
Submitted:
28 February 2023
Posted:
06 March 2023
You are already at the latest version
Abstract
Adaptation to external forces relies on a well-functioning proprioceptive system including muscle spindle afferents. Muscle length-tension control in reaction to external forces is most important regarding the Adaptive Force (AF). This study investigated the effect of different procedures, which are assumed to influence the function of muscle spindles, on the AF. 19 elbow flexors of 12 healthy participants were assessed by an objectified manual muscle test (MMT) with different procedures: regular MMT, MMT after pre-contraction (self-estimated 20% MVIC) in lengthened position with passive return to test position (CL) and MMT after CL with a second pre-contraction in test position (CL-CT). During regular MMTs, muscles maintained their length up to 99.7±1.0% of the maximal AF (AFmax). After CL, muscles started to lengthen at 53.0±22.5% of AFmax. For CL-CT, muscles were again able to maintain the isometric position up to 98.3±5.5% of AFmax. AFisomax differed highly significantly between CL vs. CL-CT and regular MMT. CL is assumed to generate a slack of muscle spindles which led to a substantial reduction of the holding capacity. This was immediately erased by a pre-contraction in test position. The results substantiate that muscle spindle sensitivity seems to play an important role for neuromuscular functioning and musculoskeletal stability.
Keywords:
Maximal isometric adaptive force
; Holding capacity
; Muscle stability
; Neuromuscular functioning
; Neuromuscular control
; Motor control
; Muscle spindle
; Muscle physiology
; Regulatory physiology
1. Introduction
The term proprioception, presumably first named in 1882 by Ardigo [1], includes the senses of tension and force, effort, balance as well as the senses of limb position and movement [2]. The term kinaesthesia, introduced by Bastian in 1888 [3], refers to the latter two sensations [2]. Proske and Gandevia argued “that muscle spindles play the major role in kinaesthesia, with some skin receptors providing additional information.”[2]. It is known that muscle spindles provide information to the central nervous system, e.g., muscle length and limb position, changing status of muscle tone and movement [4]. An elaborated overview on the current neurophysiological knowledge about muscle spindles was given by Macefield & Knellwolf [5]. Most investigations regarding muscle spindles considered the behavior under conditions like stretching or contraction [5,6,7,8,9,10]. Meanwhile, it is commonly accepted that a slack in muscle spindles can occur [11,12]. This was based on the early suggestion that “…following movements the intrafusal fibre will always form stable bridges; when this is at a long length the fibre on returning to its rest length will be (stiff but) slack…” [13]. Blum et al. presented a mathematical model in 2020 which underpins the experimental assumptions by providing information that under particular conditions a slack of spindle cells could appear.[14] The ability of muscle fibres to fall slack is considered as one important consequence of the thixotropic behavior of muscles [8,15,16]. Shortened or slacked muscle spindles are mainly examined in terms of reflex reactions [2,5,17,18,19,20]. The research group around Proske introduced a procedure in humans which is suggested to generate a slack in muscle spindles: “…if the muscle is stretched, contracted at the stretched length and held there for several seconds, stable cross-bridges will form at the longer length (…). On return to the initial length, the intrafusal fibres, stiffened by the stable cross-bridges, are unable to shorten themselves and fall slack.” [15]. They showed that this lowered background discharge rate [15,21]. Gregory et al. found that the stretch reflex was significantly reduced by this procedure, specifically, when a muscle was passively brought into middle length (test position) after it has been contracted briefly in a lengthened position with 25% of the maximal voluntary isometric contraction (MVIC) [18]. The procedure prior to the reflex test was assumed to lead to a slack in muscle fibres, both extrafusal and intrafusal [18]. Under such conditioning the muscle spindles provide sensory information which are not in line with the overall muscle length. This was discussed to lower the reflex intensity [18]. The phenomenon of a reduced reflex following such a ‘slack-procedure’ was immediately revoked by a short submaximal voluntary contraction (2 s at 5%, 10% or 25% of MVIC) at the test length. Hereinafter, the reflex response increased significantly, especially for a pre-contraction of 10% of MVIC. For 25% of MVIC no further significant increase occurred. It was assumed that the slacked muscle spindles get tightened again by that second contraction in test length [18]. Applying a percutaneous electrical muscle stimulation (assumed to be solely extrafusal) instead of the voluntary second contraction did not lead to this normalization of reflex activity. Therefore, it was assumed that a voluntary fusimotor activation of at least 10% of MVIC is necessary to fully remove the slack in muscle spindles [18]. Héroux and colleagues showed for vastus lateralis muscle that already 5% of MVIC was sufficient to reduce muscle slack length [20]. Meanwhile, it is common knowledge that the reflex behavior of muscles can change in dependence of the previous history of contraction and length changes.
Although investigations on such particular pre-conditioning of muscle fibres mostly use reflex behavior as target parameter it is conceivable that also other motor functions can be affected thereby. The sense of force, for example, was found to not react to a preceding contraction in lengthened position [22]. To our best knowledge, there are no studies which investigated muscle strength after such pre-conditioning – except for studies regarding common stretching exercises [6,10,23] which clearly differ from the procedure meant here. Investigations on the effect of conditioning procedures as mentioned before on muscle strength are indicated. Since muscle spindles are especially relevant for length control, the effect of a presumed slack of muscle spindles on adaptive capabilities in the sense of length-tension control in reaction to external forces are especially relevant.
A promising new approach to assess the adaptability of the sensorimotor system is the Adaptive Force (AF). “AF not only requires muscle strength but also sensorimotor control. It reflects the neuromuscular functionality to adapt adequately to external forces with the intention of maintaining a desired position or movement.” [24]. An appropriate adaptation to external forces provides dynamic stability of the musculoskeletal system. Adaptation to external forces doubtlessly relies, inter alia, on a well-functioning proprioceptive system including muscle spindle afferents. The latter provide information about muscle length and its change which is inevitable for appropriate motor responses to external impacts. Hence, it was questioned whether a pre-conditioning procedure like the one mentioned above [15,18] would affect the AF, and thus, the musculoskeletal stability. In case the stabilizing holding capacity of muscles would be impaired, instability and, thus, risk of injury could be a consequence. Despite an abundance of investigations, the occurrence of muscle or tendon injuries in sports but also in everyday life without trauma or other comprehensible causation is still an unsolved enigma. The detailed mechanisms of such injuries remain unclear. Researchers mainly agree that damages mostly occur during non-contact actions while muscles try to decelerate external loads [25,26]. It was suggested that a crucial mechanism could be “when active muscular restraints are unable to adequately reduce joint torques during dynamic movements involving deceleration and high forces“ [27,28,29]. Hence, investigating the AF and its reactions to pre-conditionings which presumably alter muscle spindle afferents might be a beneficial approach also regarding further information on injury mechanisms.
This study investigated the behavior of AF of elbow flexors – as an approach to describe musculoskeletal stability and neuromuscular functioning – after two different procedures which are assumed to influence muscle spindles. The crucial parameter of AF is the maximal isometric AF (maximal holding capacity; AFisomax) which characterizes the maximal force under which a muscle is able to stabilize a given limb position (isometric condition) against an increasing external force. In case the muscle starts to lengthen during the external force increase (exceeding AFisomax), the force usually increases further during the subsequent eccentric action until the maximal AF (AFmax) is reached.
It has been shown previously that AFisomax was significantly reduced under disturbing conditions like unpleasant smell or imagery in healthy participants, whereby AFmax stayed on the baseline level [30,31,32]. Recently it was shown that the holding capacity was significantly reduced in patients with Long COVID and stabilized with recovery [33,34]. The AFmax again did not show this behavior and was on a considerably high level already in Long COVID state. Hence, the maximal holding capacity (AFisomax) seems to be especially sensitive to inputs.
Bases on these findings it was hypothesized that (1) AFisomax would be significantly reduced by a brief submaximal pre-contraction in lengthened position followed by a passive return to test position (procedure CL), whereby AFmax would not be affected. (2) An additional brief pre-contraction in test position (directly after CL-procedure; procedure CL-CT) would immediately revoke the reduction of the holding capacity.
The study gains novel insights regarding the behavior of musculoskeletal stability and neuromuscular functioning in the sense of AF after specific procedures which are assumed to manipulate the function of muscle spindles. As part of muscle physiology this is relevant for the understanding of neuromuscular control during stabilizing actions and, hence, might provide further insights into injury mechanisms.
2. Materials and Methods
Measurements were conducted at one appointment at the Neuromechanics Laboratory of the University of Potsdam (Potsdam, Germany). One experienced male tester (m, 65 yrs. old, 185 cm, 87 kg, 27 yrs. of manual muscle test (MMT) experience) performed all tests of the elbow flexor muscles which were objectified by a handheld device.
2.1. Participants
Twelve healthy participants (m = 9, f = 3) volunteered to participate in this study. Females were 31.33 ± 6.81 yrs. old (range: 26 – 39), weighted 56.33 ± 3.79 kg and were 170.00 ± 6.00 cm tall, males accordingly 30.89 ± 9.23 yrs. (range: 22 – 52), 79.22 ± 12.42 kg and 184.33 ± 8.92 cm, respectively. Exclusion criteria were any current orthopaedic diagnosis, injuries and/or surgery of cervical spine and upper extremities within the last 12 months. Furthermore, an affected neuromuscular function of elbow flexors, assessed by a MMT in the sense of a break test (see below) prior to the measurements, led to exclusion as well as any complaints during its assessment. Elbow flexors of both sides were examined. Four participants could only be measured on one side due to an affected neuromuscular control. One further participant needed to leave after measurements of the first side. In total, 19 elbow flexor muscles were examined and considered for evaluation (n = 12 left, n = 7 right).
The study was conducted according to the guidelines of the Declaration of Helsinki and was approved by the Ethics Committee of the University of Potsdam, Germany (protocol code 35/2018; 17 October 2018). All participants gave their written informed consent to participate.
