
Submitted:
29 March 2023
Posted:
30 March 2023
You are already at the latest version
Abstract
Corneal opacity is a leading cause of vision impairment and suffering worldwide. Transplantation can effectively restore vision and reduce chronic discomfort. However, there is a considerable shortage of viable corneal graft tissues. Tissue engineering may address this issue by advancing xeno- keratoplasty as a viable alternative to conventional keratoplasty. In particular, livestock decellularization strategies offer the potential to generate bioartificial ocular prosthetics in sufficient supply to match existing and projected needs. To this end, we have examined the best practices and characterizations that have supported the current state-of-the-art driving preclinical and clinical applications. Identifying the challenges that delimit activities to supplement the donor corneal pool derived from acellular scaffolds allowed us to hypothesize a model for keratoprosthesis applications derived from livestock combining 3D printing and decellularization.
Keywords:
cornea
; xeno-keratoplasty
; decellularization
; recellularization
; 3D bioprinting
; slaughterhouse waste
1. Introduction
After cataracts and glaucoma, corneal opacity is the fourth leading cause of blindness worldwide [1]. This problem arises from structural and functional damage to the cornea. It can occur from diverse conditions and infections that lead to varying degrees of visual impairment, ultimately resulting in partial or total blindness [2]. Corneal opacity treatments are based on the underlying condition and include oral and ocular medications, phototherapeutic keratectomy (laser ablation surgery), and transplantation (keratoplasty). Advances in keratoplasty have allowed for partial or complete corneal replacements, depending on the location and severity of the injury [3]. This procedure can restore vision, reduce pain, and improve the appearance of a damaged or diseased cornea. However, this procedure carries the risk of several complications.
Partial or full-thickness keratoplasty techniques include endothelial, anterior lamellar, penetrating keratoplasties, and keratoprosthesis implantation [3]. Approximately 180,000 procedures are performed annually worldwide [4] yet the supply of corneal grafts is insufficient to meet the current and growing demand for transplantation. For instance, in 2015, there were 10 million patients left untreated worldwide [5], resulting in only 1 in 70 transplants [1]. Unfortunately, graft recipients often experience several complications resulting from surgical procedures and recovery, which lead to graft failure and rejection. Coupling the supply and demand mismatch with a 35-70% chance of graft compromise after two years of the procedure necessitates the consideration of alternative approaches that simultaneously increase the graft supply and long-term transplantability [6].
Such alternatives are being developed using artificial and bioartificial scaffolds that can form a basis for transplantable constructs. These efforts date back to reports by Nussbaum, who created the first keratoprosthetic prototype using a quartz crystal and implanted it into the rabbits’ cornea [7]. Thereafter, corneal substitutes created from glasses and quartz rimmed with platinum formed the initial generation of keratoprostheses (Kpros). Even though these Kpros could function between 6-36 months, they were gradually abandoned due to their heaviness, stiffness, and capacity to induce infections [7]. These issues drove the need for alternative materials that would be biocompatible and lighter. The discovery of poly (methyl methacrylate) (PMMA), a synthetic artificial material, during the second world war fulfilled these important requirements and provided new ways to address corneal degeneration. For instance, Boston Keratoprosthesis was the first group to devise a synthetic keratoprosthesis using a PMMA backplate secured with a titanium locking ring [7]. With this approach, donor corneal tissues are placed in between the anterior PMMA layer and the backplate, however it does not eliminate the need for donor human corneas. Since then, advancements in the field have led to various synthetic alternatives, such as the Osteo-Odonto-Keratoprosthesis (OOKP) that is composed of a donor root tooth and alveolar bone to support a PMMA optical cylinder [8]. This system was then further combined with a larger biconvex optic to enhance its design.
A major drawback of OOKP is that is requires a complex surgical technique that often results in complications involving the mucosa, retina, and lamina that affect visual outcomes [7]. Ultimately, such issues, along with high costs and prerequisites that limited the patient pool, led to the system being discontinued. In comparison, the rigidity of PMMA ensured that Kpros designed from this material required a resilient skirt material to assist the tight attachment with host eye, which in turn led to further complications [7]. Therefore, scientists have searched for other materials, like cross-linked poly (2-hydroxyethyl methacrylate) (PHEMA), fibronectin, poly(ethylene glycol) (PEG) and fluorocarbon polytetrafluoroethylene (PTFE) to produce better corneal alternatives or skirts for PMMA-made Kpros [7,9]. Two examples are, the Alphacor™, which is composed of PHEMA, and the Korea Seoul-type keratoprosthesis, which contains PMMA and a PEG skirt [7]. A third example of a synthetic cornea alternative is the most recent addition, the CorNeat KPro. This artificial corneal implantation device is composed of electrospun nanofibers and a biocompatible, nondegradable biomimetic material that imitates the microstructure of the ECM [14]. It is a collagen mesh that provides structural and biochemical support to surrounding cells differing from scaffolding and collagen matrices used in tissue repair due to its nondegradable nature. Its ECM is designed to resemble the imitate the native microarchitecture, to support fibroblast migration and colonization, which play a crucial role in wound healing [14]. Interestingly, in vivo studies have shown increased proliferation of fibroblasts and collagen fibrils within several weeks of implantation, indicating progressive tissue integration and graft remodeling that can benefit such Kpros [14]. Regardless, synthetic corneal replacements are criticized due to multiple complications, including severe levels of inflammation and their non-aesthetic appearance []. Moreover, the currently explored synthetic materials used for generating suitable keratoprosthesis are quite limited as aforementioned.
In comparison, bioartificial corneal scaffolds have been considered effective substitutes for reducing immunogenicity and enhancing compatibility and integration into the recipient [10,11]. As mentioned before, the supply of human donor corneas is incapable of meeting existing and projected transplantation needs. As a result, researchers turned their attention to obtaining replacement corneal tissues from xenogeneic resources. One promising approach to support this process is tissue/organ decellularization, which supports the generation of ECM-rich scaffolds that can be as templates to create viable corneal substitutes. Decellularization removes the cellular and genetic components of original tissues thereby decreasing immunogenicity, while maintaining biocompatibility, innate architecture, and various bioactive factors that can drive regeneration and remodeling in vivo [12,13,14,15,16,17,18,19,20,21]. For instance, Xenia® is a custom-made product derived from decellularized porcine corneas [22,23,24]. In clinical settings, these substitutes have reduced the risk for host-immune responses, compared to native (non-decellularized) xenografts, while experiencing appreciable degrees of integration into the implantation site and visual acuity [22]. Furthermore, this form of xenotransplantation offers the potential to better balance the supply/demand mismatch for corneal transplantation [25].
Throughout history, numerous attempts have generated Kpros from pigs, sheep, dogs, rabbits, and, more recently, gibbons, cows, and fish [26]. Remarkably, the cornea is considered an immune-privileged tissue, as it is not immediately vascularized. This characteristic supports its conduciveness xenografting [25]. Moreover, recent studies have also revealed the potential to generate a limitless supply of corneal xenografts using slaughterhouse waste [11,27,28,29,30]. Based on this potential, we assess current applications and performance in preclinical and clinical practices of various decellularization protocols used to create Kpros and their ability to maintain pertinent structural and physiological capacities. In addition, we propose an alternative corneal xenograft model that may be realized using 3D bioprinting and decellularization technologies. Our evaluations and research-based judgments of synthetic and bioartificial grafts may help establish and guide future research and expedite progress in clinical settings.
2. Methods of corneal decellularization
The decellularization procedure aims to effectively remove cellular and nuclear material while maintaining the biochemical composition and biomechanical integrity of the residual ECM) to support the development of new tissue. It provides a more effective alternative to ease the constraints of autologous grafting than synthetic vascular tissue engineering procedures [10,20]. The elimination of cellular components and related waste should reduce any potential host rejection or immune reaction [27]. The purpose of corneal decellularization is to yield biocompatible ECM components that possess latent biochemical cues to support in vivo tissue remodeling and long-term transplantability [10,20]. As the corneal stroma has the most organized ECM in the body, maintenance of the tissue architecture, protein, and glycosaminoglycan (GAG) content is particularly important [28]. The corneal stroma is a dense, collagen-rich ECM assembled in regularly packed collagen fibrils that are responsible for tissue transparency [10,11,31]. The collagen fibrils have a uniform distribution of small (25-35 nm) diameters, which are assembled parallel to each other in 200-250 nm thick orthogonally stacked layers called lamellae [10,31,32]. Hence, the maintenance of this distinctive structure is a crucial part of the corneal decellularization protocols.
In general, corneal decellularization involves the breakdown of the cellular membrane followed by an enzymatic process separating the cell’s constituents from the ECM. Then, cytoplasmic, nuclear components, and cellular debris are removed with detergents and other reagents/processes that disrupt plasma membranes. Afterward, it is necessary to ensure that all residual chemicals have been removed from the tissue. Unremoved decellularizing agents can continue to alter the ECM composition, adversely disrupt the scaffold ultrastructure [10], and generate immunogenic responses post-transplantation [13]. Hence, it is necessary to employ several biological, chemical, and physical methods used in the corneal decellularization process (Table 1 and Figure 1) to adequately remove the cellular and nuclear components of the tissue while keeping the intricate balance of GAG and structural proteins required to build scaffolds that closely mimic native ECM [10,32]. Most of these techniques have been examined in bovine, ovine, and porcine corneas [10,11,27,28,33,34]. An overview of some commonly used approaches, which can be primarily classified as biological, chemical, and physical, for corneal decellularization and their effects on cellular and extracellular tissue constituents is presented in the text below.
2.1. Biological techniques for the decellularization of cornea
2.1.1. Enzymatic agents
Enzyme-based treatments for decellularization disrupt the bonds and interactions between nucleic acids, as well as interacting cells in neighboring proteins and other cellular/tissue components [20]. These types of treatments are advantageous over other decellularization protocols in that they provide high specificity for removing cellular and detrimental ECM elements [10,35,36]. For example, trypsin, dispase, and phospholipase A2 (PLA2) are commonly used enzymatic treatments. Trypsin is a serine protease that targets the C-side bonds in arginine and lysine amino acids and is mostly used combined with ethylenediaminetetraacetic acid (EDTA), a chemical agent able to break cell-matrix interactions [10,36]. Notably, extended exposure to trypsin-EDTA treatment can dramatically alter the matrix’s structure, degrade laminin, and remove GAGs, reducing the tissue’s mechanically strength as it degrades collagen fibers [37,38]. As a result, it may not be well suited for corneal decellularization. Furthermore, epithelia and endothelia have been removed following treatment with Dispase II [39] before being fully decellularized using a subsequent method. It breaks down peptides linked to particular basement membranes proteins like collagen IV and fibronectin, but if administered over an extended length of time, it can also harm the basement membrane [40]. After delipidation of the dermis, a direct comparison of trypsin and dispase treatments showed superior decellularization by dispase accompanied by increased ECM disruption [41]. Likewise, PLA2 is an esterase that hydrolyses phospholipid components of cells but does not react with collagens or proteoglycans [42]. Hence, the application of PLA2 in decellularization helps maintain collagen and proteoglycans in the resulting scaffold [10,39]. It has also been demonstrated that PLA2, along with sodium deoxycholate [43], was influential in producing the acellular porcine corneal [42,44]. Other studies have also suggested that combining PLA2 with a bicarbonate salt, results in effective cellular removal and maintenance of collagen fibers [42,45].
Furthermore, with respect to combinative treatments, nucleases are mainly applied with other detergents to expedite the removal of DNAs and RNAs from scaffolds [46,47,48]. Nucleases such as RNase and DNase, are frequently used to cleave nucleic acids and aid in the removal of nucleotides after cell lysis in tissues [32]. For instance, porcine corneas treated with DNase and RNase resulted in the efficient decellularization, but the tissue became opaque due to severe distortion of the collagen structure [49]. However, other studies have identified, in many cases, as a general consequence of decellularization, and optical clearing agents like glycerol have been provided an ability to substantially reverse opacity [28,50,51,52], while providing antimicrobial benefits [53,54,55]. Compared with exonucleases, endonucleases such as benzonase [56] may be more effective because they cleave nucleotides mid-sequence and thereby more effectively remove DNA fragments [10]. Likewise, another category of enzymes, such as sera-derived enzymes, including fetal bovine serum, contain nucleases that can degrade both DNA and RNA [57]. They supports the removal of nucleic acids from tissues but fail to remove immunogenic elements [32]. The xenogeneic serum may also introduce immunogenic elements into the ECM which can cause adverse responses following recellularization or transplantation [32,58]. Moreover, the human serum has also been used as a standalone decellularizing agent to produce porcine decellularized cornea [3], after first mechanically removing the epithelium [58].
2.1.2. Non-enzymatic agents
Following the complete description of enzymatic agents used in decellularization, non-enzymatic treatments include the use of chelating agents and serine protease inhibitors. Chelating agents such as ethylenediamine tetra-acetic acid (EDTA) aid cell dissociation via the separation of metal ions [10,32,35]. However, these same mechanisms can lead to the disruption of protein-protein interactions [32]. Chelating agents alone are incapable of adequate cellular removal. Thus, they are often used in combination with enzymes and detergents [32]. EDTA has also been used with sodium dodecyl sulfate (SDS), a potent ionic detergent, to effectively decellularize corneal tissues [59].
In comparison, serine protease inhibitors, like aprotinin, phenylmethylsulfonyl fluoride, and leupeptin, can prevent some of the detrimental effects to the ECM caused by intracellular proteases released after cellular lysing process [10]. Specifically, protease inhibitors often accompany harsh detergents and decellularizing agents. One common agent used for corneal decellularization is aprotinin [10], an inhibitor of trypsin and related proteolytic enzymes. In studies that utilized these agents, authors have reported minimal damage to the ECM despite the use of harsh decellularizing agents [60,61]. A summary of enzymatic and non-enzymatic decellularization techniques is presented in Table 1 below.

Table 1.
Methods for cornea decellularization and associated mechanisms, advantages, and disadvantages.
Table 1.
