Submitted:
28 March 2023
Posted:
29 March 2023
You are already at the latest version
Abstract
Background: Pathologic complete response (pCR) of breast cancer after neoadjuvant chemotherapy (NAC) is highly related to molecular subtypes. Patients who achieved tumor pCR after NAC have a better prognosis. However, despite of better prognosis, pCR patients have a potential for recurrence. There is little evidence of risk factors of recurrence in patients with pCR. We aim to analyze factors associated with tumor recurrence in patients who achieved pCR. Methods: This study retrospectively reviewed the data of patients diagnosed with breast cancer who achieved pCR after receiving NAC between January 2009 and December 2018 in Samsung Medical Center. pCR was defined as no residual invasive cancer in the breast and axillary nodes even if there is residual ductal carcinoma in situ (ypT0 or ypTis with ypN0). Breast cancers are classified into 4 subtypes based on hormone receptors (HR) and human epithelial growth factor receptor 2 (HER2) status. Patients who had bilateral breast cancer, inflammatory breast cancer, distant metastasis, unknown subtype, and histologically unique case were excluded from the study. Results: In total 483 patients were included in this study except for patients who corresponded to the exclusion criteria. The median follow-up duration was 59.0 months (range, 0.5-153.3 months). Breast cancer recurred in 4.1% of patients (20 of 483). There was a significant difference in clinical T (p = .004) and clinical N (p = .034) stage in the Kaplan-Meier curve for disease-free survival. Molecular subtypes (p = .573), Ki67 (p = 1.000), and breast surgery type (p = .574) were not associated with tumor recurrence in patients who achieved pCR after NAC. In the clinical T stage and clinical N stage, there was a significant difference between recurrence and no-recurrence groups (clinical T stage; p = .045, clinical N stage; p = .002). Univariable Cox regression revealed statistical significance in the clinical T stage (p = .049) and clinical N stage (p = .010), while multivariable Cox regression demonstrated non-significance in the clinical T stage (p = .320) and clinical N stage (p = .073). Conclusion: Results in this study showed that clinical T, clinical N stage, and molecular subtypes were not statistically significant predictors of recurrence in patients who achieved pCR after NAC. It is hypothesized that a multicenter-based study would lead to the identification of factors as predictors of recurrence after achieving pCR.
Keywords:
Breast Neoplasm
; Neoadjuvant Chemotherapy (NAC)
; pathologic Complete Response (pCR)
; Risk Factor
; recurrence
1. Introduction
Neoadjuvant chemotherapy (NAC) as a treatment for advanced breast cancer is generally practiced to increase the rate of breast-conserving surgery and minimize axillary surgery [1,2]. Also, NAC is advantageous in the assessment of the chemosensitivity of cancer [3]. According to former studies and randomized trials, the pathologic complete response (pCR) achieving rate after NAC ranges from 17% to 66%; the percentage varies mostly because of molecular subtypes and the different NAC regimens. Trastuzumab or pertuzumab for human epithelial growth factor receptor 2 (HER2) positive type tumor has demonstrated significantly improved pCR rate [4,5,6]. Importantly, patients who achieved tumor pCR after NAC have a higher opportunity of disease-free survival (DFS) and overall survival (OS) [7,8].
However, despite a higher opportunity to achieve pCR in patients who received NAC, a proportion of pCR achieved breast cancer still recurs (13-25%) [9,10]. Hence, it is necessitated to escalate the treatments after NAC for a portion of pCR-achieved patients with associated risk factors of recurrence. According to recent randomized control trials (RCTs), escalated treatments such as the administration of atezolizumab and pembrolizumab led to successful improvement in the oncologic outcomes in non-pCR breast cancer after NAC [11,12]. Also, these escalated treatments are believed to aid pCR-achieved patients in preventing cancer recurrence. However, these treatments are not the standard treatments for pCR-achieved patients due to a lack of sufficient evidence.
Therefore, it is hypothesized that the ascertainment of factors related to the recurrence of pCR achieving breast cancer after NAC would lead to recognition of the high-risk patients of breast cancer recurrence and aid in the escalation of treatments. We aimed to investigate the factors associated with breast cancer recurrence in pCR-achieving patients after NAC.
2. Maretials and Methods
2.1. Patients’ selection
We retrospectively reviewed the data of patients diagnosed with breast cancer who underwent a breast surgery at Samsung Medical Center between January 2009 and December 2018. Patients who achieved pCR after receiving preoperative NAC were included. Patients who were diagnosed with bilateral breast cancer and inflammatory breast cancer were excluded. In addition, patients who had ipsilateral supraclavicular or internal mammary lymph node metastasis, distant metastasis, unknown subtype, and histologically unique case like neuroendocrine differentiation were excluded.
2.2. Definition
The factors like age at diagnosis, type of surgery, clinical T stage and clinical N stage of tumors before receiving NAC, the molecular subtype of tumors, hormone receptors (HR) status (estrogen receptor (ER) status or progesterone receptor (PR) status), HER2 status and Ki67 expression, and axillary node metastasis were included in the study. The positivity of ER, PR, and HER2 was determined according to the American Society of Clinical Oncology/College of American Pathologists (ASCO/CAP) guidelines [13]. ER status and PR status were assessed by immunohistochemistry (IHC) and categorized as positive if there were at least 1% of stained cancer cells. HER2 was considered positive if there was evidence of protein overexpression (immunohistochemistry staining 3+) or gene amplification (fluorescent in situ hybridization with a HER2/CEP17 ratio ≥ 2 or average HER2 copy number ≥ 6 signals/cell) [14]. A low level of Ki67 expression was indicated as a percentage of cells with positive nuclei staining < 20% and a high level of Ki67 expression as ≥ 20% [15]. Axillary node positivity was determined by cytological metastasis in axillary fine needle aspiration biopsy. Breast cancers were classified into 4 subtypes based on the HR and HER2 status as follows: HR + / HER2 –, HR + / HER2 +, HR – / HER2 +, and triple-negative subtype (both HR – and HER2 –). pCR was defined as no residual invasive cancer in the breast and axillary nodes even if there is residual ductal carcinoma in situ (ypT0/is/ypN0). A locoregional recurrence (LRR) was defined as a local recurrence and a regional recurrence. A local recurrence was defined as a recurrence of ipsilateral breast, chest wall, and skin. A regional recurrence was defined as a recurrence of ipsilateral axillary, internal mammary, infraclavicular, and supraclavicular lymph nodes. A distant metastasis included only contralateral axillary, internal mammary, infraclavicular, and supraclavicular lymph nodes without contralateral breast cancer. Contralateral breast cancer was not included in the recurrence.
