
Submitted:
25 February 2023
Posted:
27 February 2023
You are already at the latest version
Abstract
Background: Chronic kidney disease (CKD) is a common complication of non-kidney solid organ transplant (NKSOT). Identifying predisposing factors is crucial for an early approach and correct referral to nephrology. Methods: This is a single-center retrospective observational study of a cohort of CKD patients under follow-up in Nephrology Department between 2010 to 2020. Statistical analysis was performed between all the risk factors and four dependent variables: end-stage renal disease (ESKD), increased serum creatinine ≥50%, renal replacement therapy (RRT), and death in pre-transplant, peri-transplant and post-transplant period. Results: 74 patients were studied (7 heart transplant, 34 liver transplants, and 33 lung transplant). Patients who were not followed-up by nephrology in the pre-transplant (p<0.027), peri-transplant (p<0.046), and the longest time until outpatient clinic follow-up (HR 1,032) were associated with a higher risk of creatinine increase ≥50%. Receiving a lung transplant conferred higher risk than liver or hear transplant for developing a creatinine increase ≥50% and ESKD. Peri-transplant mechanical ventilation, peri-transplant and post-transplant anticalcineurin overdose, nephrotoxic and the number of hospital admissions were significantly associated to present a creatinine increase ≥50% and develop ESKD. Conclusion: An early follow-up by the nephrology department was associated with a decrease in the worsening of renal function.
Keywords:
chronic kidney disease
; solid organ transplant
; nephrology
1. Introduction
Chronic kidney disease (CKD) is a common complication of non-kidney solid organ transplant (NKSOT), causing increased morbidity and mortality in this group of patients. The increase in overall survival due to advancements in surgical techniques and immunosuppression management has promoted growth in the absolute number of patients who develop these complications [1,2].
A large study published in 2003 by Ojo AO et al. [3], with a population cohort of 69,321 patients who received NKSOT between 1990 and 2000, presented exciting results on the predisposing factors for CKD of each type of NKSOT. In this study, 11,426 patients (16.5%) developed End Stage Kidney Disease (ESKD) during a median follow-up of 36 months. The cumulative incidence ranged varied from 6.9% for those with heart-lung transplants to 21.3% for those with intestine transplants. Currently, the absolute number of transplants performed has increased worldwide [4,5,6]. Together with improved surgical techniques and more effective immunosuppressive regimens [7,8,9], this means that new revisions on the complications and risk factors, specifically on ESKD, should be carried out.
Generally, there are pre-transplant, peri-transplant, and post-transplant predisposing factors in the middle and long-term periods. However, specific characteristics in each type of transplant give different risks to developing CKD. In a series of renal biopsies from patients with NKSOT, variations in the histological pattern were observed, demonstrating differences between the types of organ transplantation. For example, arteriolar hyalinosis was more common in heart and lung transplant recipients than in liver transplant recipients, while primary glomerular disease being more common in the latter [10].
The knowledge of all the general and specific predisposing factors of each type of transplant may allow an early approach and minimize the progressive worsening of renal function and its short- and long-term complications. CKD is currently the eighth leading cause of death in developed countries, such as Spain. However, its incidence continues to grow, and it is estimated that it will be the second leading cause of death in Spain by 2100, after Alzheimer's disease [11]. This incidence increases when there are risk factors to develop it, as it is the case of patients with NKSOT. Thus, to identify these risk factors and address them on an early stage seem to be crucial; we believe that the Nephrologist plays an important role on these interventions. Therefore, this study aimed to analyze the nephrologist’s contribution to managing patients with NKSOT.
2. Materials and Methods
This is a single-center retrospective observational study on a cohort of CKD patients under follow-up in the department of nephrology at La Fe University and Politècnic Hospital in Valencia (Spain) from January 2010 to December 2020.
This study was performed in accordance with the ethical principles of the Declaration of Helsinki as revised in 2013. This study belonged to the project " Enfermedad renal crónica en trasplante de órgano sólido no renal. Análisis de la incidencia, factores de riesgo y pronóstico global de los diferentes tipos de trasplante de órgano sólido no renal", approved by the Hospital Universitari i Politècnic La Fe Clinical Research Ethics Committee, with the reference number 2021-302-1.
Study Population
The cohort of patients was extracted from our hospital's nephrology outpatient clinic and the End Stage Renal Disease Unit records, with a total of 212 patients: 44 heart transplant recipients, 93 liver transplant recipients, and 75 lung transplant recipients. Patients transplanted before 2010 (101 patients) or with combined renal transplantation (9 patients), and those with no follow-up in the outpatient clinic (28 patients) were excluded. A final population of 74 patients, 7 with a heart transplant, 34 with liver transplants, and 33 with a lung transplant, was obtained. [Figure 1]. Subjects older than 18 years at the onset of the follow-up in the outpatient clinic or End Stage Renal Disease Unit, NKSOT recipients between 2010 and 2020, and those with CKD-EPI estimated glomerular filtration rate (eGFR) <60 mL/min/1.73 m2 at baseline were included.
Patients who met the inclusion/exclusion criteria were evaluated retrospectively in three different periods [Figure 2]:
- Pre-transplant period: Clinical and analytical variables present before the solid organ transplant until day 0 of the transplant.
- Peri-transplant period: From the transplant to hospital discharge.
- Post-transplant period: From hospital discharge to one year of follow-up in nephrology consultations.
Data Collection
Baseline demographics, including age, gender, major comorbidities, etiology of kidney disease, etiology of disease associated with the transplantation, and clinical and analytical data in the different study periods [Figure 2] were collected from the medical records. Laboratory parameters included creatinine, eGFR, proteinuria, glucose, HbA1c, total cholesterol, low-density lipoprotein (LDL) cholesterol, high-density lipoprotein (HDL) cholesterol, and uric acid were determined in the hospital biochemistry laboratory by assays following Good Laboratory Practice standards. The KDIGO guidelines were adopted to manage CKD from the start of follow-up in nephrology.
Statistical Analysis
Statistical analysis was performed between all the risk factors and the four dependent variables: ESKD, increased serum creatinine ≥50%, renal replacement therapy, and death. These associations were evaluated with the Chi-square test or the Fisher's test for qualitative variables depending on the sample size, as well as with the Student's T test or the Mann-Whitney U test for quantitative variables depending on the result of the Kolmogorov Smirnov normality test. Subsequently, the statistically significant variables were evaluated with a multinomial regression and a Pearson or Spearman correlation based on the normality parameters for the quantitative variables. Kaplan Meier statistic was used for survival analysis. A two-sided p-value < 0.05 was considered statistically significant. Analyses were performed with IBM SPSS® Statistics version 26.
Data Availability
The datasets used and/or analyzed during the current study are available from the corresponding author upon request.