Methods for cornea decellularization and associated mechanisms, advantages, and disadvantages.
| Methods/Techniques | Mechanism of Action | Advantages | Disadvantages |
|---|---|---|---|
| Biological | |||
| Enzymatic Agents | |||
| Trypsin [35,39,62] | Hydrolyzes protein and disrupts protein-protein interactions | Breaks cell-matrix interactions | An extended exposure can disrupt the collagen structure |
| Dispase [56] | Cleaves peptides associated with basement membrane proteins | Can aid the decellularization process by initially removing epithelium and endothelium | May cause damage to the basement membrane |
| Phospholipases A2 (PLA2) [42] | Hydrolyzes phospholipid components of cells | Effective at the removal of DNA and residual cellular components that tend to adhere to ECM proteins Helps maintain collagen and proteoglycans in the corneal tissue |
|
| Nucleases (RNase and DNase) [63] | Cleaves nucleic acids and aid in their removal | Effective at the removal of DNA and residual cellular components that tend to adhere to the stroma’s ECM proteins | Incomplete removal of the enzymes may impede recellularization and successful transplantation |
| Sera [42] | Serum nucleases degrade DNA and RNA. | Effectively removes cells while maintaining tissue transparency | The use of non-human sera carries a risk of cross-species transmission of pathogens |
| Non-enzymatic Agents | |||
| EDTA [64] | Dissociates cells by separating metal ions | Can be used for effective when combined with other agents | Ineffective at cell removal when used unaccompanied |
| Chemical | |||
| Alcohols | |||
| Ethanol [10,65] | Dehydrates and lyses cells. Removes lipids from tissues. |
More effective in removing lipids from tissues than lipase Antimicrobial, antifungal, and antiviral properties |
Can cause damage to the ultrastructure of tissue |
| Glycerol [20,66] | Dehydrates and lyses cells Removes lipids from tissues |
Can maintain or restore corneal transparency Cryoprotectant for long-term cornea storage |
Can cause damage to the ultrastructure of tissue |
| Acids and Alkalis | |||
| Peracetic acid [62,65] | Solubilizes cytoplasmic components of cells Removes nucleic acids via hydrolytic degradation |
Acts to simultaneously sterilize tissue | Ineffective decellularization that can also disrupt the ECM |
| Ammonium hydroxide [67,68] | Hydrolytic degradation of biomolecules | Results in complete DC with little effect on collagen architecture | Can eliminate GFs and reduce mechanical properties |
| Ionic Detergents | |||
| Sodium dodecyl sulfate(SDS) [60,65] | Solubilizes cell membranes and dissociates DNA from protein Disrupts protein-protein interactions |
Complete removal of cells can be achieved | Can be highly detrimental to ECM structure including disorganization of collagen fibrils and loss of GAGs Loss of tissue transparency |
| Sodium deoxycholate [20,43,63] | Solubilizes cell membranes and dissociates DNA from protein Disrupts protein-protein interactions |
Complete removal of cells can be achieved when used with other agents | Less effective at removal of cells |
| Non-ionic Detergents | |||
| Triton X-100 [63] | Breaks up lipid-lipid and lipid-protein interactions | Mild and non-denaturing | Less effective than ionic detergent treatments Can cause damage to the ECM |
| Zwitterionic Detergents | |||
| CHAPS [64,69] | Has properties of non-ionic and ionic detergents | Better cell removal than non-ionic detergents Improved preservation of the ECM ultrastructure than ionic detergents |
Poor cellular removal Very disruptive to stromal architecture |
| Hypo- and Hypertonic Solutions | |||
| Sodium Chloride (NaCl) [10,64,70] | Detaches DNA from proteins | Can maintain optically clarity Ability to maintain the stromal architecture and retain GAG content |
Does not remove cellular residues Mixed reports on the success of cell removal efficiency |
| Tris-HCl [10,64] | Lyses cells by osmotic shock | Reduces decellularization time | Mixed reports on cell removal |
| Physical | |||
| Freeze-thawing [20,32] | Ice crystal formation causes cell lysis | Effectively destroys tissue and organ cells | Expensive Needs subsequent treatment to remove cells Enhanced pore formation and disruptions to ECM |
| Hydrostatic Pressure [10,20,32,62] | Increase in pressure results in cell lysis | Effectively decellularizes whilst maintaining collagen fibril structure Kills bacteria and viruses |
Expensive |
| Sonication and Mechanical Agitation [71] | Cell lysis and removal | Does not remove DNA remnants from the corneal tissue | Only effective with enzymatic treatments |
2.2. Chemical techniques for the decellularization of cornea
2.2.1. Acid and alkali treatment
As one of the common chemical techniques for decellularizing, acids, and bases cause or catalyze hydrolytic degradation of biomolecules. Acids were found to dissociate nuclear DNA from ECM by disrupting nucleic acids and solubilizing cytoplasmic components. Additionally, solutions with extreme pH levels were indicated to be highly effective in the decellularization process [12]. For instance, it has been shown that increasing the pH of the zwitterionic agent, cholamidopropyl dimethyl ammonio-1- propane sulfonate (CHAPS) during decellularization increases the effectiveness of cell and protein removal [12]. Significantly, increasing the pH of a compound could also eliminate growth factors and disrupt the mechanical structure of the scaffold. Overall, acid and alkali treatments are effective at solubilizing cytoplasmic components and eliminating nucleic acids [72], by catalyzing hydrolytic degradation of biomolecules [32]. However, such solutions may also degrade essential bioactive molecules such as GAGs from collagenous tissues. To illustrate this point, the use of potent acids to facilitate decellularization have resulted in retention of sulfated GAGs, but the damage and removal of collagen from scaffolds, thereby reducing the structural integrity ECM [12,32].
Apart from CHAPS, peracetic acid is a highly corrosive and commonly used disinfectant and oxidizing agent used in sterilization [62]. It doubles as a decellularization agent by removing residual nucleic acids with minimal effect on the ECM composition and structure [32]. Limited success has been reported with corneal tissue when used alongside ethanol, however, Kao et al. considered further optimization was necessary [10]. In addition, peracetic acid has been reported to retain GAG content and preserve the structure and function of important growth factors [72].
In addition to acids, ammonium hydroxide, in its capacity as an alkaline-based treatment, has been used in conjunction with the detergent Triton X-100 to decellularize human corneas [46]. The treatment effectively decellularized the tissue with little apparent effect on the collagen architecture and basement membrane proteins [10]. Nevertheless, ammonium hydroxide is also known to degrade growth factors and adversely alter the mechanical properties of the ECM.
2.2.2. Alcohols
Another class of decellularizing agents is alcohols. The mechanism by which these compounds decellularize tissues is based on is their ability to dehydrate tissues, and ultimately lyse cells [32,34]. Alcohols such as ethanol and isopropanol are commonly used to degrade lipids, which are integral components of the plasma membrane [10]. They are more effective in removing lipids from tissues than lipases [32]. Previous reports have shown that ethanol treatments have resulted in complete corneal decellularization whilst maintaining the overall tissue structure [65]. Interestingly, corneal stromal cells cultured on ethanol-treated decellularized corneas (DCs) were reported to proliferate slower and produce more new ECM components, in comparison to those cultured on DCs produced using detergents [65]. However, care should be taken while using alcohols as a decellularizing agent, as they can act as a tissue fixative [73] that can crosslink or precipitate proteins [73], damage the ECM ultrastructure [32], and disrupt collagen fiber alignment, leading to corneal opacity [66].
Apart from ethanol and isopropanol, glycerin dehydration has been used since the 1960s for prolonged storage of donor corneas for later transplantation [10]. More recently, in vivo confocal microscopy techniques have shown that antigen-presenting cells and stromal cells were, in fact, absent in glycerine-cryopreserved allografts (GCA) used in transplantation procedures into human recipients [74]. These DCs showed promising results when transplanted into patients, but were also plagued by a high risk of rejection due to infection and inflammation [45]. Afterward, in a clinical study, no rejection was seen with the GCA, whilst only 10% of eyes that received fresh corneal allografts (FCA) reported episodes of stromal rejection [45]. Another clinical study reported similar findings with no rejection cases in the GCA group and one case of stromal rejection in the FCA group [74]. This suggests that glycerol cryopreservation may be a promising technique for producing DCs for use in corneal grafting procedures, with apparent clinical efficacy. Glycerol has also been used as a post-treatment to restore corneal transparency [64] and as a preservation technique for DCs.
2.2.3. Surfactants
By far the most commonly employed methods of decellularization are based on the use of surfactants. Surfactants are chemical agents used to solubilize cell membranes and to dissociate their inner structure. These agents also dissociate DNA from proteins, and they are therefore effective in removing cell materials from tissues [32]. Surfactants are classified into three genres: ionic, non-ionic, and zwitterionic. For example, polyethylene glycol (PEG), an amphiphilic copolymer, which is non-ionic compound that damages cell membranes and has been shown to satisfactory decellularize pig and human corneas [61]. Whereas SDS, an anionic surfactant agent, rapidly ablates cells and cell membranes [20]. SDS is widely used for corneal decellularization, yet the protocols are not standardized [75]. According to the reported studies, Zhou et al. employed 0.1% (wt./vol.) SDS for cornea decellularization that lasted 7 hours at 37 °C [35,76], whereas Gonzalez-Andrades et al. recommended to immerse corneas in 0.1% (vol/vol) SDS for 48 hours at room temperature accompanied with 300 rpm successive shaking [35,77].These procedures resulted in varying degrees of decellularization.
Similarly, zwitterionic detergents, like 3-[(3-cholamidopropyl dimethylammonio]-1-propane sulfonate)] (CHAPS), have been applied in both immersion and perfusion decellularization procedures [62]. Zwitterionic detergents possess properties of both ionic and non-ionic detergents, and have shown to better support cell removal from native tissues than non-ionic detergents, and preserve of the ECM ultrastructure than ionic detergents (Hudson et al., 2004; Gupta et al., 2018; Heath, 2019). However, CHAPS have been criticized as cytoplasmic proteins and cell fragments were retained in stromal tissue scaffolds, indicating ineffective decellularization [10,72,78]. When used for corneal decellularization, poor cellular removal, as well as damage to ECM proteins has been reported [78]. Except for CHAPS, some surfactant-treated samples will unfortunately succumb to detrimental structural disruptions, namely the unwanted removal of valuable ECM proteins as evidenced by proteomic studies [10,32,57]. For example, the use of Triton X-100 to facilitate decellularization is not appropriate for tissues where GAG and lipid retention are essential [62]. Triton X-100 can often denature cell membranes without denaturing proteins, however at higher concentrations this non-anion detergent can breaks protein-to-protein interactions and degrade tissue architectures, while providing lower decellularization efficiencies and degree of transparencies, than ionic agents like SDS [10,61]. As a result, to decellularize the cornea it has been used in combination with other agents including hydroxylamine [56], and Dispase II, for the removal of the corneal epithelium [10] and nucleases, to aid in the complete removal of cellular debris. These confounding factors have made it difficult to assess detergent efficiency and the effects on the ECM, in the latter cases. However, in all cases adequate levels of decellularization was reported and the tissue’s ultrastructure and mechanical properties were well preserved following the decellularization process [10,62].
2.2.4. Hypotonic and hypertonic solutions
Excluding the aforementioned chemical treatments, hypertonic and hypotonic solutions can also disrupt cell stability owing to osmotic pressure generated between internal and external tissue membranes, resulting in cellular lysis [20,36]. This lysing process, however, is not known to remove the cellular residues that it releases into the ECM, which reduces this processes effectiveness as a decellularization technique. Nevertheless, improve decellularization efficacies can be obtained in conjunction with other chemical reagents, since they do not disturb ECM composition [12]. The use of hypertonic sodium chloride (NaCl) solution has been investigated for DCs [56] Results from such studies have shown that the hypertonic solution caused minimal damage to stromal architecture and retained many extracellular growth factors and proteoglycans [79]. As a result, the DCs produced from this method are known to retain optical clarity after decellularization. Moreover, using tris-HCl buffers as a pretreatment at 4 °C, to initially lyse cells before further treatment with previously mentioned reagents has the advantage of reducing the incubation time needed in the harsher decellularizing techniques [10].
2.3. Physical techniques for the decellularization of cornea
2.3.1. Freeze-thaw cycles
Physical technologies are also considered as an essential component in decellularization protocols. The application of freeze-thaw cycle have been shown to effectively degrade cells in tissue via the formation of intracellular crystals [32]. Freeze thaw cycles are generated by fluctuating between freezing temperature (−87 °C) and biological temperature (37 °C) [12,20]. such fluctuations help frozen water crystals occupy significant volumes inside cells, and thus cause their membranes to rupture. This process aids uniform degree of decellularization [36,80]. However, varied crystalline geometries may damage the scaffold, and alter the mechanical stability of the ECM [20,69]. Experiments by Xaio et al. utilized snap freezing followed by lyophilization to induce pore formation in DCs. The ice crystals formed during pre-freezing were sublimated under vacuum conditions leaving a network of interconnected pores that enabled infiltration by cells [10]. Pulver et al., 2014 [81], Xing et al., 2015 [82], and Rahman et al., 2018 [44] have also shown that multiple freeze-thaw cycle can be used for decellularization [12]. Freezing and incubating the tissue in nitrogen gas has been used to induce apoptosis, as freezing alone can be insufficient [10]. Furthermore, nitrogen freezing of tissues is a relatively mild, yet costly treatment when compared to enzymatic or detergent treatments [10].
2.3.2. High hydrostatic pressure
Compared with freeze-thaw cycle, high hydrostatic pressure (HHP) processes disrupt cellular membranes within the corneal tissue via the generation of isostatic pressures. Pulses of water are sprayed on tissues immersed in saline to generate acellular scaffolds [20,80]. The use of high hydrostatic pressure is non-cytotoxic and successfully removes cells whilst destroying bacteria and viruses [66]. Studies have demonstrated that this approach of decellularization can be more effective than detergents or enzymes while providing an ample platform for recellularization, despite the fact that the ice crystal formation may alter ECM ultrastructure [32,80]. However, in order to prevent non-ideal structural alterations in the ECM, the amount of force applied needs to be accurately managed [20]. High hydrostatic pressure has been reported to successfully decellularize porcine corneas whilst maintaining the collagen fibril matrix and GAG content [10] Nevertheless, this procedure is costly, as it requires specialized equipment to induce pressures of up to 1 GPa that are need to generate viable acellular corneal tissues [66].
2.3.3. Sonication and mechanical agitation
Unlike HHP and freeze-thaw cycles, which can be applied independently, sonication and mechanical agitation are used in combination with chemical and enzymatic treatments for decellularization [72]. For example, a porcine retinal specimen was completely decellularized using a hydrostatic pressure of 980 MPa for 10 minutes in a study by Hashimoto et al. [83]. The aorta of a pig sample was likewise the subject of a similar study. In both instances, a chemical agent was required to destroy and remove DNA remnants from the tissue because the physical approach by itself was unable to do so [80]. As a result, sonication, and mechanical agitation work better when used with chemical and enzymatic decellularization agents.
