
Submitted:
17 March 2023
Posted:
22 March 2023
You are already at the latest version
Abstract
Maximal heart rate (HRmax) is a widely used measure of cardiorespiratory fitness. Prediction of HRmax is an alternative to cardiopulmonary exercise testing (CPET), but its accuracy among endurance athletes (EA) requires evaluation. This study aimed to externally validate HRmax prediction models in the EA independently for running and cycling CPET. 4043 runners (age=33.58 (8.12) years; 83.53% males; BMI=23.66 (2.54) kg·m−2) and 1026 cyclists (age=36.88 (9.03) years; 89.67% males; BMI=24.04 (2.65) kg·m−2) underwent maximum CPET. Student t-test, mean absolute percentage error (MAPE), mean absolute error (MAE), and root mean square error (RMSE) were applied to externally validate 8 running and 5 cycling HRmax equations. HRmax was 184.60 (9.79) beats·min−1 and 182.66 (10.28) beats·min−1 respectively for running and cycling, p=0.001. Measured and predicted HRmax differed significantly (p=0.001) for 9 of 13 (69.23%) models. HRmax was overestimated by 8 (61.54%) and underestimated by 5 (38.46%) formulae. Overestimated HRmax ranged 0.08-4.94 beats·min−1 and underestimated HRmax ranged 0.03-4.90 beats·min−1. MAE and RMSE were 0.18-4.94 beats·min−1 and 9.13-10.47, respectively. MAPE ranged 3.95-4.69%. Prediction models do not allow for accurate estimation of HRmax. HRmax was more often underestimated than overestimated. Predicted HRmax can be implemented for EA as a supplemental method but CPET is the preferable approach.
Keywords:
maximal heart rate
; endurance athletes
; cardiopulmonary exercise test
; HRmax
; cardiac rehabilitation
; running
; cycling
1. Introduction
Maximal heart rate (HRmax) is a widely used variable to recommend training intensity by exercise practitioners [1] and prescribe treatment by medical professionals [2]. HRmax usually means the highest heart rate (HR) achieved during maximum symptom-limited cardiopulmonary exercise test (CPET) [3]. Verification of achieving HRmax can be carried out based on volitional CPET termination or by HR plateau (lack of growth in the HR with increasing intensity) [4,5]. Currently performed CPET often leads to nondiagnostic results because participants terminate them at the submaximal intensity (without signs of ischemia or <85% of HRmax) based only on prespecified HRmax calculated from various prediction models. The clinical value of such CPET is sub-optimal and this was confirmed by ECG and imaging data [4,5].
HRmax shows significant variability [1,6]. Measuring the HR during exercises, and calculating its proportion to HRmax, resting HR, or relative workload (% of HRmax) is a common practice and has been implemented in many wearable devices [6]. Results help to optimize exercise intensity for both healthy endurance athletes (EA) and rehabilitating patients. It has been confirmed that people with better fitness level, in particular EA, are able to achieve higher HRmax and maintain slower declines in HRmax with ageing [6,7]. They also have lower all-cause mortality, especially due to CVD [6].
CPET results differ significantly between treadmill and cycle modality[8]. The differences apply not only to HRmax but also to other performance indicators[9,10]. Usually, higher scores are observed in running CPET[9]. Cycling CPET has a lower occurrence of attributes because it is performed in a more stable position[8]. In consequence, cycling test is more recommended when higher measurement accuracy is required (e.g. in the clinical settings)[3].
There is a demand for individualized, risk-based, stratified therapy and exercise programs. It points out that medical decisions, intensity prescriptions, and diagnostic examinations are precisely tailored to the individual [11,12]. Knowledge of the endurance capacity remains therefore essential. Prediction models are usually developed to share decision-making [11]. Numerous regression equations were derived to obtain the HRmax setpoint without maximal CPET [13]. However, their accuracy is often questioned and there is a lack of large studies comparing different prediction models among EA and stratifying them between CPET modalities. Recently, endurance sports are gaining popularity, hence the number of EAs with suspected CVD and veteran EAs, for whom the exact value of HRmax is particularly important, increased.
The majority of prediction models include a baseline value (around 200-220) and different age covariates [14]. Their authors postulate that such a univariate analysis with the inclusion of only one key factor is sufficient and other variables remain negligible [2]. Indirect estimation of HRmax has found wide application in fitness equipment and is a common method for preparing medical recommendations (e.g. for treatment of heart failure) [1,15].
The aims of this study are: (1) to assess the accuracy of HRmax prediction models in the population of EA independently for running and cycling CPET, (2) to evaluate their practical application based on the precision of estimations, and (3) to provide further research recommendations to improve the accuracy of novel prediction models. According to our knowledge, this is the first external validation of HRmax prediction models stratified between CPET type that includes up to 13 formulae and has been performed on such a large EAs population.
2. Materials and Methods
2.1. Study setting
This is a population study on a cohort of healthy adult EA who declared regular training and a planned exercise regimen (≥3 weekly training sessions). A retrospective analysis of CPET data collected between 2013-2021 from the tertiary care sports medicine center SportsLab (www.sportslab.pl, Warsaw, Poland) was performed. All CPETs were conducted at the individual request of athletes as part of the optimization of a training program or periodic performance evaluation. Exclusion criteria were: (1) age <18 years old, (2) any medical contraindications (both acute and chronic), (3) usage of any medications at the date of study (both acutely and chronically), (4) smoking, (5) missing data in HRmax. The selection procedure is presented in Figure 1. Validation was performed following the TRIPOD guidelines (see Supplementary Material 1 S1: TRIPOD Checklist: Prediction Model Development and Validation) [16].
