
Submitted:
22 February 2023
Posted:
03 March 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Vaccination against SARS-CoV-2 has significantly contributed to the recent pandemic control. COVID-19 vaccines are available with different platforms and the primary clinical trials results presented acceptable safety profile of the approved vaccines. Nevertheless, the long-term assessment of the adverse events or rare conditions need to be investigated. The present systematic review, aimed at classification of Iranian case reports following COVID-19 immunization. To achieve this goal, the related published case reports were explored via PubMed, Web of Science and Google scholar according to PRISMA guideline and available up to 14th Dec, 2022. Out of 437 explored studies, the relevant data were fully investigated which totally led to 40 studies including 64 case reports with a new onset of a problem. The cases were then classified according to the various items such as the type of adverse event manifestations and COVID-19 vaccine.
The reported COVID-19 vaccines in the studied cases included Sinopharm, AstraZeneca, and COVAXIN. The results showed that the adverse events presented in 8 different categories from which cutaneous problems accounted as the most prevalent manifestations (43.7%) in which rare diseases were also screened such as Steven-Johnson syndrome, Morphea and Toxic Epidermal Necrolysis. Notably, almost 60% of the cases had no comorbidities. Moreover, the obtained data revealed nearly half of the incidences occurred after the first dose of injection and the mean duration of improvement after the symptom onset was 18.72±24.69 days. 73% of all the cases were either significantly improved or fully recovered. Although the advantages of COVID-19 vaccination is undoubtedly significant, the high risk individuals including those with a history of serious disease or comorbidities immunodeficiency conditions should be vaccinated with the utmost caution.
Keywords:
COVID-19
; Vaccination
; Adverse event
; Case report
; Iran
Introduction
COVID-19 as the most recent global pandemic typically presents as lower respiratory tract infection which may lead to severe symptoms (1, 2). Fortunately, vaccination against COVID-19 was explored at the right time and led to fast outcomes through different platforms and hopefully pandemic control (3, 4). Nevertheless, booster shots are still recommended as the immunity wanes over the time and new variants are capable to escape from immune system (5, 6).
From another point of view, the quick procedure of vaccine development could possibly have lately unsolicited events beside the immunity protection. Many studies have shown SARS-CoV-2 manifestations through which the virus affect body in various presentations even in a late episode (7, 8). As the number of vaccinated individuals grows up, the knowledge of possible and probable vaccine impact develops through case reports and long-term safety studies (9, 10).
Although the exact mechanism through which the vaccine components can manipulate human body is not clear yet, the cumulative and comparative data would bring sufficient data especially by the follow-up outcomes.
Comparison of advantages and disadvantages of COVID-19 vaccines has shown that it is still recommended. It has been assumed that there will be more in cardiovascular diseases due to spike proteins encoded in vaccines (11, 12). Furthermore, there is a possible threat of unknown organ hurt caused by the immunization which is still hidden.
In the present study, analysis of documented case reports of Iranian individuals who developed any new disorders following administration of either COVID-19 vaccines was aimed.
Methodology
The present study was conducted according to preferred reporting items for systematic reviews and meta-analyses (PRISMA) guideline (13).
Three databases, PubMed, Web of Science and Google scholar, were explored and all the relevant data available up to 14th Dec, 2022 were collected. The relevant data were targeted with terms of: “COVID-19 vaccine”, “SARS-CoV-2”, “case reports”, “adverse events” and “Iran”.
In order to exclude the irrelevant data, titles and abstracts were initially screened. At the next step, the full text of the articles were evaluated regarding the eligibility of inclusion in the study. The data including the case reports after COVID-19 disease were also removed. Moreover, only the new onsets were considered which means the cases who had a history of the exactly same disorder were not considered (Figure 1). The following data were extracted according to a valid datasheet including: age, gender, vaccine type, date of injection, date of disorder appearance, duration of the symptoms, type of the developed disorder, medical history of the case, hospitalization, response to the treatment, follow-up and outcomes.
Results
The initial search yielded 437 studies. After duplication removal, 250 papers were investigated regarding the titles and abstracts from which 128 articles were excluded according to the eligibility of the criteria including the case reports which had the same medical history or those with insufficient data. Eventually 40 manuscripts met the criteria of the systematic review.
A total of 64 cases including 31 females and 33 males with a mean age of 47.67±17.69 and a range of 18 to 91 were investigated from whom 60% had no remarkable medical history. The previous history of COVID-19 was rare among the cases and all the COVID-19 PCR tests were negative at the time of manifestation (Table 1).
The reported COVID-19 vaccines in the studied cases included Sinopharm (n=36), AstraZeneca (n=22), Sputnik (n=5) and Bharat (n=1).
The mean duration between the vaccination and any appeared event was 9.3±9.11 days. Of 64 cases, 52 ones experienced a type of manifestation post-first dose, 10 post-second dose and only 2 after the booster shot.
COVID-19 vaccine triggered different manifestations from which cutaneous disorders were spotted as the most frequent one accounting for 43.7% (n=28) followed by neurologic problems in 25% of the cases (n=16). Other unsolicited events included blood/vessel involvement (n=6), cardiovascular involvement (n=5), ocular disorders (n=4), liver disorder/failure (n=2), graft rejection (n=2) and one metabolic disorder (Figure 2). The mean duration of improvement after the symptom onset was 18.72±24.69 days.
Cutaneous involvement presented in various forms such as alopecia, lichen planus, rash, dermatitis and stromal keratitis. Notably, the dermal manifestation occurred equally on both men and women among whom only one person had a history of COVID-19. The other interesting finding is that rare diseases were also screened such as Steven-Johnson syndrome, Morphea and Toxic Epidermal Necrolysis (TEN).
In addition to type of disorders, we also evaluated the recovery time as well. To achieve that, the provided data were categorized to 6 outcomes as resolved, significant improvement, partial improvement, under treatment, not-treated and expired. Based on the outcome statement of the manuscripts, of 64 incidences, 13 were resolved, 33 were significantly improved and 10 were partially improved. 4 cases were under treatment, one remained untreated and 2 cases expired. Three studies did not mention the outcome. Therefore, 73% of all the cases were either significantly improved or fully recovered from the incidence.
According to the available statements, 20 cases were hospitalized and 22 ones were recommended to be followed-up in the schedule varying from 14 days to six months.
Discussion
Massive vaccination campaigns have been launched Since December 2020, applying mRNA vaccines and also the viral vector-based vaccine as well as inactivated viral-based and recombinant protein vaccines. By the end of January 2023, more than 5 billion individuals were fully vaccinated (54). Thus, there is an increasing rate of reports over the adverse events associated with the administrated vaccines in real world. General symptoms which have been normally screened includes weakness, fever/chills, body pain, headache and local injection-site reactions. These symptoms are usually transient and do not normally need to be treated with specific medicine care.
Herein, we discussed 64 cases who experienced unsolicited events after vaccinating against COVID-19. The applied vaccines included viral-vector and inactivated virus-based vaccines. We tried to select the case reports with new onset of the symptoms in whom the pre-existing comorbidity was not as same as the triggered adverse events. Various disorders were captured induced by different vaccines suggesting that the type of a specific regimen is not the only factor in outcomes. Moreover, there is not enough clues to support the triggered manifestations and their association with the applied vaccine. However, the healthy individuals who did not have any remarkable medical history and experienced serious events suggest that this potency of COVID-19 vaccine must be considered.
