
Submitted:
29 March 2023
Posted:
30 March 2023
You are already at the latest version
Abstract
Purpose: Hearing assistive technology (HAT) has been shown to be a viable solution to the speech-in-noise perception (SPIN) issue in children with autism spectrum disorder (ASD); however, little is known about its efficacy in tonal language speakers. This study compared sentence-level SPIN performance between Chinese children with ASD and neurotypical (NT) children and evaluated HAT use in improving SPIN performance and easing SPIN difficulty. Methods: Children with ASD (n=26) and NT children (n=19) aged 6-12 performed two adaptive tests in steady-state noise and three fixed-level tests in quiet and steady-state noise with and without using HAT. Speech recognition thresholds (SRT) and accuracy rates were assessed using adaptive and fixed-level tests, respectively. Parents or teachers of the ASD group completed a questionnaire regarding children’s listening difficulty under six circumstances before and after a ten-day trial period of HAT use. Results: Although the two groups of children had comparable SRTs, the ASD group showed a significantly lower SPIN accuracy rate than the NT group. Also, a significant impact of noise was found in the ASD group’s accuracy rate, but not in the NT group’s. There was a general improvement in the ASD group’s SPIN performance with HAT and a decrease in their listening difficulty ratings across all conditions after the device trial. Conclusion: The findings indicated inadequate SPIN in the ASD group using a relatively sensitive measure to gauge SPIN performance among children. The markedly increased accuracy rate in noise during HAT-on sessions for the ASD group confirmed the feasibility of HAT for improving SPIN performance in controlled laboratory settings, and the reduced post-use ratings of listening difficulty further confirmed the benefits of HAT use in daily scenarios.
Keywords:
Autism spectrum disorder
; Auditory stream segregation
; Hearing assistive technology
; Speech-in-noise perception
; Tonal language speakers
Introduction
Autism spectrum disorder (ASD) is a pervasive neurodevelopmental disorder characterized by persistent social communication and interaction deficiencies across multiple scenarios (American Psychiatric Association, 2013). One outstanding issue associated with the difficulty with social communication and interaction is unusual sensory responsivity. Despite having normal hearing, a considerable number of children with ASD reported classroom noises as explicitly agonizing sensory experiences (Cooperative Research Centre for Living with Autism, 2018) and exhibited varying degrees of speech-in-noise perception (SPIN) issues (for a review, see O'Connor, 2012), which notably hindered their academic advancement and undermines their quality of life. The inadequacy of coping with classroom noises and perceiving speech with distracting sounds in the background could be implicated in higher-level linguistic and cognitive problems in individuals with ASD. Several studies have documented a correlation between disadvantaged SPIN and early language delays in children and adolescents with autism (Arunachalam & Luyster, 2016; Eigsti & Fein, 2013; Kujala et al., 2010). There is also evidence that an individual’s SPIN ability interplays with executive functions, including attention, inhibitory control, and working memory (Dryden et al., 2017; Perrone-Bertolotti et al., 2017). Considering the potential influences on language, cognitive, and social development, it is important to study the nature of the excessive variability in SPIN in ASD and how to ameliorate the problem.
Auditory Stream Segregation and Hearing Assistive Technology
Atypical SPIN can arise from incomplete auditory stream segregation of simultaneous sound sources; that is, individuals with ASD may fail to efficiently separate and focus on target speech from other concurrent sounds. This disadvantage is vividly depicted in an autistic adolescent's autobiography that his ears are like microphones picking up all sounds, amplifying faint ones, and transmitting the whole lot to the brain; hence, he can write, think, or solve problems only in absolute silence (Brattberg, 2003). If the sensory load for hearing presents a problem in daily experiences, a better listening condition or strategy would be crucial to education or intervention programs for children with ASD. One viable solution is improving the signal-to-noise ratio (SNR) to boost speech intelligibility in noise using hearing assistive technology (HAT). HAT is a personalized wearable technology that selectively boosts the SNR of the target speech. It has been referred to as the "personal frequency modulation system" as it selectively processes target sounds by adding frequency modulation in the signal for audio transmission and reception in a way analogous to radio signal treatment (Schafer et al., 2013). Although their components and working principles are similar, the transmission system of HAT has been upgraded to digital/infrared signals, thus providing higher compatibility, shorter audio delay, and better intelligibility (van der Kruk et al., 2017). HAT consists of a microphone and transmitter worn by the speaker and a high-fidelity ear-level receiver worn by the listener. The microphone plus transmitter picks up sounds from the specified direction and sends them to the ear-level receiver with the set SNR, by which the HAT renders target speech salient from distracters and avoids signal degradation caused by attenuation during propagation through air and interference from background noise. When in use, the transmitter continuously measures the surrounding noise level. If the noise surpasses 57 dB SPL (a relatively high noise level), the transmitter relays the receiver's signal to increase its volume. Through this adaptive-gain approach, HAT ensures an ideal SNR in the listener's ear. For individuals who cannot tolerate ear-level HAT, a system called sound-field amplification (SFA) has been adopted alternatively. The SFA is an inclusive classroom adjustment similar to HAT in principle. Instead of ear-level receivers, it uses self-adaptive control loudspeakers to convey the signal.
Previous Studies on SPIN Performance in the ASD Population
Most prior studies on adolescents and adults observed significantly worse speech recognition/reception thresholds (SRTs; the minimum hearing level where an individual can recognize 50% of the speech material in noise) in individuals with ASD than in NT individuals (Alcántara et al., 2004; DePape et al., 2012; Groen et al., 2009; Mair, 2013; Schelinski & Kriegstein, 2020), and established the SRT as a key indicator of the ASD population’s SPIN. However, some of the aforementioned studies also indicated that significantly lower SRTs are not an across-the-board phenomenon in the ASD population. Alcántara et al. (2004) found that although SRTs for young adults with ASD (mean age: 21 years) were generally worse than those for the NT group (mean age: 19 years), a statistically significant difference was not detected in purely energetic masker noise and steady-state noise. Moreover, Groen et al. (2009) revealed no significant difference in SRTs between ASD and NT adolescents aged 12-17 years under pink noise with temporal dips (10 Hz amplitude modulation) and ripple sounds with and without temporal dips. Similarly, Mair (2013) found that the SRTs of young adults with ASD aged 19-31 years were comparable to the SRTs of age-matched NT individuals under steady-state noise.
The extant SRT findings suggest that the SPIN performance in individuals with ASD may be relatively insusceptible to the energetic masking on the physical level, as opposed to the informational masking caused by highly variable sounds or sounds similar to the target stimuli (Pollack, 1975). However, this conjecture does not stand up to scrutiny. In this regard, language background could make a difference. Several studies on neurotypicals suggested that unlike English, Mandarin Chinese are more susceptible to energetic masking due to considerable differences in phonology and semantic processes (see Wang & Xu, 2021 for a review). SPIN-related research has been scarce in Chinese individuals with ASD. To our knowledge, there is one recent study on Chinese children with ASD (mean age:11.7), which reported no between-group SRT difference in steady-state noise (Yu et al., 2021). However, most participants in that study were aged above 10 years, and their SPIN abilities might be nearly adult-like in at least one ear as suggested by Chandni et al. (2020). Another complication is that the measures in previous studies may leave subtle differences undetected in statistical analysis. For instance, although the SRTs for SPIN with steady-state noise may be similar, the accuracy rate data could show significant between-group differences. The adaptive tests in earlier SRT research mainly used a standard 2-dB step size, which may not be a very sensitive measure as the individual differences near the step size would be subject to the measurement error associated with each SRT estimate. In a simulated study, the fixed-SNR procedure demonstrated superior efficiency to the adaptive procedure in screening tests, especially when data were close to the cutoff for statistical significance (Smits, 2017). Furthermore, previous SRT studies did not consider the possible gap in the speech perception ability when accounting for differences in the SPIN performance between the two groups. Even in quiet, individuals with ASD have been frequently reported to demonstrate speech-specific processing deficits and atypical speech-evoked subcortical or cortical responses (e.g., Manfredi et al., 2020; Wang et al., 2017; Zhang et al., 2018). Thus, it remains unclear whether the SPIN abilities of younger Mandarin-speaking children with ASD would remain intact under energetic maskers. A study on younger Chinese children using a more sensitive and efficient protocol with a baseline assessment of the participants’ speech perception in quiet is in need for addressing the issue.
Previous HAT Studies in the ASD Population
Several studies have substantiated the efficacy of HAT in ameliorating difficulties and tension related to SPIN among children and adolescents with ASD. Schafer et al. (2013) adopted a single group ABAB (alternating no-intervention and intervention trial periods) design in seven children with ASD and four children with attention deficit hyperactivity disorder (ADHD) and found significant improvements in average speech recognition scores in noise and classroom observations of on-task behavior. Rance et al. (2014) applied a single-group balanced design (ABBA) in ten children with ASD and obtained results with children reporting significant listening and communication benefits and teachers reporting a perceived improvement in the children’s listening comprehension and classroom behavior. Similarly, Schafer et al. (2016) chose single-group repeated measures to assess the use of HAT through a series of functional questionnaires and auditory tests, which showed substantially less listening difficulty, improved recognition scores, better working memory, and comprehension performance, and better acceptable noise levels. From the standpoint of emotional well-being, Rance et al. (2017) compared salivary cortisol measurements with and without the use of SFA and found mean cortisol concentrations decreased significantly during the SFA sessions, which is often associated with reduced stress after behavioral interventions. On a more representative sample including both autistic children and adults with frequently co-occurring conditions, Schafer et al. (2019) also detected significant improvements in both speech recognition tests and qualitative measures using a pre-post HAT comparison. A recent study (Wilson et al., 2021) using a questionnaire for teachers and a video analysis of listening behaviors found improved ratings of students’ listening behavior with the use of SFA with more benefits for children with ASD compared to NT peers in the phonological processing of nonsense words in noise. More recently, Feldman et al. (2022) observed a significant enhancement in SPIN accuracy across stimuli of different linguistic complexity, with the greatest benefit found in sentence-level stimuli, and a relief of listening effort for autistic children with high IQs during HAT-on sessions.
However, several questions remain to be explored. The first is about the viability and efficacy of extending HAT use in autistic populations with distinct linguistic and social backgrounds. The existing evidence is mainly based on English-speaking children and adolescents. It remains unknown whether the observed benefits are generalizable to speakers using typologically different languages with distinct phonological systems, such as Mandarin Chinese. Theoretically, the distributional patterns of acoustic and phonological features vary significantly across English and Chinese, and the systemic differences would help shape the development of language-specific sound prototypes in memory and alters children's speech perception in particular ways (Kuhl et al., 2008).
Another concern is related to several limitations in previous research. Due to the single group design adopted in most prior HAT studies, it remains to be discussed whether the assistance of HAT could bridge the gap in SPIN perception between children with ASD and age-matched neurotypical children. Also, most ASD samples in the reviewed studies were relatively small in size or mixed with a cohort of children having other developmental conditions, and several studies did not provide explicit information of diagnostic instruments or procedures.
Furthermore, there has been a severe lack of linguistic diversity in this area of research. With China being the world’s most populous country that has its prevalence of ASD at around 1 in 142 cases accompanied by a lack of public awareness and social support in the education system (Zhou et al., 2020), it is of great practical significance to assess the use of HAT in Chinese school-age children with ASD. Audiological data show that individuals with hearing loss or substandard auditory processing like ASD generally require at least a +15 dB SNR for relatively easy and accurate speech perception (American National Standard, 2010). However, classroom acoustics are often not up to the mark, with the average classroom SNR varying from -20 to +5 dB (Richards et al., 1993). The situation would be exacerbated in well-populated countries such as China, where, according to an official report, the average class size reaches 38 students in elementary schools and 46 students in junior high schools (China Ministry of Education, 2020). Moreover, resource constraints including a shortage of funding and professionally trained staff make it difficult to implement individualized interventions for children with ASD in the short term (Sun, Allison, Auyeung, et al., 2013). Under such circumstances, improvement of classroom SNR would be a viable and necessary option for improving the learning experience and academic performance of school-age children with ASD in China.
Overview of the Present Study
The present study aimed to address three main research questions: (1) whether energetic masking would exert greater influences on the SPIN performance of Chinese-speaking younger children with ASD in comparison with NT children, (2) whether the use of HAT could improve the SPIN performance of Chinese-speaking younger children with ASD and whether their assisted SPIN performance would be comparable to the unassisted level of their NT peers, and (3) whether the use of HAT could alleviate the listening difficulty of Chinese-speaking younger children with ASD across different daily scenarios. For the laboratory tests, we assessed sentence recognition accuracy in quiet vs. in a steady-state masker (Research Question 1) and with the use of HAT vs. without (Research Question 2). Based on the previous literature, we hypothesized that the Chinese-speaking children with ASD would be more susceptible to energetic masking than their NT peers. With regard to HAT use, the ASD group would have significantly improved accuracy that may come close to the NT group. In addition to laboratory settings, we compared the difficulty rating of daily experience in the ASD group before and after a ten-day HAT trial (Research Question 3) and hypothesized that the post-trial ratings would significantly improve.