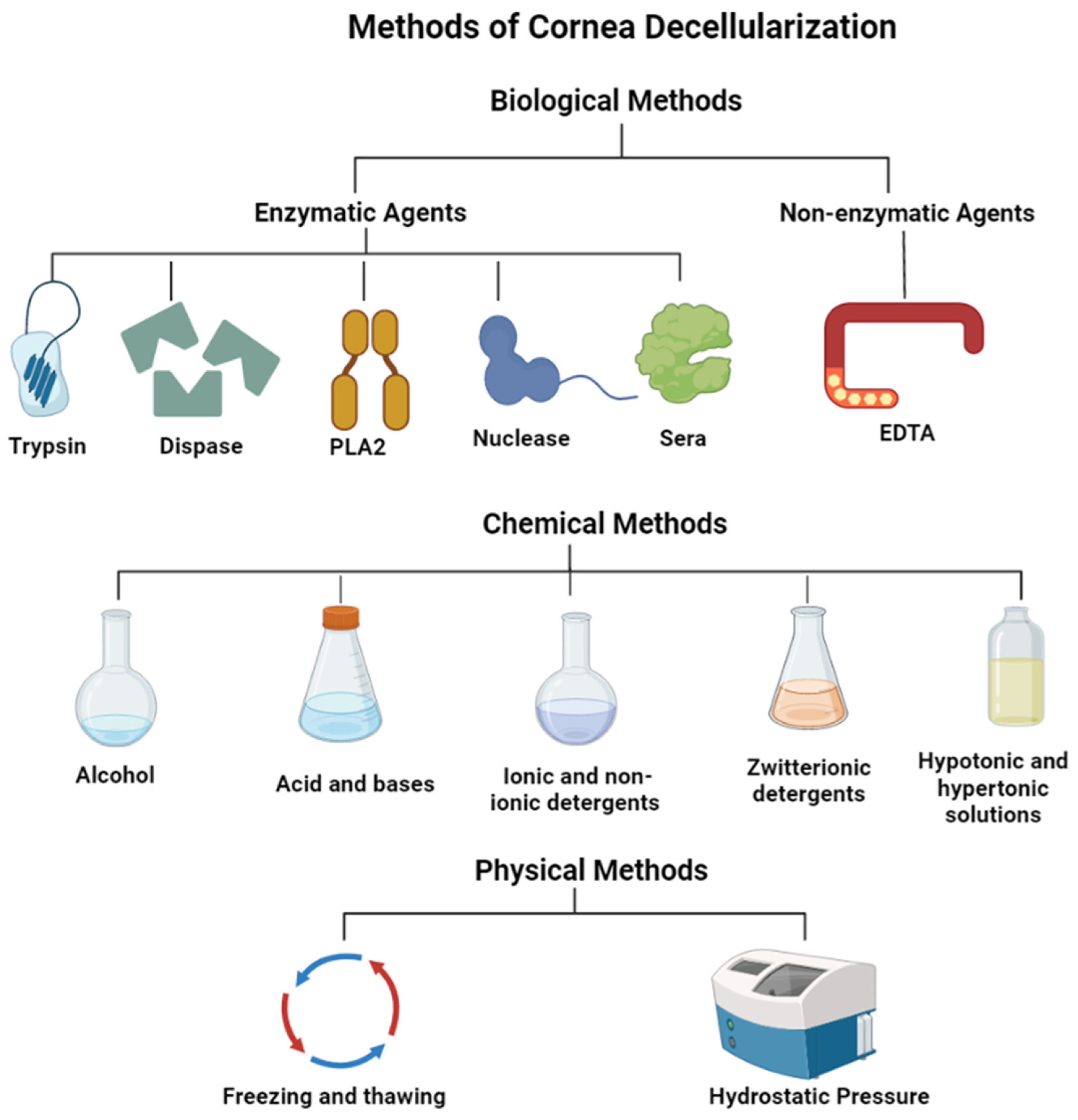
Figure 1.
Methods for cornea decellularization.
3. Characterization of decellularized cornea prostheses
Various techniques are capable of creating corneal scaffolds through decellularization. Meanwhile, each of them has pros and cons, targeting distinct components of tissues/cells to form scaffolds with different properties, which necessitates their individual characterization. To create corneal scaffolds with favorable biological and mechanical performances, characterizations of these substitutes before in vivo studies is extremely crucial. Such characterizations involve the assessment of the cellular removal efficacy, maintenance of structure and function of scaffolds, biocompatibility, biodegradability, potential for remodeling, cytotoxicity, pathogenicity, and immunogenicity with the post-transplantation environment [84].
Accordingly, incomplete removal of cellular materials can trigger unfavorable host responses as well as associated cytocompatibility issues [85,86]. Hence, the protocols for decellularization of cornea should be monitored to discern whether complete decellularization, including removal of all cellular debris has occurred, and ECM integrity has been maintained after processing [10]. As a further step, characterizations can be done to determine the retention of the native ECM components and their resulting mechanical and physiological characteristics. This is because ECM is extremely pivotal for sustaining normal structure and function of corneas and no other tissues of human body rely more on ECM and its components compared with corneas [87]. Except for the biocompatibility and biodegradability, the prerequisite for in vivo grafting, the functionalization characterizing of decellularized cornea grafts such as the ability of cell repopulation and anti-infections, mechanical properties like pressure resistance, elastic stiffness, and optical features including proper anterior refractive power for the eye, high transparency and so forth are quite critical for clinical applications [88]. As a result, standardized metrics and approaches are required. Additionally, an ability to routinely gauge decellularization efficacy in an efficient and consistent manner would support future manufacturing purposes [10]. In so doing, computational and artificial intelligence techniques may provide pivotal support in this area [17,18,89,90,91,92]. For the purposes of this study, we will now discuss the characterization of decellularized keratoprostheses in detail by focusing on ways to cellular removal, scaffold biocompatibility, preservation of innate biological attributes, and scaffold recellularization.
3.1. Removal of cellular materials
It has been established that residual DNA is a primary contributor to adverse host reactions [85,86], the associated characterizations are focused mainly on removal of DNA. Currently, effective decellularization criteria require ECM contain <50ng of dsDNA per mg dry weight, DNA fragments shorter than 200bp, and no visible nuclear components [32]. Techniques that facilitate sch characterizations rely on conventional histological and biochemical methods. Brightfield microscopy, hematoxylin-based DNA staining protocols are widely used for evaluating nuclear debris, and it is typically employed in conjunction with eosin to evaluate the fundamental ECM architecture of DCs [9,10,11]. Fluorescent nuclear stains such as DAPI [56,60,79], Hoechst [14,33,42,93], and propidium iodide [79] are also frequently utilized.
By fluorescently labeling the terminal end of nucleic acids, assays like the TUNEL assay, which detect levels of DNA fragmentation, can be used to measure cell death that takes place throughout the decellularization process [33]. DNA staining and imaging are the standard for assessing decellularization, used throughout the body of literature, relatively insensitive and offer a means to quantitatively gauge decellularization efficiency. Additional quantitative information can be extracted from various spectrophotometric assays [57]. Residual DNA fragment sizes can also be assessed by gel electrophoresis. However, the disadvantage of performing these assays and staining protocols to assess residual DNA is that destruction of the sample is required [10].
As complete preservation of ECM ultrastructure is ideal, decellularization protocols aim to minimize its disruption. Unfortunately, there is no reliable reagent or standardized protocol that can achieve complete decellularization [10,32,35] as the term “complete decellularization” is currently not well defined [32]. Hence, the term “sufficient decellularization” is suggested [35]. This term refers to conditioning minimal criteria since it is currently impossible to remove 100% of cellular material while maintaining a viable ECM.
3.2. Biocompatibility evaluation of corneal scaffolds
Following the confirmation of the effective eradication of cellular materials, evaluating the biocompatibility of tissues and organs is critical to limit the potential to induce adverse in vivo consequences. These evaluation studies should be performed based on the rules and guidelines provided by the International Standards Organization (ISO) [84]. Regarding the biocompatibility evaluation, several techniques are presented. In particular, to examine the cytotoxicity of corneal replacements, assays are applied to monitor compounds and characterize the latent harmful effects of scaffolds before clinical use. One of the major parameters considered is an in vitro cytotoxicity evaluation, which measures cell culture viability qualitatively and quantitatively [94]. Such studies are essential, since main concerns are related to the risks using decellularizing and sterilizing agents. For instance, using SDS for decellularization could not only damage the ECM inhibiting future recellularization but also be toxic to the human who is using it [95]. Likewise, sterilizing processes are required to eliminate harmful antigens in scaffolds, so that implantation regimens can generate minimal or untraceable immunogenic responses [32,96]. However sterilizing procedures can denature the scaffold structure, and the ineffective removal of harmful foreign agents can induce toxicity [84]. Therefore, it would be indispensable to test the cytocompatibility after performing sterilizing.
The other concern is the cytotoxicity tests. Cytotoxicity is defined as significant damage on a cellular, functional, and structural level due to a cascade molecular events that interfere with macromolecular synthesis [97]. Studies used to evaluate cytotoxicity expose segments of scaffolds to distinct cell culture lines. By identifying the characteristic signs of toxicity shown by cells, it is not difficult to identify whether cells can thrive in the scaffold environment [98]. Cytotoxicity is preferred to be tested in vitro, since cells cultured in vitro are generally more sensitive to toxic substances compared to in vivo tissues [99]. There are two main methods to estimate in vitro cytotoxicity: indirect contact essay and direct contact essay. Nevertheless, the current methods assume that cytotoxicity is studied on a cellular level rather than the molecular level, which means, the components of decellularized scaffolds will influence cells on a more magnifying level than that of molecules [84]. This indicates that more solid techniques such as mRNA microarray should be considered to provide an enhanced perspective on this issue [84]. This is because the mRNA microarray can provide an unbiased insight into all transcripts, thereby supporting the detection of adverse molecular components [100].
In addition to the cytotoxicity, pathogenic problems that may arise from decellularization have raised concerns. This is because decellularized tissues or organs mostly come from cross-species. These species normally carry the paramount virus, bacteria, and other potentially dangerous pathogens. Even though some trials ruled out by U.S. Food and Drug Administration [101] require that mandatory testing be done before xenotransplantation, the risks can’t be avoided completely [102,103]. Furthermore, scientists ought to contribute to a deep, rigorous, and wide exploration of studies for pathogen identification and removal [103].
Apart from pathogenicity, immunogenicity is also a complicated problem that requires special addressing for decellularization and grafting. To ensure the biocompatibility of xenografts in vivo transitions, it is mandatory to avoid hyper-acute and acute rejections [104]. This relates to the ultimate removal of cellular components, antigens, and nucleic materials along with the immunogenicity tests. Nowadays, the techniques of removing immune components of decellularized kerato-substitutes can’t reach 100%, meaning these scaffolds may induce immune rejections. Regarding the immunogenicity assessment, in vitro, inflammatory response mainly uses macrophage and lymphocyte cell lines with indirect or direct contact assay to observe the immune performance of macrophages [105]. In vivo, inflammatory studies have been investigated by diverse quantitative assays. Cell adhesion, the quantification of infiltrated leukocytes at the transplantation site, and phenotyping of cellular infiltrates and cytokine profiles are commonly applied and analyzed [106,107,108]. Additionally, new techniques including mRNA microarray and proteomics will enable the investigation of the interaction between cells and decellularized tissue referring to a response to surface-adsorbed proteins and the proteins expressed from reseeded cell signaling [84]. Via these methods, we could gain more knowledge and insights into cell-scaffold correlations.
3.3. Preservation of innate biological attributes post-decellularization
After the adequate removal of cellular materials and biocompatibility evaluations of decellularized scaffolds are properly conducted, the next step should be to perform characterizations that provide insight on how the decellularization protocol can preserve structural and functional characteristics of the native tissues. An overview of various characterization techniques used to evaluate decellularized corneal scaffolds are outlined in Table 2.
3.3.1. ECM architecture preservation
Although the preservation of the native tissue architecture and ECM composition during tissue decellularization is crucial for all tissues, it is of particular interest to corneas. This is because the cornea has the highly organized ECM, which is responsible for its primary function, light transmission [109]. Basic histological assays can be used to compare the architecture of DCs with the native cornea. Studies have shown that stains such as eosin and van Gieson’s have shown instant changes in collagen structure [60,78]. However, basic histological approaches do not always provide adequate specificity, and under these circumstances, immunohistochemistry is a helpful tool since it is possible to identify ECM proteins that are specific to the cornea [10]. Corneal-specific proteins commonly utilized include collagens I, II, III, IV, and V, keratin, fibronectin, and laminin, present in the basement membrane [60,67]. The presence and integrity of the Bowman’s layer and Descemet’s membrane must be determined if a fully intact acellular scaffold is the end goal. This can be done by identifying specific proteins rather than using a broad eosin stain, which will provide additional information. To identify other components of the scaffold, stains such as Alcian blue have been used as a way of assessing whether the GAG content within the corneal stroma has been retained [10,56].
3.3.2. Transparency
The corneal stroma is mainly composed of dense connective tissue [110]. The cornea protects the inner content of the eye and the refractive capability of the lens is based on the precise shape of the cornea [111]. The corneal layers include epithelium, Bowman’s layer, stroma, Descemet’s membrane, and endothelium. Optical transparency and clarity are two things needed for good vision. Assessing the transparent nature of corneal tissue is very challenging and techniques are extremely limited. Previously, the transparency was assessed subjectively by placing the cornea on top of a grid and evaluating how the lines were seen. Luckily, throughout the years, the quantitative measurement of cornea tissue has improved using various methods, and each technique has its advantage and disadvantage. Below is a discussion of various conventional and emerging microscopic techniques that can be used to measure and monitor the transparency of corneal scaffolds.
Light microscopy is a simple technique that uses visible light to detect small objects. It offers high-resolution magnitudes to the image [112]. A major drawback is that the specimen needs to be stained to visualize it, but this stain could interfere with the decellularization protocol and may cause the distortion of the specimen. The presence of light on the specimen will cause a reflection and scatter the light to cause the image to be concealed. While confocal microscopy offers a high-resolution optical imaging technique that can be used as a rapid non-invasive diagnostic tool to observe corneal nerves in vivo, assess cell organelle and provide a high-resolution image [16,113,114,115,116,117,118,119,120,121]. In a study, confocal microscopy was used to assess the structural architecture of a human cornea. The Bowman’s membrane, stroma, and endothelium were all visualized at a resolution of 1–2 μm. It was able to get a high resolution by limiting the field of view to a single spot and thus eliminating out-of-focus structure [113]. A drawback of this tool is that it can only precisely analyze a small part of the specimen and provide a limited field of view, so it will take a long time to analyze multiple scans. Overall confocal microscopy can reconstruct a full view by rapid scanning of the cornea but it is still not a feasible screening tool because it can’t assess the quality of the ECM or evaluate collagen organization after decellularization. In comparison, transmission electron microscopy uses a beam of electrons at the specimen to visualize ultrastructural details of the cornea and generate a high-resolution magnified image [34]. This form of microscopy was used to assess rabbit cornea stroma opacity. Researchers were able to achieve remarkable images of the regeneration of the epithelial basement membrane [122]. However, a drawback of technique is that it uses potent fixatives, which could distortion of the specimen and affect decellularization.
Alternatively, anterior segment, Fourier-domain optical coherence tomography [123] is a non-invasive tool that uses light waves to take cross-section images of the eye. It Is essential for diagnosing a broad spectrum of diseases that affect the eye, such as glaucoma, macular degeneration, and diabetic eye disease [124], as observed with other forms of comparable spectroscopic applications for easily accessible regions of the body [125]. It can provide microstructure information such as stromal thickness, stromal morphology with an axial resolution, and the Bowman layer, providing another tool to assess decellularization. In comparison, ultrasound biomicroscopy uses a probe that emits high-frequency sound waves (50 to 100 MHz) that reflect through the tissue and generate an image [126]. It Is useful for diagnosing a broad spectrum of diseases that affect the eye and giving an accurate, detailed image of the cornea. This form of microscopy provides advantages over the previously mentioned techniques as it does not require staining and can delineate the microarchitecture and measure variations in the corneal layer. Nevertheless, this approach is limited by its need for direct contact with the eye and low (4mm to 5mm) tissue depth penetration [127].
3.3.3. Biomechanical properties
Decellularization is a process that removes all the cellular and nuclear material from the tissue while trying to maintain the remaining and innate composition, biological and mechanical properties of the tissue [66]. Some decellularization protocols can damage the cornea by changing the 3D architecture of the tissue, altering the biomechanical properties, and reducing the transparency of the cornea [66]. Historically, quantitative measurements of cornea tissue biomechanical properties have improved. We are now able to measure the cornea intraocular pressure, load-bearing capacity, elasticity properties, central cornea thickness, stiffness, and many more properties. However further means are needed to assess the effect decellularization protocols could have on the viscoelastic properties of the cornea [66]. Below is a summary table of some of the mechanical techniques and their advantages and disadvantages in assessing the biomechanical properties of the cornea.
Table 2.
A summary of characterization techniques used to evaluate decellularized corneal scaffolds.
Table 2.