2.3. Statistical analyses
Patients’ characteristics were compared using the Chi-square test and Fisher’s exact test for categorical variables. Risk factor analysis was conducted using multivariable analysis with logistic regression. Statistical significance was established at p < .050. All statistical analyses were performed using the Statistical Analysis System (SAS) version 9.4 (SAS Institute Inc., Cary, NC, USA) and International Business Machines Corporation Statistical Package for the Social Sciences (IBM SPSS) Statistics Version 27.
2.4. IRB number
This study adhered to the ethical tenets of the Declaration of Helsinki and was approved by the Institutional Review Board (IRB) of SMC (IRB number: 2022-08-139). The need for informed consent was waived because of the retrospective nature of the study.
3. Results
3.1. Patients’ and tumor characteristics
Among the 2,316 included patients, a total of 560 patients who were diagnosed with breast cancer achieved pCR after receiving NAC between January 2009 and December 2018 at Samsung Medical Center. In total, 483 patients were included in this study except for patients who corresponded to the exclusion criteria. Of 483 patients in the study group, 20 patients had a recurrence of breast cancer (recurrence group) and 463 patients had no recurrence (no recurrence group) (Figure 1). The median follow-up duration was 59.0 months (range, 0.5-153.3 months). Most of the patients had clinical T2 stage in recurrence (50%) and no recurrence (68.5%) groups. In the recurrence group, most of the patients had clinical N2 stage (40%) and a maximum number of patients in the no recurrence group had clinical N0 stage (35.9%). There was a significant difference between the recurrence and no recurrence groups at the clinical T stage (p = .045 and clinical N stage (p = .002). Typically, 10% of the recurrence group and 11% of the no-recurrence group had types of HR+/HER2 – breast cancer. Whereas, 70% of the recurrence group and 58.3% of the other group had HER2 positivity. The proportion of triple-negative breast cancer (TNBC) was 20% in the recurrence group and 30.7% in the no-recurrence group. However, there was no statistically significant difference in the correlation between molecular subtypes and recurrence risk in patients who achieved pCR after NAC (p = .573). Ki67 (p = 1.000) and breast surgery type (p = .574) were also not associated with tumor recurrence (Table 1).
3.2. Clinicopathologic factors associated with RFS
Out of 483 patients who achieved pCR in the study group, 20 patients eventually developed a recurrence of cancer. In a univariable Cox regression analysis, the clinical T stage (p = .049) and clinical N stage (p = .010) were identified to be associated with recurrence. Molecular subtype (p = .584) and Ki67 (p = .857) were not statistically associated with recurrence. Treatments of breast cancer including breast surgery (p = .603), axillary surgery (p = .273), and adjuvant radiotherapy (p = .664) were not identified as factors of recurrence to be associated with recurrence-free survival (RFS). In a multivariable analysis which included variables with a p-value of < 0.05 on univariable analysis, the clinical T stage (p = .320) and clinical N stage (p = .073) were not statistically significant (Table 2).
3.3. Prognosis of pCR patients with clinicopathologic factors
The clinical T stage demonstrated a significant difference in the Kaplan-Meier curve for RFS (p = .004). The clinical N stage also exhibited a significant effect. (p = .034). However, molecular subtypes did not show any statistically significant effect on RFS (p = .394) (Figure 2).
3.4. Clinicopathologic characteristics of patients with a recurrence and metastases
The mean follow-up of RFS for 480 patients achieving pCR was 26.5 months (range, 6.0-92.1 months). Out of 483 patients achieving pCR, 20 finally developed a recurrence of cancer. Out of these 20 patients, 2 (10%) had HR + / HER2 – tumors, 14 (70%) had HER2 + tumors, and 4 (20%) had TNBC. Only 2 (10%) had clinical T1 tumors and 3 (15%) had clinical N0 tumors without any overlap. The other patients (75%) had clinical T2-4 or clinical N1-3 tumors. Ten patients (50%) developed LRR, 14 (70%) underwent distant metastases and among them, 4 (20%) had both. Six patients (30%) in the recurrence group finally expired due to breast cancer (Table 3).
4. Discussion
In this retrospective study, we demonstrated that the clinical T stage and clinical N stage were relative to the risk of breast cancer recurrence after achieving pCR following NAC in univariable Cox regression analysis. In addition, the Kaplan-Meier curve demonstrated the association between these factors and recurrence-free survival after achieving pCR. However, these factors were not correlative with a risk of tumor recurrence after achieving pCR in multivariable Cox regression analysis. In previous studies, the predictive significance of pre-NAC clinicopathological variables in pCR patients has been primarily evaluated [16,17,18]. These studies have demonstrated a relationship between the higher pre-NAC clinical stage and a higher risk of tumor recurrence after achieving pCR. Similarly, our results showed that pCR patients who had tumors with aggressive molecular subtypes such as HER2 + tumors or TNBC and more advanced tumors in terms of pre-NAC clinical T or clinical N stages had worse outcomes although it was not statistically significant.
