
Submitted:
28 February 2023
Posted:
02 March 2023
You are already at the latest version
Abstract
Today, various questionnaires are available to assess Adverse Childhood Experiences (ACEs) in children; however, it is uncertain if these questionnaires comprehensively address the adversities of vulnerable subgroups, specifically refugee children. This review's objectives are to (1) identify current ACE questionnaires and determine if they are suitable for assessing refugee children’s adversities, and (2) identify those previously used within a refugee population. A systematic literature search was conducted across five databases for articles published since 2010, including studies using an ACE questionnaire that recognized multiple adversities in healthy children and were published in English. A total of 103 ACE questionnaires were identified in 506 studies. Only 14 of the 103 questionnaires addressed a refugee-specific adversity. Their ability to capture refugee children’s experiences was limited: available questionnaires used a maximum of three items to assess refugee-specific adversities, covering only a fraction of forms of adversities relevant to refugee children. Psychometric characteristics were rarely reported. In addition, only two ACE questionnaires were used within a refugee population. With the tools currently available, it is not possible to comprehensively assess the exposure to and severity of the adversities faced by refugee children. The perpetuation of ongoing crises necessitates assessing refugee children's adversities to understand how their well-being is affected and to identify children at risk.
Keywords:
Adverse Childhood Experiences (ACEs)
; Refugee children
; Systematic review
; Questionnaires
Introduction
Adverse Childhood Experiences (ACEs) are highly stressful, and potentially traumatic, events or situations that occur during childhood and/or adolescence [1]. The Centers for Disease Control and Prevention (CDC) and the Kaiser Permanente popularised this term in their pioneering study exploring the effects of adversity on people's health and behaviour [2]. Their research revealed that children who experience an increasing number of adverse events are more likely to face serious life-long consequences in adulthood such as alcohol abuse and have increased odds for non-communicable diseases such as diabetes or chronic obstructive pulmonary disease [2]. The last two decades of research revealed that ACEs are common and rarely occur individually, thus they have become of global importance [3].
Given global estimates that over half of all children between ages 2 and 17 (i.e., over 1 billion children) experienced some form of adverse event [4], a variety of tools for screening and assessing ACEs in children and adolescents have been developed. These tools aim to identify children most at risk, encourage prevention of further exposure to ACEs, help determine an appropriate treatment for children who had been exposed as well as drive policy and action to better tailor health care measures based on an understanding of how many children might suffer [5].
Some questionnaires primarily focused on a specific type of event (e.g., child sexual abuse), others examined several ACEs yet are limited to the perpetrator (e.g., family member or caregiver) or location (e.g., within the home or at school) [6]. The conventional ACEs (originating from the CDC-Kaiser Permanente study) concentrated on adversities within the home: physical, emotional, and sexual abuse, physical and emotional neglect, and household dysfunction [7,8]. However, given that a child’s wellbeing can be affected by the community and society in which they live, it is also important to acknowledge experiences in these settings that contribute to a child’s quality of life [9]. More recent work, therefore, includes experiences referred to as expanded ACEs that assess exposures such as crime, discrimination, poverty, parents’ unemployment, food insecurity and bullying [10,11]. Despite the expansion of types of adversities, it is unclear whether existing questionnaires are extensive enough to encompass ACEs that may occur in subgroups of vulnerable children.
Refugee children represent one such subgroup given their frequent exposure to adverse experiences [12], including escaping from war zones, violence, conflict or persecution to find safety in another country – often without warning [13]. The estimated number of forcibly displaced children in 2021 was 36.5 million [14] with more than four million children resettling abroad or being internally displaced in 2022 as a result of the war in Ukraine [15]. As nearly 600 million young people live in conflict-prone regions, it is likely these numbers will be sustained or even increase in the future [16].
The adverse events encountered during flight appear to have profound effects, especially in children. Developmental and epidemiological studies suggest, for example that displacement, detention, separation from family, and resettlement [17], may have long-lasting physical and psychological consequences [18], including a higher prevalence of post-traumatic stress disorder (PTSD), anxiety, depression and conduct disorders [19].
The utility of available instruments in assessing these refugee-specific ACEs is currently unclear. The purpose of this review is to identify available questionnaires that assess ACEs in children, and (1) to examine whether and to what extent these questionnaires may be useful in assessing the diverse and often unique adverse experiences encountered by refugee children and (2) to examine which ACE questionnaires have already been used within a refugee population. Identifying gaps in current ACE questionnaires may help guide the development of tools for children subjected to the refugee experience.
Methods
Search strategy
A search of articles published since January 2010 was conducted in four databases: PubMed, Web of Science Core Collection, PsychINFO, and Academic Search Complete. The systematic literature search was initially conducted on October 9, 2018, with updates on February 14, 2020, and on March 1, 2022. The latter two updates were made to identify publications capturing more recent refugee events. Search terms included abuse, sexual abuse, neglect, maltreatment, trauma, violence, stress, household dysfunction, adverse child experience, adverse childhood event, child, infant, adolescent, teenager, youth, questionnaire and survey. The full search strategy for all databases can be found in Appendix 1. In order to avoid limiting the search, the term "refugee" was not included as items might be applicable to refugee children even though they were not intended for application in refugee populations. The study protocol was registered on the international database of prospectively registered systematic reviews PROSPERO (ID: CRD42019121587).
This review aims at identifying questionnaires that recognise multiple adversities in healthy children, as previous literature has identified that many children experience multiple co-occurring ACEs that might impact their wellbeing [20,21]. Thus, included articles used questionnaires that measured more than one ACE, in children under the age of 18 (as per the United Nations definition of a child), and were written in English [22,23]. As interest was only in questionnaires, studies were excluded if adversities were assessed using interviews in the form of a structured conversation. Articles that evaluated children who had a mental disorder prior to measuring ACEs were also excluded due to the focus on examining healthy children, and due to differences in how mental disorders are measured and defined. Additionally, owing to inherent differences between adults and children such as limited vocabulary, cognition, experiences and understanding [24], studies that used the same questionnaire to measure ACE exposure in both adults and children were also excluded, as the questionnaire was not designed specifically for children.
Screening
Two reviewers independently screened all identified articles at the title, abstract, and full-text level using Rayyan (a free web application developed by Qatar Computing Research Institute) to facilitate the screening process. Figure 1 displays the process of selecting articles included in this study. Disputes over the eligibility of studies were resolved through discussion until consensus was achieved.
Figure 1: Method of identifying articles and questionnaires (adapted from the PRISMA flow diagram)
Data extraction and item assessment
A standardised data extraction form, developed by the first author, was used when reviewing information found in a study reporting use of a questionnaire. Extracted data included the country where each study took place, study population characteristics, mode of data collection, name of the questionnaire, questionnaire items and psychometric properties.
Questionnaire items were retrieved either from the published article, survey websites or from personal communication with the original study authors. In this review, ACEs were categorised into 11 categories defined by the research team. The first six categories as displayed in Table 1 were referred to as the conventional ACEs originating from the CDC-Kaiser Permanente study [7,8]. The following four categories were considered expanded ACEs including adversities identified in recent literature such as community violence [25,26,27,28,29]. ACEs were classified as refugee-specific based on the definition of a refugee and also guided by our recent qualitative findings [30]. A refugee is someone who has been forced to flee his or her country because of persecution, war or violence [13], accordingly refugee-specific ACEs include, but are not limited to, exposure to war/conflict, shootings, bombs and riots, displacement and family separation. Different forms of adversities for each category are listed in Table 1 (expanded on findings by Laurin et al., 2018 [31]).
Psychometric properties help assess the degree to which a questionnaire measures the desired content and whether the data it yields are reproducible [32]. Therefore, as a quality assessment, we identified whether retest reliability, internal consistency, inter-observer reliability, content validity, criterion validity, construct validity including cross-cultural validity (if applicable) had been reported as outlined in previous work by de Souza et. al, 2017 [32] .
A second research team member independently crosschecked all the extracted data of 100 randomly selected articles with the original articles. Minor differences, such as labelling of demographic information were discussed until agreement was achieved. Since there were no major differences, duplicate checking of all reports was deemed unnecessary.
