
Submitted:
14 March 2023
Posted:
15 March 2023
You are already at the latest version
Abstract
An out-of-hospital cardiac arrest (OHCA) is one of the leading causes of death in the world. The survival rate can be influenced by the Chain of Survival. The school is the institution that has the opportunity to promote the education of citizens in Basic Life Support (BLS), increasing the number of trained bystanders. This study aimed to identify the theoretical and practical knowledge and self-reported skills in BLS, in order to characterise the motivation to intervene in an emergency situation. A quantitative, descriptive, cross-sectional, and analytical study of the survey type was developed with a sample of 1215 students enrolled in 10th grade of secondary education in 2019-2020 in Portugal. The results point to a fragile appropriation of theoretical and practical knowledge in the field of BLS. Self-declared competences tend to rank below the theoretical knowledge manifested. Motivation to intervene is high: students are sensitive to the topic, willing to learn and highlight the importance and social relevance of the topic. We conclude that students do not feel nor are able to intervene in an OHCA episode. It seems necessary to develop didactic proposals that align the teaching of BLS with the Essential Learning at the end of compulsory education in Portugal.
Keywords:
basic life support education
; student’s perceptions
; education quality
; skills to intervene.
1. Introduction
Cardiac arrest can be caused by any heart disease, with electrical malfunctions of the heart being the most common cause [1]. Most cardiac arrests that are not of cardiac origin have respiratory causes, namely drowning and asphyxia [2]. Failure to recognise out-of-hospital cardiac arrest (OHCA) remains a barrier to saving more lives [36]. Several studies reinforce the importance of Basic Life Support (BLS), practiced bystander, as a factor that contributes to improving the survival rate of OHCA [3,4,5,6,7,8,9,10,11].
More people can survive an OHCA when the Chain of Survival (CoS) sequence runs as quickly as possible [12]. Despite advances, less than 40% of adults receive BLS initiated by bystanders [13]. Therefore, increasing the motivation of non-professionals to perform BLS may have a direct impact on OHCA survival rates [14]. One of the most important steps in increasing the rate of resuscitation and improving survival is to educate all school-age children and youth on BLS [2]. The training in BLS should take place across the board from pre-school to university education and the skills to be developed should take into account the age of the students [15].
Teachers can play a key role in teaching BLS in school [16,17,18] and investment in the training of young people, attending high school, in a period between 45–60 minutes, per school year, would imply significant gains in terms of BLS skills [19]. Large-scale youth training is possible through a peer-training programme and a two-hour training programme contributes to improving the ability of pupils under the age of 13 to start CoS [17,20], in both cases with minimal implementation costs. Among 10th, 11th and 12th grade students in Portugal, the training provided by teachers in schools, with lower financial expenditure, shows similar levels of effectiveness to the training provided by health professionals [16].
In Europe, children's BLS education is currently regulated in six countries: Belgium, Denmark, France, Italy, Portugal and the United Kingdom. In Portugal, the objectives referring to BLS can be found in the Essential Learning in the subject of Natural Sciences in 9 th grade of Basic Education [21], and in Physical Education, in Secondary School [22].
As there are few studies on the teaching and learning of BLS in Portugal, this study applied a questionnaire to students of the 10th grade which aimed to: 1) assess the appropriation of theoretical and practical knowledge in BLS of students made in the 9th grade; 2) to analyse the students' perceptions of the theoretical and practical training received in that year of schooling; 3) to analyse the self-reported skills and motivation to intervene in BLS of 10th grade. Based on the theoretical and conceptual framework, the following general hypothesis was established - The motivation to intervene in BLS is related to the self-perception of the competence acquired in this domain -, with the definition of the operational hypothesis: The self-perception of competence in BLS is positively correlated with the motivation to intervene.
The study fills a gap in the literature and presents recommendations, based on the results and conclusions, to support decision makers in optimising BLS training in the Natural Sciences discipline. Suggestions for future work are also made.
In addition to this introduction, the following section presents the methodological options, including the study design, the population and sample, how the data was collected and analysed. Subsequently, the results are presented and discussed, according to the hypothesis and the variables considered: socio-demographic information; perceptions on the appropriation of theoretical and practical knowledge on BLS, on the theoretical and practical training received and on the acquisition of skills; conceptions on the intervention in the community on BLS.
2. Materials and Methods
2.1. Study design
A descriptive, cross-sectional and analytical survey design was adopted, with a representative sample of students from the 10th grade (15-16 years old), in order to assess the quality of learning achieved in the Natural Sciences subject in the 9th grade with regard to BLS learning.
2.2. Population and sampling
The population is made up of students enrolled in the 10th grade, of scientific-technological courses, in the academic year 2019-2020, in Portugal: 68,769, of which 31,100 (45.2%) are male and 37,669 (54.8%) are female [23]. A non-probability accidental sample was chosen: all respondents attended the 10th grade. Both genders were represented. 1215 valid responses were obtained (confidence interval = 99% and sampling error = 3.67%).
2.3. Information collection tool and questionnaire validation
An original questionnaire was designed with six dimensions: a) socio-demographic information (D1); b) theoretical knowledge (D2); c) perceptions about the theoretical (D3) and practical (D4) training received; d) perceptions about the acquisition of skills (D5); e) conceptions about community intervention (D6). In D1, identification questions were designed. D2 aims to assess the learning of facts and concepts about BLS. Predictably, such knowledge will have been taught, as stipulated in the Essential Learning, in the subject of Natural Sciences of the 9th grade. For this purpose, we chose to write closed-ended information questions, with a nominal scale with dichotomous items: "disagree" and "agree". Ninety-two items were formulated which, after the pilot testing process, formed a group of 57 items (Table 1).
D3 and D4 assess students' perceptions of the training received, respectively theoretical and practical. Opinion questions and a numerical quantity rating scale were developed, with five response categories [24]: 1) “the topic has not been addressed”, 2) “I do not feel prepared”, 3) “I feel underprepared”, 4) “I feel well prepared”, 5) “I feel very well prepared”. To conclude D3 and D4, two opinion questions were created with an ordinal scale, so that students could position themselves according to their self-perception of the theoretical and practical training received, using a 10-point scale as a reference matrix [from 1 ("very weak") to 10 ("excellent")]. The D3 initially had 17 items, which was reduced to 16 items with piloting. D4 was initially composed of 16 items, which was increased to 18 items with the judges' opinion. D5 aimed to assess the self-perceptions on the acquisition of skills in the various domains of BLS. Opinion questions and a numerical quantity rating scale of four response categories were developed: 1) “I do not feel prepared”, 2) “I feel underprepared”, 3) “I feel well prepared”, 4) “I feel very well prepared”. To conclude D5, an opinion question was created with an ordinal scale, so that students could position themselves according to their self-perception of the acquisition of competences, using a 10-point scale as a reference matrix [from 1 (“very weak”) a 10 (“excellent”)]. This dimension has 23 items. At the end of the questionnaire, students' conceptions about the BLS intervention in the community were assessed through 5 items. A final question with an ordinal scale was created so that students could position themselves according to their motivation to intervene in BLS, using a 10-point scale as a reference matrix. [from 1 (“very weakly motivated") to 10 (“highly motivated”)].
The questionnaire matrix was submitted to a panel of five jurors and their contributions were considered [25]. The pilot questionnaire was applied to a sample of 134 students (56.0% female) attending the 10th grade in the 2018-2019 school year in three schools, which were excluded from the sample. The internal consistency of each item was calculated using the Cronbach’s alpha (α), with moderate to high reliability and high: D2 = .838, D3 = .949, D4 = .960, D5 = .965. The questionnaire was formatted in computer support and applied online, using Google Forms.
2.4. Information analysis
The information collected in the platform was exported in .xls format; the file was imported directly into the Software IBM SPSS Statistics 24. Data were treated and analysed using descriptive and inferential analysis techniques (univariate, bivariate and multivariate). For data treatment, the answers were scored, with the highest value being agreement with the theoretical framework / I feel very well prepared. The study of the normality of the distribution was performed using the Kolmogorov-Smirnov (K-S) test, with Lilliefors correction.
To assess the degree of association between variables (theoretical knowledge, perceptions of theoretical training, perceptions of practical training, perceptions of the acquisition of skills, motivation to intervene) we used bivariate analysis, which can be done by calculating parameters that allow quantifying the linear association between two variables, the covariance or correlation coefficient. Therefore, Pearson's coefficients and the Chi-square test were calculated. Multivariate analysis was used to study three or more variables simultaneously. The model used in the logistic regression took into account the variables that appeared to be potential regressors, which considered the possible associations between variables, for a model created in a context of non-multicollinearity, i.e., the independent variables were not strongly correlated among themselves.
3. Results and discussion
3.1. Sociodemographic information
About 59.3% of the respondents are female (4.5 points above the national average). The average age is 15.8 years with a median and mode of 16 (standard deviations - SD = .72). The minimum age is 14 and the maximum 19.