3. Results
Baseline Characteristics
The baseline characteristics are summarized in Table 1. The average age at the time of transplantation was 54.39 years. Fifty-four patients were males (73%). Recipients of heart, liver, and lung transplants accounted for 9.5 % (7 patients), 45.9 % (34 patients), and 44.6 % (33 patients), respectively.
In the pre-transplant period, 37.8% of patients were reported to have hypertension, 27.1% had diabetes mellitus, 25.7% had dyslipidemia, 14.9% had hyperuricemia, 23% had overweight, 18.9% had obesity, 55.4% were ex-smoker, 8.1% smokers, 6.8% had cardiorenal syndrome and 18.9% suffered from hepatorenal syndrome. The pre-transplantation eGFR was <60 ml per minute per 1.73 m2 (CKD) in 23% of the patients, and only 14.9% of the sample were followed-up by the nephrologist. The differences between transplants are summarized in Table 1.
In the peri-transplant period, 58.1% of the patients presented acute kidney injury (AKI), 5.4% required RRT, and only 18.9% were under nephrology follow-up n. During their hospital admission, 51.4% of the patients showed surgical complications, 87.8% had blood transfusion requirements, 54.1% required vasoactive drugs, 44.6% required mechanical ventilation, and 62.6% had related infections. Eighty-two percent (81.8%) of the patients received tacrolimus, versus 23% of those who received cyclosporine. Nighty-nine percent (98.6%) of the sample received mycophenolate, 8.2% of everolimus, and 90.5% of patients received corticosteroids. Changes were made in the initial immunosuppression in 14.9% of the patients, fundamentally motivated by renal failure. Twenty percent (20.3%) of the patients presented graft rejection. Fifty percent (50%) overdosed on calcineurin inhibitors for their reference levels, and 64.9% received nephrotoxic agents (4.16% received NSAIDs, 31.27% nephrotoxic antimicrobials, and 20.8% intravenous contrast) or a combination of them (43.77%).
In the post-transplant period, 23% of the patients developed hypertension, 23% had post-transplant diabetes mellitus (PTDM), and 17.5% had dyslipidemia. The mean number of hospital admissions was 6.8, with a maximum of 23 and a minimum of 1. Seventy-eight percent (78.4%) had infections in their evolution. Sixty-six percent (66.2%)of the patients presented an overdose of calcineurin inhibitors in more than three determinations, 68.9% required changes in immunosuppression due to its side effects, including worsening renal function, and 31.1% presented graft rejection. Seventy-seven percent (77%) of the sample received nephrotoxic drugs, 1.75% due to NSAIDs, 17.53% due to nephrotoxic antimicrobials, 19.35% due to contrast agents, and 1.75% due to other nephrotoxic drugs. However, most patients had combined these nephrotoxic drugs (59.62%). Finally, 9.5% of the sample presented secondary thrombotic microangiopathy (TMA).
The mean time from the transplant to the start of follow-up in the nephrology outpatient clinic was 33 months. The mean eGFR was 39.24 ml/min/1.73 m2. From the start of outpatient follow-up, 45.9% of the sample worsened renal function, versus 54.1% who improved or maintained it stable. Of the total sample, 45 patients (59.5%) increased their baseline creatinine value by 50%, 24 patients (32.43%) reached ACKD (GFR <30 ml/min/1.73 m2), 8 patients (10.8%) ended up in RRT and 21 patients (28.4%) died.
Increased Baseline Creatinine by 50%
In 45 patients increased their baseline creatinine levels by 50%. The mean age of these patients was 36.55 years, and most of them (75%) were men. The type of transplant was significantly associated with a 50% increase in baseline creatinine (p<0.05). Lung transplant recipients were at the highest risk. Compared with them, receiving a heart transplant had a 13.33-fold lower risk (HR 0.075 [95% CI] 0.01 to 0.5), and receiving a liver transplant was 20.83-fold lower (HR 0.048 [95% CI] 0.012 to 0.192).
Increased baseline creatinine serum levels by 50% were significantly associated with not having previous CKD (p <0.001), peri-transplant mechanical ventilation (p.<0.001), peri-transplant calcineurin inhibitor overdose (p<0.006), peri-transplant total nephrotoxic (p <0.029), peri-transplant antimicrobials nephrotoxic (p<0.012), peri-transplant intravenous contrast (p<0.009), absence of everolimus (p<0.001), not making changes in immunosuppression (p<0.027), post-transplant calcineurin inhibitor overdose (p<0.004), post-transplant intravenous contrast (p<0.022) and the number of hospital admissions (p<0.006). Concerning nephrotoxic factors in the peri-transplant period, after doing a multinomial regression adjusted for the rest of the factors, the use of nephrotoxic antimicrobials lost its statistical significance, preserving that of intravenous contrast, with an increased risk of 3.16 tines of increased 50% of serum creatinine. Statistically significant results are summarized in Table 2.
Analyzing these variables in each transplant, not taking everolimus, and not making changes in immunosuppression in the peri-transplant period and hypertension in the post-transplant period were statistically significant (p< 0.05) for lung transplant recipients.
Not having follow-up by nephrology in the pre-transplant (p<0.027) was associated with the increased baseline serum creatinine by 50%, showing a 4.97-fold increased risk (HR 4.97 [95% CI] 1.19 to 20.65). Not presenting nephrology follow-up in the peri-transplant period was significantly associated (p<0.046) with worsening of kidney function, showing a 3.34-fold increased risk (HR 3.34 [95% CI] 1.01 to 11.26). Time until outpatient nephrology consultation was significantly associated (p<0.002). A delay in follow-up by nephrology (each month), was associated with a 1.03-fold increased risk of increased serum creatinine.
End Stage Kidney Disease (ESKD)
Twenty-four patients reached ESKD. The mean age was 55.63 years, and most of them (66.7%) were men. The type of organ transplanted was significantly associated with reaching ESKD (p<0.05). Lung transplant recipients were at the highest risk. Compared with them, receiving a liver transplant presented a 6.94 times lower risk (HR 0.14 [95% CI] 0.045 to 0.463) and receiving a heart transplant, 7.19 times lower, although the latter was not significantly (HR 0.13 [95% CI] 0.015 to 1.28).
Peri-transplant mechanical ventilation (p<0.035), peri-transplant (p<0.015) and post-transplant (p<0.037) anticalcineurin overdose, peri-transplant (p<0.028) and post-transplant nephrotoxic antimicrobials (p<0.032), peri-transplant intravenous contrast (p <0.004) and the number of hospital admissions (p<0.02) were significantly associated with the worsening of renal function. In relation to nephrotoxic associated factors in the peri-transplant period, after doing a multinomial regression adjusted for the rest of the factors, the use of nephrotoxic antimicrobials lost its statistical significance; however, intravenous contrast showed an increased risk (3.62 times) to develop ESKD. Statistically significant results are summarized in Table 3.