Methods
Participants
We tested 26 children with ASD and 19 NT children (see Table 1 for a summary of participant profiles). All eligibility criteria were determined through a literature review and pilot testing. Details of the recruitment criteria are summarized in Table 2. Recruitment and research procedures were approved by the Institutional Review Board of the Shanghai Mental Health Center in accordance with the Declaration of Helsinki. Fully informed parents or guardians of the young children were required to provide written consent. Financial compensation was provided for participation.
The two groups of children were matched for sex composition, mean chronological age, attention, and handedness (all right-handed). Most participants of the ASD group were outpatients from the Child and Adolescent Psychiatry of Shanghai Mental Health Center, and some were students or members from partner institutions. Participants from partner institutions were diagnosed at Grade III Level A hospitals between 3 and 7 years of age. To investigate SPIN abilities and the effects of HAT use among children with autism before auditory and cognitive stabilization, we recruited participants aged between 6 and 12 years. The working definition of auditory and cognitive stabilization here refers to the status of having adult-like auditory skills and cognitive abilities and maintaining generally consistent auditory and cognitive processing as a child grows older. According to previous behavioral and neurological studies (e.g., Edgar et al., 2020; Nettelbeck & Burns, 2010), children or adolescents aged above 12 years typically exhibit relatively stable and adult-like performance in both cognitive and auditory processing tasks. As dialectal influence could be an important factor, we made sure that the language background across participants or between the two groups were comparable with most participant families from Shanghai and some from neighboring cities speaking variants of the Wu dialect that are similar in phonological features and mutually intelligible to a great extent.
All participants with ASD were further confirmed to meet the latest diagnostic criteria, the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-Ⅴ, American Psychiatric Association, 2013) by two veteran pediatric neurologists at the Child and Adolescent Psychiatry of Shanghai Mental Health Center, who are unrelated to the present study. The current diagnostical procedure could not utilize standardized diagnostic instruments widely applied in English-speaking populations, e.g., the Autism Diagnostic Observation Schedule (ADOS; Lord et al., 2000; Lord et al., 2012; Lord et al., 1989) and the Autism Diagnostic Interview–Revised (ADI-R; Lord et al., 1994) due to a series of practical issues, including no officially validated Chinese version, limited application, a lack of normative data, and a small number of certified examiners (Huang et al., 2012; Sun, Allison, Auyeung, et al., 2013; Sun, Allison, Matthews, et al., 2013). Instead, the Chinese versions of Autism Behavior Checklist (ABC; Krug et al., 1980) and Childhood Autism Rating Scale (CARS; Schopler et al., 1980) were jointly adopted to confirm the diagnosis and assess the severity level. In mainland China, both ABC and CARS have long been validated and widely adopted for diagnosing ASD in both research and clinical practice (e.g., Li et al., 2005; Li et al., 2018; Lu et al., 2004; Shan et al., 2021; Yang et al., 1993). Parents or relatives living with the child for at least three years filled out the ABC under the guidance of two licensed psychologists on the research team. All ASD participants’ scores were higher than 68. As suggested by Krug et al. (1980), total scores above 68 points indicate a high probability of autism. Meanwhile, the two pediatric neurologists, who are trained and qualified CARS examiners, accomplished the evaluation based on behavioral observations of children during other testing, inquiry of their past medical and/or developmental history, and reports of their parents and/or relatives. According to the CARS manual, a score at or above 30 strongly indicates the existence of ASD; more specifically, a score from 30 to 37 suggests mild to moderate symptoms, whereas a score from 38 to 60 suggests severe autism. In the current study, only one participant (Number 6) was characterized by severe symptoms with a total score of 40, while the rest had scores between 30 and 36.
All participants had an IQ above 70 and could repeat simple sentences. Their IQ was assessed by two certified examiners using the age-appropriate Wechsler Intelligence Scale for Children 4th edition-Chinese version (WISC-IV-Chinese) short form (Zhang, 2009), which is commonly used in clinical practice among children with neurodevelopmental conditions owing to its implementation efficiency and estimation accuracy (Hrabok et al., 2014). Noticeably, IQ differed significantly between the two groups and was included as a covariate in the statistical analyses.
Two subsets (inattention and hyperactivity/impulsivity) of the Chinese version of the Swanson, Nolan, and Pelham version IV scale (SNAP-IV) reported by parents (Gau et al., 2009) were used to screen for behavioral symptoms of attention-deficit/hyperactivity disorder (ADHD). Each subset includes nine items rated on a 4-point Likert scale (0 = never, 1 = occasionally, 2 = often, and 3 = very often). Subset scores below 13 indicate no clinically significant attention issues. None of the groups showed significant differences or clinically significant ADHD symptoms.
Pure tone audiometry was conducted in a separate sound booth with a noise level lower than 30 dB A to test children's audibility ≤20 dB HL across 0.25 to 8 kHz bilaterally under the guidance of a certified audiologist through an Inventis Bell Plus diagnostic audiometer calibrated following ANSI S3.6 standards (American National Standards Institute, 1996). There was no medical history of cerebral injuries, visual impairments, hearing loss, comorbid diseases, or psychotropic medication within three months before participation. Comorbid diseases here refer to co-occurring medical conditions restricted to neurological disorders, such as severe somatic complications, Fragile X syndrome, Down syndrome, and epilepsy, with symptoms that are physically apparent and distinct from ASD and would potentially make the experimental design very difficult to implement. Two participants (Number: 6, 18) were confirmed with ASD-associated mental health conditions (see Appendix 2 for details), according to parents’ report of medical history or clinical judgments of the mentioned two pediatric neurologists.
Target Measures
This study included two SPIN experiments on children and a parental/teacher survey questionnaire. For the SPIN tests, two types were implemented: adaptive and fixed-level. All tests were conducted using a custom program on a ThinkPad X1 Carbon Gen 7 laptop in laboratory rooms with a background noise below 35 dBA. The test stimuli were presented via an M-Audio M-Track 2 × 2 sound card and a pair of M-Audio BX8 D2 studio monitor loudspeakers. In line with previous studies, speakers were sited at 0° azimuth (speech signal) and 180° azimuth (noise) at head level at a distance of one meter from the participant to simulate an ideal class scenario in which the participant was seated in the front row, listening to a teacher speaking in the front with distractions from behind (Figure 1).
Because few studies had tested SPIN in young Chinese children with autism, several considerations were taken to adopt appropriate materials and tasks to ensure feasibility and validity. The Mandarin Hearing in Noise Test for Children (MHINT-C, Chen & Wong, 2020) was used for both types of tests. It consists of 12 highly equivalent test lists, with the mean deviation of each list in the SRTs within ±1 dB. Every list includes ten simple sentences, each of which contains ten characters (e.g., “爸爸带回来一个大西瓜。” 1) and is presented in a male voice with the same 2-s duration. During the SPIN tests, participants were required to repeat each sentence as accurately as possible after hearing a prompt tone; accordingly, the experimenter listened to each word in the sentence and clicked right or wrong in the program. As a preliminary exploration, this study chose a speech-spectrum-shaped steady-state masker matching each target sentence's long-term average spectrum as background noise. From a neural decoding perspective, disembedding speech signals from speech-shaped steady-state noise is relatively simple, as these two stimuli differ greatly in spectro-temporal features (i.e., the spectrogram of speech is dynamic, both temporally and spectrally, whereas that of the masker is not). For young children whose sensory perception and linguistic skills are yet to mature, maskers involving complex acoustic features and speech or speech-like elements are rather demanding (Maamor & Billings, 2017), which would be aggravated by speech-specific difficulty in most children with ASD. As the participants in the current study were at a relatively young age, adopting a steady-state masker would be less of a concern for subject attrition/dropout that could arise from potential emotional reactions when facing adverse listening conditions. Another consideration for choosing the steady-state masker was to compare the results with those from older Chinese children with ASD in steady-state noise in a previous study (Yu et al., 2021).
While the steady-state masker was relatively easy to implement and test, it has its drawback on the ground of ecological validity. What children experience in everyday life, particularly at school, is much more complex and generally mixed with informational masking. In prior studies on SRTs, the Bamford-Kowal-Bench Speech-in-Noise test (BKB-SIN, 2005), a sentence-level SPIN test similar to MHINT-C, documented significant enhancements among children with ASD and other auditory disorders with the aid of the HAT (Schafer et al., 2013; Schafer, Traber, et al., 2014; Schafer et al., 2016). Compared to BKB-SIN, MHINT-C has a slightly lower test-retest reliability for SRT measures with a 95% confidence interval of 2.8 dB (1.8 dB for BKB-SIN) but best suits the age group in the current study among all available tests of the same type. Importantly, previous BKB-SIN studies generally adopted multi-talker babble rather than steady-state noise we used, thereby more involving the effect of informational masking in addition to energetic masking.
In our study, participants took two adaptive tests in noise without HAT use, with the results averaged as the final SRT. The starting presentation level was set at -5 dB SNR with a steady-state masker fixed at 60 dB A, which was calibrated using a sound level meter (Aihua AWA6228+) and a default calibration track. Based on the participants’ responses, the signal volume was adaptively altered to achieve different SNRs. The first four sentences were conducted with a 4-dB step size, while the rest with a 2-dB step size. The SNR presentation levels from Number five to Number ten sentences were averaged to obtain the participants' SRTs. In addition, fixed-level accuracy tests were supplemented to provide a comprehensive profile of the participants' SPIN abilities and the effects of HAT use with knowledge of the baseline situation. Participants completed four fixed-level tests wearing the receiver of the HAT on the right ear, with the microphone plus transmitter attached to the monitor at 0° azimuth (Figure 1). A unilateral fitting was chosen because it could allow the user to have one ear open for surrounding sounds (Feldman et al., 2022), and bilateral fitting would be inappropriate for listeners with normal hearing bilaterally (Tharpe et al., 2004). Following a recent HAT study from Feldman et al. (2022), we also fit the receiver on the right ear. It has been shown that the maturation of SPIN abilities are more advanced on children’s right ear, with the SPIN abilities becoming adult-like on the right ear by 10 years and on the left ear by around 13–14 years (Chandni et al., 2020). The order of the 2 (Noise/Quiet) × 2 (HAT-on/HAT-off) testing conditions was counterbalanced across participants and test sessions. In noisy conditions, 0 dB SNR (intensity of speech signal equal to the noise power) was chosen based on a pilot study where 5 dB SNR, 0 dB SNR, and - 5 dB SNR were examined, respectively, among seven children with ASD. Significant differences were detected between the HAT-on and HAT-off sessions at 0 dB SNR and -5 dB SNR, but the latter appeared too challenging for some autistic children to bear and cooperate.
For the questionnaire, the ASD group’s listening difficulty under various circumstances at school was assessed by their parents/teachers using the Children's Auditory Performance Scale (CHAPS, Smoski et al., 1998) before and after a ten-day trial period of HAT use. In previous studies, CHAPS recorded less listening difficulty in sum scores for all conditions among children with ASD after an at-school trial of HAT (Schafer et al., 2013; Schafer et al., 2016). The Chinese translation version of CHAPS was generated by two graduate students from the Department of Translation and Interpreting at Shanghai Jiao Tong University. Examples of test items are listed in the Appendix 1. The CHAPS uses a 7-point Likert scale from +1 (less difficulty) to -5 (cannot function at all) for 36 items to discern behaviors related to auditory processing disorders among children above six years of age in six conditions (Auditory Attention Span/Auditory Memory Sequencing/ Ideal/ Multiple Inputs/ Noise/ Quiet) with reference to NT peers. All conditions of CHAPS were conducted in the current study because each of them represents a common scenario in daily life, which could comprehensively contextualize autistic children’s SPIN abilities and device efficacy across various situations.
Experimental Procedures
All participants paid two visits to the laboratory. During the first visit, recruitment screening and device fitting were completed, after which the family was counseled and provided with written instructions on the use, care, and maintenance of the HAT. The HAT for this study includes a microphone plus transmitter (Sonova Roger Touchscreen Mic, CMIIT ID:2016DP1845) and an ear-level receiver (Roger Focus, CMIIT ID:2016DP1847). The fitting procedure was performed according to a documented manual (Schafer, Bryant, et al., 2014). This step aimed to select the dome and tube appropriate for each child's ear canal size. Previous studies have adjusted the receiver volumes of participants with ASD to maximize SNR gains, considering their desired sensation level for conversational speech. In this study, we set all receiver volumes to zero (i.e., the default setting) to avoid confounds due to the differences in amplification settings in interpreting the improvements in SPIN accuracy and the potential between-group differences in benefits from HAT use. During the second visit, an MHINT-C test was conducted. Between the two visits, the ASD group experienced a ten-day HAT trial, during which the ASD group's parents or teachers were required to complete the CHAPS based on observation of the children's listening behaviors at school. The additional details are presented in Figure 2.
