
Submitted:
28 February 2023
Posted:
03 March 2023
You are already at the latest version
Abstract
This case study features an observation of an obese female (body mass index ≥ 30 kgm-2) who undertook a 10-day water and electrolyte fast with the aim of reducing body fat and improving physiological markers of health. A comprehensive range of physiological measures (body mass, girths, blood pressure, body fluid balance, urine osmolarity, and resting oxygen consumption), mood indicators, metabolic markers (blood ketones, blood glucose, breath ketones, urine ketones), and measurement of intake and expenditure (fluid intake, food intake, nutritional macros, steps taken, and estimated movement caloric expenditure) were measured before, during and after the fasting period to determine the effectiveness of undertaking extended therapeutic fasting for improving markers of health and weight loss. Body mass on the first day of the fast was 95.1 kg and on the tenth and final day of the fast it was 88.1 kg representing a loss of 7 kg at a rate of 0.7 kg·day1. Mean body mass in the 15 days after the fast was 88.3 ± 0.4 kg. This case study is novel in reporting key physiological and psychological markers over a 10-day fast, and in pre- and post-fast periods. A 10-day fast appears to be a safe and effective method of weight loss, mood is positively affected by fasting and weight loss from fasting can be sustained providing care is taken in the approach to post-fasting nutrition.
Keywords:
Fasting
; weight loss
; obese
; ketones.
1. Introduction
The omission of food for more than 24 hours (extended fasting) as a therapeutic treatment to reduce excess body fat and lower the risk of co-morbidities is not new, but it is rarely prescribed as a weight loss strategy, possibly because of perceived risks associated with large energy deficits [1] and the view that such an approach is not support by evidence [2]. Consequently, there is limited contemporary evidence to substantiate the potential benefits of extended fasting on health and wellbeing. In the 1960s an individual undertook a supervised 382 day fast, during which non-caloric fluids were allowed ad libitum and in which no drug treatments were administered. The fast resulted in consistent reductions in body mass with no medical complications suggesting that prolonged and controlled fasting is an effective and safe method of achieving weight loss [3]. More recent evidence has demonstrated the potential safety of such energy reduction via intermittent fasting [4], however, anthropometric, metabolic, and psychological responses to extended fasting is largely unreported.
The aim of this case study was two-fold 1) to observe the effects of a 10-day water and electrolyte fast on biochemical and metabolic markers of an obese female (body mass index ≥ 30 kg.m-2) who had previously undertaken similar extended fasts as a strategy to reduce body mass and 2) to observe anthropometric, metabolic and psychological responses to a low carbohydrate and high fat (LCHF) diet in the subsequent four-week period following the 10-day fasting period..
2. Materials and Methods
2.1. Presentation of the Participant
The participant was a 43-year-old female who had experimented with various commercial diets in the past, some of which were successful. Seven years ago, the participant had reduced body mass from 127 kg to 67 kg and had maintained that body mass (± 5 kg) for more than 3 years. 4 years ago, she experienced a cycling road accident which resulted in a traumatic injury limiting her exercise capability. Since that time her body mass had gradually increased and a calorie deficit, low-fat diet, was not realising the previously achieved results for body mass reduction. In the last 2 years, the participant reported carrying out a range of "fat loss" strategies including low carbohydrate high fat diet (LCHF) diets (25 g∙d-1 of CHO), intermittent (where meals were omitted or time between them increased) and extended (more than 24 h) fasting. The client reported positive outcomes for body mass reduction with no specific issues when fasting and when implementing a LCHF diet. The client was known to the research team and volunteered to participate in an observational study of a ten-day fast which she had planned to undertake with the intention of achieving rapid reduction in body mass and maintaining that mass reduction thereafter by adopting a LCHF diet. The client reported as early onset perimenopausal and taking hormone replacement therapy. No other medications were being taken.
Overnight fasting glucose average in the pre-fasting phase was 5.4 (± 0.9) mmol/L which was just below the threshold value where values greater than 5.5 and up to 6.9 mmol/L are considered to indicate that an individual is at high risk of developing type 2 diabetes [5]. Haemoglobin A1c (HbA1c) measures were taken at the start of the fasting period (31 mmol/mol) and at the end of the post-fasting period (29 mmol/mol). No significant change occurred with both measurements being in the range considered ‘normal’. Measurements made in pre-baseline period did not meet the threshold criteria for metabolic syndrome as defined by the revised National Cholesterol Education Program’s Adult Treatment Panel III (NCEP: ATP III cited in [6]).