2.2. Technical equipment
A wireless handheld device (Figure 1a) was used to record the reaction force (dynamometry) and angular velocity (gyrometry) during the MMTs [30,31,32,33,34,35]. It combines strain gauges (co. Sourcing map, model: a14071900ux0076, precision: 1.0 ±0.1%, sensitivity: 0.3 mV/V) and kinematic sensors (Bosch BNO055, 9-axis absolute orientation sensor, sensitivity: ±1%). Data was recorded with a sampling rate of 180 Hz, AD converted and transmitted via Bluetooth to a tablet (Sticky notes, comp.: StatConsult, Magdeburg, Germany).
2.3. Manual Muscle Tests
The AF was examined by means of a MMT in the sense of a break-test. This has been described previously [30,31,32,33,34,35,36]. In brief, the task of the participant was to maintain the isometric test position despite an external increasing force applied by the tester. Hence, the participant had to perform a holding isometric muscle action (HIMA) [37,38,39]. The tester applied the external force rise by pushing against the participant’s limb in direction of muscle lengthening. The suggested optimal force profile (S-shaped) was described in detail by Bittmann et al. [35]. This force profile needs to be reproducible to achieve valid empirical data [35]. The tester of this study proofed his ability to test reproducibly (CV = 4.6%; ICC = 0.995) [35]. Basically, two qualities during MMT could arise [30,31,32]: (1) If the participant was able to maintain the isometric starting position during the entire force increase applied by the tester, the MMT was rated as “stable”. This does not per se test the maximal holding force of the participant, since the applied force under stable conditions depends on the tester’s maximal force. The tester was instructed to increase the force up to a considerably high intensity. If the tester’s pushing force exceeded the maximal holding capacity of the participant, the limb gave way during the force increase. The MMT was rated as “unstable”. The force is usually increasing further during the subsequent eccentric phase until the maximal AF (AFmax) is reached.
Before and after the measurements using the MMT in the sense of a break test to assess the AF (named MMT in the following) the MVIC was assessed by means of a make-test [36]. Actually, this is also a manual muscle test. For better differentiation, it will be named MVIC test in the following. For this, the participant had the task to push as strong as possible against the handheld device which was placed in the palm of the tester who just provided a stable resistance. Hence, the participant performed a pushing isometric muscle action (PIMA) [37,38,39].
2.4. Setting and Measurement Procedure
The setting for measuring elbow flexor muscles is shown in Figure 1b. The participant was placed supine. The starting (test) position of all tests was a flexed elbow joint in 90° and a maximally supinated forearm. The tester placed the handheld device in his palm and contacted the distal part of the forearm. For standardization of the test position the contact point at the forearm was marked.
Two MVIC tests and two MMTs without any procedure (regular MMT) were performed for reference – each one at the start and one at the end. For that, the participants took up the test position by themselves. In between four MMTs were conducted after two different procedures:
-
Procedure CL: pre-contraction in lengthened position with passive returnFrom the test position, the elbow joint was brought passively into maximal extension by the tester (neutral zero position with maximal supination of the forearm). In that position, the participant was instructed to push shortly (~1 s) with self-estimated 20% of the MVIC against a stable resistance which was provided by the tester. The handheld device recorded the force of pre-contraction between tester’s palm and participant’s forearm. Afterwards the tester guided the limb back to the test position of the MMT. To ensure that the elbow flexors stayed passively thereby and did not support the flexion actively the participant should push slightly against the tester (activation of elbow extensors) during the return. Due to the passive shortening after pre-contraction in lengthening position, this procedure was assumed to produce a slack in muscle fibres. Back in test position after the CL procedure, the tester started the MMT after ~2 s to achieve a temporal sequence similar to the second procedure.
-
Procedure CL-CT: CL with subsequent second pre-contraction in test positionFor that, procedure CL was extended by a second pre-contraction immediately after the forearm was returned to test position. The second contraction should also amount self-estimated ~20% of the MVIC and should last ~1 s. Immediately after this second pre-contraction the MMT was performed to assess the AF. It was assumed that procedure CL-CT eliminates the slack in muscle fibres. A minimal intensity of 10% of the MVIC was regarded as necessary to resolve the reflex activity [18]. Hence, 20% of the MVIC was chosen to ensure that this minimal level would be certainly achieved (considering that the self-estimation would show some variance).
Both procedures were practiced before measurements and were accompanied by commands starting from the test position: ‘stay relaxed‘ (forearm was positioned passively into neutral zero position with maximal supination); ‘contract’ (short contraction (1 s) with ~20% of MVIC), ‘stop’ (contraction was released), ‘stay relaxed and push’ (passive repositioning of the forearm to 90° elbow flexion with slight activity of elbow extensors), followed by either ‘stay relaxed’ (wait for 2 s) and ‘hold’ (MMT started) for procedure CL or by ‘contract’ (second short contraction), ‘stop’ (release contraction) and ‘hold’ (MMT started) for procedure CL-CT. Both procedures were alternately conducted twice.
In total, eight trials were performed: (1) MVIC test, (2) regular MMT, (3) MMT after CL, (4) MMT after CL-CT, (5) MMT after CL, (6) MMT after CL-CT, (7) regular MMT, and (8) MVIC test. The tester rated the stability of the participant’s resistance during the MMTs with ‘stable’ or ‘unstable’.
2.5. Data processing and statistical analyses
The evaluation was performed according to Schaefer et al. [30,31,32,34]. Force and gyrometer signals were analysed by use of DIAdem 2017 (National Instruments, Austin, TX, USA). To ensure equidistant time channels, signals were interpolated (linear spline, sampling rate: 1000 Hz). Furthermore, Butterworth low pass filter was applied (cut-off frequency 20 Hz, filter degree 5). The following parameters were extracted:
- MVIC: the peak value of each MVIC test was determined. The peak value of first MVIC test refers to the individual’s MVIC. The second MVIC test was analysed to investigate possible fatiguing effects in comparison to the initial MVIC.
- Maximal Adaptive Force (AFmax): the peak value of each MMT trial was selected and referred to AFmax of a single MMT. This was either reached during isometric actions (stable MMT) or during eccentric ones (unstable MMTs). For the former, AFmax = AFisomax. For the latter, AFmax > AFisomax (Figure 2).
- Maximal isometric Adaptive Force (AFisomax): this refers to the highest force value under isometric conditions during the MMT. The gyrometer signal was used to determine if the forearm moved in direction of elbow extension during the force increase (breaking point) – indicating muscle lengthening. If muscle lengthening occurred, the force value at the breaking point referred to AFisomax (Figure 2a). In case the isometric position was maintained up to the peak value, AFisomax = AFmax (Figure 2b). For a detailed description see [30,31,32,34].
- Slope: the difference quotient was used to determine the slope before the breaking point. Reference points were time and force of 70% and 100% of the averaged AFisomax of all as unstable assessed MMTs of one muscle. The decadic logarithm was taken from slope values since the slope rise was exponential [lg(N/s)].
Additionally, the ratios , were calculated (%).
