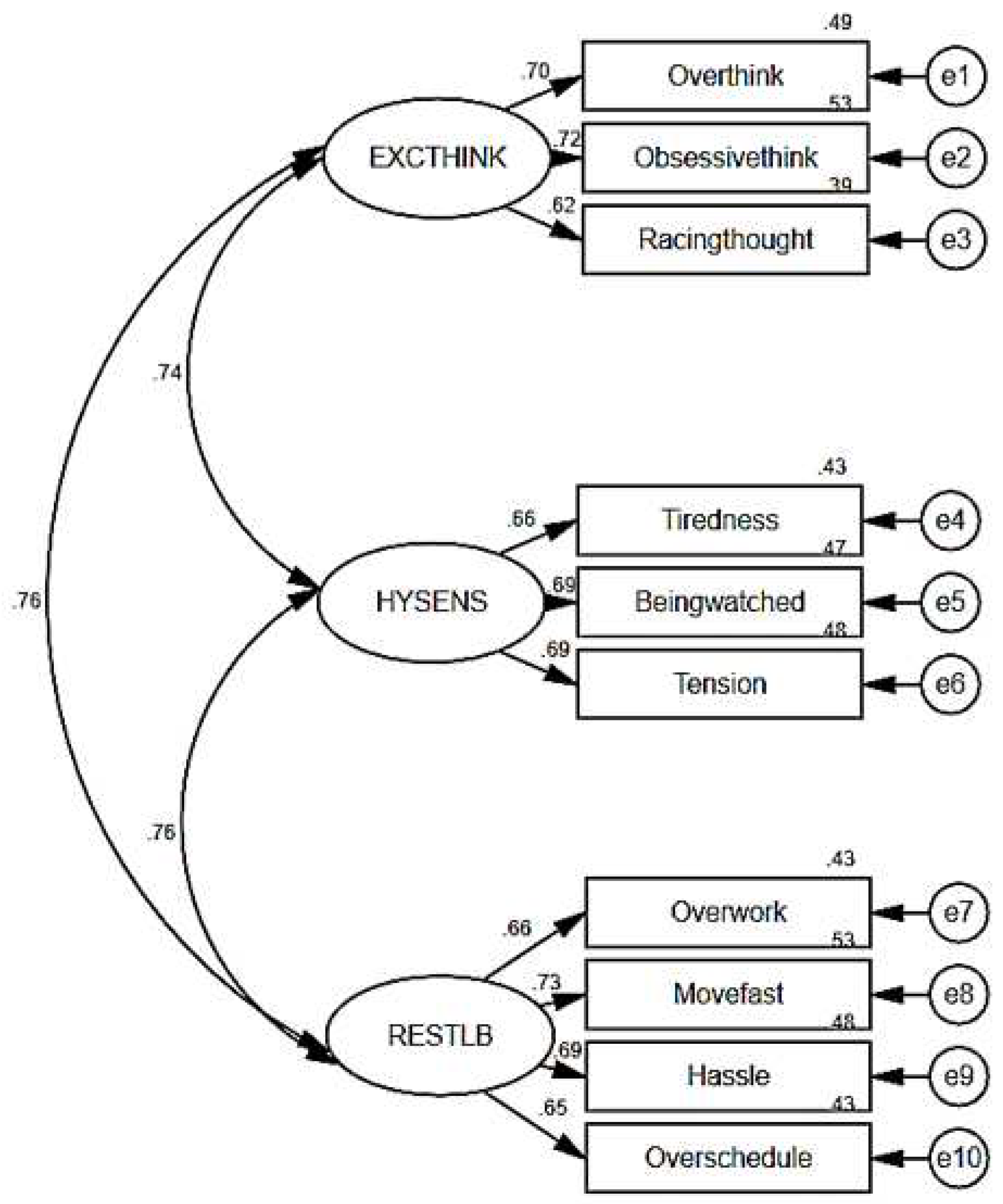

Table 1.