Analytic Strategy
The unit of analysis in this study is the questionnaire itself. To determine whether ACE questionnaires are useful in evaluating adversities that refugee children may encounter, a descriptive record of characteristics (i.e., the adversity categories and forms measured and psychometric properties reported) was made. With attention on those questionnaires that measured refugee-specific ACEs, the analytic strategy involved two focuses: (1) to assess ACEs of each category by recording which questionnaires measured which form of adversity. (2) To examine the extent to which each adversity category had been measured by recording the number of questions addressing each category; the use of multiple rather than single questions indicated a higher extent.
To recognise the quality of the questionnaires, information regarding three aspects of reliability and four aspects of validity was extracted from all the studies identified in this review that reported this information. For the questionnaires that addressed a refugee-specific ACE, the number of studies that reported on the individual psychometric aspects were assessed. These topics are discussed further in the following sections.
Results
A total of 506 full-text articles fulfilled the inclusion criteria, in which use of 103 unique questionnaires was reported. Questionnaires were administered mostly via self-report (n= 286 studies), and data collection usually was by means of a household survey (n= 237 studies). The number of participants varied from 29,696,808 to 14, as some of the questionnaires were used as part of national surveys. Most of the studies were conducted in the United States of America (USA) (n= 274 studies), and most of the questionnaires were in English (n= 315 studies).
Adversities measured
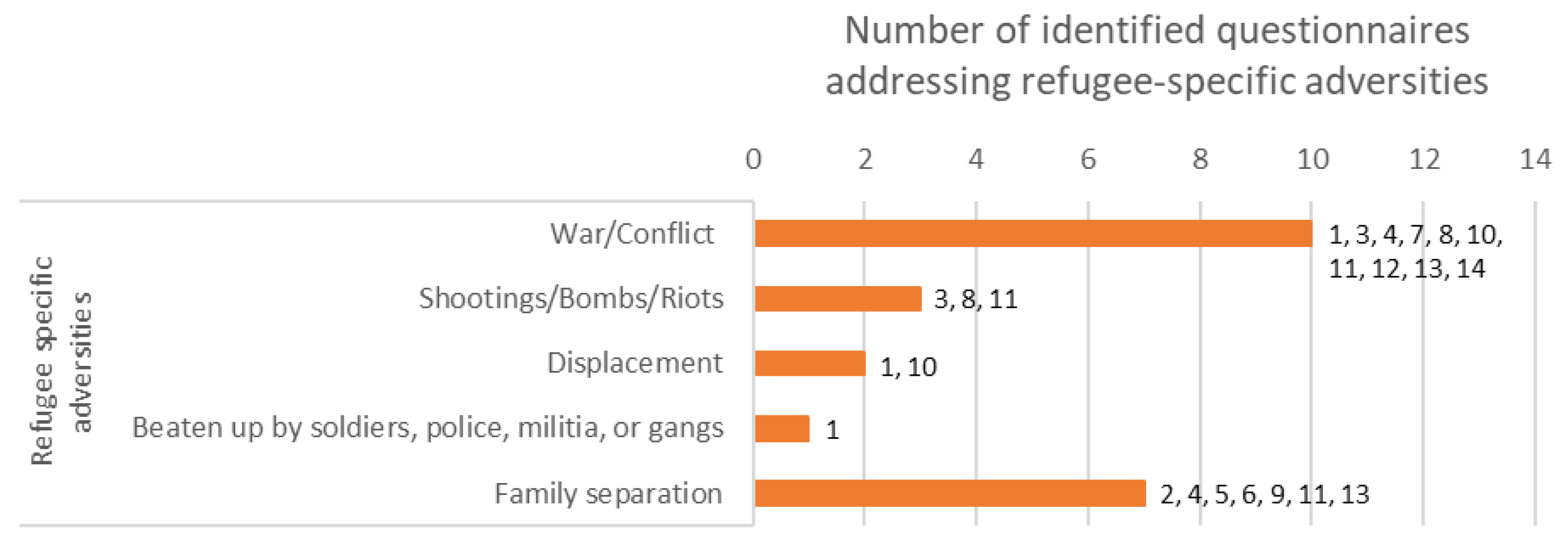
The identified questionnaires measured different adversity categories that could be relevant to refugee children, yet only 14 included one or more questions addressing a refugee-specific adversity. Exposure to war/conflict and family separation were the forms of refugee-specific ACEs being addressed most frequently with 10 questionnaires addressing war/conflict and seven addressing family separation. Being beaten up by soldiers, police, militia or gangs was addressed by only one questionnaire, displacement by two and exposure to shootings/bombs/riots by three questionnaires. An overview of which form of adversity is assessed by which of these 14 questionnaires can be found in Figures 2a-2c.
Figure 2a.
Conventional ACEs addressed by identified questionnaires
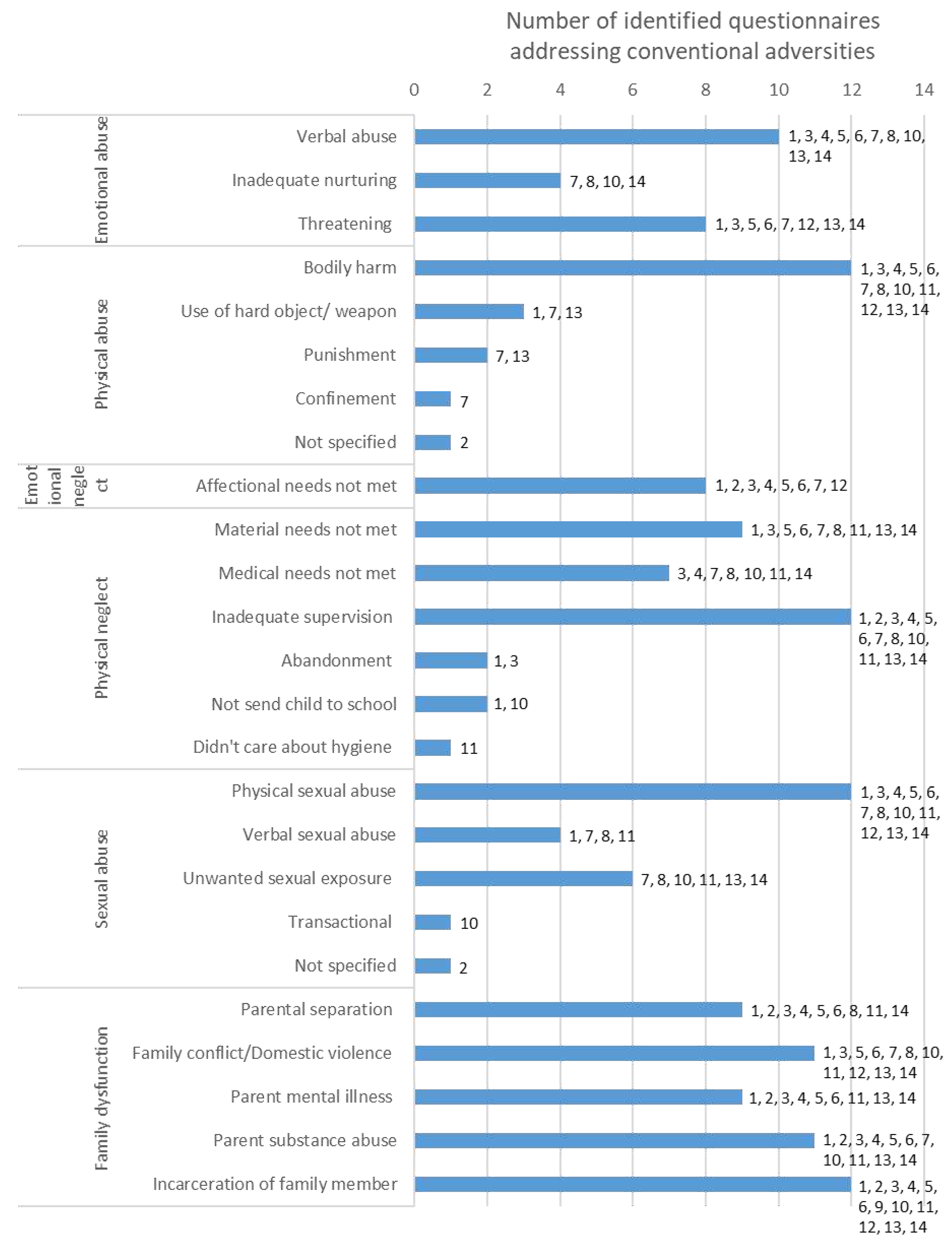
Figure 2b.