The common adverse events of AstraZeneca vaccine were pain at the injection site, fever, lethargy, muscle pain and headache which were mostly screened after the first dose of vaccine (55). Moreover, irritability, nausea, myalgia, and chills some hours after vaccination with AZD1222 were reported in Nepal (56). In addition to common adverse events, severe disorders were captured as postural drop in blood pressure, abdominal cramps, syncope and urticaria (57).Fever/chills, general discomfort, headache arthralgia, myalgia, asthenia, tenderness were among the common side effects following Sputnik V COVID-19 Vaccine which seemed to be more frequents after the second dose (58, 59). In this review, we found that AstraZeneca mostly led to neurological incidences including encephalopathy (14), acute vestibular neuritis (28) and Guillain-Barre syndrome (32). Although the safe administration of vaccines is a crucial factor many unusual events following AstraZeneca vaccine have been reported. The Concern about neurological abnormalities regarding COVID-19 vaccines firstly rose in 2020 when some cases of Guillain-Barré syndrome and transverse myelitis were screened post-Oxford/AstraZeneca vaccine (60, 61). Furthermore, in the investigated cases in this review, AstraZeneca has been the only cause of liver disorder in forms of Fulminant hepatitis (50) and acute liver failure which led to death in both cases (51). Liver injury following COVID-19 vaccination is also investigated in a systematic review on individuals who got to Moderna (mRNA)–1273, Pfizer-BioNTech BNT162b2 mRNA or ChAdOx1 nCoV-19 vaccine. Nevertheless in those cases, pre-existing comorbidities was common as 69.6% such as liver disease. The mortality rate due to live disorders was reported 4.3% (62).
According to conducted studies in China, inactivated viral-based vaccines led to adverse events including injection site pain, lethargy and muscle pain 15.6% after the first and 14.6% after the second dose among the healthcare workers. The most common is pain at the injection site, followed by fatigue, muscle pain, and headache (63, 64). Furthermore, two serious events as multiple sclerosis and emesis were also recorded with hospitalization requirement (65, 66).
In the present review, Sinopharm vaccine resulted in corneal graft rejection in to cases a week after the first dose of injection (53).In a study by Shah AP et al., four cases with a history of keratoplasty developed rejection after being vaccinated with mRNA-1273 (67). This incidence has also been reported after adenovirus vector (AZD1222) and mRNA (BNT162) vaccines (68).
A systematic review also showed that Cornea rejection was the most reported organ rejection after vaccination against COVID-19, followed by kidney and liver rejections (69).
Dermal abnormalities have been the most frequent reported incidences after Sinopharm vaccine among which new-onset lichen planus (LP) was observed in 6 cases (23). Nevertheless, rare conditions were also screened such as Toxic Epidermal Necrolysis (21), Morphea (19) and Pemphigus vulgaris (22). Notably, of 28 skin disorders in the reported cases from Iran, 20 cases got Sinopharm vaccine. The other study from Iran evaluated the cutaneous reactions post-COVID-19 vaccination which presented that most of the individuals showed symptoms after injection of AstraZeneca, Sinopharm, Sputnik V, and COVAXIN vaccines (70).
Herpes zoster has been reported in case series and has also been documented in the Center of Disease Control following COVID-19 vaccines (VAERS). There are more than 1000 cases with mRNA vaccine-triggered herpes zoster in VAERS, mostly aged over 60 (71). We also found a reported case of Herpes Zoster in a 60-year-old healthy woman 6 days after the first dose of Sinopharm vaccine (19). It has been suggested that molecular mimicry between the human components and vaccine-induced proteins could lead to pathological autoantibodies generation and hence, autoimmunity accordingly (72).
Neurological disorders also counted a quarter of the investigated cases mostly with Guillain–Barré syndrome (32) and Bell’s palsy caused (29) by AstraZeneca, Sinopharm and Sputnik vaccines. Although the most incidences were captured post-first dose, a 60-year-old man presented Guillain–Barré syndrome 20 days after the Sinopharm booster shot (73). The correlation between Bell’s palsy and vaccinations has been introduced previously such as influenza H1N1 monovalent vaccine and intranasal inactivated influenza vaccine (74, 75). Similar to other unknown mechanisms of vaccine induced problems, precise pattern of neurologic disorders is still under question. Some hypothetical thoughts though propose that autoimmune phenomenon as a result of host molecules mimicry with the vaccine antigen could activate auto-reactive T cells (76).
Blood/vessels involvement were also reported in 6 cases as vasculitis, thrombotic thrombocytopenia, Cerebral venous sinus thrombosis, acquired thrombotic and lymphocytic vasculopathy caused by Sinopharm and AstraZeneca (14, 38-40, 77). Notably, all the cases presented the manifestation after the first dose of vaccination. A review study showed that thrombotic complications occurred 5–25 days post-first dose of AstraZeneca vaccinated individuals in which the thrombosis site was mostly in cerebral veins (78). Although the exact mechanism of the events is not well understood, the pre-existing antibodies like heparin-PF4 antibody in the cases might give rise to the manifestations (79) . In addition, vasculitis precipitation has been also detected after other vaccines against hepatitis B virus (HBV), influenza virus and human papillomavirus (HPV) (80).
Although the discussed disorders have been screened post-vaccination, it is suggested that hot immune responses are strong potential cause of the events. It is to say that, anti-spike immune responses might be linked to post-vaccine syndromes as all the vaccines against COVID-19 encode the whole or a part of spike protein. In addition to spike protein, anti-idiotypic antibodies can bind to the ACE-2 receptor as well (81). Furthermore, the generated autoantibody stemming from molecular mimicry and independent immune-dysregulation may both contribute to a symptom onset (82).
Conclusions
The present review showed that various unsolicited adverse events have been captured as case reports in Iran. Interestingly, all the vaccine platforms could result in similar unsolicited events. Although, clinical trials provide safety data, the long-term evaluation of newly launched vaccines are essential to keep the public trust balanced.
COVID-19 has been the most recent mass vaccination program due to the broad range of infection world-wide. Thus, it is not far from view to face some rare disorders or late onset of a disease. Considering the advantage of the vaccination against SARS-CoV-2 which eventually led to the chaos management globally, the number of unsolicited AEs are not significant. However, the collective data from different populations would result in a better perspective for further vaccination program. The high risk individuals including those with a history of serious disease or comorbidities and those with immunodeficiency conditions should be vaccinated with the utmost caution.
Acknowledgments
We would like to thank Pasteur Institute of Iran to support this study.
Author Contributions
Methodology, M.SL.; Software, M.SL, A.B.; Validation, A.R., Data Curation, M.SL, D.D, A.K, M.B., F.A. ; Writing Original Draft Preparation, M.SL; Writing Review & Editing, M.SL. & A.R.
Conflicts of Interest
All the authors declare that they have no conflict of interest.
References
- Fotouhi F, Salehi-Vaziri M, Farahmand B, Mostafavi E, Pouriayevali MH, Jalali T, et al. Prolonged Viral Shedding and Antibody Persistence in Patients with COVID-19. Microbes and Infection. 2021 2021/03/17:104810. Pubmed Central PMCID: PMC7963517. [CrossRef]
- Mostafa Salehi-Vaziri TJ, Behrokh Farahmand, Fatemeh Fotouhi, Mohammad Banifazl, Mohammad Hassan Pouriayevali, Mona Sadat Larijani, Neda Afzali and Amitis Ramezani. Clinical Characteristics of SARS-CoV-2 by Re-infection Vs. Reactivation: A Case Series From Iran. European Journal of Clinical Microbiology & Infectious Diseases. 2021 2021/02/05. [CrossRef]
- Lurie N, Saville M, Hatchett R, Halton J. Developing Covid-19 Vaccines at Pandemic Speed. New England Journal of Medicine. 2020. [CrossRef]
- Menni C, May A, Polidori L, Louca P, Wolf J, Capdevila J, et al. COVID-19 vaccine waning and effectiveness and side-effects of boosters: a prospective community study from the ZOE COVID Study. The Lancet Infectious Diseases. 2022;22(7):1002-10. [CrossRef]
- Immunogenicity and safety of pastocovac vaccine as a booster dose in comparison with sinopharm and pastocovac Plus boosters in Iranian adults aged 18 to 80 who received 2 doses of Sinopharm vaccine: a parallel group clinical trial [Internet]. IRCT Iranian Registry of Clinical Trials. 2022 [cited 2022/04/07].