Data Analysis
All statistical analyses were conducted in R version 3.6.3 (R Core Team, 2020). The SPIN tests yielded two types of data: SRTs and accuracy rates. This study defined SRTs as the lowest SNRs in which participants recognized 50% of the speech signals. Lower SRTs indicate better signal recognition from concurrent noise. The SRTs of the two groups were compared using the Mann-Whitney U test. A linear mixed-effects model (LMM) was adopted to analyze accuracy rates because of its strength in fitting non-independent and repeated-measures data. Before modeling, raw accuracy data were converted into rationalized arcsine units (RAU; Studebaker et al., 1995) to reduce potential ceiling effects, given the participants’ high accuracy rates in this study. We constructed two LMMs using the lmerTest package (Kuznetsova et al., 2017) to examine (1) the effect of listening condition (Noise vs. Quiet) on two groups’ sentence recognition accuracy without the HAT use, and (2) the effect of HAT use (Off vs. On) on two groups’ sentence-in-noise recognition accuracy. The first LMM on HAT-off accuracy (then referred to as the baseline LMM) started with a random-effect term subject, three fixed-effect terms group (NT vs. ASD), listening condition (quiet vs. noise), IQ (continuous), and all interaction terms. The second LMM for analyzing the effect of HAT (then referred to as the HAT LMM) on SPIN accuracy included Group (NT vs. ASD), HAT use (HAT-off vs. HAT-on), IQ (continuous), and possible interactions, with Subject as a random effect. Parsimonious models were determined by AIC in a stepwise algorithm using the step function from the stats package and visually inspected for no obvious deviations from homoscedasticity or normality through residual plots. Post hoc tests were implemented using the emmeans or emtrends function from the emmeans package (Lenth, 2020).
The CHAPS questionnaires provided children’s sum scores for difficulty rating and the number of children rated at risk for each listening condition before and after HAT use. The sum scores for each condition were obtained by dividing the total condition score (i.e., the sum of the circled responses for each condition) by the number of condition items (Noise: 7, Quiet: 7, Ideal: 3, Multiple Inputs: 3, Auditory Memory Sequencing: 8, Auditory Attention Span: 8). A sum score of -1 or lower implies a risk of having significant difficulties in a certain area of auditory processing. However, the results of the “at-risk” numbers in the current study need to be interpreted with caution because the cut-off score has not been validated in Chinese norms. The sum scores were analyzed using the Wilcoxon-signed-rank test on paired samples, whereas the number of children at risk before and after device use was compared using Fisher's exact test.
Results
The findings are provided below, starting with relatively easy-to-interpret pre- and post-HAT-use questionnaire results on listening difficulty across six conditions, followed by results of the baseline/HAT-off SRTs and accuracy rates across the ASD and NT groups. Then, the model analyses of the accuracy rate in noise are presented as a function of HAT use.
Impact of HAT Use on Behavioral Ratings of Listening Difficulties
A two-tailed Fisher's exact test showed no significant difference in the pre-post change in the number of at-risk children (i.e., autistic children whose sum score was -1 or lower) for each condition of CHAPS. However, the number of at-risk children decreased across all conditions in the post-use evaluation, while participants in the pass category before HAT use remained the same (n = 6), and several of those in the at-risk category improved under at least one CHAPS condition (n = 14). Noticeably, the paired Wilcoxon Signed Rank test (p values–adjusted using ‘Holm’ correction) unveiled a significant decrease in difficulty ratings across all conditions after HAT use (see Figure 3 for statistical details). Specifically, participants with a high pre-rating of difficulty (-4 and below) improved substantially by 1-4 points.
Baseline SPIN Data
The Mann-Whitney U test (Figure 4) disclosed that the mean SRT of the ASD group (-3.42 ± 2.27 dB) did not differ significantly from the NT group (-4.42 ± 1.53 dB; p = 0.053), which is in line with previous findings (Alcántara et al., 2004; Mair, 2013; Yu et al., 2021).
In the linear mixed effects model (LMM) analysis (see Table 3 for the model formula and output), there were significant main effects of Group, Listening Condition, and IQ. These effects were further qualified by three significant two-way interactions: Group × Listening Condition, IQ × Group, and IQ× Listening Condition. Table 4 shows a summary of the results. We further explored the first interaction by calculating the contrasts between the estimated marginal means with the Bonferroni correction. The results of the post hoc analysis (Table 5) revealed that the presence of noise significantly reduced the recognition accuracy of the ASD group but not the NT group. Furthermore, we conducted two trend analyses of the second and third interaction, respectively, with detailed results provided in Table 6. The simple slope estimates indicated that the ASD group’s mean recognition accuracy was positively correlated with IQ, while the NT group exhibited a slightly inverse correlation, with the between-group difference statistically significant in pairwise contrasts. Another trend analysis of the third interaction disclosed significantly different impacts of IQ on recognition accuracy in the two listening environments; each one-unit increase in IQ led to a larger improvement in participants’ perception accuracy in noise compared with the quiet condition.
Impact of HAT on SPIN Accuracy
Table 7 depicts the formula and output of the HAT LMM. There were robust main effects of Group, HAT-use, and IQ. On average, both groups’ accuracy rates significantly improved during the HAT-on sessions, yet this effect differed between the two groups. The analysis revealed three significant interactions: Group × HAT-use, HAT-use × IQ, and Group × IQ. Statistical details of the fixed effects and interaction terms are summarized in Table 8. In the post hoc analysis of the first interaction, the SPIN accuracy of the ASD group improved significantly with the use of HAT and bridged its gap to the unassisted level of the NT group (Table 9). To parse out the second and the third interaction, we conducted two separate trend analyses, with the results presented in Table 10. When estimating simple slopes of IQ for different HAT-use sessions, the positive trend of IQ for HAT-off sessions turned out to be significant, as well as the contrast between IQ slopes for HAT-on and HAT-off sessions, but not significant for HAT-on sessions. These results indicated that the impact of HAT use on SPIN accuracy was relatively less susceptible to variance in participants’ cognitive features. In addition, the trend analysis of the Group × IQ interaction suggested that SPIN accuracy was significantly higher with increasing IQ in the ASD group, but not for the NT group, with the effect of IQ differing significantly between the two groups’ trends of SPIN performance.
Discussion
The present study on Mandarin-speaking children with ASD served two purposes: (1) to examine their SPIN abilities in energetic masking, and (2) to assess the efficacy of HAT on SPIN accuracy in laboratory settings and listening difficulty in daily scenarios. The results provided evidence that SPIN abilities in energetic masking were compromised in Mandarin-speaking children with ASD, and that the use of HAT showed beneficial effects on their SPIN performance and daily experience.
SPIN Issues under Energetic Maskers
Consistent with previous studies (Alcántara et al., 2004; Mair, 2013; Yu et al., 2021), no between-group difference in SRTs under steady-state noise was found to be statistically significant in this study. Nevertheless, a closer examination revealed noteworthy distinctions. The mean SRTs for both ASD (-3.42±2.27 dB) and NT groups (-4.42±1.53 dB) in the current study were significantly higher/worse than those in earlier studies on English-speaking adolescents and adults, ranging from about -5 to -17 dB (Alcántara et al., 2012; Groen et al., 2009; Mair, 2013). Noticeably, the SRT results from a recent study on Chinese children and teenagers (Yu et al., 2021) were just slightly lower/better (ASD: -5.99 ± 1.84 dB; NT: -5.75 ±1.49 dB) than ours. Two potential explanations are available here, which seem plausible a priori but are not fully supported by data. One of the contributing factors is age, which is known to modulate auditory processing maturation in SPIN abilities. Another possible reason is the language difference between Mandarin and English. For example, Mandarin has more voiceless consonants than English and is a tonal language. Because voiceless consonants have less energy than voiced ones, and a failure to detect the tonal contour correctly would undermine phoneme recognition and meaning comprehension, Chinese listeners will be more susceptible to energetic masking (Wu et al., 2011).
Additionally, the results of the fixed-level tests indicated that the SPIN abilities of the ASD group under energetic masking were not as intact as previously suggested. The accuracy rates of the ASD group substantially declined with steady-state noise, whereas the NT group did not. Moreover, significantly lower accuracy rates were detected in the ASD group than in the NT group in noisy, but not quiet conditions. Atypical SPIN in energetic masking is essential on yet another level, because it implies poor functioning of the auditory periphery among children with ASD. Several studies have indicated that auditory filters may be abnormally broad in autism (Bhatara et al., 2013; Plaisted et al., 2003).
Furthermore, our findings suggest that the accuracy rate is a relatively more sensitive predictor of variances in children’s sentence-level SPIN abilities. An earlier study on English-speaking NT individuals aged between 17 and 45 years substantiated that a relatively small change in SRTs might reflect a larger difference in actual SPIN performance, with a 1-dB change comparable to a roughly 10% change in accuracy rate when using BKB-SIN (Nilsson et al., 1994). Measuring accuracy rate, however, requires a more time-consuming fixed-level test procedure (around 20-30 mins per participant) than the adaptive SRT procedure (about 5-15 mins per participant), for which this study faced a high rate of participant loss and was restricted to autistic children with milder issues.
Effectiveness of HAT
Overall, the laboratory tests and questionnaire results demonstrated that the use of HAT could alleviate SPIN problems among Mandarin-speaking children with ASD. Our study was the first to document clear perceptual benefits with sentence-level SPIN accuracy improved considerably during HAT-on sessions to a level comparable to that of the age-matched NT peers (unaided). This is a compelling message because the improved SPIN ability has been a remarkable predictor of better educational performance and social interaction in children on the spectrum (Ashburner et al., 2008). Of the related publications on the use of HAT in individuals with ASD, two studies (Rance et al., 2017; Rance et al., 2014) most closely agreed with the research design and age group tested in the current study, which also showed similar SPIN accuracy rates between children with ASD (aided) and NT peers (unaided). However, previous studies have focused on the auditory processing of words and phonemes in informational masking using the Consonant-Nucleus-Consonant Word test (CNC test, Peterson & Lehiste, 1962) and four-talker babbles, while the current study had a different focus on sentence-level perception in energetic masking. There is still lack of evidence to support the list equivalency of the CNC test in noise and the age-appropriate use of it in young children.
Parental questionnaire results showed that the SNR advantage ensured by the HAT brought about significant decreases in the ASD group’s difficulty rating across the six listening conditions, which is consistent with the finding of Schafer et al. (2016) but slightly differs from that of Schafer et al. (2013) who found no enhancement in the condition of multiple inputs. Such inconsistencies probably result from the small sample sizes with different participant profiles. Despite the substantial improvement in rating scores, there was no qualitative decline in the number of “at-risk” children whose sum score were -1 or lower in any of the six listening conditions of CHAPS. This finding suggests that a compound intervention may be necessary to disentangle issues in auditory attention (Lepistö et al., 2006), multisensory speech integration (Foxe et al., 2015), or verbal working memory (Millman & Mattys, 2017) entwined with the ASD population’s SPIN difficulty.
Limitations
Our preliminary results need to be interpreted with caution. There were several limitations in our HAT fitting procedure. First, we fit the receiver on the participants’ right ear without considering ear differences across individuals. Children with ASD might have significant interaural asymmetry (see James et al., 2022 for a review) and the choice of which ear to wear the receiver could potentially influence the efficacy of HAT as suggested in an early study (Schafer, Traber, et al., 2014). Also, the volume amplification setting was not personalized, which could compromise the efficacy of HAT use for some individuals. A more customized fitting procedure should be considered for comparison in the future to achieve the optimal outcome.
The current design of SPIN tests was also restricted in ecological validity. The evaluation tests were conducted in the laboratory with a steady-state noise masker. We attempted to simulate a natural listening environment; however, the laboratory setting was greatly simplified, with signal and noise presented at a consistent intensity from fixed spatially separated locations. Although we supplemented some real-situation data by conducting the CHAPS, this measure has yet to be validated in Chinese norms and was potentially susceptible to parents’ or teachers’ personal bias. In this regard, a daily observational evaluation by trained professionals can be helpful for future studies. While questionnaire results from a small sample may lack scientifical reliability, they could still be useful references for the quantitative assessment, especially considering that similar scales for assessing auditory processing have been particularly scarce in mainland China. The validation of CHAPS or the development of alternative scales in Chinese is of great necessity in the future.