In the literature, HER2 + breast cancer has demonstrated a higher risk of LRR and distant metastases even after achieving pCR [17,19,20,21]. Tanioka M. et al. showed that 88 (19.6%) of 449 patients achieved pCR after NAC and among 88 patients, 43 (48.9%) patients had HER2 + tumors. Through multivariate analysis, the HER2 + tumor was identified as a significant risk factor for recurrence after achieving pCR (HR, 5.0; p < .019) [20]. In addition, Liedtke C. et al. showed that 255 (20.1%) of 1,118 patients who had TNBC received NAC and they had significantly higher pCR achieving rates, compared with non-TNBC patients (22% vs. 11%; p = .034) [22]. In this study, the tendency of LRR and distant metastasis after achieving pCR was similar to previous studies; pCR achieving rates in HER2 + tumor and TNBC were high. However, these tumors still were associated with a recurrence including LRR and distant metastases after achieving pCR. Among 20 patients who developed recurrence after pCR, 10 patients had LRR. Among them, most of them had HER2 + tumors (8 patients) or TNBC (2 patients), and there were no patients with HR + / HER2 – tumors. Among 14 patients who had distant metastases after achieving pCR, 9 patients had HER2 + type, 3 patients had TNBC, and 2 patients had HR+ / HER2 – type. Furthermore, a pattern of expired patients due to breast cancer (6 of 483) was similar to that of the pattern of tumor recurrence after achieving pCR; HER2 + tumors (3 patients), TNBC (2 patients), and HR + / HER2 – (only 1 patient). This study supported the idea that HER2 + tumors and TNBC tend to achieve pCR and remain in a high-risk group, which has been constantly suggested in the literature [23,24].
In previous studies, other risk factors except for molecular subtypes of tumors have been reported. Young age, clinical T stage, and clinical N stage were referred to as risk factors for recurrence including LRR and distant metastases after achieving pCR [25,26,27,28,29,30,31]. According to Ishitobi M. et al., patients who were younger than 40 years at the time of diagnosis had significantly worse IBTR-free survival than those who were 40 years or older (5-year IBTR-free survival, 87.7 vs 96.9%; p = .002) [25]. Li-Yun Xie et al. identified that among 1,913 patients who received NAC, 420 achieved pCR (22.0%), and clinical T stage and clinical N stage were associated with tumor recurrence in the pCR achieving patients after NAC (hazard ratio: 2.57, 95% confidence interval: 1.01-6.51, p = .047 for clinical T stage, and hazard ratio: 3.48, 95% confidence interval: 1.37-8.83, p = .009 for clinical N stage) [31]. Comparatively, this study showed that age, clinical T, clinical N stage, and molecular subtypes were not statistically significant predictors of recurrence in patients who achieved pCR after NAC. A possible explanation for the different recurrent risk factors between this study and previous studies is the difference in the proportion of patients who received anti-HER2 targeted therapy. In this study, a portion of HER2 + patients did not receive anti-HER2 treatment because they were diagnosed before national insurance coverage of anti-HER2 targeted therapy. Thus they did not benefit from anti-HER2 treatment. Another explanation for age, clinical T stage, and clinical N stage are that the distribution of patients was unequal in the study groups. In the recurrence group, the total number of patients was only 20, which was too small to obtain a statistical significance, compared to the no recurrence group (n = 463).
Recently, progressive adjuvant treatments have been evaluated by RCTs such as the ExteNET trial. Adding neratinib, an irreversible pan-HER tyrosine kinase inhibitor, after neoadjuvant and adjuvant anti-HER2 treatment for patients with stage 2-3 HER2 + tumor resulted in favorable prognosis; hazard ratio: 0.58, 95% confidence interval: 0.41-0.82, p = .002 for 5-year invasive DFS, hazard ratio: 0.79, 95% confidence interval: 0.55-1.13, p = .203 for OS; but in HR + / HER + group the results were; hazard ratio: 0.60, 95% confidence interval: 0.33-1.07, p = .086 for 5-year invasive DFS, hazard ratio: 0.47, 95% confidence interval: 0.23-0.92, p = .031 for OS [32]. However, even though achieving pCR is undoubtedly a significant purpose for patients who received NAC, the toxicity of these treatments should not be ignored [33]. Thus, strict screening is mandatory to identify whether patients correspond to a high-risk group to minimize unnecessary adverse effects. Consequently, tailoring NAC for breast cancer patients is important to not only prevent recurrence but also avoid over-treatment for low-risk patients [34,35].
This study had several limitations. First, as this study was retrospective, some parts of the data were missing and none were replaceable. Second, the study lacked a sufficient number of patients who had a recurrence and distant metastasis after achieving pCR. A single-center study design was another limitation of this study. Consequently, further study with a sufficient number of patients in a multicenter is expected to demonstrate a correlation with recurrence rate and insignificant factors such as age, clinical T stage, clinical N stage, and molecular subtypes. Nevertheless, some tentative conclusions were achieved from this retrospective study. It is suggested that HER2 + tumors and TNBC have a high potential to achieve pCR, but these tumors remain in a high-risk group for recurrence. Therefore, patients with HER2 + tumors should be given additional treatments with a strict patient selection strategy to prevent over-treatment as well as achieve pCR.
Author Contributions
Conceptualization: Ryu JM; Data curation: Choi JY; Investigation: Chae BJ, Yu JH, Jang SY, Shin DS; Methodology: Lee JE, Kim SW, Nam SJ, Lee HJ, Kwak YJ; Supervision: Chae BJ, Yu JH, Lee JE, Kim SW, Nam SJ, Ryu JM; Visualization: Woen D; Writing - original draft: Choi JY, Woen D; Writing - review & editing: Ryu JM.