2.2. Previously published HRmax prediction models
Candidates of prediction models were identified from systematic reviews for normative exercise reference values by Paap et al. and Takken et al. up to 2019 [17,18]. Screening for models derived between 2019 and 2023 was conducted by a manual literature search in four electronic databases PubMed, MEDLINE, Scopus, and Web of Science using keywords: "prediction model", "prediction equation", “prediction algorithm”, “endurance athletes”, “cardiopulmonary exercise testing” and “maximal heart rate”. Inclusion criteria were: (1) usage only of somatic or exercise variables which were available in our database, (2) providing HRmax defined as the peak value (not averaged), and (3) providing data about the primarily derived population stratified by CPET modality. Exclusion criteria were: (1) being derived primarily for pediatric or geriatric populations, (2) being derived exclusively for one sex, and (3) focusing on clinical population, Additionally, Fox et al. [19] and Tanaka et al. [2] equations were added due to their wide usage. Finally, 13 different prediction models from 9 studies were qualified. Their classification is presented in the left part of Table 2. Original derivation studies are presented in Supplementary Material 3 S3: Selected prediction models for maximal heart rate.
2.3. Cardiopulmonary exercise testing procedures
All CPETs were performed in a single laboratory under unified protocols both for treadmill and cycle ergometry. EA underwent graded maximal effort CPET on either a mechanical treadmill (h/p/Cosmos quasar, Germany) or cycle ergometer (Cyclus 2, RBM elektronik-automation GmbH, Leipzig, Germany). Briefly, the testing modality was selected by the agreement of the subject and the physiologist to suit the primary training discipline.
The cycling CPET started with a 5 min free wheel pedaling as a warmup and continued with a gradual increase in resistance every 2 min until termination (20W for females and 30W for males). The running CPET begins with a 5 min walking or slow jogging warmup and continued with a gradual increase in velocity every 2 min (1 km·h-1 for both females and males). The treadmill was set at a constant inclination equal to 1%. The intensity was adjusted by the physiologist in conjunction with the trainee to reach their maximum exertion. The termination points considered as a maximal effort were: (1) volitional exhaustion and inability to continue the protocol with declared exertion ≥18 in Borg’s RPE, (2) an HR or oxygen uptake (VO2) plateau (a stable level of HR or levelling-off in VO2, defined as an increase <100 mL·min−1 with growing exercise intensity before CPET termination)[20,21,22].
Exercise indices were obtained breath-by-breath by the Hans Rudolph V2 Mask (Hans Rudolph, Inc, Shawnee, KS, USA), a gas exchange monitor Cosmed Quark CPET (Rome, Italy), and analyzed using dedicated software Omnia. HR was measured via ANT+ chest strap as a part of the Cosmed Quark CPET set (manufacturer product accuracy comparable to ECG; ± 1 beats·min−1). HRmax was defined as the peak value and was not averaged in the interval preceding CPET termination. Maximal VO2 (VO2max) was considered as the average VO2 during the 15-s period at the end of the CPET. The maximal oxygen pulse was calculated as VO2max/HRmax, maximal respiratory exchange ratio as the maximal volume of exhaled carbon dioxide/ maximal volume of oxygen uptake, and maximal minute ventilation efficiency as maximal ventilation/ maximal volume of exhaled carbon dioxide.
2.4. Data Analysis
Continuous variables are presented as mean (standard deviation; SD) and 95% confidence intervals (CI). Categorical variables are presented as numbers (percentages). Equations were tested independently for running and cycling CPET. Data distribution was assessed by the quantile-quantile plots. Differences between both disciplines (running/cycling) were calculated by Student t-test.
Predictive performance of the selected formulae was compared by the MAPE (mean absolute percentage error), MAE (mean absolute error), and RMSE (root mean square error). MAE and RMSE were additionally adjusted to the percentage of observed HRmax (by dividing the error by the mean of observed HRmax). Differences between observed and predicted HRmax were also calculated by Student t-test.
The significance agreement was adopted at two-tailed p=0.05. Statistical analyzes were performed in the SPSS program (version 29.0, IBM, Chicago, IL, USA).
3. Results
3.1. Athletes’ characteristics
The cohort consisted of 5311 EA. There were 4043 running CPET (n=3377, 83.53% males) and 1268 cycling CPET (n=1137, 89.67% males). The age of the runners was 33.58 (8.12) years and the age of the cyclists was 36.88 (9.03) years, p<0.001. Participants were suited as normal weight and the BMI of runners was 23.66 (2.54) kg·m−2 and cyclists was 24.04 (2.65) kg·m−2, p<0.001.
During the CPET, HRmax was 184.60 (9.79) beats·min−1 and 182.66 (10.28) beats·min−1 respectively for runners and cyclists., p<0.001. VO2max also differed significantly between modalities (53.24 (7.12) mL·min−1·kg−1 for runners; 51.67 (7.86) mL·min−1·kg−1 for cyclists), p<0.001. All remaining variables, except body fat percentage (p=0.09) and maximal oxygen pulse (p=0.53), differed significantly between test types, all p<0.001. Full demographic and CPET results stratified by sex and testing modality are summarized in Table 1.