2.2. Monitoring Procedures
Daily measures of body mass (Seca 285, Hamburg, Germany); blood and urine ketones (Freestyle Optimum Neo, Abbott, Maidenhead, UK); blood glucose (Freestyle Lite, Abbott, Maidenhead, UK); resting heart rate and blood pressure (Intellisense M2 Basic, Omron, Kyoto, Japan); macronutrient, electrolyte, water and caffeinated beverage intake were recorded using a mobile phone application (Lifesum Diet and Macro Tracker, Lifesum AB); physical activity was monitored using a wrist worn activity tracker (Apple Watch Series 2, Apple Inc., California, USA) which gave an estimation of ‘movement calories’ and steps taken. The Positive and Negative Affect Schedule (PANAS) designed to determine both positive and negative emotions and is reported to be reliable and internally consistent [7] was also recorded daily.
Body composition using bio-electrical impedance analysis (720, InBody, Seoul, Korea), resting metabolic rate (GEM Open Circuit Indirect Calorimeter, GEMNutrition, UK) and urine osmolality (Pocket Osmocheck, Vitech Scientific, UK) were measured daily during FAST and at 15, 8 and 1 days prior to FAST, on day one of LCHF and each week for 4 weeks after FAST. Hips, waist and right thigh girths were measured 15, 8 and 1 days prior to FAST on day 7 of the fast using steel anthropometric tape, and on day one of the LCHF diet phase. Measurements of girths continued twice a week, every 3 or 4 days, throughout the LCHF phase with the last measurement on 28 days post FAST.
3. Results
For the anthropometric and physiologic variables that were measured daily, in all phases on the morning of the start of FAST and LCHF there were a total of 16 baseline, 10 FAST and 27 days of LCHF data.
Before FAST the participant had a diet with a macronutrient content of 79 ± 39 g∙day-1 carbohydrates, 154 ± 33 g∙day-1 fat, and 75 ± 28 g∙day-1 protein, equaling 2086 ± 305 kcal∙day-1. Daily activity was 632 ± 118 kcal of ‘movement Calories’ and 9908 ± 3201 steps∙day-1. The details and proportions of the macro nutrients for each phase of the study are detailed in Table 1.
During the FAST the participant consumed water (still and sparkling), tea (black and herbal) or black coffee. The participant also took a multi-vitamin (Multivitamins & Minerals Formula, Nu U Nutrition, York, UK) and salt tablets (Saltstick Caps, Saltstick, California, USA; containing 100 IU vitamin D3, 22 mg calcium, 11 mg magnesium, 350 mg chloride, 215 mg sodium, and 63 mg sodium) daily. Daily activity was 587 ± 136 kcal∙day--1 of ‘movement calories’ and 8604 ± 3070 steps∙day--1.
After the fasting period the participant ate within an 8-hour window (12 pm to 8 pm) and maintained a very low carbohydrate high fat diet (LCHF) with an average (± SD) macronutrient intake of 24 ± 12 g∙day-1 of carbohydrates, 118 ± 45 g∙day--1 of lipid, and 74 ± 30 g∙day-1 of protein. Total caloric intake was 1479 ± 514 kcal∙day-1 and daily activity was 588 ± 144 kcal of ‘movement Calories’ and 8283 ± 2592 steps∙day-1.
BASE Mean body mass was 93.6 ± 1.00 kg body mass on the first day of FAST was 95.1 kg and on the tenth day was 88.1 kg representing a loss of 7 kg at a rate of 0.7 kg·day-1. Mean body mass in the 15 days after the fast was 88.3 ± 0.4 kg. Final body mass at 4 weeks post fast was 86.7 kg representing a total change of 7.2 kg from starting body mass. Changes in body mass were accompanied with decreases in resting metabolic rate, body fat mass and skeletal muscle mass (Figure 1).