Expanded ACEs addressed by identified questionnaires
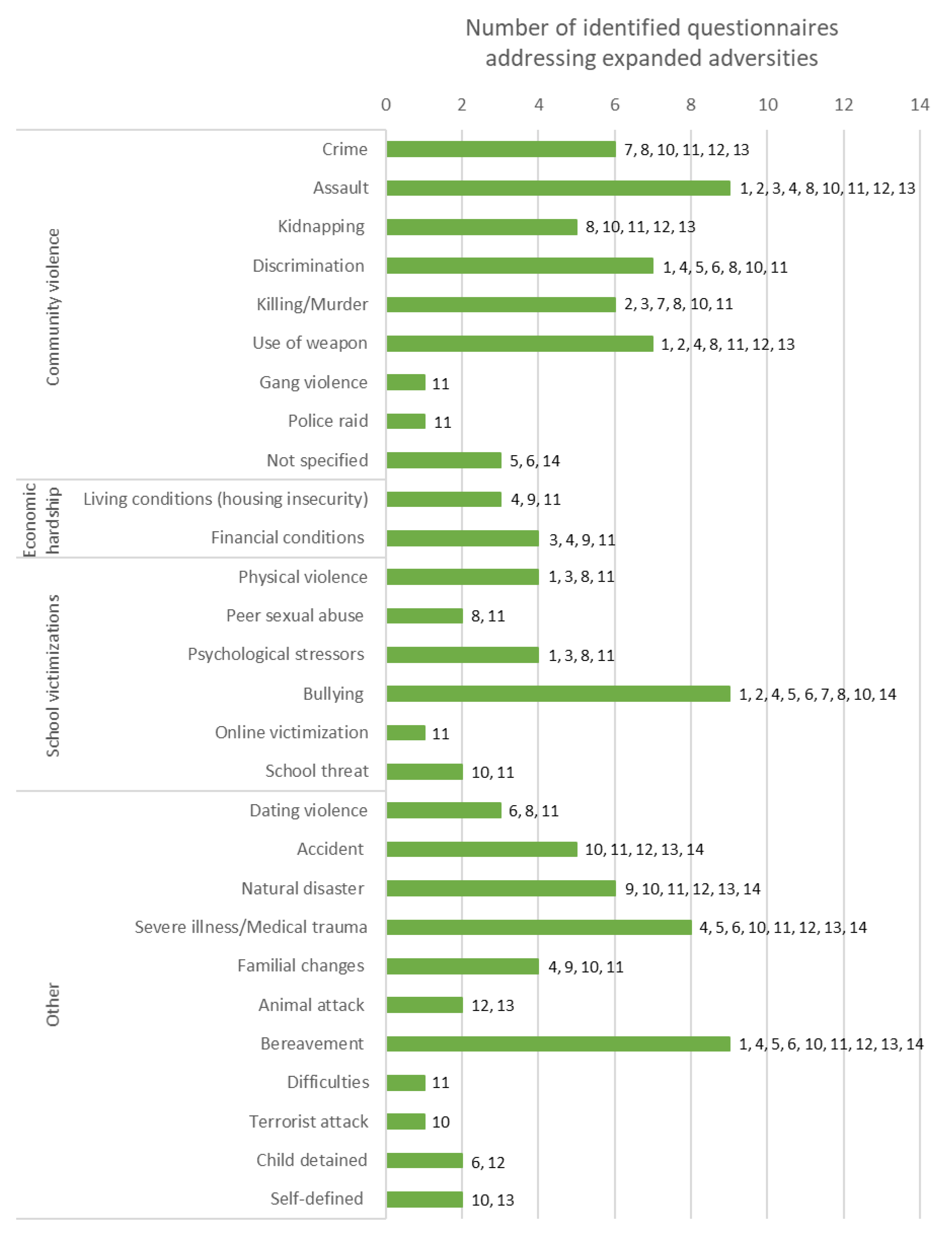
Figure 2c.
Refugee specific ACEs addressed by identified questionnaires
| Figures 2a-c | |
|
|
Within the identified 14 questionnaires, one to three questions addressed refugee-specific adversities, whereas other categories were addressed by up to 21 questions such as community violence in the National Surveys of Children’s Exposure to Violence (NatSCEV) [33]. In the NatSCEV, questions about community violence included "Has your child ever lived in a neighborhood where there were gangs?" as well as " At any time in your child’s life, has your child ever seen the police raid or enter a house in (his/her) neighborhood looking for a criminal or block off a place in (his/her) neighborhood because a crime happened there?" Table 2 shows the number of questions addressing each adversity category in each questionnaire.
Table 2: Adversity categories in identified questionnaires
Psychometrics and questionnaire quality
Very few articles reported any information related to the psychometric properties of the questionnaire used. From the 14 questionnaires that included a refugee-specific adversity, three questionnaires (JVQ, ICAST-C and ACEQ-R) had reported psychometric properties. In this review, these three questionnaires were used in more than one study; however, their psychometric properties were not always reported. For instance, as displayed in Table 3, the JVQ was used in 76 different studies, of which only 15 had reported internal consistency (cronbach’s alpha or Kruder and Richardson Formula 20), 8 reported inter-observer reliability (kappa adjunction) and only one reported content validity (reported via qualitative approach). The JVQ was originally developed in the USA and was used in nine countries beyond the USA within 39 studies identified in this review; yet only four identified studies reported the translation process. None of the studies reported retest reliability (interclass correlation coefficient value), criterion validity (correlation coefficient) or construct validity (convergent validity, discriminant validity or confirmatory factor analysis).

Table 3.
Reported psychometric properties of identified questionnaires
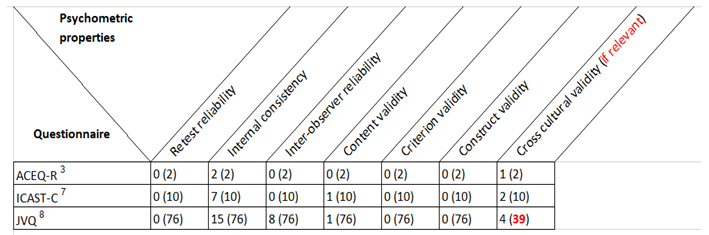
(Number of studies using the questionnaire in this review are indicated in brackets)
No psychometric properties were reported for remaining identified questionnaires 1, 2, 4-6, 9-14
|
|
Questionnaires used within a refugee population
In this review, two questionnaires were used to measure ACEs in refugee children, the first questionnaire was the ISPCAN Child Abuse Screening Tool-Child (ICAST-C), used as a self-report measure in one study with children in refugee camps in Rwanda and Uganda [46]. The other questionnaire was the ISPCAN Child Abuse Screening Tool-Parent (ICAST-P), applied in a study asking mothers about the adversities of their Palestinian children, some of whom were displaced refugees in the West Bank [47]. While the ICAST-C addresses refugee-specific ACEs, this is not the case with the ICAST-P.
Discussion
The purpose of this review was to determine if any of the existing questionnaires assessing ACEs also capture the diverse and unique adversities faced by refugee children and if so, to what extent. Further, we analysed which of the available ACE questionnaires had been applied in a refugee setting. This study identified 103 questionnaires that measure various adversity categories yet the core content included within the questionnaires differed, as did the questionnaire quality. Due to the high number of questionnaires identified, it has become apparent that ACEs are perceived globally as a problem. However, it seems that some vulnerable populations, such as refugee children, currently might go unrecognised.