Conflicts of Interest
The authors declare that they have no competing interests.
References
- Caudle, A.S., et al., Local-regional control according to surrogate markers of breast cancer subtypes and response to neoadjuvant chemotherapy in breast cancer patients undergoing breast conserving therapy. Breast Cancer Res, 2012. 14(3): p. R83. [CrossRef]
- Long-term outcomes for neoadjuvant versus adjuvant chemotherapy in early breast cancer: meta-analysis of individual patient data from ten randomised trials. Lancet Oncol, 2018. 19(1): p. 27-39.
- Ikeda, T., et al., The role of neoadjuvant chemotherapy for breast cancer treatment. Breast Cancer, 2002. 9(1): p. 8-14. [CrossRef]
- Haque, W., et al., Response rates and pathologic complete response by breast cancer molecular subtype following neoadjuvant chemotherapy. Breast Cancer Res Treat, 2018. 170(3): p. 559-567. [CrossRef]
- Gianni, L., et al., 5-year analysis of neoadjuvant pertuzumab and trastuzumab in patients with locally advanced, inflammatory, or early-stage HER2-positive breast cancer (NeoSphere): a multicentre, open-label, phase 2 randomised trial. Lancet Oncol, 2016. 17(6): p. 791-800. [CrossRef]
- Schneeweiss, A., et al., Pertuzumab plus trastuzumab in combination with standard neoadjuvant anthracycline-containing and anthracycline-free chemotherapy regimens in patients with HER2-positive early breast cancer: a randomized phase II cardiac safety study (TRYPHAENA). Ann Oncol, 2013. 24(9): p. 2278-84. [CrossRef]
- Cortazar, P., et al., Pathological complete response and long-term clinical benefit in breast cancer: the CTNeoBC pooled analysis. Lancet, 2014. 384(9938): p. 164-72. [CrossRef]
- Orsaria, P., et al., Clinical Outcomes Among Major Breast Cancer Subtypes After Neoadjuvant Chemotherapy: Impact on Breast Cancer Recurrence and Survival. Anticancer Res, 2021. 41(5): p. 2697-2709. [CrossRef]
- Fisher, B., et al., Effect of preoperative chemotherapy on the outcome of women with operable breast cancer. J Clin Oncol, 1998. 16(8): p. 2672-85. [CrossRef]
- Wolmark, N., et al., Preoperative chemotherapy in patients with operable breast cancer: nine-year results from National Surgical Adjuvant Breast and Bowel Project B-18. J Natl Cancer Inst Monogr, 2001(30): p. 96-102. [CrossRef]
- Mittendorf, E.A., et al., Neoadjuvant atezolizumab in combination with sequential nab-paclitaxel and anthracycline-based chemotherapy versus placebo and chemotherapy in patients with early-stage triple-negative breast cancer (IMpassion031): a randomised, double-blind, phase 3 trial. Lancet, 2020. 396(10257): p. 1090-1100. [CrossRef]
- Schmid, P., et al., Pembrolizumab for Early Triple-Negative Breast Cancer. N Engl J Med, 2020. 382(9): p. 810-821. [CrossRef]
- Hammond, M.E., et al., American Society of Clinical Oncology/College Of American Pathologists guideline recommendations for immunohistochemical testing of estrogen and progesterone receptors in breast cancer. J Clin Oncol, 2010. 28(16): p. 2784-95. [CrossRef]
- Wolff, A.C., et al., Recommendations for human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American Pathologists clinical practice guideline update. J Clin Oncol, 2013. 31(31): p. 3997-4013. [CrossRef]
- Coates, A.S., et al., Tailoring therapies--improving the management of early breast cancer: St Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2015. Ann Oncol, 2015. 26(8): p. 1533-46. [CrossRef]
- Fei, F., et al., Tumour size is the only predictive factor of distant recurrence after pathological complete response to neoadjuvant chemotherapy in patients with large operable or locally advanced breast cancers: a sub-study of EORTC 10994/BIG 1-00 phase III trial. Eur J Cancer, 2015. 51(3): p. 301-9.
- Gonzalez-Angulo, A.M., et al., Factors predictive of distant metastases in patients with breast cancer who have a pathologic complete response after neoadjuvant chemotherapy. J Clin Oncol, 2005. 23(28): p. 7098-104. [CrossRef]
- O'Shaughnessy, J., et al., Recurrence rates in patients with HER2+ breast cancer who achieved a pathological complete response after neoadjuvant pertuzumab plus trastuzumab followed by adjuvant trastuzumab: a real-world evidence study. Breast Cancer Res Treat, 2021. 187(3): p. 903-913. [CrossRef]
- Broglio, K.R., et al., Association of Pathologic Complete Response to Neoadjuvant Therapy in HER2-Positive Breast Cancer With Long-Term Outcomes: A Meta-Analysis. JAMA Oncol, 2016. 2(6): p. 751-60.
- Tanioka, M., et al., Predictors of recurrence in breast cancer patients with a pathologic complete response after neoadjuvant chemotherapy. Br J Cancer, 2010. 103(3): p. 297-302.
- Chou, H.H., et al., Factors affecting locoregional recurrence in breast cancer patients undergoing surgery following neoadjuvant treatment. BMC Surg, 2021. 21(1): p. 160. [CrossRef]
- Liedtke, C., et al., Response to neoadjuvant therapy and long-term survival in patients with triple-negative breast cancer. J Clin Oncol, 2008. 26(8): p. 1275-81. [CrossRef]
- Wang-Lopez, Q., et al., Can pathologic complete response (pCR) be used as a surrogate marker of survival after neoadjuvant therapy for breast cancer? Crit Rev Oncol Hematol, 2015. 95(1): p. 88-104.
