
Submitted:
24 February 2023
Posted:
27 February 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
The coronavirus disease (COVID-19) vaccine is key to reducing the probability of contracting COVID-19. The vaccine is generally known to prevent severe illness, death, and hospitalization as a result of the disease and for considerably reducing COVID-19 infection risk. Accordingly, this might significantly change an individual’s perceived risk of altering everyday behaviors. For instance, the proliferation of vaccination is anticipated to reduce preventive behaviors such as staying at home, handwashing, and wearing a mask. We corresponded with the same individuals monthly for 18 months from March 2020 (early stage of COVID-19) to September 2021 in Japan to independently construct large sample panel data (N=54,007), with a participation rate of 54.7 %. We used a fixed effects model, controlling for key confounders, to determine whether vaccination was associated with a change in preventive behaviors. The major findings are as follows. Contrary to the prediction, (1) based on the whole sample, being vaccinated against COVID-19 led people to stay at home; however, it did not change the habit of handwashing and wearing a mask. Especially after the second shot, respondents were likelier to stay at home by 0.107 (95% CIs: 0.059–0.154) points on a 5-point scale compared to before the vaccination. Dividing the entire sample into young and old, (2) those aged ≤ 40 years were more likely to go out after being vaccinated, and (3) people over 40 years of age were more likely to stay at home (similar to the first result). Preventive behaviors impact all individuals during the current pandemic. Informal social norms motivate people to increase or maintain preventive behaviors even after being vaccinated in societies where these behaviors are not enforced.
Keywords:
Vaccine
; COVID-19
; Preventive behaviors
; Norm
; Japan
; Panel data
1. Introduction
To reduce coronavirus disease (COVID-19) transmission, many countries implemented lockdowns. People were obliged to follow preventive behaviors enforced by the government; otherwise, they were penalized [1]. Economic activities were suspended following restrictions on daily movements [2,3]. Subsequently, lockdowns significantly reduced the contact rate and spread of COVID-19 [4,5,6].
However, lockdown restrictions create significant economic losses [7,8] and negatively impact individuals’ mental health [9,10,11,12]. Therefore, the Japanese government has declared a “state of emergency” wherein preventive behaviors are strongly required but not enforced. Without enforcement, Japanese people continued to adhere to preventive behaviors by staying at home, washing their hands frequently, and wearing masks [13].
Various vaccines against COVID-19 have been developed and distributed worldwide. Vaccination is expected to significantly reduce the spread of COVID-19. The number of newly reported cases of COVID-19 has been observed to have reduced in countries where the vaccines were rapidly adopted [14]. Accordingly, the mental condition of vaccinated individuals improved [15,16,17].
In Japan, the first case of COVID-19 infection was confirmed on January 16, 2020. Based on the New Infectious Diseases Law, the Japanese Government recognized COVID-19 as a “designated infectious disease.” Accordingly, the Japanese government implemented enforced hospitalization and restricted work if a person was infected with COVID-19. However, the number of infected people surged in April 2020. To mitigate the rapid spread of COVID-19, the government declared a state of emergency on April 7, 2020. However, the government only requested citizens to wash hands and wear masks and avoid direct contact and social gatherings. Unlike the lockdown adopted in other countries, they were neither punished nor penalized under the state of emergency, even if people did not follow the request. Inevitably, people could behave according to their free will, although moral and informal social norms deterred them slightly from practicing undesirable behaviors. On May 25, 2020, the state of emergency was deregulated as the number of daily infected persons remarkably reduced. Subsequently, until Autumn 2021, COVID-19 patients was cyclically observed; thus, the state of emergency was declared four times during the study period between March 2020 and September 2021. In Japan, vaccination was introduced in February 2021 [18]. Initially, vaccination was strictly limited to those who had a higher risk of contracting COVID-19. The regulation was then relaxed in stages, which led to more widespread vaccination.
Widespread vaccination can promote economic activities as vaccinated people may not exhibit rigid preventive behaviors and readopt their pre-COVID-19 lifestyle [19,20,21,22]. While Japanese people did not change their consumption behavior even after vaccination, they were likely to increase their consumption after eradication of COVID-19 [23].
Hence, analyzing the mechanism behind the unexpected consumption behavior in Japan is crucial. Using monthly individual-level panel data, we investigate whether individuals’ preventive behaviors change before and after vaccination. Further, following the COVID-19 pandemic, individuals’ reactions to changes in policies related to COVID-19 differ according to their situation [13]. Time lags exist for the diffusion of vaccination among different generations in Japan. Our simulation study shows that determining economic loss during the pandemic depends on whether COVID-19 is allocated according to age group [24]. Hence, we compared the difference in the impact of the uptake of the COVID-19 vaccine between the young and old generations, considering that they are exposed to different situations.
2. Materials and Methods
2.1. Data Collection
We commissioned the research company INTAGE to conduct an internet survey based on their experience and reliability. The first wave of queries was conducted from March 13, 2020, to March 16, 2020, recording 4,359 observations with a participation rate of 54.7 %. Participants registered with INTAGE were recruited for this study. The sampling method was designed to gather a representative sample of the Japanese population in terms of gender, age, educational background, and residential area. Basically, the overall sample is designed to be representative of the Japanese adult population and the responding sample weighted to be representative of the Japanese population. However, the sample population was restricted to ages 16–79; individuals aged 15 years and below were considered too young to be registered with INTAGE, and we considered individuals over 80 years of age too old to answer the pertinent questions. To construct a sample representative of the Japanese population, INTAGE recruits participants to a survey from among pre-registered people. Participants were randomly selected to fill the pre-specified quotas. While INTAGE provided monetary incentives to participants upon study completion, the company did not provide specific information regarding said incentives.
Japanese citizens aged 16–79 years were selected for the survey. Internet surveys were conducted repeatedly for 15 separate times (“waves”) almost every month with the same individuals to construct the panel data. However, the survey could not be conducted for the period between July 2020 and September 2020 owing to a shortage of research funds. We resumed the surveys after receiving additional funds from October 2020.
Respondents from the first wave were targeted in the subsequent waves to record how the same respondent changed their perceptions and behaviors during the COVID-19 pandemic. During the study period, some of the respondents stopped taking the surveys, while others did not take the surveys at all. The total number of observations used in this study was 54,007.
2.2. Ethical Considerations
Our study was performed according to the relevant guidelines and regulations. The ethics committee of Osaka University approved all survey procedures, and informed consent was obtained from all participants. The ethics approval number of Osaka University for this study is R021014.
After being informed about the purpose of the study and their right to quit at any time, participants agreed to participate. The completion of the entire questionnaire was considered to indicate the participants’ consent.
2.3. Measurements
The survey questionnaire contained basic questions about demographics such as age, gender, and educational background. Fifteen waves were conducted between March 2020 and September 2021. As the main variables, the respondents were asked questions concerning preventive behaviors as follows:
“Within a week, to what degree have you practiced the following behaviors? Please answer based on a scale of 1 (I have not practiced this behavior at all) to 5 (I have completely practiced this behavior).”
- (1)
- Staying indoors
- (2)
- Not going out to the workplace (or school)
- (3)
- Not going out to the events or travel
- (4)
- Washing my hands thoroughly
- (5)
- Wearing a mask
The answers to these questions served as proxies for the following variables for preventive behaviors: staying indoors, not going out for work, not participating in leisure activities outside home, frequently handwashing, and wearing masks. Larger values indicate that respondents are more likely to engage in preventive behaviors. Staying indoors generally captures the degree of staying (not going out) at home. For more specific behaviors, we asked about the type of voluntary restraint while going out. Not going out for work captures the degree of avoidance in going out for work or school. Not participating in leisure activities outside the home captures the degree of avoidance in going out for events or travel. In the case of the former, preventive behavior depends on the condition of the workplace or school. Hence, respondents may have been obliged to go to work or school. The latter is more likely to depend on an individual’s decision-making. Further, we asked about the subjective probability of contracting COVID-19 and their perception of the severity of COVID-19.
2.4. Methods
We used panel data, pooling cross-sections across time. Based on the panel data, we used a fixed effects (FE) model regression to control for time-invariant individual fixed effects. The FE model is a type of linear regression model widely used in economics. The estimation result using an FE model is equivalent to the results of a linear regression model with dummies of individuals who are frequently included in each period [25,26,27]. The FE model can also be applied not only to linear regression, but also to other types of regression such as conditional logistic regression [28]. In the case of this study, 4,358 dummies are included to control for individuals’ characteristics that do not change during the period, such as gender, educational background, childhood experience, and so on. Hence, 4,358 cofounders are included and they reflect differences between individuals. Even if various time-variant cofounders are included, unobserved individual characteristics cannot be captured. This inevitably results in omitted variable biases [25,27]. In the FE model, an individual’s time-invariant characteristics can be completely controlled, reducing the possibility of omitted variable biases. However, the estimated results for time-invariant confounders cannot be obtained. For instance, we cannot calculate how educational background is correlated with the dependent variable.
Furthermore, in the model used in this study, we also controlled for differences between different time points of the survey. Government policy and the degree of spread of COVID-19 vary in the 15 time points in the survey. Similar to time-invariant individual effects, controlling for differences between time points is impossible, even if we include various cofounders that vary according to time points (e.g., macroeconomic shocks and policy effects). We should control for this to mitigate omitted variable biases. Therefore, we included 14 dummies for different waves, while we set the first wave as the reference group. Thus, the common time-specific effects covering all parts of Japan are completely controlled. Meanwhile, the effect of government policy cannot be calculated, which was implemented throughout Japan simultaneously.
Therefore, in this model, we controlled for not only unobservable individual effects but also unobservable time effects. This type of FE model is specifically called the two-way error component regression model [27]. Estimation results are less likely to suffer from omitted variable biases in this model, however, we cannot calculate the estimated effects of various policies, educational backgrounds, and gender differences. In other words, this study focuses on the correlation between vaccination and preventive behaviors. The statistical software used in this study was Stata/MP 15.0.
The estimated function of FE model takes the following form:
Yit =α1 VACCINE FIRSTit +α2 VACCINE SECOND_1it +α3 VACCINE SECOND_2it +α4 VACCINE SECOND_3it +α5 VACCINE SECOND_4it + α6 PROB COVID19it + α7 SEVERITY COVID19 it +α8 EMERGENCY it + kt + mi + u itg
In this formula, Y itp represents the dependent variable for individual i and wave t. Y includes preventive behaviors captured by the five proxy variables defined in Table 1: STAYING INDOORS, NOT GOING TO WORK, NOT FOR LEISURE, HANDWASHING, and WEARING MASK. These are discrete ordered variables from 1 to 5. Larger values of these variables can be interpreted as meaning that the respondents are more likely to exhibit preventive behavior. In the same specification, we conduct five estimations separately, and the regression parameters are denoted as α. The error term is denoted by u, and kt represents the effects of different time points, controlled by 14 wave dummies, where the first wave is the reference group. Various shocks occurred simultaneously throughout Japan at each time point. Wave dummies were included to control for this. The estimation method is the fixed effects (FE) model, and the time-invariant individual-level fixed effects are represented by mi. This means that the model controls various individual characteristics that do not change, even if time has passed. Hence, sex, educational background, and various factors were controlled for. During the study period, respondents’ ages increased by only one year, and the timing of this change depended on their birthday. Therefore, the variation in age reflects birthdays in the FE model. Hence, age was not included in the model, even though the results did not change after including age in the model. A simple FE linear regression model was used in this study. However, proxy variables for preventive behaviors include the scores of the scale, which are ordered from 1 to 5. Therefore, these are discrete variables and not continuous ones. Hence, for closer examination, we use the FE ordered logit model to conduct the estimation because the dependent variable is a multinomial ordered response [29,30].
Key independent variables are vaccination dummies; vaccine first controls the effect of the first shot. Various pharmaceutical companies have developed vaccines. However, the Japanese government approved only those developed by Pfizer and BioNTech. People are obliged to get the second shot within a month of taking the first shot, to make the vaccine effective. This rule applied to the Pfizer and BioNTech vaccines. The effect of the second shot should then be estimated separately. Further, investigating how the association between the vaccine and preventive behaviors changes over time. Therefore, we included VACCINE SECOND_1, VACCINE SECOND_2, VACCINE SECOND_3, and VACCINE SECOND_4.