Regarding those lung transplant recipients, dyslipidemia in the post-transplant period was significantly associated with the development of ESKD (p<0.05).
Mean ESKD-free survival was 93.29 months (95% CI 79.04-107.5), 121.5 months in heart transplantation recipients (95% CI of 86.70-155.297), 104 months in liver transplantation recipients (95% CI of 86.67-122.134) and 66.86 months in lung transplantation recipients (CI at 95% of 55.93 – 80.79) (Figure 3).
Renal Replacement Therapy (RRT)
From the study population, 8 patients required RRT. The mean age of these patients was 48 years, and most of them (75%) were men. It was significantly associated with the overdose of calcineurin inhibitors in the peri-transplant period (p<0.046), with an 8.4-fold increased risk (HR 8.4 [95% CI] 1.01 to 72.155). The median survival without reaching RRT was 124.93 months [95% CI] 112.42-137.43. This differs between transplants, 142 months in heart transplant, 118 months in liver transplant [95% CI] 107.94-129.67, and 104 months in lung transplant [95% CI] 92.85-115.88. [Figure 3]. However, these differences were not statistically significant when comparing all the groups.
Death
Twenty-one of patients died during the follow-up period. The mean age at transplant was 54.25 years, most of them (76.2%) men. The type of organ transplanted was not statistically associated with any of the exitus variables. It was significantly associated with active smoking in the pre-transplant (p<0.028) period and the number of hospital admissions in the post-transplant (p<0.006) period, with a 1.18-fold increased risk of death for each hospital admission (HR 1.118 [95% CI] 1.026 to 1.217).
4. Discussion
NKSOT has expanded in number and complexity in recent years. The increase in knowledge and experience allows medical transplant teams to improve patient care , decreasing comorbidities and mortality. Many of these comorbidities affect renal function, generating a progressive growth of patients who develop CKD among NKSOT recipients and placing the nephrology care as a critical specific managing these patients.
The strategies to minimize CKD must begin at the pre-transplant stages; treating cardiovascular and renal risk factors; followed by peri-transplantation monitoring and management, treating AKI, avoiding nephrotoxicity, and adjusting immunosuppression, and finally, in post-transplantation stages, treating CKD progression factors, as well as nephroprotection and adjustment of immunosuppressants [11].
Knowing which factors are most closely related to increasing susceptibility and progression of CKD and its complications allows for identifying patients at higher risk and may help to an early referral to the nephrology department.
The type of transplant performed differs in the risk of developing and CKD complications. In a study from Ojo Ao et al. [3], the incidence of ESKD at five years ranged from 10.9% in heart transplants to 15.8% in lung transplants and 18.1% in liver transplants. In our study, lung transplants had the highest risk of increasing their baseline creatinine by 50% and developing ESKD. It is noteworthy that despite heart transplant recipients being the next at risk of increasing their creatinine by 50%, however, this does not occur for the development of ESKD, in which liver transplants present a higher risk than those with heart transplants. These findings could be related to the baseline of renal function in liver transplant patients. Thus, the renal function was worse, with 26.6% of patients with stage G3b and 13.4% with stage G4; in the case of heart transplant recipients, all were in a G3a stage. The need for RRT also occurs earlier in lung transplant recipients, followed by liver transplant recipients, and finally those with heart transplant.
One of the remarkable findings in our study was the low rate of follow-up by the nephrology department despite CKD. In the literature, joint follow-up with nephrology has been associated with fewer cardiovascular events in liver transplant patients [12] and better management both before and after liver [13], heart, and lung [14] transplantation.
In our study, we found that for those patients in the pre-transplant period, 23% had documented CKD, but nephrology had previously followed-up only in 14.9%. This proportion varies and depends on the type of transplant. Therefore, all heart transplant recipients with CKD before transplantation were followed for nephrologists, against less than half of liver transplant recipients. In the cases of lung transplants, no patient had previous CKD, but two patients underwent nephrological follow-up for episodes of recovered AKI. Not having prior nephrology follow-up was associated with a 4.97 times higher risk of increasing baseline creatinine by 50%.
During the peri-transplant period, 58.1% of the patients presented AKI, but just 18.9% of them had nephrology followed-up. Once again, this proportion changes depending on the type of transplant, with nephrology monitoring half of the heart transplant recipients who had AKI, one-third of the liver transplant, and a quarter of those with lung transplant. Not having peri-transplant follow-up was associated with a 3.34-fold increased risk of increasing baseline creatinine by 50%.
The mean time from the transplantation to the beginning of nephrology outpatient evaluation and follow-up was 33.01 months, with a shorter time for those with liver transplant (28.24 months), followed by heart transplant recipients (33.71 months) and ending with lung transplant recipients (38.64 months). The delay in follow-up was significantly associated with a 50% increase in baseline creatinine, with an increased risk of developing a renal event of 1.03 times for each month without follow-up.
In the literature, several studies has been shown that pre-transplant kidney damage increased the risk of CKD [3,15,16]. In heart transplant recipients, kidney damage is related to cardiovascular risk factors and renal hypoperfusion in form of cardiorenal syndrome. In liver transplant recipients, it is also associated with renal hypoperfusion in the form of hepatorenal syndrome, acute tubular necrosis, and glomerulonephritis. Regarding lung transplant recipients, previous renal failure is less frequent, and its etiology is the same as for the general population.
In our study, we observe no significant cardiovascular risk factor associated with the development of ESKD. Nevertheless, active smoking was associated with mortality.
Similarly, investigations has reported that peri-transplant kidney damage is significantly related to developing CKD [3,17,18]. Thus, risk factors were similar in heart and liver transplantation, attributed to surgical complications and hypovolemia secondary to surgery (need for vasoactive drugs and transfusions), as well as the use of nephrotoxic medications and overdose of calcineurin inhibitors [17,18]. For those patients withlung transplantation, the use of nephrotoxic antimicrobial agents, such as aminoglycosides and amphotericin, the need for high-dose calcineurin inhibitors due to an increased risk of acute graft rejection, and the use of mechanical ventilation are emphasized [19,20].
Analyzing our results from this period, the requirement for mechanical ventilation was associated with the development of ESKD (p<0.035) and a 50% increase in serum creatinine (p<0.001), with an increased risk of 2.95 and 6.36 times, respectively.
