
Submitted:
21 February 2023
Posted:
22 February 2023
You are already at the latest version
Abstract
This study analysed through the perspective of networks the association between physical activity (PA), sedentary behaviour (SB), and cardiovascular risk factors in overweight low-income schoolchildren from the perspective of complex systems. Methods: The sample consisted of 41 overweight children between 6 and 10 years old (56% girls). PA and SB were analysed by accelerometer, and the measures of cardiovascular factor risk were: anthropometric and hemodynamic measurements, body fat, lipid profile and glucose, cardiorespiratory fitness (CRF), left ven-tricular mass (LVM), and Sokolov-Lyon. Network analysis with Boot-strap-1000 was performed to analyze the association between PA, SB and the cardiovascular risk factors. Results: Moderate to vigorous PA was positive related with Waist circumference (WC; 0.499), HDL-C (0.307), and CRF (0.276), and negatively associated with BMI (-0.251) and Fat (-0.341). For SB, positive associations were seen with WC (0.326), CRF (0.296), LVM (0.250) and Sokolov (0.215). Adicionalment, the centrality indicators highlighted WC as the most important variable in the network. Conclu-sion: Interventions that aim to mitigate the harmful effects of obesity on cardiovascular risk factors in overweight children should consider WC as an important variable in of system.
Keywords:
Cardiovascular factors
; Network analysis
; Obese children
; Physical activity
; Sedentary behaviour.
1. Introduction
Overweight and obesity in childhood have a complex etiology, involving the simultaneous non-linear interactions between genetic, biological, environmental and behavioural factors [1]. Children from low-income settings show a high prevalence of obesity [2] and are more likely to develop cardiovascular risk factors, such as decreased glucose tolerance and type 2 diabetes mellitus, high lipid profile, high systolic blood pressure and atherosclerosis [3,4]. Furthermore, overweight children tend to have greater left ventricle mass (LVM) hypertrophy, when compared to their normal-weight peers [5]. LVM is a dysfunction that appears even before other cardiovascular risk factors, such as arterial hypertension. Despite being considered the best indicator of a coronary lesion, the analysis of LVM has still been neglected in children [6].
It is also known that children’s movement behaviours, such as low levels of physical activity (PA), and high time spent in sedentary behaviour (SB) are associated to cardiovascular risk factors incidence, and tend to be more prevalent in overweight and obese children [4], living in socially vulnerable contexts. Studies point out that in middle-income countries such as Brazil, low socio-economic status is related to lifestyle determinants for obesity, once it hinders access to healthy foods and PA opportunities [7,8]. Moderate-to-vigorous physical activity (MVPA) is related to improvements in cardiorespiratory fitness (CRF) (Ross et al. 2016) and acts as a protective factor against cardiovascular diseases [9]. Conversely, results of a recent review study show that SB, assessed through screen time, negatively influences outcomes related to cardiovascular health and childhood obesity [10], though further studies using objective measures of SB are needed.
In fact, movement behaviours such as MVPA and SB are interrelated [11]. Moreover, the different cardiovascular risk factors are also interrelated [12,13] and can cluster in the same person [14]. Therefore, factors involved in obesity´s etiology, such as movement behaviours and cardiovascular risk factors, should be seen as a dynamic, non-linear, and integrated system. Considering that the presence or absence of a single variable within a model composed by interrelated variables may completely change its nature [15], from a theoretical and statistical perspective, the possible dynamic relationships between movement behaviours and cardiovascular risk factors might be explored through a network perspective, taken into account its non-linearity [16]. Thus, the present study aimed to analyze the relationship between MVPA, SB, and cardiovascular risk factors in overweight low-income children through a network approach.
2. Materials and Methods
2.1. Study Description
This cross-sectional study used baseline data from the school-based program “Panpes”, which aimed to analyze the effects of a multicomponent intervention on health and behavioral outcomes of obese children. All the Helsinki Declarations’ ethical aspects were followed (Association, 2013). The evaluation methods and procedures were approved by the Research Ethics Committee of Health Science Center (protocol n. 1.311.598) and by the Education Board of the city.
2.2. Sample
Eligibility criteria to schools and children´s selection were established as follow:
-
School:
- -
- elementary public schools, from central and suburban and deprived areas from Petrolina-PE, Brazil;
- -
- indoor gym and with a minimum of one hundred students;
- -
- overweight children [85th percentile for sex and age, according to the World Health Organization [17]
-
Children:
- -
- overweight or obese [17];
- -
- properly enrolled in participating schools;
- -
- parental consent to participate.
Two schools met the inclusion criteria. All parents of overweight children found in both schools were invited to participate in the study (60 children in all).
2.3. Data Collection
Data were collected in February 2016 by five physical education teachers and three cardiologists, who were previously trained and supervised by the project´s coordinator. Data were collected at the school (anthropometric, hemodynamic measurements, lipid and glucose profile, cardiorespiratory fitness, physical activity, and SB) and the clinic of cardiology (left ventricular mass), during the weekend, in moments previously scheduled with the parents and the school board.
- Anthropometric measurements
Body mass (kg), body height (cm), and waist circumference (WC; cm) measurements were assessed following WHO standardization [17]. Body mass was measured using a Welmy® digital scale with 100g accuracy. To measure body height, a stadiometer attached to the scale was used. The vertex and the plantar region of the children were used as reference points, and body mass index (BMI) was calculated. Children who presented BMI above the 85th percentile for age and sex were considered overweight [17]. In all measurements, children were standing bare feet and wearing light clothes.
