
Submitted:
05 March 2023
Posted:
09 March 2023
You are already at the latest version
Abstract
Here we investigated the acute effects of an exhaustive intermittent exercise session on immunological parameters of the elderly and the subsequent incidence of upper respiratory tract infections and compare with the moderate-intensity. To do so, ixty-three old subjects were divided into three groups HIIT (n=21) submitted at one High-intensity interval training, SCG (n=21) kept in a sedentary state, and MICT (n=21) submitted at moderate intensity walking. Blood were collected at 5 time points, before, immediately after, 2h, 24h, and 48h after the intervention. In result the IL-6 and TNF-α were overexpressed immediately after the IL-10 stood overexpressed and correlated with IL-17, denoting an inflammatory process, and evidencing an immunologic competence without enhancement of the prevalence of upper respiratory infection tract (URTIs). So a modulation in the balance of Th1/Th2/Th17 cytokines and leukocytes, these modifications did not cause the effect characterized as an immunological window. Perhaps, the typical inflammation process, with IL-10 and IL-17 participation could also produce benefits to combat infections, a pertinent discussion during a post-pandemic time; we consider it a safe exercise program for older adults.
Keywords:
Exercise
; IL-17
; IL-10
; Interleukin. Exercise-Induced Inflammatory State
1. Introduction
Epidemiological shreds of evidence indicate that regular physical activity reduces the incidence of many chronic diseases in older age, including communicable diseases such as viral and bacterial infections, as well as non-communicable diseases such as cancer and chronic inflammatory disorders [1,2], a very special condition during the Sars-Cov-2 infection due to the very high susceptibility of older. Despite the apparent health benefits achieved by leading an active lifestyle, which implies that regular physical activity and frequent exercise enhance immune competency and regulation, the effect of a single bout of exercise on immune function remains a controversial topic which a vigorous bout of exercise has been implicated in temporary suppression of immune function [3] which can be undesirable.
Otherwise, prolonged, and intense exercises have been related to negative changes such as the immediate reduction of defenses against viral infections and increased risk of diseases [4,5] resulting in an increased incidence of infections [2], probably, including COVID-19. Additionally, about high-intensity exercises authors state that there may be an increased risk of upper respiratory tract infections possibly due to a high response of cytokines of the Th1 and Th2 profile, which causes significant stress on the immune system decreasing its ability to fight antigens and pathogens [6]. Furthermore, high-intensity exercises, e.g. High-intensity interval training (HIIT), may promote a transient decrease in the INF-γ/IL-4 ratio creates a possible immunological window for infections [7] demonstrating the clinical importance of this discussion. However, this immunological window hypothesis does not present scientific support due to the various methodological flaws in the studies that fail to show robust and consistent results on the subject [3].
Aging is also associated with an increase in inflammatory proteins in the circulation such as interleukin-6 (IL-6), tumor necrosis factor-alpha (TNF-α), and C-reactive protein (CRP), with the underlying development of chronic diseases [8,9]. Previous research has shown that chronic and well-structured exercises can produce chronic anti-inflammatory effects [10] mainly mediated by IL-6, however in an anti-inflammatory environment with interleukin 10 (IL-10) [11,12]. However, the effects of HIIT on the immune system of the elderly are little explored due to the intensity of this type of exercise, which often hinders its application in an elderly population leaving an important gap in this field of study.
The pandemic is a complicated situation, and many doubts, like if we can, or cannot begin a physical exercise program. In especial, the high-intensity interval training remains without robust evidence. Previously, our group displayed that the HIIT causes acute inflammation like another kind of exercise in the early stages of the program in young adults, however, the inflammation decreases from seven to fifteen days, which allows us to suppose the hypothesis that at the end of acute inflammation the subjects could be submitted for a new overload [13]. This notion became more relevant due to the pandemic of COVID-19 because it seems correct to state that previous physical exercise may play a role in infection and disease progression [14,15], however, beginning a physical exercise program during the pandemic can weaken the older adult and expose them to the risk of infection with unfavorable outcomes?
The hypothesis that guided or investigation states that the high-intensity, however, short time exercise is safe to sedentary older adults. Thus, the present study aims to investigate the acute effects of an exhaustive intermittent exercise session on the immunological parameters of the elderly and the subsequent incidence of upper respiratory tract infections and compare with the moderate-intensity.
2. Materials and Methods
2.1. Participants, design, and ethics of the study
Sixty-three volunteers of both sexes completed the study. All participants were required not to participate in another exercise program for at least fifteen days before the study. The sample size was calculated based on the effect size of previous intervention studies on healthy and sedentary older adults submitted at physical exercise intervention [16,17,18]. Thus, considering α = 0.05, 80% power, and an effect size of 0.22, a total sample of 54 individuals, 18 per group, was estimated. However, we reached sixty-three subjects, 21 per group, with 87% of power, and an effect size of 0.33. The data collection, and their processing was double blind to avoid bias risk.
The total group was divided randomically into three groups; High-Intensity Interval Training (HIIT) (n=21) which was submitted to a single both of high-intensity intermittent exercise until exhaustion, Sedentary Control Group (SCG) (n=21) kept without exercise practice, and Moderate-Intensity Continuous Training (MICT) (n=21) submitted at 40 minutes of moderate-intensity walking. Age, weight, and height were acquired by pattern tests and interviews. The participant’s characteristics were shown in Table 1. To determine the homogeneity of the groups before the division the ANOVA ONE WAY was set up at 5%. The participant’s characteristics are being shown in table 1.
Body mass and height were obtained using the mechanical scale of the Filizolla brand (Brazil) with a precision of 0.1 kg. All statistical procedures followed previously described protocols [19,20,21,22]. The Polar FT1 heart rate monitor was used for monitoring heart rate during the training session. All participants signed the informed consent form in agreement with the Brazilian Ethics Committee. This project was previously approved by the National Health Council under the number CAAE 44907715.2.0000.5653 on 27/07/2015 and followed all ethical and legal requirements. All participants were assisted by medical services one time a week to determine the upper respiratory tract infections incidence.

Table 1.
Participant’s characteristics.
| Participants Characterization | HIIT (n= 21) | SCG (n= 21) | MICT (n=21) | p value |
|---|---|---|---|---|
| Age (Years) | 67.6+8.72 | 68.4+ 7.45 | 69.1+6.73 | >0.05 |
| Weight (Kg) | 76.1+6.08 | 79.2+5.77 | 78.9+7.13 | >0.05 |
| Height (Cm) | 1.68+0.91 | 1.66+0.84 | 1.67+0.93 | >0.05 |
| BMI (Kg/m2) | 27.5+3.73 | 28.5+4.52 | 28.6+5.11 | >0.05 |
| VO2 Max (ml/kg/min) | 32.2+2.64 | 33.4+4.43 | 32.6+7.25 | >0.05 |
Legend: HIIT= High-Intensity Interval Training; SCG= Sedentary Contol Group, and MICT Moderate-Intensity Continuous Training.