A summary of characterization techniques used to evaluate decellularized corneal scaffolds.
| Mechanical techniques | Application | Advantages | Disadvantages |
|---|---|---|---|
| Compression testing [128] |
The tissue is placed under two plates and compressed The test is used to determine the mechanical behavior of the tissue under the crushing load |
It can measure the mechanical behavior of the tissue and ductile fracture limits of the tissue It also gives you a detailed assessment of the tissue’s load-bearing capacity and elasticity properties |
It flattens the tissue and damages the structural architecture Due to the corneal curvature shape, the test may not distribute the pressure equally |
| Holographic interferometry [129] |
Is a tool that uses a laser to trace the changes in the tissue and perform interferometric measurements | It is a precise method that can detect residual stresses and cracks on the tissue without mechanical contact | There is no fixed distance so the location of the structure cannot be obtained |
| Bulge and inflation testing [128] |
Is a tool that is used to biomechanical test corneal tissue by inflating the tissue and measuring the displacement | It is a reliable tool that demonstrates the intrinsic properties of the cornea layers and resembles Intraocular pressure | The inflation capacity is difficult to control and it could affect viscoelasticity |
| Corvis STL Tonometer/Pachymeter [130] |
Corvis ST is a device that uses a high-speed Scheimpflug camera to record the cornea movement | Corvis ST device evaluates the central cornea thickness, corneal stiffness, and intraocular pressure | Very expensive |
| Ultrasound | It is a device that uses sound waves to get a very detailed image of structures | It is a non-invasive technique that shows detailed surface imaging of the cornea | It depends on the user’s skill |
| Ocular Response Analyzer [131] |
Is a non-invasive device that uses rapid air pulse to make an indentation in the cornea | It measures the cornea biomechanical properties such as corneal hysteresis, intraocular pressure, and corneal resistance factor | Very expensive |
| Indentation testing [10] |
Is a test that measures the indentation left behind in the cornea after it was compressed | Determine the hardness of the cornea with minimal destruction | Doesn’t assess tensile strength |
3.4. Evaluation of recellularization performance
Beyond the initial structural and functional characterizing of corneal grafts, the cell reseeding performance of these scaffolds should be emphasized and required before in vivo implantation. Recelluarization is a dynamic process that aims to repopulate the decellularized scaffold. An important issue with the recellularization process is figuring out the benefits and drawbacks of the different cell lines [132]. Previous research has shown the feasibility of using immortalized cell lines such as Induced pluripotent stem cells (iPSCs) [132]. iPSCs can be differentiated into keratocyte cells that could be used to repopulate the scaffold [132]. Stem cells enable the development of unlimited cell sources that can be used for various therapeutic purposes. They also offer the opportunity for autogenic cell transplantation but a major problem is the iPSCs have the potential to proliferate uncontrollably and form teratomas.
Current restrictions to corneal recellularization are stroma thickness and the dense packing of collagen fibrils. Thus, it can be hard for the cells to repopulate the decellularized scaffold if they can’t reach their target. One technique is to directly inject the cells into the stroma but a major drawback to this approach is a fact that it can damage the 3D architecture [133]. Another cell seeding technique used, coats the scaffolds with biological glues to enhance cellular adhesion, and eventually penetrate and migrate into deeper layers. This technique can increase cell seeding efficiency [133].
Research has shown that different types of techniques are needed, depending on the site of cornea damage, for example, patients that have limbus damage develop limbal stem cell deficiency [134]. This damage leads to the patient developing conjunctivalization. In order to treat this disease, some studies have used limbal-derived stem cells [134]. The stem cells are isolated and transplanted onto the cornea, so they can proliferate and replenish the limbus cells. A successful procedure is assessed based on the patient’s lack of immune reaction, transparency recovery and cornea restoration. Currently, there are no specific methods or standards reported to evaluate the recellularization performance of the decellularized corneal scaffolds [135]. However, it has been indicated that the recellularization using keratocytes alone might not be sufficient for cell regrowth without other concurrent treatments []. Furthermore, work by Martin et al. have presented the differentiation of human embryonic stem cells (hESCs) into corneal epithelial-like cells on the decellularized cornea matrix has been demonstrated for the first time, which implied the potential employment of hESCs on the corneal substitutes to support repopulation []. Obviously, decellularized corneal technologies have a huge potential to alleviate the cornea shortage, whilst the current research of recellularization techniques, protocols, and reseeding cell types are improficient to support clinical translation. Therefore, it is imperative to enhance recellularizing strategies.
4. Preclinical and clinical applications
In the previous paragraphs, we focused on discussion on the relevant biological and biomechanical, functional, and structural characterizations of kerato-alternatives relevant and the associated approaches to generating decellularized replacements. Notwithstanding the need for further research, Kpros have been evaluated in preclinical and clinical settings. In the subsequent sections, current and emerging commercial options are fully elucidated.
Keratoplasties have been around since 2000 BC; however, one of the first fully described keratoprosthetic dates back to 1789 [7]. There are different types of keratoprosthetic devices, like hard ones made from rigid polymers or soft structures that can be better integrated into the transplantation site. The Boston Keratoprosthesis is an example of a rugged synthetic keratoprosthesis with a poly (methyl methacrylate) (PMMA) base that has a backplate of PMMA with a titanium locking ring to secure the backplate that was FDA approved in 1992 [136]. Donor corneal tissue is placed in between the anterior PMMA layer and the backplate; thus, it does not eliminate the need for human donor corneas. The retention rates were around 90%, with post-operative visual acuity of 20/100 or better at 6 months in 67% of patients and at 1 year in 75% of patients. However, corneal melting and graft detachment can occur due to poor biointegration between the PMMA and the corneal stroma [137].
Similarly, the OOKP was introduced in 1963 and comprised a donor root tooth and alveolar bone to support a PMMA optical cylinder [8]. It was later improved in 1998 by adding a larger biconvex optic and performing cryo-extraction of the lens to become known as the modified osteo-odonto-keratoprosthesis (MOOKP) [138]. A significant drawback of MOOKP is that it requires a complex surgical technique and patient counseling with complications involving the mucosa, retina, and lamina that affect visual outcomes. Retention failure of the device is commonly due to limited resorption, as there must be a balance between resorption and reformation to preserve the lamina. In contrast, the AlphaCorTM keratoprosthetic is an example of a soft keratoprosthetic composed of a cross-linked PHEMA that forms a hydrogel by polymerization that forms the optical and skirt components [139]. The skirt has a higher water content than the optical component, allowing it to have larger pores for biointegration [7]. It was reported that retention rates for the AlphaCorTM have been relatively high, as seen in a phase I trial where 93% of 14 devices were retained for up to 2.5 years [140]. However, due to the higher water content, there can be inadequate suturing performance and poor mechanical strength that allows for stomal melts and extrusion.
Although all of the listed solutions have succeeded, future work should deeply involve targeting solutions that reduce the use of human donor tissue through optimizing decellularized cornea scaffolds. One of the strategies is to replicate the corneal microenvironment, which is targeted by applying biopolymers to mimic ECM components. For example, a bioengineered corneal implant was documented as a solution for patients with a high risk of graft failure. The bioengineered implant was made from recombinant human collagen type III (RHCIII). In a phase 1 clinical trial, a biosynthetic cornea of RHCIII crosslinked with non-toxic zero-length human crosslinkers, it was found that there was the regeneration of corneal epithelium, partial replacement of corneal stoma, facilitation of nerve regeneration, and good biointegration with the biomimetic cornea [141]. However, the biomimetic corneal replacement was only suitable for low-risk patients as it led to neovascularization in rabbit models with severe pathological consequences [142]. Thus, efforts were made to reduce the risk of implant-related neovascularization by including a synthetic phospholipid methacryloylocyoxyethyl phosphorylcholine (MPC). The RHCIII-MPC implants prevented vascularization in a high-risk alkali burn corneal injury model. Further, the device was implanted in three patients with ulcerations, decreased corneal integrity, and near blindness, and it was shown that the implants improved vision in two out of the three patients, but in all three patients, there was no evidence of neovascularization at the 1-year follow-up.
More decellularized corneal implants have been explored due to the possibility of optimizing or improving actual corneas’ complex structure and function [134,143]. There is a wide variety of decellularization methods, with no superior method identified. However, all methods aim to achieve the same goal. The goal of decellularization of donor corneal tissue is to maximize the elimination of cellular and immunogenic components to decrease the chances of rejections while limiting impairment to the histo-architecture and mechanical properties of the conserved extracellular matrix (ECM) [22]. In addition, decellularization of the tissue should not hinder the ability to repopulate the scaffold with host cells. One example of a method for decellularization includes biological treatments. Biological treatments are enzyme-based procedures that disrupt the bonds and interactions between nucleic acids and interacting cells by disrupting neighboring proteins and other cellular components. By using enzymatic agents in the decellularization process, it is possible to eliminate cell residuals and other undesirable components of the ECM due to the high specificity that enzymatic agents provide compared to other decellularization protocols. However, using enzymatic agents can result in residual enzymes in the decellularized tissues, impairing the recellularization while stimulating an immune response, including apoptosis and inflammation, which result in early rejection [20,32]. Non-enzymatic agents can also be used, including chelating agents and serine protease inhibitors, whereby chelating agents such as ethylenediaminetetraacetic acid (EDTA) aid cell dissociation by separating metal ions [10,20]. However, these approaches can lead to the disruption of protein-protein interactions [41,85]. Chelating agents alone are insufficient for superficial cell removal. They are often combined with enzymes and detergents, as unaccompanied, they are insufficient for superficial cell removal [32]. Biological treatments are just one example of possible strategies to decellularize effectively. However, as indicated, it poses its disadvantages in successful recellularization.
The emergence of biomaterials, bio-inks, and inks can be used to mimic the corneal microenvironment. In addition, corneal bioengineering through 3D bioprinting has become an appealing method for developing a corneal equivalent. Rebuilding a stromal equivalent has been attempted by a research team that bioprinted corneal stromal keratocytes (CSK) using collagen-based bioinks [144]. Another research group constructed a 3D anatomically analogous corneal structure by using an existing 3D digital human corneal model and a composite bio-ink comprised of collagen and alginate that contained encapsulated corneal keratocytes, and while the keratocytes remained viable for 7 days post-printing, the metabolic activity and protein expression was low [145]. These are just a few of the attempts at 3D bioprinting of a corneal equivalent, yet many of the attempts did not have any evidence of testing it in implantation.
As mentioned, Xenia® corneal implants aim to reinforce biomechanically compromised corneas with evidence of an increasing number of patients undergoing the treatment with over 12 months of follow-up [146]. In particular, contemporary means of creating more viable kerato-alternatives are intended to combine decellularization with fabrication techniques and simulate the ECM structure to a large extent. There are two appropriate instances for illustrating the solutions. The development of Xenia® lenticules is comprised of a four-stage process. This process begins with decellularizing the corneal tissue, removing the cells, antibodies, and antigens of the donor tissue to decrease the host’s immune system response post-implantation. After the donor tissue is decellularized, it is washed, compressed, and crosslinked, allowing for the reduction of the thickness and increasing the stiffness of the lenticular region, further assisting in the stabilization and reshaping of the keratoconus cornea [147]. Examination of the effectiveness of developing the Xenia® lenticule on mechanical strength to further examine the load-deformation response to pulsatile, physiologically representative pressure variations showed that the mechanical properties were not homogenous across the tissue, and there was also substantial variability in the calculated corneal stiffnesses [147]. Although the current use and implementation of Xenia® corneal implants showed promising results, the sample size was small, and the follow-up was not for a prolonged period [146].
Previous attempts outline the difficulty in developing artificial Kpros due to the formation of postoperative retroprosthetic membrane, corneal melt, limited implant retention, postoperative glaucoma, and overall poor postoperative visual acuity. On the other hand, CorNeat KPro is a synthetic alternative to bioartificial corneal implants. The undercut on the device’s posterior side allows it to easily snap into a trephined cornea and quickly seal the eye. The lens is surrounded by a nondegradable porous integrating skirt, which is fabricated through electrospinning and will be implanted subconjunctivally. The porous property of the skirt allows the conjunctiva to adhere to the sclera employing bio-stitching. The implanted skirt material stimulates cellular proliferation and colonization, contributing to full tissue integration. The CorNeat KPro is combined with a biocompatible, nondegradable biomimetic material that imitates the microstructure of the human ECM. It is a collagen mesh that provides structural and biochemical support to surrounding cells differing from scaffolding and collagen matrices used in tissue repair due to its nondegradable nature. Furthermore, this manufactured matrix was designed to provide human fibroblasts with a familiar environment that could support migration and colonization, which are crucial for wound healing and remodeling [14]. The in vivo studies have shown increased proliferation of fibroblasts and collagen fibrils within several weeks of implantation, indicating progressive tissue integration. A schematic of the novel design and implantation procedure are outlined in Figure 2.
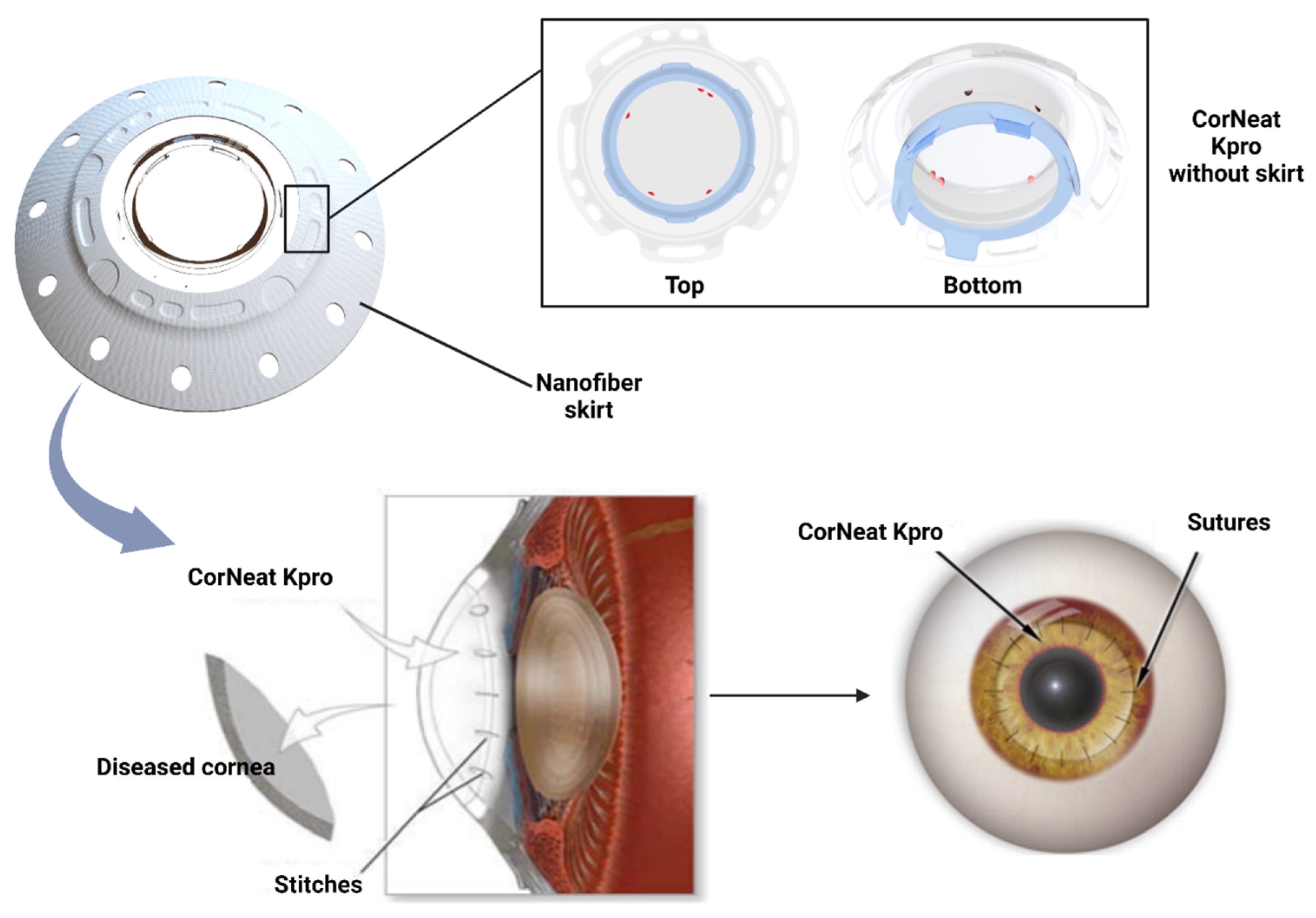
Figure 2.