Demographic characteristics of the study subjects (n=739).
| Demographic characteristics | Total | |||
|---|---|---|---|---|
| n | % | |||
| 739 | 100 | |||
| Age (years) | (mean ± SD) | 37.42 ± 14.7 | ||
| Age groups (years) | 16–29 | 281 | 38 | |
| 30–39 | 128 | 17.3 | ||
| 40–49 | 136 | 18.4 | ||
| 50–59 | 133 | 18 | ||
| >60 | 61 | 8.3 | ||
| Gender | Male | 215 | 29.1 | |
| Female | 524 | 70.9 | ||
| Residency | Ulaanbaatar city | 143 | 19.8 | |
| Rural areas | 593 | 80.2 | ||
| Marital status | Never married | 221 | 29.9 | |
| Married | 488 | 66 | ||
| Other* | 30 | 4.1 | ||
| Education level | High school or below | 411 | 55.6 | |
| Below bachelor’s degree | 166 | 22.5 | ||
| Bachelor’s degree | 146 | 19.8 | ||
| Above bachelor’s degree | 16 | 2.2 | ||
| Employment status | Employed | 287 | 38.8 | |
| Herder | 28 | 3.8 | ||
| Pensioner | 155 | 21 | ||
| Student | 201 | 27.2 | ||
| Unemployed | 68 | 9.2 | ||
| Income per month | <$175 | 500 | 67.7 | |
| $175–525 | 231 | 31.3 | ||
| >$525 | 8 | 1.1 | ||
Table 2.
Response distribution for each BOS item (n = 739).
| Item | Response category (%) * | ||||
|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | |
| Domain 1: Excessive thinking | |||||
| I tended to overthink even the (most) minor of events. | 21.8 | 41.8 | 19.9 | 12.3 | 4.2 |
| I tended to stick to one way of doing or thinking about something. | 38.2 | 31.9 | 19.1 | 8.5 | 2.3 |
| I had racing thoughts (was thinking something a lot). | 15.6 | 42.8 | 21.5 | 14.5 | 5.7 |
| Domain 2: Hypersensitivity | |||||
| I felt tired when reading newspapers / magazines. | 52.5 | 24.4 | 15.8 | 5.1 | 2.2 |
| I felt that others were watching me. | 44.8 | 29.1 | 19.4 | 3.8 | 3.0 |
| I easily felt tense in public. | 40.3 | 26.5 | 20.8 | 8.4 | 3.9 |
| Domain 3: Restless behavior | |||||
| I did not like to have leisure time. | 38.6 | 23.5 | 22.5 | 11.2 | 4.2 |
| I tended to walk or move fast. | 37.1 | 21.2 | 13.9 | 19.9 | 7.8 |
| I was not good at waiting. | 38.6 | 23.4 | 14.2 | 13.7 | 10.1 |
| My notebook was full of schedules. | 40.2 | 25.7 | 19.5 | 11.2 | 3.4 |
BOS: Brain Overwork Scale; * 1: very inaccurate / never (0 day per week), 2: moderately inaccurate / rarely (1-2 day(s) per week), 3: neutral / Sometimes (3-4 days per week), 4: moderately accurate / frequently (5-6 days per week), 5: very accurate / always (7 days per week).
Table 3.
Means, standard deviations (SD), Cronbach’s α and McDonald's ω of BOS items and domains (n=739).
Table 3.
Means, standard deviations (SD), Cronbach’s α and McDonald's ω of BOS items and domains (n=739).
| Item | Mean | SD | Cronbach's α | McDonald's ω |
|---|---|---|---|---|
| Overall reliability | 2.18 | 0.767 | 0.859 | 0.861 |
| 1. I tended to overthink even the (most) minor of events | 2.35 | 1.08 | 0.846 | 0.848 |
| 2. I tended to stick to one way of doing or thinking about something | 2.05 | 1.06 | 0.845 | 0.846 |
| 3. I had racing thoughts (was thinking something a lot) | 2.52 | 1.09 | 0.850 | 0.851 |
| 4. I felt tired when reading newspapers / magazines | 1.80 | 1.02 | 0.849 | 0.850 |
| 5. I felt that others were watching me | 1.91 | 1.03 | 0.847 | 0.848 |
| 6. I easily felt tense in public | 2.09 | 1.14 | 0.846 | 0.847 |
| 7. I did not like to have leisure time | 2.19 | 1.18 | 0.847 | 0.849 |
| 8. I tended to walk or move fast | 2.40 | 1.36 | 0.841 | 0.843 |
| 9. I was not good at waiting | 2.33 | 1.37 | 0.843 | 0.844 |
| 10. My notebook was full of schedules | 2.12 | 1.16 | 0.845 | 0.847 |
| Domain 1: Excessive thinking | 6.92 | 2.59 | 0.818 | 0.908 |
| Domain 2: Hypersensitivity | 5.80 | 2.55 | 0.821 | 0.909 |
| Domain 3: Restless behavior | 9.04 | 3.94 | 0.742 | 0.889 |
| BOS total score | 21.77 | 7.67 | 0.769 | 0.792 |
Table 4.
