
Submitted:
08 April 2023
Posted:
10 April 2023
You are already at the latest version
Abstract
Introduction: Unlike cigarette smoking, secondhand smoke (SHS) has not been as well described as an environmental risk for Multiple sclerosis (MS) nor as a risk factor for disease progression. We systematically reviewed the association between SHS and the risk of onset and/or progression of MS.Methods: We systematically screened MEDLINE/PUBMED, Science Direct, LILACs, and SCIELO searching for publications between January 1st , 2010, and July 5, 2021 with the following keywords: “multiple sclerosis and smoking”; “multiple sclerosis and passive smoking”; “multiple sclerosis and secondhand smoking”. An 11-year filter was applied from 2010 to 2021. Results: Fifteen articles were included in this review, which consisted of systematic reviews with meta-analysis (N = 2), systematic reviews (N = 2), and observational studies (N = 11). Both meta-analyses reported an impact of SHS on MS onset among secondhand smokers. One of the systematic reviews selected two observational studies showing the association between SHS and MS development, and one study that did not find a significant association between SHS and the risk of MS development. The other systematic review identified selected eight articles showing a relationship between SHS and MS. Seven observational studies reported higher odds of MS onset when associated with SHS. Four observational studies did not show a relationship between SHS and MS onset or progression.Discussion: Most articles showed a positive association between SHS exposure and the risk of developing MS. On the other hand, an association between SHS and a higher risk for MS progression could not be established.
Keywords:
Multiple Sclerosis
; Onset
; Progression
; Secondhand Smoke
; Systematic Review
1. Introduction
Multiple sclerosis (MS) is a chronic inflammatory demyelinating autoimmune disorder of the central nervous system (CNS)[1]. It is the most common demyelinating disease in highincome countries, with a prevalence of approximately 140/100,000 inhabitants in North America and 108/100,000 in Europe[2]. The etiology of MS remains unclear, but environmental and lifestyle components, accompanied by genetic susceptibility, have been associated with an increased risk of MS[1].
Tobacco smoking has been consistently reported as a MS environmental risk, increasing the propensity of developing such disorder. Moreover, smoking is additionally mentioned as a risk factor for a more aggressive disease progression. In a case-control study, smoking was associated with a 50% increase in risk for MS onset (odds ratio, OR 1.5, 95% confidence interval, CI 1.0–2.1)[3]. Furthermore, a cross-sectional study showed that smoking after MS diagnosis is associated with a reduced time for the development of secondary progressive MS[4].
Moreover, there seems to be an interaction between active smoking and human leukocyte antigen (HLA) complex genes associated with higher MS risk. A case-control study demonstrated the impact of HLA-DRB1*15 and HLA-A*02 on MS predisposition. When smoking was linked to the carriage of HLA-DRB1*15 and absence of HLA-A*02, the OR was 13.5 (95% CI 8.1– 22.6). On the other hand, smokers without both risk genotypes presented an OR of 1.4 (95% CI 0.9–2.1)[5].
The mechanism underlying the relationship between smoking and MS is not entirely understood. Okinger and colleagues showed that smoking increases the number of alveolar macrophages, in addition to altering the distribution of alveolar macrophages and lymphocytes in the bronchoalveolar lavage fluid[6]. With a proinflammatory environment, foreign antigens that are present in smoke, together with sequestered antigens, which are generated by mucosal cells injury, and neoantigens, which are promoted by reactive oxygen species, may result in a crossreaction with self-antigens, inducing autoimmunity[7].
Unlike cigarette smoking, secondhand smoke (SHS) – which is formed from the burning of cigarettes and other tobacco products and from smoke exhaled by the smoker – has not been as well described as an environmental risk for MS nor as a risk factor for disease progression[8]. It is important to note that although the overall exposure to SHS among non-smokers in the US has declined between the years of 1988 and 2014, its prevalence has not decreased significantly in recent years. In addition, 25% of nonsmokers, including 14 million children, were exposed to SHS between 2013 and 2014[9]. Thus, it would be of great importance to establish whether SHS impacts the onset or progression of MS.
Therefore, we conducted a systematic review to analyze the association between SHS and the risk of onset and/or progression of MS.
2. Methods
This systematic review was conducted according to the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (https://pubmed.ncbi.nlm.nih.gov/19621072/). There was no previous protocol registered.
2.1. Literature search
The authors systematically screened MEDLINE/PUBMED, Science Direct, LILACs, and SCIELO from July 5, 2021 to August 13, 2021, with the following keywords: “multiple sclerosis and smoking”; “multiple sclerosis and passive smoking”; “multiple sclerosis and secondhand smoking”. An 11-year filter was applied (from 2010 to 2021).
2.2. Eligibility criteria
The eligibility criteria encompassed studies that: (I) were published in English, Spanish or Portuguese; (II) described the association between passive/secondhand smoking and MS; (III) were published between January 1st , 2010, and July 5, 2021; and (IV) were either prospective or retrospective clinical trials, case reports, systematic reviews or meta-analyses. The present paper did not include studies that: (I) presented other study designs, such as non-systematic reviews; (II) were not indexed in the screened platforms; and (III) did not describe the association between passive/secondhand smoke and MS. Additionally, duplicate articles were only counted once.