The steady-state noise used in the current study mainly reflected energetic masking whereas in real-world scenarios, auditory scenes typically contain a range of sound sources and multiple speakers. The real-world speech-in-noise settings lead to more informational masking, where interference from background speech affects target intelligibility at a central processing level, in which they may be tangled with the target or deflect attention from it, rather than just acoustic overlap. Given that deficits in both bottom-up auditory and top-down linguistic processing result in reduced SPIN in ASD, there are compelling reasons to believe that increased susceptibility to informational masking in ASD is probable. In the future, sentence-level SPIN under maskers involving informational masking and close-to-real-world noises, such as multiple-talker babbles and classroom noise, should be investigated. Moreover, this study mainly employed fault-tolerant and task-oriented behavioral tests focusing on fundamental auditory processing, which left the impact of HAT on higher-level listening comprehension and the underlying cognitive mechanisms underexamined. Comprehension tasks and psychophysiological measures are recommended in future research to obtain an in-depth view of the ASD population’s SPIN issues and explore whether long-term HAT use could improve their cortical processing and comprehension of speech sounds, as observed in children with dyslexia after a long trial (Hornickel et al., 2012).
Finally, subject inclusion and exclusion criteria in our study need further refinement. For instance, information of musicianship was not collected and controlled between groups, which could influence participants’ SPIN performance. As suggested in previous studies, years of musical training improved SPIN skills and performance of children with or without auditory problems (e.g., Benitez-Barrera et al., 2022; Lo et al., 2020; Slater et al., 2015). More importantly, the current samples for the two subject groups cannot adequately reflect different socioeconomic groups or the whole spectrum of autism. Most of our participants are urban residents from the top fifteen economically developed cities in China (Slater, 2019), which may indicate higher-than-average socioeconomic status in the society. Thus, our findings need further corroborative evidence from more inclusive samples, especially given that a considerable proportion of the Chinese population resides in underdeveloped or rural areas, which remains to be challenging due to the lack of financial resources, professional services, and public awareness. To ensure that more participants could accomplish the functional outcome measure, we excluded autistic children with ADHD or other severe medical comorbidities. In reality, ADHD has been reported as one of the common neuropsychiatric comorbidities in Chinese children with ASD, and a substantial proportion was recorded with known medical comorbidities (Chen et al., 2016). Evidence supporting the efficacy of HAT has hitherto been restricted to children at the milder end of the spectrum. Whether HAT is a feasible and resultful solution for lower-functioning children or other age groups remains a question.
Analogous to all aspects of intervention for the ASD population, auditory assistance should be considered on a case-by-case basis. However, the practical difficulty associated with device fitting and testing can be overwhelming in individuals with severe autism symptoms. Even in the current study on children with moderate autism symptoms, seven out of thirty-three children failed to bear sustained HAT use, and three complained or showed signs of maladaptation during the at-home/school trial. In line with previous findings (Schafer et al., 2013; Schafer et al., 2016), parental observations indicated that tactile defensiveness and auditory hypersensitivity are two leading causes. Fortunately, an alternative to HAT, the SFA system, would solve such concerns. It includes a microphone and transmitter worn by the speaker (as per the HAT) and self-adaptive control loudspeakers that will change the output volume in keeping with the background noise to maintain a fixed ideal SNR of the signal (American Academy of Audiology, 2011; Davis, 1991; Keith & Purdy, 2014). Loudspeakers can be placed in the classroom to enhance listening conditions. Nevertheless, it should be noted that the SFA system was less effective than the HAT system among NT children or children with hearing impairments (American Academy of Audiology, 2011; Dockrell & Shield, 2012; Palmer, 1998). Assessing the use of the SFA system in the ASD population is another future direction.
Conclusion
In summary, this study provided initial empirical evidence for (a) extra sentence-level SPIN difficulty in Mandarin-speaking children with ASD despite their relatively intact listening function, and (b) the HAT as a promising tool to improve their SPIN performance and ease related difficulties. Nonetheless, the need for HAT should be evaluated individually, and its efficacy should not be overestimated. Future research involving a longitudinal design with an extensive sample and divergent methodologies to examine daily situations and neurobehavioral mechanisms is needed to refine the theoretical constructs, assess the long-term HAT effects, and direct educational practice.
Funding
This study was supported by the Major Program of the National Social Science Foundation of China (18ZDA293).
Data Availability Statement
Research data supporting this publication are publicly available as supplemental material files at https://osf.io/273yu/.
Acknowledgments
We would like to thank all participating families and undergraduate volunteers from the Faculty of Education at East China Normal University and the School of Foreign Languages at Shanghai Jiao Tong University. Special thanks are extended to Sonova Holding AG: Shanghai for loaning devices, Shanghai Qi Xing Special Education School, and Shanghai Xing Le Parent Association for assisting with recruitment.
Conflicts of Interest
The authors declare that no competing interests exist at the time of publication.
References
- Alcántara, J. I., Cope, T. E., Cope, W., & Weisblatt, E. J. (2012). Auditory temporal-envelope processing in high-functioning children with autism spectrum disorder. Neuropsychologia, 50(7), 1235-1251. [CrossRef]
- Alcántara, J. I., Weisblatt, E. J., Moore, B. C., & Bolton, P. F. (2004). Speech-in-noise perception in high-functioning individuals with autism or Asperger's syndrome. Journal of Child Psychology and Psychiatry, 45(6), 1107-1114. [CrossRef] [PubMed]
- American Academy of Audiology. (2011). Supplement B: Classroom audio distribution systems – Selection and verification.
- American National Standard. (2010). Acoustical performance criteria, design requirements, and guidelines for schools.
- American National Standards Institute. (1996). Specifications for audiometers (ANSI S3.6-1996). American National Standards Institute.
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). American Psychiatric Publishing.
- Arunachalam, S., & Luyster, R. J. (2016). The integrity of lexical acquisition mechanisms in autism spectrum disorders: A research review. Autism Research, 9(8), 810-828. [CrossRef] [PubMed]
- Ashburner, J., Rodger, S., & Ziviani, J. (2008). Sensory processing and classroom emotional, behavioural, and educational outcomes in children with autism spectrum disorder. American Journal of Occupational Therapy, 62(5), 564-573. [CrossRef] [PubMed]
- Benevides, T. W., & Lane, S. J. (2015). A review of cardiac autonomic measures: Considerations for examination of physiological response in children with autism spectrum disorder. Journal of autism and developmental disorders, 45(2), 560–575. [CrossRef] [PubMed]
- Benitez-Barrera, C. R., Skoe, E., Huang, J., & Tharpe, A. M. (2022). Evidence for a musician speech-perception-in-noise advantage in school-age children. Journal of Speech, Language, and Hearing Research, 65(10), 3996-4008. [CrossRef] [PubMed]
- Bhatara, A., Babikian, T., Laugeson, E., Tachdjian, R., & Sininger, Y. S. (2013). Impaired timing and frequency discrimination in high-functioning autism spectrum disorders. Journal of Autism and Developmental Disorders, 43(10), 2312-2328. [CrossRef] [PubMed]
- BKB-SIN. (2005). Bamford-Kowal-Bench speech in noise test. Elk Grove, IL: Etymotic Research.
- Brattberg, G. (2003). Enastående: självbiografisk berättelse om livet med högfungerande autism (Exceptional: autobiographical story of life with high functioning autism) (2nd ed. ed.). Värkstaden AB.v.
- Chandni, J., Vipin Ghosh, P. G., Chetak, K. B., & Aishwarya, L. (2020, Dec). Maturation of speech perception in noise abilities during adolescence. International Journal of Pediatric Otorhinolaryngology, 139, 110459. [CrossRef] [PubMed]
- Chen, F., Zhou, J., Wang, Y., Yu, K., Arshad, S., Khawaji, A., & Conway, D. (2016). Robust Multimodal Cognitive Load Measurement. Springer International Publishing.
- Chen, Y., & Wong, L. L. N. (2020). Development of the mandarin hearing in noise test for children. International Journal of Audiology, 1-6. [CrossRef] [PubMed]
- China Ministry of Education. (2020, October 7). Overview of educational achievements in China in 2019. Retrieved January 25 from http://en.moe.gov.cn/documents/reports/202102/t20210209_513095.html.
- Cooperative Research Centre for Living with Autism. (2018). Australian autism educational needs analysis – What are the needs of schools, parents and students on the autism spectrum? https://www.autismcrc.com.au/australian-education-needsanalysis.
- Crane, L., Goddard, L., & Pring, L. (2009). Sensory processing in adults with autism spectrum disorders. Autism, 13(3), 215-228. [CrossRef]
- Danneels, M., Degeest, S., Dhooge, I., & Keppler, H. (2021). Central auditory processing and listening effort in normal-hearing children: A pilot study. International Journal of Audiology, 60(10), 739-746. [CrossRef]
- Davis, D. (1991). Utilizing amplification devices in the regular classroom. Hearing Instruments, 42(7), 18-23.
- DePape, A. M., Hall, G. B., Tillmann, B., & Trainor, L. J. (2012). Auditory processing in high-functioning adolescents with autism spectrum disorder. PLoS One, 7(9). [CrossRef]
- Dockrell, J. E., & Shield, B. (2012). The impact of sound-field systems on learning and attention in elementary school classrooms. Journal of Speech, Language, and Hearing Research, 55(4), 1163-1176. [CrossRef] [PubMed]
- Dryden, A., Allen, H. A., Henshaw, H., & Heinrich, A. (2017). The association between cognitive performance and speech-in-noise perception for adult listeners: A systematic literature review and meta-Analysis. Trends in Hearing, 21, 2331216517744675. [CrossRef] [PubMed]
- Edgar, J. C., Blaskey, L., Green, H. L., Konka, K., Shen, G., Dipiero, M. A., Berman, J. I., Bloy, L., Liu, S., McBride, E., Ku, M., Kuschner, E. S., Airey, M., Kim, M., Franzen, R. E., Miller, G. A., & Roberts, T. P. L. (2020). Maturation of auditory cortex neural activity in children and implications for auditory clinical markers in diagnosis. Frontiers in Psychiatry, 11, 584557. [CrossRef]
- Eigsti, I. M., & Fein, D. A. (2013). More is less: pitch discrimination and language delays in children with optimal outcomes from autism. Autism Research, 6(6), 605-613. [CrossRef] [PubMed]
- Elliott, L. L. (1979). Performance of children aged 9 to 17 years on a test of speech intelligibility in noise using sentence material with controlled word predictability. Journal of the Acoustical Society of America, 66(3), 651–653.
- Elsabbagh, M., Divan, G., Koh, Y. J., Kim, Y. S., Kauchali, S., Marcin, C., Montiel-Nava, C., Patel, V., Paula, C. S., Wang, C., Yasamy, M. T., & Fombonne, E. (2012). Global prevalence of autism and other pervasive developmental disorders. Autism Research, 5(3), 160-179. [CrossRef] [PubMed]
- Feldman, J. I., Thompson, E., Davis, H., Keceli-Kaysili, B., Dunham, K., Woynaroski, T., Tharpe, A. M., & Picou, E. M. (2022). Remote microphone systems can improve listening-in-noise accuracy and listening effort for youth with autism. Ear and Hearing, 43(2), 436-447. [CrossRef] [PubMed]
- Foxe, J. J., Molholm, S., Del Bene, V. A., Frey, H. P., Russo, N. N., Blanco, D., Saint-Amour, D., & Ross, L. A. (2015). Severe multisensory speech integration deficits in high-functioning school-aged children with Autism Spectrum Disorder and their resolution during early adolescence. Cerebral Cortex, 25(2), 298-312. [CrossRef] [PubMed]
- Gau, S. S., Lin, C. H., Hu, F. C., Shang, C. Y., Swanson, J. M., Liu, Y. C., & Liu, S. K. (2009). Psychometric properties of the Chinese version of the Swanson, Nolan, and Pelham, Version IV Scale-Teacher Form. Journal of Pediatric Psychology, 34(8), 850-861. [CrossRef]
- Groen, W. B., van Orsouw, L., Huurne, N. t., Swinkels, S., van der Gaag, R.-J., Buitelaar, J. K., & Zwiers, M. P. (2009). Intact spectral but abnormal temporal processing of auditory stimuli in autism. Journal of Autism and Developmental Disorders, 39(5), 742-750. [CrossRef]
- Hornickel, J., Chandrasekaran, B., Zecker, S., & Kraus, N. (2011). Auditory brainstem measures predict reading and speech-in-noise perception in school-aged children. Behavioural Brain Research, 216(2), 597-605. [CrossRef]
- Hornickel, J., Zecker, S. G., Bradlow, A. R., & Kraus, N. (2012). Assistive listening devices drive neuroplasticity in children with dyslexia. Proceedings of the National Academy of Sciences of the United States of America, 109(41), 16731-16736. [CrossRef]
- Hrabok, M., Brooks, B. L., Fay-McClymont, T. B., & Sherman, E. M. (2014). Wechsler Intelligence Scale for Children-fourth edition (WISC-IV) short-form validity: A comparison study in pediatric epilepsy. Child Neuropsychology, 20(1), 49-59. [CrossRef]
- Huang, A. X., Jia, M., & Wheeler, J. J. (2012). Children with autism in the People’s Republic of China: Diagnosis, legal issues, and educational services. Journal of Autism and Developmental Disorders, 43(9), 1991-2001. [CrossRef]
- Huang, D., Yu, L., Wang, X., Fan, Y., Wang, S., & Zhang, Y. (2018). Distinct patterns of discrimination and orienting for temporal processing of speech and nonspeech in Chinese children with autism: An event-related potential study. European Journal of Neuroscience, 47(6), 662-668. [CrossRef]
- James, P., Schafer, E., Wolfe, J., Matthews, L., Browning, S., Oleson, J., Sorensen, E., Rance, G., Shiels, L., & Dunn, A. (2022). Increased rate of listening difficulties in autistic children. Journal of Communication Disorders, 99, 106252. [CrossRef]
- Jiang, J., Liu, F., Wan, X., & Jiang, C. (2015). Perception of melodic contour and intonation in autism spectrum disorder: Evidence from Mandarin speakers. Journal of Autism and Developmental Disorders, 45(7), 2067-2075. [CrossRef]
- Jones, P. R., Moore, D. R., & Amitay, S. (2015). Development of auditory selective attention: Why children struggle to hear in noisy environments. Developmental Psychology, 51(3), 353-369. [CrossRef]
- Keith, W. J., & Purdy, S. C. (2014). Assistive and therapeutic effects of amplification for auditory processing disorder. Seminars in Hearing, 35(1), 27–38.