In Japan, declarations of the state of emergency significantly affected behaviors [13,31]. However, the timing of the declarations differed according to the area. Therefore, the effect of the declaration could not be captured by wave dummies. Hence, we include EMERGENCY to control for the effects of the declaration of emergency. Furthermore, the subjective perception of COVID-19 is expected to influence preventive behavior. For instance, people are more likely to be cautious about COVID-19 if they consider the probability of contracting COVID-19 and the severity of the damage done by COVID-19 as higher [32,33]. To control for this, we include PROB COVID19 and SEVERITY COVID19. Although their results were not reported, we also controlled for the following factors: the number of persons infected with COVID-19 and the deaths caused by COVID-19 in residential areas at each time point. Subjective emotions, such as anxiety, fear, and anger, are also controlled by including ANGER, FEAR, and ANXIETY.
The motivation for obtaining a shot of vaccination depends on age [34,35]. Association between vaccination and preventive behaviors that vary according to an individual’s situation. Moreover, considering the whole sample, we conduct estimations by dividing it into two: young (below 40 years) and old (equivalent or over 40 years).
3. Results
As explained in the previous section, the sampling method was designed to gather a representative sample of the Japanese population in terms of gender, age, educational background, and residential area. Our survey included Japanese citizens between 16 and 79 years of age from all regions of Japan and covered all parts of Japan. The age range and demographic composition of the sample, shown in Figure 1, were almost equivalent to those of the 2015 Japan Census. However, some gaps exist in the aged population between the census data and the survey data used in this study. The percentage of younger participants in the survey sample was lower. Particularly, the gap is large for the age group 16–20, reflecting that they are too young to be registered with INTAGE. The percentage of participants belonging to the age groups 66–70 and age group 71–75 in our sample is higher than that in the Census, whereas those belonging to the age group 76–79 in our sample is lower. On the one hand, retired older people have spare time enough to participate in the survey. On the other hand, older people were not young enough to participate in the questionnaire. Figure 2 demonstrates the composition of the population in 47 residential prefectures using our survey sample and census sample. Figure 2 shows a similar geographical population distribution. Overall, the sample used in the present study can be considered representative of public opinion in Japan.
In the first survey, a questionnaire was sent to 7,968 people who were registered with a research company, and its participation rate was 54.7 %. Therefore, 4,359 observations were obtained. Subsequently, in every survey, the questionnaire was sent to respondents who participated in the first survey; thus, 4,359 people. Table 2 shows the number of observations and loss rates as some respondents did not respond. The loss rate is approximately 20% in each survey.
Table 3 suggests that the mean values of staying indoors and not going out for work were 2.91 and 2.94, respectively. Meanwhile, the value of not participating in leisure activities outside home was 4.12. This means that people are more likely to go to work or school than to engage in leisure activities. This suggests that events or travel are considered less essential than work or school. Staying indoors consists of both essential and non-essential components. Overall, not going out to work is critical in determining the probability of staying indoors. Not going out for work is determined not by an individual’s will but by instruction from the workplace or school. Similar to refraining from leisure activities, the mean values of handwashing and wearing masks were slightly larger than 4. This is because handwashing and wearing masks is likely to depend on an individual’s willingness.