2.3. Risk of bias
Two independent reviewers (CSS and VC) conducted the primary literature research using the previously described search terms. At first, titles and abstracts were screened based on the eligibility criteria. The full texts of all the screened abstract were evaluated by a third reviewer (MAMS). In case of doubt, the most experienced author (MVMG) re-evaluated the studies. Two independent reviewers (BSC and MHMC) assessed the risk of bias in each systematic review and meta-analysis according to the AMSTAR 2 guidelines[10], whereas observational studies were analyzed using The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Non-randomized Studies in Meta-analyses[11]. No study was excluded based on the risk of bias.
2.4. Data extraction and synthesis
Using the keywords, 626 articles were identified in the MEDLINE/PUBMED platform. In ScienceDirect, 15,696 articles were identified, and 12 of those were duplicated. Four articles were identified in LILACs. No articles were found in the SCIELO platform. Thus, 16,314 articles were screened for title and abstract and 16,225 were excluded because they did not fit in the inclusion criteria, especially due to study design. Subsequently, 89 full texts were reviewed (83 from MEDLINE/PUBMED and 5 from Science Direct) and 74 were excluded after full text reading, mainly for not having data on SHS and MS. Finally, 15 studies were included in this review. Figure 1 illustrates the flow chart, according to the PRISMA statement.
3. Results
The 15 studies included in this review consisted of systematic reviews with meta-analyses (N = 2), systematic reviews (N = 2) and observational studies (N = 11). Among the 11 observational studies, four were exclusively about SHS, six were non-exclusively about SHS, and the last one was about waterpipe smoking. Table 1 summarizes all studies included with their populations, main findings, and limitations.
Both meta-analyses included in the present study reported an impact of SHS on MS onset among secondhand smokers, with an OR of 1.12 in one of them and an OR of 1.24 in the other[12,13]. Furthermore, a systematic review from Canada selected 2 observational studies showing the association between SHS and MS development, reporting an OR for MS risk of 1.3 in a Swedish study from 2011, and an OR of 2.12 in a French study from 2007[14]. A study from the USA was also selected and it did not show a significant association between SHS and the risk of MS development[14]. The other systematic review identified for the present study selected eight articles showing a relationship between SHS and MS[15]. Four of them reported a positive association on SHS and MS development, whereas the other four studies showed no interaction[15].
Among the twelve observational studies identified, seven of them reported higher odds of MS onset when associated with SHS. A case-control study from Denmark showed an OR for MS risk of 1.43 among females in the first cohort studied, and an OR for MS risk of 1.593 among males in the second cohort[16]. Another study, from Japan, reported that exposure to SHS was associated with greater MS risk, displaying an OR of 1.31[17]. Moreover, a study from the USA also showed that SHS was associated with MS onset, reporting an OR of 1.37[18]. In Iran, a casecontrol study showed an OR of 1.85 for MS development[19]. Three studies from Sweden reported higher MS risk. One of them displayed an OR of 1.1, another showed an OR of 1.3, and the last one – associating SHS in a genetically predisposed cohort – revealed an OR of 7.7[20- 22].
Four observational studies did not show a relationship between SHS and MS risk. A crosssectional study from Colombia reported that this association was not statically significant (p = 0.5959)[23]. A study from Iran reported an OR of 0.79 for MS progression risk associated with SHS exposure[24]. The impact of SHS on MS progression was also analyzed in a study from Italy, revealing that no significant relationship was found[25]. In a case-control study from the United Kingdom, individualsthat were exposed to SHS at home presented an OR of 0.87, whereas exposure at the workplace showed an OR of 0.99[26].
4. Discussion
4.1. Systematic Reviews and Meta-Analyses
The present paper included two systematic reviews and two meta-analyses[12-15]. However, none of them approached SHS exclusively. Three of them were focused on the effects of smoking and MS risk, including SHS among smoking types[12,13,15]. The other one included a variety of factors associated with MS development risk, relapse, and progression[14].
Among these papers, the most recent was published in 2017 by Degelman and Herman, who performed a systematic review utilizing the Bradford Hill criteria for causation between smoking and both MS development risk and MS progression risk[15]. There were eight articles on SHS and MS risk included in this study. Four of them showed positive results between the association of SHS exposure and the risk of MS; one was exclusively focused on children, one utilized cotinine as a marker of exposure, and the other two articles detected a dose-dependent risk using time of exposure as a measure. The other four studies included, however, failed to show a significant association between SHS and the risk of MS development. Three of them were casecontrol studies while the other one was a cohort of female nurses. In this systematic review, the authors were unable to perform a meta-analysis due to the heterogeneity among the eight studies. There were discrepancies regarding the definition of SHS, and the characteristics of the populations studied were not comparable. Degelman and Herman additionally commented on mixed results from other two meta-analyses, which were also included in the present paper and are discussed further separately[12,13,15].