Adversities measured
The range of adversities covered in questionnaires available today has expanded immensely since the conventional ACEs were first revealed in 1998 [2]. Not only do current adversities vary in source (the child’s family or environment) but also in severity and exposure (either witnessed or experienced). However, only 14 of the 103 identified questionnaires included a refugee-specific ACE. Examples of refugee-specific ACEs in the identified questionnaires included experiencing war, bombings, destruction, displacement, and separation from family due to immigration. However, it is important to consider that refugee children may also face adversities similar to the general public that are relevant to their circumstances, such as economic hardship, kidnapping, bereavement and discrimination [48,49].
Table 4 depicts an overview of potential ACEs that might be relevant to the refugee population based on previous research [50,51,52,53,54,55,56,57,58,59], including several adversity forms applicable to both the refugee and general population. For a better overview the figure below also shows which adversity forms have been covered by the 14 identified questionnaires that included at least one refugee-specific item. It becomes apparent that none of the identified questionnaires addressed all forms of adversities – furthermore, several forms of adversity relevant to refugee populations (such as military groups, immigration detention, immigration stress, and acculturation stress) were not addressed within any of the questionnaires identified in this study.
One questionnaire covered all the ACE categories employed in this review: the BARC Pediatric Adversity and Trauma Questionnaire [60] (see Table 2). However, when looking at the breakdown of adversities as depicted in Table 4 it is noticeable that certain issues are missing: kidnapping (a form of community violence), a reality many refugee children might face [49], is not addressed in the BARC questionnaire. Neither is financial difficulties [61], displacement [51], or immigration process [57], all common refugee adversities acknowledged in earlier research.
Furthermore, taking a closer look at the extent to which refugee-specific ACEs are measured in the 14 identified questionnaires, it is noticeable that their measure is limited with a maximum of three refugee-specific questions. For example, the NatSCEV, only addressed refugee-specific ACEs with three questions (war/conflict, shootings/bombs/riots and family separation) while community violence and family disfunction were addressed with 21 and 18 questions respectively, as shown in Table 2. Six of the 14 questionnaires used two questions to ask about refugee-specific ACEs [62], another six tools used only one question [63]. Additionally, the majority of questionnaires addressed refugee-specific ACEs by asking about exposure to war/conflict and/or separation from family. Despite the damaging influence of such exposures, they are not the sole sources of adversity among refugee children. It is therefore unjust to simplify refugee specific adversities into three questions or less. Simply addressing only a few forms of adversities understates the gravity of the refugee experiences, as well as their mental and physical consequences.
It was also noticeable that the questionnaires addressing refugee-specific adversities focused on pre-flight and flight stressors. The tragedies refugee children experience are not only occurring in their home countries, but also on the dangerous route to safety, and in their host countries [64]. In some circumstances, the adversities faced post-flight have caused more of a negative impact on refugee’s wellbeing than that of war and conflict [65,66].
In addition, it is important to acknowledge that factors on multiple levels could be a source of adversity. These factors could arise from the individuals themselves, their families, community or society, such as psychological vulnerabilities, impaired parenting, community tensions or national policies that adversely affect refugee children. However, looking at potential factors arising from all sources with one questionnaire appears to be uncommon in ACE research.
This demonstrates that even in the 14 identified questionnaires, the refugee-specific ACEs are not capturing the full range of adversities these children may encounter. However, it has to be acknowledged that the identified questionnaires were not developed for refugee children and their importance should not be diminished in any way. It becomes apparent, nevertheless, that a gap exists concerning measuring refugee children’s adversities.
Questionnaire Quality
Most articles in this review provided little information about the psychometric properties of questionnaires used. Taking a deeper look at studies identified in this review that used a questionnaire evaluating refugee-specific ACEs, only three out of 14 questionnaires had psychometric properties reported, with several psychometric aspects lacking [67]. In some cases articles stated that the psychometric properties were reliable due to the extensive use of the questionnaire in previous studies [68]. In other cases, vague statements such as the questionnaire has shown “acceptable psychometric properties” [69], were not sufficient to estimate the quality of the tool. The articles that did provide some details about psychometric properties mainly reported on internal consistency, as shown in Table 3. This assesses whether the items of a questionnaire measure the same characteristic, usually by providing a Cronbach’s alpha value. However a Cronbach’s alpha value is greatly affected by the number of items in the questionnaire, by simply increasing the number of items the alpha values are also increased, this alone is not enough to assess the questionnaire quality [32].
Additionally, there was an underreporting of cross-cultural validity of the questionnaires. In those few studies reporting on cross-cultural validity, only the translation method, e.g. forward translation [70] or back translation [71], was described, yet the tool’s adaptability in a new cultural setting was described in none of the identified studies that used the questionnaires in a setting different from its original intent. To minimise bias when the questionnaire is administered in a different language and context, cross-cultural adaptation is essential, and this entails both linguistic and cultural considerations [72].
While psychometric properties for the respective questionnaires might be published elsewhere not included in this review, the missing report of properties within the studies identified in this review still is problematic because reliability and validity are subject to change according to the context, study type, population and purpose of the study [32].
Generally, questionnaires should meet valid and reliable criteria by measuring its psychometric properties to ensure that the questionnaire measures what it proposes and reproduces the same results over time [32]. Research has also indicated that the evidence regarding psychometric properties of adversity questionnaires is limited and usually of lower quality [73,74]. To collect accurate data, researchers should also take into account factors that influence the quality of information such as the respondent characteristics, for instance age or cultural appropriateness [24]. Consequences of ACEs might be obscured due to the variable validity and reliability of existing questionnaires. Thus, it is imperative that the psychometric properties of questionnaires, including, if applicable, cross-cultural validity, are evaluated, to ensure that the information obtained in a study is valid and reliable and can thus be used to assist in decision-making.
Questionnaires used within a refugee setting
Despite the magnitude of the humanitarian crisis that affects every continent [75], research to evaluate ACEs with standardised tools in refugee children is negligible. Only two questionnaires were used to measure ACEs in refugee children. The questionnaires used were the ICAST-P and ICAST-C, tools developed through a global collaborative effort guided by the International Society for the Prevention of Child Abuse & Neglect (ISPCAN). The ICAST questionnaires are ISPCAN's effort to provide a common tool for systematically comparing recorded incidences of all types of violence against children across cultures and time, in order to provide a more accurate and representative picture of the global problem [39]. Since the ICAST is a global endeavour it has been translated and tested in at least 20 languages [39]. In this review, the ICAST-P was used in Arabic in Palestine and the ICAST-C was used in Kinyarwanda for Rwanda and Dinka and Nuer for Uganda.
The study which used the ICAST-P, a tool with 39 questions in total, aimed to assess the prevalence of child abuse in the West Bank, of which 30.4% of the participants were refugees, and to determine some of its social and political associated factors [47]. The ICAST-P only measures three (emotional and physical abuse and neglect, economic hardship and sexual abuse) of the adversity forms depicted in Table 4 and does not address a single refugee-specific adversity [39], however that was not the goal of the identified study.
On the other hand, the study using the ICAST-C (a questionnaire with 61 items) aimed to understand patterns of violence against children in refugee camps, and associations with adverse mental health outcomes [46]. While the ICAST-C does address a refugee-specific adversity form (using only one question regarding the exposure to war/conflict), and six further adversity forms relevant to refugee children, as illustrated in Table 4, it still overlooks important struggles refugees may experience pre-flight, during flight, and post-flight specifically discrimination and economic hardship.
With a continuously growing refugee population, and previous research suggesting mental and physical health disorders related to traumatic experiences refugee children encounter [76], incorporating the adversities affecting their wellbeing into ACE questionnaires becomes highly important.
Limitations and strengths
This is the first systematic review evaluating whether and to what extent existing ACE questionnaires can be used to identify the adversities of refugee children. However, a few limitations affect this review: Some existing questionnaires might not have been identified because our search was limited to articles published in English, thus limiting the international scope of the review. Additionally, articles were excluded if some respondents were outside the desired age range because they did not fit the definition of a child, thus inferring that the questionnaire is not explicitly designed for children. This review may also be subjected to publication bias, as searches outside the mentioned databases were not made. A final limitation is that information about the modifications made by certain studies to the original version of questionnaires were not collected.