Clinical and laboratorial health state of volunteers
Three consultations were performed with the physician who attended to the patients, maintaining their monthly routine. These consultations occurred immediately before the intervention period, four weeks later, and at the end of the intervention. During these consultations, routine clinical measurements such as blood pressure, heart rate, cardiac auscultation, complete history taking, orthopedic investigations and other medical investigations were carried out according to the monthly routine of clinical consultations. These consultations served as support for the control of health conditions and for reporting intercurrences and adverse clinical events that might be related to the intervention proposed herein. The same proceeding were adopted previously for our group[23,24,25].
We measured levels of glucose, total cholesterol, triglycerides, HDL, LDL, lactate dehydrogenase, at baseline and after four and eight weeks of high-intensity intermittent exercise. These tests were performed using a Konelab 60i model analyser and Wiener Lab kits, following the protocol of the apparatus. The device was calibrated prior to performing the tests according to the manufacturer's manual. At each collection, two blood samples were collected in EDTA tubes (4 mL vacutainer tube, BD Vacutainer, Franklin Lakes, NJ, USA) and stored in a refrigerated container (4° C) until measurement, which was performed in all cases within 1 h after venipuncture. All proceedings here described was previously published [24].
Cardiorespiratory fitness assessment
The determination of the maximal VO2 and the exhaustive exercise protocol was performed by the Shuttle Run test, which is a situation of intermittent, progressive exercise until the maximum exhaustion, therefore, filling in the requirements for measuring the two factors determining physical performance. The duration of the test would depend on the cardiorespiratory fitness of each person; however, all tests were similar due to the homogeneity in the VO2 Max, and the group stopped at the same level leading to a similar exercise challenge for all groups.
Blood sampling acquisition for immunological analysis
Peripheral blood was obtained by venipuncture to quantification of immunological parameters before, immediately after, 2h after, 24h after, and 48h the single both of HIIT or MICT. The immunologic parameter was quantified at all points of blood sampling. The white blood cells were counted by differential counting in the optical microscope in duplicate. All reagents used originated from the Human Cytokine Kit (Becton Dickinson Biosciences, San Jose, CA, USA) for Th1/Th2/Th17 cytokines. The cytometer was calibrated according to the manufacturer's recommendations. Standard curves were calibrated for each cytokine (0.00 to 5000 pg/mL) and the samples were analyzed with FCAP Array software (Becton Dickinson, San Jose, CA, USA), and the values were reported as pg/mL. All experiments were performed in duplicate. The mean was calculated.
Upper respiratory tract infections assessment
The incidence of upper respiratory tract infections was assessed before, during, and until 3 months after the beginning of the physical exercise program across one survey submitted every week for 12 weeks.
Statistical Analysis
The descriptive data were expressed by the mean, percentage, and standard deviation. To determine the normality of the data the Shapiro-Wilks test was performed. Then, the ANOVA TWO-WAY with Bonferroni’s posterior test was used to determine the difference between all-time points of experiments. All tests had a significance of 5%.
3. Results
The URTI incidence don’t improved in response to the HIIT
The assessment of the incidence of upper respiratory tract infections displayed no infections to HIIT and MICT with 0% of incidence to both. However, three (14.28%) infections suggested of common cold were noted in the SGC during the three months of investigation after the beginning of the exercise program. Finally, regarding the clinical significance, no common cold, another upper respiratory tract infection, or other clinical intercurrences were related to all participants submitted or not to both exercise regimes (0 occurrences).
Biochemical markers display good health conditions
The markers investigated are within the normal range, demonstrating that all subjects were in good health conditions, which allows us to infer that all responses to exercise were not under pathological conditions. Therefore, hepatic, kidney, cardiac, muscular, tissue, fasting glucose, and C-reactive protein markers, not indicating muscle injury or systemic inflammation, as well as the four hematological factors analyzed here, hemoglobin, mean corpuscular volume and platelets. As for lipids, total cholesterol, low density lipoprotein and triglycerides are also within normal limits, discarding possible metabolic syndrome and subclinical systemic inflammations that could influence the findings of the present study.
Table 2.
Laboratorial Health of Volunteers.
| Variables | SGC | HIIT | MICT | p value |
|---|---|---|---|---|
| AST (IU/mL) | 39.0±25.6 | 40.5±13.1 | 39.25±20.3 | >0.05 |
| ALT (IU/mL) | 23.67±4.16 | 23.98±2.35 | 24.0±7.2 | >0.05 |
| Creatinine (mg/dL) | 0.75±0.13 | 0.74±0.43 | 0.73±0.1 | >0.05 |
| Urea (mg/dL) | 21.25±2.5 | 26.64±6.1 | 27.25±5.8 | >0.05 |
| CK-MB (IU/mL) | 10.75±2.2 | 10.33±6.7 | 10.25±5.4 | >0.05 |
| CK-Total (IU/mL) | 91.0±12.6 | 91.3±23.5 | 91.5±38.5 | >0.05 |
| Cholesterol (mg/dL) | 192.5±38.5 | 179.4±77.5 | 164.7±19.7 | >0.05 |
| Triglycerides (mg/dL) | 184.5±38.7 | 176.5±38.7 | 163.7±19.7 | >0.05 |
| LDH (mg/dL) | 358.7±124.2 | 358.7±124.2 | 331.5±70.2 | >0.05 |
| HDL(mg/dL) | 41.5±3.7 | 46.4±1.9 | 46.5±2.97 | >0.05 |
| PCR (mg/dL) | 3.75±4.7 | 3.11±1.9 | 2.75±3.6 | >0.05 |
| Glucose (mg/dL) | 89.5±7.1 | 89.5±7.1 | 92.5±8.2 | >0.05 |
| Haematocrit (%) | 43.4±0.2 | 43.7±0.1 | 44.2±0.2 | >0.05 |
| Haemoglobin (g/dL) | 12.96±0.7 | 12.86±0.9 | 12.81±0.7 | >0.05 |
| MCV (fl) | 86.1±1.3 | 87.9±1.1 | 88.2±1.2 | >0.05 |
| MCH (pg) | 28.8±0.7 | 29.7±0.4 | 29.8±0.6 | >0.05 |
| Platelet levels (uL) | 282650±22951.8 | 283760±22951.8 | 283830±15325 | >0.05 |
Legend: Elderly (n=63), divided into three groups, namely, SGC, HIIT and MICT, of equal size (n=21) were submitted to biochemical, hematological, lipid and glycemic profile. ALT (Alanine Amino Transferase), AST (Aspartate Amino Transferase), CK-MB (Creatine Kinase type MB), CK-Total (Creatine Total Kinase), LDH (Lactate Dehydrogenase), HDL (High Density Lipoprotein) and PCR (C-Reactive Protein), Vcm (Medium Corpuscular Volume), HCM (Middle Corpuscular Hemoglobin). The ANOVA ONE WAY with significance of 5% was used to point out the possible differences between GcS, HIIT and MICT (p>0.05).