3.2. Performance of selected prediction equations HRmax
66% of selected equations (5 of 8 for treadmill and 3 of 5 for cycle ergometer) underestimated HRmax in our athletic cohort and values ranged from 0.18 beats·min−1 (CI=184.17, 184.67; MAPE=4.35%) for Fox et al. in running CPET up to 4.90 beats·min−1 (CI=177.46, 178.08; MAPE=4.68%) for Fairbarn et al. in cycling CPET. 33% of selected equations (3 of 8 for treadmill and 2 of 5 for cycle ergometer) overestimated HRmax and values ranged from 0.08 beats·min−1 (CI=182.39, 183.11; MAPE=4.10%) for Arena et al. in cycling CPET up to 4.94 beats·min−1 (CI=189.34, 189.74; MAPE=4.94%) for Machado et al. in running CPET.
Significant differences with p<0.001 were observed less often for equations derived for treadmill CPET than for cycling CPET (in 7 of 8 compared to 2 of 5 formulae, respectively).
The lowest accuracy has been noted for the Machado et al. running formula (MAE= 4.94, %MAE=2.68; RMSE=10.47, %RMSE=5.67) and cycling equation provided by Fairbarn et al. (MAE=4.90, %MAE=2.68; RMSE=10.38, %RMSE=5.68). Selected models explained a variability in HRmax equal to 9.84 beats·min−1 when considering an absolute range of positive and negative values. Student t-test test indicated that the predicted HRmax differed significantly among all equations compared to the observed HRmax (all p<0.001), except Fox et al. (p=0.38 and p=0.23 for running and cycling CPET, respectively), Tanaka et al. (p=0.16 for cycling CPET) and Arena et al. (p=0.80 for cycling CPET). MAPE ranged 3.95-4.69%. A complete analysis of the prediction performance is presented in Table 2 (upper Part A and lower Part B respectively for running and cycling formulae). Bland-Altman plots for visual comparison of observed and predicted data are included in Supplementary Material 2 S2: Prediction performance of selected maximal heart rate prediction models.

Table 2.
Comparison of performance of selected HRmax prediction models.
| Reference | Equation | Performance in the athletic population | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Predicted HRmax (beats·min−1) |
Difference from the observed HRmax (beats·min−1) |
MAPE | MAE (beats·min−1) | %MAE† | RMSE (beats·min−1) | %RMSE‡ | p-value | |||||
| Mean (SD) | CI | Mean (SD) | CI | |||||||||
| Part A. Running CPET | ||||||||||||
| Nes et al. | 211- 0.64 · age | 188.23 (5.20) | 188.07, 188.39 | 3.63 (8.98) | 3.35, 3.91 | 4.31 | 3.63 | 1.97 | 9.69 | 5.25 | <0.001 | |
| Machado et al. | 218- 0.8 · age | 189.54 (6.50) | 189.34, 189.74 | 4.94 (9.24) | 4.66, 5.23 | 4.69 | 4.94 | 2.68 | 10.47 | 5.67 | <0.001 | |
| Tanaka et al. | 208- 0.7 · age | 183.09 (5.68) | 182.92, 183.27 | -1.50 (9.06) | -1.78, -1.22 | 3.96 | 1.50 | 0.81 | 9.18 | 4.97 | <0.001 | |
| Fox et al. | 220- age | 184.42 (8.12) | 184.17, 184.67 | -0.18 (9.79) | -0.48, -0.12 | 4.25 | 0.18 | 0.10 | 9.79 | 5.13 | 0.38 | |
| Londeree et al. | 206.3- 0.711 · age | 181.00 (5.77) | 180.82, 181.18 | -3.59 (9.07) | -3.87, -3.31 | 4.17 | 3.59 | 1.95 | 9.76 | 5.29 | <0.001 | |
| Inbar et al. | 205.8- 0.685 · age | 181.43 (5.56) | 181.26, 161.60 | -3.17 (9.04) | -3.45, -2.89 | 4.10 | 3.17 | 1.72 | 9.58 | 5.19 | <0.001 | |
| Gellish et al. | 207- 0.7 · age | 182.09 (5.68) | 181.92, 182.27 | 2.50 (9.06) | 2.22, 2.78 | 4.03 | 2.50 | 1.36 | 9.40 | 5.09 | <0.001 | |
| Arena et al. | 209.3- 0.72 · age | 183.68 (5.85) | 183.50, 183.86 | -0.91 (9.09) | -1.19, -0.63 | 3.95 | 0.91 | 0.50 | 9.13 | 4.95 | <0.001 | |
| Part B. Cycling CPET | ||||||||||||
| Tanaka et al. | 208- 0.7 · age | 182.19 (6.32) | 181.84, 182.54 | -0.48 (9.24) | -0.99, -0.03 | 4.11 | 0.48 | 0.26 | 9.26 | 5.07 | 0.16 | |
| Fox et al. | 220- age | 183.12 (9.03) | 182.62, 183.62 | 0.46 (10.06) | -0.09, 1.01 | 4.41 | 0.46 | 0.25 | 10.07 | 5.52 | 0.23 | |
| Londeree et al. | 206.3- 0.711 · age | 180.08 (6.42) | 179.73, 180.43 | -2.58 (9.26) | -3.09, -2.07 | 4.31 | 2.58 | 1.41 | 9.61 | 5.26 | <0.001 | |
| Fairbarn et al. | 201- 0.63 · age | 177.77 (5.69) | 177.46, 178.08 | -4.90 (9.16) | -5.40, -4.40 | 4.68 | 4.90 | 2.68 | 10.38 | 5.68 | <0.001 | |
| Arena et al. | 209.3- 0.72 · age | 182.75 (6.50) | 182.39, 183.11 | 0.08 (9.28) | -0.43, 0.59 | 4.10 | 0.08 | 0.05 | 9.28 | 5.08 | 0.80 | |
Abbreviations: HRmax, maximal heart rate; SD, standard deviation; CI, 95% confidence interval; MAPE, mean absolute percentage error; MAE, mean absolute error; %MAE, percentage of mean absolute error; RMSE, root mean standard error; %RMSE, percentage of root mean square error; CPET, cardio-pulmonary exercise test. Running CPET, n=4045; cycling CPET, n=1268. Data are presented as mean (standard deviation) and 95% confidence intervals. Mean (standard deviation; 95% confidence interval) of observed HRmax; running=184.60 (9.79; 184.30, 184.90); cycling=182.66 (10.28; 182.11, 183.24). Age is calculated in years. Differences between measured and predicted HRmax were calculated from the Student t-test. Significant p-values (<0.05) were bolded. Original derivation studies are presented in the Supplementary Material 3 S3 : Selected prediction models for maximal heart rate. Part A (upper) presents formulae for running and Part B (lower) for cycling. †%MAE=MAE/median of observed HRmax. ‡%RMSE=RMSE/median of observed.