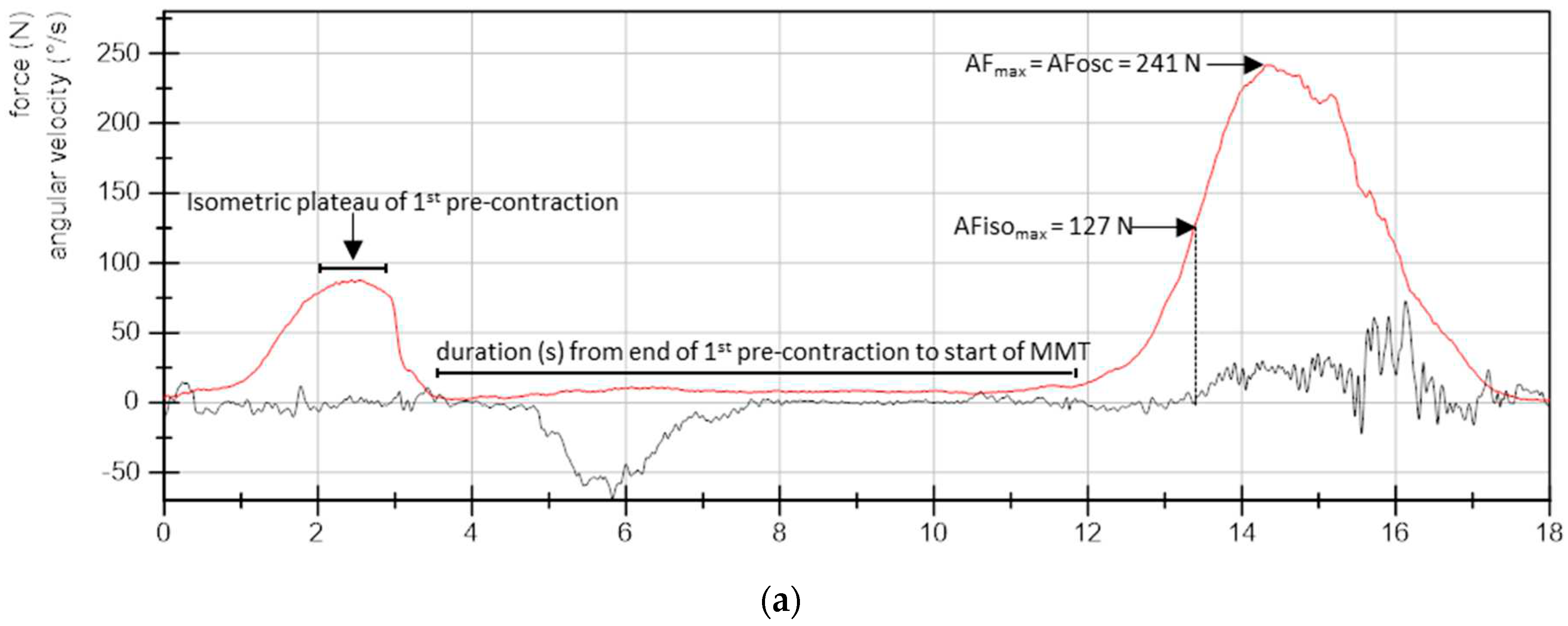
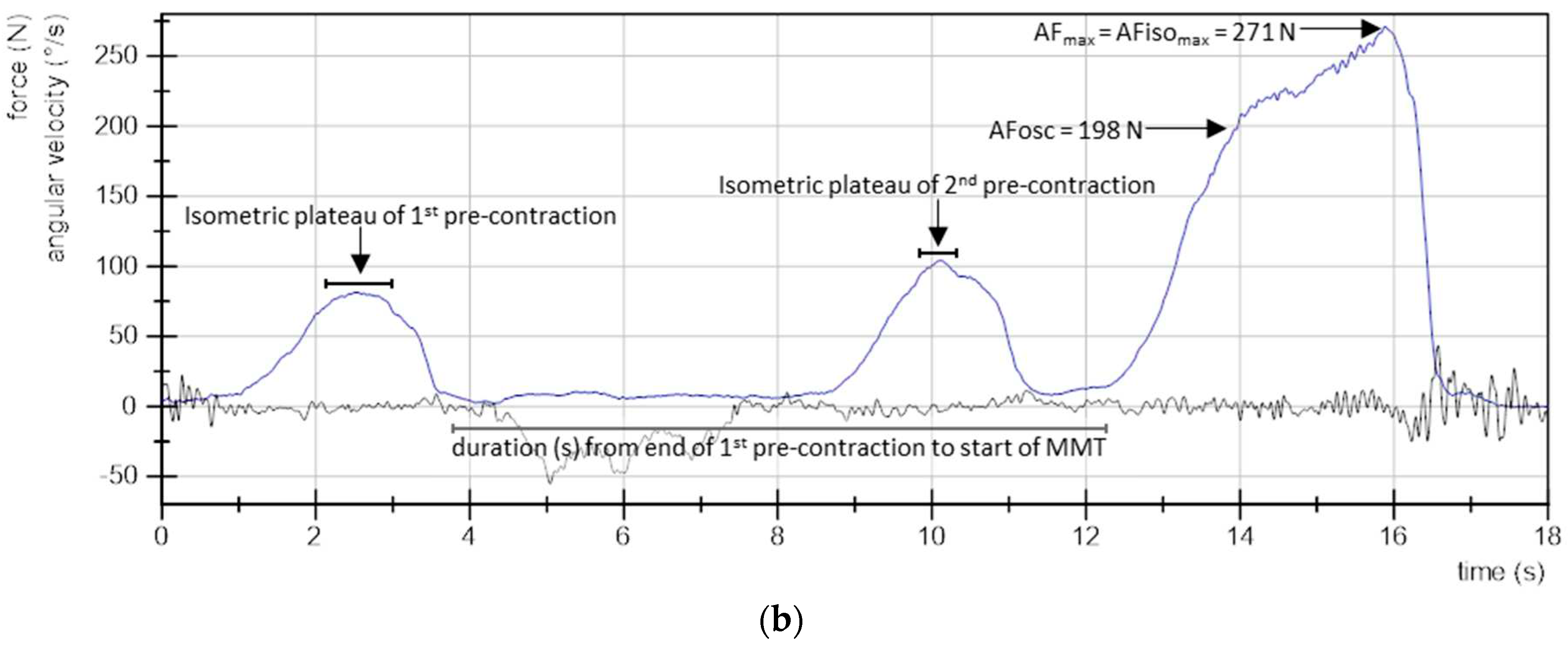
To compare the three pre-contractions (1st of procedure CL, 1st and 2nd of procedure CL-CT), the averaged force (related to MVIC (%)) as well as the duration (s) of the isometric plateaus were captured (Figure 2). Interval borders for the isometric plateaus were determined by setting 90% of the peak value of the related pre-contraction as reference. Furthermore, the duration (s) from the end of 1st pre-contraction to the start of MMT was compared between both procedures (CL vs. CL-CT) (Figure 2).
Figure 2.
Curve characteristics. Exemplary curves of force (N) and angular velocity (°/s) of (a) one MMT after procedure CL (pre-contraction in lengthened position with passive return) and (b) one MMT after procedure CL-CT (CL with a second pre-contraction in test position). The evaluated parameters are indicated: maximal Adaptive Force (AFmax), maximal isometric AF (AFisomax), AF at onset of oscillations (AFosc); isometric plateaus of pre-contractions for calculation of the averaged force and duration of pre-contractions as well as the duration from end of 1st pre-contraction to start of MMT.
Figure 2.
Curve characteristics. Exemplary curves of force (N) and angular velocity (°/s) of (a) one MMT after procedure CL (pre-contraction in lengthened position with passive return) and (b) one MMT after procedure CL-CT (CL with a second pre-contraction in test position). The evaluated parameters are indicated: maximal Adaptive Force (AFmax), maximal isometric AF (AFisomax), AF at onset of oscillations (AFosc); isometric plateaus of pre-contractions for calculation of the averaged force and duration of pre-contractions as well as the duration from end of 1st pre-contraction to start of MMT.
The arithmetic means (M), standard deviations (SD) and 95%-confidence intervals (CI) of all parameters were calculated for regular MMT, MMT after CL, and MMT after CL-CT. Since AFmax of regular MMTs before and after MMTs with procedures did not differ significantly (t(18) = 0.777, p = 0.447, two-tailed), they were considered together. Two trials of different participants (first MMT after procedure CL and first MMT after procedure CL-CT) were excluded due to technical issues and elbow pain during measurement, respectively.
For statistical evaluation SPSS Statistics 27 (Windows, Version 28.0. Armonk, NY, USA: IBM Corp.) was used. Main comparisons were the analyses of differences between regular MMT, MMT after procedure CL and MMT after procedure CL-CT for all parameters. Normal distribution was checked by Shapiro–Wilk test. Because repeated measures ANOVA (RM ANOVA) is considered to be robust against violation of normal distribution [40,41], it was also used if not all groups were normally distributed. This was the case for and slope (each two groups were not normally distributed). If sphericity was not fulfilled (Mauchly test: p < 0.05), the Greenhouse–Geisser correction was applied (FG). Effect size partial eta squared (η2) was estimated by SPSS. For pairwise comparisons, Bonferroni correction was applied (padj) and effect size Cohen’s dz was given which was interpreted as “small” (0.2), “moderate” (0.5), “large” (0.80), and as “very large” (1.3) [42].
Additionally, the MVIC before and after MMT trials as well as the duration from end of 1st pre-contraction to start of MMT (comparability between procedures CL and CL-CT) were compared by paired t test (two-tailed). Effect size was given by dz. Significance level was set at α = 0.05.
3. Results
3.1. Pre-contractions: duration and force
The values of pre-contraction phases for procedures CL and CL-CT are given in Table 1. RM ANOVA revealed no significant differences between the relative forces of pre-contractions (FG(1.23, 22.16) = 2.942, p = 0.094). The duration of pre-contraction phases revealed a significant main effect (F(2, 36) = 17.901, p < 0.001, η² = 0.499). Pairwise comparisons showed a significantly shorter 2nd pre-contraction for procedure CL-CT vs. 1st pre-contraction of both procedures (padj < 0.001 for both; CL vs. 2nd contraction of CL-CT: dz = 1.143 and 1st vs. 2nd contraction of CL-CT: dz = 1.190). Generally, the self-estimated amount of pre-contraction ranged from 10.30% to 44.46% of the MVIC for CL, and 11.51% to 46.91% and 14.82% to 43.48% for 1st and 2nd pre-contraction of CL-CT, respectively. Hence, the required minimal force for pre-contractions was reached for all trials. Furthermore, the duration from the end of 1st pre-contraction to the start of MMT did not differ significantly for both procedures (t(18) = 0.325, p = 0.650). Hence, the pre-contraction conditions can be regarded as similar between both procedures as prerequisite for further considerations.
3.2. Parameters of Adaptive Force in comparison of the different procedures
The values of all AF parameters are given in Table 2. The requirement for a valid comparison between the procedures was given, since the slope of force increase did not differ significantly between procedures CL and CL-CT (padj = 0.180). However, the slope of regular MMT was significantly lower compared to procedures CL (padj < 0.001, dz = 1.662) and CL-CT (padj = 0.002, dz = 0.977).
AFmax was statistically similar comparing all procedures (regular, CL, CL-CT) (Table 2, Figure 3a), although close to significance. The lowest value was found for MMT after procedure CL-CT, the highest for MMT after procedure CL.
For AFisomax, RM ANOVA was found to be significant (Table 2). Pairwise comparisons revealed a significantly lower AFisomax for procedure CL compared to regular MMT (padj < 0.001, dz = 1.809) and to procedure CL-CT (padj < 0.001, dz = 1.434). AFisomax did not differ significantly between regular MMT and procedure CL-CT (padj = 0.555) (Figure 3b). By contracting the muscle in lengthened position with ~25% of the MVIC and passive return to test position (procedure CL), AFisomax was reduced clearly by −45.10 ± 25.18% compared to regular MMT. In case a second slight pre-contraction was performed in middle-length test position (procedure CL-CT), AFisomax was similar to the value reached during regular MMT (−3.81 ± 12.37%).
Figure 3.
95%-confidence intervals including arithmetic mean and standard deviation (error bars) comparing regular MMT (reg, grey), MMT after procedure CL (red) and MMT after procedure CL-CT (blue) for the different parameters: (a) maximal Adaptive Force (AFmax), (b) maximal isometric AF (AFisomax), (c) AF at onset of oscillations (AFosc), (d) ratio AFisomax to AFmax, (e), ratio AFosc to AFmax and (f) ratio AFosc to AFisomax. Adjusted p-values of pairwise comparisons (Bonferroni corrected) and effect sizes Cohen’s dz are given in case of significance.