The white blood cells display little stress in response to HIIT
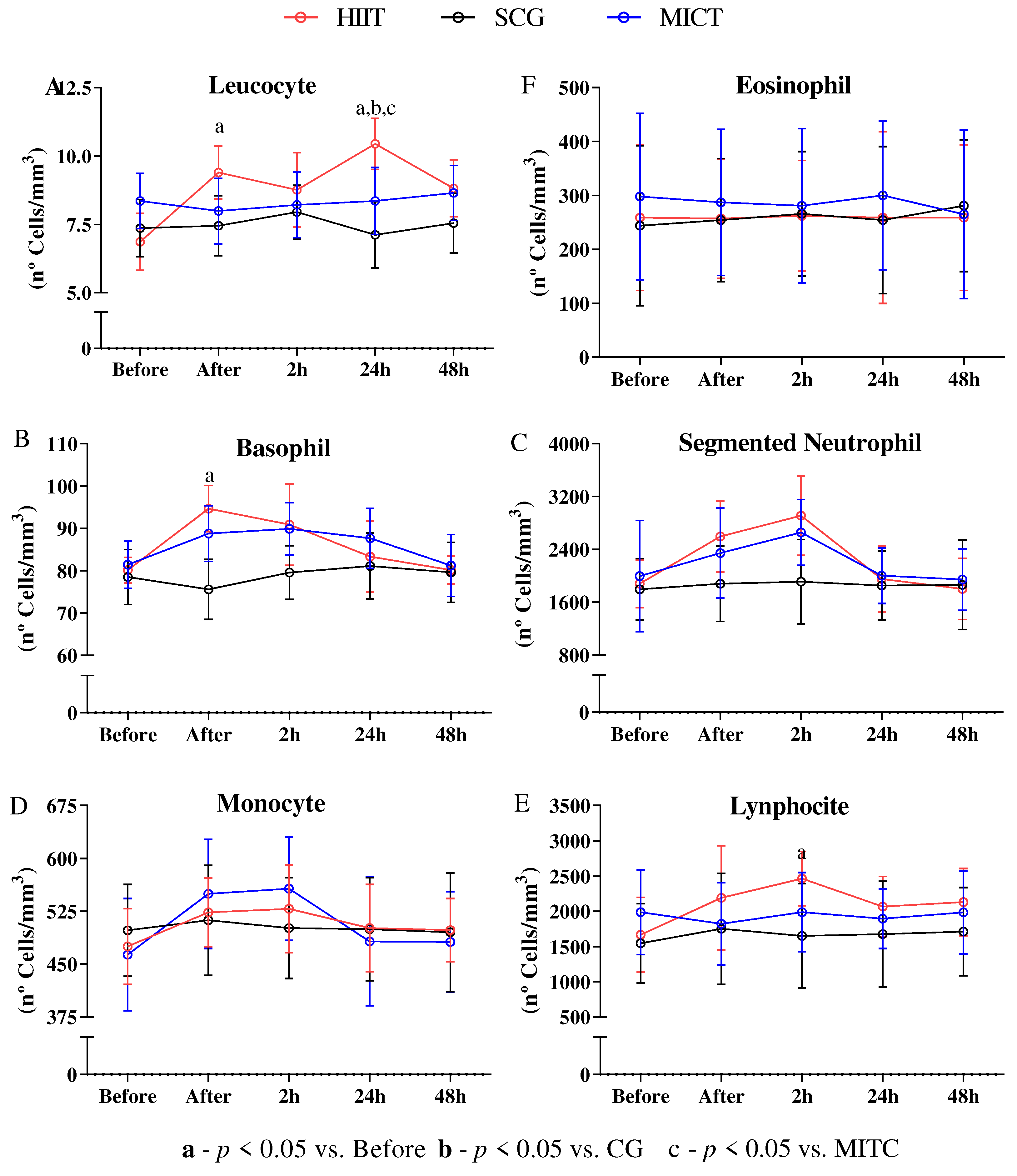
To the cell count the segmented neutrophil (Fig. 1C), monocyte (Fig. 1D), and eosinophil (Fig. 1F) did not display modulation to all-time points (P<0.05). However, was observed consistent enhancement of leucocyte (Fig. 1A) immediately after (P<0.05) if compared with baseline, and in 24h (P<0.01) if compared with the baseline, SCG and MICT. The HIIT display of the basophil (Fig. 1B) had enhancement immediately after (P>0.05), and the lymphocyte (Fig. 1E) shows enhancement in 2h (P<0.05).
Figure 1.
Leucogram. Sixty-three old persons were divided into three groups HIIT (n=21) which was submitted to a single both of high-intensity intermittent exercise until exhaustion, SCG (n=21) kept without exercise practice, and MICT (n=21) submitted at 40 minutes of walking in a moderate intensity. Five-time points of blood by venepuncture to quantification of immunological parameters before, immediately after, 2h after, 24h after, and 48h after the single both of HIIT or MICT were acquired for immunologic parameters quantification. The ANOVA TWO-WAY with Bonferroni’s posterior test at 5% was used to determine the differences between the points.
Figure 1.
Leucogram. Sixty-three old persons were divided into three groups HIIT (n=21) which was submitted to a single both of high-intensity intermittent exercise until exhaustion, SCG (n=21) kept without exercise practice, and MICT (n=21) submitted at 40 minutes of walking in a moderate intensity. Five-time points of blood by venepuncture to quantification of immunological parameters before, immediately after, 2h after, 24h after, and 48h after the single both of HIIT or MICT were acquired for immunologic parameters quantification. The ANOVA TWO-WAY with Bonferroni’s posterior test at 5% was used to determine the differences between the points.