Composition of CorNeat KPro and the implantation process.
5. Conclusion and perspectives
Decellularized Kpros have been developed rapidly in recent years and gained more positive feedback and support owing to their minimal immunogenicity, abundant xeno-resources, superior biocompatibility, and mimicked ECM structure. Distinct decellularization techniques were explored and applied to create corneal analogs with different biomechanical performances. Characterizing decellularized kerato-alternatives involves plenty of scientific studies and advanced technologies. The maintenance of ECM-similar structure, biocompatibility, and eradication of immunogenic components are the fundamental requirements to produce cornea scaffolds. Scaffolds that can support adequate cellular repopulation, and eventually long-term transplantation call for promising alternatives to meet existing challenges. Nevertheless, limited decellularization protocol standardization, biocompatibility assessments, proficiency in evaluating biomechanical features, and degree of long-term in vivo somatic tissue growth are significant challenges that must be addressed.Therefore, we hypothesized a new model of future Kpros using 3D printing and decellularization techniques.
The native cornea has a transparent and multilayered structure. The primary function of the cornea is to refract and transmit light toward the lens and, ultimately, the retina [88]. Each layer of the cornea is distinct in composition, structure, function, and resident cells [148]. The outer layer-epithelium consists of stratified epithelial cells, while the Bowman’s layer and a basement membrane are acellular collagen separating the epithelium from the stroma. Bowman’s layer consists of tiny collagen fibrils with a diameter of 18-22 nm [149,150]. Bowman’s collagen types are composed of IV and VII, which play essential roles in mechanical performance. The stroma, constituting 90% of the total corneal thickness, contains highly structured, evenly spaced, and anisotropically aligned collagen fibrils [151]. The collagen fibrils in the stroma are quite different from that in Bowman’s layer. They are majorly collagen type I. The dimension of the stroma of human corneas is 0.5 to 250 μm in width and up to 2.5 μm in thickness [152]. These collagen fibrils are surrounded by GAGs, glycoproteins, and proteoglycans [153]. The stroma contributes to the transparency, avascularity, and mechanical properties needed to maintain the structure [144]. Moreover, the stroma also includes keratocytes that help maintain homeostasis after an injury, stem cells located in the limbal stromal region which can differentiate into various cells when simulated, and dendritic cells, the most efficient antigen-presenting cells initiating the adaptive immune response [154,155].
The Descemet membrane, filled with hexagonal collagen VIII, IV, and XII networks, is connected with the endothelium, whereas the endothelium inner layer has a single layer of endothelial cells that can regulate the hydration of the whole cornea [156]. The Descemet’s membrane supports communication between the corneal endothelium and posterior stroma keratocytes. Ocular swelling and vision impairment are caused by endothelial damage and unregulated angiogenesis [157]. Since the ECM is not only the pivotal component of corneas but also supports the structure intactness and functional regulation [158]. Impairment to the ECM will result in reduced vision or even complete visual loss [159]. The cornea’s transparency is determined by the regular packing of the homogenous small collagen fibrils [160]. Different species have different diameters, amounts, and structures of collagen fibrils [161]. Collagen type I, GAGs, glycoproteins, and proteoglycans are major components of the cornea ECM. However, corneal stroma structure and ECM structure do not generally rely on the collagen type [152]. The functional and integrated stroma and ECM depend on complicated interactions and networks between collagen fibrils, cellular interfaces, and non-fibrillar collagens macromolecules, including proteoglycans, glycoproteins, GAGs, and fibrillin [152]. A comprehensive decellularized model should ideally mimic all components with the native corneas, as we have attempted to illustrate in the later section.
6. Hypothesis of proposed model for keratoprostheses
In the above section, a detailed outline of the human native corneas has been provided, illustrating the complexity of each layer’s structure and function. Thus, to create an ideal keratoprosthesis, the scaffold should mimic the intrinsic organization and components of native corneas. Therefore, we hypothesized a model generated through 3D bioprinting and decellularization. In general, we propose to utilize the Simplify3D® Desktop Software to generate multilayered scaffolds [162], while the decellularized corneal scaffolds can be used as the major constituents of the bioink. The reasons for combing these two powerful approaches is based on the fact that advances in tissue engineering and regenerative medicine have been accomplished by bioprinting layered structures using bioinks composed of various cells, polymers, and molecules [163]. Simplify3D® Desktop Software is well-suited for this complex manufacturing process. Additionally, success with this process depends heavily on the bioink.
Ideally, decellularization will remove unwanted cellular materials without harming GAGs, proteoglycans, collagen, and other acellular parts [62]. Therefore, we assumed that our decellularized corneal stroma maintained these components whose crucial functions have been explained before. The workflow of the model has been demonstrated in Figure 4. The first step is to generate the decellularized cornea stroma as use this tissues to generate a viable bioink and decellularized sclera as a nanofiber skirt. The decellularized scaffolds are resourced from discarded native sheep corneas, which an be obtained in a limitless supply from local abbatoirs. Native sheep corneas have horizontal and vertical diameters of 2.50 cm and 1.79 cm, respectively, and a thickness of 0.63 mm post-decellularized via a combination of chemical (surfactants) and physcial (agitation) processes [88]. The width of the cut sclera edge for native corneas was around 3.00 mm. The exact dimensions of decellularized corneas can be fshioned to roughly 2.20 cm, 1.55 cm, 5.00 mm, and 3.98 mm as outliend in Figure 3. It is noticed that decellularized ovine corneas are opaque, but their transparency will be significantly recovered by treatment with glycerol.
Specifically, we propose to use the decellularized corneas as a stromal layer bioink. Each scaffold in the large batch of decellularized corneas can be divided into the cornea and sclera. Both of them will be melted to form a gel or liquid. This procedure can be achieved by generating hydrogels from decellularized tissues via enzymatic and acidic digestions [164]. It has been shown that collagen type I can change into crystal liquid phases when it is concentrated in an acid solution, which may be a limiting factor [165]. Then the liquified sclera can be electrospun into a nanofiber skirt for suturing and anchoring the graft. Afterward, the second step is to prepare bioinks for 5 layers of the scaffold. The bioinks of the epithelial layer include collagen type IV, laminin, and fibronectin, while that of Bowman’s layer are made of collagen fibrils (type IV and VII) around 18–22 nm, which can be obtained via electrospinning.
The Descemet membrane’s ink should be composed of hexagonal collagen VIII networks and associated collagens IV and XII [156,166], while the endothelial layer could be primarily composed of endothelial cells. Moreover, the stroma bioinks can be rich in collagen type I [167], GAGs, glycoproteins, proteoglycans, keratocytes, stem cells, and dendritic cells. The cells in bioinks can be cell-sheeted or printed into sheets. Following the complete preparation of bioinks, All the other components will be added into the extruder and printed layer by layer. The final printed product can be designed to possess mean central and peripheral thicknesses of 0.523 mm ± 0.039 and 0.660 mm ± 0.076, respectively, which correspond to the dimensions of the human cornea [168]. After that, the bioink of the sclera, which is made of electrospun nanofibers and decellularized ovine materials, can be printed separately onto a nanofiber skirt that will be sutured using biocompatible threads to the cornea. Figure 4 provides an outline of the proposed model.
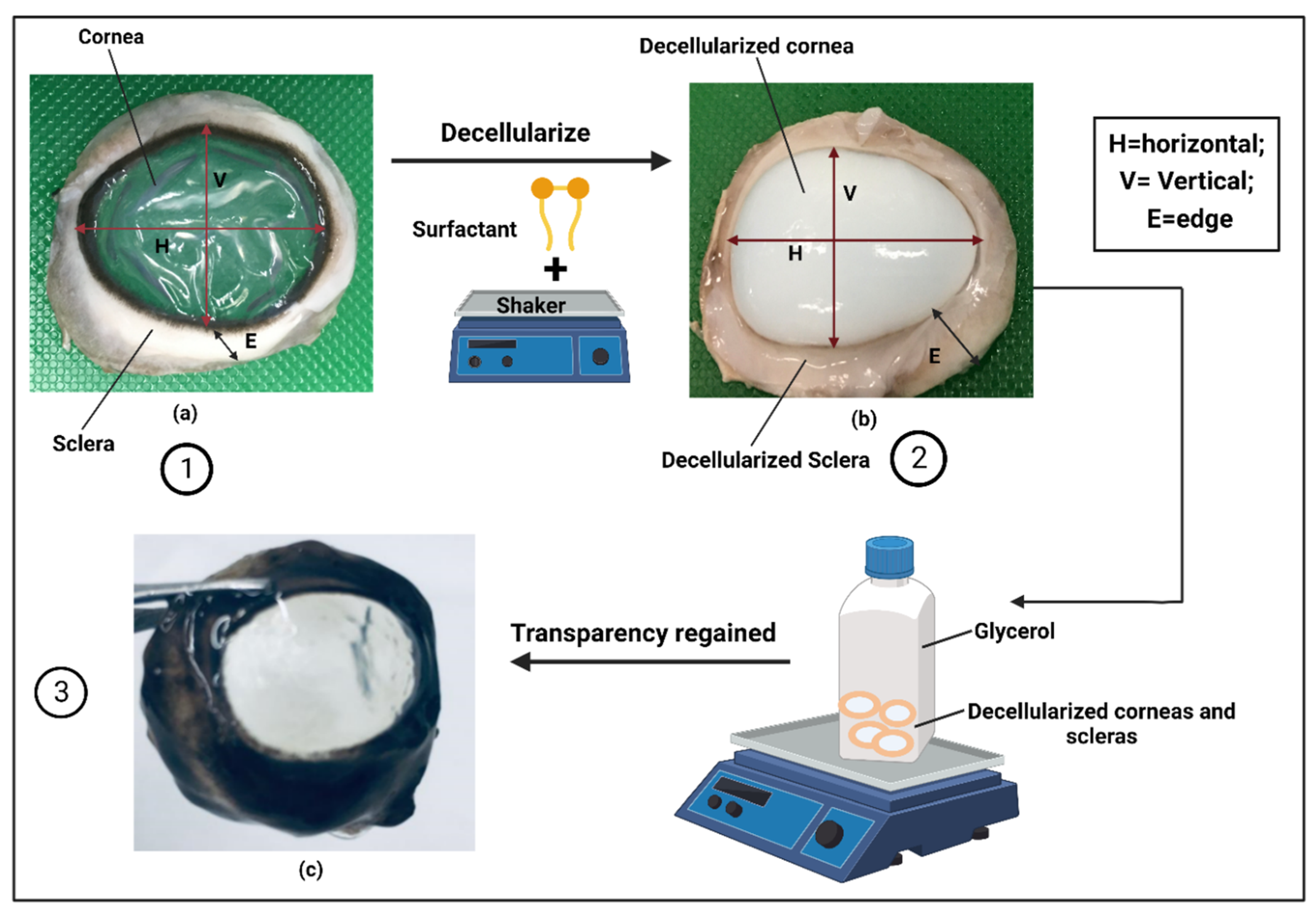
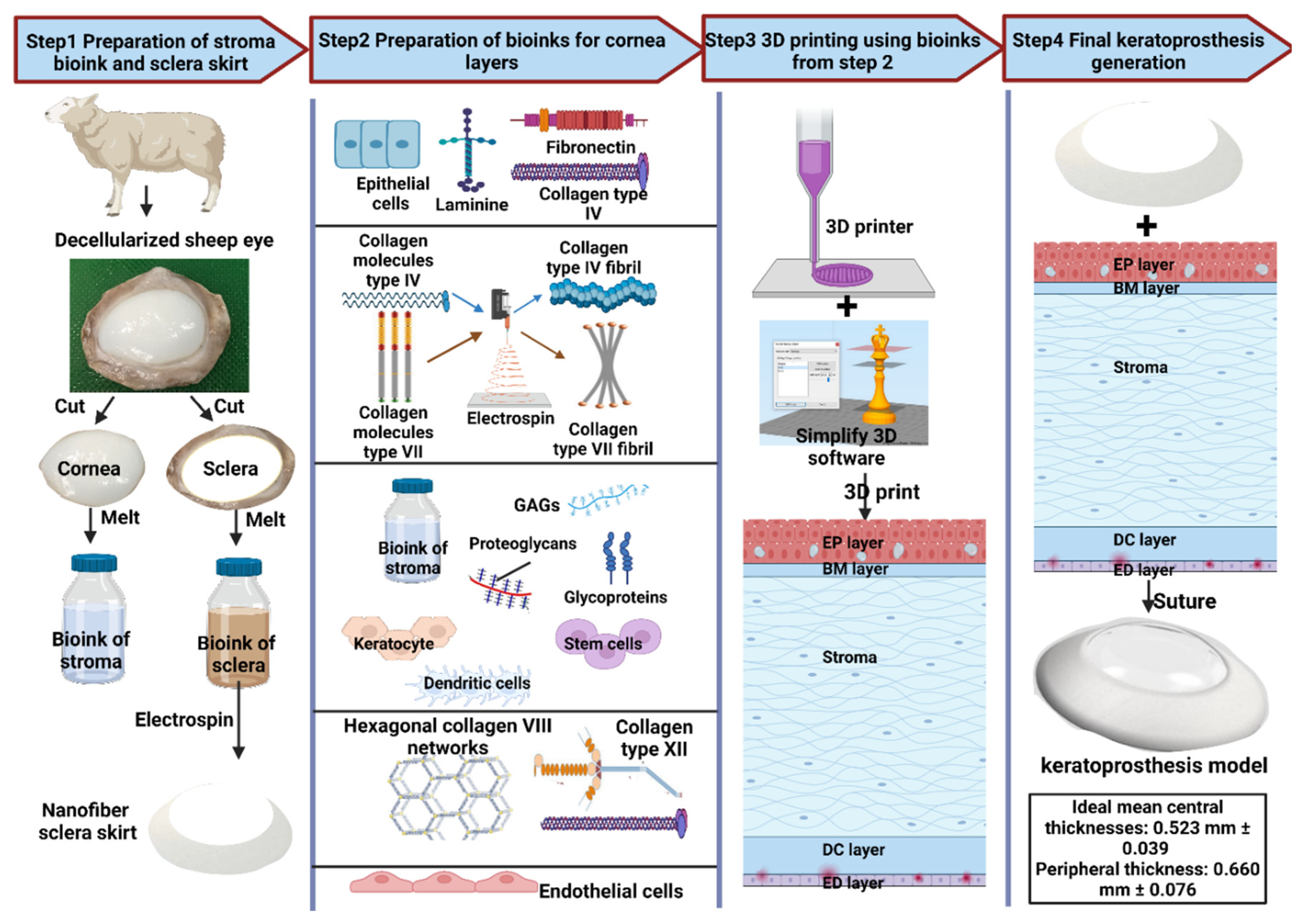
Figure 3.