3.2. Perceptions on the appropriation of theoretical and practical knowledge in BLS
3.2.1. CoS and the survival rate in OHCA
The results show that about 75.0% of the students have the appropriate theoretical knowledge about the CoS and survival rate in OHCA, results that agree with those found in other authors [12,26]. The modal value of this indicator is two, corresponding to the agreement with the propositions presented. The statement with the highest consensus (93.3%) is about the purpose of BLS performed by the bystander (q2 - "The purpose of BLS, performed by the person who witnessed an OHCA, is to maintain breathing and circulation until differentiated help arrives"). The false propositions (q1 - "BLS corresponds to any form of chest compression or artificial ventilation" and q5 – “The links in the CoS are sequentially: Early BLS (resuscitation); Early access to Emergency Medical Services (call 112); Early defibrillation (to restart the heart); Early post resuscitation care (to restore quality of life)”) are those that generated the greatest dispersion of responses, with SD, respectively, of .493 and .498. Even so, the majority disagree with the positions (respectively, 55.0% and 58.3%), aligned with the theoretical framework. The female students show less correct knowledge than the male students, in a difference of one percentage point, without significant expression (p = .269).
3.2.2. Examination of the adult and paediatric patient based on the ABC initial approach
The agreement of this indicator with the theoretical framework on the assessment of safety conditions and patient response is 67.9%. The statement receiving the highest agreement (92.3%) corresponds to the need to ensure safety conditions for the rescuer, the victim and third parties before performing the rescue (q6). The greatest departure from the theoretical framework is seen in item q15, in which 78.0% believe that it is unnecessary to call for help from the European emergency number with a responsive victim, followed by the defence of starting BLS, even if safety conditions are not guaranteed for the rescuer (q7 – 75.8%). The false items generated, in general, a higher dispersion of answers, with a SD between .414 and .496. This maximum value is only exceeded in item q14 ("A victim who reacts to the assessment of the state of consciousness should be kept in the position he/she was in"), with a 5.3:4.7 split between agreement and disagreement. The modal value of this indicator reflects the "agreement”.
Analysing each sub-indicator individually, the knowledge on the assessment of safety conditions is expressed by 69.9% of the respondents. The expression that generated the highest acceptance refers to the need for the bystander, before approaching a victim, to ensure safety conditions for him/herself, the victim and third parties (q6 – 92.3%). But, unusually, a high percentage of students (q7 - 75.8%) indicate that in OHCA, even if safety conditions are not guaranteed for the bystander, BLS manoeuvres should be initiated, which departs from current knowledge. Two other assertions were positively assumed, such as the duty, when approaching the victim, to avoid contact with blood or other bodily fluids (q8 - 88.6%) and to look for clues about what might have caused the emergency (q10 – 80.7%). This question (q10) registered mode and median with "disagree". The modal class for the assessment of safety conditions is "agree". The students' knowledge, in this sub-indicator, is higher than the girls' by approximately 8.8 percentage points, with significant expression (p ≤ .001).
With regard to the assessment of patient response, technical knowledge is weaker than above. Only 55.0% of the respondents agree with the theoretical framework. The highest expression was obtained with the technique of evaluating the reactivity of an adult victim, indicated by 78.8% of the students (q12). A roughly equally sized group, however, considers it unnecessary to call for help to the European emergency number with a responsive victim (q15), contrary to the indications of the European Resuscitation Council (ERC,) defended by the INEM [27,28]. Any of the five propositions registered SD > .40, indicating dispersion of opinions. The modal value of this sub-indicator is "agreement", assuming the value of "disagreement" in item q15. In this field, the knowledge of boys and girls seems to be more or less identical (p = .201).
Knowledge about airway permeabilization is confided by about ¾ of the students. The greatest consensus is on the essential objectives of the BLS: permeabilization of the airway and restoration of breathing (q20 – 90.6%). However, the group fails to note that in situations of suspected trauma, airway permeabilization is not done with head extension and chin lift manoeuvre, but with mandible subluxation (jaw-thrust manoeuvre – triple manoeuvre) (q19 – 50.4%), departing from the current knowledge presented by the INEM [27,28]. This was the item that recorded the highest SD of this sub-indicator (.50). Permeabilization of the infant's airway generated some division (q18), with 35.1% disagreeing with the correct technique (SD = .477). The modal value of this sub indicator is " agreement". Females have more knowledge appropriate to the state of the art than males, at around 6.0% (p ≤ .001).
The distribution of the results on the assessment of the signs of breathing generally follows the pattern described above, although with a value of < 10%. About 65.3% of the respondents have knowledge in line with the theoretical framework, with the maximum expression in how the breath assessment is carried out (q21 – 84.4%). However, the majority of the group (q25 - 61.5%) erroneously indicate that when a bystander is unsure whether the victim ventilates normally, they should act as if res-breathing is present, contrary to the literature [29,30].
The duration of the breath assessment (q22) generates the highest dispersion of positions (SD = .498), ex aequo with the installed doubt that a gasp may correspond to breathing (q24). The modal value remains in " agreement", with the value "disagree" being registered in two questions (q24 - "In the assessment of signs of breathing, a gasp from the victim is equivalent to breathing”; q25 – “When a rescuer is unsure if the victim is breathing normally, they should act as if breathing is present."). The mean dispersion is .44. The male gender shows an adequate theoretical knowledge on the assessment of res-breathing signs 3.7% higher than the female gender, with a statistically significant expression (p ≤ .001).
The assessment of circulation signs in infants is known to just over ¾ of the group of respondents, with no disagreements recorded above 28.1%. It should be noted that it is precisely this last value that is found in item q29: "A child who has signs of circulation but is not ventilating should receive up to one insufflation with exhaled air every 3 seconds”. It is on the BLS, with only insufflations and with cardiopulmonary resuscitation (CPR), that the greatest doubts and dispersion of positions fall (q29, SD = .450; q30, SD = .437). The mean dispersion is .44 and the modal value of "I agree". The male gender presents a theoretical knowledge 3.7% below the female gender, with a statistically significant expression (p ≤ .001).
According to the results, the requirements for applying the lateral safety position (LSP) are the domain of 68.8% of the students. About 51.1% consider that this is also the position for non-reactive victims without effective breathing (SD = .50), contrary to the ERC recommendations. Some 37.0% are not sure that LPS applies in the same way to children. The modal and median value of this sub-indicator is "I agree", with the highest dispersion of answers in items q29 (“A child who has signs of circulation but does not ventilate should receive up to one insufflation with exhaled air every 3 seconds," SD = .450) and q30 ("A child without signs of circulation should receive 15 chest compressions alternating with two insufflations," SD = .437). The mean dispersion is .44. The differences, although small, are significant (p ≤ .001).
3.2.3. Emergency alarm procedures
Knowledge of emergency alarm procedures is the domain of just over ¾ of respondents. In detail, students recognise the need to follow the advice of the operator of the Urgent Patient Guidance Center of the National Institute of Medical Emergency, even though these may be extensive (q39 - 91.4%), which agrees with Monsieurs et al. [2], underlined in the 2015 ERC Guidelines. Three items were selected by more than 87.0%, highlighting the exact location where the victim is, as a decisive factor for the speed of rescue (q38 - 91.1%) and communication between the Urgent Patient Guidance Center and the patient, whenever the patient can do so (q37 – 87.7). Opinions differ significantly, however, as to when to activate the European emergency number. whereas almost half of respondents believe that they should look out for signs of circulation in an adult before dialling for help on this phone number (q36 – 48.1%; SD = ,50), this value decreases to around 40.0% in another control question (q40 - "In an adult patient, contact with 112 is made from the moment when absence of breathing signs is detected"). The modal value is "I agree". The differences between genders, although reduced, are significant (p ≤ .001).
3.2.4. Adult BLS procedures
With regard to adult BLS procedures, students' knowledge falls 28.9% short of the desired level. The most favourably acknowledged item is the fact that after assessment of the signs of breathing, no signs of circulation are assessed (q46 - 85.4%); but if this is so, it is not clear the reason for q36 (“If an adult victim is not breathing normally, signs of circulation should be immediately searched for before activating 112"), of control, having been ruled out by only 51.9% of respondents. In these procedures, some disagreement of opinions also emerged. The majority (55.1%) came to the opinion that chest compressions should be performed without removal/removal of the clothes covering the victim's thorax (q43) and 45.2% doubt that these, in adults, should be performed on the lower half of the sternum (q45), questions that registered the highest SD = .498. No less important is that about 20.0% of students advocate starting the adult BLS protocol with two inflations and not stopping the manoeuvre if the victim has a spontaneous opening of the eyes. The modal value of this indicator is "I agree", assuming the value "I disagree" in q43 ("Chest compressions should be performed without removing/removing the clothes covering the victim's chest"). It should be noted that inadequate knowledge is, with statistical significance, higher among boys (p ≤ .001).
3.2.5. Paediatric BLS procedures
The value found regarding the knowledge of paediatric BLS procedures is the lowest within the BLS contents, obtaining only 57.9% of agreement with the theoretical framework. The only aspects that received approval above 70.0% is the fact that, in an infant, chest compression is performed with two fingers (q50 - 76.0%), on the lower half of the sternum, one finger above the xiphoid process (q48 - 70.1%). However, the value of the chest compression depth in the infant is unknown by more than half of the students (q49 – 58.5%).