We also asked respondents whether they had taken the first shot of the vaccine against COVID-19 and whether they had completed the second vaccine shot. In Japan, vaccination began on February 2021 [18]. During this period, the first group eligible for the shot was strictly limited to health workers, before the inoculation program was expanded to include the general public. Vaccination for the older people aged 65 and over has been implemented since April 2021, and 75 % of older people have been vaccinated as of July 2021 [36]. Additionally, the government has begun implementing COVID-19 vaccination programs at workplaces and campuses where workers and students can get vaccinations since June [37].
The 10th wave survey was conducted directly after February 2021. In the sample used in this study, respondents who received the shot appeared from the 12th wave conducted in May 2021. On the dummies for vaccination, the mean values of VACCINE SECOND_1, VACCINE SECOND_2, VACCINE SECOND_3, and VACCINE SECOND_4 are 0.03, 0.02, 0.01, and 0.001, respectively. Therefore, in the entire sample, people who received the second shot at the time of the survey accounted for 3%. The number of people who received the second shot last month, 2 months ago, and 3 months ago were 2 %, 1 %, and only 0.1%, respectively. The entire sample covered first-eleventh waves, where nobody received the shot, and so percentages were very low. The vaccine was distributed to healthcare workers first, followed by older people, and others. Therefore, the percentage declines with people who received the second shot earlier.
To check the change in vaccination rate, Table 4 shows the percentage of vaccinated people in each wave. Contrary to the vaccination dummy, Table 4 indicates the aggregated values containing both the first and second vaccinated people regardless of the vaccination time point. Therefore, the percentage of vaccinated individuals is expected to increase over time. Consistent with this inference, Table 4 indicates that the percentage of vaccinated people rapidly increased from 8.2% in May 2021 to 64.2% at the beginning of September in the sample. This rate is similar to that of 65.2 % in September using country-wide data [38]. In the subsample of people over 40, the rate increased from 9.1% in May 2021 to 72.3%, almost twice as high as that in the subsample of younger people in each wave. Thus, the data in this study are representative of the actual situation in Japan.
Figure 3 illustrates the change in five preventive behaviors from the first to the fifteenth waves by dividing the sample into vaccinated and unvaccinated groups. Figure 3 covers the periods before and after vaccination. Therefore, nobody was vaccinated from the first to the eleventh waves, and the left part of the vertical line is shown in Figure 3. In this study, people vaccinated during any period were included in the vaccinated group. Furthermore, we did not distinguish people who received the second shot from those who only received the first. For instance, one who received their first shot in the fifteenth wave was included in the vaccinated group. Thus, Figure 3 indicates how people who did not intend to be vaccinated behaved differently from vaccinated people from the period when the vaccine was not distributed.
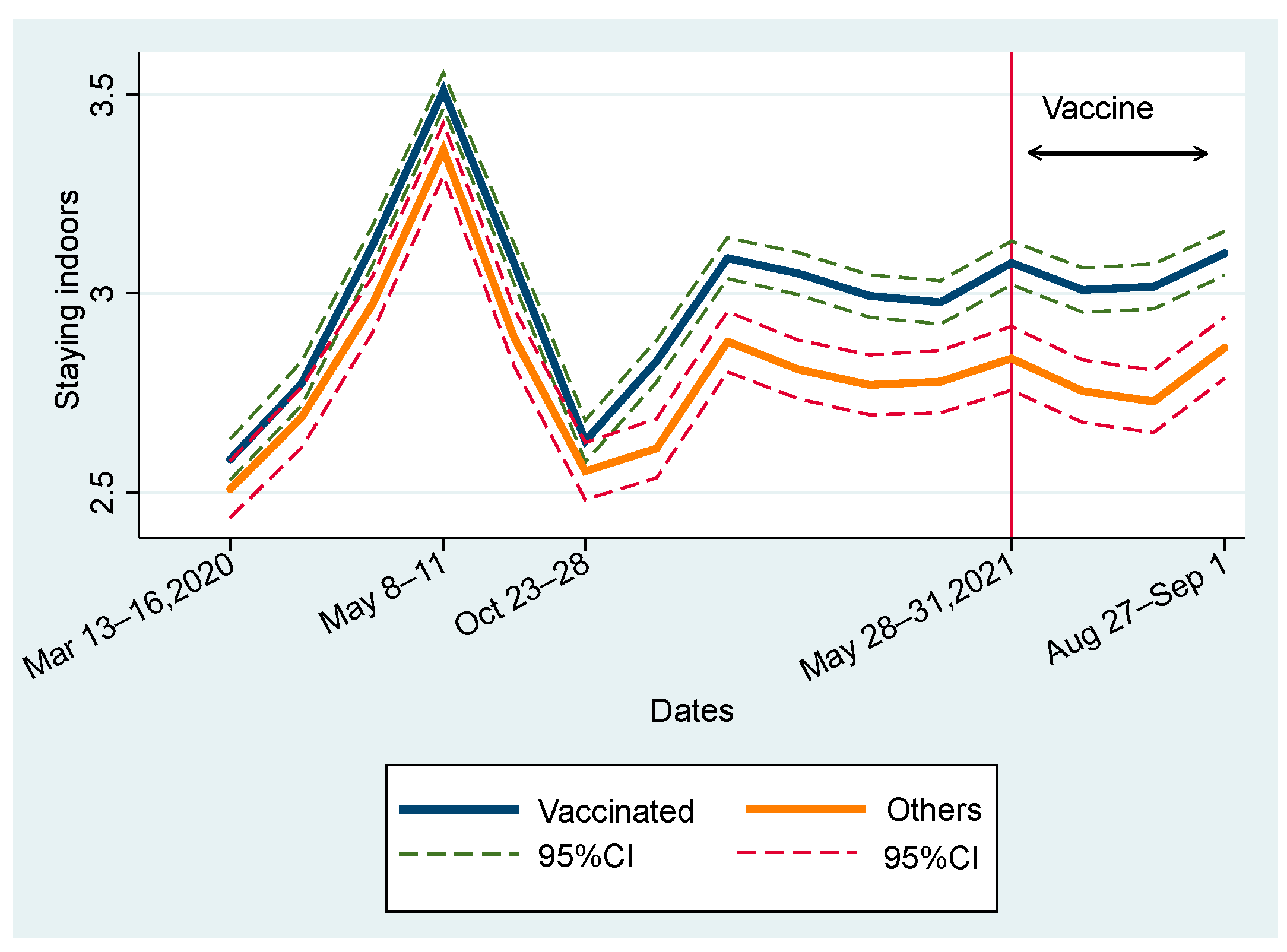
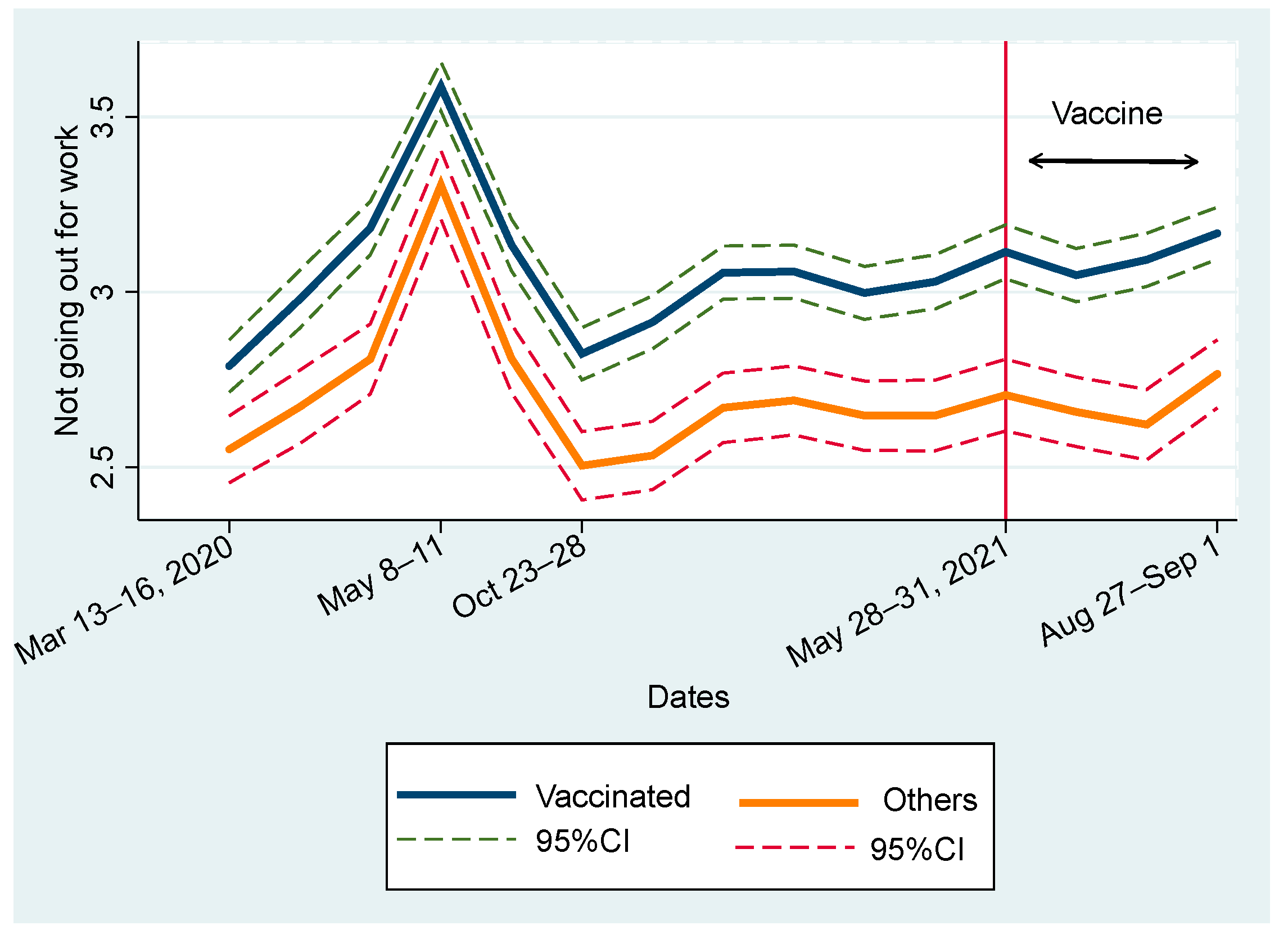
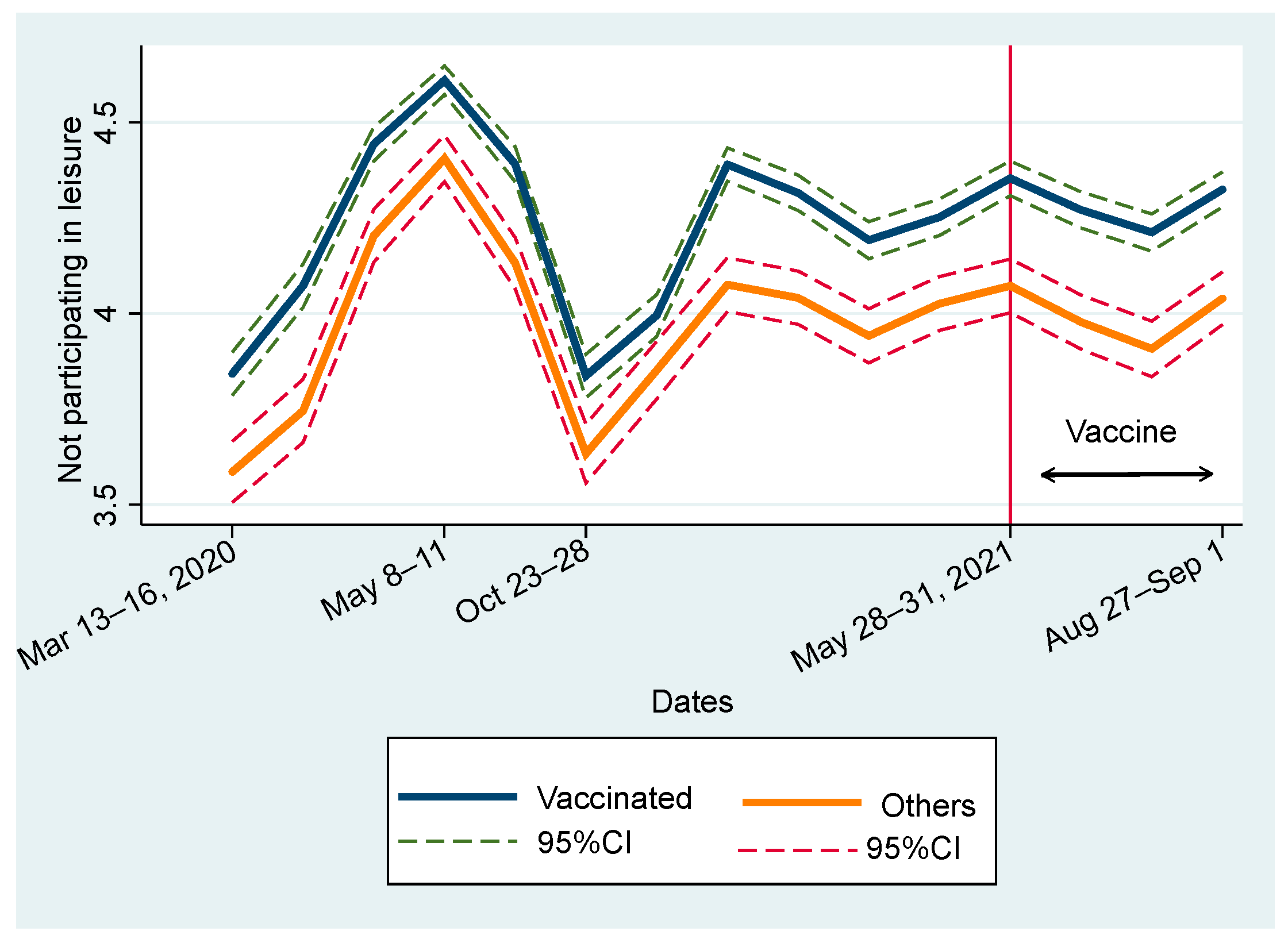
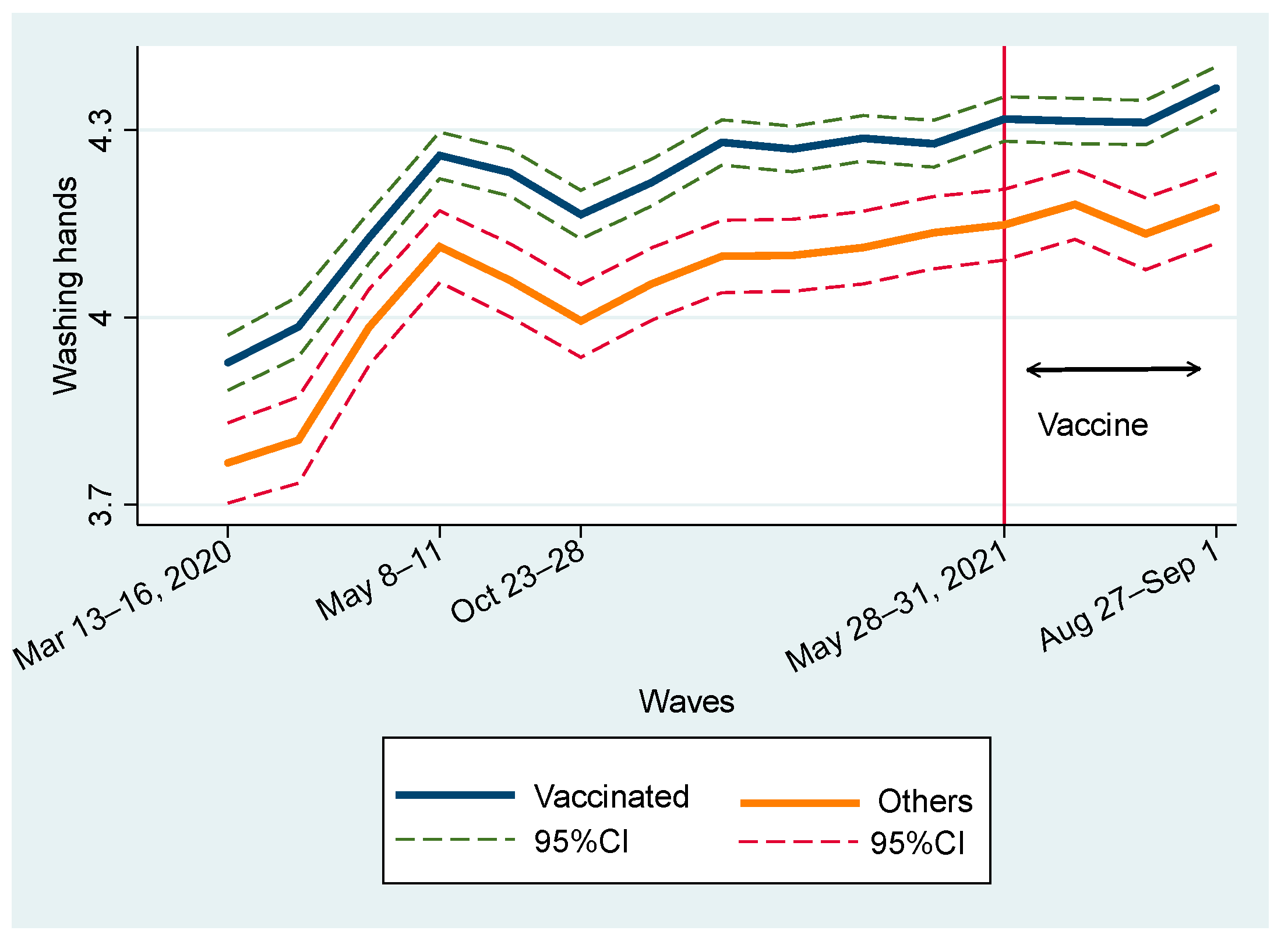
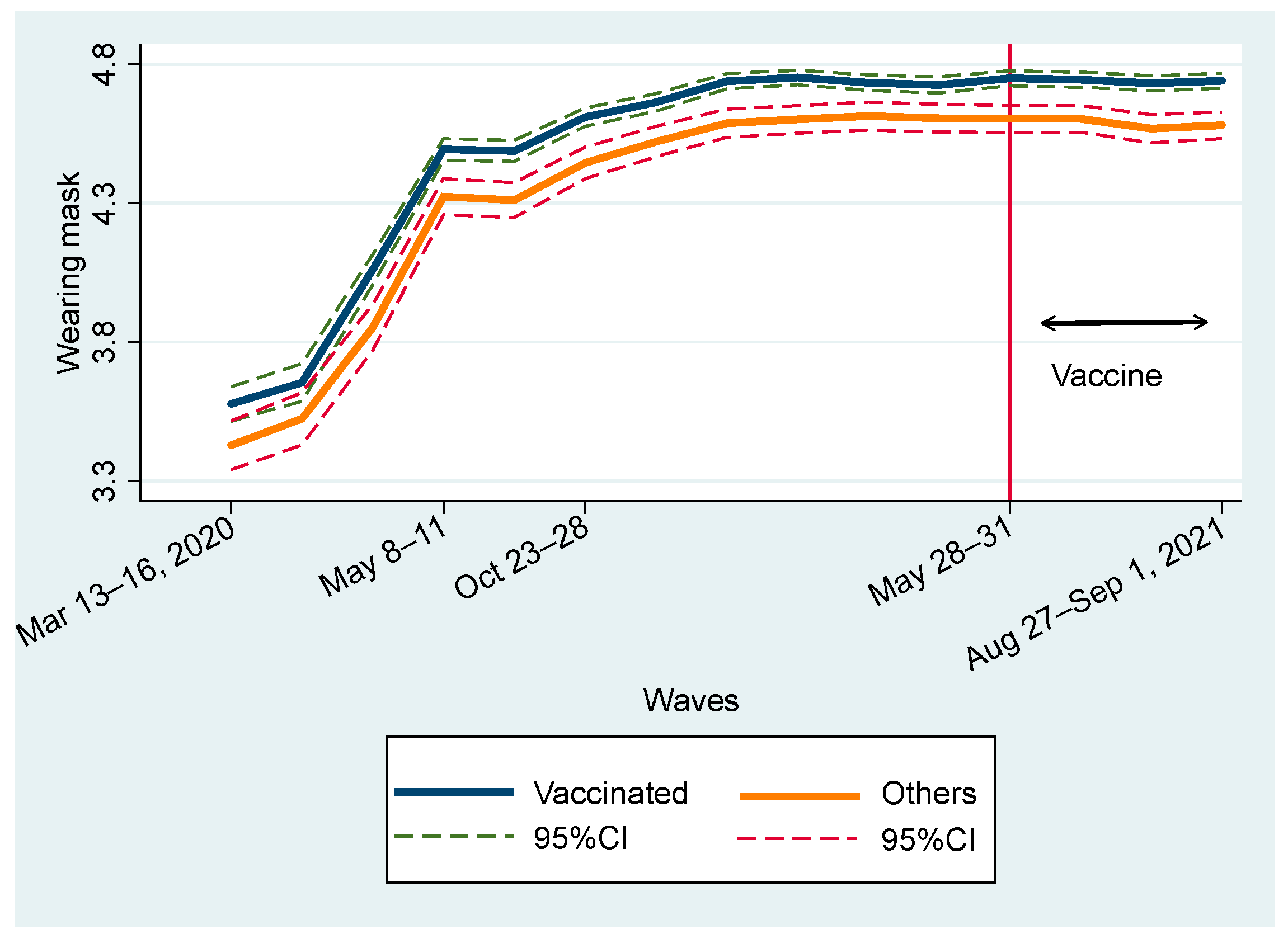
Figure 3(a).
