
Submitted:
23 March 2023
Posted:
24 March 2023
You are already at the latest version
Abstract
Carbapenems have long been considered as treatment of choice for Gram-Negative Bacteria (GNB) infections, and today the clinical utility of this class is threatened by the emergence and spread of resistance favored by its increasing use. According to the WHO, Acinetobacter baumannii, nosocomial infection agent, tops the list of priority antibiotic-resistant pathogens, considered to be the most risky for humans. This study sought to determine the prevalence of Acinetobacter baumannii strains producing carbapenemases in four health facilities in the Center and Littoral regions of Cameroon and the associated risk factors. An analytical cross-sectional study was conducted over a six-month period from January to June 2022. All Acinetobacter baumanii or suspected strains isolated from pathological samples at the bacteriology laboratory of different health facilities were systematically collected and underwent a re-identification. After successfully subculturing and growing on nutrient agar, re-identification and antimicrobial susceptibility Testing (AST) were performed using the VITEK 2 System and the Kirby-Bauer method according to the guidelines of the Clinical and Laboratory Standards Institute (CLSI). Detection and phenotypic characterization of carbapenemases was performed according to adequate standard procedures. A total of 168/226 clinical isolates of Acinetobacter baumannii were confirmed after re-identification of which 52.69% came from male patients, and 55.09% from participants aged between 10-39 years old and 46.71% from pus samples. A very high resistance rates to all families of antibiotics was noted except to colistin (10.2%). About 40.12% of these strains produced carbapenemases with 62.69% of class B and 37.31% of class A. In addition, frequent hospitalisation was significantly associated to the production of carbapenemase among Acinetobacter baumanii (Ajusted-OR=16.53, P-value<0.0001). This study highlighted the emergence of carbapenemase-producing Acinetobacter baumannii which is increasingly growing. Continuous drug-resistant monitoring and preventive measures could help to prevent and curb the dissemination of A.baumanii resistance genes, especially in hospital settings.
Keywords:
Acinetobacter baumannii
; Resistance
; carbapenemases
; Health Facilities
1. Introduction
Acinetobacter is a Gram-negative aerobic bacilli or coccobacilli that belong to the Moraxellaceae family [1]. They are ubiquitous and can survive on dry surfaces for up to a month, are frequently carried on the skin of healthcare workers, and increase the likelihood of both colonizing patients and contaminating medical equipment. There are several species of Acinetobacter which can cause disease in humans, and A. baumannii (AB) accounts for almost 80% of infections [2]. It is responsible for a variety of human infections such as ventilator-associated pneumonia, bacterial meningitis, wound and soft tissue infections, peritonitis, and urinary tract and healthcare-associated infections [3]. One of the factors contributing to chronic and persistent infection with Acinetobacter antimicrobial resistance is its ability to colonize and then form a biofilm on biotic surfaces contributing to Acinetobacter to easily survive and transfer in the hospital environment, such as attached to various biotic and abiotic surfaces eg foleys catheter ,vascular catheter, cerebrospinal fluid shunts[4,5]
Antibiotic resistance or antibiotic resistance is the ability of a microorganism to resist the effects of antibiotics [3]. In the past, clinical isolates of Acinetobacter baumanii were susceptible to most groups of available antibiotics until a few years ago when they acquired a high capacity to develop resistance against many antibiotics [5]. This can be explained by the fact that Acinetobacter baumanii has a very high capacity to adapt to stress and has undergone prolonged exposure to antibiotics in a hospital setting [5].
In Geneva in 2017, the WHO published a list of bacteria that have become resistant to several classes of antibiotics, including carbapenems and third-generation cephalosporins [6]. Multi-drug resistant Acinetobacter baumanii (MDRAB) has been identified as one of the major relevant multi-drug resistant organisms threatening human health [6]. In the modern health system, Acinetobacter baumanii is undoubtedly one of the most effective pathogens responsible for nosocomial infections, taking into account its emergent character, its opportunistic pathogenicity, its resistance to antibiotics and its power of epidemic diffusion, few antibiotics are able to treat infections caused by this pathogen [6,7].Their resistance to carbapenem is linked to the association of resistance mechanism (overexpression of extended-spectrum betalactamases with efflux pumps, impermeability or expression of carbapenem-hydrolysing betalactamase know as carbapenemase [8], Which are enzymes capable of hydrolyzing carbapenems and which belong to one of the three groups of betalactamases, namely the groups of classe A,B,D of Ambler [9].
Worldwide, several data on Acinetobacter baumanii 's resistance to antibiotics have already been reported. A systematic review and meta-analysis on the incidence and prevalence of hospital-acquired infections (HAIs) caused by Acinetobacter baumannii (HA-AB), particularly HA-carbapenem resistant A. baumanii (HA-CRAB) infections in the WHO-defined regions of Europe (EUR), Eastern Mediterranean (EMR) and Africa (AFR) was conducted by Soha et al in 2019. A comprehensive literature search was performed using MEDLINE, EMBASE and GMI databases (01/2014-02/2019). Twenty-four studies from 3,340 records were included in this review (EUR: 16, EMR: 6, AFR: 2). For carbapenem-resistant A. baumannii infections in intense care units (ICUs), the pooled incidence and incidence density were 41.7 (95% CI 21.6-78.7) cases per 1,000 patients and 2.1 (95% CI 1.2-3.7) cases per 1,000 patient days, respectively. In ICUs, A. baumannii and carbapenem-resistant A. baumannii strains accounted for 20.9% (95% CI 16.5-26.2%) and 13.6% (95% CI 9.7-18.7%) of all HAIs, respectively [10]. In Africa, high rates of MDR A. baumannii infection have been demonstrated in several countries. Laouar et al in Algeria in 2019 found that the resistance of Acinetobacter baumanii strains to Imipenem evolved impressively over time. It increased from 26% in 2007 to 88.1% in 2016, while 57.1% of carbapenemase-producing strains came from intensive care units [11]. A study done by Ogbulu et al in Nigeria in 2020 showed very high resistance (55.2%) of Acinetobacter baumanii to carbapenems following which low activity was observed only for colistin and amikacin [12]. According to Pillay et al in South Africa in 2021, hospital effluents constitute a potential risk of the formation of multi-resistant biofilm of Acinetobacter baumanii strains [13].