Despite these limitations, we were able to use explicit methodology to identify 14 questionnaires on a global level that assess at least one refugee-specific ACE in children. The results provide a detailed overview of assessed forms of adversities categorized into domains to assist future researchers in identifying useful questionnaires. Additionally, this review draws attention to the existing gaps and the need for a questionnaire that addresses the unique adversities of refugee children.
Conclusion
This review shows that regardless of the availability of numerous questionnaires there is no one-size-fits-all measure for every situation. It also illustrates that there is a need for further psychometric development for most measures. However, the most important finding is that that there is a need to incorporate adversity measures for the most vulnerable populations, specifically refugee children. Existing questionnaires are limited in terms of the extent they address refugee adversities. Given the importance and seriousness of ongoing crises that result in the displacement of children, inclusion of adversities relevant to refugees will allow for further understanding of how ACEs affect these children’s wellbeing and enable the identification of those at risk.
References
- Adebowale, V., et al., Addressing Adversity, in Prioritising adversity and trauma-informed care for children and young people in England, M. Bush, Editor. 2018, The YoungMinds Trust: Great Britain. p. 372.
- Felitti, V.J., et al., Relationship of Childhood Abuse and Household Dysfunction to Many of the Leading Causes of Death in Adults The Adverse Childhood Experiences (ACE) Study. American Journal of Preventive Medicine, 1998. 14(4): p. 1. [CrossRef]
- Zeanah, P.; Burstein, K.; Cartier, J. Addressing adverse childhood experiences: It’s all about relationships. Societies 2018, 8, 115. [Google Scholar] [CrossRef]
- Hillis, S. Global Prevalence of Past-year Violence Against Children: A Systematic Review and Minimum Estimates. Pediatrics, 2016. 137(3): p. e20154079. [CrossRef]
- Kia-Keating, M.; et al. Trauma-responsive care in a pediatric setting: Feasibility and acceptability of screening for adverse childhood experiences. Am. J. Community Psychol. 2019, 64, 286–297. [Google Scholar] [CrossRef] [PubMed]
- Hagan, M.J., M.J. Sulik, and A.F. Lieberman, Traumatic Life Events and Psychopathology in a High Risk, Ethnically Diverse Sample of Young Children: A Person-Centered Approach. Journal of Abnormal Child Psychology, 2016. 44(5): p. 833-844. [CrossRef]
- Lipscomb, S.T., et al., Adverse childhood experiences and children's development in early care and education programs. Journal of Applied Developmental Psychology, 2021. 72: p. 101218. [CrossRef]
- Cronholm, P.F.; Forke, C.M.; Wade, R.; Bair-Merritt, M.H.; Davis, M.; Harkins-Schwarz, M.; Pachter, L.M.; Fein, J.A. Adverse childhood experiences: Expanding the concept of adversity. American journal of preventive medicine 2015, 49, 354–361. [Google Scholar] [CrossRef] [PubMed]
- Lopez, M.; Ruiz, M.O.; Rovnaghi, C.R.; Tam, G.K.; Hiscox, J.; Gotlib, I.H.; Barr, D.A.; Carrion, V.G.; Anand, K.J. The social ecology of childhood and early life adversity. Pediatric research 2021, 89, 353–367. [Google Scholar] [CrossRef] [PubMed]
- Ellis, W.R. and W.H. Dietz, A New Framework for Addressing Adverse Childhood and Community Experiences: The Building Community Resilience Model. Academic Pediatrics, 2017. 17(7, Supplement): p. S86-S93. [CrossRef]
- Bethell, C.D.; et al. Methods to Assess Adverse Childhood Experiences of Children and Families: Toward Approaches to Promote Child Well-being in Policy and Practice. Academic Pediatrics, 2017. 17(7, Supplement): p. S51-S69. [CrossRef]
- Karam, E.G.; Fayyad, J.A.; Farhat, C.; Pluess, M.; Haddad, Y.C.; Tabet, C.C.; Farah, L.; Kessler, R.C. Role of childhood adversities and environmental sensitivity in the development of post-traumatic stress disorder in war-exposed Syrian refugee children and adolescents. The British Journal of Psychiatry 2019, 214, 354–360. [Google Scholar] [CrossRef] [PubMed]
- UNHCR. Refugee facts: What is a Refugee? 2021 30.06.2022]. Available online: https://www.unrefugees.org/refugee-facts/what-is-a-refugee/.
- UNHCR. Refugee Data Finder. Key Indicators 2022 16.06.2022 25.06.2022]. Available online: https://www.unhcr.org/refugee-statistics/.
- UNICEF. Two million refugee children flee war in Ukraine in search of safety across borders. 2022 30.03.2022 24.10.2002]. Available online: https://www.unicef.org/press-releases/two-million-refugee-children-flee-war-ukraine-search-safety-across-borders.
- Nations, U. Peace and Conflict Resolution. 07.09.2022]. Available online: https://www.un.org/en/academic-impact/peace-and-conflict-resolution.
- NCTSN. About Refugees 24.08.2022]. Available online: https://www.nctsn.org/what-is-child-trauma/trauma-types/refugee-trauma/about-refugees.
- Vaghri, Z.; Tessier, Z.; Whalen, C. Refugee and Asylum-Seeking Children: Interrupted Child Development and Unfulfilled Child Rights. Children (Basel) 2019, 6. [Google Scholar] [CrossRef] [PubMed]
- Frounfelker, R.L.; Miconi, D.; Farrar, J.; Brooks, M.A.; Rousseau, C.; Betancourt, T.S. Mental Health of Refugee Children and Youth: Epidemiology, Interventions, and Future Directions. Annual Review of Public Health 2020, 41, 159–176. [Google Scholar] [CrossRef] [PubMed]
- Turney, K. Cumulative adverse childhood experiences and children’s health. Children and Youth Services Review 2020, 119, 105538. [Google Scholar] [CrossRef]
- Brown, S.M.; Rienks, S.; McCrae, J.S.; Watamura, S.E. The co-occurrence of adverse childhood experiences among children investigated for child maltreatment: A latent class analysis. Child abuse & neglect 2019, 87, 18–27. [Google Scholar] [CrossRef]
- Pieper, D.; Puljak, L. Language restrictions in systematic reviews should not be imposed in the search strategy but in the eligibility criteria if necessary. Journal of Clinical Epidemiology 2021, 132, 146–147. [Google Scholar] [CrossRef]
- Assembly, U.N.G. Convention on the Rights of the Child. 1989 [cited 2022. Available online: https://www.unicef.org/child-rights-convention/convention-text#.
- Choi, B.C.; Pak, A.W. Peer reviewed: a catalog of biases in questionnaires. Preventing chronic disease 2005, 2. [Google Scholar]
- Community Violence. 24.08.2022]. Available online: https://www.nctsn.org/what-is-child-trauma/trauma-types/community-violence.
- Leventhal, T. and J. Brooks-Gunn, Poverty and Child Development, in International Encyclopedia of the Social & Behavioral Sciences, N.J. Smelser and P.B. Baltes, Editors. 2001, Pergamon: Oxford. p. 11889-11894.
- Braveman, P.; Heck, K.; Egerter, S.; Rinki, C.; Marchi, K.; Curtis, M. Economic Hardship in Childhood: A Neglected Issue in ACE Studies? Maternal and child health journal 2018, 22, 308–317. [Google Scholar] [CrossRef] [PubMed]
- Ostrov, J.M. and K.J. Perry, Bullying and Peer Victimization in Early Childhood, in Encyclopedia of Infant and Early Childhood Development (Second Edition), J.B. Benson, Editor. 2020, Elsevier: Oxford. p. 228-235.