Figure 3.
95%-confidence intervals including arithmetic mean and standard deviation (error bars) comparing regular MMT (reg, grey), MMT after procedure CL (red) and MMT after procedure CL-CT (blue) for the different parameters: (a) maximal Adaptive Force (AFmax), (b) maximal isometric AF (AFisomax), (c) AF at onset of oscillations (AFosc), (d) ratio AFisomax to AFmax, (e), ratio AFosc to AFmax and (f) ratio AFosc to AFisomax. Adjusted p-values of pairwise comparisons (Bonferroni corrected) and effect sizes Cohen’s dz are given in case of significance.
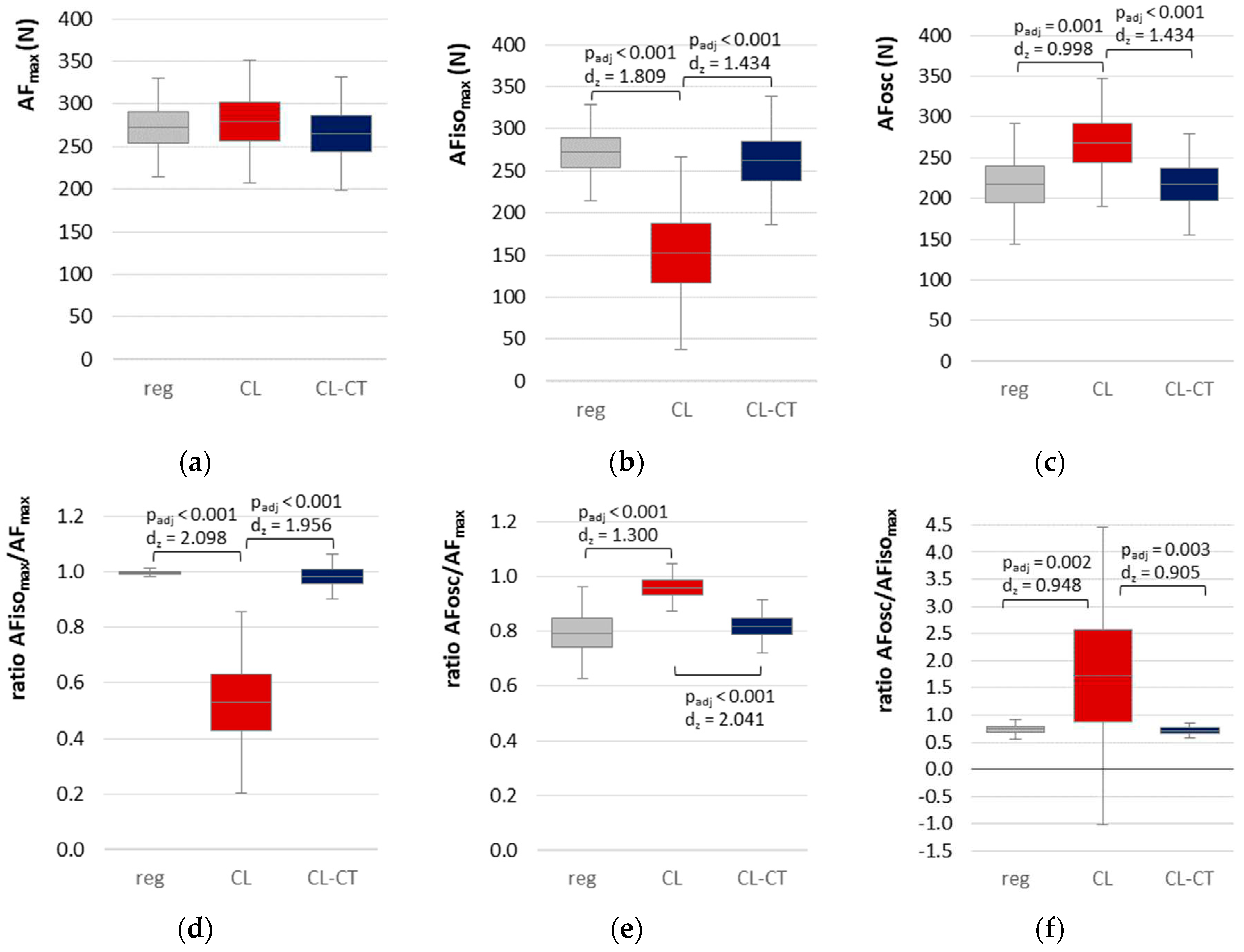
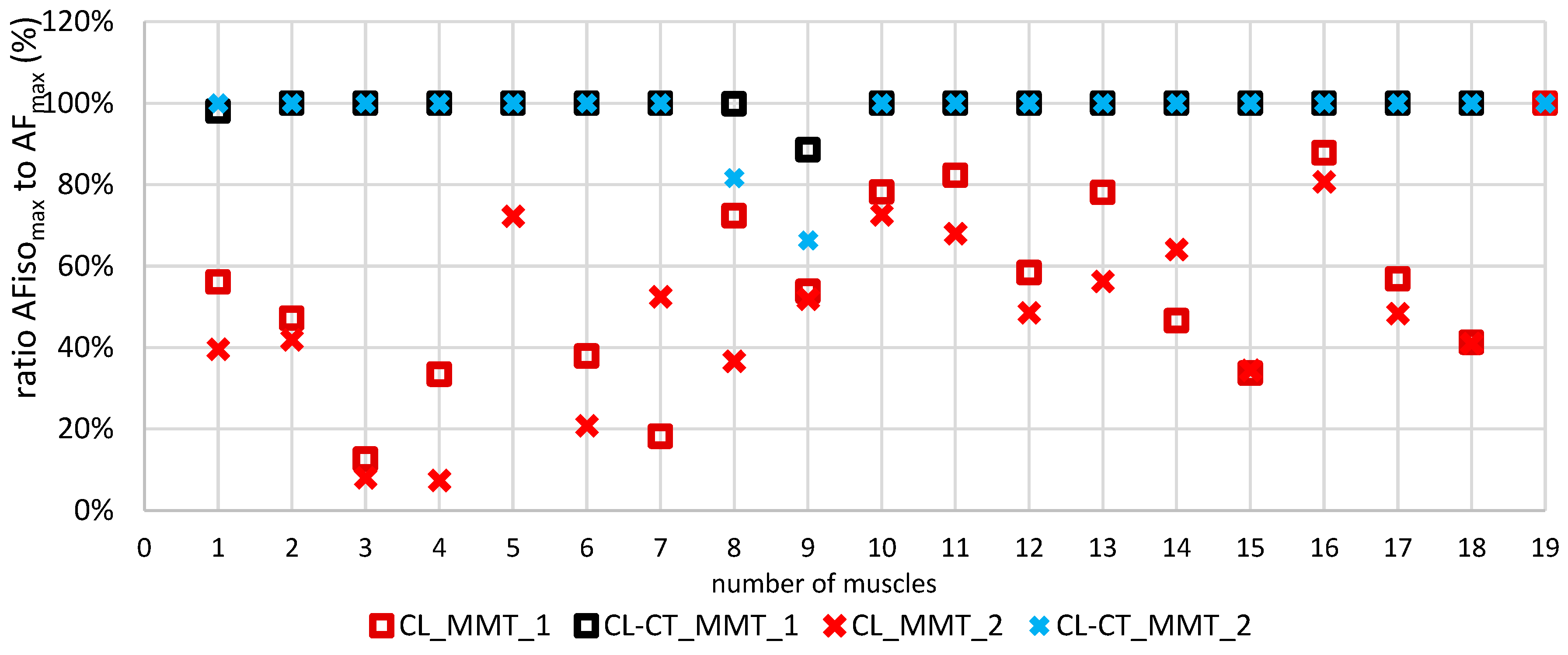
Figure 4 depicts the single values of the ratio AFisomax to AFmax of each of the 19 tested muscles for both MMT trials after procedure CL and CL-CT, respectively. It is visible that for CL-CT the ratio amounted ~100% with two exceptions showing lower values (muscle no. 8 and 9, Figure 4). In contrast, clearly lower ratios were obtained for CL with one exception (muscle no. 19, Figure 4). Accordingly, RM ANOVA was highly significant (Table 2). Pairwise comparisons revealed significantly lower ratios for CL compared to regular MMT (p < 0.001, dz = 2.098) and compared to CL-CT (p > 0.001, dz = 1.956) (Figure 3d).
This indicates that a pre-contraction in lengthened position followed by a passive return to middle-length test position immediately reduced the holding capacity significantly. Without a 2nd pre-contraction in test position, participants were only able to reach ~53% of the AFmax under isometric conditions. Hence, AFmax was then reached during muscle lengthening. Only one participant was able to reach ~100% of AFmax, thus, did not yield during the MMT after procedure CL. In contrast, for MMTs after the short and low-intensity second contraction in test position (CL-CT) as well as for regular MMT the participants were able to reach more than 98% of the AFmax. 16 of 19 muscles were able to generate 100% of the AFmax. Hence, they reached their maximal strength under isometric conditions. The remaining three muscles still showed considerably high ratios (95.67 – 99.97 %), except for one with a ratio of only 77.46%. The latter clearly lengthened the muscle during the MMT after procedure CL-CT. Overall, the second pre-contraction in test position led to an instantaneous regaining of regular holding capacity, thus, the musculoskeletal instability could be resolved thereby. The objective data support the subjective ratings of the tester in all cases. All regular MMTs were rated as ‘stable’ by the tester. For procedure CL, the tester assessed 2 of 38 MMTs as ‘stable’ (belonged to the same participant) and 36 as ‘unstable’, while with procedure CL-CT, 33 of 37 MMTs were rated as ‘stable’ and 4 as ‘unstable’ (belonged to the same participant).
Figure 4.
