
Submitted:
26 February 2023
Posted:
28 February 2023
You are already at the latest version
Abstract
Mpox (monkeypox) is a zoonotic disease that has been endemic in African countries for decades, with a recent outbreak in several countries around the world. A 39-year-old male with HIV-HBV coinfection and poor adherence to antiretroviral treatment, who was severely immunocompromised and had a concurrent diagnosis of Mpox infection, presented to our hospital with disseminated dermatosis (over 350 lesions), perianal ulcers, odynophagia, oral intolerance, diarrhea, and soft-tissue bacterial superinfection of the lower extremities. Laboratory results were consistent with HBV infection, with an absolute CD4 cell count of 40 cells/uL and a positive PCR result for Mpox. An abdominopelvic CT scan showed evidence of severe proctitis and perineal soft-tissue infection. After 65 days of Mpox PCR, new lesions in the vesicular stage continued to appear, eventually developing hemodynamic instability and sepsis, resulting in a fatal outcome. Our case highlights the importance of intentionally looking for risk factors such as HIV/HBV coinfection and evaluating immune status (CD4 cell count) in patients with severe Mpox infection because it could be related to higher mortality.
Keywords:
atypical
; coinfection
; Hepatitis B
; human immunodeficiency virus
; monkeypox
1. Introduction
Mpox (previously monkeypox) is a viral zoonosis that belongs to Orthomyxovirus genus and poxviridae family [1], and its incubation period ranges from 5 to 21 days before onset of symptom [2,3].
Mpox has been considered endemic in African countries for decades; however, in 2022 different epidemiological studies reported an increase in cases in several countries around the world, and it was declared by the World Health Organization (WHO) as a Public Health Emergency of International Concern in June 2022 [4,5]. Regarding transmission, historically, it has been mainly associated with contact with animal reservoirs such as rodents, and outside of endemic areas, there had been very few person–person cases recorded. In this wave, person–person transmission has been better described as contracting the disease through direct contact with papules, vesicles, respiratory secretions (droplets) and sexual transmission, which has played an important role, associated with a large number of reported cases [4,6]. Proctitis has now been reported in 20% of cases in different series. Fewer cases are recorded in our research, and information about clinical manifestations and prognosis are lacking.
On the other hand, the information regarding the concomitant infection of Mpox with human immunodeficiency virus (HIV) is still limited and the epidemiological studies published after the recent outbreak identify a large population affected by this coinfection [4].
A case of an Mpox, HIV/HBV co-infected patient who developed generalized ulcerative injuries, proctitis, and necrotizing fasciitis, ultimately leading to death, in a third-level hospital in Mexico is presented herein in order to highlight the possible synergistic association of a triple viral infection which would imply a greater risk of presenting severe and atypical disease in patients with monkeypox.
2. Case Presentation Section
The presented case is of a 39-year-old male with a medical history of HIV infection diagnosed in 2012. He was treated with Bictegravir, Alafenamide Tenofovir and Emtricitabine (single-tablet regimen), but his adherence was poor due to personal issues. His HIV status at the time of admission showed virological failure (over 100,000 copies/mL), and he was severely immunocompromised (absolute CD4 of 40 cells/uL). He had a history of multiple sexual partners (both same- and opposite-sex partners) and was an active intravenous drug user.
Two weeks before admission, the patient presented odynophagia, oral intolerance, diarrhea, and weight loss and said that before the first cutaneous lesions, he had anal intercourse, after which, he started experiencing fever (39.0°C) and a perianal abscess, which was treated with oral antibiotics and drainage. Subsequently, dermatosis commenced, characterized by itchy umbilicated vesicles less than 5mm in diameter, beginning on the face but spreading to the entire body, including the palms and soles, with progression to pustules, scabs and necrotic ulcers, reaching more than 350 in number by the time of his admission. (Figure 1).
Due to severe soft-tissue bacterial superinfection of the lower extremities, generalized dermatosis, and immunodeficiency status of the patient, antibiotic treatment was started with cotrimoxazole, piperacillin plus tazobactam, and fluconazole. An abdominopelvic CT scan was conducted, which showed evidence of severe proctitis (Figure 2).