A systematic review and cumulative meta-analysis of carbapenemase-producing Acinetobacter baumanii (CPAB) conducted by Mizan et al in Africa between 2014 and 2019 showed a higher prevalence of CPAB isolates across years was. The pooled prevalence CPAB among the clinical specimens in Africa was 56.97%. With the class B carbapenemase VIM (Verona integron-encoded metallo-beta-lactamase) the most prevalent [14]. In this review, data were presented for all over Africa except Central Africa were Cameroon is located [14].This might show that the lack of data on antibiotic resistance in Africa is still a problem for developing and applying evidence-based infection control and prevention measures. Moreover, it might impede patient care and public health, leaving the vulnerable population. This is the reason why we proposed to carry out this study on the prevalence of CPAB strains and the risk factors associated in Cameroon.
2. Results
2.1. Description of the Source Characteristics of the Isolates Collected
From the 226 strains collected at the baseline, 167 (73.89%) were finally confirmed as Acinetobacter baumanii after re-identification (Table 1).
The majority of isolates came from Laquintinie Hospital of Douala in Littoral region, Cameroon, 70.66% (118/167), from male patients, 52.69% (88/167) and 55.09% (92/167) of isolates were obtained from participants aged between 10-39 years old. Moreover, 46.71% (78/167) of isolates derived from pus samples and 4.79% (8/167) from vaginal samples.
2.2. Susceptibility of Acinetobacter baumanii Isolates to Beta-Lactams
The drug susceptibility profile of AB to beta-lactams is presented below (Figure 1).
The sensitivity profile of AB showed a very high resistance rate to all beta-lactams such as : penicillins (piperacillin: 94.7% and ticarcillin: 99.1%),cephalosporins (cefotaxime : 70.6%, ceftazidime :82.9% and cefepime : 74.1%) and carbapenems (imipenem : 61.7% and meropenem : 65.2%). It was also noted a high resistance to beta-lactams supplemented with beta-lactamase inhibitors (piperacillin/tazobactam :79.6% and ticarcillin/clavulanic acid : 81.9%).
2.3. Resistance Profile of Acinetobacter baumanii to Other Families of Antibiotics
Resistance Profile of AB to the family of aminoglycosides, fluoroquinolones, tetracyclines, polymyxin and cotrimoxazol were tested in prder to determine their resistance profile (Figure 2).
There was high resistance to fluoroquilonones (89.1% to levofloxacin), to tetracyclin (67.3%), to aminoglycosides (73.3% to tobramycin, 64.8% to gentamicin and 40.9% to amikacin) and to cotrimoxazol (71.2%). However, there was a low resistance rate to colistin (10.2%).
2.4. Prevalence of carbapenemase producing Acinetobacter baumanii
The frequency of production of carbapenemase and the classification of carbapenemases are shown in Figure 3.
In this study, the overall prevalence of Acinetobacter baumanii-producing carbapenemase was 40.12% (67/167) with 62.69% (42/67) of class B (metallo-beta-lactamase) and 37.31% (25/67) of class A.
In parallel, further distribution of carbapenemase producing isolates is presented in Table 2.
It can be observed from table 2 that null carbapenemase producing isolate have been recovered from DSMPH and HGY. Contrarily, frequent carbapenemase producing Acinetobacter baumanii was observed in other Health care facilities, even though no significant difference (P=0.81). Similarly, there was no significant difference between carbapenemase producing Acinetobacter baumanii prevalence within different socio-demographic (age and gender) categories (P≤0.05) (table 2).
2.5. Analysis of risk factors related to Acinetobacter baumanii’s carbapenemase production
Univariate analysis of risk factors associated to carriage of carbapenemase producing Acinetobacter baumanii among participants is presented in table 3. Significant risk factors in this previous analysis were introduced in a multivariate model (table 4).
This current research revealed that frequent hospitalisation was significantly associated to the production of carbapenemase among Acinetobacter baumanii (Ajusted-OR=16.53, P-value<0.0001).
3. Discussion
In order to fight against the emergence and spread of multiresistant bacteria, this study aimed to determine the prevalence of carbapenemase-producing Acinetobacter baumannii from four health facilities in Cameroon. The study took place in two regions of Cameroon (Central and Littoral regions). Out of 226 collected strains, 168 (74.34%) were confirmed Acinetobacter baumannii isolates. The majority of isolates came from Laquintinie Hospital of Douala in Littoral region, Cameroon (70.66%).
In the present study 88 (52.69%) clinical isolates included were from male patients with highest number of isolates from patients aged between 10-39 years old. In accordance to the current study, Rao et al. also observed male predominance (81.8%) [15]. These findings suggest that male elderly were more vulnerable for infections in both the studies. 46.71% of these strains came from suppurations, 26.35% from urine and 22.16% from blood samples. these results are in agreement with those of Okalla et al in 2015, in Cameroon which found that the majority of their strains came from suppurations, urine and urinary catheters [16]. In addition, Castilho et al in 2017 revealed that in terms of the topography of infection, the lungs were the most common site (53.1%), followed by the site of surgical intervention (postoperative wounds) (10.9%), the urinary tract (7.8%) and the blood stream (i.e., sepsis) (6.2%) [17]. This can be explained by the fact that in the hospital environment wounds and other lesions are prone to contamination with a multitude of organisms including Acinetobacter baumannii, which is one of the bacteria most incriminated in nosocomial infections. CAUTIs (catheter-associated urinary tract infections) continue to be one of the most common health-care-related illnesses in the entire globe. CAUTIs are the cause of 40% of all hospital-acquired infections and 80% of all nosocomial urinary tract infections (UTIs). A urine catheter is implanted into a high percentage of inpatients at some point during their hospitalization, and indwelling urinary catheter adoption likely to be on the rise. Urinary catheters, made of plastic materials, inhibit the urinary tract’s natural defence mechanisms and enhance the bacterial colonization or biofilm formation on the catheter surface, which may cause CAUTIs [18].