WC was assessed at the midline between the lower edge of the rib cage and the upper limit of the iliac crest and was measured with Sanny® metal tape measuring 1mm [17].
The sum of skinfolds (triceps and subscapular skinfolds) was performed according to the standardization protocol proposed by Harrison et al. [18], using a Lange® skinfold caliper.
All anthropometric measurements were performed in triplicate, by the same evaluator. For analysis, the mean value was adopted.
- Hemodynamic measurements
Systemic blood pressure was measured by a single evaluator, using a digital automatic device (Omron®); this equipment has good levels of sensitivity and specificity for blood pressure measurements in children and adolescents [19]. Three measurements were performed, with a five-minute interval, according to the Brazilian Society of Cardiology [20], and the median value was used for analysis. This procedure has already been adopted in previous studies [21]. Mean blood pressure (MBP) was considered for the analysis, the same was calculated by [(2 x diastolic blood pressure) + systolic blood pressure)/3].
- Lipid and glucose profile
For biochemical profile measurements, 10 ml of venous blood were collected from the antecubital vein after 12 hours of fasting. The blood sample was deposited in a vacuum tube with separating gel and without anticoagulant and was stored in thermal boxes for later analysis in a specialized laboratory. Triglycerides (TG), total cholesterol (TC), low-density cholesterol (LDL-C), high-density cholesterol (HDL-C), and glucose levels were determined in mg/dl [22].
- Cardiorespiratory Fitness
Cardiorespiratory fitness (CRF) was verified through the 6-minute running and walking test proposed by Gaya et al [23]. The test was conducted on the school court and was performed individually. The test was guided by a Physical Education teacher, who monitored the time and verified the distance reached by the child during the given time. During the test, motivational words were directed to the children.
- Left Ventricular Mass
Left ventricular end-diastolic and end-systolic measurements were obtained with the patient in a partial left lateral position according to recommendations by the American Society of Echocardiography [24]. Frames with optimal visualization of interfaces and showing simultaneous visualization of the septum, left ventricular internal diameter, and posterior wall were used. A Level 3 echocardiographer performed the interpretations. Left ventricular mass was calculated by using the Devereux formula: left ventricular mass (g) = 0.80 × + 0.6 g. The left ventricular mass was indexed according to body surface area.
The voltage based on the Sokolow-Lyon criteria has been used to diagnose left ventricular hypertrophy and has been associated with the presence of cardiovascular disease [25]. Individual leads were analyzed by measuring the tallest R or R′ and the deepest S or QS complex in all the precordial and using the PR segment as baseline. In cases of voltage differences within the same lead, only the largest complex was selected. The proposed criteria were obtained by adding SD to the in V4 (SD + SV4). The Sokolow-Lyon voltage was obtained by adding the amplitude of S in V1 and the amplitude of R in V5 or V6 ≥3.5 mV (SV1 + RV5 or RV6); the limb lead voltage criteria amplitude of R in aVL >1.1 mV (RaVL) and amplitude of R in L1 >1.4 mV (RL1).
- Physical activity and Sedentary Behaviour
PA and SB were objectively measured using accelerometry (GT3X+, ActiGraph®, USA). Children were instructed to use the accelerometer affixed to the waist during eight consecutive days and remove for fighting and water activities, and at night.
Data were collected at a sampling rate of 80 Hz and epochs of 15 seconds. To reduce the data, the ActiLife 6.12 software was used, and data validity was set adopting the following criteria: three weekdays, and one weekend day; at least 10 hours/day of registered data (06: 00h to 00: 00h); 10 or more consecutive minutes of zero counts were established as non-wear time [26]. The time spent in SB and MVPA were obtained by the weighted average of minutes/day, using established cut-off points proposed by Evenson et al. [27].
- Data management and statistical analysis
To characterize the sample, a Student T-test was used to compare the means of all variables between boys and girls.
A network analysis was conducted to assess the associations between MVPA, SB, and cardiovascular risk factors. The “Fruchterman-Reingold” algorithm was applied, and data were shown in a relative space in which variables with strong permanent statistics are together, and with weak applied variations repelled one another [28]. The least absolute contraction and selection operator was used to obtain regularization and to obtain a less sparse model [29]. The partial correlation parameter was adjusted to 0.25 to create a network with greater parsimony and specificity [30]. Additionally, a 1.000-bootstrap resampling was performed.
Three centrality indicators were used to determine the role of each variable in the emerged network: (1) betweenness (centrality between the parts), estimated from the number of times that a node is part of the shortest path among all the others pairs of nodes connected to the network; (2) closeness, which is determined from the inverse of the distances from one node to all others; and (3) strength (degree/centrality), which is the sum of all the weights of the paths that connect a node to the others [31]. The Jasp software version 0.12 was used.
3. Results
Sixty children were invited to participate in the study, of which 19 were not included (did not present parental consent or did not attend assessments). Thus, 41 children (56% girls; 7.85 ± 0.96 years-old) were evaluated. Boys were more active and less sedentary than girls, as they spent more 10 min/day on MVPA and less 60 min/day on SB (Table 1).
The space visualization of the network is presented in Figure 1. The blue color expresses positive relationships, and negative relationships between the variables are expressed by the red color. The thickness and saturation of the colors indicate the weight of the relationship.
Positive relationships were seen between MVPA and WC (0.499), HDL-C (0.307), and CRF (0.276). Conversely, MVPA was negatively associated with BMI (-0.251) and Fat (-0.341). For SB, positive associations were seen with WC (0.326), CRF (0.296), LVM (0.250) ans Sokolov (0.215) (Table 2).