Single values of the ratio AFisomax to AFmax (%) for the first (MMT_1, square) and second trial (MMT_2, cross) of procedure CL (red) and procedure CL-CT (blue) for each of the 19 tested elbow flexors.
Figure 4.
Single values of the ratio AFisomax to AFmax (%) for the first (MMT_1, square) and second trial (MMT_2, cross) of procedure CL (red) and procedure CL-CT (blue) for each of the 19 tested elbow flexors.
3.3. Onset of Oscillations in the course of Adaptive Force comparing the different procedures
RM ANOVA showed a significant main effect (Table 2), whereby pairwise comparisons revealed a significantly higher AFosc for procedure CL compared to regular MMT (padj = 0.001, dz = 0.998) and to procedure CL-CT (padj < 0.001, dz = 1.434), respectively. Regular MMT and procedure CL-CT did not differ significantly (padj = 1.000) (Figure 3c).
The ratios regarding the onset of oscillations make the results even clearer: the upswing of oscillations started on a −20.66% and −14.66% lower level in relation to AFmax for regular MMT and procedure CL-CT, respectively (Table 2, Figure 3e). Furthermore, the oscillatory upswing occurred under isometric conditions (ratio AFosc/AFisomax) for regular MMT and procedure CL-CT (stable MMTs), whereby for procedure CL (unstable MMTs) oscillations did not occur or arose during the lengthening phase (Figure 3f). Only in one case, the oscillations arose at 95% of AFisomax, thus, still under isometric conditions. Those findings indicate that the occurrence of oscillations might be a prerequisite for adequate adaptation and, hence, for musculoskeletal stability.
3.4. Maximal voluntary isometric contraction
The MVIC amounted initially averagely 275.02 ± 46.66 N (range: 204.87 – 356.13 N) and 265.78 ± 47.55 N (range: 202.67 – 348.74 N) after the six MMT trials. Thus, the MVIC declined by ~3.36% which was just not significant (t(18) = 2.103, p = 0.050). Hence, a significant fatiguing effect was not present. AFisomax was similar to MVIC for stable MMTs (regular MMT: −0.51 ± 7.69%; CL-CT: −4.21 ± 14.75%); after procedure CL, it was clearly lower (−45.05 ± 25.51%). Those findings indicate that under stable conditions the maximal isometric forces were similar for holding and pushing actions in the present setting. This points out that the tester applied adequate forces during the MMTs.
4. Discussion
The study investigated the effects of two different preceding procedures – assumed to manipulate muscle spindles – on AF parameters. There are two central results of the study: firstly, after the CL procedure the maximal holding capacity (AFisomax) was almost halved compared to regular MMT and MVIC. Secondly, this reduction did not appear when a second short contraction with ~25% of MVIC was added in test position immediately prior to the test. Consequently, during CL-CT procedure the muscle behaved in the same way as for regular MMT. Moreover, the maximal AF was not affected by the preceding procedures. Hence, all hypotheses were verified positively.
4.1. Methodological considerations regarding the comparison of the procedures
From the methodological point of view, it was important to assess at what force level the MMTs were executed. The reached maximum depends on the interaction of both partners. In case the force produced by the tester would be too low, a falsely as stable assessed MMT could be the result even though the tested muscle would be actually unstable. Therefore, the reached maximal forces must be taken into consideration. Compared to regular MMTs, AFmax was by 2.5% higher after CL and by −2.7% lower after CL-CT procedure, respectively. Accordingly, the developed forces were really similar. Therefore, an inappropriate maximal force produced by the tester can be ruled out for the found differences. Moreover, the forces during all MMTs reached the level of the initial MVIC. The AFmax during regular, CL and CL-CT procedures amounted to 99.77%, 102.36% and 97.07% of the MVIC, respectively. Therefore, all MMTs ran with at least approximately maximum intensities. In addition, the slope of force development should be taken into account. A fast increase would make it more difficult for the tested muscle to lock into a stable resistance (for neurophysiological considerations see [35]). The slope of regular MMT was significantly lower compared to the MMTs after both procedures, CL and CL-CT. However, it is assumed that in this study this had no relevant influence on the further outcomes because of the following points: firstly, regular MMT and CL-CT showed similar AF parameters despite of differing slopes. Secondly, the slopes matched between CL and CL-CT, but AFisomax and AFosc differed significantly.
Another prerequisite to compare both procedures were similar pre-contractions with regard to temporal sequence and intensity. No technical feedback was applied to avoid distractions so that the participant could fully concentrate on the sensations of the arm during the tests. Although the timing of both procedures (CL and CL-CT) was based solely on the temporal feeling of the tester, the duration of CL pre-contractions was very close to the instructed 1 s (± 0.1 s). It differed only by averagely 3/100s between both procedures. In addition, the time period between CL pre-contraction and start of MMT was also controlled by the commands of the tester. He had to temporize and bridge the duration of the additional second pre-contraction of CL-CT during CL procedure. Because this time period showed also only a small (0.18 s) and non-significant difference the temporal sequences can be rated as similar. In contrast, the duration of the second contraction during CL-CT was substantially shorter than instructed (0.72 s instead of 1 s). Furthermore, the intensities of the pre-contractions were mostly underestimated by the participants. Instead of the instructed 20% of the MVIC the participants applied an at least by 10% higher intensity in 65% of all pre-contractions; in 18% the intensity was lower than predefined. In the remaining 18% the self-estimated intensity of pre-contraction was within 18-22% of MVIC. Overall, the second pre-contraction during CL-CT was performed quicker but more intense than given. The mentioned differences do not mean an essential interference of the planned design but should be taken into account later in the discussion.
4.2. Neurophysiological considerations
The two main results mentioned above are in line with the findings of Gregory et al. that after a procedure similar to CL the stretch reflex was reduced and could be resolved by a second pre-contraction in test position [18]. They explained the found inhibiting effect after a pre-contraction in lengthened position followed by a passive muscle shortening (CL-procedure refers to ‘hold-long’ in Gregory et al.) by a generated slack of the intrafusal fibers [18]. It has been shown early that muscle spindles can fall slack or taut depending on the preceding history of muscle length and contraction [43]. A slack appears with CL conditioning during the subsequent passive shortening. There seems to be a specific kind of muscle spindles which fall silent under that condition – which was shown in cats [21,44]. It was suggested that muscle spindles are unable to maintain their resting discharge under slacked conditions [44]. It is assumed here that in this case the spindle afferents were not adjusted to the shortened overall muscle length at test position. The slacked fibers were not able to provide appropriate information on length and lengthening of the muscle being tested. According to several authors [19,21,45,46,47,48,49] it is suggested that the short additional pre-contraction in test position fixed this misalignment during CL-CT which then allowed an appropriate stabilization during the following MMT. Obviously, the second pre-contraction here was sufficient to resolve slack although it was significantly shorter than the first pre-contractions. This was indicated by the regained level of AFisomax approximately to the amount of AFmax. Presumably, not the duration but the intensity of the pre-contraction is the main factor to remove the slack in muscle spindles; as mentioned in the introduction, at least 5% of MVIC – partly up to 10% – are assumed to be sufficient [18,20]. Basically, the full range of mechanoreceptors of muscles, tendons, capsules, connective tissue and skin are involved in each motion and contraction. However, the CL procedure is likely to influence mostly muscle spindles. This suggests that the observed phenomena may mainly be due to those receptors.
It seems to be comprehensible that a slacked muscle spindle can affect a quick stretch reflex. In contrast, the present study showed a reduced holding function during the whole period of a MMT, which lasted around 3 s. In CL-CT, a brief contraction immediately before the MMT revoked that destabilizing effect. It has to be questioned why the muscle contraction during the MMT after CL procedure did not have the same effect. It seems the condition at the start of the MMT influences the whole process in the course of external force increase. The role of the participant could be understood as a slave system which has to execute a follow-up control in response to a varying reference input like it is done in technical motion control systems, too. It is hypothesized that the initial state of proprioceptive inputs influences the iterative processes of the adaptive control loop during the whole process of a running test. (It is likely that a subsequent second MMT would be stable then. However, this was not considered in the present study.)
Based on that hypothesis a complete holding muscle action could be understood as a prolonged reflex sequence. A sufficient muscular stabilization would be based – inter alia – on the appropriate initial adjustment of the involved muscle spindles. Preceding actions in everyday motions or sports which accidentally led to a slack could impair stability during a single motion. Such a process could have an effect on motor actions which acquire stability like, e.g., stopping a motion, changing the direction or compensating an external impact in sports. Especially muscle strain injuries are related to decelerating actions [50,51]. Sports injuries appear very often during movements which are executed a thousand times without any problem. Hence, there must be a specific condition during the one motion in which the injury occurs. Preceding actions which impair muscle spindles could be one way to trigger that.
The results showed a high interindividual variability regarding the reduction of AFisomax – interpreted as reduced stability – for CL procedure (CV = 0.517). As Figure 4 shows, the residual holding force ranged from 10% to 100% with regard to AFmax. The individual behaviors varied largely. In four cases the decrease went below 40% of AFmax for both trials after CL procedure (Figure 4, muscles no. 3, 4, 6 and 15). One muscle (no. 19) showed no reaction to the CL procedure and stayed completely stable irrespective of the conditioning. Another participant (muscles no. 8 and 9) developed a reduction of AFisomax during CL procedure (~54.5% of AFmax for first and ~52.8% for second measured side averaged over both MMTs) but did not return to full stability during CL-CT (~90.8% of AFmax for first and ~77.5% for second measured side). In this case the revoking effect of the second pre-contraction obviously was not as high as for the other participants. AFisomax after CL still amounted only ~64% of AFisomax after CL-CT. Additional trials afterwards (not included in this study) showed that in this particular participant a second contraction in test position with predefined self-estimated 50% of the MVIC was necessary to erase the inhibiting effect of a preceding CL procedure. The broad variety of reactions shows once more the individuality of the complex motor control. The afferent input of the spindles of a single muscle is only one voice in a true choir of proprioception – although likely the most important one. In contrast to monosynaptic reflexes, the voluntary action during a MMT runs not only on a spinal level but also supraspinal, where numerous additional influences could modulate the motor action. The mathematical model of Blum et al. [14] showed that muscle spindles must be understood as part of a complex multiscale biophysical framework including tendon organs and others.