From antimicrobial susceptibility testing, the percentage rates of resistance to remaining antibiotics range from 40,9% to 99.1% with the exception of colistin which had 10.2% of resistant strains detected. Carbapenem resistance of A. baumannii is a major concern since it is the drug of choice in the treatment of A. baumannii infections [19]. The results showed that Acinetobacter baumanii had a very high resistance to beta-lactams (82.9% ceftazidime and 74.1% cefepime) including carbapanems (resistant to both imipenem 61.7% and meropenem 65.2%). In according to the current study, in South Africa, a report on antimicrobial resistance surveillance from sentinel public hospitals in 2013 showed a high resistance rate of 73% to cefepime and 80% to ceftazidime [20], then, Anane et al in 2020 showed very high level resistance to beta-lactams with 81% to imipenem and 83% to meropenem [21]. Comparing the results of the present study with these earlier studies indicates that the resistant rate of A. baumannii to various antibiotics has not really decreased. High levels of resistance to third and fourth generation cephalosporins and carbapenems in this study indicated they are no longer really efficacious in the treatment of A. baumannii isolated in Cameroon and thus constitute a great challenge given that they belong to the last classes of antibiotics and are therefore used as the last therapeutic alternatives in cases of antibiotic therapy failure.
The antibiogram results also showed high resistance to fluoroquinolones (89.1% to levofloxacin), to tetracyclin (67.3%), to aminoglycosides (73.3% to tobramycin, 64.8% to gentamicin and 40.9% to amikacin) and to trimethoprim/sulfamethoxazol (71.2%). There were predominance of fluoroquinolones (FQs) resistance and a higher activity of amikacin compared to other aminoglycosides. Our results are higher than those of Okalla et al in 2013 in Cameroon which revealed 24.43% to Amikacin and 50% to fluoroquinolones [16], what testifies to the emergence of antibiotic resistance in Acinetobacter baumanii. This could be explained by the fact that FQs have the widest use and are currently recommended by different physicians as they have multiple applications and different advanced generations [22]. Nevertheless the emergence and spread of bacterial resistance to FQs among Gram-negative bacteria generally and A. baumannii specifically is becoming increasingly serious with their extensive use. The developing resistance of A. baumannii to antimicrobial agents has been described and this was attributed to the abundance of these antibiotics in multiple pharmaceutical markets [23], besides their misuse [24]. A. baumannii infection is difficult to remedy, as of its everlasting fullness to acquire antimicrobial resistance due to the suppleness of its genome [25]. Compared to the study done by Anane et al in 2020, which gave 5% resistance to colistin [21], there is an increase in the rate of resistance to colistin. The susceptibility of A. baumannii to colistin in this study indicated that colistin is still a better option of the drug for the treatment of infections caused by A. baumannii in Cameroon hospitals. However, the issue of nephrotoxicity, neurotoxicity, colistin-resistance, and heteroresistance shown by colistin monotherapy is a challenge in the management of this infection [26].
Of the 168 isolates of A. baumanii, the carbapenemase producers represented 40.12%, of which 37.31% were class A carbapenemase and 62.29% were class B. This prevalence is lower than that obtained by Mizan et al in 2020 (56.97%) [14] and could explained by the fact that it was a cumulative meta-analysis including several studies made in Africa. Metallo-beta-lactamase (MBL) was the most represented among CPAB isolates. This is consistent with other reviews that were conducted globally [27, 28]. Indeed, carbapenemases represent three classes of β-lactamases. The three classes are Ambler class A and D carbapenemase (serine carbapenemases) and class B carbapenemases (zinc dependent) which are inhibited by metal chelators, such as EDTA and are called metallo- β-lactamases (MBLs). Metallo-β-lactamases (MBLs) enzymes are able to hydrolyze all β-lactam antibiotics and MBL genes are usually located in transferable genetic elements such as plasmid and integrons along with other antibiotic resistance genes [25]. Therefore, dissemination of strains harboring MBL genes is of crucial importance, and appropriate measures should be taken into consideration by infection control programs [29].
By analyzing the risk factors, the current study revealed that frequent hospitalisation was significantly associated to the production of carbapenemase among Acinetobacter baumanii (Ajusted-OR=16.53, P-value<0.0001). According to Pillay et al in South Africa in 2021, hospital effluents pose a potential risk of multidrug-resistant biofilm formation of Acinetobacter baumanii strains [13]. The impressive spread and prevalence of A. baumannii in healthcare settings has been facilitated by its ability to withstand dry and humid environments, its resistance to disinfectants and antibiotics, and its biofilm-forming property that leads to colonization of inert surfaces and medical devices [30].
4. Materials and Methods
4.1. Type, Site, and Duration of Study
A cross-sectional and analytical study was carried out during six-month period from 7 January to 28 June 2021. Isolates were collected from four hospitals located in the two most crowded regions of Cameroon: three health facilities from the center region (the Military Hospital of Yaoundé, the Dominicain Saint Martin de Porres Hospital, and the Referral Teaching Hospital of Yaoundé), and lastly one from the littoral region (Laquintinie Hospital). The strains re-identification and downstream analyses were carried out at the laboratory setting of the Military Hospital of Yaoundé.
4.2. Sampling Method and Selection Criteria
During the study period, all AB or suspected AB strains isolated from pathological specimens (pus, wounds, probe tip, urine, blood, effusion fluid, and endocervical swab) at each bacteriology laboratory of our study sites were systematically collected, stored, and later included in the study for the upcoming re-identification and analyses. Non-confirmed cases of A. baumanii after re-identification and strains with a lack of useful clinical information were excluded from the study.