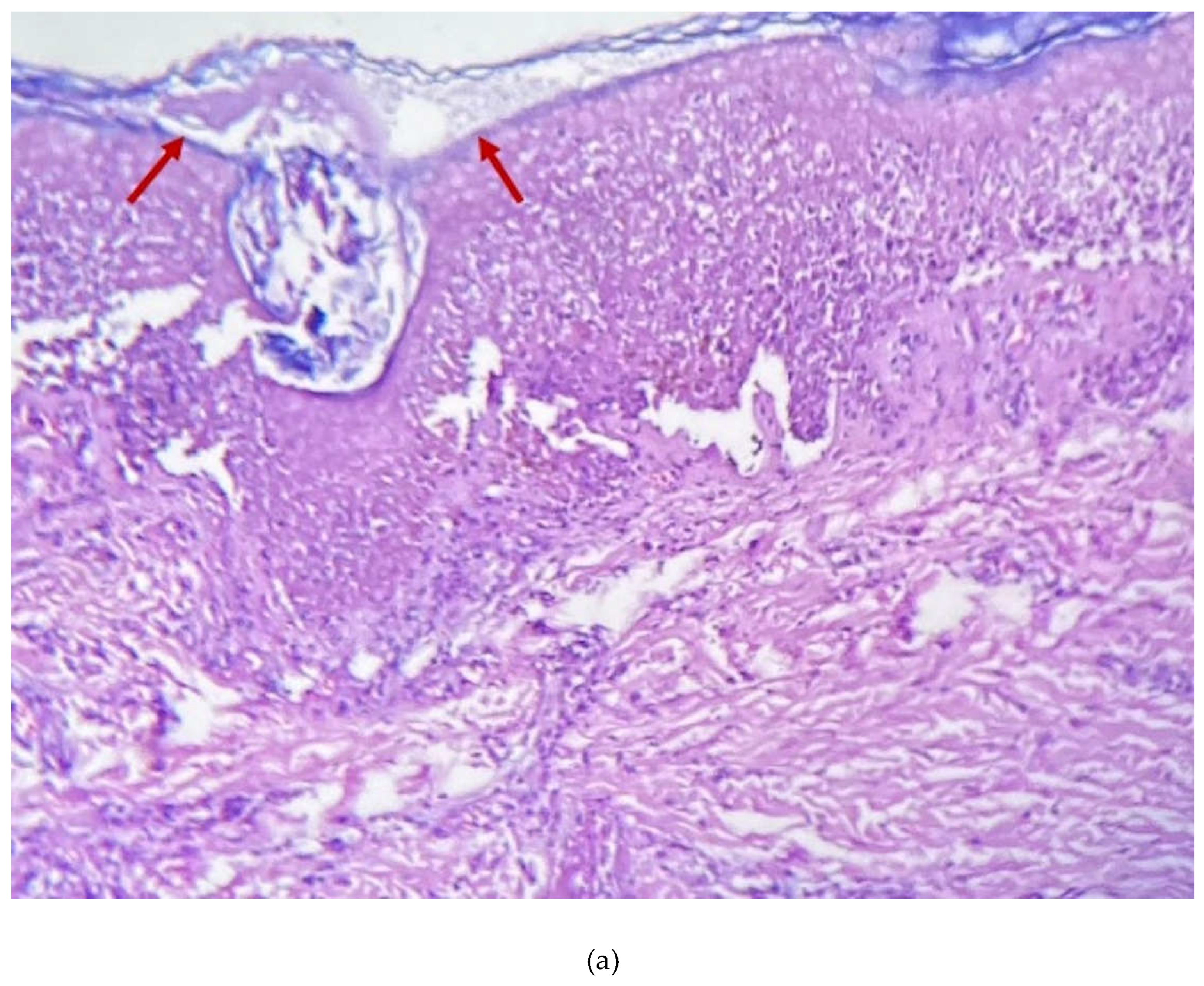
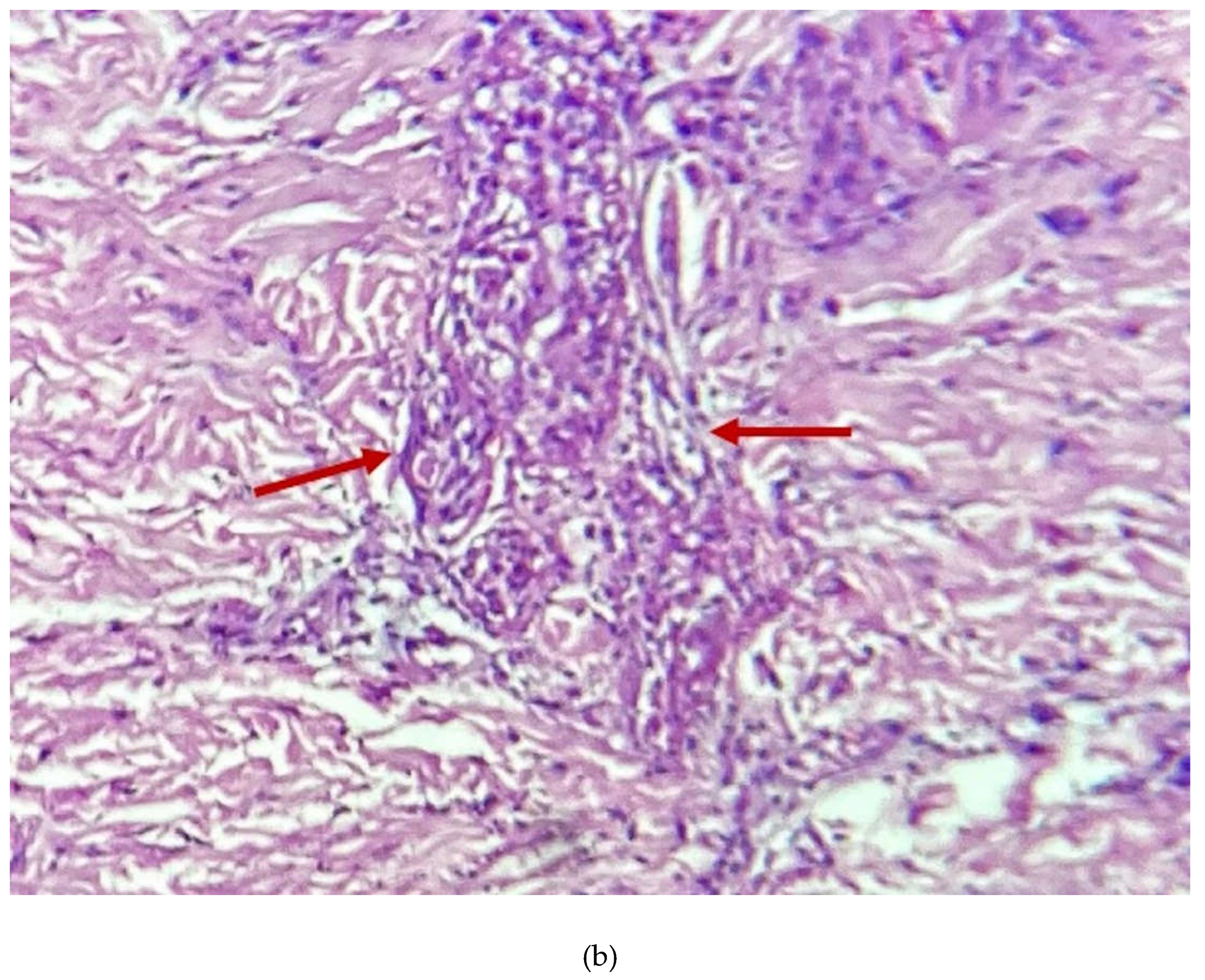
New asynchronic lesions continued developing, so skin biopsies were obtained (Figure 3). Serological tests were positive for Hepatitis B surface antigen (HBsAg) and Hepatitis B e antigen (HBeAg) and negative for Cytomegalovirus (CMV), anti-Hepatitis C antibody (anti-HCV), VDRL, and FTA-ABS. Viral load for HBV and resistance genotype to antiretrovirals results were not available in our hospital. After reviewing the case with a multi-disciplinary team (internal medicine, infectious diseases, dermatology, and anorectal surgery), due to suspected severe and deep infection, the persistence of different stages of new skin lesions 65 days after initial diagnosis of monkeypox by PCR, an absence of growth cultures from the skin, stool, and blood, and no clinical improvement, it was decided to escalate to empirical antibiotic treatment with Meropenem, Amphotericin B and cotrimoxazole.
Despite the above-mentioned treatment, improvement in his clinical condition was very slow due to hemodynamic instability, sepsis, and death. New asynchronic Mpox vesicular skin lesions continued to appear until the day of his death.
3. Discussion
The Americas have been the most affected region in the recent Mpox outbreak, accounting for 67.6% of cases and 71% of deaths worldwide (WHO as of May 9th, 2022).
Epidemiological reports on the current Mpox outbreak identify men (~97%), with a median age of ~34 years, and a high proportion of them living with HIV (36-67%), as the most affected group [6,7].
Despite this, mortality is low (<0.1%), and extensive (>100 lesions) and severe presentations (confluent lesions, sepsis, or the involvement of risky anatomic areas such as the eyes, anus, etc.) are rare [6,8] and have been associated with immunocompromised individuals. In a CDC weekly report, cases of 57 hospitalized patients with severe Mpox were