4. Discussion
In this retrospective analysis of data from CPET conducted at the tertiary care sports diagnostic center, we examine the relationship between directly measured and predicted HRmax by the 13 commonly used regression equations. We demonstrate that: (1) the predicted values differed significantly for the majority of formulae, (2) the underestimation between the predicted and observed values ranged from 0.18 beats·min−1 to 4.90 beats·min−1, (3) overestimation of HRmax was observed less often than underestimation among EA, and (4) overestimation ranged from 0.08 up to 4.94 beats·min−1. By definition, external validation is ‘assessing the predictive agreement of a prediction model in a research population other than the one from which the model was developed’ [23]. We underline the lack of external validation studies on EA performed comprehensively for numerous HRmax equations. The main novelties of the present research are a wide cohort of EA at different levels of fitness and independent analysis adjusted for treadmill and cycling CPET. Such an approach enables reliable validation showing whether current models are transferable and suitable for EAs at both testing modalities.
Accurate prediction of HR might be helpful to confirm that the maximal effort has been achieved, compare training intensity with the maximal capacity of the individual, or consider clinically focused CPET as valuable in diagnosing CVDs [6]. The most accurate way to obtain HRmax is to perform laboratory CPET or maximum effort during the competition [15]. Although, those methods are not always possible due to the limited availability of specialized diagnostic centers, high costs of fees, or participant health restrictions and limitations in locations of events[24]. Despite significant inaccuracy, indirect measurement is widely applied in practice. So far, the accuracy of Fox et al. [19] and Tanaka et al. [2] models have been most frequently evaluated. Along with their popularity, they already have some inaccuracies. Nes et al. postulate bias at the level of 4-7 beats·min−1 for the Tanaka et al. and up to 35 beats·min−1 for the Fox et al. in certain subjects [14]. Furthermore, Magri et al. report that in a clinical population consisting of patients with heart failure, Fox et al. led to 37.60% and Tanaka et al. led to 42.60% errors compared to directly measured HRmax [25]. However, a comprehensive evaluation of other previously derived models is missing, and most studies focus only on a few particular formulae.
Our validation approach directed at the EA enables a comprehensive assessment of whether models are fairly replicable. Current HRmax formulae were originally derived from varied samples. Briefly, our results indicate that they do not perform precisely in EA, despite we only selected models derived from healthy, active cohorts with comparable demographic to our’s subjects. This is especially important due to their wide usage in sports diagnostics. The bias for most of the formulae ranged from 0 to 5 beats·min−1. However, the one provided by Machado et al.[26] overestimated HRmax for up to 4.94 beats·min−1.
Relying on inaccurate results when setting the exercise intensity may lead to suboptimal, non-diagnostic effort[3]. As a rule, the intensity for exercise medical programs should be 70-80% of HRmax for moderate-intensity steady-state activity and >85% of HRmax for high-intensity interval training [27]. An underestimated HRmax of ~5 beats·min−1 (i.e. ~3% of HRmax for 30-year male individuals according to widely used Fox et al. algorithm) does not seem to be a wide inaccuracy. This level of bias fills in the range of adjusted intensity for medical programs. Thus, predicted HRmax could be applied to EA in a medical setting but we underline that this relationship for the general and clinical populations need to be confirmed.
So far, previous studies have usually postulated that models may underestimate HRmax in people with a higher level of fitness [14,25]. Physical activity allows maintaining high and stable HRmax, despite increasing age. In addition, people with lower endurance capacity experience a steeper decline [28]. Our results showed a similar relationship and only ~40% (i.e. 3 of 8 for running CPET and 2 of 5 for cycling CPET) overestimated HRmax in the athletic cohort.
Calculating MAPE is our additional approach for the evaluation of HRmax prediction performance. Briefly, MAPE indicates function loss by a regression model, and it's intuitive to interpret relative inaccuracy. MAPE indicated that Arena et al. and Tanaka et al. perform with substantial accuracy for each modality. Their MAPE was the lowest both for treadmill and cycling data. We also noticed that Arena et al. (p=0.80 for cycling), Tanaka et al. (p=0.16 for cycle) and Fox et al. (p=0.30 for treadmill and p=0.23 for cycling) equations were the only ones that did not differ significantly from measured values. Our results indicate that these models perform quite precisely for EAs. They were characterized by the lowest inaccuracies. Perhaps because they were derived from numerous populations from synthesized various studies[2,19] or cohorts with above-average physical activity levels[29]. Thus, the ratio between basic (~200-220) and age covariates requires further studies to find the most precise values.