Change in staying indoors.
Figure 3(b).
Change in not going out for work.
Figure 3(c).
Change in not participating in leisure activities outside home.
Figure 3(d).
Change in handwashing.
Figure 3(e).
Change in wearing mask.
Figure 3 (a) indicates that the vaccinated group was more likely to stay at home than the unvaccinated group throughout the study period. The trends of both groups were similar. At the first declaration of the state of emergency in all parts of Japan from the third to fourth waves, people immediately complied and stayed at home. After calling the first declaration, the level of staying at home declined to the level before the declaration. Later, the state of emergency was declared and consecutively called off four times. In response to this, the level of staying at home increased but did not peak during the first declaration. This level was more stable in 2021 than in 2020. However, we should note that the gap in the behavior increased, especially after the eighth wave, and after entering 2021. Similar tendencies were observed for Figure 3 (b) and (c) for “not going out for work” and “not participating in leisure activities outside home.”
As shown in Figure 3(d) and (e), in terms of changes in handwashing and wearing masks, similar to Figure 3 (a)–(c), the vaccinated group showed consistently higher levels of adherence than the unvaccinated group. However, the gap in handwashing was larger than that in wearing masks. Mask-wearing behavior is motivated by self-regarding risk preferences and other-regarding concerns [34,39,40,41,42]. In other words, the effect of interpersonal interaction possibly reduces the gap in wearing masks.
Compared to Figure 3(a)–(c), a remarkable difference exists in the trends shown in Figure 3(d) and (e). The level of handwashing and wearing masks almost constantly rose, indicating that people became more inclined to wash hands and wear a mask even after declaration of a state of emergency. This is consistent with the fact that many people began habitually washing their hands in response to the 2009 influenza pandemic, and their habits have persisted over the years [43].
Overall, we did not observe the effect of vaccination by comparing the time periods before and after the distribution of the COVID-19 vaccine (Figure 3). Figure 3 presents a change in mean values; thus, various factors that influence preventive behaviors are not controlled. We then examined the fixed effects regression model to closely examine the relation between vaccination and preventive behaviors. Before scrutinizing the difference in effects between the first and second vaccinations, Table 5 shows the simple mean difference test before and after vaccination. We limited the sample to those who had been vaccinated during the study period. Further, we divided the sample into subsamples before the first vaccination and subsample after it. For a rough comparison, we did not distinguish between the first and second vaccinations. Table 3 shows that all types of preventive behaviors show larger values after vaccination than before vaccination. Further, these differences were statistically significant at the 1 % level. We carefully considered the difference between before and after vaccination (DIF) for the following: STAYING INDOORS (DIF 0.14 [95% CI: 0.10-0.18]), NOT GOING TO WORK (DIF 0.19 [95% CI: 0.13-0.24]), NOT FOR LEISURE (DIF 0.10 [95% CI: 0.07-0.14]), HANDWASHING (DIF 0.16 [95% CI: 0.13-0.19]), and WEARING MASK (DIF 0.29 [95% CI: 0.26-0.32]). This implies that people are more likely to engage in preventive behaviors after than before vaccination.
3.1. Full Sample Estimations
The coefficient of confounders indicates marginal effects (ME). Table 6 presents the estimation results of the FE model using the entire sample. We begin by examining key variables of vaccination dummies. Except for Column (5), where the WEARING MASK is the dependent variable, the coefficients of the vaccination dummies show a positive sign in most cases. VACCINE FIRST is statistically significant only in columns (1) and (4), and its statistical significance is not at the 1% level. Furthermore, VACCINE SECOND_1 and VACCINE SECOND_2 are statistically significant at the 1% level in most cases in Columns (1)–(3); in contrast, VACCINE SECOND_3 and VACCINE SECOND_4 are not significant in any column. Furthermore, the effects of VACCINE SECOND_1 are (ME 0.099 [95% CI: 0.058-0.140]), (ME 0.070 [95% CI: 0.007-0.132]), (ME 0.077 [95% CI: 0.031-0.122]), in columns (1), (2), and (3), respectively. Thus, compared with the unvaccinated people, vaccinated people are more likely to stay at home by 0.099 points, not to go to work by 0.070 points, and not going out for leisure by 0.077 points on a 5-point scale. This indicates that the degree of staying home increased by 1.98%, not going to work by 1.40 %, and not going out for leisure by 1.54% directly after the second shot than before vaccination. Turning to VACCINE SECOND_2, its effects increased (ME 0.123 [95% CI: 0.061-0.187]), (ME 0.123 [95% CI: 0.042-0.204]), (ME 0.106 [95% CI: 0.047-0.165]), in Columns (1), (2), and (3), respectively. Through conversion, this indicates that the degree of staying home and not going to work increased by 2.46%, and not going out for leisure by 2.12 % two months after the second shot than before vaccination.
Overall, these imply that people who have completed their second shot choose to stay at home and not go out for work, school, or leisure. This tendency was observed in the month when they received the second shot and the next month. Particularly, the effect was larger in the following months. However, this effect was resolved.
Before estimation, we hypothesize that getting vaccinated might encourage people to go out more as COVID-19 is less likely to have a detrimental effect on vaccinated people. Our findings contradict this result. After vaccination, some side effects are normal and expected, including pain, swelling, and redness at the injection site, chills, mild fever, tiredness, headaches, joint pain, or muscle ache [44]. This may reduce the incentive to go out. However, side effects are resolved within a few days. Hence, side effects may affect one’s ability to perform daily activities for a few days [44]. However, experiencing side effects does not explain the increase in staying at home in the following months.
In our interpretation, social norms for promoting preventive behaviors were formed through the experience of COVID-19. According to an expert, “After being vaccinated, it’s important you continue the behaviours that protect yourself and others against COVID-19… This is because COVID-19 vaccines have proven effective at stopping people from developing the virus, but we don’t yet know whether they prevent people from passing the infection onto others.” [44] This instruction is considered a “nudge’ to influence human behavior [45,46,47]. Social media exposure to COVID-19 information influences the adoption of preventive attitudes and behaviors by shaping risk perception [48]. Arguably, this kind of instruction after vaccination contributes to forming social norms through the media.
People would usually perceive having done something wrong when they go against social norms. Alternatively, vaccinated people will likely be punished if they break the norm. Especially at the early stage of vaccine distribution, vaccine supply was low, so only health care workers and adults could receive shots. Furthermore, making reservations for vaccination is quite challenging. Hence, the number if highly advantaged vaccinated individuals is very small. They would be seriously criticized if they break the norm. If vaccinated people derive the inference, they refrain from going out.
Hence, the norms become more effective for vaccinated people as they are less likely to obey them. The gap in preventive behaviors between vaccinated and unvaccinated individuals returned to pre-vaccination levels, but did not decrease, despite two or three months having passed. On handwashing and wearing masks, the dummies for vaccination did not show any significant negative sign. Therefore, vaccination did not hamper people’s adherence to preventive behaviors.
The model specification shows that subjective perception about COVID-19 is controlled by PROB COVID19 and SEVERITY COVID19. Particularly, the coefficient of SEVERITY COVID19 exhibits a positive sign and is statistically significant at the 1% level in all estimations. This is consistent with the inference that people are more likely to exhibit preventive behaviors if they consider the damage done by COVID-19 to be larger.
In most cases, wave dummies presented a positive sign and statistical significance at the 1% level, except WAVE 6. This suggests that people are more likely to display preventive behaviors than in the first wave when COVID-19 arrived in Japan and did not spread significantly. At the sixth wave (Figure 3), the level of preventive behaviors temporarily returned to the levels observed during in the early stages of the first wave when the first declaration of a state of emergency had been terminated. A significantly positive sign of EMERGENCY is observed in Columns (2) and (3), which is reasonable because people were strongly urged not to go out.
Table 7 presents different specifications where the second shot dummy is used to examine the effect of the second shot instead of using four dummies to capture the timing of the second shot. Table 7 only focuses on whether respondents received their second shot. We report the key variables, although the set of control variables is the same as that in Table 6, and the results are similar to that of Table 6. Columns (1)–(3) show significant positive sign for VACCINE SECOND, but columns (4) and (5) do not. Its absolute values of coefficient and statistical significance are larger for VACCINE SECOND than VACCINE FIRST.
Table 8 shows the results of the FE ordered logit model. To interpret the results correctly, one needs to consider the marginal effects in the probability that respondents select a particular option [29,30]. For instance, they choose “1” for question about degree of “staying indoors” if respondents have not completed staying indoors at all. We can calculate how the first vaccination is correlated with this probability. The marginal effect of VACCINE_SECOND for (Prob [y=1]) is −0.036, and statistically significant at the 1 % level. This implies that the second vaccination reduced 3.6% of the probability that they had not completed staying indoors at all. Similarly, they choose “5” for question on the degree of “staying indoors” if respondents have completely achieved staying indoors. Column (1) of Table 8 shows that VACCINE_SECOND for (Prob [y=5]) is 0.021, and statistically significant at the 1 % level. This implies that the second vaccination increased 2.1% of the probability that they had completely achieved by staying indoors. The probability of choosing 2, 3, and 4 are also presented. Overall, VACCINE_SECOND shows statistical significance at the 1 % level, with the exception of Column (4). Further, the sign of VACCINE_SECOND is positive for Prob [y=5] and negative for Prob [y=1, 2]. Concerning (Prob [y=3, 4]), its sign varies according to the columns. In contrast, VACCINE_FIRST shows similar results in columns (1), (4), and (5). However, it is not statistically significant at the 1 % level, and the absolute values of the marginal effect are smaller than those of VACCINE_SECOND. Overall, the implications from the results of Table 8 are almost the same as those of Table 7. The results of the simple FE model can be more convenient and more intuitively interpreted than the FE ordered logit model. Therefore, a simple FE model was used for the estimation in Table 9 and Table 10.
3.2. Subsample Estimations (Young vs Old Ages Groups)
A previous study of preventive behaviors in Japan divided the sample into < 40 years and ≥ 40 years and found a difference between samples [49]. Following the study, Table 5 and Table 6 report the results based on subsamples below 40 and subsamples equal to or over 40. Here, we focus on the key variables, although the same set of control variables is included.
Contrary to the results in Table 6, Table 9 indicates the negative sign of vaccination dummies for staying indoors and not going out for work. Particularly, all dummies for the second shot are statistically significant for the estimations of not going out for work. Furthermore, the absolute values of the coefficients for VACCINE SECOND_1, VACCINE SECOND_2, VACCINE SECOND_3, and VACCINE SECOND_4 were 0.249, 0.392, 0.347, and 0.615, respectively, suggesting that the vaccinated people are more likely to go to work or school than the unvaccinated ones as time passes. Moreover, these values are remarkably larger than those for staying indoors. Meanwhile, considering the results for not participating in leisure activities outside home as a dependent variable, we did not observe statistical significance in the vaccination dummies.
4. Discussion
Using independently collected panel data, we found that vaccinated individuals are more likely to stay at home, frequently wash their hands, and wear masks than unvaccinated individuals, consistently from the early stages of COVID-19 to after vaccine distribution. The results obtained by analyzing the FE model indicate that the gap between vaccinated and unvaccinated individuals in terms of “staying at home” increased. In the context of “handwashing” or “wearing a mask,” the gap did not reduce.
Considering the results using both subsamples, vaccinated people in the young group are more motivated to go to work or school than those who are not vaccinated; however, they do not have a stronger motivation to go out for leisure. We found that they received the shot in the workplace or school and were encouraged or required to go out for work or education. The incentive that young people have is not common for aged groups because they consist mainly of retired older people. The sample size and observations of vaccinated people in the old group were far larger than those for the young group. Hence, the influence of vaccination dummies for the old group outweighs that of the young group (Table 6).