The results found here tend to point to what is advocated by other authors [15], stating that the contents should be adapted to the target audience, simplifying them as much as possible in order to allow for simpler but effective procedures regarding the insecurity that prevents any intervention. It should be noted that the paediatric BLS protocol is more complex than the adult protocol. Some studies show that research on CPR teaching has mostly focused on adult training of the adult algorithm, which reveals a lack of knowledge about the practices with children and young people [29]. High minorities ignore the protocol, regarding the performance of five breaths after detecting that a child does not ventilate normally (q47 - 39.8%) and that chest compression can be done with only one hand or using both hands (q51 – 44.7%). Most are also unaware that in paediatric BLS, with only one resuscitator, the manoeuvres are maintained for one minute and only then, if you are still alone, are you contacted the European emergency number (q52 – 56.0%), which recorded the highest SD (= .497) for this indicator, ex aequo with q51 ("In a child, chest compression can be done with one hand only or using both hands”). The modal value is "agreement" and SD = .48. There is a difference in adequate knowledge, with statistical significance, more favourable to males (p ≤ .001).
3.2.6. Airway obstruction
The knowledge on airway manoeuvres for foreign body airway obstruction does not exceed 66.7%. A group slightly above ¾ considers that in a light foreign-body airway obstruction the victim should be suggested to cough (q57 - 77.3%), which is in line with the current knowledge advocated by the ERC and included in INEM's manuals [27,28], recording the highest value of this indicator. The airway clearance algorithm is recognised by 75.1% of the sample (q55); but there is controversy regarding its application to an infant (q56 – 57%). The identification of airway obstruction by signs is dubious: 37.8% consider that the victim, in a sign of distress, places his hand on the thorax area (q53); 38.3% do not know the signs of choking by severe tin body, results that do not agree with those advocated by the INEM [27,28]. The average dispersion of the answers was 0.46, with the highest value in question 56 ("In an infant with airway obstruction due to a foreign body, back blows and chest compression are applied”, SD = .495). The median and modal value is "I agree". In this field, female students show more solid theoretical knowledge than male students, with a differential of about 4.2%. (p ≤ .002).
Having arrived at this point, we are now in a position to make a synthesis of the results found. The graph in Figure 1 shows the agreement and disagreement for each indicator.
If we make an overall analysis of the results, it is clear that about 68.5% of the students have adequate knowledge of the state of the art of adult and paediatric BLS, LSP and methods to clear the airway. The topics with the lowest proficiency concern patient response assessment (55.0%) and paediatric BLS procedures (57.9%). The median and modal values are, ex aequo, 1.9. Still, about 47.3% of the assertions received ≥ 75% favourable points. Seven propositions registered agreement values ≤ 50.0% and two were even ≤ 25.0%.
Data analysis points to some specific differences in relation to the "gender" variable, with better results for females, which overall are reduced to half a percentage point in relation to males (68.8%) (p ≤ .001). These results agree with those found by other authors [32], who reveal that female students have a better level of theoretical knowledge.
3.3. Perceptions of the theoretical training received
The analysis of the information reveals that 22.9% of the respondents declare that they are not prepared, in theoretical terms, on the themes of the BLS, either because the themes have not been approached (7.7%), or because, despite having been approached, they do not feel effectively prepared (15.2%). About 35.5% of the students feel poorly prepared. Only a fringe of 41.6% feel prepared (33.0% well prepared and 8.6% very well prepared).
Among the various topics in which students feel prepared, LSP (q72) is the one with the highest expression, still without exceeding 60 percentage points. It is followed, above 50%, by the assessment of safety conditions when approaching a victim (q59), with 54.3% of choices, the vital sign assessment (q63), with 54.0%, and the procedures in case of emergency (q65), with 51.4%. Little preparation has its maximum expression in CoS and survival rate in OHCA (q58), with 43.7%, accompanied by knowledge of the paediatric BLS algorithm (q67), with 43% of preferences. Regarding the lack of preparation, 38.8% do not know how to provide help for severe airway obstruction in infants, 35.1% do not know how to assess the response of the paediatric patient and 32.1% and do not know the paediatric algorithm. The modal value is "I feel unprepared”.
Overall, 77.1% of the respondents were relatively well prepared (between a little and very well prepared) about the theoretical concepts on BLS. This value is higher than that measured in D2, in which 68.5% of students showed adequate knowledge of the state-of-the-art. That is, between the perception of preparation and its demonstration there is a deficit of 8.6%. But if we look at the effective conceptual preparation, we see that the students' self-perception falls short of 26.9% of what was revealed in the knowledge test.
Let us now compare the students' self-perceived theoretical preparation with that revealed in this study. For this purpose, the preparation revealed was considered as the results to indicators 1-6 of questions 1-57. With regard to the perceived preparation, two scales were considered: a) “reasonably prepared", the agglutination of the perceptions "poorly prepared" and "well prepared”; b) “well prepared", the combination of the perceptions "well prepared" and "very well prepared". It should be noted that the self-perception of theoretical preparation (well prepared and not very well prepared) is below the revealed preparation, as assessed in this study. Poor preparation falls on average, 6.1 percentage points short of good preparation.
In summary, the students' perception is more pessimistic than what was revealed, which may condition their self-efficacy beliefs on this topic. Despite a relatively low command of theoretical subjects (67.0%), it is significantly higher than the average of those who feel well prepared (41.6%) and those who feel poorly prepared (36.5%). It should be noted that the female students who answered the questionnaire feel better prepared theoretically (2.7%) than the boys. The latter outnumber the females by five percentage points in the absence of preparation (p ≤ .002).
As a summary of this section, students were asked to rate their theoretical training received on BLS by placing themselves on a 10-point interval scale (where 1 corresponds to "very poor" and 10 to "excellent"). The results are shown in the graph in Figure 2.
The mode and median value found is 7, with a mean of 6.41 and SD = 1.96. The graph in Figure 3 distributes the results between the two genders. Even though in the perceptions about the theoretical training received, reflected in the 15 themes presented (q58-q72) boys feel less well prepared than girls, when they position themselves on a scale they self-assess with an average of 7.2 points, 1.0 percentage point higher than females, a statistically significant result (p ≤ .001).
3.4. Perceptions of the practical training received
The analysis of the information reveals that 27.4% of the respondents do not consider themselves prepared, in practical terms, on the subjects of the BLS, either because the subjects have not been approached (10.7%) or because, although they have been approached, they do not feel effectively prepared (16.7%). Some 35.2% of the students feel poorly prepared. Only a fraction of 37.4% feels prepared (30.8% well prepared and 6.5% very well prepared).
Among the various subjects in which students feel prepared, LSP (q90) is the one with the highest expression, even though it does not exceed 58.7 percentage points. This is followed, above 50.0%, by practical training on assessment of respiration signs (q77), with 54.1% of choices, and on chest compressions in adults (q81), with 50.1%. All other subjects are below the average line in terms of preparedness. Low preparedness assumes maximum value with the practices of ventilation support for children (q85 – 40,2). At this stated level of proficiency, 14 items assume values above 30.0%. About 47.0% of the topics presented on BLS register an absence of preparation higher than 25.0% of the students.
Overall, 72.6% of the respondents were reasonably prepared (between a little and very well prepared) with BLS practices. This value is lower than that measured in D3, in which 77.1% of students were found to be relatively prepared in theoretical concepts. But if we consider the effective conceptual preparation, we see that the students' self-perception, in the practical domain, is 31.1 percentage points behind the revealed in the knowledge test.
A comparison between the self-perception of good achievements reveals that the perceptions of theoretical and practical learning are always below the revealed theoretical knowledge. There is no pattern of correspondence between a greater mastery of a subject and a greater perception of theoretical/practical preparation. Thus, for example, while theme 5 reveals the highest value of theoretical knowledge revealed (76.6%), it is in theme 11 that perceptions about theoretical and practical training are highest (60.0% and 58.7%, respectively). In fact, as seen above, the difference between theoretical preparation and its perception is, on average, 25.4%.
To summarize this section, students were asked to rate their perceptions of the practical training received on BLS by placing them on a 10-point interval scale (where 1 corresponds to "very poor" and 10 corresponds to "excellent"). The results are shown in the graph in Figure 4.
The mean value was 6.23, the median 6.00 and the mode 7, with SD = 2.048. The results are distributed by both genders in Figure 5. Men were found to have a perception of better practical training than women, with a difference of 0.57 percentage points, with statistical significance (p ≤ .001).
3.5. Perceptions on skills acquisition
The analysis of the information reveals that 17.8% of the respondents consider that they have not acquired sufficient skills to intervene in OHCA. However, if we consider, as a whole, the students who perceive themselves to be poorly prepared, we obtain a majority group of 56.8%. In other words, only 42.8% consider that they have acquired sufficient skills to be prepared; and of these, a small fraction see themselves as very well prepared (7.9%). This is a self-perceived reality that falls far short of what is desired with the introduction of BLS teaching in the 9th grade of basic education, as will be discussed below.
Let us look at the case in some more detail. The highest competence is at the level of ensuring the safety of the rescuer and the patient, still not exceeding 58.2%. Next is the LSP practice (57.6). Among the 22 training areas, 59.0% assume values lower than 50.0%, i.e., they do not reflect the students' ability to intervene. The worst situation concerns the lack of skills regarding the paediatric BLS. Not being prepared to perform artificial ventilation in an infant has the highest value (q110 - 77.0%) among respondents, followed by chest compressions (q 109 - 73.6% in infants and q106 - 72.6% in children) and helping airway obstruction (q112 - 72.6%).