(a) Native ovine cornea; (b) Decellularized ovine cornea; (c) Decellularized cornea regained transparency.
Figure 3.
(a) Native ovine cornea; (b) Decellularized ovine cornea; (c) Decellularized cornea regained transparency.
Figure 4.
Idea model for multilayered keratoprosthesis. EP = epithelial; BM = Bowman’s layer; DC = Descemet’s membrane; ED = endothelial.
Figure 4.
Idea model for multilayered keratoprosthesis. EP = epithelial; BM = Bowman’s layer; DC = Descemet’s membrane; ED = endothelial.
Author Contributions
P.R.C. conceived and designed the project. X.W., R.T.E., A.M.A., Z.M.A., V.C. and P.R.C. contributed to the final draft of the manuscript.
Funding
The project was supported by funds granted to Dr. Corridon from Khalifa University of Science and Technology, Grant Numbers: FSU-2020-25, ESIG-2023-005 and RC2-2018-022 (HEIC), and the Center for Biotechnology and the College of Medicine and Health Sciences. The project was also funded by the support P.R.C. received from the Abu Dhabi Automated Slaughterhouse, Municipality of the City of Abu Dhabi.
Acknowledgments
The authors would like to thank Mrs. Maja Corridon for reviewing the manuscript.
References
- P. Gain et al., “Global Survey of Corneal Transplantation and Eye Banking,” (in eng), JAMA ophthalmology, vol. 134, no. 2, pp. 167-73, Feb 2016. [CrossRef]
- M. J. Burton, “Prevention, treatment and rehabilitation,” (in eng), Community eye health, vol. 22, no. 71, pp. 33-5, Dec 2009.
- W. J. Armitage et al., “High-risk Corneal Transplantation: Recent Developments and Future Possibilities,” Transplantation, vol. 103, no. 12, pp. 2468-2478, 2019. [CrossRef]
- H. Gao et al., “Survey report on keratoplasty in China: A 5-year review from 2014 to 2018,” (in eng), PloS one, vol. 15, no. 10, p. e0239939, 2020. [CrossRef]
- S. L. Wilson, L. E. Sidney, S. E. Dunphy, H. S. Dua, and A. Hopkinson, “Corneal Decellularization: A Method of Recycling Unsuitable Donor Tissue for Clinical Translation?,” (in eng), Curr Eye Res, vol. 41, no. 6, pp. 769-82, Jun 2016. [CrossRef]
- B. Gurnani, C. N. Czyz, N. Mahabadi, and S. J. Havens, “Corneal Graft Rejection,” in StatPearls. Treasure Island (FL): StatPearls Publishing Copyright © 2022, StatPearls Publishing LLC., 2022.
- G. Holland et al., “Artificial Cornea: Past, Current, and Future Directions,” (in eng), Frontiers in medicine, vol. 8, p. 770780, 2021. [CrossRef]
- R. Sc, T. I, and T. D. T, “Osteo-odonto keratoprosthesis in Stevens-Johnson syndrome: a case report,” (in eng), International journal of ophthalmology, vol. 4, no. 2, pp. 212-5, 2011. [CrossRef]
- M. Vacalebre et al., “Current State of the Art and Next Generation of Materials for a Customized IntraOcular Lens according to a Patient-Specific Eye Power,” Polymers, vol. 15, no. 6, p. 1590, 2023. [Online]. Available: https://www.mdpi.com/2073-4360/15/6/1590.
- S. L. Wilson, L. E. Sidney, S. E. Dunphy, J. B. Rose, and A. Hopkinson, “Keeping an eye on decellularized corneas: a review of methods, characterization and applications,” (in eng), J Funct Biomater, vol. 4, no. 3, pp. 114-61, Jul 10 2013. [CrossRef]
- J. C. Igor Pantic, Svetlana Valjarevic et al., “Computational approaches for evaluating morphological changes in the corneal stroma associated with decellularization,” PREPRINT (Version 1) available at Research Square [https://doi.org/10.21203/rs.3.rs-2480023/v1], 16 January 2023.
- A. Neishabouri, A. Soltani Khaboushan, F. Daghigh, A. M. Kajbafzadeh, and M. Majidi Zolbin, “Decellularization in Tissue Engineering and Regenerative Medicine: Evaluation, Modification, and Application Methods,” Front Bioeng Biotechnol, vol. 10, p. 805299, 2022. [CrossRef]
- P. R. Corridon, “In vitro investigation of the impact of pulsatile blood flow on the vascular architecture of decellularized porcine kidneys,” Sci Rep, vol. 11, no. 1, p. 16965, Aug 20 2021. [CrossRef]
- P. R. Corridon, “Intravital microscopy datasets examining key nephron segments of transplanted decellularized kidneys,” Sci Data, vol. 9, no. 1, p. 561, Sep 10 2022. [CrossRef]
- P. R. Corridon, “Still finding ways to augment the existing management of acute and chronic kidney diseases with targeted gene and cell therapies: Opportunities and hurdles,” (in English), Frontiers in Medicine, Mini Review vol. 10, 2023-March-07 2023. [CrossRef]
- P. R. Corridon, I. K. Ko, J. J. Yoo, and A. Atala, “Bioartificial Kidneys,” Curr Stem Cell Rep, vol. 3, no. 2, pp. 68-76, Jun 2017. [CrossRef]
- V. Pantic, A. Shakeel, G. A. Petroianu, and P. R. Corridon, “Analysis of Vascular Architecture and Parenchymal Damage Generated by Reduced Blood Perfusion in Decellularized Porcine Kidneys Using a Gray Level Co-occurrence Matrix,” Front Cardiovasc Med, vol. 9, p. 797283, 2022. [CrossRef]
- A. Shakeel and P. R. Corridon, “Mitigating challenges and expanding the future of vascular tissue engineering-are we there yet?,” Front Physiol, vol. 13, p. 1079421, 2022. [CrossRef]
- X. Wang, V. Chan, and P. R. Corridon, “Acellular Tissue-Engineered Vascular Grafts from Polymers: Methods, Achievements, Characterization, and Challenges,” Polymers (Basel), vol. 14, no. 22, Nov 9 2022. [CrossRef]
- X. Wang, V. Chan, and P. R. Corridon, “Decellularized blood vessel development: Current state-of-the-art and future directions,” Front Bioeng Biotechnol, vol. 10, p. 951644, 2022. [CrossRef]
- P. Corridon, “Enhancing the expression of a key mitochondrial enzyme at the inception of ischemia-reperfusion injury can boost recovery and halt the progression of acute kidney injury,” ed: Research Square, 2023.
- A. Wilson, J. Jones, and J. Marshall, “Biomechanical Evaluation of Decellularized and Crosslinked Corneal Implants Manufactured From Porcine Corneas as a Treatment Option for Advanced Keratoconus,” (in eng), Frontiers in bioengineering and biotechnology, vol. 10, p. 862969, 2022. [CrossRef]
- M. M. Islam et al., “Effects of gamma radiation sterilization on the structural and biological properties of decellularized corneal xenografts,” (in eng), Acta Biomater, vol. 96, pp. 330-344, Sep 15 2019. [CrossRef]
- S. Sharifi et al., “Toward electron-beam sterilization of a pre-assembled Boston keratoprosthesis,” (in eng), The ocular surface, vol. 20, pp. 176-184, Apr 2021. [CrossRef]
- D. K. Cooper et al., “Alpha1,3-galactosyltransferase gene-knockout pigs for xenotransplantation: where do we go from here?,” (in eng), Transplantation, vol. 84, no. 1, pp. 1-7, Jul 15 2007. [CrossRef]
- H. Hara and D. K. Cooper, “Xenotransplantation--the future of corneal transplantation?,” (in eng), Cornea, vol. 30, no. 4, pp. 371-8, Apr 2011. [CrossRef]
- R. L. Khan, A. A. Khraibi, L. F. Dumée, and P. R. Corridon, “From waste to wealth: Repurposing slaughterhouse waste for xenotransplantation,” (in English), Frontiers in Bioengineering and Biotechnology, Perspective vol. 11, 2023-February-03 2023. [CrossRef]
- A.S. Xinyu Wang, Ahmed E. Salih et al., “A scalable corneal xenograft platform: simultaneous opportunities for tissue engineering and circular economic sustainability by repurposing slaughterhouse waste,” PREPRINT (Version 1) available at Research Square [https://doi.org/10.21203/rs.3.rs-2480068/v1], 16 January 2023.
- E. Yoeruek et al., “Decellularization of porcine corneas and repopulation with human corneal cells for tissue-engineered xenografts,” Acta Ophthalmologica, vol. 90, no. 2, pp. e125-e131, 2012. [CrossRef]
- E. Yoeruek et al., “Reconstruction of corneal stroma with decellularized porcine xenografts in a rabbit model,” Acta Ophthalmologica, vol. 90, no. 3, pp. e206-e210, 2012. [CrossRef]
- S. Chen, M. J. Mienaltowski, and D. E. Birk, “Regulation of corneal stroma extracellular matrix assembly,” (in eng), Experimental eye research, vol. 133, pp. 69-80, Apr 2015. [CrossRef]
- P. M. Crapo, T. W. Gilbert, and S. F. Badylak, “An overview of tissue and whole organ decellularization processes,” (in eng), Biomaterials, vol. 32, no. 12, pp. 3233-43, Apr 2011. [CrossRef]
- S. Amano, N. Shimomura, S. Yokoo, K. Araki-Sasaki, and S. Yamagami, “Decellularizing corneal stroma using N2 gas,” (in eng), Molecular vision, vol. 14, pp. 878-82, May 14 2008.
- D. Gusnard and R. H. Kirschner, “Cell and organelle shrinkage during preparation for scanning electron microscopy: effects of fixation, dehydration and critical point drying,” (in eng), Journal of microscopy, vol. 110, no. 1, pp. 51-7, May 1977. [CrossRef]
- A. Isidan et al., “Decellularization methods for developing porcine corneal xenografts and future perspectives,” (in eng), Xenotransplantation, vol. 26, no. 6, p. e12564, Nov 2019. [CrossRef]
- U. Mendibil, R. Ruiz-Hernandez, S. Retegi-Carrion, N. Garcia-Urquia, B. Olalde-Graells, and A. Abarrategi, “Tissue-Specific Decellularization Methods: Rationale and Strategies to Achieve Regenerative Compounds,” (in eng), International journal of molecular sciences, vol. 21, no. 15, Jul 30 2020. [CrossRef]
- M. Yang, C. Z. Chen, X. N. Wang, Y. B. Zhu, and Y. J. Gu, “Favorable effects of the detergent and enzyme extraction method for preparing decellularized bovine pericardium scaffold for tissue engineered heart valves,” (in eng), Journal of biomedical materials research. Part B, Applied biomaterials, vol. 91, no. 1, pp. 354-61, Oct 2009. [CrossRef]
- E. Rieder et al., “Decellularization protocols of porcine heart valves differ importantly in efficiency of cell removal and susceptibility of the matrix to recellularization with human vascular cells,” The Journal of thoracic and cardiovascular surgery, vol. 127, no. 2, pp. 399-405, 2004.
- C. Zhang et al., “Survival and integration of tissue-engineered corneal stroma in a model of corneal ulcer,” (in eng), Cell and tissue research, vol. 329, no. 2, pp. 249-57, Aug 2007. [CrossRef]
- F. Wang, Z. Wang, X. Sun, F. Wang, X. Xu, and X. Zhang, “Safety and efficacy of dispase and plasmin in pharmacologic vitreolysis,” (in eng), Investigative ophthalmology & visual science, vol. 45, no. 9, pp. 3286-90, Sep 2004. [CrossRef]
- Prasertsung, S. Kanokpanont, T. Bunaprasert, V. Thanakit, and S. Damrongsakkul, “Development of acellular dermis from porcine skin using periodic pressurized technique,” (in eng), Journal of biomedical materials research. Part B, Applied biomaterials, vol. 85, no. 1, pp. 210-9, Apr 2008. [CrossRef]
- Z. Wu et al., “The use of phospholipase A(2) to prepare acellular porcine corneal stroma as a tissue engineering scaffold,” (in eng), Biomaterials, vol. 30, no. 21, pp. 3513-22, Jul 2009. [CrossRef]
- M. Blum et al., “Tissue engineered vascular grafts transform into autologous neovessels capable of native function and growth,” Communications Medicine, vol. 2, no. 1, p. 3, 2022/01/10 2022. [CrossRef]
- R. S. S. Azevedo et al., “In situ immune response and mechanisms of cell damage in central nervous system of fatal cases microcephaly by Zika virus,” (in eng), Sci Rep, vol. 8, no. 1, p. 1, Jan 8 2018. [CrossRef]
- N. Li et al., “Tectonic lamellar keratoplasty with acellular corneal stroma in high-risk corneal transplantation,” (in eng), Molecular vision, vol. 17, pp. 1909-17, 2011.
- R. W. Grauss, M. G. Hazekamp, F. Oppenhuizen, C. J. van Munsteren, A. C. Gittenberger-de Groot, and M. C. DeRuiter, “Histological evaluation of decellularised porcine aortic valves: matrix changes due to different decellularisation methods,” (in eng), Eur J Cardiothorac Surg, vol. 27, no. 4, pp. 566-71, Apr 2005. [CrossRef]
- D. E. Heath, “A Review of Decellularized Extracellular Matrix Biomaterials for Regenerative Engineering Applications,” Regenerative Engineering and Translational Medicine, vol. 5, no. 2, pp. 155-166, 2019/06/01 2019. [CrossRef]
- A. Neishabouri, A. Soltani Khaboushan, F. Daghigh, A.-M. Kajbafzadeh, and M. Majidi Zolbin, “Decellularization in Tissue Engineering and Regenerative Medicine: Evaluation, Modification, and Application Methods,” (in English), Frontiers in Bioengineering and Biotechnology, Review vol. 10, 2022-April-25 2022. [CrossRef]
- Y. Oh, M. K. Kim, H. J. Lee, J. H. Ko, W. R. Wee, and J. H. Lee, “Processing porcine cornea for biomedical applications,” (in eng), Tissue engineering. Part C, Methods, vol. 15, no. 4, pp. 635-45, Dec 2009. [CrossRef]
- R. Bochert, A. Zhivov, R. Kraak, J. Stave, and R. Guthoff, “Contribution to comprehension of image formation in confocal microscopy of cornea with Rostock cornea module,” Br J Ophthalmol, vol. 89, pp. 1351-5, 11/01 2005. [CrossRef]
- Hedhly, Y. Wang, S. Zeng, F. Ouerghi, J. Zhou, and G. Humbert, “Highly Sensitive Plasmonic Waveguide Biosensor Based on Phase Singularity-Enhanced Goos–Hänchen Shift,” Biosensors, vol. 12, no. 7, p. 457, 2022. [Online]. Available: https://www.mdpi.com/2079-6374/12/7/457.