The centrality indicators highlighted WC as the most important variable in the network, according to the Betweenness, Closeness, and Strength indexes (Table 3).
4. Discussion
This study analyzed the association between different factors involved in obesity etiology, considering the synergic relationships between them as a network, in a sample of overweight low-income schoolchildren. Our main results showed a positive association between MVPA and HDL, CRF, and WC.
It is well known that in general, overweight/obese children tend to spend less time on MVPA than their normal-weight peers [32]. Although the assessed children do not comply with the recommended 60 minutes/day of MVPA, our results are, at least partially, in line with previous studies, as MVPA was positively associated with several cardiovascular outcomes. CRF is an important cardiovascular health indicator [33], negatively related to body fat (Fairchild, 2016), which mediates the association between CRF and clustered cardiovascular risk factors [34]. Cardiovascular benefits are seen at higher PA intensities (Tarp, 2018), as higher intensities may provide sympathetic activity reduction, increased vasodilation, and consequently, increased vascular benefits when comparing to low PA intensities [35]. So, in children, CRF develops as a consequence of MVPA (Andersen, 2011). The observed positive association between MVPA and CRF is somehow expectable, as even in obese children, this association may be seen [36].
Our results also showed a negative association between MVPA and BMI and body fat. Such results are already evidenced in the literature, and MVPA interventions in obese children promote a decrease in body fat and also in BMI [37,38] (xxx). The most pointed explanation in the literature is related to changes in the energy balance [39].
The results showed a positive association between SB and LVM and Sokolov index. The indicators of hypertrophy of left ventricle represent a worrying variable, since obese children may be more prone to this condition. However, no study analyzed the relationship between SB and LVM in this population, though the increase in the thickness of the left ventricular wall and the sedentary lifestyle has been identified as the main characteristics among children and young adults’ victims of sudden death [40]. It is important to consider that the high duration and frequency of SB are associated with metabolic markers with a higher cluster cardiovascular risk score [10].
Moreover, this study highlighted a positive association between MVPA and WC, SB, and CRF. Regarding WC, some factors may partially explain this adverse association: firstly, PA may promote a compensatory effect, increasing caloric intake [41], additionally, studies suggest that MVPA is positively associated with time spent in SB in children [42]. Euklend et al. showed that positive changes in WC may be seen only for those children who spend longer MVPA periods [43].
The positive association between SB and CRF, and although its association is most often verified with MVPA it has been observed in association with time in sedentary activities [44] and when the time in SB is not prolonged [45]. Again, this situation can also be the result of the compensatory effect, since the CRF is improved with more intense BP.
The cardiovascular risk factors and obesity, especially in childhood, present confusing relationships, since several factors can influence these associations, such as the period of intrauterine life [46], genetic aspects [47] and even eating behaviour [48].
The network system also showed WC as the most important variable in the network, reinforcing its importance as a useful and easy-assessing measure. A priori studies have shown that WC can be used to stratify risk groups in children [49,50]. In the study by Sonmez et al. [51] it was found that WC was associated with greater carotid artery thickness in obese children, while BMI was not. This situation demonstrates the importance of this variable in the detection of subclinical cardiovascular diseases, including left ventricular hypertrophy [52]. This result is in line with the International Diabetes Federation when suggesting that due to the impossibility of detecting metabolic syndrome in children under 10 years old, WC should be considered as the main predictor of cardiovascular risk factor [53], considering its strong association with insulin resistance, hyperlipidemia, and blood pressure [54].
There are some limitations that authors are aware of. The results of this study should be interpreted with caution, considering its limited sample, although the statistical analysis used is robust enough to support small sample sizes without compromising the results, and the Bootstrap resampling process used, which minimize possible bias. Moreover, the assessment of several cardiovascular risk factors in a low-income overweight/obese child´s sample, and the use of objectively measures of MVPA, SB, and LVM are strengths that should be highlighted.
The present study demonstrated that cardiovascular risk factors are interrelated, and showed that even in overweight low-income children, more time spent in MVPA and less time in SB, are related to cardiovascular health. Interventions targeting cardiovascular health in this population should focus on reducing abdominal fat.
Author Contributions
Conceptualization, T.B., A.S.F and F.C.; methodology, T.B., A.S.F. and F.C.; formal analysis, N.Q., L.C. and P.B.; data curation, T.B., A.S.F., N.Q., L.C., and P.N; writing—original draft preparation, T.B., A.S.F., N.Q., L.C., P.B., and C.R.; writing—review and editing, C.R., C.M. and F.C.; visualization, C.M. and F.C.; supervision, F.C.; project administration, F.C. All authors have read and agreed to the published version of the manuscript.
Funding
No financial or material support of any kind was received for the work described in this article.
Institutional Review Board Statement
All the Helsinki Declarations’ ethical aspects were followed (Association, 2013). The evaluation methods and procedures were approved by the Research Ethics Committee of Health Science Center (protocol n. 1.311.598) and by the Education Board of the city.
Informed Consent Statement
All children participating in the study had their parent/guardian’s authorization registered in the Consent Form. By signing the Consent Form, all parents/guardians of the children participating in the study authorized the publication of the data, as long as the identification and integrity of the children remained safe.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors have no conflict of interest relevant to this article.