- Chenchula S, Karunakaran P, Sharma S, Chavan M. Current evidence on efficacy of COVID-19 booster dose vaccination against the Omicron variant: A systematic review. Journal of Medical Virology. 2022;94(7):2969-76. [CrossRef]
- Anjana NKN, Annie TT, Siba S, Meenu MS, Chintha S, Anish TSN. Manifestations and risk factors of post COVID syndrome among COVID-19 patients presented with minimal symptoms – A study from Kerala, India. Journal of Family Medicine and Primary Care. 2021;10(11). [CrossRef]
- Sadat Larijani M, Ashrafian F, Bagheri Amiri F, Banifazl M, Bavand A, Karami A, et al. Characterization of long COVID-19 manifestations and its associated factors: A prospective cohort study from Iran. Microbial Pathogenesis. 2022 2022/08/01/;169:105618. [CrossRef]
- Graña C, Ghosn L, Evrenoglou T, Jarde A, Minozzi S, Bergman H, et al. Efficacy and safety of COVID-19 vaccines. Cochrane Database Syst Rev. 2022 Dec 7;12(12):Cd015477. PubMed PMID: 36473651. Pubmed Central PMCID: PMC9726273 known. Alexander Jarde: none known. Silvia Minozzi: no relevant interests; Joint Co-ordinating Editor and Method editor of the Drugs and Alcohol Group. Hanna Bergman: Cochrane Response – consultant; WHO – grant/contract (Cochrane Response was commissioned by the WHO to perform review tasks that contribute to this publication). Brian Buckley: none known. Katrin Probyn: Cochrane Response – consultant; WHO – consultant (Cochrane Response was commissioned to perform review tasks that contribute to this publication). Gemma Villanueva: Cochrane Response – employment (Cochrane Response has been commissioned by WHO to perform parts of this systematic review). Nicholas Henschke: Cochrane Response – consultant; WHO – consultant (Cochrane Response was commissioned by the WHO to perform review tasks that contributed to this publication). Hillary Bonnet: none known. Rouba Assi: none known. Sonia Menon: P95 – consultant. Melanie Marti: no relevant interests; Medical Officer at WHO. Declan Devane: Health Research Board (HRB) – grant/contract; registered nurse and registered midwife but no longer in clinical practice; Editor, Cochrane Pregnancy and Childbirth Group. Patrick Mallon: AstraZeneca – Advisory Board; spoken of vaccine effectiveness to media (print, online, and live); works as a consultant in a hospital that provides vaccinations; employed by St Vincent’s University Hospital. Jean-Daniel Lelievre: no relevant interests; published numerous interviews in the national press on the subject of COVID vaccination; Head of the Department of Infectious Diseases and Clinical Immunology CHU Henri Mondor APHP, Créteil; WHO (IVRI-AC): expert Vaccelarate (European project on COVID19 Vaccine): head of WP; involved with COVICOMPARE P et M Studies (APHP, INSERM) (public fundings). Lisa Askie: no relevant interests; Co-convenor, Cochrane Prospective Meta-analysis Methods Group. Tamara Kredo: no relevant interests; Medical Officer in an Infectious Diseases Clinic at Tygerberg Hospital, Stellenbosch University. Gabriel Ferrand: none known. Mauricia Davidson: none known. Carolina Riveros: no relevant interests; works as an epidemiologist. David Tovey: no relevant interests; Emeritus Editor in Chief, Feedback Editors for 2 Cochrane review groups. Joerg J Meerpohl: no relevant interests; member of the German Standing Vaccination Committee (STIKO). Giacomo Grasselli: Pfizer – speaking engagement. Gabriel Rada: none known. Asbjørn Hróbjartsson: no relevant interests; Cochrane Methodology Review Group Editor. Philippe Ravaud: no relevant interests; involved with Mariette CORIMUNO-19 Collaborative 2021, the Ministry of Health, Programme Hospitalier de Recherche Clinique, Foundation for Medical Research, and AP-HP Foundation. Anna Chaimani: none known. Isabelle Boutron: no relevant interests; member of Cochrane Editorial Board. Epub 2022/12/07. eng.
- Liu Q, Qin C, Liu M, Liu J. Effectiveness and safety of SARS-CoV-2 vaccine in real-world studies: a systematic review and meta-analysis. Infectious Diseases of Poverty. 2021 2021/11/14;10(1):132. [CrossRef]
- Correction to: Abstract 10712: Mrna COVID Vaccines Dramatically Increase Endothelial Inflammatory Markers and ACS Risk as Measured by the PULS Cardiac Test: a Warning. Circulation. 2021 Dec 21:CIR0000000000001053. PubMed PMID: 34932387. Epub 2021/12/22. eng.
- Lai FTT, Li X, Peng K, Huang L, Ip P, Tong X, et al. Carditis After COVID-19 Vaccination With a Messenger RNA Vaccine and an Inactivated Virus Vaccine. Annals of Internal Medicine. 2022 2022/03/15;175(3):362-70. [CrossRef]
- Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ (Clinical research ed). 2009 Jul 21;339:b2535. PubMed PMID: 19622551. Pubmed Central PMCID: PMC2714657. Epub 2009/07/23. eng. [CrossRef]
- Khajavirad N, Salehi M, Haji Ghadery A, Khalili H, Arab Ahmadi M, Dehghan Manshadi SA, et al. Serious events following COVID-19 vaccination with ChAdOx1 nCoV-19 vaccine (Vaxzevria): A short case series from Iran. Clin Case Rep. 2022 Feb;10(2):e05390. PubMed PMID: 35145690. Pubmed Central PMCID: PMC8818285. Epub 2022/02/12. eng. [CrossRef]
- Sepaskhah M, Ansari Asl F, Taheri M, Akbarzadeh Jahromi M. COVID-19 vaccine-induced Radiation Recall Dermatitis: Report of a case. Clin Case Rep. 2022 Feb;10(2):e05490. PubMed PMID: 35228886. Pubmed Central PMCID: PMC8864568. Epub 2022/03/02. eng. [CrossRef]
- Aryanian Z, Balighi K, Hatami P, Tootoonchi NM, Goodarzi A, Mohseni Afshar Z. Morphea in two patients after being infected to and being vaccinated against SARS-CoV-2 infection. Clinical case reports. 2022 Apr;10(4):e05667. PubMed PMID: 35449768. Pubmed Central PMCID: PMC9014706. Epub 2022/04/23. eng. [CrossRef]
- Sahraei Z, Abtahi-Naeini B, Saffaei A. Sputnik-V vaccine-induced panniculitis as a local reactions. Clin Case Rep. 2022 Jun;10(6):e05923. PubMed PMID: 35662784. Pubmed Central PMCID: PMC9163468. Epub 2022/06/07. eng. [CrossRef]
- Ganjei Z, Yazdan Panah M, Rahmati R, Zari Meidani F, Mosavi A. COVID-19 vaccination and alopecia areata: a case report and literature review. Clin Case Rep. 2022 Sep;10(9):e6039. PubMed PMID: 36172335. Pubmed Central PMCID: PMC9468559. Epub 2022/09/30. eng. [CrossRef]
- Shakoei S, Kalantari Y, Nasimi M, Tootoonchi N, Ansari MS, Razavi Z, et al. Cutaneous manifestations following COVID-19 vaccination: A report of 25 cases. Dermatologic therapy. 2022 Aug;35(8):e15651. PubMed PMID: 35716105. Pubmed Central PMCID: PMC9349410. Epub 2022/06/19. eng. [CrossRef]
- Mohamadzadeh D, Assar S, Pournazari M, Soufivand P, Danaei S. Disseminated cutaneous herpes simplex infection after COVID-19 vaccination in a rheumatoid arthritis patient: a case report and review. Reumatismo. 2022 Sep 13;74(2). PubMed PMID: 36101991. Epub 2022/09/15. eng. [CrossRef]
- Mardani M, Mardani S, Asadi Kani Z, Hakamifard A. An extremely rare mucocutaneous adverse reaction following COVID-19 vaccination: Toxic epidermal necrolysis. Dermatologic therapy. 2022 May;35(5):e15416. PubMed PMID: 35238119. Pubmed Central PMCID: PMC9111664. Epub 2022/03/04. eng. [CrossRef]
- Saffarian Z, Samii R, Ghanadan A, Vahidnezhad H. De novo severe pemphigus vulgaris following SARS-CoV-2 vaccination with BBIBP-CorV. Dermatologic therapy. 2022 Jun;35(6):e15448. PubMed PMID: 35289040. Pubmed Central PMCID: PMC9111647. Epub 2022/03/16. eng.
