Submitted:
22 February 2023
Posted:
24 February 2023
You are already at the latest version
Abstract
Gout is not only associated with obstructive sleep apnea (OSA), but the intermittent episodes of hypoxia that occur with OSA may also have a role in causing gout. Epidemiological studies have documented a higher incidence and prevalence of gout in individuals diagnosed with OSA than in individuals never diagnosed with OSA. The pathophysiology of OSA’s chronic episodes of hypoxia leading to hyperuricemia and gout involves boththe overproduction and underexcretion of uric acid. Treating OSA may be an additional way to control gout and its life-threatening comorbidities. Clinicians are urged to evaluate their patients with hyperuricemia/gout for OSA as it may lead to alternative ways to control gout with superior outcomes that simply pharmacologic treatment alone.
Keywords:
sleep apnea
; hypoxia
; gout
; hyperuricemia
; urate
; metabolic comorbidities
1. Introduction
Gout, while once thought to be a self-limited arthritis, is now recognized as being an important systemic disease that warrants aggressive treatment1. There are classically four commonly recognized causes of gout that are discussed in the literature, namely, genetics2, diet (especially from fructose-containing sugars, animal purine foods, or alcohol)3-5, impaired kidney function6, and insulin resistance7. While hyperuricemia commonly precedes and predicts insulin resistance8, there is evidence that chronically elevated insulin may stimulate the reabsorption of uric acid (along with sodium) in the proximal tubule. Here we would like to emphasize that there is a fifth common cause, which is obstructive sleep apnea (OSA). In fact, it is common enough that the presence of OSA should encourage the physician to measure uric acid and inquire about gout, and also that the physician who diagnoses gout should consider evaluating the individual for OSA.
2. Epidemiological Association of OSA with Gout
Epidemiological studies have documented a strong association of OSA with gout (Table 1)9-14. The relative risk for gout among subjects with OSA is exceeds 2-fold, on average. Not only are both hyperuricemia and gout associated with OSA, but those subjects with higher uric acid levels tend to have worse hypoxia and poorer cardiovascular outcomes14.
The frequency of OSA in subjects with gout may be higher than assumed from epidemiological data base studies. In one clinical study conducted by rheumatologists, 89% of 54 gout patients were diagnosed by polysomnography with OSA15, a percentage which is about as high as the sensitivity for OSA of one night of polysomnography16
3. How is OSA Connected with Gout?: Understanding the Pathophysiology
Sleep apnea is not simply associated with hyperuricemia and gout, it also has a causal role17. Sleep apnea is classically associated with intermittent hypoxic spells that can activate hypoxia-mediated pathways. One of the most important hypoxic pathways is driven by activation of the nuclear transcription factor, HIF-1α, and levels of HIF-1α are elevated in the plasma of patients with OSA18. In turn, HIF-1α is known to activate a survival pathway known as the polyol-fructokinase-xanthine oxidase pathway that can generate uric acid19-21. This pathway tends to protect against hypoxia by reducing mitochondrial function while stimulating glycolysis, thereby reducing oxygen needs22,23. However, chronic activation can lead to worsening feature of metabolic syndrome and chronic inflammation.
Moreover, in chondrocytes hypoxia induces GLUT1 and HIF-1alpha expression and a glycolytic shift that favors the Warburg effect, which causes the accumulation of lactate and the increased acidity of the extracellular microenvironment 24. The acidification of the microenvironment causes the release of calcium ions which has been shown to nucleate the crystallization of monosodium urate (MSU). This, along with the release of IL-1beta, attracts resident macrophages that are activated by the MSU crystals leading downstream to a gout flare 25,26. A similar metabolic mechanism has been shown to exist in MSU stimulated macrophages 26.
Other mechanisms are also involved in the rise of uric acid that occurs with hypoxia. Figure 1 depicts those hyperuricemic mechanisms, with overproduction shown in the leftmost pathway of the figure, and underexcretion shown in the other two pathways. The hypoxic episodes lead to nucleotide turnover from ATP degradation culminating in irreversible cellular generation of excess uric acid17. The hypoxic episodes also are associated with both a respiratory acidosis from hypoventilation27 as well as a lactic acidosis from tissue ischemia28, which both act to reduce serum pH and that might increase the risk for urate crystallization in the synovial joint and elsewhere. In addition, the lactate can act on the renal tubule to increase urate reabsorption29. The hypercapnia can also induce an increase in renal vascular resistance30 that might also reduce urate excretion. The net effect is both an increase in urate production with a reduction in excretion, resulting in hyperuricemia with MSU precipitation, and a gout flare in an individual genetically predisposed to gout.