reviewed, where there were 12 deaths (21%), and it was noted that 82.5% were persons living with HIV and 72.1% had a CD4 count < 50 cells/mm3 (97% < 200) [9]. This contrasts with the mortality rates reported in studies of patients with CD4 counts averaging 462 cells/mm3 (0.17% mortality) 7, 510 cells/mm3 (0.0% mortality) 8, or 664 cells/mm3 (0.0% mortality) [10].
Our patient, who unfortunately died, had an extensive presentation of >350 confluent lesions and severe rectal complications and was probably experiencing virologic failure despite antiretroviral treatment and severely compromised immunity (CD4 of 40 cells/uL). In the response to Mpox infection, effector CD4 T cells play a central role in the memory and differentiation of B lymphocytes to antibody-producing cells. Likewise, there is an immune cellular response to Mpox infection characterized by the rapid expansion of activated effector CD4 and CD8 cells, which generate a Th1 immune response (with production of cytokines such as IFN-γ, IL-1β, IL-6, IL-8, TNF, and MCP-1). This response is observed in HIV patients with CD4 >350 cells/mm3; however, there are no data regarding patients with CD4 <350 cells/mm3 [11].
In any case, HIV/HBV coinfection has been shown to be associated with increased risk of advanced HIV disease and lower CD4 count at diagnosis [12], as well as poor immune response and significantly decreased CD4 count recovery after antiretroviral therapy [13,14].
Therefore, it is likely that possible appropriate humoral and cellular responses against Mpox were hampered due to the low CD4 levels secondary to virological and immune failure and exacerbated by HIV/HBV coinfection, leading to active replication of Mpox (by the presence of new vesicular phase lesions (Figure 3) even after 4 weeks of onset) [15] and ultimately to death; although this was not completely attributable to Mpox as a cause, the latter was certainly a contributing factor.