One of the meta-analyses cited by Dengelman and Herman was published in 2017 by Poorolajal and colleagues, with a focus on the evaluation of different types of smoking exposure and their influence on MS onset[12]. Regarding SHS, this study included three articles with an overall OR of 1.12 (95% CI: 0.87-1.36) and substantial heterogeneity of I2 = 66%. These results were briefly shown and were not described in detail in the meta-analyses[12].
The other meta-analysis was published in 2016[13]. Zhang and colleagues included 3 studies – of which 2 were also selected in the study by Poorolajal et al. – and found a significant relationship between SHS and MS with an OR of 1.24 (95% CI 1.03-1.49) and a similar heterogeneity found in the study by Poorolajal and colleagues (I 2 = 67%)[13].
The fourth systematic review included in the present study, published in 2017, was not focused on SHS and neither on smoking; instead, it encompassed all factors associated with MS onset, relapse, and progression[14]. McKay and colleagues included two articles on SHS that were published before 2010, which were not included in the present review due to the established publication year restriction[14]. The first one was a French study that evaluated the risk of parental home smoking and MS development, showing a significant relationship between SHS in childhood and early MS onset (OR of 2.12). In addition, this study showed a higher risk in older children - older than 10 years - when compared to younger ones (relative risk, RR of 2.49)[14]. The other study was the cohort of female nurses included in Degelman and Herman article as well [14,15]. A third study, carried out by Hedström et al., was also included by McKay and colleagues, and also selected for the present article, which will be further discussed[14,21].
Hence, SHS was never the main topic of a systematic review. Even in papers published over the same period of time – with similar methodologies –, there is an important disparity in the results displayed. An important factor that may have caused this variety regards the large number of different terms representing SHS found in the databases (“passive smoking”; “secondhand smoking”; “smoking exposure”; “environmental smoking”). This can make it more difficult to select all articles of interest.
4.2. Observational Studies
There are eleven observational studies included in the present paper that analyzed the association between SHS and MS[16-26]. They are either case-control or cohort studies evaluating either SHS and MS development risk or the impact of SHS on MS progression. Four of these articles were designed exclusively to assess the relationship between SHS and MS, whereas the others assessed SHS among other different factors for MS development or progression.
Among the four studies designed exclusively to analyze SHS as an environmental risk factor for developing MS, the oldest one is a case-control study (695 cases and 1,635 controls), published in 2011, that included only subjects that had never smoked, evaluating the impact of SHS on the risk of developing MS[21]. The authors also analyzed confounding factors such as serum vitamin D levels and Epstein Barr virus status in this population. The results showed that 39% of cases and 34% of controls were exposed to SHS, and that the exposure occurred almost exclusively at home. The study found a higher MS risk (OR 1.3, 95% CI 1.1-1.6) in subjects exposed to SHS compared to those who have never been exposed. In addition, the article revealed a trend suggesting that longer exposure time resulted in higher risk, showing an OR of 1.8 (95% CI 1.2-2.6) with a 20-year exposure[21].
Another study by Hedström and colleagues included in our review provided data on the interaction between the HLA-DRB1 * 15 and HLA-A * 02 genotypes – the former being associated with an increased risk of MS and the latter having a protective effect for MS[22]. As in their previous study, confounding factors, such as vitamin D and Epstein Barr virus status, were analyzed and the selection of subjects was restricted to people who never smoked. Non-smokers who also have never been exposed to SHS presented a higher risk of developing MS when they presented both genetic risks (OR 4.5, 95% CI 3.3-6.1). When individuals with the same genotype were exposed to SHS, the risk of developing MS increased significantly (OR 7.7, 95% CI 5.5- 10.8), showing that SHS may be an independent risk factor for MS onset[22].
Lavery and colleagues explored the effects of SHS in a USA cohort composed by 216 children with acquired demyelinating syndromes (ADS) and 81 children with MS[18]. They showed that 37% of patients that progressed to MS were exposed to SHS, whereas among patients with monophasic ADS, 29.5% were exposed. In addition, an investigation between the interaction of HLA-DRB1*15 and SHS was carried out, showing that carriage of this genotype – which was observed in 41.9% of the MS cohort – without SHS exposure did not increase the risk of developing MS. When both SHS exposure and the genotype were present, the OR for MS increased to 3.71 (95% CI 1.17-11.9). Together, these two factors accounted for a 54% MS risk[18].
The most recent study that focused on SHS as a risk factor for developing MS was published in 2021[16]. Oturai and colleagues explored the exposure to SHS during adolescence (from 10 to 19 years old) and its relationship with MS. Subjects that were smokers before the age of 19 years were excluded. Also, the population included, comprising a total of 2,589 individuals, was divided into never-smokers, with 342 cases and 590 controls, and those who became smokers after the age of 19 years, with 577 cases and 1,080 controls. Interestingly, SHS was not associated with MS in men who had never smoked. However, in men who became active smokers in adulthood, the association between SHS and the disorder showed an OR of 1.593 (95% CI 1.070- 2.372). In contrast, among women who had never smoked, SHS was associated with MS risk (OR 1.43, 95% CI 1.02 to 2.01), increasing the odds of developing the disorder by 4.6% for each year of exposure. Also, in women who became active smokers after 19 years of age, SHS during adolescence did not increase the chances of developing MS[16].