- Ray, D.C.; Angus, E.; Robinson, H.; Kram, K.; Tucker, S.; Haas, S.; McClintock, D. Relationship between adverse childhood experiences, social-emotional competencies, and problem behaviors among elementary-aged children. Journal of child and adolescent counseling 2020, 6, 70–82. [Google Scholar] [CrossRef]
- Abdelhamid, S., et al., Voices of the displaced: A qualitative study of potentially traumatising and protective experiences faced by refugee children. medRxiv, 2022: p. 2022.07.26.22277918. [CrossRef]
- Laurin, J.; Wallace, C.; Draca, J.; Aterman, S.; Tonmyr, L. Youth self-report of child maltreatment in representative surveys: a systematic review. Health promotion and chronic disease prevention in Canada : research, policy and practice 2018, 38, 37–54. [Google Scholar] [CrossRef] [PubMed]
- Souza, A.C.d.; Alexandre, N.M.C.; Guirardello, E.d.B.; Souza, A.C.d.; Alexandre, N.M.C.; Guirardello, E.d.B. Psychometric properties in instruments evaluation of reliability and validity [Propriedades psicométricas na avaliação de instrumentos: avaliação da confiabilidade e da validade]. Epidemiology and Health Services [Epidemiologia e Serviços de Saúde] 2017, 26, 649–659. [Google Scholar] [CrossRef]
- Finkelhor, D. and H. Turner. National Survey of Children's Exposure to Violence III, 1997-2014 [United States] (ICPSR 36523). 2016 [cited 2022 17/10/2022]. Available online: https://www.icpsr.umich.edu/web/NACJD/studies/36523.
- WHO. Adverse Childhood Experiences International Questionnaire (ACE-IQ). 2020 28.01.2020 28.10.2022]. Available online: https://www.who.int/publications/m/item/adverse-childhood-experiences-international-questionnaire-(ace-iq).
- Selvaraj, K.; Ruiz, M.J.; Aschkenasy, J.; Chang, J.D.; Heard, A.; Minier, M.; Osta, A.D.; Pavelack, M.; Samelson, M.; Schwartz, A. , et al. Screening for Toxic Stress Risk Factors at Well-Child Visits: The Addressing Social Key Questions for Health Study. The Journal of pediatrics 2019, 205, 244–249. [Google Scholar] [CrossRef] [PubMed]
- Finkelhor, D.; Shattuck, A.; Turner, H.; Hamby, S. A revised inventory of Adverse Childhood Experiences. Child Abuse & Neglect 2015, 48, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Koita, K.; Long, D.; Hessler, D.; Benson, M.; Daley, K.; Bucci, M.; Thakur, N.; Burke Harris, N. Development and implementation of a pediatric adverse childhood experiences (ACEs) and other determinants of health questionnaire in the pediatric medical home: A pilot study. PloS one 2018, 13, e0208088–e0208088. [Google Scholar] [CrossRef] [PubMed]
- Wellness, C.f.Y. ACE-Q Materials. 2015 26.10.2022]. Available online: https://centerforyouthwellness.org/aceq-pdf/.
- ISPCAN. ISPCAN Child Abuse Screening Tools (ICAST). 2020 25.08.2022]. Available online: https://www.ispcan.org/learn/icast-abuse-screening-tools/?v=402f03a963ba.
- Finkelhor, D.; Hamby, S.L.; Ormrod, R.; Turner, H. The Juvenile Victimization Questionnaire: reliability, validity, and national norms. Child abuse & neglect 2005, 29, 383–412. [Google Scholar]
- Merrick, M.T.; Henly, M.; Turner, H.A.; David-Ferdon, C.; Hamby, S.; Kacha-Ochana, A.; Simon, T.R.; Finkelhor, D. Beyond residential mobility: A broader conceptualization of instability and its impact on victimization risk among children. Child abuse & neglect 2018, 79, 485–494. [Google Scholar] [CrossRef]
- Pynoos, R.S. and A.M. Steinberg, UCLA PTSD Reaction Index for DSM-5 (e-mail from Alan to first author). 2021. p. 28.
- Ford, J., et al., Traumatic events screening inventory for children (TESI-C) Version 8.4. National Center for PTSD and Dartmouth Child Psychiatry Research Group, 2002.
- Ghosh-Ippen, C., et al., Trauma events screening inventory-parent report revised. San Francisco: The Child Trauma Research Project of the Early Trauma Network and The National Center for PTSD Dartmouth Child Trauma Research Group, 2002.
- Hudziak, J. and J. Kaufman. Yale-Vermont Adversity in Childhood Scale (Y-VACS): Adult, Child, Parent, & Clinician Questionnaires. 2014. Available online: https://www.kennedykrieger.org/sites/default/files/library/documents/faculty/Y-VACS_Child_Self-Report_4.2020.pdf.
- Meyer, S.; Yu, G.; Hermosilla, S.; Stark, L. Latent class analysis of violence against adolescents and psychosocial outcomes in refugee settings in Uganda and Rwanda. Global Mental Health 2017, 4. [Google Scholar] [CrossRef] [PubMed]
- Harsha, N.; Lynch, M.A.; Giacaman, R. Child abuse in the West Bank of the occupied Palestinian territory (WB/oPt): social and political determinants. BMC public health 2020, 20, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Fazel, M.; Reed, R.V.; Panter-Brick, C.; Stein, A. Mental health of displaced and refugee children resettled in high-income countries: risk and protective factors. Lancet 2012, 379, 266–282. [Google Scholar] [CrossRef] [PubMed]
- Dehnel, R.; Dalky, H.; Sudarsan, S.; Al-Delaimy, W.K. Resilience and mental health among Syrian refugee children in Jordan. Journal of Immigrant and Minority Health 2022, 24, 420–429. [Google Scholar] [CrossRef] [PubMed]
- Scharpf, F.; Kaltenbach, E.; Nickerson, A.; Hecker, T. A systematic review of socio-ecological factors contributing to risk and protection of the mental health of refugee children and adolescents. Clinical Psychology Review 2021, 83, 101930. [Google Scholar] [CrossRef] [PubMed]
- Mangrio, E.; Zdravkovic, S.; Carlson, E. A qualitative study of refugee families’ experiences of the escape and travel from Syria to Sweden. BMC Research Notes 2018, 11, 594. [Google Scholar] [CrossRef]
- cFarlane, C.A.; Kaplan, I.; Lawrence, J.A. Psychosocial Indicators of Wellbeing for Resettled Refugee Children and Youth: Conceptual and Developmental Directions. Child Indicators Research 2011, 4, 647–677. [Google Scholar] [CrossRef]
- Sim, A.; Fazel, M.; Bowes, L.; Gardner, F. Pathways linking war and displacement to parenting and child adjustment: A qualitative study with Syrian refugees in Lebanon. Social Science & Medicine 2018, 200, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Porter, M.; Haslam, N. Predisplacement and Postdisplacement Factors Associated With Mental Health of Refugees and Internally Displaced PersonsA Meta-analysis. JAMA 2005, 294, 602–612. [Google Scholar] [CrossRef] [PubMed]
- McGregor, L.S.; Melvin, G.A.; Newman, L.K. An exploration of the adaptation and development after persecution and trauma (ADAPT) model with resettled refugee adolescents in Australia: A qualitative study. Transcultural Psychiatry 2016, 53, 347–367. [Google Scholar] [CrossRef]
- Sleijpen, M.; Mooren, T.; Kleber, R.J.; Boeije, H.R. Lives on hold: A qualitative study of young refugees’ resilience strategies. Childhood 2017, 24, 348–365. [Google Scholar] [CrossRef] [PubMed]
- urtis, P.; Thompson, J.; Fairbrother, H. Migrant children within Europe: a systematic review of children's perspectives on their health experiences. Public Health 2018, 158, 71–85. [Google Scholar] [CrossRef]
- Lindner, K.; Hipfner-Boucher, K.; Yamashita, A.; Riehl, C.M.; Ramdan, M.A.; Chen, X. Acculturation through the lens of language: Syrian refugees in Canada and Germany. Applied Psycholinguistics 2020, 41, 1351–1374. [Google Scholar] [CrossRef]
- Filler, T.; Georgiades, K.; Khanlou, N.; Wahoush, O. Understanding Mental Health and Identity from Syrian Refugee Adolescents’ Perspectives. International Journal of Mental Health and Addiction 2021, 19, 764–777. [Google Scholar] [CrossRef]
- !!! INVALID CITATION !!! [37].
- Culbertson, S. and L. Constant, Education of Syrian Refugee Children: Managing the crisis in Turkey, Lebanon and Jordan. 2015: RAND Corporation.
- !!! INVALID CITATION !!! [36, 37, 40, 42-44].
- !!! INVALID CITATION !!! [35, 38, 39, 41, 45].