To our knowledge, severe, extensive, and fatal Mpox infection, with the risk factors of HIV/HBV coinfection and immune failure despite antiretroviral treatment, has not been reported, which highlights the importance of intentionally searching for such coinfections.
4. Conclusions
In the face of severe Mpox infection, it is important to intentionally search for coinfections such as HIV and HBV, as well as to conduct evaluation of immune status (CD4 cell count), since a deteriorated immune status (CD4 <200 cells/mm3) seems to be related to higher mortality; however, large epidemiological studies are required to corroborate this association.
Author Contributions
Conceptualization, V.A. and F.P.; methodology, A.H.; investigation, M.C.; data curation, C.F.; writing—original draft preparation, V.A.; writing—review and editing, F.P.; visualization, V.A.; supervision, D.T.; project administration, F.P.; funding acquisition, F.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Informed Consent Statement
The patient died before the writing of this paper, so informed consent could not be obtained.
Acknowledgments
Carlos David Franco Gonzalez, Jorge Lopez Garcia (literature research, students), Alma Leticia Rodriguez Guzman (medical resident who was directly involved in patient care).
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Petersen, E.; Kantele, A.; Koopmans, M.; Asogun, D.; Yinka-Ogunleye, A.; Ihekweazu, C.; Zumla, A. Human Monkeypox: Epidemiologic and Clinical Characteristics, Diagnosis, and Prevention. Infect. Dis. Clin. North Am. 2019, 33, 1027–1043. [Google Scholar] [CrossRef] [PubMed]
- Tarín-Vicente, E.J.; Alemany, A.; Agud-Dios, M.; Ubals, M.; Suñer, C.; Antón, A.; Arando, M.; Arroyo-Andrés, J.; Calderón-Lozano, L.; Casañ, C.; Cabrera, J.M.; Coll, P.; Descalzo, V.; Folgueira, M.D.; García-Pérez, J.N.; Gil-Cruz, E.; González-Rodríguez, B.; Gutiérrez-Collar, C.; Hernández-Rodríguez, Á.; López-Roa, P.; de los Ángeles Meléndez, M.; Montero-Menárguez, J.; Muñoz-Gallego, I.; Palencia-Pérez, S.I.; Paredes, R.; Pérez-Rivilla, A.; Piñana, M.; Prat, N.; Ramirez, A.; Rivero, Á.; Rubio-Muñiz, C.A.; Vall, M.; Acosta-Velásquez, K.S.; Wang, A.; Galván-Casas, C.; Marks, M.; Ortiz-Romero, P.L.; Mitjà, O. Clinical Presentation and Virological Assessment of Confirmed Human Monkeypox Virus Cases in Spain: A Prospective Observational Cohort Study. Lancet (London, England) 2022, 400, 661. [Google Scholar] [CrossRef] [PubMed]
- Minhaj, F.S.; Ogale, Y.P.; Whitehill, F.; Schultz, J.; Foote, M.; Davidson, W.; Hughes, C.M.; Wilkins, K.; Bachmann, L.; Chatelain, R.; Donnelly, M.A.P.; Mendoza, R.; Downes, B.L.; Roskosky, M.; Barnes, M.; Gallagher, G.R.; Basgoz, N.; Ruiz, V.; Kyaw, N.T.T.; Feldpausch, A.; Valderrama, A.; Alvarado-Ramy, F.; Dowell, C.H.; Chow, C.C.; Li, Y.; Quilter, L.; Brooks, J.; Daskalakis, D.C.; McClung, R.P.; Petersen, B.W.; Damon, I.; Hutson, C.; McQuiston, J.; Rao, A.K.; Belay, E.; McCollum, A.M.; Angelo, K.; Arduino, M.; Arthur, R.; Baird, N.; Batross, J.; Beeson, A.; Bhingarde, J.; Bowen, M.; Brown, C.; Brown, C.M.; Burakoff, A.; Charniga, K.; Chen, T.-H.; Chen, S.; Clay, P.; Cope, J.; Cope, J.; Dankwa, M.A.; Delaney, L.; Perio, M. De; Decenteceo, M.; Delea, K.; Doty, J.B.; Duchin, J.; Dunlap, J.; Fagan, R.; Furness, B.; Gearhart, S.; Gigante, C.; Gilliland, A.; Gosdin, L.; Griffin, I.; Groccia, A.; Guagliardo, S.; Hercules, Y.; Jackson, K.; Jarquin, P.; Kachur, R.; Kallen, A.; Kao, R.; Kelly, A.; Khan, M.; Khan, T.; Kofman, A.; Kornylo, K.; Kuhar, D.; LaFlam, M.; Lash, R.; Lashombe, A.; Lowe, D.; MacGurn, A.; Masters, N.; McCaffrey, K.; Mink, J.L.; Monroe, B.; Morgan, C.N.; Nakazawa, Y.; Nash, J.; Navarra, T.; Newton, D.; Osinubi, M.; Osorio, V.; Pearson, C.; Petras, J.; Philpott, D.; Pickrel, A.; Potvin, B.; Priyamvada, L.; Rey, A.; Ricketts, E.; Rodriguez, S.; Rushmore, J.; Satheshkumar, P.S.; Segaloff, H.; Sekkarie, A.; Sharma, A.; Sims, E.; Smith, D.; Smith, T.; Smith, T.; Solanky, D.; Spiknall, I.; Stanek, D.R.; Stenger, M.; Strona, F.; Tardivel, K.; Tyagi, E.; Wortley, P.; Valencia, D.; Waltenburg, M.; Whitehouse, E.; Wong, M. Monkeypox