Mean hip, waist, and thigh girths before the fast were 119.5 ± 0.9, 97.4 ± 0.4 and 67.9 ± 0.3 cm respectively and decreased to 116, 89 and 66 cm immediately after the fast representing a total change of 13.8 cm. The mean hip, waist and thigh girths 4 weeks post intervention were 116.2 ± 0.5, 90.8 ± 0.7 and 66.7 ± 0.4 cm.
Total body water (Figure 1) decreased in accordance with changes in body mass and composition, whilst morning urine osmolality indicated euhydration (<800 mOsmol·kg-1·H2O) throughout the observed period (676 ± 167 mOsmol·kg-1·H2O). Fluid intake before the fast was 2673 ± 205 ml·day-1 and increased to 4140 ± 833 ml·day-1 during the fast and was 3441 ± 866 ml·day-1 after the fast.
Measurements of positive and negative affect were recorded daily to indicate mood state [7]. In the BASE pre-fasting phase, positive mood was lower and negative mood was higher than both the FAST and POST phases. Split middle trend analysis for single-case data [8] indicates a decreasing mood trend during BASE, a strong increasing mood trend during FAST and a very slight decreasing mood trend during LCHF.
Blood ketones increased to an average of 3.4 ± 1.9 mmol.L-1 during the FAST from 0.2 ± 0.1 mmol.L-1 during BASE. Blood glucose decreased during the fasting phase from an average of 5.4 ± 0.9 mmol.L-1 before the FAST to an average of 3.9 ± 0.7 mmol.L-1. It took 3 days to reach sustained elevated levels of ketones (>3.7 mmol.L-1) as shown in Figure 2. Following a LCHF diet post-fasting resulted in ketone levels remaining elevated above pre-fasting measures between 0.7 and 2.7 mmol.L-1. Glucose levels were overall lower during LCHF with a range of measures between 3.6 and 5.8 mmol.L-1 compared to a range of 3.2 to 7.3 mmol.L-1 during BASE.
4. Discussion
This case study is novel in reporting key physiological and psychological markers over a 10-day fast, and pre- and post-fast periods. The major outcomes from this case study were that; 1) 10-day fasting, carried out with sufficient hydration and electrolyte replacement, appears to be a safe and effective method of weight loss (the a priori goal of reducing body mass by 5kg was attained). 2) Mood is positively affected by fasting, and 3) weight loss from fasting can be sustained providing care is taken in the approach to post-fasting nutrition.
Monitoring of blood glucose, ketones, hydration status and mood state indicates the therapeutic status of the fasting and ketosis. We recommend providing dietary guidance on return to eating to optimise therapeutic outcomes.
As this was an opportunistic single participant case study, some baseline (BASE) and post-fast (LCHF) data was limited to between 3 and 15 data points and only estimates of typical error could be used to indicate differences between phases of the intervention. Typically, more than 16 data points are required for statistical analysis in single-case experimental designs [9] we have taken the position that both visual analysis of graphed data and appropriate statistical procedures can serve as judgment aids to determine whether changes have occurred over time, both within and between experimental conditions [10]. When changes in variables between phases are not easy to detect by visual analysis findings should be viewed with caution in the absence of supporting statistical analysis.
5. Conclusions
Fasting for 10 days is an unusual weight loss technique and practitioners claim it may be unsafe, a ‘fad’, and unsustainable for longer term weight loss [2]. However, our findings in this case study clearly show that a 10-day fast appears to be a safe method for weight loss and that weight loss is sustained after 4 weeks without reduction in mood. Other research into intermittent and extended fasting also demonstrates the low-risk nature of therapeutic fasting and that it should be considered as a suitable treatment for weight loss [11] We recommend that future research should examine the response to fasting in a random control trial. However, recruiting individuals to be able to carry out such research will be challenging.
Author Contributions
Conceptualization, all authors; methodology, all authors; formal analysis, A.P., A.R., M.R. and D.C.; investigation, A.P., A.R., D.H and D.C; resources, A.P. and A.R..; data curation, A.P..; writing—original draft preparation, all authors; writing—review and editing, A.P., A.R. and D.C..; visualization A.P.; supervision, A.P.; project administration, A.P. All authors have read and agreed to the published version of the manuscript. All authors have contributed substantially to the work reported.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Ethics Committee of Sheffield Hallam University (ER6023620).