- Klatte, M., Hellbrück, J., Seidel, J., & Leistner, P. (2017). Effects of classroom acoustics on performance and well-being in elementary school children: A field study. Environment and Behavior, 42(5), 659-692. [CrossRef]
- Krug, D. A., Arick, J., & Almond, P. (1980). Behavior checklist for identifying severely handicapped individuals with high levels of autistic behavior. Journal of Child Psychology and Psychiatry, 21(3), 221-229. [CrossRef]
- Kuhl, P. K., Conboy, B. T., Coffey-Corina, S., Padden, D., Rivera-Gaxiola, M., & Nelson, T. (2008). Phonetic learning as a pathway to language: New data and native language magnet theory expanded. Philosophical Transactions of the Royal Society B: Biological Sciences, 363(1493), 979-1000. [CrossRef] [PubMed]
- Kujala, T., Kuuluvainen, S., Saalasti, S., Jansson-Verkasalo, E., Wendt, L. V., & Lepisto, T. (2010). Speech-feature discrimination in children with Asperger syndrome as determined with the multi-feature mismatch negativity paradigm. Clinical Neurophysiology, 121(9), 1410-1419. [CrossRef] [PubMed]
- Leekam, S. R., Nieto, C., Libby, S. J., Wing, L., & Gould, J. (2007). Describing the sensory abnormalities of children and adults with autism. Journal of Autism and Developmental Disorders, 37(5), 894-910. [CrossRef] [PubMed]
- Lenth, R. V. (2020). emmeans: Estimated Marginal Means, aka Least-Squares Means. R package version 1.5.3. https://CRAN.R-project.org/package=emmeans.
- Lepistö, T., Silokallio, S., Nieminen-von Wendt, T., Alku, P., Naatanen, R., & Kujala, T. (2006). Auditory perception and attention as reflected by the brain event-related potentials in children with Asperger syndrome. Clinical Neurophysiology, 117(10), 2161-2171. [CrossRef] [PubMed]
- Li, J., Zhong, J., Cai, L., Chen, Y., & Zhou, M. (2005). Clinical application of the Childhood Autism Rating Scale. Chinese Journal of Child Health Care, 13(3), 267-268. (in Chinese). [CrossRef]
- Li, L., Li, M., Lu, J., Ge, X., Xie, W., Wang, Z., Li, X., Li, C., Wang, X., Han, Y., Wang, Y., Zhong, L., Xiang, W., Huang, X., Chen, H., & Yao, P. (2018). Prenatal progestin exposure is associated with autism spectrum disorders. Frontiers in Psychiatry, 9, 611. [CrossRef] [PubMed]
- Li, Y., Xing, H., Zhang, L., Shu, H., & Zhang, Y. (2021). How visual word decoding and context-driven auditory semantic integration contribute to reading comprehension: A test of additive vs. multiplicative models. Brain Sciences, 11(7), 830. [CrossRef] [PubMed]
- Lo, C. Y., Looi, V., Thompson, W. F., & McMahon, C. M. (2020). Music training for children with sensorineural hearing loss improves speech-in-noise perception. Journal of Speech, Language, and Hearing Research, 63(6), 1990-2015. [CrossRef] [PubMed]
- Lord, C., Risi, S., Lambrecht, L., Cook, E. H., Jr, L., B. L., DiLavore, P. C., Pickles, A., & Rutter, M. (2000). The Autism Diagnostic Observation Schedule-Generic: A standard measure of social and communication deficits associated with the spectrum of autism. Journal of Autism and Developmental Disorders, 30(3), 205–223.
- Lord, C., Rutter, M., DiLavore, P. C., Risi, S., Gotham, K., & Bishop, S. L. (2012). Autism Diagnostic Observation Schedule (2nd ed.). Western Psychological Services.
- Lord, C., Rutter, M., Goode, S., Heemsbergen, J., Jordan, H., Mawhood, L., & Schopler, E. (1989). Austism Diagnostic Observation Schedule: A standardized observation of communicative and social behavior. Journal of Autism and Developmental Disorders, 19, 185–212. [CrossRef]
- Lord, C., Rutter, M., & Le Couteur, A. (1994). Autism Diagnostic Interview-Revised: a revised version of a diagnostic interview for caregivers of individuals with possible pervasive developmental disorders. Journal of Autism and Developmental Disorders, 24, 659–685.
- Lu, J., Yang, Z., Shu, M., & Su, L. (2004). Reliability, validity analysis of the Childhood Autism Rating Scale. China Journal of Modern Medicine, 14(13), 119–121. (in Chinese).
- Maamor, N., & Billings, C. J. (2017, Jan 1). Cortical signal-in-noise coding varies by noise type, signal-to-noise ratio, age, and hearing status. Neuroscience Letters, 636, 258-264. [CrossRef]
- Mair, K. R. (2013). Speech perception in autism spectrum disorder: Susceptibility to masking and interference [Dissertation, University College London]. London.
- Manfredi, M., Cohn, N., Sanchez Mello, P., Fernandez, E., & Boggio, P. S. (2020). Visual and verbal narrative comprehension in children and adolescents with autism spectrum disorders: An ERP study. Journal of Autism and Developmental Disorders, 50(8), 2658-2672. [CrossRef]
- Millman, R. E., & Mattys, S. L. (2017). Auditory verbal working memory as a predictor of speech perception in modulated maskers in listeners with normal hearing. Journal of Speech Language and Hearing Research, 60(5), 1236-1245.
- Nettelbeck, T., & Burns, N. R. (2010). Processing speed, working memory and reasoning ability from childhood to old age. Personality and Individual Differences, 48(4), 379-384. [CrossRef]
- Nilsson, M., Soli, S. D., & Sullivan, J. A. (1994). Development of the Hearing in Noise Test for the measurement of speech reception thresholds in quiet and in noise. Journal of the Acoustical Society of America, 95(2), 1085–1099. [CrossRef] [PubMed]
- Nittrouer, S., Krieg, L. M., & Lowenstein, J. H. (2018). Speech recognition in noise by children with and without dyslexia: How is it related to reading? Research in Developmental Disabilities, 77, 98-113.
- O'Connor, K. (2012). Auditory processing in autism spectrum disorder: A review. Neuroscience and Biobehavioral Reviews, 36(2), 836-854. [CrossRef]
- Palmer, C. M. (1998). Quantification of the ecobehavioral impact of a soundfield loudspeaker system in elementary classrooms. Journal of Speech, Language, and Hearing Research, 41, 819-833.
- Perrone-Bertolotti, M., Tassin, M., & Meunier, F. (2017). Speech-in-speech perception and executive function involvement. PLoS One, 12(7), e0180084. [CrossRef] [PubMed]
- Peterson, G. E., & Lehiste, I. (1962). Revised CNC lists for auditory tests. Journal of Speech and Hearing Disorders, 27(1), 62–70.
- Plaisted, K., Saksida, L., Alcantara, J., & Weisblatt, E. (2003). Towards an understanding of the mechanisms of weak central coherence effects: experiments in visual configural learning and auditory perception. Philosophical Transactions of the Royal Society of London B: Biological Sciences, 358(1430), 375–386. [CrossRef] [PubMed]
- Pollack, I. (1975). Auditory informational masking. The Journal of the Acoustical Society of America, 57(S5). [CrossRef]
- R Core Team. (2020). R: A language and environment for statistical computing. https://www.R-project.org/.
- Rance, G., Chisari, D., Saunders, K., & Rault, J. L. (2017). Reducing listening-related stress in school-aged children with autism spectrum disorder. Journal of Autism and Developmental Disorders, 47(7), 2010-2022. [CrossRef] [PubMed]
- Rance, G., Saunders, K., Carew, P., Johansson, M., & Tan, J. (2014). The use of listening devices to ameliorate auditory deficit in children with autism. Journal of Pediatrics, 164(2), 352-357. [CrossRef]
- Richards, C., Flexer, C., Brandy, W., & Wray, D. (1993). Signal-to-noise enhancing devices can improve kids' reading skills. Hearing Instruments, 44(11), 12-15.
- Schafer, E. C., Amlani, A. M., Paiva, D., Nozari, L., & Verret, S. (2011). A meta-analysis to compare speech recognition in noise with bilateral cochlear implants and bimodal stimulation. International Journal of Audiology, 50(12), 871-880. [CrossRef]
- Schafer, E. C., Bryant, D., Sanders, K., Baldus, N., Algier, K., Lewis, A., Traber, J., Layden, P., & Amin, A. ( 2014). Fitting and verification of frequency modulation systems on children with normal hearing. Journal of the American Academy of Audiology, 25(6), 529–540. [CrossRef]
- Schafer, E. C., Gopal, K. V., Mathews, L. A., Kaiser, K., Canale, E., & Creech, A. (2019). Verification and validation of remote-microphone technology on children and college-age adults who have autism spectrum disorder. Journal of Educational, Pediatric and (Re)Habilitative Audiology(24), 2-7.
- Schafer, E. C., Mathews, L., Mehta, S., Hill, M., Munoz, A., Bishop, R., & Moloney, M. (2013). Personal FM systems for children with autism spectrum disorders (ASD) and/or attention-deficit hyperactivity disorder (ADHD): An initial investigation. Journal of Communication Disorders, 46(1), 30-52. [CrossRef] [PubMed]
- Schafer, E. C., Traber, J., Layden, P., Amin, A., Sanders, K. H., Bryant, D., & Baldus, N. (2014). Use of wireless technology for children with auditory processing disorders, attention-deficit hyperactivity disorder, and language disorders. Seminars in Hearing, 35, 193-205. [CrossRef]
- Schafer, E. C., Wright, S., Anderson, C., Jones, J., Pitts, K., Bryant, D., Watson, M., Box, J., Neve, M., Mathews, L., & Reed, M. P. (2016). Assistive technology evaluations: Remote-microphone technology for children with autism spectrum disorder. Journal of Communication Disorders, 64, 1-17. [CrossRef] [PubMed]
- Schelinski, S., & Kriegstein, K. (2020). Brief report: Speech-in-noise recognition and the relation to vocal pitch perception in adults with autism spectrum disorder and typical development. Journal of Autism and Developmental Disorders, 50, 356-363. [CrossRef]
- Schopler, E., Reichler, R. J., DeVellis, R. F., & Daly, K. (1980). Toward objective classification of childhood autism: Childhood Autism Rating Scale (CARS). Journal of Autism and Developmental Disorders, 10(1), 91–103. [CrossRef]
- Seep, B., Glosemeyer, R., Hulce, E., Linn, M., & Aytar, P. (2000). Classroom acoustics I: A resource for creating learning environments with desirable listening conditions. Melville, NY: Acoustical Society of America.
- Shan, L., Feng, J. Y., Wang, T. T., Xu, Z. D., & Jia, F. Y. (2021). Prevalence and developmental profiles of Autism Spectrum Disorders in children with global developmental delay. Frontiers in Psychiatry, 12, 794238. [CrossRef]
- Slater, J., Skoe, E., Strait, D. L., O'Connell, S., Thompson, E., & Kraus, N. (2015). Music training improves speech-in-noise perception: Longitudinal evidence from a community-based music program. Behavioural Brain Research, 291, 244-252. [CrossRef] [PubMed]
- Slater, M. (2019). The 100 Largest China City Economies by GDP. Retrieved Jan 25 from https://www.chinacheckup.com/blog/china-city-economies.