Regarding the remaining studies included in this article, none of them were designed exclusively to assess the impact of exposure to SHS on MS risk[17,19,20,23-26]. Among these studies, two of them – one from a Japanese cohort comprising 227 individuals and the other from a Swedish cohort with 7,791 individuals – showed that SHS was associated with an increased risk for MS[17,20]. In the Japanese study, SHS exposure was evaluated in subjects older than 16 years, showing a positive relationship with MS (OR of 1.31, 95% CI 1.05-1.63)[17]. In the Swedish cohort, individuals who were exposed to SHS for more than 20 years and reported actively smoking more than 10 pack-years had an almost three-times higher risk of developing MS. Interestingly, this cohort also showed a dose-response relationship between years of exposure to SHS and the risk of MS. Individuals who were exposed to SHS for less than 20 years displayed an OR of 1.1 (95% CI 1.0-1.3) for MS, while exposure for more than 20 years showed an OR of 1.4 (CI 95% 1.1-1.8)[20].
With regards to studies that found negative results, a Canadian case-control study performed a questionnaire to investigate lifetime cigarette smoking and SHS exposure with MS development[26]. The study comprised 3,157 MS cases and 756 controls. Among never-smoker subjects (N = 1,394) there was no association between MS risk and SHS exposure either at home (OR of 0.87, 95% CI 0.71-1.41) or at the workplace (OR of 0.99, 95% CI 0.71-1.41)[26]. The other is a Colombian study composed of 87 MS cases and 87 controls, all older than 18 years[23]. Subjects were interviewed to assess environmental risk factors for MS. Regarding SHS, subjects were asked if they were exposed between the ages of 19 to 25 years. Neither cigarette nor SHS history had a statistically significant association with an increased risk for MS onset[23].
Two additional studies evaluated the impact of SHS in the disease’s severity and progression; however, they showed no association[24,25]. An Italian cohort composed of 131 individuals with MS completed a questionnaire about lifetime smoking habits. Moreover, the authors of the study considered SHS exposure only over the 12 months prior to the questionnaire. The study did not identify a significant association between either cigarette smoking status or exposure to SHS and the severity of MS[25]. In the other study, an interview regarding environmental risk factors for MS severity was carried out with an Iranian cohort composed of 660 individuals with MS. This study showed that SHS was not related to MS severity, showing an OR of 0.79 (95% CI 0.47-1.43)[24].
The last one, an Iranian case-control study evaluated the risk between waterpipe smoke and MS development[19]. This article showed that, besides active waterpipe smoke, SHS was associated with MS risk, displaying an important impact (OR of 1.85, 95% CI 1.48-2.32) with a dose-dependent increase in risk. Interestingly, in this study, SHS during childhood and adolescence was not statistically significant for increasing the risk of MS. Furthermore, the study shows that subjects exposed to all three modes analyzed (waterpipe smoke, tobacco smoke, and SHS) had a 4.1 higher odds of having MS compared to subjects that were not exposed[19].
As with the systematic reviews and meta-analysis, the majority of observational studies also did not focus on SHS exclusively. In addition, there may be imprecision in the methods of quantifying exposure to SHS. Unlike active smoking, which has some quantitative measures such as pack-years, exposure to SHS is usually measured based on questionnaires referring to the subject’s exposure history, which makes the information more susceptible to recall bias.
5. Conclusion
As shown from the studies selected by the present review, the majority of articles displayed a positive association between SHS exposure and the risk of developing MS. In addition, when considering only studies that were exclusively designed to evaluate SHS exposure, the association was found in all of them. Some articles showed that exposure during childhood resulted in a considerably higher risk. Also, the reviewed data about the relationship between SHS and genetic risk factors, such as HLA-DRB1 * 15 and HLA-A * 02 genotypes, show a strong impact on the odds of developing the disorder. Moreover, a dose-dependent risk relationship between years of exposure to SHS and MS risk was observed in some cohorts. On the other hand, the association between SHS and a higher risk for MS progression could not be established.
The large number of different terms representing SHS found in the databases may have led to difficulties in selecting all articles of interest; however, the researchers examined a large number of studies, including all different terms that could represent SHS. Overall, the present study shows evidence of the impact of SHS on the development of MS and encourages further studies addressing this topic to strengthen the establishment of this association.
Author Contributions
All authors contributed equally to the writing of this manuscript.
Funding
There was no specific financial support or sponsorship for the writing of this manuscript.
Statement of Ethics
An ethics statement is not applicable because this study is based exclusively on published literature.
Conflicts of Interest
The authors have no conflicts of interest to declare.