In a previous related study conducted in the UK, individuals’ COVID-19 preventive behaviors did not decrease after vaccination [50,51]. These findings are consistent with those of the present study. This indicates that preventive behaviors against COVID-19 are motivated by self-interest and other related concerns. This is in line with the expectation that the COVID-19 vaccine protects vaccinated individuals and society by reducing disease transmission. Moreover, vaccinated individuals exhibit less generosity toward unvaccinated individuals [52].
Public health messages from governments/scientists are considered to encourage vaccinated people to continue to engage in preventive behaviors. In other words, information was diffused through various media calling for a cautious attitude, which possibly formed social norms to engage in preventive behaviors. People display preventive behaviors that depend on caring and fairness concerns [53]. Vaccinated people will be criticized by members of society if they do not engage in preventive behaviors. This increased the incentive of vaccinated individuals to engage in preventive behaviors.
A closer examination found that young individuals aged ≥ 40 years tended to go out to work post vaccination. They are likely to be vaccinated at their workplace so they can work safely. They need to go to work as working from home is yet to be firmly established in Japan, and they are also less likely to hold a management position, which makes working from home possible. Inevitably, vaccinated young workers seem reluctant to obey the norms. However, apart from going out to work, they continued displaying other preventive behaviors, such as refraining from participating in leisure activities outside home, frequently washing their hands, and wearing masks.
4.1. Strength
Many researches investigated preventive behaviors against COVID-19. However, most of studies are based on cross-section data, rather than the panel data [54,55]. Hence, these studies suffered omitted variables biases and did not explore causality between dependent variables and preventive behaviors. According to Liang et al [56], even after vaccination, preventive behaviors against COVID-19 is important because there is no guarantee of full protection from COVID-19 [54,57]. However, it is not unknown whether preventive behaviors depend on completing vaccination [54,55,56,58]. Contribution of this study is to explore correlation between vaccination and preventive behaviors by comparing before and after the vaccination using the individual level panel data.
Overall, our key findings are consistent with the argument that “individuals act upon the social contract. The stronger they perceive it as a moral obligation, the more they act upon it. Emphasizing the social contract could help increase vaccine uptake, prevent free riding, and eventually support elimination of infectious diseases.” [52]
Our findings provide the following policy recommendations.: First, the government and scientists should send messages to strengthen social norms to maintain caution against COVID-19 before herd immunity is realized. Meanwhile, rapidly increasing the rate of vaccinations within 2 months after commencement of vaccination diffusion is critical for developing herd immunity as vaccinated people become less likely to stay at home after 3 months have passed. The sample used in this study is representative of the Japanese population. Therefore, the conclusions can be extrapolated to Japan as a whole.
4.2. Limitation
Selection bias may have occurred because those who pay more attention to COVID-19 are more likely to participate in the surveys. People may be motivated to follow socially desired responses when answering questions, resulting in biases. Despite using panel data, causality between vaccination and preventive behaviors has not been scrutinized. In order to examine the causality, experimental study to control endogenous biases should be called for. Further, careful attention should be given to the fact that those without internet access were underrepresented. This is a limitation of the present study.
Author Contributions
EY and FO participated in the conceptualisation of the study and analysed the patient data. YK organized the panel data for statistical estimation. YT designed the panel survey and performed data collection. EY wrote the main text and made the tables for the original manuscript. All authors reviewed, edited, and approved the final manuscript. The authors are responsible for any errors in this study.
Funding
This study was supported by the Fostering Joint International Research B (Grant No. 18KK0048) and the Grant-in-Aid for Scientific Research S (Grant No. 20H05632) from the Japan Society for the Promotion of Science to Yoshiro Tsutsui and Fumio Ohtake, respectively.
Availability of data and materials:
The datasets used and analysed in this study are available from the corresponding author upon reasonable request.
Declarations
Ethics Approval and Consent to Participate:
This study was conducted with the ex-ante approval of the Ethics Committee of the Graduate School of Economics, Osaka University, and all methods were carried out in accordance with the relevant guidelines and regulations. The ethics approval number of Osaka University for this study is R021014. Informed consent for study participation was obtained from all subjects.
Consent for publication:
Not applicable.
Conflicts of Interest:
The authors declare that they have no competing interests.
References
- Born, B.; Dietrich, A.M.; Müller, G.J. The Lockdown Effect: A Counterfactual for Sweden. PLoS One 2021, 16. [Google Scholar] [CrossRef] [PubMed]
- Tian, H.; Liu, Y.; Li, Y.; Wu, C.-H.; Chen, B. Kraemer MUG An Investigation of Transmission Control Measures during the First 50 Days of the COVID-19 Epidemic in China. Science (1979) 2020, 368, 638–642. [Google Scholar] [CrossRef] [PubMed]
- Imperial College COVID-19 Response Team; Flaxman S; Mishra S; Gandy A; Unwin HJT; Mellan TA Estimating the Effects of Non-Pharmaceutical Interventions on COVID-19 in Europe. Nature 2020, 584, 257–261.
- Hyafil A; Moriña D Analysis of the Impact of Lockdown on the Reproduction Number of the SARS-Cov-2 in Spain. Gac Sanit 2020, S0213911120300984.
- Alfano V; Ercolano S The Efficacy of Lockdown Against COVID-19: A Cross-Country Panel Analysis. Appl Health Econ Health Policy 2020, 18, 509–517. [CrossRef]
- Ambikapathy, B.; Krishnamurthy, K. Mathematical Modelling to Assess the Impact of Lockdown on COVID-19 Transmission in India: Model Development and Validation. JMIR Public Health Surveill 2020, 6, e19368. [Google Scholar] [CrossRef] [PubMed]
- Mottaleb, K.A.; Mainuddin, M.; Sonobe, T. COVID-19 Induced Economic Loss and Ensuring Food Security for Vulnerable Groups: Policy Implications from Bangladesh. PLoS One 2020, 15. [Google Scholar] [CrossRef]
- Inoue, H.; Murase, Y.; Todo, Y. Do Economic Effects of the Anti-COVID-19 Lockdowns in Different Regions Interact through Supply Chains? PLoS One 2021, 16. [Google Scholar] [CrossRef] [PubMed]
- Chinna, K.; Sundarasen, S.; Khoshaim, H.B.; Kamaludin, K.; Nurunnabi, M.; Baloch, G.M.; Hossain, S.F.A.; Sukayt, A.; Dalina, N.; Rajagopalan, U.; et al. Psychological Impact of COVID-19 and Lock down Measures: An Online Cross-Sectional Multicounty Study on Asian University Students. PLoS One 2021, 16. [Google Scholar] [CrossRef]
- Fiorenzato, E.; Zabberoni, S.; Costa, A.; Cona, G. Cognitive and Mental Health Changes and Their Vulnerability Factors Related to COVID-19 Lockdown in Italy. PLoS One 2021, 16. [Google Scholar] [CrossRef]
- Greyling, T.; Rossouw, S.; Adhikari, T. The Good, the Bad and the Ugly of Lockdowns during Covid-19. PLoS One 2021, 16. [Google Scholar] [CrossRef] [PubMed]
- Ogden, R. Distortions to the Passage of Time during England’s Second National Lockdown: A Role for Depression. PLoS One 2021, 16. [Google Scholar] [CrossRef]
- Yamamura, E.; Tsutsui, Y. Impact of the State of Emergency Declaration for Covid-19 on Preventive Behaviours and Mental Conditions in Japan: Difference in Difference Analysis Using Panel Data. Covid Economics Vetted and Real-Time Papers 2020, 23, 303–324. [Google Scholar]
- WHO Coronavirus (COVID-19) Dashboard WHO Coronavirus Disease (COVID-19) Dashboard.
- Perez-Arce, F.; Angrisani, M.; Bennett, D.; Darling, J.; Kapteyn, A.; Thomas, K. COVID-19 Vaccines and Mental Distress. PLoS One 2021, 16, e0256406. [Google Scholar] [CrossRef]
- Pandey, K.; Thurman, M.; Johnson, S.D.; Acharya, A.; Johnston, M.; Klug, E.A.; Olwenyi, O.A.; Rajaiah, R.; Byrareddy, S.N. Mental Health Issues During and After COVID-19 Vaccine Era. Brain Res Bull 2021, 176, 161–173. [Google Scholar] [CrossRef] [PubMed]
- Yuan, Y.; Deng, Z.; Chen, M.; Yin, D.; Zheng, J.; Liu, Y.; Liu, X.; Zou, H.; Zhang, C.; Sun, C. Changes in Mental Health and Preventive Behaviors before and after COVID-19 Vaccination: A Propensity Score Matching (PSM) Study. Vaccines (Basel) 2021, 9. [Google Scholar] [CrossRef]
- Japan Times Japan Gives First COVID-19 Vaccines to Health Workers. Japan Times 2021.
- Mantzari, E.; Rubin, G.J.; Marteau, T.M. Is Risk Compensation Threatening Public Health in the Covid19 Pandemic? BMJ 2020, 370, m2913. [Google Scholar] [CrossRef] [PubMed]
- Ioannidis, J.P.A. Benefit of COVID-19 Vaccination Accounting for Potential Risk Compensation. NPJ Vaccines 2021, 6. [Google Scholar] [CrossRef]
- Trogen, B.; Caplan, A. Risk Compensation and COVID-19 Vaccines. Ann Intern Med 2021, 174, 858–859. [Google Scholar] [CrossRef]
- Rubin, G.J.; Brainard, J.; Hunter, P.; Michie, S. Are People Letting down Their Guard Too Soon after Covid-19 Vaccination? BMJ Opinion 2021. [Google Scholar]
- Morikawa, M. COVID-19, Vaccination, and Consumper Behavior; RIETI; 2021.
- Sunohara, S.; Asakura, T.; Kimura, T.; Ozawa, S.; Oshima, S.; Yamauchi, D.; Tamakoshi, A. Effective Vaccine Allocation Strategies, Balancing Economy with Infection Control against COVID-19 in Japan. PLoS One 2021, 16, e0257107. [Google Scholar] [CrossRef]
- Wooldridge, J. Introductory Econometrics; 4th ed.; South-Western Cengage Learning, 2009.
- Hsiao, C. Aalysis of Panel Data; Cambridge University Press: New York, 1986. [Google Scholar]
- Baltagi, B. Econometric Analysis of Panel Data; John Wiley & Sons: New York, 1995. [Google Scholar]
- Nagasu, M.; Yamamoto, I. Impact of Socioeconomic- And Lifestyle-Related Risk Factors on Poor Mental Health Conditions: A Nationwide Longitudinal 5-Wave Panel Study in Japan. PLoS One 2020, 15. [Google Scholar] [CrossRef]
- Wooldridge, J. Econometric Analysis of Cross Section and Panel Data; MIT Press: Cambridge, 2002. [Google Scholar]
- Greene, W. Econometric Analysis, 6th ed.; Pearson, Preantice Hall: New York, 2008. [Google Scholar]
- Yamamura, E.; Tsutsui, Y. The Impact of Closing Schools on Working from Home during the COVID-19 Pandemic: Evidence Using Panel Data from Japan. Rev Econ Househ 2021, 19, 41–60. [Google Scholar] [CrossRef] [PubMed]
- Rosenstock, I. The Health Belief Model and Preventive Behavior. Health Education & Behavior 1974, 2, 27–59. [Google Scholar]
- Rosenstock, I.; Strecher, V.; Becker, M. Social Learning Theory and the Health Belief Model. Health Education & Behavior 1988, 15, 175–183. [Google Scholar] [CrossRef]
- Asri, A.; Asri, V.; Renerte, B.; Föllmi-Heusi, F.; Leuppi, J.D.; Muser, J.; Nüesch, R.; Schuler, D.; Fischbacher, U. Wearing a Mask-For Yourself or for Others? Behavioral Correlates of Mask Wearing among COVID-19 Frontline Workers. PLoS One 2021, 16. [Google Scholar] [CrossRef] [PubMed]
- Travis, J.; Harris, S.; Fadel, T.; Webb, G. Identifying the Determinants of COVID-19 Preventative Behaviors and Vaccine Intentions among South Carolina Residents. PLoS One 2021, 16, e0256178. [Google Scholar] [CrossRef]
- Japan Times 75% of Japan’s Older Residents Have Received First COVID-19 Vaccine Shot. Japan Times 2021.