- Smaldino, J. J., Crandell, C. C., Kreisman, B. M., John, A. B., & Kreisman, N. V. (2008). Room acoustics for listeners with normal hearing and hearing impairment. In M. Valente, H. Hosford-Dunn, & R. Roeser (Eds.), Audiology Treatment (pp. 418–451). New York, NY: Thieme Medical Publishers.
- Smits, C. (2017). Improving the efficiency of speech-in-noise hearing screening tests. Ear and Hearing, 38(6), e385-e388. [CrossRef]
- Smoski, W., Brunt, M. A., & Tannahill, J. C. (1998). Children’s auditory performance scale (CHAPS). Educational Audiology Association.
- Studebaker, G. A., Mcdaniel, D. M., & Sherbecoe, R. L. (1995). Evaluating relative speech recognition performance using the proficiency factor and rationalized arcsine differences. Journal of The American Academy of Audiology, 6(2), 173-182.
- Sun, X., Allison, C., Auyeung, B., Baron-Cohen, S., & Brayne, C. (2013). A review of healthcare service and education provision of Autism Spectrum Condition in mainland China. Research in Developmental Disabilities, 34(1), 469-479. [CrossRef]
- Sun, X., Allison, C., Matthews, F. E., Sharp, S. J., Auyeung, B., Baron-Cohen, S., & Brayne, C. (2013). Prevalence of autism in mainland China, Hong Kong and Taiwan: A systematic review and meta analysis. Molecular Autism, 4(7). [CrossRef]
- Talarico, M., Abdilla, G., Aliferis, M., Balazic, I., Giaprakis, I., Stefanakis, T., Foenander, K., Grayden, D. B., & Paolini, A. G. (2007). Effect of age and cognition on childhood speech in noise perception abilities. Audiology and Neuro-Otology, 12(1), 13-19. [CrossRef] [PubMed]
- Tharpe, A. M., Ricketts, T., & Sladen, D. P. (2004). FM systems for children with minimal to mild hearing loss. In D. Fabry & C. D. Johnson (Eds.), ACCESS: Achieving Clear Communication Employing Sound Solutions (pp. 191–197). Phonak AG.
- van der Kruk, Y., Wilson, W. J., Palghat, K., Downing, C., Harper-Hill, K., & Ashburner, J. (2017). Improved signal-to-noise ratio and classroom performance in children with autism spectrum disorder: A systematic review. Review Journal of Autism and Developmental Disorders, 4(3), 243-253. [CrossRef]
- Wang, X., Wang, S., Fan, Y., Huang, D., & Zhang, Y. (2017). Speech-specific categorical perception deficit in autism: An event-related potential study of lexical tone processing in Mandarin-speaking children. Scientific Reports, 7(1). [CrossRef] [PubMed]
- Wang, X., & Xu, L. (2021). Speech perception in noise: Masking and unmasking. Journal of Otology, 16(2), 109-119. [CrossRef] [PubMed]
- Ward, K. M., & Grieco-Calub, T. M. (2022). Age and hearing ability influence selective attention during childhood. Ear and Hearing, 43(4), 1125-1138. [CrossRef] [PubMed]
- Wilson, W. J., Harper-Hill, K., Armstrong, R., Downing, C., Perrykkad, K., Rafter, M., & Ashburner, J. (2021). A preliminary investigation of sound-field amplification as an inclusive classroom adjustment for children with and without Autism Spectrum Disorder. Journal of Communication Disorders, 93, 106142. [CrossRef] [PubMed]
- Wu, X., Yang, Z., Huang, Y., Chen, J., Li, L., Daneman, M., & Schneider, B. A. (2011). Cross-language differences in informational masking of speech by speech: English versus Mandarin Chinese. Journal of Speech, Language, and Hearing Research, 54(6), 1506-1524. [CrossRef] [PubMed]
- Yang, W., & Bradley, J. S. (2009). Effects of room acoustics on the intelligibility of speech in classrooms for young children. The Journal of the Acoustical Society of America, 125(2), 922-933. [CrossRef] [PubMed]
- Yang, X., Huang, L., Jia, M., & Chen, S. (1993). Validation study of the Chinese version of Autism Behavior Checklist. Chinese Mental Health Journal(7), 279-280. (in Chinese).
- Yu, L., Fan, Y., Deng, Z., Huang, D., Wang, S., & Zhang, Y. (2015). Pitch processing in tonal-language-speaking children with autism: an event-related potential study. Journal of Autism and Developmental Disorders, 45(11), 3656-3667. [CrossRef]
- Yu, L., Huang, D., Wang, S., Wu, X., Chen, Y., & Zhang, Y. (2021). Evidence of altered cortical processing of dynamic lexical tone pitch contour in Chinese children with autism. Neuroscience Bulletin, 37(11), 1605-1608. [CrossRef]
- Yu, Y. H., & Shafer, V. L. (2020). Behavioral and Neurophysiological Evidence of Speech Processing in Chinese-Speaking Individuals with Autism Spectrum Disorder: A Review and Future Directions. In H. M. Liu, F. M. Tsao, & P. Li (Eds.), Speech Perception, Production and Acquisition: Multidisciplinary approaches in Chinese languages (pp. 243-279). Singapore: Springer Singapore.
- Zhang, H. (2009). The revision of WISC-IV Chinese version. Psychological Science, 32(5), 1177-1179. [CrossRef]
- Zhang, J., Meng, Y., Tong, X., Yuan, Z., Wu, C., & Ieong, S. L. (2018). Exploring the neural correlates of lexical stress perception in english among Chinese-English bilingual children with autism spectrum disorder: An ERP study. Neuroscience Letters, 666, 158-164. [CrossRef] [PubMed]
- Zhou, H., Xu, X., Yan, W., Zou, X., Wu, L., Luo, X., Li, T., Huang, Y., Guan, H., Chen, X., Mao, M., Xia, K., Zhang, L., Li, E., Ge, X., Zhang, L., Li, C., Zhang, X., Zhou, Y., Ding, D., Shih, A., Fombonne, E., Zheng, Y., Han, J., Sun, Z., Jiang, Y. H., Wang, Y., & Team, L.-N. S. (2020). Prevalence of autism spectrum disorder in China: A nationwide multi-center population-based study among children aged 6 to 12 years. Neuroscience Bulletin. [CrossRef] [PubMed]
Figure 1.
Diagram for MHINT-C room setup. (MHINT-C= the Mandarin Hearing in Noise Test for Children; SNRs=signal-to-noise ratios)
Figure 1.
Diagram for MHINT-C room setup. (MHINT-C= the Mandarin Hearing in Noise Test for Children; SNRs=signal-to-noise ratios)
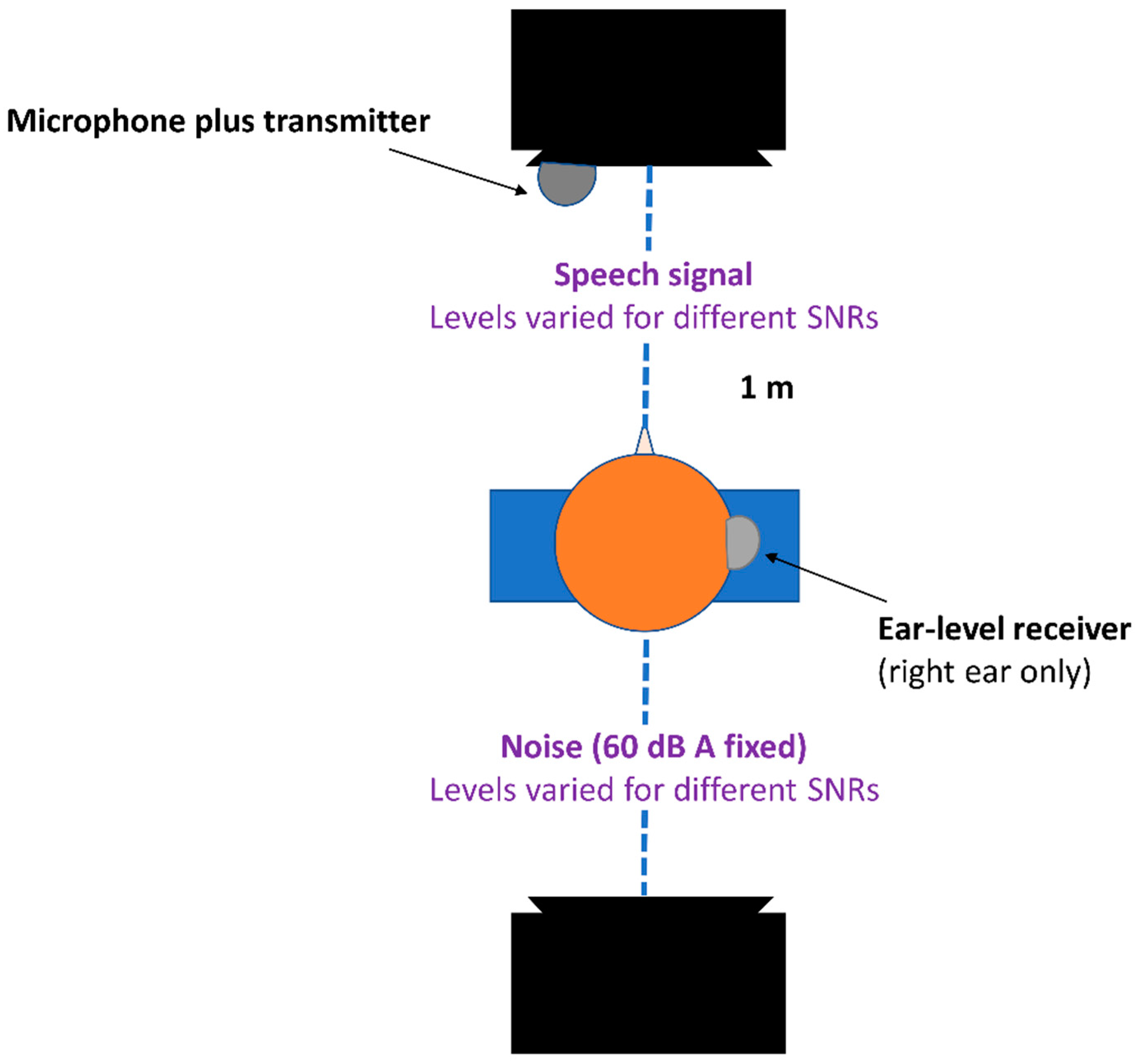
Figure 2.
Flow chart for the overall research process. (ASD=autism spectrum disorder; WISC-Ⅳ-Chinese=the Wechsler Intelligence Scale for Children 4th edition-Chinese version; SNAP-IV=the Chinese version of the Swanson, Nolan, and Pelham version IV scale; CHAPS=the Children’s Auditory Performance Scale; MHINT-C=the Mandarin Hearing in Noise Test for Children; SRTs=speech recognition/reception thresholds; HAT=hearing assistive technology; SNR=signal-to-noise ratio)
Figure 2.