- Wood, S.; et al. Adverse Childhood Experiences in child refugee and asylum seeking populations. 2020.
- Henley, J.; Robinson, J. Mental health issues among refugee children and adolescents. Clinical Psychologist 2011, 15, 51–62. [Google Scholar] [CrossRef]
- Zwi, K. Refugee children and their health, development and well-being over the first year of settlement: A longitudinal study. Journal of Paediatrics and Child Health, 2017. 53(9): p. 841-849. [CrossRef]
- !!! INVALID CITATION !!! [36, 39, 40].
- Jiang, H.; Hu, H.; Zhu, X.; Jiang, H. Effects of school-based and community-based protection services on victimization incidence among left-behind children in China. Children & Youth Services Review 2019, 101, 239–245. [Google Scholar] [CrossRef]
- Li, X.; You, J.; Ren, Y.; Zhou, J.; Sun, R.; Liu, X.; Leung, F. A longitudinal study testing the role of psychache in the association between emotional abuse and suicidal ideation. Journal of Clinical Psychology 2019, 75, 2284–2292. [Google Scholar] [CrossRef]
- Miller-Graff, L.E.; Scheid, C.R.; Guzmán, D.B.; Grein, K. Caregiver and family factors promoting child resilience in at-risk families living in Lima, Peru. Child Abuse & Neglect 2020, 108, 104639. [Google Scholar] [CrossRef] [PubMed]
- Ward, C.L.; Artz, L.; Leoschut, L.; Kassanjee, R.; Burton, P. Sexual violence against children in South Africa: a nationally representative cross-sectional study of prevalence and correlates. The Lancet. Global health 2018, 6, e460–e468. [Google Scholar] [CrossRef]
- Gjersing, L.; Caplehorn, J.R.; Clausen, T. Cross-cultural adaptation of research instruments: language, setting, time and statistical considerations. BMC medical research methodology 2010, 10, 1–10. [Google Scholar] [CrossRef]
- Yoon, S.; Speyer, R.; Cordier, R.; Aunio, P.; Hakkarainen, A. A systematic review evaluating psychometric properties of parent or caregiver report instruments on child maltreatment: Part 1: Content validity. Trauma, Violence, & Abuse 2021, 22, 1013–1031. [Google Scholar]
- Yoon, S.; Speyer, R.; Cordier, R.; Aunio, P.; Hakkarainen, A. A systematic review evaluating psychometric properties of parent or caregiver report instruments on child maltreatment: Part 2: Internal consistency, reliability, measurement error, structural validity, hypothesis testing, cross-cultural validity, and criterion validity. Trauma, Violence, & Abuse 2021, 22, 1296–1315. [Google Scholar]
- Relations’s, C.o.F. Global Conflict Tracker. 07.09.2022]. Available online: https://www.cfr.org/global-conflict-tracker.
- Fazel, M.; Stein, A. The mental health of refugee children. Archives of Disease in Childhood 2002, 87, 366. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Method of identifying articles and questionnaires (adapted from the PRISMA flow diagram)
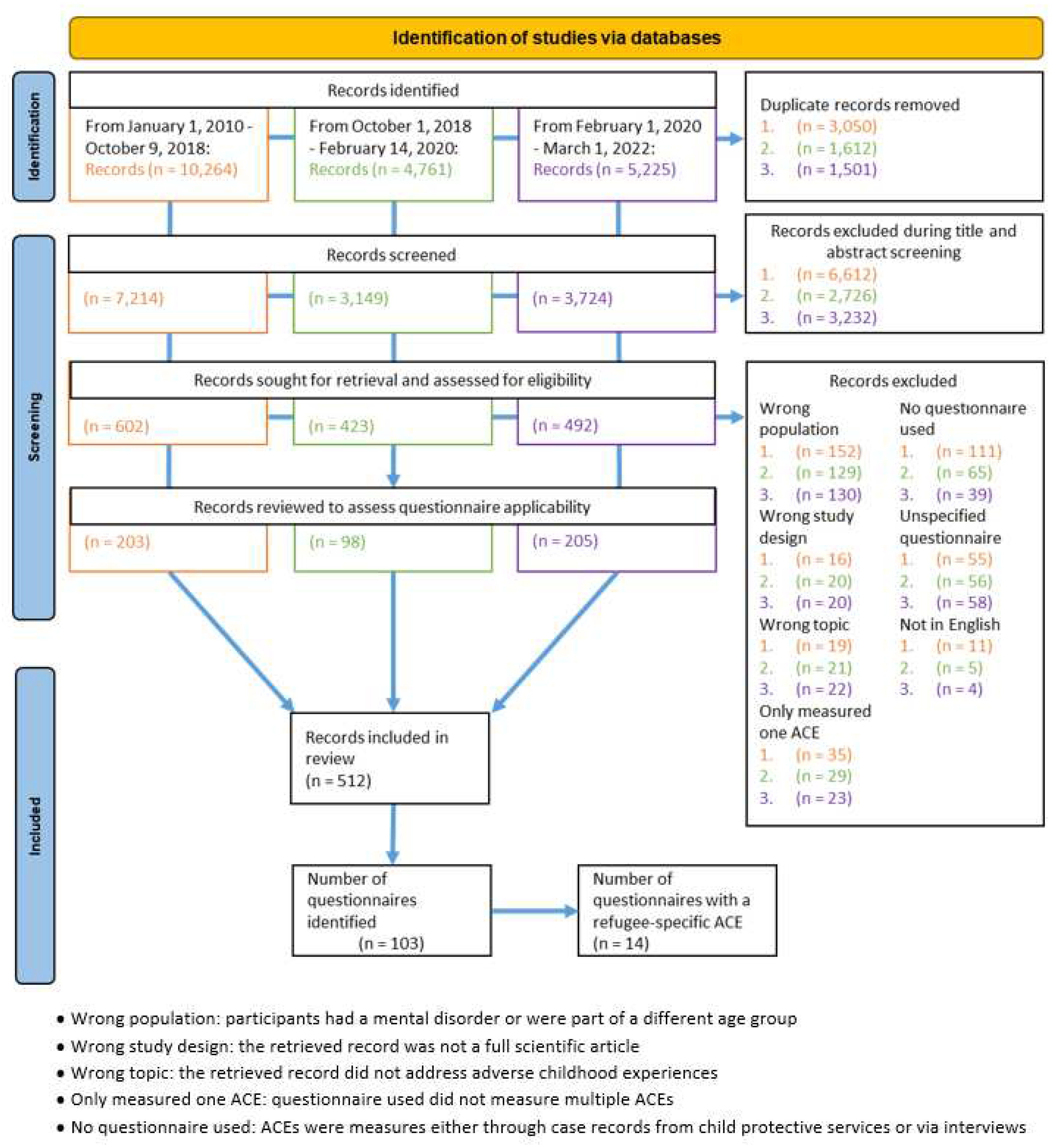
Table 1.