A further aspect regarding the complex neuromuscular control circuitries are the oscillations appearing during interpersonal muscle actions [39,52,53,54]. This observed oscillatory synchronization presumably requires undisturbed functionality of the involved neuromuscular systems including proprioception. The MMT is a special kind of muscular interaction between two persons. It was found here that in case muscles showed high stability (regular MMT, CL-CT) the muscular interaction was accompanied by an early onset of oscillations at ~80% of AFmax. This characteristic mostly disappeared when muscles got unstable after CL procedure. The combination of a high AFisomax with an early upswing of mutual oscillations of both involved partners was already found in previous studies as a sign of muscular stability [30,31,32,34]. When muscles lose this property, the partners seem to be unable to find a common muscular rhythm. The results of the present study suggest that appropriate adjusted muscle spindles could be one necessary condition to link two interacting neuromuscular systems to generate mutual oscillation. With CL procedure the presumed impairment of spindles occurred on the side of the participant whereas the tester was not influenced. It remains unclear whether a manipulation on the tester´s side would have led to missing or late oscillations, too. It is assumed that the side of the participants could be the decisive one because they perform the HIMA which includes the reaction to the external force given by the pushing tester. The frequency of such interpersonal oscillations occur at ~10 Hz [39,52,53,54]. The 10 Hz rhythm in muscles is interpreted as physiological tremor which presumably originates by multiple factors including reflex loop resonances [55]. The long latency reflex lasts ~100 ms reflecting the latency of proprioceptive signals [56,57]. Such low-frequency oscillations are also found in different brain areas which participate in motor control, as the inferior olivary nucleus, the cerebellum, the thalamus and others [58,59,60]. Impairing muscle spindles by generating a slack seems to impede the ability to create a common interpersonal rhythm and to reduce the ability to adapt to an external force in a holding manner. This highlights the importance of undisturbed muscle spindle afferents for musculoskeletal stability and neuromuscular functioning.
4.3. Limitations
The performed measurements are based on a manual muscle test which is subjective by nature. Using the handheld device, the MMTs can be objectified. In regard of scientific quality criteria, it is necessary to point out again that the tester´s ability to generate reproducible force profiles was proved in a previous study.[35] All methodological aspects of the measured biomechanical parameters in comparison of the different procedures are given and discussed above and can be rated as suitable. Despite the low number of included participants the clear results gave an unambiguous picture. Nevertheless, the findings should be verified in future studies with a greater number of participants.
5. Conclusions
The investigated adaptive holding muscle function was significantly reduced by a generated slack in muscle spindles which supports the hypothesis. Hence, it reacted similar as the monosynaptic reflex which was previously examined by others. This suggests that holding against (varying) external forces requires appropriate proprioception and likely contains reflex components. During the eccentric phase of MMT which occurred after CL procedure the force rose further up to maximum intensities. Obviously, the muscle was able to generate its maximal strength but not under holding isometric conditions. The maximal AF was not affected by the different procedures. Therefore, the holding isometric Adaptive Force (AFisomax) should be considered as an independent type of muscle action mirroring interference in the complex control circuitries more sensitive than the usual measurements of the MVIC or other pushing forces.
A reduced muscular holding function is interpreted as musculoskeletal instability which is considered to be a risk for injury or for the development of musculoskeletal complaints in sports or everyday activities where adaptation of force to the external circumstances is almost always necessary. It is suggested that assessing the holding function of muscles in the sense of the Adaptive Force provides information on the functionality of, inter alia, the proprioceptive system especially regarding the length-tension-control which is mainly based on information coming from the muscle spindles. Based on that it is concluded that assessing the holding capacity could be used as supportive diagnostic approach to investigate the functional state of the neuromuscular system. This could be more beneficial compared to the conventional measurements of maximal forces because the latter seems not to react to impairments of muscle spindles like the CL procedure did.
Eventually, of course, further investigations are needed to clarify the question if there are specific motions in everyday activities or sports with a certain risk to impair muscle spindles and, therefore, the quality of motion. The considered procedures including AF measurements could also be an approach to assess the processing of muscle spindle afferents in motor control in subjects with specific conditions like ageing, pathologies or during convalescence after muscle injuries.
Author Contributions
Conceptualization, F.N.B, L.V.S. and S.D.; methodology, F.N.B, L.V.S. and S.D.; validation, F.N.B, L.V.S. and S.D.; formal analysis, S.D. and L.V.s.; investigation, F.N.B; data curation, S.D. and L.V.S.; writing—original draft preparation, L.V.S., F.N.B. and S.D.; writing—review and editing, F.N.B, L.V.S. and S.D.; visualization, L.V.S.; supervision, F.N.B.; project administration, F.N.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding. The publication was funded by the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation) – Project no. 491466077.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Ethics Committee of the University of Potsdam (protocol code 35/2018; 17 October 2018).
Informed Consent Statement
Informed consent was obtained from all participants involved in the study.
Data Availability Statement
The data presented in this study are available in the article.
Acknowledgments
We acknowledge the support of two student interns in accompanying the measurements.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Ardigo, A. Histoire Du Concept de Force. Revue Philosophique de la France Et de l’Etranger 1882, 14, 117. [Google Scholar]
- Proske, U.; Gandevia, S.C. The Proprioceptive Senses: Their Roles in Signaling Body Shape, Body Position and Movement, and Muscle Force. Physiological Reviews 2012, 92, 1651–1697. [Google Scholar] [CrossRef] [PubMed]
- Proske, U.; Gandevia, S.C. The Kinaesthetic Senses: The Kinaesthetic Senses. The Journal of Physiology 2009, 587, 4139–4146. [Google Scholar] [CrossRef] [PubMed]
- Giuriati, W.; Ravara, B.; Porzionato, A.; Albertin, G.; Stecco, C.; Macchi, V.; De Caro, R.; Martinello, T.; Gomiero, C.; Patruno, M.; et al. Muscle Spindles of the Rat Sternomastoid Muscle. Eur J Transl Myol 2018, 28. [Google Scholar] [CrossRef] [PubMed]
- Macefield, V.G.; Knellwolf, T.P. Functional Properties of Human Muscle Spindles. Journal of Neurophysiology 2018, 120, 452–467. [Google Scholar] [CrossRef] [PubMed]
- Behm, D.G.; Chaouachi, A. A Review of the Acute Effects of Static and Dynamic Stretching on Performance. Eur J Appl Physiol 2011, 111, 2633–2651. [Google Scholar] [CrossRef] [PubMed]
- Hill, D.K. Tension Due to Interaction between the Sliding Filaments in Resting Striated Muscle. the Effect of Stimulation. The Journal of Physiology 1968, 199, 637–684. [Google Scholar] [CrossRef] [PubMed]
- Hagbarth, K.-E.; Nordin, M. Postural After-Contractions in Man Attributed to Muscle Spindle Thixotropy. The Journal of Physiology 1998, 506, 875–883. [Google Scholar] [CrossRef] [PubMed]
- Avela, J.; Kyröläinen, H.; Komi, P.V. Altered Reflex Sensitivity after Repeated and Prolonged Passive Muscle Stretching. Journal of Applied Physiology 1999, 86, 1283–1291. [Google Scholar] [CrossRef]
- Padilha, U.C.; Vieira, A.; Vieira, D.C.L.; De Lima, F.D.; Rocha Junior, V.A.; Tufano, J.J.; Bottaro, M. Could Inter-Set Stretching Increase Acute Neuromuscular and Metabolic Responses during Resistance Exercise? Eur J Transl Myol 2019, 29. [Google Scholar] [CrossRef]
- Lakie, M.; Campbell, K.S. Muscle Thixotropy—Where Are We Now? Journal of Applied Physiology 2019, 126, 1790–1799. [Google Scholar] [CrossRef] [PubMed]
- Stubbs, P.W.; Walsh, L.D.; D’Souza, A.; Héroux, M.E.; Bolsterlee, B.; Gandevia, S.C.; Herbert, R.D. History-Dependence of Muscle Slack Length Following Contraction and Stretch in the Human Vastus Lateralis: History-Dependence of Muscle Slack Length. J Physiol 2018, 596, 2121–2129. [Google Scholar] [CrossRef] [PubMed]
- Morgan, D.L.; Prochazka, A.; Proske, U. The After-Effects of Stretch and Fusimotor Stimulation on the Responses of Primary Endings of Cat Muscle Spindles. The Journal of Physiology 1984, 356, 465–477. [Google Scholar] [CrossRef] [PubMed]
- Blum, K.P.; Campbell, K.S.; Horslen, B.C.; Nardelli, P.; Housley, S.N.; Cope, T.C.; Ting, L.H. Diverse and Complex Muscle Spindle Afferent Firing Properties Emerge from Multiscale Muscle Mechanics. eLife 2020, 9, e55177. [Google Scholar] [CrossRef]
- Proske, U.; Tsay, A.; Allen, T. Muscle Thixotropy as a Tool in the Study of Proprioception. Exp Brain Res 2014, 232, 3397–3412. [Google Scholar] [CrossRef] [PubMed]