It is worth to underline that MAPE is more biased toward clinical than healthy, athletic populations. Our MAPE was lower for the athletic cohort than for the patients with heart failure in Magri et al.[30] study (4.25% and 4.41% vs 37.60% for Fox et al. or 3.96% and 4.11% vs 42.60% for Tanaka et al.). This indicates that HRmax prediction could be more accurate for active than diseased individuals and perhaps find its wider practical application among EA. We stipulate that these results emerge other confounding variables in participants with heart failure or CVDs (i.e. impact of medications, heart anatomy, etc.) [30].
All selected studies included just two variables, i.e. age and sex. The formulas used varied proportions of multipliers. It is well documented, that EAs achieve higher HRmax and a slower decline in HRmax with age than general population [7]. However, the majority of them differ significantly compared to observed values. We suggest that predicting HRmax only in this way may not be the most optimal method, and other estimation possibilities could exist. Previous reports indicate that there could be an impact of resting HR or submaximal HR at first and second ventilatory thresholds, BMI, body mass, VO2max, body fat, and testing modality [31,32]. All of them are parameters regularly measured by most diagnostic centers. Recently derived more specified models consider blood counts, left ventricular ejection fraction (LVEF), and diet [30]. However, these variables are difficult to implement in a unified form under practical circumstances. Measuring them for all subjects could be problematic. Therefore, staying with predicting HRmax based on additional somatic and exercise variables other than the age-only approach seems to be simultaneously a more accurate and feasible tool.
The limitation of this study is the slightly underrepresented group of female EA (15.01%). Our cohort was also more advanced in age. We recommend that future research consider a more equal proportion of male-to-female and include a higher number of younger participants. We also advise validation on equations derived exclusively for one sex.
Perspective and further studies directions
The accuracy of the predicted HRmax leaves considerable room for improvement. Recent reports suggest the involvement of other contributing variables, but their precise impact remains understudied. We suggest that the way to accurately predict HRmax is not by looking for the perfect ratio age-basic multiplier ratio. Perhaps including new, more advanced predictors (resting or submaximal exercise performance, past medical history, laboratory blood results- hemoglobin concentration, heart anatomy- LVEF, daily habits- diet, pharmaceutics- usage of β-blockers, etc.) may allow for more adjusted analyses [30,31,32,33,34,35]. We recommend more detailed research to assess their relationship with HRmax and their possible inclusion in predictive modeling directly for EA.
5. Conclusions
We conducted external validation of 13 commonly used prediction equations for HRmax in EA cohort. Predicted HRmax was significantly different from observed in CPET across the majority (11 of 13) of models. Underestimation of HRmax occurred more often than overestimation. HRmax predictions can be implemented as a supplemental method in sports diagnostics when direct measurement is not possible and cannot replace full CPET. Although, medical professionals and fitness practitioners should acknowledge the remaining inaccuracies, and predicted HRmax should not be the primary, preferable way of evaluating and adjusting exercise intensity.
Supplementary Materials
The following supporting information can be downloaded at: www.mdpi.com/xxx/s1, Supplementary Material 1 S1: TRIPOD Checklist: Prediction Model Development and Validation; Supplementary Material 2 S2: Prediction performance of selected maximal heart rate prediction models; Supplementary Material 3 S3: Selected prediction models for maximal heart rate.
Author Contributions
PSK: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Software, Validation, Visualization, Writing - Original Draft, Writing - Review & Editing. SW: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Supervision, Visualization, Writing - Review & Editing. IC: Data curation, Validation, Formal analysis, Resources, Methodology, Software. TT: Investigation, Project Administration, Validation, Supervision, Visualization. JL: Data curation. ML: Funding acquisition. MB: Funding acquisition. AM: Supervision. DŚ: Funding acquisition, Project administration.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Bioethics Committee of the Medical University of Warsaw (AKBE/32/2021).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to not obtaining consent from respondents to publish the data.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Karvonen, J.; Vuorimaa, T. Heart rate and exercise intensity during sports activities. Practical application. Sports Med 1988, 5, 303-311. [CrossRef]
- Tanaka, H.; Monahan, K.D.; Seals, D.R. Age-predicted maximal heart rate revisited. J Am Coll Cardiol 2001, 37, 153-156. [CrossRef]
- Guazzi, M.; Arena, R.; Halle, M.; Piepoli, M.F.; Myers, J.; Lavie, C.J. 2016 Focused Update: Clinical Recommendations for Cardiopulmonary Exercise Testing Data Assessment in Specific Patient Populations. Circulation 2016, 133, e694-711. [CrossRef]
- Iskandrian, A.S.; Heo, J.; Kong, B.; Lyons, E. Effect of exercise level on the ability of thallium-201 tomographic imaging in detecting coronary artery disease: analysis of 461 patients. J Am Coll Cardiol 1989, 14, 1477-1486. [CrossRef]
- Gianrossi, R.; Detrano, R.; Mulvihill, D.; Lehmann, K.; Dubach, P.; Colombo, A.; McArthur, D.; Froelicher, V. Exercise-induced ST depression in the diagnosis of coronary artery disease. A meta-analysis. Circulation 1989, 80, 87-98. [CrossRef]
- Balady, G.J.; Arena, R.; Sietsema, K.; Myers, J.; Coke, L.; Fletcher, G.F.; Forman, D.; Franklin, B.; Guazzi, M.; Gulati, M.; et al. Clinician's Guide to cardiopulmonary exercise testing in adults: a scientific statement from the American Heart Association. Circulation 2010, 122, 191-225. [CrossRef]
- Kaminsky, L.A.; Arena, R.; Myers, J. Reference Standards for Cardiorespiratory Fitness Measured With Cardiopulmonary Exercise Testing: Data From the Fitness Registry and the Importance of Exercise National Database. Mayo Clin Proc 2015, 90, 1515-1523. [CrossRef]
- Millet, G.P.; Vleck, V.E.; Bentley, D.J. Physiological differences between cycling and running: lessons from triathletes. Sports Med 2009, 39, 179-206. [CrossRef]
- Price, S.; Wiecha, S.; Cieśliński, I.; Śliż, D.; Kasiak, P.S.; Lach, J.; Gruba, G.; Kowalski, T.; Mamcarz, A. Differences between Treadmill and Cycle Ergometer Cardiopulmonary Exercise Testing Results in Triathletes and Their Association with Body Composition and Body Mass Index. International Journal of Environmental Research and Public Health 2022, 19, 3557.