4.3. Re-Identification and Samples Processing
Subculture of collected isolates: The isolates in cryotubes containing 1.5 mL of brain-heart broth supplemented with 10% glycerol were inoculated around the flame on nutrient agar by the streaking method. Identification and Antimicrobial Susceptibility Testing (AST): The colonies obtained were firstly subjected to macroscopic examination (description of the size, color, and appearance of the colonies), followed by an oxidase test (oxidase-) on one pure colony. Identification and AST were performed on a bacterial suspension (The 0.5 McFarland bacterial suspension was diluted to 1.5 × 107 CFU/ml in 0.45% saline) using the VITEK 2 System (VITEK® 2, BioMerieux, France). The minimum inhibitory concentration (MIC) was determined for the available 12 antibiotics, in Vitek 2 GN ID card (Biomeriux, France), which are ceftazidime, cefotaxime, cefepime, piperacillin/tazobactam, imipenem, meropenem, gentamicin, amikacin, tobramycin, levofloxacin, tetracycline and sulfamethoxazole/trimethoprim. Card was automatically filled, sealed, and loaded into the VITEK 2 instrument for incubation and reading. Kirby-Bauer method was used to test the susceptibility to the four others antibiotics (ticarcillin, ticarcillin/clavulanic acid, piperacillin and colistin), that are not available in the Vitek® system. Results were interpreted according to the guidelines of the Clinical and Laboratory Standards Institute (CLSI) [31]. Detection of carbapenemases : All isolates of imipinem-resistant AB (IRAB) isolates were subjected to the carbapenemase phenotypic control tests resistance using Boronic acid and Chelating agent (EDTA) tests for class A and class B (Metallo-B-Lactamases carbapenemase respectively. IRAB isolates were tested for KPC carbapenemases production on disks containing boronic acid. A disk containing imipenem (Mast,UK) and another containing imipenem with 400 μg of boronic acid (Sigma-Aldrich, Germany) were placed on the Muller hinton agar on which the test organism was seeded. The diameter of the growth-inhibitory zone around the imipenem disk with boronic acid was compared with that around the corresponding imipenem disk without boronic acid. The test was considered positive for the detection of class A carbapenemase production when the diameter of the growth-inhibitory zone around the imipenem disk with boronic acid was ≥ 5 mm larger than that around the disk containing the imipenem substrate alone [32]. The detection of MBL production was performed using the same principle based on inhibition by EDTA. This technique consisted of two imipenem disks with or without 10 μl of 0.5 M EDTA. An increase of 10 mm in the inhibition zone diameter in the presence of EDTA was considered a positive result [33].
4.4. Data Evaluation and Analysis
The different variables and results obtained were recorded in Excel 2013 software and then analyzed with the statistical software, Statview 5.0 (SAS Institute Inc., Cary, NC, USA). The analysis included the calculation of the frequency and their intervals at 95% (for qualitative variables) and the mean or the median (for quantitative variables). Odds ratios were used to determine the risk factors associated with Acinetobacter baumanii-producing carbapenemases. A chi-square test was used to compare the proportion of categorical variables, and a value of p < 0.05 was considered statistically significant.
4.5. Ethical Considerations
An ethical clearance was issued by the institutional research ethics committee of the University of Douala (Authorization N◦2737 CEI-Udo/07/2021/M; 13 July 2021 and Autorisation N°3041 CEI-Udo/04/2022/M; 11April 2022) and research authorizations from the directors of each hospital were obtained.
6. Limitations
The limitation of this study was the inability to carry out a molecular characterization of the Acinetobacter baumanii isolates due to the lack of funding. This aspect makes it possible later to deepen the research by molecular analyses for a complete evaluation of the genes encoding the production of carbapenemases, including class D beta-lactamases which are not inhibited by β-lactamase inhibitors [34].
7. Conclusions
This study highlighted a high prevalence of Acinetobacter baumanii-producing carbapenemase. The patients being frequently hospitalised were the most affected. However, only amikacin and colistin were antibiotic remaining susceptible to A.baumanii-resistant strains to B-lactams. Continuous drug-resistant monitoring and preventive measures could help to prevent and curb the dissemination of AB resistance genes, especially in hospital settings.
Author Contributions
CID and BN conceived the project and designed the study. CID, BN and PDDD searched relevant literature, scrutinized all relevant information and draft the manuscript. CID and BDTP conducted and coordinated the field study. CG, HVSN, CKP, YGK and MJTT collected and processed the samples and data. PDDD, CSN and RKW analyzed the data and wrote the article. CID, BN, BDTP and TA revised the manuscript. All authors read and approved the final manuscript.
Funding
Self-financing
Institutional Review Board Statement
The study was approved by the Institutional Human Health Research ethics committee of the University of Douala (Authorization N◦2737 CEI-Udo/07/2021/M; 13 July 2021). We obtained research authorizations issued by the directors of the various hospitals (Authorization N◦0187AAR/MINSANTE/DRSPL/BCASS, 10 May 2022; Authorisation N°1AR/MINSANTE/DHL, 25 March 2022 and Authorization N◦210211/DV/MIMDEF/DSM/RSM1/HMR1/12; 6 October 2021).
Informed Consent Statement
Not applicable.
Data Availability Statement
All data generated or analysed in the course of this study are included in this manuscript.
Acknowledgments
The authors are grateful to the directors and staff of the various hospitals.
Conflicts of Interest
The authors declare no conflict of interest.
Consent for Publication
All authors consented to the publication.
References
- Bouvet PJM, Grimont PAD. Taxonomy of the genus Acinetobacter with the recognition of Acinetobacter baumannii sp. Nov., Acinetobacter haemolyticus sp. Nov., Acinetobacter johnsonii sp. Nov., and Acinetobacter junii sp. Nov. and emended descriptions of Acinetobacter calcoaceticus and Acinetobacter lwoffii. Int J Syst Bacteriol. 1986;36:228-240.
- Lo, Gora & Dieng, Assane & Diallo, Awa & Samb, Marieme & Tine, Alioune & Mbaye, Serigne & Ndiaye, Lo & Farba, Karam & Diagne-Samb, Habsa & Ngom-Cisse, Safietou & Ndoye, Aissatou & Diop-Ndiaye, Halimatou & Kane, Coumba & Gaye-Diallo, Aissatou & Mboup, Souleymane & Saad, Cheikh & Boye, Bouh & Camara, Makhtar. (2022). Molecular Epidemiology of Carbapenem-resistant Acinetobacter baumannii Isolates in a Senegalese University Teaching Hospital. Journal of Advances in Microbiology. 22. 73-82. [CrossRef]
- Mizan K, Lemma D, Baye G, Feleke M. Bacilles Gram négatifs non fermantaires du glucose produisant des carbapénémases en Afirque, Pseudomonas aeruginosa et Acinetobacter baumanii. Revue internationale de Microbiologie 2020.P42.