- Proske, U.; Morgan, D.L.; Gregory, J.E. Thixotropy in Skeletal Muscle and in Muscle Spindles: A Review. Progress in Neurobiology 1993, 41, 705–721. [Google Scholar] [CrossRef]
- Banks, R.W.; Ellaway, P.H.; Prochazka, A.; Proske, U. Secondary Endings of Muscle Spindles: Structure, Reflex Action, Role in Motor Control and Proprioception. Experimental Physiology 2021, 106, 2339–2366. [Google Scholar] [CrossRef] [PubMed]
- Gregory, J.E.; Wise, A.K.; Wood, S.A.; Prochazka, A.; Proske, U. Muscle History, Fusimotor Activity and the Human Stretch Reflex. The Journal of Physiology 1998, 513, 927–934. [Google Scholar] [CrossRef] [PubMed]
- Budini, F.; Tilp, M. Changes in H-Reflex Amplitude to Muscle Stretch and Lengthening in Humans. Reviews in the Neurosciences 2016, 27, 511–522. [Google Scholar] [CrossRef]
- Héroux, M.E.; Anderman, I.; Nykvist Vouis, S.; Diong, J.; Stubbs, P.W.; Herbert, R.D. History-Dependence of Muscle Slack Length in Humans: Effects of Contraction Intensity, Stretch Amplitude, and Time. Journal of Applied Physiology 2020, 129, 957–966. [Google Scholar] [CrossRef]
- Wood, S.A.; Gregory, J.E.; Proske, U. The Influence of Muscle Spindle Discharge on the Human H Reflex and the Monosynaptic Reflex in the Cat. The Journal of Physiology 1996, 497, 279–290. [Google Scholar] [CrossRef]
- Monjo, F.; Forestier, N. Muscle Spindle Thixotropy Affects Force Perception through Afferent-Induced Facilitation of the Motor Pathways as Revealed by the Kohnstamm Effect. Exp Brain Res 2018, 236, 1193–1204. [Google Scholar] [CrossRef] [PubMed]
- Chaabene, H.; Behm, D.G.; Negra, Y.; Granacher, U. Acute Effects of Static Stretching on Muscle Strength and Power: An Attempt to Clarify Previous Caveats. Front. Physiol. 2019, 10, 1468. [Google Scholar] [CrossRef] [PubMed]
- Dech, S.; Bittmann, F.N.; Schaefer, L.V. Assessment of the Adaptive Force of Elbow Extensors in Healthy Subjects Quantified by a Novel Pneumatically Driven Measurement System with Considerations of Its Quality Criteria. Diagnostics 2021, 11, 923. [Google Scholar] [CrossRef] [PubMed]
- Myer, G.D.; Brent, J.L.; Ford, K.R.; Hewett, T.E. Real-Time Assessment and Neuromuscular Training Feedback Techniques to Prevent Anterior Cruciate Ligament Injury in Female Athletes. Strength & Conditioning Journal 2011, 33, 21–35. [Google Scholar] [CrossRef]
- Garrett, W.E. Muscle Strain Injuries: Clinical and Basic Aspects. Med Sci Sports Exerc 1990, 22, 436–443. [Google Scholar] [CrossRef] [PubMed]
- Read, P.J.; Oliver, J.L.; De Ste Croix, M.B.A.; Myer, G.D.; Lloyd, R.S. Neuromuscular Risk Factors for Knee and Ankle Ligament Injuries in Male Youth Soccer Players. Sports Med 2016, 46, 1059–1066. [Google Scholar] [CrossRef] [PubMed]
- Beynnon, B.D.; Fleming, B.C. Anterior Cruciate Ligament Strain In-Vivo: A Review of Previous Work. Journal of Biomechanics 1998, 31, 519–525. [Google Scholar] [CrossRef] [PubMed]
- Powell, J.W.; Barber-Foss, K.D. Sex-Related Injury Patterns among Selected High School Sports. Am J Sports Med 2000, 28, 385–391. [Google Scholar] [CrossRef]
- Schaefer, L.V.; Dech, S.; Wolff, L.L.; Bittmann, F.N. Emotional Imagery Influences the Adaptive Force in Young Women: Unpleasant Imagery Reduces Instantaneously the Muscular Holding Capacity. Brain Sciences 2022, 12, 1318. [Google Scholar] [CrossRef]
- Schaefer, L.V.; Dech, S.; Bittmann, F.N. Adaptive Force and Emotionally Related Imaginations – Preliminary Results Suggest a Reduction of the Maximal Holding Capacity as Reaction to Disgusting Food Imagination. Heliyon 2021, 7, e07827. [Google Scholar] [CrossRef] [PubMed]
- Schaefer, L.V.; Dech, S.; Aehle, M.; Bittmann, F.N. Disgusting Odours Affect the Characteristics of the Adaptive Force in Contrast to Neutral and Pleasant Odours. Sci. Rep. 2021, 11, 16410. [Google Scholar] [CrossRef] [PubMed]
- Schaefer, L.V.; Bittmann, F.N. Case Report: Individualized Pulsed Electromagnetic Field Therapy in a Long COVID Patient Using the Adaptive Force as Biomarker. Frontiers in Medicine 2022. [Google Scholar] [CrossRef] [PubMed]
- Schaefer, L.V.; Bittmann, F.N. The Adaptive Force as Potential Biomechanical Parameter in the Recovery Process of Patients with Long COVID; 2022. [Google Scholar] [CrossRef]
- Bittmann, F.N.; Dech, S.; Aehle, M.; Schaefer, L.V. Manual Muscle Testing - Force Profiles and Their Reproducibility. Diagnostics 2020, 10, 996. [Google Scholar] [CrossRef] [PubMed]
- Conable, K.M.; Rosner, A.L. A Narrative Review of Manual Muscle Testing and Implications for Muscle Testing Research. J Chiropr Med 2011, 10, 157–165. [Google Scholar] [CrossRef] [PubMed]
- Schaefer, L.V.; Bittmann, F.N. Are There Two Forms of Isometric Muscle Action? Results of the Experimental Study Support a Distinction between a Holding and a Pushing Isometric Muscle Function. BMC Sports Sci. Med. Rehabil. 2017, 9, 11. [Google Scholar] [CrossRef]
- Schaefer, L.V.; Bittmann, F.N. Paired Personal Interaction Reveals Objective Differences between Pushing and Holding Isometric Muscle Action. PLoS ONE 2021, 16, e0238331. [Google Scholar] [CrossRef]
- Schaefer, L.V.; Bittmann, F.N. Case Study: Intra- and Interpersonal Coherence of Muscle and Brain Activity of Two Coupled Persons during Pushing and Holding Isometric Muscle Action. Brain Sciences 2022, 12, 703. [Google Scholar] [CrossRef]
- Khan, A.; Rayner, G.D. Robustness to Non-Normality of Common Tests for the Many-Sample Location Problem. Journal of Applied Mathematics and Decision Sciences 2003, 7, 187–206. [Google Scholar] [CrossRef]
- Blanca, M.J.; Alarcón, R.; Arnau, J. Non-Normal Data: Is ANOVA Still a Valid Option? Psicothema 2017, 552–557. [Google Scholar] [CrossRef]
- Sullivan, G.M.; Feinn, R. Using Effect Size—or Why the P Value Is Not Enough. J Grad Med Educ 2012, 4, 279–282. [Google Scholar] [CrossRef] [PubMed]
- Proske, U.; Morgan, D.L.; Gregory, J.E. Thixotropy in Skeletal Muscle and in Muscle Spindles: A Review. Progress in Neurobiology 1993, 41, 705–721. [Google Scholar] [CrossRef] [PubMed]
- Gregory, J.E.; Morgan, D.L.; Proske, U. Two Kinds of Resting Discharge in Cat Muscle Spindles. Journal of Neurophysiology 1991, 66, 602–612. [Google Scholar] [CrossRef] [PubMed]
- Proske, U. Exercise, Fatigue and Proprioception: A Retrospective. Exp Brain Res 2019, 237, 2447–2459. [Google Scholar] [CrossRef] [PubMed]
- Allen, T.J.; Ansems, G.E.; Proske, U. Evidence from Proprioception of Fusimotor Coactivation during Voluntary Contractions in Humans: Fusimotor Coactivation during Voluntary Contractions. Experimental Physiology 2008, 93, 391–398. [Google Scholar] [CrossRef] [PubMed]
- Jahnke, M.T.; Proske, U.; Struppler, A. Measurements of Muscle Stiffness, the Electromyogram and Activity in Single Muscle Spindles of Human Flexor Muscles Following Conditioning by Passive Stretch or Contraction. Brain Research 1989, 493, 103–112. [Google Scholar] [CrossRef] [PubMed]
- Van Hooren, B.; Bosch, F. Influence of Muscle Slack on High-Intensity Sport Performance: A Review. Strength & Conditioning Journal 2016, 38, 75–87. [Google Scholar] [CrossRef]
- Proske, U.; Morgan, D.L.; Gregory, J.E. Muscle History Dependence of Responses to Stretch of Primary and Secondary Endings of Cat Soleus Muscle Spindles. The Journal of Physiology 1992, 445, 81–95. [Google Scholar] [CrossRef] [PubMed]
- Garrett, W.E. Muscle Strain Injuries. Am J Sports Med 1996, 24, S2-8. [Google Scholar] [CrossRef]
- Kieb, M.; Lorbach, O.; Engelhardt, M. Muskelverletzungen: Diagnostik und Behandlungen. Orthopäde 2010, 39, 1098–1107. [Google Scholar] [CrossRef]
- Schaefer, L.V.; Bittmann, F.N. Coherent Behavior of Neuromuscular Oscillations between Isometrically Interacting Subjects: Experimental Study Utilizing Wavelet Coherence Analysis of Mechanomyographic and Mechanotendographic Signals. Sci Rep 2018, 8, 15456. [Google Scholar] [CrossRef]
- Schaefer, L.V.; Torick, A.H.; Matuschek, H.; Holschneider, M.; Bittmann, F.N. Synchronization of Muscular Oscillations Between Two Subjects During Isometric Interaction. Eur J Transl Myol 2014, 24, 2237. [Google Scholar] [CrossRef]
- Schaefer, L.V. Synchronisationsphänomene myotendinöser Oszillationen interagierender neuromuskulärer Systeme – mit Betrachtung einer Hypothese bezüglich unterschiedlicher Qualitäten isometrischer Muskelaktion. Dissertation, Universität Potsdam, Potsdam, 2014. [Google Scholar]
- McAuley, J.H. Physiological and Pathological Tremors and Rhythmic Central Motor Control. Brain 2000, 123, 1545–1567. [Google Scholar] [CrossRef] [PubMed]
- Pruszynski, J.A.; Scott, S.H. Optimal Feedback Control and the Long-Latency Stretch Response. Exp Brain Res 2012, 218, 341–359. [Google Scholar] [CrossRef] [PubMed]
- Manning, C.D.; Tolhurst, S.A.; Bawa, P. Proprioceptive Reaction Times and Long-Latency Reflexes in Humans. Exp Brain Res 2012, 221, 155–166. [Google Scholar] [CrossRef] [PubMed]
- Bengtsson, F.; Ekerot, C.-F.; Jörntell, H. In Vivo Analysis of Inhibitory Synaptic Inputs and Rebounds in Deep Cerebellar Nuclear Neurons. PLoS ONE 2011, 6, e18822. [Google Scholar] [CrossRef]
- Lang, E.J.; Apps, R.; Bengtsson, F.; Cerminara, N.L.; De Zeeuw, C.I.; Ebner, T.J.; Heck, D.H.; Jaeger, D.; Jörntell, H.; Kawato, M.; et al. The Roles of the Olivocerebellar Pathway in Motor Learning and Motor Control. A Consensus Paper. Cerebellum 2017, 16, 230–252. [Google Scholar] [CrossRef]
- Vitek, J.L.; Ashe, J.; DeLong, M.R.; Alexander, G.E. Physiologic Properties and Somatotopic Organization of the Primate Motor Thalamus. Journal of Neurophysiology 1994, 71, 1498–1513. [Google Scholar] [CrossRef]
Figure 1.