- Hanson, N.J.; Scheadler, C.M.; Lee, T.L.; Neuenfeldt, N.C.; Michael, T.J.; Miller, M.G. Modality determines VO2max achieved in self-paced exercise tests: validation with the Bruce protocol. Eur J Appl Physiol 2016, 116, 1313-1319. [CrossRef]
- Moons, K.G.; Kengne, A.P.; Woodward, M.; Royston, P.; Vergouwe, Y.; Altman, D.G.; Grobbee, D.E. Risk prediction models: I. Development, internal validation, and assessing the incremental value of a new (bio)marker. Heart 2012, 98, 683-690. [CrossRef]
- Moons, K.G.; Royston, P.; Vergouwe, Y.; Grobbee, D.E.; Altman, D.G. Prognosis and prognostic research: what, why, and how? BMJ 2009, 338, b375. [CrossRef]
- Wiecha, S.; Price, S.; Cieslinski, I.; Kasiak, P.S.; Tota, L.; Ambrozy, T.; Sliz, D. Transferability of Cardiopulmonary Parameters between Treadmill and Cycle Ergometer Testing in Male Triathletes-Prediction Formulae. International Journal of Environmental Research and Public Health 2022, 19. [CrossRef]
- Nes, B.M.; Janszky, I.; Wisloff, U.; Stoylen, A.; Karlsen, T. Age-predicted maximal heart rate in healthy subjects: The HUNT fitness study. Scand J Med Sci Sports 2013, 23, 697-704. [CrossRef]
- Gulati, M.; Shaw, L.J.; Thisted, R.A.; Black, H.R.; Bairey Merz, C.N.; Arnsdorf, M.F. Heart rate response to exercise stress testing in asymptomatic women: the st. James women take heart project. Circulation 2010, 122, 130-137. [CrossRef]
- Collins, G.S.; Reitsma, J.B.; Altman, D.G.; Moons, K.G.M.; members of the, T.g. Transparent Reporting of a Multivariable Prediction Model for Individual Prognosis or Diagnosis (TRIPOD): The TRIPOD Statement. Eur Urol 2015, 67, 1142-1151. [CrossRef]
- Takken, T.; Mylius, C.F.; Paap, D.; Broeders, W.; Hulzebos, H.J.; Van Brussel, M.; Bongers, B.C. Reference values for cardiopulmonary exercise testing in healthy subjects - an updated systematic review. Expert Review of Cardiovascular Therapy 2019, 17, 413-426. [CrossRef]
- Paap, D.; Takken, T. Reference values for cardiopulmonary exercise testing in healthy adults: a systematic review. Expert Rev Cardiovasc Ther 2014, 12, 1439-1453. [CrossRef]
- Samuel, M.F.a.J.P.N.a.W.L.H. Physical activity and the prevention of coronary heart disease. Annals of clinical research 1968, 3 6, 404-432.
- Bouchard, C.; An, P.; Rice, T.; Skinner, J.S.; Wilmore, J.H.; Gagnon, J.; Perusse, L.; Leon, A.S.; Rao, D.C. Familial aggregation of VO(2max) response to exercise training: results from the HERITAGE Family Study. J Appl Physiol (1985) 1999, 87, 1003-1008. [CrossRef]
- Wiecha, S.; Kasiak, P.S.; Cieslinski, I.; Takken, T.; Palka, T.; Knechtle, B.; Nikolaidis, P.; Malek, L.A.; Postula, M.; Mamcarz, A.; et al. External validation of VO2max prediction models based on recreational and elite endurance athletes. PLoS One 2023, 18, e0280897. [CrossRef]
- Scherr, J.; Wolfarth, B.; Christle, J.W.; Pressler, A.; Wagenpfeil, S.; Halle, M. Associations between Borg's rating of perceived exertion and physiological measures of exercise intensity. Eur J Appl Physiol 2013, 113, 147-155. [CrossRef]