- Japan Times Japan to Start COVID-19 Vaccinations at Workplaces and Universities on June 21. Japan Times 2021.
- Department of Medical Genome Sciences, R.I. for F.M.S.M.U.S. of M.JAPAN. Transition of COVID-19 Vaccination Rates by Country.
- Rose, G. The Determinants of Individual Cases Sick Individuals and Sick Populations; 2001; Vol. 30.
- Cheng, K.K.; Lam, T.H.; Leung, C.C. Wearing Face Masks in the Community during the COVID-19 Pandemic: Altruism and Solidarity. The Lancet 2020. [CrossRef] [PubMed]
- Powdthavee, N.; Riyanto, Y.E.; Wong, E.C.L.; Yeo, J.X.W.; Chan, Q.Y. When Face Masks Signal Social Identity: Explaining the Deep Face-Mask Divide during the COVID-19 Pandemic. PLoS One 2021, 16. [Google Scholar] [CrossRef] [PubMed]
- Weisel, O. Vaccinationasasocialcontract:ThecaseofCOVID-19 and US Political Partisanship. Proc Natl Acad Sci U S A 2021, 118. [Google Scholar]
- Agüero, J.; Beleche, T. Health Shocks and Their Long-Lasting Impact on Health Behaviors: Evidence from the 2009 H1N1 Pandemic in Mexico. J Health Econ 2017, 54, 45–55. [Google Scholar] [CrossRef] [PubMed]
- Health Experts of UNICEF What to Do before, during and after Getting Vaccinated for COVID-19.
- Allcott, H. Social Norms and Energy Conservation. J Public Econ 2011, 95, 1082–1095. https://doi.org/0/?tab=wm&ogbl#inbox.
- Allcott, H.; Knittel, C. Are Consumers Poorly Informed about Fuel Economy? Evidence from Two Experiments. Am Econ J Econ Policy 2019, 11, 1–37. [Google Scholar] [CrossRef]
- Sasaki, S.; Kurokawa, H.; Ohtake, F. Effective but Fragile? Responses to Repeated Nudge-Based Messages for Preventing the Spread of COVID-19 Infection. Japanese Economic Review 2021, 72, 371–408. [Google Scholar] [CrossRef] [PubMed]
- Zeballos Rivas, D.R.; Lopez Jaldin, M.L.; Nina Canaviri, B.; Portugal Escalante, L.F.; Alanes Fernández, A.M.C.; Aguilar Ticona, J.P. Social Media Exposure, Risk Perception, Preventive Behaviors and Attitudes during the COVID-19 Epidemic in La Paz, Bolivia: A Cross Sectional Study. PLoS One 2021, 16, e0245859. [Google Scholar] [CrossRef] [PubMed]
- Muto, K.; Yamamoto, I.; Nagasu, M.; Tanaka, M.; Wada, K. Japanese Citizens’ Behavioral Changes and Preparedness against COVID-19: An Online Survey during the Early Phase of the Pandemic. PLoS One 2020, 15. [Google Scholar] [CrossRef] [PubMed]
- Desrichard, O.; Desrichard@unige, O.; Moussaoui, L.; Ofosu, N. Do Vaccinated People Reduce Their Precautionary Behaviours? A Test on a British Cohort. 2021. [Google Scholar] [CrossRef]
- Wright, L.; Steptoe, A.; Mak, H.W.; Fancourt, D. Do People Reduce Compliance with COVID-19 Guidelines Following Vaccination? A Longitudinal Analysis of Matched UK Adults. Journal of Epidemiology & Community Health (Forthcoming), 2021. [Google Scholar] [CrossRef]
- Korn, L.; Böhm, R.; Meier, N.W.; Betsch, C. Vaccination as a Social Contract. PNAS 2020, 117, 14890–14899. [Google Scholar] [CrossRef]
- Chan, Y. Eugene Moral Foundations Underlying Behavioural Compliance during the COVID-19 Pandemic. Pers Individ Dif 2021, 171. [Google Scholar] [CrossRef] [PubMed]
- Duan, Y.; Lippke, S.; Liang, W.; Shang, B.; Keller, F.M.; Wagner, P.; Baker, J.S.; He, J. Association of Social-Cognitive Factors with Individual Preventive Behaviors of COVID-19 among a Mixed-Sample of Older Adults from China and Germany. Int J Environ Res Public Health 2022, 19. [Google Scholar] [CrossRef]
- Li, F.; Liang, W.; Rhodes, R.E.; Duan, Y.; Wang, X.; Shang, B.; Yang, Y.; Jiao, J.; Yang, M.; Supriya, R.; et al. A Systematic Review and Meta-Analysis on the Preventive Behaviors in Response to the COVID-19 Pandemic among Children and Adolescents. BMC Public Health 2022, 22. [Google Scholar] [CrossRef] [PubMed]
- Liang, W.; Duan, Y.; Li, F.; Rhodes, R.E.; Wang, X.; Peiris, D.L.I.H.K.; Zhou, L.; Shang, B.; Yang, Y.; Baker, J.S.; et al. Psychosocial Determinants of Hand Hygiene, Facemask Wearing, and Physical Distancing during the COVID-19 Pandemic: A Systematic Review and Meta-Analysis. Annals of Behavioral Medicine 2022, 56, 1174–1187. [Google Scholar] [CrossRef] [PubMed]
- Lopez Bernal, J.; Andrews, N.; Gower, C.; Gallagher, E.; Simmons, R.; Thelwall, S.; Stowe, J.; Tessier, E.; Groves, N.; Dabrera, G.; et al. Effectiveness of Covid-19 Vaccines against the B.1.617.2 (Delta) Variant. New England Journal of Medicine 2021, 385, 585–594. [Google Scholar] [CrossRef]
- Duan, Y.; Shang, B.; Liang, W.; Lin, Z.; Hu, C.; Baker, J.S.; Wang, Y.; He, J. Predicting Hand Washing, Mask Wearing and Social Distancing Behaviors among Older Adults during the Covid-19 Pandemic: An Integrated Social Cognition Model. BMC Geriatr 2022, 22. [Google Scholar] [CrossRef]
Figure 1.
Comparison of the age distribution of our survey sample with that of the 2015 Japan population census. Sources: Statistics Bureau, Ministry of Internal Affairs and Communications (2015). 2015 Japan Population Census. https://www.e-stat.go.jp/stat-search/files?page=1&layout=datalist&toukei=00200521&tstat=000001080615&cycle=0&tclass1=000001089055&tclass2=000001089056&result_page=1&second=1&second2=1 (accessed on February 18, 2018).
Figure 1.
Comparison of the age distribution of our survey sample with that of the 2015 Japan population census. Sources: Statistics Bureau, Ministry of Internal Affairs and Communications (2015). 2015 Japan Population Census. https://www.e-stat.go.jp/stat-search/files?page=1&layout=datalist&toukei=00200521&tstat=000001080615&cycle=0&tclass1=000001089055&tclass2=000001089056&result_page=1&second=1&second2=1 (accessed on February 18, 2018).
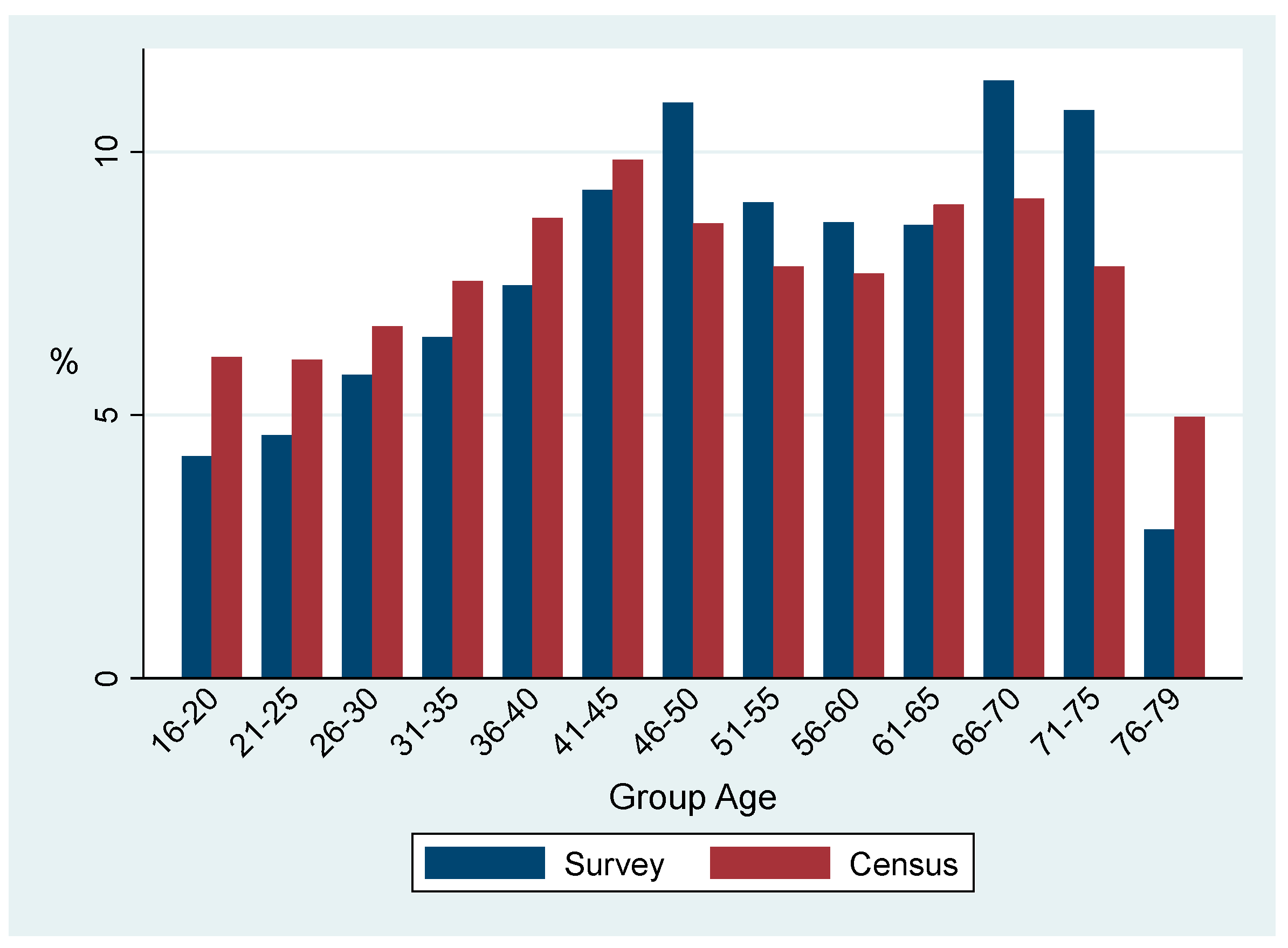
Figure 2.
Comparison of the geographical distribution of our survey sample with that of the 2015 Japan population census. Note: Darker shaded areas indicate more populated areas. Number in the map indicates the percentage of population in each residential prefecture. Sources: Statistics Bureau, Ministry of Internal Affairs and Communications (2015). 2015 Japan Population Census. https://www.stat.go.jp/data/nihon/02.html.
Figure 2.
Comparison of the geographical distribution of our survey sample with that of the 2015 Japan population census. Note: Darker shaded areas indicate more populated areas. Number in the map indicates the percentage of population in each residential prefecture. Sources: Statistics Bureau, Ministry of Internal Affairs and Communications (2015). 2015 Japan Population Census. https://www.stat.go.jp/data/nihon/02.html.