Equipment and setting. (a) Handheld device. (b) Starting (test) position of the manual muscle test and MVIC test of elbow flexors (modified according to [30,32]).
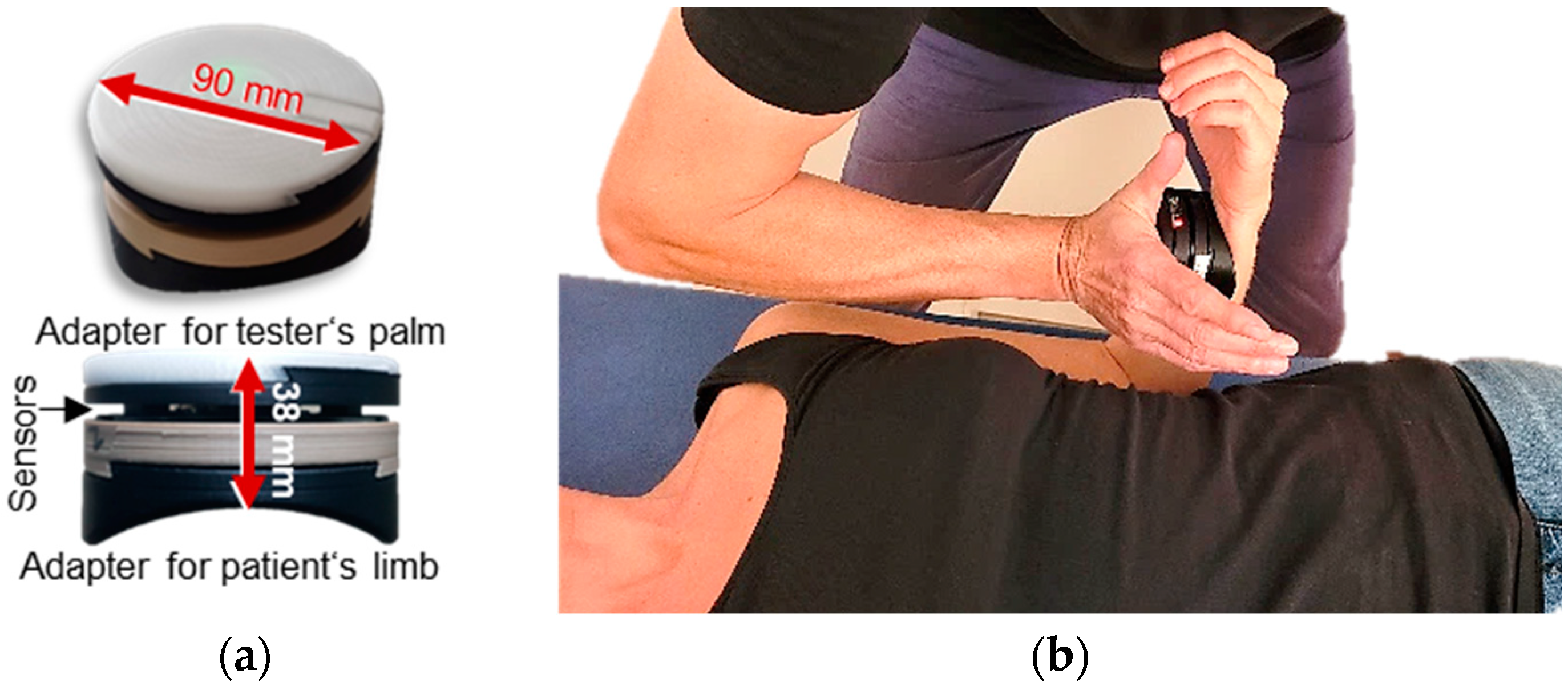

Table 1.
Pre-contractions. Arithmetic means ± standard deviations of the proportion of force of pre-contraction related to the individual’s MVIC (%), the duration of pre-contraction phases (s), and of the duration from the of 1st pre-contraction to start of MMT (s) for procedures CL and CL-CT.
Table 1.
Pre-contractions. Arithmetic means ± standard deviations of the proportion of force of pre-contraction related to the individual’s MVIC (%), the duration of pre-contraction phases (s), and of the duration from the of 1st pre-contraction to start of MMT (s) for procedures CL and CL-CT.
| parameters | Procedure CL) | Procedure CL-CT |
|---|---|---|
| force 1st pre-contraction / MVIC (%) | 25.04 ± 9.44 | 26.44 ± 9.11 |
| force 2nd pre-contraction / MVIC (%) | - | 28.47 ± 8.81 |
| duration of 1st pre-contraction (s) | 1.09 ± 0.33 | 1.12 ± 0.33 |
| duration of 2nd pre-contraction (s) | - | 0.72 ± 0.12 |
| duration 1st pre- contraction to MMT (s) | 7.51 s ± 0.96 | 7.33 ± 1.76 |
MMT = manual muscle test
CL = pre-contraction in lengthened position with passive return
CL-CT = CL with second subsequent pre-contraction in test position.
Table 2.
Arithmetic means (M) and standard deviations (SD) of the maximal Adaptive Force (AFmax), the maximal isometric Adaptive Force (AFisomax) and the Adaptive Force at onset of oscillations (AFosc) (all in N) as well as the respective ratios and slope [lg(N/s)] for the regular MMT, MMT after procedure CL and MMT after procedure CL-CT. Statistical values (F value, degrees of freedom (df), significance p and effect size η²) of RM ANOVA are given. Superscript indicates significant pairwise comparisons.
Table 2.
Arithmetic means (M) and standard deviations (SD) of the maximal Adaptive Force (AFmax), the maximal isometric Adaptive Force (AFisomax) and the Adaptive Force at onset of oscillations (AFosc) (all in N) as well as the respective ratios and slope [lg(N/s)] for the regular MMT, MMT after procedure CL and MMT after procedure CL-CT. Statistical values (F value, degrees of freedom (df), significance p and effect size η²) of RM ANOVA are given. Superscript indicates significant pairwise comparisons.
| parameter | procedure | M | SD | F | df | p | η² |
|---|---|---|---|---|---|---|---|
| AFmax | regular | 272.574 | 38.846 | 3.193 | 2, 36 | 0.053 | - |
| CL | 279.512 | 49.427 | |||||
| CL-CT | 265.259 | 46.158 | |||||
| AFisomax | regular | 271.774 | 39.367 | 44.946* | 1.24, 22.36 | < 0.0011 | 0.714 |
| CL | 152.146 | 78.607 | |||||
| CL-CT | 262.033 | 52.597 | |||||
| AFosc | regular | 217.580 | 51.058 | 18.992 | 2, 36 | < 0.0011 | 0.512 |
| CL | 268.585 | 53.937 | |||||
| CL-CT | 217.255 | 43.088 | |||||
| ratio AFisomax/AFmax | regular | 0.997 | 0.100 | 75.660 | 1.09, 19.64 | < 0.0011 | 0.808 |
| CL | 0.530 | 0.225 | |||||
| CL-CT | 0.983 | 0.055 | |||||
| ratio AFosc/ AFmax | regular | 0.795 | 0.115 | 26.644* | 1.47, 26.54 | < 0.0011 | 0.597 |
| CL | 0.959 | 0.059 | |||||
| CL-CT | 0.818 | 0.066 | |||||
| ratio AFosc/AFisomax | regular | 0.797 | 0.119 | 16.264* | 1.01, 18.12 | 0.0011 | 0.475 |
| CL | 2.566 | 1.885 | |||||
| CL-CT | 0.836 | 0.089 | |||||
| slope | regular | 2.017 | 0.140 | 19.686 | 2,34 | < 0.0012 | |
| CL | 2.210 | 0.201 | 0.537 | ||||
| CL-CT | 2.137 | 0.121 |
* Greenhouse-Geisser correction. Significant results are written in bold.
1 Significant pairwise comparisons between CL vs. CL-CT and CL vs. regular MMT.
2 Significant pairwise comparison between regular MMT vs. CL and vs. CL-CT, respectively.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