References
- Olsson, T. , Barcellos, L.F., Alfredsson, L., 2016. Interactions between genetic, lifestyle and environmental risk factors for multiple sclerosis. Nat. Rev. Neurol. [CrossRef]
- Leray, E. , Moreau, T., Fromont, A., Edan, G., 2016. Epidemiology of multiple sclerosis. Rev. Neurol. (Paris). [CrossRef]
- Salzer, J. , Hallmans, G., Nyström, M., Stenlund, H., Wadell, G., Sundström, P., 2013. Smoking as a risk factor for multiple sclerosis. Mult. Scler. J. [CrossRef]
- Ramanujam, R. , Hedström, A.K., Manouchehrinia, A., Alfredsson, L., Olsson, T., Bottai, M., Hillert, J., 2015. Effect of smoking cessation on multiple sclerosis prognosis. JAMA Neurol. [CrossRef]
- Hedström, A.K. , Sundqvist, E., Bäärnhielm, M., Nordin, N., Hillert, J., Kockum, I., Olsson, T., Alfredsson, L., 2011. Smoking and two human leukocyte antigen genes interact to increase the risk for multiple sclerosis. Brain. [CrossRef]
- Öckinger, J. , Hagemann-Jensen, M., Kullberg, S., Engvall, B., Eklund, A., Grunewald, J., Piehl, F., Olsson, T., Wahlström, J., 2016. T-cell activation and HLA-regulated response to smoking in the deep airways of patients with multiple sclerosis. Clin. Immunol. [CrossRef]
- Rosso, M. , Chitnis, T., 2020. Association between Cigarette Smoking and Multiple Sclerosis: A Review. JAMA Neurol. [CrossRef]
- Öberg, M. , Jaakkola, M.S., Prüss-Üstün, A., Schweizer, C., Woodward, A., 2010. Second-hand smoke: Assessing the environmental burden of disease at national and local levels. WHO Environmental Burden of Disease Series No. 18., World Health Organization.
- Tsai, J. , Homa, D.M., Gentzke, A.S., Mahoney, M., Sharapova, S.R., Sosnoff, C.S., Caron, K.T., Wang, L., Melstrom, P.C., Trivers, K.F., 2018. Exposure to Secondhand Smoke Among Nonsmokers — United States, 1988–2014. MMWR. Morb. Mortal. Wkly. Rep. [CrossRef]
- Shea, B.J. , Reeves, B.C., Wells, G., Thuku, M., Hamel, C., Moran, J., Moher, D., Tugwell, P., Welch, V., Kristjansson, E., Henry, D.A., 2017. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. [CrossRef]
- Wells, G. , Shea, B., O’Connell, D., Peterson, J., Welch, V., Losos, M., Tugwell, P., 2012. The Newcastle-Ottawa Scale (NOS) for assessing the quality if nonrandomized studies in meta-analyses. (Available from URL http//www.ohri.ca/programs/clinical_epidemiology/oxford.asp). [CrossRef]
- Poorolajal, J. , Bahrami, M., Karami, M., Hooshmand, E., 2017. Effect of smoking on multiple sclerosis: A meta-analysis. J. Public Heal. (United Kingdom). [CrossRef]
- Zhang, P. , Wang, R., Li, Z., Wang, Y., Gao, C., Lv, X., Song, Y., Li, B., 2016. The risk of smoking on multiple sclerosis: A meta-analysis based on 20,626 cases from casecontrol and cohort studies. PeerJ. [CrossRef]
- McKay, K.A. , Jahanfar, S., Duggan, T., Tkachuk, S., Tremlett, H., 2017. Factors associated with onset, relapses or progression in multiple sclerosis: A systematic review. Neurotoxicology. [CrossRef]