Outbreak — Nine States, May 2022. MMWR. Morb. Mortal. Wkly. Rep. 2022, 71, 764–769. [Google Scholar] [CrossRef] [PubMed]
- Thornhill, J.P.; Barkati, S.; Walmsley, S.; Rockstroh, J.; Antinori, A.; Harrison, L.B.; Palich, R.; Nori, A.; Reeves, I.; Habibi, M.S.; Apea, V.; Boesecke, C.; Vandekerckhove, L.; Yakubovsky, M.; Sendagorta, E.; Blanco, J.L.; Florence, E.; Moschese, D.; Maltez, F.M.; Goorhuis, A.; Pourcher, V.; Migaud, P.; Noe, S.; Pintado, C.; Maggi, F.; Hansen, A.-B. E.; Hoffmann, C.; Lezama, J.I.; Mussini, C.; Cattelan, A.; Makofane, K.; Tan, D.; Nozza, S.; Nemeth, J.; Klein, M.B.; Orkin, C.M. Monkeypox Virus Infection in Humans across 16 Countries — April–June 2022. N. Engl. J. Med. 2022, 387, 679–691. [Google Scholar] [CrossRef] [PubMed]
- Multi-country monkeypox outbreak: situation update. (accessed 2023-01-22). Available online: https://www.who.int/emergencies/disease-outbreak-news/item/2022-DON393.
- Mitjà, O.; Ogoina, D.; Titanji, B.K.; Galvan, C.; Muyembe, J.-J.; Marks, M.; Orkin, C.M. Monkeypox. Lancet 2023, 401, 60–74. [Google Scholar] [CrossRef] [PubMed]
- Núñez, I.; García-Grimshaw, M.; Ceballos-Liceaga, S.E.; Toledo-Salinas, C.; Carbajal-Sandoval, G.; Sosa-Laso, L.; García-Rodríguez, G.; Cortés-Alcalá, R.; Torre, A. de la; Fragoso-Saavedra, S.; Quintero-Villegas, A.; López-Gatell, H.; Reyes-Terán, G.; Valdés-Ferrer, S.I. Epidemiological and Clinical Characteristics of Patients with Human Monkeypox Infection in Mexico: A Nationwide Observational Study. Lancet Reg. Heal. - Am. 2023, 17, 100392. [Google Scholar] [CrossRef]
- Fink, D.L.; Callaby, H.; Luintel, A.; Beynon, W.; Bond, H.; Lim, E.Y.; Gkrania-Klotsas, E.; Heskin, J.; Bracchi, M.; Rathish, B.; Milligan, I.; O’Hara, G.; Rimmer, S.; Peters, J.R.; Payne, L.; Mody, N.; Hodgson, B.; Lewthwaite, P.; Lester, R.; Woolley, S.D.; Sturdy, A.; Whittington, A.; Johnson, L.; Jacobs, N.; Quartey, J.; Ai Payne, B.; Crowe, S.; Elliott, I.A.; Harrison, T.; Cole, J.; Beard, K.; Cusack, T.-P.; Jones, I.; Banerjee, R.; Rampling, T.; Specialist and High Consequence Infectious Diseases Centres Network for Monkeypox; Dunning, J. Clinical Features and Management of Individuals Admitted to Hospital with Monkeypox and Associated Complications across the UK: A Retrospective Cohort Study. Lancet. Infect. Dis. 2022, 0. [Google Scholar] [CrossRef]
- Miller, M.J.; Cash-Goldwasser, S.; Marx, G.E.; Schrodt, C.A.; Kimball, A.; Padgett, K.; Noe, R.S.; McCormick, D.W.; Wong, J.M.; Labuda, S.M.; Borah, B.F.; Zulu, I.; Asif, A.; Kaur, G.; McNicholl, J.M.; Kourtis, A.; Tadros, A.; Reagan-Steiner, S.; Ritter, J.M.; Yu, Y.; Yu, P.; Clinton, R.; Parker, C.; Click, E.S.; Salzer, J.S.; McCollum, A.M.; Petersen, B.; Minhaj, F.S.; Brown, E.; Fischer, M.P.; Atmar, R.L.; DiNardo, A.R.; Xu, Y.; Brown, C.; Goodman, J.C.; Holloman, A.; Gallardo, J.; Siatecka, H.; Huffman, G.; Powell, J.; Alapat, P.; Sarkar, P.; Hanania, N.A.; Bruck, O.; Brass, S.D.; Mehta, A.; Dretler, A.W.; Feldpausch, A.; Pavlick, J.; Spencer, H.; Ghinai, I.; Black, S.R.; Hernandez-Guarin, L.N.; Won, S.Y.; Shankaran, S.; Simms, A.T.; Alarcón, J.; O’Shea, J.G.; Brooks, J.T.; McQuiston, J.; Honein, M.A.; O’Connor, S.M.; Chatham-Stephens, K.; O’Laughlin, K.; Rao, A.K.; Raizes, E.; Gold, J.A.W.; Morris, S.B.; Duessel, S.; Danaie, D.; Hickman, A.; Griffith, B.; Sanneh, H.; Hutchins, H.; Phyathep, C.; Carpenter, A.; Shelus, V.; Petras, J.; Hennessee, I.; Davis, M.; McArdle, C.; Dawson, P.; Gutelius, B.; Bisgard, K.; Wong, K.; Galang, R.R.; Perkins, K.M.; Filardo, T.D.; Davidson, W.; Hutson, C.; Lowe, D.; Zucker, J.E.; Wheeler, D.A.; He, L.; Jain, A.K.; Semeniuk, O.; Chatterji, D.; McClure, M.; Li, L.X.; Mata, J.; Beselman, S.; Cross, S.L.; Menzies, B.; Keller, M.; York, N.; Chaturvedi, V.; York, N.; Thet, A.; Carroll, R.; Hebert, C.; Patel, G.; Gandhi, V.; Abrams-Downey, A.; Nawab, M.; Landon, E.; Lee, G.; Kaplan-Lewis, E.; Miranda, C.; Carmack, A.E.; Traver, E.C.; Lazarte, S.; Perl, T.M.; Chow, J.; Kitchell, E.; Nijhawan, A.; Habib, O.; Bernus, A.; Andujar, G.; Davar, K.; Holtom, P.; Wald-Dickler, N.; Lorio, M.A.; Gaviria, J.; Chu, V.; Wolfe, C.R.; McKellar, M.S.; Farran, S.; Diaz Wong, R.A.; Schliep, T.; Shaw, R.; Tebas, P.; Richterman, A.; Aurelius, M.; Peterson, L.; Trible, R.; Rehman, T.; Sabzwari, R.; Hines, E.; Birkey, T.; King, J.; Farabi, A.; Jenny-Avital, E.; Touleyrou, L.; Sandhu, A.; Newman, G.; Bhamidipati, D.; Bhamidipati, D.; Vigil, K.; Caro, M.; Banowski, K.; Chinyadza, T.W.; Rosenzweig, J.; Jones, M.S.; Camargo, J.F.; Marsh, K.J.; Liu, E.W.; Guerrero-Wooley, R.; Pottinger, P. Severe Monkeypox in Hospitalized Patients — United States, August 10–October 10, 2022. MMWR. Morb. Mortal. Wkly. Rep. 2022, 71, 1412–1417. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.; Bilinska, J.; Tam, J.C.H.; Da Silva Fontoura, D.; Mason, C.Y.; Daunt, A.; Snell, L.B.; Murphy, J.; Potter, J.; Tuudah, C.; Sundramoorthi, R.; Abeywickrema, M.; Pley, C.; Naidu, V.; Nebbia, G.; Aarons, E.; Botgros, A.; Douthwaite, S.T.; Van Nispen Tot Pannerden, C.; Winslow, H.; Brown, A.; Chilton, D.; Nori, A. Clinical Features and Novel Presentations of Human Monkeypox in a Central London Centre during the 2022 Outbreak: Descriptive Case Series. BMJ 2022, 378. [Google Scholar] [CrossRef]
- Agrati, C.; Cossarizza, A.; Mazzotta, V.; Grassi, G.; Casetti, R.; De Biasi, S.; Pinnetti, C.; Gili, S.; Mondi, A.; Cristofanelli, F.; Lo Tartaro, D.; Notari, S.; Maffongelli, G.; Gagliardini, R.; Gibellini, L.; Aguglia, C.; Lanini, S.; D’Abramo, A.; Matusali, G.; Fontana, C.; Nicastri, E.; Maggi, F.; Girardi, E.; Vaia, F.; Antinori, A. Immunological Signature in Human Cases of Monkeypox Infection in 2022 Outbreak: An Observational Study. Lancet Infect. Dis. 2022, 0. [Google Scholar] [CrossRef]
- Afrashteh, S.; Fararouei, M.; Ghaem, H.; Aryaie, M. Factors Associated with Baseline CD4 Cell Counts and Advanced HIV Disease among Male and Female HIV-Positive Patients in Iran: A Retrospective Cohort Study. J. Trop. Med. 2022, 2022. [Google Scholar] [CrossRef]
- Chiesa, A.; Ochola, E.; Oreni, L.; Vassalini, P.; Rizzardini, G.; Galli, M. Hepatitis B and HIV Coinfection in Northern Uganda: Is a Decline in HBV Prevalence on the Horizon? PLoS One 2020, 15, e0242278. [Google Scholar] [CrossRef]
- Anderson, M.; Gaseitsiwe, S.; Moyo, S.; Thami, K.P.; Mohammed, T.; Setlhare, D.; Sebunya, T.K.; Powell, E.A.; Makhema, J.; Blackard, J.T.; Marlink, R.; Essex, M.; Musonda, R.M. Slow CD4+ T-Cell Recovery in Human Immunodeficiency Virus/Hepatitis B Virus-Coinfected Patients Initiating Truvada-Based Combination Antiretroviral Therapy in Botswana. Open Forum Infect. Dis. 2016, 3, 1–8. [Google Scholar] [CrossRef]
- Menezes, Y.R.; de Miranda, A.B. Severe Disseminated Clinical Presentation of Monkeypox Virus Infection in an Immunosuppressed Patient: First Death Report in Brazil. Rev. Soc. Bras. Med. Trop. 2022, 55, 2022. [Google Scholar] [CrossRef]
Figure 1.