In summary, it seems clear that about ¾ of the students have not been taught paediatric BLS manoeuvres and do not feel competent about this algorithm (q106 - 72.6%). The average dispersion of the answers has the value of .830, with maximum expression in the competences on chest compression in infants (q109 - .862) and minimum in the competences on the assessment of the response of the adult patient (q93 - .799).
Let us now compare the perceptions of the practical training received and the skills acquired, including the assurance of safety conditions (q59 and q92). This is where some dissonance arises in the answers given by the respondents: their perceptions of the practical training received (37.4%) are lower than the perceptions of the skills acquired (40.3%). In other words, they perceive practical training to be weaker than the skills they self-perceive. It should be noted, however, that both values are below the mid-point line, which is an indicator of the tenuous preparation received and the self-perceived developed skills. The results associated to the variable "gender" reveal that the students who answered the questionnaire feel better prepared (5.1%) than the girls. Girls outperform males by 1.6 percentage points in the absence of preparation (p ≤ .001).
As a summary of this section, students were asked to rate their acquired BLS skills, positioning themselves on a 10-point interval scale (where value 1 corresponds to "very poor" and value 10 translates as "excellent") (Figure 6).
The mean and median values found are 6.00, with a mode of 7 and SD = 2.068, values in line with those found for perceptions of the practical training received. The graph in Figure 7 distributes the results between the two genders. It can be seen that males perceived better skills than females, with a difference of .57 percentage points, with statistical significance. This self-reported result associates with others found [33], which expose the greater confidence in BLS proficiency by male students.
3.6. Community intervention
Students were asked to name one constraint that prevented them from intervening in the community in a real emergency. Most consider that the greatest risk would be the possibility of the patient having a contagious disease (27.5%), followed by the presence of an apparent traumatic accident, with other injuries (24.3%). The fact that the victim is a relative does not prevent that it was the choice of only 8.8% of the respondents. Some of these barriers coincide with others already identified [31], such as the particular cases of the victim being a family member.
Finally, they were asked to assess their motivation to intervene (MtI) in BLS by positioning themselves on a 10-point interval scale (where 1 corresponds to "very weakly motivated" and 10 corresponds to "highly motivated"). The mean was 6.71, the median 7.00 and the mode 8, with SD = 2.217. We see that males have a higher MtI than females, a difference of .1 percentage point, which is not significant (p = .59). This result opposes another [30], which reveals a higher motivation to respond to OHCA by female schoolchildren.
In a more detailed analysis, relationships between variables were sought by testing the heterogeneity of two ordinal samples. The results are presented in Table 2.
From Table 2, significant associations can be identified between:
- 1)
- The motivation to intervene and perceptions about the practical training received and the acquisition of skills;
- 2)
- The perceptions about the acquisition of skills and the perceptions about the theoretical and practical training received and the theoretical knowledge
In order to determine the variables under study that are predictors of MtI in the BLS community, a logistic regression model was used. Table 3 presents the results inherent to MtI.
The estimated equation, based on the logistic regression model (Table 4), is given by:
MtI = 6.001 + 0.201PPT + 0.106 PTT – 0.038TK + 0.140PSA
It is difficult to determine the relative importance of each independent variable based on the partial regression coefficients [32]. In this sense, it is preferable to examine the standardized coefficients ßeta. These allow comparisons to be made of the relative contribution of each independent variable in predicting the dependent variable. Thus, analysing the standardized ßeta coefficients, it can be seen that MtI in BLS would vary in direct proportion to perceptions of the practical training received - PPT (ß = .021; p = .005) and, likewise, in direct proportion to perceptions of the skills acquisition – PSA (ß = .140; p = .022) e in the inverse ratio of theoretical knowledge (TK). The effects of the variable "perceptions on theoretical training received" (PTT) were not significant.
This finding allows us to conclude that the greater the perception of the practical training received and the acquisition of BLS skills, regardless of theoretical knowledge, the greater is the MtI in the community in case of emergency. It should be noted that, overall, the regression model is statistically significant (p = .04). These results are in line with those of other authors [10,14,15,33,34,35,36].
3. Conclusions
The introduction of BLS in basic education was made with the assumption of the technical training of young people to intervene in the much-desired proactive citizenship. Without this training, the CoS and, consequently, the survival of people suffering from OHCA is compromised [12]. The results of this study reveal that students have weaknesses in theoretical and practical knowledge, in procedures and in procedural sequences necessary for the effectiveness of first aid interventions, with the same perception about the theoretical and practical training received, with a minority considering that they have acquired sufficient skills in BLS.
It can thus be inferred that the teaching and learning of BLS in schools, in Portugal, is far from what is defined in the Essential Learning for 9th grade, in the subject of Natural Sciences [23]. There are weaknesses in the recognition of episodes requiring urgent intervention, which agrees with another study [39].
The need to train people who are not health and emergency services professionals, but who are trained and feel safe to act is advocated, which agrees with Monsieurs et al. [2], and that this training occurs transversally, from the initial levels of schooling to higher education, as advocated by Greif et al. [15].
The lack of knowledge of contents and sequential procedures for intervention in OHCA compromises a rapid, safe and effective action, which is aimed at the end of the 3rd cycle of basic education.
The evidence collected allows us to conclude that students do not feel and are not empowered to intervene in an OHCA episode. Increased perception that the practical training received and the acquisition of BLS skills generates greater MtI in the community. It should be noted, however, that the greater the perception of the practical training received and the acquisition of BLS skills, regardless of theoretical knowledge, the greater the MBI in the community in case of emergency [10,14,15].
The students surveyed are motivated towards the topic of BLS, but lack the empowerment, which builds confidence to intervene, which tends to meet with the findings of McCarthy et al. [14] who state that increasing the motivation of non-professionals to perform BLS will tend to have a direct impact on OHCA survival rates. In the present study, students recognized the importance of BLS practiced bystanders in improving the survival rate in OHCA, which is in line with what has been advocated by authors [3,4,5,6,7,8,9,10,11].
The representativeness of the study allows for the generalisation and extrapolation of the results. Therefore, this study will enable the dissemination of recommendations, based on the results and conclusions found, to support decision-makers in the optimisation of BLS training in the discipline of Natural Sciences.
In the education of basic school students, in Portugal, it will be important to establish a level of regular training and education with a view to the global implementation of rescue in a proactive citizenship, ensuring the effective achievement of the first two links of the CoS and the multiplying effect of these skills among family members, friends and the community. Saving lives is within everyone's reach.
To this end it is argued that:
- a)
- Early training of students in BLS, with recognised quality standards, during mandatory schooling, accompanied by regular training;
- b)
- Teaching BLS-AED in initial and continuing teacher education;
- c)
- The commemoration of events related to the theme: e.g., European 112 Day (February 11), World First Aid Day (September second Saturday in World Heart Day (September 29); European Day of the Restart of the Heart (October 16);
- d)
- The creation of a school first aid culture, translated into altruistic gestures of citizenship that promote the health and well-being of the community.
The declaration of a pandemic by the new SAR-Cov-2 on 11 March 2020 was a constraint to this study. Portugal's government closed the schools on 16 March 2020 and moved ahead with distance learning (art. 9.º, No. 3.º of Decree-Law No. 10-A/2020, of March 13). Successive reassessments of the situation led to the maintenance of the closure of the schools, until the end of the 2019/2020 school year. This constraint had consequences for the process of information collection. On the one hand, we were unable to apply any questionnaire in paper format, for health safety reasons and, mainly, because the students were, since March 16, 2020, in their residences. On the other hand, the tense social atmosphere of concern was not conducive to arousing interest and altruism on the part of the leaders in responding to enquiries.
In view of the study carried out, which underlines the importance of the subject and the lack of success in the training of students in the 10th grade of schooling, guidelines are put forward for future research to continue the work we have undertaken, in particular:
- -
- Observational studies, using direct observation techniques, in school groups, with a view to gaining in-depth knowledge of the contexts and building evidence to support successful practices in the teaching and learning of BLS;
- -
- Descriptives studies that allow us to know the teachers' training for teaching and intervention in BLS and
- -
- Studies to make it possible to know the reality of initial teacher training in higher education in relation to the teaching of BLS;
- -
- Action-research with the various actors of school communities that contribute to knowing and intervening uniquely, in an adapted and dialogical manner, with a view to optimising results;
- -
- Studies to find out how the topic is dealt with in the pupils' textbooks;
- -
- Longitudinal studies, both locally and nationally, with the aim of knowing and analysing the evolution of pedagogical practices and the gains in skills and motivation for the performance of students in emergency situations in BLS;
- -
- Similar studies to what is presented in this article, referring to the subject of Physical Education, in the 10th grade of schooling and in higher education.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
The following statements should be used “Conceptualization and methodology, Jorge Bonito; validation and formal analysis, Maria João Loureiro; investigation, Maria Boné; writing—original draft preparation, Jorge Bonito and Maria Boné; supervision, Jorge Bonito and Maria João Loureiro.
Funding
This work is financially supported by National Funds through FCT – Foundation for Science and Technology, I.P., under the projects UIDB/00194/2020 and UIDB/04312/2020.
Institutional Review Board Statement
The questionnaire was submitted to the platform for Monitoring School Surveys of the Ministry of Education (authorization No. 0732600001) and approved by the Directorate-General of Education for application in school groupings.
Informed Consent Statement
No informed consent statement was issued for education guardian. The questionnaire was to be completed in the household of each family and a decision on response / non-response would be made there. The anonymity of respondents was ensured.