- Degelman, M.L. , Herman, K.M., 2017. Smoking and multiple sclerosis: A systematic review and meta-analysis using the Bradford Hill criteria for causation. Mult. Scler. Relat. Disord. [CrossRef]
- Oturai, D.B. , Bach Søndergaard, H., Koch-Henriksen, N., Andersen, C., Laursen, J.H., Gustavsen, S., Kristensen, J.T., Magyari, M., Sørensen, P.S., Sellebjerg, F., Thørner, L.W., Ullum, H., Oturai, A.B., 2021. Exposure to passive smoking during adolescence is associated with an increased risk of developing multiple sclerosis. Mult. Scler. J. [CrossRef]
- Sakoda, A. , Matsushita, T., Nakamura, Y., Watanabe, M., Shinoda, K., Masaki, K., Isobe, N., Yamasaki, R., Kira, J. ichi, 2020. Environmental risk factors for multiple sclerosis in Japanese people. Mult. Scler. Relat. Disord. [CrossRef]
- Lavery, A.M. , Collins, B.N., Waldman, A.T., Hart, C.N., Bar-Or, A., Marrie, R.A., Arnold, D., O’Mahony, J., Banwell, B., 2019. The contribution of secondhand tobacco smoke exposure to pediatric multiple sclerosis risk. Mult. Scler. J. [CrossRef]
- Abdollahpour, I. , Nedjat, S., Sahraian, M.A., Mansournia, M.A., Otahal, P., van der Mei, I., 2017. Waterpipe smoking associated with multiple sclerosis: A populationbased incident case–control study. Mult. Scler. [CrossRef]
- Hedström, A.K. , Olsson, T., Alfredsson, L., 2016. Smoking is a major preventable risk factor for multiple sclerosis. Mult. Scler. [CrossRef]
- Hedström AK, Bäärnhielm M, Olsson T, Alfredsson L, 2011. Exposure to environmental tobacco smoke is associated with increased risk for multiple sclerosis. Mult Scler. [CrossRef]
- Hedström, A.K. , Bomfim, I.L., Barcellos, L.F., Briggs, F., Schaefer, C., Kockum, I., Olsson, T., Alfredsson, L., 2014. Interaction between passive smoking and two HLA genes with regard to multiple sclerosis risk. Int. J. Epidemiol. [CrossRef]
- Toro, J. , Reyes, S., Díaz-Cruz, C., Burbano, L., Cuéllar-Giraldo, D.F., Duque, A., Reyes-Mantilla, M.I., Torres, C., Ríos, J., Rivera, J.S., Cortés-Muñoz, F., Patiño, J., Noriega, D., 2020. Vitamin D and other environmental risk factors in Colombian patients with multiple sclerosis. Mult. Scler. Relat. Disord. [CrossRef]
- Abbasi, M. , Nabavi, S.M., Fereshtehnejad, S.M., Ansari, I., Zerafatjou, N., Shayegannejad, V., Mohammadianinejad, S.E., Farhoudi, M., Noorian, A., Razazian, N., Abedini, M., Faraji, F., 2016. Risk factors of multiple sclerosis and their relation with disease severity: A cross-sectional study from Iran. Arch. Iran. Med. 2016, 19, 852–860.
- Mandia, D. , Ferraro, O.E., Nosari, G., Montomoli, C., Zardini, E., Bergamaschi, R., 2014. Environmental factors and multiple sclerosis severity: A descriptive study. Int. J. Environ. Res. Public Health. [CrossRef]
- Ramagopalan, S. V. , Lee, J.D., Yee, I.M., Guimond, C., Traboulsee, A.L., Ebers, G.C., Sadovnick, A.D., 2013. Association of smoking with risk of multiple sclerosis: A population-based study. J. Neurol. [CrossRef]
Figure 1.
Flow chart, according to the PRISMA statement.
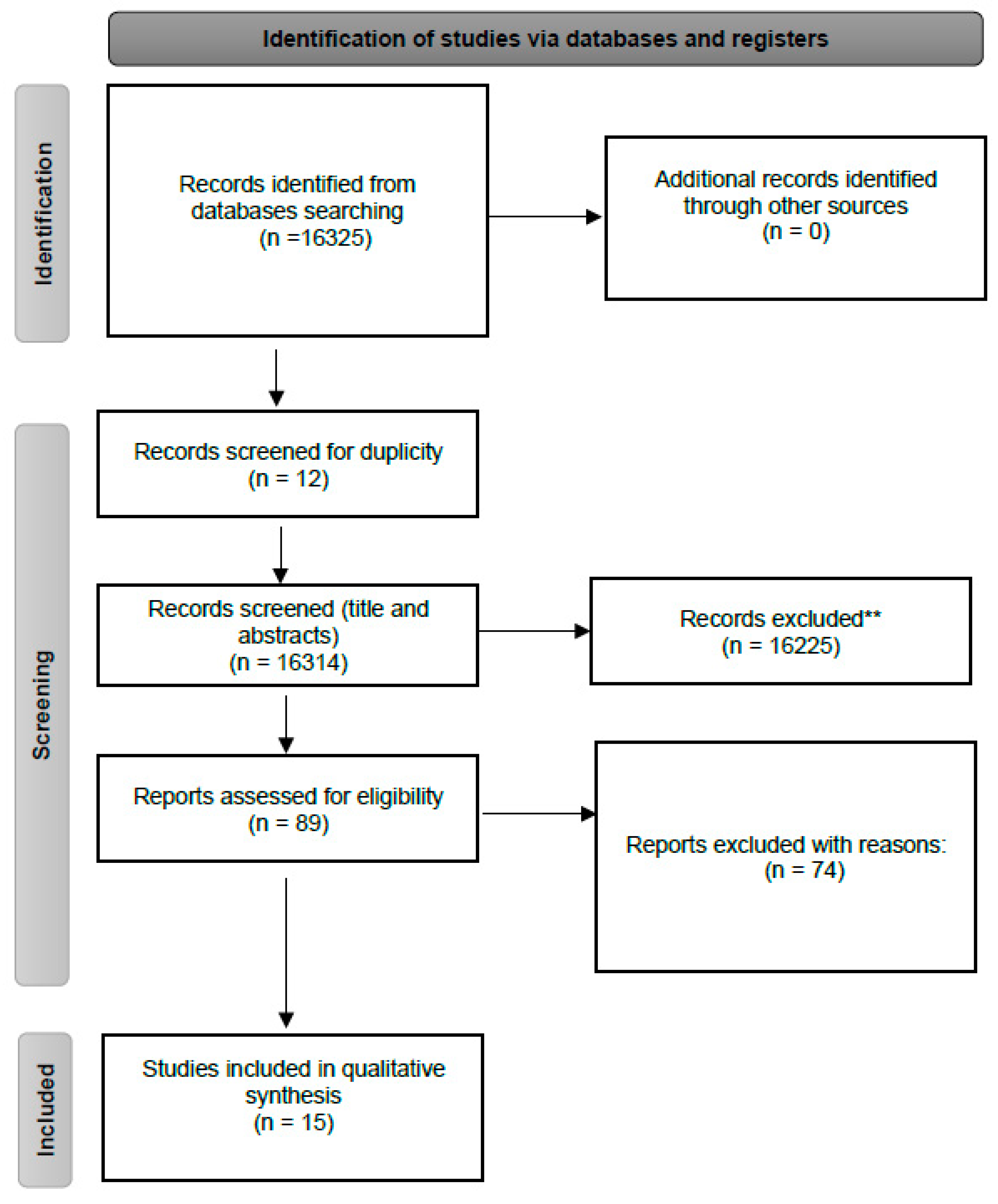

Table 1.