- Babazadeh A, Miladi R, Barary M, Shirvani M, Ebrahimpour S, Aryanian Z, et al. COVID-19 vaccine-related new-onset lichen planus. Clinical case reports. 2022 Feb;10(2):e05323. PubMed PMID: 35140945. Pubmed Central PMCID: PMC8810943. Epub 2022/02/11. eng. [CrossRef]
- Mansouri P, Farshi S. A case of Steven-Johnson syndrome after COVID-19 vaccination. Journal of cosmetic dermatology. 2022 Apr;21(4):1358-60. PubMed PMID: 35020263. Epub 2022/01/13. eng. [CrossRef]
- Mahmoudi Hamidabad N, Mafi AR, Abolmaali M. Mild Facial Paresis in a Recipient of Gam-COVID-Vac Vaccine: A Case Report. Clinical medicine insights Case reports. 2022;15:11795476221129120. PubMed PMID: 36225861. Pubmed Central PMCID: PMC9548508. Epub 2022/10/14. eng. [CrossRef]
- Moslemi M, Ardalan M, Haramshahi M, Mirzaei H, Sani SK, Dastgir R, et al. Herpes simplex encephalitis following ChAdOx1 nCoV-19 vaccination: a case report and review of the literature. BMC infectious diseases. 2022 Mar 3;22(1):217. PubMed PMID: 35241013. Pubmed Central PMCID: PMC8892827. Epub 2022/03/05. eng. [CrossRef]
- Maroufi SF, Naderi Behdani F, Rezania F, Tanhapour Khotbehsara S, Mirzaasgari Z. Longitudinally extensive transverse myelitis after Covid-19 vaccination: case report and review of literature. Human vaccines & immunotherapeutics. 2022 Dec 31;18(1):2040239. PubMed PMID: 35240927. Pubmed Central PMCID: PMC9009891. Epub 2022/03/05. eng. [CrossRef]
- Shahali H, Hamidi Farahani R, Hazrati P, Hazrati E. Acute vestibular neuritis: A rare complication after the adenoviral vector-based COVID-19 vaccine. Journal of neurovirology. 2022 Dec;28(4-6):609-15. PubMed PMID: 35877063. Pubmed Central PMCID: PMC9310685. Epub 2022/07/26. eng. [CrossRef]
- Mirmosayyeb O, Barzegar M, Rezaei M, Baharlouie N, Shaygannejad V. Bell’s palsy after Sputnik V COVID-19 (Gam-COVID-Vac) vaccination. Clinical case reports. 2022 Feb;10(2):e05468. PubMed PMID: 35228880. Pubmed Central PMCID: PMC8867017. Epub 2022/03/02. eng. [CrossRef]
- Shahali H, Farahani RH, Asgari A, Hazrati E. Thalamic hemi-chorea: a rare complication after receiving the adenoviral vector-based COVID-19 vaccine: a case report. Clinical and experimental vaccine research. 2022 May;11(2):217-21. PubMed PMID: 35799877. Pubmed Central PMCID: PMC9200646. Epub 2022/07/09. eng. [CrossRef]
- Fakhari MS, Poorsaadat L, Mahmoodiyeh B. Guillain-Barré syndrome following COVID-19 vaccine: A case report. Clin Case Rep. 2022 Oct;10(10):e6451. PubMed PMID: 36254149. Pubmed Central PMCID: PMC9558586. Epub 2022/10/19. eng. [CrossRef]
- Tabatabaee S, Rezania F, Alwedaie SMJ, Malekdar E, Badi Z, Tabatabaei SM, et al. Post COVID-19 vaccination Guillain-Barre syndrome: three cases. Human vaccines & immunotherapeutics. 2022 Nov 30;18(5):2045153. PubMed PMID: 35240922. Pubmed Central PMCID: PMC9196795. Epub 2022/03/05. eng. [CrossRef]
- Bazrafshan H, Mohamadi Jahromi LS, Parvin R, Ashraf A. A case of Guillain-Barre syndrome after the second dose of AstraZeneca COVID-19 vaccination. Turkish journal of physical medicine and rehabilitation. 2022 Jun;68(2):295-9. PubMed PMID: 35989967. Pubmed Central PMCID: PMC9366477. Epub 2022/08/23. eng. [CrossRef]
- Zavari A, Hamidabad NM, Hassanzadeh M. Aseptic meningitis following AZD1222 COVID-19 vaccination. The American journal of emergency medicine. 2022 May;55:225.e5-.e6. PubMed PMID: 34955313. Pubmed Central PMCID: PMC8684093. Epub 2021/12/28. eng. [CrossRef]
- Sepahvand M, Yazdi N, Rohani M, Emamikhah M. Cervical longitudinally extensive myelitis after vaccination with inactivated virus-based COVID-19 vaccine. Radiology case reports. 2022 Feb;17(2):303-5. PubMed PMID: 34849183. Pubmed Central PMCID: PMC8614237. Epub 2021/12/02. eng. [CrossRef]
- Ahmad HR, Timmermans VM, Dakakni T. Acute Disseminated Encephalomyelitis After SARS-CoV-2 Vaccination. The American journal of case reports. 2022 Jun 19;23:e936574. PubMed PMID: 35717556. Pubmed Central PMCID: PMC9218399. Epub 2022/06/20. eng. [CrossRef]
- Rahmanian E, Alikhani M, Loghman M, Beikmohamadi Hezaveh S, Zangeneh S, Shahriarirad R, et al. COVID-19 vaccine-induced vasculitis in a patient with sarcoidosis: A case report. Clinical Case Reports. 2022 2022/12/01;10(12):e6501. [CrossRef]
- Haj Mohamad Ebrahim Ketabforoush A, Molaverdi G, Nirouei M, Abbasi Khoshsirat N. Cerebral venous sinus thrombosis following intracerebral hemorrhage after COVID-19 AstraZeneca vaccination: A case report. Clinical case reports. 2022 Nov;10(11):e6505. PubMed PMID: 36397844. Pubmed Central PMCID: PMC9664546. Epub 2022/11/19. eng.
- Yaghoubi F, Dalil D. Acquired thrombotic thrombocytopenic purpura after AstraZeneca vaccine: A case report. Caspian journal of internal medicine. 2022;13(Suppl 3):299-302. PubMed PMID: 35872667. Pubmed Central PMCID: PMC9272963. Epub 2022/07/26. eng. [CrossRef]
- Saffarian Z, Samii R, Hadizadeh A, Ghanadan A, Vahidnezhad H. Purpuric dermatosis and lymphocytic vasculopathy following SARS-CoV-2 vaccination: Report of two patients. Dermatologic therapy. 2022 Nov;35(11):e15898. PubMed PMID: 36196579. Pubmed Central PMCID: PMC9874540. Epub 2022/10/06. eng. [CrossRef]
- Naghashzadeh F, Shafaghi S, Dorudinia A, Naji SA, Marjani M, Amin A, et al. Myocarditis following rAd26 and rAd5 vector-based COVID-19 vaccine: case report. ESC heart failure. 2022 Apr;9(2):1483-6. PubMed PMID: 35106967. Pubmed Central PMCID: PMC8934948. Epub 2022/02/03. eng. [CrossRef]
- Servatyari K, Hassani A. The first report of myocarditis followed by AstraZeneca vaccination in Iran. Chronic Diseases Journal. 2022 06/20;10(2):117-20.