The overdose of calcineurin inhibitors was associated with the development of ESKD, 50% increase in baseline creatinine, and RRT needed, with an increased risk by 3.63, 4.08, and 8.4 times, respectively. Not using everolimus as the immunosuppressive treatment and/or adjust the changes in immunosuppression drugs were also associated with a 50% increase in baseline creatinine. This is explained because the cause of switching immunosuppressants is usually associated to the development of AKI. When analyzing these variables in each transplant, only the no uses of everolimus nor changes in immunosuppression kept their statistical significance for lung transplant recipients.
Finally, nephrotoxic antimicrobials and intravenous contrast were associated with the risk of developing ESKD and increase of 50% in baseline creatinine. However, in the multinomial regression adjusted for the rest of the factors, this variable lost statistical significance; on the contrary, for intravenous contrast, an increased risk of 3.62 and 3.16 times for the development of ESDR and increased 50% of creatinine was observed.
Regarding the kidney damage in the post-transplant period, study findings mainly attributed to chronic damage from calcineurin inhibitors for all transplants. For heart transplants, in addition to calcineurin inhibitors, the development of cardiovascular risk factors and nephrotoxicity also contribute to the development of ESKD [14]. To reduce calcineurin inhibitors, nephrotoxicity, dose reduction protocols, and changes in immunosuppression are being studied with satisfactory results. Low-dose everolimus associated with low-dose calcineurin inhibitors in combination with mycophenolate and steroids has been associated with improved renal function, less vascular disease, and similar cardiac function at one year of follow-up studies [14,22]. In the case of liver transplants, it is estimated that in approximately 50% of patients who develop CKD, calcineurin inhibitor nephrotoxicity is the leading cause. Added this medication contribute to metabolic syndrome [18,21]. Anticalcineurin drug toxicity is the leading cause of renal dysfunction for lung transplants due to the high need for immunosuppression [14,20].
In the post-transplant period, no cardiovascular risk factor was associated with studied variables. However, analyzing each type of transplant, lung transplant recipients, the dyslipidemia variable was associated with the development of ESKD; moreover, hypertension was associated with a 50% increase in baseline creatinine.
The number of admissions was significantly associated with the development of ESKD, a 50% increase in creatinine, and death, with an increased risk for each admission of 1.103, 1.16, and 1.118, respectively.
Regarding immunosuppression, overdose of calcineurin inhibitors on more than three occasions was associated with developing ESKD and with an increase of 50% of baseline creatinine, with an augmented risk of 3.62 and 4.44 times, respectively.
Nephrotoxic drugs uses (nephrotoxic antimicrobials) were significantly associated with progression to ESKD. Nonetheless, this variable lost significance when was adjusted for other variables of risk, although it maintains a 2.6-fold increased risk of developing it. Similarly, it occurs with the uses of intravenous contrast for a 50% increase in baseline creatinine. When adjusting for other nephrotoxic drugs, despite having a 2.59-fold increased risk, it loses significance.
5. Conclusions
Currently, there is a growing increase in the number and comorbidity in patients who receive a NKSOT, the multidisciplinary management of these patients is of vital importance, especially with the collaboration of the different hospital departments and units. Thus, an early follow-up by the nephrologist is associated with a decrease in the decline of renal function, mainly, by acting on the renal-specific risk factors, such as the nephrotoxicity related to the overdose of calcineurin inhibitors, preventing AKI and allowing the identification of patients at higher risk during the pre-surgical period. Of interest, those patients requiring mechanical ventilation during peri-transplantation or those with the highest number of hospital admissions need special attention and monitoring by the nephrology department.. Further studies are required to evaluate these findings.
Author Contributions
Conceptualization, IVB. and LCLR.; methodology, IVB and LCLR.; software, IVB.; validation, IVB and LCLR.; formal analysis, IVB, LCLR, LDM and ACR.; investigation, IVB and LCLR.; resources, EGA, MCRT, APD and JHJ.; data curation, IVB and LCLR.; writing—original draft preparation, IVB and LCLR.; writing—review and editing, LCLR, LDM, ACR, MPF.; visualization, LDM, ACR, MPF.; supervision, EGA, JHD.; project administration, EGA, JHJ.; funding acquisition, IVB, JHJ. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Valencian Society of Nephrology by “María Isabel Buches” grant for research in Nephrology.
Institutional Review Board Statement
This study was performed in accordance with the ethical principles of the Declaration of Helsinki as revised in 2013. This study belonged to the project " Enfermedad renal crónica en trasplante de órgano sólido no renal. Análisis de la incidencia, factores de riesgo y pronóstico global de los diferentes tipos de trasplante de órgano sólido no re-nal", approved by the Hospital Universitari i Politècnic La Fe Clinical Research Ethics Committee, with the reference number 2021-302-1.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy and ethical reasons.
Conflicts of Interest
Prof. Dr. Luis D’Marco received lecture fees from AstraZeneca, Esteve and Novonordisk. Others authors declare no conflict of interest.
References
- Bloom, R.D.; Reese, P.P. Chronic kidney disease after nonrenal solid-organ transplantation. J Am Soc Nephrol. 2007, 18, 3031–3041. [Google Scholar] [CrossRef] [PubMed]
- Miller, B.W. Chronic kidney disease in solid-organ transplantation. Adv Chronic Kidney Dis. 2006, 13, 29. [Google Scholar] [CrossRef] [PubMed]
- Ojo, A.O.; Held, P.J.; Port, F.K.; Wolfe, R.A.; Leichtman, A.B.; Young, E.W.; Arndorfer, J.; Christensen, L.; Merion, R.M. Chronic renal failure after transplantation of a nonrenal organ. N Engl J Med. 2003, 349, 931–940. [Google Scholar] [CrossRef] [PubMed]
- González-Vílchez, F.; Almenar-Bonet, L.; Crespo-Leiro, M.G.; et al. Registro español de Trasplante Cardiaco. XXX Informe oficial de la Sección de Insuficiencia Cardiaca de la SEC (1984-2018). Rev Esp Cardiol. 2019, 72, 954–962. [Google Scholar] [CrossRef] [PubMed]
- Memoria de Resultados del Registro Español de Trasplante Hepático. Disponible en: http://www.sethepatico.org.
- Registro Español de Trasplante Pulmonar. Resultados 2001-2016. Disponible en: http://www.ont.es/.