Compilation of the included primary articles.
| Author | Study Design, country, and year | Population | Main findings | Study limitations |
|---|---|---|---|---|
| Poorolajal et al.[12] | Meta-analysis, Iran, 2017. | - | The study indicated that both former and current smokers are predisposed to develop Multiple Sclerosis (MS). The risk increases proportionally to the number of cigarettes smoked per day. The meta-analysis selected 3 studies that show the association between MS and second-hand smoke (SHS). Among second-hand smokers, the estimated Odds Ratio (OR) of MS was 1.12, when compared with nonsmokers. | (I) Does not identify which studies had the association between MS and second-hand smoke. (II) Data regarding second-hand smokers was not detailly provided. (III) Does not detailly described selected studies. (IV) Limited number of studies in some subgroups. (V) The majority of articles selected were low-quality studies. |
| Zhang et al.[13] | Meta-analysis, China, 2016. | - | The study shows that smoking is an environmental risk to MS. The meta-analysis also identified three studies containing four study populations that show the association between secondhand smoke and MS, reporting an overall OR of 1.24. | The study did not use a technique for assessing the risk of bias in the individual studies included. |
| McKay et al.[14] | Systematic review, Canada, 2017. | - | Three studies selected evaluate the correlation between SHS and MS. Hedström et al. (2011), reported an OR of 1.3 for MS among never-smoker patients who were exposed to SHS. A French study, by Mikaeloff et al. (2007) reported an association between parental smoking and the early onset of MS in their children (OR 2.12), with a higher risk in older children, when compared to younger ones. Gardener et al. (2009) showed that children whose parents used to smoke at home had an increased risk of MS; however, when restricted to the cases that were non-smokers as adults, it was not statistically significant (OR 1.2, CI 0.90-1.5). | The vast literature present in the study limited the full discussion of some papers included, for example the strengths and limitations of each study. |
| Degelman and Herman.[15] | Systematic review, Canada, 2017. | - | Four out of the eight articles analyzed, which cited the correlation between SHS and MS, demonstrated a statistically significant association. Meta-analysis was not performed due to heterogeneity among studies. | (I) Studies included regarding the association between SHS and MS were not described in detail. (II) Quality of study evidence for each outcome was either low or very low. |
| Oturai et al.[16] | Case-control, Denmark, 2021. | N = 2,589. First cohort analyzed was composed by never-smokers (cigarettes), with 342 cases and 590 controls. The second was composed by individuals who started cigarette smoking above the age of 19, with 577 cases and 1,080 controls. | The association between exposure to SHS during adolescence (10-19 years of age) and MS was evaluated. In males, SHS exposure was not correlated to MS in neveractive smoking subjects. However, for those who became cigarette smokers in adulthood, previous SHS exposure history showed up with an OR of 1.593 for MS. SHS exposure in female neveractive smoking subjects demonstrated an OR of 1.43. There was no correlation between SHS in adolescence and MS in female patients that became active smokers after the age of 19 years. | (I) Selection of blood donors as controls. (II) Recall bias may be present, as subjects were asked about their experience and habits. (III) Authors considered SHS exposure only in the workplace or at home and did not consider the experience in other places, for example while outdoors. |
| Sakoda et al.[17] | Case-control, Japan, 2020. | N = 227. Patients with MS: 103. Controls: 124. | MS patients were evaluated regarding environmental exposure risk factors. A history of exposure to SHS was observed to have a positive correlation with MS, with an OR of 1.31. | (I) Small sample size study. (II) Recall bias may be present, as subjects were asked about their past experience and habits. (III) Cases were hospital-based and at various clinical stages, potentially producing selection bias and heterogeneity between MS subjects (IV) Not possible to distinguish patients exposed to SHS as current smokers, ex-smokers, or never-smokers |
| Lavery et al.[18] | Case-control, United States of America, 2019. | N = 297. All subjects aged less than 16 years; 216 children with monophasic acquired demyelinating syndromes (ADS); 81 children with MS. | The study concluded that SHS exposure was 37% more common in MS, in comparison to monophasic acquired demyelinating syndromes (29.5%); however, it was not an independent factor. When associated with the presence of HLADRB1*15, an OR of 3.7 for MS was reached. | (I) Recall bias may be present, as subjects were asked about their past experience and habits. (II) Authors considered SHS exposure only at home and did not consider the experience in other places, for example while outdoors. |