- Polisetti et al., “A decellularized human corneal scaffold for anterior corneal surface reconstruction,” Scientific Reports, vol. 11, no. 1, p. 2992, 2021/02/04 2021. [CrossRef]
- Gupta and P. Upadhyay, “Use of glycerol-preserved corneas for corneal transplants,” Indian J Ophthalmol, vol. 65, no. 7, pp. 569-573, Jul 2017. [CrossRef]
- S. Chaurasia, S. Das, and A. Roy, “A review of long-term corneal preservation techniques: Relevance and renewed interests in the COVID-19 era,” (in eng), Indian J Ophthalmol, vol. 68, no. 7, pp. 1357-1363, Jul 2020. [CrossRef]
- H. C. Lin, S. J. Ong, and A. N. Chao, “Eye preservation tectonic graft using glycerol-preserved donor cornea,” Eye, vol. 26, no. 11, pp. 1446-1450, 2012/11/01 2012. [CrossRef]
- M. Gonzalez-Andrades, J. de la Cruz Cardona, A. M. Ionescu, A. Campos, M. Del Mar Perez, and M. Alaminos, “Generation of bioengineered corneas with decellularized xenografts and human keratocytes,” (in eng), Investigative ophthalmology & visual science, vol. 52, no. 1, pp. 215-22, Jan 5 2011. [CrossRef]
- L. Gui, S. A. Chan, C. K. Breuer, and L. E. Niklason, “Novel utilization of serum in tissue decellularization,” (in eng), Tissue engineering. Part C, Methods, vol. 16, no. 2, pp. 173-84, Apr 2010. [CrossRef]
- Y. Shao et al., “Evaluation of novel decellularizing corneal stroma for cornea tissue engineering applications,” (in eng), International journal of ophthalmology, vol. 5, no. 4, pp. 415-8, 2012. [CrossRef]
- T. Bayyoud et al., “Decellularized bovine corneal posterior lamellae as carrier matrix for cultivated human corneal endothelial cells,” (in eng), Current eye research, vol. 37, no. 3, pp. 179-86, Mar 2012. [CrossRef]
- L. Du and X. Wu, “Development and characterization of a full-thickness acellular porcine cornea matrix for tissue engineering,” (in eng), Artificial organs, vol. 35, no. 7, pp. 691-705, Jul 2011. [CrossRef]
- E. Yoeruek et al., “Decellularization of porcine corneas and repopulation with human corneal cells for tissue-engineered xenografts,” (in eng), Acta ophthalmologica, vol. 90, no. 2, pp. e125-31, Mar 2012. [CrossRef]
- A. Gilpin and Y. Yang, “Decellularization Strategies for Regenerative Medicine: From Processing Techniques to Applications,” Biomed Res Int, vol. 2017, p. 9831534, 2017. [CrossRef]
- S. Cebotari et al., “Detergent decellularization of heart valves for tissue engineering: toxicological effects of residual detergents on human endothelial cells,” (in eng), Artificial organs, vol. 34, no. 3, pp. 206-10, Mar 2010. [CrossRef]
- M. S. Alhamdani, C. Schröder, J. Werner, N. Giese, A. Bauer, and J. D. Hoheisel, “Single-step procedure for the isolation of proteins at near-native conditions from mammalian tissue for proteomic analysis on antibody microarrays,” (in eng), Journal of proteome research, vol. 9, no. 2, pp. 963-71, Feb 5 2010. [CrossRef]
- S. Ponce Márquez et al., “Decellularization of bovine corneas for tissue engineering applications,” (in eng), Acta biomaterialia, vol. 5, no. 6, pp. 1839-47, Jul 2009. [CrossRef]
- A. P. Lynch and M. Ahearne, “Strategies for developing decellularized corneal scaffolds,” (in eng), Experimental eye research, vol. 108, pp. 42-7, Mar 2013. [CrossRef]
- S. Choi et al., “Bioengineering endothelialized neo-corneas using donor-derived corneal endothelial cells and decellularized corneal stroma,” (in eng), Biomaterials, vol. 31, no. 26, pp. 6738-45, Sep 2010. [CrossRef]
- Y. Dai et al., “Characterizing the effects of VPA, VC and RCCS on rabbit keratocytes onto decellularized bovine cornea,” (in eng), PloS one, vol. 7, no. 11, p. e50114, 2012. [CrossRef]
- T. J. Keane, I. T. Swinehart, and S. F. Badylak, “Methods of tissue decellularization used for preparation of biologic scaffolds and in vivo relevance,” (in eng), Methods (San Diego, Calif.), vol. 84, pp. 25-34, Aug 2015. [CrossRef]
- B. Ekser et al., “Clinical xenotransplantation: the next medical revolution?,” (in eng), Lancet (London, England), vol. 379, no. 9816, pp. 672-83, Feb 18 2012. [CrossRef]
- Y. G. Xu, Y. S. Xu, C. Huang, Y. Feng, Y. Li, and W. Wang, “Development of a rabbit corneal equivalent using an acellular corneal matrix of a porcine substrate,” (in eng), Molecular vision, vol. 14, pp. 2180-9, 2008.
- T. W. Gilbert, T. L. Sellaro, and S. F. Badylak, “Decellularization of tissues and organs,” (in eng), Biomaterials, vol. 27, no. 19, pp. 3675-83, Jul 2006. [CrossRef]
- M. C. Jamur and C. Oliver, “Cell fixatives for immunostaining,” (in eng), Methods in molecular biology (Clifton, N.J.), vol. 588, pp. 55-61, 2010. [CrossRef]
- W. Chen et al., “Comparison of fresh corneal tissue versus glycerin-cryopreserved corneal tissue in deep anterior lamellar keratoplasty,” (in eng), Investigative ophthalmology & visual science, vol. 51, no. 2, pp. 775-81, Feb 2010. [CrossRef]
- A. Isidan et al., “Comparison of porcine corneal decellularization methods and importance of preserving corneal limbus through decellularization,” (in eng), PLoS One, vol. 16, no. 3, p. e0243682, 2021. [CrossRef]
- Y. Zhou et al., “Development and characterization of acellular porcine corneal matrix using sodium dodecylsulfate,” (in eng), Cornea, vol. 30, no. 1, pp. 73-82, Jan 2011. [CrossRef]
- M. González-Andrades et al., “Effects of Detergent-Based Protocols on Decellularization of Corneas With Sclerocorneal Limbus. Evaluation of Regional Differences,” (in eng), Transl Vis Sci Technol, vol. 4, no. 2, p. 13, Apr 2015. [CrossRef]
- Du, X. Wu, K. Pang, and Y. Yang, “Histological evaluation and biomechanical characterisation of an acellular porcine cornea scaffold,” (in eng), The British journal of ophthalmology, vol. 95, no. 3, pp. 410-4, Mar 2011. [CrossRef]
- A. Shafiq, R. A. Gemeinhart, B. Y. Yue, and A. R. Djalilian, “Decellularized human cornea for reconstructing the corneal epithelium and anterior stroma,” (in eng), Tissue engineering. Part C, Methods, vol. 18, no. 5, pp. 340-8, May 2012. [CrossRef]
- Rabbani, N. Zakian, and N. Alimoradi, “Contribution of Physical Methods in Decellularization of Animal Tissues,” (in eng), Journal of medical signals and sensors, vol. 11, no. 1, pp. 1-11, Jan-Mar 2021. [CrossRef]
- Pulver, A. Shevtsov, B. Leybovich, I. Artyuhov, Y. Maleev, and A. Peregudov, “Production of organ extracellular matrix using a freeze-thaw cycle employing extracellular cryoprotectants,” Cryo Letters, vol. 35, no. 5, pp. 400-6, Sep-Oct 2014. [Online]. Available: https://www.ncbi.nlm.nih.gov/pubmed/25397955.
- Q. Xing, K. Yates, M. Tahtinen, E. Shearier, Z. Qian, and F. Zhao, “Decellularization of fibroblast cell sheets for natural extracellular matrix scaffold preparation,” (in eng), Tissue Eng Part C Methods, vol. 21, no. 1, pp. 77-87, Jan 2015. [CrossRef]
- C. Azuma, H. Tohyama, H. Nakamura, F. Kanaya, and K. Yasuda, “Antibody neutralization of TGF-beta enhances the deterioration of collagen fascicles in a tissue-cultured tendon matrix with ex vivo fibroblast infiltration,” (in eng), Journal of biomechanics, vol. 40, no. 10, pp. 2184-90, 2007. [CrossRef]
- K. H. Hussein, K. M. Park, K. S. Kang, and H. M. Woo, “Biocompatibility evaluation of tissue-engineered decellularized scaffolds for biomedical application,” (in eng), Materials science & engineering. C, Materials for biological applications, vol. 67, pp. 766-778, Oct 1 2016. [CrossRef]
- S. Nagata, R. Hanayama, and K. Kawane, “Autoimmunity and the clearance of dead cells,” (in eng), Cell, vol. 140, no. 5, pp. 619-30, Mar 5 2010. [CrossRef]
- B. N. Brown, J. E. Valentin, A. M. Stewart-Akers, G. P. McCabe, and S. F. Badylak, “Macrophage phenotype and remodeling outcomes in response to biologic scaffolds with and without a cellular component,” (in eng), Biomaterials, vol. 30, no. 8, pp. 1482-91, Mar 2009. [CrossRef]
- E. M. Espana and D. E. Birk, “Composition, structure and function of the corneal stroma,” (in eng), Experimental eye research, vol. 198, p. 108137, Sep 2020. [CrossRef]
- S. Sridhar, “Anatomy of cornea and ocular surface,” (in eng), Indian journal of ophthalmology, vol. 66, no. 2, pp. 190-194, Feb 2018. [CrossRef]
- R. Corridon, X. Wang, A. Shakeel, and V. Chan, “Digital Technologies: Advancing Individualized Treatments through Gene and Cell Therapies, Pharmacogenetics, and Disease Detection and Diagnostics,” Biomedicines, vol. 10, no. 10, Sep 30 2022. [CrossRef]
- L. M. Davidovic et al., “Gray-Level Co-occurrence Matrix Analysis for the Detection of Discrete, Ethanol-Induced, Structural Changes in Cell Nuclei: An Artificial Intelligence Approach,” Microsc Microanal, vol. 28, no. 1, pp. 265-271, Feb 2022. [CrossRef]
- Pantic, J. Cumic, S. Dugalic, G. A. Petroianu, and P. R. Corridon, “Gray level co-occurrence matrix and wavelet analyses reveal discrete changes in proximal tubule cell nuclei after mild acute kidney injury,” Scientific Reports, vol. 13, no. 1, p. 4025, 2023/03/10 2023. [CrossRef]
- Pantic, J. Paunovic, J. Cumic, S. Valjarevic, G. A. Petroianu, and P. R. Corridon, “Artificial neural networks in contemporary toxicology research,” Chemico-Biological Interactions, vol. 369, p. 110269, 2023/01/05/2023. [CrossRef]
- R. Corridon, “Capturing effects of blood flow on the transplanted decellularized nephron with intravital microscopy,” bioRxiv, p. 2021.02.10.430561, 2023. [CrossRef]
- L. C. Keong and A. S. Halim, “In vitro models in biocompatibility assessment for biomedical-grade chitosan derivatives in wound management,” (in eng), International journal of molecular sciences, vol. 10, no. 3, pp. 1300-1313, Mar 2009. [CrossRef]
- M. M. Singer and R. S. Tjeerdema, “Fate and effects of the surfactant sodium dodecyl sulfate,” (in eng), Reviews of environmental contamination and toxicology, vol. 133, pp. 95-149, 1993. [CrossRef]
- A. M. Kajbafzadeh, N. Javan-Farazmand, M. Monajemzadeh, and A. Baghayee, “Determining the optimal decellularization and sterilization protocol for preparing a tissue scaffold of a human-sized liver tissue,” (in eng), Tissue engineering. Part C, Methods, vol. 19, no. 8, pp. 642-51, Aug 2013. [CrossRef]
- E. Murray, C. García Godoy, and F. García Godoy, “How is the biocompatibilty of dental biomaterials evaluated?,” (in eng), Medicina oral, patologia oral y cirugia bucal, vol. 12, no. 3, pp. E258-66, May 1 2007.