Clinical Manifestations. (a) Presence of scars and necrotic ulcers on the face as well as the involvement of the nasal and buccal mucosa with cheilitis. (b) Involvement of the first, third, and fourth toes of the right foot with edema and color changes, as well as the presence of purulent discharge and necrotic ulcers. (c, d, e, f) Disseminated necrotic ulcers in the face, thorax, anterior abdomen, and palms with involvement of the perianal region as well as the rectal mucosa and umbilicated papules around the necrotic ulcers. (g) Erythematous plaque with color changes and edema, suggesting infection with limitation of mobility in the said joint.
Figure 1.
Clinical Manifestations. (a) Presence of scars and necrotic ulcers on the face as well as the involvement of the nasal and buccal mucosa with cheilitis. (b) Involvement of the first, third, and fourth toes of the right foot with edema and color changes, as well as the presence of purulent discharge and necrotic ulcers. (c, d, e, f) Disseminated necrotic ulcers in the face, thorax, anterior abdomen, and palms with involvement of the perianal region as well as the rectal mucosa and umbilicated papules around the necrotic ulcers. (g) Erythematous plaque with color changes and edema, suggesting infection with limitation of mobility in the said joint.

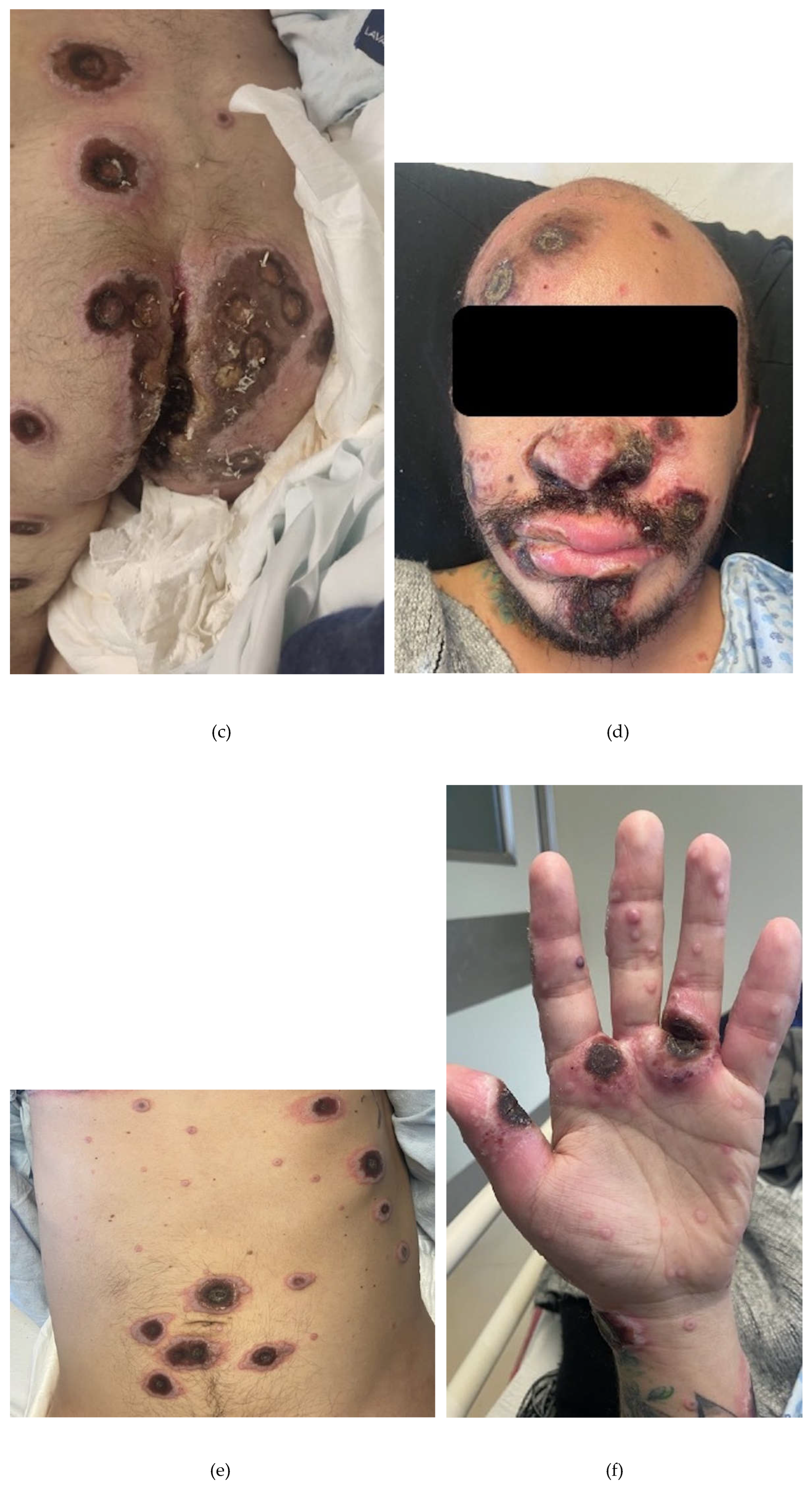

Figure 2.