- Kim, I.C.; Youn, J.C.; Kobashigawa, J.A. The Past, Present and Future of Heart Transplantation. Korean Circ J. 2018, 48, 565–590. [Google Scholar] [CrossRef] [PubMed]
- Adams, D.H.; Sanchez-Fueyo, A.; Samuel, D. From immunosuppression to tolerance. J Hepatol. 2015, 62 (Suppl. 1), S170–S185. [Google Scholar] [CrossRef] [PubMed]
- Ivulich, S.; Westall, G.; Dooley, M.; Snell, G. The Evolution of Lung Transplant Immunosuppression. Drugs 2018, 78, 965–982. [Google Scholar] [CrossRef]
- Schwarz, A.; Haller, H.; Schmitt, R.; et al. Biopsy-diagnosed renal disease in patients after transplantation of other organs and tissues. Am. J. Transplant. Of. J. Am. Soc. Transplant. Am. Soc. Transpl. Surg. 2010, 10, 2017–2025. [Google Scholar] [CrossRef] [PubMed]
- Ortiz, A.; Sanchez-Niño, M.D.; Crespo-Barrio, M.; De-Sequera-Ortiz, P.; Fernández-Giráldez, E.; García-Maset, R.; Macía-Heras, M.; Pérez-Fontán, M.; Rodríguez-Portillo, M.; Salgueira-Lazo, M.; Sánchez-Álvarez, E.; Santamaría-Olmo, R.; Simal-Blanco, F.; Pino-Pino, M.D. The Spanish Society of Nephrology (SENEFRO) commentary to the Spain GBD 2016 report: Keeping chronic kidney disease out of sight of health authorities will only magnify the problem. Nefrologia (Engl Ed) 2019, 39, 29–34. [Google Scholar] [CrossRef]
- Wiseman, A.C. CKD in Recipients of Nonkidney Solid Organ Transplants: A Review. Am. J. Kidney Dis. 2022. [Google Scholar] [CrossRef]
- Campbell, P.T.; Kosirog, M.; Aghaulor, B.; Gregory, D.; Pine, S.; Daud, A.; Das, A.; Finn, D.J.; Levitsky, J.; Holl, J.L.; Lloyd-Jones, D.M.; VanWagner, L.B. Comanagement With Nephrologist Care Is Associated With Fewer Cardiovascular Events Among Liver Transplant Recipients With Chronic Kidney Disease. Transplant Direct. 2021, 7, e766. [Google Scholar] [CrossRef] [PubMed]
- Vondran, F.W.R.; Wintterle, S.; Bräsen, J.H.; Haller, H.; Klempnauer, J.; Richter, N.; Lehner, F.; Schiffer, M. Abdominalchirurgie trifft Nephrologie: Wichtige nephrologische Aspekte vor und nach Nieren- bzw. Lebertransplantation [Transplant Surgeon Meets Nephrologist: Important Nephrological Aspects Before and After Kidney or Liver Transplantation]. Zentralbl Chir. 2017, 142, 180–188. [Google Scholar] [PubMed]
- Bloom, R.D.; Doyle, A.M. Kidney disease after heart and lung transplantation. Am J Transplant. 2006, 6, 671–679. [Google Scholar] [CrossRef] [PubMed]
- Bahirwani, R.; Campbell, M.S.; Siropaides, T.; Markmann, J.; Olthoff, K.; Shaked, A.; Bloom, R.D.; Reddy, K.R. Transplantation: impact of pretransplant renal insufficiency. Liver Transpl. 2008, 14, 665–671. [Google Scholar] [CrossRef] [PubMed]
- Banga, A.; Mohanka, M.; Mullins, J.; Bollineni, S.; Kaza, V.; Torres, F.; Tanriover, B. Association of pretransplant kidney function with outcomes after lung transplantation. Clin Transplant. 2017, 31. [Google Scholar] [CrossRef] [PubMed]
- Fortrie, G.; Manintveld, O.C.; Caliskan, K.; Bekkers, J.A.; Betjes, M.G. Acute Kidney Injury as a Complication of Cardiac Transplantation: Incidence, Risk Factors, and Impact on 1-year Mortality and Renal Function. Transplantation 2016, 100, 1740–1749. [Google Scholar] [CrossRef] [PubMed]
- Pacheco, M.P.; Carneiro-D'Albuquerque, L.A.; Mazo, D.F. Current aspects of renal dysfunction after liver transplantation. World J Hepatol. 2022, 14, 45–61. [Google Scholar] [CrossRef] [PubMed]
- Atchade, E.; Barour, S.; Tran-Dinh, A.; Jean-Baptiste, S.; Tanaka, S.; Tashk, P.; Snauwaert, A.; Lortat-Jacob, B.; Mourin, G.; Mordant, P.; Castier, Y.; Mal, H.; De Tymowski, C.; Montravers, P. Acute Kidney Injury After Lung Transplantation: Perioperative Risk Factors and Outcome. Transplant Proc. 2020, 52, 967–976. [Google Scholar] [CrossRef] [PubMed]
- Rocha, P.N.; Rocha, A.T.; Palmer, S.M.; Davis, R.D.; Smith, S.R. Acute renal failure after lung transplantation: incidence, predictors and impact on perioperative morbidity and mortality. Am J Transplant. 2005, 5, 1469–1476. [Google Scholar] [CrossRef]
- Nevens, F.; Pirenne, J. Renal disease in the allograft recipient. Best Pract Res Clin Gastroenterol 2020, 46–47, 101690. [Google Scholar] [CrossRef]
- Andreassen, A.K.; Andersson, B.; Gustafsson, F.; Eiskjaer, H.; Rådegran, G.; Gude, E.; Jansson, K.; Solbu, D.; Karason, K.; Arora, S.; Dellgren, G.; Gullestad, L.; SCHEDULE Investigators. Everolimus Initiation With Early Calcineurin Inhibitor Withdrawal in De Novo Heart Transplant Recipients: Three-Year Results From the Randomized SCHEDULE Study. Am J Transplant. 2016, 16, 1238–1247. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Patient selection.