Data Availability Statement
Not applicable here.
Acknowledgments
The authors of this paper would like to express their gratitude to the directors of the school clusters where this research was carried out, for their collaboration and welcome; to the students who participated in this study, for their availability.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A
Questionnaire
References
- AHA. Cardiac arrest. Causes of cardiac arrest 2020. Available online: https://www.heart.org/en/health-topics/cardiac-arrest/causes-of-cardiac-arrest (accessed on Sep 22, 2022).
- Monsieurs, K. G. et al. European Resuscitation Council guidelines for resuscitation. Resuscitation 2015, 95, 1-80. [CrossRef]
- Geri, G. et al. Effects of bystander CPR following out-of-hospital cardiac arrest on hospital costs and long-term survival. Resuscitation 2017, 115, 129-134. [CrossRef]
- Hinchey, P. R. et al. Improved out-of-hospital cardiac arrest survival after the sequential implementation of 2005 AHA guidelines for compressions, ventilations, and induced hypothermia: the Wake County experience. Ann Emer Med 2010, 56(4), 348-357. [CrossRef]
- Kragholm, K. et al. Bystander efforts and 1-year outcomes in out-of-hospital cardiac arrest. N Eng J Med 2017, 376, 1737-1747. [CrossRef]
- Panchal, A. R. et al. Chest compression-only cardiopulmonary resuscitation performed by lay rescuers for adult out-of-hospital cardiac arrest due to non-cardiac aetiologies. Resuscitation 2013, 84, 435-439. [CrossRef]
- Riddersholm, S. et al. Association of bystander interventions and hospital length of stay and admission to intensive care unit in out-of-hospital cardiac arrest survivors. Resuscitation 2017, 119, 99-106. [CrossRef]
- Semeraro, F. et al. Kids save lives implementation in Europe: A survey through the ERC research NET. Resuscitation 2016, 107, e7-e9. [CrossRef]
- Tanaka, H. et al. Modifiable factors associated with survival after out-of-hospital cardiac arrest in the pan-Asian resuscitation outcomes study. Ann Emerg Med 2018, 71(5), 608-617.e15. https://doi.org 10.1016/j.annemergmed.2017.07.484.
- Trevisanuto, D. et al. Supreme laryngeal mask airway versus face mask during neonatal resuscitation: A randomized controlled trial. J Paediatr 2015, 167(2), 286-291. [CrossRef]
- Yan, S. et al. The global survival rate among adult out-of-hospital cardiac arrest patients who received cardiopulmonary resuscitation: a systematic review and meta-analysis. Critical Care 2020, 24(61). [CrossRef]
- Cummins, R. O. et al. Improving survival from sudden cardiac arrest: the “chain of survival” concept. A statement for health professionals from the advanced cardiac life support subcommittee and the emergency cardiac care committee. American Heart Association. Circulation 1991, 83, 1832-1847. [CrossRef]
- AHA. Highlights of the 2020 AHA Guidelines Update for CPR and ECC, 2020. Available online: https://cpr.heart.org/en/resuscitation-science/cpr-and-ecc-guidelines (accessed on Sep 22, 2022).
- McCarthy, J. J. et al. Out-of-hospital cardiac arrest resuscitation systems of care: A scientific statement from the American Heart Association. Circulation 2018, 137(21), e645-e660. [CrossRef]
- Greif, R. et al. European Resuscitation Council guidelines 2021: Education for resuscitation. Resuscitation 2021, 161. [CrossRef]
- Lanzas, D.; Nunes, P.; Perelmen, J. Training program in resuscitation maneuvers delivered by teachers in a school setting: An economic argument. Rev Port Card 2022, 4, 135-144. [CrossRef]
- Martínez-Isasi, S. et al. Learning to resuscitate at school. Study in 8-12 year-old schoolchildren. Anal Pedi 2022, 96(1), 17-24. [CrossRef]
- Pichel, M. et al. Un primer paso en la enseñanza del soporte vital básico en las escuelas: la formación de los profesores. Anal Pedi 2018, 89(5), 265-271. [CrossRef]
- Watanabe, K. et al. Efficacy and retention of basic life support education including automated external defibrillator usage during a physical education period. Prev Med Rep 2017, 5, 263-267. [CrossRef]
- Gonçalves, C. et al. Peer-training model in basic life support in high education health students. Resuscitation 2015, 96(1), 61. [CrossRef]
- DGE. Aprendizagens essenciais. 9.º ano. 3.º ciclo do ensino básico. Ciências naturais, 2018a. Available online: http://www.dge.mec.pt/sites/default/files/Curriculo/Aprendizagens_Essenciais/3_ciclo/ciencias_naturais_3c_9a_ff.pdf (accessed on Sep 22, 2022).
- DGE. Aprendizagens essenciais. 10.º ano. Ensino secundário. Educação física, 2018b. Available online: http://www.dge.mec.pt/sites/default/files/Curriculo/Aprendizagens_Essenciais/3_ciclo/ciencias_naturais_3c_9a_ff.pdf (accessed on Sep 22, 2022).
- DGEST. Estatísticas da educação 2018/2019, 2020. Available online: https://www.dgeec.mec.pt/np4/17/ (accessed on Sep 22, 2022).
- Moreira, J. M. Questionários: Teoria e prática. Almedina, Coimbra, Portugal, 2009.
- Boné, M.; Loureiro, M. J.; Bonito, J. Perceções de alunos sobre a aprendizagem do suporte básico de vida no 9.º ano de escolaridade: do questionário. In IV Encontro Nacional de Jovens Investigadores em Educação: Livro de atas, Sebastião, A., Rebelo, H., Eds.; Centro de Investigação em Educação e Psicologia da Universidade de Évora, Évora, Portugal, 2020, pp. 57-66. https://dspace.uevora.pt/rdpc/handle/10174/30562.
- AHA. Part 12: From science to survival. Circulation 2000 102, I-358-I-370. https://www.ahajournals.org/doi/10.1161/circ.102.suppl_1.I-358.
- INEM. Manual de suporte básico de vida – adulto. Instituto Nacional de Emergência Médica, Lisboa, Portugal, 2017a. https://www.inem.pt/wp-content/uploads/2017/09/Suporte-B%C3%A1sico-de-Vida-Adulto.pdf.
- INEM. Manual de suporte básico de vida – pediátrico. Instituto Nacional de Emergência Médica, Lisboa, Portugal, 2017b. https://www.inem.pt/wp-content/uploads/2017/09/Suporte-B%C3%A1sico-de-Vida-Pedi%C3%A1trico.pdf.
- Plant, N.; Taylor, K. How best to teach CPR to schoolchildren: A systematic review. Resuscitation 2013, 84(4), 415-421. [CrossRef]
- Finke, S. R. at al. Gender aspects in cardiopulmonary resuscitation by schoolchildren: A systematic review. Resuscitation 2018, 125, 70-78. [CrossRef]
- Kanstad, S.; Nilsen, K.; & Fredriksen, K. CPR knowledge and attitude to performing bystander CPR among secondary school students in Norway. Resuscitation 2011, 82(8), 1053-1059. https://www.ncbi.nlm.nih.gov/pubmed/21531067.
- Pestana, M. H.; Gageiro, J. N. Análise de dados para as ciências sociais. A complementaridade do SPSS (6.ª ed.). Edições Sílabo, Lisboa, Portugal, 2014.
- Martins, M. (2014). Revisão bibliográfica. Outcome da paragem cardíaca, intra e extra hospitalar (Master’s thesis, Universidade do Porto). Universidade do Porto, Porto, Portugal, 2014. https://repositorio-aberto.up.pt/bitstream/10216/76589/2/32690.pdf.
- Nielsen, A. M.; Isbye, D. L.; Lippert, F. K.; Rasmussen, L. S. Can mass education and a television campaign change the attitudes towards cardiopulmonary resuscitation in a rural community? Scand J Trau, Resus Emer Med 2013, 21, 21-39. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3666962/.
- Saraç, L.; Ok, A. The effects of different instructional methods on students' acquisition and retention of cardiopulmonary resuscitation skills. Resuscitation 2010, 81(5), 555-561. https://pubmed.ncbi.nlm.nih.gov/20149946/.
- Olasveengen, T. M. et al. European Resuscitation Council guidelines 2021: Basic life support, 2021. https://www.cprguidelines.eu/.
Figure 1.
Relative frequencies, expressed in percentage of the indicators of BLS knowledge. 1 - CoS / survival rate in OHCA; 2 – Physical examination; 2.1 - Safety assessment; 2.2 – Response assessment; 2.3 - Airway permeabilization; 2.4 - Breathing assessment; 2.5 – Circulation assessment; 2.6 - LPS; 3 - Emergency procedures; 4 - BLS adult algorithm; 5 - BLS paediatric algorithm; 6 – Airway obstruction.
Figure 1.
Relative frequencies, expressed in percentage of the indicators of BLS knowledge. 1 - CoS / survival rate in OHCA; 2 – Physical examination; 2.1 - Safety assessment; 2.2 – Response assessment; 2.3 - Airway permeabilization; 2.4 - Breathing assessment; 2.5 – Circulation assessment; 2.6 - LPS; 3 - Emergency procedures; 4 - BLS adult algorithm; 5 - BLS paediatric algorithm; 6 – Airway obstruction.