Intraclass correlation coefficients (ICC) of the BOS (n=366).
| Domains | Mean ± standard deviation | ICC | |
|---|---|---|---|
| Test | Retest | ||
| Domain 1: Excessive thinking | 9.11± 2.91 | 8.72± 2.98 | 0.730 |
| Domain 2: Hypersensitivity | 7.72± 2.66 | 7.49± 2.55 | 0.690 |
| Domain 3: Restless behavior | 11.8± 3.01 | 11.7± 2.97 | 0.650 |
| BOS total score | 28.7± 6.85 | 27.9± 7.11 | 0.750 |
Table 5.
Principal component analysis of the BOS (n=739).
| Components | Factor loadings (explained variance %) | Uniqueness | ||
|---|---|---|---|---|
| Excessive thinking (22.9) | Hypersensitivity (20.3) | Restless behavior (20) | ||
| I tended to overthink even the (most) minor of events. | 0.766 | 0.332 | ||
| I tended to stick to one way of doing or thinking about something. | 0.727 | 0.329 | ||
| I had racing thoughts (was thinking something a lot). | 0.722 | 0.398 | ||
| I felt tired when reading newspapers / magazines. | 0.772 | 0.341 | ||
| I felt that others were watching me. | 0.727 | 0.362 | ||
| I easily felt tense in public. | 0.712 | 0.383 | ||
| I did not like to have leisure time. | 0.807 | 0.311 | ||
| I tended to walk or move fast. | 0.713 | 0.367 | ||
| I was not good at waiting. | 0.651 | 0.405 | ||
| My notebook was full of schedules. | 0.646 | 0.451 | ||
BOS: Brain Overwork Scale.
Table 6.
Convergent validity of the BOS (n=739).
| Items/ Domains | Domains | ||
|---|---|---|---|
| Excessive thinking | Hypersensitivity | Restless behavior | |
| Item convergence (r ≥ 0.4) | 3/3 | 3/3 | 4/4 |
| Corrected item-total correlations | |||
| Domain 1: Excessive thinking | |||
| I tended to overthink even the (most) minor of events | 0.799*** | 0.415*** | 0.466*** |
| I tended to stick to one way of doing or thinking about something | 0.789*** | 0.483*** | 0.467*** |
| I had racing thoughts (was thinking something a lot) | 0.770*** | 0.388*** | 0.459*** |
| Domain 2: Hypersensitivity/brain fatigue | |||
| I felt tired when reading newspapers / magazines | 0.384*** | 0.784*** | 0.481*** |
| I felt that others were watching me | 0.477*** | 0.797*** | 0.476*** |
| I easily felt tense in public | 0.466*** | 0.836*** | 0.530*** |
| Domain 3: Restless behavior | |||
| I did not like to have leisure time | 0.411*** | 0.492*** | 0.783*** |
| I tended to walk or move fast | 0.500*** | 0.531*** | 0.826*** |
| I was not good at waiting | 0.533*** | 0.498*** | 0.815*** |
| My notebook was full of schedules | 0.445*** | 0.540*** | 0.757*** |
| Inter-item correlations for domains | |||
| Domain 1: Excessive thinking | - | - | - |
| Domain 2: Hypersensitivity/brain fatigue | 0.547*** | - | - |
| Domain 3: Restless behavior | 0.590*** | 0.615*** | - |
BOS: Brain Overwork Scale; ***p<0.001; p-values were calculated using Spearman’s correlations.
Table 7.
Criterion validity of the BOS (n=739).
| Questionnaires | BOS | ||||
|---|---|---|---|---|---|
| BOS Total | Excessive thinking | Hypersensitivity | Restless behavior | ||
| HADS (Hospital Anxiety and Depression Scale) | |||||
| Anxiety | 0.429*** | 0.481*** | 0.417*** | 0.248*** | |
| Depression | 0.288*** | 0.292*** | 0.330*** | 0.160*** | |
| WHOQOL-BREF (An Abbreviated Version of the World Health Organization Quality of Life) | |||||
| Perception on quality of life | -0.086* | -0.114** | -0.126*** | -0.003 | |
| Perception on general health | -0.254*** | -0.263*** | -0.268*** | -0.150*** | |
| Physical health | -0.396*** | -0.367*** | -0.389*** | -0.296*** | |
| Psychological health | -0.277*** | -0.278*** | -0.354*** | -0.138*** | |
| Social relations | -0.161*** | -0.168*** | -0.250*** | -0.033 | |
| Environmental health | -0.323*** | -0.287*** | -0.346*** | -0.221*** | |
BOS: Brain Overwork Scale, *p<0.05, **p<0.01, ***p<0.001; p-values were calculated using Spearman’s correlations.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