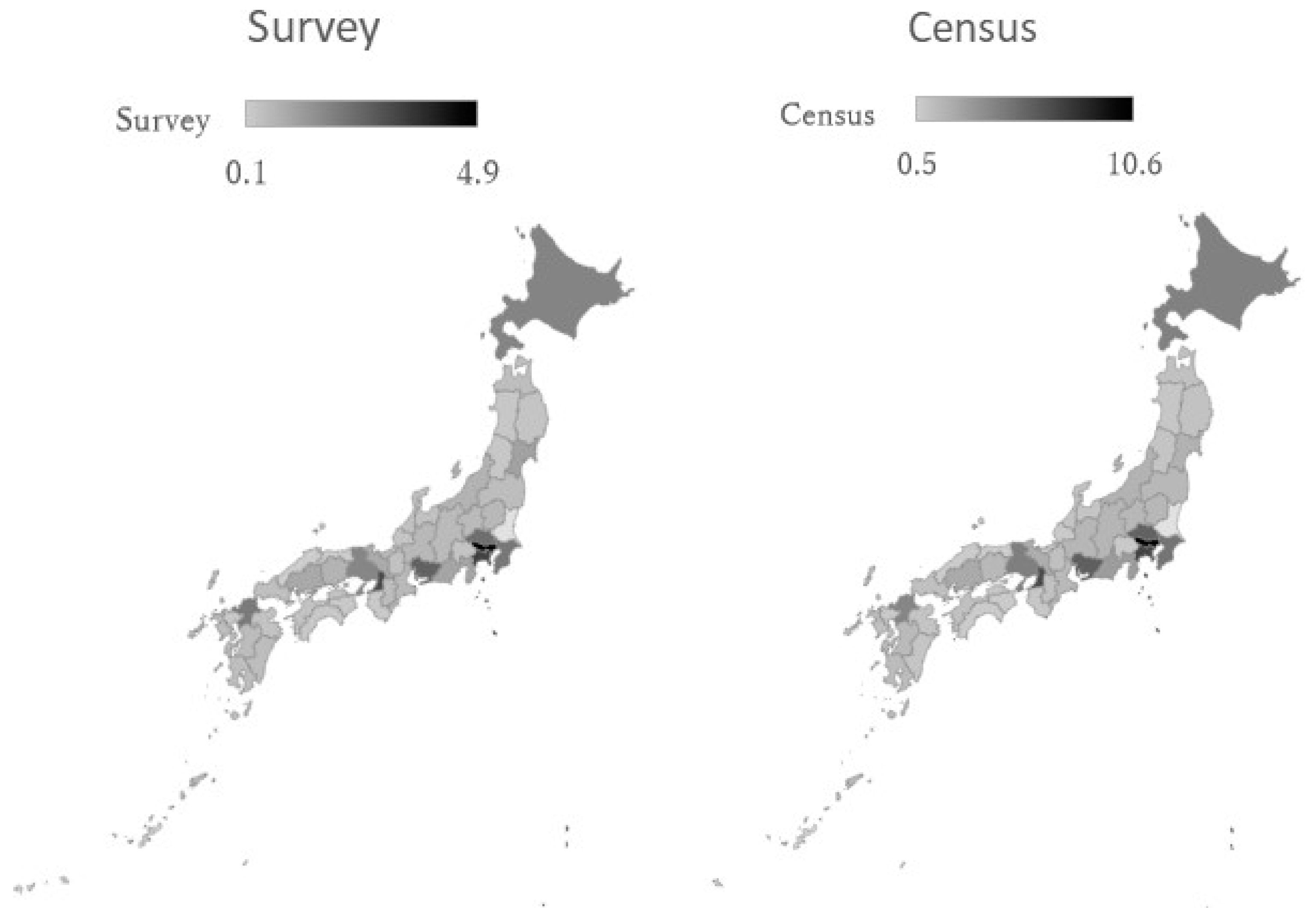

Table 1.
Definitions of key variables.
| Variables | Definition |
| Dependent variables | |
| STAYING INDOORS | In the last week, how consistent were you at “not going out of home?” Please choose among 5 choices. 1 (not completed at all) to 5 (completely consistent). |
| NOT GOING TO WORK | In the last week, how consistent were you at “not going out to work (or school)?” Please choose among 5 choices. 1 (not completed at all) to 5 (completely achieved). |
| NOT FOR LEISURE | In the last week, how consistent were you at “not going out to events or travel?” Please choose among 5 choices. 1 (not completed at all) to 5 (completely achieved). |
| HANDWASHING | In the last week, how consistent were you at “washing your hands?” Please choose among 5 choices. 1 (not completed at all) to 5 (completely achieved). |
| WEARING MASK | In the last week, how consistent were you at “wearing a mask?” Please choose among 5 choices. 1 (not completed at all) to 5 (completely achieved). |
| Confounders (Independent variables) | |
| VACCINE FIRST | Did you get the first shot (but not yet the second one)? 1 (Yes) or 0 (No) |
| VACCINE SECOND | Did you get the second shot? 1 (Yes) or 0 (No) |
| VACCINE SECOND_1 | Did you get the second shot in this month? 1 (Yes) or 0 (No) |
| VACCINE SECOND_2 | Did you get the second shot last month? 1 (Yes) or 0 (No) |
| VACCINE SECOND_3 | Did you get the second shot two months ago? 1 (Yes) or 0 (No) |
| VACCINE SECOND_4 | Did you get the second shot three months ago? 1 (Yes) or 0 (No) |
| PROB_COVID19 | What percentage do you think the probability of your taking the COVID-19? 0 to 100 (%) |
| SEVERITY COVID19 | How serious are your symptoms if you are infected with the novel coronavirus? Choose from 6 choices. 1 (very small influence) to 6 (death) |
| EMERGENCY | Is your area under a state of emergency. 1 (Yes) or 0 (No) |
| FEAR | How intense is your feeling of fear? Please answer in a scale from 1 (I have not felt this emotion at all) to 5 (I have felt this emotion strongly). |
| ANXIETY | How intense is your feeling of anxiety? Please answer in a scale from 1 (I have not felt this emotion at all) to 5 (I have felt this emotion strongly). |
| ANGER | How intense is your feeling of anger? Please answer in a scale from 1 (I have not felt this emotion at all) to 5 (I have felt this emotion strongly). |
| AGE | Ages |
| MALE | Select 1 if you are male and 0 if otherwise. |
| UNIVERSITY | Select 1 if you graduated from university and 0 if otherwise. |
Table 2.
Sample size (observations) and loss rates for each survey.
| Waves | Obs. | Loss rate % |
| 1 | 4,359 | 0 |
| 2 | 3,495 | 19.8 |
| 3 | 4,013 | 7.9 |
| 4 | 3,996 | 8.3 |
| 5 | 3,877 | 11.1 |
| 6 | 3,626 | 16.8 |
| 7 | 3,491 | 19.9 |
| 8 | 3,509 | 19.5 |
| 9 | 3,529 | 19.0 |
| 10 | 3,440 | 21.1 |
| 11 | 3,304 | 24.2 |
| 12 | 3,280 | 24.8 |
| 13 | 3,392 | 22.2 |
| 14 | 3,349 | 23.2 |
| 15 | 3,347 | 23.2 |
Table 3.
Definitions of key variables and their basic statistics.
| Variables | Mean | s.d. |
| STAYING INDOORS | 2.91 | 1.25 |
| NOT GOING TO WORK | 2.94 | 1.73 |
| NOT FOR LEISURE | 4.12 | 1.18 |
| HANDWASHING | 4.14 | 0.95 |
| WEARING MASK | 4.41 | 1.05 |
| VACCINE FIRST | 0.03 | 0.17 |
| VACCINE SECOND | 0.06 | 0.24 |
| VACCINE SECOND_1 | 0.03 | 0.18 |
| VACCINE SECOND_2 | 0.02 | 0.14 |
| VACCINE SECOND_3 | 0.01 | 0.08 |
| VACCINE SECOND_4 | 0.001 | 0.04 |
| PROB_COVID19 | 20.4 | 22.3 |
| SEVERITY COVID19 | 3.57 | 1.21 |
| EMERGENCY | 0.29 | 0.45 |
| FEAR | 3.06 | 1.14 |
| ANXIETY | 3.28 | 1.15 |
| ANGER | 2.98 | 1.10 |
| AGE | 48.7 | 17.3 |
| MALE | 0.50 | 0.50 |
| UNIVERSITY | 0.43 | 0.49 |
Table 4.
Percentage of those who took the COVID-19 vaccine.
| Waves | Dates | All % |
Age>40 % |
Age<=40 % |
| 1 | March 13–16, 2020 | 0 | 0 | 0 |
| 2 | March 27–30, 2020 | 0 | 0 | 0 |
| 3 | Apr. 10–13, 2020 | 0 | 0 | 0 |
| 4 | May 8–11, 2020 | 0 | 0 | 0 |
| 5 | June 12–15, 2020 | 0 | 0 | 0 |
| 6 | Oct 23–28, 2020 | 0 | 0 | 0 |
| 7 | Dec 4–8, 2020 | 0 | 0 | 0 |
| 8 | Jan. 15–19, 2021 | 0 | 0 | 0 |
| 9 | Feb. 17–22, 2021 | 0 | 0 | 0 |
| 10 | Mar. 24–29, 2021 | 0 | 0 | 0 |
| 11 | Apr. 23–26, 2021 | 0 | 0 | 0 |
| 12 | May 28–31, 2021 | 8.2 | 9.1 | 5.4 |
| 13 | June 25–30, 2021 | 25.1 | 30.7 | 7.8 |
| 14 | July 30–Aug 4, 2021 | 50.0 | 58.3 | 23.8. |
| 15 | Aug 27–Sep. 1, 2021 | 64.2 | 72.3 | 39.5 |
Note: We did not distinguish between respondents who took only the first shot and those who took the second shot.
Table 5.
Mean difference test before and after vaccination using a sample of respondents who were vaccinated during the studied period.
Table 5.
Mean difference test before and after vaccination using a sample of respondents who were vaccinated during the studied period.
| Dates | Before (1) |
After (2) |
Difference (2) – (1) |
|
STAYING INDOORS |
2.96 | 3.11 | 0.14*** (0.10-0.18) |
|
NOT GOING TO WORK |
3.03 | 3.22 | 0.19*** (0.13-0.24) |
|
NOT FOR LEISURE |
4.21 | 4.32 | 0.10*** (0.07-0.14) |
|
HANDWASHING |
4.19 | 4.36 | 0.16*** (0.13-0.19) |
|
WEARING MASK |
4.45 | 4.75 | 0.29*** (0.26-0.32) |
Note: Numbers within parentheses are 95% CI. ***p<0.01.
Table 6.
FE model. Dependent variables are preventive behaviors.