It is of interest that most gout attacks occur during the night31. While this is often thought to be due to dietary indiscretion, as a high purine load can increase serum uric acid three to four hours after ingestion32, it may also relate to the presence of sleep apnea and the acute effects of hypoxia on urate metabolism.
4. Does Treating OSA Provide Another Means for Controlling Gout and Its Comorbidities?
Gout has been reported to have so many of the same life-threatening metabolic syndrome comorbidities already known to be consequences of long-term untreated OSA (eg., cardiovascular diseases, diabetes, kidney disease, hypertension)33,34, some of which are reversible just by resolving the OSA35.
Following effective OSA treatment, the OSA-induced gout flares cease because OSA’s episodic effects no longer occur, and the reduced glomerular filtration rate may improve and potentially reverse within three months of effective treatment for OSA36,37. The slow dissolution of MSU stores after OSA has been resolved is likely to be assisted by ULT.
OSA been shown to elevate the risk for cardiovascular disease38. The rate of cardiovascular events has been shown to be the same in those with OSA resolved by controlled positive airway pressure (CPAP) vs. healthy individuals39. CPAP has been shown to reduce the recurrence of atrial fibrillation40, and to restore cardiac mechanical function41. CPAP also has been shown to ameliorate the progression of chronic kidney disease, and to reverse it in some cases36,37,42.
5. Summary
In summary, OSA is not only common in gout, but likely is a causal risk factor, similar to the role of genetics, diet, and kidney function. Subjects presenting with gout should be questioned for signs and symptoms of OSA with a low threshold for testing. Likewise, subjects presenting with OSA should be screened for hyperuricemia and gout and treated appropriately. The treatment of OSA appears to be beneficial for preventing gout flares, and may also have some effect on reducing uric acid levels. Treating OSA provides an additional approach for controlling hyperuricemia besides diet and medications.
Author Contributions
Conceptualization, all authors; writing—original draft preparation, RJ, BA, PD; writing—review and editing- RJ, BA. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
Not applicable
Conflicts of Interest
The authors declare no conflict of interest.
References
- Dalbeth N, Choi HK, Terkeltaub R. Review: Gout: A Roadmap to Approaches for Improving Global Outcomes. Arthritis Rheumatol 2017;69(1):22-34. [CrossRef]
- Major TJ, Dalbeth N, Stahl EA, Merriman TR. An update on the genetics of hyperuricaemia and gout. Nat Rev Rheumatol 2018;14(6):341-353. [CrossRef]
- Choi HK. Diet, alcohol, and gout: how do we advise patients given recent developments? Curr Rheumatol Rep 2005;7(3):220-6. (In eng) (http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=15918999). [CrossRef]
- Choi HK, Atkinson K, Karlson EW, Willett W, Curhan G. Purine-rich foods, dairy and protein intake, and the risk of gout in men. N Engl J Med 2004;350(11):1093-103. (In eng) (http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=15014182). [CrossRef]