- D. Granchi et al., “Adhesive protein expression on human endothelial cells after in vitro contact with woven Dacron,” (in eng), Biomaterials, vol. 19, no. 1-3, pp. 93-8, Jan-Feb 1998. [CrossRef]
- E. Cenni et al., “Established cell lines and primary cultures in testing medical devices in vitro,” (in eng), Toxicology in vitro: an international journal published in association with BIBRA, vol. 13, no. 4-5, pp. 801-10, Aug-Oct 1999. [CrossRef]
- M. S. Rao et al., “Comparison of RNA-Seq and Microarray Gene Expression Platforms for the Toxicogenomic Evaluation of Liver From Short-Term Rat Toxicity Studies,” (in eng), Frontiers in genetics, vol. 9, p. 636, 2018. [CrossRef]
- M. G. Hayat, N. Farahani, E. Safdarian, A. Roointan, and A. Sahebkar, “Gene Delivery Using Lipoplexes and Polyplexes: Principles, Limitations and Solutions,” (in eng), Crit Rev Eukaryot Gene Expr, vol. 29, no. 1, pp. 29-36, 2019. [CrossRef]
- M. G. Michaels, F. J. Jenkins, K. St George, M. A. Nalesnik, T. E. Starzl, and C. R. Rinaldo, Jr., “Detection of infectious baboon cytomegalovirus after baboon-to-human liver xenotransplantation,” (in eng), Journal of virology, vol. 75, no. 6, pp. 2825-8, Mar 2001. [CrossRef]
- A. Fishman, L. Scobie, and Y. Takeuchi, “Xenotransplantation-associated infectious risk: a WHO consultation,” (in eng), Xenotransplantation, vol. 19, no. 2, pp. 72-81, Mar-Apr 2012. [CrossRef]
- F. Naso, A. Gandaglia, L. Iop, M. Spina, and G. Gerosa, “Alpha-Gal detectors in xenotransplantation research: a word of caution,” (in eng), Xenotransplantation, vol. 19, no. 4, pp. 215-20, Jul-Aug 2012. [CrossRef]
- F. Groell, O. Jordan, and G. Borchard, “In vitro models for immunogenicity prediction of therapeutic proteins,” (in eng), European journal of pharmaceutics and biopharmaceutics: official journal of Arbeitsgemeinschaft fur Pharmazeutische Verfahrenstechnik e.V, vol. 130, pp. 128-142, Sep 2018. [CrossRef]
- M. Park, S. M. Park, S. R. Yang, S. H. Hong, and H. M. Woo, “Preparation of immunogen-reduced and biocompatible extracellular matrices from porcine liver,” (in eng), Journal of bioscience and bioengineering, vol. 115, no. 2, pp. 207-15, Feb 2013. [CrossRef]
- H. Mirmalek-Sani, D. C. Sullivan, C. Zimmerman, T. D. Shupe, and B. E. Petersen, “Immunogenicity of decellularized porcine liver for bioengineered hepatic tissue,” (in eng), The American journal of pathology, vol. 183, no. 2, pp. 558-65, Aug 2013. [CrossRef]
- G. Orlando et al., “Production and implantation of renal extracellular matrix scaffolds from porcine kidneys as a platform for renal bioengineering investigations,” (in eng), Annals of surgery, vol. 256, no. 2, pp. 363-70, Aug 2012. [CrossRef]
- Musselmann, B. Kane, B. Alexandrou, and J. R. Hassell, “Stimulation of collagen synthesis by insulin and proteoglycan accumulation by ascorbate in bovine keratocytes in vitro,” (in eng), Investigative ophthalmology & visual science, vol. 47, no. 12, pp. 5260-6, Dec 2006. [CrossRef]
- M. Meek and C. Knupp, “Corneal structure and transparency,” (in eng), Progress in retinal and eye research, vol. 49, pp. 1-16, Nov 2015. [CrossRef]
- W. Teng et al., “Multiphoton autofluorescence and second-harmonic generation imaging of the ex vivo porcine eye,” (in eng), Investigative ophthalmology & visual science, vol. 47, no. 3, pp. 1216-24, Mar 2006. [CrossRef]
- Morishige et al., “Second-harmonic imaging microscopy of normal human and keratoconus cornea,” (in eng), Investigative ophthalmology & visual science, vol. 48, no. 3, pp. 1087-94, Mar 2007. [CrossRef]
- Jalbert, F. Stapleton, E. Papas, D. F. Sweeney, and M. Coroneo, “In vivo confocal microscopy of the human cornea,” (in eng), The British journal of ophthalmology, vol. 87, no. 2, pp. 225-36, Feb 2003. [CrossRef]
- Cai, A. C. Lai, K. Liao, P. R. Corridon, D. J. Graves, and V. Chan, “Recent Advances in Fluorescence Recovery after Photobleaching for Decoupling Transport and Kinetics of Biomacromolecules in Cellular Physiology,” Polymers (Basel), vol. 14, no. 9, May 7 2022. [CrossRef]
- A. Collett et al., “Hydrodynamic Isotonic Fluid Delivery Ameliorates Moderate-to-Severe Ischemia-Reperfusion Injury in Rat Kidneys,” J Am Soc Nephrol, vol. 28, no. 7, pp. 2081-2092, Jul 2017. [CrossRef]
- R. Corridon, “Enhancing the expression of a key mitochondrial enzyme at the inception of ischemia-reperfusion injury can boost recovery and halt the progression of acute kidney injury,” Front Physiol, vol. 14, p. 1024238, 2023. [CrossRef]
- R. Corridon et al., “A method to facilitate and monitor expression of exogenous genes in the rat kidney using plasmid and viral vectors,” (in eng), Am J Physiol Renal Physiol, vol. 304, no. 9, pp. F1217-29, May 1 2013. [CrossRef]
- A.M. Hall, G. J. Rhodes, R. M. Sandoval, P. R. Corridon, and B. A. Molitoris, “In vivo multiphoton imaging of mitochondrial structure and function during acute kidney injury,” Kidney Int, vol. 83, no. 1, pp. 72-83, Jan 2013. [CrossRef]
- L. Kolb et al., “Exogenous Gene Transmission of Isocitrate Dehydrogenase 2 Mimics Ischemic Preconditioning Protection,” J Am Soc Nephrol, vol. 29, no. 4, pp. 1154-1164, Apr 2018. [CrossRef]
- Shaya et al., “Design, photophysical properties, and applications of fluorene-based fluorophores in two-photon fluorescence bioimaging: A review,” Journal of Photochemistry and Photobiology C: Photochemistry Reviews, vol. 52, p. 100529, 2022/09/01/2022. [CrossRef]
- R. Corridon, S. H. Karam, A. A. Khraibi, A. A. Khan, and M. A. Alhashmi, “Intravital imaging of real-time endogenous actin dysregulation in proximal and distal tubules at the onset of severe ischemia-reperfusion injury,” Scientific Reports, vol. 11, no. 1, p. 8280, 2021/04/15 2021. [CrossRef]
- A. Torricelli, V. Singh, V. Agrawal, M. R. Santhiago, and S. E. Wilson, “Transmission electron microscopy analysis of epithelial basement membrane repair in rabbit corneas with haze,” (in eng), Investigative ophthalmology & visual science, vol. 54, no. 6, pp. 4026-33, Jun 10 2013. [CrossRef]
- Goswami et al., “Gene Therapy Leaves a Vicious Cycle,” Front Oncol, vol. 9, p. 297, 2019. [CrossRef]
- W. Drexler, U. Morgner, R. K. Ghanta, F. X. Kärtner, J. S. Schuman, and J. G. Fujimoto, “Ultrahigh-resolution ophthalmic optical coherence tomography,” (in eng), Nature medicine, vol. 7, no. 4, pp. 502-7, Apr 2001. [CrossRef]
- M. Corridon, R. Ascázubi, C. Krest, and I. Wilke, “Time-domain terahertz spectroscopy of artificial skin,” in Society of Photo-Optical Instrumentation Engineers (SPIE) Conference Series, February 01, 2006 2006, vol. 6080, p. 608007, doi: 10.1117/12.646632. [Online]. Available: https://ui.adsabs.harvard.edu/abs/2006SPIE.6080E..07C.
- He, D. Wang, and Y. Jiang, “Overview of Ultrasound Biomicroscopy,” (in eng), Journal of current glaucoma practice, vol. 6, no. 1, pp. 25-53, Jan-Apr 2012. [CrossRef]
- L. Alexander et al., “A systematic review of ultrasound biomicroscopy use in pediatric ophthalmology,” (in eng), Eye (London, England), vol. 35, no. 1, pp. 265-276, Jan 2021. [CrossRef]
- J. A. Stammen, S. Williams, D. N. Ku, and R. E. Guldberg, “Mechanical properties of a novel PVA hydrogel in shear and unconfined compression,” (in eng), Biomaterials, vol. 22, no. 8, pp. 799-806, Apr 2001. [CrossRef]
- J. L. Calkins, B. F. Hochheimer, and W. J. Stark, “Corneal wound healing: holographic stress-test analysis,” (in eng), Investigative ophthalmology & visual science, vol. 21, no. 2, pp. 322-34, Aug 1981.
- J. Wang et al., “Effect of travoprost, latanoprost and bimatoprost PGF2α treatments on the biomechanical properties of in-vivo rabbit cornea,” (in eng), Experimental eye research, vol. 215, p. 108920, Feb 2022. [CrossRef]
- Kaushik and S. S. Pandav, “Ocular Response Analyzer,” (in eng), Journal of current glaucoma practice, vol. 6, no. 1, pp. 17-19, Jan-Apr 2012. [CrossRef]
- R. Joseph, O. P. Srivastava, and R. R. Pfister, “Modeling Keratoconus Using Induced Pluripotent Stem Cells,” (in eng), Investigative ophthalmology & visual science, vol. 57, no. 8, pp. 3685-97, Jul 1 2016. [CrossRef]
- G. A. Villalona et al., “Cell-seeding techniques in vascular tissue engineering,” (in eng), Tissue engineering. Part B, Reviews, vol. 16, no. 3, pp. 341-50, Jun 2010. [CrossRef]
- J. Fernández-Pérez and M. Ahearne, “Decellularization and recellularization of cornea: Progress towards a donor alternative,” (in eng), Methods (San Diego, Calif.), vol. 171, pp. 86-96, Jan 15 2020. [CrossRef]
- Nouri Barkestani, S. Naserian, G. Uzan, and S. Shamdani, “Post-decellularization techniques ameliorate cartilage decellularization process for tissue engineering applications,” Journal of Tissue Engineering, vol. 12, p. 2041731420983562, 2021/01/01 2021. [CrossRef]
- S. Avadhanam, H. E. Smith, and C. Liu, “Keratoprostheses for corneal blindness: a review of contemporary devices,” (in eng), Clin Ophthalmol, vol. 9, pp. 697-720, 2015. [CrossRef]
- G. Holland et al., “Artificial Cornea: Past, Current, and Future Directions,” (in English), Frontiers in Medicine, Review vol. 8, 2021-November-12 2021. [CrossRef]
- Gulati, S. K. Salaria, V. Anand, N. Jain, and S. Pandey, “Periodontium bestows vision!!,” (in eng), Journal of Indian Society of Periodontology, vol. 20, no. 3, pp. 349-51, May-Jun 2016. [CrossRef]
- V. Chirila, “An overview of the development of artificial corneas with porous skirts and the use of PHEMA for such an application,” (in eng), Biomaterials, vol. 22, no. 24, pp. 3311-7, Dec 2001. [CrossRef]
- G. J. Crawford et al., “The Chirila Keratoprosthesis: phase I human clinical trial,” (in eng), Ophthalmology, vol. 109, no. 5, pp. 883-9, May 2002. [CrossRef]
- Fagerholm et al., “A biosynthetic alternative to human donor tissue for inducing corneal regeneration: 24-month follow-up of a phase 1 clinical study,” (in eng), Science translational medicine, vol. 2, no. 46, p. 46ra61, Aug 25 2010. [CrossRef]
- J. M. Hackett et al., “Biosynthetic corneal implants for replacement of pathologic corneal tissue: performance in a controlled rabbit alkali burn model,” (in eng), Investigative ophthalmology & visual science, vol. 52, no. 2, pp. 651-7, Feb 3 2011. [CrossRef]
- Brunette et al., “Alternatives to eye bank native tissue for corneal stromal replacement,” (in eng), Progress in retinal and eye research, vol. 59, pp. 97-130, Jul 2017. [CrossRef]
- D. F. Duarte Campos et al., “Corneal bioprinting utilizing collagen-based bioinks and primary human keratocytes,” (in eng), Journal of biomedical materials research. Part A, vol. 107, no. 9, pp. 1945-1953, Sep 2019. [CrossRef]
- A. Isaacson, S. Swioklo, and C. J. Connon, “3D bioprinting of a corneal stroma equivalent,” (in eng), Experimental eye research, vol. 173, pp. 188-193, Aug 2018. [CrossRef]
- El-Massry, O. Ibrahim, M. Abdalla, I. Osman, and S. Mahmoud, “Safety and Indicative Effectiveness of Porcine Corneal Lenticular Implants in Patients with Advanced Keratoconus and Post Lasik Ectasia: A Retrospective Clinical Study,” (in eng), Clinical ophthalmology (Auckland, N.Z.), vol. 15, pp. 3165-3171, 2021. [CrossRef]
- Elsheikh, D. Alhasso, and P. Rama, “Biomechanical properties of human and porcine corneas,” (in eng), Experimental eye research, vol. 86, no. 5, pp. 783-90, May 2008. [CrossRef]
- H. S. Dua, L. A. Faraj, D. G. Said, T. Gray, and J. Lowe, “Human corneal anatomy redefined: a novel pre-Descemet’s layer (Dua’s layer),” (in eng), Ophthalmology, vol. 120, no. 9, pp. 1778-85, Sep 2013. [CrossRef]
- D. E. Birk, J. M. Fitch, and T. F. Linsenmayer, “Organization of collagen types I and V in the embryonic chicken cornea,” (in eng), Investigative ophthalmology & visual science, vol. 27, no. 10, pp. 1470-7, Oct 1986.
- K. Gordon, J. W. Foley, D. E. Birk, J. M. Fitch, and T. F. Linsenmayer, “Type V collagen and Bowman’s membrane. Quantitation of mRNA in corneal epithelium and stroma,” (in eng), The Journal of biological chemistry, vol. 269, no. 40, pp. 24959-66, Oct 7 1994.
- K. Gipson, S. J. Spurr-Michaud, and A. S. Tisdale, “Anchoring fibrils form a complex network in human and rabbit cornea,” (in eng), Investigative ophthalmology & visual science, vol. 28, no. 2, pp. 212-20, Feb 1987.
- Y. Komai and T. Ushiki, “The three-dimensional organization of collagen fibrils in the human cornea and sclera,” (in eng), Investigative ophthalmology & visual science, vol. 32, no. 8, pp. 2244-58, Jul 1991.
- A.J. Quantock et al., “From nano to macro: studying the hierarchical structure of the corneal extracellular matrix,” (in eng), Experimental eye research, vol. 133, pp. 81-99, Apr 2015. [CrossRef]
- C. Davies, S. J. Jenkins, J. E. Allen, and P. R. Taylor, “Tissue-resident macrophages,” (in eng), Nature immunology, vol. 14, no. 10, pp. 986-95, Oct 2013. [CrossRef]
- Kawakita, E. M. Espana, H. He, W. Li, C. Y. Liu, and S. C. Tseng, “Intrastromal invasion by limbal epithelial cells is mediated by epithelial-mesenchymal transition activated by air exposure,” (in eng), The American journal of pathology, vol. 167, no. 2, pp. 381-93, Aug 2005. [CrossRef]
- M. Fitch, D. E. Birk, C. Linsenmayer, and T. F. Linsenmayer, “The spatial organization of Descemet’s membrane-associated type IV collagen in the avian cornea,” (in eng), The Journal of cell biology, vol. 110, no. 4, pp. 1457-68, Apr 1990. [CrossRef]
- S. Penn, A. Madan, R. B. Caldwell, M. Bartoli, R. W. Caldwell, and M. E. Hartnett, “Vascular endothelial growth factor in eye disease,” (in eng), Progress in retinal and eye research, vol. 27, no. 4, pp. 331-71, Jul 2008. [CrossRef]
- R. Hassell and D. E. Birk, “The molecular basis of corneal transparency,” (in eng), Experimental eye research, vol. 91, no. 3, pp. 326-35, Sep 2010. [CrossRef]
- D. M. Maurice, “The structure and transparency of the cornea,” (in eng), The Journal of physiology, vol. 136, no. 2, pp. 263-86, Apr 30 1957. [CrossRef]
- M. Meek and D. W. Leonard, “Ultrastructure of the corneal stroma: a comparative study,” (in eng), Biophysical journal, vol. 64, no. 1, pp. 273-80, Jan 1993. [CrossRef]
- D. E. Birk and R. L. Trelstad, “Extracellular compartments in matrix morphogenesis: collagen fibril, bundle, and lamellar formation by corneal fibroblasts,” (in eng), The Journal of cell biology, vol. 99, no. 6, pp. 2024-33, Dec 1984. [CrossRef]
- M. Griffith, R. d. Cataldo, and K. H. Fogarty, “Do-It-Yourself: 3D Models of Hydrogenic Orbitals through 3D Printing,” Journal of Chemical Education, vol. 93, no. 9, pp. 1586-1590, 2016/09/13 2016. [CrossRef]
- Z. Gu, J. Fu, H. Lin, and Y. He, “Development of 3D bioprinting: From printing methods to biomedical applications,” (in eng), Asian journal of pharmaceutical sciences, vol. 15, no. 5, pp. 529-557, Sep 2020. [CrossRef]
- J. Kort-Mascort et al., “Decellularized ECM hydrogels: prior use considerations, applications, and opportunities in tissue engineering and biofabrication,” Biomaterials Science, 10.1039/D2BM01273A vol. 11, no. 2, pp. 400-431, 2023. [CrossRef]
- M. Giraud Guille, G. Mosser, C. Helary, and D. Eglin, “Bone matrix like assemblies of collagen: from liquid crystals to gels and biomimetic materials,” (in eng), Micron (Oxford, England: 1993), vol. 36, no. 7-8, pp. 602-8, 2005. [CrossRef]
- Hemmavanh, M. Koch, D. E. Birk, and E. M. Espana, “Abnormal corneal endothelial maturation in collagen XII and XIV null mice,” (in eng), Investigative ophthalmology & visual science, vol. 54, no. 5, pp. 3297-308, May 7 2013. [CrossRef]
- K. Olivero and L. T. Furcht, “Type IV collagen, laminin, and fibronectin promote the adhesion and migration of rabbit lens epithelial cells in vitro,” (in eng), Investigative ophthalmology & visual science, vol. 34, no. 10, pp. 2825-34, Sep 1993.
- E.-L. Martola and J. L. Baum, “Central and Peripheral Corneal Thickness: A Clinical Study,” Archives of Ophthalmology, vol. 79, no. 1, pp. 28-30, 1968. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