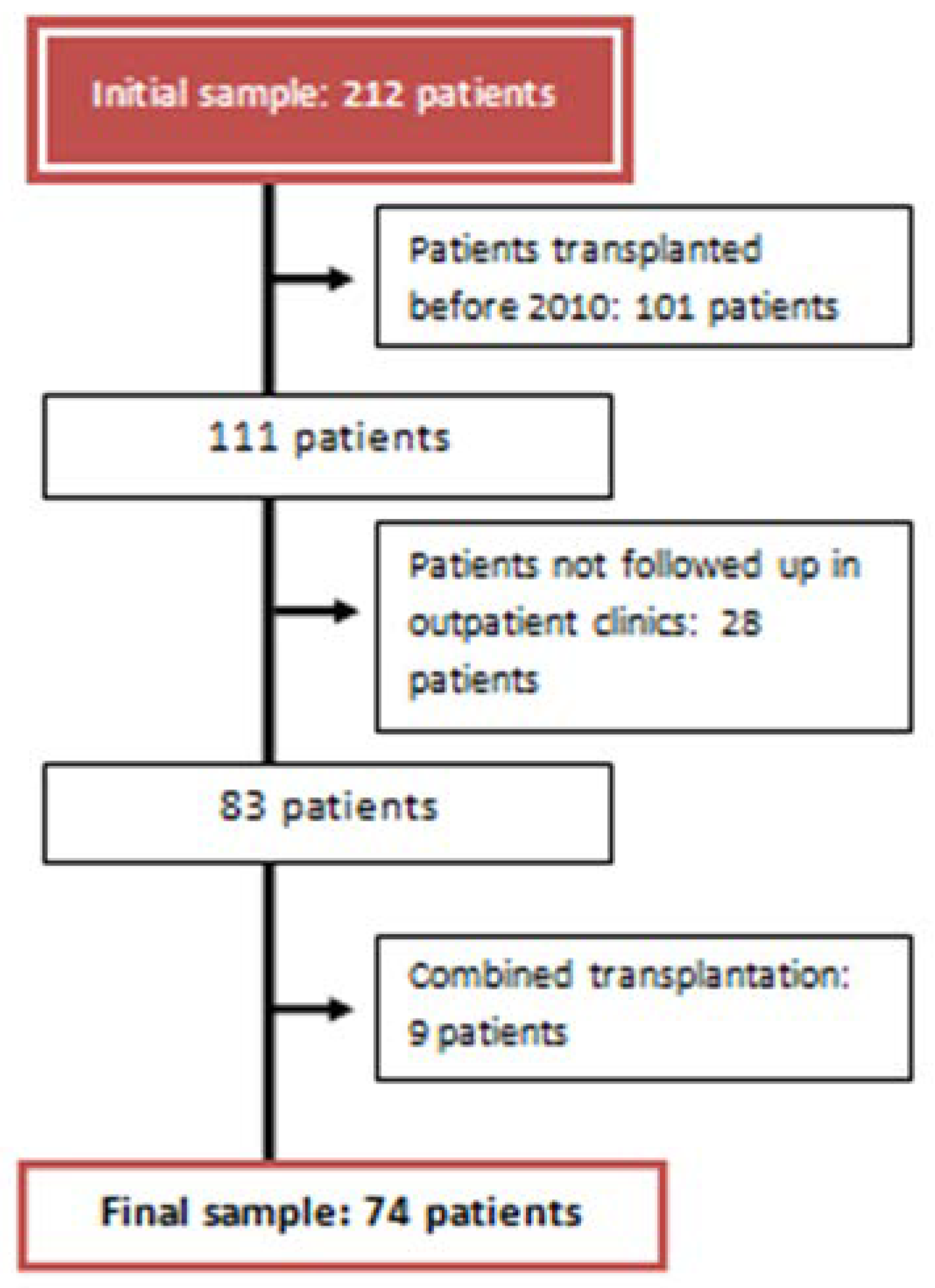
Figure 2.
Variables analyzed in each period.
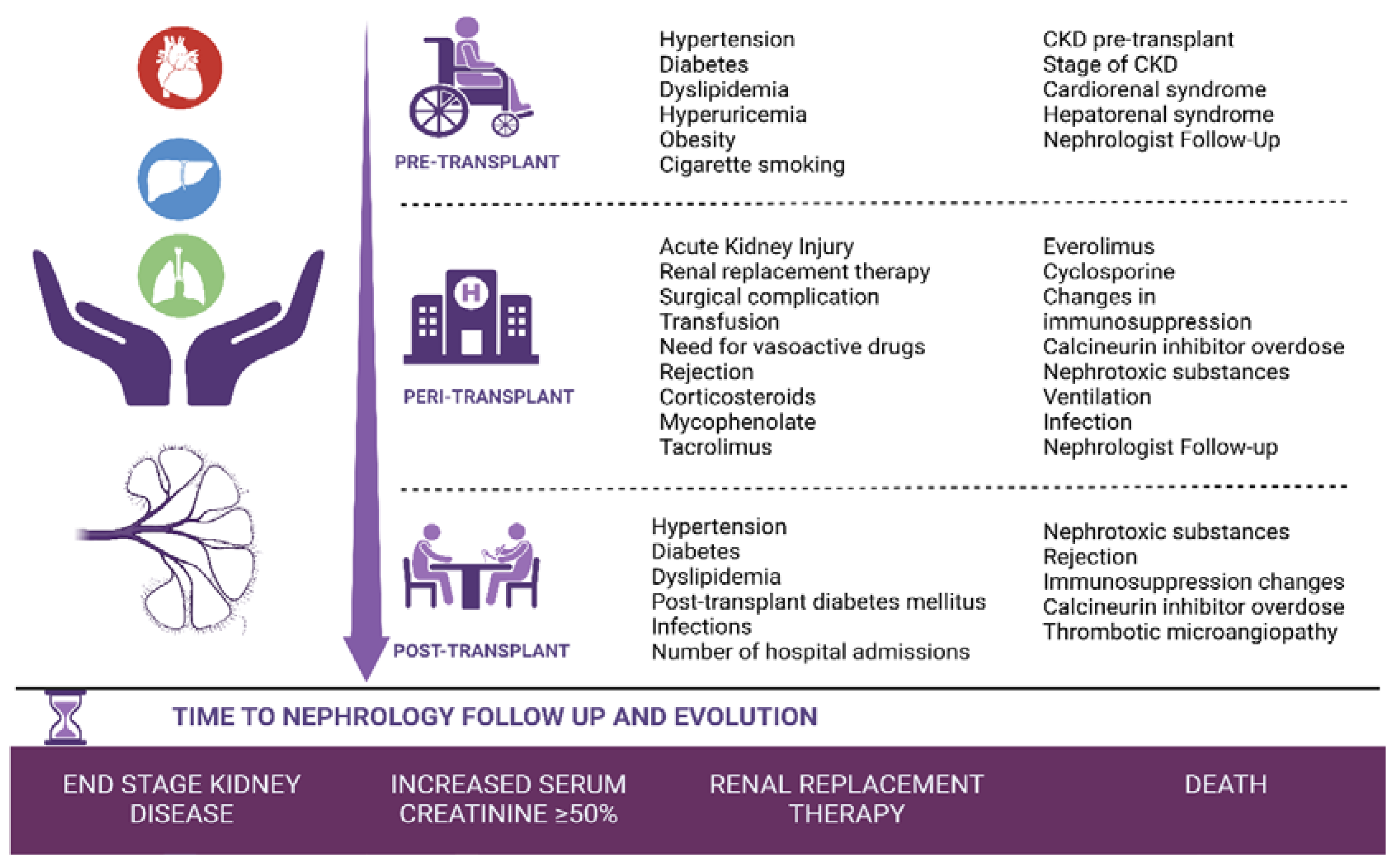
Figure 3.
Mean ESKD-free survival of heart transplant recipients, liver transplant recipients and lung transplant recipients.
Figure 3.
Mean ESKD-free survival of heart transplant recipients, liver transplant recipients and lung transplant recipients.