- Chica-Parrado, M.R., et al., Resistance to Neoadjuvant Treatment in Breast Cancer: Clinicopathological and Molecular Predictors. Cancers (Basel), 2020. 12(8). [CrossRef]
- Ishitobi, M., et al., Risk Factors for Ipsilateral Breast Tumor Recurrence in Triple-Negative or HER2-Positive Breast Cancer Patients Who Achieve a Pathologic Complete Response After Neoadjuvant Chemotherapy. Ann Surg Oncol, 2021. 28(5): p. 2545-2552. [CrossRef]
- Werutsky, G., et al., Locoregional recurrence risk after neoadjuvant chemotherapy: A pooled analysis of nine prospective neoadjuvant breast cancer trials. Eur J Cancer, 2020. 130: p. 92-101. [CrossRef]
- Swisher, S.K., et al., Locoregional Control According to Breast Cancer Subtype and Response to Neoadjuvant Chemotherapy in Breast Cancer Patients Undergoing Breast-conserving Therapy. Ann Surg Oncol, 2016. 23(3): p. 749-56. [CrossRef]
- Chaudry, M., et al., Recurrence and survival among breast cancer patients achieving a pathological complete response to neoadjuvant chemotherapy. Breast Cancer Res Treat, 2015. 153(2): p. 417-23. [CrossRef]
- Spring, L.M., et al., Pathologic Complete Response after Neoadjuvant Chemotherapy and Impact on Breast Cancer Recurrence and Survival: A Comprehensive Meta-analysis. Clin Cancer Res, 2020. 26(12): p. 2838-2848. [CrossRef]
- Liu, H., et al., Pathologic Complete Response and Its Impact on Breast Cancer Recurrence and Patient's Survival after Neoadjuvant Therapy: A Comprehensive Meta-Analysis. Comput Math Methods Med, 2021. 2021: p. 7545091. [CrossRef]
- Xie, L.Y., et al., Markers Associated With Tumor Recurrence in Patients With Breast Cancer Achieving a Pathologic Complete Response After Neoadjuvant Chemotherapy. Front Oncol, 2022. 12: p. 860475. [CrossRef]