References
- Swinburn B, Egger G Fau - Raza F, Raza F (1999) Dissecting obesogenic environments: the development and application of a framework for identifying and prioritizing environmental interventions for obesity. Prev Med 29 (0091-7435 (Print)):8. [CrossRef]
- Rogers R, Eagle TF, Sheetz A, Woodward A, Leibowitz R, Song M, Sylvester R, Corriveau N, Kline-Rogers E, Jiang Q, Jackson EA, Eagle KA (2015) The Relationship between Childhood Obesity, Low Socioeconomic Status, and Race/Ethnicity: Lessons from Massachusetts. Child Obes 11 (6):6. [CrossRef]
- Ajala OA-O, Mold F, Boughton C, Cooke D, Whyte M (2017) Childhood predictors of cardiovascular disease in adulthood. A systematic review and meta-analysis. Obes Rev 18 (1467-789X (Electronic)):9. [CrossRef]
- Weihrauch-Blüher S, Wiegand S (2018) Risk Factors and Implications of Childhood Obesity. Curr Obes Rep 7 (4):6. [CrossRef]
- de Simone G, Devereux Rb Fau - Daniels SR, Daniels Sr Fau - Koren MJ, Koren Mj Fau - Meyer RA, Meyer Ra Fau - Laragh JH, Laragh JH (1995) Effect of growth on variability of left ventricular mass: assessment of allometric signals in adults and children and their capacity to predict cardiovascular risk. J Am Coll Cardiol 25 (5):7. [CrossRef]
- Dušan P, Tamara I Fau - Goran V, Goran V Fau - Gordana M-L, Gordana Ml Fau - Amira P-A, Amira PA (2015) Left ventricular mass and diastolic function in obese children and adolescents. Pediatr Nephrol 30 (4):8. [CrossRef]
- Wang Y, Lim H (2012) The global childhood obesity epidemic and the association between socio-economic status and childhood obesity. Int Rev Psychiatry 24 (3):13. [CrossRef]
- Dinsa GD, Goryakin Y Fau - Fumagalli E, Fumagalli E Fau - Suhrcke M, Suhrcke M (2012) Obesity and socioeconomic status in developing countries: a systematic review. Obes Rev 13 (11):13. [CrossRef]
- Ruiz JR, Cavero-Redondo I, Ortega FB, Welk GJ, Andersen LB, Martinez-Vizcaino V (2016) Cardiorespiratory fitness cut points to avoid cardiovascular disease risk in children and adolescents; what level of fitness should raise a red flag? A systematic review and meta-analysis. Br J Sports Med 50 (23):8. [CrossRef]
- Carson V, Hunter S, Kuzik N, Gray CE, Poitras VJ, Chaput JP, Saunders TJ, Katzmarzyk PT, Okely AD, Connor Gorber S, Kho ME, Sampson M, Lee H, Tremblay MS (2016) Systematic review of sedentary behaviour and health indicators in school-aged children and youth: an update. Appl Physiol Nutr Metab 6 (1715-5320 (Electronic)):25. [CrossRef]
- Pearson N, Braithwaite Re Fau - Biddle SJH, Biddle Sj Fau - van Sluijs EMF, van Sluijs Em Fau - Atkin AJ, Atkin AJ (2014) Associations between sedentary behaviour and physical activity in children and adolescents: a meta-analysis. Obes Rev 15 (8):12. [CrossRef]
- Liu M, Li Xc Fau - Lu L, Lu L Fau - Cao Y, Cao Y Fau - Sun RR, Sun Rr Fau - Chen S, Chen S Fau - Zhang PY, Zhang PY (2014) Cardiovascular disease and its relationship with chronic kidney disease. Eur Rev Med Pharmacol Sci 18 (19):8.
- Zoran G, Bozidarka Z, Ivana R, Milan O, Aleksandar M, Djordje R, Esma RI (2017) Link between Metabolic Syndrome and Insulin Resistance. Current Vascular Pharmacology 15 (1):30-39. [CrossRef]
- Andersen LB, Wedderkopp N Fau - Hansen HS, Hansen Hs Fau - Cooper AR, Cooper Ar Fau - Froberg K, Froberg K (2003) Biological cardiovascular risk factors cluster in Danish children and adolescents: the European Youth Heart Study. Prev Med 37 (4):4. [CrossRef]
- Borsboom D, Cramer AO (2013) Network analysis: an integrative approach to the structure of psychopathology. Annu Rev Clin Psycho 9 (1548-5951 (Electronic)):30. [CrossRef]
- Schmittmann VD, Cramer AOJ, Waldorp LJ, Epskamp S, Kievit RA, Borsboom D (2013) Deconstructing the construct: A network perspective on psychological phenomena. New Ideas in Psychology 31 (1):43-53. [CrossRef]
- Organization W-WH (1995) Physical status: the use and interpretation of anthropometry. Report of a WHO Expert Committee. World Health Organ Tech Rep Ser, vol 854.
- Harrison K, Bost KK, McBride BA, Donovan SM, Grigsby-Toussaint DS, Kim J, Liechty JM, Wiley A, Teran-Garcia M, Jacobsohn GC (2011) Toward a Developmental Conceptualization of Contributors to Overweight and Obesity in Childhood: The Six-Cs Model. Child Development Perspectives 5 (1):50-58. [CrossRef]
- Furusawa EA, Ruiz Mf Fau - Saito MI, Saito Mi Fau - Koch VH, Koch VH (2005) Evaluation of the Omron 705-CP blood pressure measuring device for use in adolescents and young adults (Avaliação do monitor de medida de pressão arterial OMRON 705-CP para uso em adolescentes e adultos jovens. DEP - 20050524). Arq Bras Cardiol 84 (5):8. [CrossRef]
- Brandão AA, Rodrigues CIS, Consolim-Colombo F, Plavnik FL, Malachias MVB, Kohlmann Junior O, Ferreira Filho SJABC (2010) VI diretrizes brasileiras de hipertensão. vol 95.