- Damen, J.A.A.; Moons, K.G.M.; van Smeden, M.; Hooft, L. How to conduct a systematic review and meta-analysis of prognostic model studies. Clin Microbiol Infect 2022. [CrossRef]
- Stensvold, D.; Sandbakk, S.B.; Viken, H.; Zisko, N.; Reitlo, L.S.; Nauman, J.; Gaustad, S.E.; Hassel, E.; Moufack, M.; Bronstad, E.; et al. Cardiorespiratory Reference Data in Older Adults: The Generation 100 Study. Medicine and Science in Sports and Exercise 2017, 49, 2206-2215. [CrossRef]
- Lach, J.; Wiecha, S.; Sliz, D.; Price, S.; Zaborski, M.; Cieslinski, I.; Postula, M.; Knechtle, B.; Mamcarz, A. HR Max Prediction Based on Age, Body Composition, Fitness Level, Testing Modality and Sex in Physically Active Population. Frontiers in Physiology 2021, 12, 695950. [CrossRef]
- Machado, F.A.; Kravchychyn, A.C.P.; Peserico, C.S.; da Silva, D.F.; Mezzaroba, P.V. A new age-based equation for predicting maximum heart rate in endurance-trained runners. Revista Brasileira de Ciências do Esporte 2018, 40, 100-105. [CrossRef]
- McGregor, G.; Powell, R.; Begg, B.; Birkett, S.T.; Nichols, S.; Ennis, S.; McGuire, S.; Prosser, J.; Fiassam, O.; Hee, S.W.; et al. High-intensity interval training in cardiac rehabilitation (HIIT or MISS UK): A multi-centre randomised controlled trial. Eur J Prev Cardiol 2023. [CrossRef]
- Kostis, J.B.; Moreyra, A.E.; Amendo, M.T.; Di Pietro, J.; Cosgrove, N.; Kuo, P.T. The effect of age on heart rate in subjects free of heart disease. Studies by ambulatory electrocardiography and maximal exercise stress test. Circulation 1982, 65, 141-145. [CrossRef]
- Arena, R.; Myers, J.; Kaminsky, L.A. Revisiting age-predicted maximal heart rate: Can it be used as a valid measure of effort? Am Heart J 2016, 173, 49-56. [CrossRef]
- Magri, D.; Piepoli, M.; Gallo, G.; Corra, U.; Metra, M.; Paolillo, S.; Filardi, P.P.; Maruotti, A.; Salvioni, E.; Mapelli, M.; et al. Old and new equations for maximal heart rate prediction in patients with heart failure and reduced ejection fraction on beta-blockers treatment: results from the MECKI score data set. Eur J Prev Cardiol 2022, 29, 1680-1688. [CrossRef]
- Zavorsky, G.S. Evidence and possible mechanisms of altered maximum heart rate with endurance training and tapering. Sports Med 2000, 29, 13-26. [CrossRef]
- Miller, W.C.; Wallace, J.P.; Eggert, K.E. Predicting max HR and the HR-&OV0312;2 relationship for exercise prescription in obesity. Medicine & Science in Sports & Exercise 1993, 25. [CrossRef]
- Wiecha, S.; Kasiak, P.S.; Cieslinski, I.; Maciejczyk, M.; Mamcarz, A.; Sliz, D. Modeling Physiological Predictors of Running Velocity for Endurance Athletes. J Clin Med 2022, 11. [CrossRef]
- Sliz, D.; Wiecha, S.; Gasior, J.S.; Kasiak, P.S.; Ulaszewska, K.; Postula, M.; Malek, L.A.; Mamcarz, A. The Influence of Nutrition and Physical Activity on Exercise Performance after Mild COVID-19 Infection in Endurance Athletes-CESAR Study. Nutrients 2022, 14. [CrossRef]