(a, b) Inflammatory-looking thickening of the region of the rectum and anal canal.
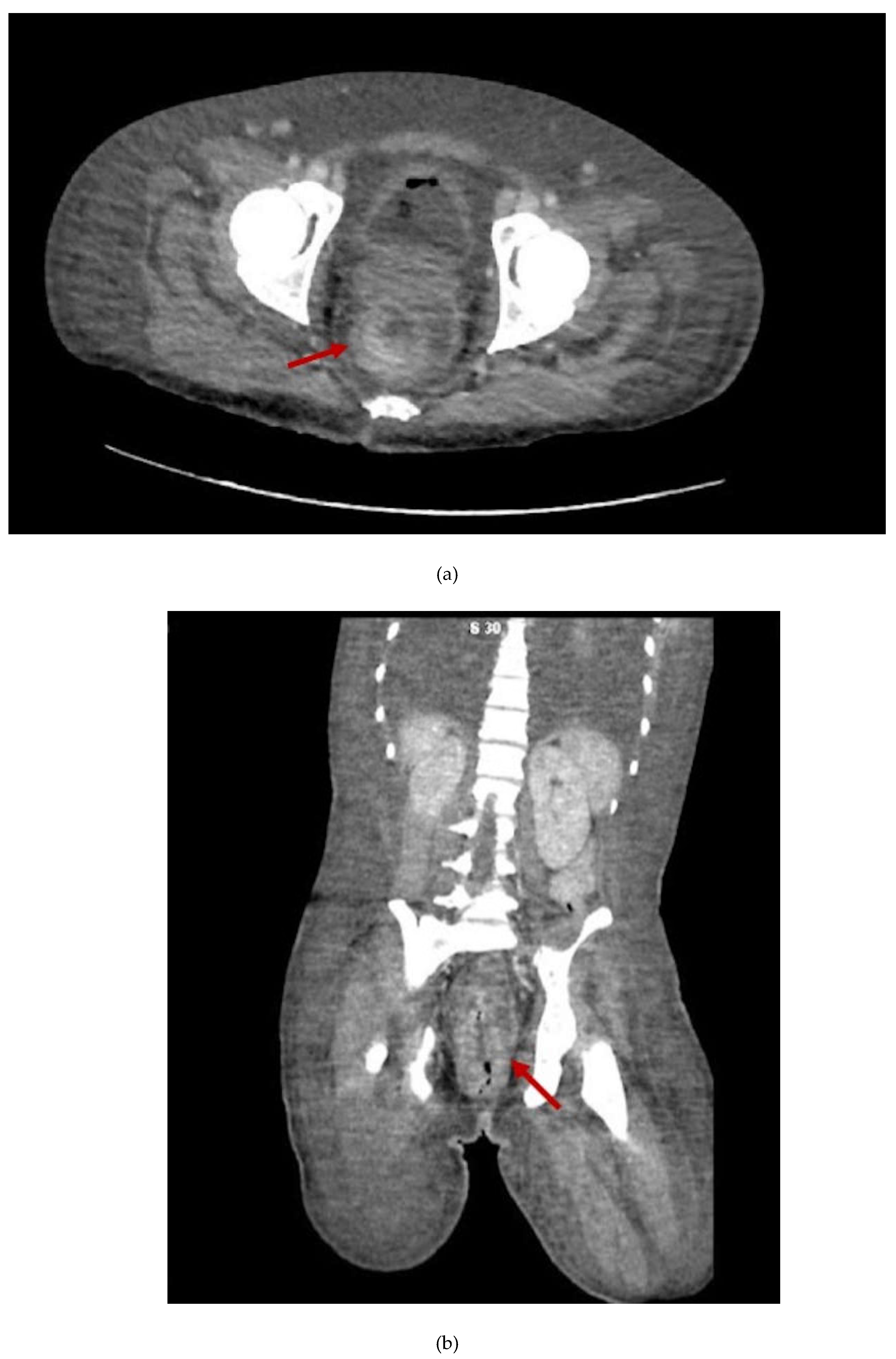
Figure 3.
Punch biopsy of umbilicated lesions in the palms with acanthosic epidermis. (a) Diffuse necrosis of keratinocytes, with full-thickness epithelial involvement, presence of ballooning degeneration in central areas, and intraepidermal bulla formation. (b) Presence of mixed periadnexal and mild perivascular infiltrate, conclusive of vesicular dermatitis.
Figure 3.
Punch biopsy of umbilicated lesions in the palms with acanthosic epidermis. (a) Diffuse necrosis of keratinocytes, with full-thickness epithelial involvement, presence of ballooning degeneration in central areas, and intraepidermal bulla formation. (b) Presence of mixed periadnexal and mild perivascular infiltrate, conclusive of vesicular dermatitis.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