- Choi HK, Curhan G. Soft drinks, fructose consumption, and the risk of gout in men: prospective cohort study. BMJ 2008;336(7639):309-12. (In eng) (http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=18244959). [CrossRef]
- Juraschek SP, Kovell LC, Miller ER, 3rd, Gelber AC. Association of kidney disease with prevalent gout in the United States in 1988-1994 and 2007-2010. Semin Arthritis Rheum 2013 (In Eng). DOI: S0049-0172(12)00266-1 [pii]. [CrossRef]
- Quinones GA, Natali A, Baldi S, et al. Effect of insulin on uric acid excretion in humans. Am J Physiol 1995;268(1 Pt 1):E1-5. (http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=7840165). [CrossRef]
- Johnson RJ, Nakagawa T, Sanchez-Lozada LG, et al. Sugar, uric acid, and the etiology of diabetes and obesity. Diabetes 2013;62(10):3307-15. (In eng). DOI: 62/10/3307 [pii]. [CrossRef]
- Blagojevic-Bucknall M, Mallen C, Muller S, et al. The Risk of Gout Among Patients With Sleep Apnea: A Matched Cohort Study. Arthritis Rheumatol 2019;71(1):154-160. [CrossRef]
- Roddy E, Muller S, Hayward R, Mallen CD. The association of gout with sleep disorders: a cross-sectional study in primary care. BMC Musculoskelet Disord 2013;14:119. [CrossRef]
- Singh JA. Self-reported sleep quality and sleep disorders in people with physician-diagnosed gout: an Internet cross-sectional survey. Arthritis Res Ther 2019;21(1):36. [CrossRef]
- Singh JA, Cleveland JD. Gout and the Risk of Incident Obstructive Sleep Apnea in Adults 65 Years or Older: An Observational Study. J Clin Sleep Med 2018;14(9):1521-1527. [CrossRef]
- Zhang Y, Peloquin CE, Dubreuil M, et al. Sleep Apnea and the Risk of Incident Gout: A Population-Based, Body Mass Index-Matched Cohort Study. Arthritis Rheumatol 2015;67(12):3298-302. [CrossRef]
- Kanbay A, Inonu H, Solak Y, et al. Uric acid as a potential mediator of cardiovascular morbidity in obstructive sleep apnea syndrome. Eur J Intern Med 2014;25(5):471-6. [CrossRef]
- Cantalejo Moreira M, Veiga Cabello RM, Garcia Diaz V, Racionero Casero MA, Zapatero Gaviria A. Gout, hyperuricaemia, sleep apnoea-hypopnoea syndrome and vascular risk. Rheumatology (Oxford) 2013;52(9):1619-22. [CrossRef]
- Edinger JD, Ulmer CS, Means MK. Sensitivity and specificity of polysomnographic criteria for defining insomnia. J Clin Sleep Med 2013;9(5):481-91. [CrossRef]
- Hasday JD, Grum CM. Nocturnal increase of urinary uric acid:creatinine ratio. A biochemical correlate of sleep-associated hypoxemia. Am Rev Respir Dis 1987;135(3):534-8. [CrossRef]
- Gabryelska A, Szmyd B, Szemraj J, Stawski R, Sochal M, Bialasiewicz P. Patients with obstructive sleep apnea present with chronic upregulation of serum HIF-1alpha protein. J Clin Sleep Med 2020;16(10):1761-1768. [CrossRef]
- Kanbay M, Altintas A, Yavuz F, et al. Responses to Hypoxia: How Fructose Metabolism and Hypoxia-Inducible Factor-1a Pathways Converge in Health and Disease. Curr Nutr Rep 2023. [CrossRef]