Flow chart for the overall research process. (ASD=autism spectrum disorder; WISC-Ⅳ-Chinese=the Wechsler Intelligence Scale for Children 4th edition-Chinese version; SNAP-IV=the Chinese version of the Swanson, Nolan, and Pelham version IV scale; CHAPS=the Children’s Auditory Performance Scale; MHINT-C=the Mandarin Hearing in Noise Test for Children; SRTs=speech recognition/reception thresholds; HAT=hearing assistive technology; SNR=signal-to-noise ratio)
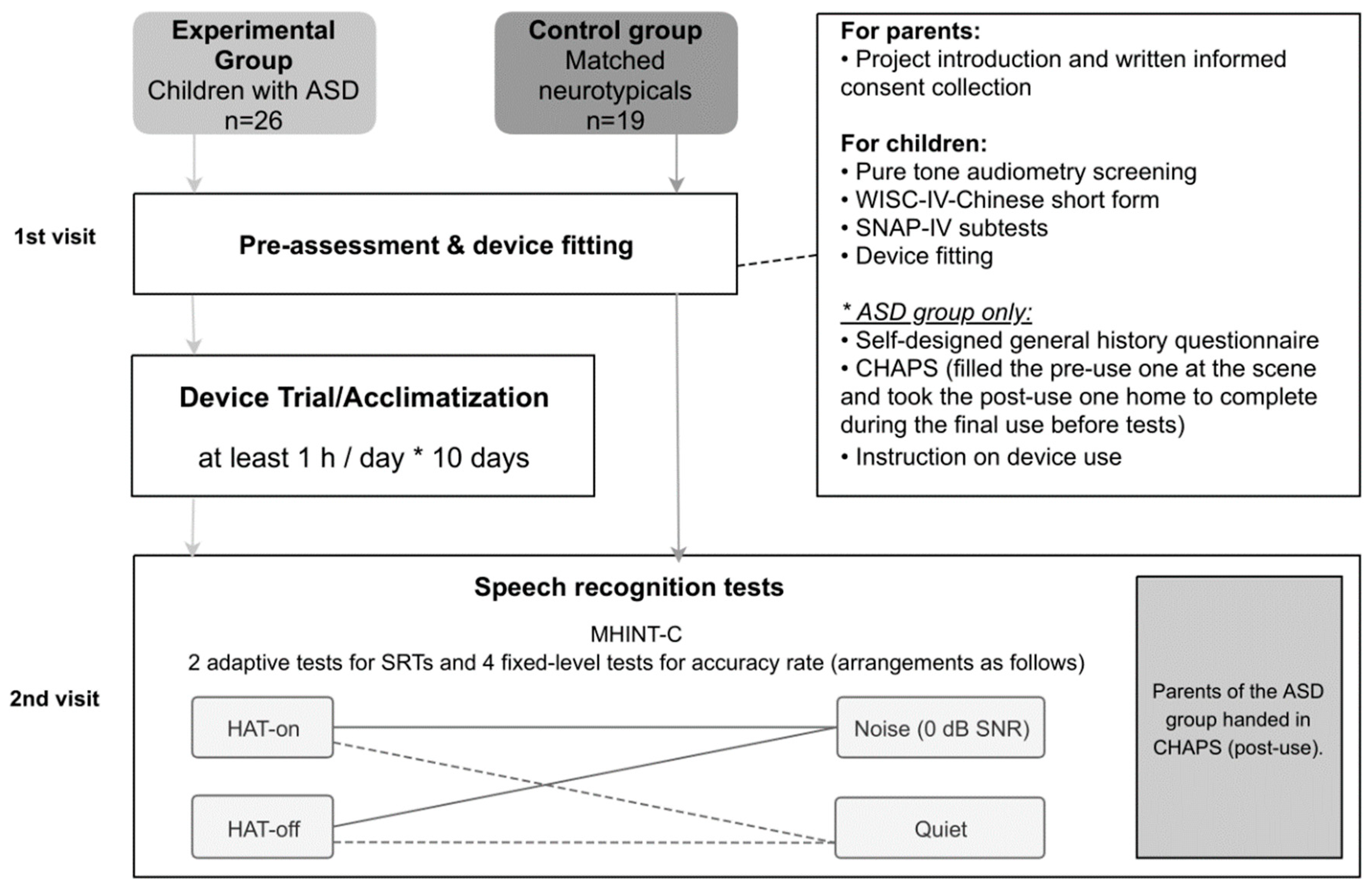
Figure 3.
The ASD group’s parental ratings of difficulty pre- and post-HAT use in six CHAPS listening conditions. (HAT=hearing assistive technology; CHAPS=the Children’s Auditory Performance Scale)
Figure 3.
The ASD group’s parental ratings of difficulty pre- and post-HAT use in six CHAPS listening conditions. (HAT=hearing assistive technology; CHAPS=the Children’s Auditory Performance Scale)
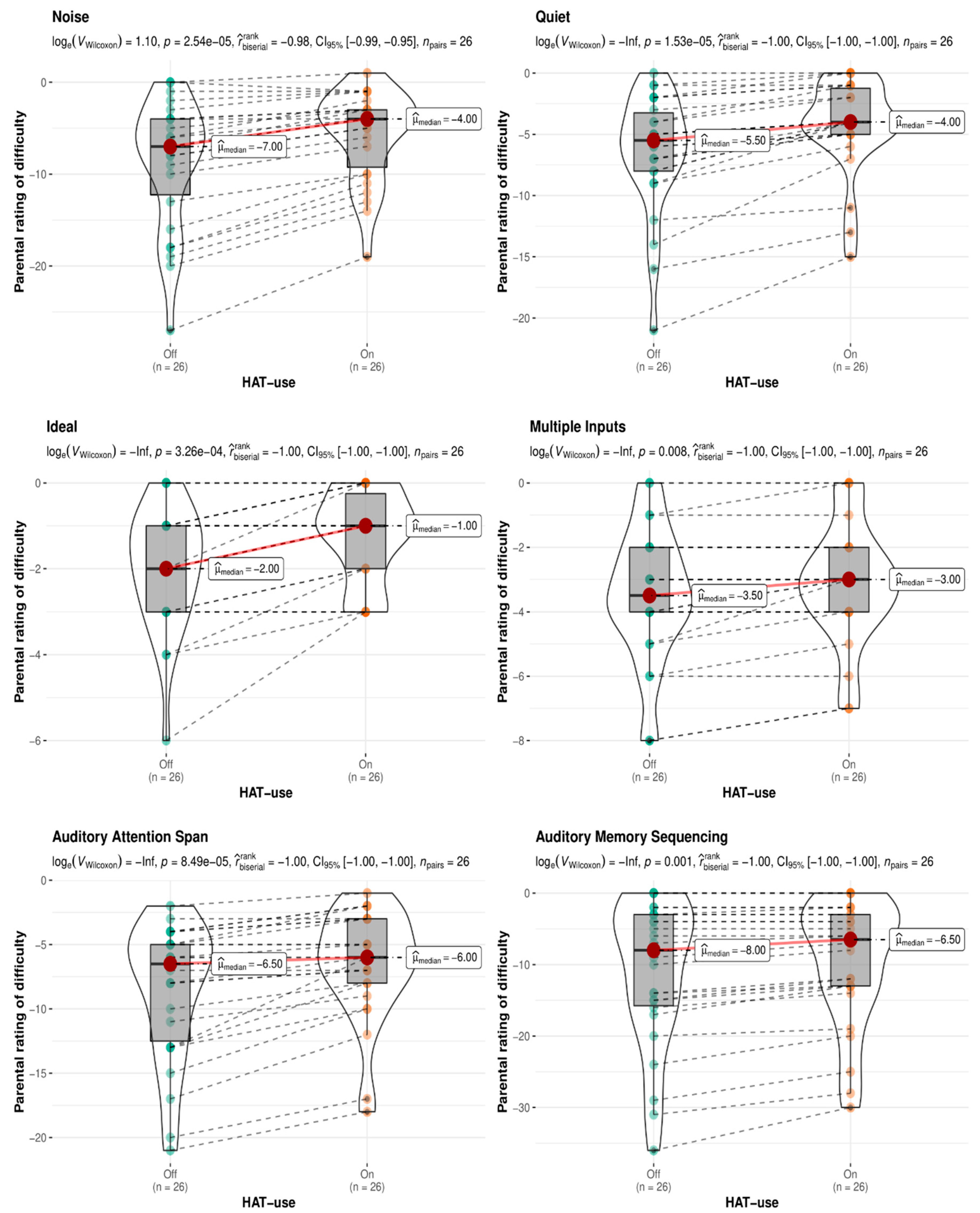
Figure 4.
Unaided speech recognition thresholds for the ASD and NT groups. (ASD=autism spectrum disorder; NT=neurotypical; SNR=signal-to-noise ratio)
Figure 4.
Unaided speech recognition thresholds for the ASD and NT groups. (ASD=autism spectrum disorder; NT=neurotypical; SNR=signal-to-noise ratio)
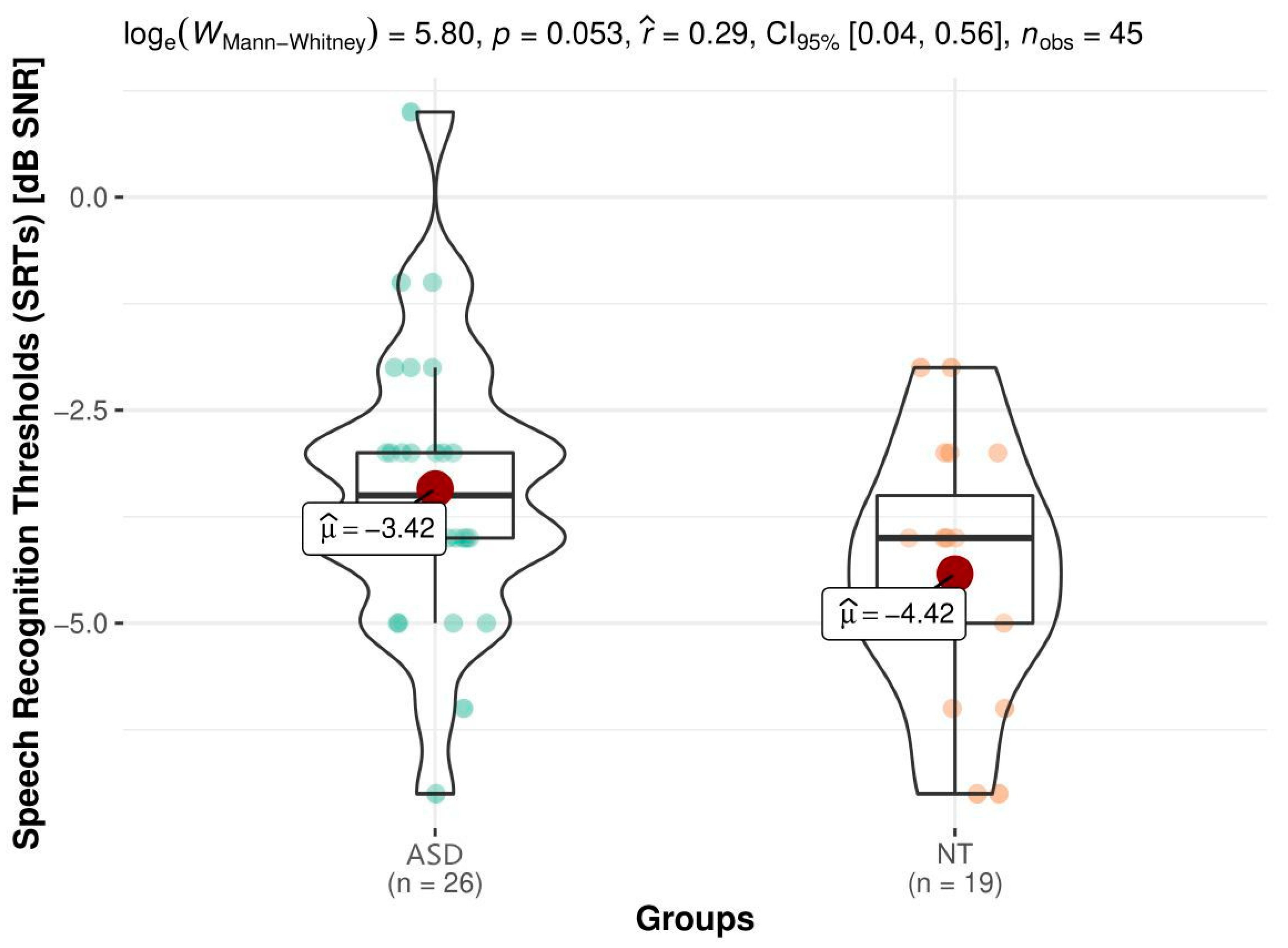

Table 1.
General information about ASD and NT groups. The data range was listed in the top row and mean±SD in the bottom row for each group. (ASD=autism spectrum disorder; NT=neurotypical; SD=standard deviation; M/F=Males/Females; IQ= intelligence quotient; SNAP-IV=the Chinese version of the Swanson, Nolan, and Pelham version IV scale).
Table 1.
General information about ASD and NT groups. The data range was listed in the top row and mean±SD in the bottom row for each group. (ASD=autism spectrum disorder; NT=neurotypical; SD=standard deviation; M/F=Males/Females; IQ= intelligence quotient; SNAP-IV=the Chinese version of the Swanson, Nolan, and Pelham version IV scale).
| ASD (n=26) | NT (n=19) | t value | p1 | |
|---|---|---|---|---|
| Age(year) | 6.8-12.1(8.81±1.70) | 6.6-11.2(8.42±1.39) | 1.03 | 0.31 |
| Sex (M/F) | 23/3 | 17/2 | / | 0.71 |
| IQ | 70-130(103.62±18.67) | 96-137(121.16±11.33) | -3.77 | 0.0005 |
| SNAP-IV-sub 1 | 5-13(7.8±3.1) | 6-9(6.9±2.3) | 1.87 | 0.57 |
| SNAP-IV-sub 2 | 4-12(7.5±2.5) | 4-11(6.3±2.1) | 1.63 | 0.60 |
1 p for sex was computed using the two-tailed Fisher’s exact test, while the others were computed using the two-sample two-tailed t-test.
Table 2.
Inclusion and exclusion criteria for participation in the study. (ASD=autism spectrum disorder; NT=neurotypical; IQ=intelligence quotient; HAT=hearing assistive technology; WISC-Ⅳ-Chinese=the Wechsler Intelligence Scale for Children 4th edition-Chinese version)
Table 2.