- Souza CBd, Dourado CdS, Mill JG, Salaroli LB, Molina MdCBJIJoCS (2017) Prevalência de Hipertensão em Crianças de Escolas Públicas. International Journal of Cardiovascular Sciences 30 (1):42-51. [CrossRef]
- Xavier HT, Izar M, Faria Neto J, Assad M, Rocha V, Sposito A, Fonseca F, Dos Santos J, Santos R, Bertolami MJAbdc (2013) V Diretriz brasileira de dislipidemias e prevenção da aterosclerose. vol 101.
- Gaya A, Gaya A (2016) Projeto Esporte Brasil: manual de testes e avaliação versão 2016. UFRGS, Porto Alegre.
- Devereux Rb Fau - Alonso DR, Alonso Dr Fau - Lutas EM, Lutas Em Fau - Gottlieb GJ, Gottlieb Gj Fau - Campo E, Campo E Fau - Sachs I, Sachs I Fau - Reichek N, Reichek N (1986) Echocardiographic assessment of left ventricular hypertrophy: comparison to necropsy findings. Am J Cardiol 57 (6):9. [CrossRef]
- Kohsaka S, Sciacca Rr Fau - Sugioka K, Sugioka K Fau - Sacco RL, Sacco Rl Fau - Homma S, Homma S Fau - Di Tullio MR, Di Tullio MR (2005) Additional impact of electrocardiographic over echocardiographic diagnosis of left ventricular hypertrophy for predicting the risk of ischemic stroke. Am Heart J 149 (1):7. [CrossRef]
- Engelen L, Bundy Ac Fau - Naughton G, Naughton G Fau - Simpson JM, Simpson Jm Fau - Bauman A, Bauman A Fau - Ragen J, Ragen J Fau - Baur L, Baur L Fau - Wyver S, Wyver S Fau - Tranter P, Tranter P Fau - Niehues A, Niehues A Fau - Schiller W, Schiller W Fau - Perry G, Perry G Fau - Jessup G, Jessup G Fau - van der Ploeg HP, van der Ploeg HP (2013) Increasing physical activity in young primary school children--it’s child’s play: a cluster randomised controlled trial. Prev Med 56 (5):6. [CrossRef]
- Evenson KR, Catellier Dj Fau - Gill K, Gill K Fau - Ondrak KS, Ondrak Ks Fau - McMurray RG, McMurray RG (2008) Calibration of two objective measures of physical activity for children. J Sports Sci 26 (14):10. [CrossRef]
- Fruchterman TMJ, Reingold EM (1991) Graph drawing by force-directed placement. Software: Practice and Experience 21 (11):1129-1164. [CrossRef]
- Friedman J, Hastie T, Tibshirani R (2008) Sparse inverse covariance estimation with the graphical LASSO. Biostatistics (Oxford, England) 9:432-441. [CrossRef]
- Foygel R, Drton M Extended Bayesian information criteria for Gaussian graphical models. In: Advances in neural information processing systems, 2010. pp 604-612.
- Epskamp S, Cramer AOJ, Waldorp LJ, Schmittmann VD, Borsboom D (2012) qgraph: Network Visualizations of Relationships in Psychometric Data. Journal of Statistical Software; Vol 1, Issue 4 (2012). [CrossRef]
- Raistenskis J, Sidlauskiene A, Strukcinskiene B, Uğur Baysal S, Buckus R (2016) Physical activity and physical fitness in obese, overweight, and normal-weight children. Turk J Med Sci 46 (2):8. [CrossRef]
- Bailey DP, Charman SJ, Ploetz T, Savory LA, Kerr CJ (2017) Associations between prolonged sedentary time and breaks in sedentary time with cardiometabolic risk in 10-14-year-old children: The HAPPY study. J Sports Sci 35 (22):8. [CrossRef]
- Ekelund U, Anderssen SA, Froberg K, Sardinha LB, Andersen LB, Brage S (2007) Independent associations of physical activity and cardiorespiratory fitness with metabolic risk factors in children: the European youth heart study. Diabetologia 50 (9):9. [CrossRef]
- García-Hermoso A, Cerrillo-Urbina AJ, Herrera-Valenzuela T, Cristi-Montero C, Saavedra JM, Martínez-Vizcaíno V (2016) Is high-intensity interval training more effective on improving cardiometabolic risk and aerobic capacity than other forms of exercise in overweight and obese youth? A meta-analysis. Obes Rev 17 (6):10. [CrossRef]
- Valeria C, Daniela L, Erwan C, Annalisa De S, Paola B, Sebastiano A, Marisa A, Matteo V (2013) Improved metabolic and cardiorespiratory fitness during a recreational training program in obese children. Journal of Pediatric Endocrinology and Metabolism 26 (3-4):271-276. [CrossRef]
- Rajjo T, Mohammed K, Alsawas M, Ahmed AT, Farah W, Asi N, Almasri J, Prokop LJ, Murad MH (2017) Treatment of Pediatric Obesity: An Umbrella Systematic Review. The Journal of Clinical Endocrinology & Metabolism 102 (3):763-775. [CrossRef]
- Brown T, Moore Th Fau - Hooper L, Hooper L Fau - Gao Y, Gao Y Fau - Zayegh A, Zayegh A Fau - Ijaz S, Ijaz S Fau - Elwenspoek M, Elwenspoek M Fau - Foxen SC, Foxen Sc Fau - Magee L, Magee L Fau - O’Malley C, O’Malley C Fau - Waters E, Waters E Fau - Summerbell CD, Summerbell CD (2019) Interventions for preventing obesity in children. Cochrane Database Syst Rev 7 (7). [CrossRef]
- Hills A, Andersen L, Byrne N (2011) Physical activity and obesity in children. British journal of sports medicine 45:866-870. [CrossRef]
- Maron BJ, Fananapazir L (1992) Sudden cardiac death in hypertrophic cardiomyopathy. Circulation 1 (0009-7322 (Print)):7. 0009.