- Mirtschink P, Krek W. Hypoxia-driven glycolytic and fructolytic metabolic programs: Pivotal to hypertrophic heart disease. Biochim Biophys Acta 2016;1863(7 Pt B):1822-8. [CrossRef]
- Mirtschink P, Krishnan J, Grimm F, et al. HIF-driven SF3B1 induces KHK-C to enforce fructolysis and heart disease. Nature 2015;522(7557):444-9. [CrossRef]
- Nakagawa T, Lanaspa MA, Millan IS, et al. Fructose contributes to the Warburg effect for cancer growth. Cancer Metab 2020;8:16. [CrossRef]
- Nakagawa T, Sanchez-Lozada LG, Andres-Hernando A, et al. Endogenous Fructose Metabolism Could Explain the Warburg Effect and the Protection of SGLT2 Inhibitors in Chronic Kidney Disease. Front Immunol 2021;12:694457. [CrossRef]
- Zheng L, Zhang Z, Sheng P, Mobasheri A. The role of metabolism in chondrocyte dysfunction and progression of osteoarthritis. Ageing Research Reviews 2020; 66: 101249. [CrossRef]
- Wilcox WR, Khalaf AA. Nucleation of monosodium urate crystals. Ann. Rheum Dis. 1975; 34: 332-339. [CrossRef]
- Renaudin F, Orliaquet L, Castelli F, et al. Gout and pseudo-gout-related crystals promote GLUT1-mediated glycolysis that governs NLRP3 and interleukin-1beta activation on macrophages. Ann. Rheum Dis 2020; 0: 1-9. [CrossRef]
- Shivaram U, Cash ME, Beal A. Nasal continuous positive airway pressure in decompensated hypercapnic respiratory failure as a complication of sleep apnea. Chest 1993;104(3):770-4. [CrossRef]
- Lin T, Huang JF, Lin QC, et al. The effect of CPAP treatment on venous lactate and arterial blood gas among obstructive sleep apnea syndrome patients. Sleep Breath 2017;21(2):303-309. [CrossRef]
- Nakanishi T, Ohya K, Shimada S, Anzai N, Tamai I. Functional cooperation of URAT1 (SLC22A12) and URATv1 (SLC2A9) in renal reabsorption of urate. Nephrol Dial Transplant 2013;28(3):603-11. [CrossRef]
- Chapman CL, Schlader ZJ, Reed EL, Worley ML, Johnson BD. Renal and segmental artery hemodynamic response to acute, mild hypercapnia. Am J Physiol Regul Integr Comp Physiol 2020;318(4):R822-R827. [CrossRef]
- Choi HK, Niu J, Neogi T, et al. Nocturnal risk of gout attacks. Arthritis Rheumatol 2015;67(2):555-62. [CrossRef]
- Clifford AJ, Riumallo JA, Youn VR, Scrimshaw NS. Effect of Oral Purines on Serum and Urinary Uric Acid of Normal, Hyperuricemic and Gouty Humans. J Nutr 1976;106:428-450. [CrossRef]
- Huang CF, Liu JC, Huang HC, et al. Longitudinal transition trajectory of gouty arthritis and its comorbidities: a population-based study. Rheumatol Int. 2017 Feb; 37(2):313-22. [CrossRef]
- Chiang CL, Chen YT, Wang KL, et al. Comorbidities and risk of mortality in patients with sleep apnea. Ann Med. 2017 Aug; 49(5): 377-83. [CrossRef]
- Abrams B. Update on reversibility of obstructive sleep apnea consequences. Med Res Arch. 2020 Apr 8(4). [CrossRef]
- Kinebuchi S, Kazama JJ, Satoh M, et al. Short-term use of continuous positive airway pressure ameliorates glomerular hyperfiltration in patients with obstructive sleep apneoa syndrome. Clin Sci (Lond). 2002 Sep; 107(3):317-22. [CrossRef]
- Koga S, Ikeda S, Yasunaga T, et al. Effects of nasal continuous positive airway pressure on the glomerular filtration rate in patients with obstructive sleep apnea syndrome. Intern Med. 2013 Mar; 52(3):345-9. [CrossRef]