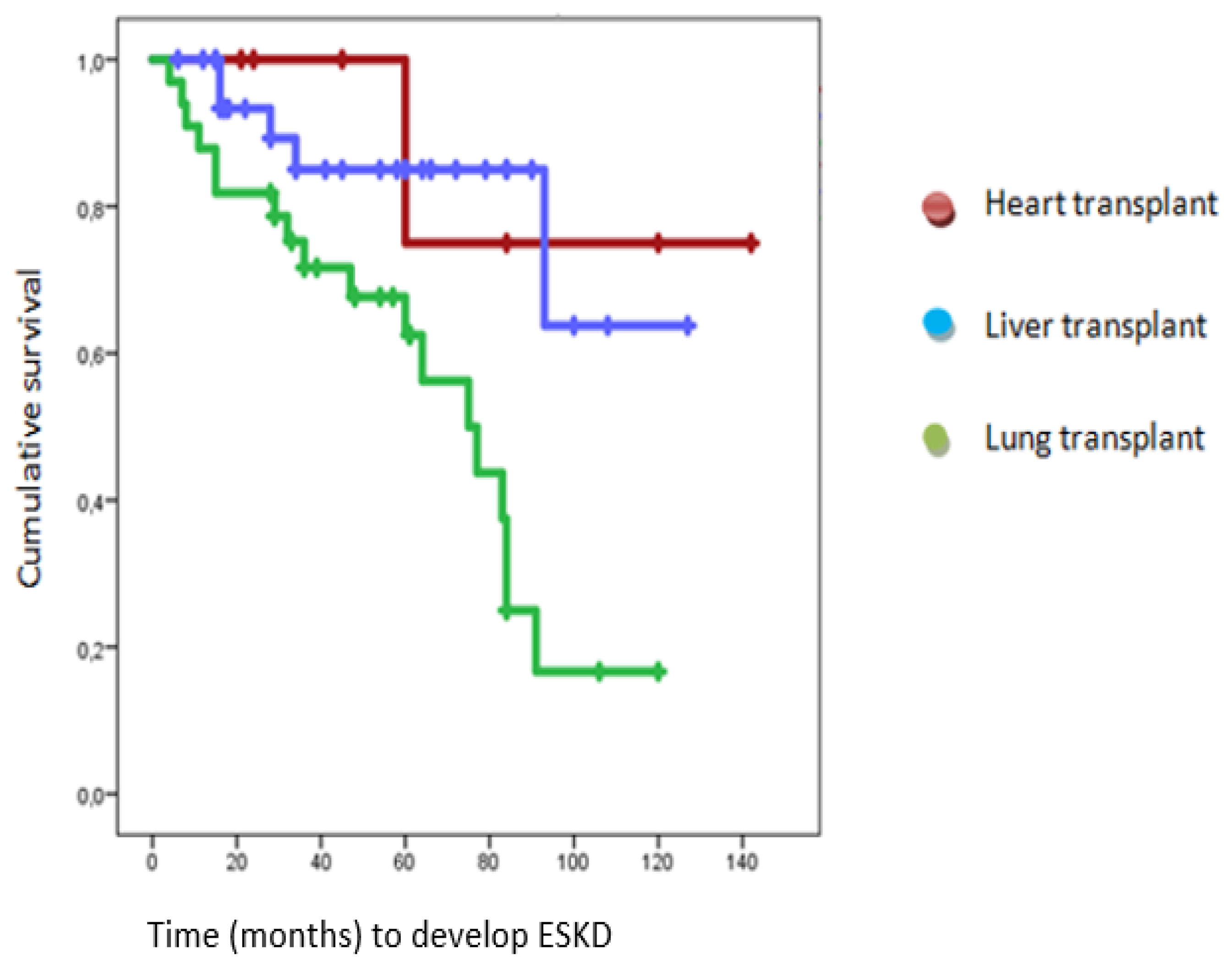

Table 1.
Baseline characteristics.
| GLOBAL (74) | HEART (7) | LIVER (34) | LUNG (33) | |
| Age (years) | 54.39 | 49.42 | 58.71 | 51 |
| Sex (%) | Men: 73 Women: 27 |
Men: 85.7 Women: 14.3 |
Men: 79.4 Women: 20.6 |
Man: 63.6 Women: 36.4 |
| Pre-transplantation | ||||
| Hypertension (%) | 37.8 | 57.1 | 39.4 | 33.3 |
| Diabetes (%) | 27.1 | 14.3 | 51.5 | 26.1 |
| Dyslipidemia (%) | 25.7 | 42.9 | 18.2 | 27.3 |
| Hyperuricemia (%) | 14.9 | 14.3 | 15.2 | 15.2 |
| Overweight (%) | 23 | 28.6 | 33.3 | 12.1 |
| Obesity (%) | 18.9 | 28.6 | 27.3 | 9.1 |
| Ex-smoker (%) | 55.4 | 42.9 | 42.4 | 72.7 |
| Smoker (%) | 8.1 | 28.6 | 12.1 | 0 |
| Cardiorenal syndrome (%) | 6.8 | 28.6 | 3 | 6.1 |
| Hepatorenal syndrome (%) | 18.9 | 0 | 39.4 | 0 |
| CKD (%) | 23 | 28.6 | 45.5 | 0 |
| Stage or CKD (%) | G3a: 65.21 G3b: 23.91 G4: 10.88 |
G3a: 100 G3b: 0 G4: 0 |
G3a: 60 G3b: 26.6 G4: 13.4 |
G3a: 0 G3b: 0 G4: 0 |
| Nephrologist Follow-up (%) | 14.9 | 28.6 | 18.2 | 6.1 |
| Peri-transplantation | ||||
| AKI (%) | 58.1 | 85.7 | 63.6 | 48.5 |
| RRT (%) | 5.4 | 28.6 | 0 | 6.1 |
| Surgical complications (%) | 51.4 | 57.1 | 30.3 | 72.7 |
| Transfusion requirements (%) | 87.8 | 71.4 | 97 | 81.8 |
| Vasoactive drugs (%) | 54.1 | 85.7 | 98.5 | 54.5 |
| Mechanical ventilation (%) | 44.6 | 42.9 | 15.2 | 75.8 |
| Infections (%) | 62.6 | 57.1 | 36.4 | 90.9 |
| Tacrolimus (%) | 81.8 | 57.1 | 78.8 | 87.9 |
| Cyclosporine (%) | 23 | 42.9 | 18.2 | 24.2 |
| Mycophenolate (%) | 98.6 | 100 | 97 | 100 |
| Everolimus (%) | 8.2 | 14.3 | 9.1 | 6.1 |
| Corticosteroids (%) | 90.5 | 100 | 78.8 | 100 |
| Changes in immunosuppression (%) | 14.9 | 28.6 | 12.1 | 15.2 |
| Graft rejection (%) | 20.3 | 71.4 | 9.1 | 21.2 |
| Calcineurin inhibitor overdose (%) | 50 | 42.9 | 21.2 | 81.8 |
| Nephrotoxic substances (%) | 64.9 | 100 | 33.3 | 91 |
|
NSAIDS (%) Antimicrobials (%) Intravenous contrast (%) Combinations of nephrotoxic (%) |
4.16 31.27 20.80 43.77 |
14.2 42.9 42.9 0 |
9 63.66 18.31 9 |
0 16.7 16.7 66.6 |
| Nephrologist Follow-up (%) | 18.9 | 42.9 | 21.2 | 12.1 |
| Post-transplantation | ||||
| New hypertension (%) | 23 | 28.6 | 15.1 | 30.3 |
| PTDM (%) | 23 | 28.6 | 15.2 | 30.3 |
| New dyslipidemia (%) | 17.5 | 57.1 | 12.1 | 18.2 |
| Admissions (mean) | 6.8 | 6.8 | 3.79 | 9.15 |
| Infections | 78.4 | 42.9 | 69.7 | 93.9 |
| Calcineurin inhibitor overdose (%) | 66.2 | 71.4 | 36.4 | 97 |
| Changes in immunosuppression (%) | 68.9 | 57.1 | 51.5 | 90.9 |
| Graft rejection (%) | 31.1 | 85.7 | 15.2 | 36.4 |
| Nephrotoxic substances (%) | 77 | 100 | 57.6 | 93.9 |
|
NSAIDS (%) Antimicrobials (%) Intravenous contrast (%) Others (%) Combinations of nephrotoxic (%) |
1.75 17.53 19.35 1.75 59.62 |
0 0 71.4 0 28.6 |
5.2 42.84 15.79 5.2 31.97 |
0 6.49 9.69 0 82.82 |
| TMA (%) | 9.5 | 14.3 | 0 | 18.2 |
| Final results | ||||
| Time to Nephrology follow up (mean, months) | 33.01 | 33.71 | 28.24 | 38.64 |
|
Worsened renal function (%) Improved or maintain renal function stable (%) |
45.9 54.1 |
28.57 74.43 |