- Hassanzadeh S, Sadeghi S, Mirdamadi A, Nematollahi A. Myocarditis following AstraZeneca (an adenovirus vector vaccine) COVID-19 vaccination: A case report. Clinical Case Reports. 2022 2022/04/01;10(4):e05744. [CrossRef]
- Mehrabi Nasab E, Athari SS. The first report of 2:1 atrioventricular block following COVID-19 vaccination. Clin Case Rep. 2022 May;10(5):e05797. PubMed PMID: 35540716. Pubmed Central PMCID: PMC9066801. Epub 2022/05/12. eng. [CrossRef]
- Azdaki N, Farzad M. Long QT interval and syncope after a single dose of COVID-19 vaccination: a case report. The Pan African medical journal. 2021;40:67. PubMed PMID: 34804335. Pubmed Central PMCID: PMC8590254. Epub 2021/11/23. eng. [CrossRef]
- Dehghani A, Ghanbari H, Houshang-Jahromi M-h, Pourazizi M. Paracentral acute middle maculopathy and COVID-19 vaccination: Causation versus coincidence finding. Clinical Case Reports. 2022 2022/03/01;10(3):e05578. [CrossRef]
- Mohammadpour M, Farrokhpour H, Sadeghi R. Herpetic endotheliitis and stromal keratitis following inactivated COVID-19 vaccination. Clin Case Rep. 2022 Oct;10(10):e6397. PubMed PMID: 36237947. Pubmed Central PMCID: PMC9536498. Epub 2022/10/15. eng. [CrossRef]
- Farahani AA, Shahali H. Intracranial Hypertension and Papilledema: An Unusual Complication After the Adenoviral DNA Vector-Based Coronavirus Disease 2019 Vaccination in an Air Medical Transportation Pilot. Air medical journal. 2022 Nov-Dec;41(6):560-5. PubMed PMID: 36494173. Pubmed Central PMCID: PMC9350672. Epub 2022/12/10. eng. [CrossRef]
- Fekri S, Khorshidifar M, Dehghani MS, Nouri H, Abtahi SH. Acute macular neuroretinopathy and COVID-19 vaccination: Case report and literature review. Journal francais d’ophtalmologie. 2023 Jan;46(1):72-82. PubMed PMID: 36496293. Pubmed Central PMCID: PMC9684098. Epub 2022/12/11. eng. [CrossRef]
- Barary M, Sharifi-Razavi A, Rakhshani N, Sio TT, Ebrahimpour S, Baziboroun M. Fulminant hepatitis following COVID-19 vaccination: A case report. Clinical case reports. 2022 Jul;10(7):e6066. PubMed PMID: 35865787. Pubmed Central PMCID: PMC9295676. Epub 2022/07/23. eng. [CrossRef]
- Sohrabi M, SobheRakhshankhah E, Ziaei H, AtaeeKachuee M, Zamani F. Acute liver failure after vaccination against of COVID-19; a case report and review literature. Respiratory medicine case reports. 2022;35:101568. PubMed PMID: 34926142. Pubmed Central PMCID: PMC8668601. Epub 2021/12/21. eng. [CrossRef]
- Bennet WM, Elamin A, Newell-Price JD. Subacute thyroiditis following COVID-19 vaccination: Case report and Society for Endocrinology survey. Clinical endocrinology. 2023 Mar;98(3):452-3. PubMed PMID: 35261054. Pubmed Central PMCID: PMC9111779. Epub 2022/03/10. eng. [CrossRef]
- Mohammadzadeh M, Hooshmandi S, Jafari M, Hassanpour K. Presumably Corneal Graft Rejection after COVID-19 Vaccination. Case reports in ophthalmology. 2022 May-Aug;13(2):562-9. PubMed PMID: 36160489. Pubmed Central PMCID: PMC9386427. Epub 2022/09/27. eng. [CrossRef]
- WHO Coronavirus (COVID-19) Dashboard [Internet]. World Health Organization. [cited 2023/6/2]. Available from: https://covid19.who.int/.
- Menni C, Klaser K, May A, Polidori L, Capdevila J, Louca P, et al. Vaccine side-effects and SARS-CoV-2 infection after vaccination in users of the COVID Symptom Study app in the UK: a prospective observational study. The Lancet Infectious Diseases. 2021 2021/07/01/;21(7):939-49. [CrossRef]
- Sah R, Shrestha S, Mehta R, Sah SK, Rabaan AA, Dhama K, et al. AZD1222 (Covishield) vaccination for COVID-19: Experiences, challenges, and solutions in Nepal. Travel Medicine and Infectious Disease. 2021 2021/03/01/;40:101989. [CrossRef]
- Shrestha S, Devbhandari RP, Shrestha A, Aryal S, Rajbhandari P, Shakya B, et al. Adverse events following the first dose of ChAdOx1 nCoV-19 (COVISHIELD) vaccine in the first phase of vaccine roll out in Nepal. Journal of Patan Academy of Health Sciences. 2021;8(1):9-17. [CrossRef]
- Pagotto V, Ferloni A, Soriano MM, Díaz M, Braguinsky Golde N, González MI, et al. Active monitoring of early safety of Sputnik V vaccine in Buenos Aires, Argentina. MEDICINA (Buenos Aires). 2021;81(3):408-14.