The immunologic markers display little stress in response to HIIT
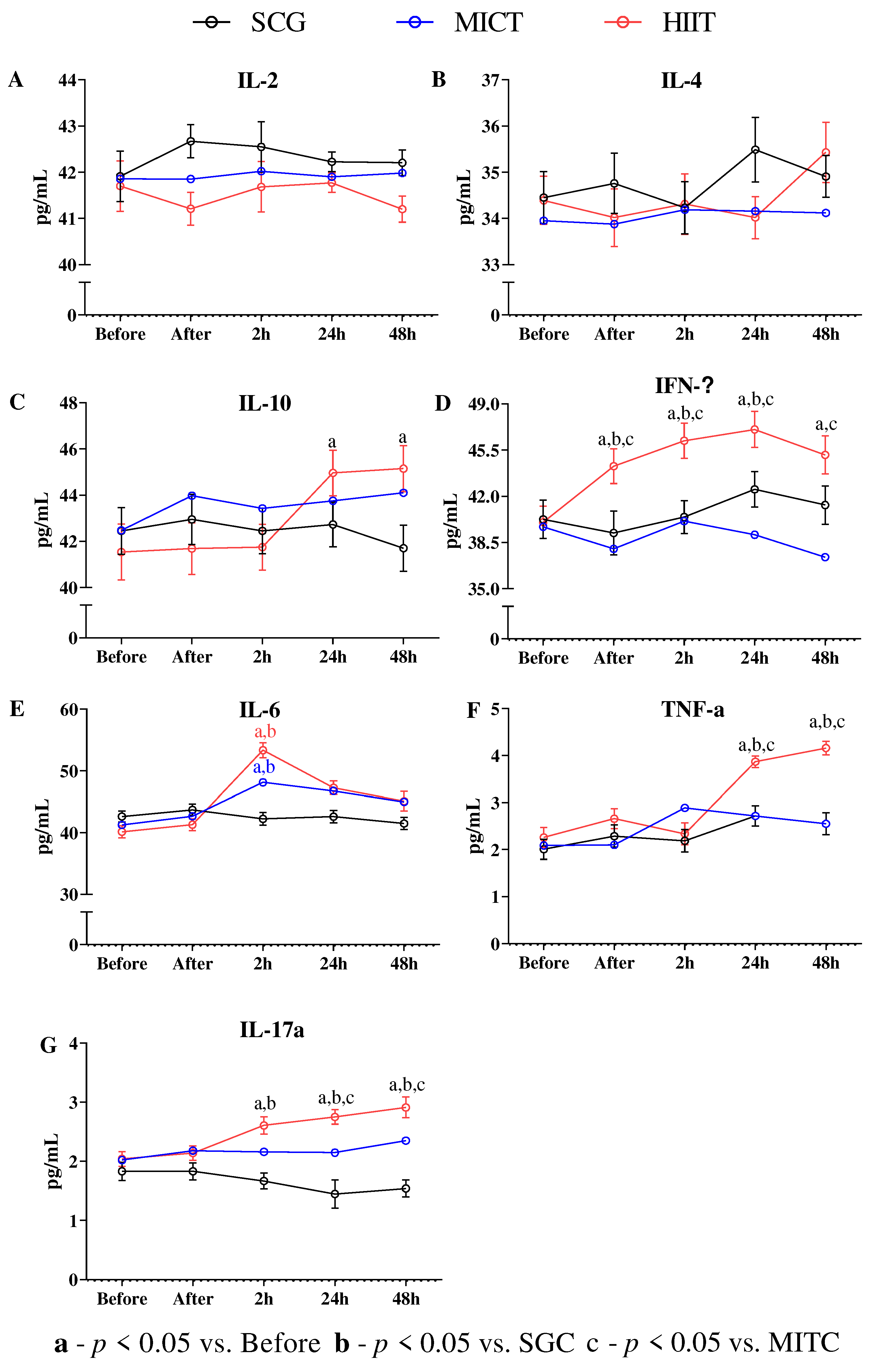
Between the Th2, the IL-2 and IL-4 did not show modulation in all groups (P>0.05) (Fig 2A, and 2B), however, the IL-10 showed improvement in MICT and HIIT 24 and 48h after the exercise challenge if compared with the baseline and SCG (p<0.0001) (Fig. 2C). The IL-6 showed improvement in 2h (p<0.0001) if compared with before (Fig. 2E), and after decreased in all data points. The IFN-γ in HIIT was improved after, 2, 24 and 48h before the exercise (p<0.01) (Fig. 2D) if compared with the baseline and back to previous levels 24h after. The TNF-α showed enhancement at 24h and 48h (p<0.01). Similar behavior was found in the IL17-a showing enhancement 2, 24 and 48h after the exercise. The IFN-ϒ/IL-4 ratio was decreased by 2h (P3) (p<0.01) before the exercise challenge and recovered 24h and 48h after.
Figure 2.
Interleukin and immunoglobulin. Sixty-three old persons were divided into three groups HIIT (n=21) was submitted to a single high-intensity intermittent exercise until exhaustion, SCG (n=21) was kept without exercise practice, and MICT (n=21) submitted at 40 minutes of walking at a moderate intensity. Five-time points of blood by venipuncture to quantification of immunological parameters before, immediately after, 2h after, 24h after, and 48h after the single both of HIIT or MICT was acquired to immunologic parameters quantification. The ANOVA TWO-WAY with Bonferroni’s posterior test at 5% was used to determine the differences between the points.
Figure 2.
Interleukin and immunoglobulin. Sixty-three old persons were divided into three groups HIIT (n=21) was submitted to a single high-intensity intermittent exercise until exhaustion, SCG (n=21) was kept without exercise practice, and MICT (n=21) submitted at 40 minutes of walking at a moderate intensity. Five-time points of blood by venipuncture to quantification of immunological parameters before, immediately after, 2h after, 24h after, and 48h after the single both of HIIT or MICT was acquired to immunologic parameters quantification. The ANOVA TWO-WAY with Bonferroni’s posterior test at 5% was used to determine the differences between the points.
All cytokines analyzed were correlated
As shown in Table 2, is possible to observe that the Cytokines IL-6 x IL-10, IL-6 x TNF-α, and IL-10 x IL-17 are positively associated. While IL-2 x IL-17 expressions are inversely proportional.
Table 2.
Analysis of Correlation of Cytokines.
| IL-4 | IL-10 | IL-6 | IFN-ϒ | TNF-α | IL-17 | |
|---|---|---|---|---|---|---|
| IL-2 | 0.2839 | 0.9567 | 0.9744 | 0.1779 | 0.4750 | (neg) 0.0050 |
| 1L-4 | 0.5244 | 0.9976 | 0.2435 | 0.4819 | 0.1446 | |
| IL-10 | 0.0002 | 0.5512 | 0.0816 | 0.0269 | ||
| IL-6 | 0.7435 | 0.0355 | 0.0122 | |||
| IFN-ϒ | 0.1033 | 0.6270 | ||||
| TNF-α | 0.1121 |
4. Discussion
The hypothesis that guided or investigation states that the high-intensity, however, short time exercise is safe to sedentary older adults, so, to challenge this hypothesis we analyzed of the acute response of white blood cells, and cytokine kinetics in two exercise models, high-intensity interval training, and moderate-intensity interval training and compare both.