- Yoon-Kyoung Hong & Hyunkeun Kim and Kwan Soo Ko: Two types of colistin hetero-resistance in Acinetobacter baumannii isolates, 2020, Emerging Microbes & Infections.
- Raro OHF, Gallo SW, Ferreira CAS, Oliveira SD. Carbapenem-resistant Acinetobacter baumannii contamination in an intensive care unit. Rev Soc Bras Med Trop. 2017;50(2):167-172. [CrossRef]
- Organization WHO. WHO Publishes List of Bacteria for Which New Antibiotics Are Urgently Needed. Geneva, Switzerland: WHO; 2017. http://www.who.int/mediacentre/news/releases/2017/bacteria-antibiotics-needed/en/ [Google Scholar].
- Yoon-Kyoung Hong & Hyunkeun Kim and Kwan Soo Ko : Two types of colistin hetero-resistance in Acinetobacter baumannii isolates, 2020, Emerging Microbes & Infections.
- Nordmann P.Carbapenemase-proucing Enterobacteriaceae : overview of a major public health challenge.Med Mal Infect 2004 ; 44 :51-56.
- Nordman P,Naas T,Poirel L Global spread of carbapenemase-producing Enterobacteriaceae Emerg Infect Dis 2012 ; 17 : 1791-1798.
- Olaniyi Ayobami, Niklas Willrich, Thomas Harder, Iruka N. Okeke, Tim Eckmanns and Robby Markwart; The incidence and prevalence of hospital-acquired (carbapenem-resistant) Acinetobacter baumannii in Europe, Eastern Mediterranean and Africa: a systematic review and meta-analysis, 2019, Emerging Microbes & Infections.
- Nabila Benamrouche, Ourida Lafer, Lahcen Benmahdi, Akila Benslimani, Wahiba Amhis, Houria Ammari, and al; Phenotypic and genotypic characterization of multidrug-resistant Acinetobacter baumannii isolated in Algerian hospitals, 2020, Journal of Infection in Developing Countries.
- David O. Ogbolu, Oyebode A. Terry Alli, Adeolu S. Oluremi, Y. Temilola, Ogunjimi, D, Contribution of NDM and OXA-type carbapenemases to carbapenem resistance in clinical Acinetobacter baumannii from Nigeria, 2020, Infectious Diseases. [CrossRef]
- Emmanuel C. Eze1, Mohamed E. El Zowalaty and Manormoney Pillay. Medical Microbiology, Laboratory Medicine and Medical Sciences, College of Health Sciences. Antibiotic resistance and biofilm formation of Acinetobacter baumannii isolated from high risk effluent water in tertiary hospitals in South Africa, 2021, Journal of Global Antimicrobial Resistance. [CrossRef]
- Mizan Kindu, Lemma Derseh, Baye Gelaw, Feleke Moges. Carbapenemase-Producing Non-Glucose-Fermenting Gram-Negative Bacilli in Africa, Pseudomonas aeruginosa and Acinetobacter baumannii: A Systematic Review and Meta-Analysis. Hindawi. International Journal of Microbiology. Volume 2020, Article ID 9461901, 18 pages. [CrossRef]
- Rao MR, Urs TA, Chitharagi VB, et al. Rapid identification of carbapenemases by CarbAcineto NP test and the rate of beta-lactamases among Acinetobacter baumannii from a teaching hospital. Iranian Journal of Microbiology. 2022 Apr;14(2):174-180. [CrossRef] [PubMed]
- Okalla Ebongue, Cecile & Mengue, Emmanuel & Jean Pierre, Nda Mefoo & Tsiazok, Martial & Raymond, N'GUESSAN & Ngo Bum, Elisabeth. (2015). Antimicrobial Multi-Resistance of Acinetobacter baumanii Isolated from Clinical Specimens in Douala (Cameroon). Journal of Diseases and Medicinal Plants. Vol. 1. pp. 31-36. [CrossRef]
- Castilho SRA, Godoy CSM, Guilarde AO, Cardoso JL, André MCP, Junqueira-Kipnis AP, Kipnis A. Acinetobacter baumannii strains isolated from patients in intensive care units in Goiânia, Brazil: Molecular and drug susceptibility profiles. PLoS One. 2017 ;12(5):e0176790. 5 May. [CrossRef] [PubMed]
- Venkataraman R, Yadav U. Catheter-associated urinary tract infection: an overview. J Basic Clin Physiol Pharmacol. 2022 Aug 29;34(1):5-10. [CrossRef] [PubMed]
- Oikonomou O., Sarrou S., Papagiannitsis C. C, et al. Rapid dissemination of colistin and carbapenem resistant Acinetobacter baumannii in central Greece: mechanisms of resistance, molecular identification and epidemiological data. BMC Infectious Diseases. 2015;15:p. 559. doi: 10.1186/s12879-015-1297-x. [PMC free article] [PubMed] [CrossRef] [Google Scholar] [Ref list]. [CrossRef]
- Perovic O., Chetty V. Antimicrobial Resistance Surveillance from sentinel public hospitals, South Africa. Commun Dis Surveill Bull. 2015;14:56–67. [Google Scholar] [Ref list].
- Anane YA, Apalata T, Vasaikar S, Okuthe GE, Songca S. Molecular Detection of Carbapenemase-Encoding Genes in Multidrug-Resistant Acinetobacter baumannii Clinical Isolates in South Africa. Int J Microbiol. 2020 Jun 13;2020:7380740. [CrossRef] [PubMed]
- Mohammed, M. A. et al. Propranolol, chlorpromazine and diclofenac restore susceptibility of extensively drug-resistant (XDR)-Acinetobacter baumannii to fluoroquinolones. PLoS ONE 15, e0238195. [CrossRef]
- Verma, P. , Maurya, P., Tiwari, M. & Tiwari, V. In-silico interaction studies suggest RND efflux pump mediates polymyxin resistance in Acinetobacter baumannii. J. Biomol. Struct. Dyn. 37, 95–103. [CrossRef]
- Asif, M. , Alvi, I. A. & Rehman, S. U. In sight into Acinetobacter baumannii: pathogenesis, global resistance, mechanisms of resistance, treatment options, and alternative modalities. Infect. Drug Resist. 11, 1249. [CrossRef]
- Abd El-Baky, R. M. et al. Antimicrobial resistance pattern and molecular epidemiology of ESBL and MBL producing Acinetobacter baumannii isolated from hospitals in Minia. Egypt. Alex Med. 56, 4–13. [CrossRef]
- Tunyapanit W., Pruekprasert P., Laoprasopwattana K., Chelae S. Antimicrobial susceptibility of Acinetobacter baumannii isolated from hospital patients. ScienceAsia. 2014;40(1):28–34. doi: 10.2306/scienceasia1513-1874.2014.40.028. [CrossRef] [Google Scholar]. [CrossRef]
- D. van Duin and Y. Doi, “The global epidemiology of carbapenemase-producing Enterobacteriaceae,” Virulence, vol. 8, no. 4, pp. 460–469, 2017. View at: Publisher Site | Google Scholar.