- Montalti M, Soldà G, Di Valerio Z, Salussolia A, Lenzi J, Forcellini M, et al. ROCCA observational study: Early results on safety of Sputnik V vaccine (Gam-COVID-Vac) in the Republic of San Marino using active surveillance. EClinicalMedicine. 2021;38:101027. [CrossRef]
- Das AS, Regenhardt RW, Feske SK, Gurol ME. Treatment Approaches to Lacunar Stroke. Journal of stroke and cerebrovascular diseases : the official journal of National Stroke Association. 2019 Aug;28(8):2055-78. PubMed PMID: 31151838. Pubmed Central PMCID: PMC7456600. Epub 2019/06/04. eng. [CrossRef]
- Blauenfeldt RA, Kristensen SR, Ernstsen SL, Kristensen CCH, Simonsen CZ, Hvas AM. Thrombocytopenia with acute ischemic stroke and bleeding in a patient newly vaccinated with an adenoviral vector-based COVID-19 vaccine. Journal of thrombosis and haemostasis : JTH. 2021 Jul;19(7):1771-5. PubMed PMID: 33877737. Pubmed Central PMCID: PMC8250306. Epub 2021/04/21. eng. [CrossRef]
- Roy A, Verma N, Singh S, Pradhan P, Taneja S, Singh M. Immune-mediated liver injury following COVID-19 vaccination: A systematic review. Hepatology Communications. 2022 2022/09/01;6(9):2513-22. [CrossRef]
- Ella R, Vadrevu KM, Jogdand H, Prasad S, Reddy S, Sarangi V, et al. Safety and immunogenicity of an inactivated SARS-CoV-2 vaccine, BBV152: a double-blind, randomised, phase 1 trial. The Lancet Infectious Diseases. 2021 2021/05/01/;21(5):637-46. [CrossRef]
- Zhang M-X, Zhang T-T, Shi G-F, Cheng F-M, Zheng Y-M, Tung T-H, et al. Safety of an inactivated SARS-CoV-2 vaccine among healthcare workers in China. Expert Review of Vaccines. 2021 2021/07/03;20(7):891-8. [CrossRef]
- Al Kaabi N, Zhang Y, Xia S, Yang Y, Al Qahtani MM, Abdulrazzaq N, et al. Effect of 2 Inactivated SARS-CoV-2 Vaccines on Symptomatic COVID-19 Infection in Adults: A Randomized Clinical Trial. JAMA. 2021;326(1):35-45. [CrossRef]
- Bhandari B, Rayamajhi G, Lamichhane P, Shenoy AK. Adverse Events following Immunization with COVID-19 Vaccines: A Narrative Review. BioMed Research International. 2022 2022/08/16;2022:2911333. [CrossRef]
- Shah AP, Dzhaber D, Kenyon KR, Riaz KM, Ouano DP, Koo EH. Acute Corneal Transplant Rejection After COVID-19 Vaccination. Cornea. 2022 Jan 1;41(1):121-4. PubMed PMID: 34620770. Epub 2021/10/09. eng. [CrossRef]
- Molero-Senosiain M, Houben I, Savant S, Savant V. Five Cases of Corneal Graft Rejection After Recent COVID-19 Vaccinations and a Review of the Literature. Cornea. 2022;41(5):669-72. PubMed PMID: 00003226-202205000-00028. [CrossRef]
- Alhumaid S, Rabaan AA, Dhama K, Yong SJ, Nainu F, Hajissa K, et al. Solid Organ Rejection following SARS-CoV-2 Vaccination or COVID-19 Infection: A Systematic Review and Meta-Analysis. Vaccines. 2022 Aug 10;10(8). PubMed PMID: 36016180. Pubmed Central PMCID: PMC9412452. Epub 2022/08/27. eng. [CrossRef]
- Pourani MR, Shahidi Dadras M, Salari M, Diab R, Namazi N, Abdollahimajd F. Cutaneous adverse events related to COVID-19 vaccines: A cross-sectional questionnaire-based study of 867 patients. Dermatologic therapy. 2022 Feb;35(2):e15223. PubMed PMID: 34820975. Epub 2021/11/26. eng. [CrossRef]
- Gambichler T, Boms S, Susok L, Dickel H, Finis C, Abu Rached N, et al. Cutaneous findings following COVID-19 vaccination: review of world literature and own experience. Journal of the European Academy of Dermatology and Venereology. 2022 2022/02/01;36(2):172-80. [CrossRef]
- Essam R, Ehab R, Al-Razzaz R, Khater MW, Moustafa EA. Alopecia areata after ChAdOx1 nCoV-19 vaccine (Oxford/AstraZeneca): a potential triggering factor? Journal of cosmetic dermatology. 2021 Dec;20(12):3727-9. PubMed PMID: 34559937. Pubmed Central PMCID: PMC8661988. Epub 2021/09/25. eng. [CrossRef]
- Fakhari MS, Poorsaadat L, Mahmoodiyeh B. Guillain–Barré syndrome following COVID-19 vaccine: A case report. Clinical case reports. 2022 2022/10/01;10(10):e6451. [CrossRef]
- Mutsch M, Zhou W, Rhodes P, Bopp M, Chen RT, Linder T, et al. Use of the Inactivated Intranasal Influenza Vaccine and the Risk of Bell’s Palsy in Switzerland. New England Journal of Medicine. 2004 2004/02/26;350(9):896-903. [CrossRef]
- Zhou W, Pool V, DeStefano F, Iskander JK, Haber P, Chen RT. A potential signal of Bell’s palsy after parenteral inactivated influenza vaccines: reports to the Vaccine Adverse Event Reporting System (VAERS)—United States, 1991–2001. Pharmacoepidemiology and Drug Safety. 2004 2004/08/01;13(8):505-10. [CrossRef]
- Principi N, Esposito S. Do Vaccines Have a Role as a Cause of Autoimmune Neurological Syndromes? Frontiers in public health. 2020;8:361. PubMed PMID: 32850592. Pubmed Central PMCID: PMC7399175. Epub 2020/08/28. eng. [CrossRef]
- Rahmanian E, Alikhani M, Loghman M, Beikmohamadi Hezaveh S, Zangeneh S, Shahriarirad R, et al. COVID-19 vaccine-induced vasculitis in a patient with sarcoidosis: A case report. Clinical case reports. 2022 Dec;10(12):e6501. PubMed PMID: 36478972. Pubmed Central PMCID: PMC9718919. Epub 2022/12/09. eng. [CrossRef]
- Khajavirad N, Salehi M, Haji ghadery A, Khalili H, Arab Ahmadi M, Dehghan Manshadi SA, et al. Serious events following COVID-19 vaccination with ChAdOx1 nCoV-19 vaccine (Vaxzevria): A short case series from Iran. Clinical case reports. 2022 2022/02/01;10(2):e05390. [CrossRef]
- Huynh A, Kelton JG, Arnold DM, Daka M, Nazy I. Antibody epitopes in vaccine-induced immune thrombotic thrombocytopaenia. Nature. 2021 2021/08/01;596(7873):565-9. [CrossRef]
- Bonetto C, Trotta F, Felicetti P, Alarcón GS, Santuccio C, Bachtiar NS, et al. Vasculitis as an adverse event following immunization - Systematic literature review. Vaccine. 2016 Dec 12;34(51):6641-51. PubMed PMID: 26398442. Epub 2015/09/24. eng. [CrossRef]
- Arthur JM, Forrest JC, Boehme KW, Kennedy JL, Owens S, Herzog C, et al. Development of ACE2 autoantibodies after SARS-CoV-2 infection. PloS one. 2021;16(9):e0257016. PubMed PMID: 34478478. Pubmed Central PMCID: PMC8415618. Epub 2021/09/04. eng. [CrossRef]
- Dutta D, Nagappa M, Sreekumaran Nair BV, Das SK, Wahatule R, Sinha S, et al. Variations within Toll-like receptor (TLR) and TLR signaling pathway-related genes and their synergistic effects on the risk of Guillain-Barré syndrome. Journal of the Peripheral Nervous System. 2022 2022/06/01;27(2):131-43. [CrossRef]
Figure 1.
The review flowchart based on PRISMA.