- Chan, A., et al., Final Efficacy Results of Neratinib in HER2-positive Hormone Receptor-positive Early-stage Breast Cancer From the Phase III ExteNET Trial. Clin Breast Cancer, 2021. 21(1): p. 80-91.e7. [CrossRef]
- Poggio, F., et al., Platinum-based neoadjuvant chemotherapy in triple-negative breast cancer: a systematic review and meta-analysis. Ann Oncol, 2018. 29(7): p. 1497-1508. [CrossRef]
- Li, X., et al., Tailoring neoadjuvant chemotherapy for patients with breast cancer who have achieved pathologic complete response. Transl Cancer Res, 2020. 9(2): p. 1205-1214. [CrossRef]
- Hassett, M.J., et al., Neoadjuvant treatment strategies for HER2-positive breast cancer: cost-effectiveness and quality of life outcomes. Breast Cancer Res Treat, 2020. 181(1): p. 43-51. [CrossRef]
Figure 1.
Schematic diagram for the inclusion of participants. Abbreviations: NAC = neoadjuvant chemotherapy, SMC = Samsung medical center, pCR = pathologic complete response, SCN = supraclavicular node, IMN = internal mammary node.
Figure 1.
Schematic diagram for the inclusion of participants. Abbreviations: NAC = neoadjuvant chemotherapy, SMC = Samsung medical center, pCR = pathologic complete response, SCN = supraclavicular node, IMN = internal mammary node.
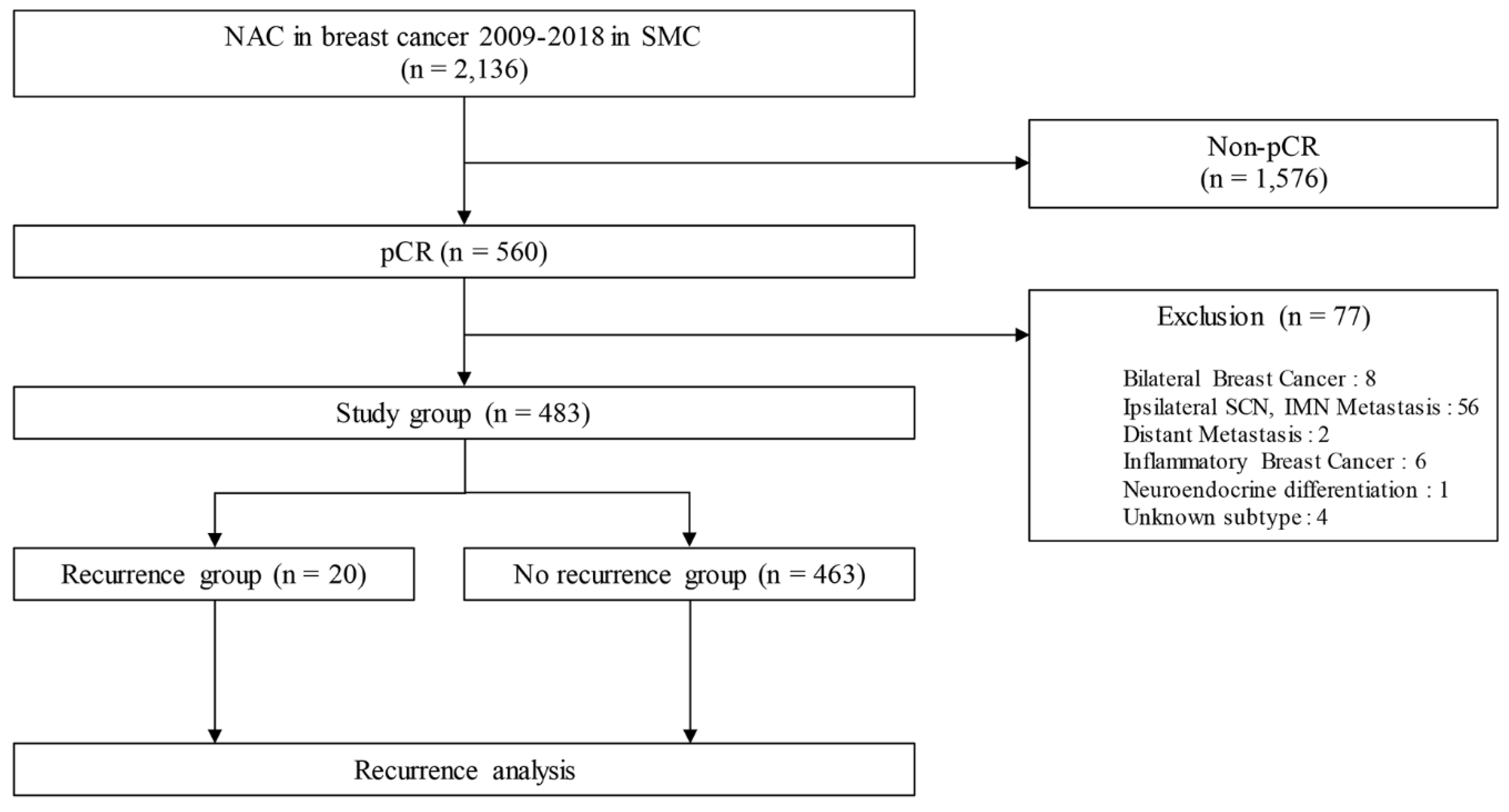
Figure 2.
Comparison of recurrence-free survival (RFS) rate in the pCR group with cT stage (A), cN stage (B), and molecular subtypes (C). Abbreviations: pCR = pathologic complete response, HR = hormone receptors, HER2 = human epithelial growth factor receptor 2.
Figure 2.
Comparison of recurrence-free survival (RFS) rate in the pCR group with cT stage (A), cN stage (B), and molecular subtypes (C). Abbreviations: pCR = pathologic complete response, HR = hormone receptors, HER2 = human epithelial growth factor receptor 2.
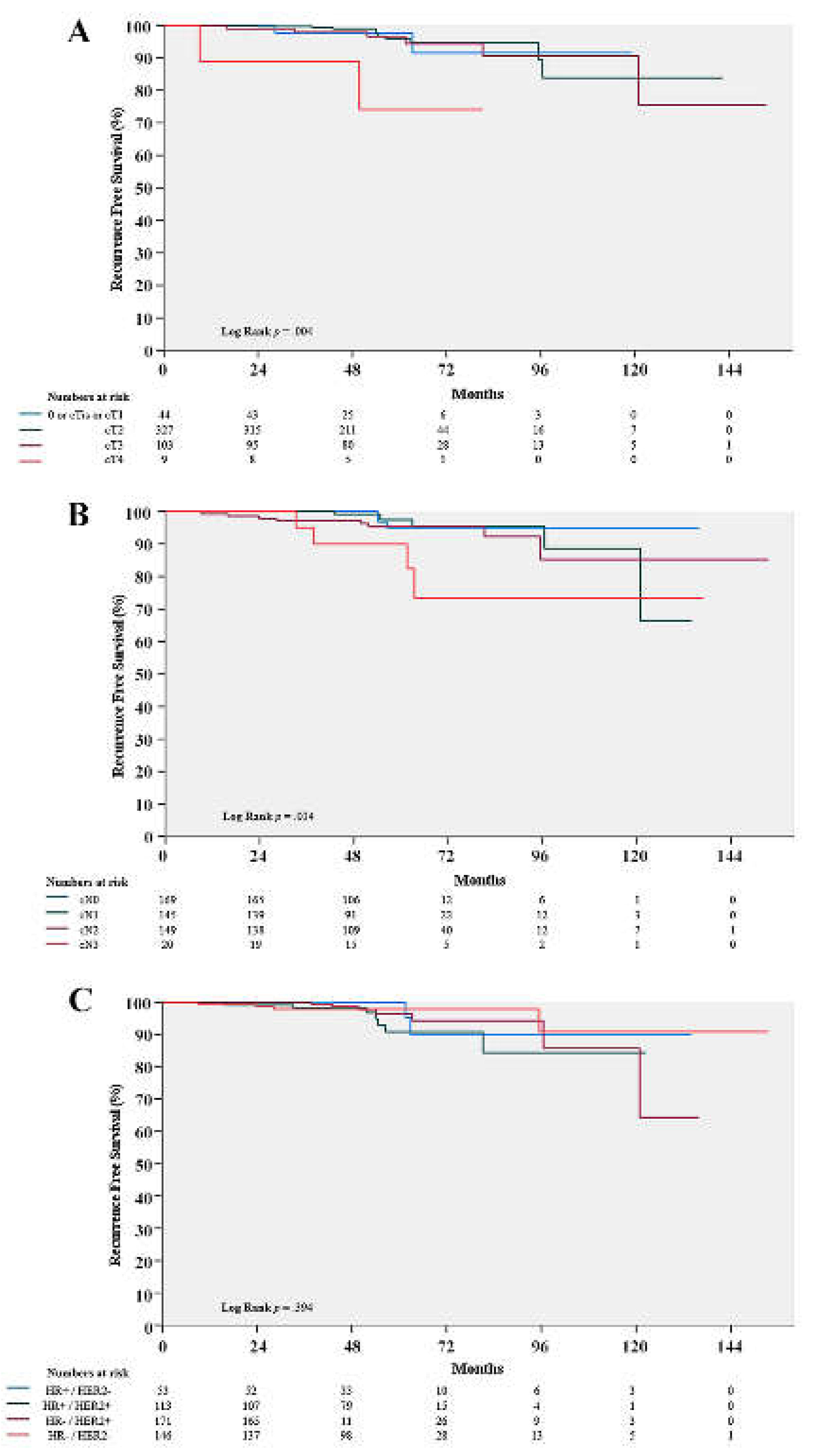

Table 1.