Figure 2.
Self-evaluation of the theoretical training received on BLS. N = 1215.
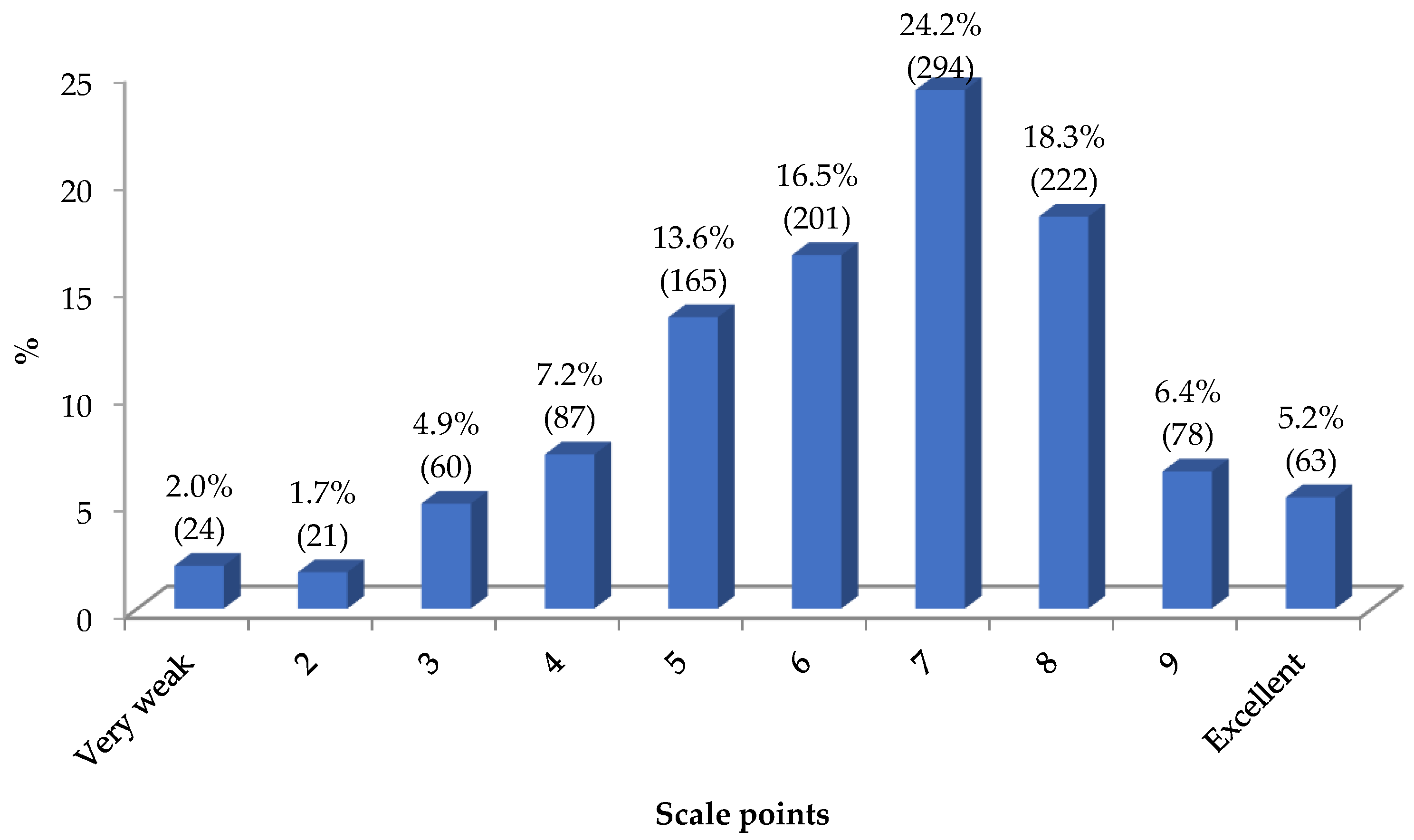
Figure 3.
Self-evaluation of the theoretical training received in BLS according to the variable "gender". N = 1215.
Figure 3.
Self-evaluation of the theoretical training received in BLS according to the variable "gender". N = 1215.
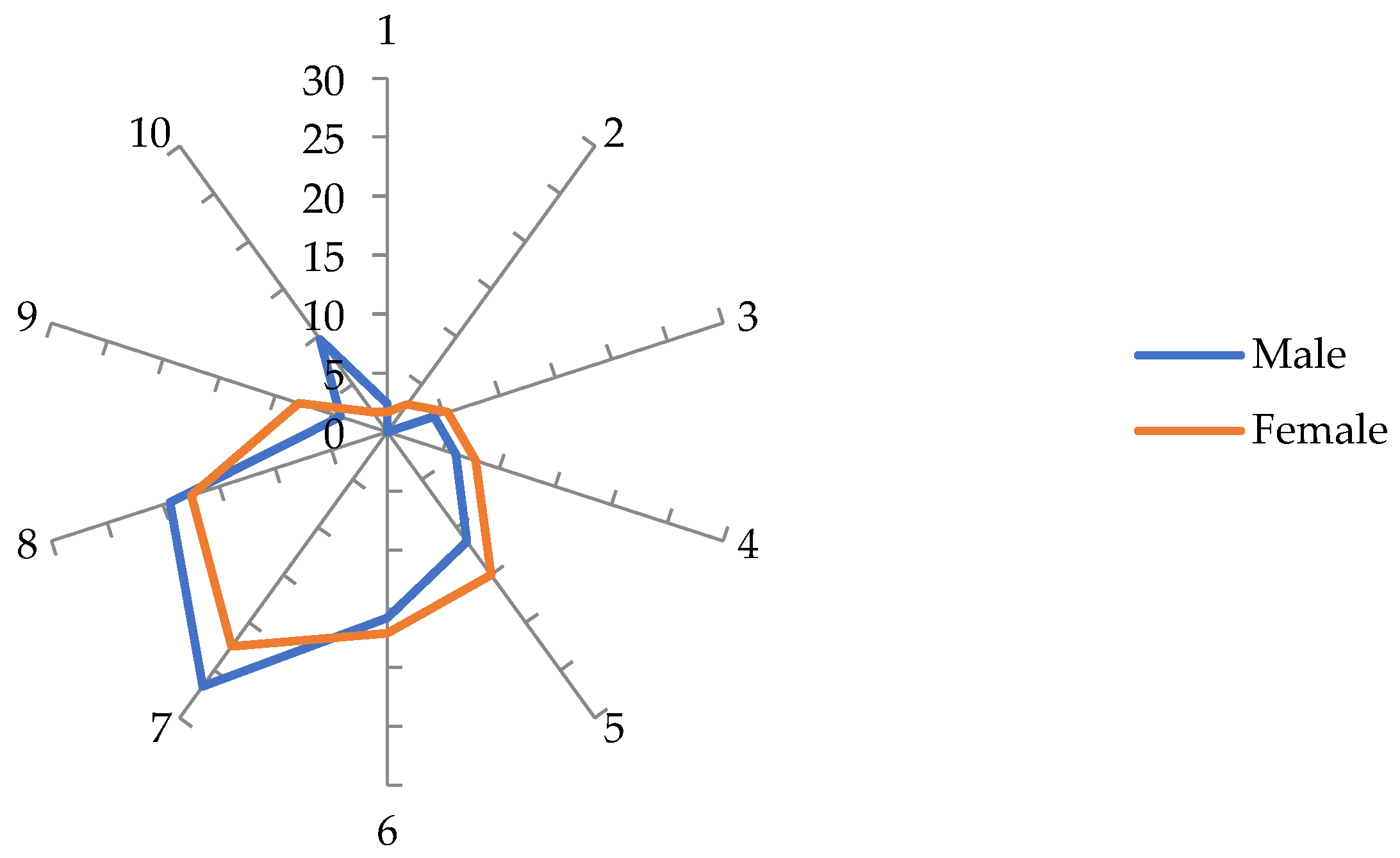
Figure 4.
Self-evaluation of practical training received in BLS. N = 1215.