- L. Dortet, L. Poirel, and P. Nordmann, “Worldwide dissemination of the NDM-type carbapenemases in Gram-negative bacteria,” BioMed Research International, vol. 2014, Article ID 249856, 12 pages, 2014. View at: Publisher Site | Google Scholar.
- H. Solgi, F. Badmasti, C. G. Giske, S. Aghamohammad, and F. Shahcheraghi, “Molecular epidemiology of NDM-1-and OXA-48-producing Klebsiella pneumoniae in an Iranian hospital: clonal dissemination of ST11 and ST893,” Journal of Antimicrobial Chemotherapy, vol. 73, no. 6, pp. 1517–1524, 2018. View at: Publisher Site | Google Scholar.
- McConnell M.J., Actis L., Pachon J. Acinetobacter baumannii: Human infections, factors contributing to pathogenesis and animal models. FEMS Microbiol. Rev. 2013;37:130–155. doi: 10.1111/j.1574-6976.2012.00344.x. [PubMed] [CrossRef] [Google Scholar] [Ref list]. [CrossRef]
- CLSI. Performance standards for antimicrobial susceptibility testing. Twentieth informational supplement, document M100s-S27. Clinical and Laboratory Standards Institute. Wayne, PA. USA (2017).
- Giani T, Tascini C, Arena F, Ciullo I, Conte V, Leonildi A, et al. Rapid detection of intestinal carriage of Klebsiella pneumoniae producing KPC carbapenemase during an outbreak. J Hosp Infect. 2012;81(2):119–22. [CrossRef]
- Franklin C, Liolios L, and Peleg AY. 2006. Phenotypic detection of carbapenem-susceptible metallo-β-lactamase-producing gram-negative bacilli in the clinical laboratory. J. Clin. Microbiol. 44:3139–3144. [CrossRef]
- Lowe M, Ehlers MM, Ismail F, Peirano G, Becker PJ, Pitout JDD, et al. Acinetobacter baumannii: epidemiological and beta-lactamase data from two tertiary academic hospitals in Tshwane, South Africa. Front Microbiol 2018;9:1280. [CrossRef]
Figure 1.
Susceptibility profile of Acinetobacter baumanii isolates to beta-lactams.
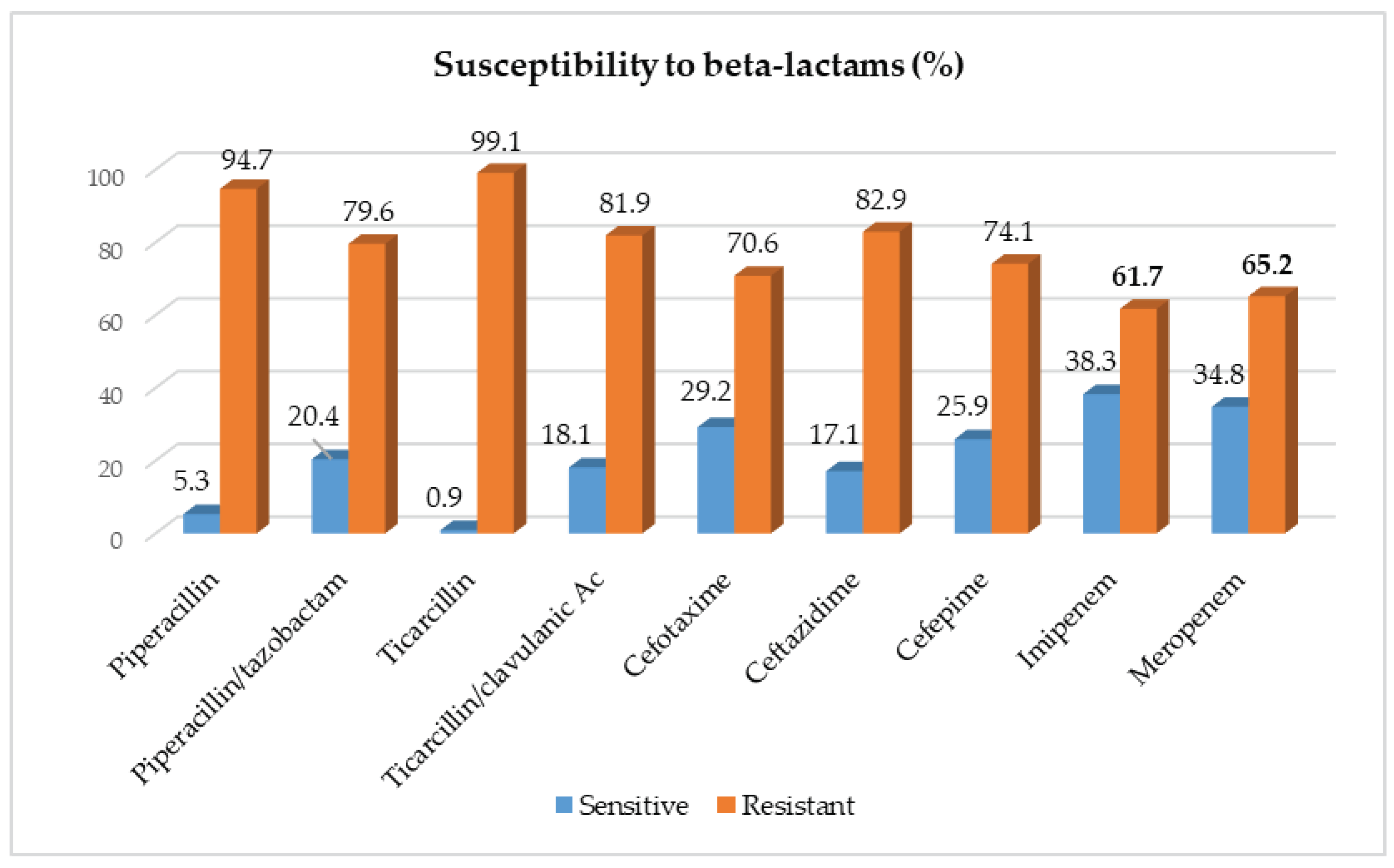
Figure 2.