ACE categories and forms of adversities
| ACE Category | Forms of adversities |
|---|---|
| Conventional ACEs | |
| Emotional abuse |
A child's family member: • Verbal abuse: swore, insulted or put them down • Threatening: behaved in a way that made the child fearful they would be physically harmed • Inadequate nurturing: says things such as not wanting the child or wished the child were dead • Torment: afflicts mental suffering by hurting the child’s pet, withholding a meal, or singling out the child to do chores |
| Physical abuse | A child’s family member: • Bodily harm: pushed, grabbed, slapped, etc. the child • Use or hard object/weapon: hit child with a belt, cord, etc. or cut child with sharp object • Punishment: harsh treatment as a retribution for an offence such as wash mouth with soap or pepper, child dug, slashed a field, or other labour as punishment • Confinement: tied the child up, gagged the child, blindfolded them, or locked them in a closet or a dark place |
| Emotional neglect |
|
| Physical neglect |
The failure, refusal or inability on the part of a caregiver, for reasons other than poverty, to provide for their child’s • Material needs: child sometimes went without food, clothing, shelter or protection • Medical needs: child not taken to the doctor when sick • Supervisory needs: parents do not ensure a safe place for child to stay, child left at home alone, or child is left in charge of younger siblings for long periods of time |
| Sexual abuse |
• Physical sexual abuse: someone attempted to have sexual intercourse with the child, touched the child’s private parts, or asked child to touch their private parts in a sexual way that was unwanted, uncomfortable or against child’s will • Verbal sexual abuse: someone said/wrote something sexual about the child, talked to child in a sexual way or made sexual comments about child’s body • Unwanted sexual exposure: someone attempted or made child watch sexual things (e.g. magazines, pictures, videos, internet sites), made child look at their private parts or wanted child to look at theirs, took sexual picture/video of child, or child was present when someone was being forced to engage in sexual activity • Threatening: someone threaten to have sex with child, or hurt/tell lies about them unless they did something sexual • Transactional: child traded sex or sexual activity to receive money, food, drugs, alcohol, a place to stay, or anything else. |
| Family dysfunction | • Parental separation or divorce: child’s parents are divorced or separated • Domestic violence: child witnessed a parent hit, slap, kick, push or physically hurt another parent or siblings, child has seen or heard family members arguing very loudly or threaten to seriously harm each other • Mental illness: a family member was depressed, mentally ill, or (attempted) suicide • Substance abuse: a family member is a problem drinker/alcoholic or uses street drugs • Incarceration: a family member served time in jail or was or taken away (by police, soldiers, or other authorities) |
| Community violence |
Interpersonal violence committed in public areas by individuals who are not intimately related to the child. Examples include • Crime: robbery, theft, vandalism, exposure to drug activity • Assault: child witnessed or was exposed to being attacked with/without an object or weapon • Kidnaping: child was kidnaped • Discrimination: child was hit or attacked verbally because of skin colour, religion, family origin, physical condition, or sexual orientation • Killing: hear about/witness to murder • Use of a weapon: hearing about/witness to random shootings/stabbings |
| Economic hardship | Child’s family facing financial hardship: • Financial instability: income loss, unemployment, job instability, not being able to afford food and necessities • Housing insecurity: child was living in a car, a homeless shelter, a battered women’s shelter, or on the street |
| School victimisations |
• Physical violence: another child and/or teacher physically hit, kicked, pushed, taken things forcibly from the child • Psychological stressors: another child and/or teacher emotionally mistreats a child by social exclusion, threatening relationship termination, gossip and secret spreading • Sexual offence: another child or teen pressures the child to so sexual things or did something sexual to child against their wishes • Bullying: child threatened or harassed by a bully • Online victimisations: cyber bullying or online sexual harassment |
| Other |
• Dating violence: being hit, verbally hurt or controlled by partner • Accident: experience/witness a serious car/bicycle accident, near drowning experience or fire • Natural disaster: child experiences a disaster such as a tornado, hurricane, big earthquake, flood or mudslide • Severe illness/Medical trauma: child or loved one had to undergo frightening medical treatment or was hospitalized for a long time period • Animal attack: child badly hurt by an animal • Bereavement: death of someone close to the child • Familial changes: child completely separated from parent/caregiver for a long time under very stressful circumstances, such as going to a foster home, the parent living far apart from him/her, or never seeing the parent again. Addition of third adult to family (e.g. marriage of parent to step-parent) • Child detained: child was detained, arrested or incarcerated • Difficulties: move to a new school, home, or town, repeat a grade in school, etc. |
| Refugee-specific adversities |
• War/conflict: child is exposed to war or conflict • Shootings, bombs and riots: child could see or hear people being shot, bombs going off, or street riots • Displacement: child is forced to flee their home • Beaten up by soldiers, police, militia, or gangs: child is hurt badly by armed adults • Family separation: child is separated from their caregiver due to immigration or war |
Table 2.
Adversity categories in identified questionnaires
| Name of Questionnaire | Adversity categories | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Emotional abuse | Physical abuse | Emotional neglect | Physical neglect | Sexual abuse | Family dysfunction | Community Violence | Economic Hardship | School victimizations | Other | Refugee-specific adversity | |
| ACE-International Questionnaire (ACE-IQ) [34] | 2 | 2 | 1 | 4 | 4 | 7 | 4 | 1 | 1 | 3 | |
| Addressing Social Key (ASK) Questions for Health Questionnaire [35] | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 1 | 1 | 1 | |
| Adverse Childhood Experience Questionnaire-Revised (ACEQ-R) [36] | 1 | 1 | 4 | 4 | 4 | 16 | 2 | 2 | 11 | 2 | |
| BARC Pediatric Adversity and Trauma Questionnaire [37] | 1 | 1 | 1 | 1 | 1 | 5 | 2 | 2 | 1 | 3 | 2 |
| Center for Youth Wellness ACE-Questionnaire (CYW ACE-Q Child) [38] | 1 | 1 | 1 | 1 | 1 | 5 | 2 | 1 | 3 | 1 | |
| Center for Youth Wellness ACE-Questionnaire (CYW ACE-Q Teen) [38] | 1 | 1 | 1 | 1 | 1 | 5 | 2 | 1 | 5 | 1 | |
| ISPCAN Child Abuse Screening Tool (ICAST-C) [39] | 7 | 8 | 3 | 4 | 6 | 4 | 2 | 1 | 1 | ||
| Juvenile Victimization Questionnaire (JVQ) [40] | 1 | 1 | 1 | 7 | 3 | 13 | 5 | 1 | 2 | ||
| Lifetime Destabilizing Factor (LDF) Index [41] | 1 | 2 | 2 | 1 | |||||||
| Modified UCLA Trauma History Profile [42] | 1 | 1 | 1 | 3 | 2 | 4 | 2 | 6 | 2 | ||
| National Surveys of Children’s Exposure to Violence (NatSCEV) [33] | 1 | 5 | 7 | 18 | 21 | 2 | 17 | 9 | 3 | ||
| Traumatic Events Screening Inventory for Children (TESI-C) [43] | 1 | 1 | 1 | 1 | 3 | 4 | 6 | 2 | |||
| Traumatic Events Screening Inventory for Children (TESI-PRR) [44] | 2 | 1 | 1 | 2 | 4 | 3 | 9 | 2 | |||
| Yale-Vermont Adverse Childhood Experiences Scale (Y-VACS) [45] | 1 | 1 | 1 | 2 | 5 | 1 | 1 | 7 | 1 | ||
| (Values indicate the number of questions addressing each adversity category in the questionnaire) | |||||||||||
Table 4.
Migration stages in which refugee-relevant ACEs occurred (based on previous research [50,51,52,53,54,55,56,57,58,59])
| Stage of migration | ||||
| Refugee relevant ACES | Pre-flight | Flight | Post-flight | |
| War/Conflict 1, 3, 4, 7, 8, 10-14 | ||||
| Shootings/bombs & riots 3, 8, 11 | ||||
| Destruction of infrastructure | ||||
| Presence of militant groups | ||||
| Displacement1, 10 | ||||
| Deprivation of basic necessities 3, 9, 11 | ||||
| Beaten up by police/soldiers/militia etc. 1 | ||||
| Witnessing/Experiencing violence 1-8, 10-14 | ||||
| Kidnapping 8, 10-13 | ||||
| Extortion/exploitation/fraud | ||||
| Housing insecurity 4, 9, 11 | ||||
| Arrest of the child 6, 12 | ||||
| Assault 1- 4, 8, 10-13 | ||||
| Family dysfunction 1-14 | ||||
| Emotional and physical abuse and neglect 1, 3-7 | ||||
| Sexual abuse 1-8, 10-14 | ||||
| Parent missing | ||||
| Bereavement 1, 4-6, 10-14 | ||||
| Crime/Theft 7, 8, 10, 11, 12, 13 | ||||
| Economic hardship (unemployment, financial difficulties) 3, 9, 11 | ||||
| Bullying 1-8, 10, 11, 14 | ||||
| Interruption of education | ||||
| Separation from family 2, 4-6, 9, 11, 13 | ||||
| Discrimination 1, 4-6, 8, 10, 11 | ||||
| Immigration detention | ||||
| Immigration process | ||||
| Acculturation stress | ||||
| Refugee specific adversity forms identified within this review are accentuated in bold | ||||
|
|
|||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