- Sliz, D.; Wiecha, S.; Ulaszewska, K.; Gasior, J.S.; Lewandowski, M.; Kasiak, P.S.; Mamcarz, A. COVID-19 and athletes: Endurance sport and activity resilience study-CAESAR study. Front Physiol 2022, 13, 1078763. [CrossRef]
Figure 1.
Flow diagram for inclusion procedure. Abbreviations: CPET, cardiopulmonary exercise test; HRmax, maximal heart rate. From 6439 endurance athletes screened for inclusion in years 2013-2021, 5311 of them (82.48%) met study criteria.
Figure 1.
Flow diagram for inclusion procedure. Abbreviations: CPET, cardiopulmonary exercise test; HRmax, maximal heart rate. From 6439 endurance athletes screened for inclusion in years 2013-2021, 5311 of them (82.48%) met study criteria.
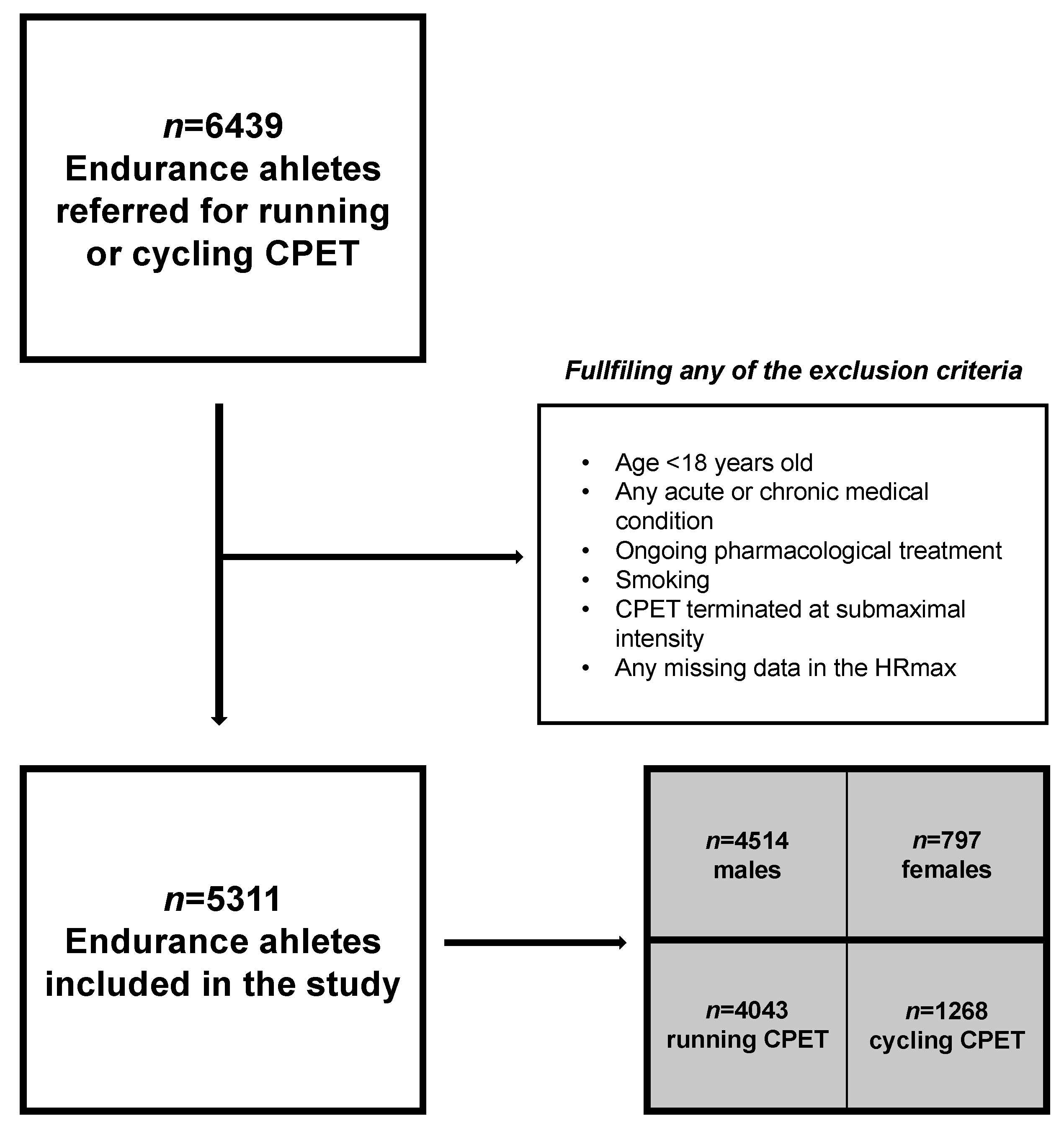
Table 1.
Participants characteristics.
| Variable | Running CPET | Cycling CPET | p-value | ||||||
|---|---|---|---|---|---|---|---|---|---|
| All [n=4043] | Males [n=3377] | Females [n=666] | All [n=1268] | Males [n=1137] | Females [n=131] | ||||
| Age [years] | 33.58 (8.12) | 33.96 (8.15) | 33.66 (7.67) | 36.88 (9.03) | 37.30 (9.11) | 33.19 (7.37) | <0.001 | ||
| Weight [kg] | 74.87 (11.18) | 77.68 (9.38) | 60.60 (8.36) | 76.99 (10.76) | 78.81 (9.53) | 61.18 (7.30) | <0.001 | ||
| Height [cm] | 177.52 (7.84) | 179.55 (6.24) | 167.22 (7.00) | 178.77 (7.26) | 180.01 (6.38) | 168.05 (5.41) | <0.001 | ||
| BMI [kg·m−2] | 23.66 (2.54) | 24.06 (2.41) | 21.65 (2.18) | 24.04 (2.65) | 24.32 (2.56) | 21.63 (2.11) | <0.001 | ||
| BF [%] | 16.47 (5.17) | 15.48 (4.52) | 21.48 (5.33) | 16.75 (5.07) | 16.09 (4.68) | 22.46 (4.66) | 0.09 | ||
| FFM [kg] | 62.45 (9.27) | 65.40 (6.44) | 47.49 (6.55) | 63.93 (8.17) | 65.86 (6.02) | 47.23 (4.40) | <0.001 | ||
| HRmax [beats·min−1] | 184.60 (9.79) | 184.47 (9.88) | 185.22 (9.33) | 182.67 (10.27) | 182.46 (10.30) | 184.38 (9.97) | <0.001 | ||
| RERmax | 1.12 (0.04) | 1.12 (0.04) | 1.12 (0.04) | 1.13 (0.04) | 1.13 (0.05) | 1.12 (0.03) | <0.001 | ||
| VE/VCO2max | 31.75 (3.89) | 31.70 (3.83) | 32.02 (4.22) | 29.39 (4.18) | 29.33 (4.17) | 29.92 (4.28) | <0.001 | ||
| fR [breaths·min−1] | 57.22 (9.11) | 57.57 (9.22) | 55.44 (8.31) | 56.37 (9.32) | 56.51 (9.47) | 55.18 (7.92) | 0.004 | ||
| VO2max [mL·min−1·kg−1] | 53.24 (7.12) | 54.09 (6.92) | 48.90 (6.54) | 51.67 (7.86) | 51.95 (7.96) | 49.21 (6.53) | <0.001 | ||
| O2pulsemax [mL·beat−1] | 21.58 (4.03) | 22.69 (3.24) | 15.95 (2.73) | 21.66 (3.62) | 22.28 (3.18) | 16.31 (2.67) | 0.53 | ||
Abbreviations: CPET, cardiopulmonary exercise test; BMI, body mass index; BF, body fat; FFM, fat-free mass; HRmax, maximal heart rate; RERmax, maximal respiratory exchange ratio; VE/VCO2max, maximal minute ventilation efficiency; fR, breathing frequency; VO2max, maximal oxygen uptake; O2pulsemax, maximal oxygen pulse. Categorical data are presented as numbers (percentages). Continuous data are presented as mean (standard deviation). Differences between running and cycling CPET were calculated by Student t-test. Significant p-values (<0.05) were bolded.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