| (1) STAYING INDOORS |
(2) NOT GOING TO WORK |
(3) NOT FOR LEISURE |
(4) HANDWASHING |
(5) WEARING MASK |
|
| VACCINE FIRST | 0.057** (0.007-0.106) |
0.032 (−0.016-0.080) |
0.027 (−0.014-0.069) |
0.026* (−0.001-0.054) |
−0.001 (−0.047-0.045) |
| VACCINE SECOND_1 | 0.099*** (0.058-0.140) |
0.070** (0.007-0.132) |
0.077*** (0.031-0.122) |
0.006 (−0.029-0.041) |
−0.006 (−0.046-0.034) |
| VACCINE SECOND_2 | 0.123*** (0.061-0.187) |
0.123*** (0.042-0.204) |
0.106*** (0.047-0.165) |
−0.012 (−0.051-0.027) |
−0.0003 (−0.048-0.047) |
| VACCINE SECOND_3 | 0.097 (−0.023-0.217) | 0.092 (−0.020-0.206) |
0.018 (−0.097-0.133) |
0.035 (−0.023-0.095) |
−0.027 (−0.094-0.040) |
| VACCINE SECOND_4 | 0.014 (−0.335-0.365) |
−0.019 (−0.167-0.128) |
−0.106 (−0.341-0.128) |
−0.018 (−0.142-0.105) |
−0.040 (−0.177-0.095) |
| PROBABILITY COVID19 | −0.291 (−1.064-0.480) |
−0.532 (−1.657-0.591) |
0.103 (−0.328-0.535) |
0.428* (−0.079-0.936) |
−0.472 (−1.208-0.263) |
| SEVERITY COVID19 | 0.016*** (0.007-0.026) |
0.017* (−0.001-0.036) |
0.036*** (0.019-0.053) |
0.018*** (0.006-0.030) |
0.033*** (0.021-0.045) |
|
EMERGENCY |
0.022 (−0.008-0.054) |
0.034** (0.007-0.062) |
0.047*** (0.017-0.078) |
−0.001 (−0.016-0.014) |
0.013 (−0.002-0.020) |
|
ANGER |
0.035*** (0.025-0.046) |
0.023*** (0.007-0.039) |
0.054*** (0.038-0.069) |
0.018*** (0.009-0.027) |
0.009 (−0.002-0.020) |
|
FEAR |
0.051*** (0.035-0.066) |
0.031*** (0.009-0.053) |
0.045*** (0.024-0.067) |
0.018*** (0.007-0.028) |
0.036*** (0.021-0.052) |
|
ANXIETY |
0.037*** (0.023-0.051) |
0.021* (−0.001-0.044) |
0.049*** (0.034-0.063) |
0.026*** (0.015-0.036) |
0.029*** (0.012-0.047) |
| WAVE 1 | <Default> | ||||
|
WAVE 2 |
0.126*** (0.085-0.167) | 0.092*** (0.048-0.137) |
0.170*** (0.113-0.226) |
0.043** (0.009-0.077) |
0.047*** (0.016-0.079) |
|
WAVE 3 |
0.446*** (0.355-0.536) |
0.273*** (0.181-0.365) |
0.516*** (0.450-0.582) |
0.177*** (0.144-0.210) |
0.386*** (0.332-0.440) |
|
WAVE 4 |
0.829*** (0.738-0.920) | 0.687*** (0.592-0.782) |
0.698*** (0.622-0.773) |
0.329*** (0.286-0.373) |
0.833*** (0.755-0.915) |
|
WAVE 5 |
0.435*** (0.353-0.517) |
0.269*** (0.185-0.354) |
0.517*** (0.456-0.577) |
0.289*** (0.260-0.318) |
0.862*** (0.802-0.924) |
|
WAVE 6 |
0.052 (−0.014-0.119) |
−0.010 (−0.082-0.060) |
0.025 (−0.038-0.090) |
0.237*** (0.203-0.272) |
1.010 (0.942-1.079) |
|
WAVE 7 |
0.161*** (0.101-0.221) | 0.017 (−0.046-0.081) |
0.157*** (0.108-0.206) |
0.267*** (0.235-0.300) |
1.061*** (0.993-1.130) |
|
WAVE 8 |
0.389*** (0.307-0.470) |
0.141*** (0.061-0.220) |
0.458*** (0.391-0.525) |
0.317*** (0.278-0.356) |
1.122*** (1.040-1.204) |
|
WAVE 9 |
0.368*** (0.306-0.431) |
0.153*** (0.095-0.210) |
0.417*** (0.0357-0.477) |
0.319*** (0.274-0.365) |
1.146*** (1.068-1.224) |
|
WAVE 10 |
0.344*** (0.271-0.416) | 0.140*** (0.070-0.210) | 0.323*** (0.259-0.387) |
0.339*** (0.305-0.374) |
1.133*** (1.065-1.201) |
|
WAVE 11 |
0.304*** (0.239-0.369) |
0.132*** (0.071-0.192) |
0.373*** (0.309-0.436) |
0.336*** (0.300-0.372) |
1.126*** (1.053-1.198) |
|
WAVE 12 |
0.375*** (0.304-0.446) |
0.195*** (0.132-0.259) |
0.442*** (0.375-0509) |
0.363*** (0.322-0.405) |
1.139*** (1.064-1.213) |
|
WAVE 13 |
0.309*** (0.233-0.385) | 0.141*** (0.079-0.201) |
0.365*** (0.206-0.350) |
0.372*** (0.334-0.410) |
1.132*** (1.059-1.206) |
|
WAVE 14 |
0.282*** (0.207-0.357) |
0.156*** (0.078-0.232) | 0.278*** (0.206-0.350) |
0.355*** (0.315-0.395) |
1.111*** (1.036-1.185) |
|
WAVE 15 |
0.346*** (0.248-0.444) |
0.231*** (0.141-0.322) |
0.384*** (0.299-0.469) |
0.413*** (0.360-0.467) |
1.135*** (1.051-1.219) |
| Adj R2 Obs. |
0.37 54,007 |
0.65 54,007 |
0.37 54,007 |
0.62 54,007 |
0.49 54,007 |
Note: Numbers within parentheses are 95% CI. For convenience, the coefficient of probability COVID-19 is multiplied by 1000. The model includes the number of deaths and infected persons in residential prefectures in surveys and proxied for mental conditions such as fear, anxiety, and anger. However, these results have not been reported. These are included, although the results have not been reported. ***p<0.01. **p<0.05. *p<0.10.
Table 7.
FE model. Dependent variables are preventive behaviors.
| (1) STAYING INDOORS |
(2) NOT GOING TO WORK |
(3) NOT FOR LEISURE |
(4) HANDWASHING |
(5) WEARING MASK |
|
| VACCINE FIRST | 0.057** (0.007-1.077) | 0.032 (−0.015-0.080) |
0.028 (−0.014-0.069) |
0.028** (0.0003-0.057) | 0.003 (−0.044-0.050) |
| VACCINE SECOND | 0.107*** (0.059-0.154) |
0.090*** (0.028-0.152) |
0.079*** (0.0355-0.123) |
0.008 (−0.024-0.041) |
0.005 (−0.038-0.048) |
| Adj R2 Obs. |
0.52 54,007 |
0.66 54,007 |
0.37 54,007 |
0.62 54,007 |
0.49 54,007 |
Note: Numbers within parentheses are 95% CI. The set of control variables used in Table 6 is included, although the results are not reported. ***p<0.01. **p<0.05. *p<0.10.
Table 8.
FE Ordered Logit model. Dependent variables are preventive behaviors.
| (1) STAYING INDOORS |
(2) NOT GOING TO WORK |
(3) NOT FOR LEISURE |
(4) HANDWASHING |
(5) WEARING MASK |
|
|
VACCINE FIRST |
|||||
| (Prob [y=1]) |
−0.019** (−0.036 - −0.003) |
−0.016 (−0.047 - 0.014) |
−0.003 (−0.011 - 0.004) |
−0.003** (−0.006 - −0.001) |
−0.009* (−0.019 - 0.0004) |
| (Prob [y=2) | −0.010** (−0.019 - −0.001) |
−0.017 (−0.004 - −0.001) |
−0.002 (−0.006 - 0.002) |
−0.007** (−0.013 - −0.001) |
−0.006* (−0.014 - 0.0003) |
| (Prob [y=3) | −0.0007** (−0.001 - −0.0001) |
0.0004 (−0.0003 - 0.001) |
−0.007 (−0.024 - 0.009) |
−0.022** (−0.041 - −0.003) |
−0.014* (−0.029 - 0.0006) |
| (Prob [y=4) | 0.019** (0.003 - 0.036) |
0.002 (−0.001-0.005) |
−0.002 (−0.005 - 0.002) |
−0.006** (−0.012 - −0.001) |
−0.015* (−0.032 - 0.007) |
| (Prob [y=5) | 0.011** (0.001 - 0.021) |
0.011 (−0.013-0.046) |
0.015 (−0.018 - 0.049) |
0.004** (0.007 - 0.073) |
0.047* (−0.002 - 0.096) |
|
VACCINE SECOND |
|||||
| (Prob [y=1]) |
−0.036*** (−0.054 - −0.018) |
−0.050*** (−0.084 - −0.015) |
−0.012*** (−0.020 - −0.004) |
−0.002 (−0.005 - 0.001) |
−0.014*** (−0.023 - −0.004) |
| (Prob [y=2) | −0.019*** (−0.029 - −0.009) |
−0.005*** (−0.008 - −0.001) |
−0.007*** (−0.011 - −0.002) |
−0.004 (−0.010 - 0.001) |
−0.010*** (−0.017 - −0.003) |
| (Prob [y=3) | −0.001*** (−0.002 - −0.0006) |
0.001*** (0.0003 - 0.002) |
−0.027*** (−0.043 - −0.010) |
−0.013 (−0.032 - 0.005) |
−0.021*** (−0.035 - −0.006) |
| (Prob [y=4) | 0.036*** (0.018 - 0.053) |
0.005*** (0.001 - 0.009) |
−0.006*** (−0.010 - 0.002) |
−0.004 (−0.009 - 0.002) |
−0.023*** (−0.039 - 0.006) |
| (Prob [y=5) | 0.021*** (0.010 - 0.031) |
0.048*** (0.015 - 0.081) |
0.053*** (0.020 - 0.086) |
0.023 (−0.010 - 0.057) |
0.068*** (0.020 - 0.115) |
| Wald-chi2 Obs. |
2,551 54,007 |
1,269 54,007 |
2,340 54,007 |
1,232 54,007 |
3,426 54,007 |
Note: Numbers within parentheses are 95% CI. Values without parentheses are marginal effects. The set of control variables used in Table 6 is included, although the results are not reported. ***p<0.01. **p<0.05. *p<0.10.
Table 9.
FE model: Dependent variables are preventive behaviors (ages<=40 years).
| (1) STAYING INDOORS |
(2) NOT GOING TO WORK |
(3) NOT FOR LEISURE |
(4) HANDWASHING |
(5) WEARING MASK |
|
| VACCINE FIRST | −0.095 (−0.127-0.108) |
−0.037 (−0.167 - 0.092) |
−0.025 (−0.143 - 0.093) |
−0.031 (−0.056 - 0.092) |
0.017 (−0.053 - 0.027) |
| VACCINE SECOND_1 | −0.106 (−0274 - 0.60) |
−0.249*** (−0.386 - −0.111) |
0.049 (−0.083 - 0.187) |
−0.060 (−0.068 - 0.111) |
0.021 (−0.059 - 0.025) |
| VACCINE SECOND_2 | −0.283** (−0.556 - −0.010) |
−0.392** (−0.594 - − 0.191) |
0.029 (−0.210 - 0.269) |
0.0002 (−0.069 - 0.176) |
0.053 (−0.074 - 0.031) |
| VACCINE SECOND_3 | −0.288* (−0.600 - 0.022) |
−0.347* (−0.713 – 0.017) |
−0.079 (−0.337 - 0.179) |
−0.053 (−0.129 - 0.413) |
0.142 (−0.101 - 0.013) |
| VACCINE SECOND_4 | −0.467 (−1.086 - 0.151) |
−0.615*** (− 0.875 - −0.355) |
−0.140 (−0.740 - 0.458) |
0.004 (−0.116 - 0.245) |
0.064 (−0.243 - 0.088) |
| Adj R2 Obs. |
0.49 15,407 |
0.56 15,407 |
0.37 15,407 |
0.52 15,407 |
0.58 15,407 |
Note: Numbers within parentheses are 95% CI. The set of control variables used in Table 6 is included, although the results are not reported. ***p<0.01. **p<0.05. *p<0.10.
Table 10.
FE model: Dependent variables are preventive behaviors (ages>40 years).
| (1) STAYING INDOORS |
(2) NOT GOING TO WORK |
(3) NOT FOR LEISURE |
(4) HANDWASHING |
(5) WEARING MASK |
|
| VACCINE FIRST | 0.036 (−0.022 - 0.095) |
0.026 (−0.034 - 0.086) |
0.013 (−0.030 - 0.056) |
0.024* (−0.003 - 0.051) |
− 0.012 (−0.003 - 0.051) |
| VACCINE SECOND_1 | 0.089*** (0.036 - 0.143) |
0.105** (0.040 - 0.170) |
0.051* (−0.001 - 0.103) |
−0.001 (−0.046 - 0.043) |
−0.016 (−0.046 - 0.043) |
| VACCINE SECOND_2 | 0.120*** (0.053 - 0.187) |
0.175*** (0.097 - 0.252) |
0.084*** (0.023 - 0.144) |
−0.024 (−0.074 - 0.025) |
−0.021 (−0.074 - 0.025) |
| VACCINE SECOND_3 | 0.118* (− 0.002 - 0.239) |
0.170*** (0.058 - 0.282) |
0.005 (− 0.123 - 0.135) |
0.012 (−0.052 - 0.078) |
−0.043 (−0.052 - 0.078) |
| VACCINE SECOND_4 | 0.131 (−0.219 - 0.481 ) |
0.167* (−0.024 - 0.358) |
−0.123 (−0.384 - 0.136) |
−0.048 (−0.211 - 0.115) |
−0.077 (−0.211 - 0.115) |
| Adj R2 Obs. |
0.52 38,600 |
0.68 38,600 |
0.35 38,600 |
0.63 38,600 |
0.53 38,600 |
Note: Numbers within parentheses are 95% CI. The set of control variables used in Table 6 is included here, but the results are not reported. ***p<0.01. **p<0.05. *p<0.10.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