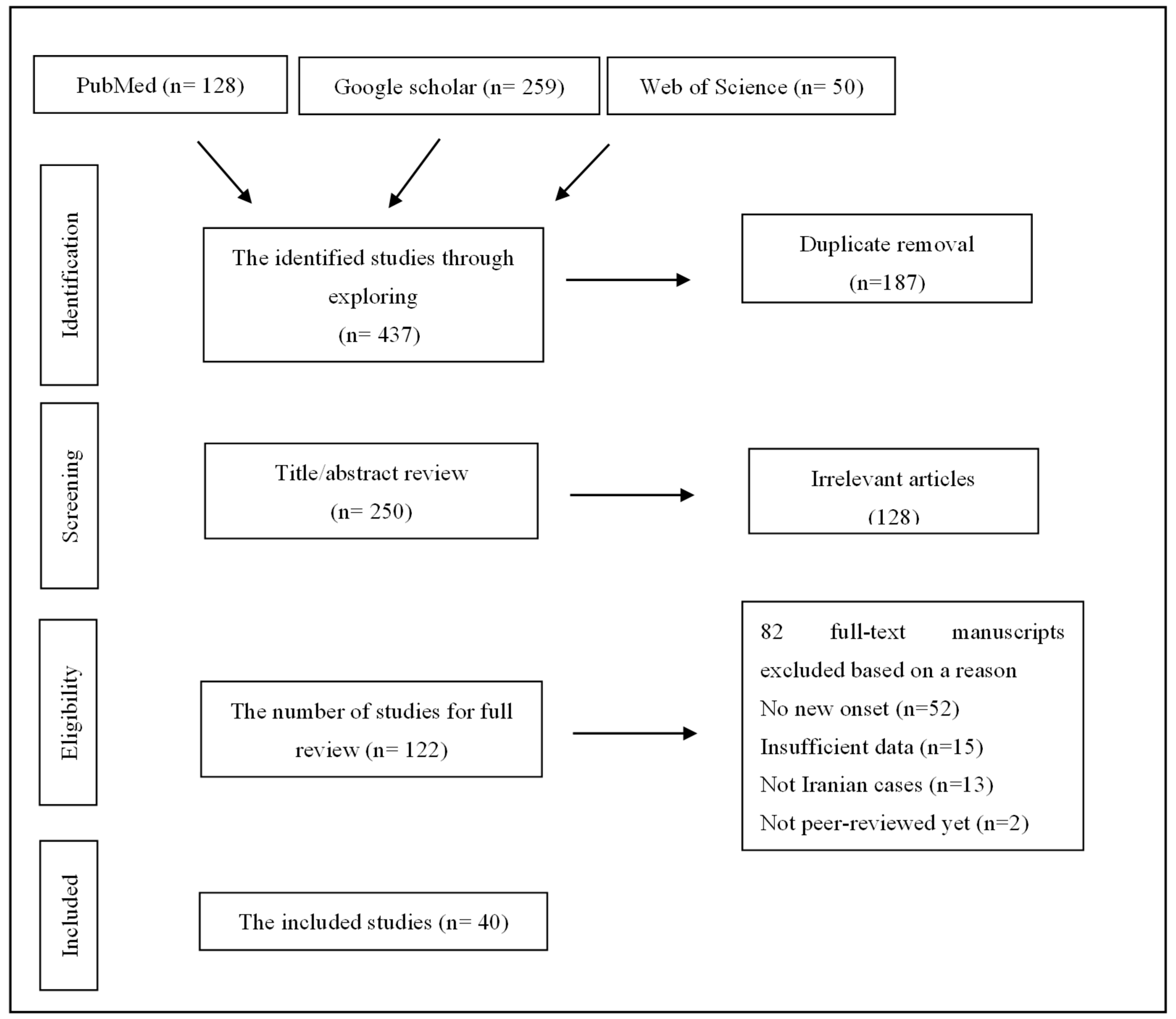
Figure 2.
COVID-19 vaccines and their potential association with disorders in case reports.
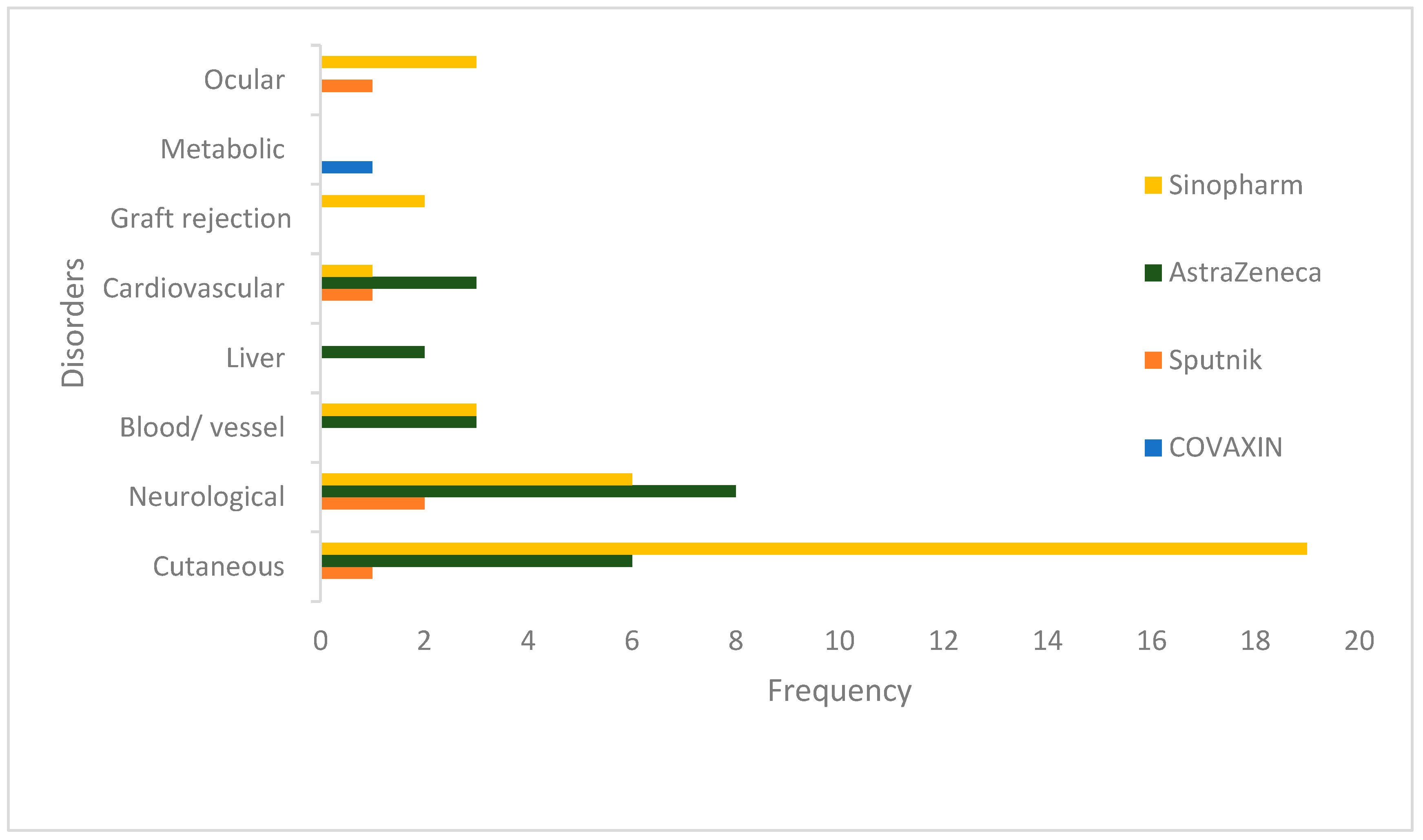

Table 1.
The categorized adverse events manifestations following COVID-19 vaccines in Iran.