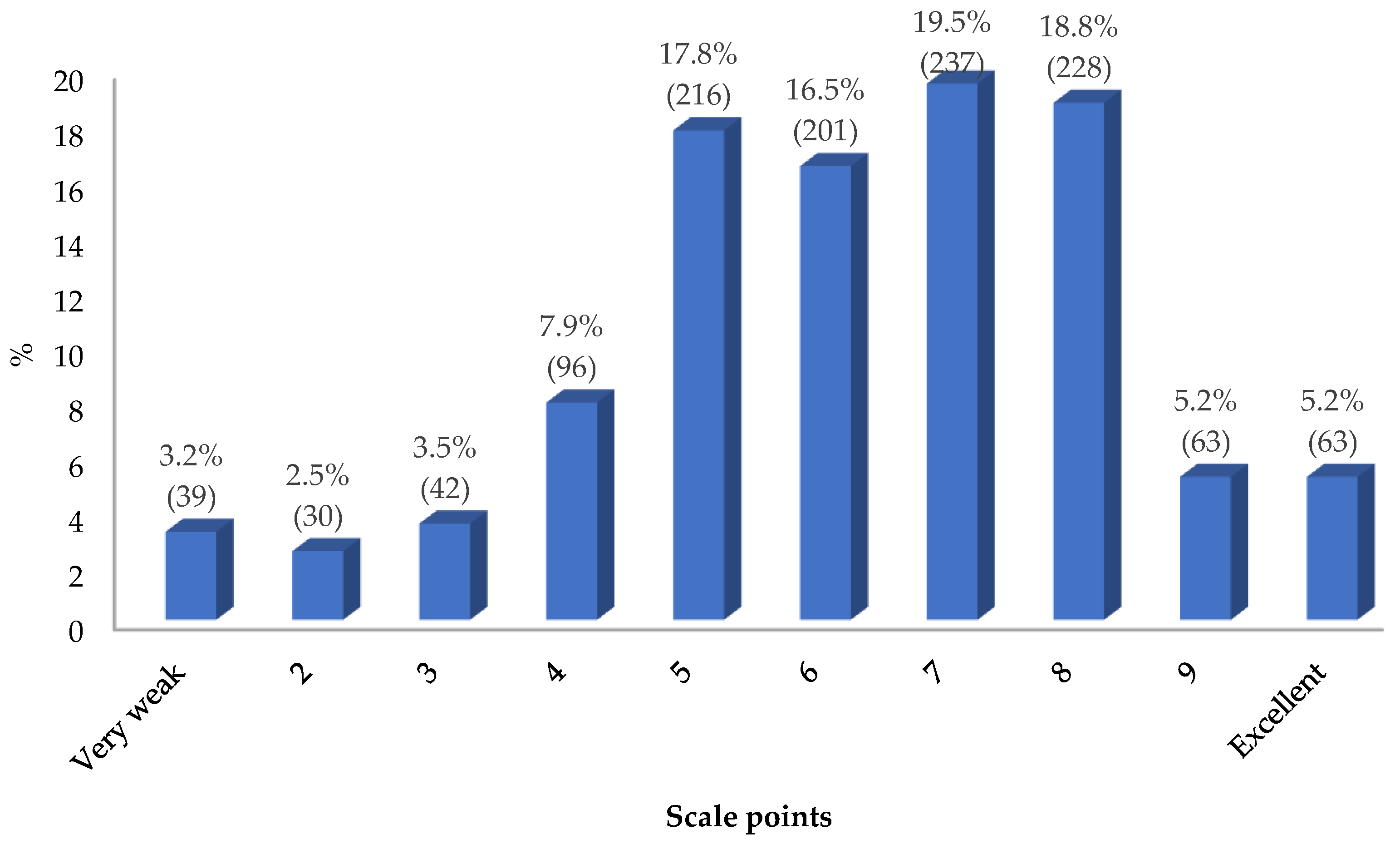
Figure 5.
Self-evaluation of practical training received in BLS according to the variable "gender". N = 1215.
Figure 5.
Self-evaluation of practical training received in BLS according to the variable "gender". N = 1215.
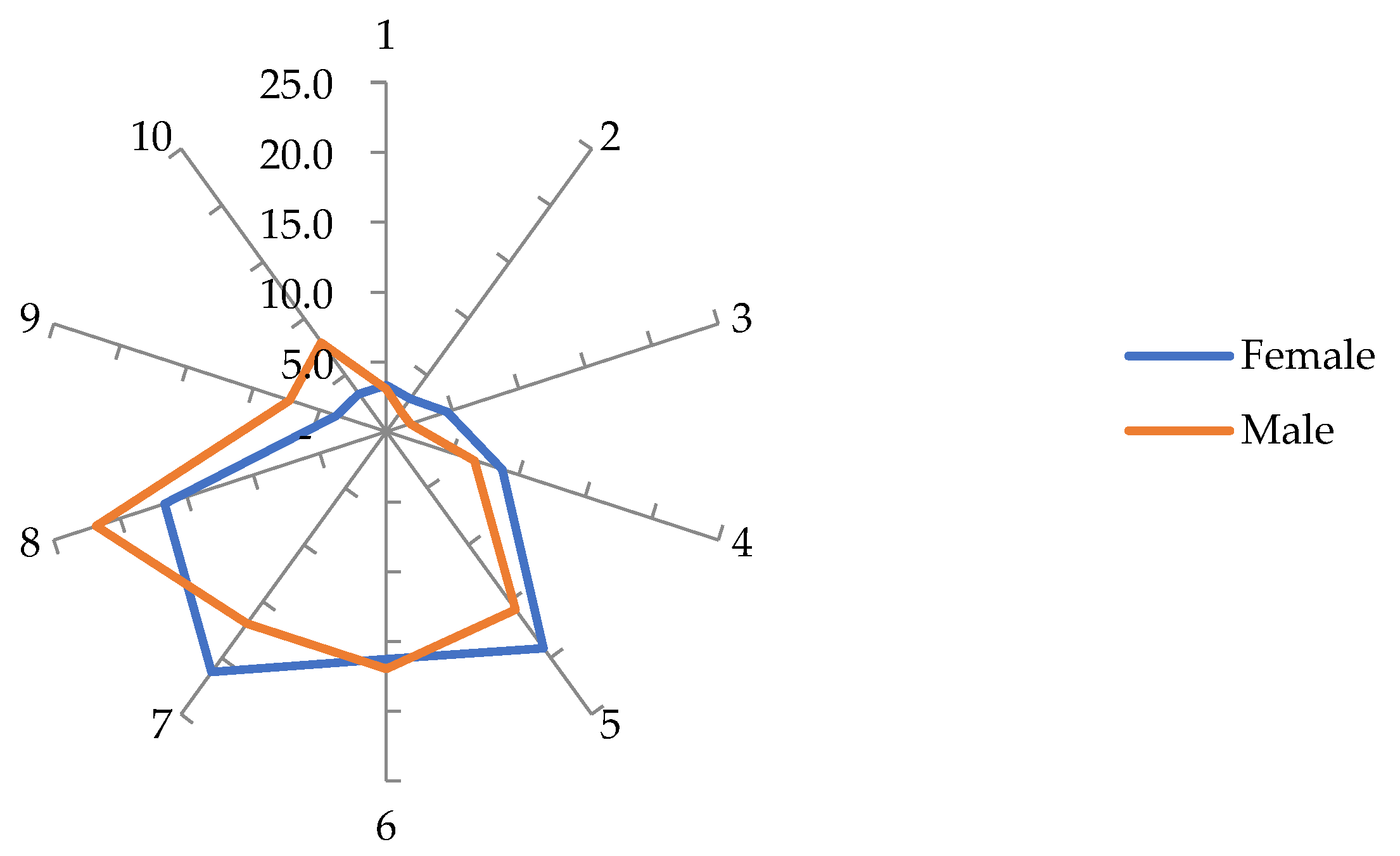
Figure 6.
Self-assessment of the skills acquired in BLS. N = 1215.
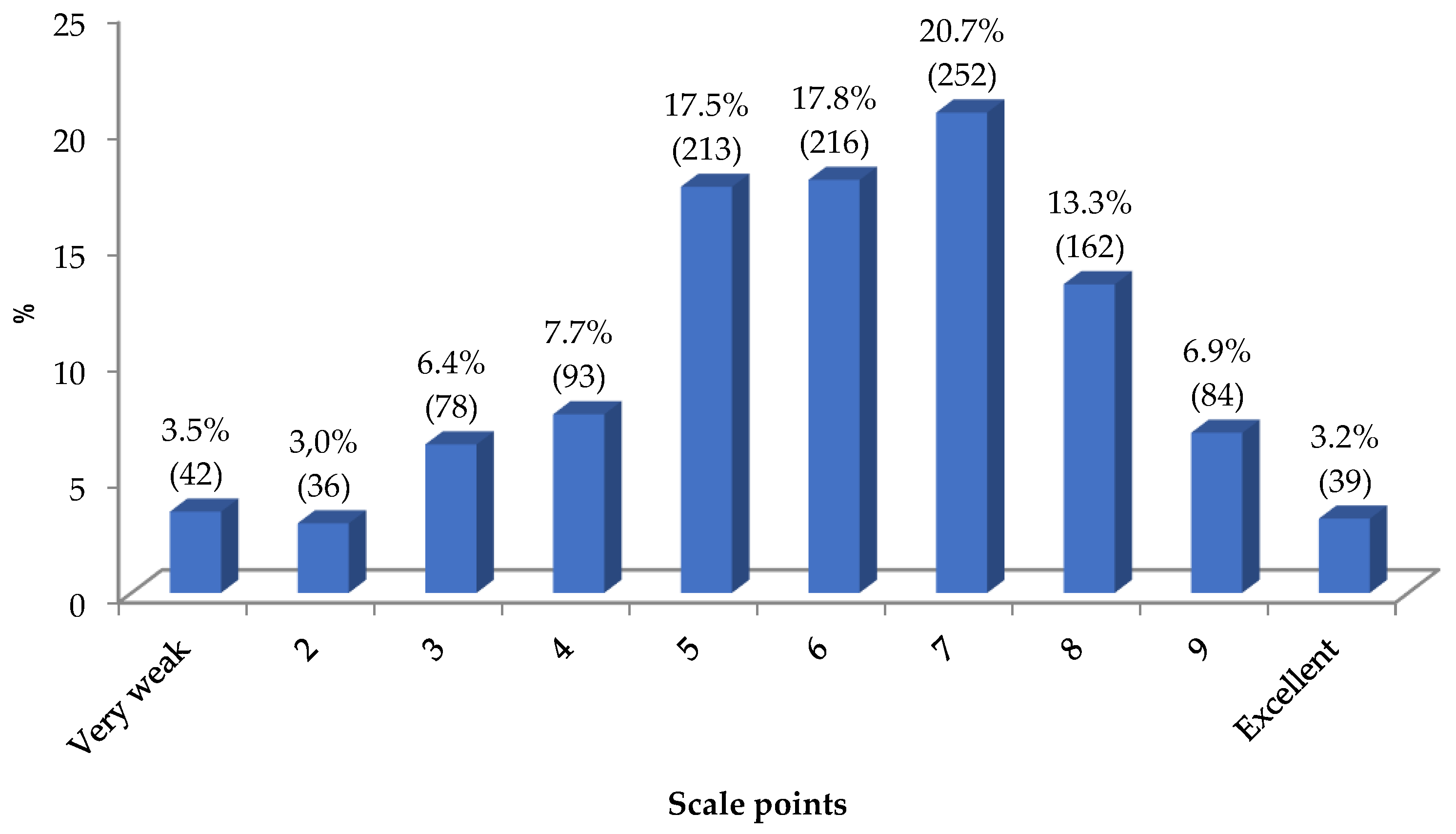
Figure 7.