Susceptibility profile of Acinetobacter baumanii isolates to others families of antibiotics.
Figure 2.
Susceptibility profile of Acinetobacter baumanii isolates to others families of antibiotics.
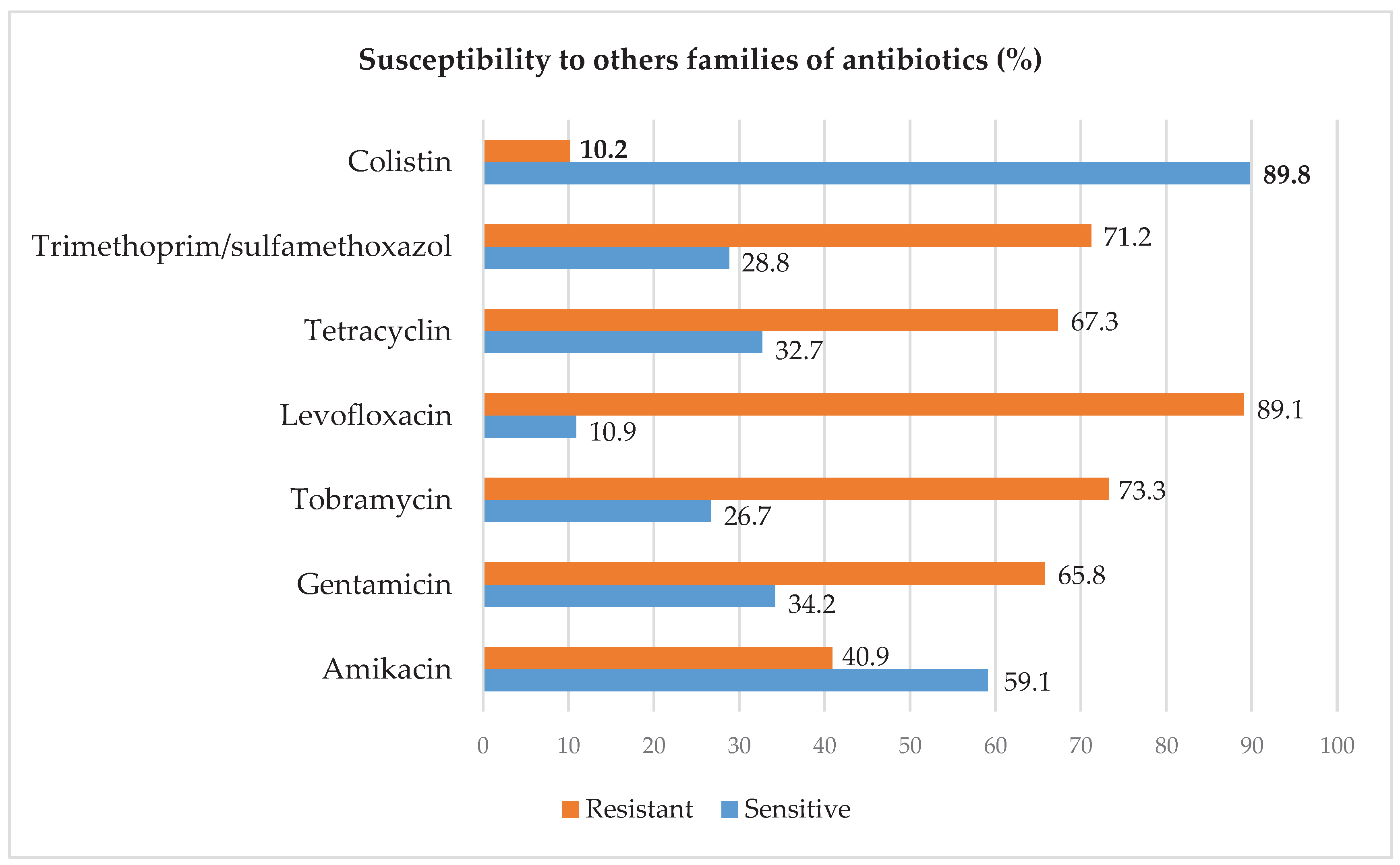
Figure 3.
Prevalence and classification of carbapenemase producing Acinetobacter baumanii.