Clinicopathologic characteristics of patients.
| Characteristics | Recurrence No. (%) N = 20 (4.1) |
No Recurrence No. (%) N = 463 (95.9) |
% | p-value | |
|---|---|---|---|---|---|
| Mean F/U duration (month) | 59.0 (0.5 - 153.3) | ||||
| Age at diagnosis (years) | 0.162 | ||||
| ≤ 35 | 2 (10.0) | 58 (12.5) | 12.4 | ||
| 36 - 50 | 6 (30.0) | 226 (48.8) | 48.0 | ||
| > 50 | 12 (60.0) | 179 (38.7) | 39.5 | ||
| Clinical T stage | 0.045 | ||||
| cT0 or Tis or T1 | 2 (10.0) | 42 (9.1) | 9.1 | ||
| cT2 | 10 (50.0) | 317 (68.5) | 67.7 | ||
| cT3 | 6 (30.0) | 97 (21.0) | 21.3 | ||
| cT4 | 2 (10.0) | 7 (1.5) | 1.9 | ||
| Clinical N stage | 0.002 | ||||
| cN0 | 3 (15.0) | 166 (35.9) | 35.0 | ||
| cN1 | 5 (25.0) | 140 (30.2) | 30.0 | ||
| cN2 | 8 (40.0) | 141 (30.5) | 30.8 | ||
| cN3 | 4 (20.0) | 16 (3.5) | 4.1 | ||
| FNA of metastatic lymph node | 0.450 | ||||
| negative by proven Bx | 4 (20.0) | 106 (22.9) | 22.8 | ||
| positive by proven Bx | 13 (65.0) | 235 (50.8) | 51.3 | ||
| Did not Bx | 3 (15.0) | 122 (26.3) | 25.9 | ||
| Molecular subtype at diagnosis | 0.573 | ||||
| HR+ / HER2- | 2 (10.0) | 51 (11.0) | 11.0 | ||
| HR+ / HER2+ | 7 (35.0) | 106 (22.9) | 23.4 | ||
| HR- / HER2+ | 7 (35.0) | 164 (35.4) | 35.4 | ||
| HR- / HER2- (TNBC) | 4 (20.0) | 142 (30.7) | 30.2 | ||
| Ki67 at diagnosis | 1.000 | ||||
| < 20% | 2 (10.0) | 51 (11.0) | 11.0 | ||
| ≥ 20% | 18 (90.0) | 407 (87.9) | 88.0 | ||
| Unknown | 0 (0.0) | 5 (1.1) | 1.0 | ||
| Breast surgery | 0.574 | ||||
| Mastectomy | 5 (25.0) | 93 (20.1) | 20.3 | ||
| BCS | 15 (75.0) | 370 (79.9) | 79.7 | ||
| Axillary surgery | 0.189 | ||||
| SLNB only | 12 (60.0) | 346 (74.7) | 74.1 | ||
| ALND | 8 (40.0) | 117 (25.3) | 25.9 | ||
| Adjuvant RT | 0.665 | ||||
| Yes | 18 (90.0) | 427 (92.2) | 92.1 | ||
| No | 2 (10.0) | 36 (7.8) | 7.9 | ||
| NAC regimen | 0.020 | ||||
| AC | 0 (0.0) | 13 (2.8) | 2.7 | ||
| T | 0 (0.0) | 4 (0.9) | 0.8 | ||
| AC+T | 9 (45.0) | 240 (51.8) | 51.6 | ||
| ACTH | 5 (25.0) | 19 (4.1) | 5.0 | ||
| TCHP | 6 (30.0) | 139 (30.0) | 30.0 | ||
| Others | 0 (0.0) | 48 (10.4) | 9.9 | ||
Abbreviations: F/U, follow-up; FNA, fine needle aspiration; Bx, biopsy; HR, hormone receptors; HER2, human epithelial growth factor receptor 2; TNBC, triple-negative breast cancer; BCS, breast-conserving surgery; SLNB, sentinel lymph node biopsy; ALND, axillary lymph node dissection; RT, radiotherapy; NAC, neoadjuvant chemotherapy; AC, Adriamycin Cyclophosphamide; T, Taxane; AC+T, Adriamycin Cyclophosphamide + Taxane; ACTH, Adriamycin Cyclophosphamide Taxane Herceptin(trastuzumab); TCHP, Taxane Carboplatin Herceptin(trastuzumab) Perjeta(pertuzumab).
Table 2.