| Case no. | Type of disorder | Age | Gender | Comorbidity | Covid-19 test/history | Vaccine type | Time of incidence | Ref. |
|---|---|---|---|---|---|---|---|---|
| Cutaneous involvement | ||||||||
| 1 | Extensive rash and edema | 77 | Female | Hypertension | Negative | AstraZeneca | 2 days after the 1st dose | (14) |
| 2 | Radiation Recall Dermatitis | 50 | Female | History of breast cancer and radical mastectomy | Not stated | Sinopharm | 1week after the 2nd dose | (15) |
| 3 | Erythemato-violaceous and sclerotic lesions | 70 | Female | - | Negative | AstraZeneca | 2 days after the 1st dose | (16) |
| 4 | Panniculitis | 40 | Female | - | Not stated | Sputnik | 13 days after the 1st dose | (17) |
| 5 | Alopecia areata | 23 | Female | - | Not stated | AstraZeneca | 1 week after the 1st dose | (18) |
| 6 | 74 | Male | Fatty liver | Not stated | Sinopharm | 2 days after the 2nd dose | (19) | |
| 7 | 37 | Male | - | Not stated | Sinopharm | 6 days after the both doses | (19) | |
| 8 | Herpes simplex | 63 | Female | Rheumatoid arthritis | Not stated | Sinopharm | 7 days after the 2nd dose | (20) |
| 9 | Toxic Epidermal Necrolysis (TEN) | 76 | Male | Atorvastatin 10 mg/day taken for several years | Not stated | Sinopharm | 1 day after vaccination | (21) |
| 10 | 71 | Male | - | Not stated | Sinopharm | 10 days after the 1st dose | (19) | |
| 11 | Pemphigus vulgaris (PV) | 76 | Female | Diabetes mellitus, hyperlipidemia, and ischemic heart disease | Not stated | Sinopharm | 1 month after the 2nd dose | (22) |
| 12 | 30 | Female | - | Not stated | Sinopharm | 16 days after 1st dose | (19) | |
| 13 | New-onset lichen planus (LP) | 52 | Female | - | Positive | Sinopharm | 1 week after the 2nd dose | (23) |
| 14 | 45 | Female | Hypertension | Not stated | Sinopharm | 14 days after the 1st dose | (19) | |
| 15 | 40 | Male | - | Not stated | Sinopharm | 10 days after the both | (19) | |
| 16 | 45 | Male | - | Not stated | Sinopharm | 7 days after the both | (19) | |
| 17 | 45 | Male | - | Not stated | AstraZeneca | 7 days after the 1st dose | (19) | |
| 18 | 49 | Female | - | Not stated | Sinopharm | 10days after the 1st dose | (19) | |
| 19 | Psoriasis exacerbation | 50 | Male | Arthritis | Not stated | Sinopharm | 4 days after the first dose, 6 days after the 2nd dose | (19) |
| 20 | Bullous pemphigoid | 85 | Female | - | Not stated | Sinopharm | 20days after the 1st dose | (19) |
| 21 | 91 | Male | - | Not stated | Sinopharm | 19 days after the 1st dose | (19) | |
| 22 | Cutaneous vasculitis | 45 | Male | - | Not stated | Sinopharm | 2 days after the 1st dose | (19) |
| 23 | Pytriasis rosea | 26 | Male | Hypertension, diabetes mellitus | Not stated | Sinopharm | 14 days after the booster | (19) |
| 24 | Herpes zoster | 60 | Female | - | Not stated | Sinopharm | 6 days after the 1st dose | (19) |
| 25 | Urticaria and erythema multiform | 31 | Male | - | Not stated | Sinopharm | 11 days after the 2nd dose | (19) |
| 26 | 32 | Female | - | Not stated | AstraZeneca | 20 days after the 1st | (19) | |
| 27 | Morphea | 35 | Female | Hyperlipidemia, diabetes | Not stated | AstraZeneca | 10 days after the 1st | (19) |
| 28 | Steven-Johnson syndrome | 63 | Female | Mild plaque-type psoriasis type II diabetes mellitus |
Not stated | Sinopharm | 24h after vaccination | (24) |
| Neurologic involvement | ||||||||
| 29 | Facial Paresis | 34 | Female | Migraine attacks (under treatment) | Not stated | Sputnik V | 1 day after the 1st dose | (25) |
| 30 | Encephalopathy | 27 | male | - | Not stated | AstraZeneca | 8 days after the 1st dose | (26) |
| 31 | 56 | Female | - | Negative | AstraZeneca | 2 days after the 1st dose | (14) | |
| 32 | Transverse myelitis | 31 | Female | - | Negative | AstraZeneca | 3 weeks after the 1st dose | (27) |
| 33 | Acute vestibular neuritis | 51 | Male | - | Negative | AstraZeneca | 11 days after the 1st dose | (28) |
| 34 | Bell’s palsy | 27 | Female | - | Negative | Sputnik V | 3-5 days after the 1st dose | (29) |
| 35 | 58 | Male | Controlled diabetes mellitus | Not stated | Sputnik | 10 days after the 1st dose | (29) | |
| 36 | Thalamic hemi-chorea | 72 | Male | History of laparoscopic cholecystectomy | Negative | AstraZeneca | 9 days after the 1st dose | (30) |
| 37 | Guillain-Barre syndrome | 60 | Male | Controlled hypertension and hypothyroidism | Negative | Sinopharm | 20 days after the booster | (31) |
| 38 | 46 | Male | - | Negative | AstraZeneca | 3 days after the 2nd dose | (32) | |
| 39 | 36 | Male | - | Negative | Sinopharm | 5 days after the 1st dose | (32) | |
| 40 | 32 | Male | - | Negative | Sinopharm | 14 days after the 1st dose | (32) | |
| 41 | 68 | female | - | Negative | AstraZeneca | 4 days post the 2nd | (33) | |
| 42 | Aseptic meningitis | 26 | Female | - | Negative | AstraZeneca | A few hours the 1st dose | (34) |
| 43 | extensive myelitis | 71 | Male | Diabetes mellitus, hypertension and Ischemic Heart Disease | Not stated | Sinopharm | 5 days after the 1st dose | (35) |
| 44 | Acute disseminated encephalomyelitis | 37 | Male | - | Negative | Sinopharm | few days to one month after the 1st dose | (36) |
| Vessel/Blood involvement | ||||||||
| 45 | Thrombotic thrombocytopenia | 70 | Female | Diabetes mellitus type 2, hypertension, and coronary artery disease | Not stated | AstraZeneca | 1day after the 1st dose | (14) |
| 46 | Vasculitis | 55 | Female | controlled sarcoidosis | Not stated | Sinopharm | 3 days after the 1st dose | (37) |
| 47 | Cerebral venous sinus thrombosis | 55 | Female | Hypertension/ a surgery history of hysterectomy 10 years ago | Negative | AstraZeneca | After the 1st dose | (38) |
| 48 | Acquired thrombotic thrombocytopenic purpura (aTTP) | 22 | Female | - | Negative | AstraZeneca | 3 weeks after the 1st dose | (39) |
| 49 | Purpuric dermatosis &lymphocytic vasculopathy | 53 | Female | History of treated breast cancer | Not stated | Sinopharm | 9 days after the 1st dose | (40) |
| 50 | 50 | Male | - | Not stated | Sinopharm | 2 months after vaccination | (40) | |
| Cardiac involvement | ||||||||
| 51 | Myocarditis | 29 | Male | - | Negative | Sputnik V | 2days after the 2nd dose | (41) |
| 52 | 26 | Male | - | Negative | AstraZeneca | 4 days after the 2nd dose | (42) | |
| 53 | 32 | Female | - | Negative | AstraZeneca | 3 days after the 1st dose | (43) | |
| 54 | Atrioventricular block | 65 | Male | - | Not stated | Sinopharm | A few days after vaccination | (44) |
| 55 | Long QT interval and syncope | 70 | Male | Hypertension (HTN) and diabetes mellitus under medical treatment | Negative | AstraZeneca | 3days after the 1st | (45) |
| Ocular involvement | ||||||||
| 56 | Paracentral acute middle maculopathy | 38 | Male | - | Negative | Sinopharm | 2 weeks after vaccination | (46) |
| 57 | Herpetic endotheliitis and stromal keratitis | 30 | Female | Hypothyroidism | Not stated | Sinopharm | 2weeks after vaccination | (47) |
| 58 | Intracranial hypertension and papilledema | 32 | Male | - | Not stated | Sputnik V | 3 days after the 1st dose | (48) |
| 59 | Acute macular neuroretinopathy | 18 | Female | - | Negative | Sinopharm | 5 days after the 1st dose | (49) |
| Liver involvement | ||||||||
| 60 | Fulminant hepatitis | 35 | Male | Controlled psychological problems | Not stated | AstraZeneca | 8 days after the 1st dose | (50) |
| 61 | Acute liver failure | 34 | Male | - | Not stated | AstraZeneca | 2 days after the 1st dose | (51) |
| Thyroid disorder | ||||||||
| 62 | Subacute thyroiditis | 34 | Female | - | Negative | COVAXIN | 11 days after the 1st dose | (52) |
| Graft rejection | ||||||||
| 63 | Corneal Graft Rejection | 36 | Female | Penetrating keratoplasty (PKP) secondary to herpes simplex keratitis (HSK) | Not stated | Sinopharm | 7 days after the 1st dose | (53) |
| 64 | 54 | Female | Not stated | Sinopharm | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