- Yoshihisa A, Takeishi Y. Sleep disordered breathing and cardiovascular disease. J Atheroscler Thromb. 2019 Apr; 26(4): 315-27. [CrossRef]
- Mandal S, Kent BD. Obstructive sleep apnea and coronary artery disease. J Thorac Dis. 2018 Dec; 10(Suppl 34):S4212-20. [CrossRef]
- Geovanini GR, Lorenzi-Filko G. Cardiac rhythm disorders in obstructive sleep apnea. J Thorac Dis. 2018 Dec; 10(Suppl 34):S4221-30. [CrossRef]
- Kim D, Shim CY, Cho YJ, et al. Continuous positive airway pressure restores cardiac mechanical function in patients with severe obstructive sleep apnea: A randomized sham-controlled study. J An Soc Endocardiogr. 2019 Jul; 32(7):826-35. [CrossRef]
- Li X, Liu C, Zhang H, et al. Effect of 12-month nasal continuous positive airway pressure therapy for obstructive sleep apnea on progression of chronic kidney disease. Medicine (Baltimore). 2019 Feb; 98(8):e14545. [CrossRef]
Figure 1.
Pathophysiology of OSA Leading to a GOUT FLARE.
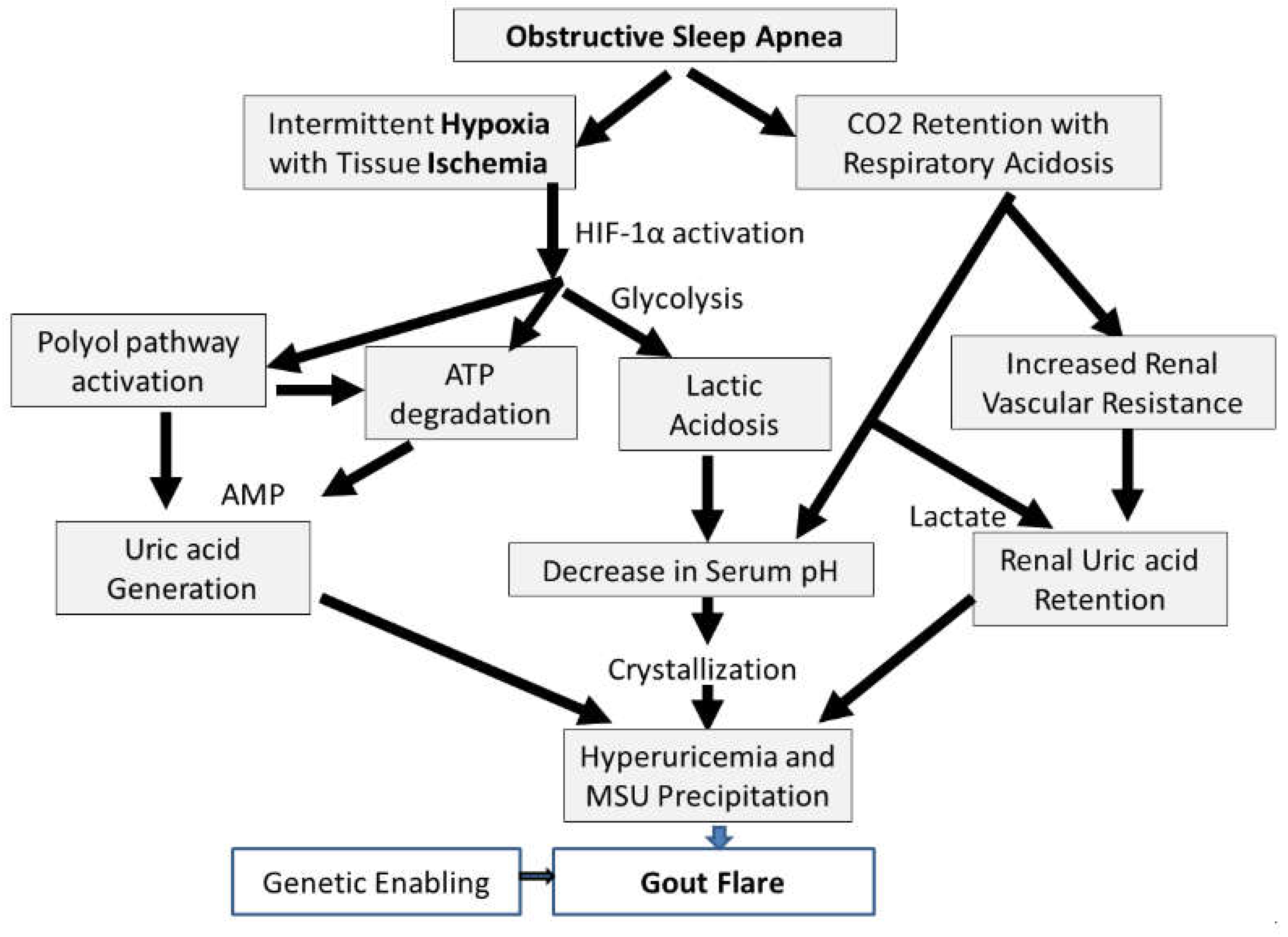

Table 1.
Synopses of Epidemological Studies Connecting Gout with OSA.
| Ref # |
Description of Study | Number of Participants | Results | Risk Ratio |
|---|---|---|---|---|
| 9 | Data from UK Clinical Practice Research Datalink. Comparison of gout incidence rate in cohort diagnosed with OSA vs. cohort (matched by age, sex, practice) never diagnosed with OSA. 5.8 yrs. median follow-up. |
15,878 diagnosed with OSA. 63,296 never diagnosed with OSA* |
OSA: 4.9% with gout. Incidence rate 7.83/KPyr No OSA: 2.6% with gout. Incidence rate 4.03/KPyr |
1.9 |
| 10 | Data from UK general practice data base. Comparison of gout prevalence in those diagnosed with OSA vs. those never diagnosed with OSA. |
1,689 diagnosed with OSA. 6,756 never diagnosed with OSA* |
OSA: 0.7% No OSA: 0.3% |
2.3 |
| 11 | Internet questioning about sleep disorders of people with physician-diagnosed gout who visited a gout education website. |
454 | 320 with gout. 77 with diagnosed OSA. |
N/A |
| 12 | Data from 5% US Medicare beneficiary sample 2006-2012. Selected entries with new diagnosis of OSA. |
1.74 M, follow-up of 10,448,472 person-years* |
Incidence rates with OSA: 14.3/KPyr No OSA: 3.9/KPyr |
3.7 |
| 13 | Data from UK Health Improvement Network.Comparison of gout incidence rate with first SA diagnosis vs. cohort (matched by age, sex, BMI) never diagnosed with SA. |
9,865 with first SA diagnosis. 43,598 never diagnosed with SA* |
Incidence rates with SA: 8.4/KPyr No SA: 4.8/KPyr |
1.75 |
| 14 | All participants tested for OSA, and questioned about history of cardiovascular disease. |
72 controls (AHI<5) 47 mild (5<AHI<15) 75 moderate OSA (15<AHI<30) 192 severe (AHI>30) |
Serum uric acid data show monotonic increase with AHI in those who had a cardiovascular event. |
N/A |
* Not all subjects were tested for OSA so the numbers are likely to underrepresent the true number of subjects with OSA. Key: AHI = apnea-hypopnea index; KPyr = kiloperson-years; N/A = not applicable; OSA = obstructive sleep apnea; SA = sleep apnea.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