To do so sixty-three seniors started the study in the same condition: not previous physical exercise practicing and not having any health impairments identified in clinical examinations and laboratorial parameters. With that, to explore the hypothesis here established, blood collections were acquired before the experimental situation, and immediately, 2h, 24h, and 48h after promoting a time course overview. So, the biochemical tests, exhibited in Table 1 demonstrate that all groups were equal between then. The main results presented showed that the physical exercises modify the leukogram cell count and the cytokine kinetics of the Th1, and Th2 profile as expected, but, the Th17 cytokine expression was an unexpected finding because the literature on the relationship of the IL-7a cytokine with exercise is very poor. Nonetheless, the clinical important about this is that the HIIT or MICT produced a short term transitory immunologic stress in older adults. Together, we revisited the importance of IL-6 and IL-10 importance as previously showed [26,27].
Here stood evident that both exercise regimes induced to an stress of the immune system, already demonstrated by different authors [26,27], including, as previously demonstrated for our group or HIIT [28]. Even more recently, a Th-17 immune response profile, also pro-inflammatory, may be important for the long-term effects achieved by people who achieved HIIT[29,30,31], however, we did not considered this stress so wide as to cause the classic effects related to strenuous exercise where the immune system has difficulty recovering, which causes the phenomenon of the immunological window with a pronounced J curve of the immunological parameters which, at least momentarily, leaves the subjects more susceptible to opportunistic infections as provoked by marathon, triathlon of long term high-intensity athletic proves[32]. However, the classical strenuous exercise beyond high-intensity has long term of exposition, which is a fundamental difference to the approach here tested.
Following the logic rational before displayed, the infections, and diseases in older adults, in many cases, are mediated for a subclinical pro inflammatory state[10,33,34]. This affirmation could contribute against our data in a non-contextualized view, however, here, we discuss that the one acute high-intensity stimulus led to a transient inflammatory state fast and non-prevalent, which is the a desirable stimulus for beneficial adaptations. This same situation if repeated for several time, will chronically provoke an anti-inflammatory state, and also a faster and more potent reaction of immunological agents such as macrophages, neutrophils and natural killer cells[35], which has already been demonstrated to be considerably beneficial such as demonstrated several times in literature[7]. This considerations, allow us affirm that to start one exercise program even in a pandemic state could be safe because the exercise to not injure the immune system of older adults.
Specifically, the white blood cells of older adults showed a classical response to exercise challenge here tested with a fast leukocytosis and lymphocytosis, however, the magnitude of this reactions did not impact the immunity availability for the immune vigilance performed for this type of cells[36], and the effect here observed were lost after 24h for lymphocyte, and basophil, but although we had seemed a normalization in 2h and new increasing in the leucocyte levels in 24h, after 48h all come back to baseline levels. This kind of response to exercise was previously reported[37] and do not compound a inedited data.
In regards to the explication the mechanisms under the immune response here observed, a conjunct of Th1, Th2 and Th17 cytokines were investigated in response to both exercises models here tested. The data presented here show that physical exercises modify the leukogram cell count and the cytokine kinetics of the Th1, Th2, and Th17 profile, including correlations between the cytokine results. The importance of IL-6 and IL-10 has already been revisited[26,27]. This stress on the immune system, already demonstrated by different authors [26,27], was also demonstrated in our study. Even more recently, a Th-17 immune response profile, also pro-inflammatory, may be important for the long-term effects achieved by HIIT [29,30,31].
Is important to remember that sometimes the inflammatory process are a necessary stimulus to generate adaptations, for example, an important signal for muscle hypertrophy is mediated for inflammation[38,39], many immunologic battle against intracellular parasitic disease[40] and intracellular microorganisms has participation of pro inflammatory cytokines [41,42], as well as many medicines effects are mediated for Th1 cytokine profile[40]. In another hand, an incontrollable inflammation could be catastrophic to human body, for example, very recently in human history, the most important effects of COVIV-19 is linked to an exacerbated inflammatory[43], state that lead to tissue destruction and organ impairments[44]. We highlight that even in COVID-19, the physical exercise shown to be a valuable tool against the disease consequence[45], where, was proved that the previous physical exercise practice confer protection[15]. Additionally, the this same approach could help the fast recovery after the disease[45,46,47].
Our data suggest that exercise program, for the elderly population, produces an acute inflammatory profile, with emphasis on the first hours of HIIT, suggesting that they would be able to have a similar profile to other people who were experienced in terms of exercise, such as women, healthy young men, and men managing opioid disorders[31]. We observed that IL-6 was expressed in a behavior similar to that demonstrated for TNF-α, with a significant correlation, suggesting an inflammatory process initiated by TNF-α. A recent study demonstrated that the cytokines IL-6 and TNF-α are indeed increased during exercise[48] but suggest that the role of TNF-α may be related to an inflammation related to cell growth and proliferation[48].
Interestingly, we also emphasize that the correlation analysis, performed mainly with IL-10, suggests a non-classical pro-inflammatory role for this cytokine mediated AMPK/STAT3 pathway as displayed Islam and Cols.[27], which may help us to explain how immune system influences the health success of the elderly.
It is noteworthy that all the results presented here demonstrated transience and immediate recovery of baseline values quickly, however, demonstrating that there was stress in the immune system of the elderly, although these system data suggest adequate immunocompetence. This discussion is extremely timely given the situation in which the world has witnessed COVID-19, as it is evident that this disease affects the cardiovascular, blood, and immune systems, all of which can be affected by exercise at various stages of a training program. Here, the idea of immune inflammation takes time was contested, which is pertinent at this point because exercise increases the cytokine profile almost immediately.
Following this rationale, we challenge the idea about the upper respiratory tract infections (URTI) in older adults in response to on HIIT session. Our data display that no improvement in prevalence of URTI debunking the idea that the intensity of exercise is the most important factor to development of opportunistic infections, but, we argue that the combination between the intensity and volume can produce an unrecovered stress and expose older adults to diseases.