| Abdollahpour et al.[19] | Case-control, Iran, 2017. | N = 1,604. Subjects with MS: 547; Controls: 1,057. | This article demonstrated that active waterpipe (OR 1.77), cigarette (OR 1.69) or secondhand (OR 1.85) tobacco smoking exposure is associated with increased MS risk. Regarding passive smoking, a much stronger association was found in exposures after the age of 20 years (OR~2.2). | (I) Recall bias may be present, as subjects were asked about their past experience and habits. (II) Authors considered SHS exposure only at home and did not consider the experience in other places, for example while outdoors or workplace. |
| Hedström et al.[20] | Case-control, Sweden, 2016. | N = 7,791. Among cases exposed to SHS: 457 never-smokers; 775 smokers. Among controls exposed to SHS: 1,115 never-smokers; 1,321 smokers. | The study assessed the impact of smoking and SHS on MS risk. The exposure to SHS in neversmokers was associated with the occurrence of MS in a dose-dependent manner, with an obtained OR of 1.1 for 1-20 years of exposure and 1.4 for more than 20 years of exposure | (I) Recall bias may be present, as subjects were asked about their experience and habits. (II) Authors considered SHS exposure only in the workplace or at home and did not consider the experience in other places, for example while outdoors. |
| Hedström et al.[21] | Case-control, Sweden, 2011. | N = 2,330. Patients with MS: 695. Controls: 1,635. All subjects reported that they had never smoked before the year of MS onset. | This case-control study considered the exposure to SHS before the year of MS onset for cases and during the same period in the corresponding controls. Subjects who were exposed to SHS were found to be 30% more susceptible to develop MS. Furthermore, the exposure time was directly correlated with risk, when greater than or equal to 20 years, the obtained OR was 1.8, compared to individuals who had never been exposed. | (I) Recall bias may be present, as subjects were asked about their experience and habits. (II) Authors considered SHS exposure only in the workplace or at home and did not consider the experience in other places, for example while outdoors. |
| Hedström et al.[22] | Case-control, Sweden, 2014. | N = 2,879. All subjects with MS. All subjects were never-smokers. Cases (never-smokers exposed to SHS): 1,311. Controls (never-smokers not exposed to SHS): 1,568. | This study evaluated the development of MS in groups of individuals who carried HLA-DRB1*15 and lacked HLA-A*02, which are genetic conditions that increase the susceptibility of MS (OR of 4.5). These patients presented a 7.7- fold higher chance of developing MS if exposed to SHS when compared to non-smokers never exposed to SHS without these HLA genotypes. | (I) Recall bias may be present, as subjects were asked about their experience and habits. (II) Authors considered SHS exposure only in the workplace or at home and did not consider the experience in other places, for example while outdoors. |
| Toro et al.[23] | Cross-sectional, Colombia, 2020. | N = 174. Subjects with MS: 87. Subjects without MS: 87. | In the analysis, neither cigarette nor SHS history had a statistically significant association with an increased risk for MS. | (I) Recall bias may be present, as subjects were asked about their past experience and habits. (II) No detailed quantitative data on SHS amounts. (III) Subjects were asked about SHS exposure only considering when they were 19-25 years old |
| Abbasi et al.[24] | Cross-sectional, Iran, 2016. | N = 660. All subjects with MS. | From the total of 660 patients with MS included in the study, most were female, with a median age of 37 years, and with relapsing-remitting MS clinical features. The analysis showed no association between SHS and MS severity. | (I) No detailed data on quantitative SHS amount. (II) Recall bias may be present, as subjects were asked about their experience and habits. |
| Mandia et al.[25] | Cross-sectional, Italy, 2014. | N = 131. All subjects with MS. | The study examined factors that may be associated with the evolution of MS. There was no significant correlation between cigarette smoking status or exposure to SHS and the severity of MS. | (I) Small sample size study. (II) Recall bias may be present, as subjects were asked about their past experience and habits. (III) Not possible to distinguish patients exposed to SHS as current smokers, ex-smokers, or never-smokers. (IV) The study only considered the exposure to SHS 12 months prior to data collection. |
| Ramagopalan et al.[26] | Case-control, Canada, 2013. | N = 3,913. MS cases: 3,157. Controls (spouses): 756. | MS cases and spouses were asked about cigarette smoking and SHS exposure. There was no correlation between SHS and MS in never-smoking patients. Exposure to SHS at home presented an OR of 0.87, whereas at the workplace the OR was 0.99. | (I) Recall bias may be present, as subjects were asked about their experience and habits. (II) No quantitative data on SHS amounts. (III) Small control sample, possibly underpowered to detect relevant effects. (IV) Authors considered SHS exposure only in the workplace or at home and did not consider the experience in other places, for example while outdoors. (V) The study did not collect information on paternal smoking. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