Inclusion and exclusion criteria for participation in the study. (ASD=autism spectrum disorder; NT=neurotypical; IQ=intelligence quotient; HAT=hearing assistive technology; WISC-Ⅳ-Chinese=the Wechsler Intelligence Scale for Children 4th edition-Chinese version)
| Inclusion criteria | Exclusion criteria | |
| • Aged 6~12 years • Native speakers of Mandarin • Right-handedness • Normal pure-tone audibility • IQ ≥70 in the WISC-Ⅳ-Chinese short form • Able to iterate simple sentences |
• With cerebral injuries, visual impairments, hearing loss, and comorbid diseases • Having psychotropic medication within three months before the project • Unaccustomed to sustained use of HAT • Clinically significant symptoms of inattention and hyperactivity |
|
| ASD group | NT group | |
| Children meeting the latest diagnostic criteria for ASD | NT children matched by age and gender | |
Table 3.
Linear Mixed-Effects Model formula and output for the baseline accuracy data recorded in quiet and in the stationary noise. (NT=neurotypical; IQ=intelligence quotient; RAU= rationalized arcsine units; SE=standard error; 95% CI=95% confidence interval; df=degree of freedom; ICC=intraclass correlation coefficient; N SUBJ=the number of subjects)
Table 3.
Linear Mixed-Effects Model formula and output for the baseline accuracy data recorded in quiet and in the stationary noise. (NT=neurotypical; IQ=intelligence quotient; RAU= rationalized arcsine units; SE=standard error; 95% CI=95% confidence interval; df=degree of freedom; ICC=intraclass correlation coefficient; N SUBJ=the number of subjects)
| Formula code: Accuracy ~ Group+ Listening condition + IQ + Group:Listening condition + Group:IQ + Listening condition:IQ + (1|Subeject) | |||||
| Sentence recognition accuracy (RAU) | |||||
| Fixed effect | Estimate | SE | 95% CI | t value(df = 81) | p value |
| (Intercept) | 3.61 | 1.01 | 1.48 – 5.74 | 3.37 | 0.001 |
| Group: NT | 10.28 | 2.36 | 5.57 – 14.99 | 4.35 | <0.001 |
| Listening condition: Noise | -4.59 | 0.77 | -6.13 – -3.06 | -5.94 | <0.001 |
| IQ | 0.05 | 0.01 | 0.03 – 0.07 | 5.23 | <0.001 |
| Group: NT*Listening condition: Noise | 0.96 | 0.27 | 0.41 – 1.51 | 3.49 | 0.001 |
| Group: NT*IQ | -0.08 | 0.02 | -0.12 – -0.05 | -4.31 | <0.001 |
| Listening condition: Noise*IQ | 0.03 | 0.01 | 0.01 – 0.04 | 3.79 | <0.001 |
| ICC | 0.68 | ||||
| N SUBJ | 45 | ||||
| Observations | 90 | ||||
| Marginal R2 / Conditional R2 | 0.684 / 0.898 | ||||
Table 4.
Summary of the baseline LMM ANOVA. (IQ=intelligence quotient; df=degree of freedom; η²p=partial eta squared)
Table 4.
Summary of the baseline LMM ANOVA. (IQ=intelligence quotient; df=degree of freedom; η²p=partial eta squared)
| Effect | F-ratio | df | p value | η²p |
|---|---|---|---|---|
| Group | 20.77 | 1.07, 41 | <0.001 | 0.34 |
| Listening Condition | 24.09 | 1.05, 42 | < 0.001 | 0.36 |
| IQ | 6.22 | 1.08, 41 | < 0.05 | 0.13 |
| Group × Listening Condition | 12.19 | 1.05, 42 | <0.01 | 0.23 |
| IQ × Group | 18.15 | 1.07, 41 | <0.001 | 0.30 |
| IQ× Listening Condition | 14.36 | 1.05, 42 | <0.001 | 0.25 |
Table 5.
Post-hoc analysis for the Group × Listening Condition interaction in the baseline LMM ANOVA. (ASD=autism spectrum disorder; NT=neurotypical; SE=standard error; df=degree of freedom; 95% CI=95% confidence interval)
Table 5.
Post-hoc analysis for the Group × Listening Condition interaction in the baseline LMM ANOVA. (ASD=autism spectrum disorder; NT=neurotypical; SE=standard error; df=degree of freedom; 95% CI=95% confidence interval)
| Pairwise contrasts | Estimate | SE | df | t value | p value | |
|---|---|---|---|---|---|---|
| Quiet ASD – Noise ASD | 1.49 | 0.16 | 42 | 9.08 | <0.001 | |
| Quiet ASD – Quiet NT | -0.77 | 0.37 | 54 | -2.10 | 0.24 | |
| Quiet ASD – Noise NT | -0.24 | 0.36 | 51 | -0.67 | 1.00 | |
| Noise ASD – Quiet NT | -2.26 | 0.36 | 51 | -6.27 | <0.001 | |
| Noise ASD – Noise NT | -1.73 | 0.37 | 54 | -4.71 | <0.001 | |
| Quiet NT – Noise NT | 0.53 | 0.19 | 42 | 2.69 | 0.06 | |
| Estimated marginalmeans | SE | df | 95% CI | |||
| Quiet ASD | 9.56 | 0.21 | 55.8 | 9.15 – 9.98 | ||
| Noise ASD | 8.07 | 0.21 | 55.8 | 7.65 – 8.49 | ||
| Quiet NT | 10.33 | 0.29 | 50.8 | 9.73 – 10.93 | ||
| Noise NT | 9.80 | 0.30 | 50.8 | 9.20 – 10.40 | ||
Table 6.
Two post-hoc trend analyses for the IQ × Group, and IQ× Listening Condition interactions in the baseline LMM ANOVA. (ASD=autism spectrum disorder; NT=neurotypical; IQ=intelligence quotient; SE=standard error; 95% CI=95% confidence interval)
Table 6.
Two post-hoc trend analyses for the IQ × Group, and IQ× Listening Condition interactions in the baseline LMM ANOVA. (ASD=autism spectrum disorder; NT=neurotypical; IQ=intelligence quotient; SE=standard error; 95% CI=95% confidence interval)
| Interactions | Trend | SE | 95% CI | t value | p value |
|---|---|---|---|---|---|
| ASD*IQ | 0.07 | 0.01 | 0.05 – 0.09 | 7.07 | < 0.0001 |
| NT*IQ | -0.02 | 0.02 | -0.05 – 0.02 | -1.04 | 0.31 |
| Quiet*IQ | 0.01 | 0.01 | -0.01 – 0.03 | 1.02 | 0.31 |
| Noise*IQ | 0.04 | 0.01 | 0.02 – 0.06 | 3.66 | < 0.001 |
| Pairwise contrasts | Estimate | SE | t value | p value | |
| ASD*IQ – NT*IQ | 0.09 | 0.02 | 4.31 | < 0.0001 | |
| Quiet*IQ – Noise*IQ | -0.03 | 0.007 | -3.79 | < 0.001 | |
Table 7.
Linear Mixed-Effects Model formula and output for the in-noise accuracy data recorded with and without HAT use. (NT=neurotypical; IQ=intelligence quotient; HAT=hearing assistive technology; RAU= rationalized arcsine units; SE=standard error; 95% CI=95% confidence interval; df=degree of freedom; ICC=intraclass correlation coefficient; N SUBJ=the number of subjects)
Table 7.
Linear Mixed-Effects Model formula and output for the in-noise accuracy data recorded with and without HAT use. (NT=neurotypical; IQ=intelligence quotient; HAT=hearing assistive technology; RAU= rationalized arcsine units; SE=standard error; 95% CI=95% confidence interval; df=degree of freedom; ICC=intraclass correlation coefficient; N SUBJ=the number of subjects)
| Formula code: Accuracy ~ Group+ HAT-use + IQ + Group:HAT-use + Group:IQ + HAT-use:IQ + (1|Subeject) | |||||
| Sentence recognition accuracy (RAU) | |||||
| Fixed effect | Estimate | SE | 95% CI | t value | p value |
| (Intercept) | -0.94 | 1.15 | -3.23 – 1.35 | -0.82 | 0.42 |
| Group: NT | 11.02 | 2.52 | 6.02 – 16.03 | 4.38 | <0.001 |
| HAT-use: On | 4.81 | 0.89 | 3.04 – 6.58 | 5.40 | <0.001 |
| IQ | 0.08 | 0.01 | 0.06 – 0.10 | 7.37 | <0.001 |
| Group: NT*HAT-use: On | -1.28 | 0.32 | -1.91 – -0.64 | -4.02 | <0.001 |
| Group: NT*IQ | -0.08 | 0.02 | -0.12 – -0.04 | -3.97 | <0.001 |
| HAT-use: On*IQ | -0.03 | 0.01 | -0.04 – -0.01 | -3.00 | 0.004 |
| ICC | 0.63 | ||||
| N SUBJ | 45 | ||||
| Observations | 90 | ||||
| Marginal R2 / Conditional R2 | 0.671 / 0.878 | ||||
Table 8.
Summary of the HAT LMM ANOVA. (HAT=hearing assistive technology; IQ=intelligence quotient; df=degree of freedom; η²p=partial eta squared)
Table 8.
Summary of the HAT LMM ANOVA. (HAT=hearing assistive technology; IQ=intelligence quotient; df=degree of freedom; η²p=partial eta squared)
| Effect | F-ratio | df | p value | η²p |
|---|---|---|---|---|
| Group | 17.12 | 1.07, 41 | <0.001 | 0.29 |
| HAT-use | 18.67 | 1.05, 42 | < 0.001 | 0.32 |
| IQ | 6.31 | 1.07, 41 | < 0.05 | 0.12 |
| Group × HAT-use | 16.18 | 1.05, 42 | <0.001 | 0.28 |
| HAT-use × IQ | 8.98 | 1.05, 42 | <0.01 | 0.18 |
| Group × IQ | 15.73 | 1.07, 41 | <0.001 | 0.26 |
Table 9.
Post-hoc analysis for the Group × HAT-use interaction in the HAT LMM ANOVA (only research-related contrasts shown). (HAT=hearing assistive technology; ASD=autism spectrum disorder; NT=neurotypical; SE=standard error; df=degree of freedom; 95% CI=95% confidence interval)
Table 9.
Post-hoc analysis for the Group × HAT-use interaction in the HAT LMM ANOVA (only research-related contrasts shown). (HAT=hearing assistive technology; ASD=autism spectrum disorder; NT=neurotypical; SE=standard error; df=degree of freedom; 95% CI=95% confidence interval)
| Pairwise contrasts | Estimate | SE | df | t value | p value | |
|---|---|---|---|---|---|---|
| ASD off – ASD on | -1.98 | 0.18 | 42.0 | -10.48 | <0.001 | |
| NT off – ASD on | -0.26 | 0.39 | 52.3 | -0.68 | 1.000 | |
| NT off – NT on | -0.71 | 0.23 | 42.0 | -3.12 | <0.05 | |
| Estimated marginalmeans | SE | df | 95% CI | |||
| ASD off | 8.07 | 0.22 | 58.1 | 7.62 – 8.51 | ||
| ASD on | 10.05 | 0.22 | 52.5 | 9.06 – 10.50 | ||
| NT off | 9.79 | 0.31 | 50.8 | 9.14 – 10.43 | ||
| NT on | 10.50 | 0.32 | 52.8 | 9.85 – 11.14 | ||
Table 10.
Two post-hoc trend analyses for the HAT-use × IQ, and Group × IQ interactions in the HAT LMM ANOVA. (HAT=hearing assistive technology; ASD=autism spectrum disorder; NT=neurotypical; IQ=intelligence quotient; SE=standard error; 95% CI=95% confidence interval)
Table 10.
Two post-hoc trend analyses for the HAT-use × IQ, and Group × IQ interactions in the HAT LMM ANOVA. (HAT=hearing assistive technology; ASD=autism spectrum disorder; NT=neurotypical; IQ=intelligence quotient; SE=standard error; 95% CI=95% confidence interval)
| Interactions | Trend | SE | 95% CI | t value | p value | ||||
|---|---|---|---|---|---|---|---|---|---|
| HAT-off*IQ | 0.04 | 0.01 | 0.02 – 0.06 | 3.45 | 0.001 | ||||
| HAT-on*IQ | 0.01 | 0.01 | -0.009 – 0.03 | 1.21 | 0.23 | ||||
| ASD*IQ | 0.07 | 0.01 | 0.05 – 0.09 | 6.73 | < 0.001 | ||||
| NT*IQ | -0.02 | 0.02 | -0.05 – 0.02 | -0.83 | 0.41 | ||||
| Pairwise contrasts | Estimate | SE | t value | p value | |||||
| HAT-off*IQ – HAT-on*IQ | 0.03 | 0.008 | 2.99 | < 0.01 | |||||
| ASD*IQ – NT*IQ | 0.08 | 0.02 | 3.97 | < 0.001 | |||||
| 1 | English meaning: “The father brought back a large watermelon.”. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