These results corroborate previous data that affirm that the intensity alone do not is the villain in this context[3]. Evidence pointed to the existence of a protective effect as observed in another study 8,17,32,33, but the impossibility of making a direct relationship between the immunological modifications of the exercise with the protection of the upper respiratory tract is our main limitation. Therefore, it is prudent to pursue the data with caution and to avoid further exposure to infections during the first two weeks of the exercise program. Another factor to be considered is our study was performed in a cohort with no presence of comorbidities or chronic diseases, so the subjects showed good immunological competence to produce cytokines, which may not be the rule in this cohort.
Investigations with elderly people with immunodeficiency and inflammatory diseases such as diabetes and obesity may be important and represent another limitation of our study. The control of medications, daily sleep schedule, eating habits, and other daily behaviors was not carried out, however, the random composition of the group and the control group reduced the influence of this variable in our data. We cannot investigate the expression of RNA, enzymes, or proteins involved in many pathways that could help us explain the results observed here, and only cell counts and cytokine kinetics support our discussion. Another limitation example, is about the mechanisms under the observations that do not were explored.
But, what does this article add and what is the clinical significance? First, we put into the discussion that the laboratory tests related to good health did not change in a few hours, proving that the groups formed were elderly people without pre-existing clinical conditions, it is a big limitations of previous studies, however, in the acute phase it is already possible to detect that there are significant differences between the cytokines that modulate the Th1/Th2/Th1 pattern and that these cytokines are correlated with an inflammatory pattern. Studies suggest that the elderly population may benefit from significant increases in IL-10, IL-6, and TNF-α, however, no important alterations on white blood cells were noted despite the interleukin. That the presence of IFN-ϒ may also suggest an improvement in susceptibility to tolerated in the upper administered tract, as well as the increased presence of IL-17 may be something desirable [49].
Therefore, regardless of the patient's age, starting a physical exercise program, whether intense and short-term or moderate for longer, seems to be safe and even desirable, as do other studies that evaluated the benefits of exercise in other children. Finally, it is important to think about future studies that use intense physical exercise in people who use anti-inflammatory drugs for long periods to find out if the cytokines and inflammations released.
5. Conclusions
The data allow us to infer that starting a physical exercise program in elderly patients, who do not have associated diseases, is safe and desirable because no deleterious acute effects in immune system were noted. That the exercises promote a possible systemic inflammation, through cytokines that are released a few hours after the end of the program and that HIIT causes greater intakes than MICT. These findings have clinical implications, since, as we know that physical exercise participates in several biological improvements of the entire human system, the interruption of its practice can cause a decrease in the health, quality of life of the elderly, and an increase in the incidence of physical illnesses.
Author Contributions
Conceptualization, DASS, LDFN and JRVS; DASS, LDFN and JRVS; methodology, DASS, LDFN and JRVS; formal analysis, ACG, BDCM, ES, FNS, DLF, DMS, CSP, RNMS, ECL, AMML; investigation. DASS, LDFN and JRVS; data curation, DASS, LDFN, ES and JRVS; writing—original draft preparation, ACG, BDCM, ES, FNS, DLF, DMS, CSP, RNMS, ECL, AMML, JRVS; writing—review and editing, SASS, JRVS; supervision, JRVS; project administration. All authors have read and agreed to the published version of the manuscript.” Authorship must be limited to those who have contributed substantially to the work reported.
Funding
This research received no external funding.
Institutional Review Board Statement
This project was previously approved by the National Health Council under the number CAAE 44907715.2.0000.5653 on 27/07/2015 and followed all ethical and legal requirements. All participants were assisted by medical services one time a week to determine the upper respiratory tract infections incidence.
Informed Consent Statement
All participants signed the informed consent form in agreement with the Brazilian Ethics Committee.
Conflicts of Interest
The authors declare no conflict of interest.
References
- American Collegue of Sports Medicine. ACSM’s Guidelines For Exercise Testing And Prescription (10th edition). Sport & Exercise Scientist. 2016. [CrossRef]
- Gill, S.K.; Teixeira, A.; Rama, L.; Prestes, J.; Rosado, F.; Hankey, J.; Scheer, V.; Hemmings, K.; Ansley-Robson, P.; Costa, R.J.S. Circulatory endotoxin concentration and cytokine profile in response to exertional-heat stress during a multi-stage ultra-marathon competition. Exerc Immunol Rev 2015, 21, 114–28. Available online: http://www.ncbi.nlm.nih.gov/pubmed/25830597. [PubMed]
- Campbell, J.P.; Turner, J.E. Debunking the Myth of Exercise-Induced Immune Suppression: Redefining the Impact of Exercise on Immunological Health Across the Lifespan. Front. Immunol. 2018, 9, 648. [Google Scholar] [CrossRef] [PubMed]
- Riebe, D.; Franklin, B.A.; Thompson, P.D.; Garber, C.E.; Whitfield, G.P.; Magal, M.; Pescatello, L.S. Updating ACSM’s Recommendations for Exercise Preparticipation Health Screening. Med. Sci. Sports Exerc. 2015, 47, 2473–2479. [Google Scholar] [CrossRef] [PubMed]
- Nieman, D.C.; Henson, D.A.; Smith, L.L.; Utter, A.C.; Vinci, D.M.; Davis, J.M.; Kaminsky, D.E.; Shute, M. Cytokine changes after a marathon race. J. Appl. Physiol. 2001, 91, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Brunelli, D.T.; Caram, K.; Nogueira, F.R.D.; Libardi, C.A.; Prestes, J.; Cavaglieri, C.R. Immune responses to an upper body tri-set resistance training session. Clin. Physiol. Funct. Imaging 2014, 34, 64–71. [Google Scholar] [CrossRef] [PubMed]
- Zhao G, Zhou S, Davie A, Su Q. Effects of moderate and high intensity exercise on T1/T2 balance. Exerc Immunol Rev. 2012;18: 98–114.
- Nieman, D.C.; Wentz, L.M. The compelling link between physical activity and the body’s defense system. J. Sport Health Sci. 2019, 8, 201–217. [Google Scholar] [CrossRef]
- de Souza DC, Matos VAF, dos Santos VOA, Medeiros IF, Marinho CSR, Nascimento PRP, et al. Effects of high-intensity interval and moderate-intensity continuous exercise on inflammatory, leptin, IgA, and lipid peroxidation responses in obese males. Front Physiol. 2018;9: 1–9. [CrossRef] [PubMed]
- Peradini L, Gualano B. Inflammatory cytokine kinetics to single bouts of acute moderate and intense aerobic exercise in women with active and inactive systemic lupus erythematosus. Exerc Immunol Rev. 2015;21: 174–185.