44.11 55.89 |
51.5 48.5 |
| Increase in baseline creatinine by 50% (%) | 59.5 | 42.9 | 32.35 | 90.9 |
| ESKD (%) | 32.43 | 14.3 | 14.7 | 54.54 |
| RRT (%) | 10.8 | 14.3 | 6.1 | 15.2 |
| Exitus (%) | 28.4 | 0 | 32.35 | 30.3 |
Table 2.
Statistically significant results of Increase baseline by 50% variable.
| Factors | N | % | p-value | Hazard Ratio |
| Type of transplant | P < 0.05 | |||
| Heart transplantation | 3 | 42.9 | HR 0.075 [95% CI] 0.01 to 0.5 | |
| Liver transplantation | 11 | 32.4 | HR 0.048 [95% CI] 0.012 to 0.192 | |
| Lung transplantation | 30 | 90.9 | This parameter is set to zero because it is redundant. | |
| Pre-transplant period | ||||
| CKD | 3 | 17.6 | p<0.001 | HR 0.084 [95% CI] 0.021 to 0.331 |
| Not having follow-up by Nephrology | 41 | 65.1 | p<0.027 | HR 4.97 [95% CI] 1.196 to 20.651 |
| Peri-transplant period | ||||
| Mechanical ventilation | 27 | 81.8 | p<0.001 | HR 6.353 [95% CI] 2.155 to 18.726 |
| Calcineurin inhibitor overdose | 28 | 75.7 | p<0.006 | HR 4.083 [95% CI] 1.512 to 11.028 |
| Nephrotoxic | 33 | 68.8 | p<0.029 | HR 3 [95% CI] 1.116 to 8.064 |
| Antimicrobials | 26 | 74.3 | p<0.012 | HR 3.569 [95% CI] 1.324 to 9.62 |
| Intravenous contrast | 24 | 77.4 | p<0.009 | HR 3.943 [95% CI] 1.403 to 11.082 |
| No use of everolimus | 44 | 64.7 | P< 0.001 | HR 15722797292 |
| Not making changes in immunosuppression | 41 | 65.1 | p<0.027 | HR 4.97 [95% CI] 1.196 to 20.651 |
| Not having follow-up by Nephrology | 39 | 65 | P<0.046 | HR 3.34 [95% CI] 1.01 to 11.26 |
| Post-transplant period | ||||
| Calcineurin inhibitor overdose | 35 | 71.4 | p<0.004 | HR 4.444 [95% CI] 1.594 to 12.390 |
| Intravenous contrast | 31 | 70.5 | P<0.022 | HR 3.118 [95% CI] 1.182 to 8.226 |
| Number of hospital admissions | P< 0.006 | HR 1.169 [95% CI] 1.046 to 1.306 | ||
| Time until outpatient Nephrology consultation | P<0.002 | HR 1.032 [95% CI] 1.011 to 1.054 | ||
Table 3.
Statistically significant results of Advanced Chronic Kidney Disease (ACKD).
| Factors | N | % | p-value | Hazard Ratio |
| Type of transplant | P <0.001 | |||
| Heart transplantation | 1 | 14.3 | P<0.082 | HR 0.13 [95% CI] 0.015 to 1.28 |
| Liver transplantation | 5 | 14.7 | P< 0.001 | HR 0.144 [95% CI] 0.045 to 0.463 |
| Lung transplantation | 18 | 54.5 | This parameter is set to zero because it is redundant. | |
| Peri-transplant period | ||||
| Mechanical ventilation | 15 | 45.5 | P <0.035 | HR 2.963 [95% CI] 1.081 to 8.120 |
| Calcineurin inhibitor overdose | 17 | 45.9 | P<0.015 | HR 3.643 [95% CI] 1.27 to 10.372 |
| Antimicrobials | 16 | 45.7 | P< 0.028 | HR 3.158 [95% CI] 1.133 to 8.801 |
| Intravenous contrast | 16 | 51.6 | P< 0.004 | HR 4.667 [95% CI] 1.646 to 13.232 |
| Post-transplant period | ||||
| Calcineurin inhibitor overdose | 20 | 40.8 | P< 0.037 | HR 3.621 [95% CI] 1.078 to 12.161 |
| Antimicrobials | 18 | 42.9 | P<0.032 | HR 3.25 [95% CI] 1.106 to 9.548 |
| Number of hospital admissions | P< 0.020 | HR 1.103 [95% CI] 1.015 to 1.198 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