- Westerterp KR (2018) Exercise, energy balance and body composition. European Journal of Clinical Nutrition 72 (9):1246-1250. [CrossRef]
- Ridgers N, Timperio A, Cerin E, Salmon J (2014) Compensation of Physical Activity and Sedentary Time in Primary School Children. Medicine and science in sports and exercise 46. [CrossRef]
- Ekelund U, Luan Ja, Sherar L, Esliger D, Griew P, Cooper A (2012) Moderate to Vigorous Physical Activity and Sedentary Time and Cardiometabolic Risk Factors in Children and Adolescents. JAMA : the journal of the American Medical Association 307:704-712. [CrossRef]
- Kidokoro T, Suzuki K, Naito H, Balasekaran G, Song JK, Park SY, Liou YM, Lu D, Poh BK, Kijboonchoo K, Hui SS-C (2019) Moderate-to-vigorous physical activity attenuates the detrimental effects of television viewing on the cardiorespiratory fitness in Asian adolescents: the Asia-fit study. BMC Public Health 19 (1):1737-1737. [CrossRef]
- Júdice PB, Silva AM, Berria J, Petroski EL, Ekelund U, Sardinha LB (2017) Sedentary patterns, physical activity and health-related physical fitness in youth: a cross-sectional study. Int J Behav Nutr Phys Act 14 (1):25-25. [CrossRef]
- Mäkikallio K, Shah J, Slorach C, Qin H, Kingdom J, Keating S, Kelly E, Manlhiot C, Redington A, Jaeggi E (2015) Fetal growth restriction and cardiovascular outcome in early human infancy: a prospective longitudinal study. Heart and vessels 31. [CrossRef]
- Ji F, Ning F, Duan H, Kaprio J, Zhang D, Zhang D, Wang S, Qiao Q, Sun J, Liang J, Pang Z, Silventoinen K (2014) Genetic and Environmental Influences on Cardiovascular Disease Risk Factors: A Study of Chinese Twin Children and Adolescents. Twin Research and Human Genetics 17 (2):72-79. [CrossRef]
- Bull CJ, Northstone K (2016) Childhood dietary patterns and cardiovascular risk factors in adolescence: results from the Avon Longitudinal Study of Parents and Children (ALSPAC) cohort. Public Health Nutrition 19 (18):3369-3377. [CrossRef]
- Sönmez H, Canpolat N, Ağbaş A, Mehmet T, Ekmekçi Ö, Alikaşifoğlu M, Sever L, Caliskan S (2019) The Relationship between the Waist Circumference and Increased Carotid Intima Thickness in Obese Children. Childhood Obesity 15. [CrossRef]
- Bassali R, Waller J, Gower B, Allison J, Davis C (2009) Utility of waist circumference percentile for risk evaluation in obese children. International journal of pediatric obesity : IJPO : an official journal of the International Association for the Study of Obesity 5:97-101. [CrossRef]
- Sönmez H, Canpolat N, Ağbaş A, Mehmet T, Ekmekçi Ö, Alikaşifoğlu M, Sever L, Caliskan S (2019). The Relationship between the Waist Circumference and Increased Carotid Intima Thickness in Obese Children. Childhood Obesity 15.
- Zampetti S, Campagna G, Leto G, Lucantoni F, D’Onofrio L, Marandola L, Moretti C, Chiesa C, Pacifico L, Buzzetti R (2018) Relation Between Wrist Circumference and Left Ventricular Structure in Overweight Children. The American Journal of Cardiology 121. [CrossRef]
- Zimmet P, Alberti G Fau - Kaufman F, Kaufman F Fau - Tajima N, Tajima N Fau - Silink M, Silink M Fau - Arslanian S, Arslanian S Fau - Wong G, Wong G Fau - Bennett P, Bennett P Fau - Shaw J, Shaw J Fau - Caprio S, Caprio S (2007) The metabolic syndrome in children and adolescents. Lancet 369 (9579):3. [CrossRef]
- Nehus E, Mitsnefes M (2019) Childhood Obesity and the Metabolic Syndrome. Pediatric Clinics of North America 66 (1):31-43. [CrossRef]
Figure 1.
Network perspective of the relationship between moderate to vigorous physical activity, sedentary behaviour, and cardiovascular risk factors. Caption: 1 = Moderate to vigorous physical activity; 2 = Sedentary Behaviour; 3 = Age; 4 = Sex; 5 = Body mass index; 6 = waist circumference; 7 = Mean blood pressure; 8 = High density cholesterol; 9 = Low density cholesterol; 10 = Triglycerides; 11 = Glucose; 12 = Fat; 13 = Cardiorespiratory fitness; 14 = Left ventricular mass; 15 = Sokolow-Lyon.
Figure 1.
Network perspective of the relationship between moderate to vigorous physical activity, sedentary behaviour, and cardiovascular risk factors. Caption: 1 = Moderate to vigorous physical activity; 2 = Sedentary Behaviour; 3 = Age; 4 = Sex; 5 = Body mass index; 6 = waist circumference; 7 = Mean blood pressure; 8 = High density cholesterol; 9 = Low density cholesterol; 10 = Triglycerides; 11 = Glucose; 12 = Fat; 13 = Cardiorespiratory fitness; 14 = Left ventricular mass; 15 = Sokolow-Lyon.