Self-evaluation of practical training received in BLS according to the variable "gender”. N = 1215.
Figure 7.
Self-evaluation of practical training received in BLS according to the variable "gender”. N = 1215.
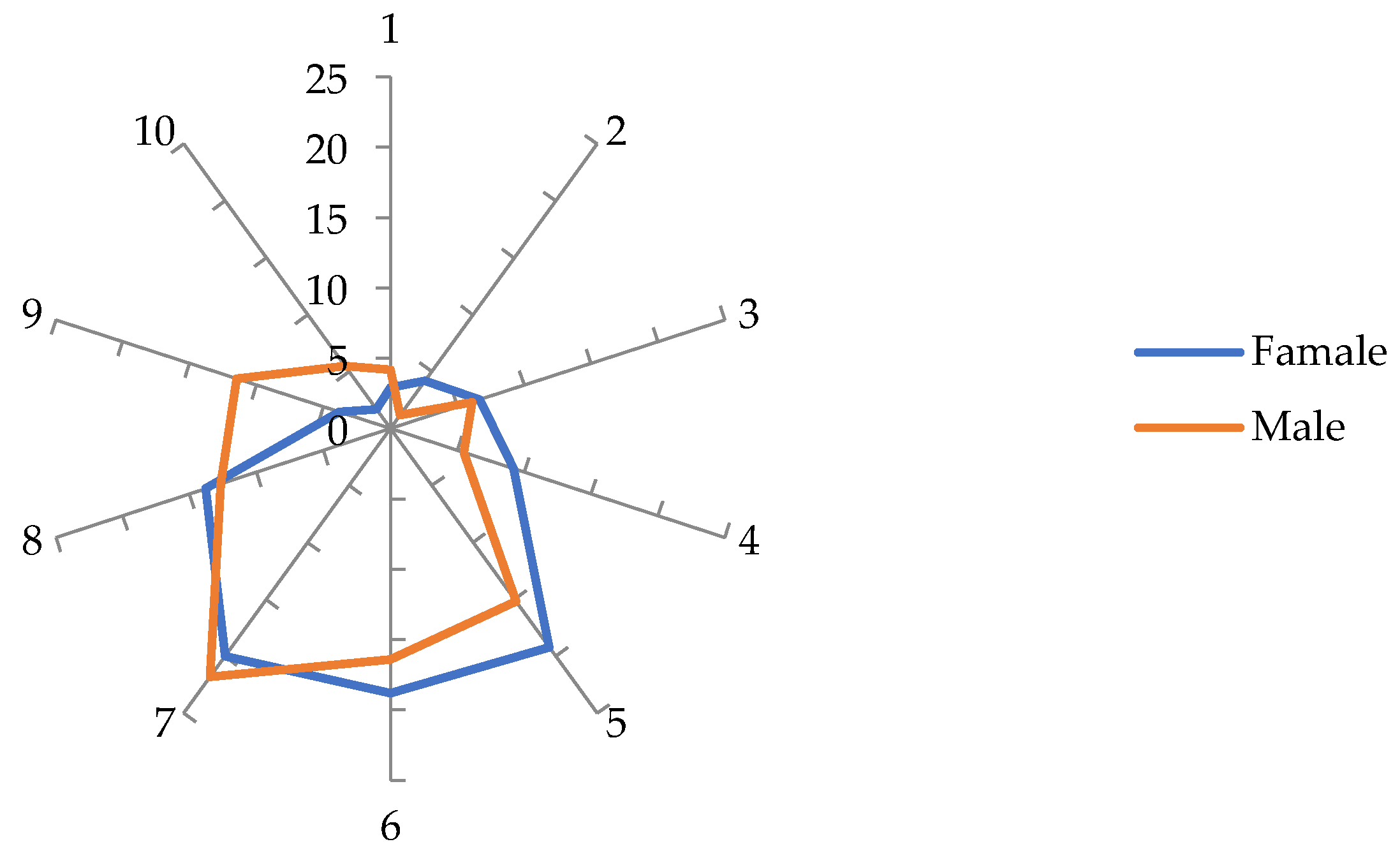

Table 1.
Indicators and respective items of dimension 2.
| Indicators * | Formulation | Items | No. of items |
|---|---|---|---|
| 1. CoS and survival rate in OHCA | True | 2, 3, 4 | 3 |
| False | 1, 5 | 3 | |
| 2. Examination of the adult and paediatric patient based on the initial approach to ABC | |||
| 2.1. Assessment of security conditions | True | 6, 8, 10 | 3 |
| False | 7, 9 | 2 | |
| 2.2. Assessment of the patient's response | True | 12, 14 | 2 |
| False | 11, 13, 15 | 3 | |
| 2.3. Airway permeability | True | 17, 18, 20 | 3 |
| False | 16, 19 | 2 | |
| 2.4. Respiration checks | True | 21, 23, 25, 26 | 4 |
| False | 22, 24 | 2 | |
| 2.5. Circulation checks | True | 27, 28, 29, 30 | 4 |
| False | - | 0 | |
| 2.6. Lateral safety position | True | 32, 33, 34, 35 | 4 |
| False | 31 | 1 | |
| 3. Emergency alarm procedures | True | 38, 39, 40 | 3 |
| False | 36, 37 | 2 | |
| 4. Adult BLS procedures | True | 41, 42, 44, 45 | 4 |
| False | 43, 46 | 2 | |
| 5. Paediatric BLS procedures | True | 47, 48, 50, 51, 52 | 5 |
| False | 49 | 1 | |
| 6. Airway obstructions | True | 55, 56, 57 | 3 |
| False | 53, 54 | 2 |
* Self elaboration.
Table 2.
Association between variables of dimensions 2-5 and q130 (MtI).
| Variables | Perceptions about the acquisition of skills | Perceptions about practical training | Theoretical knowledge | Perceptions about theoretical training | MtI |
|---|---|---|---|---|---|
| Perceptions on skills acquisition | - | <.001 *** | <.001 *** | <.001 *** | .028 * |
| Perceptions on practical training | <.001 *** | - | <.001 *** | <.001 *** | .030 ** |
| Theoretical knowledge | <.001 *** | <.001 *** | - | <.001 *** | .526 |
| Perceptions on theoretical training | <.001 *** | <.001 *** | <.001 *** | - | .721 |
| Motivation to intervene (> 5; ≤ 5) | .028 * | .030 ** | .526 | .721 | - |
Note. Data. * p < .05 (significant correlation). ** p < .01 (highly significant correlation), *** p < .001 (highly significant correlation). Spearman's correlation test. Own elaboration.
Table 3.
ANOVAa for the MtI variable.
| Model | Sum of Squares | df | Mean Square | F | Sig. |
|---|---|---|---|---|---|
| Regression | 76.368 | 4 | 19.092 | 3.920 | .004b |
| Residual | 5892.492 | 1210 | 4.870 | ||
| Total | 5968.859 | 1214 |
Note. Data. a. Dependent Variable: q130. Model: (Intercept), Perceptions on practical training, Perceptions on theoretical training, Theoretical knowledge, Perceptions on Skills Acquisition. Own elaboration.
Table 4.
Logistic regression model for the MtI variable.
| Parametrs | Unstandardized Coefficients | Standardized Coefficients | t | Sig. | |
| B | Std. Error | Beta | |||
| Intercept | 6.001 | .809 | 7.422 | <.001 *** | |
| Perceptions on practical training (PPT) | .201 | .070 | .113 | 2.845 | .005 ** |
| Perceptions on theoretical training (PTT) | .106 | .080 | .049 | 1.329 | .184 |
| Theoretical knowledge (TK) | -.038 | .016 | -.132 | -2.360 | .018 * |
| Perceptions on skills acquisition (PSA) | .140 | .061 | .092 | 2.292 | .022 * |
Note. Data. Dependent variable: MtI. Model: (Intercept), PPT, PTT, TK, PSA. * p < .05 (significant correlation). ** p < .01 (highly significant correlation), *** p < .001 (highly significant correlation). Own elaboration.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