- Suzuki, K. Chronic Inflammation as an Immunological Abnormality and Effectiveness of Exercise. Biomolecules 2019, 9, 223. [Google Scholar] [CrossRef]
- Benatti, F.B.; Pedersen, B.K. Exercise as an anti-inflammatory therapy for rheumatic diseases—myokine regulation. Nat. Rev. Rheumatol. 2015, 11, 86–97. [Google Scholar] [CrossRef]
- Furtado-da-Silva V, Braga JC, Santos KM dos, Oliveira GL de, Olivira TAP de, Teixeira AM, et al. PAIN, INFLAMMATION AND PERFORMANCE CAN PREDICT THE IDEAL MOMENT TO APPLY NEW OVERLOAD. Sport Sci. 2021;14: 32–41.
- Fallon, K. Exercise in the time of COVID-19. Aust. J. Gen. Pract. 2020, 49. [Google Scholar] [CrossRef] [PubMed]
- Narici, M.; De Vito, G.; Franchi, M.; Paoli, A.; Moro, T.; Marcolin, G.; Grassi, B.; Baldassarre, G.; Zuccarelli, L.; Biolo, G.; et al. Impact of sedentarism due to the COVID-19 home confinement on neuromuscular, cardiovascular and metabolic health: Physiological and pathophysiological implications and recommendations for physical and nutritional countermeasures. Eur. J. Sport Sci. 2020, 21, 614–635. [Google Scholar] [CrossRef]
- da Silva, V.F.; Silva, D.A.S.; Martins, P.C.; Calomeni, M.R.; Freire, I.d.A.; Militão, A.G.; Borges, C.J.; Junior, G.d.B.V.; de Moraes, M.A.; Silva, A.J.R.M.; et al. Effect of physical exercise and noninvasive brain stimulation on cognition and dementia of elderly people with frailty: A randomized study. Int. J. Imaging Syst. Technol. 2022, 32, 1941–1952. [Google Scholar] [CrossRef]
- Simpson RJ, Campbell JP, Gleeson M, Krüger K, Nieman DC, Pyne DB, et al. Can exercise affect immune function to increase susceptibility to infection? Exercise immunology review. 2020.
- Song, Y.; Ren, F.; Sun, D.; Wang, M.; Baker, J.S.; István, B.; Gu, Y. Benefits of exercise on influenza or pneumonia in older adults: A systematic review. International Journal of Environmental Research and Public Health. 2020, 17, 2655. [Google Scholar] [CrossRef]
- Nogueira TRB, Oliveira GL de, Oliveira TAP de, Pagani MM, Valentim-Silva JR. Efeito do método Pilates nas adaptações neuromusculares e na composição corporal de adultos jovens. Rev Bras Prescrição e Fisiol do Exerc. 2014;8: 296–303. Available: file:///C:/Users/profe/Documents/Documents/Documents/Artigos/tatiane roberta buratti pilates.pdf.
- Silva, J.R.V.; Marques, A.A.; Nogueira, T.R.B.; da Silva, V.F.; de Oliveira, T.A.P.; de Oliveira, G.L.; Dantas, E.H.M.; Gonçalves, P.S.d.P.; Filho, J.F. Pilates plus Cardiovascular Training in Body Composition: Effects of Adding Continuous Cardiovascular Training to the Pilates Method on Adult Body Composition. MOJ Sports Med. 2018, 2, 1–5. [Google Scholar] [CrossRef]
- Lameira-de Oliveira G, Gonçalves PS de P, Perini-de Oliveira TA, Valentim-Silva JR, Roquetti-Fernandes P, Fernandes-Filho J. Body composition and somatotype of athletes of Brazilian w5-a-side football team: Paralympic team rio 2016. Rev Fac Med. 2018;66: 25–29. [CrossRef]
- de Oliveira GL, de Oliveira TAP, de Pinho Gonçalves PS, Silva JRV, Fernandes PR, Filho JF. Body image and eating disorders in female athletes of different sports. J Exerc Physiol. 2017;20: 44–54.
- Silva VF da, Junior G de BV, Filho GO, Vieira MAM, Coelho EC da S, Araújo TS de, et al. ACUTE EFFECT OF RESISTANCE VS AEROBIC TRAINING ON EXECUTIVE FUNCTIONS OF OLDER ADULTS. Sport Sci. 2020;13: 122–128.
- Louzada-Júnior, A.; Da-Silva, J.M.; Da-Silva, V.F.; Castro, A.C.M.; De-Freitas, R.E.; Cavalcante, J.B.; Dos-Santos, K.M.; Albuquerque, A.P.A.; Brandão, P.P.; Bello, M.d.N.D.; et al. Multimodal HIIT is More Efficient Than Moderate Continuous Training for Management of Body Composition, Lipid Profile and Glucose Metabolism in the Diabetic Elderly. Int. J. Morphol. 2020, 38, 392–399. [Google Scholar] [CrossRef]
- Braga, J.C.; de Freitas, R.E.; dos Santos, K.M.; da Silva, R.P.; da Silva, J.M.; Junior, A.L.; de Oliveira, G.L.; Oliveir, T.A.P.; Pernambuco, C.S.; da Silva, V.F.; et al. Twelve Weeks of High-Intense Interval Training Enhance the Neuromuscular and Cardiorespiratory Performance of Elderly. Open Sports Sci. J. 2020, 13, 42–48. [Google Scholar] [CrossRef]
- Fischer, C.P. Interleukin-6 in acute exercise and training: what is the biological relevance? Exerc Immunol Rev. 2006, 12, 6–33. [Google Scholar]
- Islam, H.; Neudorf, H.; Mui, A.L.; Little, J.P. Interpreting ‘anti-inflammatory’ cytokine responses to exercise: focus on interleukin-10. J. Physiol. 2021, 599, 5163–5177. [Google Scholar] [CrossRef] [PubMed]
- Silva VF, Marinho DA, Dantas EHM, Santos SS, Teixeira AM, Silva AJRM, et al. Short Exhaustive Intermittent Exercise Results in Acute Inflammatory and Rheumatic Markers Release. J Exerc Physiol Online. 2019.