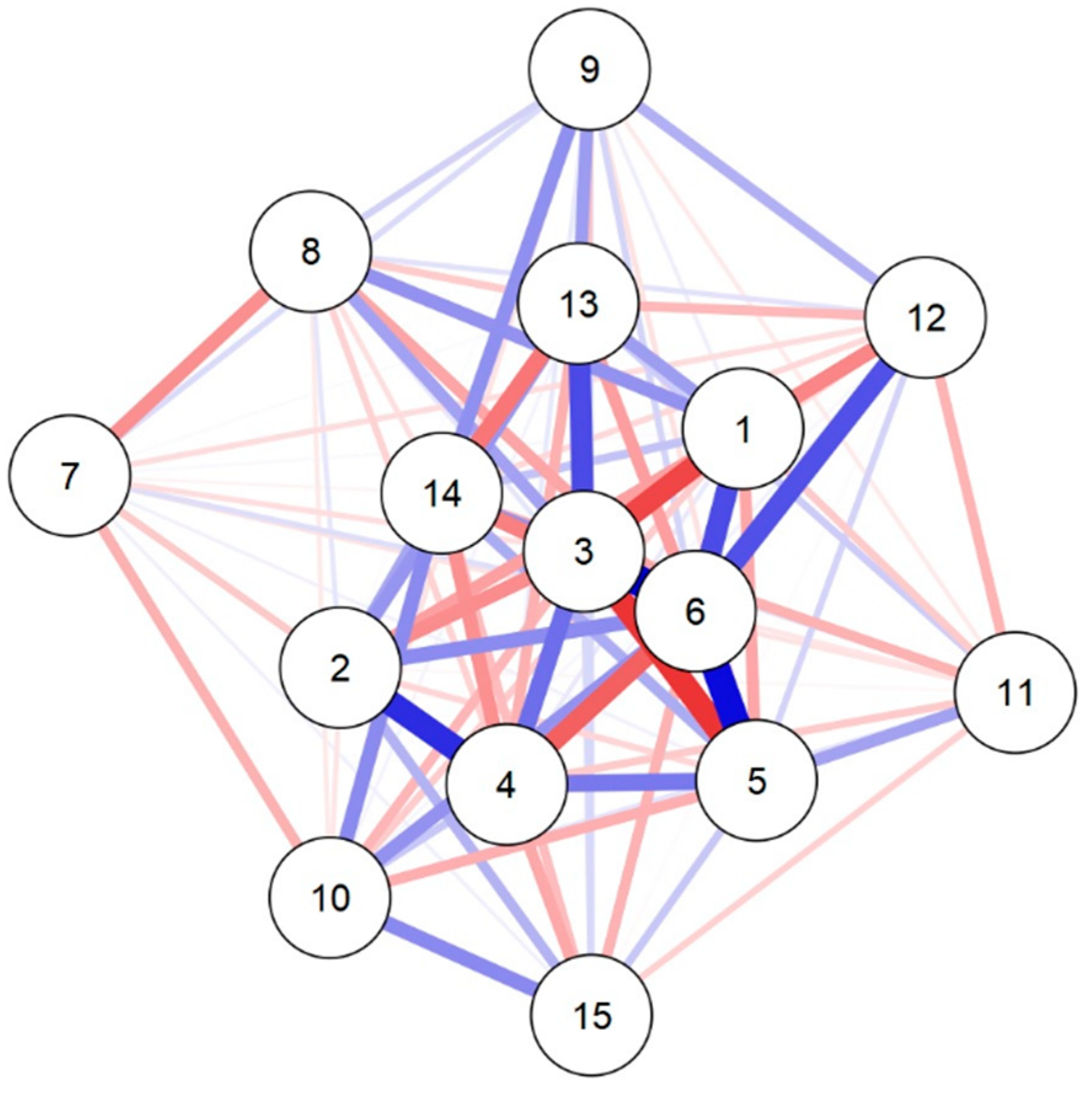

Table 1.
Sample Characterization. Petrolina-PE,2016.
| Variables | Boys (n = 18) (Mean ± SD) |
Girls (n = 23) (Mean ± SD) |
p | d’ Cohen |
|---|---|---|---|---|
| Age | 7.7 ± 0.9 | 8.0 ± 1.0 | 0.277 | -0.347 |
| MVPA (min/day) | 34.6 ± 16.4 | 24.6 ± 13.5 | 0.037 | 0.679 |
| SB (min/day) | 330.4 ± 44.6 | 389.0 ± 68.6 | 0.003 | -0.987 |
| BMI (kg/m²) | 21.7 ± 3.2 | 22.1 ± 2.6 | 0.621 | -0.157 |
| WC (cm) | 68.8 ± 3.2 | 22.1 ± 2.6 | 0.822 | 0.071 |
| Fat (%) | 34.2 ± 9.2 | 34.7 ± 6.5 | 0.841 | -0.063 |
| MBP (mmHg) | 84.5 ± 6.9 | 80.3 ± 8.2 | 0.091 | 0.546 |
| TC (mg/dl) | 159.2 ± 35.3 | 156.6 ± 35.4 | 0.800 | 0.080 |
| HDL-C (mg/dl) | 37.4 ± 3.8 | 37.3 ± 7.8 | 0.962 | 0.015 |
| LDL-C (mg/dl) | 101.9 ± 29.8 | 97.8 ± 25.7 | 0.635 | 0.151 |
| TG (mg/dl) | 96.3 ± 45.1 | 100.9 ± 52.3 | 0.769 | -0.093 |
| Glucose (mg/dl) | 82.4 ± 5.8 | 82.7 ± 6.2 | 0.891 | -0.044 |
| CRF (meters) | 748.6 ± 73.7 | 752.0 ± 95.3 | 0.901 | -0.039 |
| LVM (g) | 49.9 ± 9.4 | 48.2 ± 12.4 | 0.629 | 0.153 |
| Sokolow-Lyon | 33.4 ± 6.9 | 31.7 ± 5.6 | 0.384 | 0.277 |
MVPA = Moderate to vigorous physical activity; SB = Sedentary Behaviour; BMI = Body mass index; WC = waist circumference; MBP = Mean blood pressure; TC = Total cholesterol; HDL-C = High density cholesterol; LDL-C = Low density cholesterol; TG = Triglycerides; CRF = Cardiorespiratory fitness; LVM = Left ventricular mass.