Univariable and multivariable Cox regression.
| Characteristics | Hazard ratio | 95% CI | p-value | Hazard ratio | 95% CI | p-value | |
|---|---|---|---|---|---|---|---|
| Age at diagnosis (years) | 0.141 | ||||||
| ≤ 35 | 1.19 | 024 - 5.90 | 0.836 | ||||
| 36 - 50 | 1 | ||||||
| > 50 | 2.57 | 0.96 - 6.85 | 0.060 | ||||
| Clinical T stage | 0.049 | 0.320 | |||||
| cT0 / cTis / cT1 | 1 | 1 | |||||
| cT2 | 0.66 | 0.14 - 3.02 | 0.594 | 0.83 | 0.18 - 3.84 | 0.807 | |
| cT3 | 1.2 | 0.24 - 5.95 | 0.826 | 1.19 | 0.24 - 5.91 | 0.830 | |
| cT4 | 5.64 | 0.79 - 40.11 | 0.084 | 4.14 | 0.54 - 31.8 | 0.172 | |
| Clinical N stage | 0.010 | 0.073 | |||||
| cN0 | 1 | 1 | |||||
| cN1 | 1.9 | 0.45 - 7.97 | 0.379 | 1.75 | 0.41 - 7.38 | 0.449 | |
| cN2 | 2.9 | 0.77 - 10.94 | 0.117 | 2.89 | 0.76 - 10.93 | 0.119 | |
| cN3 | 10.93 | 2.44 - 48.94 | 0.002 | 7.35 | 1.47 - 36.82 | 0.015 | |
| Molecular subtype at diagnosis | 0.584 | ||||||
| HR+ / HER2- | 1 | ||||||
| HR+ / HER2+ | 1.75 | 0.36 - 8.45 | 0.488 | ||||
| HR- / HER2+ | 1.15 | 0.24 - 5.56 | 0.861 | ||||
| HR- / HER2- (TNBC) | 0.75 | 0.14 - 4.09 | 0.738 | ||||
| Ki67 at diagnosis | |||||||
| < 20% | 1 | ||||||
| ≥ 20% | 1.14 | 0.27 - 4.93 | 0.857 | ||||
| Breast surgery | |||||||
| Mastectomy | 1 | ||||||
| BCS | 0.76 | 0.28 - 2.10 | 0.603 | ||||
| Axillary surgery | |||||||
| SLNB only | 1 | ||||||
| ALND | 1.66 | 0.67 - 4.13 | 0.273 | ||||
Abbreviations: BCS, breast-conserving surgery; SLNB, sentinel lymph node biopsy; ALND, axillary lymph node dissection; HR, hormone receptor; HER2, human epithelial growth factor receptor 2; TNBC, triple-negative breast cancer; RT, radiotherapy.
Table 3.
Characteristics of patients with recurrence.
| Initial diagnosis | State at recurrence | Initial treatment information | Expire | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No. | Age (years) | HR | HER2 | cT | cN | Ki67 | LRR | Distant metastasis | RFS (months) | Breast OP | Axilla OP | Adjuvant RT | |
| 1 | 32 | + | - | cT2 | cN1 | ≥ 20% | sternum, lung | 16.6 | mastectomy | SLNB only | - | - | |
| 2 | 50 | + | - | cT3 | cN3 | < 20% | sternum, lung, Rt paratracheal LN | 37.8 | mastectomy | ALND | + | + | |
| 3 | 52 | + | + | cT3 | cN2 | ≥ 20% | brain | 13.3 | mastectomy | SLNB only | + | - | |
| 4 | 55 | + | + | cT3 | cN2 | ≥ 20% | ipsilateral SCN | C6-spine, vertebral cervical LN | 47.5 | BCS | ALND | + | - |
| 5 | 45 | + | + | cT3 | cN2 | ≥ 20% | brain | 6.3 | BCS | SLNB only | + | - | |
| 6 | 56 | + | + | cT2 | cN0 | ≥ 20% | ipsilateral breast | contralateral ALN | 46.8 | BCS | SLNB only | + | + |
| 7 | 50 | + | + | cT2 | cN1 | ≥ 20% | ipsilateral breast | 8.9 | BCS | SLNB only | + | - | |
| 8 | 58 | + | + | cT2 | cN0 | < 20% | ipsilateral SCN | 45.0 | BCS | ALND | + | - | |
| 9 | 56 | + | + | cT3 | cN3 | ≥ 20% | brain | 6.0 | BCS | SLNB only | + | + | |
| 10 | 45 | - | + | cT2 | cN1 | ≥ 20% | brain | 20.5 | BCS | ALND | + | - | |
| 11 | 38 | - | + | cT2 | cN1 | ≥ 20% | ipsilateral breast | 12.3 | BCS | SLNB only | + | - | |
| 12 | 53 | - | + | cT4 | cN2 | ≥ 20% | ipsilateral breast | contralateral ALN | 30.8 | BCS | ALND | + | - |
| 13 | 44 | - | + | cT3 | cN1 | ≥ 20% | ipsilateral breast | 9.1 | mastectomy | ALND | + | - | |
| 14 | 60 | - | + | cT2 | cN3 | ≥ 20% | lung, mediastinum | 20.5 | BCS | SLNB only | + | - | |
| 15 | 52 | - | + | cT1 | cN3 | ≥ 20% | brain | 29.1 | BCS | ALND | + | + | |
| 16 | 61 | - | + | cT2 | cN0 | ≥ 20% | ipsilateral breast | 49.2 | BCS | SLNB only | + | - | |
| 17 | 55 | - | - | cT4 | cN2 | ≥ 20% | brain | 8.2 | mastectomy | ALND | - | - | |
| 18 | 32 | - | - | cT2 | cN2 | ≥ 20% | ipsilateral breast | 92.1 | BCS | SLNB only | + | + | |
| 19 | 42 | - | - | cT1 | cN2 | ≥ 20% | ipsilateral breast/ALN | brain, paratracheal LN | 12.8 | BCS | SLNB only | + | - |
| 20 | 60 | - | - | cT2 | cN2 | ≥ 20% | brain | 17.0 | BCS | SLNB only | + | + | |
Abbreviations: HR, hormone receptor; HER2, human epithelial growth factor receptor 2; LRR, locoregional recurrence; RFS, recurrence-free survival; OP, operation; RT, radiotherapy; SLNB, sentinel lymph node; Rt, right; ALND, axillary lymph node dissection; LN, lymph node; SCN, supraclavicular node; ALN, axillary lymph node; BCS, breast-conserving surgery.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