- Siasos, G.; Athanasiou, D.; Terzis, G.; Stasinaki, A.; Oikonomou, E.; Tsitkanou, S.; Dimitropoulos, S.; Kolokytha, T.; Tzirogiannis, K.; Giannaki, A.; et al. The Acute Impact of Different Types of Aerobic Exercise on Arterial Wave. Cardiology 2016, 135, 81–86. [Google Scholar] [CrossRef]
- Durmus, P.T.; Vardar, M.E.; Kaya, O.; Tayfur, P.; Sut, N.; Vardar, S.A. Evaluation of the Effects of High Intensity Interval Training on Cytokine Levels and Clinical Course in Treatment of Opioid Use Disorder. Turk. J. Psychiatry 2020, 31, 151–158. [Google Scholar] [CrossRef] [PubMed]
- Minuzzi, L.G.; Lira, F.S.; de Poli, R.A.B.; Lopes, V.H.F.; Zagatto, A.M.; Suzuki, K.; Antunes, B.M. High-intensity intermittent exercise induces a potential anti-inflammatory response in healthy women across the menstrual cycle. Cytokine 2022, 154, 155872. [Google Scholar] [CrossRef]
- Pyne, D.B.; Gleeson, M. Effects of Intensive Exercise Training on Immunity in Athletes. Int. J. Sports Med. 1998, 19, S183–S194. [Google Scholar] [CrossRef]
- Manna, P.; Jain, S.K. Obesity, Oxidative Stress, Adipose Tissue Dysfunction, and the Associated Health Risks: Causes and Therapeutic Strategies. Metab. Syndr. Relat. Disord. 2015, 13, 423–444. [Google Scholar] [CrossRef] [PubMed]
- Ringseis R, Eder K, Mooren FC, Krüger K. Metabolic signals and innate immune activation in obesity and exercise. Exerc Immunol Rev. 2015;21: 58–68. Available online: http://www.ncbi.nlm.nih.gov/pubmed/25825956.
- Idorn, M.; Hojman, P. Exercise-Dependent Regulation of NK Cells in Cancer Protection. Trends Mol. Med. 2016, 22, 565–577. [Google Scholar] [CrossRef]
- Wardyn, G.G.; Rennard, S.I.; Brusnahan, S.K.; McGuire, T.R.; Carlson, M.L.; Smith, L.M.; McGranaghan, S.; Sharp, J.G. Effects of exercise on hematological parameters, circulating side population cells, and cytokines. Exp. Hematol. 2008, 36, 216–223. [Google Scholar] [CrossRef]
- Freidenreich DJ, Volek JS. Immune responses to resistance exercise. Exerc Immunol Rev. 2012;18: 8–41.
- Communications S, Kraemer WJ, Adams K, Cafarelli E, Dudley GA, Dooly C, et al. American College of Sports Medicine position stand. Progression models in resistance training for healthy adults. Med Sci Sports Exerc. 2002. [CrossRef] [PubMed]
- Peake, J.M.; Della Gatta, P.; Suzuki, K.; Nieman, D.C. Cytokine expression and secretion by skeletal muscle cells: regulatory mechanisms and exercise effects. Exerc. Immunol. Rev. 2015, 21, 8–25. Available online: http://www.ncbi.nlm.nih.gov/pubmed/25826432. [PubMed]
- Valentim-Silva, J.R.; Macedo, S.R.A.; de Barros, N.B.; Ferreira, A.d.S.; da Silva, J.H.M.; Nicolete, L.D.d.F.; Nicolete, R. Antileishmanial drugs activate inflammatory signaling pathways via toll-like receptors (docking approach) from Leishmania amazonensis-infected macrophages. Int. Immunopharmacol. 2020, 85, 106640. [Google Scholar] [CrossRef] [PubMed]
- Carvalho-Gontijo, R.; Peruhype-Magalhães, V.; Costa-Silva, M.F.; Martins-Filho, O.A.; Quaresma, P.F.; Freire, J.d.M.; Moreno, E.d.C.; Teixeira-Carvalho, A.; Gontijo, C.M.F. Protective Profile Involving CD23/IgE-mediated NO Release is a Hallmark of Cutaneous Leishmaniasis Patients from the Xakriabá Indigenous Community in Minas Gerais, Brazil. Scand. J. Immunol. 2015, 81, 515–524. [Google Scholar] [CrossRef] [PubMed]
- Gantt, K.R.; Goldman, T.L.; McCormick, M.L.; Miller, M.A.; Jeronimo, S.M.B.; Nascimento, E.T.; Britigan, B.E.; Wilson, M.E. Oxidative Responses of Human and Murine Macrophages During Phagocytosis ofLeishmania chagasi. J. Immunol. 2001, 167, 893–901. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Z.; Xu, L.; Xie, X.; Yan, H.; Xie, B.; Xu, W.; Liu, X.; Kang, G.; Jiang, W.; Yuan, J. Pulmonary pathology of early-phase COVID-19 pneumonia in a patient with a benign lung lesion. Histopathology 2020, 77, 823–831. [Google Scholar] [CrossRef] [PubMed]
- de Alencar, J.C.G.; Marchini, J.F.M.; Marino, L.O.; Ribeiro, S.C.D.C.; Bueno, C.G.; da Cunha, V.P.; Neto, F.L.; Neto, R.A.B.; Souza, H.P.; COVID U. S., P. Registry Team. Lung ultrasound score predicts outcomes in COVID-19 patients admitted to the emergency department. Ann. Intensiv. Care 2021, 11, 6. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Lázaro, D.; González-Bernal, J.J.; Sánchez-Serrano, N.; Navascués, L.J.; Ascaso-Del-Río, A.; Mielgo-Ayuso, J. Physical Exercise as a Multimodal Tool for COVID-19: Could It Be Used as a Preventive Strategy? Int. J. Environ. Res. Public Heal. 2020, 17, 8496. [Google Scholar] [CrossRef] [PubMed]
- Barker-Davies, R.M.; O'Sullivan, O.; Senaratne, K.P.P.; Baker, P.; Cranley, M.; Dharm-Datta, S.; Ellis, H.; Goodall, D.; Gough, M.; Lewis, S.; et al. The Stanford Hall consensus statement for post-COVID-19 rehabilitation. Br. J. Sports Med. 2020, 54, 949–959. [Google Scholar] [CrossRef]
- Humphreys, H.; Kilby, L.; Kudiersky, N.; Copeland, R. Long COVID and the role of physical activity: a qualitative study. BMJ Open 2021, 11, e047632. [Google Scholar] [CrossRef]
- Shobeiri, P.; Seyedmirzaei, H.; Karimi, N.; Rashidi, F.; Teixeira, A.L.; Brand, S.; Sadeghi-Bahmani, D.; Rezaei, N. IL-6 and TNF-α responses to acute and regular exercise in adult individuals with multiple sclerosis (MS): a systematic review and meta-analysis. Eur. J. Med Res. 2022, 27, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Wan, M.T.; Shin, D.B.; Winthrop, K.L.; Gelfand, J.M. The risk of respiratory tract infections and symptoms in psoriasis patients treated with interleukin 17 pathway–inhibiting biologics: A meta-estimate of pivotal trials relevant to decision making during the COVID-19 pandemic. J. Am. Acad. Dermatol. 2020, 83, 677–679. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