Informed Consent Statement
Written informed consent has been obtained from the participant to publish this paper.
Data Availability Statement
Data may be available upon request. Some data may be personal to the single participant and therefore may not be shared.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Veech, R.L. The therapeutic implications of ketone bodies: the effects of ketone bodies in pathological conditions: ketosis, ketogenic diet, redox states, insulin resistance, and mitochondrial metabolism. Prostaglandins Leukot. Essent. Fatty Acids 2004, 70, 309–319. [Google Scholar] [CrossRef] [PubMed]
- Hart, K. Fad diets and fasting for weight loss in obesity, in: Ad. Nutr. Diet. Obes., Hankey, C.; Publisher John Wiley & Sons Ltd., UK, 2018; pp. 177-182. Available online: https://cpncampus.com/biblioteca/files/original/8b1d39783657ab16f2a9d1df431ef11d.pdf.
- Stewart W.K. and Flemming L.W. Features of a successful therapeutic fast of 382 days' duration. Postgraduate Medical Journal 1973, 49, 203-209. [CrossRef]
- Varady, K.A., Bhutani , S., Church, E.C., Klempel, M.C. Short-term modified alternate-day fasting: a novel dietary strategy for weight loss and cardioprotection in obese adults. The American Journal of Clinical Nutrition 2009, Volume 90, Issue 5, 1 November 2009, Pages 1138–1143. [CrossRef]
- National Institute for Health and Care Excellence (NICE) Type 2 diabetes in adults: management, NICE guideline [NG28]. Last updated 2022. Available online: https://www.nice.org.uk/guidance/ng28.
- Grundy S.M., Cleeman, J.I., Daniels, S.R., Donato, K.A., Eckel, R.H., Franklin, B.A. Diagnosis and management of the metabolic syndrome: an American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation 2005. 112, 2735–2752. [CrossRef]
- Watson, D., Clark, L.A., Tellegen, A. Development and validation of brief measures of positive and negative affect: The PANAS scales. J. Pers. Soc. Psychol. 1988, 54, 1063–1070. [CrossRef]
- Fisher, W. W., Kelley, M. E., and Lomas, J. E. Visual aids and structured criteria for improving visual inspection and interpretation of single-case designs. Journal of Applied Behavior Analysis 2003, 36,387–406. [CrossRef]
- Kinugasa, T., Cerin, E. Hooper, S. Single-subject research designs and data analyses for assessing elite athletes' conditioning. Sports Med. 2004, 34 (15) 1035-1050. [CrossRef]
- Wolery,M. and Harris, S.R. Interpreting results of single-subject research designs. Phys. Ther. 1982, 62(4) 445-452. [CrossRef]
- Johnstone, A.M. (2007) Fasting – the ultimate diet? Obes. Rev. 2007, 8, 211–222. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Resting metabolic rate, body mass (A), fat mass, skeletal muscle mass, and total body water (B), measured every 3-days pre and post fast, and daily during the fasting phase.
Figure 1.
Resting metabolic rate, body mass (A), fat mass, skeletal muscle mass, and total body water (B), measured every 3-days pre and post fast, and daily during the fasting phase.

Figure 2.
Blood ketones and blood glucose measured daily.