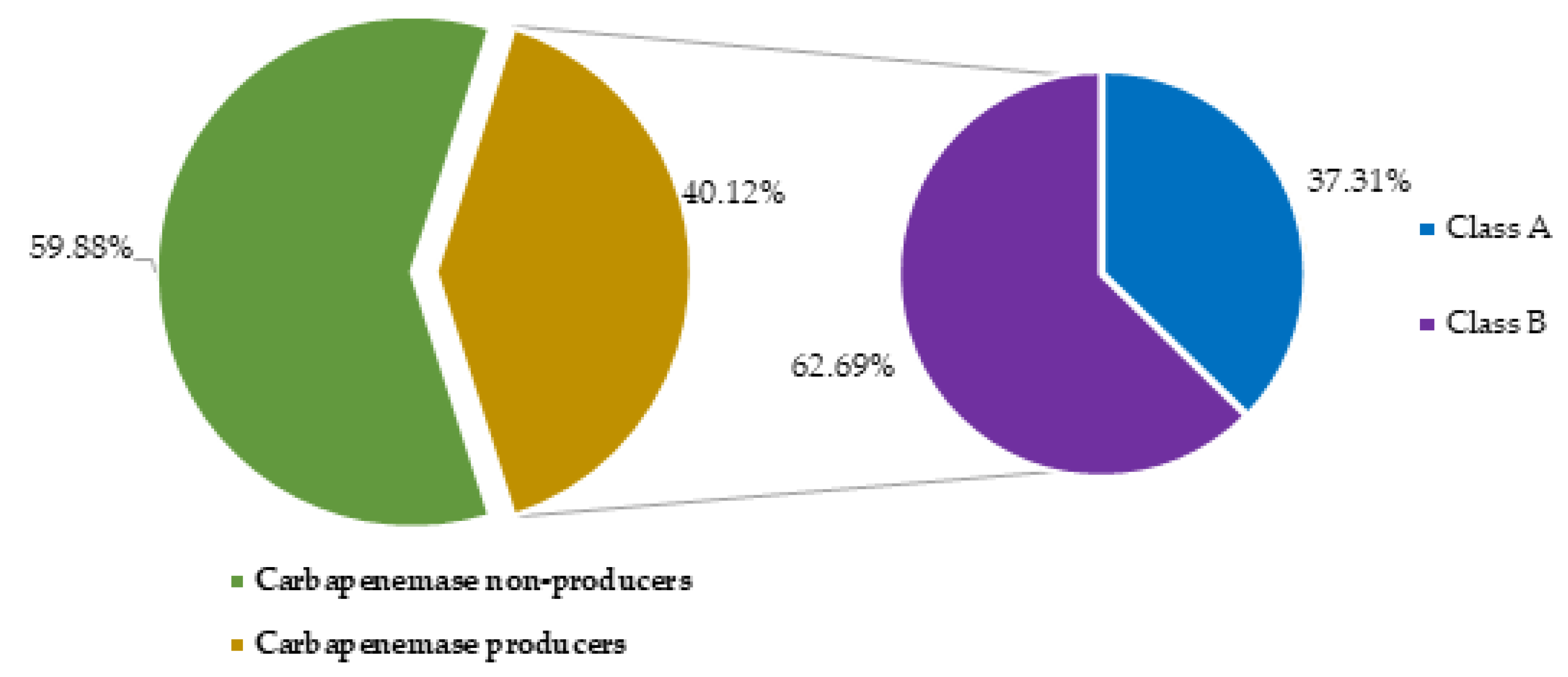

Table 1.
Frequency distribution of AB isolates according to source characteristics.
| Characteristcs | Categories | Number (N=167) | Percentage (%) |
| <10 | 29 | 17.37 | |
| Partcipant’s age (years) | [10-39[ | 92 | 55.09 |
| 40≤ | 46 | 27.54 | |
| Participant’s gender | Female | 79 | 47.31 |
| Male | 88 | 52.69 | |
| DSMPH | 14 | 8.38 | |
| Health care facility | HGY | 20 | 11.98 |
| HMR1 | 15 | 8.98 | |
| Laquintinie | 118 | 70.66 | |
| Urine | 44 | 26.35 | |
| Sample type | Blood | 37 | 22.16 |
| Vaginal swab | 8 | 4.79 | |
| Pus | 78 | 46.71 | |
| Antibiotherapy | Non | 66 | 39.52 |
| Oui | 101 | 60.48 | |
| Frequent hospitalisation | Non | 85 | 50.90 |
| Oui | 82 | 49.10 |
Table 2.
Distribution of carbapenemase producing Acinetobacter baumanii according to source characteristics.
Table 2.
Distribution of carbapenemase producing Acinetobacter baumanii according to source characteristics.
| Characteristics | CPAB | P-value | ||||
| N | n | n/N(%) | ||||
| Total | 167 | 67 | 100 | - | ||
| Age | <10 | 29 | 15 | 51.72 | ||
| [10-39] | 92 | 32 | 34.78 | 0.23 | ||
| 40≤ | 46 | 20 | 43.48 | |||
| Gender | Female | 79 | 26 | 32.91 | 0.07 | |
| Male | 88 | 41 | 46.59 | |||
| Health care facility | DSMPH | 14 | 0 | 0.00 | ||
| HGY | 20 | 0 | 0.00 | |||
| HMR1 | 15 | 8 | 53.33 | 0.81 | ||
| Laquintinie | 118 | 59 | 50.00 | |||
| Urine | 44 | 23 | 52.27 | |||
| Sample type | Blood | 37 | 17 | 45.95 | 0.11 | |
| Vaginal swab | 8 | 2 | 25.00 | |||
| Pus | 78 | 25 | 32.05 | |||
Table 3.
Univariate analysis of risk factors related to carbapenemase producing Acinetobacter baumanii.
Table 3.
Univariate analysis of risk factors related to carbapenemase producing Acinetobacter baumanii.
| Variables | Categories | Carbapenemase producing Acinetobacter baumanii | OR (95%CI) | P-value |
| n (%) | ||||
| Antibiotherapy | No | 2 (3.03) | 1 | Ref |
| Yes | 65 (64.36) | 57.78 (13.35-250.07) | <0.0001 | |
| Hospial food consumption | No | 55 (40.15) | 1 | Ref |
| Yes | 12 (40.00) | 0.99 (0.44-2.23) | 0.99 | |
| Frequent hospitalisation | No | 5 (5.88) | 1 | Ref |
| Yes | 62 (75.61) | 49.60 (17.63-139.57) | <0.0001 | |
| Using common toilet | No | 2 (20.00) | 1 | Ref |
| Yes | 65 (41.40) | 2.83 (0.58-13.74) | 0.32 |
Table 4.
Multivariate analysis of risk factors related to carbapenemase producing Acinetobacter baumanii.
Table 4.
Multivariate analysis of risk factors related to carbapenemase producing Acinetobacter baumanii.
| Variables | Categories | Ajusted-OR (95%CI) | P-value |
| Antibiotherapy | No | 1 | Ref |
| Yes | 6.00 (0.92-38.98) | 0.06 | |
| Frequent hospitalisation | No | 1 | Ref |
| Yes | 16.53 (4.36-62.66) | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