Table 2.
Weight matrix of variables MVPA, SB, age, sex, and cardiovascular risk factors. Petrolina-PE, 2016.
Table 2.
Weight matrix of variables MVPA, SB, age, sex, and cardiovascular risk factors. Petrolina-PE, 2016.
| Variables | MVPA | SB | Age | Sex | BMI | WC | MBP | HDL | LDL | TGL | Glucose | Fat | CRF | LVM | Sokolov |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| MVPA | 0.000 | ||||||||||||||
| SB | -0.267 | 0.000 | |||||||||||||
| Age | -0.513 | -0.319 | 0.000 | ||||||||||||
| Sex | 0.062 | 0.581 | 0.408 | 0.000 | |||||||||||
| BMI | -0.251 | -0.116 | -0.561 | 0.378 | 0.000 | ||||||||||
| WC | 0.499 | 0.326 | 0.716 | -0.444 | 0.664 | 0.000 | |||||||||
| MBP | 0.016 | -0.097 | -0.094 | -0.151 | 0.037 | 0.092 | 0.000 | ||||||||
| HDL-C | 0.307 | 0.069 | 0.263 | -0.127 | 0.072 | -0.253 | -0.315 | 0.000 | |||||||
| LDL-C | 0.047 | 0.008 | -0.174 | 0.065 | -0.086 | 0.122 | 0.105 | 0.129 | 0.000 | ||||||
| TG | -0.144 | -0.073 | -0.204 | 0.156 | -0.228 | 0.305 | -0.219 | -0.062 | -0.083 | 0.000 | |||||
| Glucose | -0.148 | -0.020 | 0.084 | -0.150 | 0.265 | -0.072 | -0.080 | 0.004 | -0.060 | 0.079 | 0.000 | ||||
| Fat | -0.341 | -0.092 | -0.115 | 0.035 | 0.123 | 0.485 | -0.099 | 0.084 | 0.224 | 0.021 | -0.212 | 0.000 | |||
| CRF | 0.276 | 0.296 | 0.503 | -0.223 | 0.164 | -0.271 | 0.011 | -0.146 | 0.277 | 0.031 | 0.144 | -0.199 | 0.000 | ||
| LVM | 0.171 | 0.250 | 0.318 | -0.311 | 0.237 | -0.355 | -0.027 | -0.089 | 0.314 | 0.329 | -0.217 | -0.108 | -0.386 | 0.000 | |
| Sokolov | 0.203 | 0.215 | 0.110 | -0.248 | 0.158 | -0.216 | 0.038 | -0.093 | 0.112 | 0.331 | -0.128 | -0.012 | -0.075 | -0.187 | 0.000 |
MVPA = Moderate to vigorous physical activity; SB = Sedentary Behaviour; BMI = Body mass index; WC = waist circumference; MBP = Mean blood pressure; HDL = High density cholesterol; LDL = Low density cholesterol; TG = Triglycerides; CRF = Cardiorespiratory fitness; LVM = Left ventricular mass.
Table 3.
Centrality measures of the network analysis MVPA, SB, age, sex, and cardiovascular risk factors. Petrolina-PE,2016.
Table 3.
Centrality measures of the network analysis MVPA, SB, age, sex, and cardiovascular risk factors. Petrolina-PE,2016.
| Variables | Network | ||
|---|---|---|---|
| Betweenness | Closeness | Strength | |
| MVPA | -0.502 | 0.585 | 0.480 |
| SB | -0.662 | -0.029 | -0.044 |
| Age | 0.459 | 1.506 | 1.628 |
| Sex | -0.182 | 0.596 | 0.576 |
| BMI | 0.139 | 0.504 | 0.574 |
| WC | 3.182 | 1.809 | 2.069 |
| Fat | -0.662 | 0.074 | -0.627 |
| MBP | -0.662 | -1.602 | -1.403 |
| HDL-C | 0.299 | -0.831 | -0.764 |
| LDL-C | -0.662 | -1.062 | -0.976 |
| TG | -0.182 | -0.211 | -0.510 |
| Glucose | -0.662 | -1.307 | -1.120 |
| CRF | -0.021 | 0.159 | 0.233 |
| LVM | 0.779 | 0.717 | 0.536 |
| Sokolow-Lyon | -0.662 | -0.908 | -0.651 |
MVPA = Moderate to vigorous physical activity; SB = Sedentary Behaviour; BMI = Body mass index; WC = waist circumference; SBP = Systolic blood pressure; DBP = Dyastolic blood pressure; TC = Total cholesterol; HDL = High density cholesterol; LDL = Low density cholesterol; TG = Triglycerides; CRF = Cardiorespiratory fitness; LVM = Left ventricular mass.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