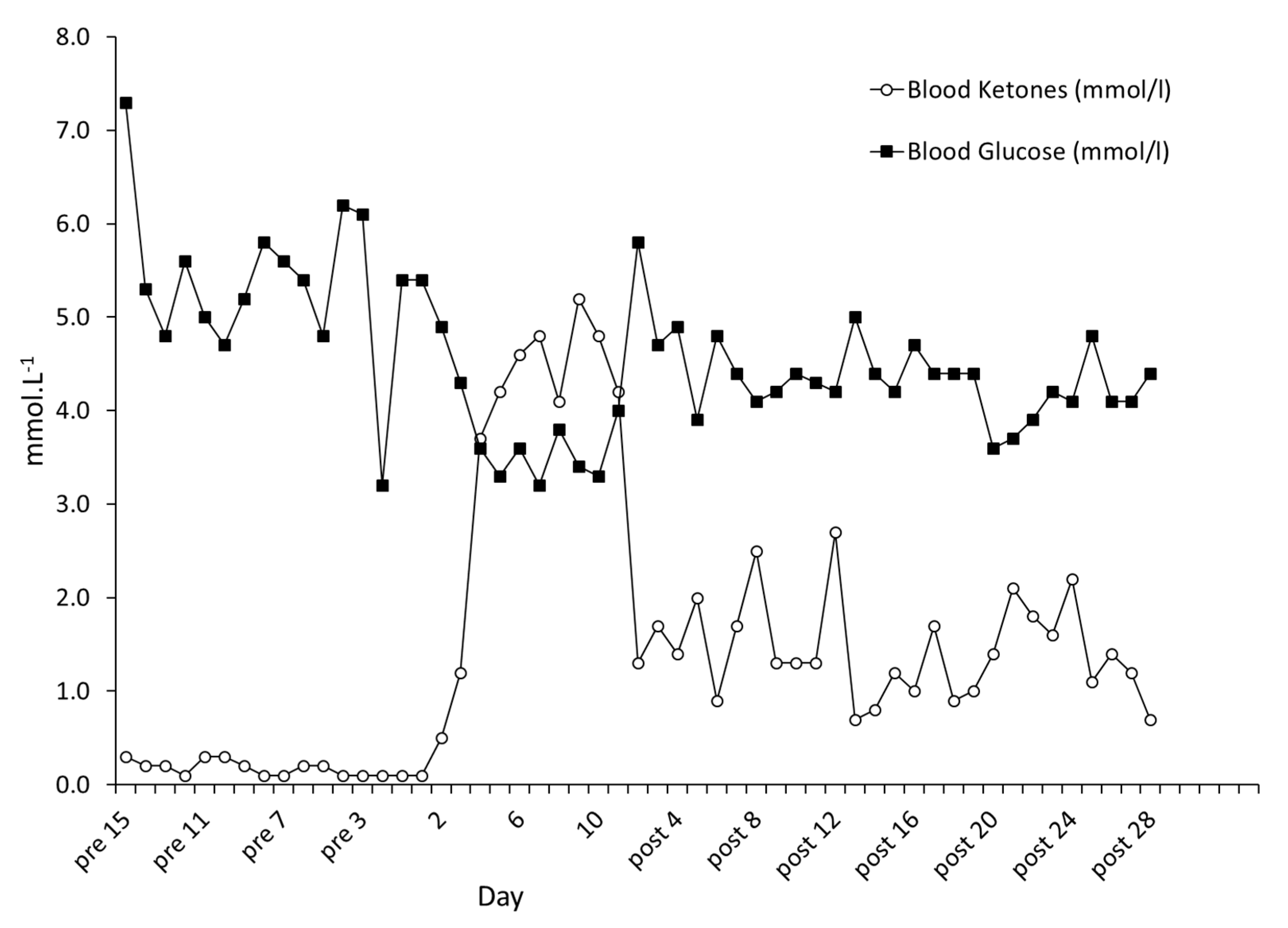

Table 1.
Amounts of macronutrients during BASE and LCHF phases.
| Carbohydrate (g.kg-1) |
Protein (g.kg-1) |
Fat (g.kg-1) |
|
| BASE average ± SD | 0.8 ± 0.4 | 0.8 ± 0.3 | 1.6 ± 0.4 |
| BASE min-max (range) | 0.2 – 1.7 (1.5) | 0.3 – 1.3 (1.0) | 0.9 – 2.1 (1.2) |
| LCHF average ± SD | 0.3 ± 0.1 | 0.8 ± 0.3 | 1.3 ± 0.5 |
| LCHF min-max (range) | – 0.6 (0.6) | 0.2 – 1.8 (1.6) | 0.4 – 2.5 (2.1) |
| Carbohydrate (%) |
Protein (%) |
Fat (%) |
|
| BASE average ± SD | 15 ± 8 | 14 ± 6 | 67 ± 13 |
| BASE min-max (range) | 5 – 35 (30) | 7 – 17 (10) | 41 – 87 (46) |
| LCHF average ± SD | 7 ± 3 | 20 ± 6 | 71 ± 7 |
| LCHF min-max (range) | 1 – 11 (10) | 12 – 35 (23) | 41 – 87 (46) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



